Urgent Care
Walk-in acute care, laceration repair, fracture management, rapid diagnostic evaluation, point-of-care testing, and every protocol, disposition criteria, and management algorithm across the full scope of urgent care medicine.
01 Urgent Care Scope & Triage
Urgent care occupies a critical niche between primary care and the emergency department, providing walk-in evaluation and management of acute, non-life-threatening conditions. The scope encompasses minor trauma, acute infections, exacerbations of chronic disease, occupational injuries, and a broad range of procedural services. Effective triage is the cornerstone of safe urgent care practice — rapidly identifying patients who require emergency department transfer while efficiently managing the vast majority who can be treated and discharged.
Scope of Practice
Urgent care centers typically manage conditions with low-to-moderate acuity that require same-day evaluation but are not immediately life-threatening. Common presentations include upper respiratory infections (25–30% of visits), musculoskeletal injuries (15–20%), lacerations and wound care (10–15%), urinary complaints (5–10%), skin conditions (5–10%), and eye/ear complaints (5–8%). Most centers offer on-site X-ray, point-of-care testing, laceration repair, splinting, I&D of abscesses, and basic IV capabilities.
ESI Triage Adaptation for Urgent Care
The Emergency Severity Index (ESI) is a five-level triage system designed for EDs but widely adapted for urgent care intake. Patients presenting at ESI levels 1–2 generally require ED transfer; levels 3–5 fall within urgent care scope.
| ESI Level | Description | Examples | Urgent Care Action |
|---|---|---|---|
| 1 — Resuscitation | Immediate life-saving intervention | Cardiac arrest, respiratory failure, active hemorrhage | Call 911, initiate BLS/ACLS, transfer |
| 2 — Emergent | High risk, confused/lethargic, severe pain/distress | Chest pain with ACS features, stroke symptoms, sepsis, anaphylaxis | Stabilize, activate EMS, transfer |
| 3 — Urgent | Stable but needs multiple resources | Abdominal pain needing labs + imaging, moderate asthma exacerbation | Evaluate; treat if within scope, transfer if workup exceeds capability |
| 4 — Less Urgent | Stable, needs one resource | Simple laceration, ankle sprain needing X-ray, UTI with UA | Treat and discharge |
| 5 — Non-Urgent | Stable, no resources needed | Medication refill, minor rash, cold symptoms | Treat and discharge |
Red Flags Requiring ED Transfer
The following presentations exceed urgent care scope and require emergency department evaluation:
Cardiovascular: Chest pain with ischemic features (ST changes, troponin elevation, diaphoresis, radiation to arm/jaw), acute heart failure (severe dyspnea, hypoxia, bilateral rales), suspected aortic dissection (tearing chest/back pain, pulse differential), hemodynamic instability (SBP <90 or MAP <65).
Neurological: Acute stroke symptoms (sudden weakness, speech difficulty, facial droop — last known well <24 hours), seizure (first-time or prolonged), altered mental status, signs of meningitis (fever + nuchal rigidity + headache).
Respiratory: Severe respiratory distress (SpO₂ <90%, accessory muscle use, inability to speak in full sentences), suspected pulmonary embolism (pleuritic chest pain + tachycardia + hypoxia + risk factors), tension pneumothorax.
Sepsis: qSOFA ≥2 (altered mentation, RR ≥22, SBP ≤100) or SIRS criteria with suspected source — fever >38.3°C or <36°C, HR >90, RR >20, WBC >12K or <4K.
Trauma: High-mechanism injury, suspected spinal injury, open fractures, significant head injury (GCS <15, vomiting, amnesia, LOC), penetrating wounds to chest/abdomen/neck.
Other: Acute abdomen with peritoneal signs, GI hemorrhage (hematemesis, melena, hematochezia with instability), ectopic pregnancy (positive HCG + abdominal pain + vaginal bleeding), testicular torsion, diabetic emergencies (DKA, HHS).
Triage Workflow
Upon arrival, each patient undergoes a rapid triage assessment: (1) chief complaint documented, (2) vital signs obtained (HR, BP, RR, SpO₂, temperature — and pain score), (3) acuity determination using ESI adaptation, (4) red flag screening using the transfer criteria above, and (5) disposition decision — urgent care treatment track vs. EMS activation. Abnormal vital signs that mandate immediate reassessment: HR >120 or <50, SBP >200 or <90, RR >28 or <10, SpO₂ <92%, temperature >40°C or <35°C.

Vital Sign Interpretation Pitfalls
Several triage pitfalls deserve emphasis: (1) Pulse oximetry may be falsely normal in carbon monoxide poisoning (SpO₂ reads carboxyhemoglobin as oxyhemoglobin) and falsely low with nail polish, poor perfusion, or dark skin pigmentation. (2) Blood pressure can be falsely elevated by inappropriate cuff size (too-small cuff overestimates BP — always use a cuff with bladder width ≥40% of arm circumference), white-coat effect, or pain. Recheck after pain is addressed. (3) Temperature measurement varies by site: rectal is the gold standard (most accurate), oral is ~0.5°F lower, axillary is ~1°F lower, temporal artery is convenient but variable. In infants <3 months, rectal temperature is mandatory. (4) Heart rate in children is age-dependent — neonates 120–160, infants 100–150, toddlers 80–130, school age 70–110, adolescents 60–100 bpm. Always use age-appropriate reference ranges.
Common Urgent Care Chief Complaints by Frequency
| Rank | Chief Complaint Category | Approximate % | Typical Diagnoses |
|---|---|---|---|
| 1 | Respiratory / ENT | 25–35% | URI, pharyngitis, sinusitis, otitis, bronchitis, cough |
| 2 | Musculoskeletal / Injury | 15–25% | Sprains, strains, fractures, back pain, joint pain |
| 3 | Skin / Wound | 10–15% | Lacerations, abscesses, rashes, bites, burns |
| 4 | Genitourinary | 5–10% | UTI, STI symptoms, vaginal discharge, testicular pain |
| 5 | GI complaints | 5–10% | Nausea/vomiting, diarrhea, abdominal pain, constipation |
| 6 | Eye complaints | 3–5% | Conjunctivitis, corneal abrasion, foreign body, stye |
| 7 | Administrative / Screening | 5–10% | DOT physicals, drug screens, work comp, sports physicals |
| 8 | Other | 5–10% | Allergic reactions, insect bites, medication refills, mental health |
02 Point-of-Care Testing & Diagnostics
Urgent care centers rely heavily on point-of-care testing (POCT) to provide rapid diagnostic results that guide same-visit clinical decisions. Unlike send-out laboratory testing that may take hours to days, POCT delivers results within minutes, enabling efficient evaluation, treatment, and disposition.
Rapid Antigen & Molecular Tests
| Test | Methodology | Turnaround | Sensitivity | Specificity | Clinical Use |
|---|---|---|---|---|---|
| Rapid Strep (GAS) | Immunoassay | 5–10 min | 70–90% | 95–99% | Pharyngitis; if negative in children, send throat culture |
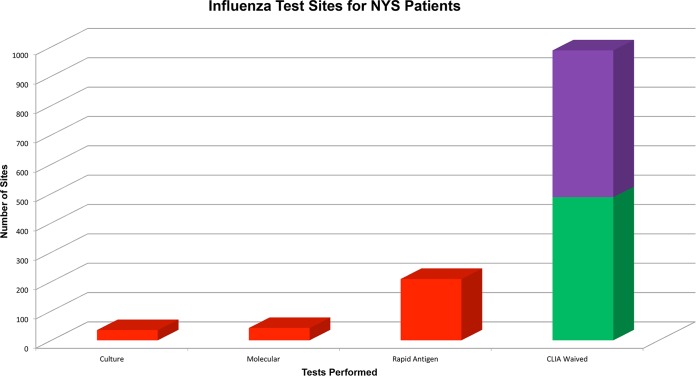
| Influenza A/B rapid | Immunoassay | 10–15 min | 50–70% | 90–99% | ILI during flu season; negative does not rule out |
| Influenza molecular (NAAT) | PCR-based | 15–30 min | 95–99% | 95–99% | Superior to rapid antigen; preferred if available |
| COVID-19 rapid antigen | Lateral flow immunoassay | 15 min | 70–85% | 95–99% | Symptomatic patients; negative may need PCR confirmation |
| COVID-19 NAAT | RT-PCR | 30–60 min | 95–99% | 99% | Gold standard; higher sensitivity than antigen |
| RSV rapid | Immunoassay | 15 min | 80–90% | 90–95% | Pediatric bronchiolitis; cohorting decisions |
| Mono spot (heterophile Ab) | Agglutination | 5 min | 70–90% | 95–100% | EBV mononucleosis; may be negative in first week |
Urinalysis & Urine Studies
Urine dipstick provides immediate semi-quantitative assessment: leukocyte esterase (sensitivity 75–96% for UTI), nitrites (specificity >90% but sensitivity only 45–60% — not all uropathogens reduce nitrates, e.g., Enterococcus, Pseudomonas), blood, protein, glucose, ketones, and pH. Microscopic urinalysis identifies WBCs, RBCs, bacteria, casts, and crystals. Urine culture (UCx) should be sent when: complicated UTI suspected, pyelonephritis, pregnancy, treatment failure, recurrent UTI, or male UTI. Results take 24–48 hours; empiric therapy is started based on dipstick/microscopy.
Urine Pregnancy Test
Qualitative urine beta-HCG detects pregnancy at levels ≥20–25 mIU/mL (positive approximately 1 week after implantation, or by the expected period). Mandatory before any imaging involving radiation in women of reproductive age, and essential in any female of childbearing age presenting with abdominal pain, vaginal bleeding, or syncope.
Cardiac Biomarkers
Some urgent care centers offer point-of-care troponin (qualitative or quantitative). A positive troponin mandates ED transfer for serial trending and cardiology consultation. POC troponin is useful for risk stratification in atypical chest pain, but a single negative troponin does not exclude ACS — serial measurements at 3–6-hour intervals are standard of care, which typically exceeds urgent care capability.
Other POC Labs
| Test | Turnaround | Key Uses in Urgent Care |
|---|---|---|
| Glucose (fingerstick) | 5 seconds | Diabetic emergencies, altered mental status, hypoglycemia |
| CBC (POC analyzer) | 5–10 min | Anemia evaluation, WBC for infection risk stratification |
| BMP/CMP | 10–15 min | Electrolytes, creatinine, glucose; dehydration, renal function |
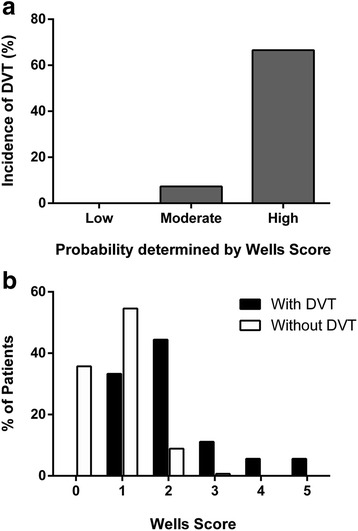
| D-dimer | 10–20 min | Low-probability PE/DVT rule-out (use only with low Wells score) |
| CRP | 5–10 min | Inflammatory marker; helps distinguish bacterial vs viral |
| Procalcitonin | 20 min | Bacterial infection marker; antibiotic stewardship |
| HbA1c (POC) | 5 min | Diabetes screening/monitoring |
| Lipid panel (POC) | 5 min | Cardiovascular risk screening |
Imaging Capabilities
Most urgent care centers have on-site plain radiography (X-ray) for evaluating fractures, dislocations, pneumonia, foreign bodies, and bowel obstruction patterns. Radiographs are typically read by the treating provider with overread by a radiologist within 24–48 hours. Some centers also offer point-of-care ultrasound (POCUS) for FAST exam, soft-tissue abscess localization, DVT evaluation, and pregnancy confirmation. CT, MRI, and advanced imaging require referral to an imaging center or ED.

Urgent care X-ray cannot evaluate for: pulmonary embolism (need CT-PA), appendicitis (need CT or US), aortic dissection (need CT-A), intracranial pathology (need CT/MRI), ligamentous knee/ankle injury (need MRI), or subtle fractures requiring CT (scaphoid, hip, vertebral). When advanced imaging is needed acutely, transfer to the ED; when non-urgent, arrange outpatient imaging with follow-up.
03 Terminology & Abbreviations
Familiarity with urgent care terminology is essential for efficient documentation and communication. The following terms appear frequently in urgent care clinical notes, triage records, and disposition documentation.
| Term / Abbreviation | Definition |
|---|---|
| ACS | Acute coronary syndrome |
| AOM | Acute otitis media |
| AOE | Acute otitis externa |
| BSA | Body surface area (burn assessment) |
| CAP | Community-acquired pneumonia |
| DOT | Department of Transportation (physicals) |
| ED | Emergency department |
| EMS | Emergency medical services |
| ESI | Emergency Severity Index (triage) |
| GAS | Group A Streptococcus |
| I&D | Incision and drainage |
| ILI | Influenza-like illness |
| LNW | Last known well (stroke timing) |
| MDM | Medical decision-making |
| MRSA | Methicillin-resistant Staphylococcus aureus |
| NAAT | Nucleic acid amplification test |
| OTC | Over-the-counter |
| PEP | Post-exposure prophylaxis |
| POC / POCT | Point-of-care (testing) |
| POCUS | Point-of-care ultrasound |
| PRN | As needed (pro re nata) |
| RICE | Rest, ice, compression, elevation |
| RTC | Return to clinic |
| SIRS | Systemic inflammatory response syndrome |
| TM | Tympanic membrane |
| TMP-SMX | Trimethoprim-sulfamethoxazole |
| UA | Urinalysis |
| UCx | Urine culture |
| URI | Upper respiratory infection |
| UTI | Urinary tract infection |
| WC | Workers' compensation |
04 Upper Respiratory Infections & Pharyngitis
Upper respiratory infections account for the single largest category of urgent care visits. The clinical challenge lies in distinguishing viral URI (the vast majority) from bacterial infections requiring antibiotics, and in identifying dangerous complications such as peritonsillar abscess, epiglottitis, or retropharyngeal abscess.
Viral URI (Common Cold)
Caused by rhinovirus (30–50%), coronavirus (10–15%), adenovirus, RSV, parainfluenza, and others. Typical course: nasal congestion, rhinorrhea (initially clear, then may become mucopurulent — this does NOT indicate bacterial infection), sore throat, cough, low-grade fever. Duration 7–10 days with peak symptoms at days 3–4. Treatment is entirely supportive: analgesics (acetaminophen, ibuprofen), decongestants (pseudoephedrine or oxymetazoline spray ≤3 days), antihistamines for rhinorrhea, honey for cough (≥1 year of age), adequate hydration. Antibiotics are never indicated for viral URI.
Pharyngitis — Centor & McIsaac Criteria
The primary clinical question in pharyngitis is whether Group A Streptococcus (GAS) is the cause, since GAS pharyngitis requires antibiotic treatment to prevent acute rheumatic fever. The Centor criteria (modified by McIsaac with age adjustment) guide testing and treatment decisions:
| Criterion | Points |
|---|---|
| Tonsillar exudates or swelling | +1 |
| Tender anterior cervical lymphadenopathy | +1 |
| Fever (history or >38°C / 100.4°F) | +1 |
| Absence of cough | +1 |
| McIsaac age modification: | |
| Age 3–14 years | +1 |
| Age 15–44 years | 0 |
| Age ≥45 years | −1 |
Score 0–1: No testing, no antibiotics. Treat symptomatically. Risk of GAS <10%.
Score 2–3: Perform rapid strep test. Treat only if positive. In children/adolescents, send backup throat culture if rapid test is negative (sensitivity of rapid test ~70–90%). In adults, a negative rapid test is sufficient (lower incidence of rheumatic fever).
Score 4–5: Perform rapid strep test. Consider empiric treatment if high clinical suspicion while awaiting results. Treat if positive.


GAS Pharyngitis Treatment
First-line: Amoxicillin 500 mg PO BID or 1000 mg PO daily × 10 days (children: 50 mg/kg/day divided BID, max 1000 mg/day). Penicillin allergy (non-anaphylactic): Cephalexin 500 mg PO BID × 10 days. Penicillin allergy (anaphylactic): Azithromycin 500 mg day 1, then 250 mg days 2–5 (Z-pack); or clindamycin 300 mg PO TID × 10 days. Note: macrolide resistance in GAS is 5–10% in the US, making azithromycin a second-line choice.
Peritonsillar Abscess (PTA)

Suspect when pharyngitis is accompanied by: unilateral tonsillar swelling, deviation of the uvula, "hot potato" or muffled voice, trismus (difficulty opening mouth), drooling, and severe unilateral pain. Patients appear more toxic than typical pharyngitis. Management: needle aspiration or I&D (if trained), IV/IM antibiotics (ampicillin-sulbactam or clindamycin), and often ED referral for definitive drainage and observation. PTA can progress to parapharyngeal abscess or airway compromise if untreated.
05 Otitis Media & Externa
Acute Otitis Media (AOM)
Diagnostic criteria (AAP 2013 guidelines) require ALL of the following: (1) moderate-to-severe bulging of the tympanic membrane (TM), or new onset otorrhea not due to otitis externa, or mild bulging of the TM with recent onset of ear pain (<48 hours) or intense erythema of the TM; AND (2) presence of middle ear effusion evidenced by bulging TM, limited or absent TM mobility on pneumatic otoscopy, air-fluid level behind TM, or otorrhea. Simple middle ear effusion without signs of acute inflammation is otitis media with effusion (OME) — not AOM — and does NOT require antibiotics.

AOM Management — Watchful Waiting vs. Antibiotics
| Age | Unilateral, Non-Severe | Bilateral, Non-Severe | Severe (Temp ≥39°C or Severe Otalgia ≥48h) |
|---|---|---|---|
| 6–23 months | Antibiotics OR observe* | Antibiotics | Antibiotics |
| ≥24 months | Observe* | Antibiotics OR observe* | Antibiotics |
*Observation option requires: reliable follow-up within 48–72 hours, shared decision-making with parent, and a "safety net" prescription to fill if symptoms worsen or fail to improve. Provide analgesics (ibuprofen or acetaminophen) regardless of antibiotic decision.
AOM Antibiotic Regimens
First-line: Amoxicillin 80–90 mg/kg/day divided BID × 10 days (for age <2 years or severe disease) or × 5–7 days (age ≥2 with mild disease). If amoxicillin failure (no improvement in 48–72 hours): amoxicillin-clavulanate 90 mg/kg/day (amoxicillin component) divided BID × 10 days. Penicillin allergy: cefdinir 14 mg/kg/day divided BID, cefuroxime 30 mg/kg/day divided BID, or cefpodoxime 10 mg/kg/day divided BID × 10 days. Severe penicillin allergy (anaphylaxis): azithromycin 10 mg/kg day 1, then 5 mg/kg days 2–5.
TM Perforation
Spontaneous perforation may occur with AOM, presenting as sudden otorrhea with pain relief. Most perforations heal spontaneously within 2–4 weeks. Management: keep ear dry (cotton ball with petroleum jelly during bathing), topical otic drops (ofloxacin otic — avoid aminoglycoside drops which are ototoxic with perforated TM), oral antibiotics if concurrent AOM. Refer to ENT if perforation persists >3 months.
Acute Otitis Externa (AOE) — "Swimmer's Ear"
Infection of the external auditory canal, most commonly caused by Pseudomonas aeruginosa and Staphylococcus aureus. Presentation: ear pain worsened by tragal pressure or pinna traction, pruritus, canal edema and erythema, purulent discharge. The TM appears normal (if visible).
Treatment: Topical therapy is first-line. Ciprofloxacin 0.3%-dexamethasone 0.1% otic suspension, 4 drops to affected ear BID × 7 days. Alternatives: ofloxacin 0.3% otic drops, or neomycin-polymyxin-hydrocortisone otic (avoid if TM perforation — neomycin is ototoxic). If canal edema is severe, place an ear wick to facilitate drop delivery. Oral antibiotics are added only for: extension beyond the canal (cellulitis of pinna/face), immunocompromised patients, or failed topical therapy.
Suspect malignant otitis externa in diabetic or immunocompromised patients with severe, unrelenting ear pain, granulation tissue in the ear canal floor (at the bony-cartilaginous junction), cranial nerve palsies (especially CN VII), and failure to respond to topical therapy. This is an osteomyelitis of the temporal bone caused by Pseudomonas and requires IV anti-pseudomonal antibiotics and urgent ENT referral. Mortality is significant if untreated. Transfer to ED or arrange urgent ENT consultation.
06 Sinusitis
Acute rhinosinusitis is one of the most common diagnoses in urgent care. The vast majority (90–98%) of cases are viral and self-limited. The critical clinical skill is distinguishing viral from bacterial sinusitis to avoid unnecessary antibiotic prescribing.
Viral vs. Bacterial Sinusitis Criteria
Bacterial sinusitis should be diagnosed when one of the following patterns is present:
1. Persistent symptoms: Symptoms lasting ≥10 days without improvement (nasal discharge, congestion, facial pain/pressure, cough).
2. Worsening pattern ("double-sickening"): Initial improvement followed by new onset of fever, headache, or increased nasal discharge around day 5–7.
3. Severe onset: High fever (≥39°C / 102.2°F) AND purulent nasal discharge or facial pain lasting ≥3 consecutive days at onset of illness.
Treatment of Acute Bacterial Sinusitis
First-line: Amoxicillin-clavulanate 875/125 mg PO BID × 5–7 days (adults) or 45 mg/kg/day (amoxicillin component) divided BID × 10–14 days (children). High-dose amoxicillin-clavulanate (2000/125 mg PO BID) is recommended in areas with high S. pneumoniae resistance (>10%), recent antibiotic use, or daycare attendance. Penicillin allergy: doxycycline 100 mg PO BID × 5–7 days (adults), or respiratory fluoroquinolone (levofloxacin 500 mg daily or moxifloxacin 400 mg daily) × 5 days as a second-line option. Watchful waiting for 7 days with analgesics and nasal saline irrigation is an acceptable option in uncomplicated ABRS without severe symptoms, with antibiotics started if no improvement.
Adjunctive Treatment
Nasal saline irrigation (neti pot or squeeze bottle), intranasal corticosteroids (fluticasone, mometasone) for symptom relief, analgesics (acetaminophen or ibuprofen), and decongestants (pseudoephedrine PO or oxymetazoline nasal ≤3 days to avoid rhinitis medicamentosa). Antihistamines are NOT recommended for sinusitis unless concurrent allergic rhinitis.
Imaging Indications
Routine imaging is NOT recommended for uncomplicated acute sinusitis. Imaging (CT sinus without contrast) is indicated for: suspected complications (orbital or intracranial extension), recurrent sinusitis (≥4 episodes/year), chronic sinusitis (>12 weeks), or when diagnosis is uncertain. Plain sinus X-rays have poor sensitivity and specificity and are no longer recommended.
Complications Requiring Transfer
Orbital complications (Chandler classification): periorbital (preseptal) cellulitis may be manageable with oral antibiotics and close follow-up, but orbital cellulitis (post-septal — proptosis, restricted extraocular movements, vision changes) requires IV antibiotics and CT imaging — transfer to ED. Intracranial complications: meningitis, epidural abscess, subdural empyema, cavernous sinus thrombosis (bilateral orbital signs, CN III/IV/VI palsies) — all require emergent ED transfer.
07 Lower Respiratory — Bronchitis, Asthma Exacerbation, Pneumonia
Acute Bronchitis
An acute cough illness (typically 1–3 weeks) with or without sputum production, in the absence of pneumonia. Etiology is viral in >90% of cases (same pathogens as URI). Sputum color (yellow/green) does NOT distinguish bacterial from viral. Antibiotics are NOT indicated for acute bronchitis. This is one of the most common sources of inappropriate antibiotic prescribing in urgent care. Treatment: symptom management with dextromethorphan, guaifenesin, honey, inhaler for bronchospasm (albuterol PRN), and acetaminophen/ibuprofen for associated discomfort. Duration may be up to 3 weeks — counsel patients on expected timeline to prevent return visits and antibiotic demands.
Asthma Exacerbation
Patients present with wheezing, dyspnea, chest tightness, and cough. Severity assessment includes peak expiratory flow (PEF), respiratory rate, accessory muscle use, ability to speak, and oxygen saturation.
Green zone (80–100% predicted): Mild exacerbation. Treat with albuterol 2–4 puffs via MDI with spacer or nebulizer. Reassess in 20–30 minutes.
Yellow zone (50–80% predicted): Moderate exacerbation. Albuterol nebulizer (2.5 mg) × 3 treatments q20 min, add ipratropium 0.5 mg nebulizer, systemic corticosteroids (prednisone 40–60 mg PO or equivalent).
Red zone (<50% predicted): Severe exacerbation. Continuous albuterol nebulization, ipratropium, systemic corticosteroids, consider ED transfer if no rapid improvement. SpO₂ <90%, inability to speak in sentences, or declining PEF despite treatment = transfer immediately.
Nebulizer Protocol
Albuterol 2.5 mg/3 mL via nebulizer q20 min × 3 doses, then reassess. Ipratropium bromide 0.5 mg may be combined with the first 3 albuterol treatments for moderate-severe exacerbations. Prednisone burst: adults 40–60 mg PO daily × 5 days (no taper needed for ≤7 days); children 1–2 mg/kg/day (max 60 mg) × 3–5 days. Discharge criteria: PEF ≥70% predicted, sustained improvement ≥60 minutes after last treatment, adequate oxygenation (SpO₂ ≥94%), ability to use home medications.
Community-Acquired Pneumonia (CAP)
Suspect pneumonia when cough is accompanied by: fever, productive sputum, pleuritic chest pain, dyspnea, or abnormal lung exam (crackles, decreased breath sounds, egophony). Obtain CXR — an infiltrate on CXR confirms the diagnosis. Vital signs, oxygenation, and clinical appearance determine disposition.
CAP Disposition Decision
| Factor | Treat in Urgent Care | Consider ED Transfer |
|---|---|---|
| Age | <65 with no comorbidities | ≥65 or significant comorbidities |
| Vital signs | Stable (HR <120, RR <24, SBP >90) | Tachycardia, tachypnea, hypotension |
| Oxygenation | SpO₂ ≥94% on room air | SpO₂ <94% or supplemental O₂ needed |
| Mental status | Alert, oriented | Confusion, altered mentation |
| Oral tolerance | Tolerating PO meds/fluids | Unable to take PO, vomiting |
| Imaging | Unilobar infiltrate | Multilobar, pleural effusion, cavitation |
Outpatient CAP treatment (no comorbidities): amoxicillin 1 g PO TID × 5 days; OR doxycycline 100 mg PO BID × 5 days; OR azithromycin 500 mg day 1 then 250 mg days 2–5 (only if local macrolide resistance <25%). With comorbidities (diabetes, COPD, CKD, heart failure, alcoholism): amoxicillin-clavulanate 875/125 mg PO BID PLUS azithromycin or doxycycline; OR respiratory fluoroquinolone alone (levofloxacin 750 mg daily × 5 days).
Influenza Management
During influenza season, patients presenting with acute onset of fever, myalgias, cough, and headache should be tested with rapid molecular assay (preferred) or rapid antigen test. Antiviral treatment with oseltamivir (Tamiflu) 75 mg PO BID × 5 days is recommended for: (1) all hospitalized patients, (2) high-risk outpatients (age ≥65, <2 years, pregnant, immunosuppressed, chronic medical conditions), and (3) any patient within 48 hours of symptom onset. Oseltamivir provides the greatest benefit when started within 24–48 hours but may still be considered beyond 48 hours in high-risk patients. Baloxavir (Xofluza) 40–80 mg PO × 1 dose is an alternative (single-dose convenience). Advise on return precautions: difficulty breathing, persistent vomiting, sudden dizziness, or confusion.
08 Fracture Evaluation & Management
Musculoskeletal injuries are among the most common urgent care presentations. Clinical decision rules help determine which patients need X-rays, and knowledge of splinting techniques allows definitive urgent care management for stable fractures.
Ottawa Ankle Rules
An ankle X-ray series is required only if there is pain in the malleolar zone AND any of the following:
Ankle X-ray indicated if malleolar pain PLUS:
• Bone tenderness at the posterior edge or tip of the lateral malleolus (distal 6 cm), OR
• Bone tenderness at the posterior edge or tip of the medial malleolus (distal 6 cm), OR
• Inability to bear weight (4 steps) both immediately after injury AND in the urgent care center.
Foot X-ray indicated if midfoot pain PLUS:
• Bone tenderness at the base of the 5th metatarsal, OR
• Bone tenderness at the navicular bone, OR
• Inability to bear weight (4 steps) both immediately after injury AND in the urgent care center.
Sensitivity for fracture: 97–100%. These rules reduce unnecessary ankle X-rays by 30–40%. Not validated for age <18 years in all studies, though widely applied to children ≥6 years.
Ottawa Knee Rules
A knee X-ray is required only if any of the following are present: (1) age ≥55 years, (2) tenderness at the head of the fibula, (3) isolated tenderness of the patella (no other bony tenderness), (4) inability to flex the knee to 90°, (5) inability to bear weight (4 steps) both immediately and in the UC center. Sensitivity ~99% for fractures.
X-ray Interpretation Pearls
Systematic approach: assess alignment (joint congruence, angulation), bones (cortical break, trabecular disruption), cartilage/joint space (widening = ligament injury, narrowing = arthritis), soft tissues (swelling, fat pad signs). Key signs: posterior fat pad sign at the elbow is always pathologic and indicates occult fracture (radial head fracture in adults, supracondylar in children) even with normal-appearing bone. Sail sign = anterior fat pad elevation at the elbow. Scaphoid fat stripe obliteration may indicate scaphoid fracture.
Splinting Techniques by Location
| Injury | Splint Type | Position | Key Points |
|---|---|---|---|
| Distal radius (Colles/Smith) | Volar or sugar-tong forearm | Wrist neutral to slight extension | Include elbow in sugar-tong for forearm rotation control |
| Boxer's fracture (5th MC) | Ulnar gutter | Wrist 20° extension, MCP 70° flexion | Acceptable angulation: ≤40° for 5th MC, ≤20° for 2nd/3rd MC |
| Ankle fracture (stable) | Posterior ankle with U-splint (stirrup) | Ankle at 90° (neutral) | Non-weight-bearing; crutches provided |
| Finger fracture (phalanx) | Buddy tape or aluminum splint | Slight flexion at DIP/PIP | Ensure no rotational deformity (cascade sign) |
| Knee immobilization | Knee immobilizer (commercial) | Full extension | Used for patellar fractures, suspected ligament injuries |
| Thumb (gamekeeper/UCL) | Thumb spica | Thumb abducted, IP free | Include wrist; refer orthopedics for Stener lesion |
Fractures Requiring ED or Urgent Orthopedic Referral
Transfer to ED or arrange urgent orthopedic consultation for: open fractures (bone exposed, wound communicating with fracture), neurovascular compromise (absent pulses, diminished sensation, compartment syndrome signs), hip fractures, femur fractures, displaced intra-articular fractures, dislocations that cannot be reduced, supracondylar fractures in children (risk of Volkmann contracture), and fracture-dislocations (ankle bimalleolar/trimalleolar with dislocation, Lisfranc injury).
09 Sprains & Strains
Ankle Sprain Classification
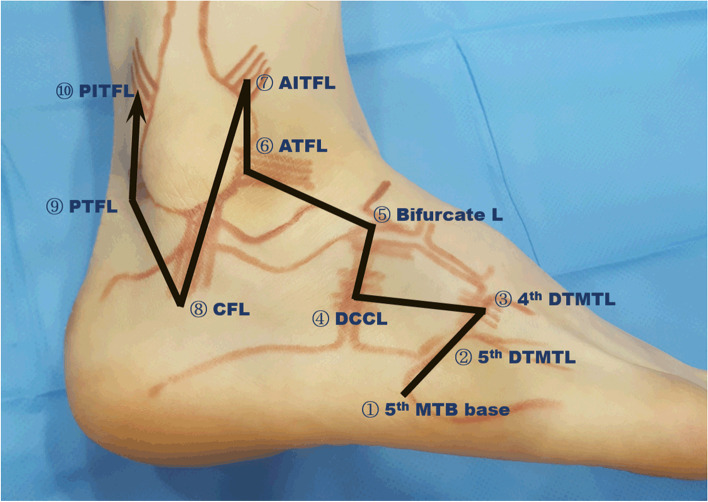
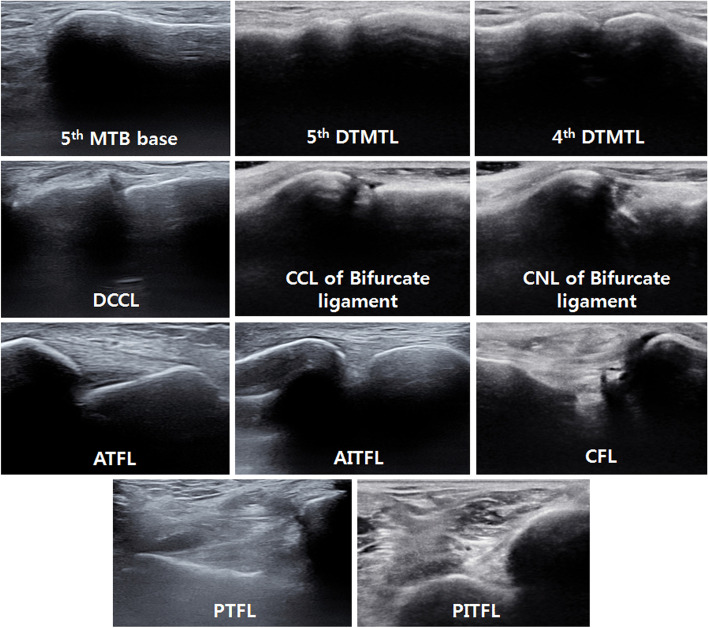
The lateral ankle ligament complex (anterior talofibular [ATFL], calcaneofibular [CFL], posterior talofibular [PTFL]) is involved in ~85% of ankle sprains, with ATFL most commonly injured (inversion mechanism).
| Grade | Pathology | Exam Findings | Weight-Bearing | Recovery |
|---|---|---|---|---|
| I — Mild | Ligament stretch, microscopic tears | Mild tenderness, minimal swelling, no instability, negative anterior drawer | Able to bear weight | 1–3 weeks |
| II — Moderate | Partial ligament tear | Moderate tenderness and swelling, ecchymosis, mild instability, positive anterior drawer with endpoint | Difficulty bearing weight | 3–6 weeks |
| III — Severe | Complete ligament rupture | Severe swelling and ecchymosis, significant instability, positive anterior drawer without endpoint, positive talar tilt | Unable to bear weight | 6–12 weeks |
Management — RICE/PRICE Protocol
Protection (brace, splint, or walking boot), Rest (relative — avoid aggravating activities), Ice (20 minutes on/off, first 48–72 hours), Compression (ACE wrap), Elevation (above heart level). NSAIDs (ibuprofen 400–600 mg TID or naproxen 500 mg BID) for pain and inflammation. Grade I: weight-bearing as tolerated, ankle brace, early mobilization. Grade II: air stirrup brace or walking boot, may need crutches initially, physical therapy referral. Grade III: walking boot or short-leg posterior splint, non-weight-bearing initially, orthopedic referral for possible surgical evaluation.
Weight-Bearing Progression
Progress through: (1) non-weight-bearing with crutches, (2) partial weight-bearing (toe-touch), (3) weight-bearing as tolerated with brace, (4) full weight-bearing with brace, (5) full weight-bearing without brace. Advance based on pain tolerance. Begin range-of-motion exercises (alphabet drawing with foot) as soon as tolerated to prevent stiffness.
Knee Injuries — When to Order MRI
MRI is not performed in urgent care but should be arranged outpatient for: suspected ACL tear (positive Lachman test, anterior drawer, pivot shift — mechanism of pivoting/deceleration with pop and rapid effusion), suspected meniscal tear (joint line tenderness, McMurray test, locking/catching), suspected PCL injury (posterior drawer test positive), and suspected patellar dislocation with recurrent instability. Acute large effusion (<2 hours post-injury) is highly suggestive of ACL tear or intra-articular fracture. Provide knee immobilizer, crutches, ice, and orthopedic referral.
10 Back Pain
Acute low back pain is an exceedingly common urgent care presentation. The vast majority (85–90%) is mechanical/non-specific and self-limited. The primary role of the urgent care clinician is to identify the rare but serious causes ("red flags") and provide appropriate symptomatic management.
Red Flags — TUNA FISH Mnemonic
T — Trauma (significant mechanism, fragility fracture risk)
U — Unexplained weight loss (malignancy)
N — Neurologic deficit (progressive weakness, sensory loss, gait disturbance)
A — Age >50 with new onset back pain (increased cancer/fracture risk)
F — Fever (spinal epidural abscess, diskitis, osteomyelitis)
I — IV drug use (epidural abscess, endocarditis with septic emboli)
S — Steroid use / immunosuppression (fracture risk, infection risk)
H — History of cancer (metastatic disease to spine)
Cauda Equina Syndrome
A surgical emergency requiring immediate ED transfer. Signs: saddle anesthesia (numbness in perineum/inner thighs), urinary retention or incontinence (check post-void residual or bladder scan if available), fecal incontinence, bilateral lower extremity weakness, and decreased rectal tone. Caused by massive disc herniation, tumor, abscess, or hematoma compressing the cauda equina. MRI is diagnostic; decompressive surgery within 24–48 hours is critical to prevent permanent neurologic deficit.
Imaging Indications
Imaging is NOT indicated for acute low back pain without red flags in the first 4–6 weeks. Obtain lumbar X-rays for: trauma, osteoporosis risk (age >70, steroid use), suspected compression fracture. Obtain MRI (arrange outpatient or ED if acute) for: progressive neurologic deficit, suspected cauda equina syndrome, suspected spinal infection (fever + back pain + IVDU/immunosuppression), suspected malignancy (history of cancer + new back pain). CT myelography is an alternative if MRI is contraindicated.
Treatment of Non-Specific Low Back Pain
First-line: NSAIDs (ibuprofen 600 mg TID or naproxen 500 mg BID, with food, for 7–10 days). Second-line: Muscle relaxants as adjunct (cyclobenzaprine 5–10 mg TID PRN, or methocarbamol 750–1500 mg QID; caution: sedation). Activity modification: Avoid bed rest — encourage continued activity within pain tolerance. Bed rest beyond 1–2 days worsens outcomes. Heat therapy: Superficial heat (heating pad, warm packs) for muscle spasm. Opioids are generally NOT recommended for acute back pain and, if used at all, should be limited to ≤3 days for severe pain unresponsive to other measures.
Return Precautions
Instruct patients to return or go to the ED for: new or worsening weakness in legs, loss of bladder or bowel control, saddle numbness, fever developing with back pain, or pain not improving after 2 weeks of conservative management. Document these return precautions in the chart.
11 Joint Complaints
Acute Monoarticular Arthritis
The critical rule-out in any acute monoarticular joint presentation is septic arthritis, which is a medical emergency. Until proven otherwise, an acutely swollen, hot, painful joint with limited ROM should be considered septic. Risk factors: prosthetic joint, diabetes, immunosuppression, IVDU, recent joint procedure, overlying skin infection.
Gout
Acute gouty arthritis presents with rapid onset of severe pain, swelling, warmth, and erythema of a joint (most commonly the 1st MTP — podagra — but also midfoot, ankle, knee, wrist). The overlying skin may be tense and shiny. Differentiation from septic arthritis can be challenging clinically; definitive diagnosis requires joint aspiration showing negatively birefringent monosodium urate crystals under polarized microscopy.

Treatment of acute gout:
• NSAIDs (first-line if no contraindications): indomethacin 50 mg TID × 5–7 days, or naproxen 500 mg BID, or ibuprofen 800 mg TID. Start at full dose and taper as symptoms improve.
• Colchicine: 1.2 mg at onset, then 0.6 mg one hour later (total 1.8 mg on day 1); then 0.6 mg BID until flare resolves. Most effective if started within 24 hours of symptom onset. Avoid in CKD (GFR <30) and hepatic impairment.
• Corticosteroids (for patients who cannot take NSAIDs or colchicine): prednisone 0.5 mg/kg/day × 5–7 days, or intra-articular triamcinolone injection (40 mg for large joints, 10–20 mg for small joints) if septic arthritis has been excluded.
Knee Effusion
Distinguish traumatic (hemarthrosis if rapid onset <2 hours — likely ACL tear or fracture) from non-traumatic (inflammatory vs. mechanical). Physical exam: ballottement test (patella tap) for moderate-to-large effusions, fluid wave test, and bulge sign for small effusions. If aspiration is performed in urgent care: send for cell count, crystal analysis, Gram stain, and culture. Grossly bloody = hemarthrosis; turbid/purulent = infection vs. severe crystal arthropathy; clear yellow = osteoarthritis or meniscal tear.
Shoulder Assessment — Rotator Cuff
The rotator cuff comprises the supraspinatus (abduction, most commonly injured), infraspinatus (external rotation), teres minor (external rotation), and subscapularis (internal rotation). Tests: Empty can test (supraspinatus) — arms at 90° abduction, 30° forward flexion, thumbs down; weakness or pain = positive. External rotation resistance (infraspinatus) — elbows at sides, 90° flexion; resist external rotation. Lift-off test (subscapularis) — hand behind back, lift off. Drop arm test — inability to slowly lower arm from full abduction = complete tear. X-ray to rule out fracture; MRI outpatient for suspected tear.
Wrist — Scaphoid Fracture
Suspect scaphoid fracture with: fall on outstretched hand (FOOSH), anatomic snuffbox tenderness, scaphoid tubercle tenderness (volar), or pain with longitudinal compression of the thumb. Initial X-rays may be normal in up to 15–20% of scaphoid fractures. If clinical suspicion is high but X-ray is negative: apply thumb spica splint, presume fracture, and arrange repeat X-ray or MRI in 10–14 days. The scaphoid has a tenuous blood supply (retrograde via the distal pole); missed fractures risk avascular necrosis and nonunion.
Common Urgent Care Eye Complaints
Eye complaints account for 3–5% of urgent care visits. Key assessment: always check and document visual acuity (Snellen chart) before any examination or treatment — this is the "vital sign" of ophthalmology.
Conjunctivitis: Bacterial (purulent discharge, crusting, unilateral then bilateral) — treat with erythromycin 0.5% ophthalmic ointment or polymyxin-trimethoprim drops QID × 5–7 days. Viral (watery discharge, preauricular lymphadenopathy, bilateral, often follows URI) — supportive care, artificial tears, cold compresses; highly contagious for 10–14 days. Allergic (bilateral, itching prominent, chemosis) — antihistamine drops (olopatadine BID), cool compresses, oral antihistamines.
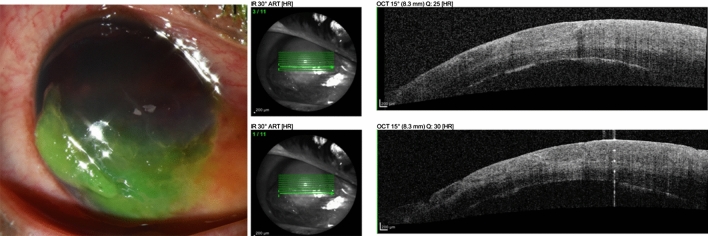
Corneal abrasion: Fluorescein staining under cobalt blue light reveals epithelial defect. Treatment: topical antibiotic (erythromycin ointment or ciprofloxacin drops QID), cycloplegic for pain (cyclopentolate 1%), oral analgesics. Do NOT patch (does not improve healing and impairs vision). Contact lens wearers require anti-pseudomonal coverage (fluoroquinolone drops) and lens discontinuation until healed. Refer to ophthalmology for: large abrasions, penetrating injury, rust ring from metallic foreign body, or failure to heal in 48–72 hours.
Subconjunctival hemorrhage: Benign, painless, bright-red blood under the conjunctiva. No treatment needed; resolves in 1–3 weeks. Check blood pressure (may be associated with hypertension). If recurrent, consider coagulopathy evaluation.
12 Laceration Repair
Laceration repair is one of the most common and satisfying procedures in urgent care. A systematic approach to wound assessment, anesthesia, irrigation, closure technique, and follow-up ensures optimal outcomes and minimizes infection and scarring.
Wound Assessment
Before closure, evaluate: (1) Mechanism (clean vs. contaminated, crush vs. sharp), (2) Depth (superficial/dermal vs. through subcutaneous tissue, fascia, or muscle), (3) Tendon integrity (test active ROM against resistance through full ROM for all tendons in the zone of injury), (4) Nerve function (two-point discrimination, light touch, sharp/dull in nerve distributions distal to wound), (5) Vascular status (capillary refill, pulses distal to wound), (6) Foreign body (explore wound, consider X-ray for glass/metal), (7) Contamination (dirt, debris, bite vs. clean cut). Wounds involving tendons, nerves, major vessels, or joint capsules require surgical consultation.
Local Anesthesia
Lidocaine 1% (10 mg/mL): maximum dose 4.5 mg/kg without epinephrine, 7 mg/kg with epinephrine. For a 70 kg adult: max 31.5 mL of 1% lidocaine without epi, or 49 mL with epi. Onset 2–5 minutes, duration 30–60 min (without epi) or 60–120 min (with epi). Lidocaine with epinephrine provides vasoconstriction (hemostasis) and prolongs duration. Traditional teaching was to avoid epinephrine in fingers, toes, nose, ears, and penis ("end-arteriole" areas), but current evidence supports safe use of lidocaine with epinephrine in digits. Buffering with sodium bicarbonate (1 mL NaHCO₃ per 9 mL lidocaine) reduces injection pain significantly.
Wound Irrigation
High-pressure irrigation with normal saline (or potable tap water — equivalent in evidence) using a 20–60 mL syringe with an 18-gauge angiocatheter or splash guard. Target pressure: 5–8 psi. Minimum volume: 50–100 mL per cm of laceration length, or at least 250 mL for most wounds. Irrigation is the single most important step in preventing wound infection — it is more important than antibiotic prophylaxis.
Wound Closure Timing
The "golden period" for primary wound closure depends on location and contamination level. Face and scalp: may be closed up to 24 hours after injury (excellent blood supply, low infection rate). Trunk and proximal extremities: within 12–18 hours. Distal extremities (hands, feet): within 6–12 hours. Contaminated wounds: shorten all time windows. Wounds beyond these windows or with high contamination burden should be managed with delayed primary closure (clean, pack open, reassess in 3–5 days for closure) or secondary intention healing. Exceptions: bite wounds to hands (generally leave open regardless of timing), and highly contaminated wounds (leave open).
Antibiotic Prophylaxis for Wounds
Routine prophylactic antibiotics are NOT indicated for most clean, sutured lacerations — proper irrigation is far more effective at preventing infection. Prophylaxis IS indicated for: animal/human bites, heavily contaminated wounds, crush injuries, wounds with devitalized tissue, intra-oral lacerations, open fractures, wounds in immunocompromised patients, and through-and-through lip lacerations. Agent of choice for most prophylaxis: amoxicillin-clavulanate 875/125 mg BID × 5 days.
Suture Selection by Location
| Location | Suture Type | Size | Removal (days) | Notes |
|---|---|---|---|---|
| Scalp | Staples or nylon | 3-0 to 4-0 | 7–10 | Staples are faster; inspect for skull fracture |
| Face / lip | Nylon or fast-absorbing gut | 5-0 to 6-0 | 3–5 | Meticulous closure; align vermilion border precisely |
| Eyelid | Nylon or silk | 6-0 | 3–5 | Refer if through lid margin or involving canaliculus |
| Trunk / abdomen | Nylon or polypropylene | 3-0 to 4-0 | 7–10 | Deep dermal sutures (Vicryl/Monocryl) may be needed |
| Extremities | Nylon | 4-0 | 10–14 | Joint surfaces: 14 days due to tension |
| Hand / fingers | Nylon | 4-0 to 5-0 | 10–14 | Assess tendons carefully before closure |
| Foot / sole | Nylon | 3-0 to 4-0 | 10–14 | Horizontal mattress for thick plantar skin |
Tissue Adhesive (Dermabond/2-Octylcyanoacrylate)
Appropriate for: superficial, linear, low-tension lacerations with well-approximated edges. Best locations: face, scalp, trunk. NOT appropriate for: wounds over joints (high tension), hands/feet (high moisture), puncture wounds, bites, infected wounds, mucous membranes, or wounds requiring deep-layer closure. Application: hold wound edges together, apply adhesive in 3–4 thin layers, each layer drying for 30 seconds. No suture removal needed (sloughs off in 5–10 days).
Tetanus Prophylaxis
| Vaccination History | Clean Minor Wound | Contaminated / Tetanus-Prone Wound |
|---|---|---|
| ≥3 doses, last dose <5 years | No Td/Tdap; no TIG | No Td/Tdap; no TIG |
| ≥3 doses, last dose 5–10 years | No Td/Tdap; no TIG | Td/Tdap; no TIG |
| ≥3 doses, last dose >10 years | Td/Tdap; no TIG | Td/Tdap; no TIG |
| <3 doses or unknown | Td/Tdap; no TIG | Td/Tdap; AND TIG 250 units IM |
Tetanus-prone wounds: contaminated with dirt/feces/saliva, puncture wounds, avulsion injuries, crush injuries, burns, frostbite, wounds >6 hours old.
13 Wound Infections & Abscesses
Cutaneous Abscess — Incision & Drainage (I&D)
A fluctuant, tender, erythematous, often warm collection of pus within the skin/subcutaneous tissue. I&D is the definitive treatment and is the single most important intervention — antibiotics alone without drainage are inadequate. Technique: (1) prep skin with chlorhexidine or betadine, (2) local anesthesia — field block around the abscess (injection into the abscess cavity is painful and ineffective), (3) incision with #11 blade along the length of the abscess, (4) express purulent material, (5) break up loculations with hemostat or finger, (6) irrigate cavity, (7) pack loosely with iodoform gauze (or loop drain), (8) cover with gauze dressing. Send wound culture for MRSA surveillance. Follow up in 48–72 hours for wound check and packing removal/replacement.

Antibiotic Indications for Abscess
Antibiotics post-I&D are recommended for: abscess >2 cm, multiple abscesses, extensive surrounding cellulitis, immunocompromised patient, systemic signs (fever, tachycardia), prosthetic device, or high-risk location (face, hand, genitalia). MRSA coverage: TMP-SMX DS 1–2 tabs PO BID × 7–10 days, or doxycycline 100 mg PO BID × 7–10 days. For MSSA coverage: cephalexin 500 mg PO QID or dicloxacillin 500 mg PO QID. If both MRSA coverage AND streptococcal coverage needed (cellulitis + abscess): TMP-SMX plus cephalexin, or clindamycin 300–450 mg PO TID (covers both).
Animal & Human Bites
Dog bites: most common bite pathogen is Pasteurella spp. Irrigate copiously, assess tendon/nerve/vessel integrity. Primary closure may be performed for face/scalp bites (cosmesis, good blood supply); hand bites should generally be left open. Prophylactic antibiotics: amoxicillin-clavulanate 875/125 mg BID × 5–7 days. Penicillin allergy: doxycycline + metronidazole, or moxifloxacin.
Cat bites: higher infection rate than dog bites (30–50% vs. 5–10%) due to deep puncture inoculation. Pasteurella multocida is the primary concern. ALL cat bites require prophylactic antibiotics: amoxicillin-clavulanate. Cat bite to the hand = high risk for septic arthritis and tenosynovitis — close follow-up essential.
Human bites: "fight bites" (closed-fist injury over MCP joint) are high risk for joint space infection with Eikenella corrodens and oral flora. Require X-ray (fracture, tooth fragment), prophylactic antibiotics (amoxicillin-clavulanate), and hand surgery referral if joint space violation suspected. Do NOT close human bite wounds primarily.
Rabies Post-Exposure Prophylaxis (PEP)
High-risk animals (PEP indicated): bats (any contact, even in room with sleeping person), raccoons, skunks, foxes, coyotes, groundhogs. Also any domestic animal behaving erratically or confirmed rabid.
Low-risk animals (PEP generally NOT indicated): squirrels, hamsters, guinea pigs, gerbils, chipmunks, rats, mice, rabbits. These rodents/lagomorphs are almost never rabid.
Dog/cat bites: If animal is available for 10-day observation and remains healthy, PEP is not needed. If animal unavailable, consult local health department for rabies prevalence data. Stray or feral animals in endemic areas warrant PEP.
PEP regimen (previously unvaccinated): Human rabies immune globulin (HRIG) 20 IU/kg infiltrated around wound (remainder IM at distant site) on day 0, PLUS rabies vaccine IM (deltoid) on days 0, 3, 7, and 14.
14 Burns
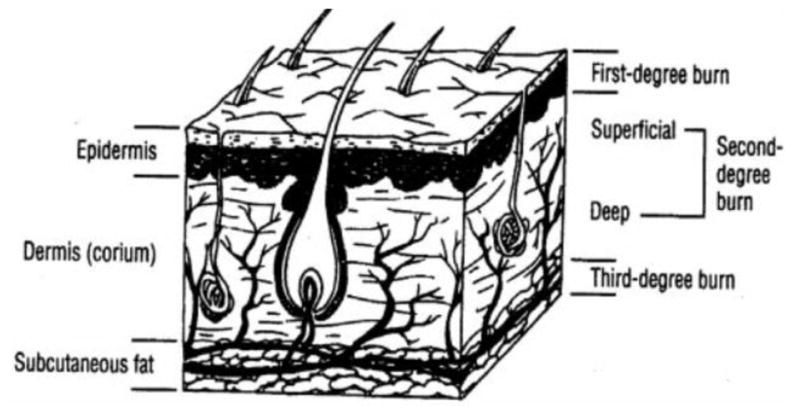
Burn Degree Classification
| Degree | Depth | Appearance | Sensation | Healing |
|---|---|---|---|---|
| Superficial (1st) | Epidermis only | Red, dry, no blisters (sunburn-like) | Painful | 3–5 days, no scarring |
| Superficial partial (2nd) | Epidermis + superficial dermis | Red, moist, blisters, blanches with pressure | Very painful (intact nerve endings) | 7–21 days, minimal scarring |
| Deep partial (2nd) | Epidermis + deep dermis | White or mottled, may blister, does not blanch | Pressure only (damaged nerve endings) | >21 days, significant scarring, may need grafting |
| Full thickness (3rd) | Through entire dermis | White, waxy, leathery, or charred; dry | Painless (destroyed nerves) | Does not heal spontaneously; requires grafting |
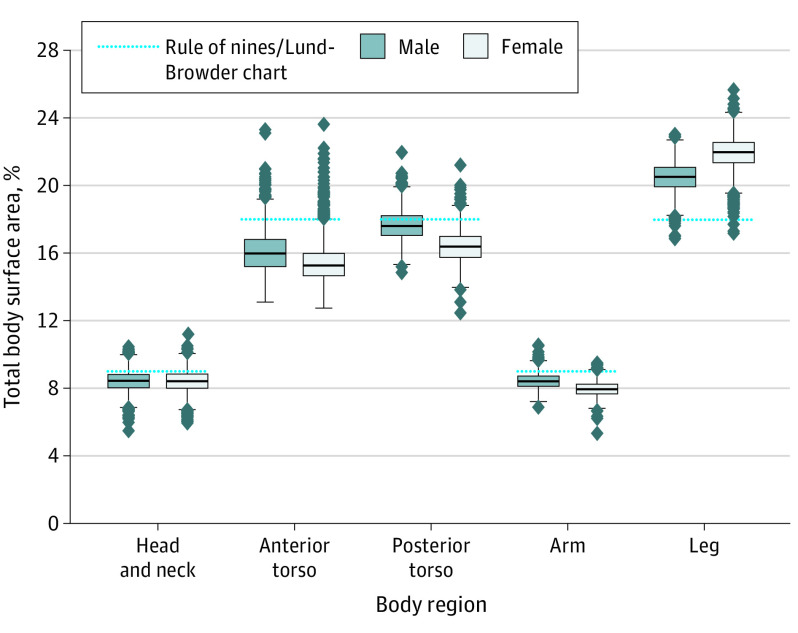
BSA Estimation
Rule of 9s (adults): head 9%, each upper extremity 9%, anterior trunk 18%, posterior trunk 18%, each lower extremity 18%, perineum 1%. Lund-Browder chart is more accurate, especially in children where head is proportionally larger (head 18% at age 1, decreasing with age) and legs proportionally smaller. Patient's palm (including fingers) ≈ 1% BSA — useful for estimating scattered burn areas.
ED Transfer Criteria for Burns
• Partial-thickness burns >10% BSA
• Burns involving the face, hands, feet, genitalia, perineum, or major joints
• Full-thickness (3rd degree) burns of any size
• Circumferential burns (risk of compartment syndrome / eschar constriction)
• Electrical or chemical burns
• Inhalation injury (singed nasal hairs, soot in oropharynx, hoarseness, stridor)
• Burns in patients with significant comorbidities (diabetes, immunosuppression)
• Burns with associated trauma (fractures, blast injuries)
• Suspected non-accidental trauma (child abuse — stocking/glove distribution, cigarette burns, pattern burns)
Burn Wound Care in Urgent Care
For minor burns manageable in urgent care (superficial and small partial-thickness <10% BSA, not involving critical areas): (1) Cool with running cool water × 20 minutes (NOT ice). (2) Gently debride loose/broken blisters; intact blisters <2 cm may be left intact (controversial — some providers drain large blisters). (3) Topical wound care: silver sulfadiazine 1% cream (Silvadene) applied BID with non-adherent dressing (avoid on face — can cause argyria; avoid in sulfa allergy). Alternatives: bacitracin (face burns), honey-based dressings, or petrolatum-impregnated gauze (Adaptic/Xeroform). (4) Non-adherent inner layer + gauze wrap + elastic bandage. (5) Follow-up wound check in 24–48 hours.
Pain Management for Burns
Burns are extremely painful. Mild burns: ibuprofen 600–800 mg TID + acetaminophen 1000 mg Q6H (multimodal). Moderate burns: add short course of opioid (hydrocodone 5–10 mg or oxycodone 5 mg Q4–6H PRN, 3–5 day supply). Adequate pain control prior to wound care/dressing changes is essential. Topical lidocaine gel may provide adjunctive relief for superficial burns.
15 Common Dermatologic Conditions
Cellulitis vs. Abscess
Cellulitis is a non-purulent, spreading skin infection (erythema, warmth, tenderness, edema without a drainable collection) most commonly caused by beta-hemolytic streptococci (GAS) and Staphylococcus aureus. Treatment: cephalexin 500 mg QID or dicloxacillin 500 mg QID × 5–7 days. Mark the border with a skin marker to monitor progression. If MRSA cellulitis suspected (purulent drainage, known MRSA colonization, community with high MRSA prevalence): add TMP-SMX DS BID or doxycycline 100 mg BID. ED referral for: rapidly spreading cellulitis, facial cellulitis (risk of cavernous sinus thrombosis), orbital cellulitis, cellulitis with systemic signs (fever, tachycardia), or failed outpatient therapy.
Herpes Zoster (Shingles)
Reactivation of varicella-zoster virus (VZV) in a dermatomal distribution. Presents with unilateral, vesicular rash on an erythematous base, often preceded by 2–3 days of prodromal pain/burning. Thoracic dermatomes most common. Treatment: antiviral therapy is most effective when started within 72 hours of rash onset: valacyclovir 1000 mg PO TID × 7 days (preferred for bioavailability), or acyclovir 800 mg PO 5×/day × 7 days, or famciclovir 500 mg PO TID × 7 days. Even beyond 72 hours, treat if new vesicles are still appearing. Pain management: gabapentin, TCAs, NSAIDs, or short opioid course. Refer ophthalmology urgently if herpes zoster ophthalmicus (V1 distribution — especially if Hutchinson sign [vesicles on nose tip] is present, indicating nasociliary nerve involvement with high risk of corneal involvement).

Contact Dermatitis
Allergic contact dermatitis (poison ivy/oak/sumac, nickel, latex) presents with intensely pruritic, well-demarcated, vesicular or papular rash at the site of exposure, often with linear streaks. Treatment: Mild/localized: high-potency topical steroid (triamcinolone 0.1% cream BID or clobetasol 0.05% for severe areas × 2 weeks). Moderate/widespread: oral prednisone taper — 60 mg × 4 days, 40 mg × 4 days, 20 mg × 4 days (total 12 days minimum for poison ivy; shorter courses result in rebound). Antihistamines (hydroxyzine 25 mg TID or cetirizine 10 mg daily) for pruritus. Calamine lotion and cool compresses for comfort.
Urticaria & Angioedema
Urticaria (hives): raised, pruritic, erythematous wheals that blanch with pressure and are typically transient (individual lesions last <24 hours). Most cases are idiopathic or related to viral illness. Treatment: non-sedating antihistamine (cetirizine 10 mg, loratadine 10 mg, or fexofenadine 180 mg daily). If refractory, double the dose or add a sedating antihistamine (diphenhydramine 25–50 mg Q6H, or hydroxyzine 25 mg TID). Angioedema: deeper swelling involving dermis/subcutaneous tissue, often affecting lips, tongue, periorbital area, and extremities. If involving airway (tongue swelling, voice change, stridor, dyspnea) — administer epinephrine 0.3–0.5 mg IM (1:1,000) immediately and transfer to ED. ACE-inhibitor-induced angioedema is bradykinin-mediated and does NOT respond to antihistamines or epinephrine — manage airway, discontinue ACE-I permanently, and transfer to ED.
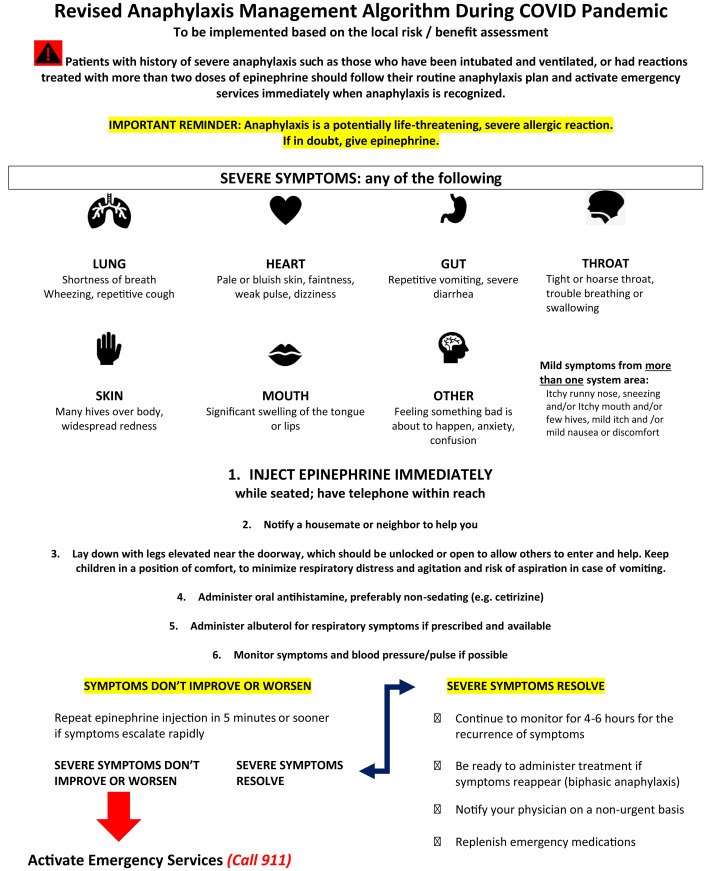
Allergic Reactions & Anaphylaxis
Allergic reactions range from mild (localized urticaria, pruritus) to life-threatening anaphylaxis. Anaphylaxis criteria (any ONE of): (1) acute onset of skin/mucosal involvement (hives, flushing, lip/tongue swelling) PLUS respiratory compromise OR hypotension; (2) two or more of the following after exposure to a likely allergen: skin/mucosal involvement, respiratory compromise, hypotension, persistent GI symptoms; (3) hypotension after exposure to a known allergen for that patient.
Step 1: Epinephrine 0.3–0.5 mg IM (1:1,000 / 1 mg/mL) in the anterolateral thigh. Pediatric: 0.01 mg/kg (max 0.3 mg). May repeat every 5–15 minutes if needed.
Step 2: Position supine with legs elevated (if hypotensive) or upright (if dyspneic). Do NOT stand the patient up (risk of cardiovascular collapse).
Step 3: Call EMS for transfer. Establish IV access if available. Normal saline bolus 1–2 L for hypotension.
Step 4: Adjunctive medications: diphenhydramine 50 mg IV/IM, famotidine 20 mg IV, albuterol nebulizer for bronchospasm, methylprednisolone 125 mg IV (prevents biphasic reaction but does NOT treat acute anaphylaxis).
Step 5: Observe or transfer for observation (biphasic reactions occur in 5–20% of cases, typically within 4–12 hours).
At discharge (mild allergic reactions): Prescribe epinephrine auto-injector (EpiPen), allergy referral, anaphylaxis action plan education.
Scabies & Lice
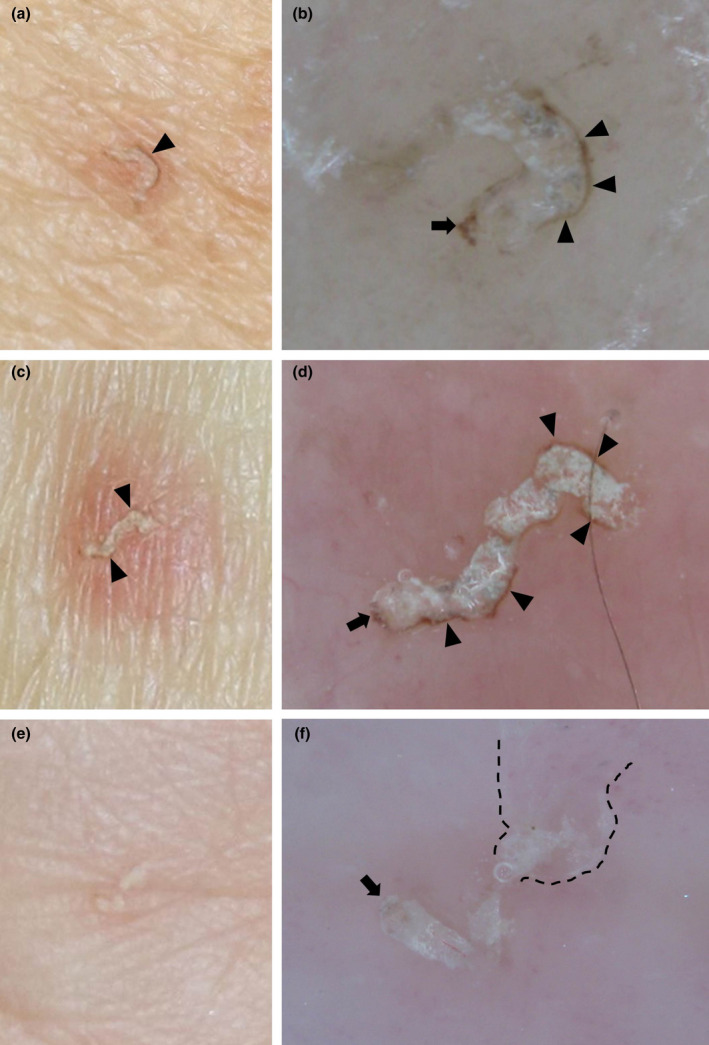
Scabies (Sarcoptes scabiei): intensely pruritic, worse at night. Look for burrows (linear, serpiginous) in web spaces, wrists, axillae, waistline, genitalia. Treatment: permethrin 5% cream applied from neck down, left on 8–14 hours, then washed off; repeat in 7–14 days. Alternative: ivermectin 200 mcg/kg PO, repeat in 7–14 days. Treat all household contacts simultaneously. Wash bedding/clothing in hot water.
Head lice (Pediculus humanus capitis): pruritic scalp, visible nits (eggs) attached to hair shafts near scalp, live lice on exam. Treatment: permethrin 1% lotion (OTC), apply to damp hair after shampooing, leave on 10 minutes, rinse; repeat in 7–10 days. If resistant: ivermectin 0.5% lotion (Sklice) or malathion 0.5% lotion. Nit combing with a fine-tooth comb daily. No-nit policies at schools are outdated and unnecessary.
16 Urinary Tract Infections
Uncomplicated Cystitis
Defined as UTI in a non-pregnant, premenopausal woman with no urologic abnormalities. Symptoms: dysuria, frequency, urgency, suprapubic pain. UA findings: positive leukocyte esterase, nitrites, pyuria (≥10 WBC/hpf). Urine culture is NOT required for uncomplicated cystitis but should be sent if diagnosis is uncertain or treatment failure expected.
First-line antibiotics:
| Agent | Dose | Duration | Notes |
|---|---|---|---|
| Nitrofurantoin (Macrobid) | 100 mg PO BID | 5 days | First-line; avoid if GFR <30; covers E. coli well; poor tissue penetration (not for pyelo) |
| TMP-SMX DS | 160/800 mg PO BID | 3 days | First-line if local resistance <20%; avoid in 1st trimester and near term |
| Fosfomycin (Monurol) | 3 g PO × 1 dose | Single dose | Convenient; slightly lower efficacy than nitrofurantoin or TMP-SMX |
Fluoroquinolones (ciprofloxacin, levofloxacin) should be reserved for complicated UTI or pyelonephritis due to resistance concerns, tendon injury risk, and FDA black box warning. Avoid as first-line for uncomplicated cystitis.
Complicated UTI Criteria
A UTI is considered complicated if any of the following are present: male sex, pregnancy, urologic abnormality (obstruction, stent, catheter, neurogenic bladder), renal transplant, immunosuppression, diabetes with poor control, recent urologic procedure, or failure of initial antibiotic therapy. Complicated UTIs require culture-guided therapy and often broader-spectrum antibiotics.
Pyelonephritis
Upper tract UTI presenting with fever, flank pain, costovertebral angle (CVA) tenderness, and often with lower tract symptoms (dysuria, frequency). UA with pyuria and bacteriuria; send urine culture. Outpatient treatment (if tolerating PO, non-toxic, reliable follow-up): ciprofloxacin 500 mg PO BID × 7 days, or levofloxacin 750 mg daily × 5 days. If fluoroquinolone resistance is a concern: ceftriaxone 1 g IM/IV × 1 dose in office, then switch to oral cephalosporin (cefpodoxime 200 mg BID) or TMP-SMX based on culture. ED transfer for: unable to tolerate PO, toxic appearance, hemodynamic instability, suspected obstruction, pregnancy (all pregnant pyelonephritis should be admitted for IV antibiotics).
UTI in Pregnancy
Screen for asymptomatic bacteriuria in pregnancy (urine culture at first prenatal visit). Treat asymptomatic bacteriuria AND symptomatic UTI in pregnancy to prevent pyelonephritis (risk increases from 1–2% to 20–40% if untreated). Safe antibiotics: nitrofurantoin (avoid in 1st trimester and at term — risk of hemolytic anemia in G6PD-deficient neonates), cephalexin 500 mg QID × 7 days, amoxicillin-clavulanate. Avoid TMP-SMX in 1st trimester (folate antagonist) and at term (kernicterus risk). Avoid fluoroquinolones (cartilage toxicity).
Recurrent UTI
Defined as ≥2 UTIs in 6 months or ≥3 in 12 months. Non-antibiotic prevention: adequate hydration, post-coital voiding, cranberry products (modest evidence), vaginal estrogen in postmenopausal women. Antibiotic prophylaxis options (arrange through PCP): continuous low-dose (nitrofurantoin 50 mg nightly), post-coital (TMP-SMX single dose), or patient-initiated self-treatment.
Male UTI
All UTIs in males are considered complicated. Always send urine culture. Duration of treatment: 7–14 days (some guidelines recommend 7 days for uncomplicated cystitis in young men with ciprofloxacin or TMP-SMX). Consider prostatitis in men with UTI + perineal/suprapubic pain + voiding difficulty. Urologic referral for: recurrent male UTI, hematuria, structural abnormality, or poor response to therapy.
17 STI Screening & Treatment
Gonorrhea & Chlamydia
Often co-transmitted; test for both simultaneously. NAAT (urine or swab) is the diagnostic test of choice. Typical presentation: dysuria, urethral/vaginal discharge, cervicitis. May be asymptomatic (especially chlamydia in women). Treatment (CDC 2021 guidelines):
Gonorrhea: Ceftriaxone 500 mg IM × 1 dose (for patients <150 kg; 1 g IM for ≥150 kg). If ceftriaxone unavailable: gentamicin 240 mg IM + azithromycin 2 g PO. Always co-treat for chlamydia if not ruled out.
Chlamydia: Doxycycline 100 mg PO BID × 7 days (preferred). Alternatives: azithromycin 1 g PO × 1 dose (now second-line due to resistance concerns and lower efficacy for rectal chlamydia).
Trichomoniasis
Caused by Trichomonas vaginalis. Women: frothy, yellow-green, malodorous vaginal discharge, strawberry cervix. Men: often asymptomatic. Diagnosis: wet mount (motile trichomonads — sensitivity only 50–60%), NAAT (preferred, sensitivity >95%), or rapid antigen. Treatment: metronidazole 500 mg PO BID × 7 days (preferred for women; single 2 g dose is an option for men). Avoid alcohol during treatment and for 72 hours after (disulfiram-like reaction). Treat partners.
Expedited Partner Therapy (EPT)
Prescribing treatment for the patient's sexual partner(s) without examining them. Legal in most US states. Indicated for: chlamydia, gonorrhea, and trichomoniasis. Provide a prescription or medication pack for the partner. NOT appropriate if partner may have severe allergy, is pregnant, or has symptoms suggesting complicated infection.
Reportable STIs
All states require reporting of: gonorrhea, chlamydia, syphilis, HIV/AIDS, and hepatitis A/B/C. Report to your local health department. In urgent care, ensure the reporting workflow is integrated into positive test result follow-up.
Pelvic Inflammatory Disease (PID)
PID should be suspected in any sexually active woman with lower abdominal pain and cervical motion tenderness, uterine tenderness, or adnexal tenderness on bimanual exam. Additional criteria supporting diagnosis: fever >38.3°C, mucopurulent cervical discharge, elevated ESR/CRP, or laboratory-confirmed cervical gonorrhea/chlamydia.
Outpatient PID treatment: Ceftriaxone 500 mg IM × 1 dose PLUS doxycycline 100 mg PO BID × 14 days PLUS metronidazole 500 mg PO BID × 14 days. ED transfer for: surgical emergency not excluded (appendicitis, ectopic), tubo-ovarian abscess suspected, pregnant, unable to tolerate PO, failed outpatient therapy, or toxic/septic appearance. Follow up in 48–72 hours to assess improvement.
18 Acute Abdominal Pain
Abdominal pain is one of the highest-acuity presentations in urgent care, requiring careful assessment to identify surgical emergencies and conditions requiring ED transfer.
Right Lower Quadrant — Appendicitis
Classic presentation: periumbilical pain migrating to RLQ, anorexia, nausea/vomiting, low-grade fever. Exam: McBurney point tenderness, Rovsing sign (RLQ pain with LLQ palpation), psoas sign (pain with hip extension), obturator sign (pain with internal rotation of flexed hip). The Alvarado Score (MANTRELS) helps risk-stratify:
| Criterion | Points |
|---|---|
| Migration of pain to RLQ | 1 |
| Anorexia | 1 |
| Nausea/vomiting | 1 |
| Tenderness in RLQ | 2 |
| Rebound pain | 1 |
| Elevated temperature (≥37.3°C) | 1 |
| Leukocytosis (>10,000) | 2 |
| Shift to left (>75% neutrophils) | 1 |
| Total: 10 points. Score ≤4: low risk. 5–6: equivocal (imaging). 7–8: probable appendicitis. ≥9: very probable. | |
Patients with suspected appendicitis should be transferred to the ED for CT abdomen/pelvis with IV contrast and surgical consultation. Do NOT delay transfer to obtain POC labs.
Right Upper Quadrant — Cholecystitis
Presentation: RUQ pain (often post-prandial, fatty food), nausea, vomiting, fever. Murphy sign: inspiratory arrest during RUQ palpation (sensitivity ~65%, specificity ~87%). Labs: elevated WBC, possibly elevated liver enzymes (AST/ALT), bilirubin. Diagnosis confirmed by RUQ ultrasound (gallstones + gallbladder wall thickening + pericholecystic fluid + sonographic Murphy sign). Transfer to ED for imaging, IV antibiotics, and surgical consultation.
Epigastric Pain — Pancreatitis & PUD
Acute pancreatitis: epigastric pain radiating to the back, worsened by eating, nausea/vomiting. Lipase >3× upper limit of normal is diagnostic. Most common causes: gallstones and alcohol. Transfer to ED for IV fluids, pain management, and monitoring. Peptic ulcer disease: epigastric burning/gnawing pain, may improve (duodenal) or worsen (gastric) with meals. H. pylori testing (stool antigen or urea breath test) in urgent care. Treatment: PPI (omeprazole 20 mg BID) × 4–8 weeks. If H. pylori positive: triple therapy (PPI + amoxicillin 1 g BID + clarithromycin 500 mg BID × 14 days). ED transfer if: signs of perforation (rigid abdomen, free air), GI bleeding (hematemesis, melena), or hemodynamic instability.
Left Lower Quadrant — Diverticulitis
LLQ pain with fever, leukocytosis, and change in bowel habits in patients typically >40 years. Mild, uncomplicated diverticulitis can be managed outpatient with antibiotics (historically, though recent evidence suggests antibiotics may not always be necessary for uncomplicated cases): metronidazole 500 mg TID + ciprofloxacin 500 mg BID, or amoxicillin-clavulanate 875/125 mg BID × 7–10 days. Clear liquid diet advancing as tolerated. ED transfer for: fever >39°C, peritoneal signs, immunosuppression, inability to tolerate PO, or suspected complication (abscess, perforation, obstruction).
Testicular Torsion
Sudden onset of severe unilateral testicular pain, often with nausea/vomiting. Exam: high-riding testis, transverse lie, absent cremasteric reflex, diffuse swelling. Peak incidence: neonatal and adolescent (12–18 years). The 6-hour window is critical: testicular salvage rates are >90% if detorsion within 6 hours, dropping to <10% after 24 hours. Do NOT delay for imaging — immediate ED transfer for surgical exploration. If clinical suspicion is high, ultrasound should NOT delay operative management.
Acute Headache in Urgent Care
Most headaches presenting to urgent care are benign (tension-type, migraine). However, several dangerous headache patterns require ED transfer: "worst headache of life" or thunderclap headache (subarachnoid hemorrhage until proven otherwise), headache with fever and meningismus (meningitis), headache with new focal neurologic deficit (stroke, mass, abscess), headache with papilledema (increased ICP), headache post-trauma with red flags (GCS <15, vomiting, anticoagulation). For migraine management in urgent care: ketorolac 30 mg IM + metoclopramide 10 mg IV/IM (or prochlorperazine 10 mg IV) + IV fluids is an effective "migraine cocktail." Diphenhydramine 25 mg IV may be added for nausea and as adjunctive analgesic. Avoid opioids for primary headache management.
Ectopic Pregnancy
Suspect in any woman of reproductive age with abdominal/pelvic pain, vaginal bleeding, and positive pregnancy test. Risk factors: previous ectopic, PID history, IUD, tubal surgery. Obtain urine beta-HCG; if positive, transfer to ED for quantitative serum beta-HCG and transvaginal ultrasound. Ruptured ectopic can present with hemodynamic instability and requires emergent surgical intervention. Never discharge a patient with a positive pregnancy test and abdominal pain without ED evaluation for ectopic.
19 Pediatric Fever & Common Infections
Fever Definitions by Age
Fever is defined as a rectal temperature ≥38.0°C (100.4°F). In young infants, the management of fever varies dramatically by age group:
≤28 days (0–4 weeks): ALL febrile neonates require immediate ED transfer for full sepsis workup (blood culture, urine culture, LP, CBC, CRP/procalcitonin) and empiric IV antibiotics (ampicillin + gentamicin or cefotaxime). No exceptions — do NOT attempt to manage in urgent care.
29–60 days: High risk for serious bacterial infection (SBI). Several validated criteria help risk-stratify:
• Rochester Criteria (low risk if ALL met): previously healthy term infant, non-toxic appearing, no focal bacterial infection on exam, WBC 5,000–15,000, band count ≤1,500, normal UA (≤10 WBC/hpf), normal stool (≤5 WBC/hpf if diarrhea).
• Step-by-Step approach: Uses procalcitonin (<0.5 ng/mL), CRP (<20 mg/L), ANC (<10,000), and UA to sequentially classify risk. Low-risk infants may be managed with close outpatient follow-up if reliable.
In practice, most 29–60-day febrile infants should be referred to the ED for evaluation unless the urgent care center can perform full workup and arrange close follow-up within 24 hours.
61–90 days: Risk of SBI is lower. If well-appearing with normal UA and inflammatory markers, outpatient management with close follow-up (24 hours) is reasonable. Still send urine culture, and consider ED referral if any concern.
>3 months: Manage based on clinical appearance, source identification, and degree of fever. Well-appearing children with identified viral source can be managed with antipyretics and follow-up.
Febrile Seizures
| Feature | Simple Febrile Seizure | Complex Febrile Seizure |
|---|---|---|
| Duration | <15 minutes | ≥15 minutes |
| Type | Generalized (tonic-clonic) | Focal features |
| Recurrence in 24 hours | No | Yes (recurs within 24 hours) |
| Post-ictal | Brief, returns to baseline quickly | Prolonged or focal deficit |
| Management | Reassurance, identify fever source, no further workup needed | ED referral for evaluation; consider EEG, imaging, LP based on age/presentation |
Simple febrile seizures occur in 2–5% of children aged 6 months to 5 years. Recurrence risk ~30%. They do NOT cause brain damage, epilepsy, or developmental delay. Counsel parents extensively on benign nature and seizure first aid. No prophylactic anti-epileptic therapy is recommended.

Hand-Foot-Mouth Disease (HFMD)
Caused by coxsackievirus A16 or enterovirus 71. Presents with: fever, malaise, painful oral vesicles/ulcers (buccal mucosa, tongue, palate), and vesicular rash on palms, soles, and buttocks. Self-limited (7–10 days). Treatment: supportive — acetaminophen/ibuprofen for pain, encourage oral intake, magic mouthwash (diphenhydramine + Maalox + viscous lidocaine in equal parts) for oral pain. Dehydration is the primary complication — assess for adequate oral intake. Contagious; exclude from daycare until fever-free and lesions are crusting.

Croup (Laryngotracheobronchitis)
Parainfluenza virus is the most common cause. Peak age 6 months to 3 years. Classic presentation: barky "seal-like" cough, inspiratory stridor, hoarseness, low-grade fever, typically worse at night. Westley Croup Score assesses severity (see Section 26 for full scoring).
Treatment by severity: Mild (Westley 0–2): single dose dexamethasone 0.6 mg/kg PO (max 10 mg) and discharge. Moderate (Westley 3–7): dexamethasone 0.6 mg/kg PO/IM + nebulized racemic epinephrine 0.5 mL of 2.25% solution in 3 mL NS; observe for 2–4 hours for rebound stridor. Severe (Westley 8–11) or no improvement: nebulized epinephrine, dexamethasone, and transfer to ED. Stridor at rest is the key indicator of at least moderate severity.
Strep Pharyngitis in Children
GAS pharyngitis is more common in children 5–15 years. Always test before treating (do not treat empirically). If rapid strep is negative, send backup throat culture (sensitivity ~95% vs. ~85% for rapid test). Treatment same as adults with weight-based dosing. Centor/McIsaac scoring applies; age 3–14 gets +1 point. Children <3 years rarely get GAS pharyngitis — testing and treatment are generally not indicated unless specific risk factors (sibling with confirmed GAS).
Pediatric Respiratory Emergencies Requiring Transfer
Epiglottitis: Acute onset of high fever, toxic appearance, drooling, tripod positioning, muffled voice, stridor. Do NOT attempt to visualize the throat (risk of complete airway obstruction). Call EMS immediately. Now rare due to Hib vaccination but still occurs (non-typeable H. influenzae, GAS, S. aureus).
Retropharyngeal abscess: Fever, neck stiffness, drooling, dysphagia, muffled voice, neck swelling, refusal to extend neck. Peak age 2–4 years. Requires CT neck with contrast and IV antibiotics — ED transfer.
Bacterial tracheitis: Croup-like illness that does not respond to standard treatment, with high fever, toxic appearance, and copious purulent secretions. Usually S. aureus. Requires ED transfer for airway management and IV antibiotics.
Bronchiolitis (severe): RSV is the most common cause (infants <2 years). ED transfer for: SpO₂ <92%, apnea, respiratory distress with retractions, dehydration, age <3 months, or history of prematurity/CLD/CHD.
Pediatric Dosing Reminders
| Medication | Pediatric Dose | Max Dose | Notes |
|---|---|---|---|
| Acetaminophen | 15 mg/kg Q4–6H | 75 mg/kg/day or 4 g/day | Available as 160 mg/5 mL suspension |
| Ibuprofen | 10 mg/kg Q6–8H | 40 mg/kg/day or 2.4 g/day | Age ≥6 months; 100 mg/5 mL suspension |
| Amoxicillin (strep) | 50 mg/kg/day divided BID | 1000 mg/day | 10-day course for GAS pharyngitis |
| Amoxicillin (AOM) | 80–90 mg/kg/day divided BID | 3000 mg/day | High dose for resistant pneumococcus |
| Prednisolone | 1–2 mg/kg/day | 60 mg/day | 3–5 days for asthma; 15 mg/5 mL liquid |
| Dexamethasone (croup) | 0.6 mg/kg PO/IM | 10 mg | Single dose; long half-life (~36 hrs) |
| Ondansetron (ODT) | 0.15 mg/kg | 4 mg | Orally disintegrating tab for vomiting |
20 Pediatric Injuries & Foreign Bodies
Nursemaid's Elbow (Radial Head Subluxation)
Common in children 1–4 years. Mechanism: longitudinal traction on an extended, pronated forearm (lifting/swinging child by the hand). The annular ligament slips over the radial head and becomes interposed. The child holds the arm slightly flexed and pronated, refuses to use it ("pseudoparalysis"), and there is no swelling or deformity. X-rays are typically normal and should be obtained only if the mechanism is atypical, there is swelling, or reduction fails.
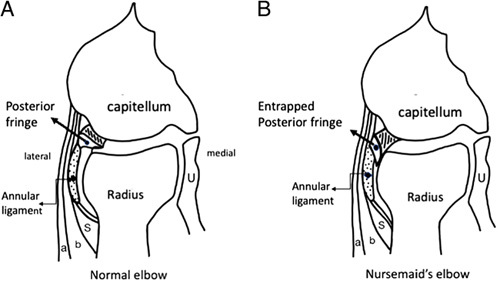
Reduction technique (supination-flexion method): Hold the elbow with one hand, thumb over the radial head. With the other hand, fully supinate the forearm, then flex the elbow fully. A palpable "click" over the radial head indicates successful reduction. The child should begin using the arm within 5–15 minutes. If unsuccessful, attempt the hyperpronation method (hyperpronation of the forearm with the elbow at 90° flexion) — success rate comparable or slightly higher. If reduction fails after 2–3 attempts, obtain X-rays to rule out fracture and consider orthopedic referral.
Toddler Fractures
A spiral or oblique non-displaced fracture of the tibial shaft in children 9 months to 3 years. Often from a twisting mechanism during walking/running. The child refuses to bear weight or limps, with point tenderness over the tibial shaft. X-ray may initially be normal or show a subtle oblique lucency. If clinical suspicion is high with negative initial X-rays, apply a posterior long-leg splint and arrange follow-up X-rays in 7–10 days (periosteal reaction will confirm the fracture). Non-accidental trauma must always be considered in a child with unexplained fractures, especially metaphyseal corner fractures, posterior rib fractures, or fractures in non-ambulatory infants.
Foreign Body in Ear
Common objects: beads, insects, small toys, paper, food. If the child is cooperative and the object is visible: use alligator forceps for graspable objects, suction catheter for round/smooth objects, or irrigation with body-temperature water (contraindicated if TM perforation suspected or vegetable matter — which swells with water). For insects: instill mineral oil or viscous lidocaine to kill the insect before removal. Limit to 2–3 attempts; excessive attempts cause canal edema and pain, making subsequent removal more difficult. Refer to ENT if removal fails.
Foreign Body in Nose
Presents with unilateral foul-smelling nasal discharge, especially if foreign body has been in place for days. If object is visible: positive-pressure technique (parent occludes uninvolved nostril and delivers a puff of air into the child's mouth — "mother's kiss"), alligator forceps, or suction. Vasoconstrict with oxymetazoline spray before attempting removal. Refer to ENT if not visible or removal fails. Button batteries in the nose are an emergency — can cause septal perforation within 1–2 hours via alkali burns.
Swallowed Foreign Bodies
Button battery in esophagus: EMERGENCY. Can cause esophageal perforation and mediastinitis within 2 hours. Immediate ED transfer for emergent endoscopic removal. Do NOT induce vomiting. X-ray shows "double ring" or "halo" sign (distinguish from coin which shows uniform density).
Button battery past esophagus (in stomach/intestines): If asymptomatic, may be observed with serial X-rays. Most pass within 48–72 hours. ED referral if >20 mm diameter or fails to progress.
Coins: Most common swallowed foreign body in children. If in esophagus and symptomatic (drooling, dysphagia, vomiting), refer to ED for removal. If asymptomatic and in stomach, observe — most pass within 1–2 weeks.
Sharp objects (pins, tacks, bone): If in esophagus, emergent removal. If in stomach, most pass spontaneously but higher perforation risk — follow with serial X-rays and refer to GI/surgery.
Magnets: Single magnet: treat like a coin. Multiple magnets: EMERGENCY — can attract across bowel loops causing pressure necrosis, perforation, and fistula. Immediate ED referral for removal.
Pediatric Dehydration Assessment
| Feature | Mild (3–5%) | Moderate (6–9%) | Severe (≥10%) |
|---|---|---|---|
| Mental status | Normal, alert | Restless, irritable | Lethargic, obtunded |
| Thirst | Slightly increased | Moderately increased | Drinks poorly or unable |
| Heart rate | Normal | Increased | Increased, weak/thready |
| Urine output | Slightly decreased | Decreased (<1 mL/kg/hr) | Minimal or absent |
| Tears | Present | Decreased | Absent |
| Mucous membranes | Slightly dry | Dry | Parched, cracked |
| Skin turgor | Normal | Decreased (tenting 1–2 sec) | Very decreased (tenting >2 sec) |
| Fontanelle (infant) | Normal | Sunken | Very sunken |
| Eyes | Normal | Sunken | Deeply sunken |
| Management | ORS at home | ORS in clinic, consider IV | IV fluid bolus 20 mL/kg NS, ED transfer |
21 Occupational Medicine in Urgent Care
Workers' Compensation Documentation
Accurate documentation is critical in occupational injury cases as it has legal and financial implications. Every work injury note must include: (1) date and time of injury, (2) detailed mechanism (how, where, what task), (3) body part(s) affected, (4) employer name and contact, (5) pre-existing conditions (if any) relevant to the injury, (6) objective findings (detailed physical exam), (7) work status (full duty, modified duty with specific restrictions, or off work — with dates), (8) follow-up plan. Work restrictions must be specific and functional: "no lifting >10 lbs with right arm," not "light duty." Always complete the employer's first report of injury form.
DOT Physical Examinations
FMCSA (Federal Motor Carrier Safety Administration) medical examinations for commercial motor vehicle (CMV) drivers. The examiner must be listed on the National Registry of Certified Medical Examiners. Key disqualifying conditions: uncontrolled diabetes on insulin (requires exemption), seizure disorder (seizure-free ≥8 years off medication), uncontrolled hypertension (stage 3: BP ≥180/110 = disqualified; stage 2: BP 160–179/100–109 = 1-year certification; stage 1: BP 140–159/90–99 = 1-year certification; normal/pre-HTN: 2-year certification), vision <20/40 in each eye (with or without correction), hearing loss (inability to perceive forced whisper at 5 feet). Complete physical exam with emphasis on cardiovascular, neurologic, musculoskeletal, and metabolic function.
Drug Screening
DOT-mandated drug panels test for: marijuana, cocaine, opiates, amphetamines/methamphetamines, and PCP. Chain of custody must be maintained: specimen collected under observation (or with split specimen), sealed with tamper-evident tape, documented on the federal CCF (Custody and Control Form), and sent to a SAMHSA-certified laboratory. MRO (Medical Review Officer) reviews and verifies results. Non-DOT employer screens may include additional substances (benzodiazepines, barbiturates, methadone, MDMA).
Needlestick / Bloodborne Pathogen Exposure Protocol
Immediate care: Wash wound with soap and water (do NOT squeeze or milk the wound). Mucous membrane exposure: irrigate with water or saline.
Source patient testing: Test source for HIV, hepatitis B (HBsAg), hepatitis C (anti-HCV). Obtain with consent.
Exposed worker baseline testing: HIV antibody, hepatitis B surface antibody (anti-HBs), hepatitis C antibody, CBC, liver function tests.
HIV PEP: Must be initiated within 72 hours of exposure (ideally within 1–2 hours). Standard 3-drug regimen: tenofovir-emtricitabine (Truvada) + raltegravir (Isentress) or dolutegravir (Tivicay) × 28 days. Consult the PEPline (1-888-448-4911) for complex exposures.
Hepatitis B: If exposed worker is unvaccinated or non-responder — HBIG 0.06 mL/kg IM within 24 hours + initiate/complete HBV vaccine series. If vaccinated with documented anti-HBs ≥10: no treatment needed.
Hepatitis C: No prophylaxis available. Baseline and follow-up HCV RNA at 4–6 weeks; anti-HCV and ALT at 4–6 months. Early identification of seroconversion allows treatment with direct-acting antivirals (cure rate >95%).
OSHA Reporting
Employers must report to OSHA: all work-related fatalities (within 8 hours), in-patient hospitalizations, amputations, or loss of an eye (within 24 hours). Maintain OSHA 300 log of recordable injuries. An injury is OSHA-recordable if it results in: death, days away from work, restricted work or job transfer, medical treatment beyond first aid, loss of consciousness, or significant injury/illness diagnosed by a physician.
Pre-Employment & Return-to-Work Evaluations
Urgent care frequently performs: pre-employment physicals (fitness-for-duty assessment based on essential job functions), return-to-work evaluations (after injury or illness — document functional capacity relative to job demands), and sports physicals (preparticipation physical examination for student athletes — focused cardiac history for sudden cardiac death risk, musculoskeletal screening, and concussion history). For sports physicals, use the AAP/AAFP standardized PPE form. Key cardiac red flags in young athletes: exertional syncope, family history of sudden cardiac death <50 years, known structural heart disease, and exertional chest pain.
Common Occupational Injuries
| Injury Type | Key Considerations | Documentation Requirements |
|---|---|---|
| Eye injuries (foreign body, chemical splash) | Irrigate chemical burns immediately (≥2 L); check visual acuity; slit lamp if available; fluorescein staining for corneal abrasion | Mechanism, chemical identity (MSDS), visual acuity pre/post treatment |
| Back strains | Most common WC claim; red flags rule-out; specific functional restrictions | Mechanism of lifting/twisting, prior back history, objective ROM limitations |
| Hand/finger lacerations | Tendon and nerve testing critical; dominant hand status; job-specific impact | Detailed mechanism, tendon/nerve exam documented, work restrictions |
| Repetitive strain (carpal tunnel) | Phalen test, Tinel sign; nerve conduction referral if persistent | Timeline of symptom onset, job tasks performed, prior treatment |
| Needlestick / splash | See bloodborne pathogen protocol above | Type of exposure, source patient status, PPE worn, PEP initiated |
22 Procedures & Minor Surgery
Incision & Drainage (I&D)
Detailed technique covered in Section 13. Key points: field block anesthesia (not into abscess cavity), #11 scalpel, full-length incision, break up loculations, irrigate, pack loosely. Document: size of abscess cavity, volume and character of drainage, packing placed, culture sent. Coding: CPT 10060 (simple) or 10061 (complicated).
Nail Removal & Subungual Hematoma Trephination
Subungual hematoma causing significant pain (>50% nail involvement or throbbing pain): trephination using an 18-gauge needle (rotated with gentle pressure) or electrocautery device through the nail plate to decompress the hematoma. Provides immediate pain relief. If the hematoma is >50% of the nail bed or the nail is disrupted, consider partial or complete nail removal with nail bed inspection/repair. Nail removal (partial or complete): digital block anesthesia (ring block at base of digit), use a hemostat to dissect the nail plate from the nail bed, starting at the free edge and advancing proximally. Inspect the nail bed for laceration requiring repair with absorbable suture (6-0 chromic gut). Replace the nail plate or apply non-adherent gauze as a splint for the eponychial fold to prevent adhesion.
Foreign Body Removal
Superficial: Splinters, glass, and superficial metallic fragments can be removed with forceps, needle tip dissection, or incision over the palpable object. Deeper objects: Use fluoroscopy (if available), ultrasound guidance, or obtain X-ray to localize. Glass ≥2 mm is visible on X-ray. Wood and organic material are radiolucent — ultrasound is more sensitive. If foreign body is deeply embedded, near vital structures, or cannot be localized, refer to surgery. Document removal attempts, retained foreign body if applicable, and imaging findings.
Joint Injection & Aspiration
Common in urgent care for gout flares (diagnostic aspiration + therapeutic steroid injection if infection excluded), knee effusion (diagnostic aspiration), and trigger finger/de Quervain's (steroid injection). Technique: sterile prep, landmark identification (or ultrasound guidance if available), 18-gauge needle for aspiration (large joints), 25-gauge for injection. Knee aspiration: lateral approach (2 cm above and 1 cm lateral to superior-lateral patella, directed medially and inferiorly) or medial approach. Send fluid for: cell count, crystals, Gram stain, culture. Injection (after infection excluded): triamcinolone 40 mg (large joints) or 10–20 mg (small joints) + 1% lidocaine for immediate pain relief.
Cerumen Removal
Irrigation: Body-temperature water via syringe (20–60 mL) directed at the superior canal wall. Contraindicated if: known or suspected TM perforation, pressure-equalization (PE) tubes, or history of ear surgery. Consider pre-treatment with cerumenolytic (carbamide peroxide or docusate sodium drops) for 15–30 minutes before irrigation. Curette: Direct visualization with otoscope, use plastic or metal curette to scoop impacted cerumen. Safer than irrigation for patients with TM concerns. Suction: Frazier suction tip under direct visualization for soft cerumen.
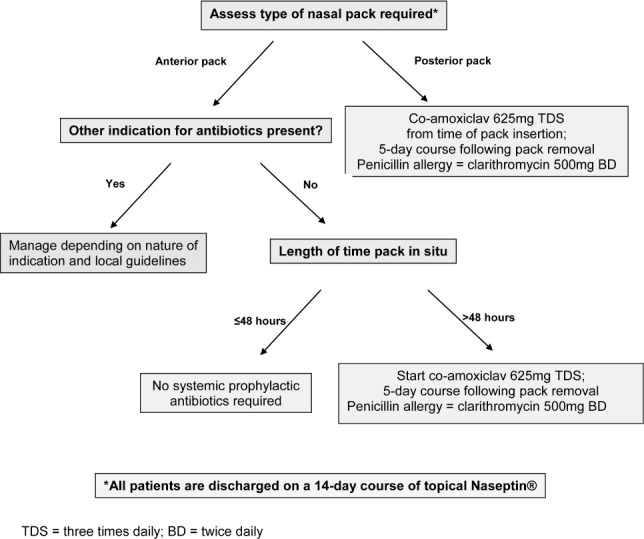
Epistaxis Management
Most nosebleeds are anterior (Kiesselbach plexus on the anterior septum). Initial management: (1) sit upright, lean forward (do NOT tilt head back — promotes swallowing blood), (2) direct pressure — pinch the soft part of the nose firmly for 15–20 minutes continuously, (3) apply topical vasoconstrictor (oxymetazoline spray) before pressure. If direct pressure fails: (4) examine with nasal speculum to identify bleeding source, (5) silver nitrate cautery of the visible bleeding vessel (apply for 5–10 seconds, cauterize only ONE side of the septum to avoid perforation), (6) anterior nasal packing if cautery fails: insert Merocel sponge (expandable PVA) or Rapid Rhino (inflatable balloon), moisten with saline or water. Leave in place 24–48 hours; arrange ENT follow-up for removal. Posterior epistaxis (profuse bleeding, unable to localize, blood in posterior pharynx) requires ED transfer for posterior packing or balloon tamponade.
23 Medication Management & Prescribing
Controlled Substance Prescribing
Urgent care providers must balance adequate pain management with responsible opioid prescribing. General principles: (1) use multimodal analgesia first (NSAIDs + acetaminophen), (2) if opioids are necessary, prescribe the lowest effective dose for the shortest duration (≤3–5 days), (3) check the Prescription Drug Monitoring Program (PDMP) before prescribing — required by law in most states, (4) do NOT prescribe long-acting opioids, methadone, or fentanyl from urgent care, (5) avoid prescribing benzodiazepines + opioids concurrently (FDA black box warning), (6) document pain assessment, failed non-opioid measures, and rationale for opioid prescribing.
Antibiotic Stewardship
Urgent care is a critical setting for antibiotic stewardship. Conditions that do NOT require antibiotics: viral URI, acute bronchitis, non-specific cough, viral pharyngitis (Centor 0–1), acute viral sinusitis (<10 days), non-specific viral gastroenteritis, asymptomatic bacteriuria in non-pregnant patients. Display patient education materials explaining why antibiotics are not always needed. Use delayed prescribing (safety net prescription) when appropriate: give the prescription but instruct the patient to fill it only if symptoms worsen or fail to improve in 48–72 hours.
Common Prescription Protocols
| Prescription | Indication | Regimen | Key Considerations |
|---|---|---|---|
| Z-pack (azithromycin) | GAS pharyngitis (PCN allergy), atypical CAP, ABRS (2nd line) | 500 mg day 1, 250 mg days 2–5 | Overused; NOT indicated for bronchitis or viral URI; QTc prolongation risk |
| Medrol dose pack (methylprednisolone) | Acute pain/inflammation, gout, allergic reactions | 4 mg tabs: 6-5-4-3-2-1 taper over 6 days | Insufficient duration for poison ivy (rebound); not needed for most back pain |
| Prednisone burst | Asthma exacerbation, gout, allergic reaction, poison ivy | 40–60 mg daily × 5 days (asthma); 12–14 day taper (contact dermatitis) | No taper needed if ≤7 days; counsel on hyperglycemia, insomnia |
| Augmentin (amox-clav) | ABRS, AOM (2nd line), bites, complicated UTI | 875/125 mg PO BID × 5–10 days | GI side effects common; take with food; diarrhea risk |
| Nitrofurantoin (Macrobid) | Uncomplicated cystitis | 100 mg PO BID × 5 days | Avoid if GFR <30; take with food; not for pyelo |
Avoiding Inappropriate Antibiotics
The most commonly over-prescribed antibiotics in urgent care: (1) azithromycin for bronchitis — never indicated for viral bronchitis, (2) fluoroquinolones for uncomplicated UTI — reserve for complicated infections, (3) antibiotics for viral URI — always inappropriate, (4) antibiotics for sinusitis before 10 days — most resolve without treatment. Use patient education handouts, shared decision-making, and symptom-management prescriptions (decongestants, analgesics) as alternatives to unnecessary antibiotics.
24 Disposition Decision-Making
Every urgent care visit concludes with a disposition decision: discharge home, transfer to the ED, direct admission (rare), or referral for follow-up. Documenting the reasoning for each disposition decision is essential for patient safety and medicolegal protection.
ED Transfer Criteria by System
Cardiovascular: Chest pain with ECG changes or positive troponin, acute HF exacerbation, hypertensive emergency (SBP >180 with end-organ damage), syncope with cardiac features, suspected DVT/PE, aortic emergency.
Neurological: New focal deficit, stroke symptoms, first seizure, status epilepticus, suspected meningitis/encephalitis, acute severe headache ("worst of life" — SAH), altered mental status.
Respiratory: SpO₂ <92% not improving, severe asthma (no improvement with 3 nebs), suspected PE, pneumothorax, respiratory distress requiring continuous monitoring.
GI: GI hemorrhage, acute abdomen (peritoneal signs), suspected appendicitis/cholecystitis/pancreatitis, bowel obstruction, inability to tolerate PO with dehydration.
GU: Testicular torsion, ectopic pregnancy, pyelonephritis in pregnancy, gross hematuria with hemodynamic changes, urinary retention.
Musculoskeletal: Open fracture, neurovascular compromise, compartment syndrome, hip fracture, unstable spine injury, dislocation that cannot be reduced.
Infectious: Sepsis/SIRS with hemodynamic instability, febrile neonate (≤28 days), epiglottitis, necrotizing fasciitis, orbital cellulitis.
Psychiatric: Active suicidal ideation with plan/intent, homicidal ideation, acute psychosis, overdose/ingestion (any symptomatic).
OB/GYN: Ectopic pregnancy, threatened abortion with hemodynamic instability, ovarian torsion, sexual assault (SANE exam).
Work & School Notes
Provide specific, time-limited documentation: "Patient may return to work on [date] with the following restrictions: [list specific restrictions]" or "Patient is excused from school from [date] to [date]." Avoid open-ended work excuses. For occupational injuries, work status must include: full duty, modified duty (with specific functional limitations), or complete work restriction, with a date for reassessment.
Return Precautions — Condition-Specific Red Flags
Document specific return precautions for every patient. Examples:
| Condition | Return Precautions to Document |
|---|---|
| Head injury | Worsening headache, vomiting, confusion, unequal pupils, seizure, weakness, slurred speech |
| Abdominal pain | Worsening pain, fever, vomiting unable to keep fluids down, blood in stool, fainting |
| Laceration repair | Increasing redness, swelling, warmth, purulent drainage, red streaking, fever, wound opening |
| Fracture/splint | Numbness, tingling, color change in fingers/toes, increasing pain despite elevation, inability to move digits |
| Asthma | Not improving with rescue inhaler, difficulty speaking in sentences, blue lips, peak flow <50% |
| UTI | Fever, back/flank pain, vomiting, blood in urine, symptoms not improving in 48 hours |
| Pediatric fever | Fever >5 days, rash, stiff neck, inconsolable, not feeding, decreased wet diapers, lethargy |
Follow-Up Timing by Condition
| Condition | Follow-Up Timing | Follow-Up Provider |
|---|---|---|
| Fractures (stable, splinted) | 5–7 days | Orthopedics |
| Lacerations (clean, sutured) | Suture removal per schedule (3–14 days by location) | Urgent care or PCP |
| Lacerations (contaminated/bite) | 48 hours wound check | Urgent care |
| Abscess post-I&D | 48–72 hours for packing change/removal | Urgent care |
| UTI (uncomplicated) | Only if not improving in 48 hours | Urgent care or PCP |
| Pyelonephritis (outpatient) | 48 hours clinical reassessment | Urgent care or PCP |
| Pneumonia (outpatient) | 48–72 hours or sooner if worsening | Urgent care or PCP |
| Asthma exacerbation | 1–4 weeks with PCP or pulmonology | PCP / pulmonology |
| Work injury (WC) | Per WC requirements (often 48–72 hours) | Occupational medicine / urgent care |
| Ankle sprain grade II–III | 1–2 weeks, sooner if not improving | PCP, sports medicine, or orthopedics |
| Abnormal X-ray overread | Contact patient within 24 hours of receiving discrepant overread | Urgent care (phone callback) |
| STI (positive result) | Partner notification; test of cure for gonorrhea in 2 weeks if pharyngeal | Urgent care or PCP |
| Burns (minor) | 24–48 hours wound check | Urgent care; refer burn center if worsening |
25 Documentation & Coding
E&M Coding in Urgent Care
Urgent care visits are coded using standard outpatient E&M codes. Under the 2021 E&M coding reforms, office/outpatient visits (99202–99215) are based on medical decision-making (MDM) complexity or total time spent on the encounter.
| Code | Patient Status | MDM Level | Time (Total) | Typical Urgent Care Example |
|---|---|---|---|---|
| 99202 | New | Straightforward | 15–29 min | Simple URI, medication refill |
| 99203 | New | Low | 30–44 min | UTI with UA, pharyngitis with rapid strep |
| 99204 | New | Moderate | 45–59 min | Laceration repair evaluation, pneumonia workup |
| 99205 | New | High | 60–74 min | Complex multi-system complaint, ED transfer decision |
| 99212 | Established | Straightforward | 10–19 min | Suture removal, wound recheck |
| 99213 | Established | Low | 20–29 min | Acute sinusitis, ankle sprain with X-ray |
| 99214 | Established | Moderate | 30–39 min | Asthma exacerbation with nebs, abscess I&D |
| 99215 | Established | High | 40–54 min | Chest pain evaluation, complex medical decision |
Medical Decision-Making Elements
MDM is determined by the highest 2 of 3 elements: (1) Number and complexity of problems addressed — from minimal (1 self-limited problem) to high (acute illness with threat to life). (2) Amount and complexity of data reviewed — from minimal/none to extensive (ordering and reviewing tests, external records, independent interpretation of imaging). (3) Risk of complications, morbidity, or mortality — from minimal to high (drug therapy requiring intensive monitoring, decision for ED transfer, major surgery).
Modifier 25
Modifier 25 appended to the E&M code indicates a significant, separately identifiable evaluation and management service performed on the same day as a procedure. Example: patient presents with an abscess — the E&M (evaluation, history, decision-making about antibiotic need, MRSA risk, follow-up planning) is billed with modifier 25, and the I&D is billed separately (10060/10061). The E&M note must clearly document the evaluation component distinct from the procedure.
Common Procedure Codes
| CPT Code | Procedure | Description |
|---|---|---|
| 10060 | I&D, simple | Single abscess, simple or superficial |
| 10061 | I&D, complicated | Multiple abscesses, complex, packing |
| 12001–12007 | Simple repair | Superficial wound closure (size-based) |
| 12031–12057 | Intermediate repair | Layered closure, extensive cleaning |
| 29125/29130 | Forearm splint | Short arm splint application |
| 29515 | Lower leg splint | Short leg splint application |
| 69200 | FB removal, ear | Foreign body removal from external auditory canal |
| 69210 | Cerumen removal | Removal of impacted cerumen (one or both ears) |
| 30300 | FB removal, nose | Foreign body removal, intranasal |
| 11730/11750 | Nail procedures | Nail avulsion (partial/complete) |
| 20600–20611 | Joint aspiration/injection | Small/intermediate/major joint |
Time-Based Billing
When time is used as the basis for code selection, document the total time spent on the encounter date, including: reviewing records, obtaining and reviewing history, examination, ordering and reviewing results, counseling, care coordination, and documentation. Time does NOT need to be face-to-face. When prolonged services extend beyond the typical time for the highest-level E&M code, use add-on codes 99417 (each additional 15 minutes beyond 99205/99215 time threshold).
Documentation Best Practices
Urgent care documentation must be thorough yet efficient. Essential elements for every note: (1) HPI with onset, location, duration, character, aggravating/alleviating factors, associated symptoms, and severity. (2) Pertinent negatives — especially red flag symptoms reviewed and absent (e.g., "denies chest pain, shortness of breath, hemoptysis" in a cough patient). (3) Physical exam focused on the complaint but including relevant systems (e.g., lung exam for abdominal pain to exclude lower-lobe pneumonia). (4) Medical decision-making narrative: document the differential diagnosis considered, why diagnoses were ruled in or out, rationale for testing or imaging, and rationale for treatment chosen. (5) Patient education and counseling including expected course, return precautions (specific red flags to watch for), and instructions given. (6) Disposition and follow-up plan. Good documentation is the best defense against malpractice claims — "if it wasn't documented, it wasn't done."
26 Scoring Systems
Ottawa Ankle Rules
See Section 8 for complete criteria. Sensitivity 97–100% for clinically significant fractures. An ankle X-ray is indicated only if there is malleolar zone pain PLUS bone tenderness at the posterior edge/tip of either malleolus OR inability to bear weight (4 steps). A foot X-ray is indicated only if there is midfoot pain PLUS bone tenderness at the 5th metatarsal base or navicular OR inability to bear weight (4 steps).
Ottawa Knee Rules
A knee X-ray is required only if ANY of: (1) age ≥55, (2) tenderness at fibular head, (3) isolated patellar tenderness, (4) inability to flex to 90°, (5) inability to bear weight (4 steps) immediately and in clinic. Sensitivity ~99% for fracture.
Centor / McIsaac Score (Full)
| Criterion | Points |
|---|---|
| Tonsillar exudates | +1 |
| Tender anterior cervical adenopathy | +1 |
| History of fever or temp >38°C | +1 |
| Absence of cough | +1 |
| Age 3–14 | +1 |
| Age 15–44 | 0 |
| Age ≥45 | −1 |
Score interpretation: ≤1 = no test, no antibiotics (~5–10% GAS probability). 2–3 = rapid strep test, treat if positive (~15–35% probability). ≥4 = rapid strep, consider empiric Rx (~50% probability).
Alvarado Score (MANTRELS) for Appendicitis
| Criterion | Points |
|---|---|
| Migration of pain to RLQ | 1 |
| Anorexia | 1 |
| Nausea/vomiting | 1 |
| Tenderness in RLQ | 2 |
| Rebound tenderness | 1 |
| Elevated temperature (≥37.3°C) | 1 |
| Leukocytosis (>10,000) | 2 |
| Shift of WBC to left | 1 |
Total 10. ≤4: low probability, observe/discharge. 5–6: equivocal, imaging recommended. 7–8: probable, surgical consult. ≥9: very probable appendicitis.
Wells Score for Pulmonary Embolism
| Criterion | Points |
|---|---|
| Clinical signs/symptoms of DVT | 3.0 |
| PE is #1 diagnosis or equally likely | 3.0 |
| Heart rate >100 bpm | 1.5 |
| Immobilization (≥3 days) or surgery in past 4 weeks | 1.5 |
| Previous DVT/PE | 1.5 |
| Hemoptysis | 1.0 |
| Malignancy (treatment within 6 months or palliative) | 1.0 |
Score ≤4: PE unlikely — check D-dimer. If D-dimer negative (<500 ng/mL, or age-adjusted: age × 10 for patients >50 years), PE effectively excluded. If D-dimer positive, CT-PA needed (ED transfer). Score >4: PE likely — CT-PA needed, transfer to ED (do not rely on D-dimer alone). Important: D-dimer is elevated in many conditions (pregnancy, malignancy, post-operative state, advanced age, infection) and has value only for its negative predictive value in low-probability patients. Never use D-dimer to "rule in" PE.
PERC Rule (Pulmonary Embolism Rule-Out Criteria)
If clinical gestalt suggests PE probability <15% (low pretest probability), the PERC rule can be applied to avoid unnecessary D-dimer testing. If ALL eight criteria are met, PE is effectively excluded without any testing:
| # | PERC Criterion |
|---|---|
| 1 | Age <50 years |
| 2 | Heart rate <100 bpm |
| 3 | SpO₂ ≥95% on room air |
| 4 | No hemoptysis |
| 5 | No estrogen use (OCP, HRT) |
| 6 | No prior DVT/PE |
| 7 | No unilateral leg swelling |
| 8 | No surgery/trauma requiring hospitalization in past 4 weeks |
If any ONE criterion is not met, proceed to Wells score and D-dimer pathway. PERC rule sensitivity is ~97% and reduces unnecessary testing in low-risk patients.
Wells Score for DVT
| Criterion | Points |
|---|---|
| Active cancer (within 6 months) | 1 |
| Paralysis, paresis, or recent lower extremity cast | 1 |
| Recently bedridden ≥3 days or major surgery within 12 weeks | 1 |
| Localized tenderness along deep venous system | 1 |
| Entire leg swollen | 1 |
| Calf swelling ≥3 cm compared to asymptomatic side | 1 |
| Pitting edema confined to symptomatic leg | 1 |
| Collateral superficial veins (non-varicose) | 1 |
| Previously documented DVT | 1 |
| Alternative diagnosis at least as likely as DVT | −2 |
Score ≤1: DVT unlikely — check D-dimer. Negative D-dimer excludes DVT. Score ≥2: DVT likely — obtain compression ultrasound.
Westley Croup Score
| Feature | 0 | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|---|
| Stridor | None | With agitation | At rest | — | — | — |
| Retractions | None | Mild | Moderate | Severe | — | — |
| Air entry | Normal | Decreased | Markedly decreased | — | — | — |
| Cyanosis | None | — | — | — | With agitation | At rest |
| Level of consciousness | Normal | — | — | — | — | Altered |
Total 0–17. Mild: ≤2. Moderate: 3–7. Severe: ≥8.
27 Common Medications Quick Reference
Antibiotics
| Medication | Common Indications | Adult Dose | Duration | Key Notes |
|---|---|---|---|---|
| Amoxicillin | GAS pharyngitis, AOM, dental infections | 500 mg BID or 1 g TID (CAP) | 5–10 days | First-line for strep; well tolerated |
| Amoxicillin-clavulanate | ABRS, AOM (2nd line), bites, UTI | 875/125 mg BID | 5–10 days | GI upset common; take with food |
| Azithromycin (Z-pack) | GAS (PCN allergy), CAP, chlamydia | 500 mg day 1, then 250 mg × 4 | 5 days | NOT for bronchitis; QTc risk |
| Doxycycline | CAP, ABRS (PCN allergy), MRSA skin, chlamydia, PID | 100 mg BID | 5–14 days | Photosensitivity; avoid in pregnancy/children <8 |
| Cephalexin | Cellulitis (MSSA), UTI, skin infections | 500 mg QID | 5–10 days | Does NOT cover MRSA |
| TMP-SMX DS | Uncomplicated UTI, MRSA skin infections | 160/800 mg BID | 3–10 days | Check sulfa allergy; avoid in pregnancy (1st tri/term) |
| Nitrofurantoin (Macrobid) | Uncomplicated cystitis | 100 mg BID | 5 days | Avoid if GFR <30; take with food; not for pyelo |
| Ciprofloxacin | Pyelonephritis, complicated UTI, prostatitis | 500 mg BID | 5–14 days | FDA black box (tendon, neuropathy); reserve for appropriate indications |
| Ceftriaxone | Gonorrhea, PID, pyelonephritis (initial dose) | 500 mg–1 g IM | Single dose (or series) | IM injection; reconstitute with lidocaine 1% to reduce pain |
| Metronidazole | Trichomoniasis, BV, diverticulitis, PID | 500 mg BID or TID | 7–14 days | No alcohol (disulfiram reaction); metallic taste |
| Clindamycin | MRSA + strep coverage, dental infections, GAS (allergy) | 300–450 mg TID | 7–10 days | C. difficile risk; monitor for diarrhea |
Analgesics
| Medication | Dose | Max Daily | Key Notes |
|---|---|---|---|
| Acetaminophen | 500–1000 mg Q6H PRN | 3,000 mg (4,000 mg in healthy adults) | Hepatotoxicity at high doses; check for combination products |
| Ibuprofen | 400–800 mg Q6–8H | 3,200 mg | GI, renal, CV risk; avoid in CKD, GI bleed history |
| Naproxen | 250–500 mg Q12H | 1,250 mg (acute); 1,000 mg (chronic) | Longer half-life than ibuprofen; same NSAID warnings |
| Ketorolac (Toradol) | 15–30 mg IM/IV; 10 mg PO | 120 mg (IM/IV day 1); 40 mg PO | Max 5 days total; powerful NSAID; renal/GI caution |
| Hydrocodone/APAP | 5/325 mg Q4–6H PRN | 6 tabs/day (APAP limit) | Schedule II; PDMP check; ≤3–5 day supply from UC |
| Oxycodone | 5 mg Q4–6H PRN | Titrate to effect | Schedule II; short-acting only from UC; combine with NSAID/APAP |
| Tramadol | 50–100 mg Q6H PRN | 400 mg | Schedule IV; seizure risk; serotonin syndrome risk with SSRIs |
Corticosteroids
| Medication | Indication | Typical Dose | Duration |
|---|---|---|---|
| Prednisone | Asthma exacerbation | 40–60 mg PO daily | 5 days (no taper) |
| Prednisone | Gout flare | 0.5 mg/kg/day | 5–7 days |
| Prednisone | Contact dermatitis (poison ivy) | 60-40-20 mg taper | 12–14 days minimum |
| Dexamethasone | Croup | 0.6 mg/kg PO/IM (max 10 mg) | Single dose |
| Dexamethasone | Pharyngitis (adjunctive pain relief) | 10 mg PO/IM × 1 | Single dose |
| Methylprednisolone dose pack | Acute musculoskeletal pain | 4 mg tapered over 6 days | 6 days |
| Triamcinolone acetonide | Joint injection | 10–40 mg intra-articular | Single injection |
28 Abbreviations Master List
| Abbreviation | Full Term |
|---|---|
| ABRS | Acute bacterial rhinosinusitis |
| ACE-I | Angiotensin-converting enzyme inhibitor |
| ACLS | Advanced cardiovascular life support |
| ACS | Acute coronary syndrome |
| AOM | Acute otitis media |
| AOE | Acute otitis externa |
| ATFL | Anterior talofibular ligament |
| BID | Twice daily |
| BLS | Basic life support |
| BMP | Basic metabolic panel |
| BSA | Body surface area |
| CAP | Community-acquired pneumonia |
| CBC | Complete blood count |
| CCF | Custody and control form |
| CFL | Calcaneofibular ligament |
| CKD | Chronic kidney disease |
| CMP | Comprehensive metabolic panel |
| CMV | Commercial motor vehicle |
| CN | Cranial nerve |
| CPT | Current procedural terminology |
| CRP | C-reactive protein |
| CT | Computed tomography |
| CVA | Costovertebral angle |
| CXR | Chest X-ray |
| DIP | Distal interphalangeal |
| DOT | Department of Transportation |
| DVT | Deep vein thrombosis |
| EBV | Epstein-Barr virus |
| ED | Emergency department |
| E&M | Evaluation and management |
| EMS | Emergency medical services |
| ENT | Ear, nose, and throat |
| EPT | Expedited partner therapy |
| ESI | Emergency Severity Index |
| FAST | Focused assessment with sonography for trauma |
| FMCSA | Federal Motor Carrier Safety Administration |
| FOOSH | Fall on outstretched hand |
| GAS | Group A Streptococcus |
| GCS | Glasgow Coma Scale |
| GFR | Glomerular filtration rate |
| GI | Gastrointestinal |
| GU | Genitourinary |
| HBIG | Hepatitis B immune globulin |
| HCG | Human chorionic gonadotropin |
| HFMD | Hand-foot-mouth disease |
| HIV | Human immunodeficiency virus |
| HRIG | Human rabies immune globulin |
| I&D | Incision and drainage |
| IDSA | Infectious Diseases Society of America |
| ILI | Influenza-like illness |
| IM | Intramuscular |
| IV | Intravenous |
| IVDU | Intravenous drug use |
| LOC | Loss of consciousness |
| LP | Lumbar puncture |
| MAP | Mean arterial pressure |
| MC | Metacarpal |
| MCP | Metacarpophalangeal |
| MDI | Metered-dose inhaler |
| MDM | Medical decision-making |
| MRO | Medical review officer |
| MRSA | Methicillin-resistant Staphylococcus aureus |
| MSSA | Methicillin-sensitive Staphylococcus aureus |
| MTP | Metatarsophalangeal |
| NAAT | Nucleic acid amplification test |
| NS | Normal saline (0.9% NaCl) |
| NSAID | Non-steroidal anti-inflammatory drug |
| OME | Otitis media with effusion |
| ORS | Oral rehydration solution |
| OSHA | Occupational Safety and Health Administration |
| OTC | Over-the-counter |
| PCR | Polymerase chain reaction |
| PDMP | Prescription Drug Monitoring Program |
| PE | Pulmonary embolism |
| PEF | Peak expiratory flow |
| PEP | Post-exposure prophylaxis |
| PID | Pelvic inflammatory disease |
| PIP | Proximal interphalangeal |
| POC / POCT | Point-of-care (testing) |
| POCUS | Point-of-care ultrasound |
| PPI | Proton pump inhibitor |
| PRN | As needed (pro re nata) |
| PTA | Peritonsillar abscess |
| PTFL | Posterior talofibular ligament |
| PUD | Peptic ulcer disease |
| QID | Four times daily |
| RICE | Rest, ice, compression, elevation |
| RLQ | Right lower quadrant |
| ROM | Range of motion |
| RSV | Respiratory syncytial virus |
| RTC | Return to clinic |
| RUQ | Right upper quadrant |
| SAMHSA | Substance Abuse and Mental Health Services Administration |
| SANE | Sexual assault nurse examiner |
| SBI | Serious bacterial infection |
| SIRS | Systemic inflammatory response syndrome |
| STI | Sexually transmitted infection |
| TID | Three times daily |
| TIG | Tetanus immune globulin |
| TM | Tympanic membrane |
| TMP-SMX | Trimethoprim-sulfamethoxazole |
| UA | Urinalysis |
| UCx | Urine culture |
| URI | Upper respiratory infection |
| US | Ultrasound |
| UTI | Urinary tract infection |
| VZV | Varicella-zoster virus |
| WBC | White blood cell (count) |
| WC | Workers' compensation |