Bacteriology, virology, mycology, parasitology, antimicrobial mechanisms, resistance patterns, and every organism, virulence factor, diagnostic test, and treatment principle across the full scope of medical microbiology.
01 Overview & Scope of Medical Microbiology
Medical microbiology is the study of organisms that cause human disease — bacteria, viruses, fungi, and parasites — and the host responses they provoke. It is the scientific foundation of infectious disease medicine and underpins rational antimicrobial prescribing, infection prevention, and public health policy. Every clinical specialty encounters infectious diseases, making microbiology one of the most cross-cutting foundational sciences.
Why This Matters
Infectious diseases remain the leading cause of death worldwide. Understanding the organisms, their virulence mechanisms, diagnostic approaches, and treatment principles is essential for every physician regardless of specialty. Microbiology is heavily tested on USMLE Step 1 and Step 2 CK.
Obligate intracellular, DNA or RNA genome, no ribosomes
20–300 nm
HIV, influenza, SARS-CoV-2, HSV
Fungi
Eukaryotic, chitin cell wall, ergosterol membrane
2–10 µm (yeast)
Candida, Aspergillus, Histoplasma
Parasites
Eukaryotic; protozoa (single-celled) and helminths (multicellular)
1 µm–10 m
Plasmodium, Giardia, Ascaris
Prions
Misfolded proteins (PrPSc); no nucleic acid
<100 nm
Creutzfeldt–Jakob disease (CJD), kuru
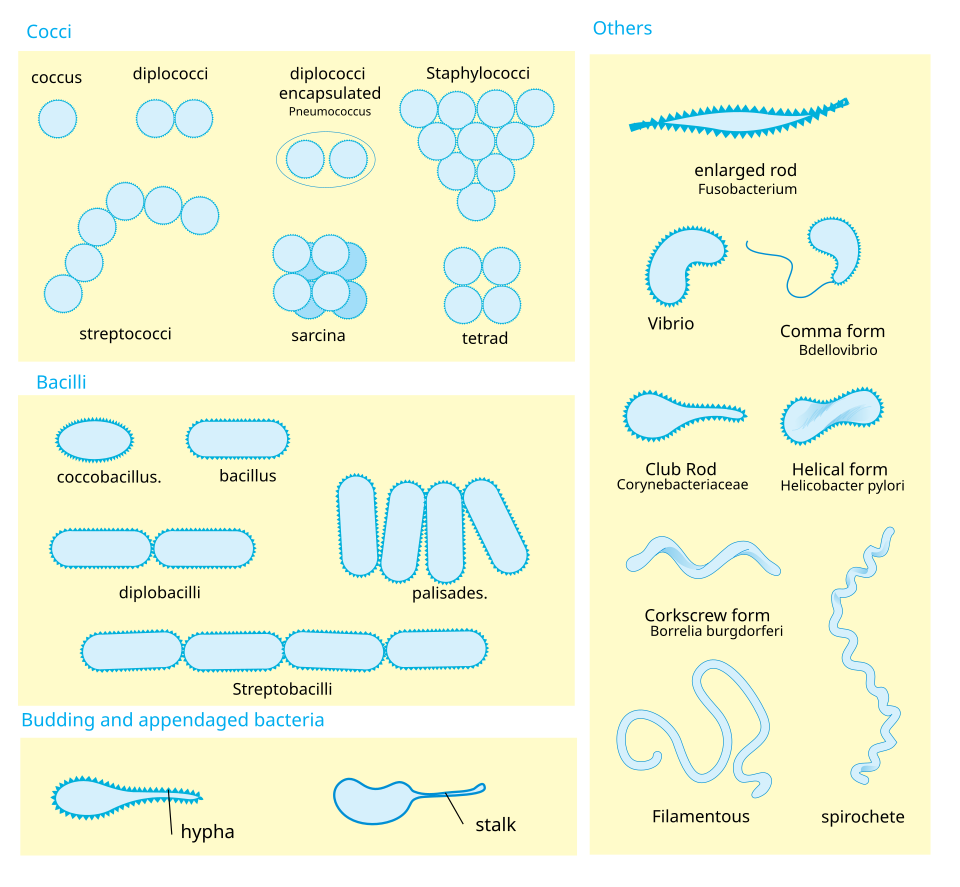
Figure 1 — Major Categories of Human Pathogens. Schematic overview of the principal morphologic types encountered in medical microbiology, including cocci, rods, spirals, viruses, yeasts, molds, protozoa, and helminths.
Koch Postulates & Modern Modifications
Robert Koch established four criteria for attributing disease to a specific organism: (1) the organism is found in all cases of the disease; (2) it can be isolated and grown in pure culture; (3) inoculation into a susceptible host reproduces the disease; (4) the organism is re-isolated from the experimental host. Molecular Koch postulates extend these criteria to virulence genes using molecular genetics (e.g., gene knockout eliminates virulence, complementation restores it).
Prions are unique pathogens — they contain no nucleic acid, cannot be cultured, and are resistant to standard sterilization. They cause transmissible spongiform encephalopathies (TSEs) through conversion of normal PrPC to the misfolded PrPSc isoform. Diagnosis is by brain biopsy showing spongiform change; 14-3-3 protein and RT-QuIC assay in CSF are supportive.
02 Core Principles & Classification
Microorganisms are classified using a hierarchical taxonomy (domain, phylum, class, order, family, genus, species). In clinical practice, bacteria are classified by Gram stain (positive vs. negative), morphology (cocci, rods, spirals), oxygen requirements (aerobic, anaerobic, facultative), and biochemical tests (catalase, coagulase, oxidase, urease).
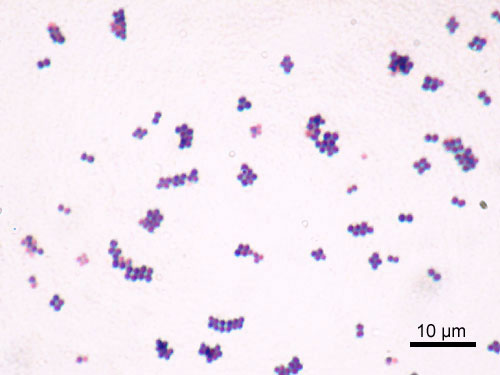
Gram Stain Fundamentals
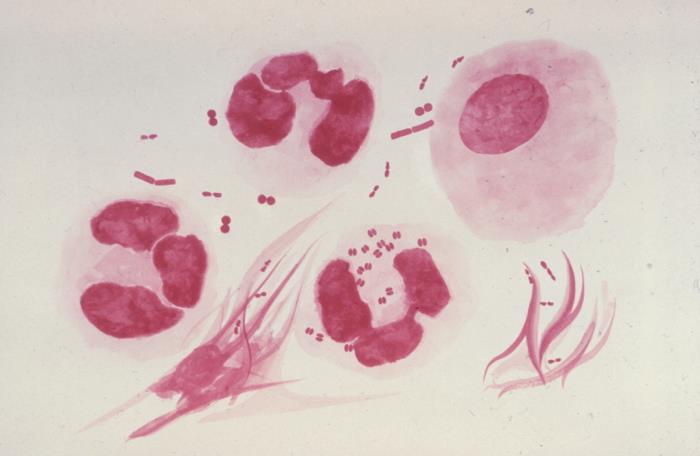
The Gram stain is the single most important rapid diagnostic test in clinical microbiology. Crystal violet binds peptidoglycan; iodine fixes the dye; alcohol/acetone decolorizes thin-walled organisms; safranin counterstains decolorized cells pink.
Property
Gram-Positive
Gram-Negative
Stain color
Purple/blue
Pink/red
Peptidoglycan thickness
20–80 nm (thick)
1–3 nm (thin)
Outer membrane
Absent
Present (contains LPS)
Teichoic acids
Present
Absent
Lipopolysaccharide (endotoxin)
Absent
Present (lipid A = toxic moiety)
Periplasmic space
Narrow
Wide
Susceptibility to penicillin
Generally more susceptible
Outer membrane barrier
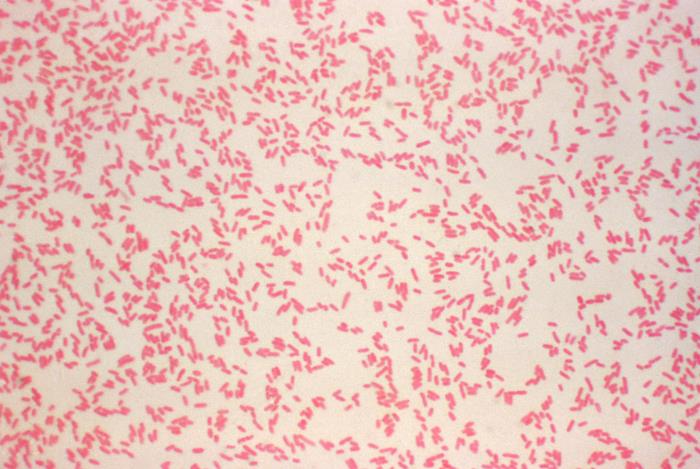
Figure 2 — Gram Stain Results. Photomicrograph demonstrating the Gram stain, the single most important rapid diagnostic test in clinical microbiology. Gram-positive organisms retain crystal violet and appear purple; Gram-negative organisms are decolorized and counterstained pink by safranin.
Oxygen Requirements
Category
Definition
Examples
Obligate aerobe
Requires O2 for growth
Mycobacterium tuberculosis, Nocardia, Pseudomonas
Obligate anaerobe
Killed by O2; lacks catalase and superoxide dismutase
S. pneumoniae (sensitive) vs. other alpha-hemolytic strep (resistant)
Bacitracin
Inhibits growth
S. pyogenes (GAS; sensitive) vs. other beta-hemolytic strep
Bile solubility
Autolysis in bile salts
S. pneumoniae (soluble) vs. Enterococcus (resistant)
Quick mnemonic for catalase-positive organisms: Staphylococci are catalase-positive (bubbles); Streptococci and Enterococci are catalase-negative. Next, coagulase separates S. aureus (coagulase-positive) from coagulase-negative staphylococci (CoNS) such as S. epidermidis and S. saprophyticus.
Bacterial Genetics & Horizontal Gene Transfer
Bacteria acquire resistance and virulence genes through horizontal gene transfer mechanisms that operate independently of vertical (parent-to-offspring) inheritance:
Mechanism
Description
Clinical Significance
Transformation
Uptake of free (naked) DNA from the environment
S. pneumoniae (Griffith experiment); penicillin resistance via PBP gene uptake
Transduction
DNA transfer via bacteriophage (virus)
Generalized: random DNA packaging; Specialized: adjacent genes transferred (e.g., shiga-like toxin in EHEC, diphtheria toxin from β-prophage)
Conjugation
Direct cell-to-cell transfer via sex pilus (F plasmid)
Plasmid-mediated resistance (ESBL genes, carbapenemase genes like KPC, NDM); most clinically significant mechanism
Transposition
Movement of transposable elements ("jumping genes") within or between DNA molecules
vanA gene in VRE; insertion sequences disrupting porin genes
Figure 3 — Selective and Differential Culture Media. MacConkey agar differentiates Gram-negative bacteria by lactose fermentation. Lactose fermenters (e.g., E. coli, Klebsiella) produce pink colonies, while non-fermenters (e.g., Salmonella, Shigella) remain colorless.
Microbial Culture Media Summary
Medium
Type
Selects/Differentiates
Blood agar
Enriched, differential
Hemolysis patterns (α, β, γ)
Chocolate agar
Enriched (lysed RBCs release factors X and V)
Neisseria, Haemophilus
MacConkey agar
Selective and differential
Gram-negative rods; lactose fermenters (pink) vs. non-fermenters (colorless)
Eosin methylene blue (EMB)
Selective and differential
Gram-negative rods; E. coli = green metallic sheen
Thayer–Martin (VCN) agar
Selective chocolate agar
Neisseria (vancomycin, colistin, nystatin inhibit normal flora)
Hektoen enteric / XLD agar
Selective and differential
Salmonella and Shigella (H2S production)
Mannitol salt agar
Selective (7.5% NaCl)
Staphylococci; S. aureus ferments mannitol (yellow)
Bile esculin agar
Selective and differential
Enterococcus and S. bovis (group D strep) — hydrolyze esculin in bile
Diagnostic Approach Algorithm
Gram stain → morphology (cocci vs. rods, clusters vs. chains) → catalase test (if Gram-positive cocci) → coagulase (if catalase-positive) or hemolysis/Lancefield grouping (if catalase-negative). For Gram-negative organisms: oxidase test separates fermenters (Enterobacterales, oxidase-negative) from non-fermenters (Pseudomonas, oxidase-positive). Lactose fermentation on MacConkey further differentiates Enterobacterales.
03 Bacterial Cell Structure & Physiology
Understanding bacterial cell architecture is essential because virtually every antibiotic targets a specific structural or metabolic component. The cell wall, cell membrane, ribosomes, and nucleic acid machinery are the principal drug targets.
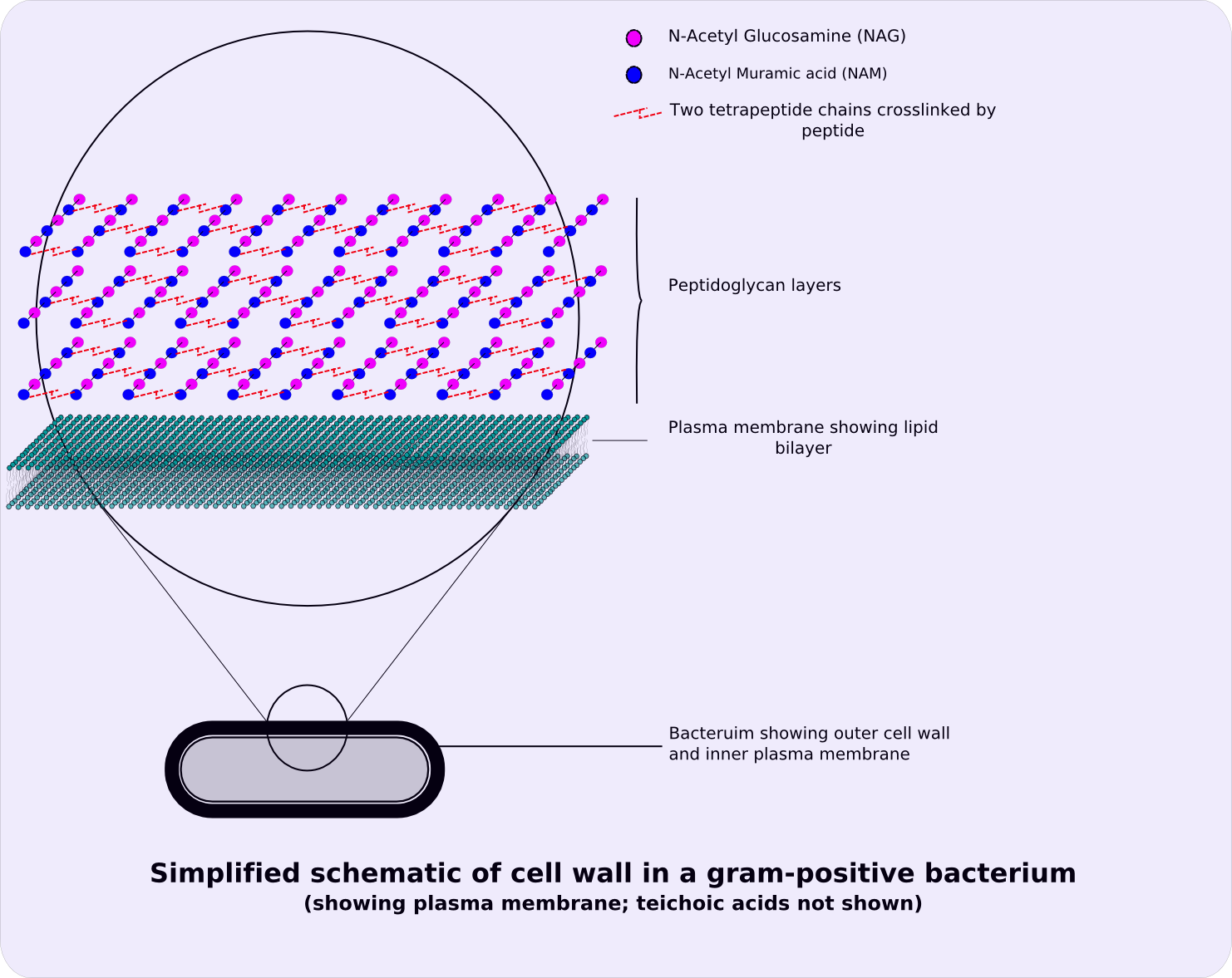
Figure 4 — Gram-Positive vs. Gram-Negative Cell Wall Architecture. Gram-positive bacteria have a thick peptidoglycan layer with teichoic acids but no outer membrane. Gram-negative bacteria have a thin peptidoglycan layer sandwiched between an inner membrane and an outer membrane containing lipopolysaccharide (LPS/endotoxin).
Cell Wall Components
Structure
Function
Drug Target
Peptidoglycan
Structural rigidity; NAG-NAM polymer cross-linked by peptide bridges
Lecithinase (phospholipase C) → destroys cell membranes
Gas gangrene (myonecrosis)
Erythrogenic toxin (SpeA/B/C)
S. pyogenes
Superantigen → rash and fever
Scarlet fever, streptococcal TSS
Toxin Classification Memory Aid
ADP-ribosylating toxins — remember "Cholera, Diphtheria, Pertussis, Pseudomonas" all ADP-ribosylate host proteins. Cholera and heat-labile toxin target Gs (↑cAMP); pertussis targets Gi (↑cAMP by a different mechanism); diphtheria and Pseudomonas exotoxin A target EF-2 (↓protein synthesis).
04 Staphylococci
Staphylococci are Gram-positive cocci in clusters, catalase-positive, and facultative anaerobes. S. aureus is the most virulent species and is distinguished from coagulase-negative staphylococci (CoNS) by the coagulase test.
Figure 5 — Staphylococcus aureus Gram Stain. Gram-positive cocci arranged in grape-like clusters, the hallmark morphology of staphylococci. S. aureus is catalase-positive and coagulase-positive, distinguishing it from coagulase-negative staphylococci.
Staphylococcus aureus
Feature
Detail
Gram stain
Gram-positive cocci in clusters
Key tests
Catalase (+), coagulase (+), mannitol fermentation (+), golden pigment on agar
Virulence factors
Protein A, coagulase, hemolysins (α, β, γ, δ), TSST-1, exfoliative toxin, PVL (Panton–Valentine leukocidin), enterotoxins (A–E)
S. aureus food poisoning is caused by preformed heat-stable enterotoxin — symptoms occur within 1–6 hours of ingestion (rapid onset vomiting, no fever). This distinguishes it from most other bacterial food poisoning, which has a longer incubation.
UTI in sexually active young women (second most common cause after E. coli)
S. lugdunensis
More virulent than typical CoNS
Aggressive native valve endocarditis; treat like S. aureus
S. saprophyticus is novobiocin-resistant — this distinguishes it from S. epidermidis (novobiocin-sensitive). Think "SaP = Pee" for its association with UTI.
Staphylococcal Toxin-Mediated Diseases
Disease
Toxin
Mechanism
Clinical Features
Toxic shock syndrome
TSST-1 (superantigen)
Nonspecific crosslinking of MHC II and TCR → massive T-cell activation → cytokine storm
High fever, diffuse macular rash with desquamation, hypotension, multiorgan involvement; associated with tampon use or wound packing
Scalded skin syndrome (SSSS)
Exfoliative toxin (ET-A, ET-B)
Serine protease cleaving desmoglein-1 in granular layer of epidermis
Widespread blistering and exfoliation in neonates/children; Nikolsky sign positive; no mucosal involvement (distinguishes from TEN)
Food poisoning
Enterotoxins (A most common)
Preformed heat-stable toxin → stimulates vagus nerve and CNS vomiting center
Large flaccid bullae on skin; more common in children
05 Streptococci & Enterococci
Streptococci are Gram-positive cocci in chains or pairs, catalase-negative. They are classified by hemolysis pattern (α, β, γ) and Lancefield grouping (carbohydrate antigens A–V).
Figure 6 — Hemolysis Patterns on Blood Agar. Streptococci are classified by their hemolysis on blood agar: alpha-hemolysis (green, partial clearing), beta-hemolysis (complete clearing), and gamma-hemolysis (no hemolysis). This distinction is the first step in streptococcal identification.
Hemolysis Patterns
Pattern
Appearance
Organisms
α-hemolysis
Green/partial clearing around colonies
S. pneumoniae, S. viridans group
β-hemolysis
Complete clearing around colonies
S. pyogenes (GAS), S. agalactiae (GBS)
γ-hemolysis
No hemolysis
Enterococcus, some group D strep
Figure 7 — Streptococcus pneumoniae Gram Stain. Lancet-shaped Gram-positive diplococci characteristic of S. pneumoniae, the leading cause of community-acquired pneumonia, bacterial meningitis, otitis media, and sinusitis. Identified by optochin sensitivity and bile solubility.
Major Streptococcal Species
Organism
Group
Key Features
Diseases
Treatment
S. pyogenes
Group A
Bacitracin-sensitive, PYR (+), M protein, SpeA superantigen
Ampicillin ± gentamicin; vancomycin for resistant strains; linezolid or daptomycin for VRE
Rheumatic Fever Criteria (Jones)
Major: Joint involvement (migratory polyarthritis), Carditis, Nodules (subcutaneous), Erythema marginatum, Sydenham chorea — mnemonic "JONES." Minor: Fever, elevated ESR/CRP, prolonged PR interval, arthralgias. Requires evidence of prior GAS infection + 2 major OR 1 major + 2 minor criteria.
Rheumatic fever follows GAS pharyngitis only (not skin infections). Post-streptococcal glomerulonephritis can follow either pharyngitis or skin infection. Penicillin prophylaxis prevents recurrent rheumatic fever but does not prevent initial PSGN episodes.
Streptococcal Post-Infectious Syndromes
Syndrome
Pathogenesis
Timing
Key Features
Acute rheumatic fever
Molecular mimicry (M protein resembles cardiac myosin, laminin, and brain tissue)
Type III hypersensitivity (immune complex deposition in glomeruli)
1–3 weeks after pharyngitis; 3–6 weeks after skin infection
Cola-colored urine (hematuria), periorbital edema, hypertension, low C3; "lumpy-bumpy" IF pattern (subepithelial humps on EM)
PANDAS
Autoimmune neuropsychiatric disorder associated with streptococcal infection
Days to weeks after GAS infection
Abrupt onset OCD and/or tics in prepubertal children
Streptococcus bovis (gallolyticus) & Colon Cancer
S. bovis/gallolyticus bacteremia or endocarditis is strongly associated with colorectal carcinoma or other GI malignancies. Every patient with S. bovis bacteremia requires a colonoscopy. S. bovis is a group D streptococcus that grows in bile but NOT in 6.5% NaCl (distinguishing it from Enterococcus).
06 Gram-Positive Rods & Anaerobes
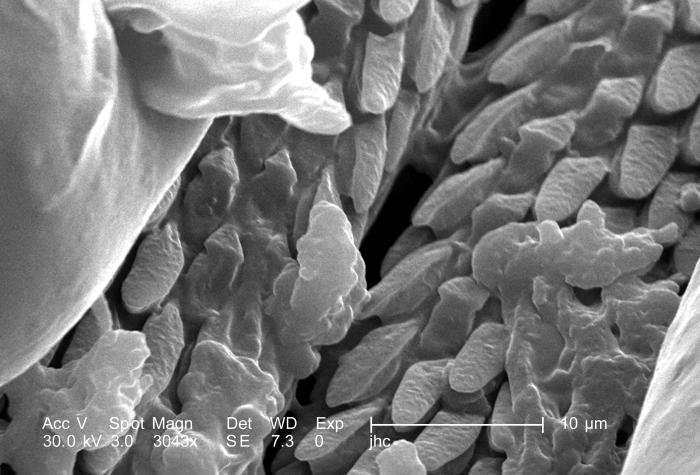
Gram-positive rods include aerobic and anaerobic species. The spore-forming genera (Bacillus, Clostridium) are especially important because spores confer environmental resistance.
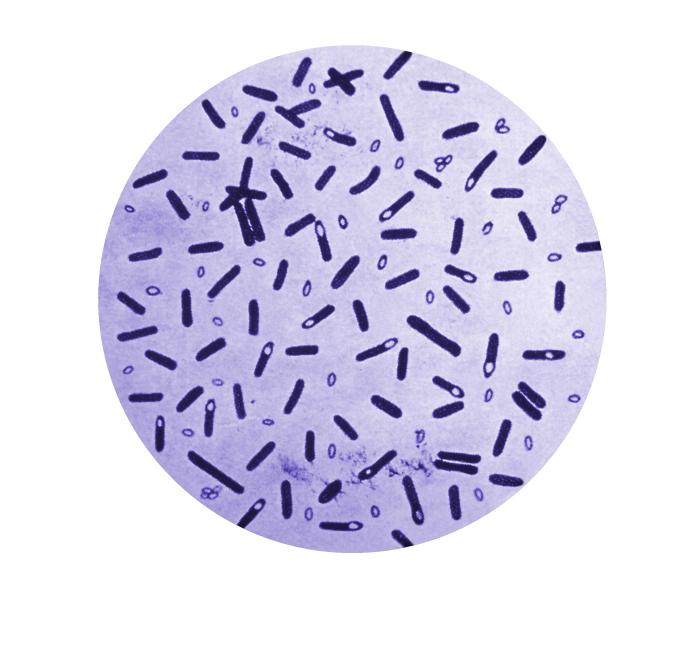
Figure 8 — Clostridium Species Morphology. Gram-positive, spore-forming anaerobic rods. The clostridia are responsible for tetanus (C. tetani), botulism (C. botulinum), gas gangrene (C. perfringens), and pseudomembranous colitis (C. difficile). Endospores confer environmental resistance.
Aerobic Gram-Positive Rods
Organism
Key Features
Disease
Treatment
Bacillus anthracis
Spore-forming, encapsulated (poly-D-glutamate — only polypeptide capsule), nonhemolytic
Cutaneous anthrax (black eschar), pulmonary anthrax (woolsorter's disease), GI anthrax
Ciprofloxacin or doxycycline
Bacillus cereus
Spore-forming, produces emetic and diarrheagenic toxins
Antitoxin (adults); BabyBIG (infant botulism); supportive (intubation if needed)
C. perfringens
Alpha toxin (lecithinase/phospholipase C)
Gas gangrene (myonecrosis), food poisoning (watery diarrhea)
Clindamycin + penicillin + surgical debridement
C. difficile
Toxin A (enterotoxin) + Toxin B (cytotoxin)
Antibiotic-associated pseudomembranous colitis
Vancomycin (oral) or fidaxomicin (oral); metronidazole for non-severe; bezlotoxumab for recurrence prevention
Listeria is naturally resistant to cephalosporins — this is why empiric meningitis therapy in neonates and adults >50 years must include ampicillin (in addition to ceftriaxone + vancomycin) to cover Listeria. Food sources include unpasteurized dairy, deli meats, and soft cheeses.
Figure 9 — Cutaneous Anthrax (Bacillus anthracis). Painless black eschar characteristic of cutaneous anthrax. B. anthracis is the only bacterium with a polypeptide (poly-D-glutamate) capsule. Pulmonary anthrax presents with widened mediastinum on chest radiograph.
Actinomyces & Other Gram-Positive Anaerobes
Organism
Key Features
Disease
Treatment
Actinomyces israelii
Branching filamentous rods; NOT acid-fast (distinguishes from Nocardia); anaerobic; normal oral flora
Cervicofacial actinomycosis (draining sinus tracts with "sulfur granules" in jaw); thoracic, abdominal, pelvic (IUD-associated)
Penicillin G (prolonged course, 6–12 months); surgical drainage of abscesses
Clostridioides difficile
Spore-forming; toxigenic strains produce toxin A (enterotoxin) and toxin B (cytotoxin); NAP1/B1/027 hypervirulent strain produces binary toxin
Antibiotic-associated diarrhea, pseudomembranous colitis; risk factors: antibiotics (clindamycin, fluoroquinolones, cephalosporins), PPI use, hospitalization, age >65
Initial non-severe: vancomycin PO or fidaxomicin PO; severe: vancomycin PO; fulminant: vancomycin PO + IV metronidazole ± rectal vancomycin; recurrent: fidaxomicin, bezlotoxumab, fecal microbiota transplant
Nocardia vs. Actinomyces
Both are branching filamentous Gram-positive rods, but they differ in critical ways: Nocardia is aerobic, weakly acid-fast, found in soil, and causes pulmonary/brain disease in immunocompromised patients (treat with TMP-SMX). Actinomyces is anaerobic, NOT acid-fast, is normal oral flora, and causes draining sinus tracts (treat with penicillin). Confusion between these two is a common board question trap.
07 Enterobacterales
The Enterobacterales (formerly Enterobacteriaceae) are Gram-negative rods, facultative anaerobes, oxidase-negative, and glucose-fermenting. They are the most common cause of urinary tract infections, intra-abdominal infections, and Gram-negative bacteremia.
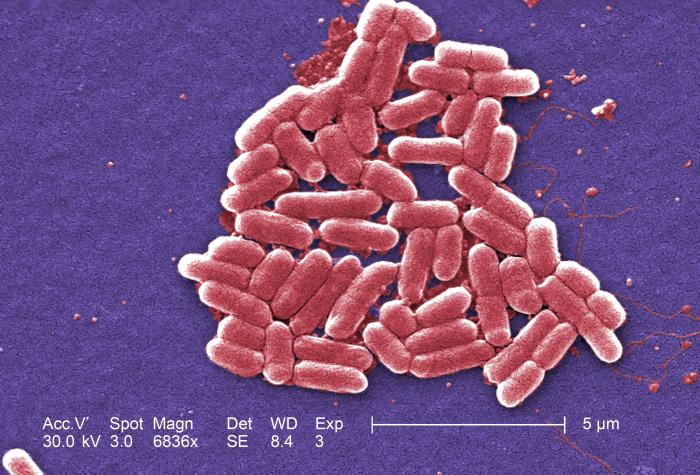
Figure 10 — E. coli on EMB Agar. E. coli produces a characteristic green metallic sheen on eosin methylene blue (EMB) agar due to vigorous lactose fermentation. E. coli is the most common cause of urinary tract infections and Gram-negative bacteremia.
Key Enterobacterales
Organism
Key Features
Diseases
Notes
E. coli
Most common GNR in clinical specimens; lactose-fermenter, green metallic sheen on EMB agar
Comma-/S-shaped, microaerophilic, grows at 42°C, oxidase (+)
#1 cause of bacterial gastroenteritis in US; bloody diarrhea; associated with Guillain–Barré syndrome (molecular mimicry with ganglioside GM1) and reactive arthritis
Triple therapy: PPI + clarithromycin + amoxicillin (or metronidazole); bismuth quadruple therapy as alternative; urea breath test for diagnosis/cure confirmation
Vibrio vulnificus causes rapidly progressive cellulitis and sepsis in patients with liver disease (cirrhosis) or iron overload (hemochromatosis) who eat raw oysters or sustain saltwater wound exposure. Mortality exceeds 50% in septic patients. Warn cirrhotic patients to avoid raw shellfish.
Non-fermenters are Gram-negative rods that cannot ferment glucose. They are typically oxidase-positive and are important causes of nosocomial infections, particularly in the ICU. Intrinsic multidrug resistance is a hallmark.
Figure 11 — Pseudomonas aeruginosa Culture. P. aeruginosa produces characteristic blue-green pigment (pyocyanin) on culture media and has a grape-like odor. It is a leading cause of hospital-acquired pneumonia, burn wound infections, and chronic pulmonary infections in cystic fibrosis.
CF pulmonary infections (poor prognosis, contraindication to lung transplant)
TMP-SMX, meropenem
Pseudomonas must be covered empirically in neutropenic fever, ventilator-associated pneumonia, and CF exacerbations. Ecthyma gangrenosum — necrotic skin lesions with black eschar in a febrile neutropenic patient — is pathognomonic for Pseudomonas bacteremia until proven otherwise.
Anti-Pseudomonal Antibiotics
Not all beta-lactams cover Pseudomonas. The following agents have reliable anti-pseudomonal activity:
Class
Anti-Pseudomonal Agent(s)
Non-Anti-Pseudomonal (Common Pitfall)
Penicillins
Piperacillin-tazobactam, ticarcillin-clavulanate
Ampicillin, amoxicillin, nafcillin
Cephalosporins
Ceftazidime (3rd gen), cefepime (4th gen)
Ceftriaxone (3rd gen — NOT anti-pseudomonal), cefazolin
Carbapenems
Meropenem, imipenem, doripenem
Ertapenem (does NOT cover Pseudomonas)
Fluoroquinolones
Ciprofloxacin (most potent), levofloxacin
Moxifloxacin (no Pseudomonas coverage)
Aminoglycosides
Tobramycin, amikacin, gentamicin
—
Monobactams
Aztreonam
—
09 Gram-Negative Cocci & Fastidious Organisms
Figure 12 — Neisseria Gram Stain. Gram-negative diplococci (kidney-bean shaped), often seen intracellularly within polymorphonuclear leukocytes. N. gonorrhoeae ferments only glucose; N. meningitidis ferments both glucose and maltose.
Cellulitis/wound infection after animal bite (rapid onset, <24 hours)
Amoxicillin-clavulanate
N. meningitidis ferments both glucose and maltose; N. gonorrhoeae ferments only glucose. Waterhouse–Friderichsen syndrome (bilateral adrenal hemorrhage from DIC) is a dreaded complication of meningococcemia — presents with acute adrenal crisis, purpura fulminans, and cardiovascular collapse.
10 Anaerobic Gram-Negative Bacteria
Anaerobic Gram-negative bacteria are normal flora of the GI tract, oral cavity, and female genital tract. They cause disease when they gain access to normally sterile sites, often in the setting of disrupted mucosal barriers.
Organism
Key Features
Diseases
Treatment
Bacteroides fragilis
Most common anaerobic isolate in clinical specimens; polysaccharide capsule; β-lactamase producer
Foul-smelling discharge, gas in tissue, infection near mucosal surface, polymicrobial Gram stain, failure to grow on routine aerobic culture, abscess formation, history of aspiration. Anaerobes are the most common organisms in lung abscess and brain abscess.
11 Mycobacterium tuberculosis
M. tuberculosis is an obligate aerobe with a mycolic acid-rich cell wall that makes it acid-fast (Ziehl–Neelsen stain: red bacilli). It grows slowly (doubling time 15–20 hours; culture takes 2–6 weeks on Löwenstein–Jensen media). One-quarter of the world's population has latent TB infection.
Figure 13 — Acid-Fast (Ziehl–Neelsen) Stain for Mycobacterium tuberculosis. Acid-fast bacilli (red rods) against a blue background. The mycolic acid-rich cell wall of mycobacteria resists decolorization with acid-alcohol after staining with carbol fuchsin. Culture on Löwenstein–Jensen media takes 2–6 weeks.
Diagnosis
Test
Mechanism
Notes
TST (PPD/Mantoux)
Type IV (delayed-type) hypersensitivity to purified protein derivative
≥5 mm (HIV, close contacts, CXR changes); ≥10 mm (high-risk groups); ≥15 mm (low risk); read at 48–72 hrs
IGRA (QuantiFERON-TB Gold, T-SPOT)
Measures IFN-γ release by T cells after TB antigen stimulation
Not affected by prior BCG vaccination (more specific); single blood draw
AFB smear
Ziehl–Neelsen or auramine-rhodamine fluorescent stain
Rifampin is a potent CYP450 inducer — it reduces the efficacy of oral contraceptives, warfarin, HIV protease inhibitors, and many other drugs. Isoniazid is metabolized by N-acetyltransferase (NAT2): slow acetylators have higher drug levels and more toxicity (hepatitis, peripheral neuropathy).
12 Non-Tuberculous Mycobacteria
Organism
Key Features
Disease
Treatment
M. avium complex (MAC)
Most common NTM; disseminated in AIDS when CD4 <50
Disseminated MAC (fever, weight loss, hepatosplenomegaly, pancytopenia); pulmonary MAC (Lady Windermere syndrome)
Azithromycin + ethambutol ± rifabutin; azithromycin prophylaxis when CD4 <50
M. kansasii
Photochromogen (pigment in light)
Pulmonary disease resembling TB
Isoniazid + rifampin + ethambutol
M. marinum
Grows at 30°C (lower than body temp)
Fish tank granuloma (skin nodules on hands)
Ethambutol + clarithromycin or rifampin
M. leprae
Cannot be cultured in vitro; grows in armadillos and in cooler body sites (skin, peripheral nerves)
Leprosy: tuberculoid (Th1, few organisms, granulomas) vs. lepromatous (Th2, many organisms, leonine facies)
M. leprae infects Schwann cells — peripheral neuropathy is the hallmark. Tuberculoid leprosy has a strong Th1 response with few bacilli and well-formed granulomas; lepromatous has a Th2 response with many bacilli and poorly formed granulomas (failed cell-mediated immunity). Lepromin test is positive in tuberculoid but negative in lepromatous.
13 Spirochetes, Rickettsiae & Atypicals
Figure 14 — Primary Syphilis Chancre. Painless, clean-based ulcer at the site of Treponema pallidum inoculation. T. pallidum cannot be cultured; diagnosis relies on darkfield microscopy, serology (RPR/VDRL screening, FTA-ABS confirmation), and clinical findings.
Spirochetes
Organism
Key Features
Disease
Treatment
Treponema pallidum
Cannot be cultured; darkfield microscopy, FTA-ABS, RPR/VDRL
Figure 15 — Erythema Migrans (Lyme Disease). Expanding erythematous lesion with central clearing (bull's-eye rash), the hallmark of Stage 1 Lyme disease caused by Borrelia burgdorferi, transmitted by the Ixodes tick. This clinical finding is pathognomonic and does not require serologic confirmation to initiate treatment.
Atypical Bacteria (Cell-Wall-Deficient)
Organism
Key Features
Disease
Treatment
Mycoplasma pneumoniae
No cell wall (no peptidoglycan → beta-lactam resistant); smallest free-living organism; Eaton agar
Atypical (walking) pneumonia in young adults; cold agglutinins (IgM vs. RBC I antigen)
For all rickettsial diseases, doxycycline is the treatment of choice — even in children and pregnant women when the diagnosis is strongly suspected, because the mortality of untreated RMSF exceeds 20%. Do not wait for serologic confirmation to treat.
Inhalation of aerosols from animal products (no arthropod vector needed)
Q fever
Chlamydophila psittaci
Birds (parrots, parakeets)
Inhalation of dried bird droppings
Psittacosis (atypical pneumonia)
Bartonella in HIV/AIDS
Bartonella henselae and B. quintana cause bacillary angiomatosis in AIDS patients — vascular proliferative lesions of the skin that can mimic Kaposi sarcoma. Unlike KS (caused by HHV-8), bacillary angiomatosis is curable with antibiotics (doxycycline or erythromycin). Biopsy with Warthin–Starry silver stain shows clumps of bacteria. B. quintana also causes trench fever (transmitted by body lice) and culture-negative endocarditis in homeless populations.
14 DNA Viruses
DNA viruses generally replicate in the nucleus (exception: poxviruses replicate in cytoplasm — they carry their own DNA-dependent RNA polymerase). All DNA viruses are double-stranded except parvoviruses (ssDNA). All are icosahedral except poxviruses (complex). Mnemonic for enveloped DNA viruses: "HHPPox" — Herpesviruses, Hepadnaviruses, Poxviruses.
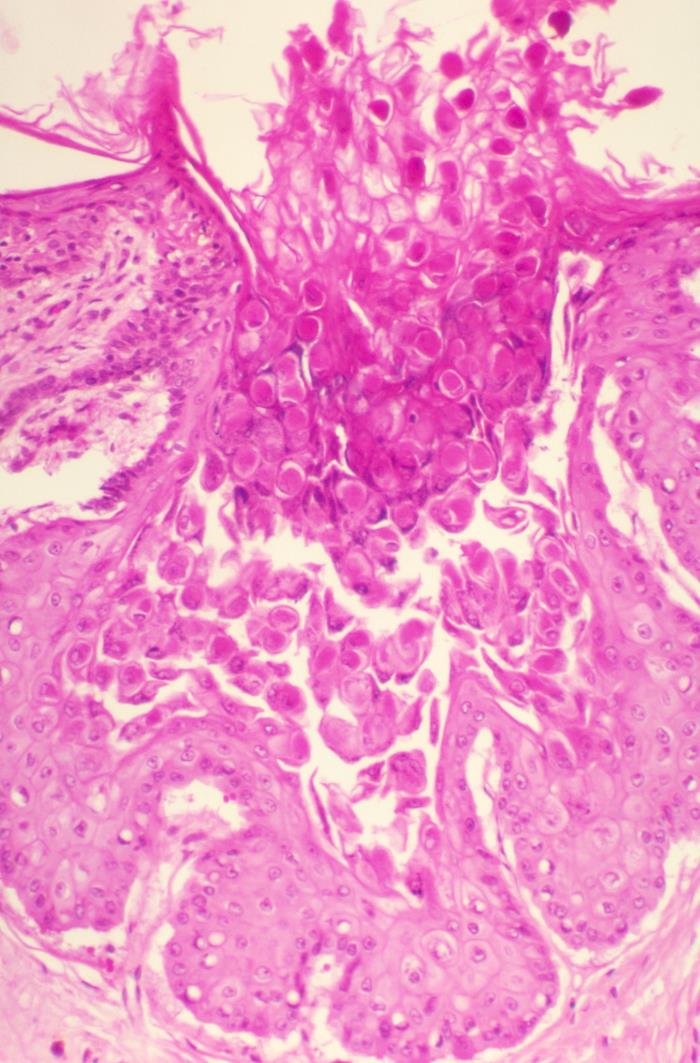
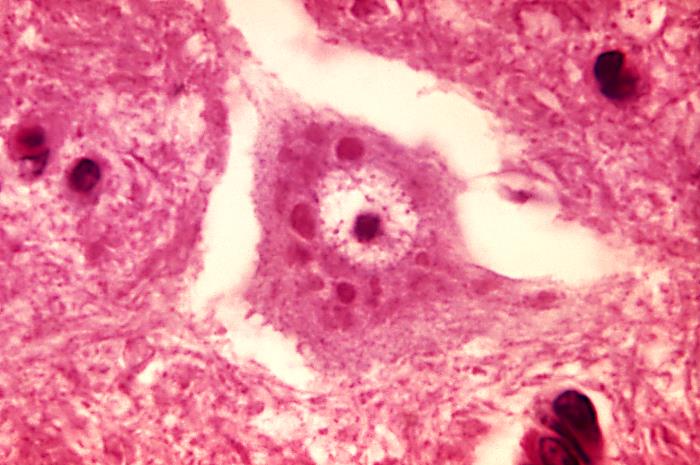
Figure 16 — Herpesvirus Cytopathic Effect. Multinucleated giant cells with Cowdry type A intranuclear inclusions, characteristic of herpes simplex virus (HSV) and varicella-zoster virus (VZV) infection. All herpesviruses establish latency and can reactivate.
Chronic inflammation → cirrhosis → HCC (always through cirrhosis, unlike HBV which can cause HCC without cirrhosis)
HTLV-1
ssRNA (retrovirus)
Adult T-cell leukemia/lymphoma
Tax protein activates NF-κB → T-cell proliferation
Vaccine-Preventable Cancers
HPV vaccine (9-valent Gardasil-9) prevents cervical, anal, and oropharyngeal cancers caused by high-risk HPV types 16 and 18 (plus 31, 33, 45, 52, 58). HBV vaccine prevents hepatitis B-associated hepatocellular carcinoma. These are the only two cancer-preventive vaccines currently in widespread use.
HSV encephalitis has a predilection for the temporal lobe — MRI shows temporal lobe hyperintensity. LP shows lymphocytic pleocytosis, elevated protein, and normal glucose; HSV PCR of CSF is the diagnostic test of choice. Start IV acyclovir empirically — do NOT wait for results.
15 RNA Viruses
RNA viruses are a diverse group. Most are single-stranded RNA; reoviruses are the exception (dsRNA). Negative-sense RNA viruses must carry their own RNA-dependent RNA polymerase (RdRp) to make mRNA. Positive-sense RNA viruses can serve directly as mRNA for translation.
Figure 17 — Measles (Rubeola) Rash. Maculopapular rash beginning on the face and spreading cephalocaudally. Measles presents with the classic triad of cough, coryza, and conjunctivitis, preceded by Koplik spots (pathognomonic white spots on buccal mucosa). Measles virus is a paramyxovirus requiring airborne precautions.
Negative-Sense ssRNA Viruses
Mnemonic: "Always Bring Polymerase" — negative-sense viruses always bring their own polymerase.
Aseptic meningitis (LCMV — hamster/mouse exposure); Lassa fever (West Africa)
Ribavirin for Lassa fever
Figure 18 — Rabies Virus — Negri Bodies. Eosinophilic intracytoplasmic inclusions (Negri bodies) in neurons, pathognomonic for rabies. The rabies virus is a bullet-shaped rhabdovirus. Post-exposure prophylaxis includes rabies immunoglobulin plus a four-dose vaccine series.
SARS-CoV-2, SARS-CoV, MERS-CoV, common cold coronaviruses
COVID-19: pneumonia, ARDS, multiorgan failure, long COVID
Largest RNA genome; remdesivir, nirmatrelvir/ritonavir (Paxlovid); mRNA vaccines
Caliciviridae
Norovirus
#1 cause of viral gastroenteritis worldwide (outbreaks in cruise ships, schools)
Non-enveloped; highly contagious; supportive care
Reoviridae
Rotavirus
#1 cause of severe infantile gastroenteritis worldwide
dsRNA (double-stranded — only dsRNA virus); non-enveloped; live oral vaccine
Only RNA virus that is double-stranded: rotavirus (Reoviridae). Only RNA virus with a segmented genome among common pathogens: influenza (Orthomyxoviridae) — segmentation enables antigenic shift through reassortment. Antigenic drift (point mutations) causes seasonal epidemics; antigenic shift (reassortment of genome segments) causes pandemics.
All RNA viruses (except influenza, which uses host nuclear machinery for mRNA capping) and poxviruses (DNA but cytoplasmic)
Viruses with reverse transcriptase
HIV (retrovirus, RNA → DNA), HBV (hepadnavirus, DNA → RNA → DNA)
Naked (non-enveloped) viruses are resistant to
Detergents, desiccation, acid (GI tract); enveloped viruses are fragile
16 Retroviruses & HIV
Retroviruses are enveloped, positive-sense ssRNA viruses that carry reverse transcriptase to convert RNA → DNA, which integrates into the host genome via integrase.
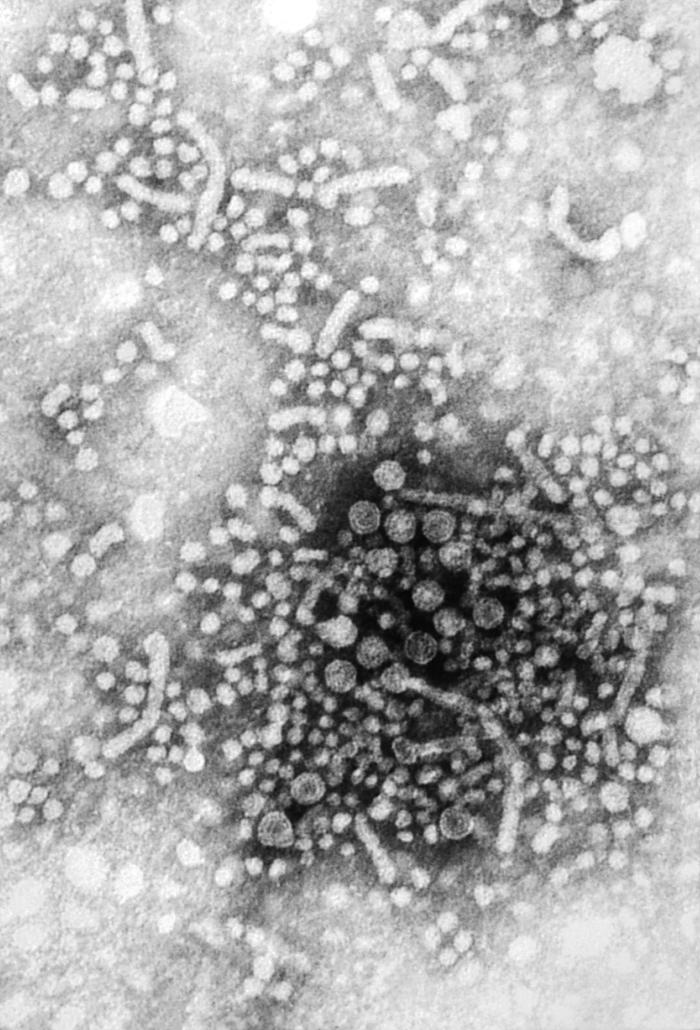
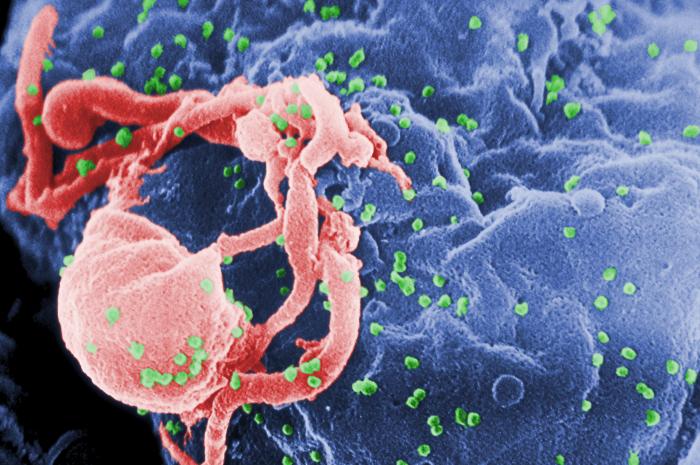
Figure 19 — HIV Virion Structure. The HIV particle contains the gp120/gp41 envelope glycoproteins (binding CD4 and co-receptors), p24 capsid protein (detected in acute infection), and three essential enzymes: reverse transcriptase, integrase, and protease — each a target for antiretroviral therapy.
Self-limited; no chronic state; IgM anti-HAV = acute; vaccine available
HBV
Hepadnavirus
Partially dsDNA
Blood, sexual, vertical
Yes (5% adults, 90% neonates)
Reverse transcriptase; HBsAg (infection), anti-HBs (immunity), HBeAg (high infectivity), anti-HBc IgM (acute); associated with hepatocellular carcinoma and PAN
HCV
Flavivirus
ssRNA (+)
Blood (IVDU #1)
Yes (75–85%)
No vaccine; curable with direct-acting antivirals (DAAs); associated with HCC, cryoglobulinemia, membranoproliferative GN
HDV
Deltavirus
ssRNA (−), circular
Blood, sexual
Only with HBV co-infection
Defective virus; requires HBsAg coat; co-infection or superinfection of HBV carrier (superinfection more severe)
HEV
Hepeviridae
ssRNA (+)
Fecal-oral (waterborne)
No (except immunocompromised)
Especially dangerous in pregnant women (mortality up to 20% in 3rd trimester)
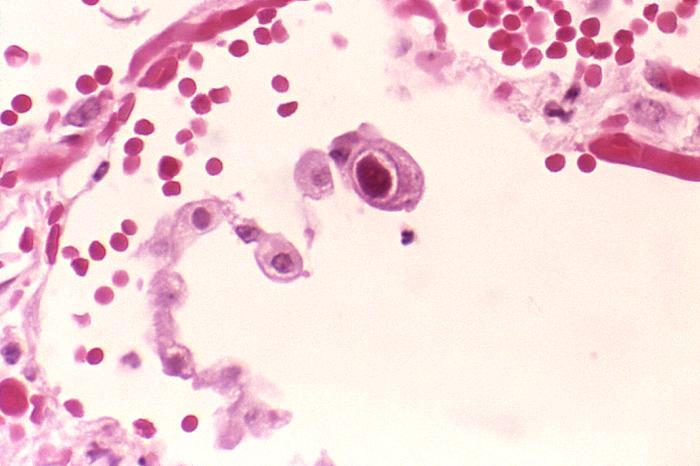
Figure 20 — CMV Owl-Eye Inclusions. Large intranuclear basophilic inclusion surrounded by a clear halo (owl-eye appearance), pathognomonic for cytomegalovirus (CMV). CMV is the most common congenital infection and causes retinitis, colitis, and pneumonitis in immunocompromised patients.
HBV Serologic Interpretation
HBsAg
Anti-HBs
Anti-HBc IgM
Anti-HBc IgG
Interpretation
+
−
+
−
Acute HBV infection
+
−
−
+
Chronic HBV infection
−
+
−
+
Recovered (immune from natural infection)
−
+
−
−
Vaccinated (immune)
−
−
+
−
Window period (acute)
−
−
−
−
Susceptible (not immune)
The window period of HBV occurs when HBsAg has cleared but anti-HBs has not yet appeared. During this time, anti-HBc IgM is the only marker of acute infection. Vaccination produces only anti-HBs (no anti-HBc, because core antigen is not in the vaccine).
Hepatitis B e Antigen & DNA Interpretation
Phase
HBsAg
HBeAg
HBV DNA
ALT
Interpretation
Immune tolerant
+
+
Very high
Normal
High viral replication, minimal liver damage; common in perinatally infected
Immune active (HBeAg+)
+
+
High
Elevated
Active liver damage; consider treatment
Inactive carrier
+
−
Low (<2000 IU/mL)
Normal
Seroconversion to anti-HBe; low risk of progression
Patients with chronic HBV (HBsAg+) or past HBV (anti-HBc+ only) are at risk for HBV reactivation when given immunosuppressive therapy, especially rituximab (anti-CD20), high-dose corticosteroids, and TNF inhibitors. Screen all patients for HBV before starting immunosuppressive therapy. Prophylaxis with entecavir or tenofovir prevents reactivation.
18 Systemic (Endemic) Mycoses
The systemic (dimorphic) fungi are mold at 25°C (environmental) and yeast at 37°C (body temperature) — "mold in the cold, yeast in the heat." They cause disease in immunocompetent individuals and are geographically restricted.
Organism
Geography
Exposure
Disease
Diagnosis
Treatment
Histoplasma capsulatum
Ohio & Mississippi River valleys; Central America
Bat/bird droppings, cave exploration, demolition of old buildings
Disseminated infection in AIDS (skin papules with central umbilication, mimics molluscum)
Yeast with central septum (divides by fission, not budding)
Amphotericin B then itraconazole
Coccidioides meningitis requires lifelong fluconazole — relapse is nearly universal if treatment is stopped. Erythema nodosum (tender red nodules on shins) in a patient from the Southwest should prompt consideration of coccidioidomycosis.
Endemic Mycoses Geography Mnemonic
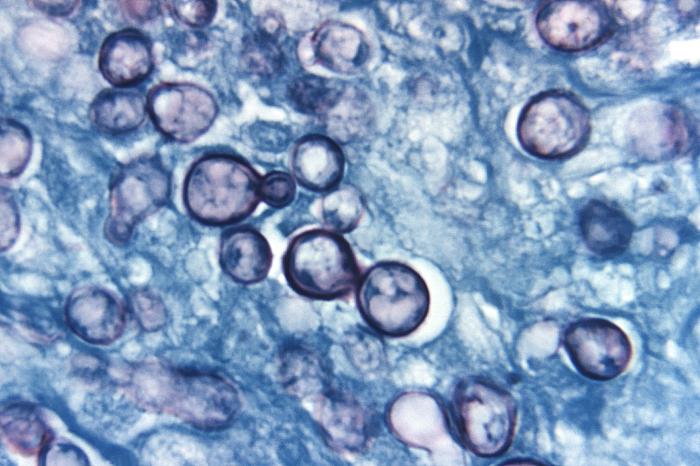
Think "Ohio/Mississippi = Histo and Blasto" (river valley fungi). "Southwest desert = Cocci" (Valley fever). Histoplasma is the most commonly tested endemic mycosis. Key exposure: spelunking (caves) or demolition of old buildings with bat/bird droppings. Organisms live in macrophages (similar to TB) — look for oval yeast within macrophages on silver stain.
Figure 21 — Histoplasma capsulatum. Small oval yeast forms (2–4 µm) within macrophages, demonstrated by methenamine silver stain. Histoplasma is the most commonly tested endemic mycosis; exposure to bat or bird droppings in the Ohio and Mississippi River valleys is the classic history.
Spherules (20–60 µm) filled with endospores (NOT true yeast)
Hyphae with arthroconidia (barrel-shaped; highly infectious)
Paracoccidioides
"Captain's wheel" or "mariner's wheel" — large yeast with multiple peripheral buds
Hyphae with conidia
Sporothrix
Cigar-shaped budding yeast
Rosette conidia ("daisy" pattern)
19 Opportunistic Fungi
Opportunistic fungi cause disease primarily in immunocompromised hosts (neutropenia, HIV/AIDS, transplant recipients, chronic corticosteroid use).
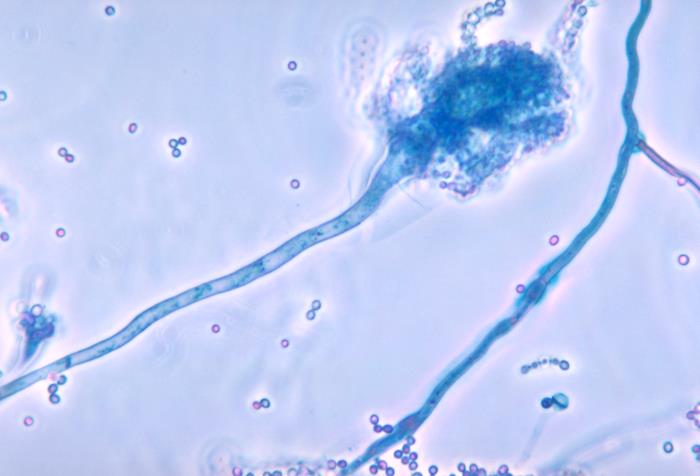
Figure 22 — Aspergillus Septate Hyphae. Septate hyphae branching at acute (45-degree) angles, characteristic of Aspergillus species. Contrast with Mucor/Rhizopus, which shows non-septate (pauciseptate) hyphae branching at 90-degree angles. Voriconazole is first-line for invasive aspergillosis.
Organism
Morphology
Disease
Diagnosis
Treatment
Candida albicans
Yeast with pseudohyphae and true hyphae; germ tube (+)
Tissue biopsy (ribbon-like hyphae); does NOT produce beta-D-glucan or galactomannan
Amphotericin B + aggressive surgical debridement; correct underlying condition (DKA)
Pneumocystis jirovecii
Atypical fungus (cannot be cultured on standard media)
PCP (Pneumocystis pneumonia) in AIDS (CD4 <200), transplant, prolonged steroids
Methenamine silver or DFA stain of BAL; beta-D-glucan elevated; bilateral ground-glass opacities on CT
TMP-SMX (first-line); alternatives: pentamidine, atovaquone, dapsone; add prednisone if PaO2 <70 or A-a gradient >35
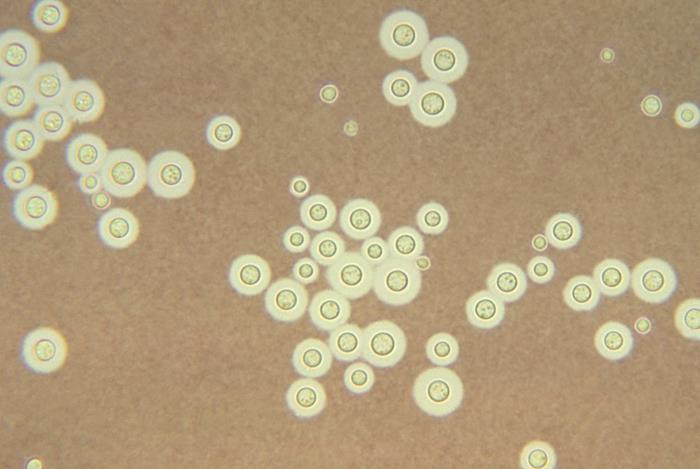
Figure 23 — Cryptococcus neoformans — India Ink Preparation. India ink stain of CSF demonstrating the polysaccharide capsule as a clear halo surrounding the yeast cells. Cryptococcal meningitis is an AIDS-defining illness (CD4 <100). Cryptococcal antigen (CrAg) in serum/CSF is the most sensitive diagnostic test.Figure 24 — Mucormycosis — Non-Septate Hyphae. Tissue section showing broad, ribbon-like, pauciseptate hyphae branching at wide (90-degree) angles, characteristic of Mucor/Rhizopus. Rhinocerebral mucormycosis classically presents in patients with diabetic ketoacidosis. Amphotericin B is the only antifungal with reliable activity.
Septate vs. Non-Septate Hyphae
Septate hyphae at 45 degrees (V-shaped) = Aspergillus. Non-septate (pauciseptate) hyphae at 90 degrees (right-angle branching) = Mucor/Rhizopus. This distinction is critical on biopsy and boards. Mucormycosis classically occurs in diabetic ketoacidosis (high glucose + acidosis + elevated iron = ideal growth conditions).
PCP prophylaxis with TMP-SMX is indicated when CD4 <200 cells/µL or CD4% <14% in HIV, and in transplant recipients or patients on prolonged high-dose corticosteroids. TMP-SMX also provides prophylaxis against Toxoplasma.
Tinea capitis (scalp), tinea corporis (body — ringworm), tinea cruris (groin), tinea pedis (feet), tinea unguium/onychomycosis (nails)
KOH prep showing septate branching hyphae; Wood lamp (Microsporum fluoresces); dermatophyte culture on Sabouraud agar
Topical azoles/terbinafine (skin); oral terbinafine or griseofulvin (nails, scalp)
Malassezia furfur (Pityrosporum)
Tinea (pityriasis) versicolor: hypo- or hyperpigmented macules with fine scale, "spaghetti and meatballs" on KOH
KOH prep; Wood lamp (yellow-green fluorescence)
Topical selenium sulfide, ketoconazole shampoo; oral fluconazole for extensive disease
Sporothrix schenckii
Sporotrichosis: rose gardener's disease — painless papule at inoculation site → ascending lymphangitic spread (nodular lymphangitis)
Cigar-shaped budding yeast at 37°C; dimorphic (mold at 25°C)
Itraconazole (cutaneous); amphotericin B (disseminated)
Tinea capitis in children requires oral antifungal therapy (topical agents do not penetrate the hair follicle). Griseofulvin has been the traditional first-line agent; terbinafine is an alternative. Kerion (inflammatory, boggy mass) is a severe form of tinea capitis that can be mistaken for a bacterial abscess.
Figure 25 — Tinea Corporis (Ringworm). Classic annular erythematous plaque with raised, scaly border and central clearing caused by dermatophyte infection. Diagnosis is confirmed by KOH preparation showing septate branching hyphae. Topical antifungals are first-line for localized disease.Figure 26 — Candida albicans — Pseudohyphae. Gram stain demonstrating budding yeast cells with pseudohyphae, characteristic of Candida species. C. albicans is germ tube-positive. Echinocandins are first-line for candidemia; fluconazole is used for mucosal disease.
T. rubrum (#1 cause of dermatophytosis), T. tonsurans (tinea capitis in US), T. mentagrophytes
Skin, hair, nails (infects all keratinized tissue)
Microsporum
Zoophilic (animal sources)
M. canis (from cats/dogs), M. audouinii
Skin, hair (NOT nails); fluoresces under Wood lamp
Epidermophyton
Anthropophilic
E. floccosum
Skin, nails (NOT hair)
KOH Preparation
KOH (potassium hydroxide) dissolves keratin and cellular debris, allowing visualization of fungal elements. A positive KOH prep from a skin scraping shows septate, branching hyphae in dermatophyte infections. For tinea versicolor (Malassezia), KOH shows the characteristic "spaghetti and meatballs" pattern (short hyphae and round yeast cells). KOH is rapid and inexpensive but has lower sensitivity than culture.
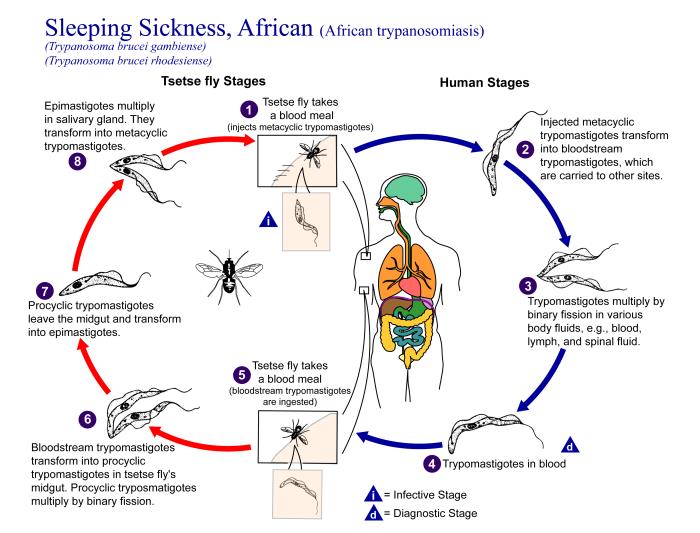
21 Protozoa
Protozoa are single-celled eukaryotic parasites. They are classified by mode of motility: amoebae (pseudopods), flagellates (flagella), ciliates (cilia), and sporozoans/apicomplexa (non-motile, intracellular).
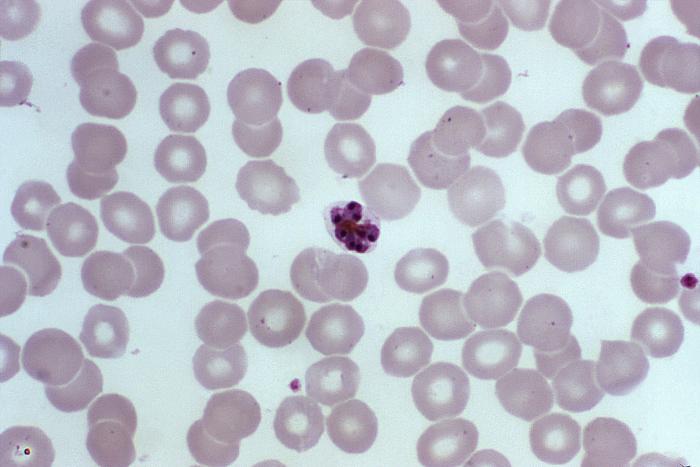
Figure 27 — Malaria — Peripheral Blood Smear. Giemsa-stained thin blood smear demonstrating intraerythrocytic ring-form trophozoites of Plasmodium. P. falciparum infects RBCs of all ages (leading to high parasitemia), while P. vivax preferentially infects reticulocytes. Banana-shaped gametocytes are pathognomonic for P. falciparum.
Blood & Tissue Protozoa
Organism
Vector/Transmission
Disease
Diagnosis
Treatment
Plasmodium (P. falciparum, P. vivax, P. ovale, P. malariae, P. knowlesi)
Female Anopheles mosquito
Malaria: cyclic fevers, anemia, splenomegaly; P. falciparum: severe malaria (cerebral, ARDS, blackwater fever); P. vivax/ovale: hypnozoites in liver (relapse)
Thick and thin blood smears; rapid diagnostic test (RDT) for HRP-2 antigen
P. falciparum: ACT (artemisinin-based combination therapy) or IV artesunate (severe); P. vivax/ovale: chloroquine + primaquine (hypnozoites — check G6PD first)
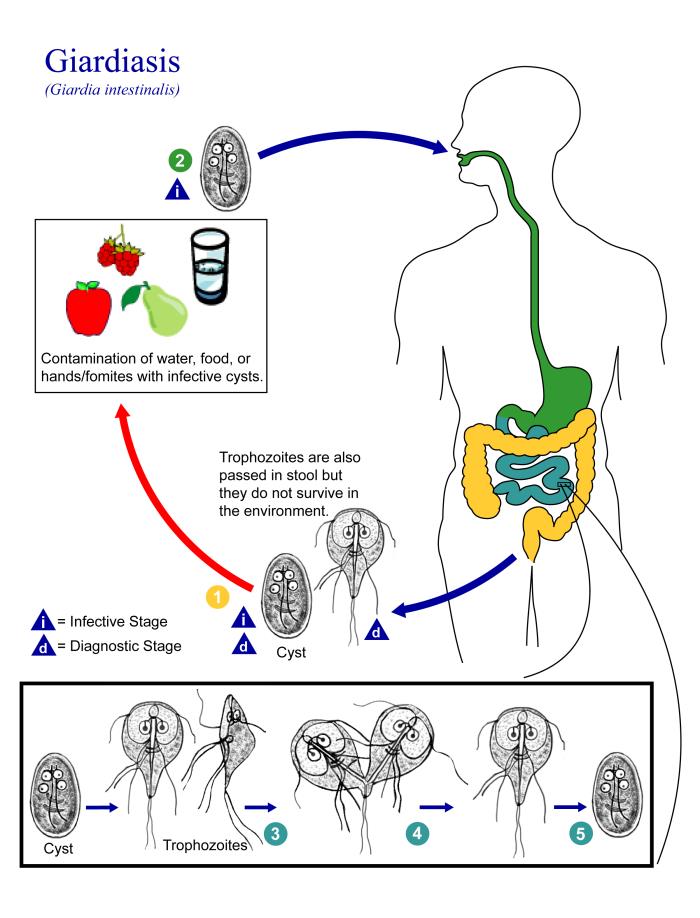
Figure 28 — Giardia lamblia Trophozoite. Pear-shaped trophozoite with two nuclei giving a characteristic face-like appearance. Giardia causes watery, foul-smelling, fatty diarrhea (steatorrhea) without blood, transmitted by fecal-oral route through contaminated water. Common in hikers and daycare settings.
Wet mount (motile trophozoites), NAAT (most sensitive)
Metronidazole (treat both partners)
Cryptosporidium oocysts are resistant to chlorination — this is why waterborne outbreaks occur even in treated municipal water. Modified acid-fast stain is the key diagnostic test (oocysts stain red). In HIV/AIDS patients, the only effective treatment is immune reconstitution with antiretroviral therapy.
Most severe; cerebral malaria, ARDS, severe anemia
Moderate
Mild; nephrotic syndrome
Fever cycle
Irregular or daily (malignant tertian)
Every 48 hr (benign tertian)
Every 72 hr (quartan)
RBC preference
All ages of RBCs (high parasitemia)
Reticulocytes
Older RBCs
Hypnozoites (liver dormancy)
No
Yes — requires primaquine for radical cure
No
Banana-shaped gametocytes
Yes (pathognomonic)
No
No
Before giving primaquine or tafenoquine for P. vivax/ovale radical cure, always check G6PD levels. These drugs cause oxidative hemolysis in G6PD-deficient patients. P. falciparum malaria can progress rapidly to death — any patient with suspected severe malaria should receive IV artesunate immediately while confirmatory testing is pending.
22 Helminths
Helminths are multicellular parasitic worms classified as nematodes (roundworms), cestodes (tapeworms), and trematodes (flukes). A hallmark of helminthic infections is eosinophilia.
Nematodes (Roundworms)
Organism
Transmission
Disease
Diagnosis
Treatment
Ascaris lumbricoides
Fecal-oral (eggs in soil)
Most common helminth worldwide; intestinal obstruction (worm bolus), Loeffler syndrome (pulmonary eosinophilia during larval migration), biliary/pancreatic obstruction
Stool O&P (fertilized eggs)
Albendazole or mebendazole
Enterobius vermicularis
Fecal-oral (autoinfection)
Pinworm: perianal itching (worse at night when female deposits eggs)
Scotch tape test (eggs on perianal skin, collected in morning)
Figure 29 — Ascaris lumbricoides Egg. Fertilized Ascaris egg with characteristic mammillated (bumpy) outer coat seen on stool ova and parasite examination. Ascaris is the most common helminth infection worldwide and can cause intestinal obstruction and Loeffler syndrome during larval pulmonary migration.
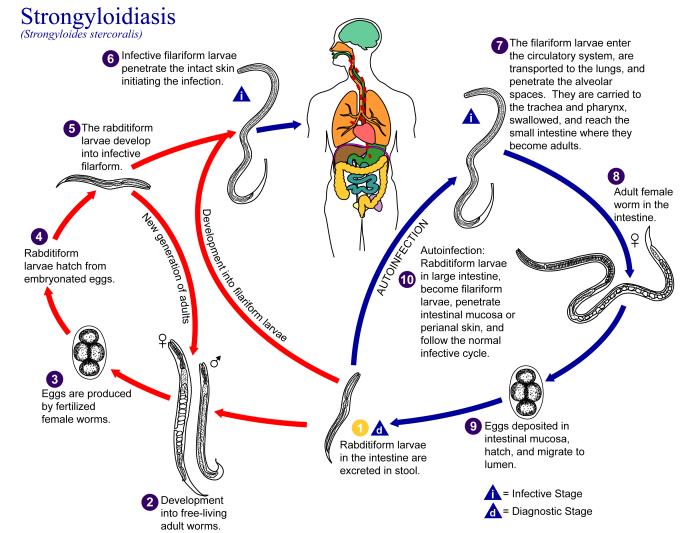
Strongyloides hyperinfection syndrome occurs when immunosuppression (especially corticosteroids) accelerates the autoinfective cycle. Patients can develop disseminated disease with larvae invading virtually every organ, complicated by Gram-negative sepsis as intestinal bacteria translocate with migrating larvae. Screen for Strongyloides before starting immunosuppressive therapy in patients from endemic areas.
Figure 30 — Taenia solium (Pork Tapeworm). Microscopic preparation of T. solium. Ingestion of undercooked pork causes intestinal tapeworm infection. Ingestion of T. solium eggs (fecal-oral) causes neurocysticercosis, the most common cause of seizures in endemic regions. Treatment of neurocysticercosis requires corticosteroids before antiparasitic therapy.
Nematode Larval Migration Patterns
Several nematodes have a pulmonary migration phase through the lungs that can cause Loeffler syndrome (transient pulmonary eosinophilia with cough, wheezing, and migratory infiltrates on CXR):
Marked eosinophilia (>1500/µL) is a hallmark of tissue-invasive helminths (those with a tissue migration phase). The most common causes include: Strongyloides, Ascaris (during migration), hookworms, Toxocara, Trichinella, filarial worms, and Schistosoma (acute Katayama fever). Protozoa generally do NOT cause eosinophilia (exception: Isospora belli).
23 Ectoparasites
Organism
Clinical Presentation
Associated Diseases
Treatment
Sarcoptes scabiei
Scabies: intense pruritus (worse at night), burrows in web spaces, wrists, genitalia; crusted (Norwegian) scabies in immunocompromised
Crusted (Norwegian) scabies occurs in immunocompromised patients and the elderly — it is highly contagious due to the massive mite burden (millions vs. 10–15 mites in typical scabies). It presents as hyperkeratotic, crusted plaques rather than the classic burrows. Oral ivermectin is the treatment of choice for crusted scabies.
Figure 31 — Sarcoptes scabiei (Scabies Mite). Microscopic view of the scabies mite recovered from a skin scraping. Scabies causes intense pruritus worse at night, with burrows in web spaces and wrists. Crusted (Norwegian) scabies in immunocompromised patients carries a massive mite burden and is highly contagious.
Free-Living Amoebae
Organism
Exposure
Disease
Diagnosis
Treatment
Naegleria fowleri
Warm freshwater (lakes, hot springs, poorly maintained pools); enters via nasal passages (cribriform plate)
Naegleria fowleri PAM typically affects healthy young individuals who swim in warm freshwater. It presents like bacterial meningitis (headache, fever, nuchal rigidity) but CSF Gram stain is negative and cultures are sterile. CSF may show RBCs. Suspect when purulent meningitis has negative bacterial cultures and a history of freshwater exposure.
24 Antibacterial Mechanisms & Agents
Antibiotics are classified by their mechanism of action, which determines their spectrum, side effects, and resistance patterns. The five major targets are: (1) cell wall synthesis, (2) cell membrane, (3) protein synthesis (30S and 50S ribosomal subunits), (4) nucleic acid synthesis, and (5) metabolic pathways.
Cell Wall Synthesis Inhibitors
Drug Class
Mechanism
Examples
Spectrum/Notes
Penicillins
Bind PBPs → inhibit transpeptidation of peptidoglycan
The combination of vancomycin + piperacillin-tazobactam is associated with a higher rate of acute kidney injury compared to vancomycin + cefepime or vancomycin + meropenem. When possible, consider alternatives to this combination, especially in patients with baseline renal impairment.
Bactericidal vs. Bacteriostatic
Bactericidal agents kill bacteria: beta-lactams, vancomycin, aminoglycosides, fluoroquinolones, metronidazole, daptomycin. Bacteriostatic agents inhibit growth: macrolides, tetracyclines, clindamycin, chloramphenicol, linezolid, TMP-SMX. Bactericidal agents are preferred in meningitis, endocarditis, and neutropenic patients where host immune function is impaired.
25 Antimicrobial Resistance
Antimicrobial resistance is one of the greatest threats to global health. Understanding resistance mechanisms is essential for rational antibiotic selection and antimicrobial stewardship.
Major Resistance Mechanisms
Mechanism
Description
Clinical Examples
Enzymatic inactivation
Bacteria produce enzymes that destroy or modify the antibiotic
Ampicillin-sulbactam (intrinsic activity of sulbactam), polymyxins, tigecycline, cefiderocol
ESKAPE Pathogens
Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, Enterobacter spp. — the leading causes of nosocomial infections that "escape" commonly used antibiotics. These organisms are the primary focus of antimicrobial stewardship efforts and new drug development.
When an ESBL-producing organism is identified, switch to a carbapenem regardless of in vitro susceptibility to cephalosporins — clinical outcomes are better with carbapenems. For KPC-producing CRE, ceftazidime-avibactam is the preferred agent; for metallo-beta-lactamase producers (NDM, VIM), cefiderocol or aztreonam-based combinations are needed (avibactam does not inhibit metallo-beta-lactamases).
Inducible resistance to 3rd-gen cephalosporins; "SPACE" organisms
D (serine)
OXA-type (oxacillinases)
OXA-48 (carbapenemase), OXA-23 (Acinetobacter)
Variably by avibactam
Major carbapenem resistance mechanism in Acinetobacter
AmpC Induction — The "SPACE" Bug Pitfall
Serratia, Pseudomonas, Acinetobacter, Citrobacter, and Enterobacter carry chromosomal AmpC beta-lactamases. Exposure to 3rd-generation cephalosporins (e.g., ceftriaxone) can induce AmpC overexpression, leading to resistance during therapy. A patient with Enterobacter bacteremia may initially appear susceptible to ceftriaxone but develop resistance on treatment. Use cefepime (stable to AmpC) or carbapenems for serious SPACE infections.
Intrinsic (Natural) Resistance Patterns
Organism
Intrinsic Resistance
Clinical Pearl
MRSA
All beta-lactams except ceftaroline
mecA → PBP2a
Enterococcus faecalis
Cephalosporins, aminoglycosides (low-level), TMP-SMX (in vivo)
Use ampicillin + gentamicin for synergy; cephalosporins have zero activity
Listeria
Cephalosporins
Must add ampicillin to meningitis regimen in neonates and elderly
Klebsiella
Ampicillin (chromosomal SHV-1 beta-lactamase)
Always resistant to ampicillin and amoxicillin
Proteus, Morganella, Providencia
Colistin/polymyxins
Intrinsic LPS modification; cannot use colistin as last resort
Stenotrophomonas
Carbapenems (L1 metallo-beta-lactamase)
TMP-SMX is first-line; one of few bugs where carbapenems worsen outcomes
Anaerobes
Aminoglycosides
Require O2-dependent transport into cells; no activity in anaerobic conditions
Mycoplasma
All cell wall-active agents (beta-lactams, vancomycin)
No peptidoglycan = no target
26 Antifungal, Antiviral & Antiparasitic Agents
Antifungal Agents
Drug Class
Mechanism
Examples
Key Uses & Side Effects
Polyenes
Bind ergosterol → membrane pore formation
Amphotericin B (liposomal preferred), nystatin (topical)
Increases Ca2+ permeability → paralysis and tegumental damage
All trematodes (flukes) and cestodes (tapeworms); schistosomiasis
Primaquine/tafenoquine
Generates reactive oxygen species in hypnozoites
P. vivax/ovale radical cure (kills hepatic hypnozoites); check G6PD before use (hemolytic anemia)
Amphotericin B is the broadest-spectrum antifungal but also the most toxic. The mnemonic "ampho-terrible" captures its side effect profile. Liposomal formulations have significantly reduced nephrotoxicity. It is the drug of choice for severe systemic mycoses, mucormycosis, and induction therapy for cryptococcal meningitis.
Antifungal Spectrum Summary
Agent
Candida
Aspergillus
Mucor
Cryptococcus
Endemic Mycoses
Amphotericin B
Yes
Yes
Yes
Yes
Yes
Fluconazole
Yes (not C. krusei, variable C. glabrata)
No
No
Yes
Cocci only
Voriconazole
Yes
Yes (first-line)
No
Yes
Yes
Posaconazole
Yes
Yes
Yes
Yes
Yes
Echinocandins
Yes (first-line candidemia)
Yes (salvage)
No
No
No
Antifungal Coverage Gaps
Fluconazole: No mold coverage (no Aspergillus, no Mucor). Voriconazole: No Mucor coverage (and may actually worsen mucormycosis if used empirically). Echinocandins: No Cryptococcus coverage, no Mucor coverage. Only amphotericin B has activity against Mucor/Rhizopus. When mucormycosis is suspected (DKA + rhinocerebral symptoms), use amphotericin B immediately.
27 Clinical Correlates & Empiric Therapy
Rational antimicrobial prescribing requires matching the most likely pathogen to the clinical syndrome, local resistance patterns, and patient factors (allergies, renal function, immunocompromise).
Empiric Antibiotic Therapy by Syndrome
Clinical Syndrome
Most Likely Pathogens
Empiric Therapy
Community-acquired pneumonia (outpatient)
S. pneumoniae, Mycoplasma, Chlamydophila, H. influenzae
Amoxicillin OR doxycycline; azithromycin (if low resistance)
Community-acquired pneumonia (inpatient, non-ICU)
Same + Legionella
Beta-lactam (ceftriaxone or ampicillin-sulbactam) + macrolide OR respiratory fluoroquinolone alone
N95 respirator; negative-pressure room; door closed
The mnemonic for airborne precautions is "MTV" — Measles, TB, Varicella (chickenpox/disseminated zoster). These require an N95 respirator and a negative-pressure room. C. difficile requires contact precautions with soap and water hand washing (alcohol-based hand sanitizers do NOT kill C. difficile spores).
Antimicrobial Stewardship Principles
De-escalation: Narrow spectrum once culture and susceptibility data are available. Duration: Use the shortest effective course supported by evidence. Biomarkers: Procalcitonin can guide antibiotic discontinuation in respiratory infections and sepsis. IV-to-oral switch: Transition when clinically improving, afebrile, and tolerating oral intake. Antibiogram: Use local resistance data to guide empiric choices.
28 High-Yield Review
Board-relevant and frequently tested topics across medical microbiology, organized for rapid review.
Encapsulated Organisms — "SHiNE SKiS"
Salmonella, Haemophilus influenzae, Neisseria meningitidis, Escherichia coli (K1), Streptococcus pneumoniae, Klebsiella, Group B Strep. Asplenic patients are at extreme risk for infections by encapsulated organisms — the spleen is essential for opsonization and clearance of encapsulated bacteria. Vaccinate asplenic patients against S. pneumoniae, N. meningitidis, and H. influenzae type b.
Organisms by Unique Laboratory Features
Feature
Organism
Quellung reaction (capsular swelling)
S. pneumoniae
Satellite colonies around S. aureus (factors X and V)
H. influenzae
Chocolate agar with CO2
N. gonorrhoeae, H. influenzae
Charcoal yeast extract (BCYE) agar with iron and cysteine
Legionella
Lowenstein–Jensen agar
M. tuberculosis
Sabouraud agar (low pH)
Fungi (dermatophytes)
Bordet–Gengou agar
B. pertussis
Thayer–Martin agar (chocolate + VCN antibiotics)
N. gonorrhoeae, N. meningitidis
MacConkey agar (lactose fermenters = pink)
E. coli, Klebsiella (pink); Salmonella, Shigella (colorless)
Eosin methylene blue (EMB) agar (green metallic sheen)
The most common cause of sepsis is Gram-negative bacteria (E. coli #1), but S. aureus is the most common Gram-positive cause of bacteremia. Always send 2 sets of blood cultures (4 bottles) from 2 separate sites BEFORE starting antibiotics. A single positive blood culture for S. aureus or Candida is NEVER a contaminant.
Skin vesicles, encephalitis, disseminated disease; C-section indicated if active lesions at delivery
CMV is the most common congenital infection and the most common infectious cause of sensorineural hearing loss in children. Periventricular calcifications (CMV) are distinguished from diffuse/scattered calcifications (Toxoplasma). Most congenital CMV cases are asymptomatic at birth but may develop hearing loss later.
Bioterrorism Category A Agents
Agent
Disease
Key Features
Bacillus anthracis
Anthrax
Inhalational anthrax: widened mediastinum on CXR; cutaneous: painless black eschar
Live attenuated (varicella) / recombinant adjuvanted (Shingrix)
VZV
PCV20, PPSV23
Conjugate / polysaccharide
S. pneumoniae
MenACWY, MenB
Conjugate / recombinant
N. meningitidis
Hib
Conjugate (PRP-protein)
H. influenzae type b
HPV (Gardasil-9)
Recombinant VLP
HPV types 6, 11, 16, 18, 31, 33, 45, 52, 58
HBV
Recombinant (HBsAg)
Hepatitis B
Influenza
Inactivated or live attenuated (nasal)
Influenza A and B
Rotavirus
Live oral
Rotavirus
Exam Focus: Key high-yield topics: (1) Toxin mechanisms (especially A-B toxins and superantigens); (2) Gram stain morphology → organism identification; (3) Antibiotic mechanisms and resistance; (4) Empiric therapy by syndrome; (5) HIV opportunistic infections by CD4 count; (6) Hepatitis B serology interpretation; (7) Endemic mycoses by geography; (8) Parasite life cycles and treatment; (9) ESKAPE pathogens and resistance mechanisms; (10) Vaccine-preventable diseases; (11) TORCH infections and congenital findings; (12) Organisms that do not Gram stain and their alternative diagnostic methods.