Medical Documentation
SOAP notes, H&P, progress notes, discharge summaries, procedure notes, consult notes, telephone encounters, billing/coding fundamentals, ICD-10, CPT, E/M coding, electronic health records, and every documentation standard for accurate, compliant, and clinically useful medical writing.
01 Purposes & Significance of Documentation
Medical documentation is the permanent written record of a patient encounter — what was said, seen, thought, and done. It is simultaneously a clinical communication tool, a medicolegal record, a billing instrument, a quality measurement substrate, and a research dataset. A well-crafted note transmits the clinician's reasoning to every future provider; a poor note obscures the patient's story and exposes the clinician to liability, denied claims, and patient harm. The adage "if it wasn't documented, it wasn't done" is both a medicolegal principle and a reminder that the note is the only permanent artifact of the encounter.
Documentation is where medicine meets law, finance, and quality. The same note is read by the next shift's physician, the insurer's claims auditor, the malpractice attorney, the quality reviewer, and potentially the patient. Writing for all of these audiences simultaneously — while still being clinically useful — is a core physician skill that is rarely formally taught but ubiquitously required.
The Five Purposes of the Medical Record
| Purpose | Description | Primary Audience |
|---|---|---|
| Clinical Communication | Transfer of information between providers across time and shifts | Physicians, nurses, consultants, future self |
| Legal Record | Evidence of care provided, standard of care met, informed consent | Attorneys, courts, licensing boards |
| Billing & Reimbursement | Justification for services rendered; supports CPT/ICD-10 coding | Payers, coders, auditors |
| Quality & Performance | Data for quality metrics, HEDIS, MIPS, and institutional benchmarks | Regulators, hospital administration |
| Research & Public Health | Source data for registries, epidemiology, and clinical research | Researchers, public health agencies |
Who Reads the Note?
A single outpatient note may be read, within weeks of its creation, by the patient (through the patient portal, now mandatory under the 21st Century Cures Act information-blocking rule), the patient's family, the covering physician at 2 AM, a specialist at another institution, a prior-authorization reviewer, a coding auditor, a medical student, and potentially an attorney. Each audience weighs different elements — but clarity, accuracy, and organization serve them all.
Historical Context
Medical record-keeping dates to Hippocrates, but the modern problem-oriented medical record (POMR) was introduced by Lawrence Weed in 1968, giving rise to the SOAP format. The transition from paper to electronic health records (EHRs) accelerated dramatically after the 2009 HITECH Act, which incentivized adoption of "meaningful use" certified EHRs. By 2023, over 96% of U.S. hospitals used a certified EHR — a transformation that solved legibility and access problems while introducing new ones: copy-forward errors, note bloat, and clinician burnout.
02 Core Principles: Accuracy, Timeliness & Legibility
Five principles govern every clinical note regardless of setting, specialty, or format: accuracy, completeness, timeliness, legibility, and objectivity. Violations of any of these principles can render an otherwise thorough note clinically useless or medicolegally indefensible.
The Five Principles
| Principle | Standard | Common Violation |
|---|---|---|
| Accuracy | Every statement must be factually true and verifiable | Copying a prior exam that was not actually performed |
| Completeness | All relevant findings (positive and negative) are documented | Omitting pertinent negatives that drive the differential |
| Timeliness | Notes completed contemporaneously with the encounter (typically within 24–48 hours) | Back-dating or batch-writing notes days later |
| Legibility | Readable by any provider; standardized abbreviations only | Handwritten scrawl; non-standard acronyms |
| Objectivity | Observed facts distinguished from inferences; neutral language | Editorializing about patient behavior or character |
A concise, accurate two-paragraph note beats a four-page template-generated note full of unverified copy-forwarded data. Auditors and attorneys scrutinize volume for inconsistencies; the more you write, the more you can be cross-examined on.
Timeliness Standards
The Joint Commission requires that history and physical examinations be completed and documented within 24 hours of admission (and no more than 30 days prior for elective procedures). Operative reports should be dictated immediately after surgery. Discharge summaries should be completed within 24–48 hours of discharge. CMS considers notes written more than 48 hours after the encounter "late entries" and requires explicit labeling as such.
Objectivity & Neutral Language
| Avoid (Subjective / Stigmatizing) | Preferred (Objective / Neutral) |
|---|---|
| "Drug-seeking behavior" | "Requested additional opioid medication; pattern suggests possible opioid use disorder, see assessment" |
| "Non-compliant" | "Reports missing 3 doses this week due to cost; discussed patient assistance programs" |
| "Poor historian" | "History limited by cognitive impairment; corroborated with family member present" |
| "Frequent flyer" | "Third ED visit this month for similar complaint" |
| "Denies abuse despite suspicious findings" | "Patient states no abuse occurred; physical findings and history raise concern, social work consulted" |
| "Refused" | "Declined after discussion of risks, benefits, and alternatives" |
The "Golden Rules" of Documentation
- Write what you see, think, and do — in that order.
- Never alter a note without a formal amendment or addendum — retroactive edits destroy credibility.
- If it wasn't documented, it wasn't done — but the inverse is also true: if it was documented but not done, that's fraud.
- Document informed consent discussions verbatim when high-stakes decisions are involved.
- Avoid speculation about other providers' care or motives.
03 Medicolegal Aspects & HIPAA Basics
The medical record is the single most important piece of evidence in a malpractice action. Plaintiff attorneys evaluate cases primarily by chart review, and the quality of documentation often determines whether a case is pursued, settled, or dismissed. Simultaneously, the record itself is protected health information (PHI) subject to federal privacy law under HIPAA.
HIPAA at a Glance
The Health Insurance Portability and Accountability Act (HIPAA), enacted in 1996, establishes national standards for the privacy and security of protected health information. The Privacy Rule governs use and disclosure of PHI; the Security Rule governs electronic PHI (ePHI); and the Breach Notification Rule requires notification of affected individuals when unsecured PHI is compromised.
| HIPAA Concept | Definition |
|---|---|
| PHI | Any individually identifiable health information, including name, DOB, MRN, address, diagnosis, photos |
| Covered Entity | Health plans, health care clearinghouses, and health care providers who transmit health information electronically |
| Business Associate | Third parties handling PHI on behalf of a covered entity (e.g., billing companies, EHR vendors) |
| TPO | Treatment, Payment, Operations — uses of PHI that do not require patient authorization |
| Minimum Necessary | Disclose only the minimum PHI necessary to accomplish the intended purpose |
| 18 Identifiers | The 18 HIPAA identifiers that, when removed, render data "de-identified" under the Safe Harbor method |
Civil penalties range from $100 to $50,000 per violation (up to $1.5 million per year for identical violations). Criminal penalties for willful disclosure can reach $250,000 and 10 years imprisonment. Common inadvertent violations: discussing patients in elevators, leaving charts open on public screens, texting PHI over unencrypted SMS, and improperly disposed paper records.
Elements of a Malpractice Claim
A plaintiff must prove all four elements, often called the "4 Ds":
| Element | Meaning | Documentation Role |
|---|---|---|
| Duty | A physician–patient relationship existed | Established by the note itself |
| Dereliction (Breach) | The standard of care was violated | Note shows (or fails to show) appropriate workup and reasoning |
| Damages | The patient suffered harm | Injury documented in subsequent records |
| Direct Cause | The breach caused the harm | Timeline and clinical reasoning in notes |
The Note as Legal Evidence
In malpractice litigation, juries assign enormous weight to contemporaneous documentation. A detailed note written at the time of the encounter is credible; a terse note "augmented" by memory years later is not. Courts generally consider the chart the most reliable record of what happened, and inconsistencies between the chart and testimony are devastating to the defense.
Informed Consent Documentation
For any significant procedure, test, or treatment carrying meaningful risk, document that you discussed the risks, benefits, and alternatives (including the alternative of no treatment), that the patient had the opportunity to ask questions, and that they agreed to proceed. The classic shorthand is "RBAQ" (Risks, Benefits, Alternatives, Questions) — but a brief narrative is more defensible than a checkbox.
04 Chief Complaint & HPI Structure
The History and Physical (H&P) is the foundational narrative document of inpatient and outpatient medicine. It establishes the reason for the encounter, the relevant background, the clinician's physical findings, and the initial diagnostic and therapeutic plan. The H&P sets the stage for every subsequent note and decision; a sloppy or incomplete H&P haunts the entire hospitalization.
Chief Complaint (CC)
The chief complaint is the patient's own words explaining why they are seeking care, ideally in quotes and one sentence. It should describe a symptom, not a diagnosis:
| Weak CC | Strong CC |
|---|---|
| "COPD exacerbation" | "I can't catch my breath" × 3 days |
| "Chest pain, r/o MI" | "Pressure in the middle of my chest" for 2 hours |
| "Admission for pneumonia" | "Cough and fever" × 1 week |
History of Present Illness (HPI)
The HPI is a chronological narrative of the current problem from onset to presentation. Two mnemonics organize the elements; both are equivalent but emphasize different dimensions:
| OLDCARTS | PQRST | Element |
|---|---|---|
| O — Onset | — | When did the symptom begin? Sudden or gradual? |
| L — Location | — | Where is it? Point with one finger. |
| D — Duration | — | Constant or intermittent? Episode length? |
| C — Character | Q — Quality | Sharp, dull, crushing, burning, pressure |
| A — Aggravating/Alleviating | P — Provoking/Palliating | What makes it better or worse? |
| R — Radiation | R — Radiation | Does it move or refer elsewhere? |
| T — Timing | T — Timing | Continuous, waxing/waning, episodic |
| S — Severity | S — Severity | 0–10 pain scale; functional impact |
| — | — | Associated symptoms; pertinent positives and negatives |
Under legacy 1995/1997 E/M guidelines (still used for inpatient and many non–office services), a "brief" HPI requires 1–3 elements and an "extended" HPI requires 4+ elements (or status of 3+ chronic conditions). The 2021 outpatient revision eliminated the HPI element count for office visits, but the HPI remains clinically essential.
HPI Narrative Structure
A polished HPI reads like a short story. Begin with a one-sentence summary identifying the patient, relevant context, and the presenting problem. Then provide a chronological narrative that ends at the time of presentation. Close with pertinent positives and negatives from the ROS that refine the differential.
"Mr. Jones is a 64-year-old man with hypertension, type 2 diabetes, and a 40-pack-year smoking history who presents with 3 hours of substernal chest pressure radiating to the left arm."
"Ms. Kim is a 28-year-old previously healthy woman who presents with 5 days of progressive right lower quadrant abdominal pain, anorexia, and a low-grade fever."
Pertinent Positives & Negatives
The HPI should close with findings from the ROS that matter to the differential. For chest pain, document presence or absence of dyspnea, diaphoresis, nausea, radiation, and exertional component. For abdominal pain, document nausea, vomiting, diarrhea, urinary symptoms, last menstrual period, and fever. A skilled clinician's choice of pertinent negatives reveals the differential diagnosis being worked through.
05 Past Medical, Surgical, Family & Social History
Past Medical History (PMH)
List active and relevant resolved medical conditions. For each, include the year of diagnosis, current control, and treating specialist when relevant. Avoid listing obsolete problems that no longer affect care (e.g., "strep throat 1985").
| Domain | Elements to Capture |
|---|---|
| Chronic conditions | Diagnosis, year, current control, complications |
| Hospitalizations | Year, indication, hospital, outcome |
| Childhood illnesses | Rheumatic fever, polio, measles (relevant to current care) |
| Screening history | Colonoscopy, mammography, Pap, DEXA, immunizations |
| Transfusion history | Year, indication, reactions |
Past Surgical History (PSH)
List surgeries with year, indication, surgeon (if relevant), and outcome. Note any anesthetic complications (malignant hyperthermia, prolonged paralysis, difficult intubation).
Medications
List every medication with name, dose, route, frequency, and indication. Include prescription drugs, over-the-counter agents, herbal supplements, and vitamins. Medication reconciliation at each transition of care (admission, transfer, discharge) is a Joint Commission National Patient Safety Goal.
Allergies & Adverse Reactions
Document the allergen, the type of reaction (rash, anaphylaxis, GI upset, known side effect), and the year of the reaction. Differentiate true allergies from intolerances — labeling a GI side effect as an "allergy" narrows future therapeutic options unnecessarily.
| Reaction Type | Example | Documentation |
|---|---|---|
| True allergy (IgE mediated) | Hives, anaphylaxis after penicillin | Document as allergy; avoid class |
| Intolerance / side effect | Nausea from erythromycin | Document as intolerance, not allergy |
| Severe cutaneous reaction | SJS/TEN from sulfa | Document as severe allergy with alert |
| Idiosyncratic reaction | Statin myopathy | Document reaction, consider class avoidance |
Family History (FH)
Document first-degree relatives (parents, siblings, children) with age, health status, and major illnesses. Ask specifically about cancer (type and age of onset), cardiovascular disease, diabetes, mental illness, and sudden cardiac death. A family history of early-onset disease (e.g., colon cancer before age 50, MI before age 55 in men or 65 in women) alters screening recommendations.
Social History (SH)
The social history is often the highest-yield section for understanding a patient's risk factors, functional status, and social determinants of health.
| Domain | Specific Questions |
|---|---|
| Tobacco | Type, pack-years, current use, quit date, prior attempts |
| Alcohol | Drinks/day, drinks/week, CAGE or AUDIT-C screen |
| Substances | Marijuana, cocaine, methamphetamine, opioids, IV drug use |
| Occupation | Current/past, exposures (asbestos, silica, solvents, radiation) |
| Living situation | Home, apartment, facility; stairs; caregivers |
| Relationships | Marital status, sexual activity, partners, practices, protection |
| Functional status | ADLs, IADLs, mobility aids, work status |
| Diet & exercise | Dietary pattern, caffeine, physical activity |
| Social determinants | Housing, food security, transportation, insurance |
06 Review of Systems
The Review of Systems (ROS) is a structured inventory of symptoms organized by body system. It is distinct from the HPI: the HPI focuses on the chief complaint, while the ROS screens broadly for symptoms the patient may not have spontaneously reported. A complete ROS covers 10+ systems; a problem-pertinent ROS covers 2–9 systems relevant to the chief complaint.
The 14 Body Systems of the ROS
| System | Key Symptoms to Screen |
|---|---|
| Constitutional | Fever, chills, night sweats, fatigue, weight change, appetite |
| HEENT | Headache, vision changes, hearing loss, tinnitus, epistaxis, sore throat, congestion |
| Cardiovascular | Chest pain, palpitations, orthopnea, PND, edema, claudication, syncope |
| Respiratory | Cough, sputum, hemoptysis, dyspnea, wheezing |
| Gastrointestinal | Nausea, vomiting, diarrhea, constipation, abdominal pain, hematochezia, melena, reflux |
| Genitourinary | Dysuria, frequency, urgency, hematuria, incontinence, flank pain, discharge |
| Musculoskeletal | Joint pain, swelling, stiffness, back pain, weakness, gait |
| Neurologic | Headache, syncope, seizures, weakness, numbness, tremor, memory |
| Psychiatric | Mood, anxiety, sleep, suicidal/homicidal ideation, hallucinations |
| Endocrine | Polyuria, polydipsia, heat/cold intolerance, hair or skin changes |
| Heme/Lymph | Easy bruising, bleeding, lymphadenopathy, anemia symptoms |
| Allergic/Immunologic | Hives, anaphylaxis, frequent infections, rhinitis |
| Skin | Rash, itching, lesions, hair loss, nail changes |
| Eyes | Vision loss, diplopia, pain, redness, photophobia |
"A 10-system ROS was performed and is negative except as documented in the HPI." This phrasing is acceptable under 1995/1997 E/M guidelines when the full ROS was actually obtained, but should not be used as a default when systems were not truly reviewed. The 2021 outpatient E/M revision eliminated ROS counting for office visits, but ROS remains essential for clinical completeness and inpatient services.
Common ROS Pitfalls
- Copy-forward without review — documenting "no change" when the patient has new symptoms.
- Contradicting the HPI — "denies chest pain" in ROS when HPI describes chest pain.
- Over-documentation — a 14-system negative ROS for a simple wart removal.
- Template default values — unchecked boxes that auto-populate as "normal."
07 Physical Exam Documentation
The physical examination is documented in a standard head-to-toe sequence. Only document exams you actually performed — fabricating or copy-forwarding exam findings is the fastest way to lose a malpractice case and potentially your license.
Standard Physical Exam Sequence
| System | Standard Elements |
|---|---|
| Vitals | T, HR, BP, RR, SpO2, weight, BMI, pain score |
| General | Appearance, distress, hydration, body habitus, mood |
| HEENT | Normocephalic, PERRL, EOMI, TMs, oropharynx, thyroid, JVP |
| Neck | Supple, no lymphadenopathy, no thyromegaly, no carotid bruits |
| Cardiovascular | Rate, rhythm, S1/S2, murmurs, rubs, gallops, peripheral pulses, edema |
| Pulmonary | Effort, symmetry, breath sounds, wheezes, rales, rhonchi |
| Abdomen | Bowel sounds, distension, tenderness, guarding, rebound, organomegaly, masses |
| GU/Rectal | When indicated; include chaperone documentation |
| Musculoskeletal | ROM, strength, joint swelling, deformity, gait |
| Skin | Color, temperature, turgor, rashes, lesions, wounds |
| Neurologic | Mental status, CN II–XII, motor, sensory, DTRs, coordination, gait |
| Psychiatric | Appearance, behavior, speech, mood, affect, thought, insight, judgment |
Comprehensive vs. Problem-Focused Exam
| Exam Type | 1995 Guidelines | 1997 Guidelines | Use Case |
|---|---|---|---|
| Problem-focused | 1 body area/system | 1–5 bullets | Minor complaint |
| Expanded problem-focused | 2–7 systems (limited) | 6–11 bullets | Limited problem |
| Detailed | 2–7 systems (extended) | ≥12 bullets, 2 systems | Moderate complexity |
| Comprehensive | 8+ systems | All bulleted elements of 9 systems | New patient H&P, admission |
Document what you found, not what you expect to find. "Heart RRR, no murmurs" is only acceptable if you auscultated the heart. Never document "normal" for an exam you did not perform.
Chaperone Documentation
For sensitive exams (pelvic, breast, rectal, genital), document the presence of a chaperone by name and role: "Pelvic exam performed in the presence of Ms. Rodriguez, RN, as chaperone." This protects both patient and clinician.
08 Subjective & Objective Sections
The SOAP note — Subjective, Objective, Assessment, Plan — is the workhorse format for progress notes, outpatient visits, and consults. Introduced by Lawrence Weed in the 1960s as part of the Problem-Oriented Medical Record, SOAP imposes a logical flow: gather data (S + O), interpret it (A), and act on it (P).
Subjective
The subjective section contains information obtained from the patient or other informants: the chief complaint, interval history since the last visit, current symptoms, medication adherence, and responses to treatment. In a progress note, this is focused on changes since the last note, not a repeat of the full H&P.
"HD3. Patient reports improved breathing overnight, no further chest pain. Tolerated regular diet this morning. Ambulated in hallway with PT. No new complaints."
Objective
The objective section contains measurable, observable data: vital signs, physical exam findings, laboratory results, imaging, and other diagnostic data. This section is factual — it should not contain interpretation.
| Element | Example Documentation |
|---|---|
| Vitals | T 37.2, HR 82, BP 128/74, RR 16, SpO2 96% RA |
| Ins/Outs | I: 2400 mL; O: 2100 mL (UOP 1600 mL) |
| Physical exam | Focused findings relevant to active problems |
| Labs | Na 138, K 4.1, Cr 1.2 (baseline 1.1), WBC 11.2 (down from 14.5) |
| Imaging | CXR (AM): interval improvement in right lower lobe infiltrate |
| Micro | Blood cultures 2/2 negative at 48 hours |
Trending Data
Show the trajectory of key values, not just the current number. "Creatinine 1.2 (from 1.8 on admission)" is more useful than "Creatinine 1.2." Trends drive clinical decisions; isolated numbers do not.
09 Assessment & Plan
The Assessment and Plan (A/P) is the intellectual core of the note — where the clinician synthesizes the data into a diagnosis and a management strategy. Auditors, consultants, and attorneys read the A/P first; the S and O sections exist to support it.
Assessment Structure
Begin with a one-sentence summary statement: "Mr. Jones is a 64-year-old man with CAD, HTN, and T2DM admitted with NSTEMI, currently on dual antiplatelet therapy and stable." This single sentence frames the entire note.
Follow the summary with a numbered problem list, each problem addressed individually:
1. NSTEMI — Peak troponin 2.4; cath planned today. Continue ASA, clopidogrel, atorvastatin 80, metoprolol, heparin gtt.
2. HTN — Controlled on home regimen. Continue lisinopril 20 mg daily.
3. T2DM — A1c 7.8 on admission. Hold metformin until after cath; sliding scale insulin.
4. DVT ppx — Heparin gtt sufficient; enoxaparin held.
5. Dispo — Remains on telemetry; anticipate cath lab transfer 0900.
Assessment-and-Plan Integration vs. Separation
Two conventions exist. The integrated A/P lists each problem followed immediately by its plan — this is the dominant modern style because it puts reasoning and action side by side. The separated A/P lists all problems first, then all plans — this is older and harder to follow in complex patients.
| Style | Advantages | Disadvantages |
|---|---|---|
| Integrated (A/P per problem) | Clarity; pairs diagnosis with action | Slightly longer |
| Separated (A, then P) | Emphasizes overall diagnosis | Harder to follow in complex patients |
Key Elements of a Strong Plan
- Diagnostics — What tests are pending, what you'll order, why.
- Therapeutics — Medications continued, added, adjusted, held.
- Monitoring — Vitals, labs, clinical parameters to follow.
- Consultations — Specialists involved, reason for consult.
- Disposition — Anticipated trajectory and discharge criteria.
- Patient communication — Discussions with patient/family, decisions made.
10 Clinical Reasoning & Differential Diagnosis
The best A/Ps make clinical reasoning explicit. Rather than jumping to a single diagnosis, document the differential considered and why one diagnosis is favored over alternatives. This serves three purposes: it forces rigorous thinking, it communicates your reasoning to colleagues, and it provides a robust medicolegal defense if the diagnosis is later proven wrong.
Documenting a Differential
"The patient's substernal pressure radiating to the left arm, associated with diaphoresis and exertional pattern, is most consistent with acute coronary syndrome. Aortic dissection is less likely given the non-tearing character, absence of radiation to back, and symmetric pulses and blood pressures. Pulmonary embolism is possible but lower priority without dyspnea, tachycardia, or risk factors. Esophageal spasm and GERD are lower on the differential given exertional pattern and diaphoresis. Initial workup with ECG, troponin, and CXR underway; will reassess after results."
The "Can't Miss" Principle
For every chief complaint, document that you considered the "can't miss" (life-threatening, time-sensitive) diagnoses, even if you rule them out. For chest pain: ACS, aortic dissection, PE, tension pneumothorax, pericardial tamponade, esophageal rupture (the "deadly six"). For headache: subarachnoid hemorrhage, meningitis, temporal arteritis, mass, stroke, carbon monoxide. For back pain: cauda equina, epidural abscess, aortic dissection/AAA, spinal cord compression.
Shared Decision-Making
When reasonable options exist, document the options discussed, the patient's values and preferences, and the shared decision reached. This is both ethically essential and a strong medicolegal defense.
11 Inpatient Daily Progress Notes
The inpatient progress note documents the daily clinical status, events, decisions, and plan for a hospitalized patient. It is the primary communication tool between the day team, the night team, consultants, and the following day's team. Progress notes follow the SOAP format but are condensed — they should describe changes and decisions, not repeat the entire H&P.
Standard Inpatient Progress Note Format
HD [#], POD [# if post-op]
Subjective: Overnight events, current symptoms, tolerance of diet/meds/therapy.
Objective: Vitals (range and current), I&Os, focused exam, new labs, new imaging, cultures.
Assessment: One-sentence summary of clinical status and trajectory.
Plan: Problem-by-problem, numbered, with action items for the day.
Disposition: Anticipated discharge date and barriers.
Elements to Include Daily
- Hospital day number and post-op day if applicable.
- Overnight events — any new symptoms, rapid responses, code events.
- Vitals range (Tmax, BP range, HR range) — not just the morning values.
- I&Os — intake, output, net balance.
- Drips and devices — continuous infusions, lines, tubes, drains.
- Culture data — day of each positive result.
- Antibiotic day — "vancomycin D4/14" or "ceftriaxone D3."
- DVT prophylaxis — actively documented each day.
- Disposition planning — anticipated discharge date, barriers.
Post-Op Progress Note Essentials
| Element | Why It Matters |
|---|---|
| POD number | Tracks expected recovery trajectory |
| Procedure | Context for exam findings and complications |
| Pain control | Route, agent, adequacy |
| Diet advancement | NPO, sips, clears, full, regular |
| Ambulation | Level (bed, chair, hallway, independent) |
| Drains/lines | Output, character, plan for removal |
| Wound | Dressing, appearance, signs of infection |
12 Outpatient Follow-Up Notes
The outpatient follow-up note is shorter and more focused than inpatient notes. It addresses the specific reason for the visit, updates active problems, and documents the plan until the next encounter. The 2021 E/M revision made these notes dramatically simpler by eliminating HPI and ROS counting requirements.
Outpatient Note Structure
Reason for visit: Follow-up HTN, DM.
Interval history: Feeling well. Home BP avg 128/78. FBS 110–130. No hypoglycemia. Taking all medications.
ROS: Negative except as above.
Exam: BP 130/80, HR 72, BMI 29.4. Heart RRR, lungs clear, no edema. Monofilament intact bilaterally.
Labs (today): A1c 6.9 (prior 7.1), Cr 0.9, LDL 88.
Assessment/Plan:
1. T2DM — improved control. Continue metformin 1000 BID. Annual eye exam due.
2. HTN — at goal. Continue lisinopril 20. Home BP log reviewed.
3. Health maintenance — colonoscopy due 2027, flu vaccine today.
Follow-up: 3 months with A1c and BMP.
Focused Visit Notes
For acute problem visits (URI, sprain, rash), document only the focused HPI, relevant exam, and plan. A two-paragraph note is appropriate and often ideal. Resist the urge to over-document simple problems.
Chronic Care Management Elements
For Medicare chronic care management billing, document coordination activities: medication reconciliation, specialist communications, care planning discussions, and time spent. Each discrete activity should have its own entry or timestamp.
13 Problem List Management
The problem list is the structured summary of a patient's active and resolved medical problems. In the EHR, the problem list drives clinical decision support, billing, risk adjustment, and care gap alerts. A well-curated problem list is one of the highest-impact documentation habits a clinician can develop; a neglected problem list accumulates errors that propagate across future encounters.
Problem List Best Practices
| Practice | Action |
|---|---|
| Specificity | Use most specific ICD-10 code available (e.g., "DM2 with diabetic neuropathy" not "DM") |
| Active vs. resolved | Mark resolved problems as such (e.g., pneumonia that recovered) |
| Duplicates | Merge duplicate entries (e.g., "HTN" and "Essential HTN") |
| Stale problems | Remove problems no longer relevant (e.g., "URI, 2019") |
| Chronic conditions | Every visit should confirm and address chronic conditions for HCC capture |
| Staging | Include stage/severity where relevant (CKD stage, CHF NYHA class) |
For Medicare Advantage and ACO-attributed patients, chronic conditions must be re-documented at least once per calendar year to count for Hierarchical Condition Category (HCC) risk adjustment. A chronic condition documented in 2025 that is not re-documented in 2026 "drops off" the patient's risk score. See Section 24 for details.
Transitioning Problems to Active vs. Resolved
Active problems are those requiring ongoing management, monitoring, or affecting current care. Resolved problems are completed episodes (e.g., acute pneumonia that recovered, fractures that healed) — these should be moved to a "past medical history" or "resolved" section to keep the active list manageable. Some EHRs automate this via problem status fields.
14 Admission H&P & Discharge Summary
Admission H&P
The admission H&P is the most comprehensive note in a hospitalization. It must be completed within 24 hours of admission per Joint Commission standards and contains the full history, physical exam, differential diagnosis, and initial plan.
| Section | Contents |
|---|---|
| Demographics & CC | Patient identifiers; chief complaint in patient's words |
| HPI | Full chronological narrative of current illness |
| PMH/PSH | All relevant history |
| Medications | Home medications with doses; reconciled at admission |
| Allergies | With reaction types |
| FH/SH | Complete family and social history |
| ROS | Complete 10+ system review |
| Physical exam | Comprehensive |
| Data | Admission labs, imaging, ECG |
| Assessment | Summary statement, differential, problem list |
| Plan | By problem, with admission orders referenced |
| Code status | Explicitly documented with whom it was discussed |
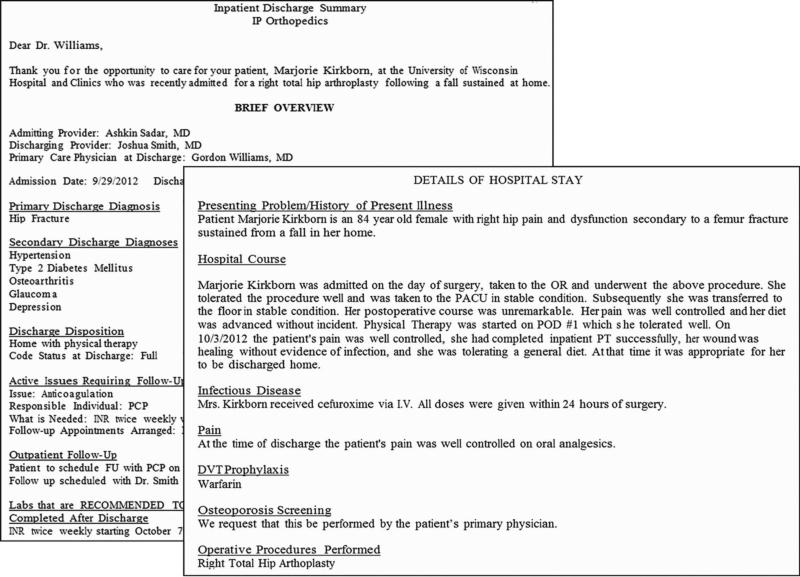
Discharge Summary
The discharge summary is arguably the most important document for patient safety during the vulnerable post-hospital period. It is the primary communication tool between the inpatient team and the outpatient providers who will assume care. Incomplete discharge summaries are a leading cause of post-discharge adverse events and readmissions.
1. Admission and discharge dates
2. Admitting and principal diagnoses
3. Secondary diagnoses addressed during stay
4. Brief hospital course (narrative, by problem)
5. Procedures performed
6. Pertinent lab and imaging results
7. Consultations obtained
8. Discharge medications with changes highlighted
9. Follow-up appointments (specific, with dates if possible)
10. Pending tests at discharge (critical for follow-up)
11. Discharge condition and disposition
12. Code status
13. Patient and family education provided
Joint Commission Discharge Summary Requirements
- Reason for hospitalization
- Significant findings
- Procedures and treatment provided
- Patient's discharge condition
- Patient and family instructions (as appropriate)
- Attending physician's signature
15 Transfer, Code Blue & Death Notes
Transfer Note
When a patient transfers between services, units, or facilities, a transfer note summarizes the hospital course to date and transfers responsibility. At minimum, include: reason for transfer, current problems, active medications, pending tests, code status, and the accepting provider.
ICU Transfer
Transfers to or from the ICU require particularly thorough notes documenting the precipitating event, the interventions performed, and the current status.
Code Blue / Rapid Response Note
| Element | Documentation |
|---|---|
| Time called / arrived | Exact times |
| Trigger | What prompted the call (e.g., unresponsive, hypotension) |
| Pre-event status | Relevant history and recent events |
| Initial exam | Airway, breathing, circulation, rhythm, GCS |
| Interventions | Compressions, defibrillation, airway, medications (with times) |
| Response | ROSC, rhythm changes, clinical response |
| Outcome | Transferred to ICU, expired, stabilized on floor |
| Team members | Who ran the code, who was present |
| Family communication | Who was notified, when, by whom |
Death Note (Pronouncement Note)
The death pronouncement note documents the physical findings confirming death, the time of death, and the family notification. Required elements:
- Called to bedside at [time] to evaluate patient for pronouncement.
- Physical findings: no spontaneous respirations observed for [≥1 minute], no heart sounds auscultated for [≥1 minute], no palpable pulses, pupils fixed and dilated, no response to noxious stimuli.
- Time of death: [exact time].
- Family notification: family present/notified by phone, name of contact, time.
- Attending notified: name, time.
- Autopsy: discussed/declined/accepted.
- Organ donation: state organ procurement organization contacted per protocol.
- Medical examiner: case referred (if required) or not required.
16 Procedure & Operative Notes
Procedure notes document any invasive intervention, from a paracentesis to a cardiac catheterization. They are required immediately after the procedure and must contain specific elements to support billing, quality, and medicolegal purposes.
Standard Procedure Note Elements
| Element | Contents |
|---|---|
| Pre-procedure diagnosis | Working diagnosis indicating the procedure |
| Post-procedure diagnosis | Diagnosis confirmed or revised by findings |
| Procedure performed | Exact name, including laterality and approach |
| Indication | Why the procedure was needed |
| Consent | Informed consent obtained; RBA discussed; questions answered |
| Time-out / universal protocol | Time-out performed, correct patient/procedure/site confirmed |
| Anesthesia / sedation | Type, agent, dosage, provider |
| Prep and drape | Sterile technique described |
| Technique | Step-by-step description of what was done |
| Findings | What was seen, felt, or obtained |
| Specimens | Sent to pathology, microbiology, etc. |
| EBL | Estimated blood loss |
| Complications | None, or description of any adverse events |
| Disposition | Patient's condition and where they went after |
| Operator and assistants | Names and roles |
Operative Note vs. Operative Report
After surgery, the surgeon writes a brief operative note immediately (handwritten or EHR note) and then dictates a full operative report within 24 hours. The brief op note contains the essential information for the recovering team; the full operative report is the definitive legal document.
1. Pre-op diagnosis
2. Post-op diagnosis
3. Procedure performed
4. Surgeon
5. Assistants
6. Findings
7. EBL
8. Specimens removed
9. Complications
10. Anesthesia type
11. Fluids administered
12. Urine output
13. Disposition
Sample Bedside Procedure Note
Procedure: Diagnostic and therapeutic paracentesis
Indication: New-onset ascites, rule out SBP
Consent: Obtained from patient after discussion of risks (bleeding, infection, visceral injury, persistent leak) and benefits. Questions answered.
Time-out: Performed with nursing. Correct patient/procedure/site confirmed.
Technique: Left lower quadrant chosen after ultrasound identification of fluid pocket avoiding inferior epigastric vessels. Site prepped with chlorhexidine, draped sterilely. Local anesthesia with 1% lidocaine. 16-gauge catheter-over-needle advanced under ultrasound guidance until fluid return. Catheter advanced, needle withdrawn. 50 mL sent for cell count, culture, total protein, albumin. Therapeutic drainage of 4500 mL straw-colored fluid performed. Catheter removed, sterile dressing applied.
EBL: Minimal
Complications: None
Disposition: Patient tolerated well, hemodynamically stable, returned to room.
17 Consult, Telephone & ED Notes
Consultation Notes
A consult note answers a specific question posed by a referring provider. A good consult note has three essential elements: the question asked, the answer, and the recommendations. Never write a consult note without explicitly naming the question.
Reason for consult: "Evaluation of new-onset atrial fibrillation in 68yo with CHF exacerbation; requesting recommendations on rate vs rhythm control."
HPI and relevant history: Focused on the consult question.
Exam: Focused on relevant systems.
Data reviewed: ECG, echo, labs.
Impression: New AF with RVR in setting of decompensated HF. CHADS-VASc score 4.
Recommendations: Numbered, specific, actionable.
Availability: "Happy to follow; please call with questions."
Telephone / Patient Portal Encounter
Telephone encounters and patient portal messages are discoverable legal documents and must be documented with the same care as in-person visits. Elements: who called, when, reason for contact, clinical assessment, advice given, disposition (come in, ED, continue home care), and verification of understanding.
| Element | Example |
|---|---|
| Who / when | Call from patient 4/2/26 at 1430 |
| Reason | Reports 2 days of increased SOB, worse with exertion |
| Assessment | Symptoms concerning for CHF exacerbation vs pneumonia |
| Plan | Advised to come to clinic same day; if unable, go to ED |
| Verification | Patient agreed; understood red flags reviewed (chest pain, worsening SOB) |
Emergency Department Note
ED notes are high-stakes, high-volume documentation. They must be completed contemporaneously and capture the clinical reasoning for time-sensitive decisions. Key unique elements:
- Arrival mode and time (ambulance, walk-in, transfer).
- Triage vitals and chief complaint as documented at arrival.
- Focused HPI with emphasis on "can't miss" diagnoses.
- Serial exams documenting changes over time.
- Medical decision-making with differential explicitly addressed.
- Re-evaluation before disposition.
- Disposition conversation (admit, discharge, transfer, against medical advice).
- Discharge instructions with explicit return precautions.
18 Psychiatric & Pediatric Notes
Psychiatric Notes
Psychiatric notes require additional elements beyond standard medical documentation: mental status exam, suicide/homicide risk assessment, capacity evaluation, and treatment rationale. Because of heightened confidentiality concerns, psychotherapy process notes receive special HIPAA protection.
| Section | Elements |
|---|---|
| Identifying data | Age, sex, legal status (voluntary vs involuntary), referral source |
| Chief complaint | Patient's words |
| HPI | Psychiatric symptoms, onset, stressors, treatment history |
| Past psychiatric history | Hospitalizations, medications, suicide attempts, substance use |
| Mental status exam | Appearance, behavior, speech, mood, affect, thought process/content, perception, cognition, insight, judgment |
| Risk assessment | Suicide and homicide risk with risk factors, protective factors, and plan |
| Capacity | When relevant: ability to make specific medical decisions |
| Diagnosis | DSM-5 diagnosis with supporting features |
| Formulation | Biopsychosocial understanding of the case |
| Plan | Pharmacologic, therapeutic, disposition |
Mental Status Exam Template
Appearance: Well-groomed, appropriate for age/weather, no acute distress.
Behavior: Cooperative, good eye contact, no psychomotor abnormalities.
Speech: Normal rate, rhythm, volume, prosody.
Mood: "Depressed" (patient's words).
Affect: Constricted, congruent with mood.
Thought process: Linear, goal-directed.
Thought content: No SI/HI, no delusions, no hallucinations.
Cognition: Alert, oriented × 3, attention intact, recent and remote memory intact.
Insight: Fair.
Judgment: Fair.
Pediatric Well-Child Note
Pediatric notes incorporate growth, development, feeding, safety, and anticipatory guidance in addition to standard elements. Each well-child visit has age-specific required content from Bright Futures guidelines.
| Element | Pediatric-Specific Content |
|---|---|
| Growth | Weight, length/height, head circumference, percentiles |
| Development | Gross/fine motor, language, social milestones |
| Feeding | Breast/formula/solids; amount; frequency |
| Elimination | Stool/urine patterns |
| Sleep | Hours, location, safe sleep practices |
| Immunizations | Given today, up to date, deferred |
| Screening | Hearing, vision, developmental screens, lead, anemia |
| Safety | Car seat, pool, firearms, screen time |
| Anticipatory guidance | Age-appropriate topics discussed |
19 2021 Outpatient E/M Revision
Evaluation and Management (E/M) codes describe physician cognitive work and are the primary billing mechanism for office visits, hospital visits, and consultations. In January 2021, CMS and the AMA implemented the most significant E/M revision in 25 years, fundamentally changing how outpatient (office) visits are coded — replacing the old "history, exam, MDM" bullet-counting system with a choice between medical decision making (MDM) or total time on the date of service.
1. History and exam no longer determine code level — document only what is "medically appropriate."
2. Code level determined by MDM OR total time on the date of service.
3. Code 99201 eliminated; new patient codes now 99202–99205, established 99211–99215.
4. Time-based coding uses total time (both face-to-face and non-face-to-face on date of service), not just face-to-face.
5. New prolonged services code G2212 (Medicare) / 99417 (non-Medicare) for 15 minutes beyond the highest level code.
Outpatient E/M Code Levels (2021)
| Code | New/Est | MDM Level | Total Time |
|---|---|---|---|
| 99202 | New | Straightforward | 15–29 min |
| 99203 | New | Low | 30–44 min |
| 99204 | New | Moderate | 45–59 min |
| 99205 | New | High | 60–74 min |
| 99211 | Est | N/A (nurse visit) | < 5 min |
| 99212 | Est | Straightforward | 10–19 min |
| 99213 | Est | Low | 20–29 min |
| 99214 | Est | Moderate | 30–39 min |
| 99215 | Est | High | 40–54 min |
New vs. Established Patient
A new patient has not received professional services from the physician (or another physician of the same specialty and subspecialty in the same group) within the past three years. Misclassifying new vs. established patients is a common billing error and a frequent audit target.
20 Medical Decision Making & Time-Based Coding
Under the 2021 revision, MDM complexity is determined by three elements; the level reached in two of the three elements sets the overall MDM level.
The Three MDM Elements
| Element | What It Measures |
|---|---|
| Problems addressed | Number and complexity of problems managed at the encounter |
| Data reviewed & analyzed | Tests reviewed, orders, discussion with other providers, independent interpretation |
| Risk | Risk of complications, morbidity, or mortality from the problem and management |
MDM Level Grid (Simplified)
| MDM Level | Problems | Data | Risk |
|---|---|---|---|
| Straightforward | Minimal (1 self-limited) | Minimal/none | Minimal |
| Low | Low (2 minor or 1 stable chronic) | Limited (1 category) | Low (OTC, minor surgery) |
| Moderate | Moderate (1 chronic with exacerbation, 2+ stable chronic, undiagnosed new problem) | Moderate (2+ categories, independent historian, interpretation) | Moderate (Rx management, minor surgery with risk, social determinants) |
| High | High (1 chronic with severe exacerbation, acute threat to life/function) | Extensive (3+ categories, discussion with external provider) | High (drug monitoring for toxicity, major surgery, decision re: hospitalization, DNR) |
Common 99214 (Moderate MDM) Triggers
- Two or more stable chronic conditions being managed.
- One chronic condition with exacerbation or side effect.
- Prescription drug management (starting, stopping, or adjusting).
- Undiagnosed new problem with uncertain prognosis.
- Acute illness with systemic symptoms.
Common 99215 (High MDM) Triggers
- Chronic condition with severe exacerbation.
- Acute or chronic illness posing threat to life or bodily function.
- Drug therapy requiring intensive monitoring for toxicity (e.g., warfarin, lithium, chemo).
- Decision regarding hospitalization or escalation of care.
- Decision regarding DNR/end-of-life care.
When MDM would only justify 99213 but the visit took 35 minutes total (including chart review, counseling, orders, documentation), bill 99214 based on time. Document the total time and specify activities: "Total time spent on date of service: 35 minutes including chart review, patient interview, physical examination, clinical decision-making, counseling on diabetes management, order entry, and documentation."
Prolonged Services
| Code | Use Case | Threshold |
|---|---|---|
| 99417 | Commercial payers — each additional 15 min beyond 99205/99215 | Begins at 15 min past the minimum of highest level (i.e., 89 min new, 69 min est) |
| G2212 | Medicare equivalent of 99417 | Begins 15 min past the MAXIMUM of highest level (i.e., 89 min new, 69 min est) |
21 Inpatient E/M, Critical Care & Modifiers
Inpatient E/M coding was revised in January 2023 to align with the 2021 outpatient principles. Hospital observation codes (99217–99220, 99224–99226) were eliminated and merged into the inpatient/observation code set.
Hospital Inpatient / Observation E/M (2023 Revision)
| Code | Service | MDM | Time |
|---|---|---|---|
| 99221 | Initial hospital/obs | Straightforward/low | 40 min |
| 99222 | Initial hospital/obs | Moderate | 55 min |
| 99223 | Initial hospital/obs | High | 75 min |
| 99231 | Subsequent hospital/obs | Straightforward/low | 25 min |
| 99232 | Subsequent hospital/obs | Moderate | 35 min |
| 99233 | Subsequent hospital/obs | High | 50 min |
| 99238 | Discharge, ≤ 30 min | — | ≤ 30 min |
| 99239 | Discharge, > 30 min | — | > 30 min |
Critical Care
Critical care codes 99291 (first 30–74 minutes) and 99292 (each additional 30 minutes) require: (1) a critically ill or injured patient with high probability of imminent or life-threatening deterioration, (2) the physician's full attention devoted to this patient, and (3) time documented.
"Patient is critically ill with septic shock requiring vasopressors and mechanical ventilation. I personally provided 65 minutes of critical care services including bedside evaluation, review of imaging and laboratory data, discussion with consultants, ventilator and vasopressor management, and family discussion. This time is exclusive of separately billable procedures."
Common Modifiers
| Modifier | Meaning | Use Case |
|---|---|---|
| -25 | Significant, separately identifiable E/M service on the same day as a procedure | Office visit for new problem + joint injection |
| -24 | Unrelated E/M service during postoperative global period | Surgeon sees patient for new unrelated problem during global period |
| -57 | Decision for major surgery made during E/M visit | Office visit where decision to proceed with major surgery is made |
| -59 | Distinct procedural service | Two procedures normally bundled, performed at separate sites or sessions |
| -95 | Synchronous telemedicine via interactive audio/video | Telehealth visit |
| -26 | Professional component only | Radiologist reads study owned by facility |
| -TC | Technical component only | Facility bills equipment/staff without interpretation |
22 ICD-10-CM Structure & Specificity
ICD-10-CM (International Classification of Diseases, 10th Revision, Clinical Modification) is the diagnosis code set used in the United States since October 2015. It contains approximately 70,000 codes (compared to 14,000 in ICD-9) organized into 22 chapters by body system and etiology.
ICD-10-CM Code Structure
| Position | Meaning | Example (E11.621) |
|---|---|---|
| 1 | Category (letter) | E = Endocrine |
| 2–3 | Category (numbers) | 11 = Type 2 diabetes |
| 4 | Etiology / anatomy | 6 = with other complications |
| 5 | Further specification | 2 = with skin complications |
| 6 | Further specification | 1 = with foot ulcer |
| 7 | Extension (encounter, laterality) | (7th character for some codes) |
Specificity Requirements
Claims are routinely denied when codes lack required specificity. "Unspecified" codes should be used only when the documentation genuinely does not support a more specific code. Common specificity failures:
| Less Specific (Often Denied) | More Specific (Preferred) |
|---|---|
| I10 — Essential hypertension | I10 is the only code; no further specificity required |
| E11.9 — T2DM without complications | E11.22 — T2DM with diabetic CKD |
| N18.9 — CKD unspecified | N18.3 — CKD stage 3 |
| R07.9 — Chest pain unspecified | I20.9 — Angina pectoris |
| J44.9 — COPD unspecified | J44.1 — COPD with acute exacerbation |
| M54.5 — Low back pain (retired) | M54.50 (now replaced with specific M54.5X codes) |
Signs/Symptoms vs. Definitive Diagnoses
When a definitive diagnosis has been established, code the diagnosis. When no definitive diagnosis is yet established, code the signs and symptoms. Never code "rule out" or "possible" diagnoses as established diagnoses in the outpatient setting — this is billing fraud. In the inpatient setting, however, ICD-10 guidelines allow coding "probable," "suspected," or "likely" conditions as if confirmed.
Sequencing Rules
The principal diagnosis (inpatient) or first-listed diagnosis (outpatient) should be the condition primarily responsible for the encounter. Secondary diagnoses are other conditions addressed during the encounter. Correct sequencing affects DRG assignment and reimbursement.
Status, History & Screening Codes (Z-codes)
| Category | Example | Code |
|---|---|---|
| Status | Long-term use of anticoagulants | Z79.01 |
| Status | Presence of cardiac pacemaker | Z95.0 |
| History | Personal history of malignant neoplasm of breast | Z85.3 |
| Screening | Screening for colon cancer | Z12.11 |
| Encounter for | General medical exam without abnormal findings | Z00.00 |
| Family history | FH of colon cancer | Z80.0 |
| Social determinant | Food insecurity | Z59.41 |
23 CPT Codes & Procedural Billing
Current Procedural Terminology (CPT) codes, maintained by the AMA, describe the services physicians provide. They are organized into three categories.
CPT Code Categories
| Category | Purpose | Examples |
|---|---|---|
| I | Primary procedure/service codes (5 digits) | 99213, 36415, 12001 |
| II | Performance measurement tracking codes (4 digits + F) | 1000F (tobacco assessed) |
| III | Temporary codes for emerging technologies (4 digits + T) | Newer experimental procedures |
Common CPT Codes
| Code | Procedure / Service |
|---|---|
| 99202–99205 | New patient office visit |
| 99212–99215 | Established patient office visit |
| 99221–99223 | Initial hospital/observation |
| 99231–99233 | Subsequent hospital/observation |
| 99238–99239 | Hospital discharge |
| 99291/99292 | Critical care |
| 99406/99407 | Tobacco cessation counseling |
| G0439 | Medicare annual wellness visit (subsequent) |
| 36415 | Venipuncture |
| 93000 | ECG with interpretation |
| 12001–12057 | Simple laceration repair |
| 20610 | Major joint injection/aspiration |
| 17110 | Destruction of benign lesions (up to 14) |
| 69210 | Cerumen removal requiring instrumentation |
| 94640 | Nebulizer treatment |
| 96372 | Therapeutic injection, IM/SC |
| G0008 | Influenza vaccine administration (Medicare) |
Bundling & the NCCI
The National Correct Coding Initiative (NCCI) maintains "edits" that bundle certain procedures together — billing the components separately is considered unbundling and is fraudulent. Modifier -59 can override some edits when procedures are genuinely distinct, but misuse of -59 is a major audit target.
Major surgeries include a global period (usually 90 days) during which routine post-op care is included in the surgical fee. Minor surgeries typically have 0 or 10 day globals. Services unrelated to the surgery during the global period can still be billed, but require modifier -24.
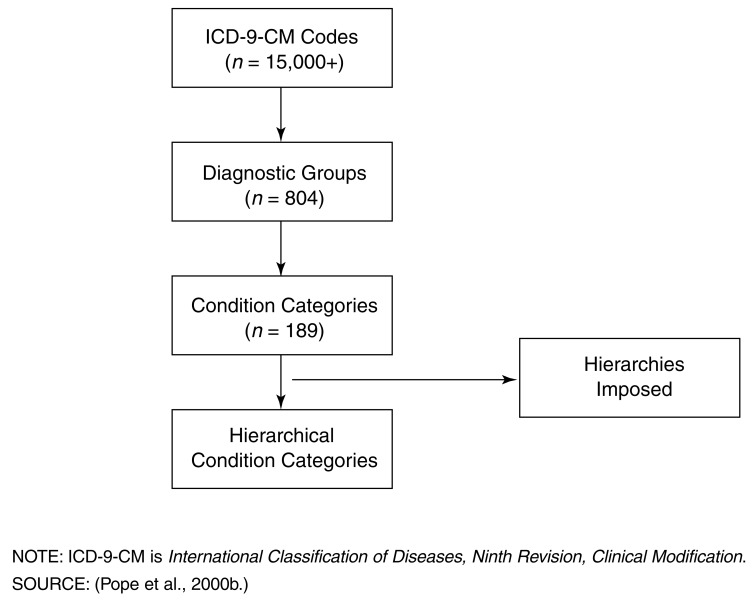
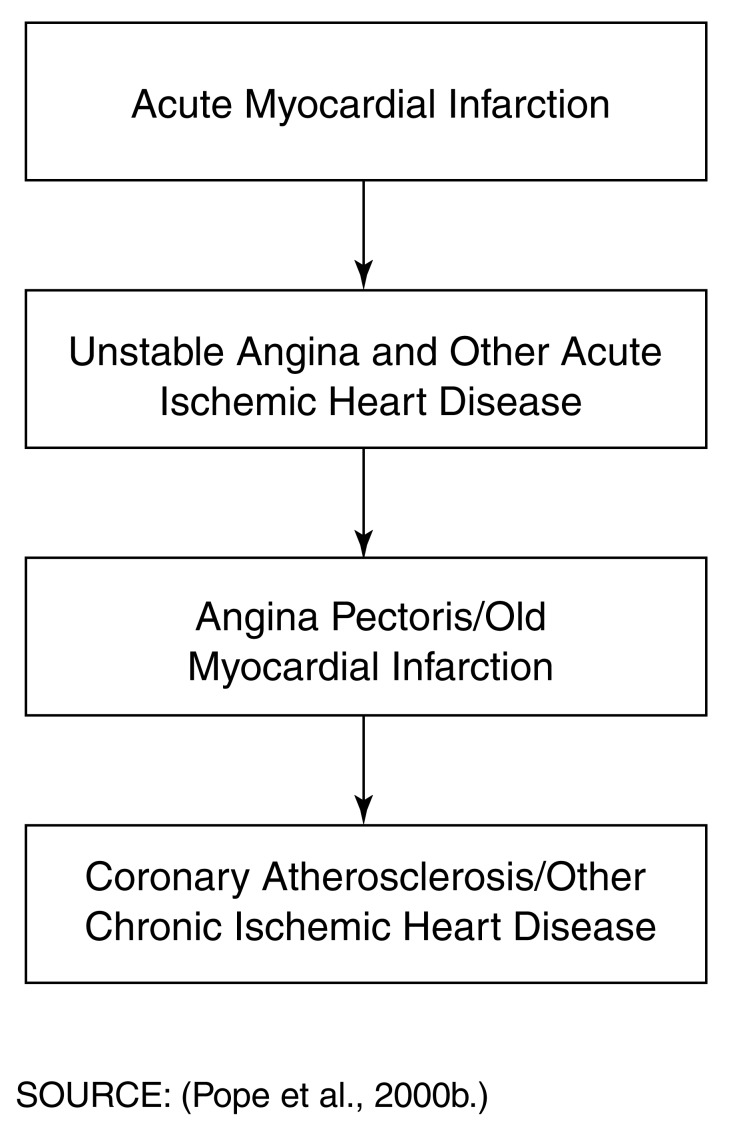
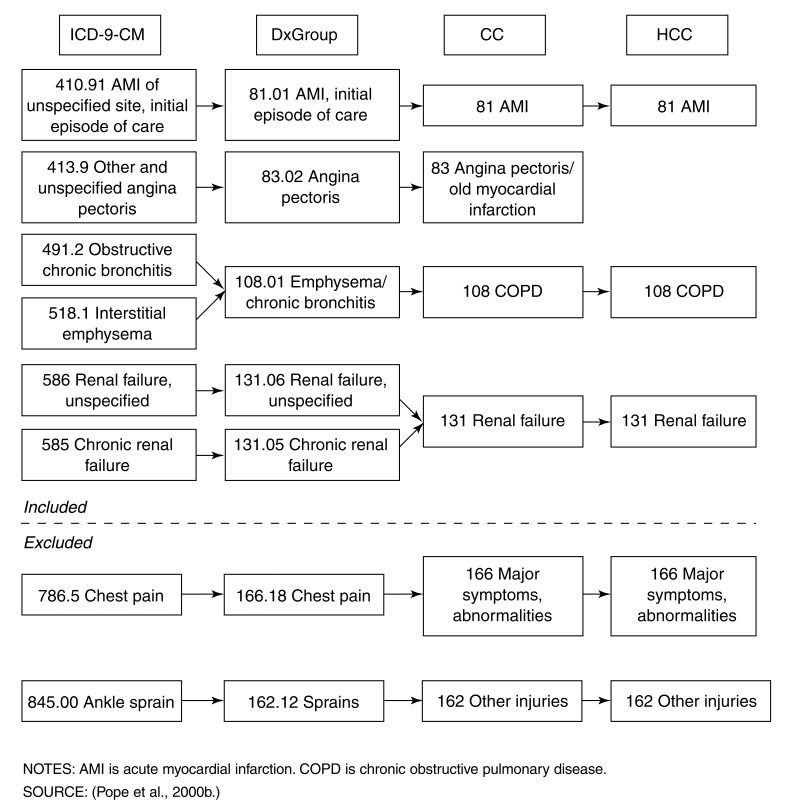
24 HCC, MEAT & Risk Adjustment
Hierarchical Condition Categories (HCCs) are the CMS risk adjustment system for Medicare Advantage and increasingly for ACOs and value-based contracts. Each HCC carries a relative weight that adjusts payment upward for sicker patients. Proper HCC capture depends on documentation, not just clinical truth — an undocumented diagnosis doesn't count.
The MEAT Criteria
For a chronic condition to count for HCC capture in a given year, the note must demonstrate that the condition was addressed. The mnemonic is MEAT:
| Letter | Criterion | Example |
|---|---|---|
| M | Monitored | "CKD stage 3 — Cr stable at 1.6, eGFR 42" |
| E | Evaluated | "T2DM — A1c reviewed, 7.2, improved from 7.8" |
| A | Assessed | "CHF — stable, NYHA II, no decompensation" |
| T | Treated | "COPD — continue tiotropium; albuterol prn" |
HCC capture resets every January 1. A chronic condition documented in 2025 that is not re-documented with MEAT criteria in 2026 drops off the patient's risk score for 2026. Every Medicare Advantage patient's annual wellness visit should systematically re-address all HCC diagnoses.
Common HCCs
| Condition | HCC Weight (relative) |
|---|---|
| Diabetes with chronic complications | Higher than uncomplicated DM |
| Major depressive disorder (recurrent) | Significant |
| Vascular disease with complications | High |
| CHF | High |
| Morbid obesity (BMI ≥40) | Significant |
| COPD | Moderate |
| CKD stage 4–5 | High |
| Metastatic cancer | Very high |
Query Process
When documentation is ambiguous or insufficient, hospital coders issue a query asking the physician to clarify. Queries must be non-leading — they cannot suggest a specific answer. A compliant query provides options; a non-compliant query hints at the desired answer.
25 EHR Pitfalls: Copy-Forward, Note Bloat & AI Tools
The EHR solved legibility and access but created a new set of documentation problems: copy-forward propagation of errors, note bloat, click fatigue, and template-driven homogeneity. These problems contribute to clinician burnout, patient safety events, and reduced clinical utility of notes.
Copy-Forward ("Copy-Paste") Issues
| Problem | Consequence |
|---|---|
| Stale exam findings | Carrying forward "abdomen soft, non-tender" from admission after patient develops peritonitis |
| Stale labs | Quoting admission Cr on day 5, missing AKI |
| Resolved problems remain | "Fever" on problem list for days after it resolved |
| Error propagation | A single mistyped history element copies forward indefinitely |
| Wrong patient data | Copy from another patient (always a sentinel event) |
1. Only copy-forward content you have verified.
2. Never copy-forward exam findings without re-examining.
3. Never copy-forward labs without checking for new results.
4. Update, don't just append — edit stale content out.
5. Some institutions now require physicians to attest they reviewed copied content.
Note Bloat
Modern EHR notes often run 4–10 pages for a simple encounter because templates auto-populate extensive data. This "note bloat" buries clinical reasoning in a sea of auto-generated text, making the note harder to read and less clinically useful. The 2021 E/M revision was partly motivated by the desire to reduce note bloat by eliminating bullet-counting requirements.
Templates & Dot Phrases
Templates and dot phrases (SmartPhrases in Epic, Auto-texts in Cerner) are double-edged: they save time but can create homogeneous, impersonal notes that gloss over unique patient features. Use templates for structure and standard language, but always add patient-specific content.
AI Documentation Tools
Ambient AI scribes (e.g., Nuance DAX, Abridge, Suki) record the patient encounter and generate draft notes via large language models. These tools can reduce documentation time by 50–75% but introduce new risks: hallucinations, omitted critical findings, and the need for vigilant clinician review and attestation. Every AI-drafted note should be reviewed and edited before signing.
Scribes
Human medical scribes accompany physicians to document in real time. Scribes improve physician efficiency and satisfaction but require training, oversight, and clear documentation of their role. Notes documented by a scribe must be reviewed, edited, and signed by the physician with an attestation that the content was reviewed.
26 Attestations, Addenda & Late Entries
Attending Attestation of Resident/Student Notes
When a resident or medical student writes a note, the supervising attending must write an attestation demonstrating personal involvement. Medicare requires the attending to have personally performed key elements (for teaching physicians) and to document their presence and agreement.
For office visits: "I have seen and examined the patient. I agree with the resident's findings and plan as documented above."
For procedures: "I was present for the entire procedure and personally performed the critical portions."
For critical care: "I have personally reviewed the patient, examined them, and participated in the management. I agree with the findings and plan."
Student Notes
Since 2018, medical student notes can be used for billing documentation as long as the teaching physician verifies and documents their presence and participation. Prior rules limited student contributions to ROS and PFSH.
Addendum vs. Amendment vs. Late Entry
| Type | Definition | When to Use |
|---|---|---|
| Addendum | Adding new information after the original note was signed | New test result available, additional clinical update |
| Amendment | Correcting or clarifying information in the original note | Typographical error, incorrect data |
| Late entry | Documenting an event that occurred earlier but was not documented at the time | Forgotten verbal order; retrospective documentation |
Proper Addendum/Amendment Format
Never delete or overwrite original content. All modifications must be time-stamped, dated, and identified as addenda or amendments. A correctly labeled late entry is honest and defensible; an undisclosed retroactive edit is legally indefensible and potentially fraudulent.
"Addendum 4/4/26 1445: Blood cultures drawn on admission 4/2/26 have resulted as positive for MSSA in 2/2 bottles. Infectious Disease consulted; antibiotics changed to cefazolin. Echocardiogram ordered to assess for endocarditis. — Dr. Smith"
27 Reference: Do-Not-Use List, Sample Notes & Pearls
The Joint Commission Official "Do Not Use" List
These abbreviations have been implicated in actual patient harm and are prohibited in medical documentation at Joint Commission–accredited facilities.
| Do Not Use | Reason | Use Instead |
|---|---|---|
| U, u (unit) | Mistaken for "0," "4," or "cc" | Write "unit" |
| IU (international unit) | Mistaken for IV (intravenous) or 10 | Write "International Unit" |
| Q.D., QD, q.d., qd (daily) | Mistaken for each other; period after Q mistaken for I | Write "daily" |
| Q.O.D., QOD, q.o.d, qod (every other day) | Mistaken for "daily" or "qid" | Write "every other day" |
| Trailing zero (X.0 mg) | Decimal point missed → 10-fold overdose | Write "X mg" |
| Lack of leading zero (.X mg) | Decimal point missed → 10-fold overdose | Write "0.X mg" |
| MS, MSO4, MgSO4 | Confusion between morphine sulfate and magnesium sulfate | Write "morphine sulfate" or "magnesium sulfate" |
Additional High-Risk Abbreviations (ISMP)
| Avoid | Confused With | Use |
|---|---|---|
| μg (microgram) | mg (milligram) → 1000-fold error | "mcg" or "microgram" |
| cc (cubic centimeter) | U (units) | "mL" |
| D/C | Discharge or discontinue | Write out the intent |
| h.s. | Half-strength or hour of sleep | "at bedtime" |
| SC, SQ | Sublingual or "5 every" | "subcut" or "subcutaneously" |
Common Documentation Pitfalls
- Cloning — Identical notes across multiple patients or encounters (audit red flag).
- Chart lore — Uncorrected incorrect history that propagates indefinitely.
- Over-coding — Billing a higher level than documentation supports.
- Under-coding — Failing to capture work actually performed (costs thousands per year).
- Template-only documentation — Notes that read identically for every patient.
- Phantom physical exams — Template exam findings for systems not actually examined.
- Unsigned/unauthenticated notes — Creating legal ambiguity about the author.
Telehealth Documentation
Telehealth visits require specific elements: modality (audio + video or audio only), patient location, physician location, patient consent to telehealth, and any limitations on the encounter (e.g., "physical exam limited to visual inspection"). Use modifier -95 for synchronous audio-video and place of service code 10 (patient home) or 02 (other telehealth).
Controlled Substance Documentation
| Element | Documentation |
|---|---|
| Indication | Specific condition being treated |
| Treatment plan | Dose, quantity, refills, duration |
| Risk–benefit discussion | With patient, documented |
| PDMP check | State prescription monitoring program reviewed |
| Urine drug screen | Baseline and periodic for chronic opioid therapy |
| Opioid treatment agreement | Signed when appropriate |
| Naloxone offered | For high-risk patients per CDC guidelines |
| Functional goals | Specific, measurable improvements tracked |
Audit-Proof Documentation Tips
- Write for the skeptical reviewer. Assume an auditor will read your note looking for inconsistencies.
- Be specific, not vague. "Counseled on diabetes" is weaker than "Discussed target A1c of 7%, importance of daily glucose monitoring, and signs of hypoglycemia."
- Time stamps matter. If you say you spent 40 minutes, write down the activities that took 40 minutes.
- Match code to content. If you bill 99214, ensure two of three MDM elements reach moderate complexity.
- Document shared decisions. "Discussed X and Y; patient chose X after understanding Z" is bulletproof.
- Document what you didn't do and why. "Imaging deferred given low pre-test probability and patient preference."
- Sign and authenticate promptly. An unsigned note is a liability.
The Ten Commandments of Medical Documentation
1. Write legibly (or type accurately).
2. Document contemporaneously.
3. Be objective and neutral.
4. Document what you see, think, and do — and why.
5. Never alter a note; use addenda.
6. Include pertinent negatives to show clinical reasoning.
7. Document shared decision-making explicitly.
8. Code honestly — not too high, not too low.
9. Protect patient privacy; follow HIPAA.
10. Remember: the note is the patient's story, the team's roadmap, and your legal record all at once.
Sample Complete Outpatient SOAP Note
CC: "Follow-up diabetes and blood pressure."
S: Ms. Taylor is a 58-year-old woman with T2DM (diagnosed 2018), essential hypertension, and hyperlipidemia returning for routine follow-up. She reports feeling well overall. Home fasting glucose values have been 120–145 mg/dL. No episodes of hypoglycemia. No polyuria, polydipsia, or blurred vision. Home BP log shows average 132/82. Adherent to metformin 1000 mg BID, lisinopril 20 mg daily, atorvastatin 40 mg QHS. No cough from lisinopril. Walking 20 minutes 4 days per week. Diet remains a challenge; reports increased snacking in evenings. Last eye exam 8 months ago (normal). Last foot exam by podiatry 4 months ago. No chest pain, dyspnea, or edema.
ROS: Negative except as noted above.
O: Vitals: BP 134/82, HR 74, RR 14, T 36.8, BMI 31.2 (weight 182 lb). General: well-appearing, NAD. Cardiovascular: RRR, no murmurs, no JVD, no peripheral edema, DP/PT pulses 2+ bilaterally. Pulmonary: clear bilaterally. Abdomen: soft, non-tender, no organomegaly. Extremities: monofilament intact at all sites bilaterally, no ulcerations, skin integrity intact. Labs today: A1c 7.1 (down from 7.4 three months ago), BMP with Cr 0.9 (baseline), K 4.2, LDL 78.
A/P:
1. Type 2 diabetes mellitus without complications (E11.9) — Improving control, A1c 7.1, meeting individualized target. Continue metformin 1000 BID. Reviewed diet, emphasized evening snacking reduction; provided written resources. Annual eye exam current; next foot exam in 8 months. Pneumococcal and influenza vaccines up to date. Continue home glucose monitoring.
2. Essential hypertension (I10) — Above goal of <130/80 for patient with DM. BP today 134/82, home average 132/82. Will increase lisinopril to 30 mg daily. Discussed DASH diet and sodium restriction. Recheck home BP in 4 weeks; patient to notify if systolic >150 or diastolic >95.
3. Hyperlipidemia (E78.5) — LDL 78 on atorvastatin 40, at goal for ASCVD risk. No myalgias. Continue current therapy.
4. Obesity, BMI 31.2 (E66.9, Z68.31) — Counseled on weight loss goal of 5–10% body weight. Discussed nutritional referral; patient interested. Referral placed.
5. Health maintenance — Mammogram due next month (order placed); colonoscopy current (2024, normal); Tdap due this year (given today). Reviewed age-appropriate screening.
Total time on date of service: 32 minutes including chart review, patient interview, physical exam, clinical decision-making, medication adjustment, counseling, order entry, and documentation.
Billing: 99214 (moderate MDM: 2 stable chronic conditions + medication management of HTN).
Follow-up: 3 months with A1c, BMP, lipid panel.
Sample Inpatient Progress Note
Mr. Patel, 72-year-old man, HD3 for community-acquired pneumonia.
S: Overnight: slept well, no fevers reported by nursing. This morning reports cough improved, productive of smaller amounts of sputum. Appetite improving, tolerated full breakfast. No chest pain or dyspnea at rest; mild dyspnea with ambulation to bathroom. Ambulated with PT yesterday 100 feet with supervision.
O: Vitals (24h): Tmax 37.6 (down from 38.4), Tcurrent 37.1, HR 72–88, BP 118–138/68–82, RR 16–20, SpO2 94–96% on 2L NC (weaned from 3L yesterday). I/O 24h: 2100/2250 (net −150). Exam: alert, NAD. Lungs: decreased breath sounds and crackles RLL, improved from admission; left clear. Cardiovascular: RRR, no murmurs, no edema. Abdomen benign. Labs (AM): WBC 10.8 (down from 14.2 admission, 12.6 yesterday), Cr 0.9 (baseline), Na 138, K 4.0. Blood cultures ×2 no growth at 48h. CXR yesterday: interval improvement in RLL infiltrate. Antibiotic day: ceftriaxone + azithromycin day 3/7.
A/P: 72-year-old man with CAP, clinically improving with appropriate response to therapy.
1. CAP, RLL — Clinically and radiographically improving. Continue ceftriaxone 1 g IV daily and azithromycin 500 mg IV daily (day 3/7). Plan to transition to oral levofloxacin tomorrow if continued improvement and afebrile × 24h.
2. Hypoxemia — Improving; weaned from 3L to 2L. Goal to wean to RA prior to discharge. Incentive spirometer q1h while awake.
3. HTN — Resumed home lisinopril 10 mg daily today.
4. DVT prophylaxis — Enoxaparin 40 mg subcut daily, continues.
5. Nutrition — Regular diet, tolerating well.
6. Disposition — Anticipate discharge tomorrow or the following day once off supplemental O2, on oral antibiotics, and afebrile. PCP follow-up arranged for 1 week post-discharge. Home with daughter, no placement needs.
Code status: Full code, confirmed with patient.
Red Flag Phrases to Avoid
| Avoid | Why |
|---|---|
| "Apparently" | Suggests uncertainty about your own observations |
| "No acute findings" | Vague; does not document what was actually assessed |
| "Stable" | Meaningless without context; stable compared to what? |
| "Will follow" | Vague; specify what, when, by whom |
| "Unable to obtain history" | Document attempts and barriers; use collateral sources |
| "WNL" (within normal limits) | Sometimes read as "we never looked"; be specific |
| "Non-contributory" | Implies you didn't ask; specify what was reviewed |
Final Note on Professional Development
Documentation is a skill that improves with deliberate practice over an entire career. Early-career physicians often over-document out of caution; mid-career physicians sometimes under-document from fatigue; experienced physicians write concise, clinically rich notes that tell the patient's story efficiently. The goal is not the longest note or the shortest note — it is the most useful note, written for all of the audiences who depend on it. Review your own notes periodically, read notes by clinicians you admire, and solicit feedback from coders and colleagues. Excellence in documentation is invisible when done well but catastrophic when done poorly.
Quick-Reference Documentation Checklist by Note Type
| Note Type | Must-Include Elements |
|---|---|
| Admission H&P | CC, HPI, PMH/PSH, meds, allergies, FH, SH, ROS, exam, data, assessment with differential, plan by problem, code status, disposition plan |
| Daily progress note | HD#, overnight events, interval history, vitals range, I/O, focused exam, new data, A/P by problem, antibiotic day, DVT ppx, disposition |
| Discharge summary | Dates, principal/secondary diagnoses, hospital course, procedures, discharge meds, pending results, follow-up, condition, instructions |
| Procedure note | Pre/post-op diagnosis, procedure, indication, consent, time-out, anesthesia, technique, findings, specimens, EBL, complications, disposition |
| Consult note | Reason for consult, focused HPI, relevant exam, data reviewed, impression, numbered recommendations |
| ED note | Arrival mode, triage vitals, focused HPI, MDM with differential, serial exams, re-evaluation, disposition, return precautions |
| Office visit | CC, focused history, medically appropriate exam, labs/data, A/P by problem, time or MDM-based E/M, follow-up |
| Telephone encounter | Who/when, reason, assessment, advice, disposition, verification of understanding |
| Death note | Time called, physical findings confirming death, time of death, family notified, attending notified, ME/autopsy status |
| Code note | Times, trigger, pre-event status, initial exam, interventions with times, response, outcome, team, family communication |
The Future of Medical Documentation
The next decade will transform documentation through ambient AI, voice recognition, automated coding, and structured-data capture. As these tools mature, the clinician's role will shift from creating notes to curating and attesting to AI-generated drafts. The core skills described in this reference — clinical reasoning, accuracy, appropriate specificity, objective language, and thoughtful synthesis — will remain essential regardless of the underlying technology. The physician who understands why a note is structured the way it is will always write (or approve) better notes than the physician who simply fills in a template.