Forensic Medicine
Cause and manner of death, medicolegal death investigation, autopsy techniques, forensic toxicology, injury pattern analysis, time-of-death estimation, mass disaster response, and every classification system, legal standard, and investigative method across the full scope of forensic medicine.
01 Medicolegal System & Death Investigation
The medicolegal death investigation system determines the cause and manner of death in cases that fall under statutory jurisdiction. In the United States, two parallel systems exist: the medical examiner system and the coroner system. Approximately 20 states use a medical examiner model, 14 use a coroner model, and the remainder use a mixed system. Understanding jurisdictional authority is essential because it dictates who has legal power to order an autopsy, take custody of the body, and issue the death certificate.
Medical Examiner vs Coroner Systems
| Feature | Medical Examiner | Coroner |
|---|---|---|
| Qualification | Board-certified forensic pathologist (MD/DO) with fellowship training | Elected official; physician qualification not required in most jurisdictions |
| Selection | Appointed by government authority | Elected by public vote (typically 2–4 year terms) |
| Authority | Performs or supervises autopsies directly | May contract forensic pathologists; authority varies by state |
| Jurisdiction | State or county level | County level (rarely statewide) |
| Death certification | Signs death certificate for cases under jurisdiction | May sign or delegate to physician |
| Quality standard | NAME accreditation available | Variable; no uniform accreditation standard |
Reportable Deaths
Specific categories of death must be reported to the medical examiner or coroner. While statutes vary by jurisdiction, the following are nearly universally reportable:
Violent deaths: homicide, suicide, accident (including motor vehicle, falls, drowning, fire, poisoning). Sudden/unexpected: death occurring in apparent good health without medical attendance within 24 hours. Unattended: no physician present and no recent medical care. Custody deaths: jails, prisons, police encounters, psychiatric facilities. Suspicious/unusual: circumstances suggesting foul play, unexpected or unusual manner. Public health threat: deaths that may represent occupational hazards, communicable diseases of public health significance, or environmental exposures. Operative/perioperative: death during or within 24 hours of surgery or anesthesia. Pediatric: all deaths of children under a certain age (typically <3 years in many jurisdictions). Unidentified bodies.
Scene Investigation
The medicolegal death investigator (MLI) is typically the first representative of the medical examiner/coroner office to respond to the scene. The MLI documents environmental conditions (ambient temperature, heating/cooling status, body position, presence of medications, drug paraphernalia, suicide notes, weapons), obtains witness statements, reviews medical records, photographs the scene and body in situ, and ensures preservation of evidence. The investigator notes the degree of rigor mortis, livor mortis distribution and fixation, body temperature (rectal or liver probe), and any signs of decomposition. Scene findings are critically important for determining manner of death and often provide information unavailable at autopsy alone.
Chain of Custody
Chain of custody refers to the documented chronological record of who has had possession of evidence from the time of collection through final disposition. Every transfer of evidence (body, clothing, projectiles, toxicology specimens, sexual assault kits) must be documented with the name of the person relinquishing, the name of the person receiving, date, time, and condition of the evidence. Breaks in chain of custody may render evidence inadmissible in court.
Key Personnel in Forensic Death Investigation
| Role | Training | Primary Responsibilities |
|---|---|---|
| Forensic pathologist | MD/DO + anatomic pathology residency + forensic pathology fellowship (1 year) | Performs autopsies, determines cause and manner of death, provides expert testimony |
| Medicolegal death investigator | Varies; ABMDI certification available (registry exam) | Scene investigation, body identification, medical record review, family notification |
| Forensic toxicologist | PhD in toxicology or related field; ABFT certification | Specimen analysis, drug/poison identification and quantitation, interpretive consultation |
| Forensic anthropologist | PhD in physical/biological anthropology; ABFA diplomate | Skeletal analysis for identification, trauma assessment, PMI estimation in decomposed/skeletal remains |
| Forensic odontologist | DDS/DMD with forensic dentistry training; ABFO diplomate | Dental identification, bite mark analysis, age estimation |
| Forensic entomologist | PhD in entomology | Insect evidence collection and analysis for PMI estimation |
02 Cause & Manner of Death
Precise determination of cause and manner of death is the central obligation of the forensic pathologist. These two concepts are distinct: cause of death identifies the disease, injury, or event that initiated the chain of pathophysiologic events leading to death, while manner of death classifies the circumstances under which the cause arose.
Cause of Death Hierarchy
The cause of death is recorded as a sequential chain on the death certificate (Part I, lines a through d):
| Level | Definition | Example |
|---|---|---|
| Immediate cause (line a) | The final disease/condition directly causing death | Pulmonary thromboembolism |
| Due to / consequence of (line b) | Sequentially antecedent condition | Deep venous thrombosis, right lower extremity |
| Due to / consequence of (line c) | Sequentially antecedent condition | Immobilization following hip fracture |
| Underlying (proximate) cause (line d) | The initiating event or disease that started the lethal sequence | Fall from height |
Part II of the death certificate lists other significant contributing conditions that contributed to death but were not part of the direct causal chain (e.g., diabetes mellitus, chronic obstructive pulmonary disease, coronary artery disease). The underlying cause of death (lowest completed line in Part I) is the basis for mortality statistics compiled by the National Center for Health Statistics.
Mechanism of death describes the physiological derangement by which the cause exerts its lethal effect (e.g., cardiac arrhythmia, exsanguination, sepsis, respiratory failure). Mechanism is not a valid cause of death on the death certificate because it is nonspecific — many different diseases and injuries can produce the same mechanism. A death certificate listing "cardiopulmonary arrest" as the sole cause of death is incomplete and uninformative: every death involves cardiopulmonary arrest.
Manner of Death — The Five Categories
| Manner | Definition | Examples |
|---|---|---|
| Natural | Death caused solely by disease processes without external contribution | Myocardial infarction, ruptured cerebral aneurysm, pneumonia, cancer |
| Accident | Death resulting from an unintentional injury or event | Motor vehicle collision, unintentional drug overdose, fall, drowning |
| Suicide | Death resulting from intentional self-inflicted injury with intent to die | Self-inflicted gunshot wound, hanging, intentional drug ingestion, jumping |
| Homicide | Death at the hand of another person; implies volitional act but does not necessarily imply criminal intent | Stabbing, shooting, strangulation, assault; also includes lawful intervention (police shooting) |
| Undetermined | Evidence is insufficient to classify into another category after thorough investigation | Drug death with unknown intent, decomposed body with limited evidence, equivocal circumstances |
Death Certification
The U.S. Standard Certificate of Death is a legal document used for vital statistics, insurance claims, estate settlement, and epidemiologic surveillance. Key principles for completing the certificate: (1) the cause-of-death statement must be etiologically specific (never "cardiac arrest" alone); (2) the sequence must be logically consistent with "due to" progressing from immediate to underlying; (3) the approximate interval between onset and death should be recorded for each line; (4) the manner-of-death checkbox should be completed for every death; (5) injury deaths require completion of the injury section (date, time, place, how injury occurred, whether work-related).
Pending Determinations
When initial autopsy findings do not establish cause of death, the case is pended awaiting toxicology results, histology, cultures, or further investigation. Pending cases should be resolved within 90 days when possible. A cause of death may remain "undetermined" after all studies are complete if no definitive etiology is established. Manner may also remain undetermined independently of cause.
Common Errors in Death Certification
Studies consistently demonstrate high error rates in death certificate completion: using mechanism rather than cause of death ("cardiac arrest" or "respiratory failure" without an underlying disease), illogical causal sequences (placing the underlying cause on line a instead of the last line), omitting the manner of death, failure to complete the injury section for non-natural deaths, and listing multiple unrelated conditions on the same causal chain. The CDC and state vital registrars provide training resources and query letters to correct deficient certificates. Accurate death certification directly affects public health surveillance, mortality statistics, and resource allocation.
Correct: Line a: Pulmonary thromboembolism (minutes). Line b: Deep venous thrombosis, right lower extremity (days). Line c: Immobilization following right hip fracture (weeks). Line d: Fall from ladder (months). Manner: Accident. Incorrect: Line a: Cardiopulmonary arrest. This tells the reader nothing — all deaths involve cardiopulmonary arrest. The cause of death is the disease or injury that initiated the lethal sequence, not the terminal physiological event.
03 Thanatology — Postmortem Changes & Time of Death
Thanatology is the scientific study of death and the changes that occur after death. Estimating the postmortem interval (PMI) — the time elapsed since death — relies on a combination of physical, chemical, and biological markers. No single finding provides a precise PMI; all methods yield an estimated range that narrows when multiple parameters are integrated together.
Algor Mortis (Postmortem Cooling)
Algor mortis is the progressive cooling of the body toward ambient temperature after death. Core body temperature (measured rectally or by hepatic probe) decreases at a rate influenced by body habitus, clothing, ambient temperature, air movement, and immersion. The classical rule of thumb is a drop of approximately 1.5°F (0.83°C) per hour, but this is highly variable. The Henssge nomogram (1988, revised 2004) provides a more accurate mathematical model using body weight, rectal temperature, and ambient temperature to estimate PMI. The nomogram incorporates corrective factors for clothing, wind, wetness, and body habitus. An initial temperature plateau of 0.5–3 hours (the sigmoid lag phase) occurs before exponential cooling begins, especially in well-insulated or obese decedents.
Livor Mortis (Hypostasis)
Livor mortis (lividity) is the gravitational settling of blood into dependent capillaries and venules after cessation of circulation. It appears as a reddish-purple discoloration of the skin in the dependent portions of the body. Livor mortis becomes visible within 30 minutes to 2 hours of death. It is initially unfixed (blanches with pressure and redistributes when the body is repositioned). Fixation occurs at approximately 8–12 hours postmortem as hemoglobin diffuses out of decomposing erythrocytes into the surrounding interstitial tissues, rendering lividity permanent and non-blanchable.
Distribution of lividity helps establish body position after death. Discordant lividity — livor mortis inconsistent with the position in which the body is found — suggests the body was moved after fixation. Contact pallor (areas of absent lividity where the body rests against a firm surface) and Tardieu spots (punctate areas of intense lividity from capillary rupture) are additional features to document.
Cherry-red: carbon monoxide poisoning (carboxyhemoglobin), cyanide poisoning, or cold environments (reduced oxygen dissociation). Pink/bright red: bodies refrigerated or exposed to cold. Brown/chocolate: methemoglobinemia (nitrites, dapsone). Dark/deep purple: typical postmortem lividity. The color of lividity can provide the first clue to the presence of a toxic exposure at the scene, before any laboratory testing.
Rigor Mortis
Rigor mortis is the progressive stiffening of skeletal muscles after death due to depletion of ATP, which is required for myosin-actin cross-bridge release. The classical timeline is: onset at 2–4 hours postmortem, progressing from small muscles (eyelids, jaw) to large muscles (extremities) over 6–12 hours; maximum rigidity at approximately 12 hours; gradual resolution at 24–48 hours as autolysis and decomposition degrade the myofilament proteins.
| Phase | Approximate Time (temperate 20°C) | Characteristics |
|---|---|---|
| Absent | 0–2 hours | Muscles flaccid; joints freely movable |
| Developing | 2–6 hours | Stiffness begins in jaw, eyelids, neck; progresses caudally (Nysten's rule) |
| Full rigor | 6–12 hours | All muscle groups rigid; joints immovable |
| Maximum | 12–24 hours | Peak rigidity throughout the body |
| Resolution | 24–48 hours | Flaccidity returns in same sequence as onset; due to autolytic protein degradation |
Accelerating factors include high ambient temperature, vigorous ante-mortem exercise (depleted ATP stores), convulsions, electrocution, and low body mass. Cadaveric spasm (instantaneous rigor) is an extremely rare phenomenon where a single muscle group (typically the hand gripping an object) enters immediate rigor at the moment of death, associated with intense emotional or physical activity — it cannot be reproduced artificially and is therefore a reliable indicator that the object was held at the moment of death.
Broken rigor: If rigor is manually overcome (by forcibly moving a joint) before resolution has occurred, it will not reform in small muscles but may partially reform in large muscle groups if ATP reserves remain. This finding indicates the body was moved or manipulated postmortem. Cold stiffening: In freezing environments, tissue freezing produces stiffness that mimics rigor mortis — but it resolves upon thawing, unlike true rigor which resolves through decomposition. Heat stiffening: Exposure to high temperatures causes protein denaturation and coagulation of muscle fibers, producing permanent rigidity that does not resolve (distinguished from rigor by the history and the cooked/pale appearance of musculature). Drug effects: Strychnine poisoning can produce ante-mortem opisthotonic rigidity that persists after death due to depleted ATP from sustained muscle contraction.
Stages of Decomposition
| Stage | Approximate Time | Features |
|---|---|---|
| Fresh | 0–2 days | Algor, livor, and rigor mortis present; no visible decomposition; autolysis begins internally |
| Bloat (Early decomposition) | 2–6 days | Green discoloration of right lower quadrant (cecal bacteria), gaseous distension, marbling (vascular pattern from hemoglobin degradation), skin slippage, purging of fluid from orifices |
| Active decay | 6–10 days | Mass loss from tissue liquefaction and insect activity; skin rupture; strong odor; organs unrecognizable grossly |
| Advanced decay | 10–25 days | Majority of soft tissue gone; cartilage and ligaments remain; bones partially exposed |
| Skeletonization | >25 days (variable) | Only bone, desiccated tissue remnants, and hair remain; timeline highly dependent on environment |
Special decomposition variants: Adipocere (grave wax) is formed by hydrolysis and hydrogenation of adipose tissue into fatty acid salts in wet, anaerobic environments; onset at 3–4 weeks, fully developed by months. Mummification occurs in hot, dry, well-ventilated environments where rapid desiccation outpaces bacterial decomposition, preserving external features. Saponification is a synonym for extensive adipocere formation.
Forensic Entomology
Insects colonize remains in a predictable ecological succession. Calliphora (blowflies) and Lucilia (greenbottle flies) are typically the first colonizers, arriving within minutes of death in outdoor settings and ovipositing in natural body orifices and wounds. The developmental rate of fly larvae (maggots) through egg → 1st instar → 2nd instar → 3rd instar → prepupa → pupa → adult is temperature-dependent and can be calculated using accumulated degree hours/days (ADH/ADD) to estimate a minimum PMI. Later succession waves include Sarcophagidae (flesh flies, larviparous), Dermestidae (skin beetles, in advanced decay), and Piophilidae (cheese skippers). Insect evidence must be collected alive (for rearing) and preserved (in 80% ethanol or hot water then ethanol) at the scene and at autopsy.
Vitreous Potassium for PMI Estimation
After death, potassium leaks from intraocular cells into the vitreous humor at a relatively predictable rate. The vitreous potassium concentration rises approximately linearly with PMI for the first 100–120 hours. Various regression formulas exist (Sturner, Madea, Munoz), with Madea's formula being the most widely cited: PMI (hours) = 5.26 × [K+] – 30.9 (with a 95% confidence interval of approximately ±10 hours). Limitations include temperature dependence, inter-individual variability, and unreliability beyond 5 days or in decomposed remains.
Other Chemical Markers of PMI
Beyond vitreous potassium, several additional postmortem biochemical markers have been investigated: vitreous hypoxanthine (a purine degradation product) rises linearly with PMI and may be more accurate than potassium in the first 24 hours. Cerebrospinal fluid electrolytes show similar trends to vitreous but are more susceptible to contamination. Synovial fluid potassium from the knee joint rises more slowly than vitreous potassium and may extend the useful window. Hydrogen sulfide in decomposition gases and volatile fatty acids in decomposition fluid have been proposed for PMI estimation in advanced decomposition. No single chemical marker has replaced the multimodal approach to PMI estimation.
Accelerating: High ambient temperature, high humidity, outdoor exposure to insects, obesity (insulating effect retains heat; large gut flora inoculum), sepsis (high bacterial load), open wounds (insect access points), and absence of embalming. Decelerating: Cold temperature (refrigeration, winter, cold water immersion), dry environment (desiccation/mummification), burial (reduced insect access), clothing (partial barrier to insects), embalming. Casper's dictum: Decomposition in air is approximately twice as fast as in water and eight times as fast as in soil (1:2:8 ratio for equivalent decomposition at the same temperature).
04 Key Terminology & Abbreviations
Forensic medicine spans pathology, toxicology, law enforcement, and the legal system, producing a dense specialized vocabulary. Mastering these terms is essential for report writing, courtroom communication, and interdisciplinary collaboration. The following tables compile essential terms and abbreviations encountered throughout forensic practice.
Core Forensic Pathology Terms
| Term | Definition |
|---|---|
| Antemortem | Before death |
| Perimortem | At or around the time of death (used particularly in bone trauma analysis) |
| Postmortem | After death |
| Artifact | Postmortem change mimicking antemortem injury (e.g., thermal fractures, animal predation) |
| Autolysis | Enzymatic self-digestion of cells after death without bacterial involvement |
| Putrefaction | Bacterial decomposition of tissues producing gas and discoloration |
| Exsanguination | Death from blood loss |
| Contrecoup | Injury on the side opposite the point of impact (especially brain contusions) |
| Coup injury | Injury at the point of impact |
| Petechiae | Pinpoint hemorrhages (<2 mm) indicating capillary rupture; seen in conjunctivae, skin, and visceral surfaces in asphyxia |
| Tardieu spots | Punctate hemorrhages in areas of dependent lividity from capillary rupture due to gravitational stasis |
| Vitality / Vital reaction | Evidence that a wound was inflicted during life (hemorrhage, inflammation, soot aspiration) |
| Patterned injury | Injury whose morphology reflects the object that caused it |
| Defense wound | Injury on hands, forearms, or arms sustained while attempting to ward off an attack |
| Hesitation mark | Superficial, tentative, parallel incised wounds near a deeper fatal wound, suggesting self-infliction |
| Stellate wound | Star-shaped laceration (e.g., contact gunshot wound over bone from expanding muzzle gases) |
| Avulsion | Forcible separation or tearing away of tissue from its attachments |
| Incised wound | Clean-cut wound longer than deep, produced by a sharp edge drawn across tissue |
| Stab wound | Clean-cut wound deeper than long, produced by a pointed instrument thrust into tissue |
| Laceration | Irregular wound with torn/ragged edges and bridging vessels, caused by blunt force |
| Abrasion | Superficial injury from friction or scraping that removes the epidermis |
| Contusion | Bruise; hemorrhage into tissue from blunt force rupturing blood vessels |
| Ecchymosis | Large area of subcutaneous hemorrhage (>1 cm) |
| Purpura | Hemorrhagic discoloration 3 mm to 1 cm |
| Marbling | Postmortem venous discoloration pattern from hemoglobin diffusion through decomposing vessel walls |
| Skin slippage | Separation of epidermis from dermis due to decomposition; sheets of epidermis peel away |
| Vitreous | Gelatinous fluid filling the posterior chamber of the eye; used for postmortem chemistry |
| Adipocere | "Grave wax"; waxy transformation of adipose tissue in wet anaerobic environments |
| Mummification | Desiccation and preservation of tissues in dry, well-ventilated environments |
Common Abbreviations
| Abbreviation | Meaning |
|---|---|
| ME / C | Medical examiner / coroner |
| MLI | Medicolegal death investigator |
| COD / MOD | Cause of death / manner of death |
| PMI | Postmortem interval |
| TOD | Time of death |
| GSW | Gunshot wound |
| BFI / SFI | Blunt force injury / sharp force injury |
| COHb | Carboxyhemoglobin |
| BAC | Blood alcohol concentration |
| GC-MS | Gas chromatography–mass spectrometry |
| LC-MS/MS | Liquid chromatography–tandem mass spectrometry |
| SIDS / SUID | Sudden infant death syndrome / sudden unexpected infant death |
| DVI | Disaster victim identification |
| NAME | National Association of Medical Examiners |
| ABMDI | American Board of Medicolegal Death Investigators |
| ABFT | American Board of Forensic Toxicology |
| STR | Short tandem repeat (DNA profiling) |
| CODIS | Combined DNA Index System |
| SAFE / SANE | Sexual assault forensic examiner / sexual assault nurse examiner |
| PMCT | Postmortem computed tomography |
| ADH / ADD | Accumulated degree hours / accumulated degree days (entomology) |
| ACE-V | Analysis, Comparison, Evaluation, Verification (fingerprint methodology) |
| AFIS | Automated Fingerprint Identification System |
| AHT | Abusive head trauma |
| ASSB | Accidental suffocation and strangulation in bed |
| ABFO | American Board of Forensic Odontology |
| ABFA | American Board of Forensic Anthropology |
| CML | Classic metaphyseal lesion |
| DMORT | Disaster Mortuary Operational Response Team |
| NAT | Non-accidental trauma |
| PMMR | Postmortem magnetic resonance imaging |
| SEM-EDX | Scanning electron microscopy with energy-dispersive X-ray analysis |
| GSR | Gunshot residue |
05 External Examination
The external examination is conducted before any incision and is arguably the most important phase of the forensic autopsy. It documents the identity of the decedent, the condition of the body, all external injuries, evidence of medical intervention, and any trace evidence. Meticulous external examination prevents the loss of fragile evidence that may be disturbed during internal dissection.
Clothing & Personal Effects
All clothing is examined before removal. Documentation includes: type, color, condition, presence of tears/defects (correlated with underlying injuries), bloodstain patterns, gunshot residue, projectile holes (measured and correlated with body wounds), and any foreign material (soil, glass, fibers). Clothing is dried at room temperature if wet, then packaged individually in paper bags (never plastic, to prevent mold and degradation of biological evidence). Jewelry, identification documents, and personal effects are inventoried and secured.
Identification
Positive identification of the decedent is a legal prerequisite before the death certificate is issued. Methods in order of reliability:
| Method | Reliability | Notes |
|---|---|---|
| Fingerprints | Positive (if antemortem prints available) | Compared against AFIS database or known prints; skin reconditioning techniques for decomposed fingers |
| Dental comparison | Positive | Requires antemortem dental records; unique dental restorations, morphology, radiographic comparison |
| DNA | Positive | STR profiling compared with known reference sample or family member; gold standard for decomposed/fragmented remains |
| Radiographic comparison | Positive (when unique features present) | Frontal sinus pattern, orthopedic hardware, healed fractures with known films |
| Visual identification | Presumptive only | High error rate; not accepted as sole method; family identification under stress is unreliable |
| Serial numbers (implants) | Presumptive to positive | Pacemakers, orthopedic devices with traceable serial numbers |
Body Surface Examination
The entire body surface is examined systematically from head to toe, anterior and posterior, with documentation of: rigor mortis (present/absent, distribution, whether broken), livor mortis (distribution, fixed vs unfixed, color), decomposition (stage, distribution), height and weight, eye color and pupil size, hair color and length, tattoos (description and location), scars (surgical, traumatic), identifying marks (birthmarks, moles, deformities), and medical devices (endotracheal tubes, IV lines, Foley catheters — left in place and documented).
Injury Documentation
Every external injury is described by type (abrasion, contusion, laceration, incised wound, gunshot wound), anatomic location (referenced to a fixed landmark such as the vertex or heel), size (measured in centimeters), shape, depth, orientation, color, margins (smooth vs irregular), and presence of foreign material. Photography includes: overall body views, mid-range views showing anatomic context, and close-up views with a ruler/scale. Body diagrams (front, back, right, left, head) are annotated with injury locations. Wound documentation must be sufficient for another forensic pathologist to independently evaluate the findings from the report alone.
Evidence Collection
Trace evidence collection occurs during external examination: fingernail clippings/scrapings (for assailant DNA), swabs (oral, vaginal, anal, penile for sexual assault cases), hair combings and standards, gunshot residue sampling (hands, if not already done at scene), blood standard (for DNA and toxicology), and any foreign material (fibers, glass, vegetation). Each item is packaged separately with chain-of-custody documentation.
In homicide cases with suspected sexual assault, the autopsy protocol includes: oral, vaginal (or penile), and anal/rectal swabs collected before internal examination; pubic hair combings; fingernail clippings/scrapings; bite mark documentation (swabs for saliva/DNA and scaled photographs); swabs from any suspicious stains or deposits on the body. An alternate light source (ALS, 450–490 nm wavelength with orange filter goggles) can highlight biological fluids (semen, saliva) that fluoresce on the skin surface. All specimens are packaged per sexual assault kit protocols with chain-of-custody documentation. The anogenital examination should be performed with colposcopy or magnification when possible.
Medical Intervention Artifacts
Resuscitative efforts and medical treatment produce artifacts that must be distinguished from injuries: CPR causes anterior rib fractures and sternal fractures (rare in young adults but common in elderly), retrosternal hemorrhage, hepatic laceration, and conjunctival/facial petechiae. Endotracheal intubation causes mucosal abrasion/hemorrhage of the posterior pharynx and arytenoids. Central line placement creates puncture wounds with underlying tract hemorrhage. Defibrillator pads leave rectangular skin marks. Intraosseous needle placement creates a small puncture wound in the proximal tibia or humeral head. All medical devices should be documented in situ and their placement verified. The forensic pathologist must review the EMS and hospital medical records to identify all interventions performed.
06 Internal Examination — Technique
The internal examination provides direct visualization of organs, body cavities, and internal injuries. The choice of technique depends on the nature of the case, the pathologist's training, and institutional protocol. Regardless of method, the goal is systematic, thorough examination of every organ system.
Incision Approaches
The standard thoracoabdominal incision is the Y-incision: two cuts from the acromioclavicular joints meeting at the xiphoid process, then a single midline cut extending to the pubic symphysis. This provides wide exposure to the thoracic and abdominal cavities. The chest plate (sternum and anterior ribs) is removed with a bone saw or rib cutters to expose the thoracic organs. For suspected pneumothorax, a water seal test is performed before opening the chest (puncture the intercostal space under water and observe for bubbling).
Organ Removal Methods
| Method | Technique | Advantage |
|---|---|---|
| Virchow method | Each organ removed individually, examined separately | Detailed individual organ examination; most common in North America |
| Rokitansky method | In-situ dissection with organs examined in place, then removed | Preserves anatomic relationships; useful for vascular studies |
| Letulle method | All thoracic and abdominal organs removed en bloc as a single evisceration | Rapid; allows later detailed dissection; preferred for teaching |
| En bloc (Ghon) method | Organ systems removed in functional blocks (cardiopulmonary, GI, urogenital) | Preserves interorgan relationships within systems |
Systematic Organ Examination
Each organ is weighed, externally inspected, and serially sectioned. The heart is opened along the direction of blood flow (inflow-outflow method) or by short-axis cross sections (bread-loaf method for evaluating ischemic injury). Coronary arteries are cross-sectioned at 3 mm intervals to assess stenosis. The lungs are examined for congestion, edema, hemorrhage, consolidation, and thromboembolism (pulmonary arteries opened before removing the lungs from the chest in PE-suspected cases). The brain is ideally fixed in 10% buffered formalin for 2 weeks before sectioning to permit proper coronal sections without distortion; fresh brain sectioning is acceptable when rapid diagnosis is needed but produces suboptimal histologic sections.
Normal Organ Weights — Adult (Summary)
| Organ | Male (g) | Female (g) | Clinical Significance |
|---|---|---|---|
| Heart | 300–350 | 250–300 | >400 g suggests cardiomegaly (hypertension, cardiomyopathy, valvular disease) |
| Brain | 1300–1400 | 1200–1300 | Increased weight: edema; decreased weight: atrophy (Alzheimer, advanced age) |
| Liver | 1400–1600 | 1200–1400 | Increased: hepatomegaly (steatosis, congestion, cirrhosis with regeneration) |
| Right kidney | 125–170 | 115–155 | Asymmetry >30 g suggests renal artery stenosis or chronic pyelonephritis |
| Left kidney | 130–175 | 120–160 | Left kidney is typically slightly larger than right |
| Spleen | 150–200 | 130–180 | >250 g: splenomegaly; infections, lymphoma, portal hypertension |
| Right lung | 450–500 | 350–450 | Combined lung weight >1000 g: pulmonary edema, pneumonia, congestion |
| Left lung | 400–450 | 300–400 | Left lung slightly lighter (cardiac notch reduces parenchymal volume) |
| Thyroid | 25–35 | 20–30 | Goiter: >40 g |
| Pancreas | 100–150 | 100–140 | Atrophy in chronic pancreatitis or diabetes |

Head Examination
A coronal (ear-to-ear) scalp incision provides access to the calvarium. The scalp is reflected anteriorly and posteriorly to inspect for subgaleal hemorrhage. The skull is opened with an oscillating saw. The dura is inspected for epidural and subdural hemorrhage before reflection. The brain is removed by cutting the cranial nerves, tentorium, and spinal cord at the foramen magnum. The base of skull is examined for fractures.
Neck Examination
In cases of suspected neck compression (strangulation, hanging), the neck is dissected after the brain and thoracic/abdominal organs have been removed and the major vessels drained. This bloodless neck dissection technique minimizes artifact hemorrhage from engorged vessels that could be mistaken for vital contusion. The anterior neck is dissected layer by layer: platysma, sternocleidomastoid muscles, strap muscles, thyroid gland, hyoid bone, thyroid cartilage, cricoid cartilage, and tracheal rings. Each structure is examined for hemorrhage, fracture, and mucosal injury. The carotid arteries are examined for intimal tears. The hyoid bone and laryngeal cartilages may be removed and examined radiographically or by dissection under a dissecting microscope to detect subtle fractures.
Spinal Cord Examination
The spinal cord is examined in cases of suspected spinal trauma, hangman's fracture, motor vehicle collisions, or sudden infant death. A posterior approach through a longitudinal midline incision exposes the vertebral column. Laminectomy or an anterior approach (after evisceration) provides access. The cord is examined for contusion, laceration, epidural hemorrhage, and compression. In AHT cases, the cervical spinal cord and nerve roots are examined for hemorrhage, which is a sensitive marker for acceleration-deceleration injury in infants.
07 Histology & Ancillary Studies
Microscopic examination and specialized ancillary tests complement gross autopsy findings. Histology can reveal subclinical disease processes, confirm suspected diagnoses, and provide crucial evidence of wound vitality and timing.
Standard Histologic Blocks
A routine forensic autopsy typically includes sections of: heart (left ventricle free wall, interventricular septum, right ventricle, each coronary artery territory), lungs (bilateral), liver, kidneys (bilateral), spleen, pancreas, and any lesions or injuries identified grossly. Additional sections are guided by case-specific findings. Tissue is fixed in 10% neutral buffered formalin, processed through paraffin embedding, sectioned at 4–5 micrometers, and stained with hematoxylin and eosin (H&E) as the primary stain.
Wound Age Estimation by Histology
The microscopic inflammatory response provides an approximate timeline of wound age, which is critical for distinguishing injuries inflicted at different times (particularly in child abuse cases):
| Time After Wounding | Predominant Finding | Additional Features |
|---|---|---|
| 0–1 hour | Hemorrhage only | No cellular reaction; margination of neutrophils may begin at vessel walls |
| 1–4 hours | Early neutrophil infiltration | Perivascular neutrophils; beginning interstitial infiltration |
| 4–12 hours | Dense neutrophilic infiltrate | Necrotic tissue debris; fibrin deposition |
| 12–24 hours | Peak neutrophils; early macrophages | Removal of debris begins |
| 1–3 days | Macrophage predominance | Hemosiderin-laden macrophages appear; early granulation tissue |
| 3–7 days | Fibroblast proliferation; granulation tissue | Capillary neoangiogenesis; macrophages continue |
| 1–2 weeks | Mature granulation tissue | Collagen deposition begins; decreased inflammatory cells |
| 2–4 weeks | Early scar formation | Fibrosis with progressive collagen maturation |
| >1 month | Mature scar | Dense collagen; minimal cellularity; remodeling |
Immunohistochemistry
Select immunohistochemical stains assist forensic diagnosis: Cardiac troponin T/I demonstrates early myocardial injury (loss of staining in necrotic myocardium) before morphologic changes are visible on H&E; CD68 highlights macrophages for wound age estimation; Glycophorin A detects red blood cell extravasation in hemorrhage, distinguishing antemortem bleeding from postmortem artifact; Fibronectin in wound margins supports vitality (deposited during coagulation cascade in living tissue); P-selectin and ICAM-1 demonstrate early endothelial activation in wounds. CD15 and myeloperoxidase identify neutrophils in equivocal cases.
Postmortem Microbiology
Postmortem cultures must be interpreted with extreme caution because of bacterial translocation from the gut into the bloodstream and tissues that begins within hours of death. Organisms recovered from blood cultures may represent antemortem sepsis, agonal bacteremia, or postmortem contamination. Correlation with clinical history, gross findings (e.g., cardiac vegetations, abscess), and histology is essential. Pericardial fluid and splenic tissue cultures are less susceptible to contamination than peripheral blood.
Vitreous Chemistry
Vitreous humor is relatively protected from autolysis and contamination due to its anatomic sequestration within the globe. Useful vitreous analytes include: glucose (elevated in antemortem hyperglycemia/diabetic ketoacidosis), urea nitrogen/creatinine (elevated in uremia), sodium (hypernatremia/dehydration), chloride, potassium (PMI estimation), and beta-hydroxybutyrate (ketoacidosis). Vitreous A1C can indicate chronic glycemic control.
Postmortem Imaging (Virtopsy / PMCT)
Postmortem computed tomography (PMCT) is increasingly used as an adjunct to autopsy. It excels at detecting: pneumothorax, subcutaneous/soft tissue emphysema, skeletal fractures, intracranial hemorrhage, retained projectiles, and gas embolism. PMMR (postmortem MRI) provides superior soft tissue contrast. Virtopsy (virtual autopsy) integrates PMCT, PMMR, and 3D surface scanning as a minimally invasive alternative or supplement to traditional autopsy. Limitations include inability to assess organ texture, color, and odor, and poor detection of coronary artery disease without contrast angiography.
PMCT vs Conventional Autopsy — Comparative Strengths
| Finding | PMCT | Conventional Autopsy |
|---|---|---|
| Skeletal fractures | Superior (3D reconstruction, subtle fractures detected) | May miss nondisplaced fractures without radiography |
| Pneumothorax / gas embolism | Superior (air is easily detected on CT) | Difficult to detect; special technique required (water submersion test) |
| Retained projectiles / foreign bodies | Superior (precise localization, 3D mapping) | Dependent on physical dissection and radiography |
| Coronary artery disease | Poor without contrast; calcification visible | Superior (direct vessel opening, luminal assessment) |
| Soft tissue organ pathology | Limited resolution | Superior (gross and microscopic examination) |
| Toxicology | Not applicable | Essential (specimen collection only at autopsy) |
| Natural disease processes | Limited | Superior (histology, microbiology, biochemistry) |
08 Pediatric Autopsy & SIDS
Pediatric forensic autopsy requires specialized protocols because the spectrum of natural disease, the recognition of inflicted injury, and the normal anatomic variants differ significantly from adults. Every unexpected death in an infant or young child must be approached with the possibility of both natural and non-natural causes.
SIDS — Definition & Epidemiology
Sudden infant death syndrome (SIDS) is defined as the sudden unexpected death of an infant under 1 year of age that remains unexplained after a thorough case investigation including a complete autopsy, examination of the death scene, and review of clinical history. Peak incidence occurs at 2–4 months of age. Risk factors include: prone sleeping position, soft bedding, bed-sharing, prematurity, low birth weight, prenatal maternal smoking, young maternal age, and male sex. The "Back to Sleep" campaign (1994) reduced SIDS rates by approximately 50% in the United States.
SUID (sudden unexpected infant death) is the broader umbrella term encompassing all sudden and unexpected deaths in infancy, including SIDS, accidental suffocation and strangulation in bed (ASSB), and deaths of unknown cause. SIDS is certified only when no cause is identified after complete investigation. Accidental suffocation may be diagnosed when a clear mechanical obstruction (overlay by co-sleeping adult, wedging between mattress and wall, soft bedding over face) is identified. The distinction can be difficult and requires meticulous scene investigation including doll reenactment of the reported sleeping position.
Triple Risk Model
The leading pathophysiologic hypothesis is the triple risk model: SIDS occurs when three factors converge: (1) a vulnerable infant with an underlying abnormality (brainstem serotonergic defect affecting arousal and cardiorespiratory control), (2) a critical developmental period (2–4 months when cardiorespiratory control is immature), and (3) an exogenous stressor (prone position, overheating, upper respiratory infection). Research has identified reduced serotonin 5-HT1A receptor binding in the arcuate nucleus and ventral medulla in SIDS victims.
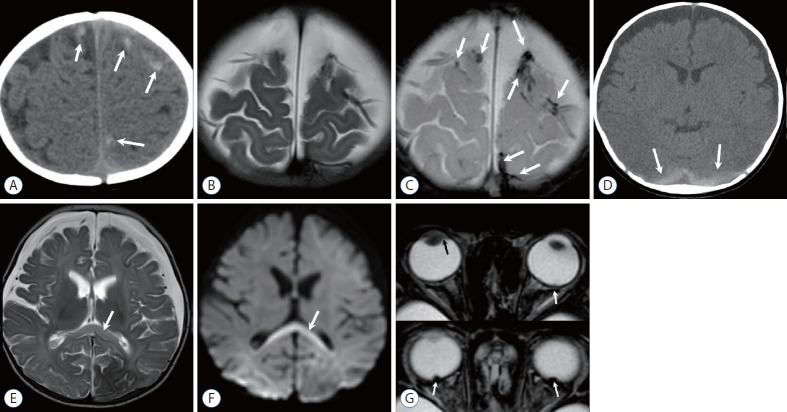
Abusive Head Trauma (AHT)
Formerly termed "shaken baby syndrome," abusive head trauma is a leading cause of traumatic death in infants. The classic triad consists of:
| Finding | Characteristics |
|---|---|
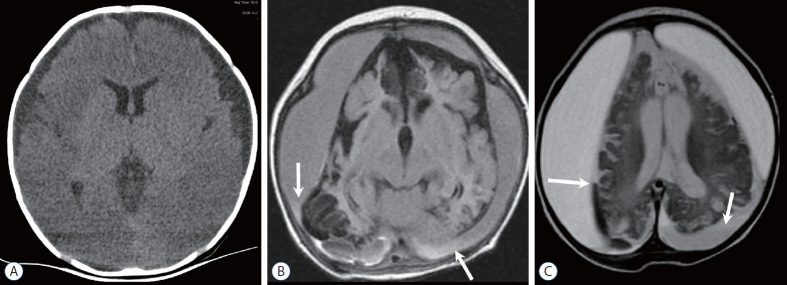
| Subdural hemorrhage | Thin film, often bilateral or interhemispheric; may be different ages indicating repeated trauma |
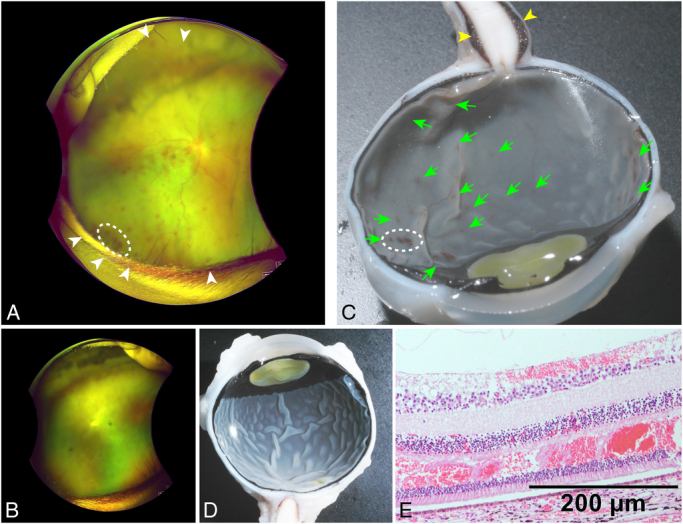
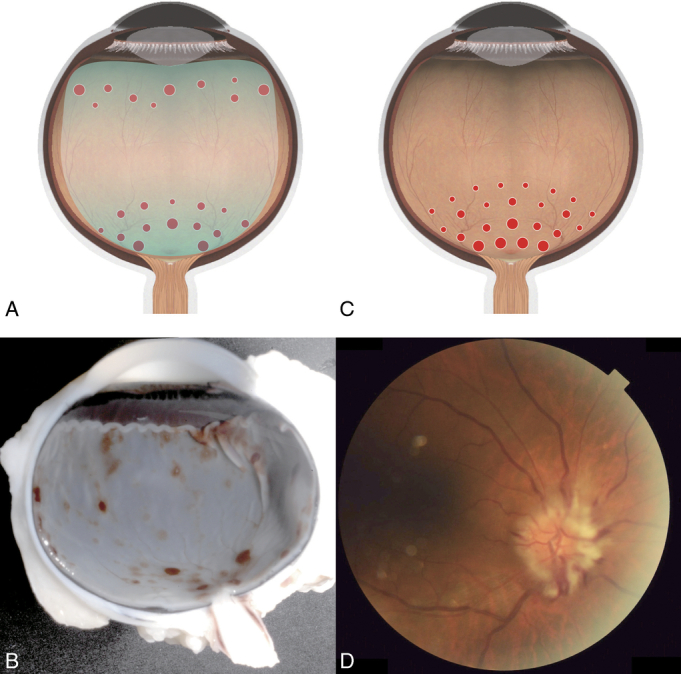
| Retinal hemorrhage | Multilayered, extending to the periphery (ora serrata); too numerous to count; highly specific for AHT in infancy |
| Encephalopathy | Diffuse cerebral edema, hypoxic-ischemic injury; may present with apnea, seizures, altered consciousness |
Additional findings supporting AHT: bridging vein thrombosis, diffuse axonal injury (beta-APP immunostaining), cervical spinal cord/nerve root injury, and absence of a credible accidental mechanism for the severity of injury. The constellation of findings must be interpreted in clinical context — short accidental falls (<3 feet) can occasionally produce isolated subdural hemorrhage or skull fracture, but they do not produce the full triad with extensive retinal hemorrhages and severe diffuse brain injury.
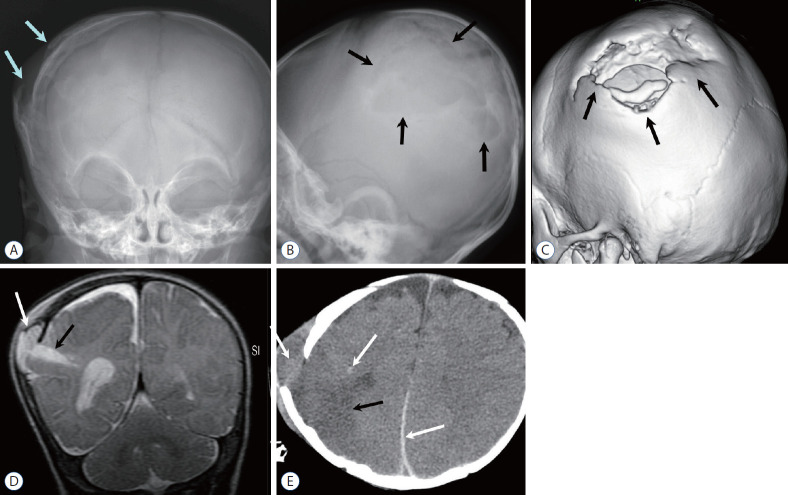
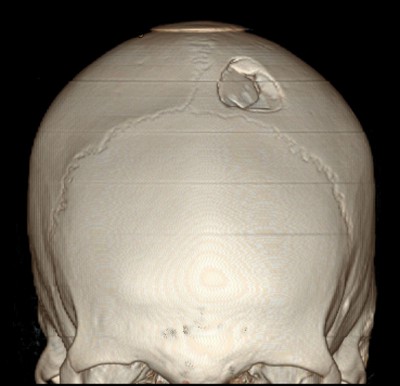
Skeletal Survey Findings in Child Abuse
Certain fracture patterns are highly specific for non-accidental trauma:
| Fracture Type | Specificity for Abuse | Mechanism |
|---|---|---|
| Classic metaphyseal lesion (CML) | High | Shearing forces across the immature physis from shaking/twisting/pulling; "bucket handle" or "corner" fracture on radiograph |
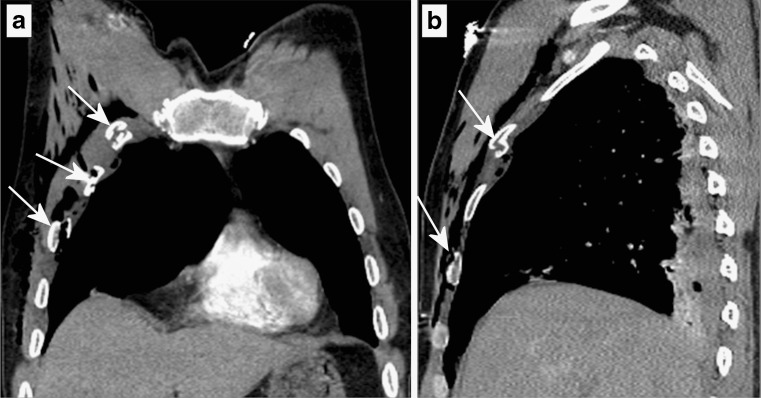
| Posterior rib fractures | High | Anteroposterior compression of the chest during squeezing; levering over the transverse process |
| Scapular fractures | High | Direct blow or forceful shaking |
| Spinous process fractures | High | Hyperflexion/extension |
| Sternal fractures | Moderate-high | Direct blow to the chest |
| Multiple fractures in different stages of healing | High | Repetitive episodes of trauma |
| Skull fractures (complex, bilateral, crossing suture lines) | Moderate | High-force impact or multiple impacts |
| Long bone diaphyseal fractures in non-ambulatory infants | Moderate | No credible mechanism in a child who cannot yet walk or pull to stand |
09 Blunt Force Injuries
Blunt force injuries result from impact with or by a blunt object or surface. The tissue response depends on the force, velocity, surface area of impact, and tissue type (skin, fat, muscle, bone). Blunt force produces four principal injury types: abrasion, contusion, laceration, and fracture.
Abrasions
An abrasion is a superficial injury caused by friction or scraping that removes the epidermal surface without penetrating the full thickness of the dermis. Abrasions do not scar if confined to the epidermis. Types include:
| Type | Mechanism | Appearance |
|---|---|---|
| Scrape (scratch) | Tangential force; object moves across skin surface | Linear; directional tags of raised epidermal flaps indicate direction of force |
| Brush burn (friction) | Broad tangential force (road rash, dragging) | Wide area of denuded epidermis; parallel striations may indicate direction |
| Patterned (imprint) | Perpendicular compression that crushes the epidermis | Reproduces the surface pattern of the striking object (e.g., tire tread, shoe sole, fabric weave, ligature) |
| Pressure (contusion-abrasion) | Sustained pressure with minor movement | Combined features; seen under ligatures and restraints |
Contusions
A contusion (bruise) is hemorrhage into subcutaneous tissue and skin caused by rupture of blood vessels from blunt force. Contusions reflect the mechanism of injury: direct blow, compression, or deceleration. Patterned contusions may reproduce the striking object (belt, knuckles, shoe). Location is important: bruises on shins and forearms are common from everyday activities, while bruises on the ears, neck, torso, buttocks, or genitalia in children are suspicious for abuse.
The traditional schema for aging bruises by color (red-blue at onset → blue-purple at 1–3 days → green at 5–7 days → yellow at 7–10 days → brown at 10–14 days → resolution at 2–4 weeks) has significant limitations. Research by Langlois and Gresham (1991) and others demonstrates that color changes are unreliable for precise aging: multiple observers show poor inter-rater agreement, colors overlap temporally, and skin pigmentation affects visibility. The only evidence-based color determination is that a yellow component indicates the bruise is at least 18 hours old. Court testimony should reflect these limitations.
Lacerations
A laceration is a full-thickness tear of the skin and underlying tissue caused by crushing or stretching from blunt force. Key features distinguishing lacerations from incised wounds: irregular/ragged wound margins, intact bridging vessels and nerves crossing the wound depth (blood vessels and nerves are more elastic than skin and stretch rather than sever), bruising of wound edges, tissue tags within the wound, and hair follicles that are crushed rather than cleanly divided. Lacerations occur preferentially over bony prominences (scalp, brow, chin) where skin is compressed between the striking object and underlying bone.
Pattern Injuries
The shape of a blunt force injury may mirror the causative object: belt buckle (rectangular bruise/abrasion), bite mark (paired crescentic bruises corresponding to dental arches, intercanine distance ~2.5–4.0 cm in adults), knuckle marks (parallel linear bruises), hammer head (circular depressed skull fracture), baseball bat (parallel tramline bruises from the edges with central sparing), fingertip bruises (oval bruises from gripping). Documentation of patterned injuries requires scaled photography and careful measurement.
Skull Fractures from Blunt Force
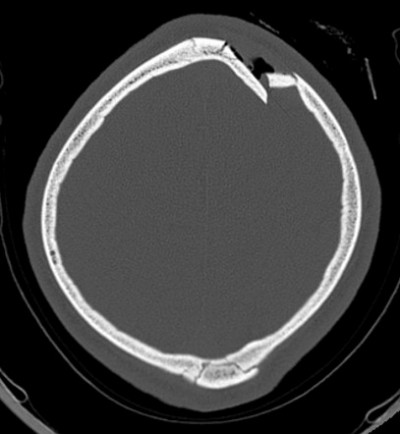
Linear fractures are the most common type and result from broad-surface low-velocity impact. Depressed fractures are caused by focal high-force impact (hammer, rock) and may mirror the impacting object. Ring (basilar) fractures around the foramen magnum result from axial loading (falls landing on feet/buttocks or blows to the vertex). Diastatic fractures separate suture lines, most common in children. Comminuted fractures involve multiple fragments from severe force. The Puppe rule states that fracture lines from a second impact terminate at fracture lines from a first impact, allowing sequencing of multiple blows.
Intracranial Hemorrhage from Blunt Force
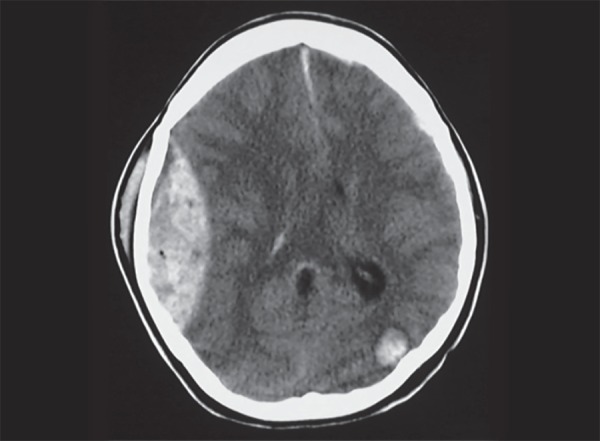
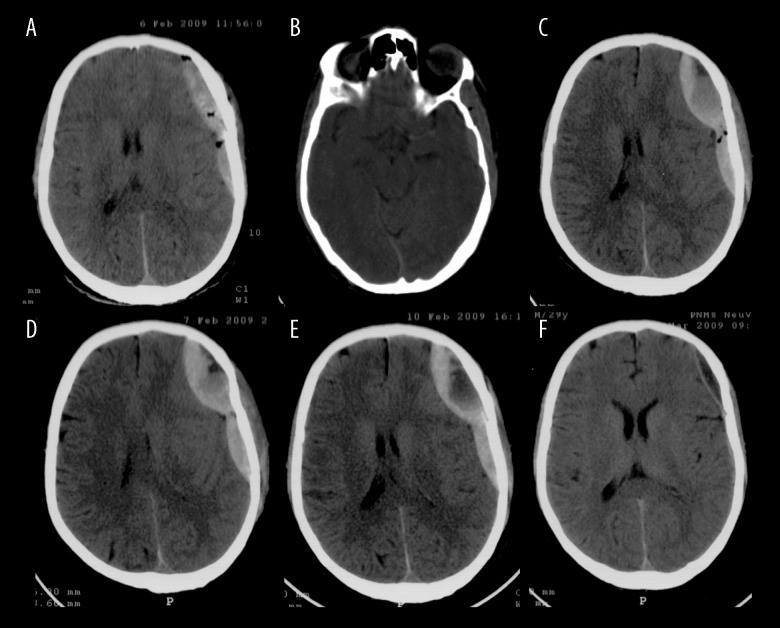
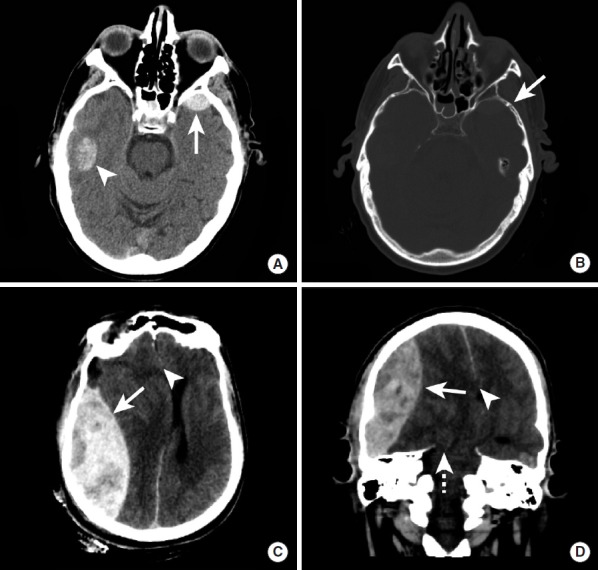
| Type | Location | Source | CT Appearance | Key Features |
|---|---|---|---|---|
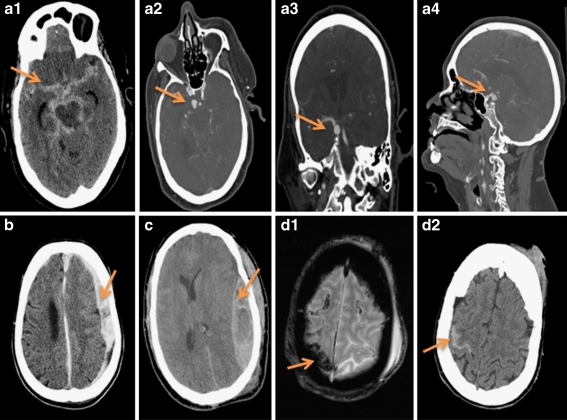
| Epidural hematoma | Between skull and dura | Middle meningeal artery (most common); dural sinuses | Biconvex (lens-shaped), hyperdense; does not cross suture lines | "Lucid interval" in 20–50% of cases; requires emergent surgical evacuation; often with temporal bone fracture |
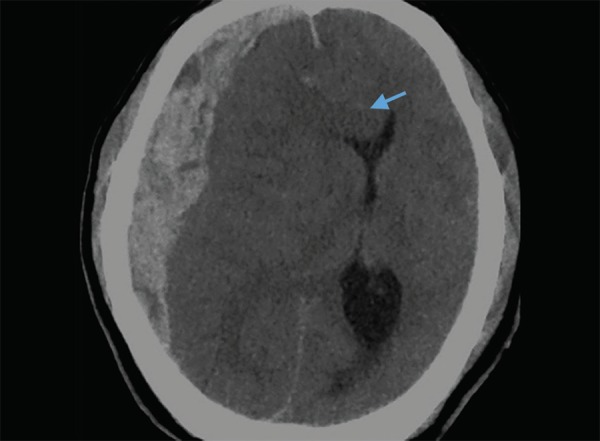
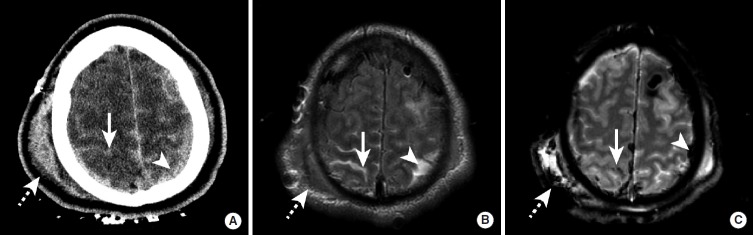
| Subdural hematoma | Between dura and arachnoid | Bridging veins from cortex to dural sinuses | Crescent-shaped, follows brain contour; crosses suture lines | Acute: hyperdense; subacute (1–3 weeks): isodense; chronic (>3 weeks): hypodense; common in elderly/alcoholics/AHT |
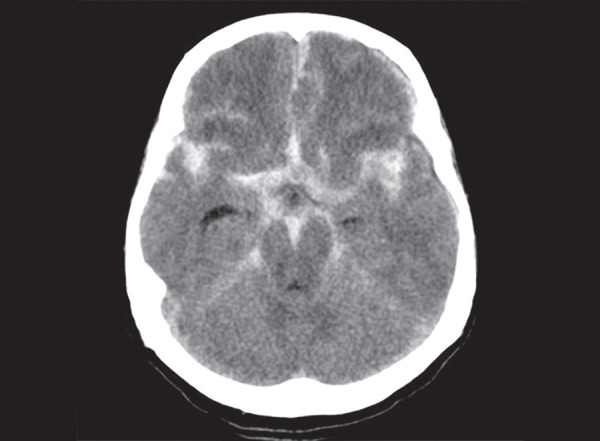
| Subarachnoid hemorrhage | Between arachnoid and pia | Cortical vessels; also ruptured aneurysm (non-traumatic) | Hyperdensity in sulci and cisterns | Traumatic: overlying contusion; non-traumatic: circle of Willis aneurysm rupture |
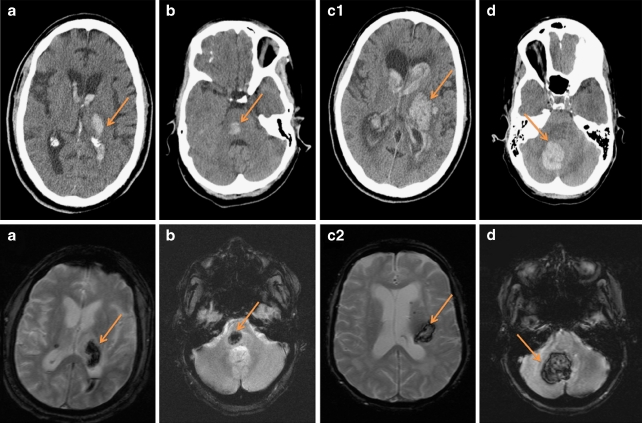
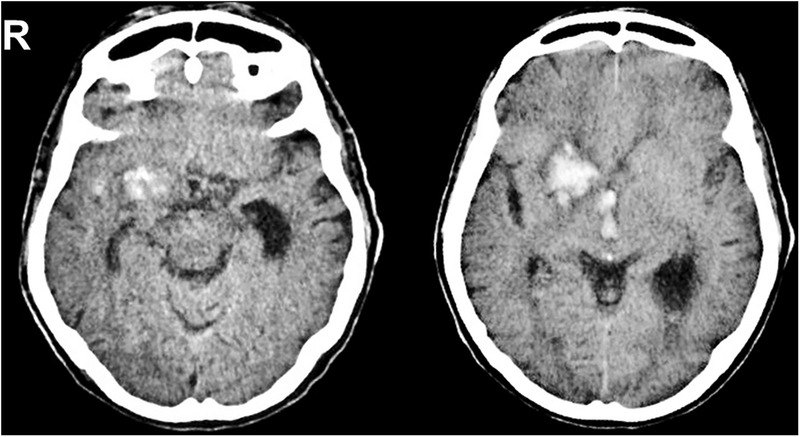
| Intracerebral hemorrhage | Within brain parenchyma | Contusion with secondary hemorrhage; shear injury to penetrating vessels | Hyperdense intraparenchymal lesion with surrounding edema | Coup (at impact) and contrecoup (opposite) distribution; frontal and temporal poles most vulnerable |
10 Sharp Force Injuries
Sharp force injuries are produced by objects with a cutting edge, a pointed tip, or both. They are distinguished from blunt force injuries by their clean-cut wound margins, absence of bridging vessels, and sharp division of tissue planes. Three principal types exist: incised wounds, stab wounds, and chop wounds.
Incised Wounds
An incised wound is longer on the skin surface than it is deep. It is produced by a sharp edge drawn across the skin (slashing or cutting action). Characteristics include: clean, well-defined wound margins; sharp (non-bruised) edges; tailing at one or both ends (the wound is deepest where the blade first engages and tapers as pressure decreases); no bridging vessels or tissue tags; cleanly divided hair follicles. The wound may gape widely depending on the underlying Langer lines (tension lines of the skin). Incised wounds bleed freely because vessels are cleanly divided and cannot retract and contract effectively.
Stab Wounds
A stab wound (puncture wound) is deeper than it is long on the skin surface. It is produced by a pointed instrument thrust into the body. The surface wound may underestimate the depth of penetration (the skin and underlying soft tissue can be compressed during thrusting, allowing the blade to penetrate deeper than its own length). Key documentation includes: wound dimensions (length and width on the skin surface), wound depth (from wound track dissection), direction of wound track, character of margins (single-edged blade produces one sharp angle and one squared-off angle; double-edged blade produces two sharp angles), and identification of internal organ and vascular injuries.
Chop Wounds
A chop wound is produced by a heavy instrument with a sharp edge (axe, machete, hatchet, propeller) combining the features of sharp and blunt force. Chop wounds demonstrate clean-cut margins (like incised wounds) but also produce underlying fractures of bone (unlike pure incised wounds). The wounds are typically deep, gaping, and may involve complete or partial amputation of extremities or portions of the skull.
Hesitation Marks
In suicidal sharp force injury, hesitation marks (tentative wounds) are shallow, superficial, parallel incised wounds adjacent to the deeper fatal wound. They are characteristically found on the wrists, neck, and antecubital fossae. Their presence strongly suggests self-infliction. Hesitation marks are typically absent in homicidal sharp force injuries.
Defense Wounds
Defense wounds are injuries sustained while the victim attempts to protect themselves from an attack. They are found on the palmar surfaces of the hands and fingers (from grasping a blade), the dorsal surfaces of the forearms (from raising arms to shield the face and body), and occasionally the lower extremities (from kicking). Defense wounds indicate the victim was conscious and mobile during the attack and strongly argue against self-infliction.
Tool Mark Analysis
Examination of wound characteristics, cartilage/bone marks, and wound track dimensions can sometimes narrow the type of weapon used. Blade width is estimated from the wound length (accounting for skin elasticity); single vs double edge is determined by the wound angle morphology; serrated blades produce irregular wound margins; scissors produce a cross-shaped or double-incised wound. In bone, tool marks may retain striations unique to a specific blade that can be compared microscopically using comparison microscopy.
Wound Documentation Principles
Every sharp force wound must be documented with: anatomic location (referenced to fixed landmarks), size (length × width × depth, measured in centimeters), orientation (referenced to the long axis of the body), character of the wound margins (smooth, irregular, bruised), wound angles (sharp, squared, fish-tailed), and internal wound track (organs traversed, depth of penetration, direction). Wounds must be photographed before and after cleaning, with and without a measurement scale. In cases with multiple wounds, each wound is numbered and mapped on body diagrams to allow reconstruction of the assault sequence.
11 Gunshot Wounds
Gunshot wound interpretation is one of the most critical competencies in forensic pathology. Proper documentation of wound morphology allows determination of range of fire, entrance versus exit, bullet trajectory, and (with limitations) firearm type. The appearance of gunshot wounds varies with the distance between the muzzle and the skin surface at the time of discharge.
Range of Fire
| Range | Distance | Wound Characteristics |
|---|---|---|
| Contact | Muzzle touching or pressed against skin | Soot deposited within wound track; muzzle stamp (abrasion ring reproducing muzzle shape); searing of wound edges; over bone — stellate laceration from expanding gases entering the subcutaneous space; cherry-red COHb discoloration of wound margins; loose contact: eccentric soot deposit |
| Near-contact | Muzzle <1 cm from skin | Soot ring around entrance; singeing of hair; minimal stippling; may have partial muzzle stamp |
| Intermediate (close) | Approximately 1 cm to 60–90 cm (varies by weapon) | Stippling (tattooing): discrete punctate abrasions and embedded partially burned/unburned gunpowder particles surrounding the entrance; soot may be absent at greater distances within this range; stippling cannot be wiped away (distinguishes it from soot) |
| Distant (indeterminate) | Beyond the range of powder deposition | Only the bullet reaches the target; entrance shows round defect with abrasion collar; no soot, stippling, or muzzle stamp |
Entrance vs Exit Wound
| Feature | Entrance | Exit |
|---|---|---|
| Shape | Round or oval (depending on angle of entry) | Irregular, slit-like, stellate, or crescent |
| Abrasion collar (margin of abrasion) | Present (caused by the bullet abrading the skin margins as it enters) | Absent (bullet pushes outward) |
| Size | Approximates bullet caliber (but unreliable for caliber determination) | Variable; may be larger or smaller than entrance |
| Margins | Inverted (pushed inward) | Everted (pushed outward) |
| Skull bone beveling | Internal beveling (cone-shaped defect widens inward) | External beveling (cone-shaped defect widens outward) |
| Bullet wipe | Dark ring of lubricant/soot on skin margin or clothing | Absent |
Bullet Trajectory Determination
Trajectory is documented relative to the anatomic position: front-to-back vs back-to-front, right-to-left vs left-to-right, upward vs downward. Trajectory is determined by connecting the entrance wound to the exit wound or to the final resting position of a retained bullet. A trajectory rod or probe can be inserted along the wound track during autopsy. Trajectory must be described relative to the body in anatomic position — the actual spatial trajectory in the scene depends on the decedent's position at the time of shooting, which may not be known.
Shotgun Wounds
Shotgun wound morphology depends on the distance from muzzle to target because the pellet spread widens with distance. Contact: single large entrance wound with scalloped edges; massive tissue destruction; wadding and pellets within wound. Close range (<1 meter): single round entrance with satellite pellet holes at the periphery. Intermediate (1–3 meters): central defect with increasing pellet spread. Distant (>3–4 meters): widely scattered individual pellet wounds; each pellet creates a separate entrance. The choke of the barrel affects the rate of spread: full choke maintains a tighter pattern at greater distances than cylinder bore.
Caliber Estimation Limitations
Wound size does not reliably indicate bullet caliber. Skin is elastic and retracts after penetration; wound margins deform with drying; bullet deformation, fragmentation, and tumbling alter wound morphology. Recovered projectiles and cartridge casings provide the most reliable evidence for caliber determination, not wound dimensions.
Special Gunshot Wound Situations
Atypical entrance wounds may occur when the bullet passes through an intermediate target (glass, door, wall) before striking the body, causing deformation and irregular wound morphology that mimics an exit wound. Shored exit wounds occur when the skin at the exit site is supported by a firm surface (wall, floor, tight clothing, body armor), producing an abrasion collar around the exit wound that mimics an entrance wound. Graze wounds (tangential wounds) produce elongated abrasions or shallow trenches; the wound is deepest where the bullet first contacts the skin and tapers at the other end, with the deeper end indicating directionality. Ricochet wounds are caused by bullets that have struck an intermediate surface and are deformed, irregular, and tumbling — producing atypical entrance wounds that may be mistaken for those caused by unusual weapons.
Gunshot Residue (GSR)
Gunshot residue consists of particles of burned and unburned propellant, primer compounds (barium, antimony, lead), and metallic fragments deposited on the hands, clothing, and surrounding surfaces when a firearm is discharged. GSR analysis by SEM-EDX (scanning electron microscopy with energy-dispersive X-ray analysis) identifies characteristic spheroidal particles containing lead, barium, and antimony. GSR on the hands of the decedent supports but does not prove that the person fired a weapon (transfer from proximity to discharge is possible). GSR is easily lost through hand washing, movement, or medical intervention; samples should be collected as early as possible at the scene.
Entrance wounds are characterized by the "ABCDE" features: Abrasion collar (marginal abrasion), Bullet wipe (dark ring of lubricant), Circular/round shape, Direct (clean) margins inverted inward, Evidence of range (soot/stippling at close range). Exit wounds are characterized by their absence of these features: irregular shape, everted margins, no abrasion collar, no bullet wipe, and no powder residue. Bone beveling confirms direction: internal bevel = entrance; external bevel = exit.
12 Asphyxia
Asphyxia is the failure of cells to receive or utilize oxygen. In forensic practice, asphyxial deaths are classified by the mechanism of oxygen deprivation. Classic autopsy findings of asphyxia (petechiae, congestion, cyanosis, fluidity of blood) are nonspecific and may be absent; scene investigation and circumstances are often more important than autopsy findings for determining the cause and manner of asphyxial death.
Ligature Strangulation
Compression of the neck by a ligature (cord, belt, wire, rope) with force applied by another person. Autopsy findings include: ligature furrow (circumferential abrasion/contusion of the neck that may reproduce the pattern of the ligature — width, texture, knot impression), petechial hemorrhages (conjunctival, facial skin, epiglottic, thymic in children), hyoid bone fracture (superior cornua, more common in victims over age 40 when the bone is calcified and brittle), thyroid cartilage fracture (superior cornua), hemorrhage in the strap muscles, and congestion/edema above the level of compression.
Manual Strangulation
Compression of the neck by hands, fingers, or forearms. External findings: fingertip contusions (oval bruises, often on both sides of the neck; may be clustered indicating grip marks), fingernail abrasions (crescentic scratches from the victim or the assailant). Internal findings: deep hemorrhage in the strap muscles (even when external bruising is minimal), hyoid bone and thyroid/cricoid cartilage fractures, laryngeal mucosal hemorrhage. Petechiae are often more prominent than in ligature strangulation due to intermittent compression and release.
Hanging
Compression of the neck by a ligature from which the force is the victim's body weight (complete suspension or partial suspension — feet or other body parts may touch the ground). The ligature furrow in hanging typically runs obliquely upward toward the point of suspension and is non-circumferential (open at the back of the neck where the ligature rises to the suspension point), contrasting with the horizontal circumferential furrow in ligature strangulation. Vital reaction (hemorrhage) in the skin beneath the furrow, neck muscles, and carotid intima supports antemortem hanging. Most suicidal hangings are partial suspension. Drop hangings from significant height (judicial-style) may produce cervical spine fractures (hangman's fracture: bilateral C2 pars interarticularis fracture) and spinal cord transection.
The vessels and structures of the neck have different compression thresholds: jugular veins: 2 kg (4.5 lbs) of force — obstructed first, causing venous congestion and petechiae; carotid arteries: 5 kg (11 lbs) of force — produces cerebral hypoxia and unconsciousness within 10–15 seconds; trachea: 15 kg (33 lbs) of force — airway occlusion. Death from neck compression is primarily vascular (carotid occlusion/jugular obstruction) rather than airway obstruction. Vagal reflex cardiac arrest from carotid body stimulation may cause rapid death with minimal anatomic findings.
Suffocation & Smothering
Smothering is mechanical obstruction of the external airways (nose and mouth) by a hand, pillow, plastic bag, or other object. Autopsy findings may be minimal or absent. Subtle perioral and intranasal contusions or abrasions may be present. Petechiae may be seen in the conjunctivae and epiglottis. This mechanism is particularly dangerous because it may leave no forensic evidence, making it a favored method in infanticide and vulnerable adult homicide.
Positional / Restraint Asphyxia
Positional asphyxia occurs when body position restricts respiratory excursion: prone restraint with weight on the back, head-down suspension (e.g., trapped inverted in a garbage bin or window), or jackknife position. Obesity, intoxication, and restraint (hog-tying, prone handcuffing with pressure on the back) are contributing factors. Death-in-custody cases involving prone restraint are an important medicolegal issue.
Drowning
Drowning is death from submersion in a liquid medium. There is no single pathognomonic finding at autopsy. Findings suggestive of drowning include: voluminous frothy fluid in the airways (mucous-air-water emulsion), hyperinflated lungs with increased weight, pleural effusions, fluid in the sphenoid sinus and middle ear, and foreign material (diatoms, sand, algae) in the airways and lungs. Wet drowning (most cases) involves aspiration of water causing surfactant washout, pulmonary edema, and electrolyte disturbances. Dry drowning (~10–20%) involves laryngospasm without significant water aspiration. The diatom test identifies siliceous algae in organs distant from the lungs (bone marrow, kidney, brain) as evidence that diatom-containing water entered the systemic circulation during life; false positives from contamination limit its reliability.
Choking
Choking (aspiration of a foreign body into the airway) accounts for the "cafe coronary" — sudden collapse during eating that mimics a cardiac event. The food bolus (most commonly meat) occludes the larynx or trachea. Risk factors include intoxication (alcohol suppresses the gag reflex), poor dentition, neurological conditions impairing swallowing, and eating while talking. At autopsy, the foreign body is found impacted in the larynx, trachea, or mainstem bronchi.
Autopsy Findings in Asphyxia — Summary
| Finding | Significance | Specificity |
|---|---|---|
| Petechial hemorrhages (conjunctival, facial, thymic, visceral) | Venous hypertension from obstructed venous return with continued arterial inflow | Nonspecific; also seen in CPR, seizures, coagulopathy, severe coughing |
| Congestion and cyanosis of face/neck | Obstruction of jugular venous return above the level of compression | Nonspecific |
| Hyoid bone fracture | Direct compression of the neck; more common in adults >40 years (ossified hyoid) | Moderate; also seen in CPR in elderly; absent in ~50% of strangulation |
| Thyroid/cricoid cartilage fracture | Neck compression with significant force | More specific than hyoid fracture when combined with soft tissue hemorrhage |
| Strap muscle hemorrhage | Deep cervical soft tissue contusion from compression | Highly significant when demonstrated by bloodless dissection technique |
| Fluidity of blood | Traditionally attributed to fibrinolysis in asphyxia | Nonspecific; fluid blood seen in many causes of rapid death |
13 Thermal, Electrical & Chemical Injuries
Injuries from thermal, electrical, and chemical agents present unique forensic challenges, particularly the distinction between antemortem and postmortem changes and the determination of whether death was caused by the environmental exposure or by an underlying condition.
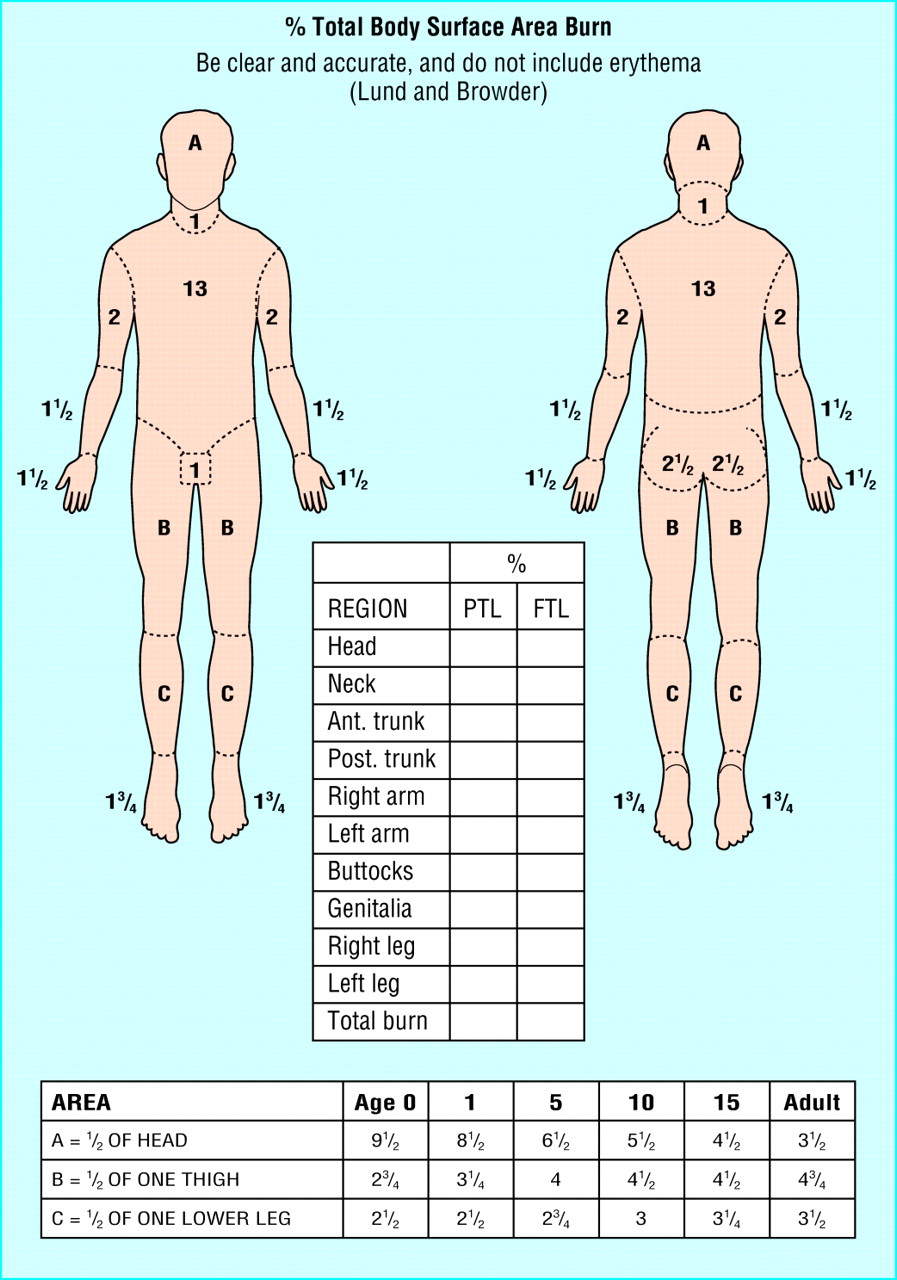
Burns — Degree Classification
| Degree | Depth | Appearance | Sensation |
|---|---|---|---|
| First (superficial) | Epidermis only | Erythema, no blisters | Painful |
| Second (partial thickness) | Epidermis + partial dermis | Blisters, moist, red base | Painful (intact nerve endings) |
| Third (full thickness) | Entire dermis destroyed | White, waxy, leathery, or charred; no blisters | Insensate (nerve endings destroyed) |
| Fourth | Through skin into subcutaneous fat, muscle, bone | Charred, contracted tissue; exposed deep structures | Insensate |

Fire Deaths — Forensic Evaluation
In fire deaths, the critical question is whether the decedent was alive when the fire started. Key findings indicating antemortem exposure: soot in the airway (below the vocal cords, in the trachea, bronchi, and even the esophagus/stomach from swallowing), elevated carboxyhemoglobin (COHb) (>10% indicates smoke inhalation; >50% is considered lethal, though death may occur at lower levels with concurrent cyanide exposure), and thermal injury to the airway mucosa with vital reaction (edema, erythema). Cherry-red discoloration of blood and tissues indicates COHb saturation. Cyanide levels should be measured in fire deaths (HCN released from burning synthetics, wool, and plastics).
The pugilistic posture (flexion of the extremities with fists clenched) is a postmortem artifact caused by heat-induced protein denaturation and shortening of flexor muscles; it does not indicate a defensive posture and can occur in bodies dead before the fire. Heat fractures of the skull may mimic traumatic fractures but are typically linear, follow heat gradient patterns, and lack associated hemorrhage. Heat-related epidural hemorrhage (thermal epidural hematoma) results from shrinkage of the brain and dura with blood extruded from diploe; it is chocolate-brown and granular, distinguishable from traumatic epidural hemorrhage which is red-purple and liquid/clotted.
Electrocution
Electrocution is death caused by the passage of electric current through the body. Alternating current (AC, 50–60 Hz) is more dangerous than direct current (DC) at equivalent voltages because AC induces tetanic muscle contraction (preventing the victim from releasing the source) and is more likely to cause ventricular fibrillation. Low-voltage (<1000 V) deaths are typically due to cardiac arrhythmia (ventricular fibrillation); high-voltage (>1000 V) deaths may cause respiratory arrest from brainstem injury or massive thermal injury.
The electrical mark (Joule burn) is a pale, firm, raised lesion at the current contact site with a central depression and a rim of pallor. Microscopically, it shows elongation and pallisading of keratinocyte nuclei in the epidermis. Electrical marks are absent in up to 50% of electrocution deaths, particularly in wet-skin contact or large surface area exposure (bathtub electrocution). Internal findings may include contraction band necrosis of the myocardium.
Lightning Injury
Lightning delivers massive current (up to 200 million volts, 20,000 amperes) for an extremely brief duration (microseconds). Lichtenberg figures (ferning or arborescent erythema) are pathognomonic but transient (fade within hours) branching reddish-brown skin patterns caused by electron shower along skin surface. Other findings include linear burns, punctate burns (at metal contact points such as zippers or jewelry), tympanic membrane rupture, and cardiac arrest (initial asystole, which may spontaneously convert if respiratory support is maintained).
Hypothermia
Death from cold exposure. Autopsy findings include: paradoxical undressing (clothing removed due to peripheral vasodilation from hypothalamic dysfunction, found in ~25% of cases), Wischnewski ulcers (multiple small, dark brown/black hemorrhagic erosions of the gastric mucosa, present in ~90% of hypothermia deaths; caused by mucosal ischemia from redistribution of blood flow), pink discoloration of the skin over the major joints (frost erythema), and pancreatic autolysis. Blood may appear bright red due to increased oxygen affinity of hemoglobin at low temperatures.


Chemical Burns
Acid burns cause coagulation necrosis (protein precipitation creates a barrier limiting depth of penetration); alkali burns cause liquefactive necrosis (saponification of fats allows deeper penetration and are therefore generally more severe). Hydrofluoric acid is uniquely dangerous because it penetrates deeply and causes lethal hypocalcemia through fluoride binding to calcium. Chemical burns may be accidental (industrial), suicidal (acid ingestion), or homicidal (acid attacks).
Distinguishing Antemortem Burns from Postmortem Thermal Artifact
When a body is recovered from a fire, the forensic pathologist must determine whether burn injuries were inflicted before or after death. Key features of antemortem burns: vital reaction in the wound margins (erythema, blistering with serous fluid containing inflammatory cells, neutrophilic infiltration microscopically), soot deposition in the airways below the vocal cords, elevated COHb (>10%), and soot in the esophagus/stomach from swallowing. Postmortem thermal artifacts: heat-induced skin splits (linear, clean-edged, resembling incised wounds but with no vital reaction and located along lines of tension), pugilistic posture, heat fractures (skull, long bones), epidural heat hematoma (brown, granular), and charring without underlying vital response. Bodies may sustain both antemortem and postmortem thermal injuries if the person was alive when the fire started but died during the fire.
14 Specimen Collection & Analysis
Forensic toxicology identifies and quantifies drugs, poisons, and metabolites in biological specimens collected at autopsy. Proper specimen collection, preservation, and chain-of-custody documentation are essential for the results to be admissible in court and scientifically interpretable.
Postmortem Redistribution
Postmortem redistribution (PMR) is the movement of drugs from higher-concentration compartments (solid organs, GI tract) into blood after death, producing artifactually elevated blood concentrations that do not reflect the antemortem level. This phenomenon is driven by passive diffusion along concentration gradients, autolysis of drug-laden cells, and putrefactive changes that disrupt membrane integrity. Drugs with large volumes of distribution (e.g., tricyclic antidepressants, digoxin, morphine) are particularly susceptible because they are concentrated in tissues rather than plasma during life. Cardiac blood (central site) is most affected because it lies adjacent to the lungs, liver, and GI tract — all major drug reservoirs. Femoral blood is the preferred specimen because it is anatomically distant from the drug-rich central organs and therefore less affected by redistribution. The degree of PMR increases with postmortem interval, making interpretation of drug levels in decomposed bodies particularly challenging.
Preferred Specimens
| Specimen | Volume | Preferred Use |
|---|---|---|
| Femoral blood | 20–30 mL (two gray-top tubes with NaF/EDTA) | Primary quantitative specimen; least affected by PMR |
| Cardiac (central) blood | 20–30 mL | Secondary specimen; useful for screening; central/peripheral (C/P) ratio informs PMR assessment |
| Vitreous humor | 2–5 mL per eye | Ethanol (less susceptible to postmortem production), glucose, potassium, urea nitrogen |
| Urine | All available | Drug screening (longer detection window for metabolites); qualitative more than quantitative |
| Bile | 5–10 mL | Opioids, benzodiazepines (concentrated by hepatobiliary excretion); useful for confirming use |
| Gastric contents | All available | Identifies unabsorbed pills/tablets; qualitative; volume and appearance documented |
| Liver tissue | 50–100 g | Quantitative analysis for drugs sequestered in tissue; useful for degraded specimens |
| Hair | Pencil-width bundle from vertex | Chronic drug use history; each cm of hair represents approximately 1 month of growth; segmental analysis |
| Cerebrospinal fluid | If available | Reflects CNS drug concentrations; limited routine use |
Analytical Methods
Forensic toxicology laboratories use a two-step process: screening (immunoassay — enzyme immunoassay, ELISA, or lateral-flow assay) to detect drug classes, followed by confirmation and quantitation using chromatographic methods. Gas chromatography–mass spectrometry (GC-MS) is the traditional gold standard for volatile and thermally stable compounds. Liquid chromatography–tandem mass spectrometry (LC-MS/MS) is now the workhorse for most drugs because it handles thermally labile compounds, requires less sample preparation, and offers superior sensitivity and specificity. All confirmatory results must meet validated criteria for accuracy, precision, linearity, and limit of detection/quantitation.
| Analytical Method | Primary Use | Advantages | Limitations |
|---|---|---|---|
| Immunoassay (EIA, ELISA) | Screening for drug classes | Rapid, high throughput, inexpensive | Cross-reactivity (false positives); does not identify specific drugs within a class; qualitative only |
| GC-MS | Confirmation and quantitation | Excellent specificity; NIST library matching; gold standard for volatiles | Requires derivatization for some compounds; thermally labile drugs may degrade; longer sample preparation |
| LC-MS/MS | Confirmation and quantitation | Handles polar/thermally labile compounds; minimal sample preparation; simultaneous multi-analyte panels | Higher instrument cost; matrix effects; requires internal standards |
| Headspace GC-FID | Volatile alcohols | Specific for ethanol, methanol, isopropanol, acetone | Limited to volatile compounds |
| ICP-MS | Metals (arsenic, thallium, lead, mercury) | Ultra-sensitive for elemental analysis | Does not distinguish chemical species; expensive |
Stability and Storage
Specimens should be refrigerated (4°C) immediately after collection. Sodium fluoride (NaF, 1–2% w/v) is added to blood specimens to inhibit glycolysis and bacterial enzymatic activity that could produce or degrade ethanol and other analytes. EDTA serves as anticoagulant. Long-term storage for retention and re-analysis is at –20°C. Specimens must be retained for the duration required by jurisdictional statute (commonly 1–3 years after case closure).
Chain of Custody for Toxicology
Every toxicology specimen must have documented chain of custody from the moment of collection through analysis, storage, and eventual disposition. The chain-of-custody form records: the specimen type, the name of the person collecting the specimen, date and time of collection, case identifiers, the names and signatures of every person who takes custody, conditions of storage and transfer, and the final disposition (retained, consumed during testing, or released). Laboratory information management systems (LIMS) track specimens electronically within the laboratory, but physical custody transfers still require written documentation. Any break in the chain may render the results inadmissible in court.
15 Common Toxicologic Findings
Interpretation of postmortem toxicology results requires understanding of pharmacokinetics, postmortem redistribution, tolerance, and the clinical significance of measured concentrations in the context of autopsy findings and circumstances.
Ethanol
Postmortem ethanol production (neoformation) by bacterial fermentation of glucose can produce artifactual ethanol levels of 0.01–0.20 g/dL or higher, particularly in decomposed bodies or those with elevated blood glucose (diabetes). Evidence supporting antemortem ethanol ingestion: (1) vitreous ethanol present (vitreous is relatively resistant to microbial contamination), (2) ethanol present in urine, (3) positive blood ethanol with NaF-preserved specimen, (4) vitreous-to-blood ethanol ratio of approximately 1.2:1 (equilibrium ratio). Back-calculation of BAC to an earlier time (e.g., time of driving) uses the Widmark formula but has significant pitfalls: individual elimination rates vary (0.010–0.025 g/dL/hour), the absorptive phase may not be complete, and food intake alters kinetics. Courts increasingly scrutinize back-calculation testimony.
Opioids
Fentanyl has become the leading cause of opioid overdose deaths. Lethal concentrations are highly variable due to tolerance: therapeutic fentanyl levels of 1–3 ng/mL may overlap with lethal levels in naive users (3–10+ ng/mL in non-tolerant individuals). Fentanyl redistributes significantly after death (C/P ratios of 2–4 are common). Morphine and codeine: the presence of both morphine and codeine in blood with a morphine-to-codeine ratio >1 (typically >2:1) is consistent with heroin use (heroin → 6-monoacetylmorphine → morphine, with codeine as an impurity in illicit heroin). Detection of 6-monoacetylmorphine (6-MAM) in blood or urine is confirmatory for heroin use but is rapidly metabolized (detectable for only ~2–8 hours).
Cocaine
Cocaine is rapidly metabolized to benzoylecgonine (BZE) (major metabolite) and ecgonine methyl ester. A BZE-to-cocaine ratio >1 indicates non-recent use (cocaine already metabolized). Concurrent alcohol use produces cocaethylene, an active metabolite formed by hepatic transesterification that has a longer half-life than cocaine and its own cardiotoxic properties. Death from cocaine may occur from cardiac arrhythmia, myocardial infarction (coronary vasospasm), aortic dissection, cerebral hemorrhage, hyperthermia, or excited delirium syndrome.
Carbon Monoxide
Carbon monoxide (CO) binds hemoglobin with 200–250 times the affinity of oxygen, forming carboxyhemoglobin (COHb). The cherry-red color of blood and tissues is visible grossly at COHb levels >30%. Lethal levels are generally considered >50–60%, but deaths may occur at 40% in patients with preexisting cardiovascular or pulmonary disease. Smokers have baseline COHb of 3–10%. Sources include house fires (most common), motor vehicle exhaust (catalytic converters have reduced this), furnaces, generators, and charcoal grills in enclosed spaces.
Cyanide
Cyanide inhibits cytochrome c oxidase (Complex IV of the electron transport chain), blocking aerobic cellular respiration. Sources include fire smoke (HCN from burning synthetics), intentional ingestion (potassium/sodium cyanide), and industrial exposure. The characteristic "bitter almond" odor is present in only ~40% of cases (ability to detect the odor is genetically determined). Whole blood cyanide levels >1.0 mg/L are potentially lethal. Combined CO and cyanide exposure in fire deaths is synergistically toxic.
Methanol & Ethylene Glycol
Methanol (wood alcohol) is metabolized to formaldehyde and then formic acid, which causes retinal toxicity (blindness) and metabolic acidosis with an elevated osmolal gap followed by elevated anion gap. Ethylene glycol (antifreeze) is metabolized to glycolic acid and then oxalic acid, causing renal tubular necrosis (calcium oxalate crystal deposition). Both produce a severely elevated osmolal gap early and elevated anion gap later. Fluorescent examination of urine (ethylene glycol contains fluorescein) is suggestive but not definitive. Forensic blood levels >80 mg/dL for methanol and >200 mg/dL for ethylene glycol are generally lethal, though treatment-naive exposure at lower levels can be fatal.
Other Toxic Agents in Forensic Practice
| Agent | Mechanism of Death | Key Forensic Features |
|---|---|---|
| Arsenic | Mitochondrial enzyme inhibition; multi-organ failure | Chronic: Mees' lines on nails, keratoses; hair/nail analysis for chronic exposure; detected in exhumed remains years later |
| Thallium | Mitochondrial toxicity; peripheral neuropathy | Alopecia (delayed 2–3 weeks); GI symptoms precede neurological; historically used as homicidal poison ("poisoner's poison") |
| Strychnine | Glycine receptor antagonist; tetanic seizures, respiratory failure | Opisthotonus posture; risus sardonicus (sardonic smile); detected by LC-MS/MS |
| Organophosphates | Acetylcholinesterase inhibition; cholinergic crisis | SLUDGE/BBB syndrome (salivation, lacrimation, urination, defecation, GI cramping, emesis, bradycardia, bronchospasm, bronchorrhea); measure RBC cholinesterase postmortem |
| Digoxin / oleander | Na+/K+ ATPase inhibition; cardiac arrhythmia | Massive postmortem redistribution; oleander ingestion produces digoxin-like compounds detectable on immunoassay |
| Insulin | Hypoglycemia; cerebral energy failure | Injection site hemorrhage on dissection; C-peptide (absent in exogenous insulin); vitreous glucose <20 mg/dL supports antemortem hypoglycemia |
16 Drug-Related Deaths
Drug-related deaths are among the most common cases in forensic pathology practice. The forensic pathologist must determine whether the drug caused, contributed to, or was incidental to the death, and whether the manner of death is accident, suicide, homicide, or undetermined.
Opioid Overdose
Autopsy findings: pulmonary edema (heavy, congested lungs weighing >1000 g combined, frothy fluid in airways), visceral congestion, needle marks (recent puncture sites, track marks from chronic injection, often in antecubital fossae, hands, feet, or groin), and potentially aspirated gastric contents. Cerebral edema may be present. Naloxone use prior to death may complicate toxicology interpretation (naloxone does not affect measured drug concentrations but changes the clinical picture). Fentanyl analogs and novel synthetic opioids may not be detected by routine immunoassay screens and require targeted LC-MS/MS testing.
Documentation of injection sites should include: Location (antecubital fossae, dorsal hands, feet, neck, groin, between toes), Age assessment (fresh puncture with surrounding erythema vs healed track scarring), Number of marks (single vs multiple), Pattern (linear track marks along veins indicating chronic IV drug use), and associated findings (subcutaneous abscess, cellulitis, thrombosed veins, skin-popping scars from subcutaneous injection). Injection sites should be excised and submitted for histologic examination to confirm the presence of needle tracks and assess the age of the injection sites. In insulin homicide cases, the injection site may show localized hemorrhage in the subcutaneous fat; serial sectioning of suspected injection areas may reveal the needle track.
Stimulant Deaths
Death from cocaine or methamphetamine may involve: cardiac arrhythmia (the most common acute mechanism), hyperthermia (core temperature >40°C with rhabdomyolysis, DIC, multi-organ failure), intracranial hemorrhage (hypertensive crisis), aortic dissection, or excited delirium syndrome (agitation, hyperthermia, sudden collapse). Chronic cocaine use produces accelerated atherosclerosis, concentric left ventricular hypertrophy, and contraction band necrosis. Chronic methamphetamine use is associated with cardiomyopathy and severe dental disease ("meth mouth").
Polypharmacy Deaths
The combination of CNS depressants produces synergistic respiratory depression: opioids + benzodiazepines, opioids + alcohol, opioids + gabapentinoids, or triple combinations. Each drug may be within its therapeutic range individually, but the combination is lethal. The forensic pathologist must evaluate the aggregate effect of all detected substances rather than each in isolation. Manner of death is typically accident unless evidence of suicidal intent is present (suicide note, internet searches, prior attempts).
Distinguishing accident from suicide in drug deaths is one of the most challenging determinations in forensic medicine. Factors suggesting suicide: suicide note (physical or electronic), internet searches regarding lethal doses, prior suicide attempts, expressed suicidal ideation, hoarding of medications, recent psychosocial stressors, and ingestion of medications not prescribed to the decedent. Factors suggesting accident: history of substance use disorder, drug paraphernalia at scene consistent with recreational use, no suicide note or communications, recently changed supply (e.g., new illicit drug source suggesting unknown potency), and witnessed recreational drug use preceding death. When evidence is truly equivocal, "undetermined" is the appropriate manner designation. Do not default to "accident" simply because there is no suicide note.
Prescription Drug Deaths
Documentation requires comparison of measured postmortem levels with published therapeutic, toxic, and lethal ranges (accounting for postmortem redistribution). Prescription medication history, pill counts, refill records, and pharmacy benefit data are reviewed. Common prescription drugs implicated in death include: methadone (long and variable half-life, QTc prolongation), oxycodone, benzodiazepines (rarely lethal alone in adults), antidepressants (tricyclics cause sodium channel blockade, QRS widening, and fatal arrhythmia), and anticonvulsants.
Drug-Facilitated Sexual Assault (DFSA)
Drugs used to facilitate sexual assault include: gamma-hydroxybutyrate (GHB) (rapidly eliminated, detection window 4–8 hours in blood, 8–12 hours in urine), flunitrazepam (Rohypnol) (detection window 24–72 hours in urine; 7-aminoflunitrazepam is the target metabolite), ketamine, zolpidem, and ethanol (most common drug used). Delayed reporting (hours to days) is the rule rather than the exception, making detection challenging. Hair analysis can extend the detection window to weeks or months for most substances except GHB.
DFSA Detection Windows
| Drug | Blood Detection Window | Urine Detection Window | Hair Detection |
|---|---|---|---|
| GHB | 4–8 hours | 8–12 hours | Unreliable (endogenous production) |
| Flunitrazepam | 12–24 hours | 24–72 hours (7-aminoflunitrazepam) | Yes (weeks to months) |
| Ketamine | 24–48 hours | 48–72 hours (norketamine) | Yes |
| Zolpidem | 6–12 hours | 24–48 hours | Yes |
| Ethanol | 6–12 hours | 12–24 hours (EtG/EtS metabolites: 24–80 hours) | EtG in hair for chronic use |
| Clonazepam | 24–48 hours | Up to 7 days (7-aminoclonazepam) | Yes |
| Diphenhydramine | 12–24 hours | 24–48 hours | Yes |
17 Forensic Identification
Positive identification of human remains is a legal requirement before a death certificate can be issued. In mass disasters, decomposed remains, or skeletonized cases, multiple identification modalities may be required. Methods are classified as positive (scientifically individuating) or presumptive (supporting but not conclusive).
Fingerprints
Fingerprint comparison follows the ACE-V methodology: Analysis (assessment of the quality and features of the unknown print), Comparison (side-by-side comparison with a known standard), Evaluation (determination: identification, exclusion, or inconclusive), and Verification (independent review by a second examiner). Prints are searched against the Automated Fingerprint Identification System (AFIS). Decomposed or macerated fingers may require reconditioning techniques: tissue builder injection, skin removal and mounting on the examiner's gloved finger, or chemical treatment (sodium hydroxide soak for wrinkled skin).
Dental Identification
Comparison of postmortem dental findings with antemortem dental records. Points of comparison include: restorations (type, material, surface involved), missing teeth, dental morphology, prosthetics, endodontic treatments, periodontal status, and radiographic comparison (root morphology, pulp chamber shape, trabecular bone pattern). The Gustafson method for age estimation uses six parameters scored 0–3: attrition, periodontosis, secondary dentin, cementum apposition, root resorption, and root transparency. Sum of scores correlates with chronological age (regression equation: Age = 11.43 + 4.56 × total score).
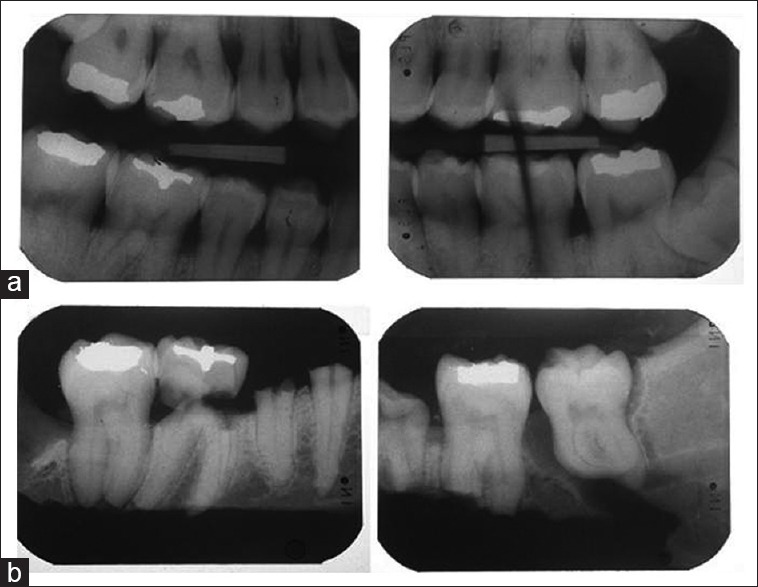
DNA Identification
Short tandem repeat (STR) profiling is the standard method: 20 or more STR loci are amplified by PCR and compared with a known reference sample or family member. The FBI's CODIS (Combined DNA Index System) database contains convicted offender, arrestee, and forensic profiles for comparison. For highly degraded or ancient remains, mitochondrial DNA (mtDNA) analysis is used: mtDNA is present in hundreds of copies per cell (vs 2 copies of nuclear DNA), survives degradation better, and is maternally inherited — but it is not individually unique (shared among maternal relatives). Y-STR profiling is used for male identification through the paternal line.
Forensic Anthropology
When remains are skeletonized, decomposed beyond recognition, burned, or fragmented, a forensic anthropologist provides skeletal analysis to establish a biological profile: estimation of sex, age at death, ancestry, and stature. The biological profile narrows the pool of potential matches for comparison with missing persons databases. In addition, the anthropologist assesses skeletal trauma (distinguishing perimortem from postmortem fractures based on fracture margin characteristics) and taphonomic changes (weathering, animal scavenging, root etching).
| Parameter | Primary Skeletal Indicators |
|---|---|
| Sex | Pelvis (subpubic angle, greater sciatic notch, ventral arc, preauricular sulcus) — most reliable; skull (mastoid process, nuchal crest, glabella, supraorbital margin, mental eminence); femoral/humeral head diameter |
| Age at death | Pubic symphysis morphology (Suchey-Brooks phases I–VI), auricular surface (Lovejoy/Buckberry-Chamberlain), sternal rib end morphology (Iscan), cranial suture closure, dental development and eruption (children), epiphyseal fusion (subadults) |
| Ancestry | Midface morphology, nasal aperture width, dental traits, metric analysis (Fordisc software using cranial measurements); increasingly supplemented by DNA ancestry markers |
| Stature | Long bone length (femur, tibia, humerus) applied to regression equations (Trotter and Gleser); ancestry and sex-specific formulas required for accuracy |
Radiographic Comparison
Comparison of antemortem and postmortem radiographs using unique anatomic features: frontal sinus pattern (unique to each individual like a fingerprint), healed fractures, orthopedic hardware, vascular calcifications, dental radiographs, and trabecular bone pattern. Radiographic superimposition of the skull onto antemortem photographs (craniofacial superimposition) is a presumptive method that can support but not confirm identification.
Facial Reconstruction
When no antemortem data is available for comparison, forensic facial reconstruction may generate a likeness from the skull to aid in recognition. Methods include: clay/sculpture-based manual reconstruction using tissue depth markers placed at standardized anthropometric points, and computer-based 3D reconstruction from CT scan data. Facial reconstruction is a recognition tool (it generates investigative leads) not an identification method — it cannot provide positive identification. Success depends on the accuracy of the biological profile and the skill of the artist or software algorithms.
Primary (positive) identifiers: fingerprints, dental comparison, DNA profiling, radiographic comparison with unique features. Any one of these can independently establish positive identification. Secondary (supporting) identifiers: visual recognition, personal effects, clothing, tattoos, scars, medical devices. These support but cannot independently confirm identification. Circumstantial identifiers: location where found, missing person reports, circumstantial evidence. Used to generate leads but never sufficient alone. In mass disasters, a minimum of one primary identifier is required for positive identification per INTERPOL DVI standards.
18 Wound Ballistics & Forensic Engineering
Understanding the biomechanics of injury production is essential for interpreting wound patterns and reconstructing the events that caused them.
Wound Ballistics
When a projectile enters tissue, it creates two zones of injury: the permanent cavity (the wound track directly crushed and destroyed by the bullet) and the temporary cavity (the transient radial displacement of tissue caused by kinetic energy transfer, which collapses within milliseconds). The temporary cavity can be many times the diameter of the permanent cavity and is responsible for injury to structures not directly in the bullet's path, particularly in tissues with low elasticity (liver, spleen, brain). Hollow-point bullets expand on impact, increasing the diameter of the permanent cavity and transferring more energy at a shallower depth. Full metal jacket bullets may pass through the body with relatively little deformation. Bullet fragmentation produces multiple wound tracks (lead snowstorm on radiograph) and increases tissue destruction. Intermediate targets (glass, bone, other objects struck before entering the body) may cause bullet deformation, fragmentation, or trajectory change and complicate wound interpretation.
Vehicular Injury Biomechanics
Pedestrian vs vehicle: The classic triad consists of (1) bumper injuries (lower extremity fractures at bumper height, typically tibia/fibula), (2) secondary impact injuries (trunk/head strike against the hood/windshield), and (3) tertiary impact injuries (landing on the ground after being thrown). Bumper height relative to the center of gravity determines whether the pedestrian is propelled forward, upward, or underneath the vehicle. Vehicle occupant injuries: frontal impact produces head/facial/chest injuries from steering wheel/windshield impact; lateral impact produces contralateral cerebral contusion from head striking the side pillar; rear impact produces cervical hyperextension (whiplash). Unrestrained drivers sustain the classic "down and under" (knees against dashboard → posterior hip dislocation, patellar fracture) or "up and over" (torso/head strikes steering wheel and windshield) pattern.
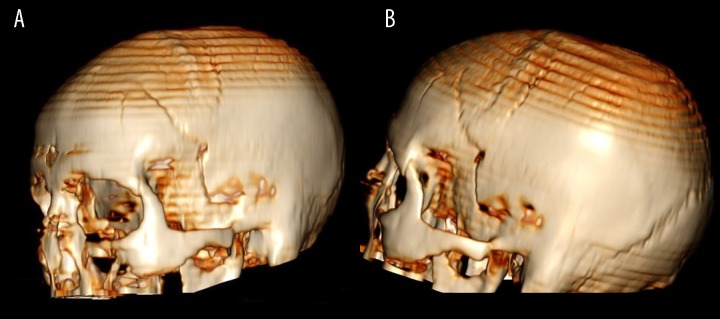
Seatbelt and Airbag Injuries
The seatbelt sign is a diagonal contusion/abrasion across the chest (shoulder belt) and horizontal contusion across the lower abdomen (lap belt). Improperly positioned lap belts (riding above the iliac crests) can cause lumbar spine fractures (Chance fracture), mesenteric tears, and hollow viscus perforation. Airbag injuries include facial abrasions/contusions, corneal abrasions, thermal/chemical burns from the propellant (sodium azide), and upper extremity fractures. Airbag deployment produces a characteristic powder residue (sodium compounds) that can be mistaken for gunshot residue on field testing.
Fall Height vs Injury Pattern
Falls from height produce injury patterns related to landing position: feet-first landing → calcaneal fractures, vertebral compression fractures, basilar skull fracture (axial loading transmitted through the spine); head-first landing → skull/cervical spine fractures with brainstem injury. Falls from >3 stories (approximately 10 meters) are generally considered potentially lethal. The presence or absence of injuries inconsistent with the reported fall mechanism may suggest an alternative scenario.
Accident Reconstruction Principles
Forensic engineering and accident reconstruction integrate physical evidence (vehicle damage profiles, tire marks, scene measurements, occupant injury patterns) with biomechanical principles to determine the sequence of events, speeds involved, and positions of occupants at the time of impact. The delta-V (change in velocity) is the primary predictor of injury severity: frontal impacts with delta-V >25 mph have a high probability of serious injury or death. The forensic pathologist contributes by correlating the occupant's specific injury pattern with the biomechanical forces predicted by the reconstruction. In pedestrian fatalities, the bumper height relative to the victim's anatomic landmarks, the pattern of leg fractures, and the head impact site on the vehicle help establish the pedestrian's stance and position at the time of impact.
19 Mass Disaster Response
Mass disasters (airline crashes, earthquakes, tsunamis, terrorist attacks, building collapses) generate large numbers of casualties requiring systematic identification and processing. The forensic response must be organized, standardized, and scalable.
Disaster Victim Identification (DVI)
The INTERPOL DVI protocol is the international standard, using a color-coded form system:
| Form Color | Content | Collected By |
|---|---|---|
| Yellow (AM) | Antemortem data: physical description, medical/dental records, DNA reference samples, clothing, personal effects, fingerprints | Antemortem team (from family, medical providers, dentists) |
| Pink (PM) | Postmortem data: autopsy findings, dental charting, fingerprints, DNA samples, personal effects found on remains, radiographs | Postmortem team (at temporary morgue) |
| White | Reconciliation: systematic comparison of AM and PM data for each proposed identification match | Reconciliation team |
| Green | Property: documentation of personal effects and property recovered at the scene | Property team |
Temporary Morgue Operations
A temporary morgue (disaster mortuary) is established near the disaster site with functional areas: receiving/triage (intake, logging, photography, radiography), pathology (external examination, autopsy when indicated), dental (charting and radiography), fingerprint, DNA sampling (buccal swab, bone, tooth), personal effects, and cold storage (refrigerated trailers or containers). The DMORT (Disaster Mortuary Operational Response Team) system in the United States deploys portable mortuary facilities and trained personnel under FEMA coordination.
Triage of Remains
Commingled, fragmented, and burned remains require triage: separating human from non-human material, sorting fragments by anatomic region, and attempting physical reassociation (matching fragments by fracture patterns, tissue type, DNA, or radiographic comparison). Each separate set of remains receives a unique identifier. Partial identifications (identifying a fragment rather than a complete body) may be necessary, with subsequent reassociation as additional fragments are identified.
Reconciliation
Reconciliation is the process of matching antemortem (AM) data with postmortem (PM) data to achieve a positive identification. Identification criteria: (1) dental comparison (most useful for intact remains), (2) fingerprints, (3) DNA (essential for fragmented/commingled remains), (4) radiographic comparison, (5) unique medical devices or implants. A reconciliation board composed of forensic pathologists, odontologists, anthropologists, and DNA analysts reviews each proposed match and issues or rejects the identification.
Psychological Support
DVI work is psychologically taxing. Responder well-being measures include: mandatory rest rotations, on-site mental health support, critical incident stress debriefing (CISD), monitoring for secondary traumatic stress and compassion fatigue, and long-term follow-up. Studies show that DVI responders have elevated rates of PTSD, depression, and substance use compared with matched controls.
Types of Mass Disasters
| Category | Examples | Forensic Challenges |
|---|---|---|
| Closed (known population) | Aircraft crash, building collapse with occupant list, ship sinking | Manifest or occupant list exists; AM data collection focused; identification goal is 100% |
| Open (unknown population) | Earthquake, tsunami, terrorist attack in public space | No definitive list of victims; PM identification must await AM data from missing person reports; may be impossible to identify all victims |
| Mixed | Hotel collapse (guests + staff + visitors) | Partial manifest; some victims unaccounted for; AM data collection more complex |
Chain of custody in mass events is particularly challenging because of the sheer volume of remains, personal effects, and specimens. Bar-code and RFID-based tracking systems are essential. Each fragment of remains receives a unique alphanumeric identifier at the point of recovery, and all subsequent movements, sampling, and analyses are logged against that identifier. Digital photography with embedded metadata (GPS coordinates, timestamp) supplements written documentation.
20 Child Abuse & Elder Abuse — Forensic Aspects
Non-accidental trauma (NAT) in children and abuse/neglect of the elderly require careful forensic evaluation to distinguish inflicted injury from accidental or natural causes. The forensic pathologist, clinician, and social worker each play critical roles.
Non-Accidental Trauma Patterns in Children
Certain injury patterns are highly suspicious for abuse when the history is absent, vague, inconsistent, or incompatible with the child's developmental capabilities:
Bruising: Any bruising in a non-mobile infant ("those who don't cruise rarely bruise"); bruising on ears, neck, trunk, buttocks, or genitalia; patterned bruises (belt, cord loop, bite marks). Burns: Immersion burns with sharp lines of demarcation and stocking/glove distribution (hands/feet held in hot water); cigarette burns (circular, 8–10 mm); iron burns (triangular patterned burn); sparing of flexural creases (child draws extremity away from water). Fractures: Multiple fractures in different stages of healing; CML; posterior rib fractures; any fracture in a non-ambulatory infant. Head injury: Subdural hematomas (especially bilateral or different ages), retinal hemorrhages, encephalopathy without credible accidental mechanism. Abdominal injuries: Duodenal/jejunal hematomas, pancreatic pseudocysts, hepatic/splenic lacerations from direct blows (second leading cause of death from child abuse after head trauma).
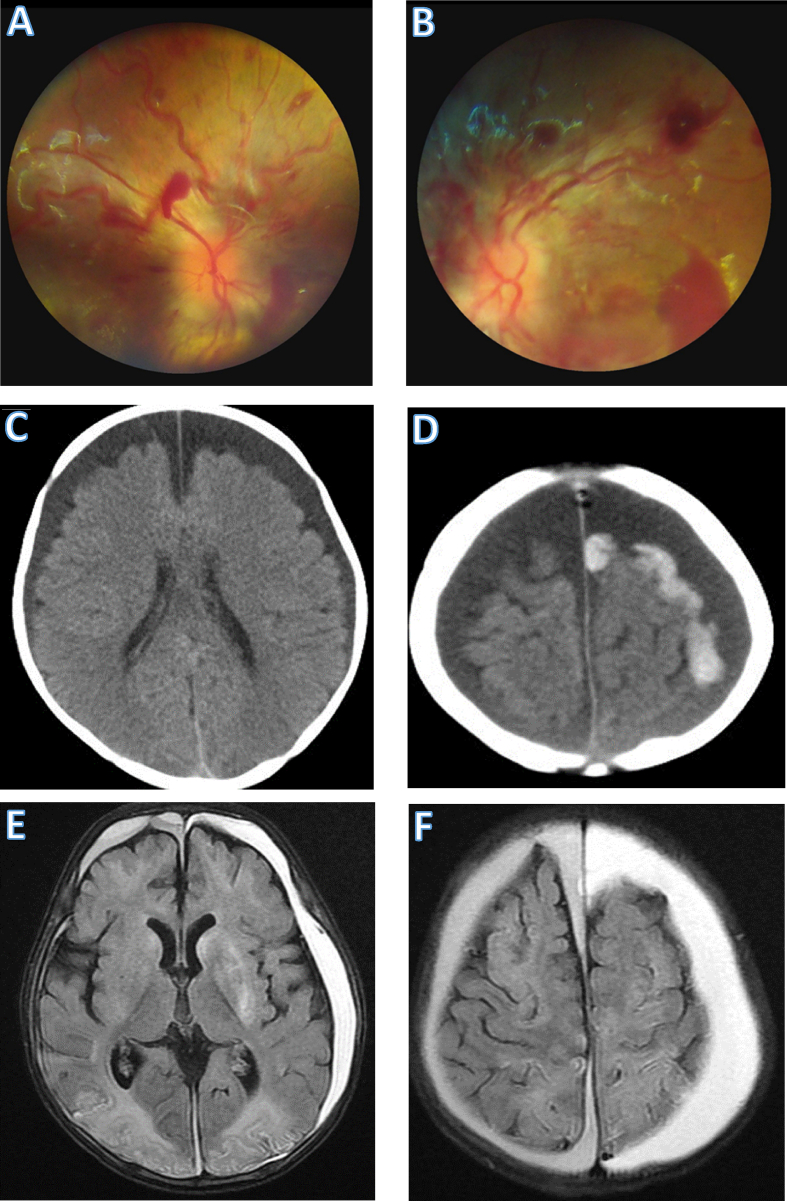
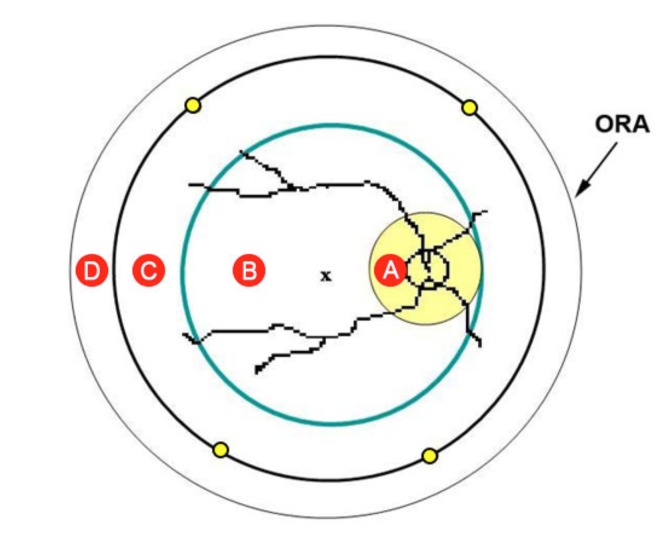
Mandated Reporting
All 50 U.S. states have mandatory reporting laws. Mandated reporters (physicians, nurses, social workers, teachers, law enforcement, and others) are legally required to report suspected child abuse or neglect to child protective services. The standard for reporting is reasonable suspicion, not certainty. Failure to report is a misdemeanor in most jurisdictions. Good faith reporters are protected from civil and criminal liability.
Elder Abuse
Elder abuse encompasses: physical abuse (unexplained bruises, fractures, burns; similar pattern analysis as in child abuse), neglect (malnutrition, dehydration, pressure ulcers, poor hygiene, untreated medical conditions), psychological/emotional abuse (verbal threats, isolation, humiliation), financial exploitation (unauthorized use of funds, coerced changes to wills/trusts), and sexual abuse. Forensic evaluation follows the same principles as child abuse assessment: detailed injury documentation, correlation with history, assessment of vulnerability and risk factors. Adult protective services is the reporting agency for elder abuse.
Documentation Standards
Thorough documentation is essential for legal proceedings: (1) high-quality photographs with scale (overall, mid-range, close-up), (2) precise written descriptions of every injury (type, size, shape, color, location), (3) verbatim documentation of explanations provided by caregivers, (4) developmental assessment of the child (what the child can and cannot do physically), (5) medical records review including growth charts and previous visits, (6) skeletal survey and head CT when indicated. Forensic medical records may be subpoenaed months or years after the examination; they must stand alone as a complete record.
Abdominal Injuries in Child Abuse
Abdominal trauma is the second leading cause of death from child abuse (after head trauma) and is frequently occult on external examination. The mechanism is typically a direct blow or compression of the abdomen against the vertebral column. Characteristic findings include: duodenal or jejunal hematoma (or rupture), pancreatic laceration or pseudocyst, hepatic laceration, mesenteric tears with hemoperitoneum, and adrenal hemorrhage. These injuries are uncommon from accidental mechanisms in the age group affected (typically infants and toddlers) and should prompt thorough investigation for non-accidental trauma. At autopsy, the peritoneal cavity must be examined carefully for hemoperitoneum, and all viscera inspected for contusion, laceration, and perforation.
21 Sexual Assault Examination
The forensic examination of sexual assault victims requires a trauma-informed approach that prioritizes patient welfare while systematically collecting evidence that may be critical for prosecution. Sexual Assault Forensic Examiners (SAFEs) or Sexual Assault Nurse Examiners (SANEs) are specially trained clinicians who perform these examinations.
SAFE/SANE Protocols
The examination follows a standardized protocol: (1) informed consent (the patient may decline any or all parts of the examination), (2) medical history (menstrual history, consensual intercourse within 5 days, tampon/douche use, prior injuries), (3) detailed history of assault (acts described, orifices involved, ejaculation, condom use, lubricant), (4) general physical examination (head-to-toe for injuries), (5) anogenital examination, (6) evidence collection, (7) STI prophylaxis (gonorrhea, chlamydia, trichomoniasis, HIV PEP if indicated), (8) pregnancy prevention (emergency contraception if applicable), and (9) safety planning and follow-up referrals.
Evidence Collection Timeline
The evidence collection window is generally up to 72 hours for adults and up to 120 hours (5 days) in some jurisdictions, though evidence quality diminishes with time. Spermatozoa may be recovered from the cervix for up to 5 days, from the vagina for up to 72 hours, and from the rectum or oral cavity for shorter periods. Non-sperm DNA (skin cells, saliva) may persist on the body or clothing for variable periods. The kit should be collected as soon as possible after the assault for optimal evidence yield.
Kit Components
A standard sexual assault evidence kit includes: clothing (placed in paper bags), oral swabs, vaginal swabs (from external genitalia, vaginal vault, and endocervix), anal/rectal swabs, penile swabs (if indicated), fingernail clippings/scrapings, pubic hair combings, buccal swab (patient's DNA reference), blood sample (toxicology if drug-facilitated assault suspected), and debris collection envelopes. Each item is packaged separately, sealed, and labeled with chain-of-custody documentation.
Anogenital Examination
The anogenital examination is conducted in the lithotomy position using adequate lighting. Findings are documented using colposcopy (magnified photography) and annotated body diagrams. Anogenital injuries in assault include: posterior fourchette tears/abrasions, hymenal tears (acute tears vs healed transections), vaginal wall lacerations, perianal lacerations/abrasions, and bruising. However, the absence of anogenital injury does not exclude sexual assault — studies show that 50–70% of confirmed sexual assaults have no visible anogenital injury, particularly in adult women. Findings must be interpreted in context of the reported acts, the time since assault, and the patient's anatomy.
Toxicology for Drug-Facilitated Assault
When drug-facilitated sexual assault (DFSA) is suspected, blood and urine specimens should be collected as early as possible. A urine specimen of at least 100 mL is preferred (many drugs are concentrated in urine). Many DFSA agents (GHB, short-acting benzodiazepines) have detection windows measured in hours, making rapid collection critical. If collection is delayed beyond the blood/urine detection window, hair analysis (collected 4–6 weeks after the event to allow hair growth) can detect most drugs.
Trauma-Informed Care
Trauma-informed principles include: explaining each step before performing it, obtaining consent throughout, allowing the patient to control the pace, providing a support person (advocate), avoiding retraumatizing language, and maintaining a calm, nonjudgmental demeanor. The examination should be conducted in a private, dedicated space. The examiner does not determine whether an assault occurred — the examiner documents findings and collects evidence; determination of whether a crime occurred is a legal function.
Documentation & Reporting
The forensic examination report includes: patient demographics, history of assault as reported by the patient (documented in the patient's own words when possible), general physical examination findings, detailed anogenital examination findings documented by description, diagrams, and colposcopic photographs, evidence collected and to whom it was released, medications provided (STI prophylaxis, emergency contraception), referrals made, and follow-up plan. Many jurisdictions allow patients to undergo evidence collection without making a police report (anonymous or non-report kits), preserving evidence for a statutory period in case the patient later decides to report. The SAFE/SANE report may be subpoenaed; it must be factual, objective, and free of opinions about whether an assault occurred unless the examiner is specifically asked to opine on injury mechanism consistency.
22 Expert Testimony & Legal Process
The forensic pathologist frequently serves as an expert witness in criminal and civil proceedings. Expert testimony requires not only technical knowledge but also an understanding of the legal framework, evidentiary standards, and the responsibilities of the expert.
Qualification as an Expert Witness
Two major standards govern the admissibility of expert testimony in the United States:
| Standard | Origin | Criteria | Jurisdictions |
|---|---|---|---|
| Daubert standard | Daubert v. Merrell Dow Pharmaceuticals (1993) | The judge acts as gatekeeper; testimony must be based on: (1) testable/falsifiable theory, (2) peer-reviewed methodology, (3) known error rate, (4) general acceptance within the scientific community. Superseded by Federal Rules of Evidence 702. | Federal courts and ~36 states |
| Frye standard | Frye v. United States (1923) | The scientific technique must be "generally accepted" in the relevant scientific community | ~14 states (including California, New York, Illinois) |
Report Writing
The forensic pathology report is a medical-legal document that must be: (1) factually complete (documenting all findings, positive and negative), (2) clearly organized (case history, external examination, internal examination, microscopic, toxicology, opinion), (3) written in language that is precise yet understandable to a non-medical audience, (4) free of unsupported speculation, and (5) issued in a timely manner. Opinions should be stated with qualifiers that accurately reflect the certainty level: "consistent with," "suggestive of," or "diagnostic of."
Deposition vs Trial Testimony
A deposition is pretrial sworn testimony given in the presence of attorneys but outside the courtroom; it is used for discovery and to preserve testimony. Trial testimony occurs in the courtroom before a judge and/or jury. In both settings, the expert is first qualified (credentials established on the record), then provides direct examination testimony (questioned by the retaining attorney), followed by cross-examination (questioned by opposing counsel), with potential redirect and recross.
Reasonable Medical Certainty
The phrase "to a reasonable degree of medical certainty" (or "medical probability") is the legal threshold for expert medical opinions. It means "more likely than not" (probability >50%) — not absolute certainty. Some jurisdictions use "reasonable medical certainty" and "reasonable medical probability" interchangeably; others distinguish them. The expert should clarify the standard being used and state opinions within that framework.
Cross-Examination Preparation & Bias Awareness
Effective cross-examination preparation includes: thorough familiarity with the case file, anticipation of challenges to methodology and conclusions, awareness of published literature that may contradict the opinion, and practice with the retaining attorney. The expert must be aware of potential cognitive biases: confirmation bias (interpreting findings to fit a predetermined theory), contextual bias (being influenced by non-medical case information), and adversarial allegiance (opinions unconsciously favoring the retaining party). NAME ethical guidelines emphasize that the expert's obligation is to the truth, not to either party.
Common Cross-Examination Strategies
Opposing counsel may employ several strategies to challenge the forensic pathologist's testimony: (1) challenging qualifications (questioning experience with the specific type of case), (2) learned treatise confrontation (citing published sources that contradict the expert's opinion), (3) hypothetical questions (asking whether alternative explanations are possible), (4) prior inconsistent statements (comparing current testimony with prior depositions, publications, or testimony in other cases), (5) compensation questioning (exploring financial motivation), and (6) scope creep (leading the expert to opine outside their area of expertise). The expert should answer truthfully, concede appropriate points, stay within their area of competence, and avoid becoming adversarial.
23 Legal Standards in Death Investigation
The forensic pathologist must understand the legal framework within which death investigation operates, including the distinctions between legal and medical terminology and the standards of proof applied in various legal proceedings.
Homicide vs Murder
In forensic medicine, homicide as a manner of death simply means "death at the hand of another." It is a neutral descriptive classification and does not imply criminal liability. Murder is a legal conclusion reached by a court, requiring proof of unlawful killing with malice aforethought (intent). Not all homicides are murders: justifiable homicide (lawful use of deadly force in self-defense or by law enforcement), excusable homicide (accidental killing without criminal negligence), and negligent homicide / manslaughter (degrees of culpability below murder) are all certified as "homicide" manner of death by the forensic pathologist while the legal system determines the level of criminal responsibility.
Standards of Proof
| Standard | Threshold | Application |
|---|---|---|
| Beyond a reasonable doubt | Approximately 95–99% certainty (not precisely quantifiable) | Criminal proceedings (prosecution must prove guilt to this standard) |
| Clear and convincing evidence | Approximately 75% certainty | Certain civil proceedings (fraud, will contests, termination of parental rights) |
| Preponderance of the evidence | >50% (more likely than not) | Most civil proceedings (tort, negligence, malpractice); also the standard for expert medical opinions |
| Probable cause | Reasonable belief based on factual evidence | Arrest warrants, search warrants |
| Reasonable suspicion | Articulable facts suggesting possible involvement | Investigative stops (Terry stop); mandatory abuse reporting |
Evidentiary Standards for Forensic Evidence
Physical evidence from the autopsy (projectiles, trace evidence, toxicology specimens) must meet admissibility requirements: proper collection and preservation, documented chain of custody, analysis by qualified personnel using validated methods, and reporting within laboratory accreditation standards. The Locard exchange principle ("every contact leaves a trace") provides the theoretical foundation for trace evidence analysis. Forensic laboratories should be accredited by bodies such as ANAB (ANSI National Accreditation Board) or A2LA.
Criminal Negligence & Medical Malpractice Deaths
When death results from medical treatment, the forensic pathologist must determine whether the death was due to the underlying disease, a recognized complication of treatment, or negligent care. Deaths from medical negligence may be certified as therapeutic complication (manner: accident) or, in egregious cases of gross deviation from the standard of care, as homicide. The distinction between expected complication, negligence, and gross negligence is ultimately a legal determination, but the forensic pathologist provides the medical foundation by establishing the causal relationship between the act or omission and the death.
Degrees of Homicide in Common Law
| Classification | Mental State (Mens Rea) | Definition |
|---|---|---|
| First-degree murder | Premeditation and deliberation | Intentional killing with advance planning; also includes felony murder (killing during commission of certain felonies) |
| Second-degree murder | Malice aforethought without premeditation | Intentional killing in the heat of the moment; extreme recklessness showing depraved indifference to human life |
| Voluntary manslaughter | Intentional but provoked | Killing in the heat of passion upon adequate provocation; "imperfect" self-defense |
| Involuntary manslaughter | Criminal negligence or during misdemeanor | Unintentional killing resulting from recklessness or criminal negligence; misdemeanor manslaughter |
| Justifiable homicide | None (legally justified) | Lawful use of deadly force: self-defense, defense of others, law enforcement in the line of duty |
The forensic pathologist certifies the manner of death as "homicide" without distinguishing between these legal categories. The legal classification is determined by the prosecutor, judge, and jury based on the totality of evidence including but not limited to the forensic findings.
24 Ethical Issues in Forensic Medicine
Forensic medicine raises unique ethical challenges that distinguish it from clinical medicine. The forensic pathologist serves the public interest and the justice system rather than an individual patient, creating a fundamentally different physician relationship.
Dual Agency
The forensic pathologist's primary obligation is to the truth and the justice system, not to any individual party. Unlike clinical medicine, where the physician-patient relationship creates a duty of care and loyalty to the patient, the forensic pathologist serves as an impartial scientist. This dual agency problem becomes acute when testimony may harm the interests of the decedent's family (e.g., ruling suicide in a life insurance case) or when retained as an expert for one side of a legal dispute. The forensic pathologist must resist pressure from law enforcement, prosecutors, defense attorneys, or families to reach a predetermined conclusion.
Consent for Forensic Examination
In medicolegal death investigation, autopsy may be performed without the consent of the next of kin if the death falls under statutory jurisdiction of the medical examiner/coroner. This distinguishes forensic autopsy from hospital (clinical) autopsy, which requires family consent. Families may object to autopsy on religious or personal grounds; the medical examiner may override these objections when the autopsy is legally mandated, but should strive to accommodate religious requirements when possible (e.g., expedited autopsy for same-day burial traditions). Living victims of assault or sexual assault must provide informed consent for forensic examination; an unconscious patient can be examined for life-threatening conditions under implied consent but evidence collection requires specific consent when the patient regains capacity. Minors require consent from a parent or guardian unless the jurisdiction provides exceptions for forensic examination in abuse cases.
Handling of Human Remains
Respect for human remains is a fundamental ethical obligation. Cultural and religious considerations must be accommodated when possible without compromising the medicolegal investigation: rapid return of the body for burial (Jewish and Muslim traditions), minimizing invasive procedures when acceptable alternatives exist (postmortem imaging as an adjunct), and respectful handling during autopsy. Retention of organs, tissues, or specimens for further study requires documentation and should follow institutional policies. Public display of autopsy photographs or findings violates the dignity of the decedent and is ethically prohibited except in the context of legitimate legal proceedings.
Organ Donation & Medicolegal Cases
Organ procurement from medicolegal cases requires coordination between the medical examiner/coroner and the organ procurement organization (OPO). The medical examiner has the legal authority to deny procurement if it would compromise the investigation (e.g., gunshot wound to the chest where heart/lung examination is essential). In practice, most medical examiners cooperate with organ procurement by documenting relevant findings before release, allowing recovery of organs that would not be affected by the investigation, and attending procurement to examine organs in situ.
Quality Assurance & Accreditation
The National Association of Medical Examiners (NAME) provides voluntary accreditation for medicolegal death investigation offices. Accreditation standards address: forensic pathologist staffing (no more than 250 autopsies per pathologist per year), facility standards, evidence handling, report turnaround time (90 days maximum for final reports), peer review processes, and continuing education. NAME accreditation serves as the benchmark for medicolegal death investigation quality in the United States.
Conflicts of Interest
Potential conflicts of interest in forensic medicine include: financial relationships with retaining attorneys (experts paid per case), institutional pressure from law enforcement or prosecutors to reach specific conclusions, personal relationships with involved parties, and political pressure on elected coroners. Mitigation strategies include: transparency regarding fees and relationships, institutional policies separating investigation from prosecution, blinded evidence review where possible, peer review of controversial cases, and adherence to professional ethics codes (NAME, College of American Pathologists). An expert whose opinions are consistently aligned with the retaining party regardless of the evidence undermines the credibility of forensic medicine as a scientific discipline.
Research Ethics
Research involving decedents raises unique ethical issues: informed consent cannot be obtained from the decedent, and consent from next of kin may be complicated by grief and the medicolegal context. Institutional review boards (IRBs) have varying approaches to postmortem research; many classify autopsy tissue research as exempt from informed consent requirements because the decedent is not a "human subject" under federal regulations. However, retention of tissues, photographs, or genetic material for research purposes should be governed by institutional policies that balance scientific value with respect for the deceased and their family's wishes.
25 Postmortem Changes Timeline
The following comprehensive table integrates all major postmortem changes with their approximate timelines under standard temperate conditions (~20°C ambient temperature). All timelines are approximate ranges and are significantly affected by environmental conditions, body habitus, cause of death, and clothing. This table is intended as a quick reference; detailed discussion of each parameter appears in Section 3.
Temperature: The single most important variable. Heat accelerates all biological processes (roughly doubling decomposition rate for every 10°C increase). Cold slows all processes; freezing essentially halts decomposition. Body habitus: Obese individuals cool more slowly (greater insulating mass), develop rigor more slowly, but may decompose faster (larger anaerobic bacterial reservoir and more substrate for putrefaction). Cause of death: Septic deaths decompose faster (high bacterial load); exsanguinated bodies decompose more slowly (reduced bacterial substrate). Clothing and coverings: Insulate the body (slower cooling, potentially faster decomposition from retained heat), but may partially exclude insect access. Environment: Indoor vs outdoor, water submersion, burial depth, sun exposure, and wind all significantly affect the rates of all postmortem changes.
| Time After Death | Algor Mortis | Livor Mortis | Rigor Mortis | Decomposition | Other Markers |
|---|---|---|---|---|---|
| 0–30 min | Plateau phase; minimal cooling; rectal temperature near 37°C | Begins forming; not yet visible externally | Absent; flaccid | None externally visible; autolysis begins at cellular level | Corneal clouding begins (open eyes); pupillary dilation |
| 30 min–2 h | Slow initial cooling; sigmoid lag phase continues | Faint discoloration visible in dependent areas; blanches completely with pressure | Earliest onset in jaw, eyelids (Nysten's rule) | No external changes | Vitreous K+ begins to rise (~0.14 mEq/L/hour) |
| 2–4 h | Exponential cooling begins; rate ~0.5–1.5°C/hour | Clearly visible; remains unfixed; redistributes with repositioning | Developing; involves neck, upper extremities | No external changes | Tache noire (dry corneal discoloration) in open eyes |
| 4–8 h | Continues exponential cooling | Becoming more pronounced; partial blanching under pressure | Progressing to full rigor; lower extremities becoming involved | Green discoloration may begin at right iliac fossa (warmer environments) | Gastric contents emptying rate may provide interval estimates |
| 8–12 h | Approaching half equilibration | Fixation begins; does not fully redistribute with repositioning | Full rigor; all muscle groups rigid | Greenish discoloration spreading; early bloat in warm environments | Vitreous K+ 8–10 mEq/L |
| 12–24 h | Approaching ambient temperature in thin individuals | Fixed; does not blanch or redistribute | Maximum rigidity; beginning resolution in jaw | Marbling (venous pattern); skin slippage may begin; bloat progressing | Fly eggs developing into first-instar larvae |
| 24–48 h | Equilibrated with environment in most cases | Fixed permanently | Resolving; flaccidity returns (same order as onset) | Bloat; purging; strong odor; skin blistering; hair loosening | Second-instar larvae; vitreous K+ 15–20 mEq/L |
| 2–7 days | N/A (equilibrated) | Obscured by decomposition color change | Absent (fully resolved) | Active decay; tissue liquefaction; maggot masses; organ architecture losing integrity | Third-instar larvae; body weight loss accelerating |
| 1–4 weeks | N/A | N/A | N/A | Advanced decay; most soft tissue gone; bones becoming exposed; adipocere may begin in wet environments | Pupal stage; beetle succession; vitreous chemistry unreliable |
| >1 month | N/A | N/A | N/A | Skeletonization (outdoor, temperate); mummification (dry) or adipocere (wet) may preserve some features | Adult fly emergence; later insect succession waves |
26 Normal Organ Weights
Reference organ weights for autopsy. Values vary by sex, age, body habitus, and ethnicity. The following tables provide commonly used ranges for adults and pediatric age groups. These values are derived from the most commonly cited sources in forensic pathology (Ludwig 2002, Molina and DiMaio 2012, Schulz et al. 1996). All weights are in grams. Organs should be weighed after draining excess blood and removing attached structures (e.g., pericardium from heart, adherent fat from kidneys).
Adult Organ Weights
| Organ | Male (g) | Female (g) | Pathologic Significance |
|---|---|---|---|
| Heart | 300–350 | 250–300 | >400 g (M) or >350 g (F): cardiomegaly |
| Brain | 1300–1400 | 1200–1300 | >1500 g: edema; <1100 g: atrophy |
| Liver | 1400–1600 | 1200–1400 | >2000 g: hepatomegaly |
| Right lung | 450–500 | 350–450 | Combined >1000 g: edema/congestion/pneumonia |
| Left lung | 400–450 | 300–400 | Left slightly lighter due to cardiac impression |
| Right kidney | 125–170 | 115–155 | >200 g: renal hypertrophy or mass |
| Left kidney | 130–175 | 120–160 | Asymmetry >30 g: unilateral pathology |
| Spleen | 150–200 | 130–180 | >250 g: splenomegaly |
| Pancreas | 100–150 | 100–140 | Atrophy in chronic pancreatitis/DM |
| Thyroid | 25–35 | 20–30 | >40 g: goiter |
| Prostate | 20–25 | N/A | >30 g: BPH; >60 g: significant enlargement |
| Adrenal (each) | 4–6 | 4–6 | Atrophy: chronic steroid use; hypertrophy: Cushing, stress |
| Uterus (nulliparous) | N/A | 40–80 | >100 g: leiomyomata or adenomyosis |
| Thymus (adult) | 10–25 (involuted) | 10–25 (involuted) | Persistent thymic tissue: thymoma vs thymic hyperplasia |
Pediatric Organ Weights by Age
| Organ | Newborn (g) | 6 months (g) | 1 year (g) | 5 years (g) | 10 years (g) |
|---|---|---|---|---|---|
| Heart | 20–24 | 35–45 | 45–55 | 85–100 | 130–170 |
| Brain | 350–400 | 660–750 | 900–1000 | 1100–1250 | 1200–1350 |
| Liver | 100–130 | 230–290 | 300–360 | 480–600 | 700–900 |
| Lungs (combined) | 40–60 | 80–120 | 120–160 | 200–280 | 400–550 |
| Kidneys (each) | 10–15 | 25–35 | 35–45 | 55–70 | 70–100 |
| Spleen | 8–12 | 18–25 | 25–35 | 50–70 | 80–120 |
| Thymus | 8–15 | 15–25 | 20–30 | 25–35 | 25–40 |
27 Toxicology Reference Ranges
The following table provides approximate therapeutic, toxic, and potentially lethal blood concentrations for commonly encountered substances in forensic toxicology. All values are subject to individual variation, tolerance, postmortem redistribution, and analytical method differences. Postmortem levels must be interpreted with caution.
| Substance | Therapeutic / Normal | Toxic | Potentially Lethal | Notes |
|---|---|---|---|---|
| Ethanol (g/dL) | 0 | >0.30 | >0.40 | Legal limit 0.08 (driving); tolerance significantly affects lethality; check vitreous to exclude neoformation |
| Acetaminophen (mcg/mL) | 10–30 | >150 (at 4 hours) | >300 (at 4 hours) | Rumack-Matthew nomogram for clinical toxicity; hepatotoxicity is the lethal mechanism |
| Salicylate (mg/dL) | 15–30 | >40 | >80 | Mixed respiratory alkalosis and metabolic acidosis |
| Morphine (ng/mL) | 10–80 | >200 | >400 (non-tolerant) | Tolerant patients may survive much higher levels; check for 6-MAM |
| Fentanyl (ng/mL) | 1–3 | >3 (non-tolerant) | >7 (non-tolerant) | Extreme variation with tolerance; significant PMR; use femoral blood |
| Methadone (ng/mL) | 100–400 | >600 | >1000 | Long half-life (15–60 hours); QTc prolongation; significant PMR |
| Oxycodone (ng/mL) | 10–100 | >200 | >500 | Postmortem redistribution moderate; check for oxymorphone metabolite |
| Cocaine (ng/mL) | 50–300 (after use) | Variable | >1000 | Rapidly metabolized; presence of parent compound indicates recent use; check BZE |
| Methamphetamine (ng/mL) | 20–60 (therapeutic) | >200 | >500 | Chronic users tolerate higher levels; cardiac death may occur at lower levels |
| Alprazolam (ng/mL) | 10–50 | >100 | >200 (rare alone) | Benzodiazepines rarely lethal alone; synergistic with opioids/alcohol |
| Diazepam (ng/mL) | 100–750 | >1500 | >5000 (rare alone) | Active metabolite nordiazepam; both should be measured |
| Amitriptyline (ng/mL) | 80–200 (with nortriptyline) | >500 | >1000 | Sodium channel blockade → QRS widening → fatal arrhythmia; significant PMR |
| Carboxyhemoglobin (%) | <3 (non-smoker); 3–10 (smoker) | >20 (symptomatic) | >50–60 | Cherry-red coloration at >30%; always test in fire deaths |
| Cyanide (mg/L, whole blood) | <0.1 | 0.5–1.0 | >1.0 | Rapidly degrades postmortem; collect and analyze promptly; NaF preservative |
| Methanol (mg/dL) | 0 | >20 | >80 | Formic acid causes retinal/CNS toxicity; elevated osmolal gap |
| Ethylene glycol (mg/dL) | 0 | >20 | >200 | Calcium oxalate crystals in urine/renal tissue; elevated osmolal gap then anion gap |
| Digoxin (ng/mL) | 0.8–2.0 | >2.5 | >5.0 | Massive PMR (C/P ratio 5–10); postmortem levels unreliable for clinical interpretation |
| Lithium (mEq/L) | 0.6–1.2 | >1.5 | >3.5 | Narrow therapeutic index; renal clearance; check creatinine |
| GHB (mg/L) | 0 (endogenous <4) | >50 | >250 | Postmortem production occurs; rapidly eliminated; detection window ~8 hours in blood |
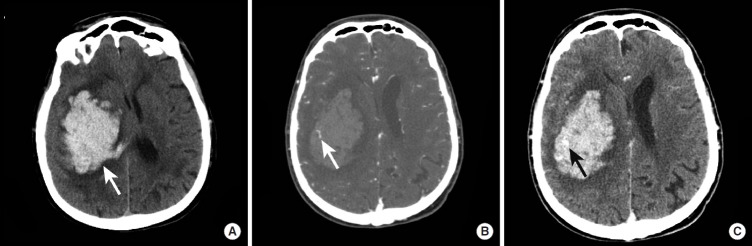
28 Abbreviations Master List
Comprehensive listing of abbreviations used throughout forensic medicine, organized alphabetically for rapid reference. This master list consolidates abbreviations from all sections and adds additional entries commonly encountered in forensic pathology reports, toxicology reports, and medicolegal documents.
| Abbreviation | Full Term |
|---|---|
| 6-MAM | 6-monoacetylmorphine (heroin metabolite) |
| ABFA | American Board of Forensic Anthropology |
| ABFO | American Board of Forensic Odontology |
| ABFT | American Board of Forensic Toxicology |
| ABMDI | American Board of Medicolegal Death Investigators |
| AC | Alternating current |
| ACE-V | Analysis, Comparison, Evaluation, Verification (fingerprint methodology) |
| ADD | Accumulated degree days |
| ADH | Accumulated degree hours |
| AFIS | Automated Fingerprint Identification System |
| AHT | Abusive head trauma |
| AM | Antemortem |
| ANAB | ANSI National Accreditation Board |
| ASSB | Accidental suffocation and strangulation in bed |
| BAC | Blood alcohol concentration |
| BFI | Blunt force injury |
| BZE | Benzoylecgonine (cocaine metabolite) |
| CML | Classic metaphyseal lesion |
| CO | Carbon monoxide |
| COD | Cause of death |
| CODIS | Combined DNA Index System |
| COHb | Carboxyhemoglobin |
| C/P ratio | Central-to-peripheral blood concentration ratio |
| CISD | Critical incident stress debriefing |
| DC | Direct current |
| DFSA | Drug-facilitated sexual assault |
| DIC | Disseminated intravascular coagulation |
| DMORT | Disaster Mortuary Operational Response Team |
| DNA | Deoxyribonucleic acid |
| DVI | Disaster victim identification |
| EDTA | Ethylenediaminetetraacetic acid (anticoagulant) |
| ELISA | Enzyme-linked immunosorbent assay |
| FEMA | Federal Emergency Management Agency |
| FRE | Federal Rules of Evidence |
| GC-MS | Gas chromatography–mass spectrometry |
| GHB | Gamma-hydroxybutyrate |
| GSW | Gunshot wound |
| H&E | Hematoxylin and eosin stain |
| HCN | Hydrogen cyanide |
| ICAM-1 | Intercellular adhesion molecule-1 |
| IHC | Immunohistochemistry |
| LC-MS/MS | Liquid chromatography–tandem mass spectrometry |
| ME | Medical examiner |
| MLI | Medicolegal death investigator |
| MOD | Manner of death |
| mtDNA | Mitochondrial DNA |
| NaF | Sodium fluoride (preservative) |
| NAME | National Association of Medical Examiners |
| NAT | Non-accidental trauma |
| OPO | Organ procurement organization |
| PCR | Polymerase chain reaction |
| PDA | Posterior descending artery |
| PM | Postmortem |
| PMCT | Postmortem computed tomography |
| PMI | Postmortem interval |
| PMMR | Postmortem magnetic resonance imaging |
| PMR | Postmortem redistribution |
| PTSD | Post-traumatic stress disorder |
| SAFE | Sexual assault forensic examiner |
| SANE | Sexual assault nurse examiner |
| SBS | Shaken baby syndrome (now AHT) |
| SFI | Sharp force injury |
| SIDS | Sudden infant death syndrome |
| STI | Sexually transmitted infection |
| STR | Short tandem repeat |
| SUID | Sudden unexpected infant death |
| TOD | Time of death |
| Y-STR | Y-chromosome short tandem repeat |
| Abbreviation | Full Term |
|---|---|
| A2LA | American Association for Laboratory Accreditation |
| APP (beta-APP) | Beta-amyloid precursor protein (axonal injury marker) |
| BSA | Body surface area |
| CISD | Critical incident stress debriefing |
| CML | Classic metaphyseal lesion |
| DAI | Diffuse axonal injury |
| DUI/DWI | Driving under the influence / driving while intoxicated |
| ED | Emergency department |
| ER | Emergency room |
| GSR | Gunshot residue |
| HIV PEP | Human immunodeficiency virus post-exposure prophylaxis |
| IPV | Intimate partner violence |
| LVOT | Left ventricular outflow tract |
| MAP | Mean arterial pressure |
| MVA / MVC | Motor vehicle accident / motor vehicle collision |
| NCHS | National Center for Health Statistics |
| PEP | Post-exposure prophylaxis |
| QTc | Corrected QT interval |
| RBC | Red blood cell |
| RUDS | Rapid unplanned drug screen |
| TBI | Traumatic brain injury |
| TBSA | Total body surface area |
| UV | Ultraviolet |
| VF / VT | Ventricular fibrillation / ventricular tachycardia |
| WHO | World Health Organization |
DiMaio VJ, DiMaio D. Forensic Pathology (2nd ed, CRC Press): the standard reference textbook. Spitz WU. Spitz and Fisher's Medicolegal Investigation of Death (5th ed, Charles C Thomas): comprehensive forensic pathology reference. Dolinak D, Matshes E, Lew E. Forensic Pathology: Principles and Practice (Elsevier): practical case-based approach. Dettmeyer RB. Forensic Histopathology (Springer): essential for microscopic forensic diagnosis. Baselt RC. Disposition of Toxic Drugs and Chemicals in Man (Biomedical Publications): the definitive toxicology reference for postmortem drug interpretation.