Podiatry
Foot and ankle anatomy, biomechanics, diabetic foot care, bunion and hammertoe correction, plantar fasciitis, nail disorders, sports injuries, and every classification system, surgical technique, and management algorithm across the full scope of podiatric medicine and surgery.
01 Foot & Ankle Anatomy
The foot and ankle constitute one of the most complex mechanical structures in the human body, containing 26 bones, 33 joints, 107 ligaments, and 19 intrinsic muscles, all working in concert to absorb shock, adapt to terrain, and provide a rigid lever for propulsion. A thorough understanding of this anatomy is the foundation of all podiatric diagnosis and treatment.
Bones of the Foot
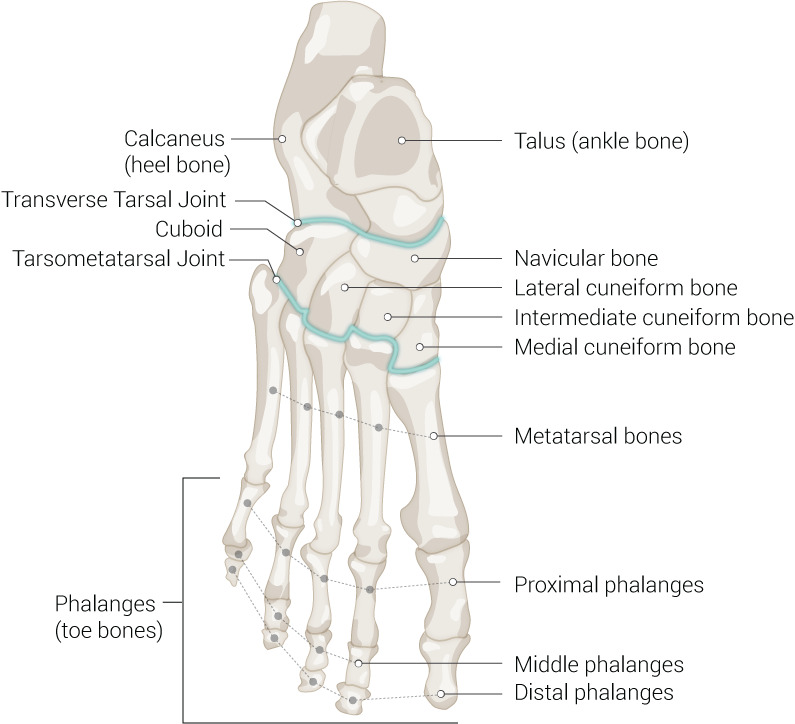
The 26 bones are divided into three functional groups:
Hindfoot (2 bones) — The talus (trochlea articulates with the tibial plafond and malleoli, forming the ankle mortise; inferiorly articulates with calcaneus at the subtalar joint; anteriorly with navicular at the talonavicular joint) and the calcaneus (largest tarsal bone, bears the body’s weight in stance; posterior tuberosity receives the Achilles tendon insertion; sustentaculum tali supports the talar neck medially; anterior process articulates with cuboid). The calcaneus has a normal Bohler angle of 20–40°; loss of this angle suggests compression fracture.
Midfoot (5 bones) — The navicular (keystone of the medial longitudinal arch; receives posterior tibialis insertion at the navicular tuberosity; blood supply is tenuous, predisposing to AVN/Kohler disease), the cuboid (lateral column, contains the peroneus longus groove on its plantar surface), and three cuneiforms: medial (largest, articulates with 1st metatarsal), intermediate (smallest, articulates with 2nd metatarsal — this recessed mortise configuration is key to Lisfranc joint stability), and lateral (articulates with 3rd metatarsal).
Forefoot (19 bones) — Five metatarsals (1st metatarsal is the shortest and thickest, bears approximately one-third of forefoot load via its two sesamoids; the 2nd metatarsal is typically the longest and most common site of stress fracture; the 5th metatarsal base has three distinct fracture zones). Fourteen phalanges — the hallux has two (proximal and distal) while digits 2–5 each have three (proximal, middle, distal). Two sesamoid bones (tibial/medial and fibular/lateral) are embedded within the flexor hallucis brevis tendons plantar to the 1st MTP joint, functioning as a fulcrum and weight-bearing surface.
Joints
Ankle (talocrural) joint — a hinge (ginglymus) joint formed by the tibial plafond, medial malleolus, and lateral malleolus (fibula) articulating with the talar dome. Primary motion: dorsiflexion (~20°) and plantarflexion (~50°). The mortise is wider anteriorly, so the ankle is inherently more stable in dorsiflexion than in plantarflexion (where inversion sprains most commonly occur).
Subtalar joint — the articulation between the inferior talus and superior calcaneus, composed of three facets (anterior, middle, posterior). Primary motion: inversion/eversion (combined with rotation, this produces pronation and supination). The axis of the subtalar joint is oriented 42° from the transverse plane and 16° from the sagittal plane.
Midtarsal (Chopart) joint — comprises the talonavicular and calcaneocuboid joints; allows forefoot adaptation to terrain. Functions as a “torque converter” between hindfoot and forefoot. When the subtalar joint pronates, the midtarsal joint axes become parallel, unlocking the midfoot (flexible, shock-absorbing). With supination, the axes diverge, locking the midfoot into a rigid lever for push-off.
Tarsometatarsal (Lisfranc) joint — articulation of the three cuneiforms and cuboid with the metatarsal bases. The Lisfranc ligament connects the medial cuneiform to the 2nd metatarsal base; there is no intermetatarsal ligament between the 1st and 2nd metatarsals, making this the weak link.
MTP joints — condyloid joints allowing flexion/extension, abduction/adduction. The plantar plate is a thick fibrocartilaginous structure on the plantar aspect; attenuation leads to predislocation syndrome and crossover toe. IP joints — hinge joints; the hallux has one (IPJ), digits 2–5 have proximal (PIPJ) and distal (DIPJ) interphalangeal joints.
Ligaments
Lateral ligament complex — (1) Anterior talofibular ligament (ATFL): weakest of the three, taut in plantarflexion, first to rupture in inversion sprains; (2) Calcaneofibular ligament (CFL): taut in dorsiflexion, crosses both ankle and subtalar joints, second to tear; (3) Posterior talofibular ligament (PTFL): strongest lateral ligament, rarely torn in isolation.
Deltoid (medial) ligament — a fan-shaped ligament with superficial (tibionavicular, tibiocalcaneal, posterior tibiotalar) and deep (anterior tibiotalar, deep posterior tibiotalar) components. The deep deltoid is the primary restraint against lateral talar shift; injury indicates significant trauma (often associated with fibula fracture — Weber B/C).
Spring (plantar calcaneonavicular) ligament — connects the sustentaculum tali to the navicular; supports the talar head and the medial longitudinal arch. Attenuation is a hallmark of adult-acquired flatfoot (PTTD Stage II+). The Lisfranc ligament runs from the medial cuneiform to the 2nd metatarsal base; disruption causes tarsometatarsal instability.
Tendons
Achilles tendon — the strongest tendon in the body, formed by the confluence of the gastrocnemius and soleus (triceps surae). Inserts on the posterior calcaneal tuberosity. Blood supply is relatively poor 2–6 cm proximal to insertion (the “watershed zone”), which is the most common site of rupture. The Thompson test (squeezing the calf with the patient prone; absent plantarflexion = positive = rupture) is the key clinical exam.
Posterior tibial tendon — the primary dynamic stabilizer of the medial longitudinal arch. Courses behind the medial malleolus, inserts on the navicular tuberosity, medial cuneiform, and bases of metatarsals 2–4. Dysfunction produces adult-acquired flatfoot deformity (AAFD). Anterior tibial tendon — the primary dorsiflexor of the ankle; inserts on the medial cuneiform and 1st metatarsal base.
Peroneal tendons — the peroneus longus courses beneath the cuboid to insert on the 1st metatarsal base and medial cuneiform (stabilizes the 1st ray); the peroneus brevis inserts on the 5th metatarsal base (primary evertor). Both tendons pass behind the lateral malleolus in the peroneal groove, held by the superior peroneal retinaculum. Retinacular injury leads to peroneal subluxation.
Plantar Fascia
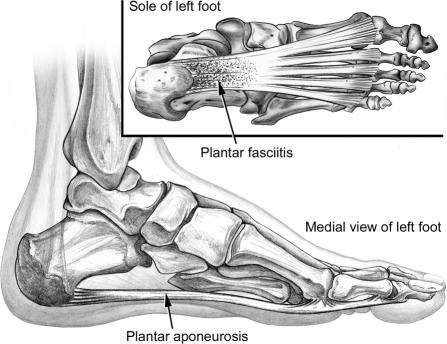
The plantar aponeurosis originates from the medial calcaneal tuberosity and fans distally to insert on the plantar plates and proximal phalanges of all five toes. It is the primary static support of the medial longitudinal arch. The windlass mechanism — dorsiflexion of the toes at the MTP joints tightens the plantar fascia, elevating the arch and converting the foot into a rigid lever for propulsion. This mechanism is tested clinically by dorsiflexing the hallux (Jack test).
Arches
Medial longitudinal arch — calcaneus → talus → navicular → cuneiforms → metatarsals 1–3. Highest arch; keystone = navicular. Supported by the spring ligament, posterior tibial tendon, and plantar fascia. Lateral longitudinal arch — calcaneus → cuboid → metatarsals 4–5. Lower, more rigid; keystone = cuboid. Transverse arch — formed by the cuneiforms and cuboid proximally and the metatarsal heads distally; the peroneus longus tendon and the deep transverse metatarsal ligament are critical supports.
Neurovascular Supply
Posterior tibial artery — passes behind the medial malleolus (palpable pulse point), enters the foot through the tarsal tunnel, and bifurcates into the medial and lateral plantar arteries. The lateral plantar artery forms the deep plantar arch (analogous to the hand). Dorsalis pedis artery — continuation of the anterior tibial artery on the dorsum of the foot, palpable between the 1st and 2nd metatarsal tendons. Assessment of both pulses is mandatory in diabetic foot evaluation.
Tibial nerve — passes through the tarsal tunnel (posterior to the medial malleolus) and divides into the medial plantar nerve (sensation to medial 3.5 digits and motor to intrinsic muscles — analogous to the median nerve in the hand) and the lateral plantar nerve (sensation to lateral 1.5 digits, motor to interossei and adductor hallucis — analogous to the ulnar nerve). Baxter nerve (first branch of the lateral plantar nerve) innervates the abductor digiti minimi and is a cause of chronic heel pain when entrapped.
Dermatomes — L4: medial foot and ankle; L5: dorsum of foot, 1st web space, lateral ankle; S1: lateral foot and sole, heel. The sural nerve (from S1-S2) supplies the lateral foot and is vulnerable during lateral ankle surgery. The superficial peroneal nerve (L5) supplies the dorsum of the foot except the 1st web space (deep peroneal nerve, L5).
02 Biomechanics & Gait Analysis
Gait analysis and lower-extremity biomechanics underpin diagnosis and treatment planning across podiatric medicine. Abnormal mechanics cause overuse injuries, deformity progression, and ulceration in the neuropathic foot.
The Gait Cycle
A complete gait cycle (stride) runs from one heel strike to the next heel strike of the same foot. It is divided into stance phase (~60% of the cycle) and swing phase (~40%). During walking, there is a period of double limb support at the beginning and end of stance; in running, a float phase replaces double support.
| Phase | % of Cycle | Key Events |
|---|---|---|
| Heel strike (initial contact) | 0% | Heel contacts ground; ankle at neutral; subtalar joint begins pronation to absorb shock |
| Foot flat (loading response) | 0–12% | Entire foot on ground; forefoot loads; tibialis anterior eccentrically controls plantarflexion; midtarsal joint unlocked (pronation) |
| Midstance | 12–31% | Body passes over the foot; subtalar joint begins resupinating; posterior tibial tendon active; single-limb support begins |
| Heel off (terminal stance) | 31–50% | Heel rises; windlass mechanism engages; midtarsal joint locks; forefoot becomes rigid lever |
| Toe off (pre-swing) | 50–62% | Propulsion via FHL and FDL; peak pressure under 1st and 2nd metatarsal heads; contralateral heel strikes |
| Initial swing | 62–75% | Foot clears ground; hip/knee flexion; ankle dorsiflexion begins |
| Mid-swing | 75–87% | Limb passes directly beneath body; foot clears ground |
| Terminal swing | 87–100% | Limb decelerates; knee extends; ankle dorsiflexed to neutral preparing for heel strike |
Pronation & Supination
Pronation is a triplanar motion consisting of calcaneal eversion, talar adduction, and talar plantarflexion. It unlocks the midtarsal joint, allowing the foot to adapt to uneven surfaces and absorb shock. Supination is the reverse: calcaneal inversion, talar abduction, and talar dorsiflexion. It locks the midfoot into a rigid lever for propulsion. Normal gait requires pronation at heel strike transitioning to supination by midstance–heel off.
Overpronation (excessive or prolonged pronation) is the single most common biomechanical abnormality seen in podiatric practice; it is associated with plantar fasciitis, posterior tibial tendon dysfunction, hallux valgus, medial tibial stress syndrome, and patellofemoral pain. Oversupination (underpronation) reduces shock absorption and is associated with lateral ankle instability, stress fractures, and peroneal tendinopathy.
Windlass Mechanism


Described by Hicks (1954): dorsiflexion of the MTP joints winds the plantar fascia around the metatarsal heads, shortening the distance between calcaneus and metatarsals, thereby raising the medial longitudinal arch, inverting the hindfoot, and externally rotating the leg. This converts the foot from a mobile adaptor to a rigid lever. Failure of the windlass mechanism (e.g., in hallux rigidus or plantar fascia rupture) impairs push-off efficiency.
Foot Types
Pes planus (flatfoot) — reduced or absent medial longitudinal arch; calcaneus everted (>6° valgus); associated with overpronation, PTTD, and medial column overload. Pes cavus — abnormally high arch; calcaneus inverted; rigid foot with poor shock absorption; associated with neurologic conditions (CMT, spinal dysraphism), lateral column overload, metatarsalgia, claw toes, and lateral ankle instability. Neutral foot — normal arch height, calcaneus near vertical (0–4° valgus); optimal mechanical alignment.
Angular Relationships (Radiographic)
| Angle | Normal Value | Measurement |
|---|---|---|
| Talocalcaneal (Kite angle) — AP | 20–40° | Angle between long axes of talus and calcaneus on AP view; increased in flatfoot, decreased in cavus |
| Talocalcaneal — Lateral | 25–50° | Same measurement on lateral view |
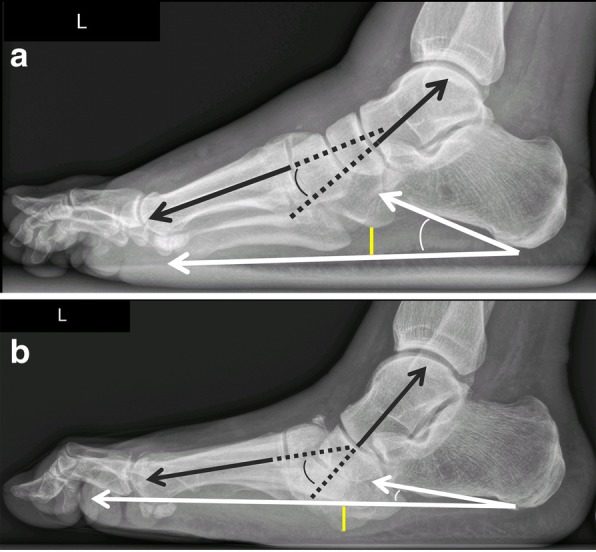
| Talo–1st metatarsal (Meary angle) — Lateral | 0° (collinear) | Angle between long axis of talus and 1st MT; apex dorsal = cavus; apex plantar = flatfoot |
| Calcaneal inclination angle | 18–25° | Angle between inferior calcaneal surface and horizontal; decreased in flatfoot, increased in cavus |
| Bohler angle | 20–40° | Angle formed by posterior facet of calcaneus; loss indicates calcaneal fracture with depression |
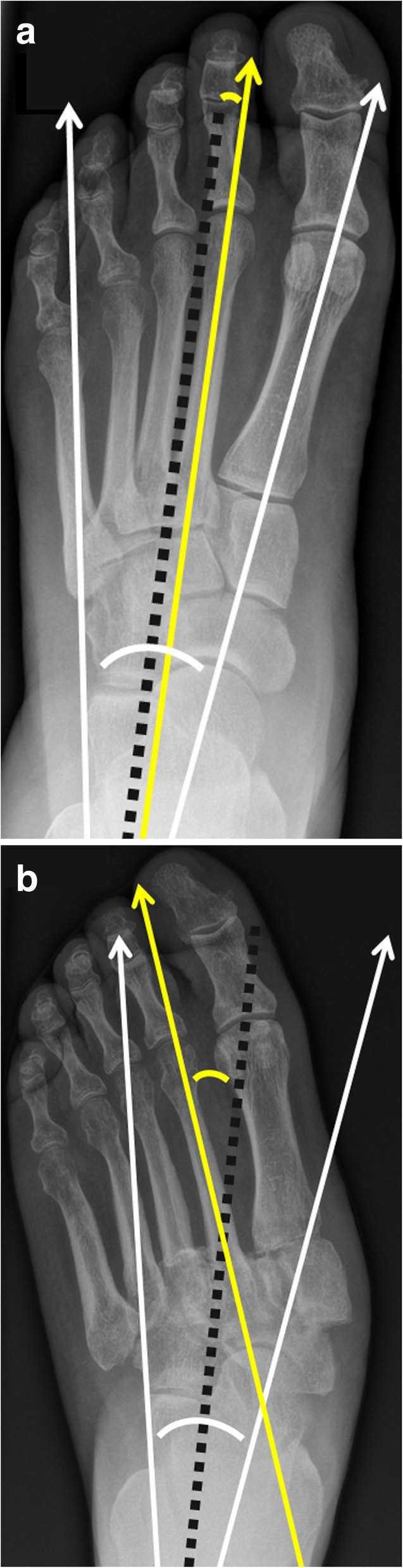
| Hallux valgus angle (HVA) | <15° | Angle between 1st MT and proximal phalanx; defines bunion severity |
| Intermetatarsal angle (IMA) | <9° | Angle between 1st and 2nd MT axes; increased in metatarsus primus varus/bunion |
Clinical Gait Assessment
A focused gait assessment in the podiatric office does not require expensive technology. The examiner observes the patient walking (barefoot and in shoes) from anterior, posterior, and lateral perspectives:
Posterior view — calcaneal alignment in stance (valgus vs. varus vs. neutral); too-many-toes sign; presence and timing of heel inversion during push-off; symmetry of step length and cadence. Lateral view — ankle dorsiflexion at initial contact; knee flexion at loading response; early heel rise (equinus); trunk lean (antalgic). Anterior view — foot progression angle (normally 10–15° external rotation); in-toeing or out-toeing patterns; abductory twist at toe-off (compensatory forefoot abduction seen in limitus/rigidus).
Pressure analysis — in-shoe or barefoot plantar pressure mapping (F-Scan, EMED) quantifies peak pressures under specific regions and identifies high-risk areas in the diabetic foot. Peak plantar pressures >200 kPa during walking identify sites at risk for ulceration. This technology also guides orthotic prescription by identifying areas that require offloading and verifying that the orthotic effectively redistributes pressure.
03 Terminology & Abbreviations
Core terminology used in clinical podiatric documentation. A comprehensive abbreviations list appears in Section 28.
Anatomic Planes & Motions
Dorsiflexion — movement toward the shin (ankle) or superior surface of the foot (toes). Plantarflexion — movement toward the sole. Inversion — sole turns medially. Eversion — sole turns laterally. Abduction — movement away from the midline of the foot (2nd ray). Adduction — movement toward the midline. Pronation — triplanar motion combining eversion, dorsiflexion, and abduction. Supination — triplanar motion combining inversion, plantarflexion, and adduction.
Positional & Structural Terms
Valgus — distal segment deviates laterally (e.g., hallux valgus, calcaneal valgus). Varus — distal segment deviates medially (e.g., rearfoot varus, metatarsus primus varus). Equinus — ankle plantarflexion or inability to dorsiflex past neutral; associated with forefoot overload and Achilles tightness. Calcaneus (as a deformity) — foot fixed in dorsiflexion. Rocker-bottom — midfoot plantar convexity, typically from Charcot collapse.
MTP = metatarsophalangeal; IPJ = interphalangeal joint; PIPJ/DIPJ = proximal/distal interphalangeal joint; TMT = tarsometatarsal; STJ = subtalar joint; ATFL = anterior talofibular ligament; CFL = calcaneofibular ligament; PTTD = posterior tibial tendon dysfunction; AAFD = adult-acquired flatfoot deformity; TCC = total contact cast; DFU = diabetic foot ulcer; ABI = ankle-brachial index; TBI = toe-brachial index; ESWT = extracorporeal shockwave therapy; CMT = Charcot-Marie-Tooth disease.
Deformity Terminology
Hallux abductovalgus — lateral deviation of the hallux with medial prominence of the 1st metatarsal head. Metatarsus primus varus — medial deviation of the 1st metatarsal shaft. Hallux rigidus — degenerative arthritis of the 1st MTP joint with limited dorsiflexion. Hallux limitus — functional or structural limitation of 1st MTP dorsiflexion (<65° normally required for gait). Digiti flexus — generic term for flexion contracture of a lesser toe (hammertoe, claw toe, mallet toe). Hallux malleus — flexion deformity at the hallux IPJ.
Metatarsalgia — general term for pain under the metatarsal heads; not a diagnosis but a symptom complex requiring identification of the specific cause (neuroma, plantar plate tear, stress fracture, IPK, sesamoiditis, synovitis). Tailor bunion (bunionette) — lateral prominence of the 5th metatarsal head with lateral deviation of the 5th toe; treated with wider footwear, padding, or distal 5th MT osteotomy if refractory.
Procedural Terminology
Osteotomy — surgical cutting of bone to realign, shorten, or lengthen. Arthrodesis — surgical fusion of a joint. Arthroplasty — reshaping or replacing a joint (resection arthroplasty removes bone; implant arthroplasty inserts a prosthesis). Exostectomy — removal of a bony prominence (exostosis). Tenotomy — surgical division of a tendon. Capsulotomy — incision into a joint capsule to release contracture or allow access. Matrixectomy — destruction or removal of the nail germinal matrix (chemical with phenol/NaOH, or surgical). Syndesmectomy — excision of a tarsal coalition.
04 Nail Disorders
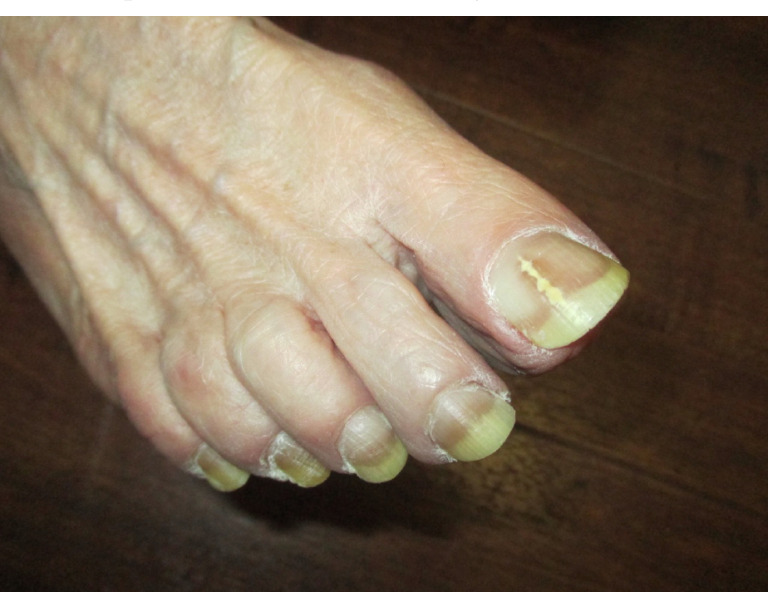
Onychomycosis
Fungal nail infection affects approximately 10% of the general population and up to 50% of adults over age 70. The most common pattern is distal lateral subungual onychomycosis (DLSO), caused predominantly by dermatophytes (Trichophyton rubrum, T. mentagrophytes). Other patterns include white superficial onychomycosis (WSO), proximal subungual (PSO — consider immunosuppression if seen), endonyx, and total dystrophic onychomycosis.




Diagnosis — clinical suspicion should be confirmed before starting systemic therapy. KOH preparation: nail clippings dissolved in 10–20% KOH; fungal hyphae visualized under microscopy (sensitivity ~60%). Fungal culture: Sabouraud dextrose agar — identifies species (4–6 weeks). PAS staining of nail clippings: most sensitive single test (~90%). PCR-based assays are increasingly available.
Treatment:
Mild (<50% nail, no matrix involvement): Topical efinaconazole 10% solution (Jublia) daily × 48 weeks, or tavaborole 5% solution daily × 48 weeks, or ciclopirox 8% lacquer daily × 48 weeks (lower efficacy, ~30% mycologic cure). Moderate–severe (>50% nail or matrix involvement): Oral terbinafine 250 mg daily × 12 weeks (toenails) — mycologic cure ~70%, check baseline LFTs. Alternatively, itraconazole pulse therapy: 200 mg BID × 1 week per month × 3–4 months (check LFTs, drug interactions — potent CYP3A4 inhibitor). Refractory: Combination oral + topical; temporary nail avulsion + topical therapy; laser (Nd:YAG — evidence limited).
Onychocryptosis (Ingrown Toenail)
The lateral nail border penetrates the periungual skin, causing pain, inflammation, and infection. Most commonly affects the hallux. Stages:
| Stage | Presentation | Treatment |
|---|---|---|
| I (mild) | Erythema, slight edema, pain with pressure along nail margin | Conservative: proper nail trimming (straight across), cotton wick/dental floss elevation, warm soaks, wider footwear |
| II (moderate) | Increased pain, drainage, infection, hypertrophy of the nail fold | Partial nail avulsion with or without chemical matrixectomy; oral antibiotics if cellulitis present |
| III (severe) | Chronic inflammation, granulation tissue, marked hypertrophy of nail fold, possible paronychia | Partial nail avulsion with phenol matrixectomy (89% phenol applied to matrix for 1–3 minutes × 3 applications) — ~95% success rate; or sodium hydroxide 10% matrixectomy |
Subungual Hematoma
Blood collection beneath the nail plate from direct trauma. If <25% of the nail plate and the nail/margins are intact, simple trephination (heated paperclip or 18-gauge needle through the nail plate) provides immediate pain relief. If >50% involvement, nail disruption, or associated distal phalanx fracture, nail removal and nail bed repair should be considered.
Melanonychia
Longitudinal melanonychia (pigmented band) requires careful evaluation to exclude subungual melanoma. The ABCDEF rule guides biopsy decisions: Age (50–70 peak), African/Asian/Native American; Band width >3 mm, irregular borders, brown-black color; Change in band morphology; Digit most commonly involved (thumb/hallux); Extension of pigment to proximal or lateral nail fold (Hutchinson sign); Family/personal history of melanoma. Any suspicious lesion requires nail matrix biopsy (punch or excisional).
Other Nail Conditions
Onychogryphosis — ram’s horn nail; hypertrophic, curved nail plate; common in elderly; debridement or avulsion. Onycholysis — distal separation of nail from bed; differential includes psoriasis, trauma, fungal infection, thyroid disease. Pincer nail — transverse overcurvature causing pain; treatment with nail avulsion ± matrixectomy or nail brace.
Psoriatic Nail Disease
Nail involvement occurs in up to 80% of patients with psoriasis and in >90% of patients with psoriatic arthritis. Key nail findings: pitting (small, well-defined depressions in the nail plate from punctate psoriatic lesions in the nail matrix — the most common psoriatic nail finding); oil drop sign (translucent yellow-brown discoloration of the nail bed); subungual hyperkeratosis (scaling beneath the distal nail plate); onycholysis (distal separation, often with erythematous border); splinter hemorrhages (linear hemorrhages in the nail bed from damaged capillaries); crumbling/dystrophy (severe matrix disease). Treatment: topical corticosteroids (clobetasol in a nail lacquer vehicle), intralesional triamcinolone acetonide (5 mg/mL injected into the nail matrix/bed — painful; limit to 2–3 sessions), and systemic therapy for moderate-severe disease (biologics targeting TNF-alpha, IL-17, or IL-23 are effective for both skin and nail psoriasis). Nail psoriasis responds slowly; set expectations for 6–12 months of treatment before full response.
05 Skin Conditions of the Foot
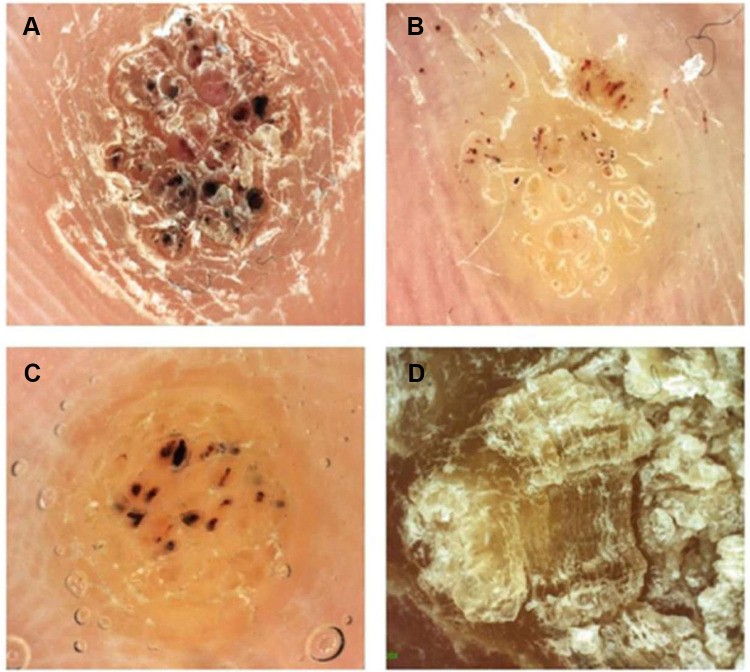
Verrucae (Plantar Warts)
Caused by human papillomavirus (HPV), most commonly types 1, 2, 4, and 27. Present as well-circumscribed hyperkeratotic lesions on the plantar surface with interruption of skin lines, pinpoint bleeding on debridement (thrombosed capillaries), and pain with lateral compression (distinguishes from callus, which hurts with direct pressure).
First line: Salicylic acid 17–40% topical (patient-applied daily after paring, 12-week course; ~75% clearance). Second line: Office cryotherapy with liquid nitrogen (−196°C, 2 freeze-thaw cycles, q2–3 week sessions × 3–4). Third line: Cantharidine 0.7% (blister beetle extract; applied in office, washed off at 4–6 hours — painless application). Refractory: Intralesional bleomycin (0.5–1 unit/mL, inject into base — ~90% cure but painful), intralesional candida antigen injection (0.1–0.3 mL, stimulates cell-mediated immunity), 5-fluorouracil topical/intralesional, surgical excision (last resort — risk of painful plantar scar).
Tinea Pedis (Athlete’s Foot)

Dermatophyte infection of the foot, most commonly Trichophyton rubrum. Three clinical patterns:
Interdigital (most common) — maceration, scaling, fissuring in web spaces (especially 4th web space). Moccasin type — chronic, diffuse hyperkeratosis and scaling of the sole, heel, and lateral foot (often bilateral); associated with toenail onychomycosis; may require oral therapy. Vesiculobullous (inflammatory) — pruritic vesicles and bullae, often on the arch or instep; may trigger id reaction (autoeczematization) on hands.
Treatment: Topical antifungals for interdigital/vesiculobullous types: terbinafine 1% cream BID × 2 weeks (most effective topical), clotrimazole 1% BID × 4 weeks, or butenafine 1% daily × 4 weeks. Moccasin type often requires oral terbinafine 250 mg daily × 2–4 weeks. Keep feet dry; moisture-wicking socks; treat shoes with antifungal powder or UV shoe sanitizer.
Xerosis & Fissures
Extremely dry skin of the feet is common in diabetic patients (autonomic neuropathy reduces sweating) and the elderly. Heel fissures can become deep, painful, and serve as a portal for infection in diabetic/immunocompromised patients. Treatment: urea-based creams (20–40% urea for hyperkeratotic skin, 10% for maintenance), emollients after bathing, debridement of callus borders, liquid cyanoacrylate skin protectant for deep fissures, avoidance of soaking (worsens dryness).
Contact Dermatitis of the Foot
Allergic contact dermatitis — delayed-type (Type IV) hypersensitivity reaction to shoe materials, adhesives, dyes, or topical medications. Common allergens: rubber accelerators (mercaptobenzothiazole, thiuram) in shoe soles and insoles, potassium dichromate in leather tanning, formaldehyde resins in shoe adhesives, and neomycin/bacitracin in topical antibiotics. Distribution pattern mirrors contact area: dorsum and sides of the foot suggest shoe allergy. Diagnosis: patch testing. Treatment: allergen avoidance, topical corticosteroids, identification of specific allergen for footwear counseling. Irritant contact dermatitis — non-immunologic reaction to friction, moisture, or chemical irritants (e.g., antiperspirant overuse); treatment: remove irritant, barrier creams, moisture management.
Hyperhidrosis
Excessive sweating of the feet predisposes to maceration, tinea, and pitted keratolysis (Corynebacterium-induced). Treatment: topical aluminum chloride 20% (Drysol) applied nightly to dry feet; iontophoresis (tap water with low-level electrical current, 20–30 min sessions 3×/week); onabotulinumtoxinA injection (100–200 units distributed across plantar surface — effective 6–9 months, painful injection); glycopyrrolate 1% topical; oral glycopyrrolate or oxybutynin for severe cases. Pitted keratolysis — clusters of superficial pits on weight-bearing sole; treat with topical erythromycin, clindamycin, or benzoyl peroxide.
06 Corns, Calluses & Keratotic Lesions
Hyperkeratotic lesions result from repetitive pressure and friction. Understanding the etiology is essential — treating the lesion without correcting the underlying biomechanical or structural cause guarantees recurrence.
Classification
| Lesion | Location | Features |
|---|---|---|
| Heloma durum (hard corn) | Dorsal/lateral toes over bony prominences (IPJ, condyles) | Well-circumscribed, central conical core (nucleus) that presses on dermal nerves causing pain; skin lines disrupted |
| Heloma molle (soft corn) | Interdigital spaces (especially 4th web space) | Macerated, white, rubberized; caused by adjacent phalangeal condyles; must distinguish from tinea or interdigital maceration |
| Heloma miliare | Non-weight-bearing plantar areas | Multiple small seed-like keratoses; less symptomatic; related to blocked sweat ducts |
| Heloma neurovasculare | Weight-bearing plantar areas | Contains nerves and blood vessels within the keratotic tissue; bleeds on debridement; extremely painful; requires careful excision |
| Callus (tyloma) | Weight-bearing plantar surface (MT heads, heel) | Diffuse, less defined borders than heloma; no central nucleus; skin lines preserved; painful with direct pressure (vs. wart: painful with lateral compression) |
Intractable Plantar Keratosis (IPK)
A discrete, painful callus beneath a metatarsal head that recurs despite conservative care. Caused by a prominent or plantarly displaced metatarsal head, metatarsal length abnormality, or loss of the transverse metatarsal arch. Treatment: regular debridement (scalpel #15 blade, enucleation of central core), accommodative padding (metatarsal pad placed proximal to MT head to redistribute pressure), custom orthotic with metatarsal offloading. Surgical options for refractory IPK include dorsiflexory metatarsal osteotomy (Weil osteotomy) or condylectomy.
Porokeratosis
A discrete keratotic lesion with a distinct peripheral ridge (cornoid lamella) on histology. Porokeratosis plantaris discreta presents as a well-circumscribed plantar lesion with a translucent core surrounded by a keratotic rim. Often misdiagnosed as a wart. Treatment: simple enucleation is usually curative; recurrence is uncommon (unlike IPK).
07 Hallux Valgus (Bunion)
Hallux valgus is the lateral deviation of the great toe at the first MTP joint, associated with medial deviation of the first metatarsal (metatarsus primus varus). It is the most common forefoot deformity, affecting approximately 23% of adults aged 18–65 and 36% of those over 65. Etiology is multifactorial: genetic predisposition, first ray hypermobility, ligamentous laxity, pes planus, constrictive footwear.
Radiographic Assessment
Weight-bearing AP and lateral radiographs are essential. Key angles:
| Angle | Normal | Mild | Moderate | Severe |
|---|---|---|---|---|
| Hallux valgus angle (HVA) | <15° | 15–20° | 20–40° | >40° |
| Intermetatarsal angle (IMA) | <9° | 9–11° | 11–16° | >16° |
| Distal metatarsal articular angle (DMAA) | <10° | Increased DMAA suggests lateral tilting of the distal articular surface; consider distal osteotomy | ||
Also assess: congruency of the MTP joint (congruent = no lateral subluxation of the proximal phalanx; incongruent = subluxed), sesamoid position (tibial sesamoid station 1–7), MTP joint arthrosis (hallux rigidus if dorsal osteophytes and limited ROM).
Surgical Procedures by Severity
Mild (HVA 15–20°, IMA 9–11°): Distal metatarsal osteotomy — Austin (Chevron) osteotomy: V-shaped cut in the distal 1st MT head, lateral translation of the capital fragment (up to 50% of MT width), fixation with 1–2 screws. High union rate, predictable correction, limited to mild/moderate deformities.
Moderate (HVA 20–40°, IMA 11–16°): Scarf osteotomy: Z-shaped diaphyseal osteotomy of the 1st MT allowing multiplanar correction (translation, rotation, shortening); stable fixation with 2 screws; allows greater correction than the chevron. Alternatively, proximal crescentic osteotomy or closing base wedge osteotomy.
Severe (HVA >40°, IMA >16°) or 1st ray hypermobility: Lapidus procedure (1st TMT arthrodesis): fuses the 1st metatarsal-cuneiform joint, correcting hypermobility at its source and providing maximum IMA correction. Weight-bearing restricted 6–8 weeks; newer locking plate technology has shortened this. Indicated when 1st TMT hypermobility is the primary driver.
Salvage / arthritic joint: 1st MTP arthrodesis (fusion) or Keller resection arthroplasty (elderly, low-demand).
AOFAS Hallux Metatarsophalangeal-Interphalangeal Score — a 100-point functional outcome score: Pain (40 points), Function (45 points: activity, footwear, MTP motion, IP motion, stability), Alignment (15 points). Though widely used, it has limitations as a patient-reported outcome measure and is being supplemented by the PROMIS Foot & Ankle module.
Conservative Management
Indicated for mild deformity, asymptomatic patients, or those who are poor surgical candidates. Footwear modification — wide toe box shoes that do not compress the forefoot; avoid pointed or high-heeled shoes. Bunion pads/shields — reduce friction over the medial eminence. Toe spacers — silicone interpositional device between the 1st and 2nd toes; provides symptomatic relief but does NOT correct the deformity. Orthotic therapy — custom orthotic with medial arch support to control pronation and reduce the deforming forces on the 1st ray; may slow progression in mild cases. Night splints — hold the hallux in a corrected position overnight; no evidence for long-term correction in adults but may provide symptomatic relief.
Surgical Complications
Recurrence — the most common reason for patient dissatisfaction; caused by inadequate IMA correction, failure to address 1st ray hypermobility, or progression of underlying biomechanical deformity. Hallux varus — overcorrection resulting in medial deviation of the hallux; may require revision surgery (extensor hallucis brevis transfer, soft tissue rebalancing, or reverse Austin osteotomy). Transfer metatarsalgia — excessive shortening of the 1st metatarsal shifts load to the 2nd and 3rd MT heads; occurs when osteotomy technique shortens the 1st MT by >3–4 mm. AVN of the metatarsal head — rare with distal osteotomies when the lateral soft tissue attachments are preserved; more common with extensive medial and lateral dissection that disrupts the nutrient artery. Stiffness — limited MTP ROM postoperatively; minimize by starting early gentle ROM exercises at 1–2 weeks.
08 Lesser Toe Deformities
Hammertoe, Claw Toe, Mallet Toe
| Deformity | MTP | PIPJ | DIPJ | Key Feature |
|---|---|---|---|---|
| Hammertoe | Extension or neutral | Flexion (primary deformity) | Extension or neutral | Most common lesser toe deformity; often 2nd toe; associated with hallux valgus pushing 2nd toe |
| Claw toe | Hyperextension | Flexion | Flexion | MTP hyperextension distinguishes from hammertoe; bilateral/all toes → neurologic cause (CMT, diabetic neuropathy, RA) |
| Mallet toe | Neutral | Neutral | Flexion (primary deformity) | Isolated DIPJ flexion; pressure on tip of toe; may cause distal callus or nail dystrophy |
Flexible vs. rigid: a flexible deformity is passively correctable; a rigid deformity is not. The distinction is the single most important factor in determining treatment:
Flexible deformity → conservative (taping, padding, toe splints, accommodative shoes with extra depth) or minimally invasive procedures (percutaneous flexor tenotomy, flexor-to-extensor transfer).
Rigid deformity → arthroplasty (resection of the proximal phalanx head) or arthrodesis (fusion) of the PIP joint; address any associated MTP instability concurrently.
Surgical options: PIP arthroplasty (resection of the proximal phalanx head, K-wire fixation × 4 weeks), PIP arthrodesis (fusion with K-wire, absorbable pin, or intramedullary implant), flexor-to-extensor transfer (Girdlestone-Taylor procedure for flexible claw toe), extensor tenotomy/lengthening, metatarsal shortening osteotomy (Weil) for associated metatarsalgia.
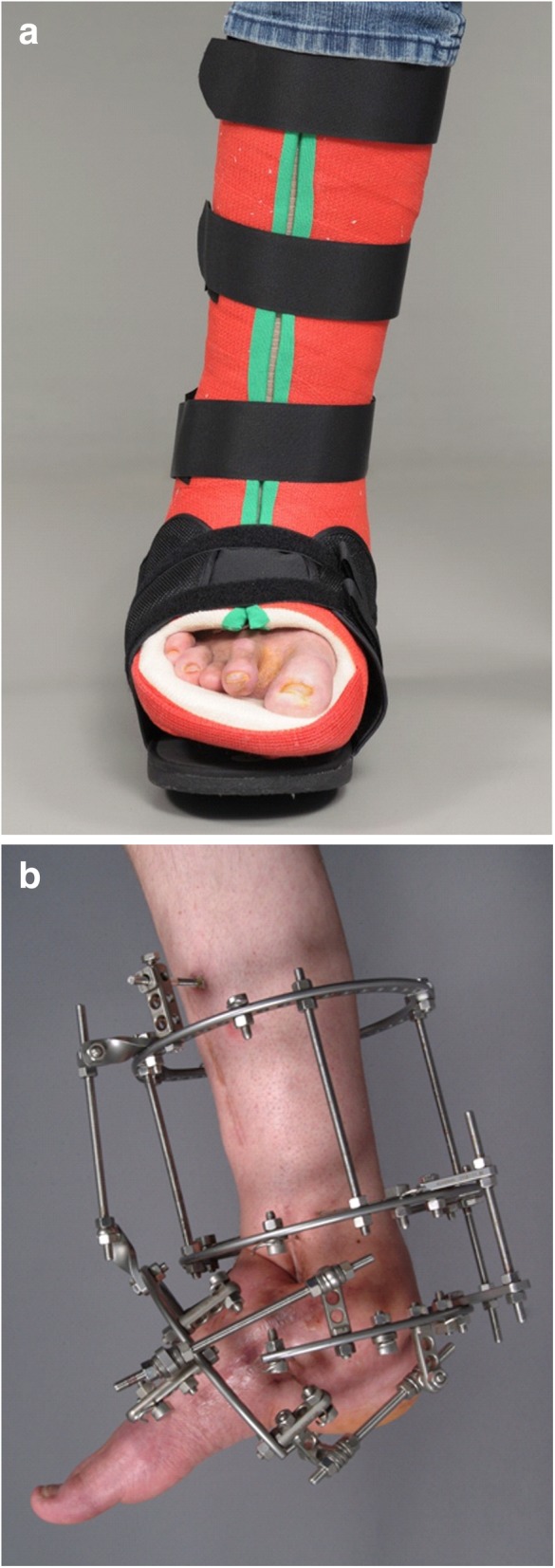
In the neuropathic patient with claw toes causing distal tip ulceration, a percutaneous flexor tenotomy is a minimally invasive office-based procedure that can heal the ulcer and prevent recurrence. Technique: after local digital block, a #15 or #11 blade is inserted plantarly at the level of the DIPJ flexion crease, and the FDL tendon is transected. The toe straightens immediately. Advantages: performed under local anesthesia, minimal wound, immediate weight-bearing, no need for K-wire fixation, and ulcer healing rates of 80–90%. This is a particularly valuable procedure in high-risk diabetic patients who are poor candidates for more extensive surgery.
Morton Neuroma
Perineural fibrosis of the common digital nerve, most commonly in the 3rd intermetatarsal space (between 3rd and 4th MT heads). Patients report burning, tingling, numbness in the affected web space, worsened by tight shoes and walking. The Mulder click (compression of the forefoot while palpating the interspace produces a palpable and sometimes audible click) is pathognomonic. Ultrasound (hypoechoic mass >5 mm) and MRI confirm the diagnosis.
Treatment ladder: wider shoes, metatarsal pad, NSAIDs → corticosteroid injection (1 mL betamethasone + 1 mL lidocaine, dorsal approach between the MT heads, advance needle until it is palpable plantarly at the interspace) — provides temporary relief in ~50%; limit to 3 injections (risk of plantar fat pad atrophy and plantar plate damage) → alcohol sclerosing injections (4% dehydrated alcohol diluted with local anesthetic to a total volume of 1–2 mL, injected into the neuroma under ultrasound guidance, series of 3–7 injections at 1–2 week intervals — causes chemical neurolysis with ~60–70% sustained improvement) → surgical excision (dorsal longitudinal incision centered over the interspace, retract the deep transverse metatarsal ligament or transect it, identify the common digital nerve proximal to its bifurcation, transect at least 1–2 cm proximal to the neuroma, allow the proximal stump to retract into soft tissue away from weight-bearing; specimen should be sent for histology; recurrence/stump neuroma rate ~15–20%).
Predislocation Syndrome & Crossover Toe
Attenuation of the 2nd MTP plantar plate and collateral ligaments leads to progressive instability, dorsal subluxation, and eventually medial crossover of the 2nd toe over the hallux. The drawer test of the 2nd MTP (dorsally directed force on the proximal phalanx) demonstrates pathologic laxity. Early treatment: taping the toe in corrected position, stiff-soled shoe, metatarsal pad. Surgical: direct plantar plate repair (Weil osteotomy + plantar plate reattachment through a dorsal approach) has become the standard for established crossover toe.
09 Plantar Fasciitis & Heel Pain
Plantar fasciitis is the most common cause of inferior heel pain, accounting for approximately 80% of cases. It is a degenerative enthesopathy (not primarily inflammatory) of the plantar fascia at its origin on the medial calcaneal tuberosity.
Risk Factors & Pathophysiology
Obesity (BMI >30), prolonged standing occupations, running (especially increased mileage), pes planus, pes cavus, limited ankle dorsiflexion (equinus), and tight gastrocnemius-soleus complex. Histopathology shows collagen degeneration, fibroblast proliferation, and mucoid degeneration (fasciosis) rather than acute inflammation.
Clinical Features
Classic presentation: first-step pain — severe heel pain with the first steps in the morning that improves after several minutes of walking, then worsens with prolonged standing or activity. Pain is localized to the medial calcaneal tuberosity on palpation. The windlass test (passive dorsiflexion of the hallux reproduces pain at the plantar fascial origin) is the most specific clinical test. Imaging is not required for diagnosis but may exclude other causes: lateral weight-bearing XR may show a calcaneal spur (present in 50% but not causative), MRI shows thickened plantar fascia (>4 mm) with increased signal. Ultrasound shows thickened hypoechoic fascia.
Treatment Ladder
Step 1 (0–6 weeks): Activity modification, ice massage, NSAIDs (short course), stretching (gastrocnemius and plantar fascia — Achilles wall stretch, plantar fascia stretch over a frozen water bottle, towel stretch), supportive footwear with cushioned heel. ~80% resolve with conservative measures within 12 months.
Step 2 (6–12 weeks): Prefabricated or custom orthotic insoles with medial arch support and cushioned heel; night splint (dorsiflexion night splint at 5° maintains stretch on the gastrocnemius-soleus and plantar fascia during sleep).
Step 3 (3–6 months): Corticosteroid injection (40 mg triamcinolone + 1 mL lidocaine, medial approach at the point of maximal tenderness under ultrasound guidance preferred — limit to 3 injections total due to risk of plantar fascia rupture and fat pad atrophy); physical therapy (eccentric loading, manual therapy, iontophoresis).
Step 4 (6–12 months): Extracorporeal shockwave therapy (ESWT — Level I evidence, 60–80% improvement; 2000–3000 pulses per session, 3 weekly sessions); platelet-rich plasma (PRP) injection; Gastrocnemius recession (Strayer procedure) if isolated gastrocnemius contracture (<5° dorsiflexion with knee extended, normal dorsiflexion with knee flexed — Silfverskiold test positive).
Step 5 (refractory, >12 months): Plantar fasciotomy (partial release of the medial one-third to one-half; endoscopic or open; avoid complete release — risk of lateral column overload and arch collapse).
Differential Diagnosis of Heel Pain
| Condition | Key Distinguishing Feature |
|---|---|
| Baxter neuritis (1st branch lateral plantar nerve entrapment) | Burning/tingling pain, maximal tenderness more medial and plantar than classic PF; may have abductor digiti minimi weakness/atrophy; MRI may show muscle denervation edema |
| Calcaneal stress fracture | Pain with medial-lateral calcaneal squeeze test (positive); history of recent increase in impact activity; XR may be negative early; MRI or bone scan diagnostic |
| Fat pad atrophy | Diffuse central heel pain (not medial); heel pad feels thin on palpation; common in elderly and patients with repeated corticosteroid injections; worsened by walking barefoot on hard surfaces |
| Tarsal tunnel syndrome | Burning, tingling in plantar foot; positive Tinel sign posterior to medial malleolus; NCS/EMG confirmatory |
| Haglund deformity (pump bump) | Posterior-superior calcaneal prominence causing retrocalcaneal bursitis and pain at the heel counter of shoes; most common in women wearing rigid-backed shoes |
| Insertional Achilles tendinopathy | Pain at the Achilles insertion on the posterior calcaneus (not plantar); calcification at insertion on lateral XR; morning stiffness; NOT first-step plantar pain |
Injection Techniques for Heel Pain
Plantar fascia corticosteroid injection — the medial approach is most common: the needle is inserted at the medial border of the heel at the point of maximum tenderness, directed laterally and slightly superiorly toward the plantar fascial origin. Use 40 mg triamcinolone acetonide (or equivalent) with 1–2 mL 1% lidocaine (or 0.5% bupivacaine for longer analgesia). Ultrasound guidance improves accuracy (needle tip visualized entering the thickened fascia at its calcaneal origin) and may improve outcomes while reducing risk of inadvertent fat pad injection.
Risks of repeated injection: plantar fascia rupture (reported in 2–10% of injected patients; presents as sudden pain relief followed by lateral column overload, loss of arch height, and lateral plantar pain); fat pad atrophy (particularly with multiple injections or injection superficial to the fascia rather than deep to it; leads to persistent heel pain from loss of shock absorption); skin depigmentation at the injection site.
Platelet-rich plasma (PRP) injection — autologous blood product concentrated in growth factors (PDGF, TGF-beta, VEGF); injected into the plantar fascia at the origin under ultrasound guidance. Mechanism: promotes tendon/fascial healing rather than suppressing inflammation. Studies show equivalent or superior long-term outcomes compared to corticosteroid injection without the risks of rupture and fat pad atrophy. Disadvantage: not covered by most insurance plans; requires centrifugation equipment and venipuncture at the time of treatment.
10 Flatfoot & Cavus Foot
Adult-Acquired Flatfoot Deformity (AAFD) / Posterior Tibial Tendon Dysfunction
Progressive degeneration of the posterior tibial tendon leads to loss of the medial longitudinal arch, hindfoot valgus, and forefoot abduction. Most common in women over 40. Risk factors: obesity, hypertension, diabetes, corticosteroid use, seronegative arthropathy.
Clinical tests: Too-many-toes sign — when viewing the patient from behind, more lateral toes are visible on the affected side due to forefoot abduction. Single-heel-rise test — patient stands on one leg and rises onto tiptoe; inability to rise or failure of the heel to invert indicates PTTD. Medial ankle pain along the PT tendon course.
Johnson-Stainsby Classification
| Stage | Pathology | Clinical Findings | Treatment |
|---|---|---|---|
| I | Tendon inflammation/tenosynovitis; tendon intact | Medial ankle pain, mild swelling along PT tendon; normal arch height; positive single-heel-rise; no deformity | Immobilization (CAM boot 4–6 weeks), then custom orthotic with medial arch support, physical therapy (PT tendon strengthening), NSAIDs |
| II | Tendon degeneration/elongation; flexible flatfoot | Arch collapse (flexible — corrects with heel rise); too-many-toes sign; weak/painful single-heel-rise; hindfoot valgus | UCBL orthotic or Arizona brace for IIA (mild); surgical for IIB: FDL tendon transfer to navicular + medializing calcaneal osteotomy (Koutsogiannis) ± spring ligament repair ± Cotton osteotomy (medial cuneiform opening wedge) ± lateral column lengthening (Evans osteotomy) |
| III | Tendon severely degenerated/ruptured; rigid flatfoot | Fixed hindfoot valgus and forefoot abduction; NOT passively correctable; subtalar joint stiffness; may have lateral impingement pain (sinus tarsi) | Triple arthrodesis (subtalar + talonavicular + calcaneocuboid fusion) or double arthrodesis (subtalar + talonavicular); must address equinus if present (gastrocnemius recession or TAL) |
| IV | Stage III + ankle valgus (deltoid insufficiency, tibiotalar tilt) | All findings of Stage III plus ankle valgus tilt visible on weight-bearing AP ankle XR; deltoid ligament incompetent | Triple arthrodesis + deltoid reconstruction; or tibiotalocalcaneal (TTC) arthrodesis; or total ankle replacement + hindfoot realignment in select cases |
Cavus Foot
An abnormally high medial longitudinal arch with hindfoot varus, plantarflexed 1st ray, and associated claw toes. Unlike flatfoot, which is usually acquired, cavus foot is frequently due to an underlying neurologic condition — an etiology should always be sought.
Neurologic causes: Charcot-Marie-Tooth disease (CMT, most common — accounts for ~50% of cavus feet), friedreich ataxia, spinal dysraphism, poliomyelitis, spinal cord tumor, cerebral palsy. All patients with new or progressive cavus foot should have a thorough neurologic exam and consider spinal MRI.
Coleman block test — patient stands with the lateral foot on a wooden block, allowing the 1st ray to plantarflex off the edge. If the hindfoot varus corrects (hindfoot moves to neutral or valgus), the deformity is forefoot-driven (flexible hindfoot) and can be addressed with a dorsiflexory 1st metatarsal osteotomy. If the hindfoot varus persists, it is a rigid hindfoot varus requiring calcaneal osteotomy (Dwyer lateralizing or closing wedge).
Surgical reconstruction: Typically multicomponent: dorsiflexory 1st MT osteotomy + calcaneal osteotomy (Dwyer) + peroneus longus-to-brevis transfer (eliminates the deforming force on the 1st ray) + plantar fascia release + claw toe correction (Jones procedure: EHL transfer to 1st MT neck + IPJ fusion). In severe/rigid cases: triple arthrodesis for global deformity correction.
Inspection: High arch visible in standing; hindfoot varus viewed from behind; claw toe deformity; calluses under the 1st and 5th MT heads (tripod loading pattern); lateral foot callus from overload; muscle wasting of the leg (intrinsic hand wasting in CMT).
Gait: Lateral foot loading; foot-slap gait (steppage gait if peroneal weakness present); ankle instability or recurrent sprains.
Muscle testing: Peroneus brevis weakness (eversion) is often the first motor finding in CMT; peroneus longus may be relatively preserved, creating the plantarflexed 1st ray deformity; tibialis anterior weakness leads to drop foot; intrinsic muscle wasting produces claw toes.
Coleman block test: Essential for surgical planning — determines whether the hindfoot varus is driven by the forefoot (1st ray plantarflexion) or is a fixed rearfoot deformity.
Neurologic workup: All patients require thorough neurologic examination including reflexes, motor and sensory testing, and consideration of NCS/EMG and spinal MRI if a specific diagnosis has not been established.
11 Ankle & Rearfoot Conditions
Ankle Sprains
Lateral ankle sprains (inversion injuries) account for 85% of all ankle sprains and are the most common musculoskeletal injury in athletes. The ATFL is injured first (weakest ligament, taut in plantarflexion), followed by the CFL (taut in dorsiflexion), and rarely the PTFL (strongest, usually intact except in dislocations). Medial (deltoid) sprains account for <5% of ankle sprains and should raise suspicion for associated injuries: fibula fracture (Weber B or C), syndesmotic injury, or Maisonneuve fracture (proximal fibula). Syndesmotic (high ankle) sprain — injury to the anterior inferior tibiofibular ligament (AITFL), interosseous membrane, and/or posterior inferior tibiofibular ligament; caused by external rotation or dorsiflexion; presents with pain at the anterior ankle joint line above the mortise, positive squeeze test (compression of the fibula to the tibia at mid-calf reproduces distal pain), and positive external rotation stress test. Recovery is significantly longer than lateral sprains (6–12 weeks); unstable syndesmotic injuries with widening of the mortise require surgical fixation.
| Grade | Pathology | Clinical Findings | Treatment |
|---|---|---|---|
| I | Ligament stretch, no macroscopic tear | Mild swelling, tenderness over ATFL; no laxity on anterior drawer; full weight-bearing | RICE, ankle brace, early mobilization, return to activity 1–2 weeks |
| II | Partial tear (ATFL ± CFL) | Moderate swelling, ecchymosis; positive anterior drawer with soft endpoint; some difficulty weight-bearing | Functional rehabilitation: ankle brace or taping, progressive weight-bearing, proprioceptive training; 3–6 weeks recovery |
| III | Complete tear (ATFL + CFL ± PTFL) | Severe swelling, ecchymosis, inability to bear weight; gross laxity on anterior drawer and talar tilt; possible peroneal subluxation or osteochondral injury | Short immobilization (1–2 weeks in walking boot), then aggressive rehabilitation; surgical repair rarely indicated acutely except in elite athletes |
Ottawa ankle rules — radiographs indicated if: bone tenderness at the posterior edge or tip of either malleolus, bone tenderness at the navicular or 5th MT base, or inability to bear weight immediately and in the ED (4 steps). Sensitivity ~98% for fractures; reduces unnecessary XR by 30–40%.
Physical examination maneuvers — the anterior drawer test is performed with the patient seated, the knee flexed, and the ankle in slight plantarflexion; the examiner stabilizes the distal tibia with one hand and draws the calcaneus/talus anteriorly with the other. Increased anterior translation or a soft endpoint compared to the contralateral side indicates ATFL insufficiency. The talar tilt test (inversion stress test) assesses CFL integrity: with the ankle in neutral, the examiner inverts the calcaneus; >10° talar tilt or >5° more than the uninjured side is positive. Both tests are most reliable when performed 4–5 days after injury (once acute guarding subsides) or under anesthesia. Stress radiographs can document laxity objectively.
Chronic Ankle Instability (CAI)
Recurrent ankle sprains and/or persistent “giving way” after an index sprain, affecting ~20% of patients. May be mechanical (ligament laxity) or functional (proprioceptive deficit). Conservative treatment: supervised proprioceptive/neuromuscular rehabilitation program, ankle bracing. Surgical: Brostrom repair (direct ATFL repair + imbrication of the inferior extensor retinaculum — Gould modification) is the gold standard; anatomic reconstruction preserving subtalar motion. Augmentation with suture tape or allograft (Brostrom-InternalBrace) may be used for revision or large patients.
Peroneal Tendon Pathology
Peroneal subluxation — rupture of the superior peroneal retinaculum allows tendons to sublux over the lateral malleolus; felt/heard as a painful snap with eversion. Acute: immobilization may suffice. Chronic/recurrent: retinacular repair ± groove-deepening procedure. Peroneal tendon tears — peroneus brevis longitudinal split tears are most common (compressed between the longus and the fibula in the retromalleolar groove); presents as lateral ankle pain and weakness with eversion. Treatment: debridement and tubularization if <50% of tendon involved; tenodesis of brevis to longus if >50%.
Achilles Tendon Rupture
Typically occurs 2–6 cm proximal to the calcaneal insertion (watershed zone). Common in “weekend warriors” aged 30–50 with sudden eccentric loading. Thompson test: patient prone, feet hanging off table; squeeze the calf — absent plantarflexion = positive = rupture. A palpable gap may be present.
Treatment: Surgical repair (Krackow suture technique, early protected weight-bearing) vs. functional rehabilitation (serial casting with progressive dorsiflexion, then boot with heel wedge). Meta-analyses show similar outcomes with accelerated functional rehab protocols, but re-rupture rates are slightly higher non-operatively (~5% vs ~2%). Surgery preferred in young, active patients.
Favors operative repair: Young, active patient (<40 years); athlete with high functional demands; significant gap between tendon ends on ultrasound (>1 cm with ankle in plantarflexion); delayed presentation (>4 weeks, chronic rupture requiring reconstruction with FHL turndown or V-Y advancement); failed non-operative treatment.
Favors non-operative management: Older, sedentary patient; significant medical comorbidities increasing surgical risk (diabetes, PVD, immunosuppression, smoking); patient preference; tendon ends approximate with ankle in equinus (assessed by palpation and ultrasound). An accelerated functional rehabilitation protocol with early weight-bearing in an equinus boot is essential for non-operative success — prolonged immobilization in a cast without a structured rehab protocol produces inferior outcomes.
Minimally invasive / percutaneous repair: Intermediate approach using small incisions or percutaneous suture devices; reduced wound complication rate compared to open repair (particularly relevant in diabetic patients); re-rupture rates comparable to open repair. Sural nerve injury risk is higher with percutaneous technique (up to 10%) but can be reduced with ultrasound guidance.
Tarsal Coalition
An abnormal connection (fibrous, cartilaginous, or osseous) between tarsal bones; affects ~1% of the population. The two most common types: calcaneonavicular (best seen on 45° oblique XR — “anteater sign”) and talocalcaneal (middle facet; best evaluated with CT — the “C sign” on lateral XR is suggestive). Presents in adolescence as rigid, painful flatfoot with limited subtalar motion and recurrent ankle sprains. Treatment: conservative (orthotic, activity modification) → surgical resection (for calcaneonavicular: bar resection with EDB muscle interposition; for talocalcaneal: resection if <50% of the posterior facet involved) → triple arthrodesis for extensive coalition with degenerative changes.
12 Diabetic Foot Assessment
Diabetic foot complications are the leading cause of non-traumatic lower-extremity amputation. Approximately 15–25% of diabetic patients will develop a foot ulcer during their lifetime, and the 5-year mortality after a major amputation exceeds 50%. Systematic foot assessment identifies risk and directs preventive strategies.
Comprehensive Diabetic Foot Exam
Neurologic assessment:
10-gram Semmes-Weinstein monofilament — the single most validated screening tool for loss of protective sensation (LOPS). Test 4 sites per foot minimum: hallux plantar surface, 1st MT head, 3rd MT head, 5th MT head. Inability to perceive the monofilament at ≥1 site = LOPS. 128 Hz tuning fork — tests vibration perception at the hallux DIP; loss correlates with large-fiber neuropathy. Ankle reflexes — absent Achilles reflex suggests sensorimotor neuropathy. Ipswich Touch Test — screening alternative: lightly touch the hallux, 3rd toe, and 5th toe bilaterally; inability to perceive ≥2 sites indicates neuropathy (no equipment needed).
Vascular assessment:
Pedal pulses — palpate dorsalis pedis and posterior tibial arteries. Ankle-brachial index (ABI): ankle systolic pressure / highest brachial pressure. Normal 1.0–1.3; <0.9 = peripheral arterial disease; >1.3 = non-compressible (calcified) arteries (common in diabetes — ABI unreliable). In diabetic patients with calcified arteries: toe-brachial index (TBI) >0.7 is normal (digital arteries rarely calcify); transcutaneous oxygen pressure (TcPO2) >40 mmHg indicates adequate perfusion for healing; skin perfusion pressure (SPP) >40 mmHg predicts healing.
Musculoskeletal assessment: Evaluate for structural deformities (Charcot, hammertoe, bunion, prominent MT heads) that create focal pressure areas. Limited joint mobility (especially limited ankle dorsiflexion from equinus or glycosylated tissue) increases plantar pressures. The Achilles tendon should be assessed (Silfverskiold test). The prayer sign (inability to fully approximate the palms when pressing hands together) indicates limited joint mobility from glycosylation of periarticular structures — a marker for elevated plantar pressures and ulceration risk.
Dermatologic assessment: Inspect all surfaces including between toes. Check for callus (precursor to ulceration), fissures, tinea, nail dystrophy, and erythema. Callus under MT heads should be debrided to reduce focal pressure. Pre-ulcerative signs include hemorrhage within callus (subkeratotic hematoma), skin discoloration, and localized warmth. Autonomic neuropathy produces anhidrosis (dry skin) increasing fissure risk, and distended dorsal foot veins from loss of sympathetic vascular tone.
Diabetic Peripheral Neuropathy Classification
Sensorimotor polyneuropathy — the most common form; symmetric, distal, length-dependent “stocking-glove” pattern; affects small fibers first (pain, temperature) then large fibers (vibration, proprioception); leads to loss of protective sensation. Autonomic neuropathy — affects sweating (anhidrosis), vascular tone (arteriovenous shunting producing a warm, dry foot with bounding pulses despite possible coexisting macrovascular disease), and skin integrity. Motor neuropathy — intrinsic muscle atrophy leads to imbalance between extrinsic flexors/extensors, producing claw toes, prominent metatarsal heads, and altered plantar pressure distribution. The triad of sensory loss + motor imbalance + autonomic dysfunction creates the perfect environment for ulceration.
Vascular: Dorsalis pedis pulse (present/absent/diminished); posterior tibial pulse; capillary refill time (<3 sec normal); skin color and temperature; hair growth pattern; ABI or TBI if indicated.
Neurologic: 10-g monofilament (4 sites per foot); 128 Hz tuning fork (hallux); ankle reflexes; report sites of absent sensation.
Musculoskeletal: Deformities (bunion, hammertoe, Charcot, prominent MT heads); ankle dorsiflexion ROM (equinus); prior amputation sites.
Dermatologic: Skin integrity; callus location and degree; fissures; interdigital maceration or fungal infection; nail pathology; pre-ulcerative changes.
Footwear assessment: Shoe type; wear pattern; appropriateness; presence/use of therapeutic shoes or orthotics.
IWGDF Risk Classification
| Risk Group | Definition | Frequency of Examination |
|---|---|---|
| 0 | No LOPS, no PAD | Annually |
| 1 | LOPS or PAD | Every 6 months |
| 2 | LOPS + PAD, or LOPS/PAD + foot deformity | Every 3–6 months |
| 3 | LOPS or PAD + history of prior ulcer or amputation | Every 1–3 months |
13 Diabetic Foot Ulcers
Wagner Classification
| Grade | Description |
|---|---|
| 0 | Intact skin; at-risk foot (bony deformity, callus, neuropathy) |
| 1 | Superficial ulcer (epidermis and dermis only; no tendon, capsule, or bone exposure) |
| 2 | Deep ulcer penetrating to tendon, joint capsule, or bone (without abscess or osteomyelitis) |
| 3 | Deep ulcer with abscess, osteomyelitis, or joint sepsis |
| 4 | Localized gangrene (forefoot or heel) |
| 5 | Extensive gangrene involving the entire foot; emergent amputation required |
University of Texas (UT) Classification
More granular than Wagner; uses a grid of grade (depth) and stage (complications):
| Stage A (no infection, no ischemia) | Stage B (infection) | Stage C (ischemia) | Stage D (infection + ischemia) | |
|---|---|---|---|---|
| Grade 0 | Pre-/post-ulcerative completely epithelialized | Infection present | Ischemia present | Infection + ischemia |
| Grade I | Superficial wound not involving tendon, capsule, or bone | Infection | Ischemia | Both |
| Grade II | Wound penetrating to tendon or capsule | Infection | Ischemia | Both |
| Grade III | Wound penetrating to bone or joint | Infection | Ischemia | Both |
Increasing stage (A → D) dramatically increases amputation risk. Stage D (infection + ischemia) carries the worst prognosis regardless of wound depth.
Wound Assessment
Depth — probe with sterile instrument. Probe-to-bone (PTB) test: a sterile metal probe reaches bone through the wound — positive predictive value for osteomyelitis is 89% in the infected diabetic foot (specificity improves in high-prevalence settings). Negative PTB does not rule out osteomyelitis. Wound dimensions should be measured (length × width × depth) at each visit. Wound bed — document tissue types present: granulation (red, beefy, healthy), slough (yellow, devitalized fibrinous tissue), eschar (black, necrotic), epithelial (pink, new skin advancing from edges). Periwound skin — assess for maceration (white, soggy from excess moisture), callus formation (reduces wound contraction), erythema/cellulitis, and undermining or tunneling (measure clock-face direction and depth).
Wound Care Products
Dry wound (needs moisture): Hydrogel (amorphous or sheet) — donates moisture to wound bed; ideal for dry eschar softening and autolytic debridement; change every 1–3 days.
Moderate exudate: Foam dressings (polyurethane) — absorb moderate drainage while maintaining moist environment; non-adherent; change every 3–7 days. Hydrofiber (Aquacel) — absorbs exudate and forms a gel; excellent for conforming to wound contours.
Heavy exudate: Alginate (calcium alginate derived from seaweed) — highly absorbent; forms gel on contact with wound fluid; hemostatic properties; change when saturated (1–3 days). Superabsorbent dressings for very high output wounds.
Infected or critically colonized: Silver-containing dressings (silver alginate, silver foam, silver hydrofiber) — broad-spectrum antimicrobial; use for 2–4 weeks then reassess. Cadexomer iodine (Iodosorb) — slow-release iodine with absorptive beads; effective for biofilm disruption.
Granulating wound needing protection: Collagen dressings — provide scaffold for cell migration; combine with oxidized regenerated cellulose (ORC) in some products. Contact layers (Adaptic, Mepitel) — non-adherent mesh to prevent dressing adherence to wound bed.
Offloading
The cornerstone of DFU management. Total contact cast (TCC) is the gold standard for plantar forefoot and midfoot ulcers — reduces plantar pressure by 60–80% and ensures compliance (non-removable). The removable walker made irremovable (wrapped with one layer of cohesive bandage or fiberglass to prevent removal) has shown similar healing rates to TCC and is more practical for many clinicians. Patients will not comply with removable offloading devices — studies show they are worn only 28% of the time when removable.
Grade 0 (at-risk): Prevention — diabetic shoes + molded insoles, patient education, regular debridement of callus.
Grade 1 (superficial): Sharp debridement of necrotic tissue and callus; moist wound environment (alginate, foam, or hydrogel); TCC or irremovable walker; reassess every 1–2 weeks; if <50% area reduction by 4 weeks, add advanced therapy (bioengineered skin substitute, negative pressure wound therapy).
Grade 2 (deep, no infection): Same as Grade 1 + assess for PAD (ABI/TBI); surgical debridement in OR if needed; consider NPWT for large wounds.
Grade 3 (infection/osteomyelitis): Urgent surgical debridement; deep tissue cultures; targeted antibiotics (see Section 15); bone biopsy if osteomyelitis suspected; may require partial ray amputation or TMA.
Grades 4–5 (gangrene): Vascular surgery consultation for revascularization if possible; amputation at the most distal viable level.
Advanced Wound Therapies
When standard wound care and offloading fail to achieve healing within 4 weeks, advanced therapies should be considered:
| Therapy | Mechanism | Evidence Level | Considerations |
|---|---|---|---|
| Bioengineered skin substitutes | Provide extracellular matrix scaffold, growth factors, and/or living cells to the wound bed | Level I (multiple RCTs) | Dermagraft (human fibroblast-derived dermal substitute); Apligraf (bilayered living cell construct); EpiFix (dehydrated human amnion/chorion membrane); applied weekly until healed or maximum 12 weeks |
| Negative pressure wound therapy (NPWT) | Subatmospheric pressure removes exudate, reduces edema, increases local perfusion, promotes granulation | Level I | −75 to −125 mmHg continuous or intermittent; dressing changes q48–72h; contraindicated over exposed vessels, nerves, or anastomoses; useful as bridge to closure or grafting |
| Hyperbaric oxygen therapy (HBOT) | 100% O2 at 2.0–2.5 ATA increases tissue oxygen tension; enhances leukocyte killing, collagen synthesis, angiogenesis | Level II (mixed evidence) | Indicated for Wagner 3+ DFU with adequate vascular inflow; 30–40 sessions at 90 min each; expensive; TcPO2 should increase to >200 mmHg in-chamber to predict benefit |
| Growth factor therapy | Becaplermin (recombinant PDGF-BB) stimulates cell migration and proliferation | Level I | FDA-approved for neuropathic DFU extending to subcutaneous tissue; applied daily with dressing; black box warning for malignancy risk with ≥3 tubes |
14 Charcot Neuroarthropathy
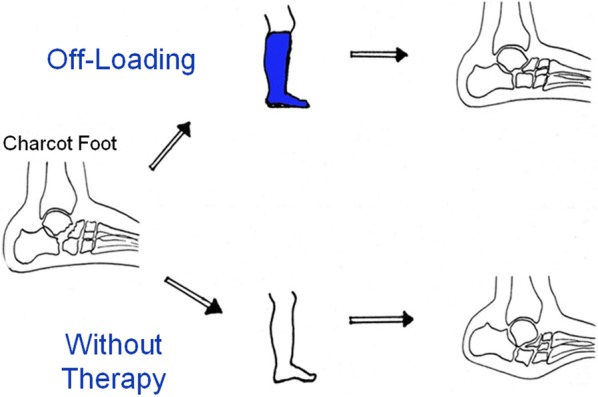
A progressive destructive arthropathy affecting the bones and joints of the foot and ankle in patients with peripheral neuropathy, most commonly diabetic. The incidence in diabetic patients is approximately 0.1–0.9%. Pathophysiology involves unrecognized repetitive microtrauma in the insensate foot triggering an uncontrolled inflammatory cascade (RANKL upregulation, osteoclastic bone resorption) leading to fracture, dislocation, and structural collapse.
Clinical Presentation

Acute Charcot presents as a hot, swollen, erythematous foot in a patient with neuropathy. Skin temperature is typically 2–6°C warmer than the contralateral foot. Pain may be present but disproportionately mild for the degree of pathology (neuropathy). The differential diagnosis includes cellulitis/osteomyelitis (look for ulcer, wound, elevated WBC/ESR/CRP), DVT (unilateral swelling, Doppler evaluation), and acute gout (sudden onset, 1st MTP most common, serum urate). Charcot is a clinical diagnosis of exclusion in the neuropathic patient.
Eichenholtz Classification

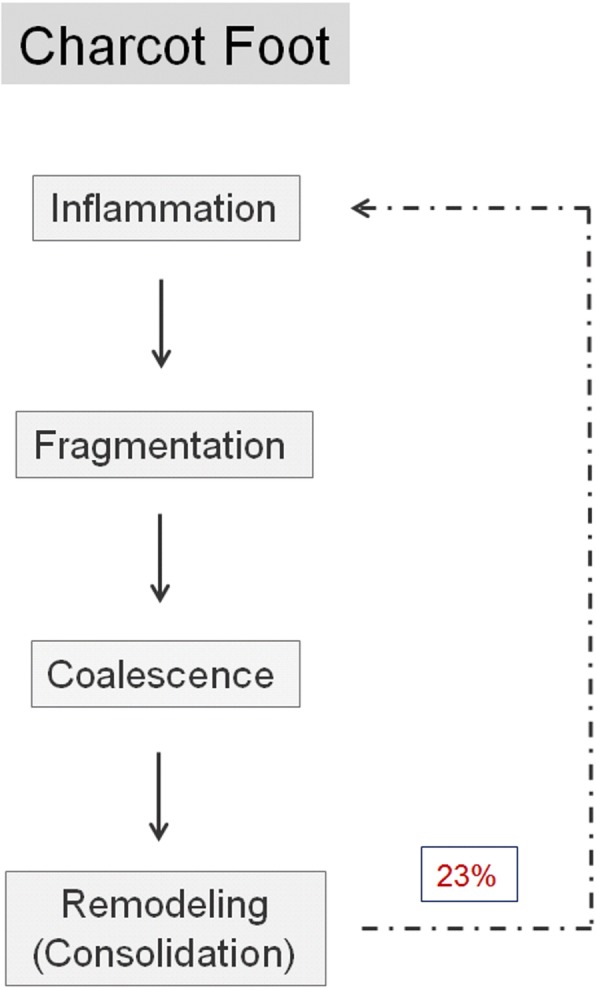
| Stage | Name | Radiographic Findings | Clinical Findings | Treatment |
|---|---|---|---|---|
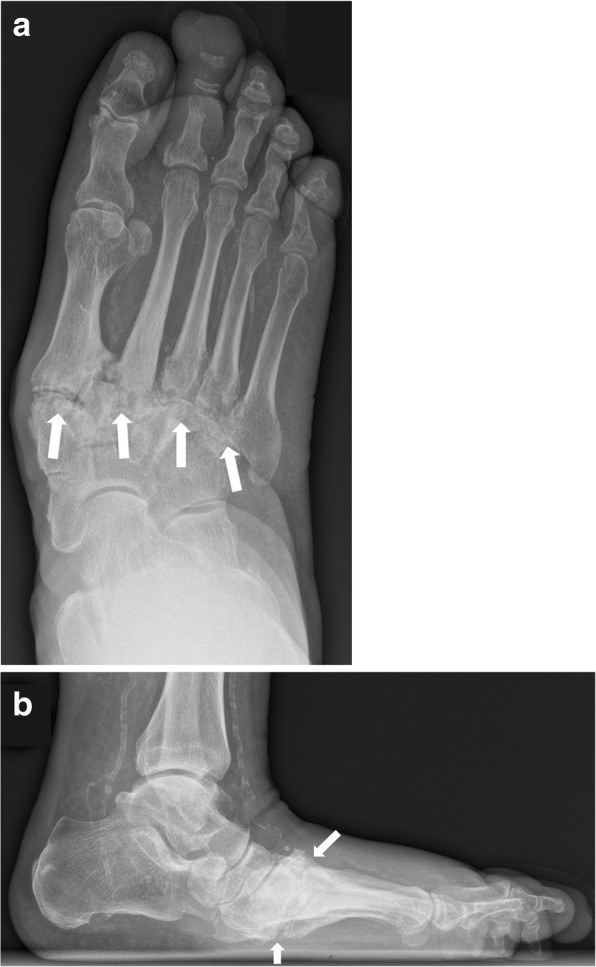
| 0 | Prodromal (Sella & Barrette addition) | Radiographs normal or minimal changes; MRI shows bone marrow edema, joint effusion | Warm, swollen foot without radiographic destruction; high clinical suspicion in neuropathic patient | Immediate offloading in TCC or irremovable walker; NWB or protected WB; serial imaging |
| I | Development (Fragmentation) | Osseous fragmentation, periarticular fractures, joint subluxation/dislocation, debris | Maximum swelling, warmth, and erythema; foot may begin to deform | Strict offloading (TCC changed every 1–2 weeks); NWB; bisphosphonates (limited evidence); calcitonin (limited evidence); monitor until coalescence |
| II | Coalescence | Absorption of debris, new bone formation, early fusion, sclerosis of fracture fragments | Decreasing warmth and swelling; temperature difference narrowing (<2°C) | Continue offloading; transition from TCC to custom accommodative brace (Charcot restraint orthotic walker — CROW boot) |
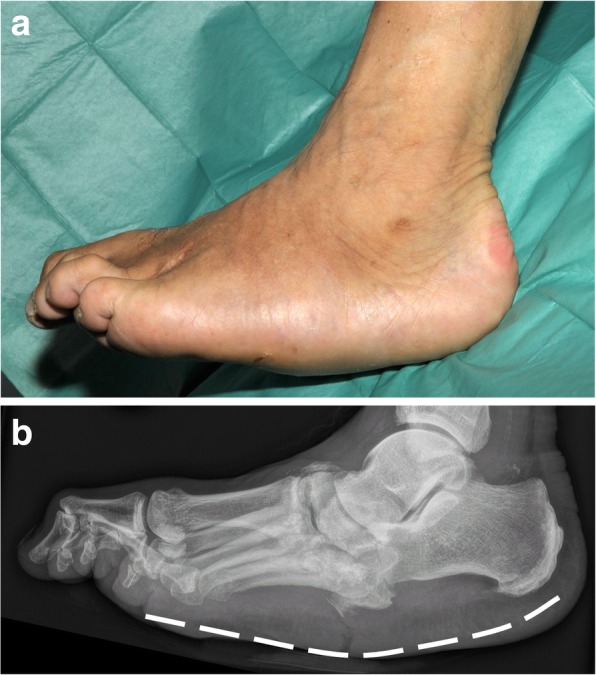
| III | Consolidation (Remodeling) | Mature reparative bone, fusion of fragments, residual deformity but stable architecture | No warmth differential; stable foot; residual deformity may be present (rocker-bottom) | Custom molded extra-depth shoes with accommodative insoles; lifetime surveillance; ulcer prevention over bony prominences |
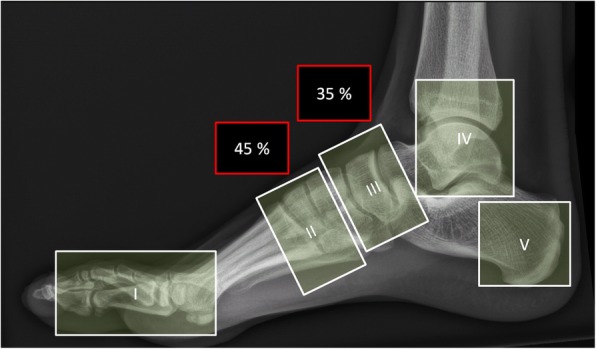
Anatomic classification (Sanders & Frykberg): Type I (forefoot, 20%), Type II (tarsometatarsal/Lisfranc, 40% — most common), Type III (naviculocuneiform/Chopart, 30%), Type IV (ankle, 10%), Type V (calcaneus, rare). Midfoot involvement (Types II–III) is the hallmark, producing the classic rocker-bottom deformity with plantar bony prominence predisposing to ulceration.

Surgical Indications
Surgery is reserved for: (1) recurrent ulceration over bony prominence not manageable with bracing/orthotics — exostectomy (plantar bony prominence removal); (2) gross instability or deformity precluding brace fitting — reconstructive arthrodesis (midfoot beaming with intramedullary bolts, plates, or external fixation); (3) ankle Charcot with valgus collapse — tibiotalocalcaneal arthrodesis with retrograde intramedullary nail; (4) limb-threatening infection. Surgery should ideally be performed during the coalescence or consolidation stage (lower complication rates).

Differentiating Charcot from Infection
The clinical overlap between acute Charcot and osteomyelitis/cellulitis is a major diagnostic challenge, as both present with a warm, swollen, erythematous foot. Key distinguishing features:
| Feature | Acute Charcot | Infection (Osteomyelitis/Cellulitis) |
|---|---|---|
| Skin integrity | Usually intact; no wound or ulcer | Typically an ulcer, wound, or break in the skin is present as the portal of entry |
| Laboratory markers | WBC usually normal; ESR mildly elevated; CRP mildly elevated or normal | WBC often elevated; ESR >70 mm/hr suggestive of osteomyelitis; CRP significantly elevated |
| Response to elevation | Swelling and erythema improve with elevation (inflammatory edema) | Cellulitic erythema may persist or worsen; purulence may be present |
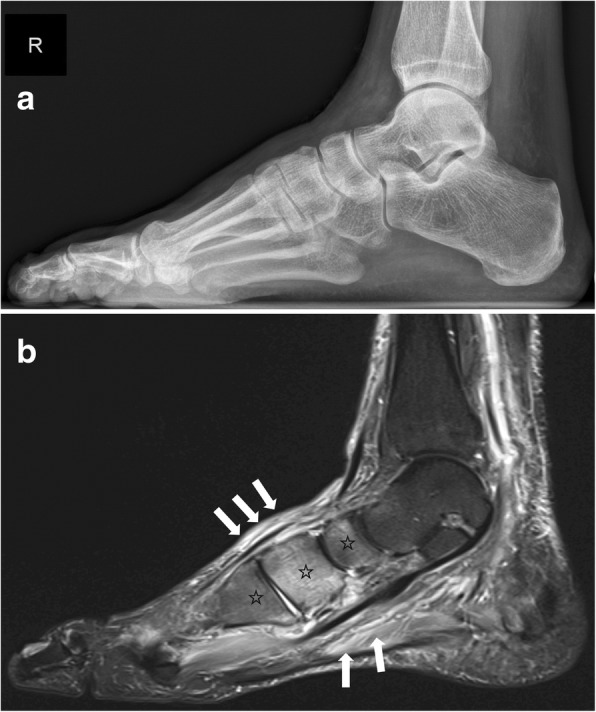
| MRI findings | Bone marrow edema in a periarticular distribution affecting both sides of a joint; no soft tissue abscess | Bone marrow edema centered on a bone adjacent to an ulcer; soft tissue abscess, sinus tract, or periosteal reaction may be present |
| Location | Midfoot (Lisfranc and Chopart joints) most common | Adjacent to a wound, often at a bony prominence under an ulcer |
When the diagnosis remains uncertain, particularly when an ulcer overlies a Charcot deformity, the conditions may coexist. Bone biopsy is the gold standard for confirming or excluding osteomyelitis in equivocal cases. Labeled white blood cell (WBC) scan combined with a bone marrow (sulfur colloid) scan can help differentiate infection from neuropathic bone changes: spatially incongruent uptake patterns suggest infection.
15 Diabetic Foot Infections
Diabetic foot infection (DFI) is the most common reason for diabetes-related hospitalization and the proximate cause of ~60% of lower-extremity amputations in diabetic patients. It is a clinical diagnosis: presence of purulent drainage, or ≥2 signs of inflammation (erythema, warmth, swelling, tenderness, induration) in a wound.
IDSA/IWGDF Severity Classification
| Severity | IWGDF Grade | Clinical Features | Treatment Setting |
|---|---|---|---|
| Uninfected | 1 | No signs of infection | Wound care, offloading only |
| Mild | 2 | Cellulitis ≤2 cm around wound; no systemic signs; infection limited to skin/subcutaneous tissue | Outpatient oral antibiotics × 1–2 weeks |
| Moderate | 3 | Cellulitis >2 cm, OR lymphangitis, OR spread beneath fascia, OR deep tissue abscess, OR muscle/tendon/joint/bone involvement; no SIRS | Often inpatient; IV antibiotics initially; surgical debridement/drainage as needed |
| Severe | 4 | Any infection with systemic inflammatory response (SIRS: temp >38°C or <36°C, HR >90, RR >20, WBC >12k or <4k) or metabolic instability (hyperglycemia, acidosis, azotemia) | Inpatient, urgent surgical debridement, IV broad-spectrum antibiotics, ICU if septic |
Microbiology & Culture
Mild, acute infections are typically monomicrobial (gram-positive cocci: Staphylococcus aureus, Streptococcus). Chronic, deep, or previously treated infections are often polymicrobial (adding gram-negatives: Enterobacteriaceae, Pseudomonas; and anaerobes: Bacteroides, Peptostreptococcus). Always obtain deep tissue cultures (curettage of the wound base after debridement, or tissue biopsy) — NOT superficial swabs, which grow colonizing organisms. Culture before antibiotics if possible.
Empiric Antibiotics
Mild (IWGDF 2): Oral therapy targeting gram-positives: amoxicillin-clavulanate 875/125 mg BID, or cephalexin 500 mg QID, or clindamycin 300 mg QID (if penicillin-allergic). Duration: 1–2 weeks.
Moderate (IWGDF 3) without MRSA risk: Ampicillin-sulbactam 3 g IV q6h, or piperacillin-tazobactam 3.375 g IV q6h (if Pseudomonas suspected), or ertapenem 1 g IV daily. Step down to oral after clinical improvement.
Moderate/Severe with MRSA risk: Add vancomycin 15–20 mg/kg IV q8–12h (trough 15–20 mcg/mL), or daptomycin 6 mg/kg IV daily, or linezolid 600 mg PO/IV BID (monitor for thrombocytopenia >2 weeks).
Severe (IWGDF 4): Broad-spectrum: vancomycin + piperacillin-tazobactam 4.5 g IV q6h, or vancomycin + meropenem 1 g IV q8h. Duration for soft tissue infection: 2–4 weeks (total); osteomyelitis: 4–6 weeks.
Osteomyelitis
Present in 50–60% of severe DFI. Suspect when bone is visible or palpable via the wound (probe-to-bone test positive). MRI is the imaging modality of choice (sensitivity 90%, specificity 80%): shows bone marrow edema (T1 hypointense, T2/STIR hyperintense). Plain XR has low sensitivity early but may show cortical erosion, periosteal reaction, or sequestrum in established disease. Bone biopsy with culture is the gold standard for confirming osteomyelitis and identifying the organism for targeted therapy.
Treatment: Surgical resection of infected bone (partial or complete) + 2–4 weeks of targeted IV/oral antibiotics is generally preferred over prolonged (6-week) antibiotic therapy alone, as surgical excision shortens the treatment course and has higher cure rates. In non-surgical candidates: 6+ weeks of culture-directed antibiotics with serial ESR/CRP monitoring. The “antibiotic-only” approach may be considered when: the patient is a poor surgical candidate, the bone involved is biomechanically essential (e.g., calcaneus or talus where resection would require amputation), or the infection is limited and the patient declines surgery. Monitor response with serial ESR (should decrease by ≥25% every 2 weeks) and CRP (normalizes faster than ESR, typically within 2–4 weeks if treatment is effective). MRI is unreliable for monitoring short-term treatment response due to persistent marrow signal changes even after successful treatment; serial plain radiographs showing osseous reconstitution and absence of progressive destruction are more useful for long-term follow-up.
Amputation Levels
| Level | Indication | Considerations |
|---|---|---|
| Toe amputation | Gangrene or osteomyelitis confined to a single toe | Preserve length when possible; avoid tight closure; highest functional preservation |
| Ray amputation | Infection/necrosis extending to metatarsal | 1st or 5th ray resection generally well tolerated; central ray resection creates transfer lesion risk |
| Transmetatarsal (TMA) | Multiple toe/ray involvement; forefoot gangrene | Requires adequate perfusion to midfoot; Achilles lengthening or gastrocnemius recession usually needed to prevent equinus and stump ulceration |
| Below-knee amputation (BKA) | Extensive gangrene, uncontrolled infection, non-reconstructable vascular disease | Preserves knee joint; prosthetic rehabilitation possible; 5-year survival after major amputation ~50% |
16 Foot & Ankle Fractures
Ankle Fractures — Weber Classification
| Type | Fibula Fracture Location | Syndesmosis | Stability | Treatment |
|---|---|---|---|---|
| Weber A | Below the syndesmosis (at or below the joint line) | Intact | Stable | Weight-bearing in a walking boot or short leg cast × 4–6 weeks; surgical fixation only if significantly displaced |
| Weber B | At the level of the syndesmosis (spiral/oblique from anteroinferior to posterosuperior) | May be partially injured | Potentially unstable | Stress views (external rotation or gravity stress) to assess deltoid competence; stable → non-operative; unstable (medial clear space >4 mm, talar shift) → ORIF with lag screw and neutralization plate |
| Weber C | Above the syndesmosis (proximal fibula — Maisonneuve variant if very proximal) | Disrupted | Unstable | ORIF: fibula fixation + syndesmotic fixation (screws or suture-button device); always assess for deltoid injury and Maisonneuve fracture (palpate proximal fibula, full-length tibia/fibula XR) |
5th Metatarsal Fractures
| Zone | Name | Mechanism | Treatment |
|---|---|---|---|
| Zone 1 | Tuberosity avulsion (pseudo-Jones) | Inversion injury; peroneus brevis or lateral plantar fascia avulsion | Weight-bearing in hard-soled shoe or walking boot × 4–6 weeks; heals reliably |
| Zone 2 | Jones fracture (metaphyseal-diaphyseal junction) | Acute adduction force on plantarflexed foot | High non-union rate (watershed vascular zone); non-operative: NWB cast × 6–8 weeks (non-union ~25%); surgical: intramedullary screw fixation preferred for athletes and active patients (faster return, lower non-union ~5%) |
| Zone 3 | Proximal diaphyseal stress fracture | Chronic repetitive stress | High risk of delayed union/non-union/refracture; intramedullary screw fixation recommended; address biomechanical factors (cavus foot, lateral overload) |
Lisfranc Injury

Disruption of the tarsometatarsal joint complex; ranges from subtle ligamentous sprain to frank fracture-dislocation. Mechanism: axial load on a plantarflexed foot (e.g., fall from height, motor vehicle, athletic injury). Often missed — up to 20% misdiagnosed initially. Weight-bearing AP XR: look for >2 mm diastasis between 1st and 2nd MT bases; loss of alignment of the medial border of 2nd MT with medial border of intermediate cuneiform. A “fleck sign” (avulsion fragment between bases) is pathognomonic. CT scan for subtle injuries. Treatment: non-displaced, stable injuries may be managed with NWB cast × 6–8 weeks; any displacement or instability on stress views → ORIF (bridge plating or screw fixation) or primary arthrodesis (increasingly favored, especially for purely ligamentous injuries).
Calcaneus Fractures
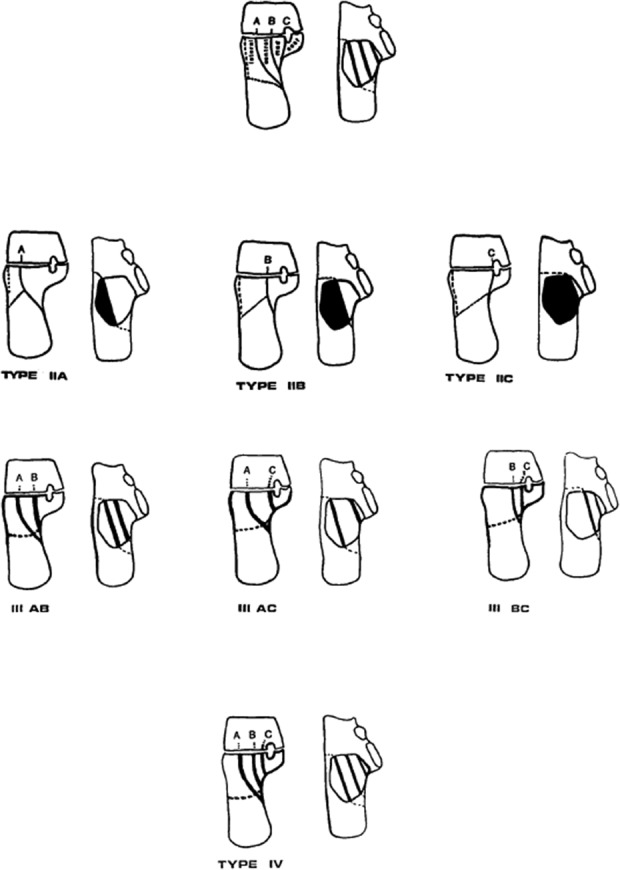
High-energy injuries (fall from height, MVC). 10% bilateral, 10% associated lumbar compression fracture. Bohler angle (normally 20–40°): decreased angle indicates posterior facet depression. Sanders classification (based on coronal CT through the widest part of the posterior facet):
| Type | Description | Treatment |
|---|---|---|
| I | Non-displaced (<2 mm) posterior facet fracture | Non-operative: NWB cast/boot × 8–12 weeks, early ROM |
| II | Two-part: single fracture line through posterior facet (IIA, IIB, IIC by location) | ORIF via extensile lateral approach or sinus tarsi approach; restore Bohler angle, articular congruity |
| III | Three-part: two fracture lines creating a central depressed fragment (IIIAB, IIIAC, IIIBC) | ORIF; increasing comminution makes anatomic reduction more difficult; higher complication rate |
| IV | Highly comminuted: ≥4 articular fragments | Primary subtalar arthrodesis (ORIF unlikely to restore articular surface); or non-operative with late subtalar fusion if symptomatic |
Talus Fractures — Hawkins Classification
| Type | Description | AVN Risk | Treatment |
|---|---|---|---|
| I | Non-displaced talar neck fracture | ~10% | NWB SLC × 8–12 weeks; close follow-up for displacement |
| II | Displaced talar neck + subtalar subluxation/dislocation | ~40% | Urgent ORIF with anatomic reduction |
| III | Displaced talar neck + subtalar AND tibiotalar dislocation | ~90% | Emergent reduction and ORIF |
| IV | Type III + talonavicular subluxation/dislocation (Canale & Kelly addition) | ~100% | Emergent reduction, ORIF; near-universal AVN |
Hawkins sign — subchondral radiolucency in the talar dome seen on AP XR at 6–8 weeks post-injury; indicates intact blood supply (disuse osteoporosis requires viable bone). Absence of the Hawkins sign does NOT confirm AVN but should raise suspicion — MRI at 3 months is definitive.
Metatarsal Fractures (Non-5th MT)
Acute metatarsal shaft fractures (2nd–4th MT) — usually result from direct trauma or twisting injury. Most are stable because adjacent metatarsals splint the fractured bone. Non-displaced or minimally displaced fractures: hard-soled shoe or walking boot × 4–6 weeks; weight-bearing as tolerated. Displacement >3–4 mm in any plane or angulation >10° in the sagittal plane (dorsal/plantar): closed reduction and immobilization; ORIF with plate or K-wires if reduction cannot be maintained. Multiple metatarsal fractures or fracture-dislocations are unstable and often require surgical fixation.
1st metatarsal fractures deserve special attention because the 1st ray bears one-third of forefoot load. Displacement that creates shortening or dorsal angulation of the 1st MT will result in transfer metatarsalgia to the 2nd MT. A lower threshold for surgical fixation (plate and screws) applies to 1st MT fractures compared to lesser metatarsals.
Pilon Fractures (Tibial Plafond)
High-energy axial loading injuries of the distal tibial articular surface. The Ruedi-Allgower classification: Type I (non-displaced cleavage fracture of the articular surface), Type II (displaced articular fracture with minimal comminution), Type III (significant comminution with impaction of the articular surface). Management follows a staged protocol: (1) initial spanning external fixation to restore length and alignment, reduce fracture, and allow soft tissue recovery (7–14 days); (2) definitive ORIF with anatomic articular reduction, bone grafting of metaphyseal void, and medial or anterolateral plating when soft tissue conditions permit (wrinkle test positive). CT scan is essential for preoperative planning. High complication rate: wound dehiscence 10–15%, infection 5–10%, post-traumatic arthritis nearly universal in Type III.
17 Sports Injuries
Turf Toe
Sprain of the 1st MTP plantar plate/capsule complex from forced hyperextension (dorsiflexion) of the hallux, classically on artificial turf.
| Grade | Pathology | Treatment |
|---|---|---|
| I | Stretching of the plantar plate; minimal swelling/ecchymosis | Taping, stiff-soled shoe, return to play as tolerated |
| II | Partial tear; moderate swelling, painful ROM, ecchymosis | Walking boot × 1–2 weeks, then taping + turf toe plate in shoe; 2–4 weeks to return |
| III | Complete tear with dorsal dislocation of the proximal phalanx; may involve sesamoid fracture | NWB boot × 2–4 weeks, then 6–8 weeks before return; consider surgical repair if sesamoid retraction, loose body, or progressive hallux valgus |
Sesamoid Pathology
Sesamoiditis — overuse inflammation of the sesamoid complex; pain localized to the plantar 1st MTP; treat with offloading (dancer pad, orthotic with sesamoid cutout), activity modification, NSAIDs. Sesamoid fracture — acute (transverse fracture line, irregular edges on XR) vs. bipartite sesamoid (smooth, rounded, corticated edges; present in 10–30% of population, usually bilateral — compare contralateral foot). Acute fracture: NWB boot × 6 weeks, then orthotic; refractory → partial sesamoidectomy (preserve at least one to prevent hallux valgus/varus drift). Sesamoid AVN — chronic pain, sclerosis/fragmentation on XR, increased signal on MRI; sesamoidectomy if non-responsive to conservative care.
Achilles Tendinopathy
Non-insertional (2–6 cm proximal to insertion, midportion): fusiform swelling, morning stiffness, pain with running. Histology: failed healing response (tendinosis) rather than inflammation. Insertional (at calcaneal attachment): associated with calcification, Haglund deformity, retrocalcaneal bursitis.
Treatment: First line for midportion: eccentric loading program (Alfredson protocol — 3 × 15 repetitions of eccentric heel drops, both straight-knee and bent-knee, twice daily for 12 weeks). Heavy slow resistance training is an alternative. Adjuncts: heel lift, NSAIDs (short-term), GTN patches (limited evidence). Second line: ESWT, PRP injection. Corticosteroid injection is contraindicated (rupture risk). Refractory: surgical debridement ± FHL transfer for tendon augmentation. For insertional tendinopathy: eccentric exercises with the heel below step level are avoided (may aggravate); Haglund resection + retrocalcaneal bursectomy + debridement of calcific insertional disease ± reattachment with suture anchors.
Plantar Plate Injuries
The plantar plate is a thick fibrocartilaginous structure on the plantar aspect of the MTP joint that is the primary restraint against dorsiflexion and hyperextension. Injury most commonly affects the 2nd MTP joint due to its length and mechanical disadvantage. Grading: Grade 0 (plantar plate attenuation without tear), Grade 1 (distal transverse tear <50%), Grade 2 (distal transverse tear >50%), Grade 3 (complete transverse tear with or without longitudinal extension), Grade 4 (extensive tear with button-hole deformity and medial/lateral deviation). MRI and ultrasound can identify plantar plate tears with high sensitivity when performed by experienced musculoskeletal radiologists.
Treatment: Grade 0–1: buddy taping of the affected toe in slight plantarflexion, stiff-soled shoe or rocker-bottom shoe, metatarsal pad to offload the MT head; 6–8 weeks of conservative care. Grade 2–4 or failed conservative management: surgical repair via dorsal approach (Weil metatarsal shortening osteotomy to access the plantar plate, followed by direct repair of the plantar plate to the base of the proximal phalanx using suture anchors). Post-operative: taping and stiff-soled shoe for 6–8 weeks; formal physical therapy starting at 4 weeks.
Stress Fractures
Overuse injuries from repetitive subthreshold loading. Most common sites in the foot: 2nd metatarsal (“march fracture”), 3rd metatarsal, navicular (high-risk — non-union prone), and calcaneus. The shin splints → stress fracture continuum: medial tibial stress syndrome (periostitis) → stress reaction (bone marrow edema on MRI, normal XR) → stress fracture (cortical fracture line). Risk factors: female athlete triad (energy deficiency, menstrual dysfunction, low BMD), rapid training increases, poor footwear, biomechanical issues. MT stress fractures: walking boot × 4–6 weeks. Navicular stress fractures: NWB cast × 6–8 weeks (high complication rate if inadequately immobilized); CT to confirm healing before return; surgical fixation (percutaneous screw) for displaced or non-healing fractures.
Posterior Ankle Impingement
Pain in the posterior ankle with forced plantarflexion (en pointe in ballet, kicking). Caused by an os trigonum (accessory ossicle posterior to the talus, present in ~7% of population) or a Stieda process (elongated lateral tubercle of the posterior talus). Impingement of the os trigonum, FHL tendon, or posterior capsule between the tibia and calcaneus. Diagnosis: posterior ankle tenderness, pain with passive plantarflexion; MRI confirms. Treatment: posterior ankle injection (diagnostic and therapeutic) → if refractory: arthroscopic or open excision of the os trigonum.
Anterior Ankle Impingement
Bony impingement — anterior tibial and talar osteophytes impinge with dorsiflexion; common in athletes (soccer players, “footballer’s ankle”) and post-traumatic arthritis. Pain at the end range of dorsiflexion; palpable anterior osteophyte. Lateral XR shows kissing osteophytes on the anterior tibial lip and talar neck. Treatment: conservative (heel lift, activity modification, steroid injection) → arthroscopic debridement and osteophyte resection for refractory cases; good results in the absence of generalized arthritis.
Soft tissue impingement — meniscoid lesion or synovial hypertrophy in the anterolateral gutter following an inversion ankle sprain; causes persistent anterolateral ankle pain despite adequate ligament healing. Positive Molloy-Bendall test (impingement sign: palpation of the anterolateral gutter with the ankle in plantarflexion, then dorsiflexion reproduces pain). MRI may show soft tissue thickening in the anterolateral gutter. Arthroscopic debridement is definitive treatment when conservative measures fail.
Osteochondral Lesions of the Talus (OLT)
Focal defects of the articular cartilage and underlying subchondral bone of the talar dome; present in up to 50% of acute ankle fractures and 6–7% of ankle sprains. The medial talar dome (posteriorly) is most commonly affected. Patients report deep ankle pain, intermittent swelling, catching, or locking. Berndt-Harty classification: Stage I (subchondral compression), Stage II (partially detached osteochondral fragment), Stage III (completely detached but non-displaced fragment), Stage IV (displaced fragment). MRI is the imaging modality of choice for staging. Treatment: Stages I–II typically respond to immobilization and protected weight-bearing × 6 weeks. Stage III–IV or symptomatic refractory lesions: arthroscopic debridement + bone marrow stimulation (microfracture) for lesions <15 mm; osteochondral autograft transfer (OATS) or particulated juvenile cartilage allograft for larger defects or failed microfracture.
18 Pediatric Foot Conditions
Clubfoot (Talipes Equinovarus)
Congenital deformity occurring in ~1:1000 live births (bilateral in 50%). Components: CAVE — Cavus (high arch), Adductus (forefoot medially deviated), Varus (hindfoot inverted), Equinus (ankle plantarflexed). The Pirani scoring system grades severity from 0 to 6 based on six clinical signs (3 midfoot + 3 hindfoot parameters, each scored 0, 0.5, or 1): higher score = more severe.

Ponseti method (gold standard — >95% success rate): sequential manipulation and serial long-leg casting, changed weekly × 5–7 casts. Correction order follows the mnemonic “CAVE” in reverse priority:

(1) Cavus correction first — supinate the forefoot on the hindfoot to align the forefoot with the hindfoot (this must be done before abducting the foot).
(2) Adductus and varus simultaneously — abduct the foot with counterpressure on the lateral talar head (NOT on the calcaneus, which would cause a rocker-bottom deformity); each cast progressively abducts the foot.
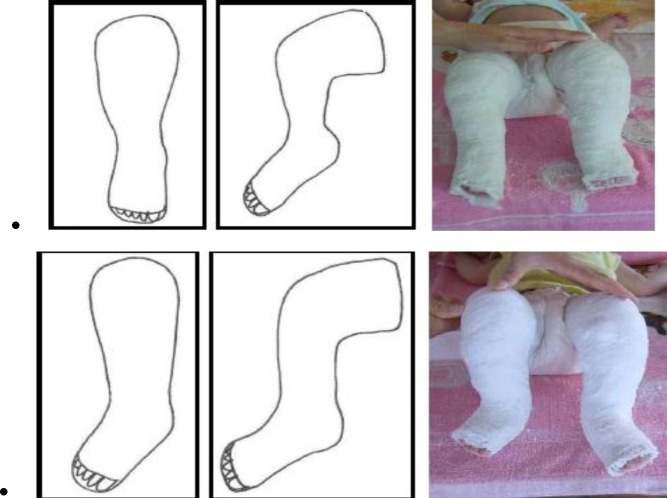
(3) Equinus last — corrected only after the foot is fully abducted to 60–70°; a percutaneous Achilles tenotomy is required in ~80% of cases (performed under local anesthesia in the clinic), followed by 3 weeks in the final cast with the foot in 60–70° abduction and 15° dorsiflexion.
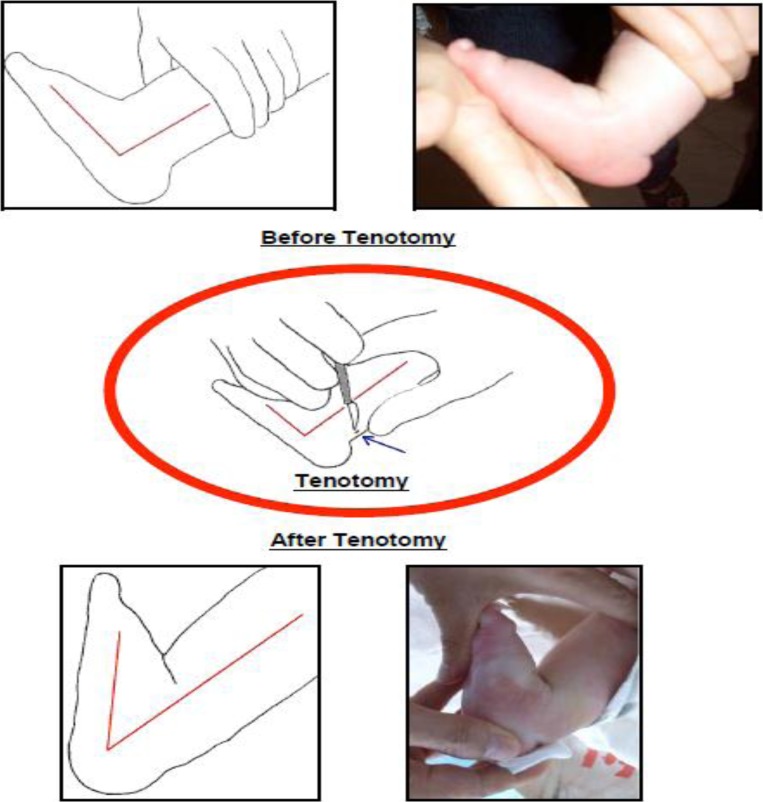
Maintenance: foot abduction brace (Denis Browne bar or Dobbs bar) worn 23 hours/day × 3 months, then nighttime and nap time until age 4–5 years. Recurrence rate with compliant bracing: ~5%; without bracing: ~80%. Non-compliance with the brace protocol is the single most common cause of recurrence.
Tibialis anterior transfer — for recurrent dynamic supination deformity (foot supinates during swing phase due to overpull of the tibialis anterior without peroneal opposition): the tibialis anterior tendon is transferred laterally to the 3rd cuneiform or cuboid to balance the foot. Performed after age 2.5–3 years.
Metatarsus Adductus
Medial deviation of the forefoot relative to the hindfoot; the most common foot deformity at birth. Flexible (passively correctable past midline) — resolves spontaneously in 85–90% by age 1 year; may use gentle stretching exercises. Rigid (not passively correctable) — serial casting starting at age 6–8 weeks for 6–8 casts (similar to Ponseti). Surgical correction (multiple MT osteotomies or midfoot osteotomy) is rarely needed and reserved for severe, rigid deformity persisting beyond age 4.
Flexible Flatfoot in Children
Physiologic flatfoot is normal in children under age 6 (medial arch develops with maturation of the tarsal ossification centers and strengthening of the posterior tibial tendon). The arch appears when standing on tiptoe or when the hallux is dorsiflexed (Jack test). No treatment is needed for asymptomatic flexible flatfoot; studies show arch supports and special shoes do NOT accelerate arch development. Intervention warranted only if: pain, functional limitation, or abnormal shoe wear — orthotic with medial arch support; UCBL for moderate cases.
Osteochondroses
Sever disease (calcaneal apophysitis) — the most common cause of heel pain in children aged 8–14, and the most common pediatric overuse injury of the foot. Traction apophysitis at the Achilles insertion on the calcaneal growth plate. Bilateral in 60%. Pain with medial-lateral calcaneal squeeze (positive calcaneal squeeze test); pain worsened by running and jumping; pain at the posterior-inferior heel (NOT plantar — plantar fasciitis is rare in children). Radiographs are generally unnecessary unless red flags are present (night pain, fever, non-mechanical pain pattern); the appearance of sclerosis or fragmentation of the calcaneal apophysis is a normal developmental variant and NOT diagnostic of Sever disease. Treatment: activity modification (reduce running volume), heel cups or cushioned heel lifts (reduce traction on the apophysis), gastrocnemius-soleus stretching program, icing after activity, temporary use of a walking boot for severe cases; self-limiting with closure of the calcaneal apophysis (typically age 12–15 in girls, 13–16 in boys).
Kohler disease — AVN of the navicular; peak age 3–7 years, boys > girls. Midfoot pain, antalgic gait. XR shows sclerosis, fragmentation, flattening of the navicular. Treatment: short leg walking cast × 6–8 weeks; uniformly self-limiting with complete reconstitution of the navicular.
Freiberg disease (infraction) — AVN/osteochondrosis of the 2nd metatarsal head (less commonly 3rd). Peak age 13–18, girls > boys. Pain at the 2nd MTP joint, limited ROM. XR: flattening, sclerosis, fragmentation of the MT head. Treatment: stiff-soled shoe, MT pad, activity modification. Refractory: surgical debridement, dorsal closing wedge osteotomy (to redirect viable plantar cartilage into the weight-bearing surface), or joint replacement.
Polydactyly & Syndactyly
Polydactyly — extra digits; postaxial (lateral, 5th toe duplication) most common in the foot. Surgical excision typically at age 9–12 months if causing shoe fitting difficulty or if cosmetically unacceptable. Syndactyly — webbing between toes; rarely causes functional problems in the foot and typically does not require surgery unless involving the hallux or causing angular deformity.
Congenital Vertical Talus
Also known as “rocker-bottom foot”; a rigid flatfoot deformity present at birth caused by irreducible dorsal dislocation of the navicular on the talar head. The talus is vertically oriented with its head pointing plantarly, and the hindfoot is in equinus and valgus. Unlike flexible flatfoot, the deformity does NOT correct with plantarflexion. Lateral radiograph in maximum plantarflexion shows persistent talonavicular dislocation with the talar axis directed toward the plantar surface. Associated with neuromuscular conditions (myelomeningocele, arthrogryposis) and chromosomal abnormalities (trisomy 13, 18) in up to 50% of cases. Treatment: reverse Ponseti method (serial casting with initial plantarflexion and inversion to reduce the talonavicular joint, followed by percutaneous Achilles tenotomy and pinning of the talonavicular joint in reduced position); open reduction if casting fails.
Curly Toes & Overlapping Toes
Curly toes — flexion and varus deviation of the lesser toes (most commonly 3rd, 4th, 5th); caused by tightness of the FDL and FDB tendons; bilateral in 25–50%. Most cases resolve spontaneously by age 6; taping may help. Persistent symptomatic cases: flexor tenotomy (simple percutaneous release of the FDL at the DIP level). Congenital overriding 5th toe (digiti quinti varus) — 5th toe dorsiflexed and adducted, overlying the 4th toe; does not resolve spontaneously. Surgical correction: Butler arthroplasty (racket-handle incision with extensor tenotomy, capsulotomy, and skin plasty) or syndactylization to the 4th toe for simple cases.
Tarsal Coalition (Pediatric Presentation)
See Section 11. Presents in adolescence (10–16 years) as the coalition ossifies. Key presentation: rigid, painful flatfoot with peroneal spasm (protective spasm limiting inversion/supination). Limited subtalar motion on clinical exam. Evaluation: oblique foot XR (calcaneonavicular), CT (talocalcaneal, gold standard for bony coalition), MRI (fibrous or cartilaginous coalition).
19 Podiatric Surgical Principles
Regional Anesthesia for Foot & Ankle Surgery
Regional anesthesia provides excellent intraoperative anesthesia and prolonged postoperative analgesia, reducing opioid requirements.
| Block | Nerves Targeted | Coverage | Technique |
|---|---|---|---|
| Ankle block | All 5 nerves at the ankle | Entire foot distal to ankle | Infiltration of: (1) posterior tibial nerve behind medial malleolus, (2) deep peroneal nerve lateral to EHL tendon at ankle crease, (3) superficial peroneal nerve subcutaneous ring across anterior ankle, (4) sural nerve between lateral malleolus and Achilles, (5) saphenous nerve anterior to medial malleolus |
| Popliteal sciatic block | Tibial + common peroneal (sciatic division) | Entire foot and ankle except medial ankle (saphenous) | Ultrasound-guided injection at the popliteal fossa where sciatic nerve divides (typically 5–8 cm proximal to popliteal crease); 20–30 mL local anesthetic; provides 12–24 hour analgesia |
| Mayo block (1st MT) | Digital nerves to hallux | Great toe | Circumferential block at the base of 1st metatarsal; used for hallux surgery (bunion, nail procedures) |
| Digital block | Proper digital nerves | Single toe | Injection at the base of the toe (dorsal approach, 1–2 mL per side); NO epinephrine historically, though recent evidence supports its safety in digital blocks |
Surgical Approaches
Dorsal — most common approach for metatarsal osteotomies, hammertoe correction, Lisfranc ORIF; between extensor tendons, protecting the neurovascular bundle. Medial — used for bunion correction (1st MTP), navicular procedures, medial column arthrodesis, posterior tibial tendon repair. Lateral — calcaneus ORIF (extensile lateral or sinus tarsi), peroneal tendon surgery, lateral ankle stabilization, 5th metatarsal fixation. Plantar — reserved for plantar fasciotomy, sesamoidectomy, plantar plate repair (increasingly done through dorsal approach), Morton neuroma excision (some prefer dorsal). Plantar incisions should avoid weight-bearing surfaces and be placed along non-weight-bearing margins when possible to reduce painful scar formation.
Tourniquet
An ankle tourniquet (pneumatic or Esmarch bandage at 250 mmHg) provides adequate hemostasis for forefoot and midfoot surgery. A thigh tourniquet (250–300 mmHg, or limb occlusion pressure + 100 mmHg) is used for rearfoot and ankle surgery. Maximum safe tourniquet time: 2 hours for a thigh tourniquet; reperfuse for 15–20 minutes before reinflation. Contraindications: severe PVD, DVT, sickle cell disease.
Fixation Principles
Screws — cortical (fully threaded, functions as a positioning device unless using lag technique with glide hole) and cancellous (partially threaded, provides lag compression across fracture). Lag screw technique: glide hole in near cortex, thread hole in far fragment → compression across fracture. Headless compression screws (Herbert-type): used in articular fractures (sesamoid, talar dome). Plates — neutralization (protects a lag screw), buttress (prevents shear), bridging (spans comminution), locking (angular stability, useful in osteoporotic bone). K-wires (Kirschner wires) — temporary fixation, hammertoe/claw toe correction; removed at 4–6 weeks; risk: pin tract infection (5–10%). Staples — memory compression staples for arthrodesis (e.g., 1st TMT). External fixation — used in Charcot reconstruction, severely comminuted calcaneus fractures, limb salvage with soft tissue compromise.
Bone Healing
Primary (direct) bone healing — occurs with anatomic reduction and rigid fixation (absolute stability, interfragmentary strain <2%); haversian remodeling without visible callus. Secondary (indirect) bone healing — occurs with relative stability (strain 2–10%); involves inflammation → soft callus → hard callus → remodeling; visible callus on XR. Most fracture healing is secondary. Time to union: forefoot osteotomies 4–6 weeks; midfoot/hindfoot arthrodesis 8–12 weeks; ankle arthrodesis 12–16 weeks.
Factors Affecting Bone Healing
| Factor | Effect on Healing | Clinical Significance |
|---|---|---|
| Smoking | Nicotine causes vasoconstriction, reduces oxygen delivery, impairs osteoblast function | Non-union rate 2–4× higher in smokers; cessation ≥4–6 weeks preoperatively strongly recommended; many surgeons will not perform elective arthrodesis in active smokers |
| Diabetes | Hyperglycemia impairs angiogenesis and collagen synthesis; neuropathy delays recognition of overloading | Perioperative glucose control (HbA1c <8%, ideally <7%); infection risk 2–3× higher; healing time may be 50% longer |
| NSAIDs | Prostaglandin inhibition may impair inflammatory phase of healing and osteoblast differentiation | Controversial; many surgeons avoid NSAIDs for 6–8 weeks after osteotomy or arthrodesis; selective COX-2 inhibitors may be less harmful than non-selective NSAIDs |
| Vitamin D deficiency | Impaired calcium absorption and bone mineralization | Check 25-OH vitamin D preoperatively; supplement if <30 ng/mL; optimize to ≥40 ng/mL for arthrodesis |
| Mechanical stability | Excessive motion at the fracture/osteotomy site prevents callus maturation | Rigid fixation, appropriate immobilization, and patient compliance with weight-bearing restrictions are essential |
Post-operative Protocols
| Procedure | Weight-Bearing | Immobilization |
|---|---|---|
| Hallux valgus (distal osteotomy) | Immediate in post-op shoe (heel-weighted) | Post-op shoe × 4–6 weeks |
| Hallux valgus (Lapidus) | NWB × 6–8 weeks (traditional) or immediate WB with locking plate | CAM boot × 6–8 weeks, then supportive shoe |
| Hammertoe arthroplasty/arthrodesis | Immediate in post-op shoe | Post-op shoe × 4–6 weeks; K-wire removal at 4 weeks |
| Calcaneus ORIF | NWB × 10–12 weeks | Splint → CAM boot; early ROM at 2 weeks |
| Ankle ORIF | NWB × 6 weeks | Splint × 2 weeks → CAM boot; progressive WB at 6 weeks |
| Ankle arthrodesis | NWB × 8–12 weeks | SLC or CAM boot; CT at 12 weeks to confirm union |
| Total ankle replacement | NWB × 4–6 weeks | Splint → CAM boot; progressive WB at 6 weeks |
| 1st MTP arthrodesis | Heel WB in post-op shoe immediately | Post-op shoe × 6–8 weeks; XR at 6 weeks to confirm union progression |
| Triple arthrodesis | NWB × 8–10 weeks | SLC × 6 weeks → CAM boot; CT at 10–12 weeks to confirm union |
| Plantar fasciotomy | Heel WB in post-op shoe day 1 | Post-op shoe × 2–3 weeks; transition to supportive shoe with orthotic |
| Achilles tendon repair | NWB × 2 weeks, then progressive WB in equinus boot | Splint in plantarflexion × 2 weeks → boot with heel wedges (remove one every 2 weeks) × 8 weeks; PT begins at 6 weeks |
| Gastrocnemius recession (Strayer) | WB in boot immediately | CAM boot × 2–4 weeks; start calf stretching at 4 weeks; full activity at 3 months |
Perioperative VTE Prophylaxis
Venous thromboembolism risk after foot and ankle surgery is lower than after hip/knee arthroplasty but must be considered, particularly with prolonged non-weight-bearing immobilization. Risk factors warranting chemoprophylaxis: NWB >4 weeks, history of VTE, active malignancy, BMI >40, combined oral contraceptive or hormone replacement use, inherited thrombophilia, age >60. For high-risk patients: low-molecular-weight heparin (enoxaparin 40 mg SC daily) or rivaroxaban 10 mg daily for the duration of immobilization. Mechanical prophylaxis (calf compression, ankle pumps, early mobilization when permitted) for all patients.
Postoperative Wound Complications
Surgical site infection (SSI) — occurs in 2–4% of clean elective foot surgery; higher in diabetic patients (up to 10%), smokers, and patients on immunosuppressants. Risk reduction: perioperative antibiotics (cefazolin 2 g IV within 60 minutes of incision), meticulous hemostasis, tension-free closure, avoidance of tourniquet time >2 hours, smoking cessation ≥4 weeks preoperatively. Wound dehiscence — more common in diabetic patients and those with vascular compromise; manage with local wound care and secondary closure or skin grafting if needed. Delayed union / non-union — risk factors: smoking (single greatest modifiable risk factor), diabetes, NSAID use during bone healing (controversial but often avoided in the early postoperative period), inadequate fixation, infection.
20 Soft Tissue Procedures
Tendon Repair Techniques
Krackow suture — a locking whipstitch pattern that provides superior pull-out strength; standard technique for Achilles tendon repair. Typically uses a strong non-absorbable suture (#2 FiberWire or equivalent). Two Krackow locking loops in each tendon stump, tied with the foot in slight (~20°) plantarflexion. Kessler suture (modified) — a core suture technique with grasping loops inside the tendon substance; commonly used for flexor and extensor tendon repairs in the foot. The Bunnell suture is a crisscrossing locking stitch used for tendon-to-bone attachment.
Tendon Transfer Principles
A tendon transfer substitutes the function of a paralyzed or ruptured tendon using a functioning expendable donor. Key principles: (1) the donor must have adequate strength (at least grade 4/5 — transfers lose one grade of strength); (2) the donor must have similar excursion to the recipient; (3) the transferred tendon should have a straight line of pull; (4) the donor should be synergistic with the intended function when possible.
FDL-to-posterior tibial transfer — the most common tendon transfer in podiatry, used in Stage II PTTD. The FDL tendon is detached from its distal insertion, rerouted, and anchored into the navicular (via bone tunnel or interference screw). The FDL is chosen because: (1) similar line of pull to the PT; (2) lies in close proximity behind the medial malleolus; (3) minimal functional deficit from harvest (FHL and intrinsic muscles compensate). Always combined with bony procedures (calcaneal osteotomy, etc.).
Jones procedure — transfer of the extensor hallucis longus (EHL) to the 1st metatarsal neck, combined with IPJ fusion of the hallux. Used for claw toe correction in cavus foot. Girdlestone-Taylor — transfer of the FDL from the plantar surface to the dorsal extensor hood of the lesser toe; corrects flexible claw toe deformity.
Wound Closure Techniques
Primary closure — standard for clean surgical wounds; suture selection: skin closure with non-absorbable monofilament (nylon 3-0 or 4-0, removed at 2–3 weeks for foot) or absorbable subcuticular (Monocryl 4-0). Deep closure with absorbable braided suture (Vicryl 3-0 or 4-0) for capsule, periosteum, and subcutaneous layers. Delayed primary closure — wound left open initially and closed at 3–5 days; used when contamination is a concern (open fractures, infected wounds after debridement). Secondary intention healing — wound left open to granulate and contract; used for infected wounds, partial nail avulsion sites after matrixectomy, and some DFU management. Skin grafts — split-thickness skin graft (STSG) for large wounds with healthy granulation bed; full-thickness skin graft for plantar coverage (more durable). Negative pressure wound therapy (NPWT) — applies subatmospheric pressure (−75 to −125 mmHg) via an occlusive dressing; promotes granulation tissue formation, reduces edema, removes exudate; commonly used as a bridge to definitive closure or grafting in complex wounds.
Ganglion Excision
Ganglion cysts in the foot most commonly arise from the dorsal midfoot joints (TMT, naviculocuneiform). They present as firm, non-tender, translucent masses that transilluminate with a penlight (distinguishing them from solid tumors). Ultrasound confirms the cystic nature (anechoic fluid-filled structure with posterior acoustic enhancement) and identifies the stalk to the originating joint. Treatment: aspiration with an 18-gauge needle + corticosteroid injection (0.5 mL triamcinolone 40 mg/mL; high recurrence ~50% because the stalk is not addressed); surgical excision with identification and removal of the stalk to its joint capsule origin (recurrence ~5–10%). Avoid dorsal digital nerve injury during dorsal foot ganglion excision. Recurrent ganglions after excision may require more aggressive capsular resection.
Plantar Fibroma Excision
Plantar fibromatosis (Ledderhose disease) produces firm nodules within the plantar fascia, analogous to Dupuytren in the hand. Conservative: orthotic with fascia accommodation, topical verapamil, corticosteroid injection (may reduce size temporarily). Surgical: wide local excision of the involved fascia (subtotal fasciectomy) to minimize recurrence (~60% recurrence with simple enucleation, ~10–25% with wide excision). Risk of painful plantar scar and arch destabilization.
Skin Plasty Techniques
Z-plasty — transposes two triangular flaps to lengthen a contracted scar or change its direction; each limb should be 60° (provides ~75% length gain). Used for contracted digital scars or web space contractures. V-Y advancement — a V-shaped flap advanced distally and closed as a Y; used for digital tip reconstruction and lengthening of contracted soft tissue. Both techniques are essential tools for addressing post-surgical or post-traumatic contractures in the foot.
21 Arthrodesis & Joint Replacement
First MTP Arthrodesis (Fusion)
The gold standard for end-stage hallux rigidus and salvage for failed hallux valgus surgery. Optimal fusion position: 10–15° dorsiflexion relative to the 1st metatarsal (allows toe-off without impingement), 10–15° valgus (matches normal alignment), slight pronation (to allow pulp of hallux to contact ground). Test position intraoperatively by placing the foot flat on a surface — the hallux should rest flat without excessive pressure. Fixation: dorsal plate + lag screw (most stable construct), or crossed screws (2 cannulated 4.0 mm screws). Union rate: 90–95%. Patients can walk normally but cannot wear high heels (>2 inches) due to loss of MTP dorsiflexion.
Ankle Arthrodesis
Tibiotalar arthrodesis — indications: end-stage ankle arthritis (post-traumatic most common), failed TAR, avascular necrosis, Charcot. Position: neutral dorsiflexion, 5° external rotation (matching contralateral limb), 0–5° hindfoot valgus, slight posterior translation of talus. Fixation: crossed lag screws (2–3 large-fragment cannulated screws), anterior plate, or arthroscopic technique (faster recovery, lower wound complication rate). Union rate: 85–95%. Adjacent joint arthritis (subtalar, midtarsal) develops in 40–60% of patients over 10–20 years.
Tibiotalocalcaneal (TTC) arthrodesis — simultaneous fusion of the tibiotalar and subtalar joints. Indications: combined ankle and subtalar arthritis, Charcot ankle, talar AVN with collapse, revision after failed tibiotalar fusion. Fixation: retrograde intramedullary nail (large diameter, locked). Significant loss of hindfoot motion; adjacent joint compensation limited.
Total Ankle Replacement (TAR)
Modern TAR uses a mobile-bearing or fixed-bearing three-component design (metallic tibial and talar components with an ultra-high-molecular-weight polyethylene [UHMWPE] insert). Current commonly used implants include STAR (mobile-bearing, most long-term data), INFINITY (fixed-bearing, anterior approach), INBONE II (fixed-bearing, intramedullary tibial fixation), Salto Talaris (fixed-bearing), and Zimmer Trabecular Metal (porous tantalum for enhanced bony ingrowth). Indications: end-stage ankle arthritis in patients >50 years, low-demand, adequate bone stock, normal alignment (correctable deformity), intact vascularity, BMI <30 preferred. Contraindications: active or recent infection, Charcot neuroarthropathy, significant talar AVN (>50%), severe malalignment (coronal >15°), peripheral neuropathy, high-demand/heavy labor, insulin-dependent diabetes (relative). TAR preserves ankle ROM (useful for patients who need to walk on uneven terrain, stairs) and reduces adjacent joint degeneration compared to arthrodesis. 10-year survivorship: 80–90%. Complications: wound healing (anterior approach — the anterior tibial tendon and superficial peroneal nerve are at risk), component subsidence (particularly talar component in osteoporotic bone), polyethylene wear, osteolysis, progressive periprosthetic lucency (radiolucent lines >2 mm or progressive are concerning for loosening), gutter impingement (bone formation in the medial or lateral gutters causing painful limitation of motion — may require arthroscopic debridement). Follow-up: weight-bearing radiographs at 6 weeks, 3 months, 6 months, 1 year, then annually; assess component alignment, subsidence, periprosthetic lucency, and gutter impingement.
Subtalar Arthrodesis
Indications: post-traumatic subtalar arthritis (commonly after calcaneus fracture), tarsal coalition (failed resection), posterior tibial tendon dysfunction (component of triple arthrodesis), inflammatory arthropathy. Fixation: 1–2 large cannulated screws from the posterior calcaneus into the talar body, or lateral plate. Position: 5° valgus. Union rate: 85–95%.
Surgical technique considerations: Joint surfaces are denuded of cartilage using a combination of osteotomes, curettes, and a sagittal saw or burr. Subchondral bone is fenestrated (“fish-scaling” or drilling multiple 2.0 mm holes) to expose bleeding bone and promote vascular ingrowth. Bone graft (autogenous iliac crest, calcaneal, or allograft) is packed into the joint for large defects or revision cases. The sinus tarsi approach (oblique incision from the tip of the fibula to the base of the 4th metatarsal) provides excellent visualization of the posterior facet with less wound complication risk than the extensile lateral approach. Arthroscopic subtalar arthrodesis is gaining popularity for straightforward cases (no significant deformity), offering faster recovery and lower wound complication rates.
Triple Arthrodesis
Fusion of three joints: subtalar (talocalcaneal), talonavicular, and calcaneocuboid. Indications: rigid flatfoot (PTTD Stage III), rigid cavovarus foot, severe tarsal coalition, neuromuscular deformity, rheumatoid hindfoot arthritis. Eliminates hindfoot inversion/eversion and forefoot abduction/adduction. Fixation: screws and/or staples at each joint. Position: neutral dorsiflexion, 5° hindfoot valgus, forefoot aligned. Powerful deformity correction but significant stiffness. Compensatory midfoot/ankle arthritis may develop over time.
22 Orthotic Therapy
Types of Orthotics
Custom orthotics — fabricated from a cast or 3D scan of the patient’s foot. They are prescribed based on individual biomechanical findings. Prefabricated (OTC) orthotics — mass-produced; available in standard sizes; adequate for mild biomechanical abnormalities and as first-line intervention. Evidence shows custom orthotics are superior to prefabricated for specific conditions (PTTD, severe pes planus) but prefabricated devices may be equivalent for plantar fasciitis.
Functional orthotics — designed to control abnormal motion (e.g., overpronation); constructed from semi-rigid to rigid materials (polypropylene, carbon fiber composite); shell extends from heel to just proximal to MT heads; prescribed for biomechanical disorders (plantar fasciitis, PTTD, hallux valgus prevention). Accommodative orthotics — designed to redistribute pressure and cushion the foot; constructed from soft materials (EVA, Plastazote, PPT foam, leather); full-length; prescribed for the diabetic/neuropathic foot, RA, and elderly patients with atrophic tissue.
Orthotic Prescription Elements
| Element | Function |
|---|---|
| Rearfoot post (medial or lateral) | Controls calcaneal position: medial post limits eversion (overpronation); lateral post limits inversion (cavus foot) |
| Forefoot extension/post | Medial forefoot post for forefoot varus; lateral forefoot post for forefoot valgus; accommodates plantarflexed 1st ray |
| Metatarsal pad | Placed proximal to the MT heads to redistribute pressure off the MT heads and support the transverse arch; key for metatarsalgia, Morton neuroma, IPK |
| Dancer pad (reverse Morton extension) | Cutout under 1st MT head with buildup under 2nd–5th MTs; offloads sesamoids and 1st MT head |
| Deep heel cup | Stabilizes the calcaneus, prevents heel slippage, improves rearfoot control |
| Topcover | Contact surface material: leather (durable), Spenco/PPT (cushioning), Plastazote (heat-moldable for diabetic) |
Specialized Bracing
UCBL (University of California Biomechanics Laboratory) orthotic — a deep-cupped, rigid heel control device that extends above the heel and up the medial and lateral walls of the foot; provides maximum rearfoot control. Indicated for pediatric flexible flatfoot, early PTTD (Stage I–IIA), and adult flexible flatfoot. Arizona brace — an ankle-foot orthosis (AFO) consisting of a custom leather gauntlet laced around the ankle and hindfoot; provides control of both the ankle and subtalar joint. Indicated for PTTD Stage II when an orthotic alone is insufficient, ankle instability, and early Charcot (after TCC). CROW boot (Charcot Restraint Orthotic Walker) — a total contact custom bivalved clamshell AFO; the definitive brace for Charcot in the consolidation phase (Stage II–III).
Diabetic Footwear — Medicare Requirements
Under the Therapeutic Shoe Bill, Medicare covers one pair of extra-depth shoes + 3 pairs of molded insoles (or 1 pair of custom-molded shoes if extra-depth shoes are inadequate) per calendar year for patients with diabetes + one of the following: history of partial/complete amputation, history of foot ulcer, callus that could lead to ulceration, peripheral neuropathy with callus formation, foot deformity, or poor circulation. A podiatrist or other qualifying prescriber must certify the need; the shoes must be fitted by a qualified individual (pedorthist, orthotist, podiatrist).
Casting and Scanning Techniques
Plaster casting — traditional gold standard for capturing the foot in its corrected (neutral subtalar) position. The Root technique positions the subtalar joint in neutral (talar head equally palpable medially and laterally) and locks the midtarsal joint by loading the 4th and 5th rays dorsally. The cast captures this corrected relationship for the orthotic lab. Foam box impression — semi-weight-bearing impression into phenolic foam; simpler and faster than plaster but less precise for capturing rearfoot position; adequate for accommodative devices. 3D scanning — optical or laser scanning of the foot; increasing adoption due to speed, digital storage, and compatibility with CAD/CAM fabrication; accuracy comparable to plaster casting when performed in the subtalar neutral position.
Condition-Specific Orthotic Prescriptions
| Condition | Orthotic Type | Key Features |
|---|---|---|
| Plantar fasciitis | Functional (semi-rigid) | Deep heel cup, medial arch support, slight medial rearfoot post (4°), cushioned topcover; prefabricated may be adequate initially |
| PTTD Stage I–II | Functional (rigid) or UCBL | Maximum medial arch support, medial rearfoot post, medial flange; UCBL for moderate cases; Arizona brace if orthotic insufficient |
| Diabetic neuropathy | Accommodative (full-length) | Multi-density: firm base (EVA) + soft topcover (Plastazote); total contact to distribute pressure; must fit in extra-depth shoe; replace every 6–12 months as materials compress |
| Cavus foot | Functional with accommodation | Lateral rearfoot post (2–4°), lateral flange; forefoot valgus post; cushioned topcover for shock absorption; accommodative fill under the high arch |
| Morton neuroma | Functional with MT pad | Metatarsal pad placed proximal to 3rd interspace to splay MT heads and decompress the nerve; wide toe box shoe essential |
| Hallux rigidus | Functional with Morton extension | Carbon fiber or rigid extension under the 1st MTP to limit dorsiflexion; turf toe plate for athletes |
23 Physical Therapy & Rehabilitation
Ankle Rehabilitation Protocol
Following ankle sprain or surgery, a progressive rehabilitation program reduces recurrence and chronic instability:
Phase 1 (Acute, 0–2 weeks): RICE (rest, ice, compression, elevation); gentle active ROM (ankle alphabet, towel pulls); isometric strengthening (submaximal); pain-free weight-bearing as tolerated. Phase 2 (Subacute, 2–6 weeks): Progressive ROM (full dorsiflexion goal — knee-to-wall test, ≥10 cm from wall); resistance band exercises (inversion, eversion, dorsiflexion, plantarflexion); early proprioception (single-leg stance on stable surface, progress to foam/wobble board). Phase 3 (Return to Activity, 6–12 weeks): Advanced proprioception (BAPS board, unstable surfaces); sport-specific agility (cutting, jumping, lateral movements); progressive return to running; functional testing (single-leg hop for distance, Y-balance test).
Eccentric Loading Protocols
Alfredson protocol (Achilles tendinopathy) — 3 sets of 15 repetitions of eccentric heel drops, performed both with the knee straight (targets gastrocnemius) and knee bent (targets soleus), twice daily (180 reps total/day) for 12 weeks. Starting position: bilateral heel raise on a step; then slowly lower the affected heel below the step level over 3–5 seconds (eccentric phase). Use the unaffected leg to return to starting position (avoid concentric loading of the affected side). Pain during the exercise is expected and acceptable; stop only if pain becomes disabling. Add weight (backpack) when exercises become pain-free. ~60–80% good/excellent outcomes in midportion tendinopathy. Heavy slow resistance (HSR) training is an alternative: 3 exercises (seated calf raise, standing calf raise, leg press calf raise), 3 sessions/week, 12 weeks; progressive loading from 15-RM to 6-RM; comparable outcomes to Alfredson with better patient satisfaction (fewer repetitions).
Intrinsic Foot Strengthening
Short foot exercise — patient contracts the intrinsic foot muscles to raise the medial longitudinal arch while keeping the toes flat on the ground (“foot doming”). Activates the abductor hallucis, flexor digitorum brevis, and quadratus plantae. Evidence supports short foot exercises for improving arch height, dynamic balance, and plantar fasciitis symptoms. Other intrinsic exercises: towel curls, marble pick-ups, toe yoga (independent great toe elevation while keeping lesser toes on ground and vice versa).
Toe spread and press exercises — actively spread the toes apart (abduction) and press them into the ground without curling; targets the interossei and lumbricals. Heel raise with toe extension — engage the windlass mechanism by maintaining toe extension while performing a heel raise; strengthens intrinsic muscles in a functional closed-chain position. A progressive intrinsic strengthening program (3–4 exercises, 3 sets of 10–15 repetitions, performed daily for 8–12 weeks) has demonstrated benefit for plantar fasciitis, early PTTD, and medial tibial stress syndrome. These exercises are best taught by a physical therapist and can be verified with EMG biofeedback in research settings.
Manual Therapy
Joint mobilization techniques: talocrural posterior glide (improves dorsiflexion — particularly after immobilization), subtalar distraction and glides, 1st MTP dorsal glide (for hallux rigidus). Soft tissue mobilization: deep tissue massage of the plantar fascia, cross-friction massage of the Achilles tendon, instrument-assisted soft tissue mobilization (IASTM/Graston technique) for chronic tendinopathy and fasciopathy.
Modalities
Extracorporeal shockwave therapy (ESWT) — radial or focused acoustic waves; Level I evidence for chronic plantar fasciitis (2000–3000 impulses, 3 sessions, weekly); Level II for Achilles tendinopathy. Mechanism: stimulates neovascularization and growth factor release. Therapeutic ultrasound — 1 MHz continuous mode for deep tissues (e.g., Achilles, plantar fascia); limited evidence for standalone efficacy; may enhance phonophoresis drug delivery. Low-level laser therapy (LLLT) — some evidence for plantar fasciitis and Achilles tendinopathy; mechanism: photobiomodulation enhancing cellular metabolism. Cryotherapy — ice massage for acute inflammation and post-exercise recovery.
Return-to-Sport Criteria
Objective functional testing should guide return-to-sport decisions rather than time alone. Key criteria include:
| Test | Criteria for Clearance | Application |
|---|---|---|
| Single-leg heel raise | ≥25 repetitions, equal to contralateral side | Achilles tendon repair/tendinopathy; gastrocnemius recession; ankle fracture |
| Single-leg hop for distance | ≥90% of contralateral limb (limb symmetry index) | All foot/ankle injuries requiring return to running/jumping sports |
| Y-balance test | Composite reach distance within 4 cm of contralateral side; no single-direction asymmetry >4 cm | Ankle sprain, CAI, post-ankle surgery; identifies dynamic balance deficits |
| Star excursion balance test | No asymmetry >4 cm in any direction | Ankle instability rehabilitation |
| Timed single-leg stance (eyes closed) | ≥30 seconds without loss of balance | Proprioceptive readiness; ankle sprain recovery |
24 Classification Systems
Wagner Classification (Diabetic Foot Ulcers)
| Grade | Description |
|---|---|
| 0 | At-risk foot: intact skin, bony deformity, neuropathy |
| 1 | Superficial ulcer |
| 2 | Deep ulcer to tendon, capsule, or bone |
| 3 | Deep ulcer with abscess, osteomyelitis, or septic arthritis |
| 4 | Localized gangrene (forefoot or heel) |
| 5 | Extensive gangrene of entire foot |
University of Texas (UT) Classification
| Grade \ Stage | A (clean) | B (infected) | C (ischemic) | D (infected + ischemic) |
|---|---|---|---|---|
| 0 (epithelialized) | 0A | 0B | 0C | 0D |
| I (superficial) | IA | IB | IC | ID |
| II (tendon/capsule) | IIA | IIB | IIC | IID |
| III (bone/joint) | IIIA | IIIB | IIIC | IIID |
Eichenholtz Classification (Charcot Neuroarthropathy)
| Stage | Name | Features |
|---|---|---|
| 0 | Prodromal | Warm, swollen foot; normal XR; MRI shows marrow edema |
| I | Fragmentation | Osseous fragmentation, subluxation, debris; maximum inflammation |
| II | Coalescence | New bone formation, debris absorption, sclerosis; decreasing warmth |
| III | Consolidation | Remodeled bone, stable architecture, residual deformity; no warmth |
Sanders Classification (Calcaneus Fractures)
| Type | Description |
|---|---|
| I | Non-displaced posterior facet (<2 mm) |
| II (A/B/C) | Two-part: single fracture line through posterior facet |
| III (AB/AC/BC) | Three-part: two fracture lines, central depressed fragment |
| IV | Highly comminuted: ≥4 articular fragments |
Hawkins Classification (Talus Fractures)
| Type | Description | AVN Risk |
|---|---|---|
| I | Non-displaced talar neck | ~10% |
| II | Displaced + subtalar dislocation | ~40% |
| III | Displaced + subtalar + tibiotalar dislocation | ~90% |
| IV | Type III + talonavicular dislocation | ~100% |
Weber Classification (Ankle Fractures)
| Type | Fibula Fracture Level | Syndesmosis | Stability |
|---|---|---|---|
| A | Below syndesmosis | Intact | Stable |
| B | At syndesmosis level | Possibly injured | Potentially unstable |
| C | Above syndesmosis | Disrupted | Unstable |
Johnson-Stainsby Classification (PTTD / AAFD)
| Stage | Tendon Status | Deformity | Treatment |
|---|---|---|---|
| I | Tenosynovitis; tendon intact | None; normal arch | Immobilization, orthotic, PT |
| II | Elongated/degenerated | Flexible flatfoot | FDL transfer + calcaneal osteotomy ± additional procedures |
| III | Severely degenerated/ruptured | Rigid flatfoot | Triple or double arthrodesis |
| IV | As Stage III + deltoid failure | Rigid flatfoot + ankle valgus | TTC fusion or deltoid reconstruction |
25 Surgical Hardware Quick Reference
| Hardware | Typical Size | Common Applications | Notes |
|---|---|---|---|
| Cortical screw | 2.7 mm, 3.5 mm, 4.5 mm | Plate fixation, lag technique in cortical bone | Fully threaded; use glide hole for lag effect |
| Cancellous screw | 4.0 mm, 6.5 mm, 7.0 mm | Arthrodesis, metaphyseal fractures, calcaneus | Partially threaded; provides interfragmentary compression |
| Cannulated screw | 3.0–7.3 mm | Guided placement over K-wire; ankle fusion, calcaneus, Jones fracture | Headless variants for articular work |
| Headless compression screw (Herbert/Acutrack) | 2.5–4.7 mm | Sesamoid fracture, talar OCD, scaphoid, 1st MTP fusion | Variable pitch provides compression; fully buried |
| K-wire (Kirschner wire) | 0.045–0.062 inch | Hammertoe fixation, temporary fracture fixation, guide for cannulated screws | Remove at 4–6 weeks; pin tract infection 5–10% |
| Locking plate | Variable | Calcaneus, Lapidus, pilon fracture, ankle fusion | Angular stability; ideal for osteoporotic bone and bridging comminution |
| 1/3 tubular plate | 3.5 mm holes | Fibula fixation (Weber B/C), 5th MT | Low-profile neutralization plate |
| Memory compression staple | Various | Arthrodesis (1st TMT, midfoot, IP joints) | Nitinol shape-memory alloy provides constant compression |
| Intramedullary nail (retrograde) | 10–12 mm diameter | TTC fusion, tibia fracture | Load-sharing device; allows early weight-bearing in some protocols |
| External fixator | Various pin/ring sizes | Charcot reconstruction, open fractures, limb salvage, Ilizarov correction | Spanning fixation; useful with compromised soft tissue |
| Suture anchor | 2.3–5.5 mm | Brostrom repair, insertional Achilles repair, plantar plate repair | Bioabsorbable or metallic; loaded with high-strength suture |
| Intramedullary toe implant | Various | Hammertoe arthrodesis (PIP fusion) | Replaces K-wire for PIP fusion; no pin protrusion; PEEK or metallic |
26 ABI & Vascular Assessment Interpretation
Ankle-Brachial Index (ABI)
| ABI Value | Interpretation | Clinical Significance |
|---|---|---|
| >1.3 | Non-compressible (calcified arteries) | Common in diabetes and ESRD; ABI unreliable; use TBI or TcPO2 instead |
| 1.0–1.3 | Normal | Adequate arterial perfusion for wound healing |
| 0.9–0.99 | Borderline / acceptable | Mild PAD; monitor; likely adequate for healing |
| 0.6–0.89 | Moderate PAD | Claudication common; wound healing may be impaired; vascular referral for non-healing ulcers |
| 0.4–0.59 | Severe PAD | Rest pain likely; high risk of non-healing; vascular consultation mandatory before surgery |
| <0.4 | Critical limb ischemia | Tissue loss/gangrene; urgent vascular intervention needed; elective surgery contraindicated |
Toe-Brachial Index (TBI)
Digital arteries are less susceptible to medial calcinosis than ankle vessels, making TBI more reliable than ABI in diabetic patients. Normal TBI: ≥0.7. Healing threshold: TBI ≥0.6 generally adequate for healing of minor wounds. TBI <0.25 indicates critical ischemia.
Transcutaneous Oxygen Pressure (TcPO2)
| TcPO2 (mmHg) | Interpretation |
|---|---|
| >40 | Adequate perfusion; good healing potential |
| 30–40 | Borderline; healing possible but delayed |
| 20–29 | Poor perfusion; healing unlikely without revascularization |
| <20 | Critical ischemia; revascularization required for wound healing |
Skin Perfusion Pressure (SPP)
SPP ≥40 mmHg predicts healing in ~80% of wounds; SPP ≥30 mmHg is the minimum threshold for healing. SPP is independent of arterial calcification and can be measured at the specific wound site. SPP is measured using a laser Doppler sensor beneath a blood pressure cuff on the dorsum or plantar surface of the foot; as the cuff deflates, the pressure at which blood flow returns to the skin is recorded as the SPP value.
Vascular Assessment Decision Algorithm
Mandatory referral (before elective surgery or for non-healing wound): ABI <0.5; TBI <0.4; TcPO2 <30 mmHg at wound site; monophasic Doppler waveforms; absent pedal pulses with non-healing ulcer; rest pain; gangrene of any extent.
Consider referral: ABI 0.5–0.8 with planned surgery that requires incisional healing; delayed wound healing (>4 weeks without progress) despite adequate offloading and infection control; claudication limiting rehabilitation.
Revascularization options: Endovascular (angioplasty ± stenting) is first-line for tibial and peroneal disease; surgical bypass (femoral-popliteal, femoral-tibial with autologous vein graft) for extensive or multi-segment disease. Angiosome-directed revascularization (restoring direct arterial flow to the angiosome containing the wound) may improve wound healing outcomes.
Segmental Pressures & Waveforms
A pressure gradient >20 mmHg between adjacent segments (high thigh → above knee → below knee → ankle) indicates a hemodynamically significant stenosis at that level. Doppler waveform morphology: triphasic (normal) → biphasic (mild disease) → monophasic (significant disease, loss of reverse flow component). Duplex ultrasound with peak systolic velocity ratios localizes stenoses for surgical planning.
Performing the ABI
Equipment: handheld continuous-wave Doppler (5–10 MHz probe), sphygmomanometer with appropriately sized cuffs for the arm and ankle. Technique: patient rests supine for 10 minutes before measurement. Measure systolic pressure in both brachial arteries (use the higher value as the denominator). At the ankle, place the cuff just above the malleoli and measure systolic pressure in the dorsalis pedis and posterior tibial arteries separately (use the higher of the two as the numerator). Calculate ABI for each leg: ABI = highest ankle pressure / highest brachial pressure.
Common pitfalls: (1) Using too small a cuff (falsely elevates pressure); cuff bladder width should be ≥40% of limb circumference. (2) Not allowing the patient to rest before measurement (exercise elevates pressure). (3) Relying on ABI alone in diabetic patients with calcified arteries (false elevation). (4) Not checking both pedal arteries (the higher value is used because a single vessel may be occluded while the other is patent). (5) Performing the test in a cold environment (vasoconstriction lowers ankle pressure).
27 Common Medications
NSAIDs
| Drug | Dose | Notes |
|---|---|---|
| Ibuprofen | 400–800 mg PO q6–8h (max 3200 mg/day) | First-line OTC NSAID; GI risk; renal caution |
| Naproxen | 250–500 mg PO BID (max 1500 mg/day) | Longer half-life; lower cardiovascular risk than other NSAIDs |
| Meloxicam | 7.5–15 mg PO daily | COX-2 preferential; once daily; favorable GI profile |
| Celecoxib | 100–200 mg PO BID | COX-2 selective; reduced GI risk; cardiovascular caution |
| Ketorolac | 15–30 mg IV/IM q6h or 10 mg PO q4–6h (max 5 days) | Potent analgesic; short-term perioperative use only; renal/GI risk with extended use |
Antibiotics for Diabetic Foot Infection
| Severity | Drug | Dose | Duration |
|---|---|---|---|
| Mild (oral) | Amoxicillin-clavulanate | 875/125 mg PO BID | 1–2 weeks |
| Cephalexin | 500 mg PO QID | 1–2 weeks | |
| Clindamycin | 300–450 mg PO QID | 1–2 weeks | |
| Moderate (IV) | Ampicillin-sulbactam | 3 g IV q6h | 2–4 weeks total |
| Piperacillin-tazobactam | 3.375–4.5 g IV q6h | 2–4 weeks total | |
| Ertapenem | 1 g IV daily | 2–4 weeks total | |
| MRSA coverage | Vancomycin | 15–20 mg/kg IV q8–12h (trough 15–20) | Per clinical response |
| Linezolid | 600 mg PO/IV BID | ≤2 weeks preferred (thrombocytopenia risk) | |
| Osteomyelitis | Culture-directed | Per susceptibilities | 4–6 weeks (or 2–4 weeks post-surgical resection) |
Antifungal Agents
| Drug | Indication | Dose | Notes |
|---|---|---|---|
| Terbinafine (oral) | Onychomycosis, moccasin tinea | 250 mg PO daily × 12 weeks (toenails) | Check baseline LFTs; best mycologic cure rate (~70%); allylamine class |
| Itraconazole | Onychomycosis (pulse) | 200 mg PO BID × 1 week/month × 3–4 months | CYP3A4 inhibitor; check LFTs; drug interactions significant; azole class |
| Efinaconazole 10% | Onychomycosis (topical) | Apply daily to nail × 48 weeks | Penetrates nail plate; ~55% mycologic cure |
| Tavaborole 5% | Onychomycosis (topical) | Apply daily to nail × 48 weeks | Boron-based antifungal; ~36% mycologic cure |
| Terbinafine 1% cream | Tinea pedis | Apply BID × 2 weeks | Most effective topical for dermatophytes |
| Clotrimazole 1% cream | Tinea pedis | Apply BID × 4 weeks | OTC; azole class; broad spectrum |
Neuropathic Pain Agents
| Drug | Dose | Notes |
|---|---|---|
| Gabapentin | Start 300 mg PO nightly, titrate to 300–600 mg TID (max 3600 mg/day) | First-line; renal dose adjustment; sedation, dizziness; no hepatotoxicity |
| Pregabalin | Start 75 mg PO BID, titrate to 150–300 mg BID (max 600 mg/day) | First-line; faster onset than gabapentin; Schedule V; renal dosing |
| Duloxetine | 30 mg PO daily × 1 week, then 60 mg daily | SNRI; first-line; also effective for musculoskeletal pain; avoid in hepatic impairment |
| Amitriptyline | 10–25 mg PO nightly, titrate to 75 mg | TCA; effective but more side effects (anticholinergic, sedation, cardiac); avoid in elderly |
| Capsaicin 8% patch | Applied in clinic × 30 min to feet (pretreat with lidocaine) | Single application provides 3 months of relief; desensitizes TRPV1 receptors |
| Lidocaine 5% patch | Up to 3 patches to affected area, 12 hours on/12 off | Topical; minimal systemic absorption; adjunctive |
28 Abbreviations Master List
| Abbreviation | Definition |
|---|---|
| AAFD | Adult-acquired flatfoot deformity |
| ABI | Ankle-brachial index |
| AFO | Ankle-foot orthosis |
| AOFAS | American Orthopaedic Foot & Ankle Society |
| ATFL | Anterior talofibular ligament |
| AVN | Avascular necrosis |
| BID | Twice daily |
| BKA | Below-knee amputation |
| BMD | Bone mineral density |
| BMI | Body mass index |
| CAI | Chronic ankle instability |
| CAM | Controlled ankle motion (boot) |
| CFL | Calcaneofibular ligament |
| CMT | Charcot-Marie-Tooth disease |
| CROW | Charcot restraint orthotic walker |
| CT | Computed tomography |
| DFI | Diabetic foot infection |
| DFU | Diabetic foot ulcer |
| DIPJ | Distal interphalangeal joint |
| DLSO | Distal lateral subungual onychomycosis |
| DMAA | Distal metatarsal articular angle |
| DVT | Deep vein thrombosis |
| EDB | Extensor digitorum brevis |
| EHL | Extensor hallucis longus |
| EMG | Electromyography |
| ESRD | End-stage renal disease |
| ESWT | Extracorporeal shockwave therapy |
| EVA | Ethylene vinyl acetate |
| FDL | Flexor digitorum longus |
| FHL | Flexor hallucis longus |
| HVA | Hallux valgus angle |
| IDSA | Infectious Diseases Society of America |
| IMA | Intermetatarsal angle |
| IP / IPJ | Interphalangeal (joint) |
| IPK | Intractable plantar keratosis |
| IV | Intravenous |
| IWGDF | International Working Group on the Diabetic Foot |
| KOH | Potassium hydroxide (preparation) |
| LFT | Liver function tests |
| LLLT | Low-level laser therapy |
| LOPS | Loss of protective sensation |
| MRSA | Methicillin-resistant Staphylococcus aureus |
| MRI | Magnetic resonance imaging |
| MT | Metatarsal |
| MTP | Metatarsophalangeal (joint) |
| NCS | Nerve conduction studies |
| NPWT | Negative pressure wound therapy |
| NSAID | Nonsteroidal anti-inflammatory drug |
| NWB | Non-weight-bearing |
| OCD | Osteochondral defect |
| ORIF | Open reduction internal fixation |
| OTC | Over-the-counter |
| PAD | Peripheral arterial disease |
| PAS | Periodic acid-Schiff (stain) |
| PF | Plantar fasciitis |
| PIPJ | Proximal interphalangeal joint |
| PO | By mouth (per os) |
| PRP | Platelet-rich plasma |
| PSO | Proximal subungual onychomycosis |
| PT | Posterior tibial (tendon) |
| PTB | Probe-to-bone (test) |
| PTFL | Posterior talofibular ligament |
| PTTD | Posterior tibial tendon dysfunction |
| QID | Four times daily |
| RA | Rheumatoid arthritis |
| RICE | Rest, ice, compression, elevation |
| ROM | Range of motion |
| SIRS | Systemic inflammatory response syndrome |
| SLC | Short leg cast |
| SNRI | Serotonin-norepinephrine reuptake inhibitor |
| SPP | Skin perfusion pressure |
| STJ | Subtalar joint |
| TAL | Tendo-Achilles lengthening |
| TAR | Total ankle replacement |
| TBI | Toe-brachial index |
| TCA | Tricyclic antidepressant |
| TCC | Total contact cast |
| TcPO2 | Transcutaneous oxygen pressure |
| TID | Three times daily |
| TMA | Transmetatarsal amputation |
| TMT | Tarsometatarsal |
| TTC | Tibiotalocalcaneal |
| UCBL | University of California Biomechanics Laboratory (orthotic) |
| US | Ultrasound |
| UT | University of Texas (classification) |
| WB | Weight-bearing |
| WSO | White superficial onychomycosis |
| XR | Radiograph (X-ray) |