Anatomy
Gross anatomy, neuroanatomy, surface landmarks, vascular territories, lymphatic drainage, fascial planes, and every clinical correlation across the full scope of human anatomy.
01 Anatomical Terminology & Planes
All anatomical descriptions reference the anatomical position: body upright, feet together, arms at sides, palms facing forward (supinated). This universal convention eliminates ambiguity regardless of the patient's actual posture. Mastery of directional terms and body planes is the prerequisite for every anatomical description in clinical medicine, radiology, and surgery.
Directional Terms
| Term | Meaning | Example |
|---|---|---|
| Superior (cranial) | Toward the head | The heart is superior to the diaphragm |
| Inferior (caudal) | Toward the feet | The bladder is inferior to the umbilicus |
| Anterior (ventral) | Toward the front | The sternum is anterior to the heart |
| Posterior (dorsal) | Toward the back | The esophagus is posterior to the trachea |
| Medial | Toward the midline | The ulna is medial to the radius |
| Lateral | Away from midline | The lungs are lateral to the heart |
| Proximal | Closer to trunk/origin | The elbow is proximal to the wrist |
| Distal | Farther from trunk/origin | The fingers are distal to the wrist |
| Superficial | Closer to the surface | Skin is superficial to muscle |
| Deep | Farther from surface | Bone is deep to muscle |
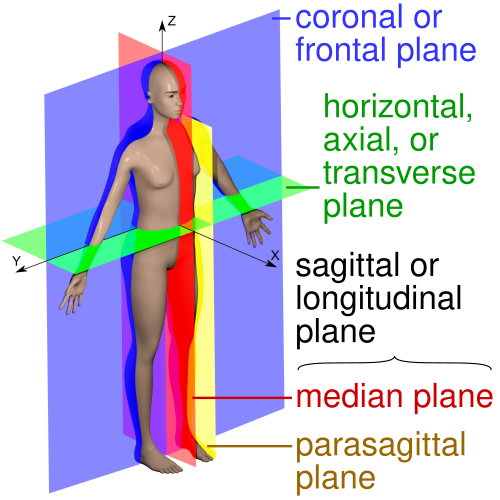
Anatomical Planes
The sagittal plane divides the body into left and right portions (midsagittal = equal halves; parasagittal = unequal). The coronal (frontal) plane divides the body into anterior and posterior portions. The transverse (axial/horizontal) plane divides the body into superior and inferior portions. In cross-sectional imaging (CT, MRI), the axial plane is the standard primary view; coronal and sagittal reconstructions complement it.
Body Regions & Quadrants
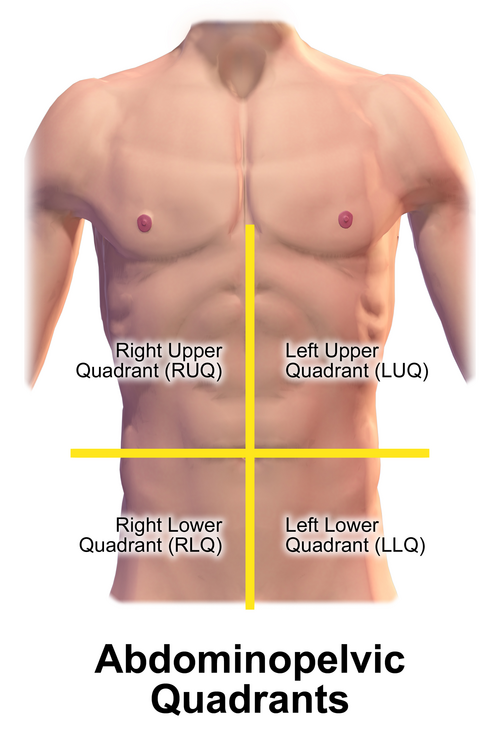
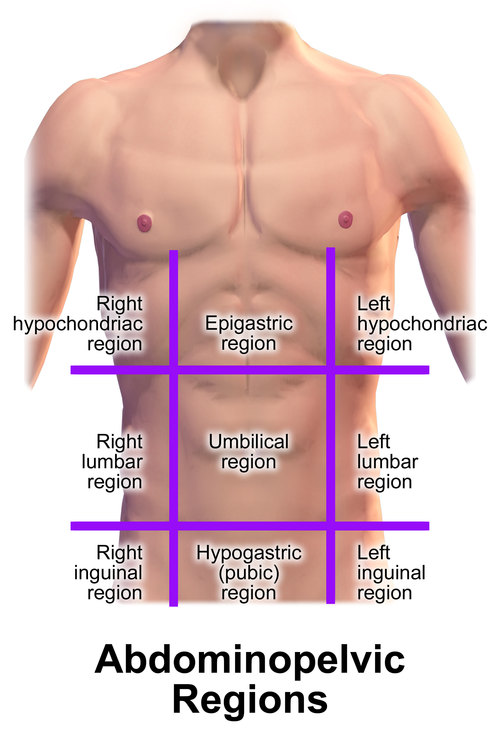
The abdomen is divided into four quadrants (RUQ, LUQ, RLQ, LLQ) by the transumbilical and median planes, or into nine regions (right/left hypochondriac, epigastric, right/left lumbar, umbilical, right/left iliac, hypogastric) by two midclavicular vertical lines and the subcostal/transtubercular horizontal lines. The quadrant system is preferred in emergent clinical settings; the nine-region system is more precise for surgical documentation.
Abdominal Quadrant Organ Map
| Quadrant | Key Organs | Common Pathology |
|---|---|---|
| RUQ | Liver, gallbladder, right kidney, duodenum, hepatic flexure of colon | Cholecystitis (Murphy sign), hepatitis, hepatic abscess, right renal colic |
| LUQ | Spleen, stomach, left kidney, splenic flexure of colon, tail of pancreas | Splenic rupture (Kehr sign), gastric ulcer, left renal colic |
| RLQ | Appendix, cecum, right ovary/tube, right ureter | Appendicitis (McBurney point), Meckel diverticulitis, ectopic pregnancy, ovarian torsion |
| LLQ | Sigmoid colon, left ovary/tube, left ureter | Diverticulitis, sigmoid volvulus, ectopic pregnancy, ovarian torsion |
Movements
| Movement | Definition | Clinical Relevance |
|---|---|---|
| Flexion / Extension | Decrease / increase joint angle | Elbow flexion = biceps; knee extension = quadriceps |
| Abduction / Adduction | Move away from / toward midline | Shoulder abduction tests supraspinatus (0–15°) then deltoid |
| Internal / External rotation | Rotate toward / away from midline | Hip IR/ER tests for femoral neck fracture |
| Pronation / Supination | Palm down / palm up | Pronator teres: median nerve; supinator: radial nerve |
| Dorsiflexion / Plantarflexion | Foot up / foot down | Foot drop (dorsiflexion loss) = common fibular nerve injury |
| Inversion / Eversion | Sole inward / sole outward | Ankle sprains: inversion injuries damage lateral ligaments |
| Protraction / Retraction | Move anteriorly / posteriorly along a horizontal plane | Scapular protraction (serratus anterior) — winged scapula if weak |
| Elevation / Depression | Move superiorly / inferiorly | Shoulder shrug (trapezius, levator scapulae); CN XI tests elevation |
| Circumduction | Conical movement combining flexion, extension, abduction, adduction | Ball-and-socket joints (shoulder, hip) |
| Opposition | Thumb pad touches finger pads | Unique to 1st CMC joint; tests recurrent branch of median nerve |
Joint Classification
| Type | Subtype | Movement | Examples |
|---|---|---|---|
| Fibrous | Suture | None (synarthrosis) | Skull sutures |
| Fibrous | Syndesmosis | Minimal | Distal tibiofibular joint, interosseous membrane |
| Cartilaginous | Synchondrosis (primary) | None | Epiphyseal growth plate, costochondral joints |
| Cartilaginous | Symphysis (secondary) | Limited | Pubic symphysis, intervertebral discs |
| Synovial | Hinge | Flexion/extension | Elbow (humeroulnar), knee, ankle (talocrural) |
| Synovial | Ball-and-socket | Multi-axial | Hip, shoulder (glenohumeral) |
| Synovial | Pivot | Rotation | Atlantoaxial (C1–C2), proximal radioulnar |
| Synovial | Saddle | Biaxial | 1st carpometacarpal (thumb) |
| Synovial | Condyloid (ellipsoid) | Biaxial (no rotation) | Radiocarpal (wrist), MCP joints |
| Synovial | Plane (gliding) | Sliding | Acromioclavicular, intercarpal, facet joints |
02 Embryology Essentials
Understanding embryologic development explains congenital anomalies, anatomical variants, and the logic of adult structural relationships. Key developmental events occur during weeks 3–8 (the embryonic period), when all major organ systems are established and the embryo is most vulnerable to teratogens.
Germ Layers & Derivatives
| Germ Layer | Key Derivatives |
|---|---|
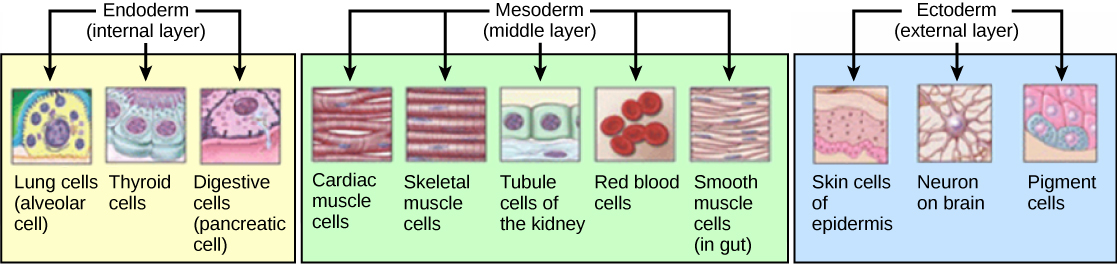
| Ectoderm | Epidermis, CNS (neural tube), PNS (neural crest), lens of eye, tooth enamel, anterior pituitary (Rathke pouch), adrenal medulla (neural crest) |
| Mesoderm | Muscle (skeletal, smooth, cardiac), bone, cartilage, connective tissue, kidneys, gonads, spleen, adrenal cortex, blood vessels, blood cells, dura mater |
| Endoderm | GI tract epithelium, liver, pancreas, thyroid, parathyroid, thymus, lungs (epithelial lining), bladder lining, urethra |
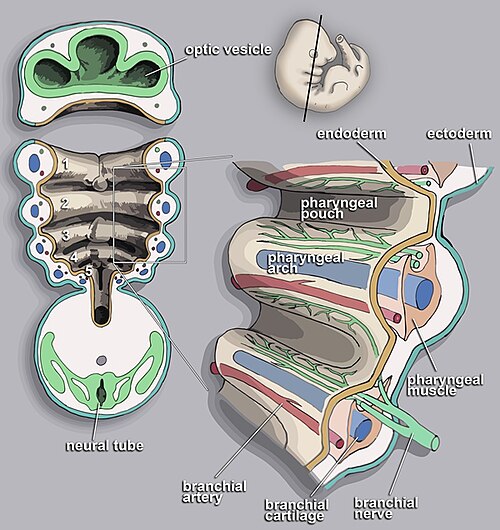
Neural Crest Derivatives
The neural crest is sometimes called the "fourth germ layer" due to its remarkable diversity of derivatives: melanocytes, dorsal root ganglia, autonomic ganglia, Schwann cells, adrenal medulla (chromaffin cells), odontoblasts, parafollicular C cells of thyroid, pharyngeal arch cartilage and bones, aorticopulmonary septum, and enteric nervous system. Neural crest defects underlie DiGeorge syndrome (22q11.2 deletion → abnormal 3rd/4th pharyngeal pouch development), Hirschsprung disease (absent enteric ganglia), and Waardenburg syndrome.
Arch 1 (CN V): mandible, maxilla, malleus, incus, muscles of mastication. Arch 2 (CN VII): stapes, styloid process, muscles of facial expression, stapedius. Arch 3 (CN IX): stylopharyngeus, common/internal carotids. Arch 4 (CN X superior laryngeal): cricothyroid, aortic arch (left), right subclavian (right). Arch 6 (CN X recurrent laryngeal): all intrinsic laryngeal muscles except cricothyroid, pulmonary arteries, ductus arteriosus (left).
Key Developmental Milestones
| Structure | Developmental Origin | Clinical Correlate |
|---|---|---|
| Neural tube | Ectoderm; closes by day 28 | Failure to close → spina bifida (caudal), anencephaly (cranial) |
| Heart | Lateral plate mesoderm; beating by day 22 | Septation defects → VSD (most common CHD), ASD |
| Kidneys | Intermediate mesoderm; pronephros → mesonephros → metanephros | Horseshoe kidney trapped under IMA; ectopic kidney |
| GI rotation | Midgut rotates 270° counterclockwise around SMA | Malrotation → volvulus; failure of return → omphalocele |
| Diaphragm | Septum transversum + pleuroperitoneal folds + body wall + esophageal mesentery | Bochdalek hernia (posterolateral defect, left > right) |
Pharyngeal Pouch Derivatives
| Pouch | Derivatives | Clinical Significance |
|---|---|---|
| 1st pouch | Middle ear cavity, eustachian tube, mastoid antrum | Chronic otitis media can erode into mastoid |
| 2nd pouch | Palatine tonsils, tonsillar fossa epithelium | Peritonsillar abscess |
| 3rd pouch (dorsal) | Inferior parathyroid glands | Variable position (descend with thymus); ectopic location common |
| 3rd pouch (ventral) | Thymus | DiGeorge syndrome: absent thymus & parathyroids (22q11 deletion) |
| 4th pouch (dorsal) | Superior parathyroid glands | More constant position than inferior parathyroids |
| 4th pouch (ventral) | Parafollicular C cells of thyroid (ultimobranchial body) | C cells produce calcitonin; medullary thyroid carcinoma |
Congenital Anomalies: High-Yield Summary
| Anomaly | Embryologic Defect | Presentation |
|---|---|---|
| Meckel diverticulum | Persistence of vitelline (omphalomesenteric) duct | "Rule of 2s": 2% of population, 2 feet from ileocecal valve, 2 inches long, 2 types of ectopic tissue (gastric/pancreatic), presents by age 2 |
| Thyroglossal duct cyst | Persistent thyroglossal duct (thyroid descent tract) | Midline neck mass that moves with swallowing and tongue protrusion; most common congenital neck mass |
| Branchial cleft cyst | Persistent 2nd branchial cleft (most common) | Lateral neck mass anterior to SCM; may have a sinus tract |
| Horseshoe kidney | Inferior poles fuse during ascent; trapped under IMA | Usually asymptomatic; found at L3 (normal = L1–L2); increased risk of UPJ obstruction |
| Tracheoesophageal fistula | Abnormal septation of foregut into trachea and esophagus | Most common type (85%): proximal esophageal atresia with distal TEF; polyhydramnios, inability to feed, gastric distension |
03 Histological Tissue Types
The human body is composed of four fundamental tissue types. Recognition of tissue architecture is essential for pathology interpretation and understanding how anatomy relates to function at the microscopic level.
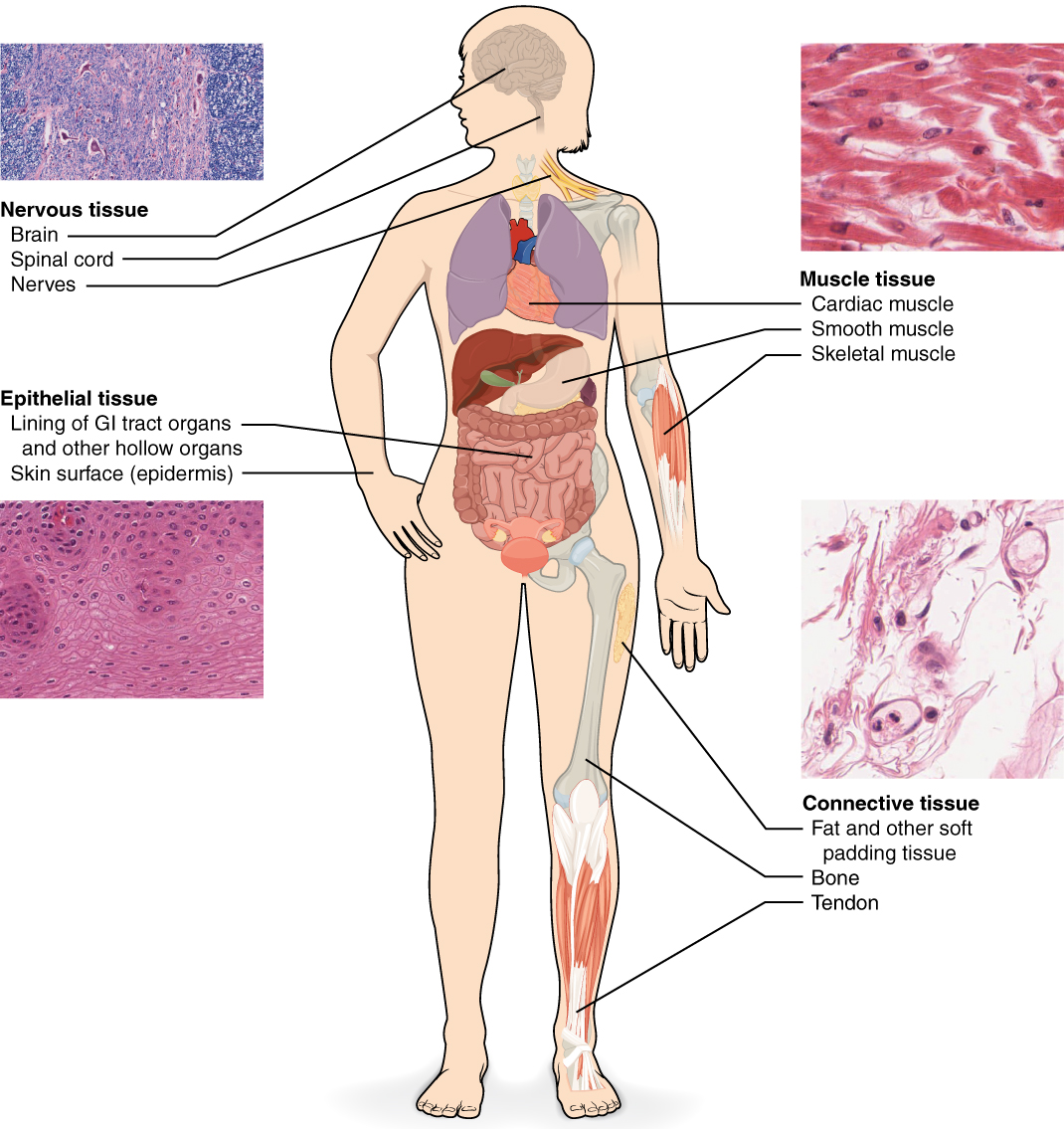
The Four Tissue Types
| Tissue | Subtypes | Key Features | Locations |
|---|---|---|---|
| Epithelial | Simple squamous, cuboidal, columnar; stratified squamous, transitional; pseudostratified columnar | Avascular, basement membrane, high regeneration, tight junctions | Skin, GI lining, airways, kidney tubules, glands |
| Connective | Loose (areolar), dense (regular, irregular), adipose, cartilage (hyaline, elastic, fibro), bone, blood | ECM-rich, vascular (except cartilage), mesoderm-derived | Tendons, ligaments, fascia, organ stroma, skeleton |
| Muscle | Skeletal (voluntary, striated), cardiac (involuntary, striated, intercalated discs), smooth (involuntary, non-striated) | Contractile proteins (actin/myosin), excitable membranes | Skeletal muscles, heart, blood vessel walls, GI tract |
| Nervous | Neurons (cell body, axon, dendrites); neuroglia (astrocytes, oligodendrocytes, microglia, Schwann cells, ependymal) | Electrochemical signaling, limited regeneration in CNS | Brain, spinal cord, peripheral nerves, ganglia |
Metaplasia is the reversible transformation of one differentiated cell type to another. Barrett esophagus (squamous → columnar in distal esophagus due to chronic GERD) increases adenocarcinoma risk. Squamous metaplasia in bronchi (columnar → squamous from chronic smoking) is a precursor to squamous cell carcinoma. The squamocolumnar junction of the cervix (transformation zone) is the primary site of cervical dysplasia and carcinoma.
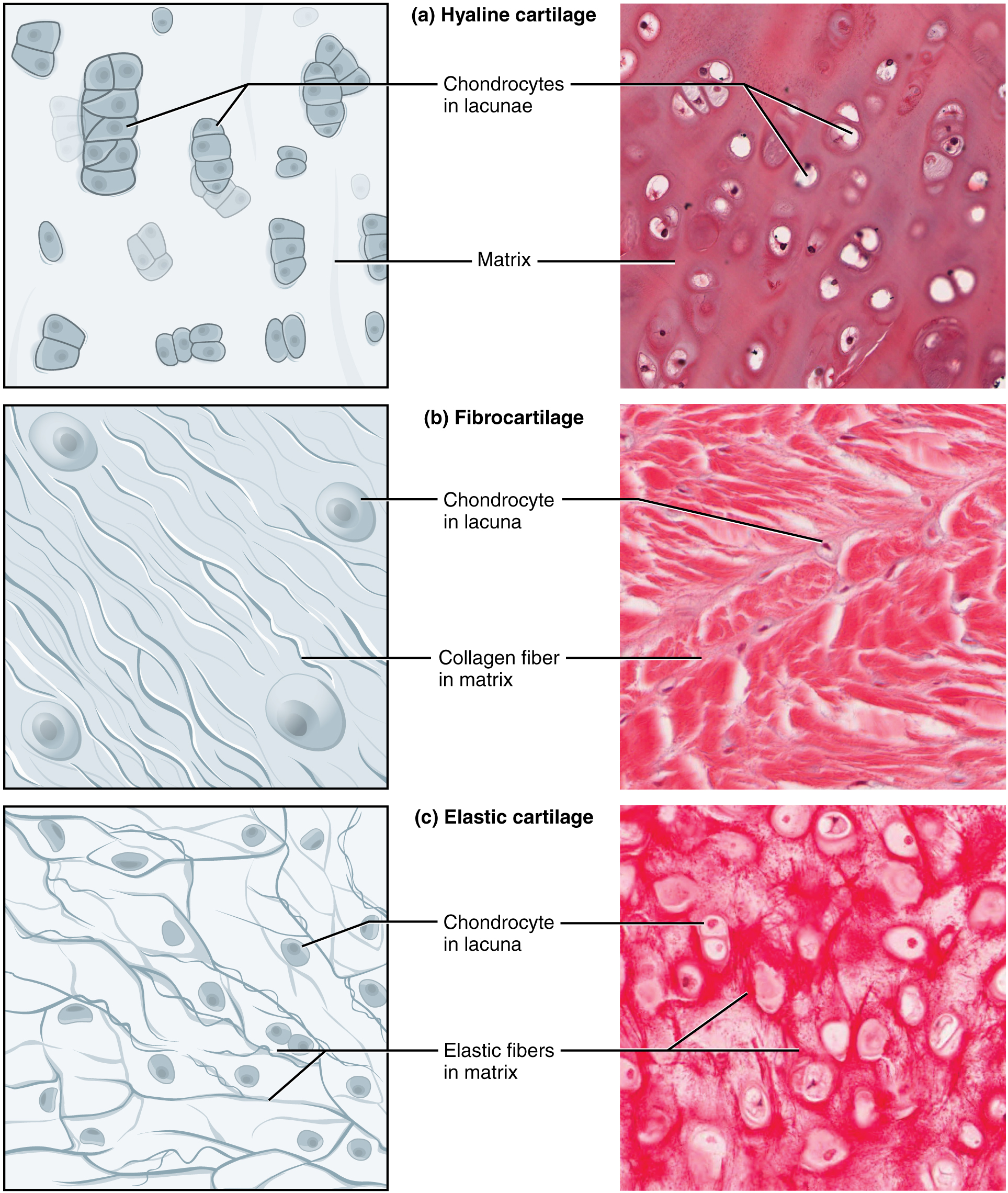
Cartilage Types
| Type | Matrix | Location | Clinical Note |
|---|---|---|---|
| Hyaline | Type II collagen, chondroitin sulfate | Tracheal rings, articular surfaces, costal cartilage, nasal septum | Most common; degenerates in osteoarthritis |
| Elastic | Elastin + type II collagen | Ear pinna, epiglottis, auditory tube | Flexible; relapsing polychondritis targets elastic cartilage |
| Fibrocartilage | Type I collagen (dense) | Intervertebral discs, menisci, pubic symphysis, TMJ disc | Strongest; absorbs compressive forces; disc herniation |
Bone Types & Ossification
| Feature | Intramembranous | Endochondral |
|---|---|---|
| Process | Mesenchyme → bone directly (no cartilage intermediate) | Mesenchyme → cartilage model → replaced by bone |
| Bones formed | Flat bones: skull vault, mandible, clavicle | Long bones, vertebrae, pelvis, base of skull |
| Growth centers | Ossification centers expand radially | Primary center (diaphysis) and secondary centers (epiphyses); growth at epiphyseal plate (physis) |
| Clinical | Craniosynostosis (premature suture fusion) | Achondroplasia (FGFR3 mutation → impaired endochondral ossification → short limbs, normal trunk) |
Bone Fracture Healing Stages
1. Hematoma formation (hours–days): blood clot at fracture site. 2. Soft (fibrocartilaginous) callus (days–weeks): fibroblasts and chondrocytes produce collagen and cartilage matrix. 3. Hard (bony) callus (weeks–months): osteoblasts replace cartilage with woven bone via endochondral ossification. 4. Remodeling (months–years): osteoclasts resorb woven bone; osteoblasts deposit lamellar bone along lines of stress (Wolff's law). Fractures heal faster in children, in well-vascularized regions, and with stable fixation. Delayed healing occurs with smoking, NSAIDs, corticosteroids, infection, and poor blood supply (e.g., scaphoid, femoral neck, talus).
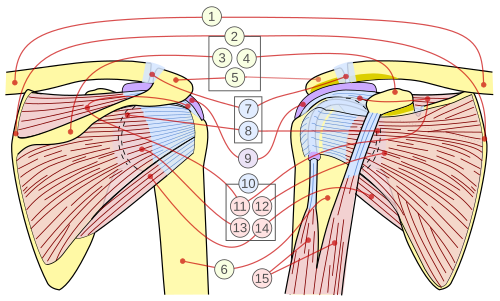
04 Shoulder & Arm
The shoulder is the most mobile joint in the body (ball-and-socket) but sacrifices stability for range of motion. The glenohumeral joint has a shallow glenoid fossa deepened by the fibrocartilaginous labrum. Stability depends primarily on the rotator cuff muscles (SITS: supraspinatus, infraspinatus, teres minor, subscapularis) and the glenohumeral ligaments.
Rotator Cuff Muscles
| Muscle | Origin | Insertion | Action | Innervation |
|---|---|---|---|---|
| Supraspinatus | Supraspinous fossa | Greater tubercle (superior) | Initiates abduction (0–15°) | Suprascapular n. (C5–C6) |
| Infraspinatus | Infraspinous fossa | Greater tubercle (middle) | External rotation | Suprascapular n. (C5–C6) |
| Teres minor | Lateral border of scapula | Greater tubercle (inferior) | External rotation | Axillary n. (C5–C6) |
| Subscapularis | Subscapular fossa | Lesser tubercle | Internal rotation | Upper & lower subscapular nn. (C5–C6) |
Arm Muscles & Compartments
The anterior compartment (musculocutaneous nerve, C5–C7) contains biceps brachii (flexion, supination), brachialis (pure flexion), and coracobrachialis. The posterior compartment (radial nerve, C5–T1) contains triceps brachii (extension at elbow). The musculocutaneous nerve pierces coracobrachialis and terminates as the lateral cutaneous nerve of the forearm. Injury causes weakness of elbow flexion and loss of sensation over the lateral forearm.
Key Shoulder Injuries
| Injury | Mechanism | Key Finding |
|---|---|---|
| Anterior dislocation (95%) | Abduction + external rotation | Axillary nerve injury → deltoid paralysis, loss of "regimental badge" sensation |
| Posterior dislocation (rare) | Seizure, electrocution, lightning | "Lightbulb sign" on AP X-ray; internally rotated, adducted arm |
| Acromioclavicular separation | Fall on adducted shoulder | Step-off deformity at AC joint; classified Types I–VI |
| Clavicle fracture | Fall on outstretched hand (FOOSH) | Middle third most common (80%); medial fragment elevated by SCM |
| Proximal humerus fracture | FOOSH in elderly/osteoporotic | Neer classification; axillary nerve at risk in surgical neck fractures |
05 Forearm, Wrist & Hand
The forearm contains 20 muscles organized into anterior (flexor) and posterior (extensor) compartments separated by the interosseous membrane. The anterior compartment is innervated primarily by the median nerve (superficial muscles) and anterior interosseous nerve (deep muscles), with the exception of flexor carpi ulnaris and medial half of flexor digitorum profundus (ulnar nerve). The posterior compartment is supplied entirely by the posterior interosseous nerve (branch of radial nerve).
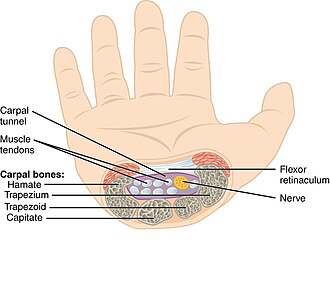
Carpal Tunnel Contents
The carpal tunnel is bounded by the carpal bones (floor and sides) and the flexor retinaculum (transverse carpal ligament, roof). It transmits 10 structures: the median nerve (most superficial and vulnerable), 4 tendons of flexor digitorum superficialis, 4 tendons of flexor digitorum profundus, and the tendon of flexor pollicis longus. The flexor carpi radialis travels in its own fibro-osseous tunnel within the retinaculum and is not technically "inside" the carpal tunnel. The ulnar nerve and ulnar artery pass through Guyon canal (superficial to the retinaculum), not the carpal tunnel.
Hand Intrinsic Muscles
| Muscle Group | Innervation | Action |
|---|---|---|
| Thenar muscles (opponens pollicis, abductor pollicis brevis, flexor pollicis brevis superficial head) | Recurrent branch of median nerve | Thumb opposition, abduction, flexion |
| Lumbricals 1–2 | Median nerve | MCP flexion + IP extension |
| Lumbricals 3–4 | Ulnar nerve (deep branch) | MCP flexion + IP extension |
| Interossei (dorsal: abduct; palmar: adduct) | Ulnar nerve (deep branch) | DAB = dorsal ABduct; PAD = palmar ADduct |
| Hypothenar muscles | Ulnar nerve (deep branch) | Little finger opposition, abduction, flexion |
| Adductor pollicis | Ulnar nerve (deep branch) | Thumb adduction; Froment sign tests this |
Patient pinches paper between thumb and index finger. With ulnar nerve palsy, the adductor pollicis is weak, so the patient compensates by flexing the thumb IP joint (using flexor pollicis longus, median nerve). A positive Froment sign = IP flexion during pinch = ulnar neuropathy.
Anatomical Snuffbox
Bordered by the tendons of extensor pollicis longus (ulnar border) and extensor pollicis brevis / abductor pollicis longus (radial border). The floor contains the scaphoid bone and the radial artery (palpable here). Tenderness in the snuffbox after FOOSH mandates scaphoid fracture workup, even with negative initial X-rays (15% false-negative rate). Scaphoid fractures risk avascular necrosis of the proximal pole because blood supply enters distally.
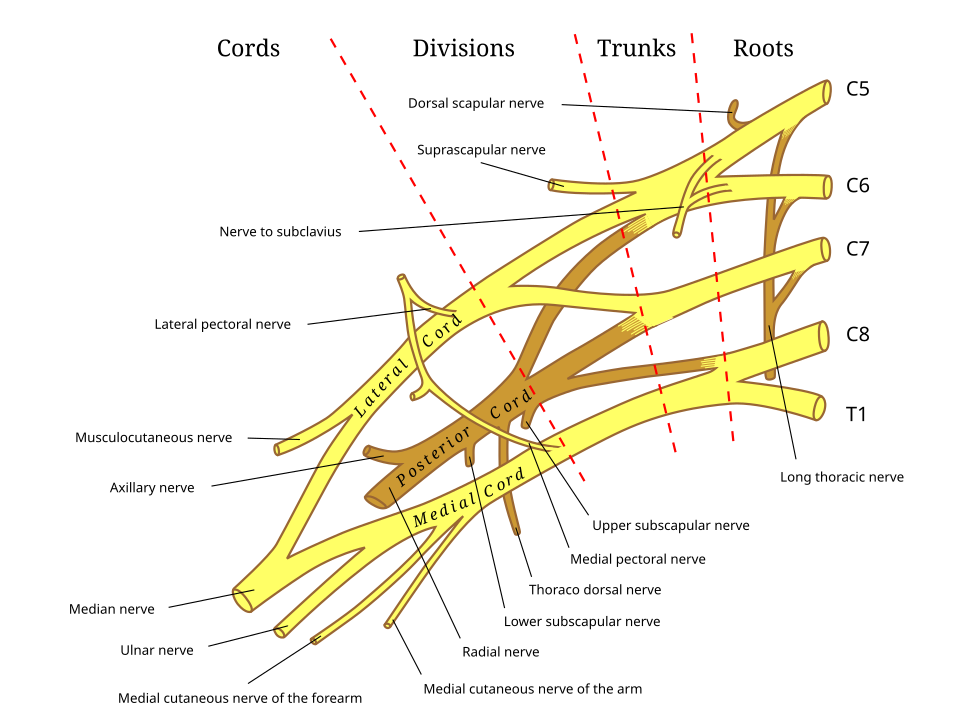
06 Brachial Plexus & Upper Limb Nerves
The brachial plexus (C5–T1) innervates the entire upper limb. It forms from ventral rami that merge into trunks, divisions, cords, and branches: "Robert Taylor Drinks Cold Beer" (Roots, Trunks, Divisions, Cords, Branches). The plexus passes between the anterior and middle scalene muscles, then beneath the clavicle and into the axilla.
Brachial Plexus Organization
| Level | Components | Key Branches |
|---|---|---|
| Roots (C5–T1) | Ventral rami | Dorsal scapular n. (C5), long thoracic n. (C5–C7) |
| Trunks | Upper (C5–C6), Middle (C7), Lower (C8–T1) | Suprascapular n. (upper trunk), nerve to subclavius |
| Divisions | Anterior & posterior from each trunk | No named branches |
| Cords | Lateral (C5–C7), Posterior (C5–T1), Medial (C8–T1) | Lateral pectoral, thoracodorsal, medial pectoral, subscapular nn. |
| Terminal branches | 5 major nerves | Musculocutaneous, median, ulnar, radial, axillary |
Classic Brachial Plexus Injuries
| Injury | Roots | Mechanism | Presentation |
|---|---|---|---|
| Erb-Duchenne palsy | C5–C6 (upper trunk) | Birth injury (shoulder dystocia), motorcycle fall | "Waiter's tip": arm adducted, medially rotated, forearm pronated, wrist flexed |
| Klumpke palsy | C8–T1 (lower trunk) | Upward arm traction, birth injury (breech) | "Claw hand": loss of intrinsic hand muscles; may have Horner syndrome (T1 sympathetics) |
| Winged scapula | Long thoracic n. (C5–C7) | Axillary node dissection, stab wounds | Medial winging; serratus anterior paralysis; cannot protract/push forward |
| Wrist drop | Radial nerve (C5–T1) | "Saturday night palsy" (mid-humerus compression) | Loss of wrist/finger extension; sensory loss dorsal hand first web space |
Upper Limb Dermatomes (Key Landmarks)
C5 = lateral arm (regimental badge area); C6 = lateral forearm, thumb, and index finger; C7 = middle finger; C8 = ring and little finger, medial forearm; T1 = medial arm; T2 = medial arm and axilla. The C6 dermatome is tested with the brachioradialis reflex, C7 with the triceps reflex, and C5–C6 with the biceps reflex.
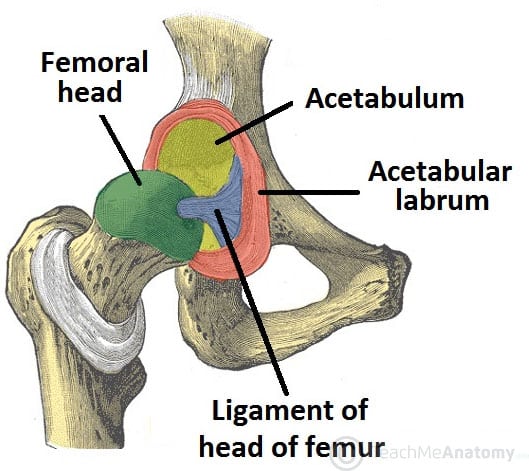
07 Hip & Thigh
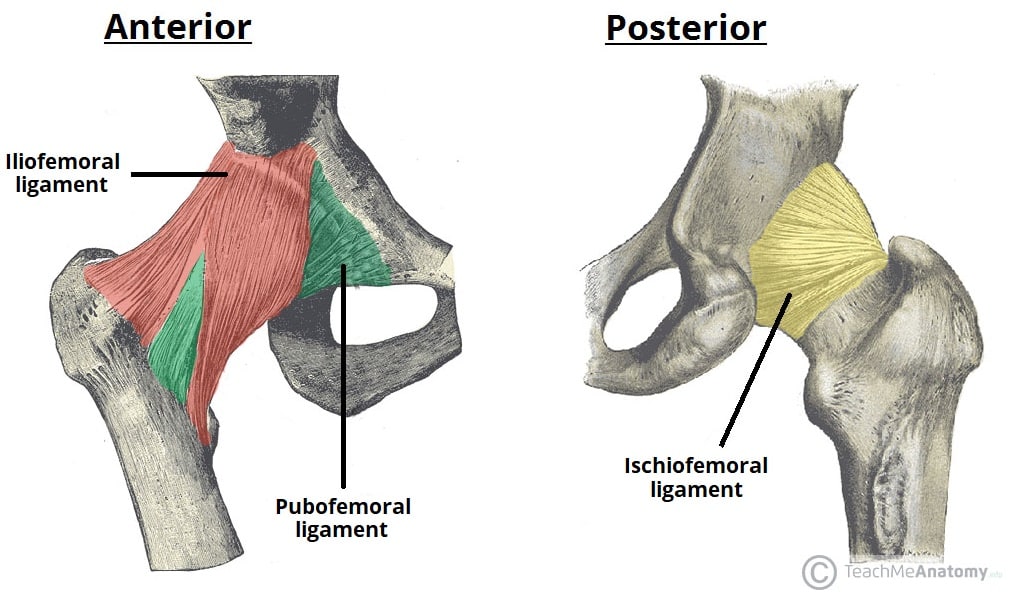
The hip joint is a ball-and-socket synovial joint with much greater inherent stability than the shoulder, owing to the deep acetabulum (deepened further by the labrum), strong capsular ligaments (iliofemoral, pubofemoral, ischiofemoral), and powerful surrounding musculature. The iliofemoral ligament (Y-ligament of Bigelow) is the strongest ligament in the body and resists hyperextension.
Thigh Compartments
| Compartment | Key Muscles | Innervation | Action |
|---|---|---|---|
| Anterior | Quadriceps (rectus femoris, vastus lateralis/medialis/intermedius), sartorius, iliopsoas | Femoral nerve (L2–L4) | Hip flexion, knee extension |
| Medial | Adductor longus, brevis, magnus; gracilis; obturator externus | Obturator nerve (L2–L4) | Hip adduction |
| Posterior | Hamstrings: biceps femoris (long & short heads), semimembranosus, semitendinosus | Sciatic nerve (tibial division; short head of biceps = common fibular) | Hip extension, knee flexion |
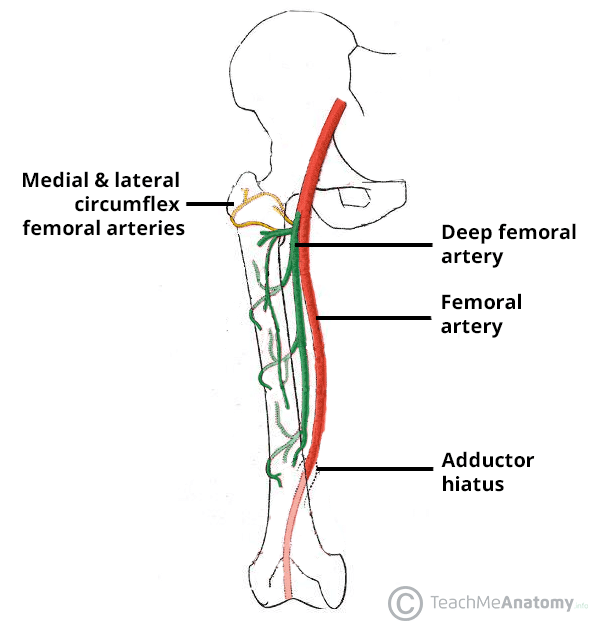
Blood Supply to the Femoral Head
The medial circumflex femoral artery (branch of profunda femoris, or directly from femoral artery) is the primary blood supply to the femoral head via retinacular arteries. The lateral circumflex femoral artery and the artery of the ligamentum teres (from obturator artery) provide minor contributions. This vascular anatomy explains why femoral neck fractures (intracapsular) disrupt the retinacular arteries and carry a high risk of avascular necrosis (AVN), while intertrochanteric fractures (extracapsular) have an intact blood supply and lower AVN risk.
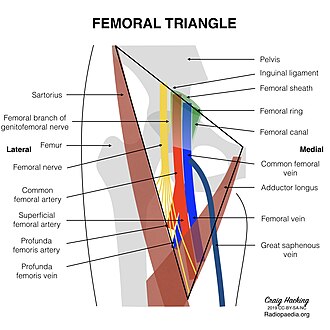
Femoral Triangle
Bounded by the inguinal ligament (superior), sartorius (lateral), and adductor longus (medial). The floor is formed by iliopsoas (laterally) and pectineus (medially). Contents from lateral to medial: N-A-V-E-L — femoral Nerve, femoral Artery, femoral Vein, Empty space (femoral canal), and Lymphatics. The femoral pulse is palpated at the midinguinal point (midway between ASIS and pubic symphysis). The femoral canal is the site of femoral hernias (more common in women; high risk of strangulation due to rigid boundaries).
08 Knee, Leg & Foot
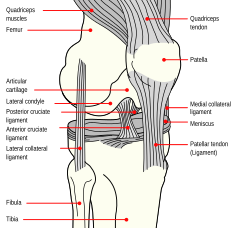
The knee is a modified hinge joint (allows flexion, extension, and slight rotation) and the largest synovial joint. Stability depends on four major ligaments: ACL (prevents anterior tibial translation; most commonly injured knee ligament), PCL (prevents posterior tibial translation; strongest knee ligament), MCL (resists valgus stress), and LCL (resists varus stress). The medial and lateral menisci are C-shaped fibrocartilage shock absorbers; the medial meniscus is more commonly torn because it is firmly attached to the MCL and joint capsule.
Classic Knee Injuries
| Injury | Mechanism | Physical Exam | Association |
|---|---|---|---|
| ACL tear | Non-contact pivot/deceleration; valgus + external rotation | Positive anterior drawer, Lachman test (most sensitive) | "Unhappy triad": ACL + MCL + medial meniscus tear |
| PCL tear | Dashboard injury (posterior force on flexed knee) | Positive posterior drawer, posterior sag sign | Associated with popliteal artery injury in dislocations |
| MCL tear | Valgus stress (blow to lateral knee) | Medial joint line tenderness, valgus laxity | Often combined with ACL and medial meniscus |
| Meniscal tear | Twisting on planted foot | Joint line tenderness, McMurray test (click with rotation) | Bucket-handle tear can cause locked knee |
Leg Compartments
| Compartment | Key Muscles | Nerve | Action |
|---|---|---|---|
| Anterior | Tibialis anterior, extensor hallucis longus, extensor digitorum longus | Deep fibular (peroneal) | Dorsiflexion, toe extension, inversion |
| Lateral | Fibularis (peroneus) longus & brevis | Superficial fibular | Eversion, plantarflexion |
| Posterior (superficial) | Gastrocnemius, soleus, plantaris | Tibial | Plantarflexion |
| Posterior (deep) | Tibialis posterior, flexor digitorum longus, flexor hallucis longus, popliteus | Tibial | Plantarflexion, inversion, toe flexion |
Foot Arches & Plantar Fascia
The medial longitudinal arch (calcaneus, talus, navicular, cuneiforms, metatarsals 1–3) is the primary weight-bearing arch, maintained by the spring ligament (plantar calcaneonavicular) and tibialis posterior tendon. The plantar aponeurosis spans from the calcaneal tuberosity to the proximal phalanges and maintains all arches. Plantar fasciitis causes heel pain, worst with first morning steps, at the medial calcaneal tubercle insertion.
Ankle Ligaments & Injuries
| Ligament | Components | Injury Mechanism | Clinical Note |
|---|---|---|---|
| Lateral ligament complex | Anterior talofibular (ATFL), calcaneofibular (CFL), posterior talofibular (PTFL) | Inversion (most common ankle injury) | ATFL is weakest and most commonly torn; anterior drawer test positive |
| Deltoid ligament (medial) | Superficial and deep components | Eversion | Strongest ankle ligament; injury suggests fracture (Maisonneuve fracture: proximal fibula fracture + deltoid disruption) |
| Syndesmosis (high ankle) | Anterior/posterior tibiofibular ligaments, interosseous membrane | External rotation with dorsiflexion | Squeeze test positive; longer recovery than lateral sprains |
Popliteal Fossa
Diamond-shaped space behind the knee. Boundaries: superolateral = biceps femoris; superomedial = semimembranosus and semitendinosus; inferolateral and inferomedial = lateral and medial heads of gastrocnemius. Contents (superficial to deep): tibial nerve (most superficial and lateral), popliteal vein, popliteal artery (deepest, against the femur — most vulnerable in posterior knee dislocation). The common fibular (peroneal) nerve travels along the medial border of the biceps femoris tendon, then winds around the fibular neck. A Baker cyst (popliteal cyst) is a distension of the semimembranosus bursa; it communicates with the knee joint and is associated with intra-articular pathology (meniscal tears, osteoarthritis).
09 Lumbosacral Plexus & Lower Limb Nerves
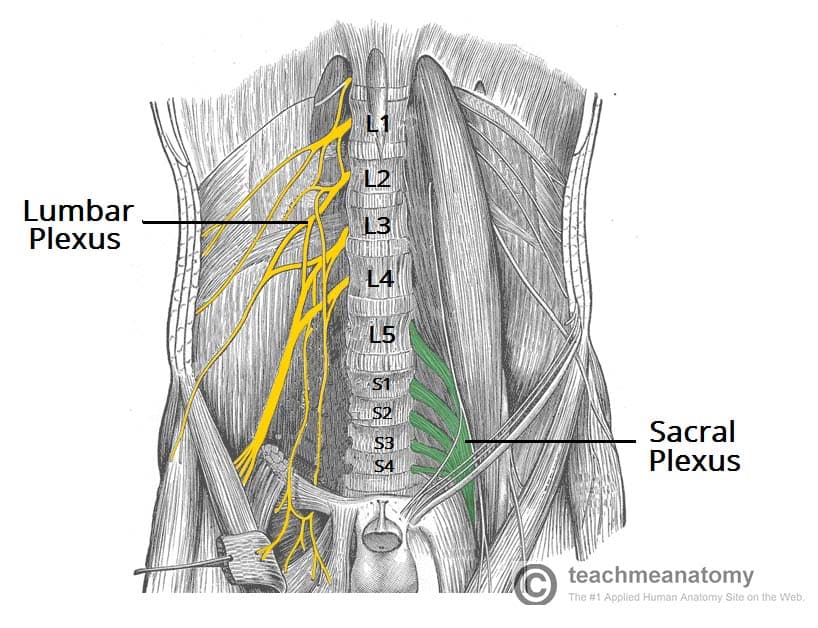
The lumbar plexus (L1–L4) forms within the psoas major muscle. The sacral plexus (L4–S3) forms on the piriformis muscle in the pelvis. Together they supply the entire lower limb.
Major Nerves of the Lower Limb
| Nerve | Roots | Motor | Sensory | Injury |
|---|---|---|---|---|
| Femoral | L2–L4 | Quadriceps (knee extension), iliopsoas (hip flexion) | Anterior thigh, medial leg (saphenous n.) | Loss of knee jerk, difficulty climbing stairs |
| Obturator | L2–L4 | Adductors of thigh | Medial thigh | Weakness of adduction; can be injured in pelvic surgery |
| Sciatic | L4–S3 | Hamstrings, all muscles below knee (via tibial & common fibular) | Posterior thigh, leg, foot | Posterior hip dislocation, IM injection (avoid!) |
| Common fibular (peroneal) | L4–S2 | Anterior & lateral compartments | Lateral leg, dorsum of foot | Foot drop; compressed at fibular neck (leg crossing, casts) |
| Tibial | L4–S3 | Posterior compartment (plantarflexion, toe flexion) | Sole of foot (via medial & lateral plantar nn.) | Loss of plantarflexion; tarsal tunnel syndrome |
Common fibular nerve injury (at fibular neck) is the most common cause of foot drop. However, also consider: L5 radiculopathy (will have hip abduction weakness and intact foot eversion, unlike fibular nerve palsy), sciatic neuropathy, or central lesion (UMN signs). Deep fibular nerve = dorsiflexion loss; superficial fibular = eversion loss. Fibular nerve palsy loses both.
Lower Limb Dermatomes (Key Landmarks)
L1 = inguinal region; L2 = anterior thigh; L3 = medial knee; L4 = medial leg and medial malleolus (patellar reflex); L5 = lateral leg, dorsum of foot, great toe; S1 = lateral foot, little toe, sole (Achilles reflex); S2–S4 = perineum and genitalia ("saddle area"). The S2–S4 dermatomes are critical — cauda equina syndrome (saddle anesthesia, bowel/bladder dysfunction, bilateral leg weakness) is a surgical emergency.
10 Vertebral Column & Spinal Cord
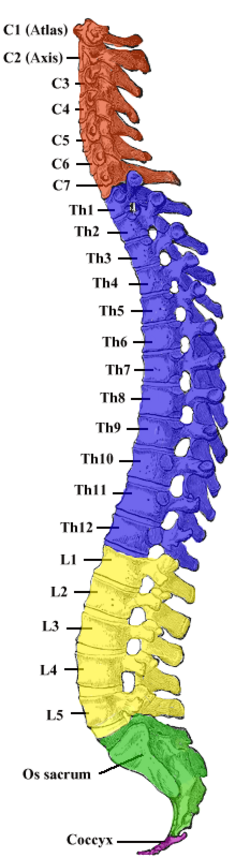
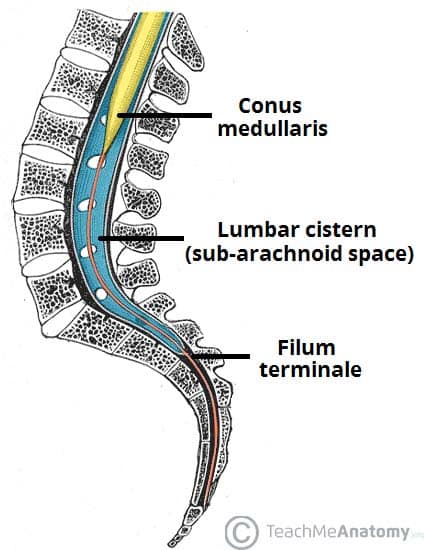
The vertebral column comprises 33 vertebrae: 7 cervical, 12 thoracic, 5 lumbar, 5 sacral (fused), and 4 coccygeal (fused). It protects the spinal cord, supports the body, and allows movement. The spinal cord extends from the foramen magnum to the conus medullaris at approximately L1–L2 in adults (L3 in neonates), below which the cauda equina (nerve roots L2–S5) descends within the lumbar cistern.
Vertebral Characteristics
| Region | Distinguishing Feature | Clinical Note |
|---|---|---|
| Cervical (C1–C7) | Bifid spinous processes (C2–C6), transverse foramina (vertebral arteries C1–C6), small bodies | C1 (atlas) = no body/spinous process; C2 (axis) = dens (odontoid); C7 = vertebra prominens |
| Thoracic (T1–T12) | Costal facets for rib articulation, heart-shaped bodies, long inferiorly angled spinous processes | Most common site of compression fractures in osteoporosis (T12–L1) |
| Lumbar (L1–L5) | Largest bodies, short thick spinous processes, no rib facets or transverse foramina | Most common disc herniations: L4–L5 (L5 root) and L5–S1 (S1 root) |
Intervertebral Disc Herniation
Disc herniations most commonly occur posterolaterally (where the annulus fibrosus is thinnest and unsupported by the posterior longitudinal ligament). A posterolateral herniation at L4–L5 compresses the L5 nerve root (which exits below the L5 pedicle). A far lateral (foraminal) herniation at L4–L5 compresses the L4 nerve root. Key pattern: posterolateral herniations compress the nerve root numbered one below the disc level.
Spinal Cord Blood Supply
The anterior spinal artery (single, from vertebral arteries) supplies the anterior two-thirds of the cord. Two posterior spinal arteries (from vertebral or PICA) supply the posterior one-third. Segmental radicular arteries reinforce the supply; the artery of Adamkiewicz (great anterior radiculomedullary artery, typically T9–T12, left side in 80%) is the major feeder for the lower cord. Damage during aortic surgery can cause anterior spinal artery syndrome: bilateral loss of motor function and pain/temperature sensation below the lesion, with preserved proprioception and vibration (posterior columns spared).
Spinal Nerve Root Compression Patterns
| Root | Disc Level (Posterolateral) | Motor Weakness | Reflex Loss | Sensory Deficit |
|---|---|---|---|---|
| C5 | C4–C5 | Deltoid, biceps (shoulder abduction weakness) | Biceps reflex | Lateral arm |
| C6 | C5–C6 | Biceps, wrist extensors | Brachioradialis reflex | Lateral forearm, thumb, index finger |
| C7 | C6–C7 | Triceps, wrist flexors, finger extensors | Triceps reflex | Middle finger |
| C8 | C7–T1 | Finger flexors, hand intrinsics | None specific | Ring and little finger, medial forearm |
| L4 | L3–L4 | Quadriceps (knee extension), tibialis anterior | Patellar reflex | Medial leg |
| L5 | L4–L5 | EHL, tibialis anterior, gluteus medius (foot drop, hip abduction weakness) | None specific (medial hamstring sometimes) | Lateral leg, dorsum of foot, great toe |
| S1 | L5–S1 | Gastrocnemius/soleus (plantarflexion), peroneals | Achilles reflex | Lateral foot, sole |
11 Thoracic Wall & Diaphragm
The thoracic cage (sternum, 12 pairs of ribs, thoracic vertebrae) protects the heart, lungs, and great vessels while allowing respiratory excursion. The intercostal neurovascular bundle (vein, artery, nerve — VAN from superior to inferior) runs in the costal groove along the inferior border of each rib. This is why thoracentesis and chest tubes are inserted just above the rib (superior border of the rib below the target interspace) to avoid the neurovascular bundle.
Rib Classification
| Type | Ribs | Attachment |
|---|---|---|
| True ribs (vertebrosternal) | 1–7 | Articulate directly with sternum via costal cartilage |
| False ribs (vertebrochondral) | 8–10 | Attach to sternum indirectly through rib 7 costal cartilage |
| Floating ribs (vertebral) | 11–12 | No anterior attachment; free-ending |
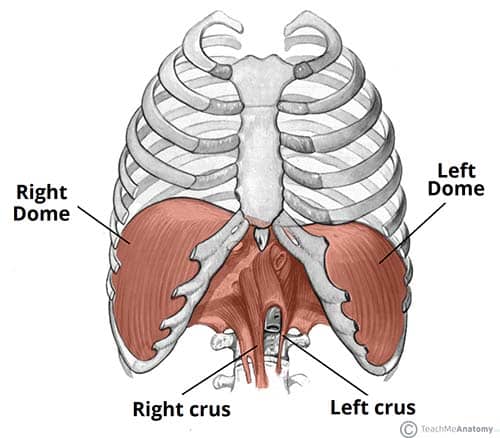
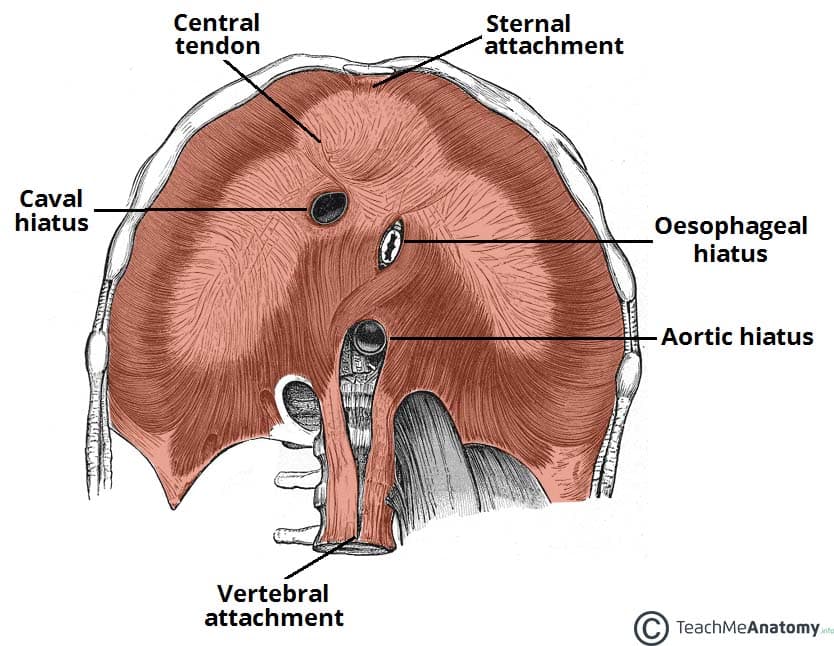
The Diaphragm
The diaphragm is the primary muscle of inspiration, innervated by the phrenic nerve (C3–C5) — "C3, 4, 5 keeps the diaphragm alive." It has three major openings:
| Opening | Level | Contents | Mnemonic |
|---|---|---|---|
| Caval opening | T8 | IVC, right phrenic nerve | "I ate (8) ten (10) eggs (esophagus) at (aorta) twelve (12)" |
| Esophageal hiatus | T10 | Esophagus, vagus nerves (anterior & posterior trunks) | |
| Aortic hiatus | T12 | Aorta, thoracic duct, azygos vein |
Intercostal Muscles & Respiration
External intercostals elevate the ribs during inspiration (hands in pockets orientation). Internal intercostals (interosseous part) depress the ribs during forced expiration. Innermost intercostals are deep to the neurovascular bundle and function similarly to internal intercostals. Accessory muscles of inspiration include the scalenes, sternocleidomastoid, and pectoralis minor; accessory muscles of expiration include the abdominal wall muscles (rectus abdominis, obliques, transversus abdominis).
Breast Anatomy & Lymphatic Drainage
The breast lies on the pectoral fascia overlying pectoralis major, with the axillary tail (of Spence) extending toward the axilla. Blood supply: internal thoracic (mammary) artery, lateral thoracic artery, and intercostal arteries. Lymphatic drainage: approximately 75% of lymph drains to the axillary lymph nodes (5 groups: pectoral/anterior, subscapular/posterior, lateral/humeral, central, apical). The medial breast drains to the internal mammary (parasternal) nodes. During breast cancer surgery, the long thoracic nerve (winged scapula if damaged) and thoracodorsal nerve (latissimus weakness) must be preserved during axillary dissection. The intercostobrachial nerve (T2 lateral cutaneous branch) is commonly divided, causing numbness of the medial upper arm.
12 Abdominal Wall & Inguinal Region
The anterolateral abdominal wall consists of four muscle layers: external oblique (fibers inferiorly and medially, "hands in pockets"), internal oblique (fibers superiorly and medially), transversus abdominis (fibers transversely), and rectus abdominis (vertical, within the rectus sheath). Below the arcuate line (roughly midway between umbilicus and pubis), all aponeuroses pass anterior to the rectus, leaving only transversalis fascia posteriorly — a weak point predisposing to herniation.
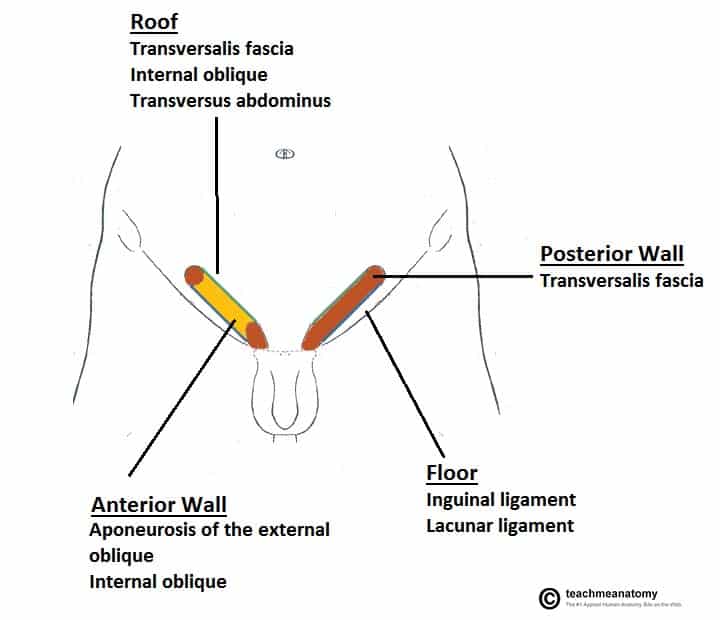
Inguinal Canal
The inguinal canal is an oblique passage through the abdominal wall, approximately 4 cm long, transmitting the spermatic cord in males and the round ligament of the uterus in females. Key boundaries:
| Wall | Structure |
|---|---|
| Anterior wall | External oblique aponeurosis (entire length); internal oblique (lateral third) |
| Posterior wall (floor) | Transversalis fascia (entire length); conjoint tendon (medial third) |
| Roof | Arching fibers of internal oblique and transversus abdominis |
| Inferior wall | Inguinal ligament (Poupart ligament, rolled-under edge of external oblique aponeurosis) |
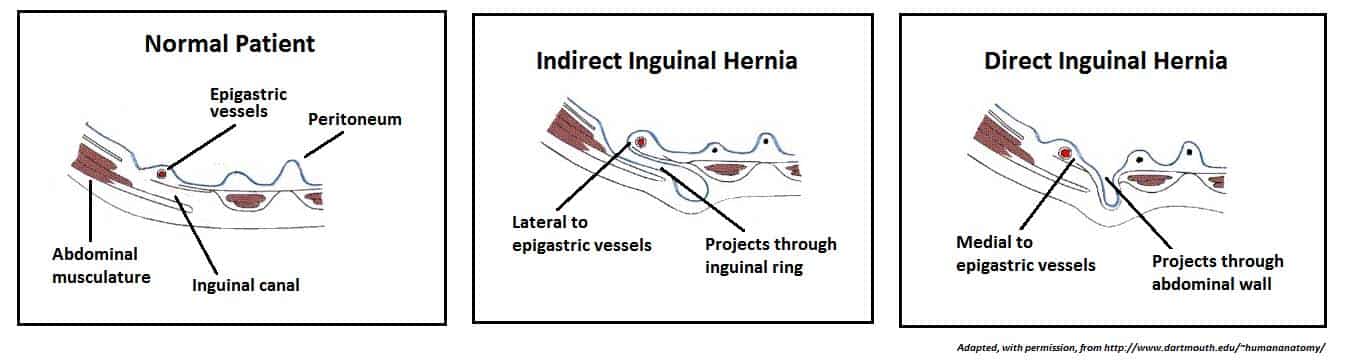
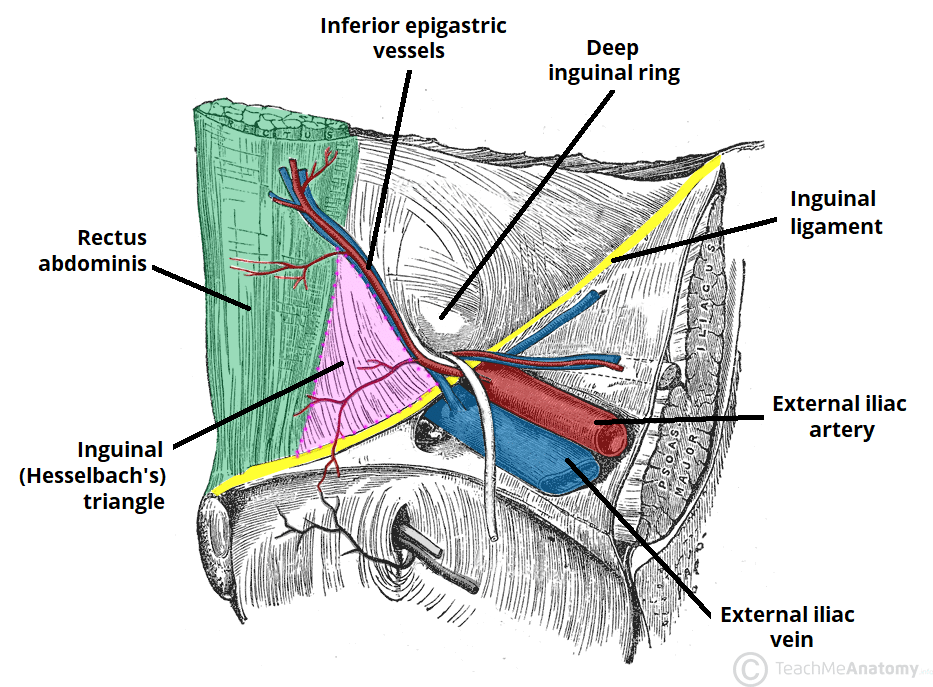
Inguinal Hernias
| Feature | Indirect Inguinal | Direct Inguinal | Femoral |
|---|---|---|---|
| Route | Through deep ring, within spermatic cord, may descend to scrotum | Through Hesselbach triangle, medial to inferior epigastric vessels | Through femoral canal, below and lateral to pubic tubercle |
| Demographics | Most common hernia in both sexes; infants & young males | Older males, bilateral common | More common in women; highest strangulation risk |
| Covered by | Internal spermatic fascia (from transversalis fascia) | Not covered by internal spermatic fascia | Femoral sheath |
| Relationship to epigastric vessels | Lateral | Medial | Below inguinal ligament |
| Congenital vs acquired | Often congenital (patent processus vaginalis) | Acquired (weakness in transversalis fascia) | Acquired |
Layers of the Spermatic Cord (from Abdominal Wall Layers)
| Abdominal Wall Layer | Spermatic Cord Covering |
|---|---|
| External oblique aponeurosis | External spermatic fascia |
| Internal oblique muscle | Cremasteric muscle and fascia |
| Transversalis fascia | Internal spermatic fascia |
Note: the transversus abdominis does not contribute a covering. Understanding these layers is essential for interpreting hernia anatomy and for open inguinal hernia repair (Bassini, Shouldice, or Lichtenstein mesh techniques).
Abdominal Incisions & Surgical Considerations
| Incision | Location | Use | Nerve at Risk |
|---|---|---|---|
| Midline (linea alba) | Vertical through midline | Exploratory laparotomy | Minimal nerve risk (avascular plane) |
| Paramedian | Vertical, lateral to midline through rectus sheath | Access to lateral structures | Segmental intercostal nerves |
| McBurney (gridiron) | Oblique at McBurney point | Appendectomy | Iliohypogastric, ilioinguinal |
| Kocher (subcostal) | Right subcostal, 2 cm below costal margin | Cholecystectomy (open) | T7–T8 intercostal nerves |
| Pfannenstiel | Transverse suprapubic | Cesarean section, pelvic surgery | Iliohypogastric, ilioinguinal |
13 Heart & Coronary Arteries
The heart is a four-chambered muscular pump (~250–350 g) located in the middle mediastinum, resting on the diaphragm. Two-thirds of the heart mass lies to the left of the midline. The heart is enclosed within the pericardium (fibrous pericardium and serous pericardium with parietal and visceral layers). The pericardial space normally contains 15–50 mL of serous fluid; rapid accumulation of >150–200 mL can cause cardiac tamponade (Beck triad: hypotension, distended neck veins, muffled heart sounds).
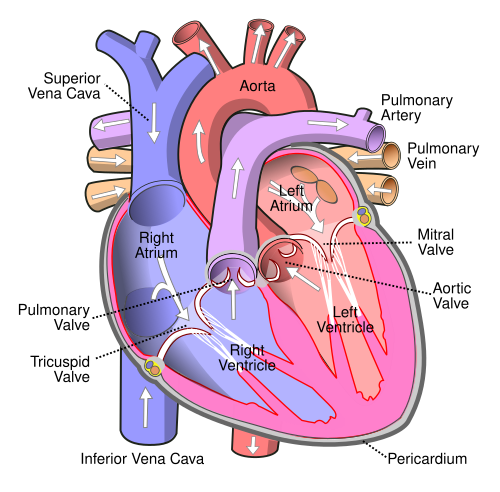
Cardiac Chambers & Valves
The right atrium receives venous blood via the SVC, IVC, and coronary sinus. The right ventricle is the most anterior chamber (most vulnerable in penetrating chest trauma) and pumps blood through the pulmonic valve into the pulmonary trunk. The left atrium is the most posterior chamber (dilated LA can compress the esophagus → dysphagia, or recurrent laryngeal nerve → hoarseness). The left ventricle is the thickest chamber (~12 mm vs RV ~4 mm) and pumps oxygenated blood through the aortic valve.
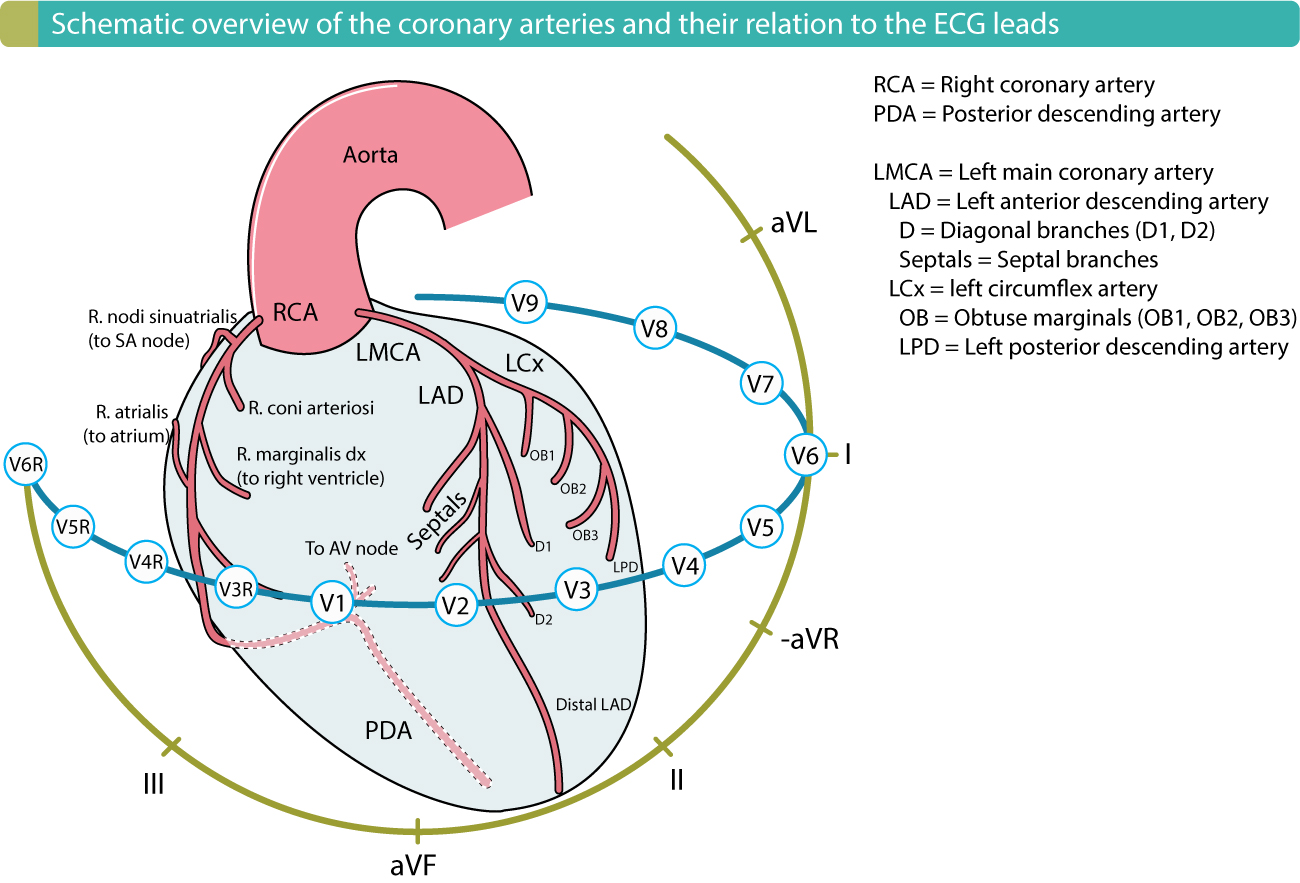
Coronary Artery Supply
| Artery | Territory | Infarct Pattern |
|---|---|---|
| LAD (left anterior descending) | Anterior wall, anterior septum, apex | Anterior STEMI (V1–V4) |
| LCx (left circumflex) | Lateral & posterolateral LV wall | Lateral STEMI (I, aVL, V5–V6) |
| RCA (right coronary artery) | Inferior wall, RV, posterior septum, SA node (60%), AV node (90%) | Inferior STEMI (II, III, aVF); may cause bradycardia |
| PDA (posterior descending) | Inferior wall, posterior septum | From RCA in 85% (right-dominant) |
Right-dominant (~85%): PDA from RCA. Left-dominant (~8%): PDA from LCx. Co-dominant (~7%): both contribute. The dominance determines which artery supplies the AV node. Inferior MI from RCA occlusion can produce heart block (AV nodal ischemia) and right ventricular infarction (requires volume loading, avoid nitroglycerin).
Cardiac Conduction System
SA node (right atrium, junction with SVC; intrinsic rate 60–100 bpm) → AV node (base of interatrial septum; 40–60 bpm; physiologic delay allows atrial contraction before ventricular systole) → bundle of His → right and left bundle branches → Purkinje fibers (15–40 bpm). The SA node is supplied by the RCA in 60% and LCx in 40%. The AV node is supplied by the RCA in 90% (via the AV nodal artery from the PDA).
Pericardial Sinuses
The transverse pericardial sinus lies posterior to the ascending aorta and pulmonary trunk and anterior to the SVC. It is used during cardiac surgery to pass a clamp or ligature around the great arteries. The oblique pericardial sinus is a blind cul-de-sac posterior to the left atrium, bounded by reflections of the serous pericardium around the pulmonary veins and IVC. Pericardial effusion collects here and can compress the LA, reducing venous return.
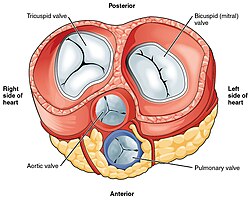
Valve Auscultation Landmarks
| Valve | Anatomic Position | Auscultation Area |
|---|---|---|
| Aortic | Behind sternum at level of 3rd intercostal space | Right upper sternal border (2nd ICS) |
| Pulmonic | Behind sternum at level of 3rd costal cartilage | Left upper sternal border (2nd ICS) |
| Tricuspid | Behind sternum at level of 4th–5th costal cartilage | Left lower sternal border (4th ICS) |
| Mitral | Behind sternum at level of 4th costal cartilage | Apex (5th ICS, midclavicular line) |
14 Great Vessels & Aortic Branches
The aorta is the largest artery in the body, originating from the left ventricle and distributing oxygenated blood to every tissue. It is divided into the ascending aorta, aortic arch, descending thoracic aorta, and abdominal aorta.
Branches of the Aortic Arch
From right to left (in the typical pattern, ~70%): brachiocephalic trunk (divides into right subclavian and right common carotid), left common carotid artery, and left subclavian artery. Variant: a "bovine arch" (left common carotid sharing origin with brachiocephalic trunk) occurs in ~15% of the population.
Abdominal Aortic Branches
| Branch | Level | Supply |
|---|---|---|
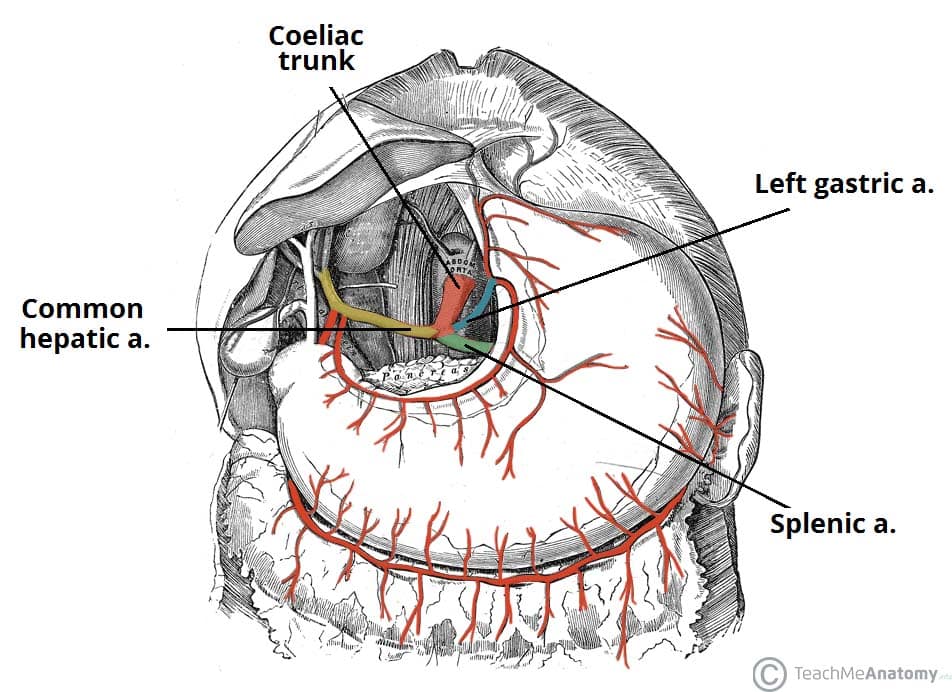
| Celiac trunk | T12 | Left gastric, splenic, common hepatic → foregut (esophagus to 2nd part of duodenum) |
| Superior mesenteric artery (SMA) | L1 | Midgut (2nd part of duodenum to splenic flexure of colon) |
| Renal arteries | L1–L2 | Kidneys (right crosses behind IVC) |
| Gonadal arteries | L2 | Ovaries or testes |
| Inferior mesenteric artery (IMA) | L3 | Hindgut (splenic flexure to upper rectum) |
| Common iliac arteries | L4 (bifurcation) | Pelvis and lower limbs |
Venous Drainage
The IVC is formed at L5 by the union of the common iliac veins. It receives the renal veins (left renal vein crosses anterior to the aorta and posterior to the SMA — "nutcracker" position), hepatic veins, and gonadal veins. The left gonadal vein drains into the left renal vein (not directly into IVC); left-sided varicocele can indicate left renal vein compression or renal cell carcinoma with tumor thrombus.
Lymphatic Drainage Patterns
| Region | Lymph Node Group | Clinical Significance |
|---|---|---|
| Upper limb, lateral thorax, breast (lateral quadrants) | Axillary lymph nodes | Breast cancer sentinel node biopsy; lymphedema post-dissection |
| Lower limb, perineum, external genitalia, lower abdominal wall (below umbilicus) | Superficial inguinal nodes | Palpable in many infections; drain to deep inguinal → external iliac |
| Testes, ovaries | Para-aortic (lumbar) nodes | NOT inguinal (because they developed retroperitoneally) |
| GI tract (celiac, SMA, IMA territories) | Mesenteric & celiac nodes | Drain via cisterna chyli to thoracic duct |
| Left head/neck, left upper limb, left thorax, entire body below diaphragm | Thoracic duct → left venous angle | Right lymphatic duct drains only right head/neck, right arm, right thorax |
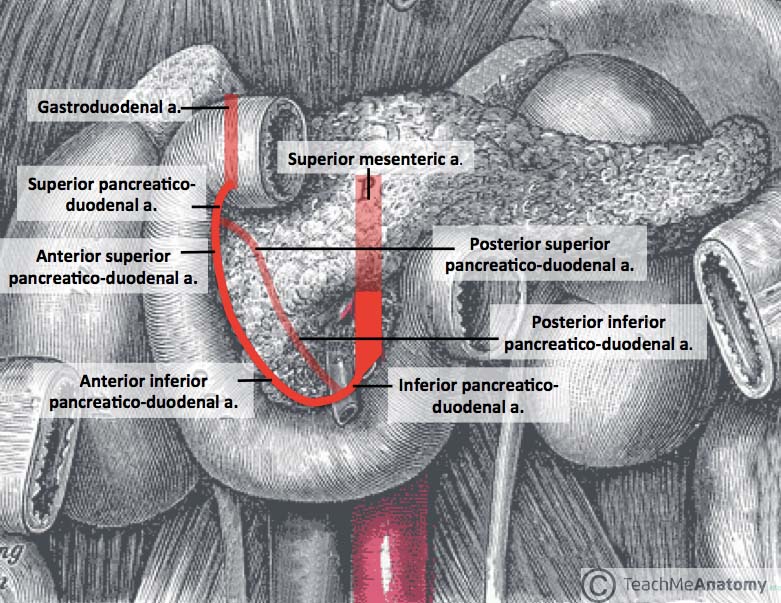
Collateral Circulation
The abdominal aortic branches form important collateral pathways: celiac ↔ SMA via the pancreaticoduodenal arcades (superior from celiac/gastroduodenal, inferior from SMA). SMA ↔ IMA via the marginal artery of Drummond (along the colon) and the arc of Riolan (near the mesenteric root). IMA ↔ internal iliac via superior rectal ↔ middle/inferior rectal anastomoses. These collaterals can maintain viability during gradual occlusion (e.g., atherosclerosis) but may be insufficient during acute occlusion (e.g., embolism → acute mesenteric ischemia).
15 Fetal Circulation & Congenital Variants
Fetal circulation has three shunts that bypass the non-functional lungs and liver: the ductus venosus (umbilical vein → IVC, bypasses liver), the foramen ovale (right atrium → left atrium, bypasses lungs), and the ductus arteriosus (pulmonary trunk → aorta, bypasses lungs). At birth, these shunts close as the lungs inflate, pulmonary vascular resistance drops, and systemic vascular resistance rises.
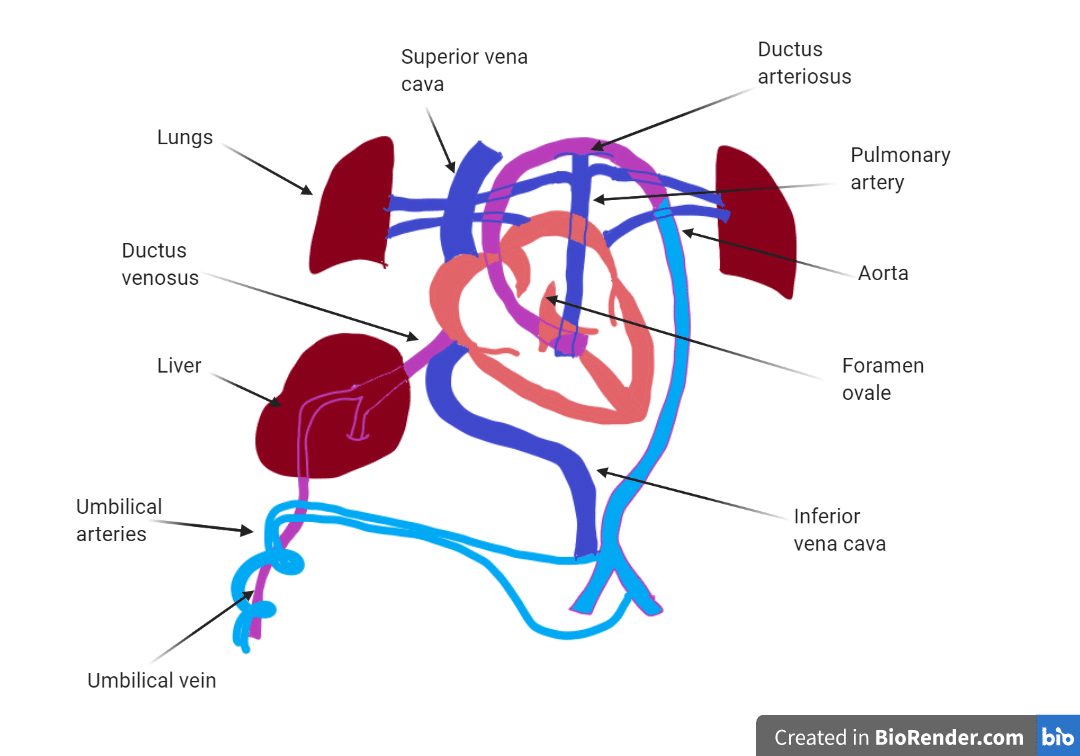
Fetal Shunts & Postnatal Remnants
| Fetal Structure | Function | Postnatal Remnant | Failure to Close |
|---|---|---|---|
| Ductus venosus | Bypasses hepatic sinusoids | Ligamentum venosum | Portal hypertension shunt |
| Foramen ovale | RA → LA shunt | Fossa ovalis | Patent foramen ovale (PFO; 25% of adults) — risk of paradoxical embolism |
| Ductus arteriosus | PA → aorta shunt | Ligamentum arteriosum | Patent ductus arteriosus (PDA) — continuous "machinery" murmur; close with indomethacin |
| Umbilical vein | Carries oxygenated blood from placenta | Ligamentum teres (round ligament of liver) | Recanalization in portal hypertension (caput medusae) |
| Umbilical arteries (2) | Carry deoxygenated blood to placenta | Medial umbilical ligaments | — |
PGE1 (prostaglandin E1) keeps the ductus arteriosus open — used therapeutically in duct-dependent congenital heart disease (e.g., transposition of great arteries, coarctation, critical pulmonary stenosis) to maintain pulmonary or systemic blood flow until surgical repair. Indomethacin or ibuprofen (COX inhibitors) close a PDA by blocking prostaglandin synthesis.
16 Airway, Lungs & Pleura
The conducting airways begin at the nose/mouth and proceed through the pharynx, larynx, trachea, bronchi, and bronchioles. Gas exchange occurs in the respiratory zone (respiratory bronchioles, alveolar ducts, alveolar sacs). The adult lung contains approximately 300 million alveoli with a combined surface area of ~70 m².
Trachea & Bronchial Tree
The trachea is 10–12 cm long, supported by 16–20 C-shaped cartilage rings (open posteriorly where the trachealis muscle abuts the esophagus). It bifurcates at the carina (T4–T5, sternal angle level) into right and left main bronchi. The right main bronchus is wider, shorter, and more vertical than the left — aspirated foreign bodies, endotracheal tubes advanced too far, and aspiration pneumonia most commonly affect the right lung (right lower lobe in upright patients, right upper lobe posterior segment in supine patients).
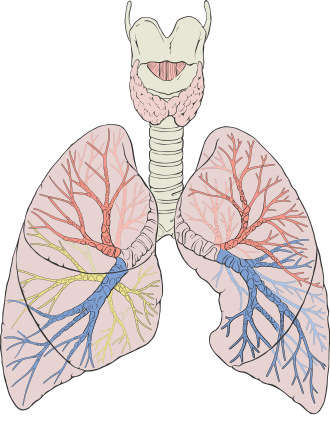
Lung Lobes & Segments
| Lung | Lobes | Fissures | Segments |
|---|---|---|---|
| Right | Upper, Middle, Lower (3 lobes) | Oblique + Horizontal | 10 bronchopulmonary segments |
| Left | Upper (includes lingula), Lower (2 lobes) | Oblique only | 8–9 bronchopulmonary segments |
Pleura & Pleural Recesses
The visceral pleura (innervated by autonomic nerves, no pain sensation) covers the lung surface. The parietal pleura (innervated by intercostal nerves and phrenic nerve, pain-sensitive) lines the chest wall, diaphragm, and mediastinum. The costophrenic recess is the lowest point of the pleural space and is where fluid first accumulates (blunting of the costophrenic angle on chest X-ray with ≥200–300 mL of effusion). The costomediastinal recess is where parietal pleura reflects from the chest wall to the mediastinum.
Pulmonary Vasculature
The pulmonary arteries carry deoxygenated blood from the RV to the lungs. The pulmonary veins (typically 4: two from each lung) carry oxygenated blood to the left atrium. The bronchial arteries (from the thoracic aorta) supply oxygenated blood to the lung parenchyma, bronchi, and visceral pleura. In massive hemoptysis, the bronchial arteries (not pulmonary arteries) are usually the bleeding source and the target for bronchial artery embolization.
Innervation of the Lungs
The pulmonary plexus (anterior and posterior) at the lung root receives sympathetic fibers (from T2–T5 sympathetic trunk ganglia) and parasympathetic fibers (from the vagus nerve). Parasympathetic stimulation (vagus) causes bronchoconstriction, increased mucus secretion, and vasodilation. Sympathetic stimulation causes bronchodilation, decreased secretions, and vasoconstriction. Beta-2 agonists (albuterol) mimic sympathetic bronchodilation; muscarinic antagonists (ipratropium) block parasympathetic bronchoconstriction.
Thoracic Drainage Anatomy
Chest tube insertion for pneumothorax or pleural effusion is performed in the safe triangle: bordered by the lateral edge of pectoralis major (anterior), the anterior border of latissimus dorsi (posterior), the base of the axilla (superior), and the 5th intercostal space (inferior). Entry is typically at the 4th or 5th intercostal space in the mid-axillary line. The needle or tube passes just superior to the rib to avoid the intercostal neurovascular bundle (VAN) running along the inferior border of the rib above.
17 Mediastinum & Thoracic Lymphatics
The mediastinum is the central compartment of the thorax, bounded laterally by the pleural cavities, anteriorly by the sternum, and posteriorly by the vertebral column. It is divided into superior (above sternal angle/T4) and inferior (anterior, middle, posterior) mediastinum.
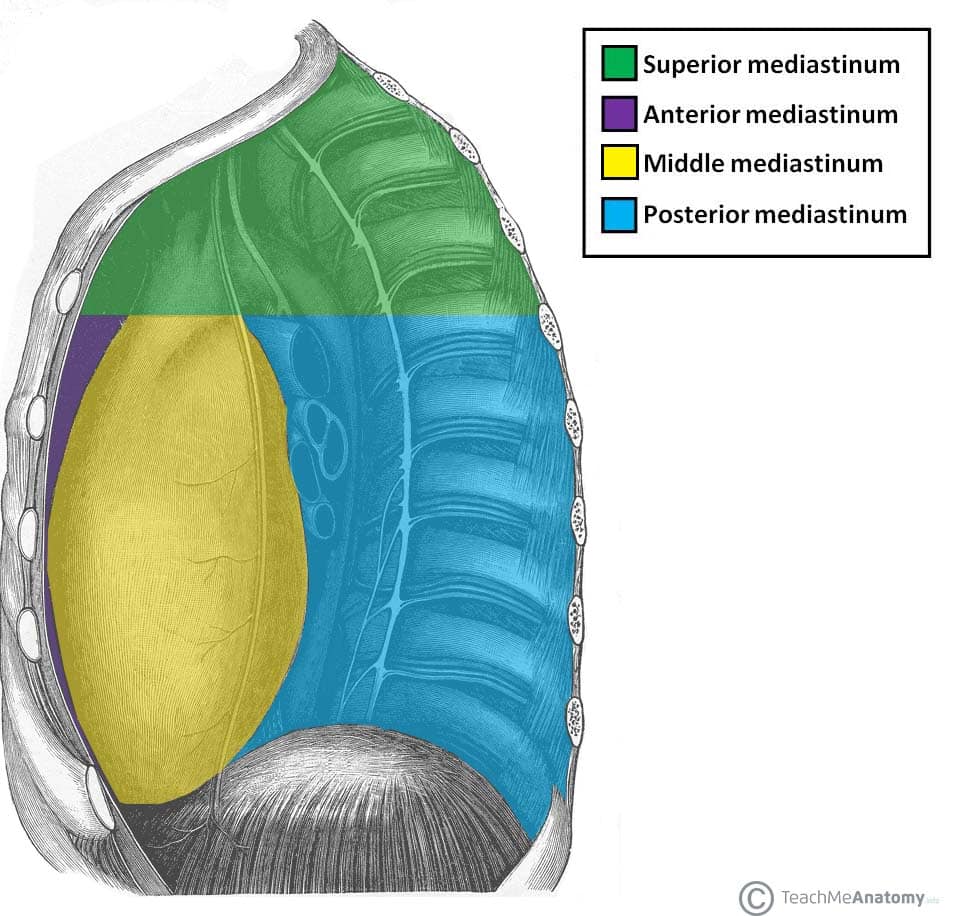
Mediastinal Compartments & Contents
| Compartment | Key Contents | Pathology |
|---|---|---|
| Superior | Aortic arch & branches, SVC, trachea, esophagus, thoracic duct, thymus (superior portion), vagus & phrenic nerves | Thymoma, lymphoma, retrosternal goiter |
| Anterior | Thymus, fat, lymph nodes, internal thoracic vessels | "4 T's": Thymoma, Teratoma/germ cell, Terrible lymphoma, Thyroid (retrosternal) |
| Middle | Heart, pericardium, great vessel roots, tracheal bifurcation, main bronchi, phrenic nerves | Pericardial cysts, bronchogenic cysts, lymphadenopathy |
| Posterior | Descending aorta, esophagus, thoracic duct, azygos/hemiazygos veins, sympathetic chain, vagus nerves | Neurogenic tumors (schwannoma, neurofibroma), esophageal tumors |
The thoracic duct is the largest lymphatic vessel. It begins at the cisterna chyli (L1–L2), ascends through the aortic hiatus (T12), travels through the posterior mediastinum on the right side of the aorta, crosses to the left at ~T5, and drains into the junction of the left internal jugular and left subclavian veins (left venous angle). It drains lymph from the entire body except the right upper limb, right thorax, and right head/neck (which drain via the right lymphatic duct). Thoracic duct injury (from trauma, surgery, or malignancy) causes chylothorax (milky pleural effusion with triglycerides >110 mg/dL).
Phrenic & Vagus Nerve Course Through the Thorax
The phrenic nerve (C3–C5) descends on the anterior surface of the anterior scalene, enters the thorax between the subclavian artery and vein, and descends anterior to the lung root on the pericardium to reach the diaphragm. The vagus nerve (CN X) enters posterior to the lung root: the left vagus gives off the left recurrent laryngeal nerve which hooks under the aortic arch (ligamentum arteriosum) — vulnerable to compression from aortic aneurysm, mediastinal tumors, or during surgery. The right recurrent laryngeal hooks under the right subclavian artery.
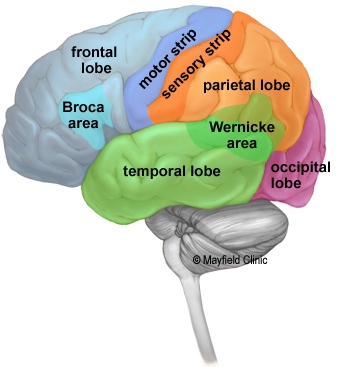
18 Brain: Cerebrum & Cortical Areas
The cerebral cortex is organized into four lobes: frontal (motor, executive function, personality, Broca area), parietal (somatosensory, spatial awareness), temporal (auditory processing, memory, Wernicke area), and occipital (visual processing). The cortex is supplied by the anterior cerebral artery (ACA), middle cerebral artery (MCA), and posterior cerebral artery (PCA).
Cerebral Artery Territories & Stroke Syndromes
| Artery | Territory | Stroke Presentation |
|---|---|---|
| ACA | Medial frontal & parietal cortex (leg motor/sensory strip) | Contralateral leg weakness & sensory loss; personality changes; urinary incontinence |
| MCA | Lateral frontal, parietal, temporal cortex (face/arm motor/sensory, language areas) | Contralateral face/arm > leg weakness; aphasia (dominant hemisphere); neglect (non-dominant); gaze deviation toward lesion |
| PCA | Occipital lobe, medial temporal lobe, thalamus | Contralateral homonymous hemianopia with macular sparing; memory deficits (hippocampus); thalamic pain syndrome |
| Lenticulostriate aa. (MCA branches) | Basal ganglia, internal capsule | Pure motor hemiparesis (lacunar stroke); most common site of hypertensive hemorrhage |
| PICA (posterior inferior cerebellar) | Lateral medulla, inferior cerebellum | Wallenberg syndrome (lateral medullary): ipsilateral face + contralateral body pain/temp loss, dysphagia, Horner syndrome, vertigo, ataxia |
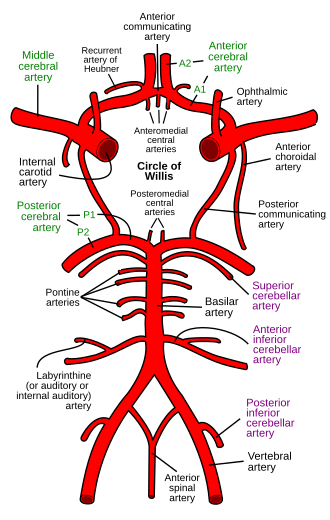
Circle of Willis
The circle of Willis is the anastomotic ring at the base of the brain connecting the anterior and posterior circulations. Components: ACA, anterior communicating artery (AComm), ICA, posterior communicating artery (PComm), and PCA. The AComm is the most common site of berry aneurysm. The PComm is the second most common; PComm aneurysm can compress CN III (oculomotor nerve), causing a "pupil-involving" third nerve palsy (ptosis, "down and out" eye, dilated pupil). Only ~20% of people have a complete, symmetric circle of Willis.
Basal Ganglia
The basal ganglia modulate movement via the direct pathway (facilitates movement: cortex → striatum → GPi/SNr inhibition → thalamus disinhibited → cortex) and indirect pathway (suppresses movement). The substantia nigra pars compacta provides dopaminergic input to the striatum; its degeneration causes Parkinson disease (resting tremor, rigidity, bradykinesia, postural instability). The caudate atrophy is characteristic of Huntington disease.
Thalamus & Hypothalamus
The thalamus is the major relay station for all sensory information (except olfaction) en route to the cortex. Key nuclei: VPL (body somatosensory — medial lemniscus and spinothalamic), VPM (face somatosensory — trigeminal), LGN (lateral geniculate nucleus — vision), MGN (medial geniculate nucleus — auditory), VL (ventral lateral — motor, receives cerebellar and basal ganglia input). The hypothalamus controls the autonomic nervous system, endocrine function (via pituitary), temperature regulation, hunger, thirst, circadian rhythms, and emotional behavior. Key nuclei: suprachiasmatic (circadian rhythm), supraoptic (ADH), paraventricular (oxytocin and CRH), ventromedial (satiety center — lesion causes obesity), lateral (hunger center — lesion causes anorexia).
Limbic System
The hippocampus (medial temporal lobe) is essential for converting short-term to long-term memory (explicit/declarative). Bilateral hippocampal damage (e.g., herpes simplex encephalitis, anoxic injury) causes anterograde amnesia. The amygdala (anterior temporal lobe) processes fear and emotional memory. The Papez circuit (hippocampus → fornix → mammillary bodies → anterior thalamus → cingulate gyrus → entorhinal cortex → hippocampus) is the anatomic substrate of emotional memory. Wernicke-Korsakoff syndrome (thiamine deficiency) damages mammillary bodies and medial thalamus, causing confabulation and memory loss.
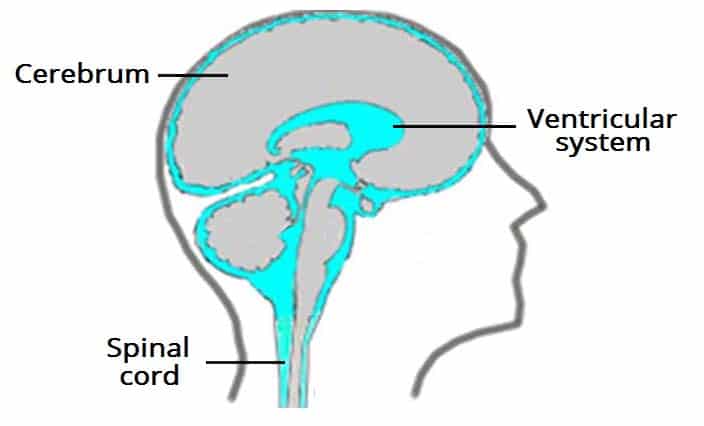
Ventricular System & CSF
CSF is produced by the choroid plexus (~500 mL/day; ~150 mL total volume at any time). Flow: lateral ventricles → foramen of Monro → 3rd ventricle → cerebral aqueduct (of Sylvius) → 4th ventricle → foramina of Luschka (lateral, 2) and foramen of Magendie (midline, 1) → subarachnoid space → absorbed by arachnoid granulations into the dural venous sinuses. Obstruction at any point causes hydrocephalus. The cerebral aqueduct is the narrowest point and the most common site of obstruction (e.g., congenital stenosis, tumor).
19 Brainstem, Cerebellum & Cranial Nerves
The brainstem (midbrain, pons, medulla) contains cranial nerve nuclei, ascending/descending tracts, reticular formation (consciousness), and vital autonomic centers (respiratory, cardiovascular). The cerebellum coordinates movement, balance, and motor learning.
Cranial Nerves: Overview
| CN | Name | Type | Function | Key Clinical Test / Lesion |
|---|---|---|---|---|
| I | Olfactory | Sensory | Smell | Anosmia; cribriform plate fracture |
| II | Optic | Sensory | Vision | Visual field defects; afferent limb of pupillary reflex |
| III | Oculomotor | Motor | Eye movement (SR, IR, MR, IO), lid elevation, pupil constriction | "Down and out" eye, ptosis, mydriasis (compression); ptosis without pupil (diabetic/ischemic) |
| IV | Trochlear | Motor | Superior oblique (intorsion, depression in adduction) | Head tilt to contralateral side; diplopia going downstairs; only CN to exit dorsally |
| V | Trigeminal | Both | Face sensation (V1/V2/V3); mastication muscles | Trigeminal neuralgia; corneal reflex (afferent V1, efferent VII); jaw deviation toward lesion |
| VI | Abducens | Motor | Lateral rectus (abduction) | Medial deviation (esotropia); long intracranial course → false localizing sign in raised ICP |
| VII | Facial | Both | Facial expression, taste (ant. 2/3 tongue), lacrimation, stapedius | Bell palsy (LMN: entire face); UMN: forehead spared (bilateral cortical innervation) |
| VIII | Vestibulocochlear | Sensory | Hearing & balance | Sensorineural vs conductive deafness (Weber/Rinne); acoustic neuroma (CN VIII schwannoma at CPA) |
| IX | Glossopharyngeal | Both | Taste (post. 1/3 tongue), pharyngeal sensation, parotid gland | Afferent limb of gag reflex; glossopharyngeal neuralgia |
| X | Vagus | Both | Palate, pharynx, larynx, parasympathetics to thoracic/abdominal viscera | Uvula deviates away from lesion; hoarseness (recurrent laryngeal n.); efferent limb of gag reflex |
| XI | Accessory | Motor | SCM (turns head contralaterally), trapezius (shrugs shoulder) | Shoulder droop, head turning weakness; vulnerable in posterior triangle of neck surgery |
| XII | Hypoglossal | Motor | Tongue muscles (all except palatoglossus = CN X) | Tongue deviates toward lesion (LMN); atrophy and fasciculations ipsilaterally |
Compressive (aneurysm, uncal herniation): pupil involved (dilated) because parasympathetic fibers travel on the outside of the nerve and are affected first. Ischemic (diabetic mononeuropathy): pupil spared because the peripheral fibers receive collateral blood supply; the ischemia affects the core motor fibers. A CN III palsy with pupil involvement is an aneurysm until proven otherwise and requires emergent imaging.
Cerebellum
The cerebellum has three functional divisions: vestibulocerebellum (flocculonodular lobe — balance, eye movements; lesion → truncal ataxia, nystagmus), spinocerebellum (vermis and paravermal zones — posture, gait, limb coordination), and cerebrocerebellum (lateral hemispheres — motor planning, coordination of voluntary movements; lesion → intention tremor, dysdiadochokinesia, dysmetria). Cerebellar lesions produce ipsilateral findings (unlike cerebral cortex lesions, which produce contralateral findings), because the cerebellum has double-crossed pathways.
Brainstem Lesion Syndromes
| Syndrome | Location | Affected Structures | Presentation |
|---|---|---|---|
| Wallenberg (lateral medullary) | Lateral medulla (PICA) | Inferior cerebellar peduncle, vestibular nuclei, spinal trigeminal nucleus/tract, nucleus ambiguus, descending sympathetics, spinothalamic tract | Ipsilateral: facial pain/temp loss, Horner, ataxia, dysphagia/hoarseness. Contralateral: body pain/temp loss. Vertigo, nystagmus |
| Medial medullary (Dejerine) | Medial medulla (ASA/vertebral) | Pyramid, medial lemniscus, CN XII nucleus | Contralateral hemiparesis (sparing face), contralateral proprioception/vibration loss. Ipsilateral tongue deviation |
| Weber | Medial midbrain (PCA branches) | Cerebral peduncle, CN III fibers | Ipsilateral CN III palsy + contralateral hemiparesis |
| Benedikt | Medial midbrain (tegmentum) | CN III, red nucleus, medial lemniscus | Ipsilateral CN III palsy + contralateral tremor/ataxia + contralateral sensory loss |
| Locked-in syndrome | Ventral pons (basilar artery) | Bilateral corticospinal and corticobulbar tracts | Quadriplegia, anarthria, preserved consciousness and vertical eye movements (only voluntary movement remaining) |
20 Spinal Cord Tracts & Lesion Syndromes
The spinal cord contains ascending (sensory) and descending (motor) tracts organized in white matter columns surrounding the central gray matter (butterfly-shaped). Understanding tract anatomy is essential for localizing spinal cord lesions.
Major Spinal Cord Tracts
| Tract | Location | Function | Decussation |
|---|---|---|---|
| Dorsal columns (fasciculus gracilis & cuneatus) | Posterior | Fine touch, proprioception, vibration | Medulla (internal arcuate fibers → medial lemniscus) |
| Lateral corticospinal tract | Lateral | Voluntary motor (UMN to LMN) | Pyramidal decussation (caudal medulla) |
| Lateral spinothalamic tract | Anterolateral | Pain & temperature | Spinal cord (ventral white commissure, 1–2 levels above entry) |
| Anterior spinothalamic tract | Anterior | Crude touch & pressure | Spinal cord |
| Anterior corticospinal tract | Anterior | Proximal/axial motor (minor) | At level of synapse (uncrossed until target) |
Spinal Cord Lesion Syndromes
| Syndrome | Cause | Findings |
|---|---|---|
| Brown-Séquard (hemisection) | Penetrating trauma, tumor | Ipsilateral: motor loss (corticospinal), proprioception/vibration loss (dorsal columns). Contralateral: pain/temp loss (spinothalamic, already crossed) |
| Anterior cord syndrome | Anterior spinal artery occlusion, burst fracture | Bilateral motor paralysis + pain/temp loss below lesion. Preserved: dorsal columns (proprioception, vibration) |
| Central cord syndrome | Hyperextension in elderly with cervical spondylosis | Upper extremity weakness > lower (arms affected more because cervical fibers are medial in corticospinal tract); variable sensory loss; bladder dysfunction |
| Posterior cord syndrome | Tabes dorsalis (tertiary syphilis), B12 deficiency, Friedreich ataxia | Loss of proprioception & vibration bilaterally. Preserved: motor, pain/temp. Sensory ataxia, positive Romberg |
| Cauda equina syndrome | Central disc herniation (L4–L5/L5–S1), tumor | LMN signs (flaccid, areflexic), saddle anesthesia (S2–S4), bowel/bladder dysfunction, bilateral leg pain. Surgical emergency. |
| Syringomyelia | Central canal dilation (often post-Chiari I) | Bilateral cape-like loss of pain/temp (crossing fibers in ventral white commissure disrupted); preserved touch. Can progress to LMN weakness at level. |
21 GI Tract & Hepatobiliary System
The gastrointestinal tract extends from the mouth to the anus, with each segment having specific histologic, vascular, and innervation characteristics that determine its clinical pathology. The GI tract is divided embryologically into foregut, midgut, and hindgut — each with its own arterial supply, venous drainage, and autonomic innervation.
GI Tract Divisions & Blood Supply
| Division | Structures | Arterial Supply | Parasympathetic Innervation |
|---|---|---|---|
| Foregut | Esophagus (lower 1/3) to 2nd part of duodenum (ampulla of Vater), liver, gallbladder, pancreas, spleen | Celiac trunk | Vagus nerve (CN X) |
| Midgut | 2nd part of duodenum to proximal 2/3 of transverse colon | Superior mesenteric artery | Vagus nerve (CN X) |
| Hindgut | Distal 1/3 transverse colon to upper anal canal (above pectinate line) | Inferior mesenteric artery | Pelvic splanchnic nerves (S2–S4) |
Peritoneal Relationships
Most GI organs are intraperitoneal (stomach, jejunum, ileum, transverse colon, sigmoid, spleen, liver). Retroperitoneal structures are memorized as "SAD PUCKER": Suprarenal (adrenal) glands, Aorta/IVC, Duodenum (2nd–4th parts), Pancreas (except tail), Ureters, Colon (ascending & descending), Kidneys, Esophagus (thoracic), Rectum.
Key Peritoneal Ligaments & Spaces
| Structure | Connects | Clinical Significance |
|---|---|---|
| Falciform ligament | Liver to anterior abdominal wall | Contains ligamentum teres (remnant of umbilical vein); divides liver surface into right and left lobes |
| Hepatoduodenal ligament | Liver to duodenum (within lesser omentum) | Contains portal triad (hepatic artery, portal vein, bile duct); Pringle maneuver compresses this |
| Gastrosplenic ligament | Stomach to spleen | Contains short gastric and left gastroepiploic arteries; ligated during splenectomy |
| Splenorenal ligament | Spleen to left kidney | Contains splenic artery and vein, tail of pancreas |
| Greater omentum | Greater curvature of stomach to transverse colon | "Abdominal policeman" — migrates to sites of inflammation to wall off infection |
| Hepatorenal recess (Morrison pouch) | Between liver and right kidney | Most dependent space in supine position; free fluid (blood, ascites) collects here first on FAST exam |
| Pouch of Douglas (rectouterine) | Between rectum and uterus (female) | Most dependent pelvic space; fluid collects here; accessed via culdocentesis |
| Epiploic foramen (of Winslow) | Communication between greater and lesser peritoneal sacs | Bounded by hepatoduodenal ligament anteriorly, IVC posteriorly; rarely, internal hernia site |
Hepatobiliary Anatomy
The portal triad (within the hepatoduodenal ligament) contains the hepatic artery proper, portal vein, and common bile duct. The Pringle maneuver (compressing the hepatoduodenal ligament) controls hepatic hemorrhage by occluding the portal triad. The cystic artery (typically from right hepatic artery) is found within Calot triangle (cystohepatic triangle), bounded by the cystic duct, common hepatic duct, and inferior surface of the liver — the critical "triangle of safety" during cholecystectomy.
The Pectinate (Dentate) Line
The pectinate line is the landmark dividing the upper and lower anal canal, with critical differences in arterial supply, venous drainage, innervation, and lymphatic drainage:
| Feature | Above Pectinate Line | Below Pectinate Line |
|---|---|---|
| Epithelium | Simple columnar | Stratified squamous (non-keratinized) |
| Arterial supply | Superior rectal artery (IMA) | Inferior rectal artery (internal pudendal) |
| Venous drainage | Superior rectal vein → portal system | Inferior rectal vein → systemic (IVC) |
| Lymphatic drainage | Internal iliac nodes | Superficial inguinal nodes |
| Innervation | Visceral (autonomic) — painless | Somatic (inferior rectal nerve) — painful |
| Hemorrhoids | Internal hemorrhoids (painless, can bleed) | External hemorrhoids (painful, can thrombose) |
Pancreatic & Biliary Duct Anatomy
The main pancreatic duct (of Wirsung) joins the common bile duct to form the hepatopancreatic ampulla (of Vater), which opens into the 2nd part of the duodenum at the major duodenal papilla, controlled by the sphincter of Oddi. The accessory pancreatic duct (of Santorini) drains the uncinate process and opens at the minor duodenal papilla. Pancreas divisum (most common congenital pancreatic variant, ~10%) occurs when the dorsal and ventral pancreatic buds fail to fuse, so the dorsal duct drains the majority of the pancreas through the minor papilla.
Portal-Systemic Anastomoses
| Site | Portal Vessel | Systemic Vessel | Clinical Manifestation |
|---|---|---|---|
| Distal esophagus | Left gastric vein | Esophageal veins (azygos) | Esophageal varices (life-threatening hemorrhage) |
| Rectum | Superior rectal vein | Middle & inferior rectal veins | Hemorrhoids (internal above pectinate line) |
| Periumbilical | Paraumbilical veins | Superficial epigastric veins | Caput medusae |
| Retroperitoneum | Colic veins | Retroperitoneal veins | Rarely clinically apparent |
22 Renal & Urogenital Anatomy
The kidneys are retroperitoneal organs at T12–L3, with the right kidney slightly lower than the left (depressed by the liver). Each kidney is ~11 cm long and weighs ~150 g. They are surrounded by (from inside out): renal capsule, perinephric fat, Gerota fascia (renal fascia), and paranephric fat. The adrenal glands sit on the superior pole of each kidney within Gerota fascia.
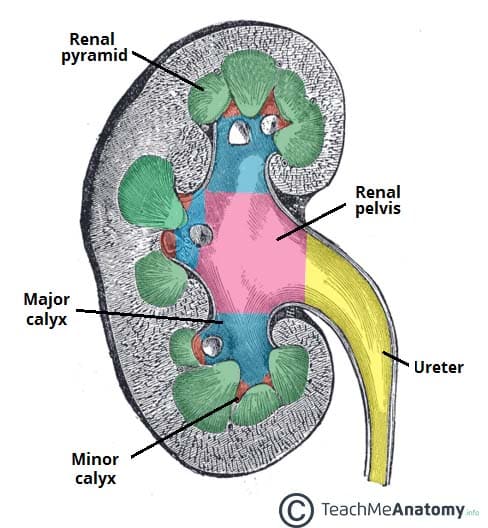
Internal Renal Anatomy
The kidney parenchyma is divided into the cortex (outer; contains glomeruli, proximal and distal convoluted tubules) and medulla (inner; contains loops of Henle and collecting ducts arranged in 8–18 pyramids). Each renal pyramid drains through a minor calyx → major calyx → renal pelvis → ureter. The renal hilum transmits the renal vein (most anterior), renal artery (middle), and renal pelvis/ureter (most posterior).
Blood Supply
Each kidney receives ~20–25% of cardiac output. The renal artery divides into segmental arteries (5 segments, each an end artery — no collateral circulation; occlusion causes segmental infarction). Segmental → interlobar → arcuate → interlobular → afferent arteriole → glomerular capillaries → efferent arteriole → peritubular capillaries (cortex) or vasa recta (medulla) → interlobular veins → arcuate → interlobar → renal vein.
The left renal vein is longer than the right and crosses anterior to the aorta, posterior to the SMA. It receives the left gonadal vein, left suprarenal vein, and left inferior phrenic vein. Nutcracker syndrome: compression of the left renal vein between the aorta and SMA causing hematuria, flank pain, and left-sided varicocele. A left-sided varicocele that does not decompress when supine should raise concern for renal vein obstruction (renal cell carcinoma with tumor thrombus).
Ureters
The ureters are 25–30 cm muscular tubes (transitional epithelium, peristalsis) connecting the renal pelvis to the bladder. Three normal points of constriction (where stones lodge): ureteropelvic junction (UPJ), pelvic brim (crossing the common iliac vessels), and ureterovesical junction (UVJ) (narrowest point, most common site of obstruction). The ureter crosses anterior to the common iliac artery at the pelvic brim and passes under the uterine artery in females ("water under the bridge") — vulnerable during hysterectomy.
Urinary Bladder & Urethra
The trigone is the smooth triangular area on the internal base of the bladder, bounded by the two ureteral orifices and the internal urethral orifice. It is the most common site for transitional cell carcinoma. The male urethra has four parts: preprostatic (within bladder neck), prostatic (through prostate; receives ejaculatory ducts and prostatic ducts), membranous (through urogenital diaphragm; most narrow, most commonly injured in pelvic fractures), and spongy/penile (through corpus spongiosum; longest part). Straddle injuries typically rupture the bulbar urethra (spongy portion).
Posterior urethral injuries (membranous urethra) occur with pelvic fractures and present with blood at the urethral meatus, high-riding prostate on DRE, and inability to void. Do NOT attempt Foley catheterization — obtain a retrograde urethrogram first. Suprapubic catheter placement is the initial management.
23 Reproductive Anatomy
Male Reproductive Anatomy
The testes develop retroperitoneally and descend through the inguinal canal into the scrotum (guided by the gubernaculum), bringing their blood supply (testicular arteries from the aorta at L2), lymphatic drainage (para-aortic lymph nodes, NOT inguinal), and the processus vaginalis. Failure of descent = cryptorchidism (increased risk of testicular cancer and infertility; orchiopexy by age 1). The pampiniform plexus of veins surrounds the testicular artery within the spermatic cord and acts as a countercurrent heat exchanger; dilation = varicocele (90% left-sided because the left testicular vein drains into the left renal vein at a right angle).
Spermatic Cord Contents
The spermatic cord contains: vas deferens, testicular artery, artery of the vas deferens (from inferior vesical artery), cremasteric artery (from inferior epigastric), pampiniform venous plexus, genital branch of genitofemoral nerve (cremasteric reflex), sympathetic nerve fibers, and lymphatics. Covered by three fascial layers: internal spermatic fascia (from transversalis fascia), cremasteric muscle and fascia (from internal oblique), and external spermatic fascia (from external oblique aponeurosis).
Female Reproductive Anatomy
The uterus is supported by the cardinal ligament (transverse cervical ligament — main support, contains uterine artery), uterosacral ligament, round ligament (through inguinal canal; maintains anteversion), and broad ligament (peritoneal fold containing uterine tubes, ovarian ligament, round ligament, uterine vessels). The ovarian artery (from aorta at L2) reaches the ovary via the suspensory ligament (infundibulopelvic ligament) — this must be ligated during oophorectomy and is at risk during appendectomy.
Lymphatic Drainage of Reproductive Organs
| Structure | Primary Lymph Node Drainage |
|---|---|
| Testes / Ovaries | Para-aortic (lumbar) lymph nodes (NOT inguinal) |
| Scrotum / Vulva (labia majora) | Superficial inguinal lymph nodes |
| Uterine body | Internal & external iliac, para-aortic nodes |
| Cervix | Internal iliac, external iliac, obturator nodes |
| Proximal vagina | Internal iliac nodes |
| Distal vagina | Superficial inguinal nodes |
| Glans penis / clitoris | Deep inguinal lymph nodes |
24 Skull, Face & Scalp
The skull consists of the cranial vault (calvaria: frontal, parietal x2, temporal x2, occipital) and the skull base (anterior, middle, and posterior cranial fossae). The bones are joined by sutures: sagittal (between parietals), coronal (frontal-parietal), lambdoid (parietal-occipital), and squamous (temporal-parietal).
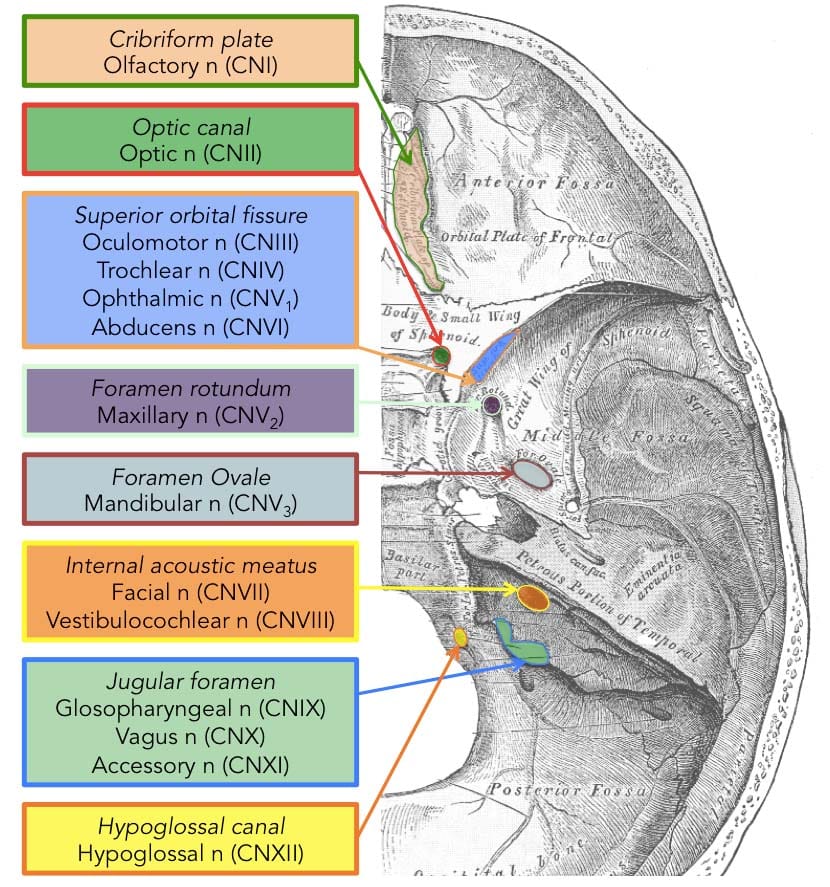
Skull Base Foramina & Contents
| Foramen | Fossa | Contents |
|---|---|---|
| Cribriform plate | Anterior | CN I (olfactory nerve fibers); fracture → CSF rhinorrhea, anosmia |
| Optic canal | Middle | CN II, ophthalmic artery |
| Superior orbital fissure | Middle | CN III, IV, V1, VI, ophthalmic veins |
| Foramen rotundum | Middle | CN V2 (maxillary) |
| Foramen ovale | Middle | CN V3 (mandibular) |
| Foramen spinosum | Middle | Middle meningeal artery |
| Internal acoustic meatus | Posterior | CN VII, VIII, labyrinthine artery |
| Jugular foramen | Posterior | CN IX, X, XI; internal jugular vein |
| Hypoglossal canal | Posterior | CN XII |
| Foramen magnum | Posterior | Spinal cord/medulla, vertebral arteries, CN XI (ascending part) |
Meningeal Layers & Intracranial Hemorrhage
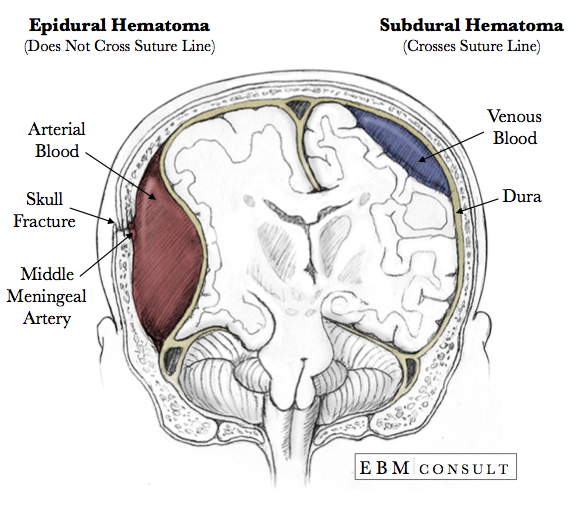
| Hemorrhage Type | Location | Vessel | CT Appearance | Clinical |
|---|---|---|---|---|
| Epidural hematoma | Between skull and dura | Middle meningeal artery (temporal bone fracture) | Biconvex (lens-shaped); does NOT cross sutures | Lucid interval → rapid deterioration; uncal herniation |
| Subdural hematoma | Between dura and arachnoid | Bridging veins (cortical veins to dural sinuses) | Crescent-shaped; crosses sutures | Acute: trauma; chronic: elderly/alcoholics; brain atrophy stretches bridging veins |
| Subarachnoid hemorrhage | Between arachnoid and pia | Berry aneurysm rupture (85%); AVM | Hyperdense blood in sulci/cisterns | "Worst headache of life"; vasospasm risk days 4–14 |
Scalp Layers
The scalp has five layers: Skin, Connective tissue (dense, highly vascular — scalp lacerations bleed profusely because arteries are tethered and cannot retract), Aponeurosis (galea aponeurotica — connects frontalis and occipitalis), Loose areolar connective tissue (the "danger layer" — emissary veins here can transmit infection intracranially to the dural venous sinuses), and Pericranium (periosteum of skull).
25 Neck Triangles, Fascial Planes & Vasculature
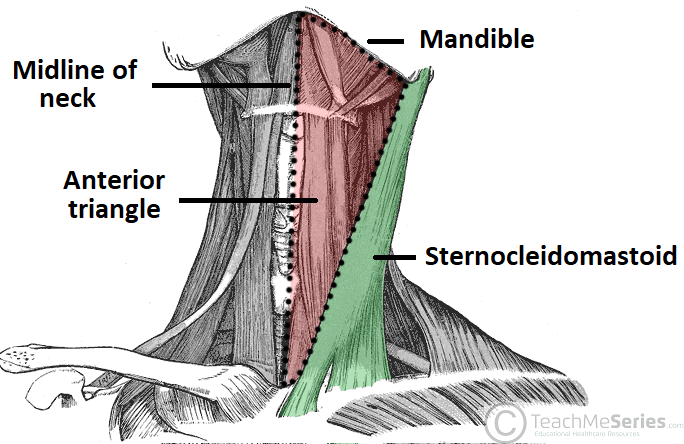
The neck is divided by the sternocleidomastoid (SCM) into the anterior and posterior triangles. These triangles organize the understanding of deep neck structures, surgical approaches, and the spread of infection.
Neck Triangles
| Triangle | Boundaries | Key Contents |
|---|---|---|
| Anterior triangle | Midline, SCM (posterior), mandible (superior) | Carotid sheath (common/internal carotid, IJV, vagus nerve), thyroid, larynx, submandibular gland, CN XII |
| Posterior triangle | SCM (anterior), trapezius (posterior), clavicle (inferior) | Accessory nerve (CN XI, superficial — at risk in surgery), external jugular vein, subclavian artery (third part), brachial plexus trunks, phrenic nerve (on anterior scalene) |
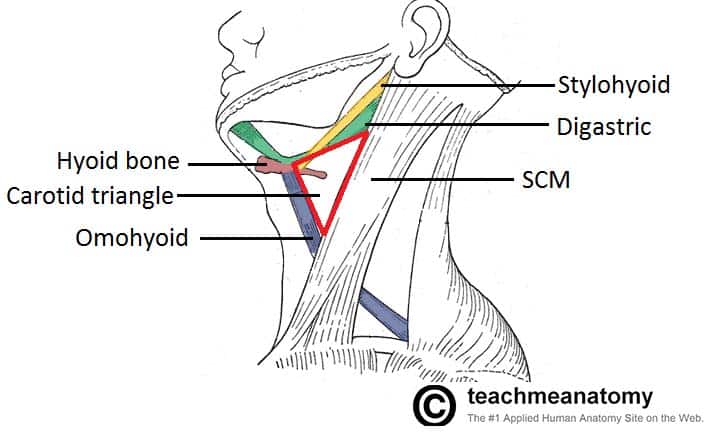
| Submental | Anterior bellies of digastric, hyoid bone | Submental lymph nodes |
| Submandibular | Mandible, anterior & posterior bellies of digastric | Submandibular gland, facial artery, CN XII, lingual nerve |
Carotid Sheath
The carotid sheath extends from the skull base to the aortic arch and contains three structures: common carotid artery (medial), internal jugular vein (lateral), and vagus nerve (posterior, between them). The common carotid bifurcates at the level of C3–C4 (superior border of thyroid cartilage) into the internal carotid (no branches in the neck; enters skull via carotid canal) and external carotid (8 branches supplying the face, scalp, and neck). The carotid body (chemoreceptor for O2/CO2/pH) and carotid sinus (baroreceptor for blood pressure) are located at the bifurcation.
Thyroid & Parathyroid Anatomy
The thyroid gland lies at C5–T1, with two lobes connected by the isthmus (overlying tracheal rings 2–4). Blood supply: superior thyroid artery (first branch of external carotid) and inferior thyroid artery (from thyrocervical trunk of subclavian artery). The recurrent laryngeal nerve (branch of CN X) ascends in the tracheoesophageal groove and enters the larynx posterior to the cricothyroid joint — it is closely related to the inferior thyroid artery and is at risk during thyroidectomy. Injury causes ipsilateral vocal cord paralysis (hoarseness); bilateral injury causes airway compromise.
Deep Cervical Fascia
Three layers of deep cervical fascia enclose neck structures: investing layer (surrounds SCM, trapezius), pretracheal layer (encloses thyroid, trachea, esophagus; visceral division; extends into superior mediastinum), and prevertebral layer (covers prevertebral muscles, vertebral column; extends laterally as the axillary sheath around the brachial plexus). The retropharyngeal space (between pretracheal and prevertebral layers) is a potential route for infection to spread from the pharynx to the posterior mediastinum — a dangerous pathway that can cause mediastinitis.
Larynx & Airway Anatomy
The larynx extends from C3 to C6 and contains the vocal cords (true vocal folds). Key cartilages: thyroid (largest, "Adam's apple"), cricoid (only complete cartilage ring; landmark for cricothyrotomy and tracheostomy), epiglottic (elastic cartilage; covers laryngeal inlet during swallowing), arytenoid (paired; vocal cord attachment). The cricothyroid membrane connects the thyroid and cricoid cartilages anteriorly and is the site of emergency cricothyrotomy (landmark: palpable depression between thyroid and cricoid cartilages in the midline).
| Muscle | Action | Innervation |
|---|---|---|
| Cricothyroid | Tenses vocal cords (increases pitch) | External branch of superior laryngeal nerve (CN X) |
| All other intrinsic muscles | Abduction, adduction, tension adjustment of vocal cords | Recurrent laryngeal nerve (CN X) |
| Posterior cricoarytenoid | ONLY abductor of vocal cords (opens glottis) | Recurrent laryngeal nerve |
Salivary Glands
| Gland | Duct | Secretion | Innervation | Clinical Note |
|---|---|---|---|---|
| Parotid | Stensen duct (opens opposite 2nd upper molar) | Serous | CN IX (glossopharyngeal, via otic ganglion) | CN VII traverses gland; parotid surgery risks facial nerve injury. Most parotid tumors are benign (pleomorphic adenoma) |
| Submandibular | Wharton duct (opens lateral to frenulum) | Mixed (serous + mucous) | CN VII (facial, via chorda tympani → submandibular ganglion) | Most common salivary gland stone (sialolithiasis); lingual nerve wraps around duct |
| Sublingual | Multiple small ducts (of Rivinus) | Mucous | CN VII (facial, via chorda tympani) | Ranula (mucocele) if duct blocked |
Orbit & Extraocular Muscles
Six extraocular muscles control eye movement: superior rectus (elevation, intorsion), inferior rectus (depression, extorsion), medial rectus (adduction), lateral rectus (abduction), superior oblique (depression in adduction, intorsion), and inferior oblique (elevation in adduction, extorsion). Innervation: LR6SO4 — lateral rectus = CN VI (abducens), superior oblique = CN IV (trochlear), all others = CN III (oculomotor). CN III also innervates levator palpebrae superioris (lid elevation) and carries parasympathetic fibers to the sphincter pupillae (pupil constriction) and ciliary muscle (accommodation).
A direct blow to the orbit can fracture the thin orbital floor (maxillary bone), trapping the inferior rectus muscle. Findings: inability to look upward (restricted upgaze), enophthalmos (sunken eye), infraorbital nerve hypesthesia (numbness of cheek, upper lip, upper teeth — V2 distribution). CT orbits is diagnostic. Surgical repair if persistent diplopia or significant enophthalmos.
26 Surface Anatomy & Landmarks
Surface anatomy translates deep structures to palpable or visible landmarks on the body surface. These landmarks are essential for physical examination, procedural guidance, and surgical planning.
Thoracic Surface Landmarks
| Landmark | Level | Clinical Significance |
|---|---|---|
| Sternal angle (angle of Louis) | T4–T5 | Rib 2 attachment; carina; aortic arch begins/ends; tracheal bifurcation; azygos vein enters SVC |
| Suprasternal (jugular) notch | T2–T3 | Palpate trachea; assess tracheal deviation |
| Xiphoid process | T9 | Landmark for CPR hand placement; anterior diaphragm attachment |
| Nipple | T4 dermatome | Overlies 4th intercostal space (males); variable in females |
| Inferior angle of scapula | T7 | Landmark for posterior thoracentesis |
Abdominal Surface Landmarks
| Landmark | Level | Clinical Significance |
|---|---|---|
| Transpyloric plane (Addison plane) | L1 | Pylorus, SMA origin, renal hilum, splenic hilum, pancreatic neck, 1st part duodenum, fundus of gallbladder (at 9th costal cartilage) |
| Subcostal plane | L3 | Inferior margin of 10th costal cartilage; IMA origin |
| Umbilicus | L3–L4 | Aortic bifurcation at L4; dermatome T10 |
| Supracristal plane | L4 | Connecting iliac crests; LP site (L4 or L4–L5 interspace) |
| McBurney point | RLQ | 1/3 distance from ASIS to umbilicus; appendix base |
| Murphy sign location | RUQ | Intersection of right midclavicular line and costal margin; gallbladder |
Upper Limb Surface Landmarks
Cubital fossa (antecubital fossa): bounded by brachioradialis (lateral), pronator teres (medial), and an imaginary line connecting the epicondyles (superior). Contents lateral to medial: radial nerve, biceps tendon, brachial artery, median nerve ("R-B-A-M" or "Really BrAve Medics"). The median cubital vein crosses superficially — the most common site for venipuncture. The brachial artery pulse is palpated medial to the biceps tendon and is the auscultation site for blood pressure measurement.
Lower Limb Surface Landmarks
Femoral pulse: midinguinal point (midway between ASIS and pubic symphysis). Popliteal pulse: deep in the popliteal fossa (flexed knee, press firmly). Posterior tibial pulse: posterior to the medial malleolus. Dorsalis pedis pulse: dorsum of foot, lateral to extensor hallucis longus tendon. Loss of peripheral pulses = peripheral arterial disease; the dorsalis pedis is absent in ~10% of normal individuals.
Vertebral Level Landmarks
| Vertebral Level | Surface Landmark or Structure |
|---|---|
| C3–C4 | Hyoid bone; carotid bifurcation |
| C4–C5 | Thyroid cartilage |
| C6 | Cricoid cartilage; carotid tubercle (Chassaignac); transition: larynx → trachea, pharynx → esophagus |
| T2–T3 | Suprasternal (jugular) notch |
| T4–T5 | Sternal angle; tracheal bifurcation; aortic arch |
| T9 | Xiphoid process |
| T10 | Esophageal hiatus |
| T12 | Aortic hiatus; celiac trunk |
| L1 | SMA origin; transpyloric plane; renal hilum; conus medullaris |
| L3 | Subcostal plane; IMA origin |
| L4 | Iliac crest (supracristal plane); aortic bifurcation; umbilicus |
| L5 | IVC formation (common iliac veins converge) |
| S2 | Posterior superior iliac spine (PSIS); termination of dural sac |
Procedural Landmarks Quick Reference
| Procedure | Anatomical Landmark | Key Anatomy |
|---|---|---|
| Lumbar puncture | L3–L4 or L4–L5 interspace (iliac crest = L4) | Below conus medullaris; needle passes through supraspinous & interspinous ligaments, ligamentum flavum, epidural space, dura, arachnoid |
| Subclavian central line | Junction of middle and medial thirds of clavicle | Subclavian vein anterior to anterior scalene; artery posterior. Risk: pneumothorax (lung apex) |
| Internal jugular central line | Apex of SCM triangle (between sternal and clavicular heads) | IJV lateral to carotid artery within carotid sheath. Risk: carotid puncture, pneumothorax |
| Thoracentesis | 7th–9th intercostal space, posterior axillary line | Insert just above rib (avoid VAN below); fluid in costophrenic recess |
| Cricothyrotomy | Cricothyroid membrane (between thyroid and cricoid cartilage) | Avascular membrane; only emergent surgical airway option below glottis |
| Pericardiocentesis | Subxiphoid approach, left of xiphoid, aimed toward left shoulder | Needle enters pericardial space avoiding coronary vessels and pleura |
27 Clinical Correlates & Surgical Anatomy
This section integrates anatomical knowledge with common clinical and surgical scenarios encountered across specialties.
High-Yield Nerve Injuries
| Nerve | Injury Mechanism | Motor Deficit | Sensory Deficit |
|---|---|---|---|
| Axillary (C5–C6) | Anterior shoulder dislocation, surgical neck fracture | Deltoid (abduction >15°), teres minor | Regimental badge area (lateral shoulder) |
| Radial (C5–T1) | Midshaft humerus fracture, "Saturday night palsy" | Wrist drop (wrist/finger extension loss) | Posterior arm/forearm, dorsal first web space |
| Median (C5–T1) | Supracondylar humerus fracture (children), carpal tunnel | Thenar atrophy ("ape hand"), loss of thumb opposition | Palmar thumb, index, middle, radial ring finger |
| Ulnar (C8–T1) | Medial epicondyle fracture, cubital tunnel | Claw hand (4th/5th digits), interossei/hypothenar loss, Froment sign | Medial 1.5 fingers, medial hand |
| Common fibular (L4–S2) | Fibular neck fracture, leg cast, habitual leg crossing | Foot drop (loss of dorsiflexion and eversion) | Lateral leg, dorsum of foot |
| Femoral (L2–L4) | Pelvic surgery, psoas abscess | Loss of knee extension (quadriceps), loss of knee jerk | Anterior thigh, medial leg (saphenous) |
| Recurrent laryngeal (CN X branch) | Thyroid surgery, aortic aneurysm, lung apex tumor | Ipsilateral vocal cord paralysis (hoarseness) | Laryngeal mucosa below vocal cords |
Key Vascular Territories & Vulnerabilities
| Scenario | Vessel at Risk | Anatomical Reason |
|---|---|---|
| Supracondylar fracture (children) | Brachial artery | Artery passes anterior to distal humerus; posterior displacement can injure it → Volkmann ischemic contracture |
| Posterior knee dislocation | Popliteal artery | Artery is tethered as it passes through the popliteal fossa; mandatory angiography/ABI assessment |
| Pelvic fracture | Internal iliac artery branches | Multiple branches within the pelvis; posterior pelvic ring disruption can cause massive hemorrhage |
| Rib fractures (lower ribs) | Spleen (left), liver (right) | Left ribs 9–11 overlie the spleen; right ribs 8–12 overlie the liver |
Referred pain occurs when visceral afferents converge on the same spinal cord segments as somatic afferents. Myocardial ischemia → left arm/jaw pain (T1–T4). Diaphragmatic irritation → shoulder pain (C3–C5 phrenic nerve). Appendicitis → periumbilical pain initially (T10 visceral afferents from midgut), then localizes to RLQ when parietal peritoneum is inflamed. Gallbladder → right shoulder (phrenic nerve irritation from right hemidiaphragm). Kidney stone → flank radiating to groin (T10–L1).
Compartment Syndrome
Compartment syndrome occurs when pressure within a closed fascial compartment rises sufficiently to compromise tissue perfusion. Most common sites: anterior compartment of the leg (after tibial fractures) and volar forearm (after supracondylar fractures in children). The intracompartmental pressure threshold for fasciotomy is typically ≥30 mmHg (or within 30 mmHg of diastolic blood pressure). Earliest clinical finding: pain out of proportion to injury and pain with passive stretch of the affected muscles. Pulselessness is a LATE finding — do not wait for absent pulses before intervening. Treatment: emergent fasciotomy of all compartments.
The feared complication of untreated forearm compartment syndrome, typically following supracondylar humerus fracture in children. Brachial artery compromise leads to ischemic necrosis of forearm flexor muscles, which fibrose and contract. The result is a fixed flexion contracture of the wrist and fingers with forearm pronation. Prevention requires early recognition of compartment syndrome signs and emergent fasciotomy.
Peripheral Nerve Entrapment Syndromes
| Syndrome | Nerve | Site of Compression | Presentation |
|---|---|---|---|
| Carpal tunnel | Median | Flexor retinaculum (wrist) | Thumb, index, middle finger numbness/paresthesias; thenar atrophy (late) |
| Cubital tunnel | Ulnar | Behind medial epicondyle (elbow) | Ring and little finger numbness; hand intrinsic weakness; clawing |
| Guyon canal | Ulnar | Hook of hamate (wrist) | Motor > sensory; intrinsic hand muscle weakness without forearm symptoms |
| Tarsal tunnel | Tibial (posterior) | Flexor retinaculum (medial ankle) | Burning/numbness of sole; positive Tinel behind medial malleolus |
| Meralgia paresthetica | Lateral femoral cutaneous (L2–L3) | Under inguinal ligament near ASIS | Lateral thigh numbness/burning; purely sensory (no motor deficit) |
| Piriformis syndrome | Sciatic | Piriformis muscle (deep gluteal) | Buttock pain radiating down leg; pain with hip internal rotation; controversial diagnosis |
| Thoracic outlet syndrome | Lower trunk of brachial plexus, subclavian vessels | Between anterior/middle scalene, under clavicle, or at costoclavicular space | Ulnar distribution numbness, hand weakness, vascular symptoms (color changes, swelling) |
Hernias: Anatomical Classification
| Type | Location | Key Feature |
|---|---|---|
| Indirect inguinal | Through deep inguinal ring, lateral to inferior epigastric vessels | Most common hernia overall; congenital (patent processus vaginalis) |
| Direct inguinal | Through Hesselbach triangle, medial to inferior epigastric vessels | Acquired; older males; rarely enters scrotum |
| Femoral | Through femoral canal, below inguinal ligament | More common in women; highest strangulation risk |
| Umbilical | Through umbilical ring | Common in infants (usually resolves by age 5); acquired in adults with ascites/obesity |
| Hiatal (sliding, 95%) | GE junction slides above diaphragm through esophageal hiatus | Associated with GERD; lower esophageal sphincter incompetence |
| Hiatal (paraesophageal, 5%) | Gastric fundus herniates through hiatus alongside esophagus | Higher risk of strangulation/volvulus |
| Bochdalek | Posterolateral diaphragm defect | Congenital; left > right; bowel in thorax → pulmonary hypoplasia |
28 High-Yield Review & Reference Tables
This section consolidates the most frequently tested anatomical facts for board examinations and clinical practice.
Muscle Innervation Quick Reference
| Action | Muscle(s) | Nerve | Root |
|---|---|---|---|
| Shoulder abduction (0–15°) | Supraspinatus | Suprascapular | C5–C6 |
| Shoulder abduction (>15°) | Deltoid | Axillary | C5–C6 |
| Elbow flexion | Biceps, brachialis | Musculocutaneous | C5–C6 |
| Elbow extension | Triceps | Radial | C6–C8 |
| Wrist extension | Extensors (ECRL, ECRB, ECU) | Radial (posterior interosseous) | C6–C7 |
| Wrist flexion | FCR, FCU, palmaris longus | Median (FCR, PL), Ulnar (FCU) | C7–C8 |
| Finger extension | ED, EI, EDM | Posterior interosseous (radial) | C7–C8 |
| Thumb opposition | Opponens pollicis | Median (recurrent branch) | C8–T1 |
| Hip flexion | Iliopsoas | Femoral + L1–L3 direct | L1–L3 |
| Hip extension | Gluteus maximus | Inferior gluteal | L5–S2 |
| Hip abduction | Gluteus medius & minimus | Superior gluteal | L4–S1 |
| Knee extension | Quadriceps | Femoral | L2–L4 |
| Knee flexion | Hamstrings | Sciatic (tibial division) | L5–S2 |
| Dorsiflexion | Tibialis anterior | Deep fibular | L4–L5 |
| Plantarflexion | Gastrocnemius, soleus | Tibial | S1–S2 |
| Foot eversion | Fibularis longus & brevis | Superficial fibular | L5–S1 |
| Foot inversion | Tibialis anterior & posterior | Deep fibular (ant.), tibial (post.) | L4–L5 |
Dermatome Key Landmarks
| Dermatome | Landmark | Reflex |
|---|---|---|
| C5 | Lateral arm (deltoid area) | Biceps reflex |
| C6 | Thumb, lateral forearm | Brachioradialis reflex |
| C7 | Middle finger | Triceps reflex |
| C8 | Ring & little finger | — |
| T1 | Medial arm | — |
| T4 | Nipple | — |
| T10 | Umbilicus | — |
| L1 | Inguinal region | Cremasteric reflex |
| L4 | Medial leg, medial malleolus | Patellar (knee jerk) reflex |
| L5 | Dorsum of foot, great toe | — |
| S1 | Lateral foot, sole | Achilles (ankle jerk) reflex |
| S2–S4 | Perianal ("saddle") region | Anal wink, bulbocavernosus |
Arterial Blood Supply: Key Upper & Lower Limb Arteries
| Artery | Origin | Key Branches / Territory | Clinical Significance |
|---|---|---|---|
| Axillary | Continuation of subclavian at lateral border of 1st rib | Thoracoacromial, lateral thoracic, subscapular, circumflex humeral | Anterior shoulder dislocation can injure the artery; posterior circumflex humeral accompanies axillary nerve |
| Brachial | Continuation of axillary at inferior border of teres major | Profunda brachii (with radial nerve in spiral groove), radial and ulnar arteries | Blood pressure measurement; at risk in supracondylar fracture |
| Radial | Brachial artery bifurcation in cubital fossa | Superficial palmar branch, princeps pollicis | Pulse at wrist (radial styloid); Allen test for palmar arch patency before radial artery cannulation |
| Femoral | Continuation of external iliac below inguinal ligament | Profunda femoris (lateral/medial circumflex femoral), descending genicular | Catheterization site; pulse at midinguinal point; profunda femoris is the main supply to the thigh |
| Popliteal | Continuation of femoral through adductor hiatus | Genicular branches, anterior tibial, posterior tibial (fibular) | At risk in posterior knee dislocation; ABI < 0.9 indicates PAD |
| Anterior tibial / Dorsalis pedis | Popliteal → anterior tibial passes above interosseous membrane → dorsalis pedis on dorsum of foot | Anterior compartment supply; arcuate artery of foot | Dorsalis pedis pulse; absent in ~10% of normals |
| Posterior tibial | Popliteal bifurcation | Fibular artery, medial & lateral plantar arteries | Pulse behind medial malleolus; terminal branches supply the sole |
Cranial Nerve Reflexes
| Reflex | Afferent | Efferent | Test |
|---|---|---|---|
| Pupillary light reflex | CN II (optic) | CN III (oculomotor) | Shine light → bilateral pupil constriction |
| Corneal reflex | CN V1 (ophthalmic) | CN VII (facial) | Touch cornea → bilateral blink |
| Jaw jerk reflex | CN V3 (mandibular) | CN V3 (mandibular) | Tap chin → jaw closure; hyperactive in UMN lesions |
| Gag reflex | CN IX (glossopharyngeal) | CN X (vagus) | Touch posterior pharynx → gag |
| Vestibulo-ocular reflex (VOR) | CN VIII (vestibulocochlear) | CN III, IV, VI | Head rotation → conjugate eye movement opposite direction |
Erb point = upper trunk (C5–C6); Klumpke = lower trunk (C8–T1). Thenar atrophy = median nerve (carpal tunnel). Claw hand = ulnar nerve (more pronounced with distal lesion "ulnar paradox"). Wrist drop = radial nerve. Foot drop = common fibular nerve. Trendelenburg gait = superior gluteal nerve (gluteus medius weakness; pelvis drops to contralateral side). Winged scapula = long thoracic nerve. Ape hand = median nerve (loss of thenar opposition). Hand of benediction = median nerve proximal lesion (cannot flex digits 2–3 when making a fist).
Muscles of the Back
| Layer | Key Muscles | Innervation | Action |
|---|---|---|---|
| Superficial (extrinsic) | Trapezius, latissimus dorsi, rhomboids, levator scapulae | Accessory (XI) for trapezius; thoracodorsal for latissimus; dorsal scapular for rhomboids/levator | Move the upper limb and shoulder girdle |
| Intermediate (extrinsic) | Serratus posterior superior & inferior | Intercostal nerves | Assist respiration (questionable clinical significance) |
| Deep (intrinsic) | Erector spinae (iliocostalis, longissimus, spinalis), transversospinales (semispinalis, multifidus, rotatores) | Dorsal rami of spinal nerves | Extend and rotate the vertebral column; postural muscles |
Autonomic Nervous System Quick Reference
| Feature | Sympathetic ("Fight or Flight") | Parasympathetic ("Rest and Digest") |
|---|---|---|
| Origin | Thoracolumbar (T1–L2 lateral horn) | Craniosacral (CN III, VII, IX, X + S2–S4) |
| Preganglionic neuron | Short; synapses in paravertebral (sympathetic chain) or prevertebral ganglia | Long; synapses in ganglia near or within target organ |
| Postganglionic neuron | Long; releases norepinephrine (except sweat glands: ACh) | Short; releases acetylcholine (ACh) |
| Pupil | Mydriasis (dilation; dilator pupillae) | Miosis (constriction; sphincter pupillae via CN III) |
| Heart | Increases rate and contractility (beta-1) | Decreases rate (vagal tone via CN X) |
| Bronchi | Bronchodilation (beta-2) | Bronchoconstriction (M3) |
| GI tract | Decreases motility and secretion; contracts sphincters | Increases motility and secretion; relaxes sphincters |
| Bladder | Relaxes detrusor; contracts internal urethral sphincter (retention) | Contracts detrusor; relaxes internal sphincter (micturition) |
Disruption of the sympathetic pathway at any level produces ipsilateral ptosis (mild; loss of Mueller muscle tone), miosis (loss of pupil dilation), and anhidrosis (loss of sweating — face only if lesion is preganglionic; entire face and arm if central). Causes: central (stroke, syringomyelia), preganglionic (Pancoast tumor at lung apex compressing T1 sympathetic fibers, neck surgery), postganglionic (carotid artery dissection, cavernous sinus lesion). Cocaine test: in Horner syndrome, the affected pupil does NOT dilate (cocaine blocks NE reuptake, but no NE is being released).
Anatomical Mnemonics Master List
| Mnemonic | What It Encodes |
|---|---|
| "Robert Taylor Drinks Cold Beer" | Brachial plexus: Roots, Trunks, Divisions, Cords, Branches |
| "SITS" | Rotator cuff: Supraspinatus, Infraspinatus, Teres minor, Subscapularis |
| "NAVEL" (lateral to medial) | Femoral triangle contents: Nerve, Artery, Vein, Empty space, Lymphatics |
| "DAB / PAD" | Dorsal interossei ABduct; Palmar interossei ADduct |
| "SAD PUCKER" | Retroperitoneal organs |
| "C3, 4, 5 keeps the diaphragm alive" | Phrenic nerve roots |
| "I 8, 10 Eggs At 12" | Diaphragm openings: IVC at T8, Esophagus at T10, Aorta at T12 |
| "Water under the bridge" | Ureter passes under the uterine artery |
| "SCALP" | Scalp layers: Skin, Connective tissue, Aponeurosis, Loose CT, Pericranium |
| "Some Say Marry Money But My Brother Says Big Brains Matter More" | Cranial nerves: Sensory/Motor/Both for each CN I–XII |
Visual Field Defects & Anatomical Localization
| Lesion Site | Visual Field Defect | Common Cause |
|---|---|---|
| Optic nerve (CN II) | Ipsilateral monocular blindness (anopia) | Optic neuritis (MS), tumor compressing optic nerve |
| Optic chiasm (central fibers) | Bitemporal hemianopia | Pituitary adenoma compressing chiasm from below |
| Optic tract | Contralateral homonymous hemianopia | Stroke, tumor |
| Meyer loop (temporal lobe) | Contralateral homonymous superior quadrantanopia ("pie in the sky") | MCA stroke affecting temporal lobe |
| Dorsal optic radiation (parietal lobe) | Contralateral homonymous inferior quadrantanopia ("pie on the floor") | MCA stroke affecting parietal lobe |
| Occipital cortex (PCA territory) | Contralateral homonymous hemianopia with macular sparing | PCA stroke (macular region has dual blood supply from MCA and PCA) |
Facial Nerve (CN VII) Pathway & Lesion Levels
The facial nerve has a complex course: motor nucleus in pons → exits at cerebellopontine angle (with CN VIII) → enters internal acoustic meatus → facial canal through temporal bone → gives off greater petrosal nerve (lacrimation) → nerve to stapedius (dampens sound) → chorda tympani (taste to anterior 2/3 tongue, salivation to sublingual/submandibular glands) → exits through stylomastoid foramen → passes through parotid gland → branches to muscles of facial expression.
| Lesion Level | Findings in Addition to Facial Paralysis |
|---|---|
| Above greater petrosal nerve | Loss of lacrimation + hyperacusis + loss of taste + facial paralysis |
| Below greater petrosal, above stapedius | Hyperacusis + loss of taste + facial paralysis (lacrimation intact) |
| Below stapedius, above chorda tympani | Loss of taste + facial paralysis (lacrimation and stapedius reflex intact) |
| Below chorda tympani (stylomastoid foramen) | Facial paralysis only (Bell palsy pattern: all ipsilateral facial muscles) |
| UMN lesion (cortex/internal capsule) | Contralateral lower face paralysis only (forehead spared because it receives bilateral UMN input) |