Occupational & Environmental Medicine
Workplace injury management, workers' compensation, occupational lung disease, toxicant exposure, ergonomics, fitness-for-duty evaluation, DOT physicals, and every regulatory standard, screening protocol, and return-to-work algorithm across the full scope of occupational and environmental medicine.
01 Occupational Health Framework
Scope of Practice
Occupational and environmental medicine (OEM) is the medical specialty devoted to the prevention, evaluation, treatment, and management of illness and injury arising from workplace or environmental exposures. The OEM physician serves as the interface between clinical medicine, public health, regulatory compliance, and the employer-employee relationship. Core activities include hazard identification, medical surveillance, fitness-for-duty evaluation, impairment and disability assessment, workers' compensation management, toxicology consultation, and return-to-work facilitation.
Hierarchy of Controls — Prevention Framework
The fundamental strategy for protecting workers from occupational hazards follows the hierarchy of controls, ranked from most to least effective. Higher-order controls are preferred because they do not depend on worker behavior.
| Level | Control Type | Description | Example |
|---|---|---|---|
| 1 (Most Effective) | Elimination | Physically remove the hazard entirely | Discontinue use of a carcinogenic chemical; automate a dangerous task |
| 2 | Substitution | Replace the hazard with something less dangerous | Use water-based paint instead of solvent-based; substitute toluene for benzene |
| 3 | Engineering Controls | Isolate workers from the hazard via physical means | Local exhaust ventilation, machine guarding, sound-dampening enclosures |
| 4 | Administrative Controls | Change the way people work | Job rotation, work-rest schedules, training, signage, standard operating procedures |
| 5 (Least Effective) | Personal Protective Equipment (PPE) | Protect the worker with wearable equipment | Respirators, gloves, hearing protection, safety glasses, steel-toed boots |
Occupational vs. Non-Occupational Disease — Causation Criteria
Determining whether a condition is occupational (work-related) or non-occupational requires systematic analysis. The physician should apply a structured causation framework using the following criteria:
| Criterion | Assessment Question | Example |
|---|---|---|
| Biologic plausibility | Is this condition known to be caused by this exposure? | Asbestosis from asbestos inhalation — well-established causal link |
| Temporal relationship | Did exposure precede disease onset by an appropriate interval? | Mesothelioma diagnosed 30 years after shipyard work — consistent latency |
| Dose-response | Was the magnitude and duration of exposure sufficient? | CWP in miner with 25 years underground — adequate dose |
| Consistency | Is the finding consistent with epidemiologic studies of similarly exposed workers? | Occupational asthma in a baker exposed to flour dust — consistent with population data |
| Exclusion of alternatives | Have non-occupational causes been considered and their contribution assessed? | Hearing loss — noise exposure vs. presbycusis vs. ototoxic medications |
For workers' compensation purposes, the standard of proof is typically "more probable than not" (>50% likelihood), not the scientific standard of 95% confidence. This lower standard means that a physician can opine that a condition is "more likely than not" work-related even when certainty is impossible.
Workers' Compensation — No-Fault System
Workers' compensation is a state-mandated, no-fault insurance system in which employers provide medical care and wage replacement for employees who sustain work-related injuries or illnesses, regardless of fault. In exchange, employees generally forfeit the right to sue employers for negligence (the exclusive remedy doctrine). Key components include:
- First Report of Injury (FROI) — employer files with the workers' compensation carrier within a state-specified timeframe (commonly 24-72 hours).
- Authorized treating physician — rules vary by state; some allow employee choice, others require employer-designated physician panels.
- Benefits — medical treatment (no copays/deductibles), temporary total disability (TTD), temporary partial disability (TPD), permanent partial disability (PPD), permanent total disability (PTD), vocational rehabilitation, death benefits.
- Independent Medical Examination (IME) — performed at the request of the carrier or employer to evaluate diagnosis, causation, treatment, or impairment; the examiner has no treatment relationship with the patient.
Fitness-for-Duty Evaluation
A fitness-for-duty (FFD) evaluation determines whether an employee can safely and effectively perform the essential functions of their job, with or without accommodation. FFD evaluations may be triggered by: observed impairment or unsafe behavior, return from medical leave, regulatory requirements (DOT, safety-sensitive positions), or employer concern about an employee's ability to work safely. The FFD examiner must review the specific job demands (physical, cognitive, sensory), the employee's medical condition and treatment status, the safety risks posed to the employee and others, and any applicable regulatory standards. The report should address only work-related functional capacity — not the underlying diagnosis (to comply with ADA confidentiality requirements). FFD evaluations differ from IMEs in that they focus on prospective safety and function rather than retrospective causation or impairment rating.
Pre-Placement Evaluation
A pre-placement evaluation (formerly "pre-employment physical") occurs after a conditional offer of employment to determine whether the individual can safely perform the essential functions of the job. Under the ADA, medical examinations may not be conducted before a conditional job offer, and the results may only be used to exclude the applicant if the condition poses a direct threat to safety that cannot be eliminated by reasonable accommodation. Pre-placement evaluations also establish medical baselines (hearing, pulmonary function, physical capacity) for future surveillance comparison. They are distinct from substance abuse screening (which may occur pre-offer in DOT-regulated positions).
OSHA Overview
The Occupational Safety and Health Administration (OSHA) was established by the Occupational Safety and Health Act of 1970 to ensure safe and healthful working conditions. Key principles:
- General Duty Clause (Section 5(a)(1)) — requires employers to provide a workplace "free from recognized hazards that are causing or are likely to cause death or serious physical harm." This clause can be cited even when no specific standard exists.
- Right to Know (Hazard Communication Standard, 29 CFR 1910.1200) — workers have the right to information about hazardous chemicals in the workplace, including access to Safety Data Sheets (SDS), proper labeling, and training.
- NIOSH — the National Institute for Occupational Safety and Health (part of CDC) is the research arm; it develops recommended exposure limits (RELs) and conducts Health Hazard Evaluations (HHE). OSHA (part of Department of Labor) is the enforcement arm.
OSHA — federal enforcement agency; sets legally enforceable Permissible Exposure Limits (PELs). NIOSH — federal research agency; publishes Recommended Exposure Limits (RELs), generally more protective than PELs. ACGIH — private professional organization; publishes Threshold Limit Values (TLVs) based on current science, updated annually, not legally enforceable but widely considered the gold standard. Many OSHA PELs have not been updated since 1971 and may be less protective than current ACGIH TLVs.
02 Exposure Assessment & Industrial Hygiene
Occupational Exposure Limits (OELs)
OELs are airborne concentration limits below which nearly all workers can be repeatedly exposed without adverse health effects. The three major systems are:
| Limit | Setting Body | Legal Status | Update Frequency | Notes |
|---|---|---|---|---|
| PEL (Permissible Exposure Limit) | OSHA | Legally enforceable | Rarely updated (many from 1971) | 8-hr TWA; some have ceiling/STEL |
| TLV (Threshold Limit Value) | ACGIH | Not enforceable; advisory | Annually reviewed | TWA, STEL, and Ceiling values |
| REL (Recommended Exposure Limit) | NIOSH | Not enforceable; advisory | Periodically | Often 10-hr TWA (for NIOSH work schedule) |
| IDLH | NIOSH | Not enforceable | Periodically | Immediately Dangerous to Life or Health — triggers SCBA use |
TWA (Time-Weighted Average) — the average airborne concentration over an 8-hour workday (OSHA/ACGIH) or 10-hour day (NIOSH). STEL (Short-Term Exposure Limit) — a 15-minute TWA not to be exceeded at any time during the workday, even if the 8-hour TWA is within limits. Ceiling (C) — an instantaneous concentration that must never be exceeded. The hierarchy: Ceiling > STEL > TWA.
Safety Data Sheets (SDS) — GHS Format
The Globally Harmonized System (GHS) standardizes chemical hazard communication. Every SDS follows a mandatory 16-section format:
| Section | Content | Section | Content |
|---|---|---|---|
| 1 | Identification | 9 | Physical & chemical properties |
| 2 | Hazard identification (GHS pictograms) | 10 | Stability & reactivity |
| 3 | Composition / ingredients | 11 | Toxicological information |
| 4 | First-aid measures | 12 | Ecological information |
| 5 | Fire-fighting measures | 13 | Disposal considerations |
| 6 | Accidental release measures | 14 | Transport information |
| 7 | Handling & storage | 15 | Regulatory information |
| 8 | Exposure controls / PPE | 16 | Other information |
Exposure Monitoring
Area monitoring measures ambient concentrations at fixed locations within the workplace — useful for identifying exposure zones but does not reflect individual worker exposure. Personal monitoring uses sampling devices attached to the worker (typically in the breathing zone, within 30 cm of the nose and mouth) and provides the most accurate estimate of actual inhalation exposure. Results are reported as 8-hour TWA concentrations and compared against applicable OELs.
Biological Exposure Indices (BEI)
BEIs are reference values established by ACGIH for biological monitoring — measurement of a substance or its metabolite in blood, urine, or exhaled air. BEIs represent the levels expected in specimens collected from healthy workers exposed at the TLV. Examples: blood lead level for lead exposure, urinary phenol for benzene, carboxyhemoglobin for CO, urinary mercury for inorganic mercury. BEIs account for all routes of absorption (inhalation, dermal, ingestion), unlike air monitoring which captures only inhalation exposure.
Common Biological Monitoring Parameters
| Exposure | Biological Marker | Specimen | Timing of Collection | BEI Value |
|---|---|---|---|---|
| Lead | Blood lead level (BLL) | Whole blood | Any time (not timing-critical) | 20 mcg/dL |
| Mercury (inorganic) | Urine mercury | Urine (pre-shift) | End of shift, end of workweek | 35 mcg/g creatinine |
| Cadmium | Blood cadmium; urine cadmium | Blood; urine | Not critical (long half-life) | Blood: 5 mcg/L; Urine: 5 mcg/g Cr |
| Carbon monoxide | Carboxyhemoglobin (COHb) | Whole blood | End of shift | 3.5% COHb |
| Toluene | Urinary o-cresol; blood toluene | Urine; blood | End of shift | 0.3 mg/L o-cresol; 0.02 mg/L blood toluene |
| n-Hexane | Urinary 2,5-hexanedione | Urine | End of shift | 0.4 mg/L |
| Benzene | Urinary S-phenylmercapturic acid (S-PMA) | Urine | End of shift | 25 mcg/g creatinine |
| Arsenic (inorganic) | Urinary inorganic arsenic + metabolites | Urine | End of workweek | 35 mcg/L |
Quantitative Fit Testing
Respirators must form a tight seal against the face. Quantitative fit testing uses instrumentation (e.g., PortaCount) to measure the ratio of ambient particle concentration outside the respirator to that inside — the fit factor. For half-face respirators, the minimum passing fit factor is 100; for full-face respirators, 500. Qualitative fit testing uses a challenge agent (saccharin for sweet taste, Bitrex for bitter, irritant smoke, or isoamyl acetate for banana odor) and relies on the wearer's subjective detection — pass/fail only.
03 Terminology & Abbreviations
| Term | Definition |
|---|---|
| Hazard | An inherent property of an agent or situation capable of causing harm (e.g., a chemical is toxic, a machine has moving parts) |
| Risk | The probability that exposure to a hazard will result in harm — a function of hazard, exposure, and vulnerability |
| Sentinel health event (occupational) | A disease, disability, or death whose occurrence may provide the impetus for prevention (e.g., mesothelioma signals asbestos exposure) |
| Latency period | Time between first exposure and clinical disease manifestation — days for irritants, decades for cancers |
| Dose-response relationship | The correlation between magnitude/duration of exposure and severity/probability of health effect |
| Total Worker Health (TWH) | NIOSH initiative integrating occupational safety/health protection with health promotion to advance worker well-being |
| Ergonomics | The science of fitting the job to the worker — designing tasks, tools, and workstations to reduce injury risk |
| Toxicant | A substance that is toxic; distinguished from "toxin" (naturally occurring biological poison) |
| Bioaccumulation | Progressive accumulation of a substance in an organism over time (e.g., lead in bone, cadmium in kidney) |
| Medical removal protection (MRP) | OSHA provision requiring employers to maintain earnings and benefits for workers removed from exposure due to elevated biological levels (e.g., lead standard) |
OSHA — Occupational Safety & Health Administration. NIOSH — National Institute for Occupational Safety & Health. ACGIH — American Conference of Governmental Industrial Hygienists. PEL — Permissible Exposure Limit. TLV — Threshold Limit Value. REL — Recommended Exposure Limit. TWA — Time-Weighted Average. STEL — Short-Term Exposure Limit. SDS — Safety Data Sheet. BEI — Biological Exposure Index. PPE — Personal Protective Equipment. IDLH — Immediately Dangerous to Life or Health. MMI — Maximum Medical Improvement. FCE — Functional Capacity Evaluation. IME — Independent Medical Examination. DOT — Department of Transportation. FMCSA — Federal Motor Carrier Safety Administration. MRO — Medical Review Officer. SAP — Substance Abuse Professional.
04 Pneumoconioses
The pneumoconioses are a group of interstitial lung diseases caused by inhalation of certain dusts and the lung tissue's reaction to that dust. They are characterized by long latency periods, irreversibility, and the critical importance of exposure history for diagnosis.
Asbestosis
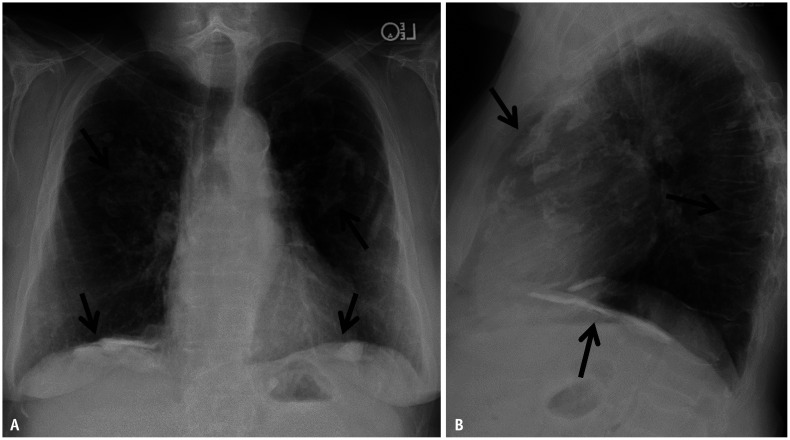
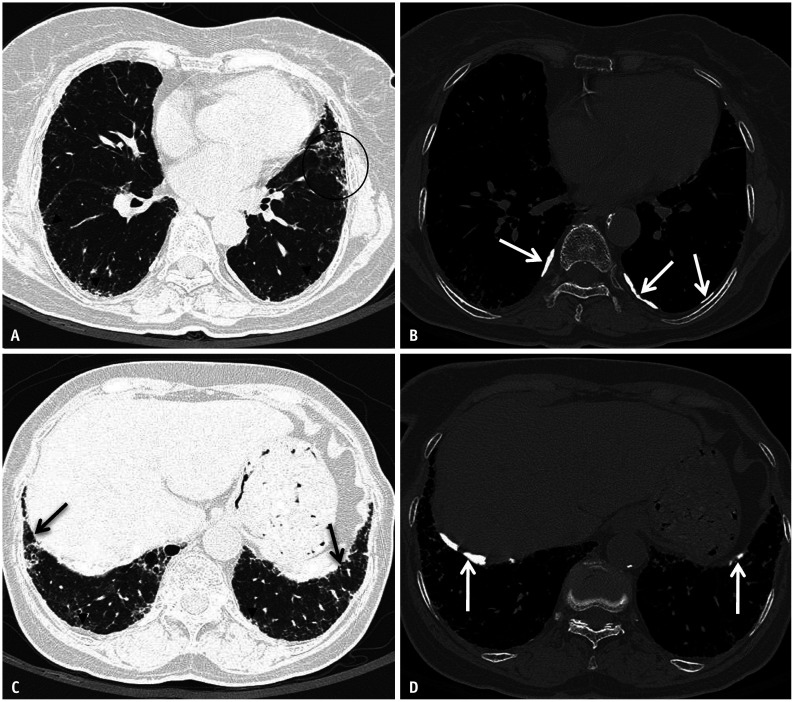
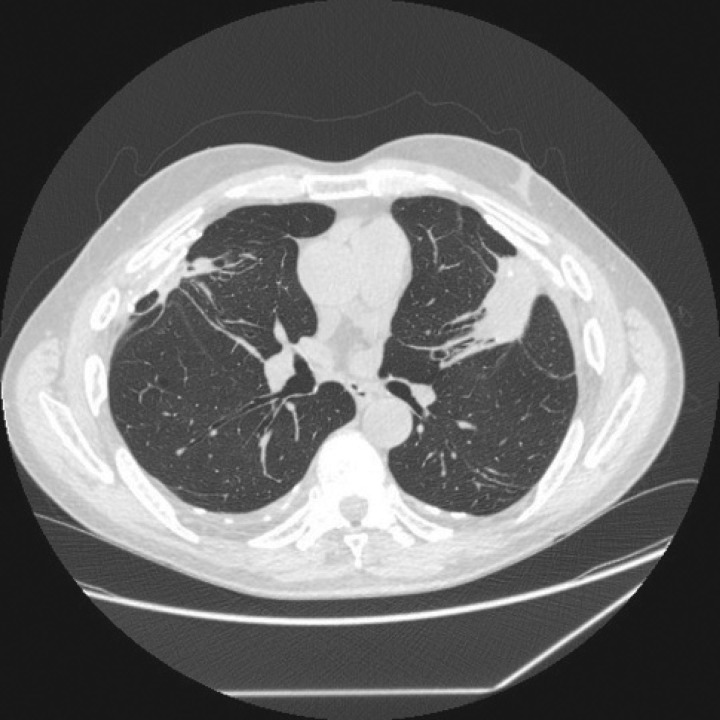
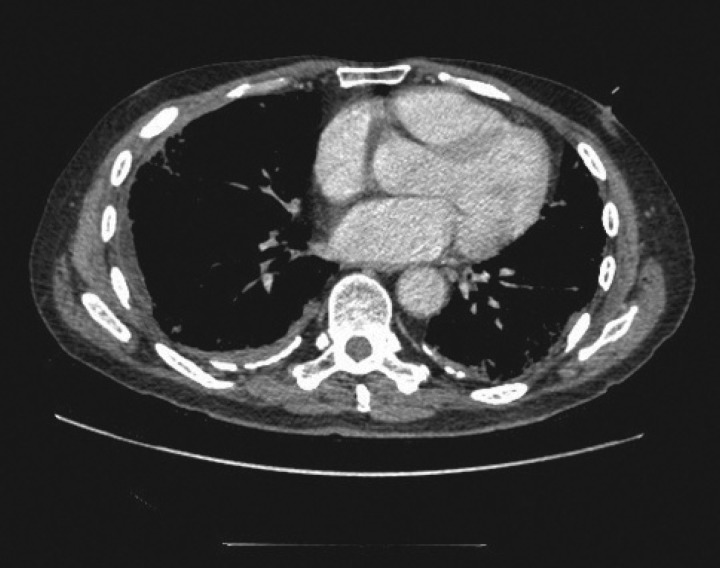
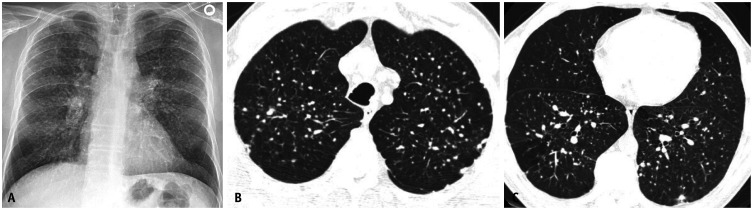
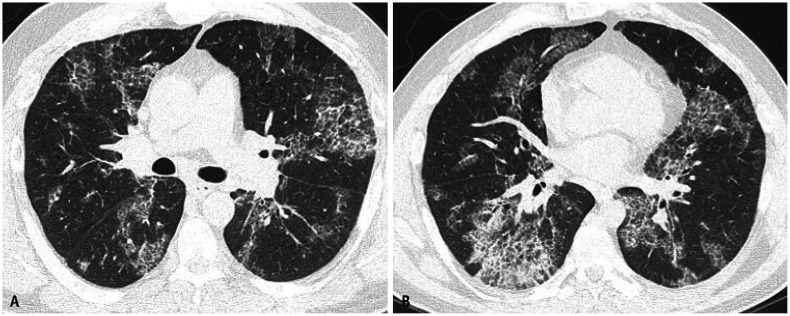
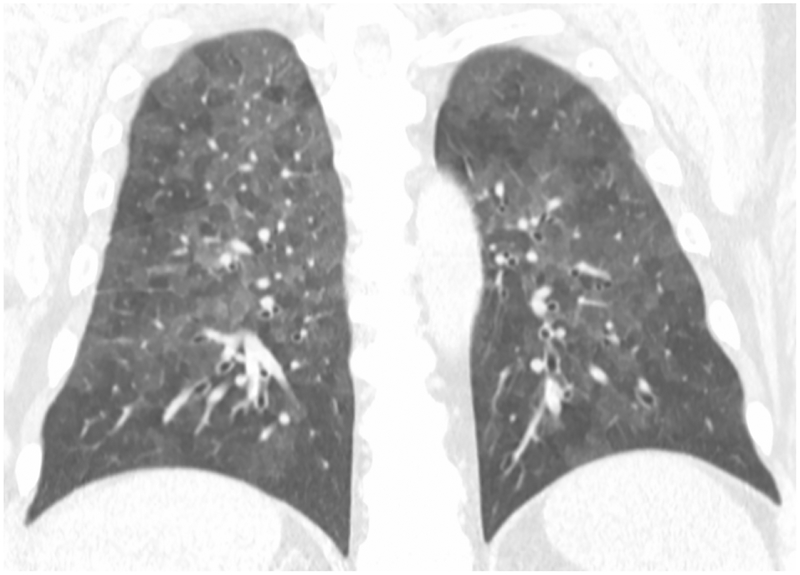
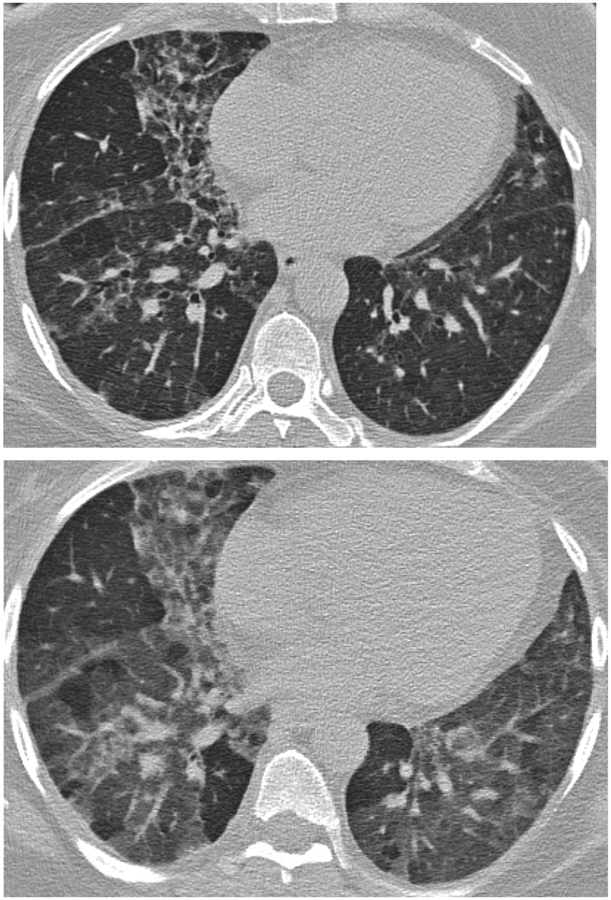
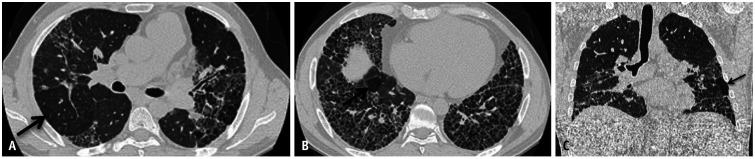
Asbestosis is diffuse interstitial pulmonary fibrosis caused by inhalation of asbestos fibers. Occupations at risk include insulation workers, shipbuilders, construction/demolition workers, brake mechanics, and pipefitters. The latency period is typically 15-20 years from first exposure. Pathologically, asbestos bodies (golden-brown, dumbbell-shaped ferruginous bodies — asbestos fibers coated with iron-containing protein) are characteristic. Imaging reveals bilateral lower lobe interstitial fibrosis with honeycombing in advanced disease. Pleural plaques (bilateral, calcified, diaphragmatic) are the hallmark of asbestos exposure — they are benign markers of exposure, not asbestosis itself, and do not cause symptoms or require treatment. PFTs show a restrictive pattern with decreased DLCO.

Silicosis
Silicosis is caused by inhalation of crystalline silica (quartz). High-risk occupations include sandblasting, mining, quarrying, stone cutting, tunneling, and foundry work. Three clinical forms exist:
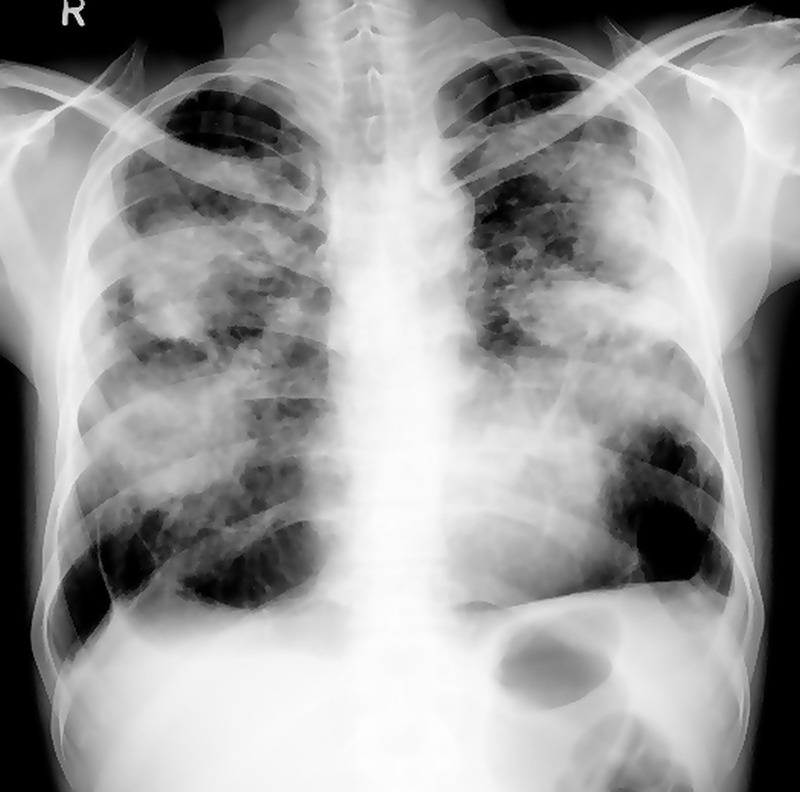
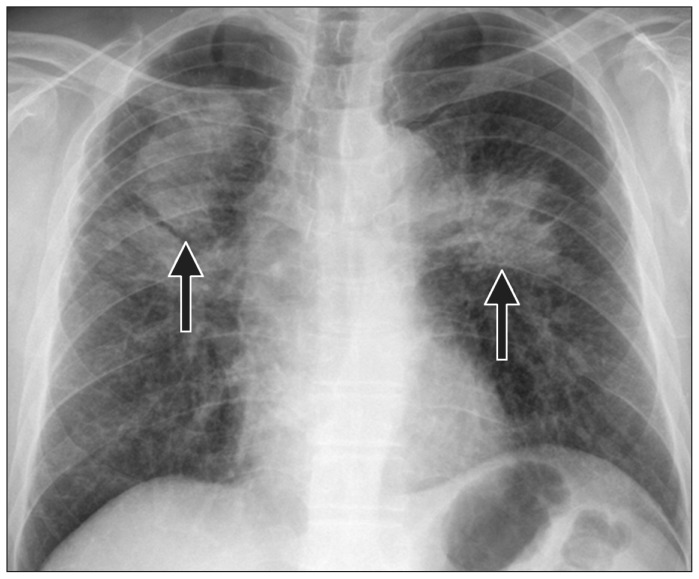
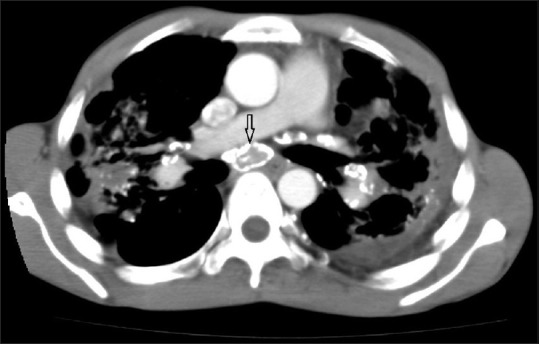
- Chronic (classic) silicosis — develops after 10-30 years of moderate exposure. CXR shows bilateral upper lobe nodular opacities (1-10 mm), often with "eggshell" calcification of hilar lymph nodes. PFTs may show obstruction, restriction, or mixed pattern.
- Accelerated silicosis — occurs 5-10 years after higher-intensity exposure. Clinically and radiographically similar to chronic form but progresses more rapidly.
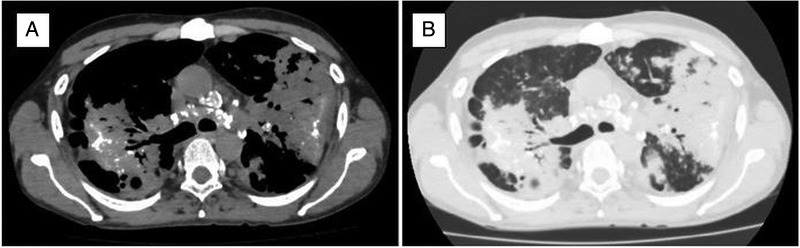
- Acute silicosis (silicoproteinosis) — develops within weeks to a few years after massive silica exposure. Pathologically identical to pulmonary alveolar proteinosis (PAP). CXR shows diffuse alveolar filling pattern. Rapidly fatal.
Progressive massive fibrosis (PMF) — also called complicated silicosis — develops when silicotic nodules coalesce into large masses (>1 cm), typically in the upper lobes. PMF is associated with severe and progressive respiratory impairment even after exposure ceases. Silicosis is also associated with increased susceptibility to tuberculosis (silicotuberculosis) due to impaired macrophage function — all silicosis patients should undergo TB screening.
Coal Workers' Pneumoconiosis (CWP)
Simple CWP manifests as small round opacities on CXR, predominantly in the upper lobes. Workers are typically asymptomatic or mildly symptomatic, and PFTs may be normal. Complicated CWP (PMF) involves coalescence into large opacities (>1 cm), with progressive dyspnea, cough, and restrictive or mixed PFT pattern. Caplan syndrome is the association of CWP (or other pneumoconiosis) with rheumatoid arthritis, manifesting as multiple well-defined peripheral lung nodules (rheumatoid pneumoconiosis).
Berylliosis (Chronic Beryllium Disease)
Chronic beryllium disease (CBD) is a granulomatous lung disease caused by sensitization to beryllium, found in aerospace, electronics, nuclear, and dental alloy industries. Unlike other pneumoconioses, CBD is an immune-mediated (type IV hypersensitivity) disease, not a dust-deposition disease — it can occur even with low-level exposure. It is clinically, radiographically, and histologically indistinguishable from sarcoidosis (noncaseating granulomas, bilateral hilar lymphadenopathy, restrictive PFTs with reduced DLCO). The distinguishing test is the beryllium lymphocyte proliferation test (BeLPT) — a blood test demonstrating sensitization to beryllium. Two abnormal BeLPTs or one abnormal BeLPT plus granulomas on biopsy confirms the diagnosis.

Asbestos-Related Malignancies
Mesothelioma — a malignancy of the pleura (or less commonly peritoneum) that is virtually pathognomonic for asbestos exposure. Latency is 20-40 years. There is no safe threshold of exposure. Mesothelioma risk is not increased by smoking. Prognosis is poor (median survival 12-18 months). Lung cancer — asbestos exposure independently increases lung cancer risk, and the risk is multiplicative (not merely additive) when combined with smoking (asbestos x smoking = 50-90 fold increased risk vs. 5 fold for asbestos alone and 10 fold for smoking alone). Benign pleural effusion — the earliest manifestation of asbestos-related disease, may occur within 10 years of exposure; exudative, often bloody; diagnosis of exclusion after ruling out malignancy.
| Pneumoconiosis | Causative Agent | Key Radiographic Finding | Distribution | Special Features |
|---|---|---|---|---|
| Asbestosis | Asbestos fibers | Interstitial fibrosis, pleural plaques | Lower lobes | Mesothelioma risk; multiplicative with smoking for lung CA |
| Silicosis | Crystalline silica | Nodular opacities, eggshell calcification | Upper lobes | TB susceptibility; PMF; autoimmune associations |
| CWP | Coal dust | Small round opacities; PMF | Upper lobes | Caplan syndrome (with RA) |
| Berylliosis | Beryllium | Hilar adenopathy, reticular opacities | Diffuse | Mimics sarcoidosis; BeLPT diagnostic |
| Siderosis | Iron oxide | Dense nodules (radio-opaque) | Diffuse | Benign; no fibrosis; "arc welder's lung" |
| Stannosis | Tin oxide | Dense nodules | Diffuse | Benign; no fibrosis |
| Byssinosis | Cotton/flax/hemp dust | Normal early; later COPD pattern | Diffuse | "Monday fever" — symptoms worst after weekend away |
05 Occupational Asthma
Occupational asthma (OA) is the most common occupational lung disease in industrialized countries. It is defined as variable airflow limitation and airway hyperresponsiveness caused by conditions attributable to a particular occupational environment. Two major categories exist:
Sensitizer-Induced Occupational Asthma
Results from immunologic sensitization to a workplace agent after a latency period (weeks to years). Once sensitized, even very low-level re-exposure triggers bronchoconstriction. Common sensitizers include:
- Diisocyanates (TDI, MDI, HDI) — the most common cause worldwide; found in polyurethane production, spray painting, insulation
- Flour/grain dust — "baker's asthma"; the most common cause in the UK
- Natural rubber latex — healthcare workers, rubber manufacturing
- Wood dust — western red cedar (plicatic acid), oak, mahogany; woodworkers, carpenters
- Laboratory animal allergens — rat, mouse urinary proteins; research workers
- Platinum salts — refinery workers
Irritant-Induced Occupational Asthma (RADS)
Reactive Airways Dysfunction Syndrome (RADS) is a non-immunologic form of occupational asthma that develops within 24 hours of a single high-level irritant exposure (e.g., chlorine gas leak, ammonia spill, acid splash). There is no latency period and no prior sensitization. Diagnosis requires: (1) absence of pre-existing respiratory disease; (2) onset after a single high-concentration irritant exposure; (3) onset within 24 hours; (4) persistence of symptoms for at least 3 months; (5) airflow obstruction and/or nonspecific bronchial hyperresponsiveness on testing.
Work-Exacerbated Asthma vs. Occupational Asthma
Work-exacerbated asthma (WEA) is pre-existing or concurrent asthma that is worsened by workplace conditions (dust, fumes, cold air, exercise, irritants) but is NOT caused by a specific workplace sensitizer. WEA accounts for approximately 20% of working adults with asthma. Unlike true occupational asthma, WEA does not require complete removal from the workplace — environmental modifications and optimized asthma therapy are usually sufficient. Distinguishing WEA from OA is clinically important: OA requires removal from the causative agent, whereas WEA requires exposure reduction and better asthma control. A detailed chronological history (Was asthma present before this job? Did symptoms begin or change character after starting this job?) is the key differentiator.
Diagnosis
Diagnosis of occupational asthma requires establishing both the presence of asthma and its work-relatedness:
- Serial peak expiratory flow (PEF) monitoring — the worker measures PEF at least 4 times daily for 2-4 weeks at work and 2-4 weeks away from work. A work-related pattern (decline during work periods, improvement away) supports OA. Sensitivity ~70%, specificity ~85%.
- Methacholine challenge testing — demonstrates nonspecific bronchial hyperresponsiveness. More useful when done at end of work exposure vs. after a period away — a shift in PC20 supports OA.
- Specific inhalation challenge (SIC) — the gold standard but available only in specialized centers. The worker is exposed to the suspected agent under controlled laboratory conditions while monitoring FEV1.
- Immunologic tests — skin prick testing or specific IgE for high-molecular-weight agents (proteins); less useful for low-molecular-weight chemicals (diisocyanates).
Early removal from exposure is the single most important prognostic factor in occupational asthma. Workers removed from exposure within 1 year of symptom onset have significantly better outcomes. Continued exposure leads to progressive, irreversible airway remodeling. Reducing (but not eliminating) exposure provides only partial benefit — complete avoidance is preferred. Even after complete removal, up to 70% of workers continue to have persistent asthma symptoms, though severity typically decreases.
06 Hypersensitivity Pneumonitis
Hypersensitivity pneumonitis (HP), also known as extrinsic allergic alveolitis, is a complex immune-mediated (type III and IV hypersensitivity) inflammatory lung disease caused by repeated inhalation of organic dusts or low-molecular-weight chemicals. Occupational HP is among the most important of the occupational interstitial lung diseases.
Common Causes of Occupational HP
| Disease Name | Antigen Source | Specific Organism/Antigen | Exposed Workers |
|---|---|---|---|
| Farmer's lung | Moldy hay/grain | Saccharopolyspora rectivirgula, Thermoactinomyces vulgaris | Farmers, grain handlers |
| Bird fancier's lung | Avian droppings/feathers | Avian serum proteins, feather bloom | Pigeon breeders, poultry workers |
| Hot tub lung | Aerosolized water | Mycobacterium avium complex (MAC) | Hot tub users/maintenance |
| Mushroom worker's lung | Mushroom compost | Thermoactinomyces spp. | Mushroom cultivators |
| Malt worker's lung | Contaminated malt/barley | Aspergillus clavatus | Brewery workers |
| Machine worker's HP | Metalworking fluids | Mycobacterium immunogenum | Machinists |
| Chemical worker's HP | Diisocyanates, trimellitic anhydride | Chemical hapten | Chemical/paint workers |
Clinical Presentations
Acute HP — onset 4-8 hours after heavy antigen exposure. Fever, chills, malaise, cough, dyspnea. Resolves within 24-48 hours of antigen avoidance. Often misdiagnosed as recurrent pneumonia or influenza. Subacute HP — insidious onset over weeks to months with continued lower-level exposure. Progressive cough, dyspnea, fatigue, anorexia, weight loss. Chronic HP — progressive fibrotic lung disease from prolonged exposure. May be indistinguishable from IPF/UIP on imaging and histology. Carries a worse prognosis; may progress even after antigen removal.
Diagnosis
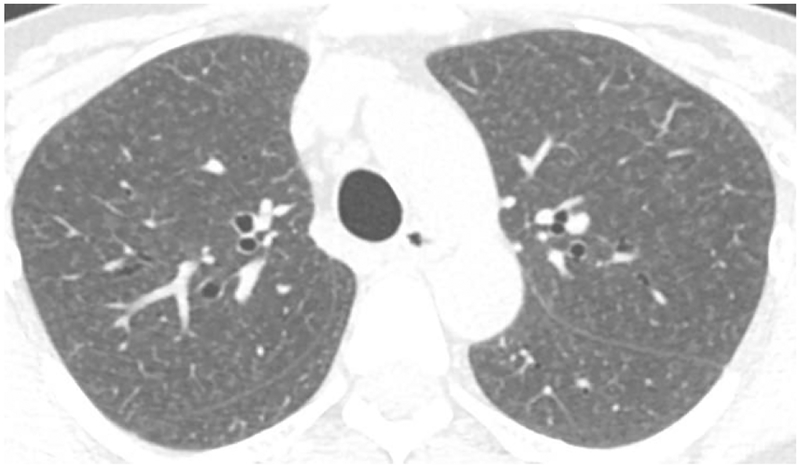
No single test is diagnostic. Diagnosis rests on a combination of: (1) compatible exposure history; (2) appropriate symptom latency and temporal pattern; (3) HRCT — acute/subacute: diffuse ground-glass opacities, centrilobular nodules, mosaic attenuation (air trapping); chronic: fibrosis with traction bronchiectasis; (4) BAL lymphocytosis — typically >40% lymphocytes (vs. <15% in IPF); (5) serum precipitins (IgG antibodies to suspected antigen) — indicate exposure/sensitization but not necessarily disease; (6) lung biopsy when needed — poorly formed granulomas, giant cells, peribronchiolar lymphocytic infiltrate.
Treatment
Antigen avoidance is the cornerstone of therapy and the only intervention that alters disease progression. Environmental remediation (improved ventilation, mold remediation) may be sufficient in some cases. Corticosteroids (prednisone 0.5-1 mg/kg/day, tapered over weeks to months) accelerate recovery in acute/subacute HP but do not prevent progression if exposure continues. There is no role for immunosuppressive agents in acute/subacute HP. Chronic fibrotic HP may require treatment analogous to IPF (antifibrotics — nintedanib has shown benefit in progressive fibrosing HP).
07 Occupational Cancer
Occupational cancers account for an estimated 4-10% of all cancers. Key features include long latency periods (typically 10-40 years), dose-response relationships, and the existence of well-established agent-cancer associations classified by the International Agency for Research on Cancer (IARC).
IARC Group 1 Carcinogens — Occupational Exposures
| Agent | Target Organ(s) | Exposed Workers | Latency |
|---|---|---|---|
| Asbestos | Lung, pleura (mesothelioma), larynx, ovary | Construction, insulation, shipbuilding | 15-40 yrs |
| Benzene | Bone marrow (AML, aplastic anemia, MDS) | Petroleum, rubber, chemical, shoe manufacturing | 5-15 yrs |
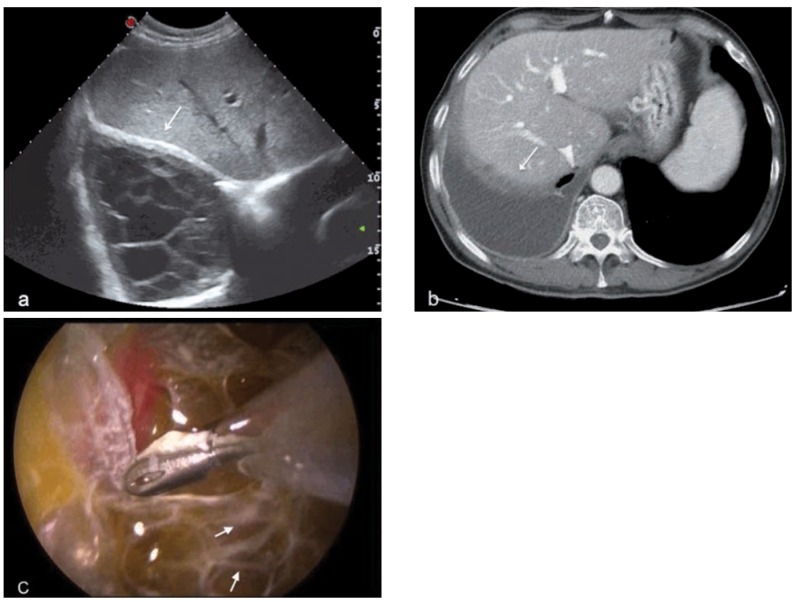
| Vinyl chloride | Liver (hepatic angiosarcoma) | PVC manufacturing | 15-30 yrs |
| Chromium VI | Lung, nasal sinuses | Welding, chrome plating, pigment production | 10-25 yrs |
| Arsenic (inorganic) | Lung, skin, bladder | Smelting, pesticide manufacturing, semiconductor | 15-40 yrs |
| Radon | Lung | Underground mining (uranium) | 10-30 yrs |
| Crystalline silica | Lung | Mining, sandblasting, quarrying | 15-30 yrs |
| Nickel compounds | Lung, nasal sinuses | Nickel refining, welding, battery manufacturing | 15-30 yrs |
| Cadmium | Lung | Battery production, smelting, electroplating | 10-25 yrs |
| Formaldehyde | Nasopharynx, leukemia (myeloid) | Funeral industry, lab workers, composite wood | 10-20 yrs |
| Bis(chloromethyl) ether | Lung (small cell) | Chemical manufacturing | 10-20 yrs |
| Beta-naphthylamine | Bladder (urothelial) | Dye/rubber industry (historical) | 15-30 yrs |
| Wood dust | Nasal cavity/sinuses (adenocarcinoma) | Woodworkers, furniture makers | 20-40 yrs |
Mesothelioma is virtually pathognomonic for asbestos exposure — >80% of cases have a documented exposure history. There is no threshold dose, and even brief or low-level exposures carry risk. Unlike lung cancer, mesothelioma risk is NOT increased by smoking. Median latency is 30-40 years. All histologic subtypes (epithelioid, sarcomatoid, biphasic) carry a poor prognosis, though epithelioid has the best survival. Immunohistochemistry (calretinin+, WT-1+, CK5/6+, CEA-, TTF-1-) distinguishes mesothelioma from adenocarcinoma.
Principles of Occupational Cancer Prevention
Prevention follows the hierarchy of controls applied specifically to carcinogenic exposures:
- Elimination/substitution — replace carcinogenic agents with non-carcinogenic alternatives where feasible (e.g., substitute benzene with toluene or cyclohexane).
- Engineering controls — closed systems for handling carcinogens, local exhaust ventilation at emission points, wet methods to suppress dust generation (silica, asbestos abatement).
- Administrative controls — limit the number of workers exposed, rotate workers to reduce individual cumulative exposure, establish regulated areas with restricted access and warning signage.
- Medical surveillance — substance-specific OSHA surveillance programs detect early effects (e.g., CBC changes with benzene, elevated urinary cadmium with cadmium) before clinical cancer develops.
- Exposure records — maintain 30-year exposure records (required by OSHA for many carcinogens) to enable future epidemiologic analysis and individual risk assessment.
Screening Recommendations
LDCT lung cancer screening follows USPSTF guidelines (annually for adults 50-80 years with a 20 pack-year smoking history who currently smoke or quit within 15 years). For asbestos-exposed workers, many occupational medicine programs offer LDCT screening even without smoking history, though formal guidelines for this population remain evolving. For benzene-exposed workers, periodic CBC with differential monitors for cytopenias. For vinyl chloride workers, liver ultrasound and AFP have been used for angiosarcoma screening, though sensitivity is limited.
The long latency of occupational cancers (often 15-40 years) means that disease may not appear until years after exposure has ceased, even after retirement. The healthy worker effect is a well-documented epidemiologic bias in which employed populations show lower overall mortality than the general population — because the severely ill and disabled are selected out of the workforce. This bias can mask true occupational cancer risk in cross-sectional studies. Proper epidemiologic study design (cohort studies with appropriate reference populations, lagged exposure analyses) is essential for accurately estimating occupational cancer risk.
08 Work-Related Musculoskeletal Disorders
Work-related musculoskeletal disorders (WMSDs) are the most common category of occupational injury and the leading cause of disability and workers' compensation claims. Low back pain is the single most common claim; carpal tunnel syndrome is the most common peripheral nerve entrapment.
Ergonomic Risk Factors
Five primary biomechanical risk factors contribute to WMSD development: (1) Force — the physical effort required (heavy lifting, forceful gripping); (2) Repetition — performing the same or similar motions repeatedly; (3) Posture — awkward or sustained positions (overhead work, prolonged wrist flexion/extension); (4) Vibration — hand-arm (power tools) or whole-body (driving, heavy equipment); (5) Contact stress — localized pressure on nerves or tendons (resting wrists on sharp desk edges). Duration of exposure, inadequate recovery time, and cold temperatures are amplifying factors.
Common Work-Related Musculoskeletal Conditions
| Condition | Affected Structure | Risk Factors | Diagnosis | Key Points |
|---|---|---|---|---|
| Carpal Tunnel Syndrome | Median nerve at wrist | Repetitive wrist motion, forceful gripping, vibration | Nerve conduction studies / EMG (gold standard); Phalen, Tinel | Most common occupational peripheral neuropathy; nocturnal symptoms classic |
| Lateral epicondylitis | Common extensor origin | Repetitive wrist extension, gripping | Clinical — pain at lateral epicondyle with resisted wrist extension | "Tennis elbow"; common in assembly workers |
| De Quervain tenosynovitis | APL/EPB tendons at radial styloid | Repetitive thumb motion, pinching | Finkelstein test positive | Common in assembly, packaging workers |
| Rotator cuff tendinopathy | Supraspinatus most common | Overhead work, repetitive shoulder motion | Impingement tests; MRI for tears | Painter, electrician, plumber overhead work |
| Low back pain/strain | Lumbar muscles, discs, facets | Heavy lifting, bending, twisting, whole-body vibration | Primarily clinical; imaging for red flags | Most common workers' comp claim overall |
| Trigger finger | Flexor tendon / A1 pulley | Repetitive gripping | Clinical — catching/locking of digit | Common in power tool operators |
NIOSH Lifting Equation
The NIOSH Revised Lifting Equation (1991) calculates a Recommended Weight Limit (RWL) for a two-handed manual lifting task. The formula: RWL = LC x HM x VM x DM x AM x FM x CM, where LC = load constant (23 kg / 51 lb), and multipliers account for Horizontal distance, Vertical height, Distance of lift, Asymmetry angle, Frequency, and Coupling quality. The Lifting Index (LI) = actual weight / RWL. An LI >1.0 indicates the task poses increased risk for low back injury. An LI >3.0 indicates a substantially increased risk and warrants immediate intervention.
Occupational Low Back Pain — Clinical Management
Acute occupational low back pain (onset within the past 4 weeks) is managed according to evidence-based guidelines emphasizing early activity, functional restoration, and avoidance of unnecessary imaging or interventions. Initial management includes:
- Activity modification, not bed rest — prolonged bed rest (>1-2 days) is harmful and delays recovery. Early return to modified duties is recommended.
- Pharmacotherapy — first-line: NSAIDs (ibuprofen 400-600 mg TID, naproxen 250-500 mg BID) and/or acetaminophen. Second-line: skeletal muscle relaxants (cyclobenzaprine 5-10 mg TID, limited to 2-3 weeks). Opioids should be avoided or used only for severe acute pain, limited to 3-7 days.
- Physical therapy — active exercise (core stabilization, McKenzie method, directional preference) is superior to passive modalities (heat, ultrasound, TENS) for promoting recovery and preventing recurrence.
- Imaging — not indicated in the first 4-6 weeks unless red flags are present. MRI findings of disc degeneration and disc bulging are present in >50% of asymptomatic adults and correlate poorly with symptoms.
Red flags requiring urgent evaluation and imaging include: cauda equina syndrome (saddle anesthesia, urinary retention, bilateral leg weakness, bowel incontinence — surgical emergency); progressive neurologic deficit (worsening weakness, foot drop); history of cancer with new back pain (metastatic disease); fever with back pain or history of IV drug use (epidural abscess, discitis, osteomyelitis); significant trauma (fall from height, motor vehicle accident — fracture); and age >50 with new-onset severe pain (pathologic fracture, malignancy).
Cumulative Trauma vs. Acute Injury
Workers' compensation distinguishes between acute traumatic injury (a specific incident — fall, struck-by event, laceration) and cumulative trauma / repetitive strain (gradual onset from repeated exposure to ergonomic risk factors). Cumulative trauma claims are more difficult to adjudicate because: onset date is ambiguous, pre-existing conditions may contribute, and the causal link between work and condition requires medical reasoning rather than witness testimony. Common cumulative trauma conditions include carpal tunnel syndrome, rotator cuff tendinopathy, lateral epicondylitis, and chronic low back pain from repetitive lifting.
09 Ergonomic Assessment & Workplace Design
Computer Workstation Ergonomics
Proper computer workstation setup reduces risk of WMSDs of the neck, shoulder, wrist, and back. Key principles:
- Monitor — top of screen at or slightly below eye level; 50-70 cm (arm's length) from eyes; tilted slightly upward; positioned directly ahead to avoid neck rotation.
- Keyboard & mouse — keyboard at elbow height or slightly below; elbows at 90-110 degrees; wrists in neutral position (not flexed, extended, or deviated); mouse at same height as keyboard and close to midline.
- Chair — seat height allowing thighs parallel to floor, feet flat; seat depth supporting full thigh without popliteal pressure; lumbar support in the curve of the lower back; armrests at elbow height to relieve shoulder load.
- Breaks — "20-20-20 rule" (every 20 minutes, look at something 20 feet away for 20 seconds); microbreaks every 30-60 minutes; alternate sitting/standing if possible.
Manual Material Handling
Beyond the NIOSH Lifting Equation, ergonomic assessment of manual handling tasks includes analysis of: pushing/pulling forces (using force gauges), carrying distances and durations, frequency of lifts per shift, team lifting requirements, and availability of mechanical aids (forklifts, hoists, conveyors, lift tables). Job redesign strategies include: reducing object weight (smaller containers), raising storage heights (eliminate floor-level lifts), providing handles/grips, using adjustable-height surfaces, and replacing manual tasks with mechanical assistance.
Hand-Arm Vibration Syndrome (HAVS)
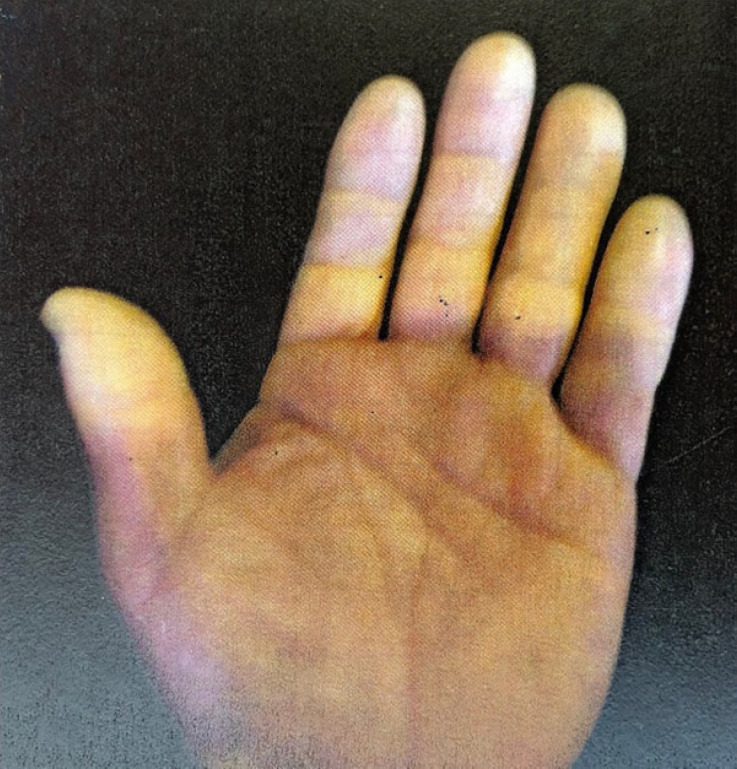
HAVS is caused by chronic use of hand-held vibrating tools (pneumatic drills, grinders, chainsaws, jackhammers). The triad includes: (1) vascular — episodic digital blanching (vibration white finger, similar to Raynaud phenomenon), typically affecting fingertips of dominant hand first; (2) neurological — numbness, tingling, reduced tactile sensitivity; (3) musculoskeletal — reduced grip strength, joint pain. The Stockholm classification grades vascular and sensorineural components separately on a 0-4 scale.

| Stockholm Vascular Stage | Description |
|---|---|
| 0 | No attacks |
| 1 (Mild) | Occasional attacks affecting tips of one or more fingers |
| 2 (Moderate) | Occasional attacks affecting distal and middle phalanges of one or more fingers |
| 3 (Severe) | Frequent attacks affecting all phalanges of most fingers |
| 4 (Very Severe) | As stage 3, with trophic skin changes in fingertips |
Rapid Upper Limb Assessment (RULA) & Rapid Entire Body Assessment (REBA)
RULA is a validated ergonomic assessment tool that evaluates posture, force, and repetition for the upper extremities during seated or standing tasks. Body segments are scored (arm, wrist, neck, trunk) and combined into a final action level (1-4), where 1 = acceptable posture and 4 = investigate and implement change immediately. REBA extends the assessment to the entire body and is especially useful for tasks involving unpredictable postures, manual handling, and dynamic movements. Both tools are observational, require minimal equipment, and can be applied to a wide range of workplace tasks. They are commonly used to prioritize ergonomic interventions and document pre- and post-intervention improvements.
Whole-Body Vibration (WBV)
Transmission of vibration through a seat or platform to the entire body occurs in vehicle operators (trucks, forklifts, tractors, heavy equipment). Chronic WBV exposure is associated with low back pain, lumbar disc degeneration, and spinal disorders. Risk mitigation includes vibration-dampening seats, limiting driving duration, maintaining equipment suspension, and reducing speed over rough terrain.
Job Hazard Analysis (JHA) for Ergonomic Risk
A Job Hazard Analysis (also called Job Safety Analysis) systematically breaks a job into component tasks and identifies hazards associated with each step. For ergonomic risk, the JHA documents: the specific physical demands of each task (lifting weight, frequency, posture, duration), the tools and equipment used, the work environment (temperature, lighting, space constraints), and the risk factors present. The output prioritizes tasks by risk level and identifies feasible controls — engineering modifications, work practice changes, or administrative adjustments. JHAs should be updated whenever job tasks change, new equipment is introduced, or injury trends emerge.
Prolonged standing increases risk of varicose veins, lower extremity edema, foot pain, and musculoskeletal fatigue. Prolonged sitting increases risk of low back pain, metabolic syndrome, and cardiovascular disease. The optimal approach is alternating between sitting and standing throughout the day, using adjustable-height workstations. Anti-fatigue mats reduce discomfort in standing workers by promoting micro-movements and reducing ground reaction forces. Job rotation and task variation reduce cumulative exposure to any single ergonomic risk factor.
10 Return to Work & Disability Management
Biopsychosocial Model of Disability
Disability is not determined solely by the medical condition. The biopsychosocial model recognizes that disability results from the interaction of biological factors (diagnosis, severity, comorbidities), psychological factors (catastrophizing, fear-avoidance behavior, depression, secondary gain), and social factors (workplace culture, job satisfaction, litigation status, family support, financial pressures). Effective return-to-work (RTW) programs must address all three domains.
Transitional Duty / Modified Work
Transitional duty (also called light duty, modified duty, or restricted work) provides temporary work accommodations that match the injured worker's current functional abilities. Evidence strongly supports early return to modified duty over prolonged absence — workers who return to some form of work within 1-2 weeks have significantly better outcomes than those kept off work entirely. Transitional duty should be: time-limited (typically 4-12 weeks), medically appropriate, productive (not "make-work"), and regularly reviewed with advancing functional goals.
Return-to-Work Protocol — Step-by-Step
A structured RTW protocol follows a systematic sequence to ensure safe, timely, and sustainable reintegration:
- Step 1 — Medical status clarification — obtain clear functional restrictions and limitations from the treating physician (e.g., "no lifting >15 lbs, no prolonged standing >30 min, no overhead reaching with left arm").
- Step 2 — Job demands analysis — document the essential physical demands of the worker's usual job (lifting weights, postures, repetitive motions, cognitive demands) using a standardized format.
- Step 3 — Gap analysis — compare medical restrictions to job demands. If restrictions preclude essential functions, identify transitional duty options or alternative positions within the organization.
- Step 4 — Transitional duty assignment — match available tasks to the worker's current functional abilities. Provide a written transitional duty agreement specifying duties, hours, restrictions, and expected duration.
- Step 5 — Progressive advancement — as the worker's condition improves and restrictions are liberalized, gradually increase job demands toward full duty. Reassess at each follow-up visit.
- Step 6 — Full duty release or MMI determination — the worker either returns to full unrestricted duty or reaches MMI with permanent restrictions, triggering impairment rating and permanent accommodation evaluation.
Psychosocial risk factors ("yellow flags") predict prolonged disability better than injury severity. Key yellow flags include: fear-avoidance beliefs (belief that activity will cause further injury), catastrophizing (exaggerated negative interpretation of pain), depression and anxiety, passive coping strategies (rest, withdrawal), workplace conflict or perceived injustice, low job satisfaction, pending litigation or compensation disputes, and lack of social support. Early screening using tools such as the Orebro Musculoskeletal Pain Questionnaire or the STarT Back Screening Tool allows targeted interventions (cognitive-behavioral therapy, motivational interviewing, workplace mediation) that significantly reduce disability duration.
Functional Capacity Evaluation (FCE)
An FCE is a comprehensive, standardized assessment of a worker's ability to perform physical demands of work. It typically includes: evaluation of lifting capacity (floor-to-waist, waist-to-shoulder, overhead), carrying, pushing/pulling, positional tolerance (standing, sitting, walking, bending, squatting, kneeling), hand function (grip, pinch strength, dexterity), and overall endurance. Validity measures are built into the FCE to assess whether the individual is providing consistent, maximal effort — including coefficient of variation testing, distraction-based testing, and comparison of observed function to self-reported limitations.
Impairment Rating — AMA Guides, 6th Edition
The AMA Guides to the Evaluation of Permanent Impairment (6th edition, 2008) provides a standardized methodology for rating permanent impairment. Key concepts:
- Maximum Medical Improvement (MMI) — the point at which a condition has stabilized and is unlikely to improve further with or without treatment; must be reached before impairment rating.
- Impairment — an objective, anatomic, or functional loss assessed by a physician (e.g., "15% whole person impairment").
- Disability — a broader concept encompassing the effect of impairment on the individual's ability to meet personal, social, or occupational demands — a legal/administrative determination, not a purely medical one.
- 6th Edition methodology — uses a diagnosis-based impairment (DBI) approach: first identify the diagnosis, determine the impairment class (0-4), place within the class using the default value, then adjust based on functional history, physical examination, and clinical studies (grade modifiers).
Work Restrictions vs. Limitations
Restrictions are physician-prescribed activities the worker should not perform (e.g., "no lifting >10 lbs with the left arm") — they are imposed to prevent harm. Limitations are activities the worker cannot perform due to the medical condition (e.g., "unable to stand for >30 minutes due to peripheral neuropathy") — they describe functional deficits. This distinction has medicolegal importance in workers' compensation and disability proceedings.
ADA Reasonable Accommodation in the RTW Context
When a worker reaches MMI with permanent restrictions that prevent performance of essential job functions, the Americans with Disabilities Act (ADA) may require the employer to provide reasonable accommodation — modifications that enable the worker to perform the essential functions of their position (or an equivalent vacant position). Examples of reasonable accommodations include: modified work schedule, ergonomic equipment (sit-stand desk, specialized tools), job restructuring (reassigning marginal functions), reassignment to a vacant position, telecommuting, and additional unpaid leave beyond FMLA entitlement. The employer is not required to create a new position, eliminate essential functions, lower production standards, or provide accommodations that impose undue hardship (significant difficulty or expense relative to the employer's resources).
11 Lead Exposure
Occupational Sources
Inorganic lead exposure remains a significant occupational hazard. High-risk industries include: battery manufacturing and recycling, lead smelting and refining, radiator repair, construction/demolition (removal of leaded paint), bridge and ship painting/scraping, soldering, stained glass work, firearms instruction (indoor ranges), and certain mining operations. Organic lead (tetraethyl lead) was historically found in leaded gasoline and is far more neurotoxic than inorganic lead due to lipid solubility; industrial use is now rare.
OSHA Lead Standards
OSHA regulates lead exposure under two separate standards: general industry (29 CFR 1910.1025) and construction (29 CFR 1926.62). Key thresholds:
- PEL — 50 mcg/m3 (8-hour TWA)
- Action level — 30 mcg/m3 (triggers medical surveillance)
- BLL trigger for medical surveillance — any BLL ≥30 mcg/dL (general industry)
- Medical removal — BLL ≥50 mcg/dL (general industry) or ≥50 mcg/dL (construction); worker is removed from exposure with medical removal protection (MRP) benefits until BLL <40 mcg/dL on two consecutive tests
Clinical Effects by Blood Lead Level
| BLL (mcg/dL) | Clinical Effects — Adults |
|---|---|
| <10 | Current reference range; subclinical effects on renal function and blood pressure may occur |
| 10-19 | Elevated zinc protoporphyrin (ZPP); subtle neurocognitive effects |
| 20-29 | Headache, fatigue, decreased libido, arthralgia; elevated free erythrocyte protoporphyrin (FEP) |
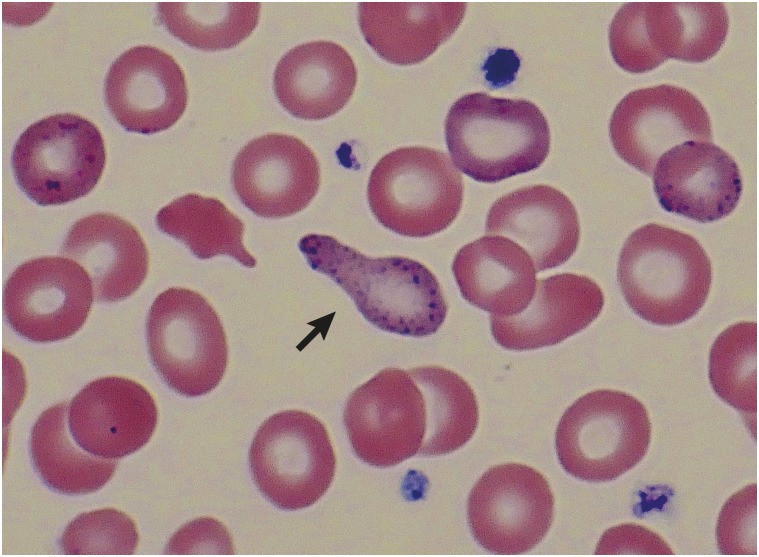
| 30-49 | Abdominal pain ("lead colic"), constipation, irritability, difficulty concentrating, peripheral motor neuropathy (wrist/foot drop), anemia (microcytic with basophilic stippling) |
| 50-69 | Severe abdominal colic, CNS symptoms (memory loss, mood disturbance), nephropathy (proximal tubular dysfunction), gout (saturnine gout) |
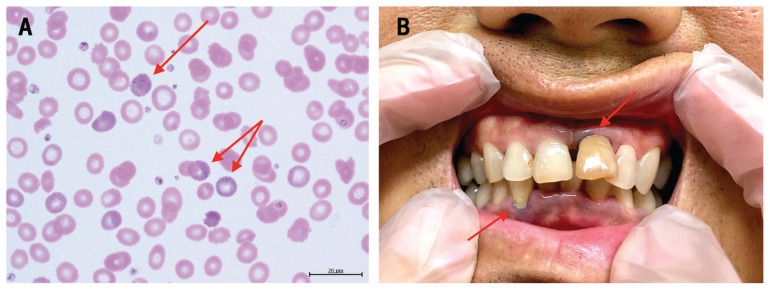
| 70-100 | Encephalopathy (seizures, coma), wrist drop, severe anemia, lead lines on gingiva (Burton lines) |
| >100 | Life-threatening encephalopathy, potentially fatal |
Diagnosis of Lead Toxicity
The cornerstone of diagnosis is the blood lead level (BLL), measured by venous blood sampling (capillary/fingerstick samples are acceptable for screening but must be confirmed by venous draw if elevated). Supporting laboratory findings include: elevated zinc protoporphyrin (ZPP) or free erythrocyte protoporphyrin (FEP) — reflects lead's inhibition of ferrochelatase in heme synthesis (rises at BLL >25-30); basophilic stippling on peripheral blood smear — reflects inhibition of pyrimidine-5'-nucleotidase, causing ribosomal RNA aggregation in erythrocytes (not specific to lead — also seen in thalassemia, MDS); elevated urine delta-aminolevulinic acid (ALA) — reflects inhibition of ALA dehydratase; and "lead lines" on long bone radiographs in children (dense metaphyseal bands representing lead deposition at growth plates — not seen in adults). Burton lines (blue-black gingival lines at the gum-tooth margin) are a classic but uncommon physical finding seen with chronic high-level exposure.
Chelation Therapy
| Agent | Route | Indications | Key Considerations |
|---|---|---|---|
| Succimer (DMSA) | Oral | BLL 45-69 (adults); 45-69 (children) | Best-tolerated oral chelator; monitor hepatic and renal function |
| CaNa2EDTA | IV | BLL ≥45 (adults); ≥45 (children); encephalopathy | Adequate hydration required; monitor renal function; do NOT use disodium EDTA (fatal hypocalcemia) |
| BAL (dimercaprol) | IM | BLL ≥70 or encephalopathy (given with CaNa2EDTA) | Must start BAL before EDTA in encephalopathy to prevent worsening CNS lead levels; peanut oil vehicle — contraindicated in peanut allergy |
| D-Penicillamine | Oral | Mild-moderate lead toxicity (rarely used) | Cross-reactivity with penicillin; multiple side effects; not FDA-approved for lead |
Medical Surveillance Program for Lead
When airborne lead exceeds the action level (30 mcg/m3), employers must provide: initial and semi-annual BLL, ZPP/FEP, CBC, BUN/creatinine, medical history and exam with focus on neurologic, GI, renal, and reproductive systems. Workers with BLL ≥40 mcg/dL require more frequent monitoring. Removed workers must be monitored monthly until BLL <40 on two consecutive tests.
Reproductive Toxicity of Lead
Lead is a potent reproductive toxicant in both men and women. In men, lead exposure is associated with decreased sperm count, abnormal sperm morphology, decreased motility, and reduced fertility. In women, lead crosses the placenta and is associated with spontaneous abortion, preterm birth, low birth weight, and neurodevelopmental impairment in offspring. Lead stored in bone is mobilized during pregnancy and lactation, potentially exposing the fetus/infant even if current exposure has ceased. OSHA's medical removal criteria (BLL ≥50) were established before the reproductive effects of lower-level exposure were fully understood. Many occupational medicine practitioners recommend removing women of childbearing potential from lead exposure at BLL ≥10-15 mcg/dL and men planning conception at BLL ≥30 mcg/dL, though these thresholds are not mandated by OSHA.
Approximately 90% of the body's lead burden is stored in bone, where it has a half-life of 20-30 years. Blood lead level reflects primarily recent or ongoing exposure (half-life ~30 days in blood). A worker with a history of high exposure may have a normal BLL years later yet carry a substantial bone lead burden. Conditions that increase bone turnover — pregnancy, lactation, menopause, immobilization, osteoporosis, hyperthyroidism — can remobilize lead from bone into blood, causing recurrent toxicity without new external exposure. K-shell X-ray fluorescence (KXRF) of the tibia and patella can quantify cumulative bone lead stores but is primarily a research tool.
12 Solvent & Chemical Exposure
Organic Solvents — General Toxicology
Organic solvents are lipophilic chemicals used as degreasers, diluents, and cleaning agents across nearly every industry. They share common toxicologic properties due to their lipid solubility: CNS depression (acute — dizziness, euphoria, narcosis; chronic — solvent encephalopathy), dermatitis (defatting of skin), hepatotoxicity, nephrotoxicity, and reproductive toxicity. Routes of absorption include inhalation (primary occupational route) and dermal (significant for many solvents — indicated by "Skin" notation on ACGIH TLV list).
Specific Agents
| Agent | Key Exposures | Primary Toxicity | Biological Monitoring | Cancer Risk |
|---|---|---|---|---|
| Benzene | Petroleum refining, rubber, chemical synthesis | Bone marrow suppression — aplastic anemia, MDS, AML | Urinary trans,trans-muconic acid; urinary S-phenylmercapturic acid | IARC Group 1 — leukemia |
| Toluene | Paint, adhesives, printing | CNS (acute intoxication, chronic encephalopathy); renal tubular acidosis (chronic abuse) | Urinary hippuric acid; blood toluene | Not classified as carcinogenic |
| Xylene | Paint, varnish, adhesives | CNS depression, mucous membrane irritation, hepatotoxicity | Urinary methylhippuric acid | Not classified as carcinogenic |
| n-Hexane | Glue, adhesives, rubber cement | Peripheral neuropathy ("glue sniffer's neuropathy") — axonal degeneration, giant axonal swelling | Urinary 2,5-hexanedione | Not classified |
| Methanol | Industrial solvent, fuel | Metabolized to formaldehyde/formic acid — metabolic acidosis with elevated osmolar gap, optic nerve toxicity (blindness) | Serum methanol; formic acid | Not classified |
| Carbon tetrachloride | Historical solvent, fire extinguishers | Hepatotoxicity (centrilobular necrosis), nephrotoxicity | Exhaled air CCl4 | IARC Group 2B |
| Carbon disulfide | Rayon/viscose manufacturing, rubber | Cardiovascular disease (accelerated atherosclerosis), CNS (psychosis, Parkinsonism), peripheral neuropathy, retinopathy | Urinary TTCA (2-thiothiazolidine-4-carboxylic acid) | Not classified |
| Formaldehyde | Funeral industry, labs, composite wood, healthcare | Mucous membrane irritation, allergic contact dermatitis, occupational asthma | Urinary formic acid (insensitive) | IARC Group 1 — nasopharyngeal carcinoma, leukemia |
Also known as "painter's syndrome" or organic solvent neurotoxicity. Classified by WHO into three types: Type 1 — organic affective syndrome (fatigue, mood changes); Type 2a — chronic toxic encephalopathy (sustained personality/mood changes, fatigue, impaired concentration); Type 2b — plus demonstrable neuropsychological impairment; Type 3 — dementia (severe, irreversible). Diagnosis requires prolonged solvent exposure (typically >10 years), appropriate symptom pattern, abnormal neuropsychological testing, and exclusion of other causes. Type 1-2a may be partially reversible with cessation of exposure; Types 2b-3 are typically irreversible.
13 Noise-Induced Hearing Loss
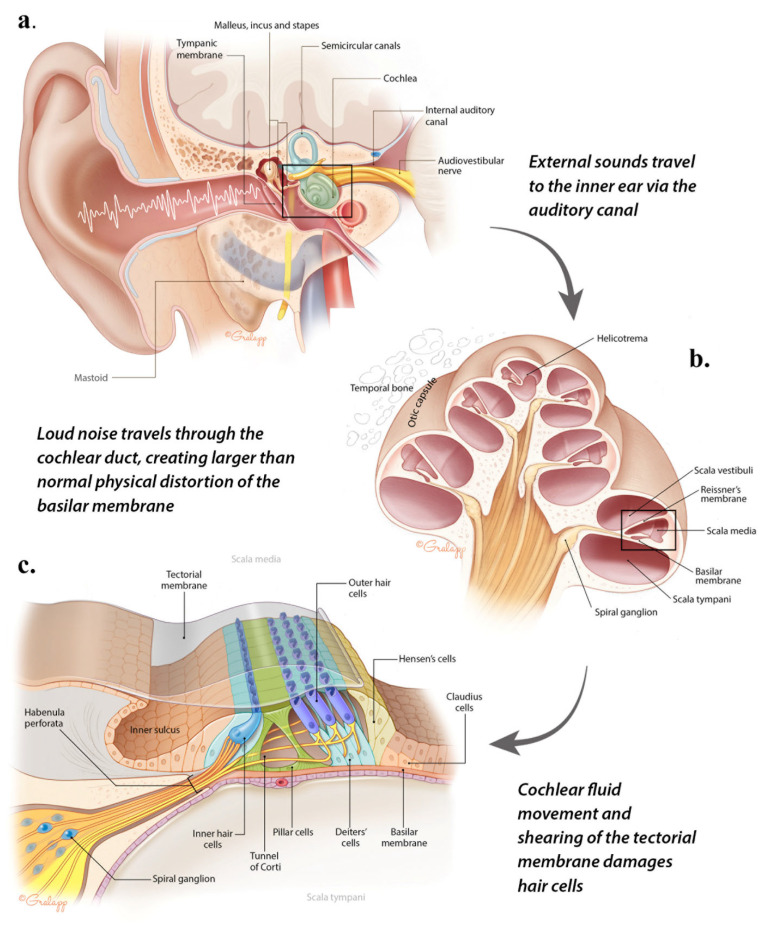
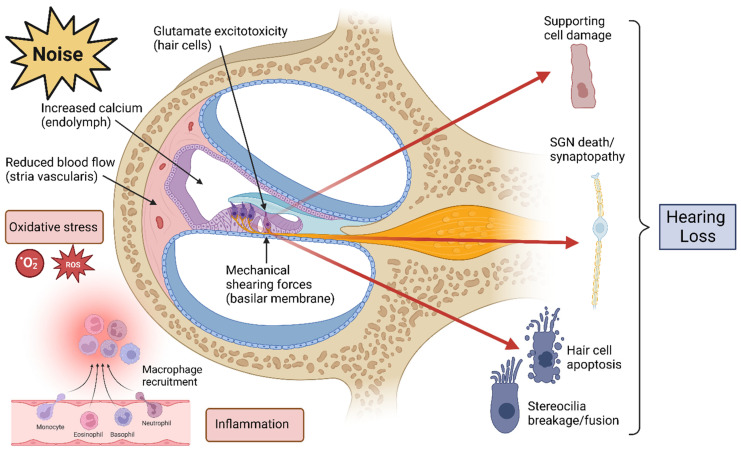
Mechanism
Noise-induced hearing loss (NIHL) results from damage to the outer hair cells of the organ of Corti in the cochlea. Outer hair cells are mechanosensory cells responsible for amplifying sound signals; they are the most vulnerable component of the auditory system. Damage begins at the basal turn of the cochlea (which processes high-frequency sound) and progresses apically. NIHL is sensorineural, bilateral, symmetric, and irreversible. It is the most common occupational disease worldwide and the second most common form of sensorineural hearing loss (after presbycusis).
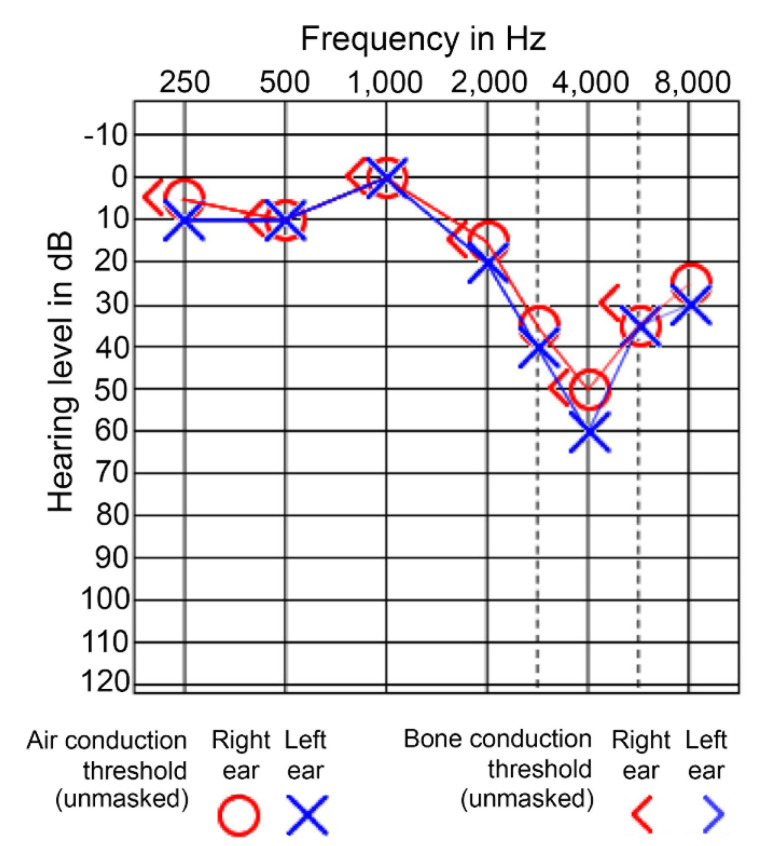
Audiometric Pattern
The characteristic audiometric finding is a 4000 Hz notch (also called a "4 kHz dip") — a dip in hearing sensitivity centered at 4000 Hz with recovery at 8000 Hz. This notch at 4 kHz (with relative preservation at adjacent frequencies) is highly suggestive of noise exposure, though 3000 Hz or 6000 Hz notches can also occur. As exposure continues, the notch deepens and broadens, eventually affecting conversational frequencies (500-3000 Hz) and impairing speech discrimination.
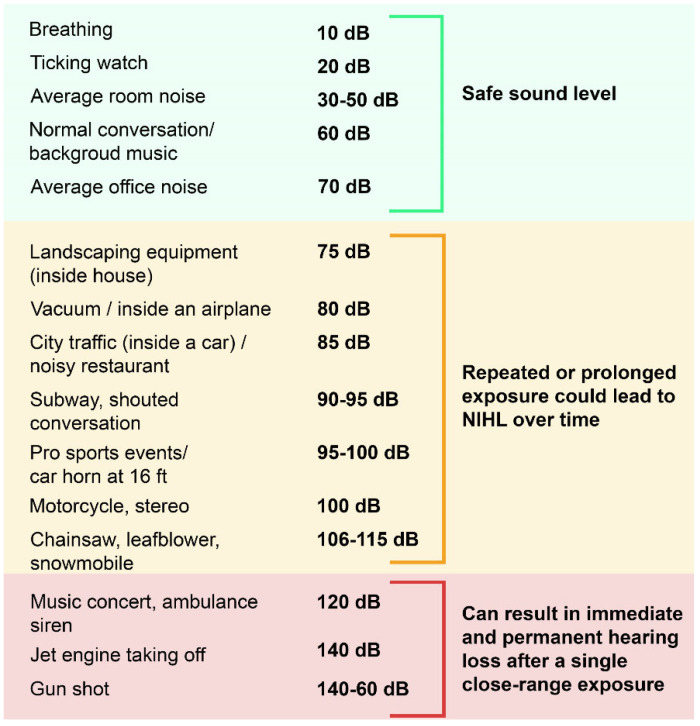
Common Noise Exposure Sources
| Source | Typical Level (dBA) | Permissible Duration (OSHA) |
|---|---|---|
| Normal conversation | 60-65 | Unlimited |
| Busy traffic / vacuum cleaner | 75-80 | Unlimited (<85 dBA) |
| Power lawn mower / shop tools | 85-90 | 8 hours (at 90 dBA) |
| Circular saw / belt sander | 93-95 | 4 hours (at 95 dBA) |
| Chain saw / pneumatic drill | 100-110 | 2 hours (100); 30 min (110) |
| Rock concert / siren at 30 m | 110-120 | 30 min (110); 7.5 min (115) |
| Jet engine at 30 m / gunshot | 130-140+ | Immediate risk of acoustic trauma |
OSHA Noise Standard (29 CFR 1910.95)
| Parameter | OSHA Value | NIOSH REL |
|---|---|---|
| PEL (8-hour TWA) | 90 dBA | 85 dBA |
| Action level (triggers HCP) | 85 dBA (8-hour TWA) | — |
| Exchange rate | 5 dB (halving rate) | 3 dB |
| Maximum impulse noise | 140 dB peak | 140 dB peak |
The exchange rate defines the trade-off between intensity and duration. OSHA uses a 5-dB exchange rate: for every 5-dB increase in noise level, the permissible exposure time is halved (e.g., 90 dBA for 8 hours = 95 dBA for 4 hours = 100 dBA for 2 hours). NIOSH uses a more protective 3-dB exchange rate, which is more aligned with bioacoustic evidence of damage risk.
Hearing Conservation Program (HCP)
Required when noise exceeds the 85 dBA action level. Components include:
- Noise monitoring — baseline and periodic area/personal dosimetry
- Engineering controls — preferred over administrative controls or PPE; includes equipment modification, vibration dampening, sound barriers, and enclosures
- Hearing protection — earplugs (NRR 15-33), earmuffs (NRR 20-30), or combination; actual attenuation is typically 50% of labeled NRR due to improper fit. OSHA-adjusted NRR: (NRR - 7) / 2 for earplugs; (NRR - 7) x 0.75 for earmuffs.
- Audiometric testing — baseline within 6 months of first exposure (preceded by 14 hours of quiet); annual thereafter. A Standard Threshold Shift (STS) is an average shift of ≥10 dB at 2000, 3000, and 4000 Hz in either ear relative to baseline. If confirmed, the worker must be notified within 21 days, refitted/retrained for hearing protection, and referred for evaluation if not already using HPD.
- Training — annual education on noise hazards, HPD use, and the purpose of audiometric testing
14 Heat & Cold Illness
Heat Stress
Occupational heat illness results from the inability to dissipate metabolic and environmental heat. The Wet Bulb Globe Temperature (WBGT) index integrates air temperature, radiant heat, humidity, and wind speed and is the standard metric for assessing heat stress. ACGIH TLVs for heat stress are based on WBGT, metabolic rate (light/moderate/heavy/very heavy work), and work-rest cycle.
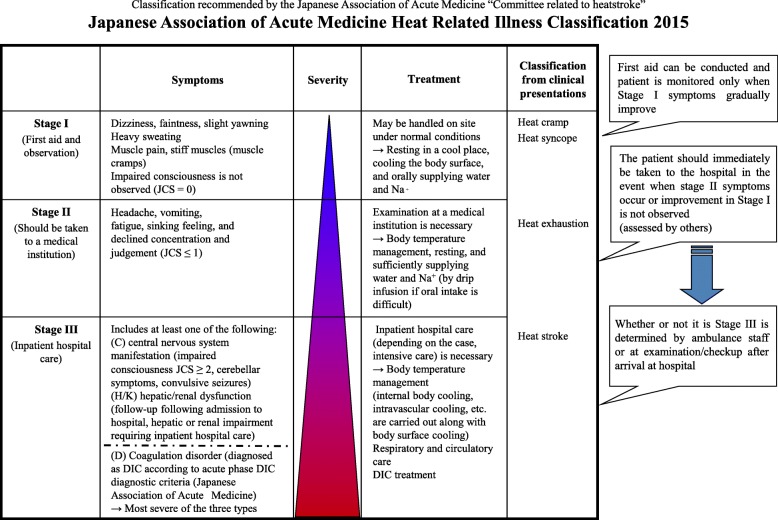
Heat-Related Conditions
| Condition | Core Temp | CNS Function | Skin | Sweating | Treatment |
|---|---|---|---|---|---|
| Heat cramps | Normal | Normal | Normal | Profuse | Rest, oral electrolyte/salt replacement, stretching |
| Heat syncope | Normal/mildly elevated | Transient LOC | Warm, moist | Present | Supine position, fluids, cooling; exclude cardiac cause |
| Heat exhaustion | <40°C (104°F) | Intact (fatigue, headache, nausea, weakness, dizziness) | Cool, clammy | Profuse | Remove from heat, supine, aggressive oral/IV rehydration, active cooling |
| Heat stroke | >40°C (104°F) | Altered (confusion, seizure, coma) | Hot, may be dry or wet | May or may not be present | EMERGENCY: rapid cooling (ice water immersion preferred), IV fluids, ICU; mortality 10-50% |
The two defining features of heat stroke that distinguish it from heat exhaustion are: (1) core temperature >40°C (104°F), and (2) CNS dysfunction (altered mental status, confusion, seizures, coma). Heat stroke is a medical emergency. Classic (non-exertional) heat stroke often presents with anhidrosis (dry skin), while exertional heat stroke may present with diaphoresis. Do not delay cooling to obtain a temperature — if CNS dysfunction is present in the setting of heat exposure, treat as heat stroke.
Heat Illness Prevention Program
OSHA's recommended elements for a comprehensive heat illness prevention program include:
- Water — potable drinking water readily accessible; workers should drink 1 cup (8 oz) every 15-20 minutes during heat exposure, even if not thirsty; avoid caffeinated beverages and energy drinks.
- Rest — scheduled rest breaks in shaded or air-conditioned areas; frequency and duration based on WBGT and workload intensity; mandatory cool-down periods when temperature or humidity rises.
- Shade — access to shaded rest areas for outdoor workers; indoor workers in hot environments should have climate-controlled break rooms.
- Buddy system — workers should monitor each other for signs of heat illness; no worker should be left alone in high-heat environments.
- Emergency planning — established protocols for recognizing and treating heat illness; cold water immersion supplies available for high-risk operations; clear instructions for calling emergency services.
Acclimatization
Heat acclimatization occurs over 7-14 days of gradually increasing heat exposure. Physiologic adaptations include: earlier onset of sweating, increased sweat rate, decreased sodium concentration in sweat, lower resting core temperature, decreased heart rate at a given workload, and increased plasma volume. NIOSH recommends that unacclimatized workers begin at 20% of the full heat exposure workload and increase by no more than 20% per day. Previously acclimatized workers returning after >1 week absence should start at 50% and increase by 10-20% per day.
Cold-Related Conditions

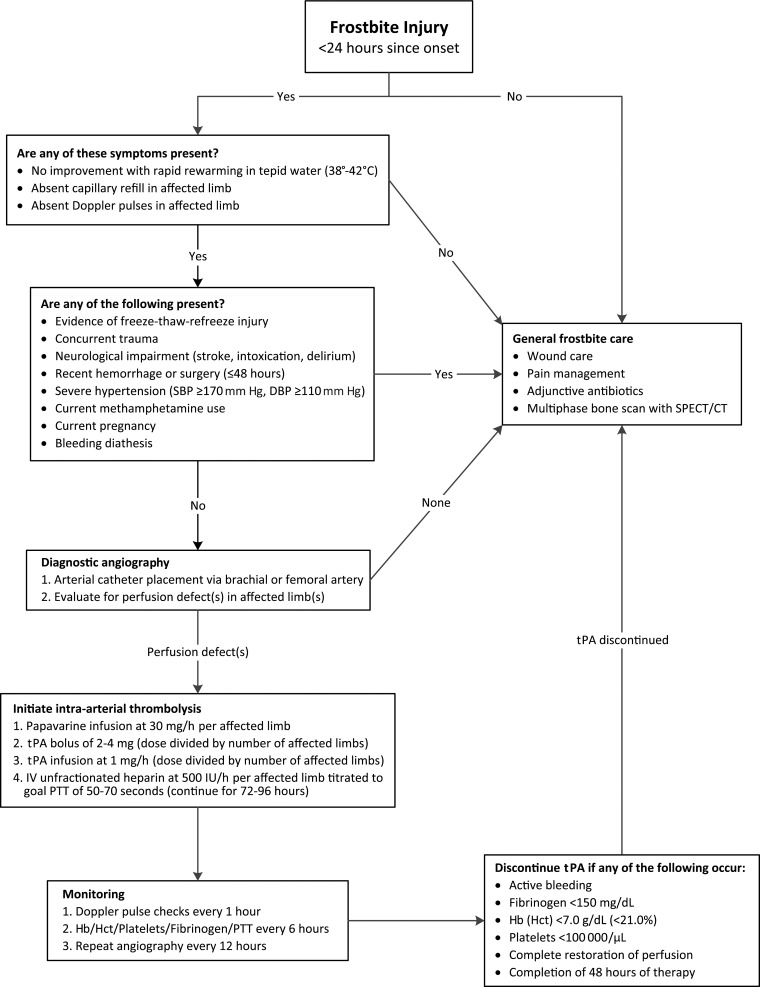
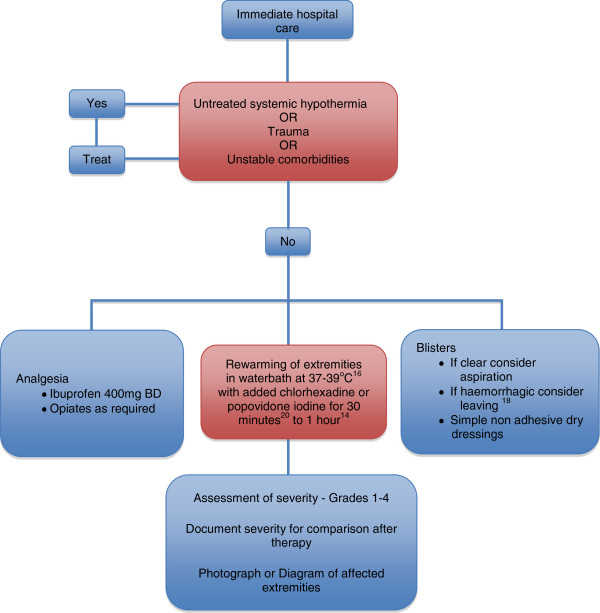
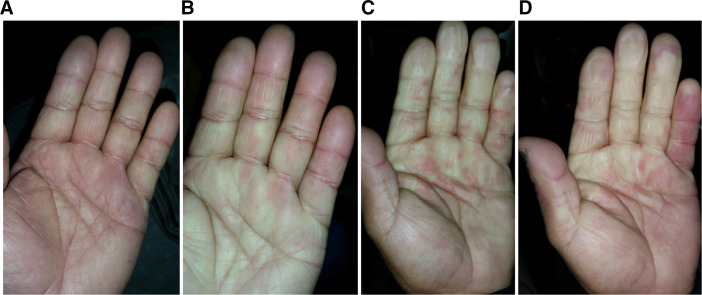
Frostbite — freezing injury to tissue. Classification: Grade I — numbness and erythema, no blistering (superficial); Grade II — clear blistering extending to fingertips; Grade III — hemorrhagic blistering, full-thickness injury; Grade IV — extension into bone/muscle/tendon, gangrene. Treatment: rapid rewarming in 37-39°C water bath for 15-30 minutes (avoid dry heat, rubbing); ibuprofen for thromboxane inhibition; consider tPA for severe frostbite within 24 hours; avoid refreezing (worse than delayed thawing).
Hypothermia — core temperature <35°C. Mild (32-35°C): shivering, tachycardia, confusion, poor judgment. Moderate (28-32°C): shivering ceases, bradycardia, atrial fibrillation, decreased level of consciousness, paradoxical undressing. Severe (<28°C): coma, ventricular fibrillation risk, absent reflexes, appears dead. Management: remove wet clothing, passive external rewarming (mild), active external rewarming with warm blankets/forced warm air (moderate), active internal rewarming with warm IV fluids/heated humidified oxygen/pleural or peritoneal lavage/ECMO (severe). The dictum: "No one is dead until they are warm and dead."
Raynaud Phenomenon vs. HAVS
Primary Raynaud is idiopathic vasospasm of digital arteries, typically bilateral and symmetric, most common in young women. Secondary Raynaud can be caused by connective tissue disease (scleroderma, SLE) or occupational vibration exposure. HAVS (hand-arm vibration syndrome) involves vasospasm plus neurological and musculoskeletal components, is related to specific tool use, and may be asymmetric (affecting the dominant hand more). Differentiation requires detailed occupational exposure history, Stockholm classification, and vascular/neurological testing (cold provocation, nerve conduction studies).
Trench Foot (Non-Freezing Cold Injury)
Trench foot (immersion foot) is a non-freezing peripheral cold injury caused by prolonged exposure (typically hours to days) to cold, wet conditions above freezing (0-15°C / 32-59°F). Occurs in military personnel, outdoor workers, agricultural workers, and homeless populations. Clinical stages: (1) During exposure — cold, numb, pale/cyanotic feet, impaired sensation; (2) After rewarming — intense hyperemia, pain, edema, paresthesias; (3) Post-hyperemic — cold sensitivity, hyperhidrosis, neuropathic pain that may persist for months to years. Treatment: gentle rewarming (not rapid rewarming as for frostbite), elevation, dry socks, pain management (gabapentin or amitriptyline for neuropathic pain), and wound care for any tissue breakdown. Prevention: waterproof footwear, regular sock changes, boot removal and foot drying during breaks, buddy-system foot inspection.
15 OSHA Regulations
Recordkeeping Requirements
Employers with >10 employees in most industries must maintain injury and illness records using three forms:
- OSHA 300 Log — the "Log of Work-Related Injuries and Illnesses," listing each recordable case with details (name, job title, date, description, outcome).
- OSHA 300A Summary — the annual summary posted in the workplace from February 1 through April 30, showing totals for the prior calendar year. Certified by a company executive.
- OSHA 301 Form — the "Injury and Illness Incident Report," a detailed form completed for each recordable case (or equivalent, such as the state workers' comp first report of injury).
A case is recordable if it is work-related and results in: death, days away from work, restricted work or job transfer, medical treatment beyond first aid, loss of consciousness, or a significant injury/illness diagnosed by a physician (e.g., cancer, fracture, chronic irreversible disease). First aid treatment alone does not make a case recordable.
First Aid vs. Medical Treatment — The Recordability Distinction
The distinction between first aid and medical treatment determines whether an injury is OSHA-recordable. First aid is defined exhaustively by OSHA (29 CFR 1904.7(a)) and includes only the following: (1) non-prescription medications at nonprescription strength; (2) wound cleaning, flushing, or soaking; (3) wound closure devices (butterfly bandages, Steri-Strips); (4) application of bandages during subsequent visits; (5) hot or cold therapy; (6) rigid splints or non-rigid supports (ace wraps, back belts); (7) eye patches; (8) removal of foreign bodies from the eye with irrigation or cotton swab; (9) finger guards; (10) massage; (11) drinking fluids for heat-related illness; (12) oxygen administration; (13) use of eye wash. Any treatment not on this list is considered medical treatment beyond first aid and makes the case recordable.
Reporting Requirements
All employers (regardless of size or exemption from recordkeeping) must report: (1) any work-related fatality within 8 hours; (2) any work-related in-patient hospitalization, amputation, or loss of an eye within 24 hours. Reports are made to OSHA by telephone, in person, or via the online reporting portal.
Inspection Process
OSHA inspections (also called surveys) follow a standard sequence: (1) Opening conference — the compliance officer presents credentials and explains the purpose and scope; (2) Walk-around inspection — the officer examines the workplace for hazards, accompanied by employer and employee representatives; may include air monitoring, photography, and employee interviews; (3) Closing conference — the officer discusses findings and potential citations. Inspections are prioritized by: imminent danger (highest), fatalities/catastrophes, employee complaints, programmed (targeted high-hazard industries), and follow-up.
Citation Types & Penalties
| Citation Type | Description | Maximum Penalty (2024) |
|---|---|---|
| Willful | Intentional or knowing violation of a standard | $161,323 per violation |
| Repeat | Same or similar violation within 5 years | $161,323 per violation |
| Serious | Violation with substantial probability of death/serious harm and employer knew or should have known | $16,131 per violation |
| Other-than-serious | Violation unlikely to cause death/serious harm | $16,131 per violation |
| De minimis | Violation with no direct/immediate safety impact | No penalty; notice only |
Whistleblower Protection
Section 11(c) of the OSH Act prohibits retaliation against employees who exercise their safety and health rights, including filing complaints, participating in inspections, or refusing to perform work that poses imminent danger. Workers must file a Section 11(c) complaint with OSHA within 30 days of the alleged retaliation. OSHA also enforces whistleblower provisions under more than 20 additional federal statutes (e.g., Sarbanes-Oxley, Surface Transportation, FDA food safety).
Multi-Employer Worksite Doctrine
On multi-employer construction or industrial sites, OSHA may cite employers who did not create a hazard but whose employees are exposed to it. The multi-employer citation policy defines four categories of employers: (1) Creating employer — caused the hazardous condition; (2) Exposing employer — whose employees are exposed to the hazard; (3) Correcting employer — responsible for correcting the hazard (often by contract); (4) Controlling employer — has general supervisory authority over the worksite. Each can be cited based on their role, knowledge, and ability to prevent or correct the hazard. This doctrine is particularly important in construction, where multiple subcontractors share a worksite.
16 Medical Surveillance Programs
OSHA-Mandated Medical Surveillance
OSHA requires specific medical surveillance programs for workers exposed to certain hazardous substances above action levels. These programs include pre-placement, periodic, and termination examinations.
| Substance/Standard | Key Exam Components | Frequency |
|---|---|---|
| Asbestos (1910.1001) | History, exam, CXR (ILO classification), PFTs (FVC, FEV1) | Pre-placement, annual, termination |
| Lead (1910.1025) | BLL, ZPP, CBC, BUN, creatinine, history/exam | Pre-placement; semi-annual BLL if >action level; medical removal at BLL ≥50 |
| Benzene (1910.1028) | CBC with differential, history/exam | Pre-placement, annual; additional if abnormal CBC |
| Cadmium (1910.1027) | BCD (blood cadmium), UCd (urine cadmium), beta-2-microglobulin, CBC, BUN, creatinine, urinalysis | Pre-placement, annual, biologic monitoring semi-annually |
| Noise (1910.95) | Audiometric testing (pure tone — 500-8000 Hz) | Baseline (within 6 months), annual |
| Respiratory protection (1910.134) | OSHA respiratory medical questionnaire; PFTs as indicated | Pre-placement; periodic as needed per physician |
| Hexavalent chromium (1910.1026) | History, exam (focus on skin/respiratory), CXR as indicated | Within 30 days of initial assignment; annually thereafter |
| Methylene chloride (1910.1052) | History, exam, CBC, carboxyhemoglobin or end-exhaled CO | Pre-placement, periodic per physician judgment |
Pulmonary Function Testing in Surveillance
PFTs in occupational surveillance measure FEV1 and FVC. Results are compared to predicted values based on age, height, sex, and race/ethnicity. Interpretation: FEV1/FVC <0.70 (or <LLN) suggests obstruction. FVC <80% predicted with normal ratio suggests restriction (confirm with TLC). Bronchodilator response (≥12% and ≥200 mL improvement in FEV1) suggests reversible obstruction. Longitudinal decline — a year-over-year decline in FEV1 exceeding the expected age-related decline (~25-30 mL/year) may indicate occupational lung disease even before values fall below the normal range.
Audiometric Testing
Baseline audiogram must be obtained within 6 months of first exposure to noise at or above the action level (85 dBA), preceded by 14 hours of quiet (<80 dBA). Annual audiograms are compared to the baseline. A Standard Threshold Shift (STS) is confirmed if the average shift at 2000, 3000, and 4000 Hz is ≥10 dB in either ear (with optional age correction per OSHA). If an STS is confirmed, the employee must be notified within 21 days, refitted for hearing protection, and the OSHA 300 log is updated if hearing level crosses the 25-dB average threshold at 2000, 3000, and 4000 Hz.
ILO Classification System for Chest Radiographs
The ILO International Classification of Radiographs of Pneumoconioses is a standardized system for describing and recording chest X-ray abnormalities caused by inhaled dusts. B-readers are physicians certified by NIOSH to classify films using this system. The classification addresses small opacities (profusion rated on a 12-point scale from 0/- to 3/+, shape — rounded or irregular, size), large opacities (categories A, B, C based on size), pleural abnormalities (plaques, thickening, calcification), and additional symbols for specific findings. Detailed ILO classification is covered in Section 27.
17 DOT / FMCSA Physical Examination
Overview
The DOT physical examination is a federally mandated fitness-for-duty evaluation for commercial motor vehicle (CMV) operators, governed by FMCSA regulations (49 CFR Part 391). The examiner must be listed on the FMCSA National Registry of Certified Medical Examiners. The medical examination certificate is valid for a maximum of 2 years, though shorter certification periods are common for conditions requiring monitoring.
Vision Standards
Distant visual acuity of at least 20/40 in each eye (with or without corrective lenses). Field of vision of at least 70 degrees in the horizontal meridian in each eye. The ability to recognize the colors red, green, and amber. Monocular vision — drivers with vision in only one eye may obtain a Federal Vision Exemption but must demonstrate compensatory skills and safe driving experience.
Hearing Standards
The driver must perceive a forced whispered voice at a distance of 5 feet or more, with or without a hearing aid; OR have average hearing loss in the better ear of no more than 40 dB (using pure tone audiometry at 500, 1000, 2000, and 3000 Hz). If a hearing aid is used, it must be worn while driving.
Cardiovascular Standards
No current diagnosis of myocardial infarction, angina pectoris, coronary insufficiency, thrombosis, or other cardiovascular disease of a variety known to be accompanied by syncope, dyspnea, collapse, or congestive heart failure is disqualifying — unless the driver is medically cleared with appropriate waiting periods. Specific cardiovascular waiting periods and clearance requirements include:
- Myocardial infarction — minimum 2-month waiting period; cardiology clearance with stress test demonstrating functional capacity ≥6 METs and no exercise-induced ischemia.
- CABG / PCI (stent) — minimum 3-month (CABG) or 6-week (PCI) waiting period; cardiology evaluation with stress test; left ventricular ejection fraction ≥40%.
- Implantable cardioverter-defibrillator (ICD) — disqualifying; no FMCSA exemption program currently available for ICD patients.
- Permanent pacemaker — may be certified with cardiology clearance demonstrating stable rhythm, adequate rate response, and no syncope history.
- Atrial fibrillation — may be certified if rate-controlled, anticoagulated if indicated, and no history of syncope or hemodynamic instability.
| BP Category | Systolic | Diastolic | Certification |
|---|---|---|---|
| Stage 1 | <140 | <90 | 2-year certification |
| Stage 2 | 140-159 | 90-99 | 1-year certification; recheck annually |
| Stage 3 | 160-179 | 100-109 | One-time 1-year certification; must be <140/90 at recheck |
| Stage 4 | ≥180 | ≥110 | Disqualified until BP <140/90; then 6-month certification |
Diabetes
Insulin-treated diabetes mellitus is disqualifying under baseline FMCSA regulations. However, drivers may apply for a Federal Diabetes Exemption, which requires: stable insulin regimen for ≥3 years, no severe hypoglycemic episode (requiring third-party assistance) within the past 5 years, annual endocrinologist evaluation, HbA1c ≤10%, and self-monitoring of blood glucose with log documentation. Oral hypoglycemics and non-insulin injectables (e.g., GLP-1 agonists) are not automatically disqualifying but require assessment for hypoglycemia risk.
Neurological & Seizure Disorder Standards
Any condition that is likely to cause loss of consciousness or loss of ability to control a CMV is disqualifying. Key neurological considerations:
- Epilepsy / seizure disorder — disqualifying under current FMCSA regulations. A Federal Seizure Exemption program exists, requiring: seizure-free for ≥8 years, off all anticonvulsant medications for ≥8 years, and neurological clearance. A single provoked seizure (e.g., post-traumatic, metabolic) with low recurrence risk may allow standard certification after appropriate evaluation.
- Stroke / TIA — minimum 1-year waiting period; neurology clearance; must demonstrate no residual cognitive or motor deficits that impair safe driving.
- Syncope — must have an identified and treated cause; recurrent unexplained syncope is disqualifying.
Sleep Apnea Screening
FMCSA does not have a formal sleep apnea standard, but examiners are expected to screen for sleep disorders. Risk factors warranting further evaluation: BMI ≥35, neck circumference >17 inches (men) or >16 inches (women), witnessed apnea, excessive daytime sleepiness, Epworth Sleepiness Scale ≥11. If OSA is diagnosed, CPAP compliance must be documented (≥4 hours/night on ≥70% of nights) before certification or recertification. Typically issued a 1-year certificate with compliance data review.
Substance Abuse — SAP Process
A CMV driver who tests positive for controlled substances or refuses a test is immediately removed from safety-sensitive duties and must be evaluated by a Substance Abuse Professional (SAP). The SAP determines appropriate treatment/education, confirms successful completion, and recommends return-to-duty testing. The driver must then pass a return-to-duty drug test and is subject to unannounced follow-up testing (minimum 6 direct-observation tests in the first 12 months).
Disqualifying Medications for CMV Operators
Certain medications are disqualifying for CMV operators under FMCSA regulations:
- Schedule I substances — all are disqualifying (e.g., marijuana, heroin, LSD), including state-legal medical marijuana — federal law governs CMV operation.
- Methadone — disqualifying regardless of indication (pain management or opioid use disorder treatment).
- Amphetamines (Schedule II) — disqualifying. Stimulant medications prescribed for ADHD (amphetamine, methylphenidate) require careful evaluation; FMCSA advisory guidance notes that stimulant use for ADHD is not automatically disqualifying if the underlying condition is well-managed, though many examiners request neuropsychological evaluation documenting safe attentional capacity.
- Other opioids — not automatically disqualifying, but examiner must determine if the medication impairs ability to safely operate a CMV (sedation, cognitive impairment, risk of withdrawal).
- Anticoagulants, anticonvulsants, sedative-hypnotics — evaluated case-by-case for impairment risk and underlying condition stability.
18 Drug & Alcohol Testing
DOT Regulations — 49 CFR Part 40
The DOT mandates drug and alcohol testing for safety-sensitive employees in transportation industries (FMCSA, FAA, FRA, FTA, PHMSA, USCG). Testing must be conducted according to the procedures in 49 CFR Part 40, which governs specimen collection, laboratory analysis, Medical Review Officer (MRO) verification, and the SAP process.
Standard 5-Panel Drug Test
| Drug Class | Initial Screen Cutoff | Confirmation Cutoff | Detection Window (Urine) |
|---|---|---|---|
| Marijuana (THC-COOH) | 50 ng/mL | 15 ng/mL | Casual: 3-4 days; Heavy: up to 30 days |
| Cocaine (benzoylecgonine) | 150 ng/mL | 100 ng/mL | 2-4 days |
| Opiates (codeine/morphine; 6-AM; oxycodone/oxymorphone; hydrocodone/hydromorphone) | 2000 ng/mL (codeine/morphine); 300 ng/mL (oxycodone, hydrocodone) | Varies by analyte | 1-3 days |
| Amphetamines (amphetamine, methamphetamine, MDMA, MDA) | 500 ng/mL | 250 ng/mL | 1-3 days |
| Phencyclidine (PCP) | 25 ng/mL | 25 ng/mL | 1-8 days (chronic: up to 30 days) |
Specimen Validity Testing
Every specimen undergoes validity testing to detect substitution, dilution, or adulteration: Creatinine — <2 mg/dL is reported as "substituted" (not consistent with normal human urine); 2-20 mg/dL is "dilute." Specific gravity — <1.0010 or >1.0200 is "substituted." pH — <3 or >11 is "invalid." Oxidizing adulterants — chromium, nitrites, pyridinium chlorochromate, and other agents are tested to detect attempts to destroy drug metabolites.
Testing Categories
- Pre-employment — required before first performance of safety-sensitive duties; negative result required.
- Random — unannounced testing using a scientifically valid random selection process; annual testing rates set by each DOT agency (e.g., FMCSA: 50% for drugs, 10% for alcohol).
- Post-accident — required after certain qualifying accidents (fatality, citation-issued accidents with bodily injury/disabling vehicle damage); must be collected within 8 hours (alcohol) or 32 hours (drugs).
- Reasonable suspicion — based on trained supervisor's specific, contemporaneous observations of appearance, behavior, speech, or body odor; requires documentation.
- Return-to-duty — required before resuming safety-sensitive duties after a violation; must test negative under direct observation.
- Follow-up — unannounced testing after return to duty; minimum 6 tests in first 12 months, may extend up to 60 months per SAP recommendation.
Medical Review Officer (MRO)
The MRO is a licensed physician with knowledge of substance abuse who receives laboratory results and conducts a medical interview with the donor before reporting a verified positive. The MRO determines whether there is a legitimate medical explanation for a positive result (e.g., prescription opioid with valid prescription, poppy seed ingestion). The MRO can change a laboratory positive to a verified negative if a legitimate medical explanation is confirmed. The MRO cannot change a laboratory negative to a positive.
Oral fluid (saliva) testing was authorized for DOT testing in 2023 (49 CFR Part 40, revised). Advantages include direct observation of collection (reduces substitution/adulteration), shorter detection window (hours to days — better reflects recent use), and ease of collection. Hair testing provides a longer detection window (up to 90 days) but is NOT currently authorized for DOT testing. It may be used by employers in non-DOT (company policy) testing programs. Hair testing has known limitations with dark/chemically treated hair and low-level use detection.
19 Needlestick & Bloodborne Pathogen Exposure
OSHA Bloodborne Pathogens Standard (29 CFR 1910.1030)
The BBP standard requires employers to have a written Exposure Control Plan, provide Hepatitis B vaccination (at no cost), use engineering and work practice controls (sharps containers, self-sheathing needles, safety-engineered sharps devices), provide PPE, ensure proper training, and maintain a Sharps Injury Log that records the type and brand of device, department/work area, and a description of the incident.
Post-Exposure Protocol
After a percutaneous or mucous membrane exposure to blood or body fluids:
- Immediate first aid — wash wound with soap and water; flush mucous membranes with water or saline. Do NOT squeeze the wound to "milk out" blood.
- Source patient testing — rapid HIV test, HBsAg, anti-HCV (consent per state law; if source cannot be tested, treat as high-risk).
- Exposed worker baseline labs — HIV antibody, HBsAg, anti-HBs (to confirm immunity if vaccinated), anti-HCV, CBC, hepatic panel, pregnancy test if applicable.
- Risk assessment — type of exposure (percutaneous > mucous membrane > intact skin), type of fluid (blood > other body fluids), and source patient status.
HIV Post-Exposure Prophylaxis (PEP)
HIV PEP should be initiated as soon as possible, ideally within 1-2 hours, and no later than 72 hours after exposure. Current recommendation is a 3-drug regimen for all occupational exposures warranting PEP (the 2-drug regimen is no longer preferred): typically tenofovir/emtricitabine + raltegravir (or dolutegravir) for 28 days. Follow-up HIV testing at 6 weeks, 12 weeks, and 6 months post-exposure (or 4 months if using 4th-generation antigen/antibody assay).
Hepatitis B
Management depends on the exposed worker's vaccination and immunity status:
| Exposed Worker Status | Source HBsAg+ | Source HBsAg- | Source Unknown |
|---|---|---|---|
| Unvaccinated | HBIG x1 + start HBV vaccine series | Start HBV vaccine series | Start HBV vaccine series |
| Vaccinated, known responder (anti-HBs ≥10 mIU/mL) | No treatment needed | No treatment | No treatment |
| Vaccinated, known non-responder | HBIG x2 (1 month apart) OR HBIG x1 + revaccination | No treatment | Consider HBIG x1 + revaccination if high-risk source |
| Vaccinated, response unknown | Test anti-HBs; if ≥10 — no treatment; if <10 — HBIG x1 + vaccine booster | Test anti-HBs; vaccinate if <10 | Test anti-HBs; vaccinate if <10 |
Hepatitis C
There is no PEP available for HCV. The average risk of seroconversion from a needlestick with an HCV-positive source is approximately 1.8% (range 0-7%). Management: baseline and follow-up HCV RNA (at 4-6 weeks) and anti-HCV (at 4-6 months). Early detection of seroconversion allows prompt treatment with direct-acting antiviral agents, which achieve sustained virologic response (cure) rates >95%.
20 Respiratory Protection
OSHA Respiratory Protection Standard (29 CFR 1910.134)
Whenever engineering and administrative controls are insufficient to reduce airborne contaminant levels below the PEL, or when such controls are being implemented, respiratory protection is required. The employer must establish a written respiratory protection program that includes: medical clearance, fit testing, selection of appropriate respirators, training, maintenance, and program evaluation.
Medical Clearance
Before an employee is fit-tested or required to use a respirator, a Physician or Other Licensed Health Care Professional (PLHCP) must determine that the worker is medically able to wear a respirator. The evaluation uses the OSHA Respiratory Medical Evaluation Questionnaire (Appendix C to 1910.134), which screens for cardiovascular disease, respiratory disease, neurological conditions, and other factors that could impair respirator use. Additional medical tests (PFTs, CXR, exercise tolerance) may be required based on questionnaire responses. The PLHCP provides a written recommendation — fit to wear, unfit, or fit with restrictions.
Respirator Selection & Protection Factors
| Respirator Type | Assigned Protection Factor (APF) | Use Setting |
|---|---|---|
| Half-face air-purifying (N95, P100, chemical cartridge) | 10 | Concentrations up to 10x PEL |
| Full-face air-purifying | 50 | Concentrations up to 50x PEL |
| Powered air-purifying respirator (PAPR) — loose-fitting | 25 | Cannot be fit-tested; useful for facial hair, glasses |
| PAPR — half-face tight-fitting | 50 | Up to 50x PEL |
| PAPR — full-face tight-fitting | 1,000 | Up to 1,000x PEL |
| Supplied-air respirator (SAR) — half-face | 10 | Airline connected to compressor |
| SAR — full-face, pressure-demand | 1,000 | Up to 1,000x PEL |
| Self-contained breathing apparatus (SCBA) — pressure-demand | 10,000 | IDLH atmospheres; oxygen-deficient (<19.5%) |
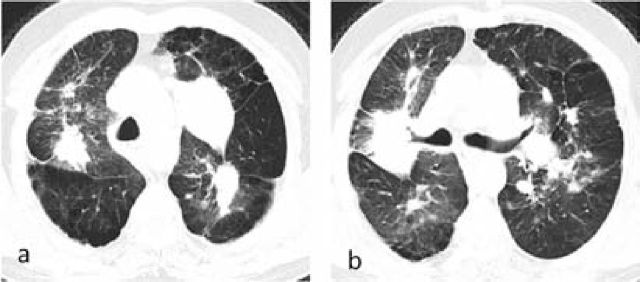
The maximum use concentration (MUC) = APF x OEL. For example, an N95 respirator (APF = 10) provides protection up to 10 times the PEL. If the PEL for a substance is 1 ppm, the N95 can be used up to 10 ppm. Above that level, a higher-protection respirator is required.
N95 vs. P100 vs. PAPR
N95 — filters ≥95% of non-oil-based aerosols ≥0.3 micrometers; standard for TB/respiratory infection control. N99 — filters ≥99%. P100 — filters ≥99.97% of all aerosols including oil-based; used for asbestos, lead, radionuclides. PAPR — uses a battery-powered blower to push air through filters, providing positive pressure inside the facepiece; does not require fit testing if loose-fitting; preferred for workers with facial hair, claustrophobia, or cardiopulmonary limitations.
IDLH Conditions
IDLH (Immediately Dangerous to Life or Health) — an atmosphere that poses an immediate threat to life, would cause irreversible health effects, or would impair the ability to escape. In IDLH atmospheres, only full-face pressure-demand SCBA or a combination full-face pressure-demand SAR with escape SCBA is permitted. IDLH values are established by NIOSH for individual chemicals (e.g., carbon monoxide IDLH = 1,200 ppm; hydrogen sulfide IDLH = 100 ppm).
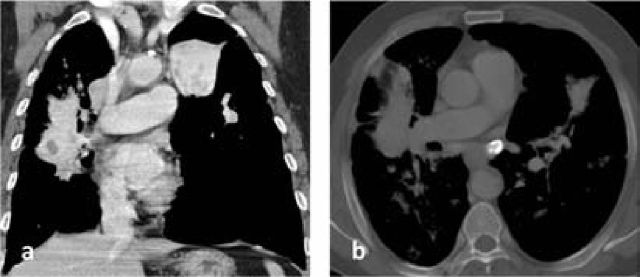
Chemical Cartridge Change-Out Schedules
Air-purifying respirators with chemical cartridges have finite service life. Cartridges do not filter forever — they become saturated ("breakthrough") and allow contaminant to pass through. OSHA requires employers to develop a change-out schedule based on the contaminant identity, concentration, humidity, breathing rate, and cartridge type. End-of-service-life indicators (ESLI) are available for some cartridges; otherwise, mathematical models or manufacturer data must be used. Conservative approach: change cartridges at the end of each shift or at the first detection of odor/taste.
21 Travel & International Occupational Health
Pre-Travel Evaluation
Workers deployed internationally require pre-travel medical assessment including: review of chronic medical conditions and stability for travel, baseline physical examination, dental clearance (for remote assignments), mental health screening, review of current medications (including availability at destination), and assessment of fitness for assignment-specific physical demands. Pre-travel evaluation should occur 4-6 weeks before departure to allow time for immunizations.
Immunizations by Region
| Vaccine | Indications | Schedule Notes |
|---|---|---|
| Yellow Fever | Sub-Saharan Africa, tropical South America; required for entry to some countries | Single dose; valid for life (per WHO 2016); must be given at approved vaccination center |
| Typhoid | South Asia, Southeast Asia, Africa, Latin America | Injectable (Vi polysaccharide) — 2 years; Oral (Ty21a) — 5 years |
| Hepatitis A | All developing countries | 2 doses, 6-12 months apart; long-term protection |
| Japanese Encephalitis | Rural Asia, Southeast Asia, Pacific | 2 doses, 28 days apart; booster at 1 year if ongoing risk |
| Meningococcal ACWY | Sub-Saharan Africa "meningitis belt"; Hajj requirement | Single dose; revaccinate every 5 years if ongoing risk |
| Rabies (pre-exposure) | Remote areas with limited PEP access; animal workers | 3 doses (days 0, 7, 21-28); simplifies post-exposure management |
| Cholera (oral) | Outbreak settings; humanitarian workers | 2 doses, 1-6 weeks apart (Vaxchora in US — single dose) |
Malaria Prophylaxis
Choice of prophylactic agent depends on destination resistance patterns, duration of stay, and patient factors. Atovaquone-proguanil (Malarone) — start 1-2 days before, continue 7 days after; preferred for short trips, well tolerated. Doxycycline — start 1-2 days before, continue 28 days after; also provides protection against rickettsial infections and leptospirosis; photosensitivity is a common side effect. Mefloquine — weekly dosing; start 2-3 weeks before; contraindicated in seizure disorders, psychiatric conditions, cardiac conduction abnormalities. Tafenoquine — weekly dosing during travel, loading dose before departure; requires G6PD testing (contraindicated in G6PD deficiency due to hemolytic risk). All travelers to endemic areas should also use mosquito avoidance measures (DEET/permethrin, bed nets, long sleeves/pants during dusk and dawn).
Altitude Illness
Acute Mountain Sickness (AMS) — headache plus at least one of: nausea/vomiting, fatigue, dizziness, insomnia. Onset 6-12 hours after arrival above 2,500 m. Lake Louise Score ≥3 with headache = diagnosis. Treatment: stop ascent, rest, acetazolamide 250 mg BID, analgesics; descend if worsening. High-Altitude Cerebral Edema (HACE) — ataxia and/or altered consciousness in the setting of AMS. Medical emergency: immediate descent, dexamethasone 8 mg then 4 mg q6h, supplemental O2, portable hyperbaric chamber if descent impossible. High-Altitude Pulmonary Edema (HAPE) — dyspnea at rest, cough (may be productive with pink frothy sputum), tachycardia, cyanosis. Most common cause of death from altitude illness. Treatment: immediate descent (most effective), supplemental O2, nifedipine 30 mg SR q12h.
Medical Evacuation & Remote Site Medicine
International occupational health programs must address medical evacuation planning: identification of nearest adequate medical facilities, air evacuation resources and response times, communication protocols, stabilization capabilities at the remote site, and contractual arrangements with evacuation providers. Remote sites should maintain medical capability proportional to risk: at minimum a trained first-aider with first-aid kit; higher-risk operations may require a paramedic, nurse, or physician with advanced life support capability.
Repatriation & Post-Assignment Evaluation
Workers returning from international assignments should undergo a post-assignment medical evaluation including: screening for endemic infectious diseases based on region of deployment (malaria smears, stool ova and parasites, schistosomiasis serology, TB screening), assessment of mental health (adjustment disorder, post-traumatic stress, repatriation stress syndrome), review of any illnesses or injuries sustained during assignment, and comparison of post-assignment biometrics to pre-deployment baseline values.
22 Workers' Compensation & Medicolegal
No-Fault System Principles
Workers' compensation is the exclusive remedy for work-related injuries and illnesses in most jurisdictions. The worker does not need to prove employer negligence; in return, the worker generally cannot sue the employer in tort. Exceptions to exclusive remedy may include intentional employer misconduct, third-party liability (equipment manufacturer), and dual-capacity doctrine (employer also acts as physician/landlord). Each state administers its own workers' compensation system; there is no single federal workers' compensation system (except for federal employees under FECA, longshore/harbor workers under LHWCA, and coal miners under the Black Lung Benefits Act).
Causation Analysis — Work-Relatedness
The occupational medicine physician must determine whether a condition is causally related to work. Levels of causation:
- Direct cause — the workplace exposure is the sole or predominant cause (e.g., occupational asthma from diisocyanates in a previously healthy worker).
- Aggravation — a pre-existing condition is permanently worsened by work activities (e.g., pre-existing mild knee arthritis permanently worsened by occupational kneeling).
- Exacerbation — a pre-existing condition is temporarily worsened by work activities but returns to baseline after cessation (e.g., carpal tunnel syndrome symptoms temporarily worsened by assembly work, improving with restricted duty).
- Apportionment — dividing the cause of impairment between occupational and non-occupational factors (e.g., 60% occupational, 40% degenerative).
Independent Medical Examination (IME)
An IME is a non-treating evaluation performed at the request of an insurance carrier, employer, or attorney. The IME physician must:
- Review all medical records, imaging, and test results.
- Obtain a thorough history (occupational, medical, social).
- Perform a focused physical examination.
- Address specific questions posed by the requesting party (diagnosis, causation, treatment reasonableness, MMI, impairment rating, restrictions).
- Provide an objective, evidence-based written report.
- Disclose the non-treatment nature of the examination to the examinee.
Impairment vs. Disability
Impairment is a medical determination — an alteration of health status assessed and rated by a physician using the AMA Guides (or other system as required by jurisdiction). Disability is an administrative/legal determination — the gap between what a person can do (functional capacity, as limited by impairment) and what the person needs to do (job demands, activities of daily living). The same impairment may produce different disability depending on the individual's occupation and circumstances.
Benefits Structure
Workers' compensation benefits fall into several categories, each with specific calculation methods that vary by state:
| Benefit Type | Description | Calculation Basis | Typical Duration |
|---|---|---|---|
| Medical treatment | All reasonable and necessary medical care related to the work injury | Fee schedule (state-specific); no copays or deductibles | Until MMI or as long as causally related treatment is needed |
| Temporary Total Disability (TTD) | Wage replacement when worker is completely unable to work | Typically 66.7% of average weekly wage (AWW), subject to state min/max | Until return to work or MMI |
| Temporary Partial Disability (TPD) | Wage differential when worker returns to modified duty at reduced pay | Typically 66.7% of wage difference (pre-injury vs. current earnings) | Until full duty or MMI |
| Permanent Partial Disability (PPD) | Compensation for permanent impairment after MMI | Based on impairment rating (AMA Guides or state schedule), AWW, and age | Lump sum or scheduled payments per state formula |
| Permanent Total Disability (PTD) | Worker permanently unable to return to any gainful employment | Typically 66.7% of AWW, subject to state max | Lifetime in most states (some have caps) |
| Vocational rehabilitation | Job retraining, education, job placement assistance | State-specific; may include maintenance allowance | Typically 1-2 years |
Fraud Indicators
Red flags for potential workers' compensation fraud include: injury claimed without witnesses, delayed reporting, history inconsistent with mechanism, examination findings inconsistent with reported symptoms, symptom magnification/Waddell signs, non-compliance with treatment while maintaining disability status, extensive prior claims history, and surveillance evidence of activity inconsistent with reported limitations. However, these are indicators warranting further investigation — not diagnoses of fraud.
Claims Process Timeline
Understanding the typical workers' compensation claims trajectory helps the occupational medicine physician anticipate decision points and documentation needs:
- Day 0 — Injury occurrence — employee reports injury to supervisor; first aid rendered; employer completes First Report of Injury (FROI) and files with carrier (24-72 hours per state law).
- Days 1-3 — Initial medical evaluation — authorized treating physician evaluates, documents history/exam/diagnosis, determines work status (full duty, modified duty, or off work), initiates treatment.
- Weeks 1-4 — Active treatment phase — follow-up visits, therapy, diagnostic workup as needed; periodic work status updates to employer and carrier; transitional duty assignment if applicable.
- Weeks 4-12 — Reassessment — if not recovering as expected, reassess diagnosis (missed pathology?), consider specialist referral, identify psychosocial barriers, ensure treatment is evidence-based.
- Months 3-6+ — MMI determination — once condition plateaus, declare MMI, perform impairment rating, establish permanent restrictions. If disputes arise, IME may be requested.
- Post-MMI — Settlement / closure — PPD benefits calculated; vocational rehabilitation if unable to return to prior job; case closure or ongoing medical maintenance if authorized.
23 Workplace Wellness Programs
Health Risk Assessment (HRA)
The HRA is a questionnaire-based tool that evaluates individual health risks including lifestyle factors (diet, exercise, smoking, alcohol), family history, psychosocial stressors, and biometric data (BP, BMI, lipids, glucose). It serves as the foundation for targeted interventions and program planning. HRAs must comply with ADA, GINA, and HIPAA requirements — employee participation must be voluntary, data must be de-identified for aggregate reporting, and incentive structures must not be coercive.
Biometric Screening
Common biometric measures include: blood pressure, BMI/waist circumference, fasting lipid panel, fasting glucose or HbA1c, and nicotine/cotinine testing. Aggregate results identify population-level health risks and inform program design. Individual results are shared confidentially with the employee along with educational resources and referral pathways. Screening programs must balance sensitivity (detecting at-risk individuals) with positive predictive value (avoiding false alarms that generate unnecessary anxiety and follow-up costs). Follow-up pathways should be clearly established — abnormal results require a defined mechanism for referral to primary care or specialist evaluation.
Core Wellness Initiatives
- Tobacco cessation — multi-component programs (counseling, pharmacotherapy access, policy support) achieve quit rates of 20-30%; essential given that smoking is the leading preventable cause of death.
- Physical activity — on-site fitness facilities, subsidized gym memberships, walking programs, standing/treadmill desks; CDC recommends 150 min/week moderate or 75 min/week vigorous activity.
- Nutrition — healthy cafeteria options, vending machine standards, educational programs, weight management support.
- Stress management — mindfulness-based stress reduction (MBSR), resilience training, flexible work arrangements, workload management.
Employee Assistance Programs (EAP)
EAPs provide confidential, short-term counseling and referral services for employees dealing with personal problems that may affect work performance — substance abuse, mental health issues, family/relationship problems, financial difficulties, and grief. Typically funded by the employer and provided at no cost to employees. EAP utilization rates average 5-8% of the workforce annually, though availability of services is broader. Critical incident stress debriefing (CISD) after traumatic workplace events is often coordinated through EAPs.
Mental Health in the Workplace
Burnout — characterized by emotional exhaustion, depersonalization (cynicism), and reduced personal accomplishment. Risk factors include excessive workload, lack of autonomy, insufficient reward, breakdown of community, absence of fairness, and values conflict. Healthcare workers, first responders, and teachers are particularly vulnerable. Organizational interventions (workload reduction, schedule flexibility, peer support) are more effective than individual-level interventions alone.
Shift Work & Circadian Disruption
Shift work disorder affects 10-40% of shift workers and manifests as excessive sleepiness during work hours and/or insomnia during the designated sleep period. Chronic circadian disruption from rotating or night shifts is associated with increased risk of cardiovascular disease, metabolic syndrome, type 2 diabetes, gastrointestinal disorders, depression, and breast cancer (IARC Group 2A — "probably carcinogenic"). Management strategies include:
- Shift scheduling — forward rotation (day → evening → night) is better tolerated than backward rotation; limit consecutive night shifts to 3-4; allow at least 11 hours between shifts; avoid permanent night shifts unless worker preference.
- Light exposure — bright light exposure during the first half of the night shift promotes circadian adaptation; dark sunglasses on the commute home reduce re-entrainment to the day.
- Strategic napping — a 20-30 minute nap during breaks improves alertness and performance; naps before a night shift ("prophylactic nap") reduce fatigue.
- Pharmacotherapy — melatonin 0.5-3 mg before daytime sleep can improve sleep quality; modafinil or armodafinil may be used for excessive shift-work sleepiness (FDA-approved indication).
The CDC Workplace Health Model provides a systematic four-step framework: (1) Assessment — organizational, individual, and community health data; (2) Planning — setting goals, identifying evidence-based interventions, aligning with organizational priorities; (3) Implementation — health education, supportive social/physical environments, policy change, integration with existing programs; (4) Evaluation — process, impact, and outcome measures. Evidence suggests well-designed workplace wellness programs can reduce health care costs by $3-6 per dollar invested, though ROI estimates vary widely.
24 Infection Control in Occupational Settings
Healthcare Worker (HCW) Screening
Pre-employment and ongoing screening for HCWs includes:
- Tuberculosis — baseline TST (two-step) or IGRA (QuantiFERON-TB Gold Plus or T-SPOT); annual screening for those with potential TB exposure. Positive result requires CXR to exclude active TB. Latent TB treatment (rifampin 4 months or isoniazid/rifapentine 3 months) is recommended per CDC/ATS guidelines.
- Immunizations — Hepatitis B series with documented anti-HBs ≥10 mIU/mL; MMR (2 doses or immunity by titer); Varicella (2 doses or immunity by titer); Tdap (1 dose, then Td q10 years); annual influenza; COVID-19 per current CDC recommendations.
- Measles/mumps/rubella — HCWs born in 1957 or later without 2 documented doses or serologic immunity require vaccination. HCWs are considered a high-risk group for measles transmission.
Latex Allergy Management
Type I (IgE-mediated) — immediate hypersensitivity to natural rubber latex proteins. Symptoms range from contact urticaria to anaphylaxis. Risk factors: frequent glove use (healthcare, rubber industry), atopy, spina bifida patients (multiple surgeries). Management: complete latex avoidance (non-latex gloves — nitrile preferred), latex-safe environment designation, epinephrine auto-injector availability. Type IV (delayed) — allergic contact dermatitis to rubber accelerators (thiurams, carbamates). Patch testing confirms the diagnosis. Management: avoidance of specific accelerator; accelerator-free gloves.
Hand Hygiene Compliance
Hand hygiene is the single most important measure for preventing healthcare-associated infections. WHO "5 Moments for Hand Hygiene": (1) before patient contact, (2) before aseptic task, (3) after body fluid exposure, (4) after patient contact, (5) after touching patient surroundings. Alcohol-based hand rub (ABHR) is preferred for routine decontamination unless hands are visibly soiled (then soap and water). ABHR is NOT effective against Clostridioides difficile spores or norovirus — soap and water required.
Occupational Dermatitis — Contact Dermatitis
Occupational skin disease accounts for approximately 15-20% of all occupational illnesses, with contact dermatitis being the most common form. Two types predominate:

- Irritant contact dermatitis (ICD) — accounts for ~80% of occupational contact dermatitis. Caused by direct chemical damage to the skin barrier. Common irritants: soaps/detergents, solvents, cutting oils, wet work, cement (alkaline), acids. Presentation: erythema, scaling, fissuring, often on hands and forearms. Does NOT require prior sensitization — any worker with sufficient exposure can develop ICD. Healthcare workers who wash hands >20 times/day are at particularly high risk.
- Allergic contact dermatitis (ACD) — type IV delayed hypersensitivity reaction requiring prior sensitization. Common occupational allergens: nickel (metalworkers), epoxy resins (construction, electronics), chromates (cement workers, leather tanners), rubber accelerators (thiurams, carbamates in gloves), p-phenylenediamine (hair dressers), formaldehyde/preservatives (healthcare, cosmetics). Diagnosis: patch testing with a standard series and workplace-specific allergens is the gold standard. Treatment: strict avoidance of the allergen, barrier creams, topical corticosteroids, emollients for skin barrier restoration.
Pandemic Preparedness
Occupational health plays a central role in pandemic response: surge respiratory protection programs, fit testing and PAPR deployment, employee health screening and clearance, exposure tracking and contact tracing, vaccine administration campaigns, return-to-work protocols for infected employees, psychological support for frontline workers, and policy guidance on essential worker classifications.
Return-to-Work After Infectious Illness
Occupational health must establish evidence-based criteria for returning healthcare and other workers to duty after communicable illness:
| Illness | Return-to-Work Criteria | Special Considerations |
|---|---|---|
| Influenza | Afebrile for ≥24 hours without antipyretics; improving symptoms | Consider antiviral treatment (oseltamivir) for HCWs to shorten exclusion period |
| COVID-19 | Per current CDC guidance (symptom-based or test-based approach); typically ≥5 days from symptom onset with improving symptoms and afebrile ≥24 hours | Masking for additional days after return; immunocompromised workers may require longer isolation |
| Norovirus / acute gastroenteritis | Symptom-free for ≥48 hours (food handlers may require longer exclusion or negative stool testing) | Strict hand hygiene with soap and water (ABHR ineffective against norovirus) |
| Active tuberculosis | Three consecutive negative AFB sputum smears collected 8-24 hours apart; on effective therapy; clinical improvement documented | Coordinated with public health department; contact investigation for exposed coworkers |
| Varicella (chickenpox) | All lesions crusted over (typically 5-7 days after rash onset) | Susceptible exposed HCWs furloughed days 8-21 post-exposure (or given PEP vaccine within 5 days) |
| Pertussis | After 5 days of appropriate antibiotic therapy (azithromycin) | Unvaccinated/under-vaccinated coworkers may require PEP (azithromycin) |
Biosafety Levels (BSL)
| Level | Agents | Practices/Equipment | Facility |
|---|---|---|---|
| BSL-1 | Not known to cause disease in healthy adults (e.g., non-pathogenic E. coli) | Standard microbiological practices; no special equipment | Open bench; sink required |
| BSL-2 | Moderate hazard; associated with human disease (e.g., HIV, hepatitis, Staphylococcus aureus) | BSL-1 + limited access, biohazard signs, sharps precautions, BSC for aerosol-generating procedures | Autoclave available; self-closing doors |
| BSL-3 | Indigenous/exotic agents with potential for aerosol transmission (e.g., M. tuberculosis, SARS-CoV-2, Coxiella burnetii) | BSL-2 + respiratory protection, all work in BSC or sealed equipment, decontamination of all waste | Negative pressure; sealed entries; HEPA-filtered exhaust |
| BSL-4 | Dangerous/exotic agents posing high risk of life-threatening disease; no vaccine/treatment (e.g., Ebola, Marburg, smallpox) | BSL-3 + positive-pressure suits OR Class III BSC line; all materials decontaminated on exit | Isolated building or zone; dedicated air/vacuum; decontamination shower |
25 OSHA PEL & ACGIH TLV Reference Table
| Substance | OSHA PEL (8-hr TWA) | ACGIH TLV (8-hr TWA) | NIOSH REL | IDLH | Primary Hazard |
|---|---|---|---|---|---|
| Asbestos | 0.1 f/cc | 0.1 f/cc | 0.1 f/cc | N/A | Asbestosis, mesothelioma, lung CA |
| Benzene | 1 ppm | 0.5 ppm | 0.1 ppm | 500 ppm | Leukemia, aplastic anemia |
| Carbon monoxide | 50 ppm | 25 ppm | 35 ppm | 1,200 ppm | CO-Hb, cardiac ischemia |
| Formaldehyde | 0.75 ppm (STEL 2 ppm) | 0.3 ppm (C) | 0.016 ppm | 20 ppm | NPC, leukemia, irritation |
| Hydrogen sulfide | 20 ppm (C) | 1 ppm (STEL 5 ppm) | 10 ppm (C) | 100 ppm | Olfactory fatigue, sudden death |
| Lead (inorganic) | 50 mcg/m3 | 50 mcg/m3 | 50 mcg/m3 | 100 mg/m3 | Encephalopathy, neuropathy, nephropathy |
| Mercury (inorganic) | 0.1 mg/m3 (C) | 0.025 mg/m3 | 0.05 mg/m3 | 10 mg/m3 | Nephrotoxicity, neurotoxicity |
| Methylene chloride | 25 ppm | 50 ppm | Lowest feasible | 2,300 ppm | CO-Hb (metabolized to CO), CNS |
| Nitrogen dioxide | 5 ppm (C) | 0.2 ppm | 1 ppm (STEL) | 20 ppm | Pulmonary edema (silo filler's disease) |
| Silica (crystalline quartz) | 50 mcg/m3 | 25 mcg/m3 | 50 mcg/m3 | 50 mg/m3 | Silicosis, lung CA, TB susceptibility |
| Toluene | 200 ppm | 20 ppm | 100 ppm | 500 ppm | CNS depression, encephalopathy |
| Trichloroethylene | 100 ppm | 10 ppm | 25 ppm (C) | 1,000 ppm | Hepatotoxicity, renal CA |
| Vinyl chloride | 1 ppm | 1 ppm | Lowest feasible | N/A | Hepatic angiosarcoma |
| Cadmium | 5 mcg/m3 | 10 mcg/m3 (inhalable) | Lowest feasible | 9 mg/m3 | Lung CA, nephrotoxicity, osteomalacia |
| Chromium VI | 5 mcg/m3 | 20 mcg/m3 | 1 mcg/m3 | 15 mg/m3 | Lung CA, nasal septum perforation |
| Ammonia | 50 ppm | 25 ppm (STEL 35 ppm) | 25 ppm | 300 ppm | Respiratory irritation, chemical burns |
| Ethylene oxide | 1 ppm | 1 ppm | 0.1 ppm (C) | 800 ppm | Lymphoid/breast CA, neuropathy |
26 Medical Surveillance Requirements by Substance
| OSHA Standard | Substance | Action Level (AL) / PEL | Medical Exam Trigger | Exam Components | Frequency | Special Provisions |
|---|---|---|---|---|---|---|
| 1910.1001 | Asbestos | AL: 0.1 f/cc; PEL: 0.1 f/cc | Exposure at or above AL for 30+ days/year | History, exam, CXR (ILO), PFTs (FVC, FEV1) | Pre-placement, annual, termination | CXR at baseline, then per B-reader/physician; annual if ≥10 yrs from onset of exposure |
| 1910.1025 | Lead | AL: 30 mcg/m3; PEL: 50 mcg/m3 | Exposure at or above AL for >30 days/year | BLL, ZPP, CBC, BUN, creatinine, history/exam | Pre-placement; BLL q6 months (q2 months if BLL ≥40) | Medical removal at BLL ≥50; MRP until BLL <40 x2 |
| 1910.1028 | Benzene | AL: 0.5 ppm; PEL: 1 ppm | Exposure at or above AL for 30+ days/year | CBC with differential, history/exam | Pre-placement, annual | Additional exam if any component >normal; referral for hematologic abnormality |
| 1910.1027 | Cadmium | AL: 2.5 mcg/m3; PEL: 5 mcg/m3 | Exposure at or above AL | Blood Cd, urine Cd, beta-2-microglobulin, CBC, BUN, creatinine, PFTs, CXR | Pre-placement, annual | Biologic monitoring triggers for additional exams; medical removal provisions |
| 1910.1026 | Hexavalent Chromium | AL: 2.5 mcg/m3; PEL: 5 mcg/m3 | Exposure at or above AL for 30+ days/year | History, exam (skin, respiratory), CXR (baseline), PFTs | Within 30 days, annual | Exam of skin and respiratory tract; nasal septum evaluation |
| 1910.1048 | Formaldehyde | AL: 0.5 ppm; PEL: 0.75 ppm | Exposure at or above AL or STEL | History, exam (respiratory, dermal), PFTs | Pre-placement, annual if symptomatic/sensitized | Medical removal for respiratory sensitization or dermatitis |
| 1910.95 | Noise | AL: 85 dBA TWA | Exposure at or above AL | Audiometry (500-8000 Hz) | Baseline (within 6 months), annual | 14-hr quiet before baseline; STS triggers notification/intervention |
| 1910.1052 | Methylene Chloride | AL: 12.5 ppm; PEL: 25 ppm | Exposure at or above AL for 30+ days/year | History/exam, CBC, COHb or end-exhaled CO, liver/renal panel | Pre-placement, periodic per physician | Emergency exposure exam within 48 hrs; cardiac risk assessment |
27 ILO Classification for Chest Radiographs
The ILO International Classification of Radiographs of Pneumoconioses (revised 2011) is a standardized system for systematically describing and recording radiographic abnormalities caused by inhaled dusts. B-readers are physicians who have passed the NIOSH-administered certification examination in ILO classification. B-reading is required for OSHA-mandated asbestos and coal dust surveillance.
Small Opacities
Profusion (Concentration/Density)
Profusion is the concentration of small opacities in the lung fields, graded on a 12-point scale by comparison with standard radiographs:
| Major Category | Subcategories | Interpretation |
|---|---|---|
| 0 (Normal) | 0/-, 0/0, 0/1 | No or very few opacities; 0/1 = few opacities but not enough for category 1 |
| 1 (Low profusion) | 1/0, 1/1, 1/2 | Opacities definitely present but few in number; underlying lung markings usually visible |
| 2 (Moderate) | 2/1, 2/2, 2/3 | Numerous opacities; lung markings partially obscured |
| 3 (High profusion) | 3/2, 3/3, 3/+ | Very numerous opacities; lung markings totally obscured |
The notation uses the format "definite/alternative" — e.g., 2/1 means category 2 was seriously considered (definite) but category 1 was the alternative.
Shape and Size of Small Opacities
| Type | Shape | Size Code | Diameter |
|---|---|---|---|
| Rounded | Round or nearly round | p | ≤1.5 mm |
| Rounded | Round or nearly round | q | 1.5-3 mm |
| Rounded | Round or nearly round | r | 3-10 mm |
| Irregular | Linear, reticular | s | ≤1.5 mm width |
| Irregular | Linear, reticular | t | 1.5-3 mm width |
| Irregular | Linear, reticular | u | 3-10 mm width |
Silicosis and CWP typically produce rounded (p, q, r) opacities. Asbestosis produces irregular (s, t, u) opacities. The primary and secondary shapes/sizes are recorded (e.g., "q/q" = predominantly type q rounded opacities).

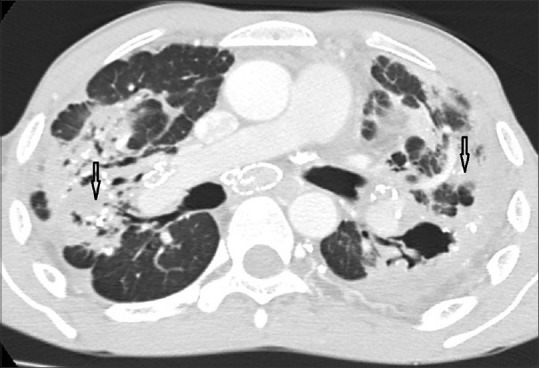
Large Opacities
| Category | Description |
|---|---|
| A | Single opacity or combined opacities with greatest dimension >10 mm and ≤50 mm |
| B | Single or combined opacities >50 mm but total area does not exceed right upper zone |
| C | Single or combined opacities exceeding the equivalent area of the right upper zone |
Pleural Abnormalities
Pleural thickening is classified by: site (chest wall, diaphragm, costophrenic angle obliteration); width (a: ≤5 mm, b: 5-10 mm, c: >10 mm for in-profile plaques); extent (total length along the lateral chest wall); and calcification (present or absent, by site). Diffuse pleural thickening is distinguished from plaques (circumscribed). Costophrenic angle obliteration is recorded separately and indicates more extensive disease.
Additional Symbols
Twenty-five defined symbols allow recording of additional findings, including: aa (atherosclerotic aorta), at (rounded atelectasis), ax (coalescence), bu (bulla), ca (cancer), cn (calcification in small opacities), co (abnormal cardiac silhouette), ef (effusion), em (emphysema), es (eggshell calcification), hi (hilar enlargement), ho (honeycomb lung), tb (tuberculosis), and others.
28 Abbreviations Master List
| Abbreviation | Full Term |
|---|---|
| ACGIH | American Conference of Governmental Industrial Hygienists |
| ADA | Americans with Disabilities Act |
| AMA | American Medical Association |
| AMS | Acute Mountain Sickness |
| APF | Assigned Protection Factor |
| BAL | British Anti-Lewisite (dimercaprol) |
| BBP | Bloodborne Pathogens |
| BEI | Biological Exposure Index |
| BeLPT | Beryllium Lymphocyte Proliferation Test |
| BLL | Blood Lead Level |
| BSL | Biosafety Level |
| CaNa2EDTA | Calcium Disodium Ethylenediaminetetraacetic Acid |
| CBD | Chronic Beryllium Disease |
| CMV | Commercial Motor Vehicle |
| CPAP | Continuous Positive Airway Pressure |
| CSE | Chronic Solvent Encephalopathy |
| CWP | Coal Workers' Pneumoconiosis |
| dBA | Decibels, A-weighted |
| DBI | Diagnosis-Based Impairment |
| DLCO | Diffusing Capacity of the Lungs for Carbon Monoxide |
| DMSA | Dimercaptosuccinic Acid (Succimer) |
| DOT | Department of Transportation |
| EAP | Employee Assistance Program |
| ESLI | End-of-Service-Life Indicator |
| FCE | Functional Capacity Evaluation |
| FECA | Federal Employees' Compensation Act |
| FEP | Free Erythrocyte Protoporphyrin |
| FEV1 | Forced Expiratory Volume in 1 Second |
| FMCSA | Federal Motor Carrier Safety Administration |
| FROI | First Report of Injury |
| FVC | Forced Vital Capacity |
| GHS | Globally Harmonized System |
| HACE | High-Altitude Cerebral Edema |
| HAPE | High-Altitude Pulmonary Edema |
| HAVS | Hand-Arm Vibration Syndrome |
| HBIG | Hepatitis B Immune Globulin |
| HBsAg | Hepatitis B Surface Antigen |
| HCP | Hearing Conservation Program |
| HCW | Healthcare Worker |
| HHE | Health Hazard Evaluation |
| HP | Hypersensitivity Pneumonitis |
| HRA | Health Risk Assessment |
| HRCT | High-Resolution Computed Tomography |
| IARC | International Agency for Research on Cancer |
| IDLH | Immediately Dangerous to Life or Health |
| IGRA | Interferon-Gamma Release Assay |
| ILO | International Labour Organization |
| IME | Independent Medical Examination |
| IPF | Idiopathic Pulmonary Fibrosis |
| LHWCA | Longshore and Harbor Workers' Compensation Act |
| LI | Lifting Index |
| LLN | Lower Limit of Normal |
| MAC | Mycobacterium avium Complex |
| MBSR | Mindfulness-Based Stress Reduction |
| MDS | Myelodysplastic Syndrome |
| MMI | Maximum Medical Improvement |
| MRO | Medical Review Officer |
| MRP | Medical Removal Protection |
| MUC | Maximum Use Concentration |
| NIHL | Noise-Induced Hearing Loss |
| NIOSH | National Institute for Occupational Safety and Health |
| NRR | Noise Reduction Rating |
| OA | Occupational Asthma |
| OEL | Occupational Exposure Limit |
| OEM | Occupational and Environmental Medicine |
| OSHA | Occupational Safety and Health Administration |
| OSH Act | Occupational Safety and Health Act of 1970 |
| PAPR | Powered Air-Purifying Respirator |
| PEF | Peak Expiratory Flow |
| PEL | Permissible Exposure Limit |
| PEP | Post-Exposure Prophylaxis |
| PFT | Pulmonary Function Test |
| PLHCP | Physician or Other Licensed Health Care Professional |
| PMF | Progressive Massive Fibrosis |
| PPD | Permanent Partial Disability |
| PPE | Personal Protective Equipment |
| PTD | Permanent Total Disability |
| RADS | Reactive Airways Dysfunction Syndrome |
| REL | Recommended Exposure Limit |
| ROI | Return on Investment |
| RTW | Return to Work |
| RWL | Recommended Weight Limit |
| SAP | Substance Abuse Professional |
| SAR | Supplied-Air Respirator |
| SCBA | Self-Contained Breathing Apparatus |
| SDS | Safety Data Sheet |
| SIC | Specific Inhalation Challenge |
| STEL | Short-Term Exposure Limit |
| STS | Standard Threshold Shift |
| TLV | Threshold Limit Value |
| TPD | Temporary Partial Disability |
| TST | Tuberculin Skin Test |
| TTD | Temporary Total Disability |
| TWA | Time-Weighted Average |
| TWH | Total Worker Health |
| WBGT | Wet Bulb Globe Temperature |
| WHO | World Health Organization |
| WMSD | Work-Related Musculoskeletal Disorder |
| ZPP | Zinc Protoporphyrin |