Systematic interpretation of radiographs, CT, MRI, ultrasound, and nuclear medicine across body systems. Modality selection, contrast considerations, normal anatomy, and the recognition patterns needed for every common imaging finding.
01 Imaging Modalities Overview
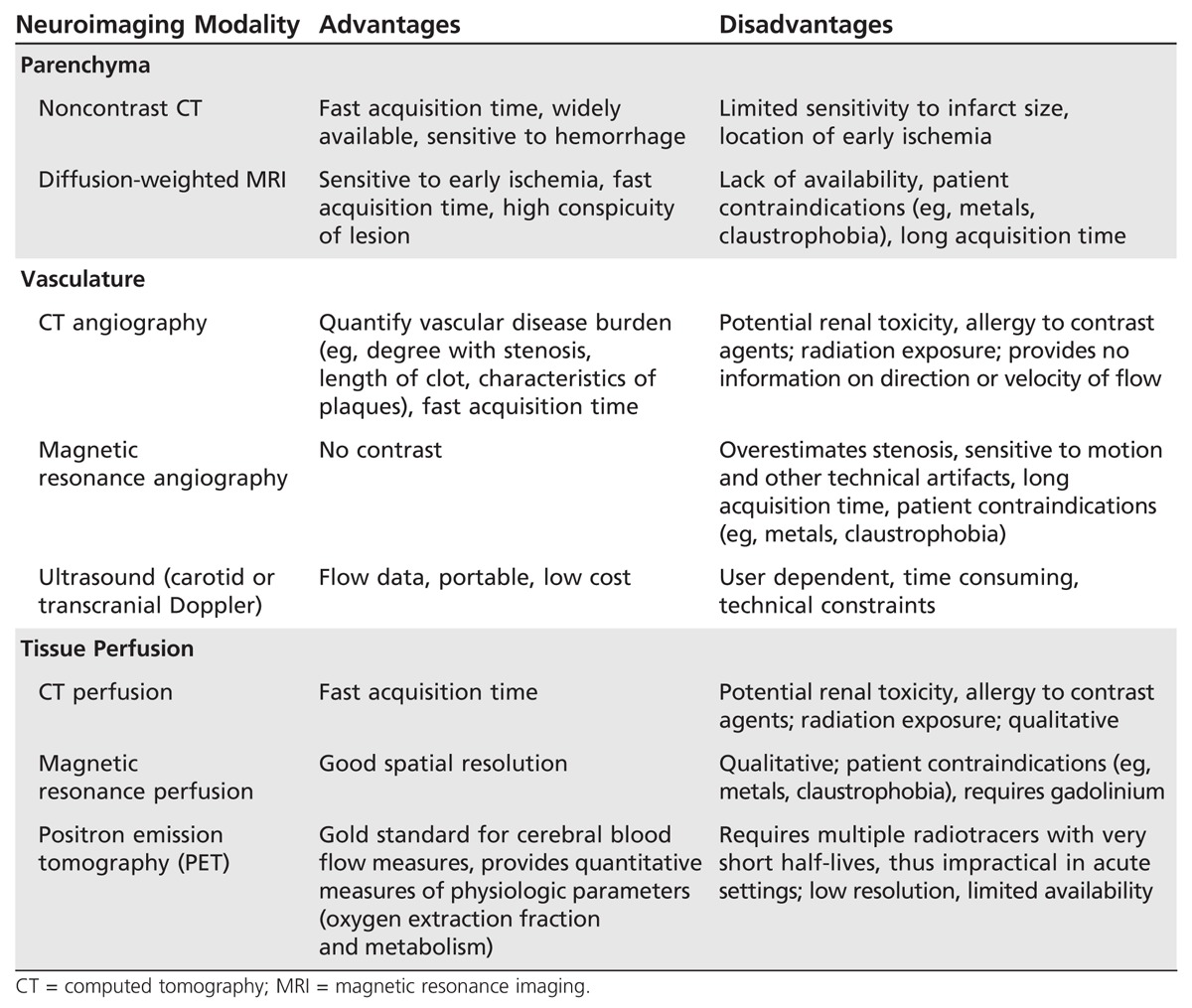
Diagnostic imaging is the most powerful clinical tool for non-invasive diagnosis, surveillance, and procedural guidance. Every clinician — not just radiologists — must be able to select the right study, understand its limitations, and interpret the most common findings. Imaging modalities are distinguished by the physical energy used to generate contrast: ionizing radiation (radiographs, CT, fluoroscopy, nuclear medicine), magnetic fields and radiofrequency (MRI), or mechanical sound waves (ultrasound). Each produces a characteristic appearance and is suited to specific anatomy and pathology.
Why This Matters
Selecting the wrong modality leads to missed diagnoses, unnecessary radiation, contrast harm, and delayed care. A physician who understands modality strengths can order appropriately, interpret independently, and communicate meaningfully with radiology colleagues. The imaging report is a draft — the treating clinician integrates it with the patient.
Modality Comparison
Modality
Energy
Strengths
Limitations
Radiation
Radiograph (X-ray)
Ionizing photons
Fast, cheap, portable, screens bones/lungs
Low soft-tissue contrast, 2D projection
Low (CXR ≈ 0.1 mSv)
CT
Ionizing photons (rotating)
Rapid, high spatial resolution, excellent for trauma, vascular
Radiation dose, IV contrast risk
Moderate–high (5–15 mSv)
MRI
Magnetic field + RF
Superb soft-tissue contrast, multiplanar, no radiation
Slow, expensive, claustrophobia, implants
None
Ultrasound
Mechanical sound waves
Portable, real-time, no radiation, pediatric/OB
Operator-dependent, limited by gas/bone
None
Nuclear medicine
Gamma emission (radiotracer)
Physiologic / functional information
Low spatial resolution, radiation
Variable (1–25 mSv)
Fluoroscopy
Continuous X-ray
Dynamic, procedural guidance, GI studies
Cumulative radiation, operator skill
Variable, can be high
Density & Signal Language
Each modality has a language for describing contrast. Radiographs and CT describe density (radiopaque/white = dense; radiolucent/black = lucent). MRI describes signal intensity (hyperintense = bright; hypointense = dark) on a given sequence. Ultrasound describes echogenicity (hyperechoic = bright; hypoechoic = dark; anechoic = black, typically fluid). Using precise language prevents ambiguity in handoffs and report dictation.
The five densities on plain film are: air (black), fat (dark gray), soft tissue/water (gray), bone/calcium (white), metal (bright white). Memorizing this hierarchy lets you identify foreign bodies, calcifications, and lipomatous lesions at a glance.
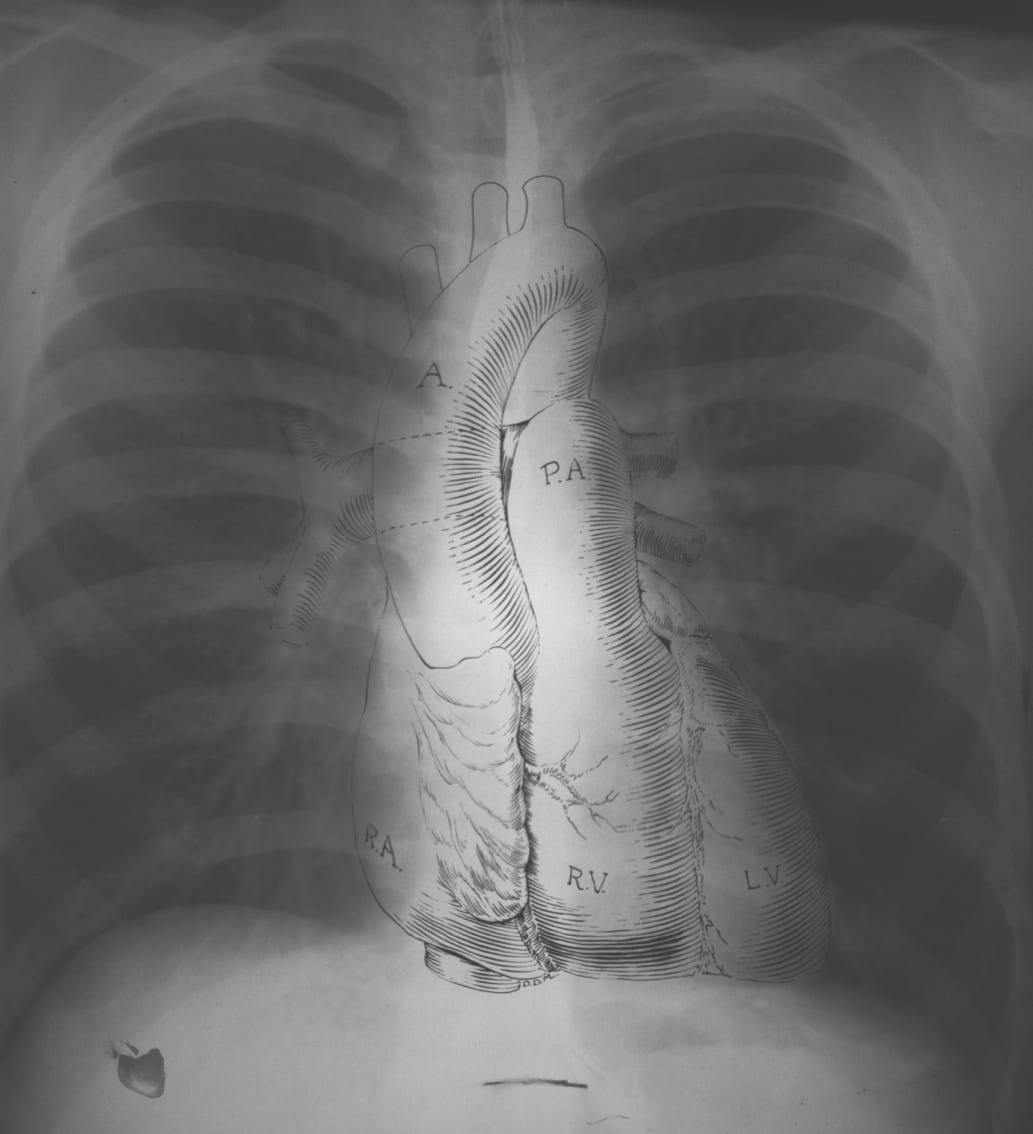
Figure 1 — Normal PA Chest Radiograph. A standard posteroanterior chest X-ray demonstrating normal cardiomediastinal silhouette, bilateral clear lung fields, and key anatomical landmarks used for systematic interpretation.
Role of the Radiologist and the Clinician
Imaging interpretation is a shared responsibility. The radiologist describes findings, generates differential diagnoses, and communicates urgent results directly. The clinician provides the context (symptoms, exam, labs, prior studies) that determines which findings matter and how they change management. The best diagnoses emerge from a dialogue, not a one-way report. Clinicians who review their own imaging alongside the radiologist develop sharper diagnostic skills and catch important subtleties that context-free reads may miss.
Common Requisition Pitfalls
Pitfall
Consequence
Prevention
Vague indication ("pain")
Radiologist under-scrutinizes the actual concern
Provide focused clinical question and exam findings
Wrong modality
Misses diagnosis, wastes radiation/time
Consult ACR Appropriateness Criteria or radiology
No prior studies available
Cannot compare stability vs new findings
Ensure PACS access before ordering
No allergy / renal information
Contrast reactions or nephropathy
Check eGFR and allergy history
Incorrect laterality
Wrong side imaged
Confirm before signing order
02 X-Ray & CT Physics
Radiograph Formation
X-rays are generated when high-energy electrons strike a tungsten anode. The beam passes through the patient and is attenuated differentially by tissues of different atomic number and density. The unattenuated photons strike the detector, producing a 2D projection image. Attenuation increases with higher atomic number (bone, iodine) and thicker tissue. The image represents a superimposition of all structures along the beam path — this is both the strength (efficient survey) and limitation (loss of depth) of radiography.
CT Physics
Computed tomography uses a rotating X-ray tube and detector array to acquire projections from multiple angles around the patient. Reconstruction algorithms (filtered back projection or iterative methods) compute a cross-sectional image in Hounsfield units (HU), which quantify tissue attenuation relative to water.
Tissue
Hounsfield Units
Appearance
Air
−1000
Black
Fat
−100 to −50
Dark gray
Water / CSF
0
Gray
White matter
20–30
Gray
Gray matter
35–45
Slightly brighter
Muscle / soft tissue
30–60
Gray
Acute blood
50–80
Hyperdense
Iodinated contrast
100–500+
Bright white
Bone / calcification
400–1000+
Bright white
Metal
>3000
Streak artifact
CT Windowing
CT images store >4000 HU of data, but the human eye can only discriminate about 30 shades of gray. Windowing selects a range (window width) around a center (window level) to optimize contrast for the tissue of interest. Common windows:
Window
Level (HU)
Width (HU)
Use
Lung
−600
1500
Lung parenchyma, nodules, emphysema
Mediastinum / soft tissue
40
400
Heart, vessels, lymph nodes
Bone
400
1800
Cortex, trabeculae, fractures
Brain
40
80
Gray/white differentiation, blood
Subdural (stroke)
80
200
Subtle subdural or subarachnoid blood
Liver
60
150
Hepatic lesions, contrast enhancement
Always review chest CT in both lung and mediastinal windows. A nodule invisible on mediastinal windowing may be obvious on lung windows, and vice versa for lymphadenopathy. Missing this step is the most common reason residents miss findings.
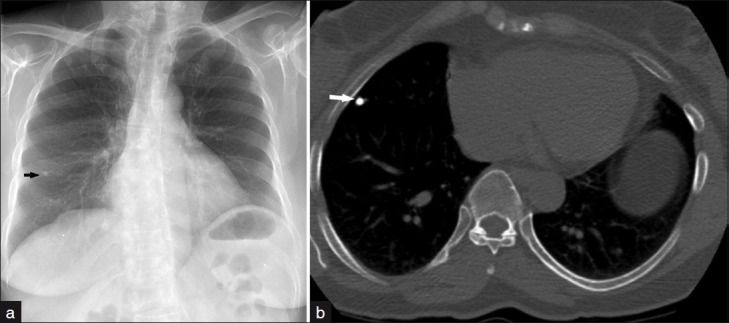
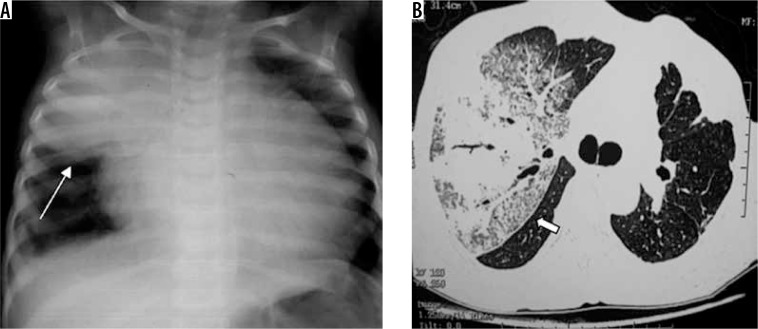
Figure 2 — Hounsfield Unit Density Demonstration. Chest radiograph (left) and axial CT (right) demonstrating a calcified pulmonary granuloma. The high-density calcification appears bright white on CT, illustrating how Hounsfield units quantify tissue attenuation from air (black) through soft tissue (gray) to calcium (white).
CT Artifacts to Recognize
Artifact
Cause
Mitigation
Beam hardening / streak
Dense objects (metal, contrast)
Dual-energy reconstruction, metal artifact reduction
Motion
Patient movement, breathing
Breath-hold, faster scan, sedation
Partial volume
Voxel contains multiple tissue types
Thinner slices
Ring artifact
Detector miscalibration
Technical service
Photon starvation
Insufficient dose in dense body regions
Increased mAs, body habitus compensation
03 MRI Physics & Sequences
MRI exploits the magnetic properties of hydrogen protons in tissue. In the main magnetic field (B0, typically 1.5 or 3 Tesla), protons align and precess at the Larmor frequency. A radiofrequency pulse tips them out of alignment; as they relax back, they emit a signal detected by coils. Two relaxation constants determine tissue contrast:
Constant
Mechanism
Weighted Sequence
T1 (longitudinal)
Return of magnetization to B0 axis
T1-weighted — anatomy
T2 (transverse)
Dephasing in xy plane
T2-weighted — pathology, fluid
Signal Characteristics by Sequence
Tissue
T1
T2
FLAIR
DWI
Water / CSF
Dark
Bright
Dark (suppressed)
Dark
Fat
Bright
Intermediate–bright
Bright
Variable
Acute infarct
Iso
Bright (hours–days)
Bright
Bright (cytotoxic edema)
White matter
Bright
Dark
Dark
Dark
Gray matter
Intermediate
Intermediate
Intermediate
Intermediate
Blood (subacute)
Bright (methemoglobin)
Bright
Bright
Variable
Calcium / cortical bone
Dark
Dark
Dark
Dark
Melanin / proteinaceous
Bright
Variable
Variable
Variable
T1 vs T2 Mnemonic
"Water is bright on T2, fat is bright on both." To identify a sequence at a glance: look at CSF. Dark CSF = T1. Bright CSF = T2. If CSF is dark but brain lesions are bright → FLAIR (fluid-attenuated inversion recovery).
A bright DWI lesion with a dark ADC map (true restricted diffusion) is pathognomonic for acute ischemic stroke within minutes to hours of onset. "T2 shine-through" (bright on both DWI and ADC) is not real restriction and should not be called stroke.
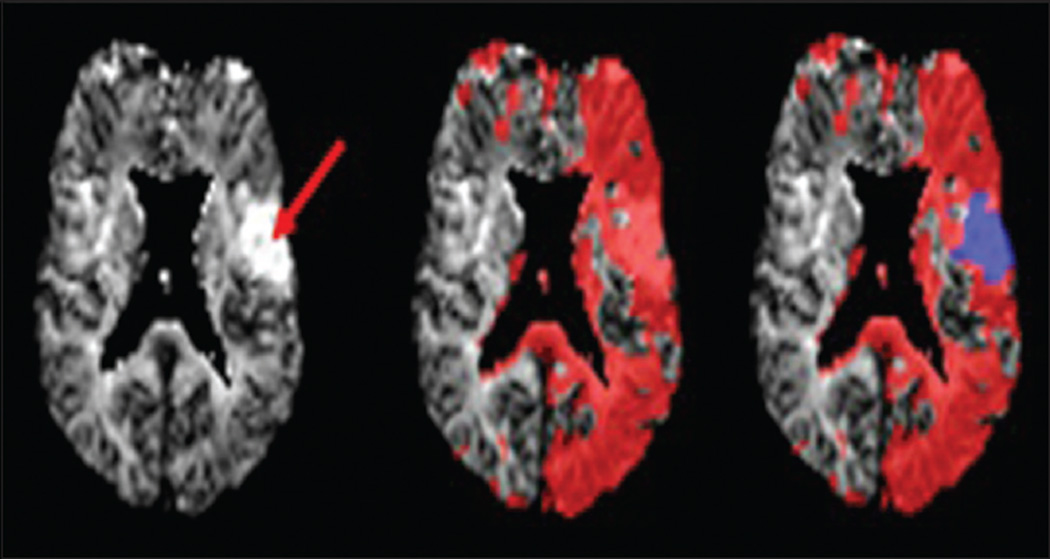
Figure 3 — Multimodal MRI in Acute Ischemic Stroke. DWI shows a bright area of restricted diffusion (acute infarct core), with corresponding dark signal on the ADC map confirming true restriction. MRA and perfusion maps demonstrate the vascular occlusion and the mismatch between infarct core and at-risk penumbra.
04 Ultrasound & Doppler Physics
Ultrasound uses high-frequency (2–18 MHz) sound waves emitted and received by a transducer. Sound reflects at acoustic impedance boundaries; the time delay is used to map depth, and echo amplitude determines pixel brightness. Higher frequencies give better resolution but less penetration; low-frequency probes (2–5 MHz) image deep structures (abdomen, OB), while high-frequency probes (7–15 MHz) image superficial structures (thyroid, vessels, MSK).
Echogenicity Lexicon
Term
Appearance
Examples
Anechoic
Black, no echoes
Simple cyst, bladder urine, ascites, bile
Hypoechoic
Darker than reference tissue
Hematoma, abscess, some tumors
Isoechoic
Same echogenicity as reference
Iso-to-liver renal lesion
Hyperechoic
Brighter than reference
Fat, gas, calcification, hemangioma
Echogenic with shadowing
Bright with posterior dark shadow
Gallstones, kidney stones, bone
Posterior acoustic enhancement
Bright behind fluid-filled structure
Simple cysts, bladder
Doppler Ultrasound
The Doppler effect measures frequency shifts from moving reflectors (red cells) to quantify flow. Color Doppler overlays flow direction on B-mode; pulsed Doppler measures velocity at a specific site. Used to evaluate vascular stenosis, DVT, arterial insufficiency, testicular torsion, and fetal wellbeing.
Ultrasound cannot see through bone or gas. Abdominal US is limited by bowel gas (why patients fast before gallbladder studies). The "acoustic window" is the reason liver, bladder, and gravid uterus are ideal because they transmit sound well.
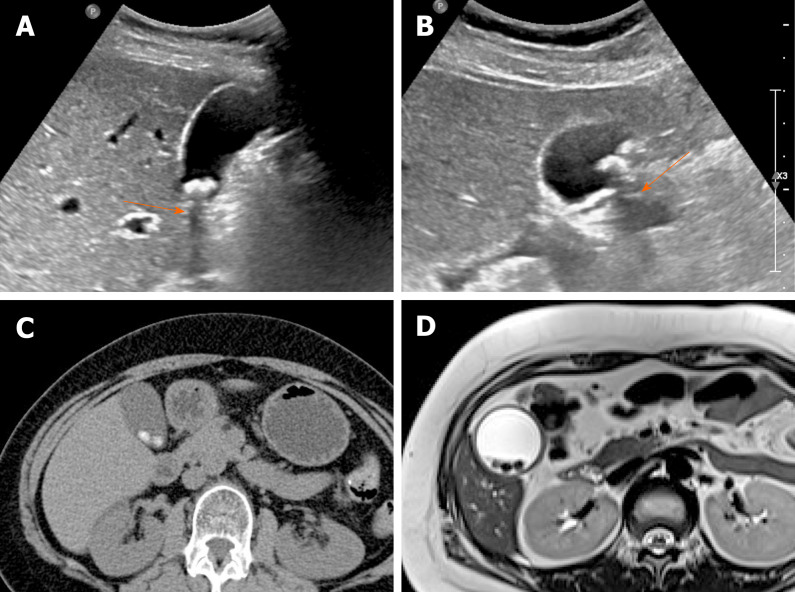
Figure 4 — Gallstones on Ultrasound with Acoustic Shadowing. Echogenic intraluminal foci within the gallbladder cast posterior acoustic shadows, the hallmark ultrasound sign of cholelithiasis. This demonstrates key sonographic principles: hyperechoic structures (bright) and shadowing artifacts that confirm the calcific nature of the lesion.
Ultrasound Artifacts with Diagnostic Value
Artifact
Appearance
Utility
Acoustic shadowing
Dark shadow posterior to reflector
Gallstones, kidney stones, calcifications, bone
Posterior enhancement
Bright area behind fluid
Confirms cystic nature of lesions
Comet tail
Reverberation echoes
Adenomyomatosis, crystals
Ring-down
Parallel echo reflections
Gas bubbles
Mirror image
Reflected duplicate structure
Above diaphragm (identifies liver border)
Twinkle artifact
Color Doppler flicker behind object
Urinary stones
05 Contrast Agents & Safety
Iodinated (CT) Contrast
Intravenous iodinated contrast opacifies vessels and enhancing tissues based on iodine's high atomic number. Modern low- or iso-osmolar non-ionic agents have substantially lower adverse event rates than older high-osmolar ionic agents. Contraindications and considerations:
Concern
Mechanism
Management
Contrast-induced nephropathy (CIN)
Direct tubular toxicity, renal vasoconstriction
Screen eGFR; hydrate if eGFR <30; hold metformin if risk of AKI
Anaphylactoid reaction
Non-IgE mediated (usually); prior reaction is biggest risk factor
Pre-medicate with steroids + diphenhydramine; have epinephrine ready
Shellfish / iodine "allergy"
Myth — no cross-reactivity
Treat as general contrast allergy risk; not a contraindication
Thyroid storm (hyperthyroid)
Iodine load precipitates storm in untreated Graves
Avoid in active hyperthyroidism; monitor if essential
Extravasation
Soft tissue injury at IV site
Elevation, warm compresses; surgical consult if compartment syndrome
Gadolinium (MRI) Contrast
Gadolinium chelates shorten T1 relaxation, producing bright enhancement on post-contrast T1 images. Gadolinium crosses disrupted blood–brain barriers, highlighting tumors, infection, and active demyelination. Key safety issue: nephrogenic systemic fibrosis (NSF) in patients with severe renal failure (eGFR <30); modern macrocyclic agents carry very low risk but caution persists. Gadolinium deposition in dentate nucleus and globus pallidus has been demonstrated but clinical significance is unclear.
Ultrasound Contrast
Microbubble agents (e.g., perflutren) enhance vascular and lesion characterization on ultrasound, with virtually no renal or thyroid toxicity. Used for liver lesion characterization, echocardiography, and vesicoureteral reflux studies.
Pre-Medication Protocol (Elective)
For patients with prior moderate/severe iodinated contrast reaction: Prednisone 50 mg PO at 13, 7, and 1 hour before scan plus diphenhydramine 50 mg PO/IV 1 hour before. Emergent alternative: hydrocortisone 200 mg IV plus diphenhydramine 50 mg IV immediately and every 4 hours until scan. Pre-medication does not eliminate but significantly reduces reaction risk.
Laryngeal edema, severe bronchospasm, shock, cardiac arrhythmias
Epinephrine (IM 0.3 mg), IV fluids, oxygen, airway support, code team
06 Radiation Safety & ALARA
ALARA (As Low As Reasonably Achievable) is the foundational principle of radiation safety. Every study should be justified (will it change management?), optimized (appropriate technique and dose), and limited (no repeats without cause). Pediatric patients are disproportionately sensitive to radiation and require weight-based dose reduction.
Effective Dose Reference
Study
Approx. Effective Dose (mSv)
Equivalent
Chest radiograph (PA + lateral)
0.1
10 days background
Mammogram
0.4
7 weeks background
Abdominal radiograph
0.7
4 months background
CT head
2
8 months background
CT chest
7
2 years background
CT abdomen / pelvis
10
3 years background
CT angiography (PE or coronary)
10–15
3–5 years background
PET/CT
14–25
5–8 years background
Fluoroscopic procedure (cath, TIPS)
5–20+
Highly variable
MRI Safety Zones
The strong static magnetic field is always on. Ferromagnetic objects become projectiles. Implanted devices must be screened: older pacemakers and ICDs are often unsafe (newer MR-conditional devices are acceptable with protocols); cochlear implants, aneurysm clips, metallic foreign bodies in the eye are contraindications unless proven MR-safe. Gadolinium and heat deposition from RF are additional considerations.
Always ask women of childbearing age about pregnancy before CT or fluoroscopy. For urgent imaging in pregnancy: ultrasound and MRI (without gadolinium if possible) are preferred. When CT is essential, shielding and dose optimization minimize fetal exposure; a single CT abdomen delivers ~25 mGy to the fetus, below the 100 mGy threshold of concern.
MRI Zones
Zone
Access
Notes
Zone I
Public access
Outside MR environment
Zone II
Supervised public
Screening and history occur here
Zone III
Restricted
MR-trained personnel only; no unscreened entry
Zone IV
Scanner room
Magnet is always on; only cleared patients and personnel
Gadolinium Classes
Class
Stability
NSF Risk
Macrocyclic (gadoteridol, gadobutrol, gadoterate)
Highest
Lowest
Linear ionic (gadobenate, gadoxetate)
Intermediate
Intermediate
Linear non-ionic (gadodiamide, gadoversetamide)
Lowest
Highest (largely withdrawn)
07 Systematic CXR Approach (A–E)
The chest radiograph is the most frequently ordered imaging study in medicine and the most diagnostically high-yield for the cost. Interpretation discipline is the difference between finding and missing pathology. Always use the same system every time. The classic mnemonic is ABCDEF or the traditional A–E approach.
Technical Assessment First
Element
Check For
Normal Finding
Projection
PA vs AP vs lateral
PA preferred (heart not magnified)
Rotation
Medial clavicle ends equidistant from spinous process
Right slightly higher than left; no subdiaphragmatic air
E — Everything else
Lung fields, pleura, mediastinum, hila, corners
Symmetry, opacities, lines/tubes, review hidden areas
Hidden Areas — Don't Miss Zones
Always explicitly check: apices (Pancoast tumor, small pneumothorax), behind the heart (retrocardiac pneumonia, hiatal hernia), costophrenic angles (small effusion blunting), below the diaphragm (free air), and bones (clavicle, rib, humerus fractures). Systematic review of these zones catches findings obscured by overlapping structures.
The silhouette sign: loss of a normal interface between two structures of different densities indicates adjacent pathology. Loss of the right heart border = right middle lobe; loss of the left heart border = lingula; loss of the diaphragm = lower lobe. This lets you localize pneumonia on a single frontal view.
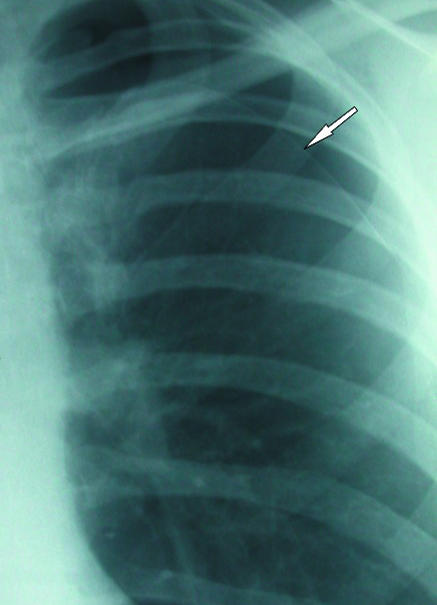
Figure 5 — Pneumothorax on Chest Radiograph. The visceral pleural line is visible as a thin white line with absent lung markings peripheral to it. Systematic CXR review using the A-to-E approach ensures hidden areas such as the apices (where small pneumothoraces may first appear) are never overlooked.
08 Pulmonary Parenchymal Patterns
Lung opacities are categorized by distribution (focal vs diffuse), anatomic pattern (airspace vs interstitial vs nodular), and location. Recognizing patterns narrows the differential efficiently.
Airspace vs Interstitial Disease
Pattern
Findings
Differential
Airspace / consolidation
Fluffy opacities, air bronchograms, segmental/lobar
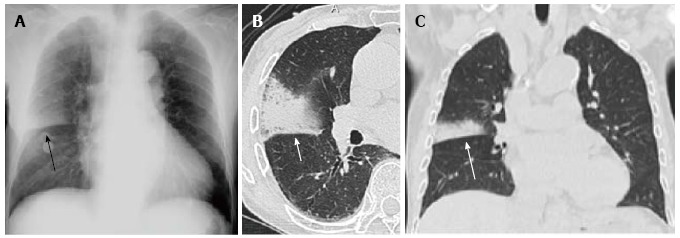
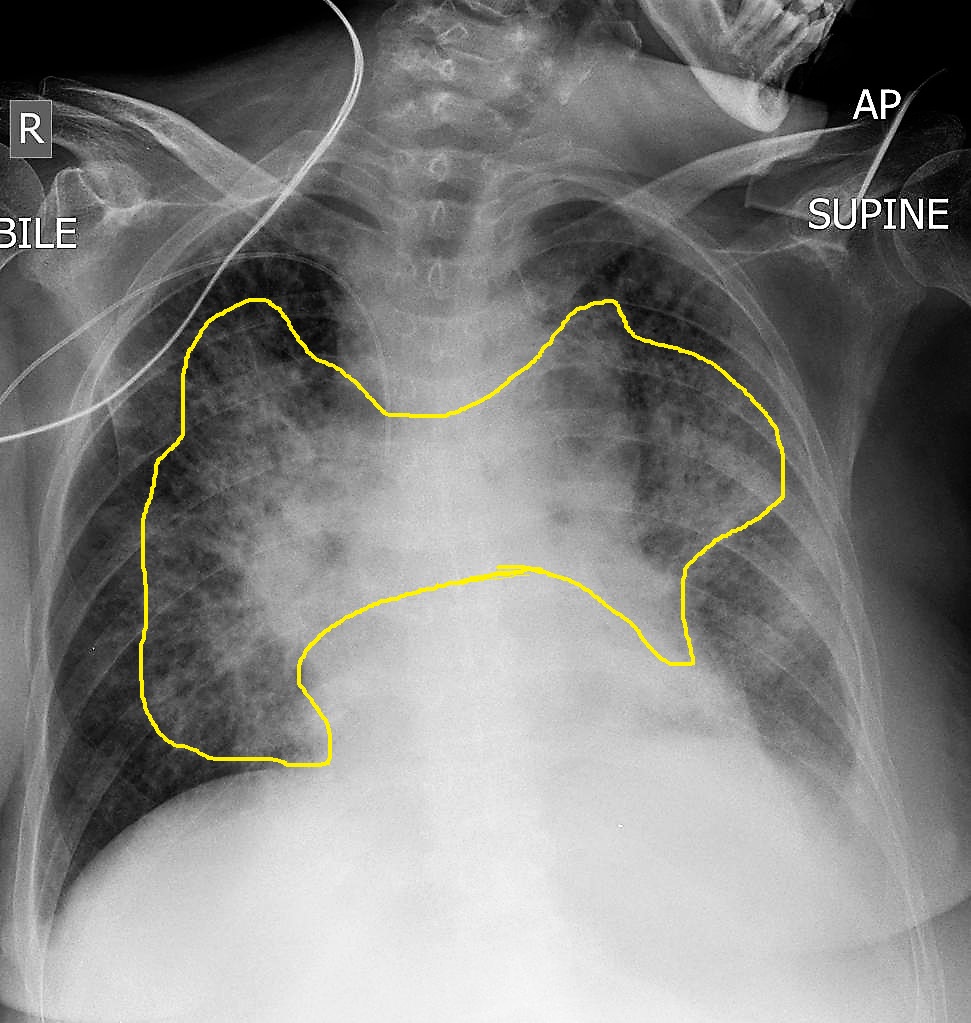
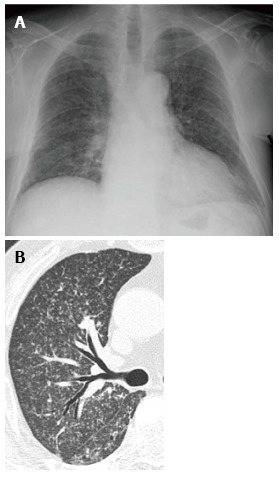
Figure 6 — Lobar Pneumonia (Streptococcus pneumoniae). Dense homogeneous consolidation within a lobe with air bronchograms, the classic airspace pattern. The opacity respects fissural boundaries, and the silhouette sign helps localize the involved lobe on a frontal radiograph.Figure 7 — Cardiogenic Pulmonary Edema — Bat-Wing Pattern. Bilateral symmetric perihilar airspace opacities creating the classic bat-wing or butterfly pattern. Associated findings include cardiomegaly, cephalization of vessels, Kerley B lines, and bilateral pleural effusions.Figure 8 — Miliary Tuberculosis. Innumerable 1-3 mm nodules diffusely distributed throughout both lung fields in a random pattern. This reticulonodular pattern results from hematogenous dissemination and is distinguished from other patterns by the uniform tiny nodule size and diffuse distribution.
Cephalization (upper-lobe vascular redistribution) is the earliest sign of pulmonary venous hypertension on an upright CXR. It precedes Kerley lines and overt alveolar edema and often correlates with a PCWP of 12–18 mmHg.
Atelectasis Subtypes
Type
Mechanism
Example
Obstructive (resorptive)
Airway blockage; distal alveoli resorb gas
Mucus plug, endobronchial tumor, foreign body
Compressive
External compression on lung
Pleural effusion, pneumothorax, mass
Passive / relaxation
Loss of apposition to chest wall
Pneumothorax recoil
Cicatrizing
Fibrosis pulling lung in
TB, radiation, chronic fibrosis
Adhesive
Surfactant deficiency
ARDS, neonatal RDS, PE
Subsegmental (linear)
Hypoventilation
Post-operative, splinting from pain
09 Pleura, Mediastinum & Cardiac Silhouette
Pleural Disease
Finding
Appearance
Clinical
Pleural effusion (small)
Blunting of costophrenic angle, meniscus sign (>200 mL)
CHF, pneumonia, malignancy
Large effusion
Opacification, mediastinal shift away, layered fluid on decubitus
Parapneumonic, empyema, hemothorax
Pneumothorax
Visceral pleural line, absent lung markings peripheral to it
The mediastinum is divided into anterior, middle, and posterior compartments, each with characteristic pathology. Widened mediastinum (>8 cm on supine AP) in trauma raises concern for aortic injury. Hilar enlargement is caused by vessels, lymphadenopathy, or masses.
On PA film, the cardiothoracic ratio (max cardiac width / max thoracic width) should be <0.5. AP films magnify the heart and inflate the ratio (do not call cardiomegaly on AP). Chamber enlargement clues: left atrial enlargement → splayed carina (>90°), double density behind right heart border, posterior displacement on lateral. Left ventricular enlargement → rounded, laterally displaced apex. Right heart enlargement → uplifted apex, filling of retrosternal space on lateral.
Figure 9 — Klebsiella Pneumonia with Bulging Fissure Sign. Dense lobar consolidation with a characteristic bulging or bowed fissure, caused by the voluminous inflammatory exudate expanding the lobe. This sign, along with air bronchograms, is classically associated with Klebsiella but can occur with any necrotizing pneumonia.
Don't call cardiomegaly on a supine AP film. AP magnification and lack of inspiration enlarge the cardiac silhouette. If the patient is stable, order a PA film before committing to the diagnosis.
Cardiac Chamber Enlargement Signs
Chamber
PA Film
Lateral Film
Left atrium
Splayed carina (>90°), double density behind right heart, straightened left heart border
Posterior displacement of esophagus with barium
Left ventricle
Rounded, laterally and inferiorly displaced apex
Posterior extension past IVC line
Right atrium
Prominence of right heart border
Difficult to assess
Right ventricle
Uplifted apex ("boot" shape)
Filling of retrosternal clear space
10 Lines, Tubes & Common Disease Patterns
Every post-procedural or ICU chest radiograph must confirm correct positioning of lines and tubes and screen for complications (pneumothorax, malposition, hemorrhage).
Line and Tube Positioning
Device
Correct Position
Complications to Assess
Endotracheal tube
Tip 3–5 cm above carina (T2–T4 level)
Right mainstem intubation, extubation, esophageal
Central venous catheter
Tip at cavoatrial junction (just above right atrium)
Pneumothorax, arterial puncture, malposition
PICC line
Tip in lower SVC / cavoatrial junction
Malposition (azygos, IJ, subclavian)
Swan-Ganz catheter
Tip in right or left pulmonary artery (not peripheral)
PA rupture, knotting
Nasogastric tube
Tip below diaphragm in stomach, side port below GE junction
Pulmonary malposition (tube in bronchus/lung)
Chest tube
Along pleural space; all side holes inside thorax
Last side hole outside chest (not draining)
Pacemaker leads
RV apex ± RA appendage ± coronary sinus (CRT)
Lead fracture, dislodgment, perforation
Line Position Disaster
A central line that appears to travel laterally (outside expected SVC course) or curves back on itself may be in a branch vessel or arterial. Do not infuse vesicants or TPN until position is confirmed. The most dangerous malposition is right atrial (perforation risk) or contralateral brachiocephalic vein.
Post-Operative Chest
Post-cardiac surgery films should be scrutinized for: sternal wires (complete, fractured, migration), mediastinal widening (bleeding, hematoma), pneumothorax, pleural effusion, atelectasis (especially left lower lobe), pericardial effusion, and position of chest tubes and lines. A rapidly increasing mediastinal contour after cardiac surgery suggests acute hemorrhage requiring urgent re-exploration.
A pulmonary nodule is a rounded opacity ≤3 cm surrounded by lung; larger lesions are masses. Solitary pulmonary nodules are common incidental findings. Characterization relies on size, margin, density, growth, and patient risk factors.
Benign vs Malignant Features
Feature
Benign
Malignant
Size
<6 mm
>8–10 mm
Margin
Smooth, well-defined
Spiculated, lobulated
Calcification
Central, laminated, popcorn (hamartoma), diffuse
Eccentric, stippled, or none
Growth (doubling time)
<20 days (infection) or >400 days (benign)
30–400 days
Density
Solid with fat (hamartoma)
Part-solid / ground-glass (adenocarcinoma)
Associated
None
Lymphadenopathy, effusion, bone lesions
Fleischner Society Guidelines (2017)
Nodule Type
Low-Risk Patient
High-Risk Patient
Solid, <6 mm, single
No routine follow-up
Optional CT at 12 months
Solid, 6–8 mm, single
CT at 6–12 months
CT at 6–12 months, then 18–24 months
Solid, >8 mm
CT at 3 months, PET/CT, or biopsy
CT at 3 months, PET/CT, or biopsy
Subsolid ground-glass <6 mm
No routine follow-up
Optional CT at 2–4 years
Subsolid ground-glass ≥6 mm
CT at 6–12 months, then every 2 years through 5 years
Same
Part-solid ≥6 mm
CT at 3–6 months; if unchanged and solid <6 mm, annual ×5
Same — biopsy if solid >6 mm
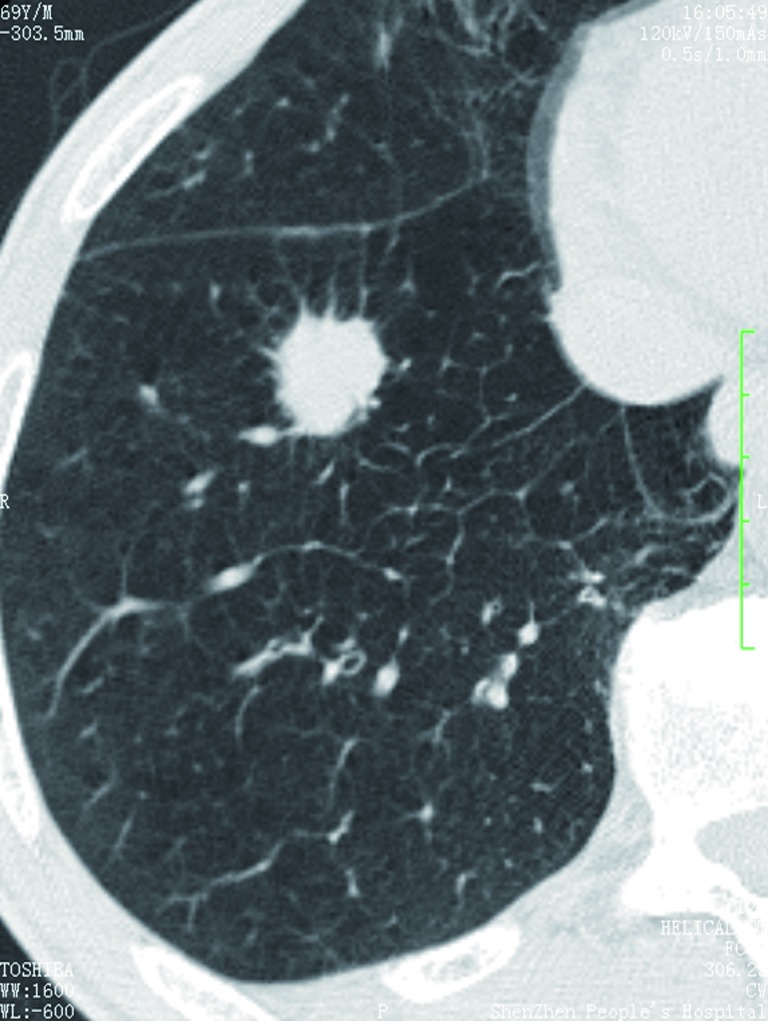
Figure 10 — Spiculated Solitary Pulmonary Nodule on CT. A pulmonary adenocarcinoma presenting as a solitary pulmonary nodule with spiculated margins on axial CT. Spiculation is the most concerning morphologic feature for malignancy and warrants further evaluation with PET/CT or tissue sampling regardless of size.
Fleischner criteria apply only to incidental nodules in adults ≥35, not to screening or cancer staging. A nodule in an active cancer patient is treated as metastatic until proven otherwise. Fleischner is for true incidentalomas.
Nodule Calcification Patterns
Pattern
Appearance
Implication
Central / bull's eye
Dense central nidus
Benign (granuloma)
Laminated / concentric
Onion-skin rings
Benign (healed granuloma)
Diffuse / solid
Entirely calcified
Benign (old granuloma)
Popcorn
Clumped chondroid
Benign (hamartoma)
Eccentric / stippled
Irregular, off-center
Indeterminate / possibly malignant
12 PE CTA & Interstitial Lung Disease
CT Pulmonary Angiography for PE
CT pulmonary angiography (CTPA) is the gold standard for diagnosing acute pulmonary embolism. Intravenous iodinated contrast is timed to peak pulmonary artery opacification. A positive study shows a filling defect (low-attenuation area) within a contrast-filled vessel, which may be occlusive or non-occlusive, central or peripheral.
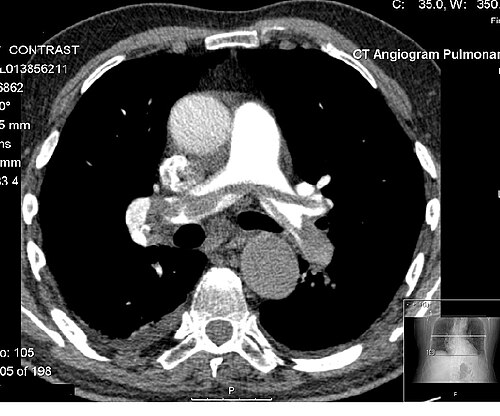
Figure 11 — Saddle Pulmonary Embolism on CTPA. A large filling defect straddles the bifurcation of the main pulmonary arteries, representing a saddle embolus with significant clot burden. This finding often correlates with right ventricular strain and warrants urgent evaluation for thrombolysis or thrombectomy.
Finding
Significance
Saddle embolus
Clot straddling the bifurcation of main pulmonary arteries — large clot burden
RV dilation (RV:LV >0.9)
RV strain, worse prognosis, consider thrombolysis
Septal bowing
Interventricular septum pushed into LV — severe RV failure
CTD-associated (scleroderma), hypersensitivity, drug
Hypersensitivity pneumonitis
Upper-lobe ground-glass, centrilobular nodules, mosaic air trapping
Bird fancier, farmer's lung
Sarcoidosis
Perilymphatic nodules, upper-lobe, hilar/mediastinal adenopathy, fibrosis in end-stage
Granulomatous disease
Organizing pneumonia (COP)
Peripheral, subpleural, or peribronchial consolidation; reverse halo
Cryptogenic, post-infectious, drug
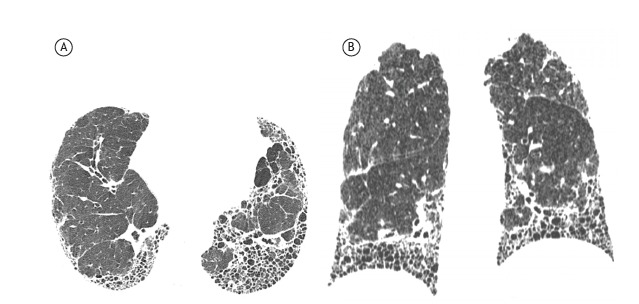
Figure 12 — Usual Interstitial Pneumonia (UIP) Pattern on HRCT. Axial and coronal high-resolution CT images demonstrating peripheral, basilar-predominant reticular opacities, traction bronchiectasis, and extensive honeycombing (clustered cystic airspaces with well-defined walls). This pattern is the hallmark of idiopathic pulmonary fibrosis.Figure 13 — Organizing Pneumonia on CT. Peripheral and subpleural consolidation, a pattern that may mimic pneumonia on imaging. The reverse halo (atoll) sign, when present, is highly suggestive. Organizing pneumonia can be cryptogenic or secondary to infection, drugs, or connective tissue disease.
Emphysema Subtypes on CT
Centrilobular (upper-lobe predominant) — smoking; small central lucencies within secondary pulmonary lobules. Panlobular (lower-lobe) — α1-antitrypsin deficiency. Paraseptal (subpleural) — risk factor for spontaneous pneumothorax in young adults. Pattern recognition on HRCT drives the diagnostic pathway.
Low-dose CT (LDCT) is the only validated lung cancer screening test. USPSTF recommends annual LDCT for adults 50–80 with ≥20 pack-year history and current smoking or quit within 15 years. Lung-RADS is the reporting system for screening LDCT.
Bronchiectasis Features
Finding
Description
Signet ring sign
Bronchus larger than adjacent pulmonary artery
Lack of tapering
Bronchi remain same caliber toward periphery
Tram tracks
Parallel thick-walled airways on radiograph
Mucus plugging
Impacted airways (finger-in-glove)
Causes include post-infectious (classic), cystic fibrosis (upper lobe), ABPA (central, finger-in-glove mucus), primary ciliary dyskinesia (with situs inversus in Kartagener), and immunodeficiency. HRCT pattern (upper vs lower, central vs peripheral) narrows etiology.
13 Abdominal Radiograph & KUB
The abdominal radiograph is a low-cost screening tool with limited sensitivity but high specificity for certain findings. The acute abdominal series includes supine abdomen, upright abdomen, and upright chest (for free air). A KUB (kidneys, ureters, bladder) is a supine film used primarily to track stones, catheters, and stents.
Key Abdominal X-Ray Findings
Finding
Appearance
Diagnosis
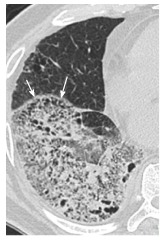
Small bowel obstruction
Dilated small bowel (>3 cm), air–fluid levels at different heights, "string of pearls," valvulae conniventes across lumen
"Coffee bean" sign, inverted U arising from pelvis
Sigmoid volvulus (elderly, bedbound)
Cecal volvulus
Dilated cecum in LUQ, "coffee bean" pointing toward LUQ
Cecal volvulus (younger adults)
Free intraperitoneal air
Subdiaphragmatic lucency on upright CXR, Rigler sign (air on both sides of bowel wall), football sign (supine)
Perforated viscus
Toxic megacolon
Colonic dilation >6 cm, loss of haustra, thumbprinting
C. difficile, IBD, ischemic colitis
Pneumatosis intestinalis
Linear air within bowel wall
Ischemia (adults), NEC (neonates)
Abdominal calcifications
Rim (AAA), multiple (gallstones, phleboliths), branching (staghorn calculus)
Varies by location
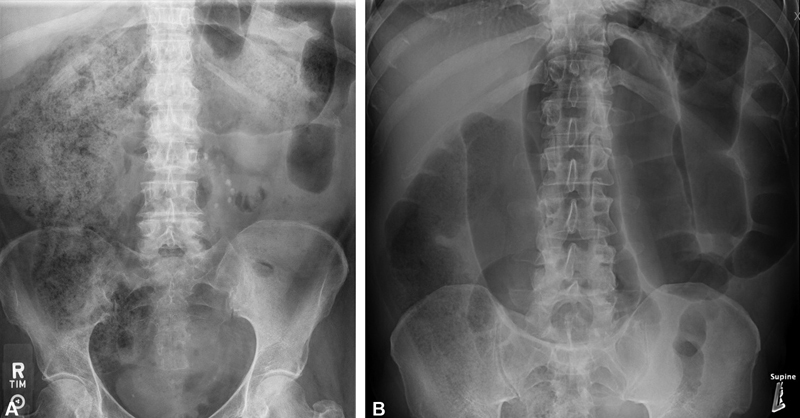
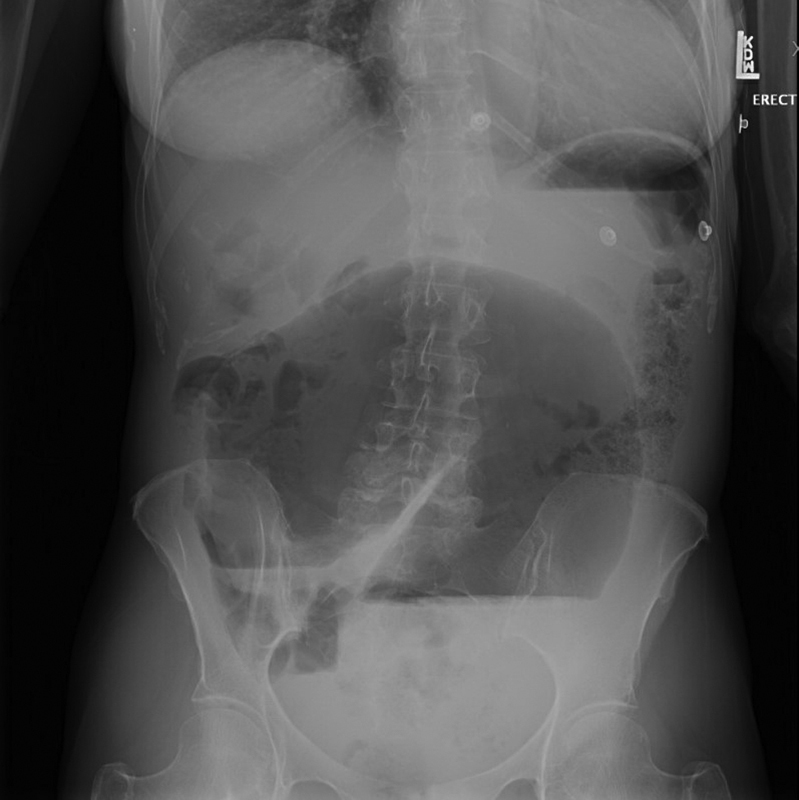
Figure 14 — Small Bowel Obstruction on Abdominal Radiograph. Dilated small bowel loops (>3 cm) with valvulae conniventes visible across the full diameter of the lumen. The differential air-fluid levels on upright films and the "string of pearls" sign confirm the diagnosis of mechanical obstruction.Figure 15 — Large Bowel Obstruction on Abdominal Radiograph. Marked colonic dilation with haustral markings that extend only partway across the lumen (unlike valvulae conniventes of small bowel). Cecal diameter >9 cm raises concern for impending perforation and requires urgent decompression.
Free air under the diaphragm on an upright CXR is the most sensitive plain-film sign of perforation (detects as little as 1–2 mL). If the patient cannot stand, order a left lateral decubitus abdominal film — free air rises over the liver. Always include a CXR in the acute abdominal series.
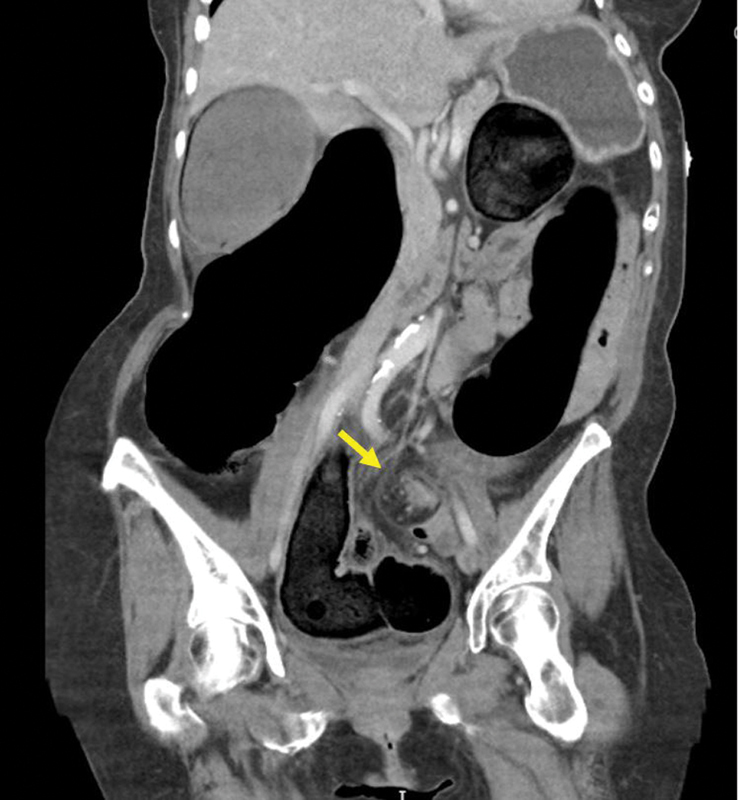
Figure 16 — Cecal Volvulus on Abdominal Radiograph. A markedly dilated cecum displaced from its normal position, forming a C-shaped or coffee-bean configuration pointing toward the left upper quadrant. Cecal volvulus typically affects younger patients compared to sigmoid volvulus and often requires surgical intervention.Figure 17 — Sigmoid Volvulus — Whirl Sign on CT. Coronal CT demonstrating the whirl sign, created by twisting of the mesentery and bowel around the vascular pedicle. The sigmoid colon is markedly dilated and rotated, producing the classic coffee-bean appearance. CT confirms the diagnosis and identifies complications such as ischemia.
Classic Abdominal Radiograph Signs
Sign
Description
Diagnosis
Rigler sign
Air outlining both sides of bowel wall
Pneumoperitoneum
Football sign
Air outlining falciform ligament on supine film
Large pneumoperitoneum
Coffee bean sign
Dilated bowel loop appearing as coffee bean
Sigmoid or cecal volvulus
Target / bull's eye
Concentric rings in RLQ
Intussusception
Double bubble
Two air-filled bubbles (stomach + duodenum)
Duodenal atresia (neonate)
String of pearls
Small gas bubbles between valvulae conniventes
Small bowel obstruction
Thumbprinting
Bowel wall thickening imprints
Ischemic or infectious colitis
Ground-glass abdomen
Diffuse opacification
Massive ascites
14 Abdominal CT — Acute Abdomen
CT with IV contrast is the workhorse for evaluating adult abdominal pain. Oral contrast is used selectively (less often now with modern multidetector scanners). Non-contrast CT is reserved for renal stones and patients who cannot receive iodinated contrast.
Common Acute Findings
Diagnosis
CT Findings
Acute appendicitis
Appendiceal dilation >6 mm, wall thickening, periappendiceal fat stranding, appendicolith, abscess if perforated
Diverticulitis
Sigmoid diverticula with wall thickening and pericolonic fat stranding; complications: abscess, fistula, perforation
Acute pancreatitis
Pancreatic enlargement, peripancreatic stranding/fluid; necrosis = non-enhancing pancreas; pseudocyst late
Figure 18 — Acute Appendicitis on CT. A dilated, thick-walled appendix (>6 mm) with periappendiceal fat stranding and mucosal hyperenhancement, the classic CT triad of acute appendicitis. Identification of an appendicolith or abscess indicates perforation and alters surgical timing.
CT Contrast Phases
Phase
Timing after Injection
Primary Use
Non-contrast
Before contrast
Stones, calcifications, baseline HU
Arterial
25–35 seconds
Vascular (dissection, active bleed), HCC detection
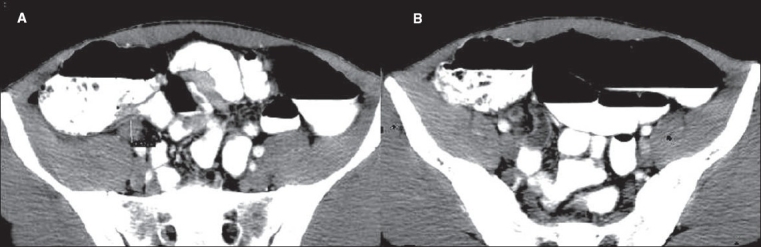
Used for suspected hepatocellular carcinoma: HCC shows arterial enhancement followed by washout on portal venous/delayed images, with a pseudocapsule. This pattern (LI-RADS 5) is diagnostic without biopsy in cirrhotic patients. Hemangiomas show peripheral nodular enhancement with centripetal fill-in; metastases typically remain hypovascular.
15 Abdominal Ultrasound & FAST
Right Upper Quadrant Ultrasound
The first-line test for suspected biliary disease, liver lesions, and unexplained RUQ pain. Patients fast 8 hours to distend the gallbladder.
Finding
Appearance
Clinical
Cholelithiasis
Echogenic, shadowing, mobile intraluminal focus
Gallstones
Acute cholecystitis
Wall >3 mm, pericholecystic fluid, sonographic Murphy sign, stones
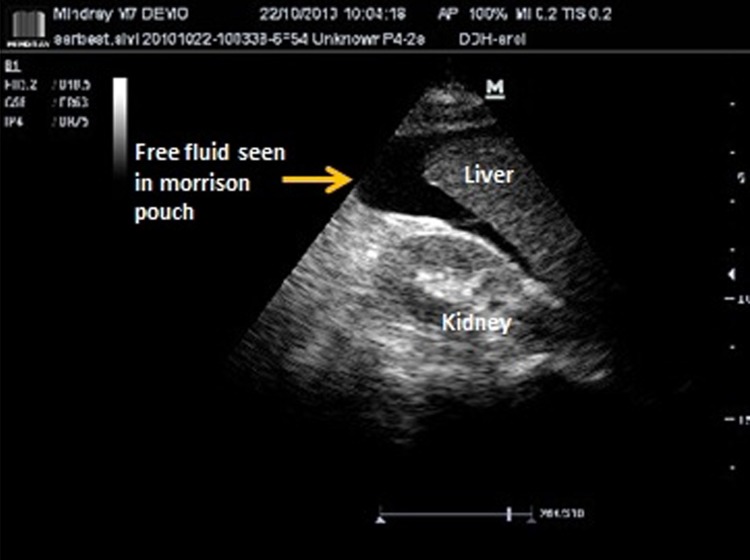
Figure 19 — Positive FAST Exam — Free Fluid in Morison Pouch. Anechoic free fluid collection (blood) in the hepatorenal recess (Morison pouch) and around the liver, the most sensitive FAST view for detecting hemoperitoneum. In an unstable trauma patient, a positive FAST mandates immediate operative intervention.
FAST Exam (Focused Assessment with Sonography for Trauma)
Rapid bedside ultrasound in blunt abdominal trauma to detect free intraperitoneal fluid. Four views:
View
Looks For
Perihepatic (Morison pouch)
Fluid between liver and right kidney (most sensitive)
Perisplenic
Fluid in splenorenal recess, subphrenic
Pelvic (rectovesical / pouch of Douglas)
Fluid in most dependent pelvic space
Subxiphoid / pericardial
Pericardial effusion, tamponade
The eFAST (extended FAST) adds bilateral thoracic views for pneumothorax (absent lung sliding, lung point) and hemothorax.
FAST has high specificity (>95%) but moderate sensitivity (~80%) for free fluid. A negative FAST does not exclude injury in a stable patient — consider CT. In an unstable patient with positive FAST, proceed directly to the OR; CT wastes critical time.
Point-of-Care Ultrasound (POCUS)
Exam
Application
Key Finding
Cardiac (echo)
Pericardial effusion, global LV function, RV strain
Tamponade, hypokinesis, dilated RV in PE
Lung
Pneumothorax, pulmonary edema, consolidation
Absent lung sliding, B-lines, hepatization
IVC
Volume status
Collapsibility index >50% suggests low CVP
Aorta
AAA screening
Diameter ≥3 cm
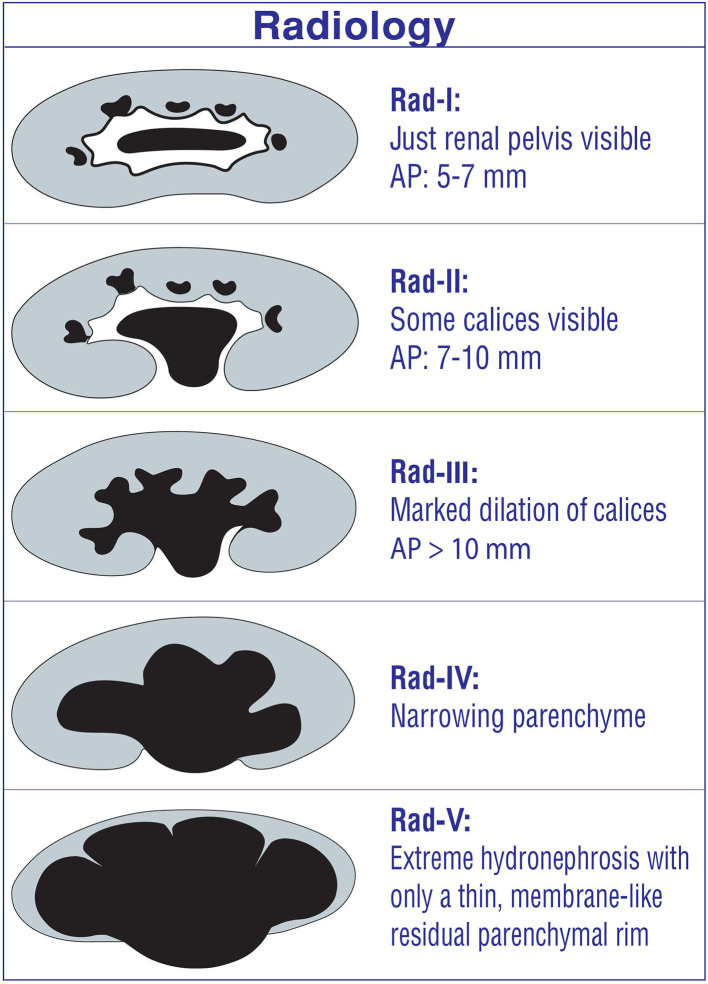
Renal
Hydronephrosis screening
Dilated pelvis and calyces
Procedural guidance
Central line, thoracentesis, paracentesis
Real-time needle visualization, safer access
16 Hepatobiliary MRI & MRCP
MRI is superior to CT for lesion characterization in the liver and biliary tree. Liver MRI uses T1, T2, in-phase/out-of-phase, DWI, and dynamic post-contrast sequences. Hepatobiliary agents (gadoxetate) provide additional delayed hepatocyte uptake information for focal lesion characterization.
Heavily T2-weighted sequence where static fluid (bile, pancreatic juice) is markedly bright while background tissue is suppressed. Non-invasive alternative to ERCP for evaluating biliary anatomy. Detects choledocholithiasis, strictures, biliary tree variants, pancreas divisum, chronic pancreatitis, and PSC (beaded bile ducts).
Liver Lesion
MRI Characteristics
Simple cyst
T1 dark, T2 very bright, no enhancement
Hemangioma
T2 very bright, peripheral nodular discontinuous enhancement with centripetal fill-in
FNH (focal nodular hyperplasia)
Iso-intense, arterial enhancement, central scar bright on T2, retains gadoxetate
Adenoma
Fat/hemorrhage on T1, variable enhancement, drops out on delayed hepatobiliary phase
T2 moderate bright, hypovascular rim enhancement (most), restricted diffusion
On in-phase / out-of-phase MRI, hepatic steatosis causes signal drop on out-of-phase images (fat and water cancel in the same voxel). This is the most sensitive imaging test for fatty liver disease and quantifies steatosis non-invasively.
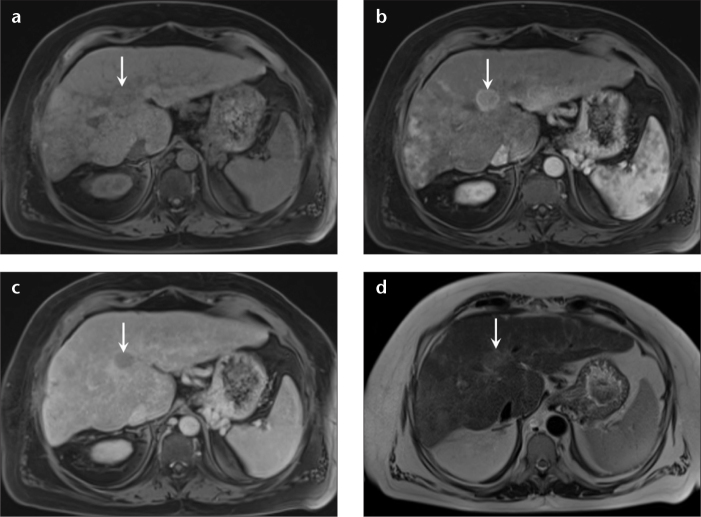
Figure 20 — Hepatocellular Carcinoma on Dynamic Contrast MRI. A liver lesion demonstrating arterial phase hyperenhancement (bright in arterial phase) followed by washout (hypointense relative to background liver on portal venous/delayed phase). This enhancement pattern with pseudocapsule is diagnostic for HCC (LI-RADS 5) in a cirrhotic liver without biopsy.
LI-RADS Major Features (HCC)
Feature
Definition
Arterial phase hyperenhancement
Unequivocally brighter than background liver in arterial phase
Non-peripheral washout
Reduced enhancement below background in portal venous or delayed phase
Enhancing capsule
Peripheral rim of enhancement in portal venous or delayed phase
Threshold growth
≥50% size increase in ≤6 months
Size
Diameter of observation
Applied only in patients with cirrhosis or chronic HBV. LR-5 lesions (definite HCC) can be diagnosed and treated without biopsy in the appropriate clinical setting.
17 Renal & Urinary Tract Imaging
Modality Selection
Indication
First-Line Modality
Suspected renal stone
Non-contrast CT (stone protocol)
Hematuria workup
CT urography (multiphase)
Hydronephrosis screening
Ultrasound
Renal mass characterization
Multiphase CT or MRI (Bosniak)
Renal artery stenosis
Doppler US, MRA, CTA
Bladder / urothelial cancer
CT urography, cystoscopy
Pyelonephritis complicated
Contrast CT
Bosniak Classification of Renal Cysts
Category
Features
Malignancy Risk
Management
I
Simple cyst, thin wall, no septa, no enhancement
~0%
No follow-up
II
Few thin septa, fine calcification
~0%
No follow-up
IIF
Multiple thin septa or minimal wall thickening
~5%
Follow with imaging
III
Thickened or nodular walls/septa with measurable enhancement
~50%
Surgery or biopsy
IV
Enhancing soft tissue components adjacent to cyst
~90%
Surgery
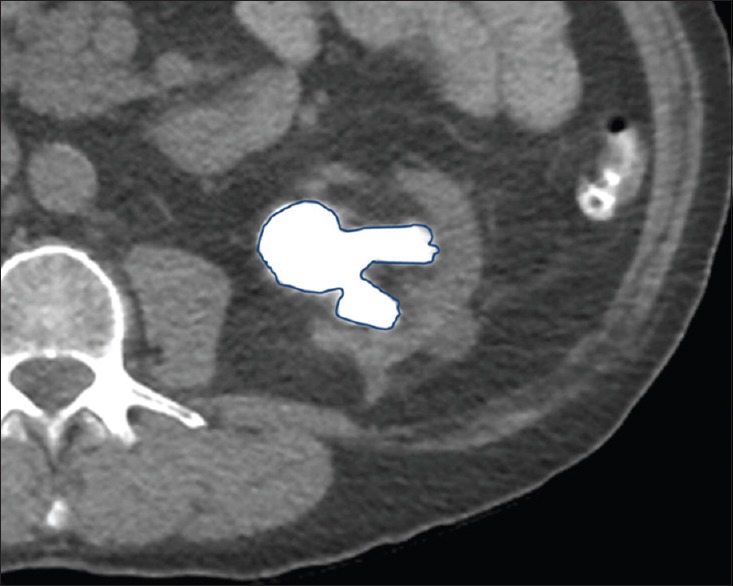
Figure 21 — Renal Stone on Non-Contrast CT. Axial non-contrast CT demonstrating a hyperdense renal calculus. Non-contrast CT has near 100% sensitivity for urinary stones regardless of composition and is the gold standard for evaluating suspected renal colic, also revealing secondary signs such as hydronephrosis and perinephric stranding.Figure 22 — Hydronephrosis Grading on Ultrasound. Progressive grades of hydronephrosis from mild renal pelvic dilation to severe calyceal dilation with parenchymal thinning. Ultrasound is the first-line screening modality for hydronephrosis, detecting the dilated collecting system as anechoic fluid-filled spaces within the renal sinus.
Renal Stone Imaging
Non-contrast CT has near 100% sensitivity for urinary stones regardless of composition (uric acid stones are radiolucent on plain film but visible on CT). Stones <5 mm typically pass spontaneously; stones 5–10 mm may require intervention; >10 mm usually require procedural removal. Key CT findings: hyperdense calculus, hydroureter, perinephric stranding (indicating obstruction), and the "tissue rim" sign distinguishing ureteral stone from phlebolith.
A ureteral stone at the ureterovesical junction can mimic a phlebolith. The "tissue rim sign" (soft-tissue edema surrounding the stone) and associated hydroureter distinguish stone from phlebolith on non-contrast CT.
Adrenal Incidentaloma Evaluation
Characteristic
Benign (Adenoma)
Concerning
Non-contrast HU
<10 HU (lipid-rich)
>10 HU
Absolute washout
>60% at 15 min
<60%
Relative washout
>40%
<40%
Size
<4 cm
≥4 cm — surgical consideration
Borders
Smooth, homogeneous
Irregular, heterogeneous
Growth on interval imaging
Stable
>1 cm/year
All adrenal incidentalomas need biochemical workup for hormonal excess (pheochromocytoma, Cushing syndrome, hyperaldosteronism) regardless of imaging features. Imaging alone does not exclude functional tumors.
18 Pelvic, Obstetric & Prostate Imaging
Pelvic Ultrasound
Transabdominal provides a global view (requires full bladder as acoustic window); transvaginal gives superior resolution of uterus, endometrium, ovaries, and adnexa. First-line for suspected ovarian pathology, pelvic pain, abnormal bleeding, and early pregnancy.
Finding
Features
Simple ovarian cyst
Anechoic, thin wall, posterior enhancement, <5 cm benign
Hemorrhagic cyst
Complex internal echoes, fishnet/reticular pattern, resolves over weeks
Endometrioma
Homogeneous low-level echoes ("ground glass")
Dermoid / mature teratoma
Hyperechoic with acoustic shadowing (fat, calcium, hair)
Extra-uterine gestational sac, adnexal ring of fire, empty uterus with positive β-hCG, free fluid
Uterine fibroid
Hypoechoic, well-defined, may shadow
Endometrial thickening
Postmenopausal >4 mm requires biopsy
Obstetric Ultrasound
Gestational Age
Expected Findings
5 weeks
Gestational sac (intrauterine)
6 weeks
Yolk sac, fetal pole, cardiac activity
8–12 weeks
Nuchal translucency screening
18–22 weeks
Anatomy scan, placental location, amniotic fluid
28–40 weeks
Growth, biophysical profile, presentation
Prostate MRI & PI-RADS
Multiparametric prostate MRI (T2, DWI, dynamic contrast enhancement) is used for detection, localization, staging, and post-treatment surveillance of prostate cancer. PI-RADS v2.1 assigns a 1–5 score indicating probability of clinically significant cancer: 1–2 (benign), 3 (equivocal), 4–5 (likely/highly likely clinically significant cancer → targeted biopsy).
Discriminator Zone Rules
Peripheral zone: DWI is dominant (cancer restricts diffusion against bright T2 background). Transition zone: T2 is dominant (cancer is homogeneous low T2 against heterogeneous benign prostatic hyperplasia). This zonal approach is core to PI-RADS scoring.
Testicular Ultrasound
Finding
Features
Clinical
Testicular torsion
Asymmetric decreased/absent intratesticular flow on Doppler; edema in late phase
Surgical emergency — 6 hour window
Epididymitis
Enlarged epididymis with hyperemia
Medical management (antibiotics)
Hydrocele
Anechoic fluid surrounding testicle
Common, usually benign
Varicocele
Dilated pampiniform plexus, "bag of worms," flow on Valsalva
Left >> right; right-sided new = r/o retroperitoneal mass
Testicular tumor
Intratesticular hypoechoic mass with flow
Seminoma, non-seminomatous germ cell tumors
Epididymal cyst / spermatocele
Anechoic lesion in epididymal head
Benign
19 Fracture Description & Principles
Every fracture description must be systematic and precise to communicate with the orthopedic surgeon. The components are: bone, location, pattern, displacement, angulation, rotation, and associated findings.
Children's bones deform before they break. Torus (buckle) and greenstick fractures are unique to pediatric immature bone. Physeal injuries may be radiographically occult; compare to the contralateral side when uncertain, and recognize that tenderness over the physis in a child is a fracture until proven otherwise.
Figure 23 — Distal Radius Fracture (Colles Type) on Radiograph. PA and lateral views showing a distal radius fracture with dorsal angulation. On the lateral view, dorsal displacement creates the classic "dinner fork" deformity. Systematic fracture description includes bone, location, pattern, displacement, angulation, and associated ulnar styloid injury.
20 Regional Fractures & Dislocations
Common Fractures by Region
Region
Fracture / Injury
Key Feature
Wrist
Colles (distal radius, dorsal angulation)
"Dinner fork" deformity, FOOSH in elderly
Wrist
Smith fracture
Distal radius with volar angulation (reverse Colles)
Wrist
Scaphoid fracture
Snuffbox tenderness, AVN risk — may be occult; repeat in 10–14 days or MRI
Hand
Boxer fracture
5th metacarpal neck, angulation after punch
Forearm
Monteggia
Proximal ulna fracture with radial head dislocation
Forearm
Galeazzi
Distal radius fracture with DRUJ dislocation
Elbow
Supracondylar humerus (pediatric)
Posterior fat pad (sail sign) = occult fracture
Shoulder
Anterior dislocation
Humeral head anteroinferior, Hill-Sachs / Bankart lesions
Shoulder
Posterior dislocation
"Lightbulb" sign on AP; seizure, electrocution
Hip
Femoral neck fracture
Shortened, externally rotated; AVN risk high
Hip
Intertrochanteric
Extracapsular; better blood supply, less AVN
Knee
Tibial plateau fracture
Lipohemarthrosis on cross-table lateral
Ankle
Weber / Lauge-Hansen classification
Location of fibular fracture relative to syndesmosis
Ankle
Maisonneuve
Proximal fibula fracture with syndesmotic injury (check knee to ankle)
Foot
Jones fracture
5th metatarsal base; poor healing
Foot
Lisfranc injury
Tarsometatarsal malalignment; subtle but devastating
Spine
Compression fracture
Vertebral height loss, wedge shape (osteoporosis)
Spine
Jefferson fracture
C1 burst fracture (axial load)
Spine
Hangman fracture
C2 pars interarticularis, hyperextension
Spine
Odontoid (dens) fracture
Type II at base is unstable; common in elderly falls
Spine
Chance fracture
Flexion-distraction, seat belt mechanism
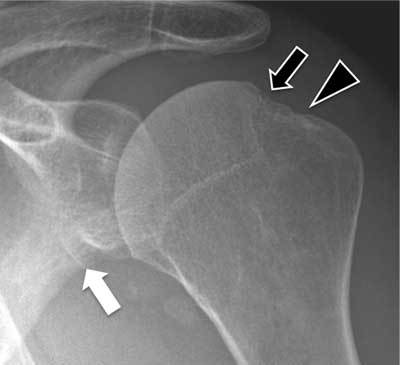
Figure 24 — Anterior Shoulder Dislocation with Associated Bony Injuries. Imaging demonstrating Hill-Sachs lesion (posterolateral humeral head impaction fracture) and Bankart lesion (anteroinferior glenoid rim fracture), the two classic osseous injuries associated with anterior glenohumeral dislocation. Always obtain post-reduction films to confirm relocation and identify associated fractures.
Occult Fracture Clues
A normal-looking radiograph with clinical suspicion still warrants concern: fat pad sign at the elbow (occult radial head or supracondylar), lipohemarthrosis at the knee (intra-articular fracture), scaphoid tenderness (occult scaphoid), pubic ramus fracture (look for contralateral posterior ring injury). Get MRI or CT when suspicion is high.
Joint Dislocation Essentials
Joint
Direction & Mechanism
Associated Injury
Glenohumeral
Anterior (95%) — abduction + external rotation
Hill-Sachs, Bankart, axillary nerve
Glenohumeral
Posterior — seizure, electrocution
Reverse Hill-Sachs, "lightbulb" sign
Elbow
Posterior — FOOSH
Coronoid, radial head fractures
Hip
Posterior (90%) — dashboard injury
Sciatic nerve, acetabular fracture, AVN
Hip
Anterior (10%) — forced abduction
Femoral artery / nerve
Knee
Any direction — high-energy
Popliteal artery injury — surgical emergency
Patella
Lateral (most common)
Medial retinaculum tear
Ankle
Usually associated with fracture
Syndesmotic injury, tibiotalar ligaments
A posterior knee dislocation is a vascular emergency. Up to 40% have popliteal artery injury. Even if pulses are present, perform an ABI and consider CTA, because intimal injuries may evolve over hours to days into thrombosis.
21 Arthritis, Bone Tumors & MSK MRI
Arthritis Radiographic Features
Feature
Osteoarthritis
Rheumatoid Arthritis
Distribution
DIP, PIP, 1st CMC, weight-bearing joints
MCP, PIP, wrists, symmetric
Joint space
Asymmetric narrowing
Symmetric narrowing
Osteophytes
Prominent
Absent
Erosions
Absent
Marginal erosions
Cysts
Subchondral cysts
Periarticular cysts
Density
Subchondral sclerosis
Periarticular osteopenia
Soft tissue
Normal
Fusiform soft tissue swelling
Other Arthropathies
Gout: punched-out erosions with overhanging edges, tophi, preserved joint space until late. Psoriatic arthritis: "pencil-in-cup" deformity, DIP involvement, periostitis, sausage digit. Ankylosing spondylitis: sacroiliitis, bamboo spine, syndesmophytes. CPPD / pseudogout: chondrocalcinosis of menisci, triangular fibrocartilage, pubic symphysis.
Bone Lesion Characterization
Feature
Benign
Malignant
Margin
Narrow zone of transition, sclerotic rim
Wide zone of transition, permeative
Periosteal reaction
Solid, thick
Sunburst, onion-skinned, Codman triangle
Matrix
Variable
Osteoid or chondroid matrix
Soft tissue mass
Absent
Present
MSK MRI Key Indications
Study
Key Findings
Knee MRI
ACL tear (empty lateral notch, increased T2 signal), meniscal tear (linear increased signal reaching articular surface), bone contusions, collateral ligaments
Spinal cord compression is a neurosurgical emergency. Any patient with severe back pain plus neurologic deficit or new urinary retention needs emergent MRI of the entire spine (not just one level) to identify all sites of compression before initiating treatment.
Non-contrast CT head is the first-line imaging in acute neurologic presentations: trauma, stroke, altered mental status, severe headache. It is fast, widely available, and exquisitely sensitive for acute blood (hyperdense on CT).
Intracranial Hemorrhage Subtypes
Type
Location
Shape
Cause
Key Features
Epidural hematoma
Between skull and dura
Biconvex "lens"
Arterial (middle meningeal), trauma
Does not cross sutures; lucid interval; surgical emergency
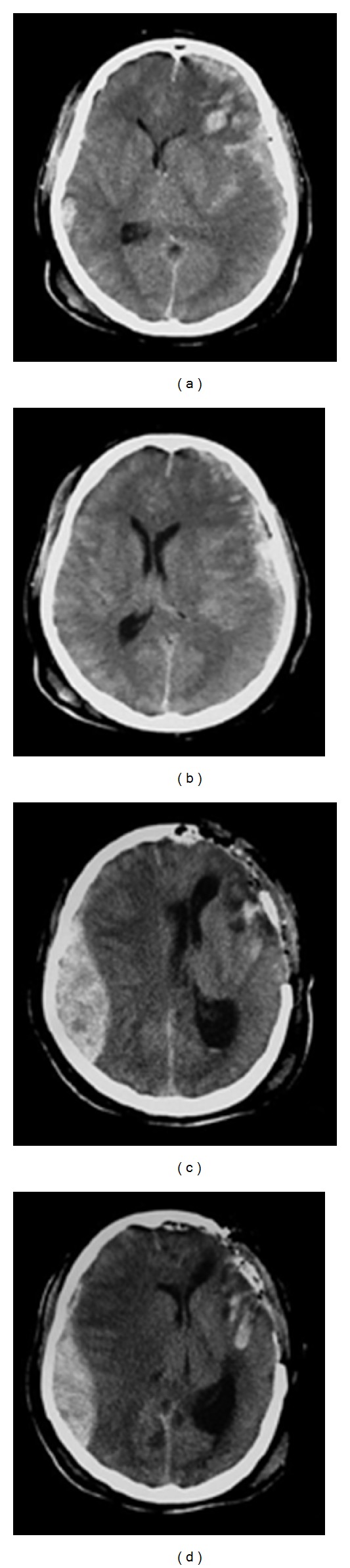
Figure 25 — Epidural Hematoma on Non-Contrast CT. Sequential CT scans showing a biconvex (lens-shaped) hyperdense collection in the epidural space. Epidural hematomas do not cross suture lines, are typically arterial (middle meningeal artery), and may present with a lucid interval before rapid deterioration requiring emergent surgical evacuation.Figure 26 — Acute Subdural Hematoma with Mass Effect. A crescentic hyperdense subdural collection conforming to the brain surface, crossing suture lines but not the midline. Note the significant mass effect with midline shift and compression of the ipsilateral lateral ventricle. The crescentic shape distinguishes subdural from the biconvex epidural hematoma.
Blood Density Over Time (CT)
Age
Appearance
Hyperacute (<6 h)
Hyperdense (50–80 HU)
Subacute (days to weeks)
Isodense to brain (easy to miss)
Chronic (weeks+)
Hypodense, approaching CSF density
Mass Effect Signs
Sulcal effacement, ventricular compression, midline shift (measure at septum pellucidum), subfalcine herniation (cingulate under falx), uncal herniation (medial temporal lobe over tentorium), tonsillar herniation (cerebellar tonsils through foramen magnum). Measure midline shift at the septum pellucidum relative to a line drawn between the anterior and posterior attachments of the falx.
Traumatic Brain Injury Patterns
Pattern
Mechanism
Imaging
Contusion
Coup / contrecoup against skull
Hemorrhagic focus at frontal / anterior temporal lobes
Diffuse axonal injury (DAI)
Rotational / deceleration shear
Small hemorrhages at gray-white junction, corpus callosum, brainstem; best on SWI/GRE
Cerebral edema
Secondary injury
Loss of gray-white differentiation, sulcal effacement, tight basal cisterns
Skull fracture
Direct impact
Lucent line on CT; look for depressed fragments and air
Basilar skull fracture
Severe head trauma
Air in sinuses or temporal bone, battle sign, raccoon eyes, CSF rhinorrhea
23 Ischemic Stroke Imaging
Stroke imaging has three goals: (1) exclude hemorrhage (non-contrast CT), (2) identify large vessel occlusion amenable to thrombectomy (CTA), (3) quantify salvageable penumbra (CT perfusion or MRI).
Early CT Signs of Ischemic Stroke
Sign
Finding
Timing
Hyperdense MCA sign
Bright M1 segment (acute thrombus)
Immediate
Loss of insular ribbon
Loss of gray-white differentiation at insula
First hours
Loss of basal ganglia definition
Obscuration of lentiform nucleus
First hours
Sulcal effacement
Cortical swelling obliterating sulci
First hours
Parenchymal hypodensity
Frank low attenuation in vascular territory
6–24 h
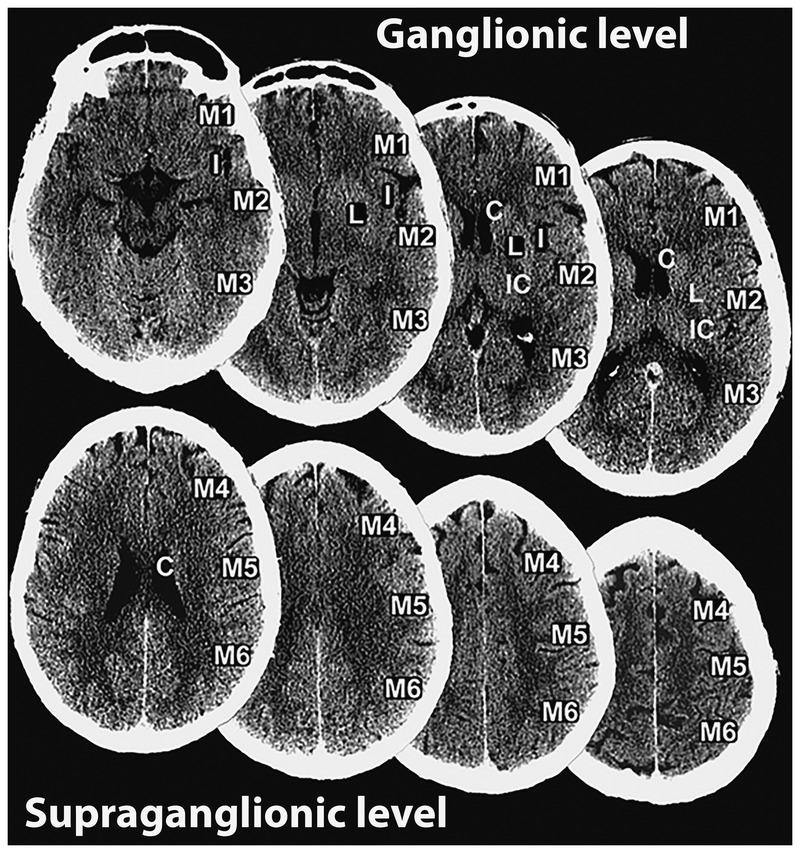
Figure 27 — ASPECTS Scoring Regions. The Alberta Stroke Program Early CT Score divides the MCA territory into 10 regions across two axial CT levels. Each region with early ischemic change (loss of gray-white differentiation, sulcal effacement, or frank hypodensity) subtracts one point from the perfect score of 10. ASPECTS ≤7 correlates with worse outcomes.
ASPECTS Score
Alberta Stroke Program Early CT Score evaluates 10 MCA territory regions; start at 10 and subtract 1 for each region with early ischemic change. ASPECTS ≤7 correlates with worse outcomes and greater hemorrhagic transformation risk with thrombolytics; ASPECTS ≥6 is commonly used as threshold for thrombectomy eligibility.
CTA & CT Perfusion
CTA identifies large vessel occlusions (ICA, M1, basilar) that are targets for mechanical thrombectomy. CT perfusion differentiates core infarct (non-salvageable) from ischemic penumbra (salvageable): core shows decreased CBV and CBF with increased MTT; penumbra shows preserved CBV but increased MTT. The mismatch (penumbra − core) represents tissue at risk that could be saved by reperfusion.
Figure 28 — CT Perfusion in Acute Ischemic Stroke. CT perfusion maps differentiating irreversible infarct core (decreased cerebral blood volume) from salvageable ischemic penumbra (preserved CBV but prolonged mean transit time). The mismatch between core and penumbra identifies tissue that may benefit from reperfusion therapy, guiding thrombolysis and thrombectomy decisions.
MRI for Stroke
DWI is the most sensitive imaging for acute ischemic stroke, detecting changes within minutes. Restricted diffusion (bright DWI, dark ADC) is seen within 30 minutes and persists for 7–10 days. DWI/FLAIR mismatch (bright DWI, still-normal FLAIR) suggests stroke onset <4.5 hours and is used to guide thrombolysis in wake-up strokes.
In a patient with suspected stroke, order non-contrast CT + CTA head and neck as a single protocol. This rules out hemorrhage, identifies LVO for thrombectomy, and assesses the neck vessels for a source — in one trip to the scanner.
Pseudoaneurysm at ligamentum arteriosum (isthmus), mediastinal hematoma
Figure 30 — Aortic Dissection on CT Angiography. CTA demonstrating an intimal flap separating the true and false lumens of the aorta. Stanford Type A dissection involves the ascending aorta and is a surgical emergency due to risk of pericardial rupture, coronary involvement, and aortic insufficiency.
Peripheral Vascular Imaging
Study
Use
Notes
Carotid duplex ultrasound
Carotid stenosis screening
Peak systolic velocity correlates with stenosis; confirm significant disease with CTA/MRA
Venous compression ultrasound
DVT diagnosis
Non-compressibility of vein = DVT (most sensitive finding)
CTA chest (PE)
Pulmonary embolism
First-line when D-dimer positive or high pre-test probability
CTA abdomen/pelvis runoff
Peripheral arterial disease, mesenteric ischemia
Alternative to angiography
MRA
Vessels without iodinated contrast
Renal artery, intracranial, aortic
Dissection Classification
Stanford A involves the ascending aorta — regardless of where the tear started — and is a surgical emergency due to risk of rupture into the pericardium, coronary involvement, and aortic insufficiency. Stanford B involves only the descending aorta; initial management is medical (strict BP and HR control) with endovascular repair for complications or progression.
Figure 31 — DVT on Compression Ultrasound. A non-compressible popliteal vein containing echogenic thrombus, the primary diagnostic criterion for acute deep vein thrombosis. Normal veins collapse completely under gentle transducer pressure; failure to compress is diagnostic with >95% sensitivity and >98% specificity for proximal DVT.
DVT Ultrasound Technique
Compression ultrasound assesses proximal veins (common femoral, femoral, popliteal) with sequential compression. Normal veins collapse completely under gentle pressure; the presence of non-compressible material within the vein is diagnostic of thrombus. Augmentation and color Doppler add flow information for partial or non-occlusive thrombus. Calf veins are less commonly evaluated but become important in recurrent symptoms. A negative proximal US with positive D-dimer may require serial imaging or whole-leg evaluation.
If bowel perforation is suspected, use water-soluble contrast (Gastrografin) rather than barium. Barium extravasation into the peritoneum causes severe chemical peritonitis and fibrosis. Water-soluble contrast is safely resorbed if it leaks.
PET/CT Interpretation
18F-FDG PET measures glucose metabolism. Cancer cells typically show increased uptake; SUVmax is the standardized uptake value. An SUVmax >2.5 in a pulmonary nodule is suspicious for malignancy. PET is integrated with CT anatomy (PET/CT) or MRI (PET/MRI) for localization. Key uses: lung cancer staging, lymphoma response assessment, head and neck cancer, colorectal recurrence, melanoma, and fever of unknown origin.
False Positive on FDG-PET
False Negative on FDG-PET
Infection / inflammation (TB, sarcoid)
Low-grade indolent tumors
Brown fat (neck, supraclavicular)
Mucinous carcinoma
Muscle activity
Bronchoalveolar carcinoma
Post-surgical change
Small lesions (<1 cm) — resolution limit
Radiation-induced pneumonitis
Hyperglycemia (reduces tumor avidity)
V/Q Scan Interpretation (PIOPED)
A ventilation/perfusion scan compares regional ventilation (inhaled Xe-133 or Tc-DTPA aerosol) to perfusion (IV Tc-MAA). A segmental perfusion defect with normal ventilation ("mismatch") in a vascular distribution is consistent with PE. Reported as normal, very low, low, intermediate, or high probability. Useful when iodinated contrast is contraindicated (renal failure, severe allergy) or in pregnancy (lower fetal dose than CTPA).
27 Modality Selection & Appropriateness
The ACR Appropriateness Criteria are evidence-based guidelines matching clinical scenarios to the most appropriate imaging studies. The goal is to minimize radiation, contrast, cost, and wasted time while maximizing diagnostic yield.
First-Line Modality by Presentation
Clinical Scenario
First-Line Imaging
Acute chest pain, r/o MI
CXR; consider coronary CTA or stress test
Acute chest pain, r/o PE
CTA chest (PE protocol)
Acute chest pain, r/o dissection
CTA chest/abdomen/pelvis
Suspected pneumonia
CXR PA and lateral
Adult RLQ pain (appendicitis)
CT abdomen/pelvis with contrast
Pediatric RLQ pain
Ultrasound; MRI if inconclusive
Pregnant RLQ pain
Ultrasound; MRI if inconclusive
RUQ pain (gallbladder)
Ultrasound
Flank pain (renal colic)
Non-contrast CT (stone protocol)
Suspected AAA
Ultrasound (screening); CTA (definitive)
Acute stroke
Non-contrast CT + CTA head/neck ± CT perfusion
Severe headache / SAH
Non-contrast CT; LP if negative; CTA if positive
First seizure
MRI brain (non-urgent); CT if acute
Trauma blunt abdominal, stable
CT abdomen/pelvis with contrast
Trauma blunt abdominal, unstable
FAST at bedside
Back pain with red flags
MRI spine
Suspected DVT
Venous compression US
Acute scrotum
Testicular ultrasound with Doppler
First-trimester bleeding
Transvaginal ultrasound + β-hCG
Suspected cholangitis
Ultrasound; MRCP or ERCP
Breast lump
Diagnostic mammogram + US
When NOT to Image
Scenario
Why Not
Uncomplicated low back pain <6 weeks
Imaging does not change management in absence of red flags
Simple syncope with normal exam
Head CT has very low yield
Uncomplicated headache with normal exam
Neuroimaging not indicated
Acute sinusitis
Clinical diagnosis
Rib contusion without red flags
Imaging rarely changes management
Red Flags for Back Pain Imaging
Image immediately for: saddle anesthesia, urinary retention, fecal incontinence, progressive neurologic deficit, history of cancer, fever with back pain, IV drug use, significant trauma, or unexplained weight loss. Absent red flags, 6 weeks of conservative management is appropriate before imaging.
Trauma Imaging Protocols
Trauma Scenario
Study
Blunt polytrauma ("pan-scan")
CT head, C-spine, chest/abdomen/pelvis with contrast
Penetrating torso
CT chest/abdomen/pelvis with IV ± triple contrast
Blunt head
Non-contrast CT head; CTA if high-risk mechanism or fracture at skull base
Blunt neck (C-spine clearance)
CT cervical spine; MRI if neurologic deficit or ligamentous concern
Pelvic trauma
CT pelvis with contrast; angiography for active extravasation
Extremity trauma
Plain radiographs; CT or MRI for complex fractures or occult injury
Pediatric Considerations
Children have higher radiosensitivity and longer lifetime to develop radiation-induced cancer. Always ask: (1) Can we use ultrasound or MRI instead? (2) Can we use reduced dose protocols? (3) Can we limit scan coverage? Image Gently and Image Wisely are national campaigns emphasizing these principles. In children with suspected appendicitis, ultrasound is first-line; MRI is a good alternative when US is non-diagnostic, avoiding CT radiation entirely.
28 High-Yield Pearls & Report Terminology
Common Radiology Report Terms
Term
Meaning
Consolidation
Airspace filling with fluid/cells/material, air bronchograms visible
Ground-glass opacity
Hazy increased density without obscuring vessels (CT term)
Reticular
Linear network pattern, suggests interstitial disease
Tree-in-bud
Small airway impaction, infection or aspiration
Honeycombing
Clustered cystic spaces, end-stage fibrosis
Mosaic attenuation
Heterogeneous lung density, air trapping or small-vessel disease
Fat stranding
Increased density of fat, indicates inflammation
Free fluid
Non-loculated fluid in peritoneum, pelvis, pleural space
Rim enhancement
Peripheral enhancement of a lesion with non-enhancing center (abscess, necrotic tumor)
Washout
Lesion hyperenhances early then becomes hypointense relative to background (HCC)
Restricted diffusion
Bright DWI + dark ADC (acute stroke, abscess, cellular tumor)
T2 shine-through
Bright on DWI from long T2, not true restriction
Mass effect
Compression / displacement of adjacent structures
Nondisplaced
Fracture with fragments in anatomic alignment
Clinical correlation recommended
Finding is non-specific; caller should integrate with clinical picture
High-Yield Modality Pairings
Scenario
Best Modality
Why
Acute stroke <6 h
CT + CTA, then MRI DWI
Rule out bleed, identify LVO, confirm infarct
Biliary colic
Ultrasound
Sensitive for stones, no radiation
Flank pain, hematuria
Non-contrast CT stone protocol
>99% stone detection
Small bowel obstruction
CT with contrast
Transition point, grade, ischemia
Occult scaphoid
MRI
Most sensitive for radiographically occult fracture
Rotator cuff tear
MRI or ultrasound
Tear size, retraction, muscle atrophy
First seizure workup
MRI brain
Structural lesions not seen on CT
Rapid-Fire Clinical Pearls
When ordering emergency CT for suspected PE, always check renal function and the D-dimer in low pre-test probability patients. A negative D-dimer in a low/moderate probability patient can avoid CT entirely. The PERC rule further identifies patients who need no testing at all.
The "reverse halo" or atoll sign (central ground-glass surrounded by denser consolidation) is classically associated with organizing pneumonia but also occurs in invasive fungal infection, sarcoidosis, and pulmonary infarct. Pattern recognition narrows but rarely finalizes the diagnosis — integrate with clinical context.
Imaging does not replace the physical exam. A tender abdomen with peritoneal signs mandates surgical evaluation regardless of negative imaging; a normal CT with equivocal exam still warrants observation. The patient in front of you — not the image — drives the decision.
Every CXR should be compared to the patient's prior film when available. A new finding is alarming; an old unchanged finding is reassuring. Always ask for priors before finalizing your read.
Structured reporting improves clarity, reduces missed findings, and supports downstream data mining. Reporting templates for stroke, PE, prostate MRI, liver lesions, and lung cancer screening are standard of care and should be used when available.
Air bronchograms mean the airways are patent and the surrounding lung is airless (filled with fluid, pus, blood, or cells). This is why pneumonia and pulmonary edema show air bronchograms but endobronchial obstructions do not.
Acute blood on CT is bright (50–80 HU) because of the iron in hemoglobin. On MRI, acute blood is complex: hyperacute is T1 iso and T2 bright (oxyhemoglobin); acute is T1 iso and T2 dark (deoxyhemoglobin); early subacute is T1 bright and T2 dark; late subacute is T1 and T2 bright; chronic is T1 and T2 dark (hemosiderin rim).
MRI is contraindicated with old pacemakers, cochlear implants, metallic foreign bodies in the eye, and some aneurysm clips. Always screen rigorously before sending a patient to the scanner — the magnet is always on, and accidents are catastrophic.
For suspected cord compression, order MRI of the entire spine (cervical, thoracic, lumbar) not just the suspected level. Metastatic disease frequently has multiple sites of involvement, and missing one level changes surgical planning and radiation fields.
In pregnancy, ultrasound and MRI (without gadolinium) are preferred. When CT or nuclear medicine is essential for maternal health, do not withhold it — a missed PE or appendicitis is far more dangerous than the radiation dose of a single study. Shield the abdomen and minimize dose when possible.
A negative FAST in a stable trauma patient does NOT exclude intra-abdominal injury. FAST is a decision tool for the unstable patient: if positive, go to the OR; if negative but unstable, keep looking. The stable patient should still receive CT when indicated.
Contrast extravasation at the IV site usually resolves with conservative care (elevation, warm compresses). Large volumes (>100 mL) or signs of compartment syndrome require surgical consultation. Document the event, reassure the patient, and update the allergy list if indicated.
"Incidentaloma" is not a diagnosis. Every incidental finding has a management algorithm — adrenal nodules (non-contrast HU <10 = adenoma), thyroid nodules (TI-RADS), liver lesions (size and density), and lung nodules (Fleischner). Know the major frameworks.
Communicate critical findings directly. If the radiology report mentions a new pneumothorax, mass, hemorrhage, or cord compression, the radiologist must call a clinician and document the conversation. As the receiving clinician, acknowledge the call, document your acknowledgment, and act on the finding without delay.
Always include the clinical question and relevant history on the imaging requisition. A radiologist reading "abdominal pain" vs "68 y/o with sudden-onset LLQ pain, fever, WBC 16" will produce very different levels of scrutiny. Good communication improves the read.
The biggest source of diagnostic error in radiology is not missing a finding — it's misinterpreting a finding that was seen. Protect against this by always describing what you see (objective) before concluding what it means (subjective). If an objective finding does not fit the conclusion, re-examine the conclusion.
Interpretation Strategy
For every study: (1) Confirm identity, indication, and technique. (2) Use a systematic approach (ABC, A–E, or region-by-region). (3) Describe each finding objectively (size, location, characteristics). (4) Compare to priors. (5) Generate a differential based on pattern. (6) Communicate the clinical impact. (7) Recommend next steps when appropriate. These seven steps apply to every modality and every anatomic region — master them and you will read imaging confidently across the full breadth of clinical medicine.