Medical Ethics & Bioethics
The four principles of biomedical ethics, informed consent, capacity and competence, surrogate decision-making, end-of-life care, confidentiality, professionalism, conflicts of interest, research ethics, and every ethical principle and clinical scenario across the full scope of medical ethics.
01 Overview & Significance
Medical ethics is the systematic analysis of moral obligations and values that govern the practice of medicine. It answers the question, "What should a physician do?" when technical capability is not enough — when the answer depends on what is right, fair, honest, or kind. Every clinical encounter involves ethical judgment: how much to disclose, how strongly to recommend, how to honor preferences, how to balance risks and benefits, and how to allocate finite resources. The field provides structured frameworks that allow physicians, patients, and institutions to reason through dilemmas in a principled, transparent way.
Ethics is not a soft adjunct to medicine — it is the core of the physician–patient relationship. Informed consent, confidentiality, end-of-life decisions, and professional boundaries are tested on every USMLE exam and encountered daily in practice. Getting them wrong causes harm, erodes trust, and exposes clinicians to legal and regulatory consequences.
Core Domains of Medical Ethics
| Domain | Central Question |
|---|---|
| Clinical ethics | What should be done for this patient in this situation? |
| Research ethics | How can knowledge be generated while protecting human subjects? |
| Public health ethics | How are population benefits balanced against individual liberties? |
| Organizational ethics | How should institutions align mission, finances, and patient welfare? |
| Professional ethics | What obligations do physicians owe patients, colleagues, and society? |
Ethics vs Law vs Morality
Ethics, law, and personal morality overlap but are distinct. Ethics is reasoned analysis of right action grounded in principles. Law is codified, enforceable rules set by the state. Morality reflects individual or cultural beliefs about right and wrong. Most ethical obligations are also legal (e.g., confidentiality), but some legal acts are unethical (exploitative advertising) and some ethical acts may be illegal (civil disobedience). When in doubt on an exam, the answer is usually what is ethical, not merely what is legally permitted.
Scope of Medical Ethics in Clinical Practice
Medical ethics touches every clinical encounter, but it becomes visible in recurring categories of decisions. These categories, which structure this reference, are: consent and refusal, capacity and surrogacy, end-of-life care, confidentiality and disclosure, professional boundaries, conflicts of interest, resource allocation, and research. Each has its own literature, case law, and professional guidance, but all are unified by the same small set of principles and by the physician's overriding commitment to the welfare of the patient.
The Physician as Fiduciary
The physician–patient relationship is a fiduciary relationship: one party (the physician) has specialized knowledge and power, and the other (the patient) is vulnerable and dependent on the first to act in good faith. Fiduciary relationships generate heightened duties of loyalty, honesty, competence, and self-restraint. Recognizing the relationship as fiduciary — not merely contractual — explains why self-dealing, deception, boundary violations, and exploitation of dependency are taken so seriously in medical ethics.

02 History of Medical Ethics
Medical ethics has evolved from ancient professional codes grounded in physician virtue to modern frameworks emphasizing patient rights, informed consent, and social justice. The arc of this evolution — from paternalism to shared decision-making — is itself a core lesson about how the discipline functions.
Ancient Foundations
Moral codes for healers are older than recorded history. Egyptian, Babylonian, Indian (Charaka Samhita), and Chinese medical traditions all contain ethical injunctions about honesty, competence, and devotion to patients. The Western canonical starting point is the Hippocratic tradition, but it should be understood as one expression of a much older, cross-cultural recognition that medicine carries moral weight.
Hippocratic Oath (circa 400 BCE)
The Hippocratic Oath, attributed to Hippocrates of Cos, is the earliest surviving Western document articulating physician duties. It emphasizes beneficence ("I will apply dietetic measures for the benefit of the sick"), non-maleficence ("I will keep them from harm and injustice"), confidentiality, and prohibitions against abortion, euthanasia, and sexual relationships with patients. Modern variants are still recited at medical school graduations, though the prohibitions have been revised to reflect contemporary values. The oath represents the first codification of medicine as a profession with duties that transcend self-interest.
Nuremberg Code (1947)
Following the prosecution of Nazi physicians for lethal human experiments, the Nuremberg Code established ten principles for ethical research on humans. Its cornerstone is the absolute requirement for voluntary informed consent: "The voluntary consent of the human subject is absolutely essential." Other principles include favorable risk–benefit ratio, freedom to withdraw, scientific validity, and qualified investigators. The Nuremberg Code transformed research ethics and is the ancestor of all modern human subjects protections.
Declaration of Helsinki (1964, revised)
Promulgated by the World Medical Association, the Declaration of Helsinki extends Nuremberg by introducing the distinction between therapeutic and non-therapeutic research, emphasizing review by independent committees (the forerunner of IRBs), requiring special protections for vulnerable subjects, and affirming that the well-being of the individual research subject must take precedence over the interests of science and society.
Tuskegee & the Belmont Report (1979)
The Tuskegee Syphilis Study (1932–1972) followed 399 Black men with untreated syphilis without disclosure or consent, even after penicillin became standard therapy in 1947. Its exposure prompted the National Research Act and the Belmont Report, which articulated three foundational principles for research ethics that underlie modern IRB review:
| Belmont Principle | Application |
|---|---|
| Respect for persons | Informed consent; protection for those with diminished autonomy |
| Beneficence | Maximize benefits, minimize harms; favorable risk–benefit assessment |
| Justice | Fair subject selection; burdens and benefits distributed equitably |
From Paternalism to Autonomy
Through most of the 20th century, American medicine was explicitly paternalistic: physicians routinely withheld cancer diagnoses, made decisions without patient input, and viewed disclosure of uncertainty as undermining care. Landmark court cases (Schloendorff 1914, Canterbury v. Spence 1972, Quinlan 1976, Cruzan 1990) progressively established the right of patients to refuse treatment, to be informed, and to have surrogates act on their behalf. By the 1980s, the patient autonomy model had become dominant, and shared decision-making emerged as the contemporary ideal.

03 Ethical Theories & Frameworks
Normative ethical theories provide the philosophical foundations from which medical principles are derived. No single theory resolves every dilemma; experienced ethicists draw on multiple frameworks depending on context. Understanding each theory helps clarify why reasonable people disagree and where moral intuitions come from.
Why Theory Matters at the Bedside
Clinicians sometimes dismiss ethical theory as academic, but theory shapes everyday reasoning whether we notice or not. Understanding the theories lets clinicians name their intuitions, examine whether those intuitions are consistent, and converse productively with colleagues whose reasoning starts from different premises. In contested cases, naming the theory behind a disagreement is often the first step to resolving it.
Deontology (Kantian Ethics)
Deontology, from the Greek deon ("duty"), holds that the morality of an action depends on whether it conforms to rules or duties, regardless of consequences. Immanuel Kant's categorical imperative requires acting only on principles that could be universalized and treating persons as ends in themselves, never merely as means. In medicine, deontology grounds absolute prohibitions: never lie to a patient, never use a patient as a means to benefit another, never violate confidentiality for convenience. Its strength is moral clarity; its weakness is rigidity when duties conflict.
Consequentialism & Utilitarianism
Consequentialism judges actions solely by their outcomes. Utilitarianism (Bentham, Mill) seeks to maximize aggregate well-being — the greatest good for the greatest number. In medicine, utilitarian reasoning underlies cost-effectiveness analysis, triage in mass casualty events, public health policy, and transplant allocation. Its strength is that it takes consequences seriously; its weakness is that it may sanction harming an individual if this produces greater aggregate benefit.
Virtue Ethics
Virtue ethics, originating with Aristotle, focuses on character rather than rules or outcomes. The ethical question becomes, "What would a virtuous physician do?" Relevant virtues include compassion, honesty, courage, prudence, integrity, and humility. Virtue ethics captures much of what makes a physician "good" beyond technical skill and aligns with the professional identity model of medical education. Its weakness is that it provides limited guidance in genuine dilemmas.
Principlism
Developed by Tom Beauchamp and James Childress in Principles of Biomedical Ethics (1979), principlism proposes four mid-level principles — autonomy, beneficence, non-maleficence, and justice — that practicing clinicians can apply directly without committing to any single overarching theory. Principlism has become the dominant framework in clinical ethics worldwide because it is pragmatic, teachable, and bridges theoretical disagreements.
Other Approaches
| Framework | Core Idea |
|---|---|
| Care ethics | Morality grounded in relationships, empathy, and responsiveness (Gilligan, Noddings) |
| Narrative ethics | Moral understanding through attending to patient stories and context |
| Casuistry | Case-based reasoning from paradigm examples, analogous to common law |
| Feminist ethics | Attention to power, vulnerability, and historically marginalized perspectives |
| Communitarian ethics | Values arise from and are sustained by communities, not isolated individuals |
Comparing Frameworks on a Single Case
Consider a terminally ill patient who requests aid in dying where it is legal. Each framework highlights different considerations:
| Framework | Analysis |
|---|---|
| Deontology | Prohibits intentional killing as inherently wrong, regardless of request or benefit |
| Utilitarianism | Weighs relief of suffering, autonomy, effects on family, and societal effects of normalization |
| Virtue ethics | Asks whether a compassionate, honest physician could participate with integrity |
| Principlism | Balances autonomy, beneficence (relief), non-maleficence (causing death), and justice (access) |
| Care ethics | Centers the relationship and the patient's particular situation, not abstract rules |



04 Codes of Ethics & Principlism
Professional codes translate abstract principles into concrete rules that govern everyday practice. They serve four functions: articulating shared norms, guiding individual conduct, holding the profession accountable, and signaling commitments to patients and society.
Function of Professional Codes
Professional codes do not create ethical obligations out of nothing; they articulate, consolidate, and update commitments the profession has already made. They are most useful as educational tools, as touchstones in disputed cases, as evidence of professional consensus, and as public declarations that the profession takes its duties seriously.
AMA Code of Medical Ethics
First adopted in 1847, the AMA Code is the oldest and most influential professional code in American medicine. It is maintained by the Council on Ethical and Judicial Affairs (CEJA), which issues formal Opinions on topics such as boundaries, fees, advertising, impaired physicians, end-of-life care, and industry relationships. The Code is not law, but its opinions are frequently cited in malpractice cases and licensing board proceedings. Key themes include the primacy of patient welfare, patient autonomy, honesty, confidentiality, continuous professional development, and responsibilities to the community.
Beauchamp & Childress: The Four Principles
Principlism rests on four principles of roughly equal weight; no principle automatically trumps the others. Each is a prima facie obligation — binding unless in conflict with another principle, in which case balancing is required.
| Principle | Core Obligation | Classic Application |
|---|---|---|
| Autonomy | Respect the self-determination of capable persons | Informed consent, refusal of treatment |
| Beneficence | Act to promote the patient’s well-being | Recommending effective therapy |
| Non-maleficence | Avoid causing harm | Declining futile or harmful interventions |
| Justice | Distribute benefits and burdens fairly | Allocation of ICU beds, organs, vaccines |
Derived Rules
From the four principles flow specific rules that guide daily practice: truth-telling, promise-keeping, confidentiality, privacy, and fidelity. These are not additional principles but specifications of how the four principles apply to recurring situations.
Specifying Principles to Concrete Rules
Abstract principles become action-guiding when they are specified to particular situations. For example, "respect autonomy" is specified as "obtain informed consent for surgical procedures using the reasonable-patient standard, including discussion of the option of no treatment." Specification is not a mechanical derivation; it requires judgment, case experience, and attention to context. The same principle may be specified differently in different cultures, institutions, and clinical settings without any loss of its core meaning.
Resolving Conflicts Between Principles
When principles conflict, resolution depends on which obligation is more stringent in context. Beauchamp and Childress propose that restriction of one principle is justified only when: (1) the alternative principle has a realistic prospect of being achieved, (2) no morally preferable alternatives are available, (3) the restriction is the least intrusive option, and (4) the agent acts to minimize the negative effects of infringement. This framework is called specified principlism.
Common Conflicts and Their Resolutions
| Conflict | Typical Resolution |
|---|---|
| Autonomy vs beneficence | Capable patient's informed choice generally controls |
| Autonomy vs non-maleficence | Physicians may decline to provide harmful interventions even if requested |
| Beneficence vs justice | Duty to this patient, tempered by duties to others and to stewardship |
| Autonomy vs justice | Individual liberty vs public health (e.g., vaccination mandates, quarantine) |
| Confidentiality vs third-party safety | Narrowly defined exceptions (Tarasoff, reportable conditions) |
| Parental authority vs child welfare | Best interest of the child, with court intervention for serious harm |

AMA Code (American physicians), ACP Ethics Manual (internists), Declaration of Geneva (WMA — modern Hippocratic Oath), ICN Code (nurses), APA Principles (psychologists), and the Physician Charter (ABIM Foundation, 2002) — the last articulates three fundamental principles: primacy of patient welfare, patient autonomy, and social justice.
05 Autonomy
Autonomy (from Greek autos "self" and nomos "rule") is the capacity of a person to govern themselves — to deliberate about personal goals and act on those deliberations. Respect for autonomy requires that clinicians acknowledge patients' right to hold views, make choices, and act based on their own values and beliefs. It is the principle most emphasized in American bioethics and is the foundation of informed consent, the right to refuse treatment, and confidentiality.
Historical Shift to Autonomy
Autonomy's central place in American bioethics reflects a specific historical and cultural trajectory. The post-war human rights movement, civil rights movement, women's movement, patient rights movement, and legal recognition of privacy rights all contributed. Internationally, autonomy is important but is often balanced more explicitly with family, community, and solidarity values. Neither extreme — atomistic individualism nor total subordination to community — is adequate; the task is thoughtful integration for each patient.
Three Conditions for Autonomous Action
| Condition | Requirement |
|---|---|
| Intentionality | The act is willed, not accidental |
| Understanding | The agent comprehends the nature and consequences of the action |
| Absence of controlling influences | Freedom from coercion, manipulation, or overwhelming pressure |
Positive and Negative Autonomy
Negative autonomy is the right to be left alone — to refuse unwanted intervention. It is nearly absolute in American law and ethics for capable adults: a competent Jehovah's Witness may refuse life-saving blood even if death will result. Positive autonomy is the right to demand specific interventions, and it is far more limited. Patients cannot demand non-indicated antibiotics, futile treatment, or medications that would harm them. Physicians retain professional autonomy to decline actions that conflict with medical standards.
Threats to Autonomy
Common threats include coercion (credible threats), manipulation (distortion of information), undue influence (exploiting dependency), and implicit paternalism (framing, nudging, or selective disclosure). Language barriers, cognitive impairment, severe pain, and power differentials all compromise the conditions for autonomous choice and must be addressed rather than ignored.
Relational Autonomy
Critics of classical autonomy argue that the "atomistic" self is a fiction — people make decisions embedded in families, cultures, and relationships. Relational autonomy recognizes that autonomous choice is socially constituted and that respecting autonomy sometimes means engaging family members rather than isolating the patient. This is especially important in cultures where decision-making is traditionally collective.
Autonomy and Shared Decision-Making
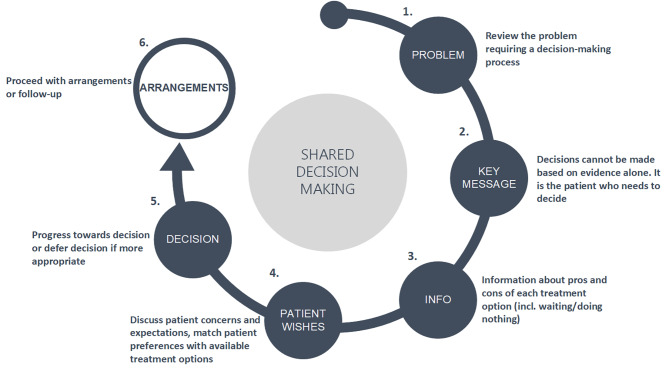
Respect for autonomy does not mean abandoning the patient to make decisions alone. Patients may feel overwhelmed by choices they do not have the background to evaluate, and pure "information dump" disclosure is a failure of clinical care. Shared decision-making combines the physician's expertise about options, probabilities, and typical outcomes with the patient's knowledge of their own goals, preferences, and circumstances. The process has three components: (1) acknowledge that a decision is needed, (2) describe the options clearly, and (3) explore the patient's values and integrate them into a joint recommendation.

06 Beneficence
Beneficence is the obligation to act for the benefit of others — to prevent harm, remove harm, and promote good. In medicine it is the physician's affirmative duty to help the patient, the oldest explicit obligation of the profession, dating to the Hippocratic tradition. Unlike autonomy, which is about respecting choices, beneficence is about actively pursuing the patient's welfare.
Beneficence as the Heart of Medicine
If autonomy is the principle most emphasized in contemporary bioethics, beneficence is the principle most central to medical identity. Patients come to physicians because they want help. They trust physicians to act in their interest. Beneficence, not autonomy, is the reason medicine exists.
Specific Beneficent Obligations
| Obligation | Clinical Expression |
|---|---|
| Protect others' rights | Advocate for patients within and outside the clinical encounter |
| Prevent harm | Vaccinate, screen, counsel on prevention, ensure follow-up |
| Remove harmful conditions | Treat disease, control pain, address social determinants |
| Help persons with disabilities | Accommodate, coordinate, advocate for equity |
| Rescue persons in danger | Respond to emergencies within one's capability |
General vs Specific Beneficence
General beneficence is the broad moral obligation to help others in distress; it is supererogatory beyond a point (one need not sacrifice everything). Specific beneficence arises from particular relationships — parent to child, physician to patient — and is more stringent. Once a physician–patient relationship is established, the physician is bound to promote that patient's welfare within the limits of competence and resources.
Paternalism
Paternalism is the overriding of a person's preferences or actions for that person's own good. It sits in tension with autonomy. Weak (soft) paternalism intervenes when autonomy is substantially compromised — preventing a delirious patient from leaving the hospital, for example. This is widely accepted. Strong (hard) paternalism overrides the voluntary, informed choices of capable persons; it is generally rejected in modern ethics but may be defensible in narrow circumstances (e.g., temporary hold to reverse reversible crisis).
Balancing Beneficence and Autonomy
The modern physician's challenge is to be beneficent without becoming paternalistic — to offer expert recommendation while ultimately honoring patient choice. This is operationalized as shared decision-making: the clinician contributes evidence, experience, and judgment, while the patient contributes values, preferences, and goals, and together they arrive at a decision each can endorse.
Beneficence and Professional Competence
Beneficence is inseparable from clinical competence. A well-intentioned but incompetent physician violates beneficence just as surely as an indifferent one. The duty to act for the patient's welfare therefore entails ongoing duties of lifelong learning, self-assessment, peer review, and practice within one's actual skill set. Referring a patient whose needs exceed one's competence is a beneficent act; attempting heroic management is not.
Limits of Beneficence
Beneficence has limits at several boundaries: at the patient's own refusal (autonomy overrides), at the threshold of futility (beneficence cannot require the impossible), at the physician's own well-being (extreme self-sacrifice is not required), and at the claims of third parties (other patients, family, society). Recognizing these limits protects physicians from burnout and moral injury and keeps the duty of beneficence from becoming an open-ended demand.


07 Non-Maleficence
Non-maleficence, the obligation to avoid causing harm, is captured in the phrase primum non nocere ("first, do no harm") — a paraphrase not actually in the Hippocratic Oath but deeply embedded in medical culture. Non-maleficence is often treated together with beneficence, but they are distinct: beneficence is active promotion of good; non-maleficence is active avoidance of harm.
Non-Maleficence in the Modern Era
Non-maleficence has taken on new meaning as medical capability has grown. The Hippocratic era had few interventions capable of serious harm; the modern era offers many, and the question is rarely whether an intervention may harm but how much harm is acceptable for how much expected benefit. This shifts the clinician's task from avoiding harm absolutely to understanding risks deeply and communicating them honestly.
Types of Harm
| Harm Type | Example |
|---|---|
| Physical | Surgical complication, drug toxicity, hospital-acquired infection |
| Psychological | Traumatic disclosure, coercive procedures, depersonalizing care |
| Social | Stigmatizing diagnoses, discriminatory documentation |
| Financial | Unnecessary testing, surprise billing, cost-induced non-adherence |
| Opportunity cost | Time, resources, or attention diverted from other patients |
The Standard of Due Care
Non-maleficence does not prohibit all harm — virtually every intervention carries some risk. It prohibits unnecessary or disproportionate harm. The operational standard is due care: the degree of attention and skill that a reasonably prudent practitioner would exercise in similar circumstances. Breach of due care is negligence, the core of malpractice law.
Rule of Double Effect
The rule of double effect justifies actions with both good and bad effects under four conditions:
- Nature of the act: the action itself is not intrinsically wrong.
- Intention: the agent intends the good effect; the bad effect is foreseen but not intended.
- Distinction of means: the bad effect is not the means to the good effect.
- Proportionality: there is a proportionately grave reason to permit the bad effect.
The classic application is escalating opioids for pain in terminal illness: respiratory depression may be foreseen, but the intent is analgesia and the doses are titrated to comfort, not death.
Withholding vs Withdrawing
Non-maleficence does not distinguish morally between withholding a treatment (not starting it) and withdrawing one (stopping it). Clinicians often feel withdrawing is worse, but most ethicists and courts treat them as ethically equivalent. This matters clinically because it removes the disincentive to start time-limited trials of therapy.
Iatrogenic Harm and Systems Thinking
Much of non-maleficence in modern medicine is a matter of systems, not individual judgment. Hospital-acquired infections, medication errors, wrong-site surgeries, diagnostic errors, and hand-off failures cause substantial harm and are best addressed through checklists, protocols, culture change, and continuous quality improvement rather than blaming individuals. A just culture framework distinguishes human error, at-risk behavior, and reckless behavior and responds proportionately to each while preserving willingness to report.
Over-Diagnosis and Over-Treatment
Recent decades have revealed a category of harm that is easy to overlook: over-diagnosis (detecting "disease" that would never have caused symptoms) and over-treatment (intervening on findings that would not benefit the patient). Screening-detected indolent cancers, incidental imaging findings, and expanding disease definitions contribute. Non-maleficence demands a critical eye on the assumption that "more is better" and attention to the harms of testing, labeling, and treating uncertain findings.

08 Justice & Balancing Principles
Justice in medical ethics concerns the fair distribution of benefits, risks, and resources. It addresses questions of who gets what care, on what basis, and at whose expense. Unlike the other principles, justice operates at individual, institutional, and societal levels simultaneously.
Justice at Multiple Levels
Justice operates at the bedside (how should I allocate my time among patients this afternoon?), at the institutional level (how should this hospital decide who gets the last ICU bed?), and at the societal level (how should the healthcare system be organized and financed?). Clinicians function primarily at the bedside but contribute to institutional and societal justice through professional organizations, advocacy, education, and voting. Ignoring system-level injustice while attending only to individual patients is itself a kind of ethical failure.
Theories of Distributive Justice
| Theory | Core Principle |
|---|---|
| Egalitarian | Equal access to a decent minimum for all persons |
| Libertarian | Free market; rights to property and voluntary exchange primary |
| Utilitarian | Maximize aggregate health benefit (QALYs, lives saved) |
| Communitarian | Distribution reflects community traditions and solidarity |
| Capabilities (Sen, Nussbaum) | Ensure people can achieve basic functionings |
Formal and Material Principles
Aristotle's formal principle of justice is that equals must be treated equally, and unequals unequally in proportion to their relevant differences. This tells us to be consistent but not what counts as a relevant difference. Material principles specify the relevant criteria: to each according to need, effort, merit, contribution, ability to pay, or social utility. Different domains invoke different criteria — emergency care is distributed by need, cosmetic surgery largely by ability to pay.
Procedural Justice
When substantive agreement is impossible, fair procedures may legitimize outcomes. Accountability-for-reasonableness (Daniels & Sabin) requires that allocation decisions be: (1) public, (2) based on reasons stakeholders can accept, (3) subject to revision in light of new arguments or evidence, and (4) enforced by a regulatory mechanism.
Balancing the Principles
In real cases the principles routinely conflict. Common clashes include autonomy vs beneficence (patient refuses beneficial treatment), autonomy vs non-maleficence (patient demands harmful intervention), beneficence vs justice (maximizing one patient's outcome consumes resources others need), and non-maleficence vs autonomy (restraint of suicidal patient). A structured approach to balancing is essential:
Box 1 — Medical Indications (beneficence, non-maleficence): diagnosis, prognosis, goals, success probability.
Box 2 — Patient Preferences (autonomy): capacity, informed consent, prior wishes.
Box 3 — Quality of Life (beneficence, non-maleficence, autonomy): expected QoL, biases, palliation.
Box 4 — Contextual Features (justice, fairness): family, economics, law, research interests, resources.
Justice and Health Disparities
Justice is not only about individual allocation decisions but also about systemic patterns. Racial, ethnic, socioeconomic, gender, and geographic disparities in access to care, quality of care, and outcomes are well documented. Implicit bias, structural racism, and fragmented insurance systems all contribute. Clinicians' obligations of justice include awareness of disparities, attention to one's own potential biases, advocacy for patients facing access barriers, and participation in institutional and policy efforts to reduce inequities.
Rescue vs Prevention
Societies predictably overinvest in the "rule of rescue" — dramatic interventions to save identifiable lives — while underinvesting in prevention that would save more statistical lives at lower cost. Utilitarian justice argues for a rebalancing toward prevention; other frameworks give weight to the special obligation to help identifiable persons in acute distress. This tension is never fully resolved and shapes debates about public health, insurance coverage, and budget priorities.

09 Elements & Standards of Disclosure
Informed consent is the process by which a patient, having been adequately informed, voluntarily authorizes a medical intervention. It is the operational expression of respect for autonomy and is both an ethical and legal requirement. Consent is not a form — it is a process, and the signed document is only its record.
Foundations in Case Law
Modern informed consent doctrine traces to Schloendorff (1914), where Justice Cardozo wrote that "every human being of adult years and sound mind has a right to determine what shall be done with his own body." Salgo v. Leland Stanford (1957) coined the phrase "informed consent." Canterbury v. Spence (1972) established the reasonable-patient (materiality) standard that governs most US jurisdictions today. These cases shifted the legal center of gravity from physician-centered disclosure to patient-centered disclosure.
Five Elements of Informed Consent
| Element | Description |
|---|---|
| 1. Disclosure | Physician provides relevant information: diagnosis, nature of intervention, risks, benefits, alternatives (including no treatment) |
| 2. Comprehension | Patient understands the information; clinician confirms via teach-back |
| 3. Voluntariness | Decision is free of coercion, manipulation, or undue influence |
| 4. Capacity | Patient has the cognitive ability to decide (see Section 11) |
| 5. Authorization | Patient affirmatively consents to (or refuses) the specific intervention |
What Must Be Disclosed
Adequate disclosure includes: the patient's diagnosis and prognosis, the nature and purpose of the proposed intervention, material risks and anticipated benefits, reasonable alternatives (including no treatment), and the risks and benefits of each alternative. Disclosure should be in language the patient understands, with attention to health literacy and cultural context. An interpreter is required for limited-English-proficient patients — family members should not substitute except in emergencies.
Standards of Disclosure
| Standard | What Must Be Disclosed | Jurisdictions |
|---|---|---|
| Professional (reasonable physician) | What a reasonable physician would disclose in similar circumstances | Minority of US states |
| Reasonable person (materiality) | What a reasonable patient would want to know to make a decision | Majority; established in Canterbury v. Spence (1972) |
| Subjective | What this particular patient would want to know | Rare; ideal when known |
Documentation
A consent form documents that the process occurred but does not prove it was adequate. Notes should describe what was discussed, alternatives considered, questions asked, the patient's decision, and any indications of comprehension. For high-risk interventions, specific disclosure of the material risks should be noted.
Common Misconceptions About Consent
| Misconception | Reality |
|---|---|
| "The form is the consent" | Consent is the conversation; the form is the record |
| "If the patient signs, we’re protected" | Signature without understanding is invalid consent |
| "General consent covers everything" | Specific high-risk procedures need specific discussion |
| "The surgeon can delegate consent to a nurse" | The physician performing the procedure must participate in the disclosure |
| "Consent once is consent forever" | Ongoing care requires ongoing agreement; patients may withdraw consent |


10 Exceptions, Refusal & Special Populations
Recognized Exceptions to Informed Consent
| Exception | Explanation |
|---|---|
| Emergency | Immediate intervention to prevent death or serious harm; consent presumed when patient incapacitated and no surrogate available |
| Incapacity | Patient lacks capacity; surrogate consent obtained |
| Waiver | Capable patient voluntarily declines to receive information ("Doctor, just do what you think is best") |
| Therapeutic privilege | Disclosure itself would cause serious psychological harm; historically invoked, now very narrowly accepted |
| Legally authorized treatment | Court-ordered treatment, public health quarantine, certain psychiatric holds |
Therapeutic privilege is the most contentious and should never be used simply because disclosure is uncomfortable or might prompt refusal. The bar is that disclosure would be medically contraindicated, a standard rarely met.
Informed Refusal
The capable patient has the same right to refuse as to consent. Informed refusal requires the same disclosure process — the patient must understand the likely consequences of refusal, including death if that is the expected outcome. Document capacity, disclosure, and the patient's understanding. Explore reasons (fear, cost, prior experience, religious belief) and address correctable factors. Acceptance of refusal is not abandonment; offer follow-up and alternatives.
Consent for Minors
In general, parents or legal guardians provide consent for minors under 18. Important exceptions empower minors to consent independently:
| Category | Scope |
|---|---|
| Emancipated minors | Married, military, legally declared; consent for all care |
| Mature minor doctrine | Judicially recognized capacity in certain states for specific decisions |
| STI testing and treatment | All 50 states allow minor consent |
| Contraception | Most states allow minor consent |
| Pregnancy care | Varies by state; many allow minor consent for prenatal care |
| Substance use treatment | Most states allow minor consent |
| Mental health (outpatient) | Many states permit minor consent above a set age |
| Emergency care | Always permitted; consent presumed |
Assent
Even when parental consent is required, children old enough to understand should be asked for assent — affirmative agreement — and their objections should be taken seriously. Assent is routinely sought from children 7 and older for research and for significant clinical decisions.
Consent for Research
Research consent requires additional disclosures beyond clinical consent: that this is research, the research purpose, the expected duration, procedures, reasonably foreseeable risks, potential benefits, alternatives, confidentiality protections, compensation for injury, contact information, and the right to withdraw without penalty. Vulnerable populations (children, prisoners, pregnant women, cognitively impaired) require additional safeguards.

11 Capacity vs Competence
Capacity and competence are often used interchangeably in conversation but have distinct technical meanings. Competence is a legal determination made by a court; an adult is presumed competent unless adjudicated otherwise. Capacity is a clinical determination made by a physician that a particular patient can make a particular decision at a particular time. A competent adult may temporarily lack capacity (delirium, intoxication), and a patient with limited competence for some matters may retain capacity for specific medical decisions.
Why the Distinction Matters
The capacity/competence distinction matters because many patients who would technically fail a formal legal competence standard nonetheless retain the practical ability to make specific medical decisions. A patient with mild dementia may not be able to manage complex finances (legal incompetence) but may fully understand that she does not want another round of chemotherapy. A patient under temporary sedation may lack capacity now but will regain it tomorrow. The clinical focus on decision-specific capacity preserves as much autonomy as possible while protecting patients from decisions they cannot truly make.
Key Features of Clinical Capacity
| Feature | Explanation |
|---|---|
| Decision-specific | Capacity is assessed for a particular decision, not globally |
| Scales with stakes | Higher-risk decisions warrant more rigorous assessment |
| Can fluctuate | Patients may regain capacity; repeat assessment when possible |
| Presumed present | Adults are presumed to have capacity unless there is reason to doubt |
| Disagreement is not incapacity | Refusing recommended treatment is not itself evidence of lacking capacity |
The Four Abilities (Appelbaum & Grisso)
| Ability | What to Assess | Sample Question |
|---|---|---|
| Understanding | Grasping the relevant information | "Can you tell me in your own words what I just explained?" |
| Appreciation | Applying the information to oneself | "What do you think is going on with your health?" |
| Reasoning | Manipulating information logically to compare options | "How did you decide between these options?" |
| Expressing a choice | Communicating a stable decision | "What would you like to do?" |
Sliding Scale
The threshold for capacity rises with the stakes of the decision. A patient may have sufficient capacity to accept a low-risk, high-benefit treatment (routine antibiotics) but insufficient capacity to refuse a life-saving intervention. This sliding scale is widely accepted because a decision with severe consequences demands a higher level of understanding and appreciation to be authentic.
Conditions That Impair Capacity
Capacity may be impaired by dementia, delirium, intoxication, severe depression, acute psychosis, intellectual disability, traumatic brain injury, severe pain, hypoxia, metabolic derangement, and medication effects. Importantly, psychiatric diagnosis does not equal incapacity — many patients with schizophrenia or bipolar disorder retain decisional capacity. Capacity must be assessed functionally, not inferred from diagnosis.

12 Capacity Assessment in Practice
When to Assess Capacity
Formal capacity assessment is warranted when: (1) the patient's decision is inconsistent with previously stated values, (2) an abrupt change in decision-making pattern occurs, (3) cognitive impairment is suspected, (4) the decision carries very high stakes, (5) the patient has known psychiatric illness relevant to the decision, or (6) the patient appears not to understand despite adequate explanation.
Conducting the Assessment
Capacity assessment is a conversation, not a checklist. Begin by ensuring the patient is in the best possible state (pain controlled, not acutely intoxicated, in a quiet environment, with hearing aids or glasses if needed). Review the information relevant to the decision in plain language. Then probe each of the four abilities with open-ended questions, asking the patient to paraphrase, describe implications for their own life, articulate reasoning, and state a choice. Bedside screening tools (MacArthur Competence Assessment Tool, Aid to Capacity Evaluation) can structure the evaluation but do not replace clinical judgment.
Role of Psychiatry
Any physician can assess capacity, and the treating team is often best positioned because they know the context. Psychiatric consultation is appropriate when the case is complex, when there is disagreement, when psychiatric illness complicates assessment, or when documentation of a thorough evaluation is needed for legal reasons.
When Capacity Is Lacking
If a patient lacks capacity, decisions fall to a surrogate (Section 13), guided by advance directives if available. The patient should still be involved to the extent possible, and assent sought. Capacity should be reassessed when medical, metabolic, or pharmacologic contributors are corrected.
Documentation
1. Reason for assessment and the specific decision at stake.
2. Information provided to the patient and manner of presentation.
3. Patient's performance on each of the four abilities with quotes.
4. Relevant medical, psychiatric, and contextual factors.
5. Conclusion about capacity for this decision at this time.
6. Plan: honor decision, obtain surrogate, reassess, or escalate.
Reassessment and Reversibility
Capacity is not a permanent label. Delirium resolves, sedation wears off, pain is controlled, oxygen is restored, psychiatric symptoms improve, and the same patient who lacked capacity yesterday may have it today. Clinicians should actively work to restore capacity whenever possible: treat pain, reduce sedating medications, correct metabolic abnormalities, minimize disruptive nighttime awakenings, and provide quiet, oriented environments for high-stakes discussions. Reassessing capacity after such interventions is both an ethical obligation and a routine clinical practice.
13 Surrogate Hierarchy & Standards
When a patient lacks capacity and the decision cannot wait, decisions are made by a surrogate. Surrogates should respect the patient's previously expressed wishes, values, and interests — they are not authorized to impose their own preferences.
Typical Surrogate Hierarchy (varies by state)
| Rank | Surrogate |
|---|---|
| 1 | Court-appointed guardian with healthcare authority |
| 2 | Durable power of attorney for health care (healthcare proxy) |
| 3 | Spouse (or domestic partner where recognized) |
| 4 | Adult children (majority where multiple) |
| 5 | Parents |
| 6 | Adult siblings |
| 7 | Other adult relatives |
| 8 | Close friend with knowledge of patient's values |
| 9 | Physician with ethics committee consultation (unbefriended patient) |
Why Surrogacy Exists
Surrogate decision-making is justified by the combined weight of two principles: respect for the patient's autonomy (continued even into incapacity through the surrogate's voice) and beneficence (someone must make decisions when the patient cannot). Surrogates are stewards of the patient's interests, not independent decision-makers. The clinician's role is to support the surrogate in this demanding task — providing information, emotional support, and reassurance that they are doing right by the patient.
Three Standards of Surrogate Decision-Making
| Standard | When Used | Basis |
|---|---|---|
| Expressed wishes | Patient previously stated preference about this situation | Honor the patient’s specific instruction |
| Substituted judgment | Patient's values known but not this exact situation | "What would this patient decide if they could?" |
| Best interest | Patient's values unknown (never had capacity, or no prior conversation) | Balance benefits and burdens objectively |
The standards are applied in descending order of priority: always use expressed wishes if known; fall back to substituted judgment; use best interest as the default only when values are unknown. Surrogates often drift toward their own preferences; clinicians should explicitly frame the question as, "What would she want?" rather than, "What would you want for her?"
The Unbefriended Patient
Patients without surrogates or advance directives present a particular challenge. Options include court-appointed guardianship (time-consuming), institutional ethics committee review, or decisions made by the treating team using the best interest standard with additional safeguards. Many jurisdictions now have statutory mechanisms for these decisions.
Common Surrogate Decision-Making Errors
| Error | Corrective |
|---|---|
| Projecting own preferences | Ask "what would she want?" not "what would you want?" |
| Ignoring prior wishes because of grief | Validate the emotion; return to substituted judgment |
| Letting a non-designated family member dominate | Clarify legal authority; convene a family meeting |
| Asking surrogates to "make the decision to let her go" | Frame as honoring the patient's wishes, not choosing death |
| Over-interpreting vague statements | Acknowledge uncertainty; triangulate with multiple sources |
14 Advance Directives & POLST
Advance directives are legal documents in which capable individuals specify preferences or designate surrogates for future decisions. They exist to extend autonomy into periods of incapacity.
Patient Self-Determination Act (1990)
The federal Patient Self-Determination Act requires Medicare- and Medicaid-participating healthcare facilities to inform patients of their rights under state law to execute advance directives, document whether patients have advance directives, educate staff and community about advance directives, and refrain from discriminating against patients based on the presence or absence of a directive. The PSDA does not itself create the right to an advance directive — it operationalizes rights already provided by state law.
Types of Advance Directives
| Type | Function |
|---|---|
| Living will | Written instructions about specific interventions (e.g., ventilation, tube feeding) the patient would accept or refuse in specified conditions |
| Durable power of attorney for health care | Designates a proxy to make decisions when the patient lacks capacity; generally broader and more flexible than a living will |
| Combined advance directive | Unified document with both instructional and proxy elements |
| Values history | Narrative describing goals and values, not legally binding but invaluable for substituted judgment |
POLST / MOLST
Physician/Medical Orders for Life-Sustaining Treatment (POLST/MOLST) are actionable medical orders, typically on a brightly colored form, signed by a physician for seriously ill patients. Unlike a living will, POLST is not an advance directive — it is a current medical order that travels with the patient across care settings (home, nursing facility, EMS, hospital). POLST is intended for patients with advanced illness or frailty with a prognosis of a year or less.
DNR/DNI Orders
Do-not-resuscitate (DNR) and do-not-intubate (DNI) orders specify withholding CPR and intubation in the event of cardiac or respiratory arrest. They do not limit other treatment and should not be conflated with "comfort care only." A DNR patient can still receive ICU care, antibiotics, surgery, and aggressive treatment of underlying disease — unless a broader decision has been made.
Limits of Advance Directives
Advance directives have known weaknesses: they may be vague, out of date, unavailable at the moment of need, or silent about the actual clinical question. Surrogates often disagree with documented preferences, and patients' future preferences may differ from their past statements (the "disability paradox"). These limitations do not defeat the directive but argue for pairing it with a designated proxy who can interpret it in context.



15 Family Conflict & Resolution
Family conflict at the bedside is common and distressing. Conflicts may arise between the patient and family, between family members, between family and the care team, or within the care team itself. Most are rooted in grief, fear, guilt, inadequate information, or unresolved family dynamics rather than genuine ethical disagreement.
Approach to Family Conflict
- Gather the facts: Confirm the medical situation, prognosis, treatment options, and realistic goals.
- Clarify roles: Identify the legally authorized surrogate; explain that other family members are welcome voices but not decision-makers.
- Convene a family meeting: Include key family, nursing, chaplaincy, social work, and relevant specialists.
- Listen first: Elicit each participant's understanding, concerns, and hopes.
- Re-center the patient: Ask, "What would he want?" not, "What do you want?"
- Make a recommendation: The team should offer a clear plan based on values and goals.
- Allow time: Many conflicts resolve with additional information, reflection, and rapport.
- Escalate when stuck: Ethics consultation, palliative care, chaplaincy, second medical opinion.
When the Conflict Cannot Be Resolved
If the surrogate's decision clearly contradicts the patient's known wishes or appears to harm rather than benefit the patient, the clinician's duty runs to the patient, not the surrogate. Options include ethics consultation, institutional review, transfer of care, and in extreme cases court involvement to seek a guardian. These steps should be pursued only after good-faith attempts at communication and mediation.
S — Setting and participants. P — Perception: "What have you been told?" I — Invitation: "How much would you like to know?" K — Knowledge: clear, honest information. E — Emotion: respond to feelings before facts. S — Strategy and summary: plan and next steps.
16 Withholding vs Withdrawing & Futility
End-of-life ethics is the domain where principles are most often in tension and where clear reasoning matters most. The patient is vulnerable, the stakes are final, and clinicians often feel emotional burden that clouds judgment.
Psychological and Moral Weight
End-of-life cases are the most common reason for ethics consultation and the source of disproportionate moral distress for clinicians. The stakes are final, emotions run high, and disagreements among clinicians, families, and patients tend to be more visible. Careful preparation, consistent communication, and attention to clinicians' own emotional response are part of good end-of-life care, not extras.
Withholding and Withdrawing: Ethical Equivalence
A strong ethical and legal consensus holds that withholding and withdrawing life-sustaining treatment are morally equivalent. Neither constitutes killing; both respect the patient's right to refuse unwanted intervention. This equivalence is crucial because it permits time-limited trials: starting a treatment to see if it helps, with a prior understanding that it will be stopped if it does not achieve agreed-upon goals. Clinicians who feel withdrawal is worse than withholding often under-treat because they hesitate to commit to therapies they might later need to stop.
What Can Be Refused or Withdrawn
Any intervention, including mechanical ventilation, dialysis, CPR, artificial nutrition and hydration, antibiotics, blood products, and vasopressors, may be refused by a capable patient or withdrawn by a surrogate consistent with the patient's wishes. Artificial nutrition and hydration via feeding tube are medical interventions, not basic care, and may be refused on the same terms as other treatments — a principle affirmed by the Cruzan decision.
Medical Futility
| Type | Definition |
|---|---|
| Physiologic futility | Intervention cannot achieve its intended physiologic effect (e.g., CPR in decapitation) |
| Quantitative futility | Intervention has vanishingly low probability of success based on evidence |
| Qualitative futility | Intervention can achieve an effect but cannot achieve a benefit meaningful to the patient |
Physiologic futility is uncontroversial — clinicians are not obligated to provide interventions that cannot work. Qualitative futility is contested because "meaningful benefit" is a value judgment on which clinicians and families may reasonably disagree. The contemporary approach avoids unilateral futility declarations in favor of potentially inappropriate treatment language, fair procedural review, and institutional dispute-resolution processes (TADA Texas Advance Directives Act is a well-known example).
Dispute Resolution for Disagreement About Limits
(1) Engage in intensive communication. (2) Obtain second medical opinion. (3) Consult ethics committee. (4) Offer transfer to another provider or institution. (5) Inform surrogate of appeal rights. (6) If all steps fail, withdrawing or withholding may proceed with institutional support.
Time-Limited Trials
When prognosis is uncertain and families are unready to forgo aggressive measures, a time-limited trial can resolve impasses. The team and family agree in advance on: (1) the specific interventions to be tried, (2) the clinical markers of success and failure, (3) the duration of the trial, and (4) the plan if the trial fails (typically transition to comfort-focused care). Time-limited trials respect hope, provide objective evidence, and often help families accept difficult transitions they could not accept prospectively.


17 Brain Death & Organ Donation
History of Brain Death
The concept of brain death emerged in the 1960s with the advent of mechanical ventilation, which allowed cardiopulmonary function to continue in patients whose brains had irreversibly ceased to function. The 1968 Harvard criteria were the first widely adopted standard; the 1981 President's Commission report and the UDDA formalized the neurologic criterion legally. Brain death is accepted in medicine and law throughout the US, though clinical protocols vary modestly by institution and state.
Determination of Death
The Uniform Determination of Death Act (UDDA, 1981) establishes two criteria for legal death: (1) cardiorespiratory — irreversible cessation of circulatory and respiratory functions, or (2) neurologic — irreversible cessation of all functions of the entire brain, including the brainstem. Both are "death," not "kinds" of death.
Brain Death Criteria
| Requirement | Detail |
|---|---|
| Known etiology | Irreversible cause established (not reversible by treatment) |
| Exclude confounders | Sedation, hypothermia (<36°C), severe metabolic or endocrine disturbance, neuromuscular blockade |
| Coma | Unresponsive to noxious stimuli in all extremities |
| Absent brainstem reflexes | Pupillary, corneal, oculocephalic, oculovestibular, gag, cough |
| Apnea test | No respiratory effort at PaCO2 ≥ 60 mmHg (or 20 mmHg rise) |
| Ancillary testing | EEG, cerebral blood flow, or TCD when clinical exam cannot be completed |
Ethical Issues Around Brain Death
Some families reject brain death as death on religious, cultural, or philosophical grounds. Most jurisdictions require clinicians to perform the declaration but allow reasonable accommodation (brief continuation of somatic support) while families process the news. A small number of states (NJ, and with accommodation, NY and CA) have formal religious exemption statutes. Communication, time, and chaplaincy support are the most effective responses.
Organ Donation
| Pathway | Description |
|---|---|
| DBD — Donation after Brain Death | Donor meets neurologic criteria for death; organs procured while circulation maintained |
| DCD — Donation after Circulatory Death | Withdrawal of life support followed by death declaration; organs procured after mandated "no-touch" interval |
| Living donation | Kidney, partial liver; requires rigorous independent advocacy and consent |
The Dead Donor Rule and Separation of Roles
The dead donor rule prohibits removal of vital organs from a living person and requires that the donor be dead before procurement (or, in living donation, that the donation not cause death). To preserve trust, the clinicians declaring death must be independent of the transplant team, and discussion of organ donation is typically initiated by the organ procurement organization (OPO), not the primary team.
Consent for Organ Donation
Authorization for donation can come from the decedent's documented first-person consent (donor registry, driver's license designation, advance directive) or from the legally authorized next of kin. First-person consent is controlling — families cannot override a documented decision to donate, though OPOs typically seek family concurrence. Disclosure should include what will happen, the process of procurement, and what the family can expect afterward.
Novel Issues in Donation
| Issue | Ethical Consideration |
|---|---|
| Normothermic regional perfusion in DCD | Debate about preserving the dead donor rule |
| HIV-to-HIV donation | HOPE Act expanded access for HIV-positive recipients |
| Opioid-era donor pool expansion | Balance utility against infectious and health risks |
| Directed donation | Permitted to family/friends; restrictions on discriminatory directions |
| Paired exchange | Ethical; increases access without commodification |
| Payment for organs | Prohibited by NOTA; concerns about exploitation |








18 Palliative Sedation & Double Effect
Principled Distinctions
End-of-life ethics relies on a set of principled distinctions that are contested but widely accepted in US ethics: killing vs allowing to die, intending vs foreseeing, ordinary vs extraordinary means, and active vs passive intervention. These distinctions do work in legal and clinical reasoning, but careful ethicists recognize that many cases fall at the boundaries and that the distinctions do not always track what matters morally. They are tools, not rigid rules.
Symptom Management at the End of Life
Aggressive symptom management for dying patients is a core ethical obligation of physicians and does not require that every intervention carry zero risk. Under the rule of double effect, opioids may be titrated to control dyspnea or pain in terminal illness even if respiratory depression is a foreseen possible consequence, provided the intent is symptom relief, doses are proportionate, and the patient has accepted (or surrogates accept) the plan.
Palliative Sedation
Palliative sedation is the monitored use of sedatives to reduce consciousness in order to relieve intractable suffering at the end of life when other measures have failed. It is a last-resort option for refractory physical symptoms (dyspnea, pain, agitated delirium, seizures). Ethical requirements include: (1) the patient is imminently dying, (2) symptoms are refractory despite expert palliative care, (3) the intent is symptom relief, not death, (4) sedation is titrated to the minimum necessary, and (5) informed consent or surrogate agreement is obtained.
| Palliative Sedation | Euthanasia |
|---|---|
| Intent: relieve refractory suffering | Intent: cause death |
| Proportionate sedative dose | Lethal dose |
| Death occurs from underlying disease | Death caused by the drug |
| Widely accepted | Legal in few jurisdictions; distinct ethical debate |
Voluntary Stopping of Eating and Drinking (VSED)
A capable patient who is not imminently dying may choose to stop eating and drinking as a means of hastening death. VSED is legal and, with palliative support for thirst and dry mouth, is generally tolerable. It respects autonomy and does not require physician action beyond supportive care, which most ethicists consider ethically permissible.
Physician-Assisted Dying
Medical aid in dying (MAID), sometimes called physician-assisted suicide, is the practice of a physician prescribing a lethal dose of medication that the patient self-administers. It is legal in a growing number of US jurisdictions with strict eligibility criteria (typically: terminal illness with prognosis ≤6 months, capable adult, voluntary repeated requests, residency). MAID differs from euthanasia, in which a physician administers the lethal agent directly. MAID remains ethically controversial: professional societies are divided, and conscientious objection is broadly protected.


19 Aid-in-Dying, CPR/DNR & Goals of Care
The Shift from "Code Status" to "Goals of Care"
Historically, code status was often the first and only end-of-life conversation, posed in procedural terms ("do you want chest compressions?"). The contemporary standard is to embed code status within a broader goals-of-care discussion: understanding of illness, values, hopes and worries, and the trade-offs among possible paths. Code status then follows naturally from the goals rather than being imposed as an abstract choice.
CPR and Code Status Discussions
Cardiopulmonary resuscitation is unusual among medical interventions in that it is the default — it will be performed unless a decision is made in advance to withhold it. CPR outcomes vary widely: in-hospital arrests in otherwise reasonably healthy adults have survival to discharge around 20–25%, while survival in metastatic cancer, advanced dementia, or multi-organ failure is typically <5% and often <1%. Many patients overestimate CPR success because of media portrayal; part of informed discussion is sharing realistic prognosis.
Framing Goals-of-Care Conversations
R — Reframe: "Given what has happened, we need to think about what to do next."
E — Expect emotion: respond before moving on.
M — Map out patient values: "What is most important to you?"
A — Align with values: summarize and confirm.
P — Propose a plan: make a specific recommendation based on values.
Making a Recommendation
Patients and families often find it hard to choose among options they do not fully understand. Offering a clinical recommendation based on articulated goals is beneficent and preserves autonomy — the patient retains veto power. "List and ask" approaches ("Do you want CPR? Do you want a ventilator? Do you want a feeding tube?") often feel cruel and lead to worse decisions than values-based recommendation.
Hospice and Palliative Care
| Service | Eligibility | Focus |
|---|---|---|
| Palliative care | Any stage of serious illness, any age | Symptom management and goals alongside disease-directed therapy |
| Hospice | Prognosis ≤6 months if disease follows usual course; willingness to forgo curative treatment | Comfort-focused care, usually at home |
Hospice does not mean "giving up" — it is active care focused on quality of life, symptom control, and dignity. Hospice enrollment is associated with improved symptom control, lower caregiver distress, and in some studies longer survival than continued aggressive care.
Common Pitfalls in Goals-of-Care Conversations
| Pitfall | Better Approach |
|---|---|
| Asking "do you want us to do everything?" | Ask about goals first; recommend interventions aligned with those goals |
| Presenting a menu without recommendation | Make a clear recommendation based on values and prognosis |
| Delaying until crisis | Introduce early; normalize serial conversations over time |
| Using euphemisms ("not doing well") | Be specific and honest: "her cancer is progressing despite treatment" |
| Talking more than listening | Aim for the patient and family to do most of the talking |
| Skipping the emotion | Name the feeling; use silence and presence |



20 Confidentiality, HIPAA & Exceptions
Confidentiality — the duty not to disclose information shared within a professional relationship — is as old as the Hippocratic Oath. It serves both individual autonomy and the public good: if patients cannot trust confidentiality, they will not disclose information needed for diagnosis and treatment. Confidentiality is a prima facie duty: strong, but not absolute.
Roots of Confidentiality
Confidentiality protects three distinct interests: the patient's privacy (control over personal information), the trust essential to diagnosis and treatment (patients must feel safe disclosing sensitive information), and the relational integrity of the physician–patient encounter. Breach harms not only the individual patient but erodes institutional trust that takes years to rebuild.
HIPAA
The Health Insurance Portability and Accountability Act (1996) Privacy Rule (2003) establishes federal standards for protecting individually identifiable health information ("protected health information," PHI). Covered entities (providers, plans, clearinghouses) may use and disclose PHI for treatment, payment, and healthcare operations (TPO) without specific authorization; other disclosures typically require patient authorization. Patients have rights to access, amend, and obtain an accounting of disclosures. HIPAA violations carry civil and criminal penalties.
Exceptions to Confidentiality
| Exception | Basis |
|---|---|
| Patient authorization | Written consent to specific disclosure |
| Treatment, payment, operations | HIPAA permitted uses within the healthcare system |
| Mandatory reporting of communicable diseases | Public health law (e.g., TB, STIs, HIV in some states) |
| Mandatory reporting of child abuse | All 50 states require reporting reasonable suspicion |
| Mandatory reporting of elder and dependent adult abuse | Most jurisdictions |
| Reporting of gunshot, stab wounds | State-specific requirements |
| Driving impairment | Some states require DMV notification (e.g., seizures) |
| Duty to warn / protect | Tarasoff v. Regents (1976): serious threat to identifiable third party |
| Court order / subpoena | Legal compulsion (physician-patient privilege may apply) |
| Emergency to prevent serious harm | Disclose minimum necessary to relevant parties |
The Tarasoff Duty
In Tarasoff v. Regents of the University of California (1976), the California Supreme Court held that mental health professionals have a duty to protect identifiable third parties from foreseeable violence by a patient. The duty may be discharged by warning the intended victim, notifying law enforcement, hospitalizing the patient, or other reasonable steps. States vary in whether the duty is to warn, to protect, or neither.
Confidentiality with Minors and Adolescents
Adolescents often have statutory rights to confidential care for sensitive services (contraception, STIs, mental health, substance use). Clinicians should explain confidentiality and its limits at the start of the visit, offer time alone, and document carefully. Confidentiality is not absolute — safety (suicidality, abuse) may require disclosure.
Spouses, Family, and Incidental Disclosure
Information should not be shared with family members without the patient's permission, even in well-meaning contexts. A common error is disclosing diagnoses or test results to a spouse who calls asking. If the patient has granted permission or is incapacitated, disclosure may be appropriate; otherwise, ask the caller to have the patient contact you.
Practical Safeguards
Confidentiality lapses most often occur through casual violations rather than deliberate disclosures: elevator conversations, hallway handoffs, unsecured workstations, misdirected faxes, social media posts, and chart browsing of acquaintances ("VIP" and celebrity patients, neighbors, ex-partners). Institutional safeguards include audit logs, break-the-glass protocols, role-based access, and periodic training. The individual clinician's obligation is to be discreet in public spaces, log out of workstations, verify recipient identity before disclosure, and access only records needed for care.


21 Professionalism & Boundaries
Professionalism is the set of attitudes, behaviors, and obligations that define the physician as a member of a profession that has made public commitments to patient welfare, competence, and integrity. Boundary issues are the most common professionalism concerns raised to licensing boards.
Treating Family and Friends
The AMA advises against treating close family and friends except in emergencies or isolated minor conditions. Problems include: inadequate history (reluctance to ask intimate questions), inadequate examination, emotional involvement impairing judgment, disruption of the family relationship, and difficulty discussing bad news. The same concerns apply to self-treatment.
Sexual Relationships with Patients
Sexual contact with a current patient is categorically unethical across every professional code. The power differential, emotional vulnerability of patients, and fiduciary nature of the relationship make authentic consent impossible. Relationships with former patients are also restricted, particularly for psychiatrists (where any post-termination relationship is unethical) and in other specialties where sufficient time and separation have not elapsed.
Gifts from Patients
Small tokens of appreciation may be accepted graciously; large or expensive gifts should generally be declined because they create obligation and may distort care. Context matters: a homemade meal differs from a check. Gifts that affect treatment decisions, bequests from current patients, and patterns of gift-giving raise concerns and should be addressed openly.
Social Media
Physicians should maintain a clear separation between professional and personal online presence, avoid "friending" current patients, never post patient information (even de-identified details may be recognizable), use privacy settings, and remember that anything posted online may become public. Institutional social media policies and state board guidance should be followed.
Physician Impairment
Physicians with conditions (substance use, mental illness, cognitive decline) that impair the safe practice of medicine have obligations to seek help. Colleagues who become aware of impairment have obligations too: first encourage the colleague to seek help, and if unsafe practice continues, report to the state physician health program or licensing board. Reporting is not punitive — physician health programs emphasize rehabilitation.
Reporting Colleague Misconduct
Reporting unethical or incompetent colleagues is required by the AMA Code. Graduated steps: (1) speak to the colleague directly if safe and appropriate, (2) escalate to department chair or chief, (3) report to institutional peer review, and (4) report to state board if patient safety is at stake. "Silence protects no one except the wrongdoer."
Boundary Crossings vs Boundary Violations
| Boundary Crossing | Boundary Violation |
|---|---|
| Minor deviation from usual practice | Deviation that harms or exploits the patient |
| May be therapeutic or neutral | Undermines the therapeutic relationship |
| Examples: attending a funeral, accepting a small gift | Examples: sexual contact, financial exploitation, dual relationships |
| Should be considered carefully and documented | Always unethical; reportable |
The Impaired Physician Pathway
State physician health programs (PHPs) provide confidential evaluation, treatment, and monitoring for physicians with substance use disorders, mental illness, cognitive decline, or disruptive behavior. Outcomes with PHP monitoring are substantially better than general treatment populations, with five-year abstinence rates commonly above 70%. Early identification and non-punitive referral pathways protect both the public and the physician.
22 Conflicts of Interest & Industry
A conflict of interest (COI) arises when a secondary interest (financial gain, career advancement, family relationship) may unduly influence a professional judgment concerning a primary interest (patient welfare, scientific integrity). COIs are not inherently unethical, but unmanaged COIs threaten trust and may cause real harm.
Identifying Conflicts of Interest
A useful test: would a reasonable patient want to know about this interest when evaluating my recommendation? If yes, the interest is significant enough to manage. COIs may involve money, personal relationships, career advancement, reputation, intellectual commitments, or ideological investments. Not all must be avoided, but all should be identified and considered.
Management Hierarchy
| Approach | Description |
|---|---|
| Avoid | Decline the secondary interest (most protective) |
| Eliminate | Remove the conflicting arrangement |
| Recuse | Step out of decisions affected by the conflict |
| Disclose | Transparent disclosure to patients, colleagues, and readers |
| Manage | Oversight, limits, and monitoring |
Disclosure alone is not sufficient when the conflict is large or directly affects patient care. It may even be counterproductive: patients disclosed to may feel more pressure to accept a physician's recommendation because of the implicit honesty signal.
Pharmaceutical Industry Relationships
Interactions with the pharmaceutical and device industries include gifts, meals, continuing education, speakers' bureaus, research funding, and consulting. Evidence from multiple studies shows that even small gifts influence prescribing. Current norms (PhRMA Code, AMA opinions, institutional policies) restrict or prohibit: gifts of more than minimal value, branded items, industry-funded travel and entertainment, ghostwritten publications, and acceptance of samples that bypass formulary review. The federal Physician Payments Sunshine Act (2010) requires public disclosure of industry payments to physicians.
Research Conflicts of Interest
Financial interests in research outcomes — equity in a sponsor, royalties, consulting fees — may bias study design, conduct, analysis, or reporting. Investigators must disclose to IRBs, sponsors, and participants; institutions may require divestment, independent oversight, or exclusion from certain roles. COI disclosure in published research is required by most major journals.
Expert Witness Ethics
Physicians who serve as expert witnesses owe honesty to the court, must base testimony on current scientific evidence, should testify only within their expertise, and must not accept contingency fees. False or negligent testimony is actionable by licensing boards.
Financial Incentives and Dual Loyalty
Contemporary payment structures create additional conflicts. Fee-for-service incentivizes volume; capitation incentivizes restraint; bundled payments reward efficiency but can encourage under-treatment; quality bonuses may penalize physicians caring for vulnerable populations. Employed physicians face institutional pressures on productivity and resource use. Dual loyalty arises when the physician owes duties to both the patient and another party (employer, insurer, military, prison, sports team). Ethical navigation requires transparency, prioritizing patient welfare whenever possible, and disclosing limits of confidentiality or advocacy to the patient at the outset.


23 Research Ethics & IRB
Research ethics applies broader ethical principles to the generation of generalizable knowledge. Because research subjects often bear risks without direct benefit, stricter safeguards apply than in clinical care.
Historical Context: Why Research Ethics Is Distinct
Clinical medicine and clinical research share methods but differ in purpose: treatment aims to benefit the individual patient, while research aims to produce generalizable knowledge. This distinction matters because patients in research may not derive direct benefit, may face risks unrelated to their own care, and require protections beyond those embedded in ordinary clinical care. Historical abuses (Tuskegee, Willowbrook, Jewish Chronic Disease Hospital, radiation experiments) revealed the dangers of conflating research and treatment, and the modern research ethics apparatus is their direct response.
Institutional Review Boards (IRBs)
IRBs are independent committees that review proposed research involving human subjects to ensure that risks are minimized, risks are reasonable in relation to benefits, selection of subjects is equitable, informed consent is adequate, privacy and confidentiality are protected, and vulnerable populations receive additional protections. IRBs operate under the Common Rule (45 CFR 46) and FDA regulations (21 CFR 50, 56).
Categories of Review
| Category | Criteria |
|---|---|
| Exempt | Minimal risk in defined categories (e.g., anonymous surveys, public data) |
| Expedited | Minimal risk in specified categories; reviewed by chair or designee |
| Full board | Greater than minimal risk or involving vulnerable populations |
Clinical Equipoise
Randomized trials are ethically justified when there is genuine uncertainty in the expert community about whether the experimental intervention is superior to the control — clinical equipoise (Freedman, 1987). When evidence accumulates that one arm is clearly superior, equipoise is broken and the trial should be stopped. This is why trials have data and safety monitoring boards (DSMBs) that monitor for early efficacy, futility, or harm.
Placebo Controls
Placebo controls are ethically acceptable when no proven effective treatment exists, when the condition is minor with low risk of harm from brief delay, or when add-on to standard care. Placebo is generally unethical when an effective treatment exists and withholding it would cause serious harm.
Vulnerable Populations
The Common Rule defines additional protections for: pregnant women and fetuses (Subpart B), prisoners (Subpart C), and children (Subpart D). Other populations warranting additional care include cognitively impaired adults, students and employees of the investigator (power asymmetry), economically disadvantaged persons, and terminally ill patients who may have "therapeutic misconception" — believing research is primarily for their benefit when it is not.
Scientific Misconduct
Research misconduct is defined by the US Office of Research Integrity as fabrication (making up data), falsification (manipulating data or results), and plagiarism. It does not include honest error or differences of opinion. Authorship disputes, salami-slicing, ghostwriting, and duplicate publication are related but distinct ethical problems.
Authorship and Publication Ethics
| Issue | Standard |
|---|---|
| Authorship criteria | ICMJE: substantial contribution, drafting/revising, final approval, accountability |
| Ghost authorship | Unethical: undisclosed contributors (often industry writers) |
| Gift authorship | Unethical: listing individuals who did not contribute |
| Duplicate publication | Unethical: publishing the same data as new findings in multiple venues |
| Salami slicing | Fragmenting a single study into multiple minimal publications |
| Pre-registration | Required for clinical trials (ClinicalTrials.gov); protects against selective reporting |


24 Pediatric & Reproductive Ethics
Constitutional and Statutory Background
Pediatric and reproductive ethics operate against a dynamic legal backdrop. Federal and state law, court decisions, and agency regulations all shape what is permitted, required, or prohibited. Clinicians must be familiar with the current law in their jurisdiction while recognizing that legal permissibility is not identical to ethical correctness, and that ethical obligations (honesty, beneficence, non-maleficence) persist regardless of the legal landscape.
Pediatric Decision-Making
Pediatric ethics operates in a triadic relationship: child, parents, and clinicians. Parents generally speak for their children under the best interest standard, but their authority is not absolute. The state has parens patriae power to override parental decisions that endanger the child.
Parental Refusal of Effective Treatment
When parents refuse clearly beneficial treatment for serious or life-threatening conditions (e.g., blood transfusion for severe anemia, insulin for DKA, chemotherapy for curable leukemia), the clinician's obligation runs to the child. Steps: engage the parents, seek common ground, address concerns, offer time and second opinions, and if the child is at serious risk, obtain a court order for treatment. Courts routinely authorize treatment in such cases.
Religious Exemptions
Parents' rights to raise children within their religion are broad but do not extend to allowing preventable serious harm. The classic formulation from Prince v. Massachusetts (1944): "Parents may be free to become martyrs themselves. But it does not follow they are free, in identical circumstances, to make martyrs of their children."
Assent and Dissent
Children who can understand what is proposed should be asked for assent. Dissent from children old enough to express it should be taken seriously, particularly for non-therapeutic research and for interventions that can ethically be delayed. In life-saving therapy, the child's dissent does not override consent from parents, but it should be acknowledged and supported.
Reproductive Ethics
| Issue | Central Tensions |
|---|---|
| Contraception | Autonomy, conscience, access, minors' rights |
| Abortion | Bodily autonomy, fetal interests, viability, legal landscape |
| Assisted reproduction | Access, commodification, disposition of embryos, multiple gestation |
| Prenatal testing | Informed choice, disability rights, selective termination |
| Surrogacy | Autonomy, exploitation, parental rights, cross-border issues |
| Maternal–fetal conflict | Refusal of cesarean, substance use in pregnancy |
Conscientious Objection
Clinicians have some latitude to refuse to provide interventions that violate their deeply held moral beliefs, but conscientious objection is bounded: clinicians must not abandon patients, must disclose their objection in advance when possible, must provide emergency care, must offer accurate information, and must facilitate transfer to a willing provider. The patient's access to legal, indicated care should not be blocked by the clinician's values.
Adolescent Autonomy
Adolescents occupy an ethically intermediate zone. They are developing decisional capacity, gaining legal rights incrementally, and often making decisions about sensitive areas where parental involvement is complicated. Clinicians should assess individual maturity rather than relying on chronological age alone, honor statutory confidentiality for sensitive services, and encourage — but not require — parental involvement where appropriate. End-of-life decisions by adolescents with life-limiting illness raise particularly difficult questions and typically involve the adolescent, parents, and clinicians in shared decision-making.
Gender-Affirming Care for Minors
Gender-affirming care for transgender and gender-diverse minors is a contested area with evolving clinical guidelines, heterogeneous political landscapes, and active ethical debate. Established frameworks emphasize multidisciplinary evaluation, staged and reversible interventions before irreversible ones, informed consent/assent processes appropriate to developmental stage, parental involvement, and attention to co-occurring mental health needs. Clinicians should follow professional society guidelines and applicable state law while preserving their core ethical commitments to autonomy, beneficence, and non-maleficence.
25 Genetic Testing & Resource Allocation
Informed Consent for Genomic Testing
Consent for clinical genomic testing should cover: the condition being tested for, the test's sensitivity and specificity, possible results (positive, negative, uncertain), implications for family members, handling of incidental/secondary findings, privacy protections, the option to decline learning specific categories of results, and storage and future use of samples. Broad sequencing (exome, genome) makes pre-test counseling especially important because the scope of possible findings is much wider than targeted testing.
Ethical Issues in Genetic Testing
Genetic information is uniquely identifying, shared with biological relatives, and potentially predictive. It can inform reproductive choices, prevention strategies, and treatment selection, but also raises risks of discrimination, family conflict, and psychological burden.
| Issue | Considerations |
|---|---|
| Predictive testing for adult-onset disease | Huntington disease, BRCA; counseling about implications before and after |
| Testing of children | Defer testing for adult-onset disease until the child can decide; exceptions for actionable pediatric conditions |
| Incidental findings | ACMG list of actionable secondary findings; patient opt-out |
| Duty to warn relatives | Encourage patient disclosure; clinician direct notification is exceptional |
| Direct-to-consumer testing | Variable accuracy, inadequate counseling, interpretation challenges |
| GINA protections | Federal law prohibits genetic discrimination in employment and health insurance; not life, disability, long-term care |
Privacy and Genetic Discrimination
GINA (2008) prohibits health insurers and employers from using genetic information to discriminate, but it does not cover life, disability, or long-term care insurance. Patients considering genetic testing should be counseled about these gaps. Disclosure of genetic information outside healthcare — to relatives, to insurers, to employers, to law enforcement through databases — involves both legal and ethical considerations, and the boundaries are evolving with technology.
Resource Allocation
Justice issues arise whenever demand exceeds supply — ICU beds, ventilators, organs, vaccines, expensive therapies. Allocation criteria vary by context but should be: publicly justified, applied consistently, sensitive to medical benefit, and free of invidious discrimination.
Triage in Mass Casualty and Crisis Standards of Care
| Framework | Description |
|---|---|
| Conventional care | Usual standards; no allocation decisions required |
| Contingency care | Adapted care maintains usual outcomes; minor allocation adjustments |
| Crisis standards of care | Scarcity forces allocation that differs from usual standards; formal protocols |
Crisis allocation protocols typically prioritize patients most likely to benefit (short-term survival), sometimes with tiebreakers such as life-cycle considerations or random allocation. Exclusion criteria must be based on evidence, applied evenhandedly, and free of categorical discrimination (age, disability, race, ethnicity, socioeconomic status).
Organ Allocation
UNOS oversees organ allocation in the United States with policies designed to balance medical urgency, probability of success, time on waiting list, and geographic proximity. Allocation policies are regularly revised to address disparities (e.g., MELD/MELD-Na revisions, lung allocation score, kidney allocation system). Public trust in allocation depends on transparency and procedural fairness.
Pandemic Allocation: Lessons from COVID-19
The COVID-19 pandemic tested allocation ethics at scale. Ventilator shortage protocols, vaccine prioritization, and crisis standards of care drew on existing frameworks while generating new lessons: categorical exclusions based on disability were challenged as discriminatory; SOFA-based scoring systems raised concerns about racial bias because of disparate comorbidity burden; transparent public engagement before crisis improved legitimacy; and vaccine allocation balanced risk of exposure (healthcare workers), risk of severe disease (elderly), and broader societal function (teachers, essential workers). Post-pandemic review continues to refine these frameworks.
26 Cross-Cultural, Truth-Telling & Error Disclosure
Overview
Some of the most difficult ethical issues in practice do not involve dramatic dilemmas but everyday patterns of communication: when and how to deliver hard news, how to navigate cultural differences without imposing one's own values, and how to respond when care has not gone as planned. This section addresses these common, consequential, and teachable domains.
Cross-Cultural Ethics
Patients come from diverse cultural, religious, and linguistic backgrounds, and clinicians must navigate value differences without imposing their own framework or retreating into relativism. Key practices: use qualified interpreters, ask about preferences for disclosure and decision-making ("Some patients want to know everything; others prefer we speak with their family first — what do you prefer?"), respect different models of illness and healing, and engage community resources. Autonomy, as operationalized in American medicine, is itself a cultural value; some cultures prioritize family-centered decision-making, which is not a defect but a different legitimate model.
Family Requests for Non-Disclosure
Families sometimes ask clinicians not to disclose a serious diagnosis to the patient ("don't tell her it's cancer — it will kill her"). This request often reflects love and fear, not malice, and should be engaged thoughtfully. The best approach is to explore with the family what they worry will happen, acknowledge their concern, and then ask the patient directly how much they want to know and from whom. Many patients, when asked, do want to know; others prefer family-centered disclosure; either preference should be respected.
Truth-Telling and Breaking Bad News
Modern ethics strongly favors honest disclosure. Historical paternalistic practices of withholding diagnoses (especially cancer) are now regarded as ethically problematic because they undermine autonomy, erode trust when patients eventually discover the truth, and preclude meaningful planning. Disclosure should be honest, compassionate, paced to the patient's readiness, and responsive to cultural preferences for how and through whom information flows.
S — Setting: privacy, sit down, minimize interruptions.
P — Perception: "What do you understand about your situation?"
I — Invitation: "How much would you like to know?"
K — Knowledge: warn ("I have difficult news"), then share clearly.
E — Emotion: acknowledge with empathic statements before moving on.
S — Strategy & Summary: next steps, follow-up, questions.
Disclosure of Medical Errors
When medical errors harm patients, disclosure is an ethical obligation. Patients have a right to know what happened, an accurate explanation, expression of regret, information about what will be done to prevent recurrence, and where appropriate, apology and fair compensation. Institutional "disclosure and apology" programs have been associated with reduced litigation, lower malpractice costs, and improved patient satisfaction. Concealment is both wrong and typically counterproductive.
| Step | Content |
|---|---|
| Prepare | Gather facts, assemble the team, plan the conversation |
| Disclose | State clearly what happened, in plain language, without blaming |
| Acknowledge | Express genuine regret and empathy for the impact |
| Explain next steps | What will be done clinically and systemically |
| Follow up | Continue the relationship; do not disappear |
Apology
Expressions of sympathy ("I am so sorry this happened") are universally appropriate. True apologies that accept responsibility should be given when responsibility is genuinely owed; over 35 states have "apology laws" that protect expressions of sympathy from being used as evidence of liability.
Moral Distress and Clinician Well-Being
Clinicians frequently experience moral distress — knowing the ethically right action but being constrained from taking it by institutional, legal, or interpersonal barriers. Recurrent moral distress contributes to burnout, attrition, and impaired care. Institutional responses include ethics consultation, peer support, debriefing after difficult cases, process changes to reduce the sources of distress, and acknowledgment that moral distress is a legitimate clinical concern rather than individual weakness.
Cultural Humility vs Cultural Competence
"Cultural competence" implies a checklist of group characteristics, which can devolve into stereotyping. Cultural humility is a lifelong commitment to self-reflection about one's own assumptions, curiosity about each patient's individual values, and recognition of power imbalances in the clinical encounter. It assumes the patient is the expert on their own life and asks rather than presumes.

27 Ethics Consultation & Landmark Cases
Integrating Ethics into Daily Practice
Ethics is not a separate activity reserved for consultations; it is a dimension of every clinical encounter. Brief ethical attention — asking the patient's goals, confirming understanding, checking for hidden concerns, acknowledging emotion — takes little additional time and shapes the quality of care. The habits of honesty, respect, and care that define ethical practice are learned through repetition and feedback, not through one-time coursework.
Clinical Ethics Consultation
Most US hospitals have ethics committees or consultation services that assist clinicians, patients, and families with value-laden decisions. Consultation is available when: principles conflict, stakeholders disagree about the right course of action, complex cases exceed usual institutional experience, or additional perspectives would be valuable. Ethics consultation is advisory — the final decision remains with the patient or surrogate and the treating team.
The Ethics Consultation Process
- Identify the question: What is the specific ethical issue?
- Gather information: Medical facts, patient preferences, context, relevant policies and law.
- Identify stakeholders: Patient, family, team, institution, community.
- Frame using principles and methods: Four Boxes, principlism, narrative.
- Facilitate communication: Convene meetings; listen; clarify misunderstandings.
- Recommend: Offer reasoned options; respect decision-making authority.
- Document and follow up: Note the reasoning, recommendations, and outcomes.
Landmark Court Cases
| Case | Year | Holding / Significance |
|---|---|---|
| Schloendorff v. Society of NY Hospital | 1914 | "Every human being of adult years and sound mind has a right to determine what shall be done with his own body" — consent foundation |
| Canterbury v. Spence | 1972 | Established the reasonable-patient standard of disclosure |
| Tarasoff v. Regents | 1976 | Duty to protect identifiable third parties from a patient’s credible threat |
| In re Quinlan | 1976 | Right of surrogates to withdraw mechanical ventilation from a permanently unconscious patient |
| Cruzan v. Director, MDH | 1990 | Competent individuals have a constitutional right to refuse treatment; states may require clear evidence for surrogate decisions; ANH is medical treatment |
| Washington v. Glucksberg | 1997 | No federal constitutional right to physician-assisted suicide; states may legislate |
| Schiavo cases | 2005 | Affirmed surrogate authority to withdraw ANH in persistent vegetative state after robust judicial review |
| Prince v. Massachusetts | 1944 | Parental religious liberty does not extend to allowing serious harm to children |
Common Dilemmas & First-Pass Frameworks
| Dilemma | First-Pass Answer |
|---|---|
| Capable patient refuses beneficial treatment | Respect refusal after thorough informed discussion and capacity confirmation |
| Family requests non-disclosure of diagnosis | Ask the patient how much they want to know and from whom |
| Surrogate wants treatment contrary to advance directive | Honor the directive; clarify substituted judgment standard |
| Parents refuse life-saving treatment for child | Engage, offer resources, seek court order if necessary |
| Colleague impaired or unethical | Address directly; escalate to supervisor, PHP, or board |
| Patient threatens third party | Assess seriousness; warn/protect as indicated (Tarasoff) |
| Medical error harms patient | Disclose promptly, honestly, compassionately |
| Industry gift or meal offered | Decline when in doubt; follow institutional policy |
Types of Ethics Consultation Models
| Model | Features |
|---|---|
| Full committee | Multidisciplinary committee reviews the case together; deliberate, inclusive, slower |
| Small team | 2–3 consultants meet with stakeholders; faster, flexible |
| Individual consultant | Single trained ethicist; efficient but less representative |
Competencies for Ethics Consultation
The ASBH (American Society for Bioethics and Humanities) core competencies include ethical assessment, process skills (facilitation, mediation, interpersonal communication), and interpersonal skills. Consultants need knowledge of moral reasoning, clinical ethics, healthcare law, organizational dynamics, and relevant professional codes. Certification pathways are emerging to standardize training and practice.

28 High-Yield Review
This section consolidates the most frequently tested concepts and the heuristics that resolve the overwhelming majority of medical ethics exam questions.
One-Page Glossary
| Term | Definition |
|---|---|
| Autonomy | Self-governance; right to make informed choices about one’s own body and care |
| Beneficence | Obligation to act for the patient’s welfare |
| Non-maleficence | Obligation to avoid causing harm; proportionate risk/benefit |
| Justice | Fair distribution of benefits, burdens, and resources |
| Capacity | Clinical ability to make a specific decision at a specific time |
| Competence | Legal status determined by a court |
| Informed consent | Process: disclosure, comprehension, voluntariness, capacity, authorization |
| Advance directive | Document expressing future care preferences or designating a proxy |
| Substituted judgment | Decision reflecting what the patient would have wanted |
| Best interest | Objective balancing of benefits and burdens when values unknown |
| Double effect | Permissibility of foreseen but unintended harm for proportionate good |
| Futility | Intervention incapable of achieving its physiologic or meaningful goal |
| Confidentiality | Duty not to disclose information shared in a professional relationship |
| HIPAA | US federal law protecting individually identifiable health information |
| Tarasoff duty | Obligation to protect identifiable third parties from a patient’s threat |
| IRB | Independent committee reviewing research involving human subjects |
| Equipoise | Genuine expert uncertainty justifying randomization |
| Therapeutic misconception | Belief that research is primarily for the subject’s benefit |
| Paternalism | Overriding preferences for the agent’s own good |
| Fiduciary | Relationship imposing heightened duties of loyalty and good faith |
Core Principles Quick Reference
| Principle | Ask |
|---|---|
| Autonomy | Does the patient get to choose, with adequate information and capacity? |
| Beneficence | What is the recommended action that promotes the patient’s welfare? |
| Non-maleficence | What harms might this cause, and are they proportionate to benefits? |
| Justice | Is the distribution of benefits and burdens fair? |
Heuristics That Win Ethics Questions
| Heuristic | Application |
|---|---|
| Talk to the patient first | Before family, ethics committee, legal, or chart review |
| Confirm capacity, then honor choice | Refusal is not incapacity; verify the four abilities |
| Address the emotion, then the question | Empathy before information in hard conversations |
| No deception, even to protect | Therapeutic privilege is almost never the answer |
| Disclose errors honestly | Promptly, with empathy and explanation |
| Honor advance directives | They outrank surrogates’ contrary preferences |
| Use minors’ confidential care laws | STIs, contraception, mental health, substance use — minors usually consent |
| Emergency: presume consent | When patient incapacitated and no surrogate reachable |
| Withholding = withdrawing | Ethically equivalent; permits time-limited trials |
| Tarasoff threats | Serious, imminent, identifiable → warn/protect |
| Don’t treat family | Outside of emergencies and trivial situations |
| Decline gifts and meals from industry | Default to institutional policy |
Capacity at a Glance
Understanding — Can the patient paraphrase the information?
Appreciation — Can the patient apply it to themselves?
Reasoning — Can the patient explain how they weighed options?
Expressing a choice — Can the patient state a stable decision?
Informed Consent Elements
Disclosure → comprehension → voluntariness → capacity → authorization. Disclosure must include diagnosis, nature and purpose of the intervention, risks, benefits, and alternatives including no treatment.
Surrogate Decision-Making Standards
Expressed wishes → substituted judgment → best interest. Always ask, "What would the patient want?" not "What would you want?"
End-of-Life Quick Rules
| Situation | Rule |
|---|---|
| Capable patient refuses treatment | Honor refusal |
| Withdrawing vs withholding | Ethically equivalent |
| ANH via feeding tube | Medical intervention; may be refused |
| Opioids for dyspnea at end of life | Permissible under rule of double effect |
| Palliative sedation | Permissible for refractory suffering in imminently dying patients |
| Physician-assisted dying | Legal status varies; conscientious objection protected |
| Brain death | Legally equivalent to cardiopulmonary death |
Confidentiality Exceptions (Memorize)
Reportable diseases, child/elder abuse, gunshot/stab wounds, Tarasoff threats, driving impairment in some states, court orders, and emergency to prevent serious harm. Always disclose the minimum necessary.
Classic Exam Traps
"Call hospital security," "ask the family to decide" (when patient has capacity), "consult ethics committee" (when direct action is correct), "override the patient's refusal because it's in their best interest," "tell the family the diagnosis but not the patient," "give the treatment anyway and document it," "refuse to disclose the error until legal clears it." These are almost always distractors.
Rapid-Fire Scenarios
| Scenario | Correct Action |
|---|---|
| 17-year-old requests confidential contraception | Provide; encourage but do not require parental involvement |
| Jehovah’s Witness refuses blood for herself | Honor refusal after confirming capacity and understanding |
| Jehovah’s Witness parents refuse blood for child with shock | Transfuse; seek emergency court order if time permits |
| Delirious patient trying to leave AMA | Assess capacity; if lacking, prevent departure with least restrictive means |
| Spouse asks for test results outside the room | Do not disclose without patient permission |
| Drug representative offers lunch for staff | Follow institutional policy; generally decline |
| Patient asks you to lie to insurer for coverage | Decline; explore legitimate appeals and alternatives |
| Dying patient requests higher opioid doses for dyspnea | Titrate to comfort under the rule of double effect |
| Family insists on not telling patient the cancer diagnosis | Explore with the patient how much they want to know |
| Colleague appears intoxicated at work | Remove from patient care; notify supervisor/PHP |
| Patient with advance directive refusing intubation now says "do everything" | The current capable voice controls; confirm capacity and update orders |
| Patient reveals intent to harm a specific person | Assess; warn/protect consistent with Tarasoff duties |
| Medication error, no apparent harm yet | Disclose to patient; monitor; report per institutional policy |
| Pregnant patient refuses recommended cesarean | Respect capable refusal; continue counseling and support |
| Unbefriended incapacitated patient | Best-interest standard with institutional ethics or legal safeguards |
| Grateful patient offers expensive gift | Decline graciously; accept only modest tokens if appropriate |
| Former patient asks to start dating you | Decline; sufficient time and separation needed (never in psychiatry) |
| Research participant wants to withdraw mid-study | Respect withdrawal; ensure it does not jeopardize clinical care |
The Single Best Default
When uncertain on an ethics question, the safest default is: respect the capable patient's informed choice, tell the truth, preserve confidentiality with narrow exceptions, and address the patient's underlying concern directly. A remarkable number of ethics questions resolve themselves under these four rules.
