Drug mechanisms, pharmacokinetics, pharmacodynamics, autonomic pharmacology, antimicrobials, cardiovascular drugs, CNS agents, endocrine pharmacology, chemotherapy, and every drug class, receptor, and clinical application across the full scope of pharmacology.
01 Overview & Significance
Pharmacology is the study of how drugs interact with biological systems to produce therapeutic effects, adverse reactions, and toxicities. It is the bridge between basic science and clinical medicine — every prescription, every dose adjustment, every adverse drug reaction, and every drug interaction traces back to pharmacologic principles. Mastery of pharmacology is essential for safe prescribing, rational therapeutics, and success on USMLE Step 1 (where pharmacology accounts for 15–22% of questions).
Why This Matters
Pharmacology integrates biochemistry, physiology, and pathology into the single most clinically actionable discipline. A physician who understands drug mechanisms can predict side effects, anticipate interactions, adjust for special populations, and make evidence-based therapeutic decisions at the bedside.
Branches of Pharmacology
Branch
Focus
Pharmacokinetics
What the body does to the drug (ADME: absorption, distribution, metabolism, excretion)
Pharmacodynamics
What the drug does to the body (receptor interactions, dose–response)
Pharmacogenomics
Genetic variation affecting drug response (e.g., CYP2D6 polymorphisms)
Pharmacovigilance
Post-marketing safety surveillance and adverse event monitoring
Toxicology
Adverse effects, poisoning, antidotes, and drug overdose management
Clinical Pharmacology
Rational drug therapy in patients, therapeutic drug monitoring
Drug Development & Regulation
Drug development proceeds through preclinical testing (in vitro and animal studies), then four clinical trial phases: Phase I (safety, pharmacokinetics in healthy volunteers; ~20–80 subjects), Phase II (efficacy and dosing in patients with the target disease; ~100–300 subjects), Phase III (large-scale randomized controlled trials confirming efficacy and monitoring adverse effects; ~1,000–3,000 subjects), and Phase IV (post-marketing surveillance after FDA approval). The entire process typically takes 10–15 years and costs over $1 billion.
Phase I trials determine the maximum tolerated dose and pharmacokinetic profile. Phase III failures are the most costly because of the large sample sizes involved. Phase IV surveillance detects rare adverse effects that Phase III was underpowered to identify.
Drug Nomenclature & Naming Conventions
Drug names follow systematic conventions that encode class information. Understanding common stems (suffixes) allows rapid identification of drug mechanism:
Stem / Suffix
Drug Class
Examples
-olol
β-Adrenergic blockers
Metoprolol, atenolol, propranolol
-pril
ACE inhibitors
Lisinopril, enalapril, ramipril
-sartan
Angiotensin II receptor blockers
Losartan, valsartan, irbesartan
-dipine
Dihydropyridine CCBs
Amlodipine, nifedipine
-statin
HMG-CoA reductase inhibitors
Atorvastatin, rosuvastatin
-azole
Antifungal azoles
Fluconazole, ketoconazole
-cillin
Penicillin antibiotics
Amoxicillin, ampicillin
-mycin / -micin
Aminoglycosides / macrolides
Gentamicin, azithromycin
-mab
Monoclonal antibodies
Rituximab, trastuzumab, infliximab
-nib / -tinib
Tyrosine kinase inhibitors
Imatinib, erlotinib, sunitinib
-gliptin
DPP-4 inhibitors
Sitagliptin, saxagliptin
-gliflozin
SGLT2 inhibitors
Empagliflozin, dapagliflozin
-glutide
GLP-1 receptor agonists
Semaglutide, liraglutide
-prazole
Proton pump inhibitors
Omeprazole, pantoprazole
-tidine
H2 receptor antagonists
Ranitidine, famotidine
-setron
5-HT3 antagonists (antiemetics)
Ondansetron, granisetron
-triptan
5-HT1B/1D agonists (migraines)
Sumatriptan, rizatriptan
Recognizing drug suffixes is a rapid shortcut on board exams. If you see an unfamiliar drug ending in "-olol," you can immediately reason about β-blocker side effects (bradycardia, bronchospasm, fatigue) and contraindications. This often gives the answer without needing to memorize the specific drug.
02 Core Principles & Drug–Receptor Theory
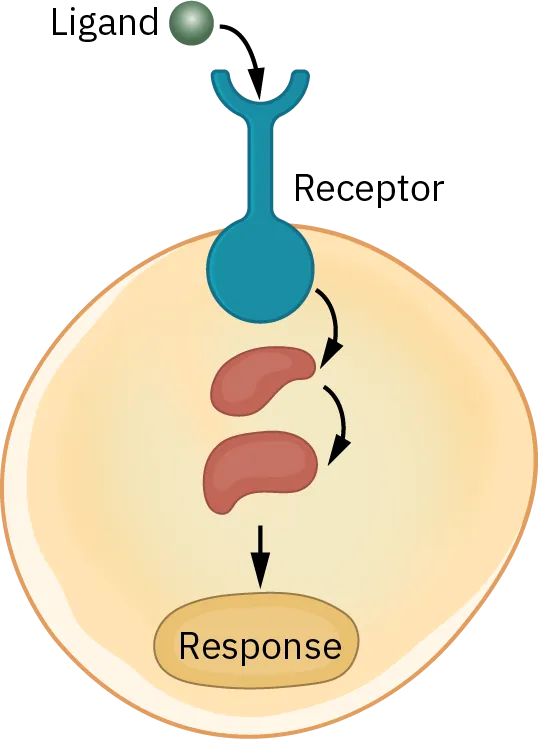
Figure 1 — Drug–Receptor Binding. A drug (ligand) binds to a specific receptor protein on or within a cell, forming a drug–receptor complex that triggers a downstream cellular response. Only the complementary ligand activates the receptor, illustrating the lock-and-key principle of receptor selectivity.
Drug–Receptor Interactions
Most drugs produce effects by binding to specific receptors — proteins (enzymes, ion channels, G-protein coupled receptors, nuclear receptors, or transporters) that transduce the drug signal into a cellular response. The binding follows the law of mass action: Drug + Receptor ↔ Drug–Receptor Complex → Effect. The affinity of a drug for its receptor determines how tightly it binds (quantified by Kd, the dissociation constant — lower Kd = higher affinity). The intrinsic activity (efficacy) determines the magnitude of response once bound.
Agonists, Antagonists & Partial Agonists
Type
Affinity
Efficacy
Example
Full agonist
Yes
Maximal (Emax)
Isoproterenol (β-adrenergic), morphine (μ-opioid)
Partial agonist
Yes
Submaximal
Buprenorphine (μ-opioid), pindolol (β-blocker with ISA)
Competitive antagonist
Yes
Zero (blocks agonist)
Naloxone (μ-opioid), atropine (muscarinic)
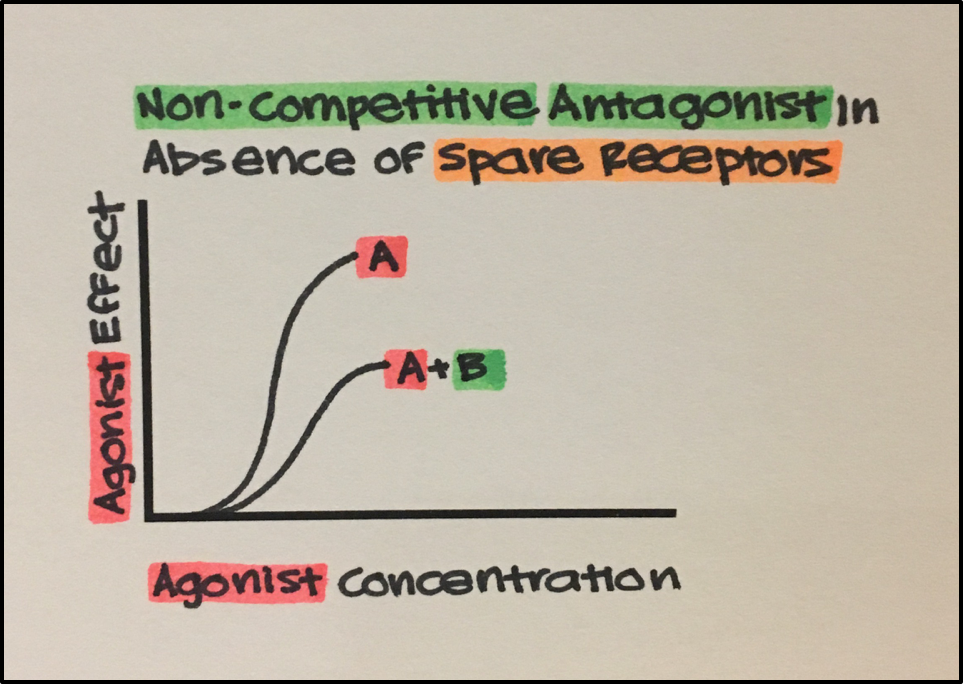
Non-competitive antagonist
Yes (allosteric or irreversible)
Zero (reduces Emax)
Phenoxybenzamine (α-adrenergic)
Inverse agonist
Yes
Negative (reduces basal activity)
Some benzodiazepine analogs, certain antihistamines
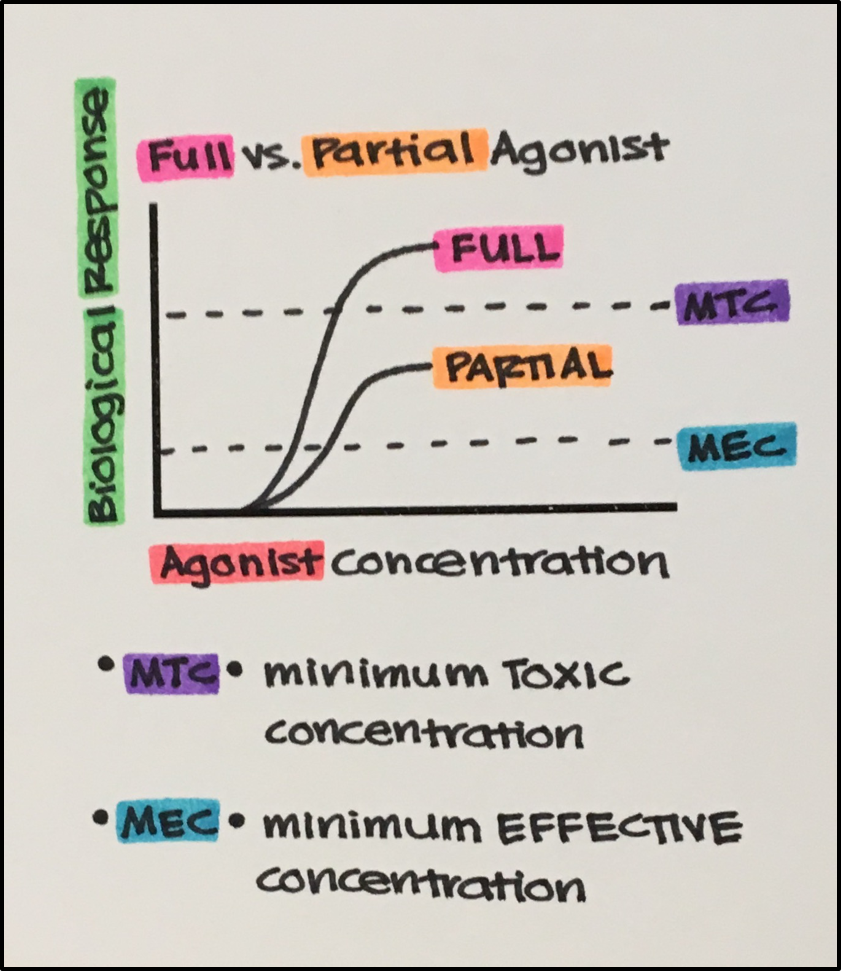
Figure 2 — Agonist Types and Dose–Response Relationships. Full agonists produce maximal response (Emax), partial agonists produce submaximal response, antagonists block the receptor without activating it, and inverse agonists reduce constitutive (basal) receptor activity below baseline.
A partial agonist in the presence of a full agonist acts as a net antagonist (it competes for receptors but produces less effect). This is why buprenorphine can precipitate withdrawal in a patient who is on a full μ-agonist such as heroin.
Receptor Types
Receptor Type
Mechanism
Speed
Examples
Ligand-gated ion channel
Ion flux through pore
Milliseconds
Nicotinic ACh, GABAA, NMDA
G-protein coupled (GPCR)
Second messengers (cAMP, IP3, DAG)
Seconds
Muscarinic, adrenergic, opioid, dopamine
Enzyme-linked (receptor tyrosine kinase)
Phosphorylation cascades
Minutes–hours
Insulin, EGF, PDGF receptors
Intracellular / nuclear
Gene transcription modification
Hours–days
Steroid, thyroid, vitamin D receptors
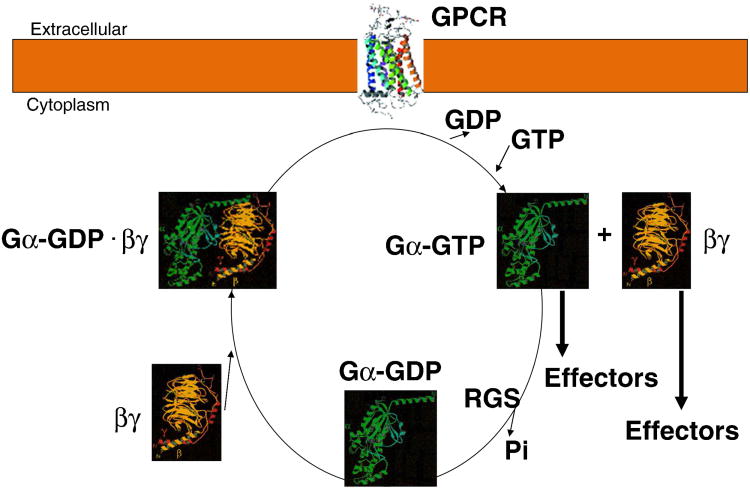
Figure 3 — GPCR Activation Cycle. When an agonist binds the GPCR, the receptor undergoes a conformational change that promotes exchange of GDP for GTP on the Gα subunit. The activated Gα-GTP dissociates from the βγ dimer and interacts with downstream effectors (adenylyl cyclase, phospholipase C, or ion channels) until GTPase activity hydrolyzes GTP back to GDP, terminating the signal.
G-Protein Signaling Pathways
GPCRs signal through heterotrimeric G proteins with distinct α-subunits:
Activates phospholipase C → ↑IP3 + DAG → Ca2+ release + PKC
α1, M1, M3, H1, V1, AT1
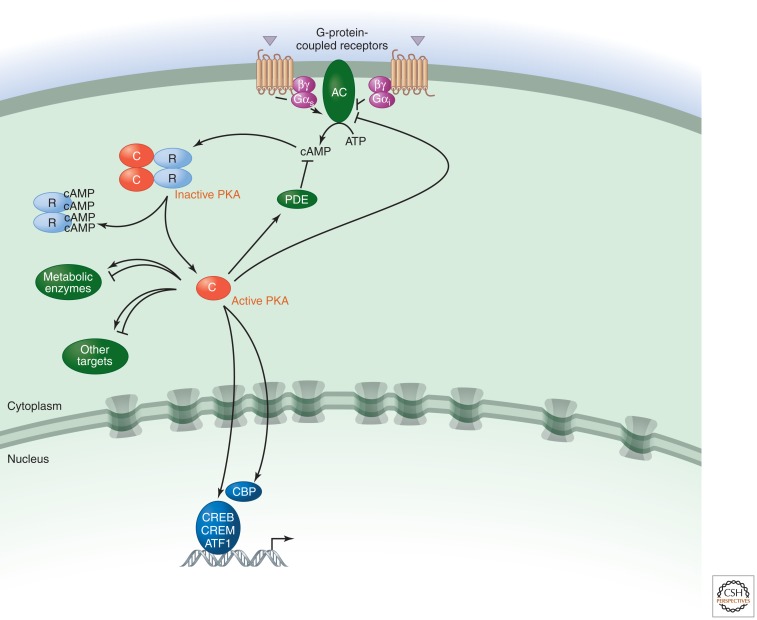
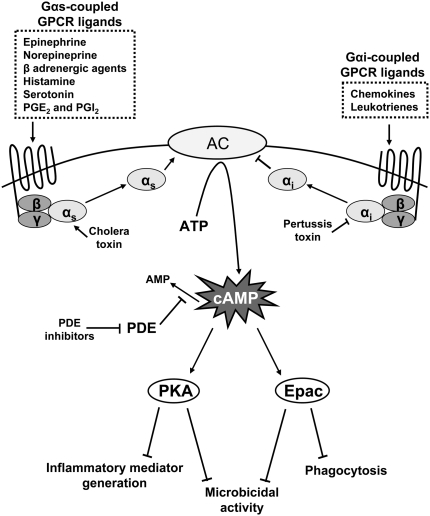
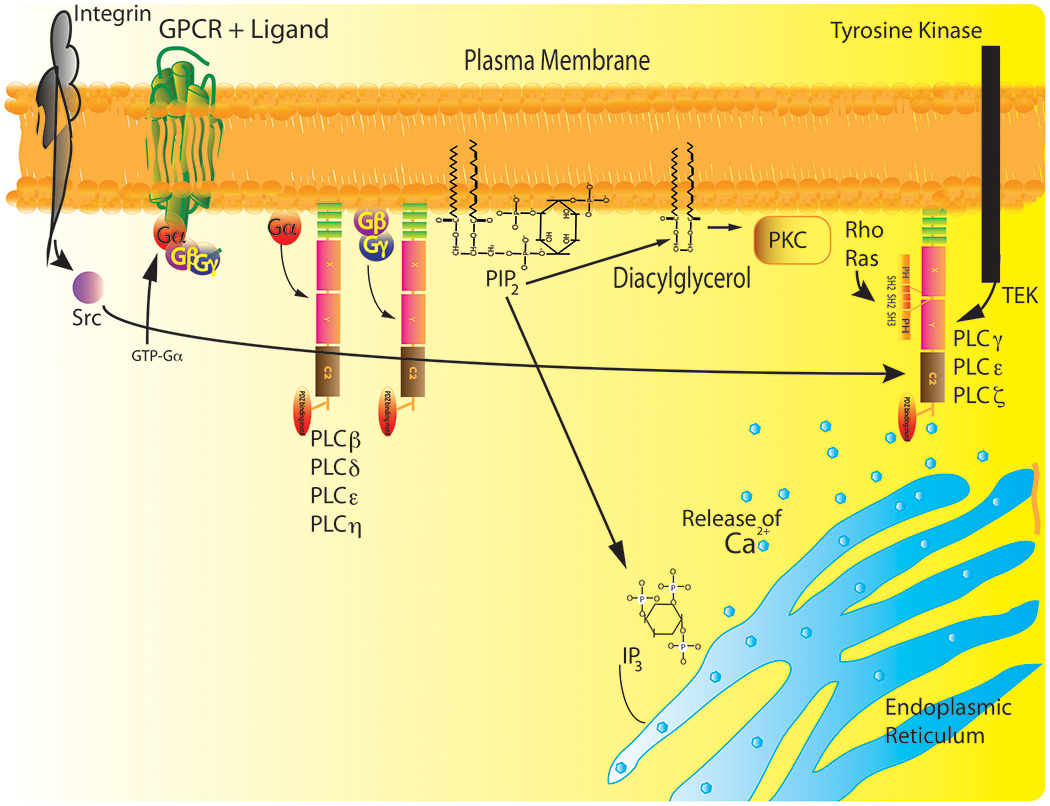
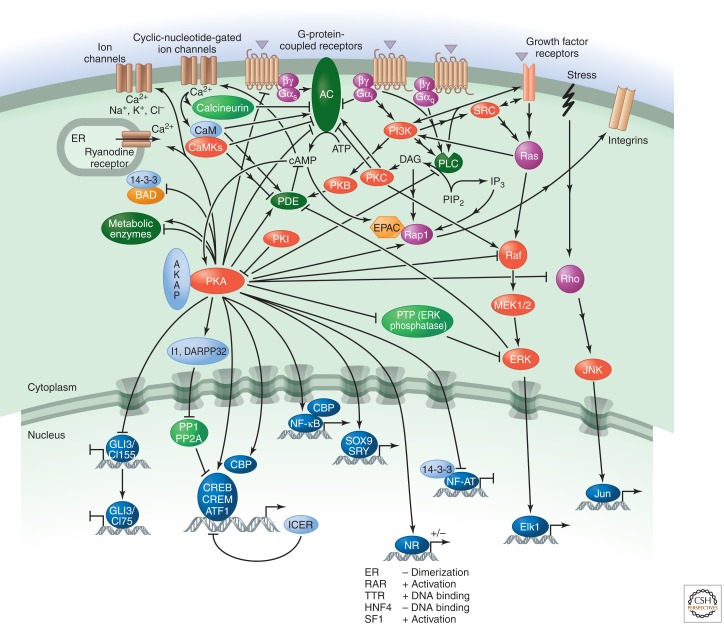
Figure 4 — Gs Stimulatory Pathway. Activation of Gs-coupled receptors (β1, β2, D1, H2, V2) stimulates adenylyl cyclase, increasing intracellular cAMP levels. cAMP activates protein kinase A (PKA), which phosphorylates target proteins to produce the cellular response.Figure 5 — Gi Inhibitory Pathway. Activation of Gi-coupled receptors (α2, M2, D2, μ-opioid) inhibits adenylyl cyclase, decreasing intracellular cAMP. This reduces PKA activity and downstream phosphorylation events, producing inhibitory cellular effects such as decreased heart rate (M2) and reduced neurotransmitter release (α2).Figure 6 — Gq–Phospholipase C Pathway. Activation of Gq-coupled receptors (α1, M1, M3, H1, V1) stimulates phospholipase C (PLC), which cleaves PIP2 into IP3 and DAG. IP3 releases Ca2+ from the endoplasmic reticulum, while DAG activates protein kinase C (PKC). This pathway mediates smooth muscle contraction, glandular secretion, and other Gq-dependent effects.Figure 7 — GPCR Signaling Summary. Overview of the three major G-protein signaling cascades. Gs stimulates adenylyl cyclase (↑cAMP), Gi inhibits adenylyl cyclase (↓cAMP), and Gq activates phospholipase C (IP3/DAG/Ca2+). Each pathway couples to distinct receptor subtypes and produces characteristic physiological effects.Figure 8 — PKA Signaling Cascade. Protein kinase A (PKA) is the primary effector of cAMP signaling. When cAMP binds the regulatory subunits of PKA, the catalytic subunits are released and phosphorylate downstream targets including ion channels, transcription factors (CREB), and metabolic enzymes, mediating the diverse effects of Gs-coupled receptor activation.
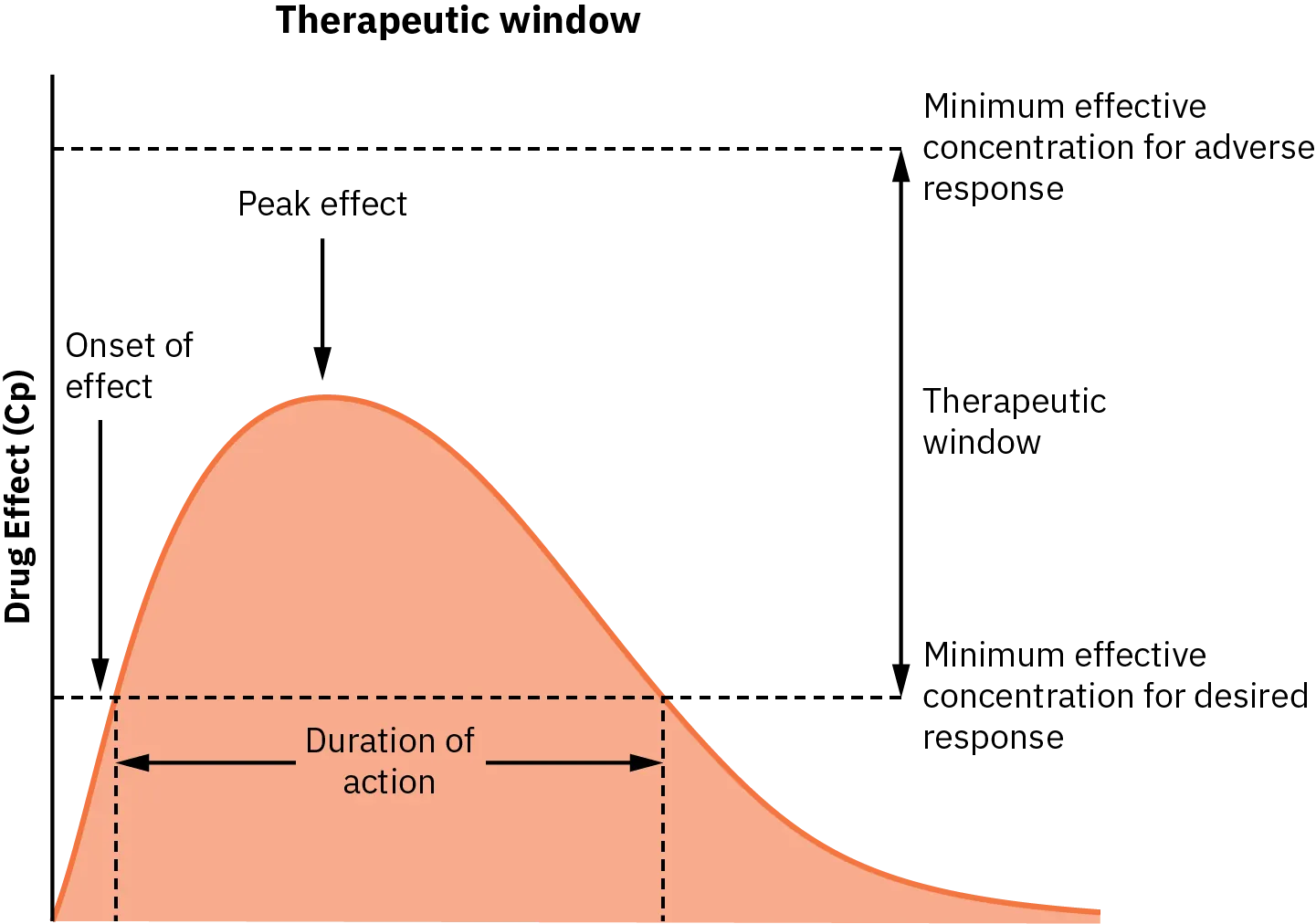
The therapeutic index (TI) = TD50 / ED50 (or LD50 / ED50 in animal studies), where TD50 is the dose producing toxicity in 50% and ED50 is the effective dose in 50% of the population. A narrow TI means the toxic dose is close to the therapeutic dose, requiring careful monitoring. Drugs with narrow TI include warfarin, lithium, digoxin, theophylline, aminoglycosides, phenytoin, and cyclosporine.
Figure 9 — Therapeutic Window. The therapeutic window is the range of plasma drug concentrations between the minimum effective concentration (MEC) and the minimum toxic concentration (MTC). Drugs with a narrow therapeutic index have a small window, requiring careful dosing and monitoring to maintain plasma levels within the safe and effective range.
The therapeutic index is the single most important safety parameter in pharmacology. Drugs with a narrow TI require therapeutic drug monitoring (TDM). Always know which drugs have a narrow TI — this is heavily tested.
03 Key Terminology & Abbreviations
Term / Abbreviation
Definition
ADME
Absorption, Distribution, Metabolism, Excretion
Vd
Volume of distribution — theoretical volume needed to contain total drug at plasma concentration
t1/2
Half-life — time for plasma concentration to decrease by 50%
Css
Steady-state concentration — reached after ~4–5 half-lives
CL
Clearance — volume of plasma cleared of drug per unit time
F
Bioavailability — fraction of administered dose reaching systemic circulation
EC50
Concentration producing 50% of maximal effect
Emax
Maximal effect achievable by a drug
Kd
Dissociation constant — concentration at which 50% of receptors are occupied
pKa
pH at which 50% of drug is ionized and 50% is non-ionized
TDM
Therapeutic drug monitoring
TI
Therapeutic index (TD50 / ED50)
AUC
Area under the curve — total drug exposure over time
P-gp
P-glycoprotein — efflux transporter limiting drug absorption/distribution
CYP
Cytochrome P450 — family of drug-metabolizing enzymes
ISA
Intrinsic sympathomimetic activity
NNT / NNH
Number needed to treat / Number needed to harm
MIC
Minimum inhibitory concentration (antimicrobials)
04 Absorption & Bioavailability
Absorption is the movement of drug from the site of administration into the systemic circulation. The rate and extent of absorption determine the bioavailability (F) — defined as the fraction of administered drug that reaches the systemic circulation in unchanged form. IV administration has F = 1.0 (100%) by definition.
Factors Affecting Absorption
Factor
Effect on Absorption
Clinical Example
Route of administration
IV > IM > SC > PO (general order of speed)
IV morphine onset ~5 min vs PO ~30 min
Drug lipophilicity
More lipophilic = better membrane penetration
Diazepam (lipophilic) absorbs rapidly PO
Ionization state (pKa)
Non-ionized (uncharged) form crosses membranes
Aspirin (weak acid, pKa 3.5) absorbed in acidic stomach
Gastric pH
Affects ionization of weak acids/bases
PPIs reduce ketoconazole absorption (needs acid)
Gastric emptying
Faster emptying = faster absorption for most drugs
Metoclopramide accelerates, opioids slow emptying
First-pass metabolism
Hepatic extraction reduces bioavailability
Nitroglycerin F <5% PO (use sublingual)
P-glycoprotein efflux
Pumps drug back into gut lumen
Digoxin, cyclosporine subject to P-gp efflux
Ion Trapping
Weak acids are non-ionized in acidic environments (stomach) and ionized in basic environments (blood). Weak bases are the opposite. Non-ionized drug crosses membranes; ionized drug is "trapped." This principle explains why aspirin overdose is treated with urinary alkalinization (traps ionized salicylate in urine) and why weak acid drugs are absorbed well in the stomach.
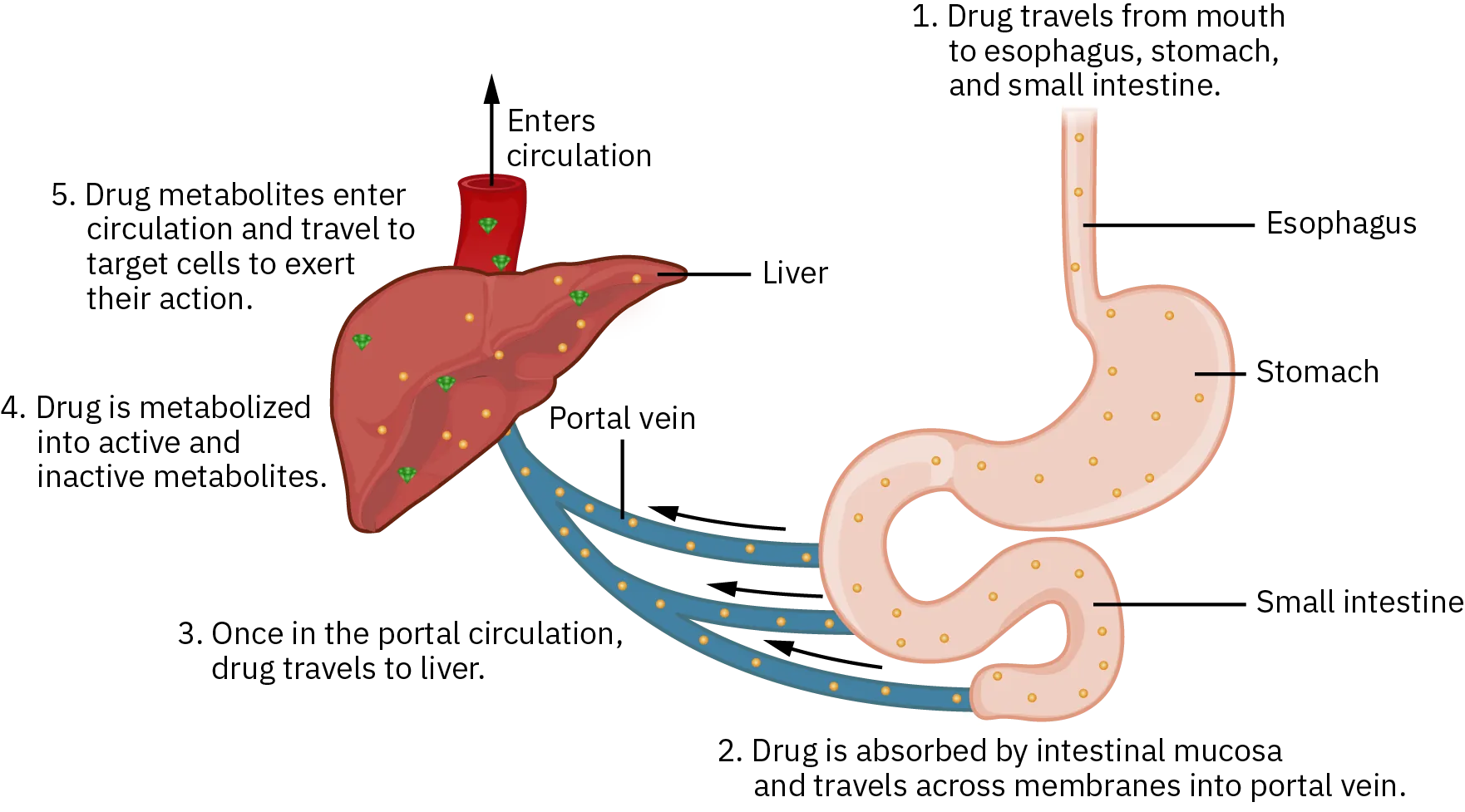
Figure 10 — First-Pass Metabolism. After oral administration, drugs are absorbed from the GI tract into the portal venous system and pass through the liver before entering the systemic circulation. Drugs with high hepatic extraction ratios undergo extensive first-pass metabolism, significantly reducing oral bioavailability. Routes bypassing first-pass include sublingual, transdermal, inhalational, and intravenous administration.
First-Pass Effect
After oral absorption, drugs enter the portal circulation and pass through the liver before reaching systemic circulation. Drugs with high hepatic extraction ratios undergo extensive first-pass metabolism, dramatically reducing oral bioavailability. Examples: nitroglycerin (F <5%), morphine (F ~25%), propranolol (F ~25%), lidocaine (F ~35%). Routes that bypass first-pass: sublingual, rectal (partially), transdermal, inhalational, IV.
Bioavailability = (AUCoral / AUCIV) × 100%. For the same drug, if the oral dose must be much higher than the IV dose, suspect high first-pass metabolism.
05 Distribution & Protein Binding
Once absorbed, drugs distribute from plasma into tissues. The volume of distribution (Vd) = Amount of drug in body / Plasma drug concentration. Vd is a theoretical volume: a large Vd means the drug distributes extensively into tissues (is not primarily in plasma); a small Vd means it stays in the vascular compartment.
Vd Range
Interpretation
Examples
<5 L (~plasma volume)
Confined to plasma, high protein binding
Warfarin (Vd ~8 L), heparin
5–15 L (~ECF)
Distributes into extracellular fluid
Aminoglycosides (Vd ~15 L)
15–40 L (~TBW)
Distributes into total body water
Ethanol, phenytoin
>40 L
Extensive tissue binding/sequestration
Chloroquine (Vd ~13,000 L), digoxin (~500 L)
Protein Binding
Drugs bind to plasma proteins, primarily albumin (acidic drugs: warfarin, phenytoin, salicylates) and α1-acid glycoprotein (basic drugs: lidocaine, propranolol). Only the free (unbound) fraction is pharmacologically active, can cross membranes, and can be metabolized/excreted. Conditions that decrease albumin (hepatic failure, nephrotic syndrome, malnutrition) increase the free fraction of highly protein-bound drugs, potentially causing toxicity.
Phenytoin is ~90% protein-bound. In hypoalbuminemia, the free fraction increases. Use the Sheiner-Tozer correction: Adjusted phenytoin = Measured phenytoin / (0.2 × albumin + 0.1). This is a classic board question.
Blood-Brain Barrier (BBB)
The BBB consists of tight junctions between brain capillary endothelial cells, limiting passage to small, lipophilic, non-ionized molecules. Drugs that cross the BBB well: diazepam, thiopental, fentanyl. Drugs that do not cross well: penicillin G (unless meninges are inflamed), aminoglycosides, first-generation antihistamines cross (causing sedation) while second-generation (e.g., loratadine) are P-gp substrates excluded from the CNS.
06 Metabolism & CYP450 System
Drug metabolism (biotransformation) converts lipophilic drugs into more hydrophilic metabolites for renal excretion. Metabolism occurs primarily in the liver and is classified into two phases:
"Queen Barb Takes Phen-Phen and Refuses Grisly Carbs Chronically" — Quinidine (minor), Barbiturates, St. John's wort (take), Phenytoin, Phenobarbital, Rifampin, Griseofulvin, Carbamazepine, Chronic alcohol. Inducers increase CYP activity → faster drug metabolism → decreased drug levels.
Pharmacogenomics & CYP Polymorphisms
CYP2D6 exhibits clinically significant genetic polymorphism: poor metabolizers (~7% Caucasians) cannot convert codeine to morphine (codeine is ineffective) but accumulate parent drugs of other substrates; ultra-rapid metabolizers (~2–10%) convert codeine to morphine excessively, risking respiratory depression. CYP2C19 poor metabolizers (~2–5% Caucasians, ~15–20% Asians) cannot activate clopidogrel (a prodrug), leading to treatment failure. FDA now recommends CYP2C19 genotyping before clopidogrel therapy.
Codeine, tramadol, and clopidogrel are prodrugs requiring CYP activation. Poor metabolizers get no benefit; ultra-rapid metabolizers of codeine may die from respiratory depression (especially neonates via breast milk). This is a board favorite.
07 Excretion & Renal Dosing
Renal excretion is the primary route of drug elimination. It involves three processes: glomerular filtration (free, unbound drug filtered at the glomerulus), tubular secretion (active transport of drug from peritubular capillaries into the tubular lumen — the most efficient mechanism), and tubular reabsorption (passive reabsorption of lipophilic, non-ionized drug from tubular lumen back into blood).
Key Renal Excretion Concepts
Concept
Detail
Clinical Relevance
Clearance (CL)
CL = (rate of elimination) / (plasma concentration); CL = Vd × ke
Determines maintenance dose: Dose rate = CL × Css
Half-life (t1/2)
t1/2 = 0.693 × Vd / CL
Steady state reached at ~4–5 half-lives; loading dose bypasses wait
Loading dose
LD = (Vd × Ctarget) / F
Achieves therapeutic level immediately (independent of clearance)
Maintenance dose
MD = (CL × Css) / F
Must be adjusted for renal impairment (reduced CL)
Zero-order kinetics
Constant amount eliminated per unit time (enzymes saturated)
Phenytoin, ethanol, aspirin (at toxic doses)
First-order kinetics
Constant fraction eliminated per unit time
Most drugs at therapeutic doses
Zero-Order Drugs
Mnemonic: "PEA" — Phenytoin, Ethanol, Aspirin (at high doses). These drugs exhibit saturation kinetics: small dose increases can cause disproportionate rises in plasma concentration, leading to toxicity. Always titrate carefully.
Renal Dose Adjustment
In renal impairment, drugs primarily excreted by the kidneys accumulate. The Cockcroft-Gault equation estimates CrCl: CrCl = [(140 − age) × weight (kg)] / [72 × serum Cr] (× 0.85 for females). Drugs requiring dose reduction in renal failure include: aminoglycosides, vancomycin, lithium, digoxin, metformin, enoxaparin, gabapentin, and acyclovir.
Other Routes of Excretion
Biliary excretion: Large, polar molecules (molecular weight >300 Da) may be excreted in bile → enterohepatic recirculation can prolong drug half-life (e.g., estrogens, digitoxin, morphine glucuronide). Pulmonary excretion: Volatile anesthetics eliminated via exhalation. Breast milk: Lipophilic, non-ionized drugs cross into breast milk (basic drugs concentrate because milk is slightly acidic, pH ~7.0).
08 Pharmacodynamics & Dose–Response
Dose–Response Relationships
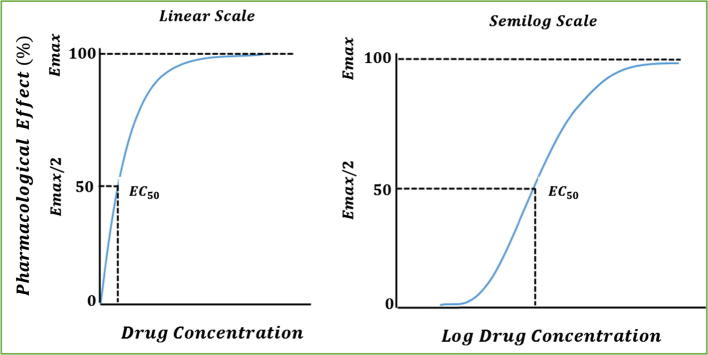
The graded dose–response curve plots drug concentration (x-axis, log scale) vs response magnitude (y-axis) for a single subject. Key parameters: EC50 (concentration at 50% Emax — measure of potency), Emax (maximal achievable effect — measure of efficacy). Potency compares EC50 values between drugs: a lower EC50 means higher potency (left-shifted curve). Efficacy compares Emax values: a higher Emax means greater efficacy.
Figure 11 — Graded Dose–Response Curves. The sigmoidal (log-concentration vs effect) curve illustrates key pharmacodynamic parameters. The EC50 (concentration producing 50% of maximal effect) reflects potency, while Emax (plateau height) reflects efficacy. A left-shifted curve indicates higher potency; a taller curve indicates greater efficacy.
Quantal Dose–Response
The quantal dose–response curve plots dose vs cumulative % of population responding (all-or-none response, e.g., sleep/no sleep). This yields ED50 (dose effective in 50% of population), TD50 (toxic dose in 50%), and LD50 (lethal dose in 50%). The therapeutic index TI = LD50 / ED50. A safer measure is the therapeutic window = TD1 / ED99.
Competitive vs Non-Competitive Antagonism
Feature
Competitive Antagonism
Non-Competitive Antagonism
Binding site
Same site as agonist (orthosteric)
Different site (allosteric) or irreversible
Overcome by increasing agonist?
Yes (surmountable)
No (insurmountable)
Effect on dose–response curve
Right-shift (increased EC50), Emax unchanged
Decreased Emax, EC50 may be unchanged
Example
Naloxone vs morphine, atropine vs ACh
Phenoxybenzamine vs norepinephrine
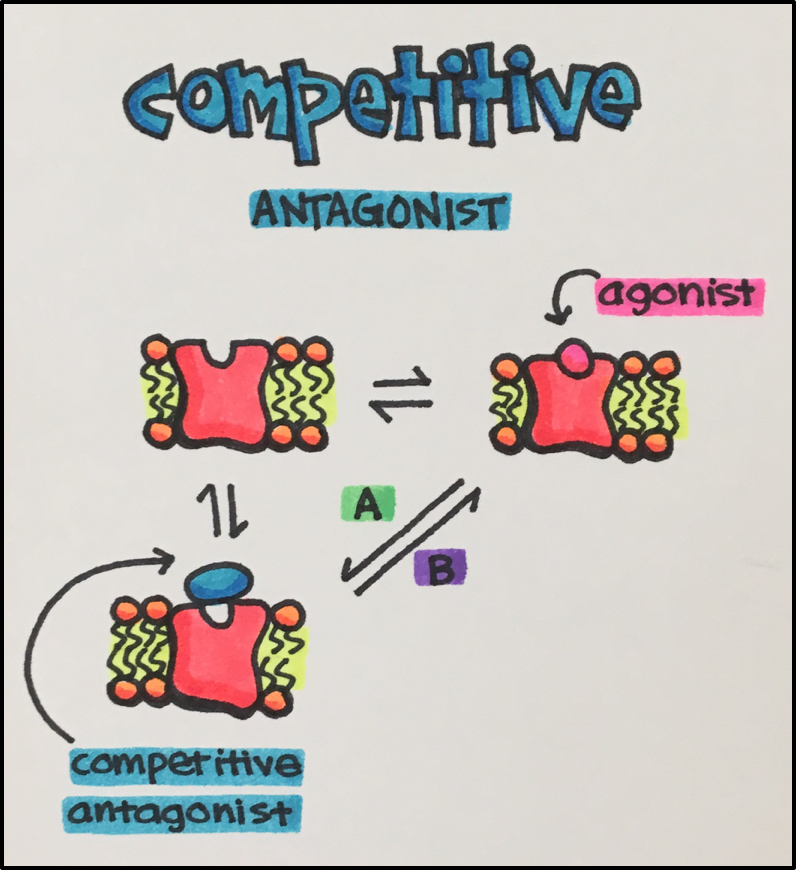
Figure 12 — Competitive Antagonism. A competitive antagonist binds the same (orthosteric) site as the agonist. Increasing antagonist concentration shifts the agonist dose–response curve progressively to the right (increased EC50), but the maximal response (Emax) is preserved because sufficiently high agonist concentrations can overcome the blockade.Figure 13 — Non-Competitive Antagonism. A non-competitive antagonist binds at an allosteric site or irreversibly at the orthosteric site. This reduces the maximal achievable response (Emax) regardless of agonist concentration, because the antagonist effectively removes receptors from the available pool. The curve is depressed rather than shifted.
On a dose–response curve: potency is position (left = more potent), efficacy is height (taller = more efficacious). A competitive antagonist shifts the curve right without changing the max. A non-competitive antagonist lowers the max. These are fundamental board concepts.
Tachyphylaxis & Tolerance
Tachyphylaxis is rapid loss of drug effect after repeated doses (minutes to hours) — due to receptor desensitization or depletion of mediator stores. Example: indirect sympathomimetics (e.g., ephedrine depletes NE stores). Tolerance is gradual loss of effect over days to weeks. Example: nitrate tolerance (give a nitrate-free interval), opioid tolerance (receptor down-regulation/desensitization).
09 Autonomic Nervous System Overview
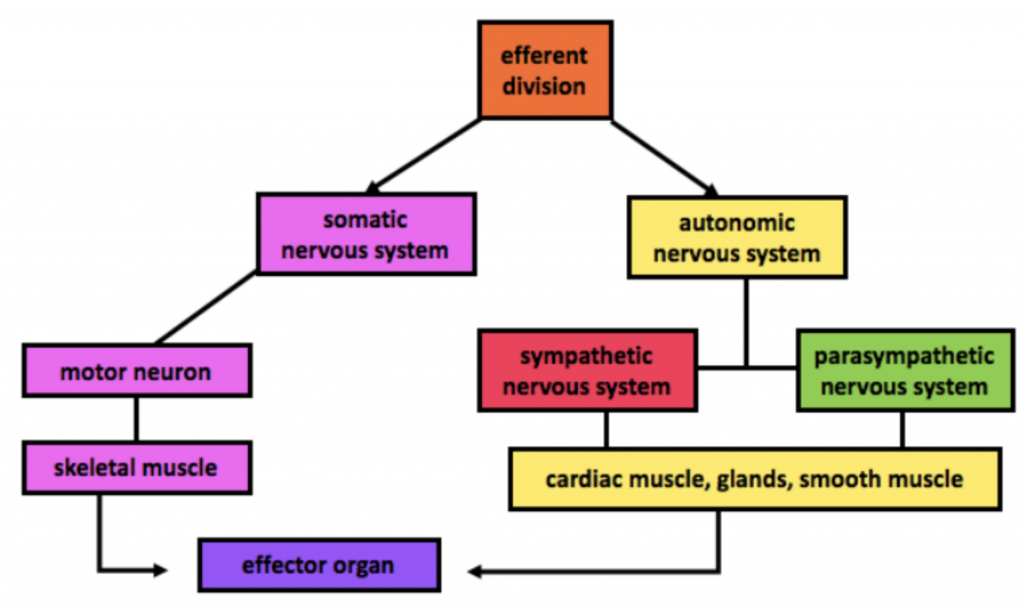
The autonomic nervous system (ANS) has two major divisions: sympathetic ("fight or flight") and parasympathetic ("rest and digest"). Both use a two-neuron chain: preganglionic neuron → ganglionic synapse → postganglionic neuron → effector organ.
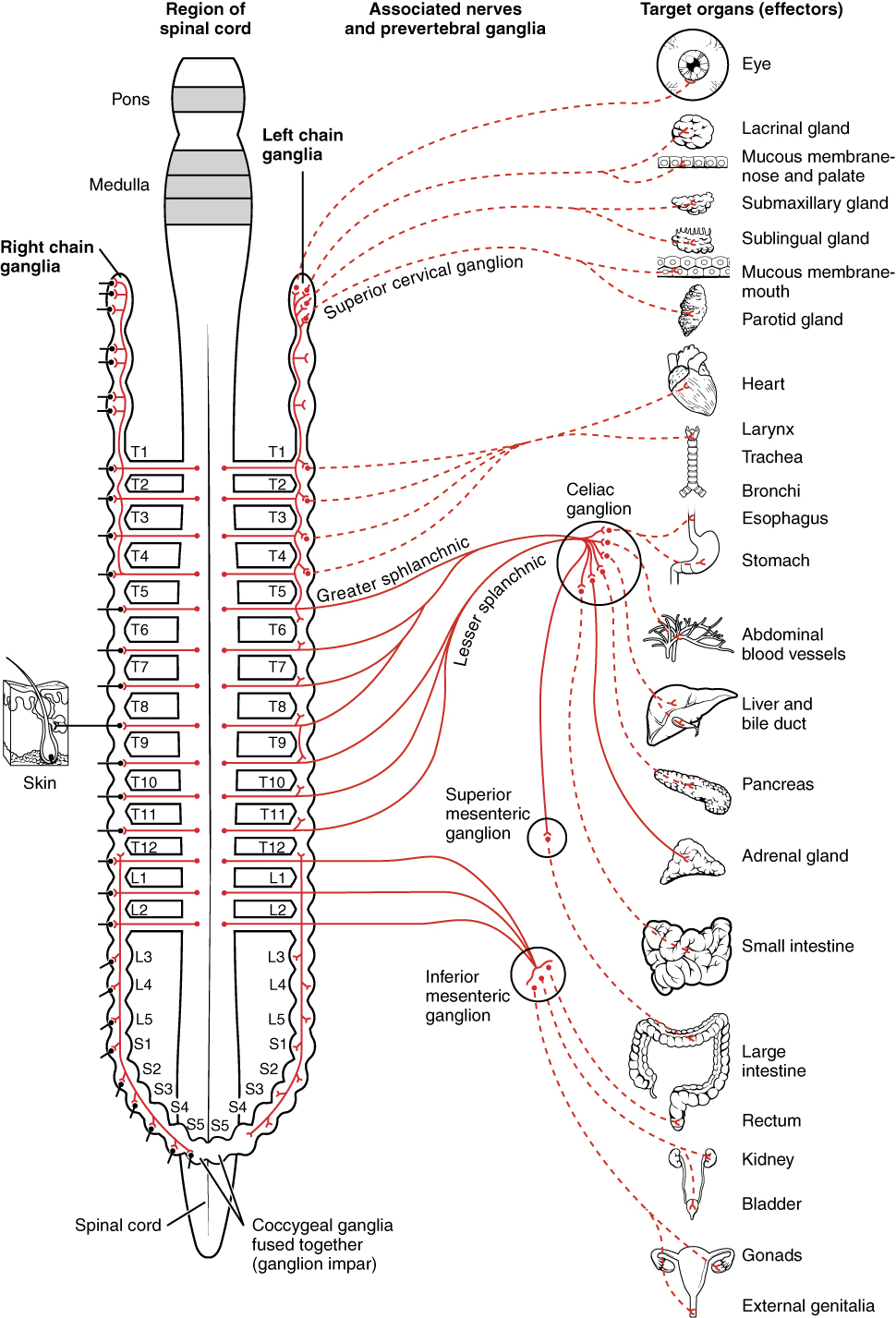
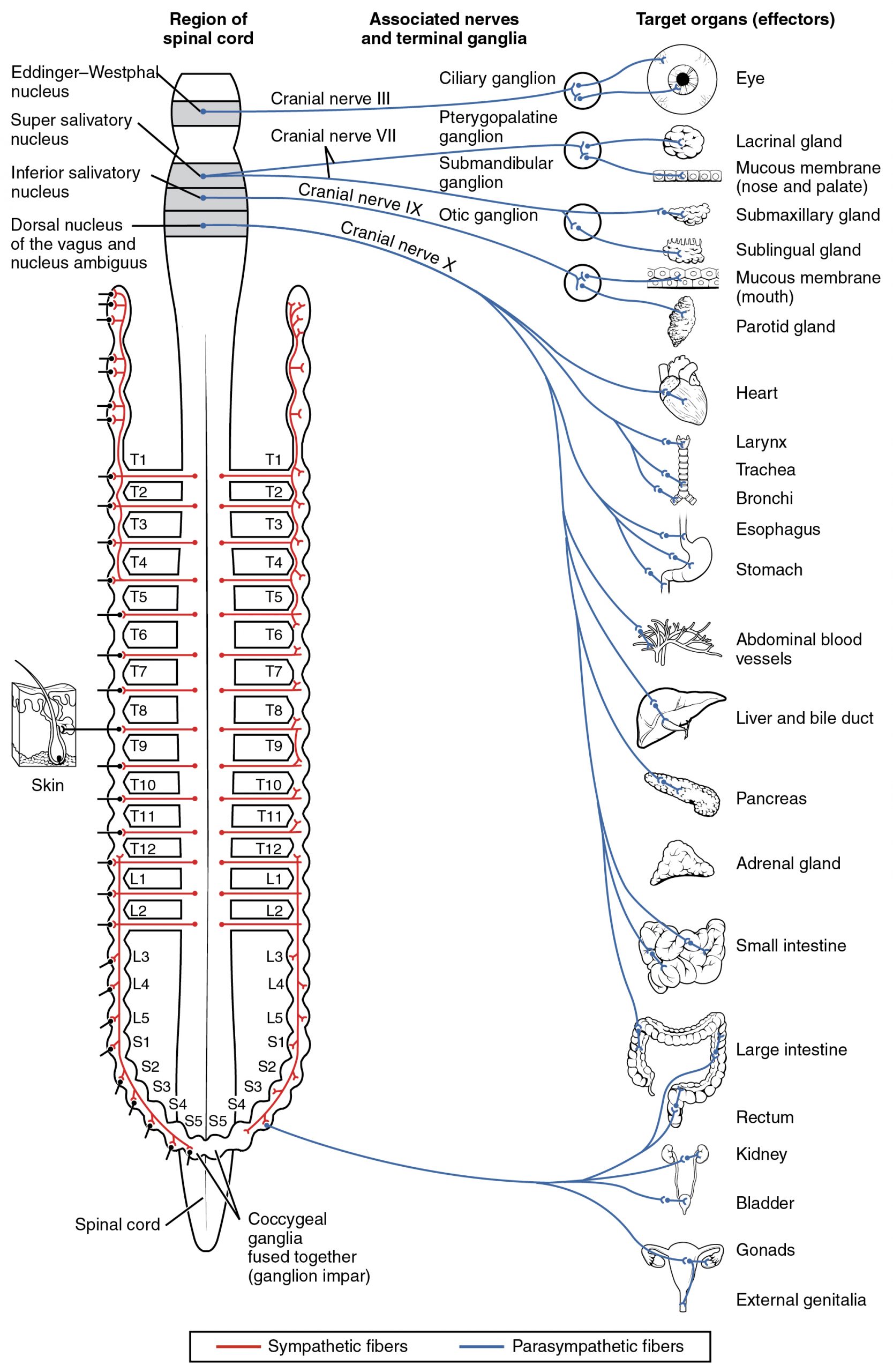
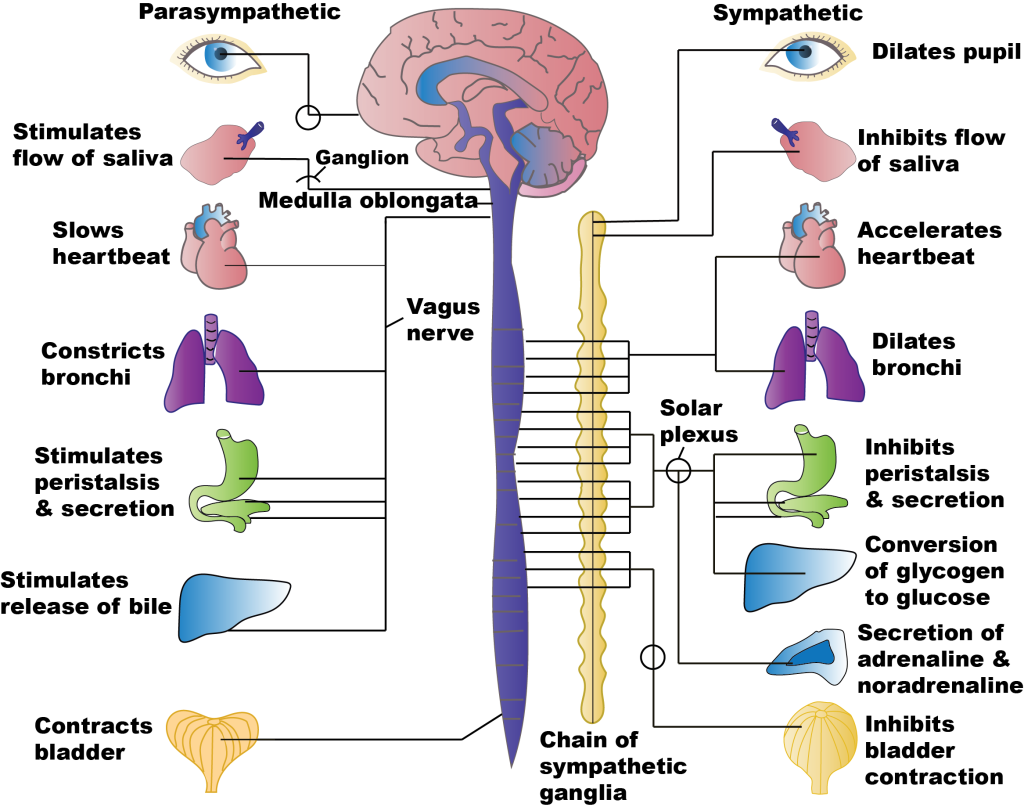
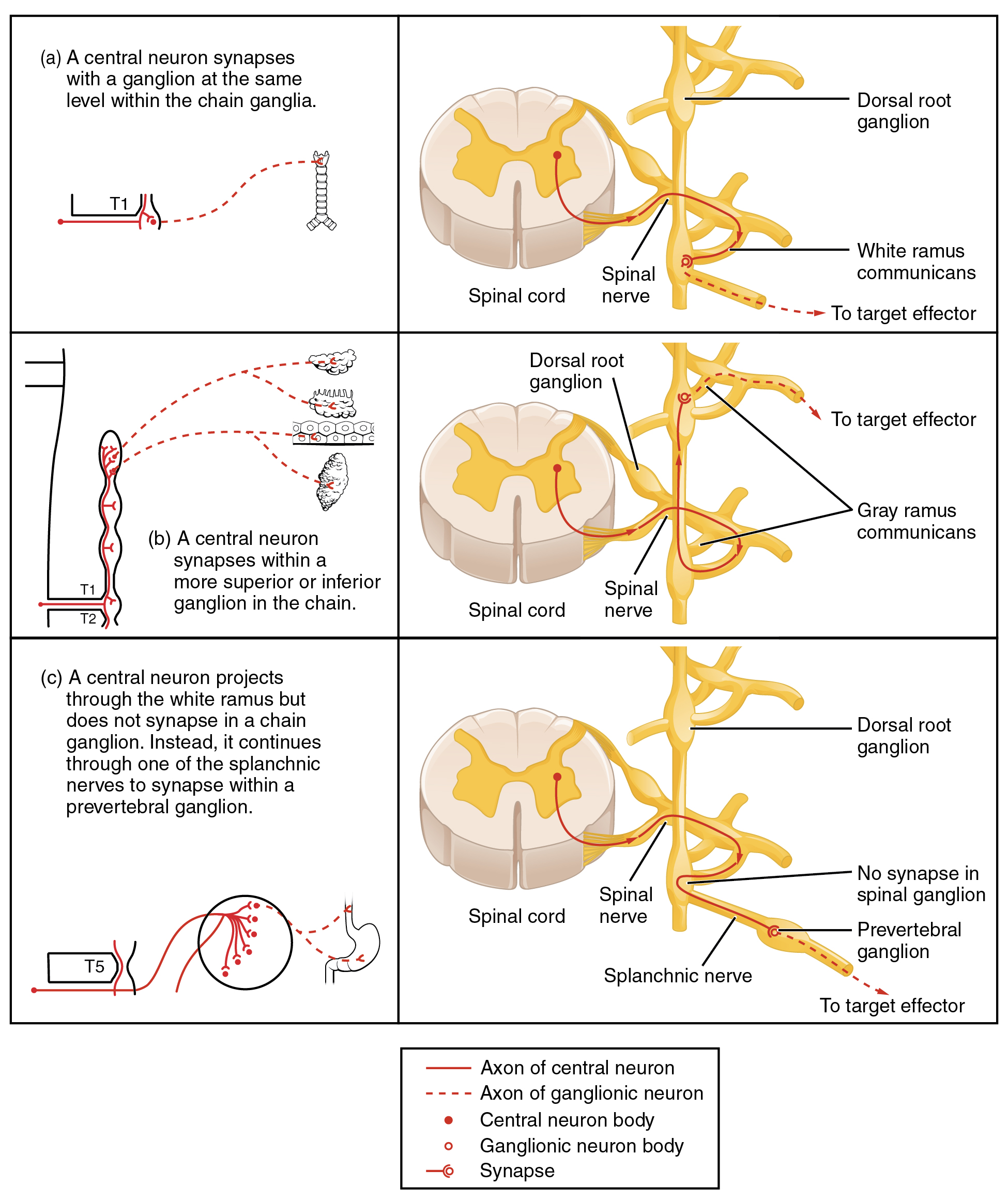
Figure 14 — ANS Neuron Pathways. Both divisions of the autonomic nervous system use a two-neuron chain. All preganglionic neurons release acetylcholine (ACh) at nicotinic NN receptors. Sympathetic postganglionic neurons release norepinephrine (NE) at adrenergic receptors (exception: sweat glands use ACh), while parasympathetic postganglionic neurons release ACh at muscarinic receptors.Figure 15 — Sympathetic Pathway. Sympathetic preganglionic neurons originate from the thoracolumbar spinal cord (T1–L2) and synapse in paravertebral or prevertebral ganglia. Short preganglionic and long postganglionic fibers release norepinephrine at target organs, mediating fight-or-flight responses including increased heart rate, bronchodilation, and vasoconstriction.Figure 16 — Parasympathetic Pathway. Parasympathetic preganglionic neurons originate from cranial nerves (CN III, VII, IX, X) and sacral spinal segments (S2–S4). Long preganglionic fibers synapse in ganglia near or within target organs. The vagus nerve (CN X) provides parasympathetic innervation to most thoracic and abdominal viscera.
Neurotransmitters & Receptors
Component
Sympathetic
Parasympathetic
Preganglionic NT
ACh (nicotinic NN)
ACh (nicotinic NN)
Postganglionic NT
Norepinephrine (NE) [exception: sweat glands use ACh]
ACh (muscarinic M1–5)
Adrenal medulla
ACh (NN) → releases epinephrine (80%) and NE (20%)
Figure 17 — Sympathetic vs Parasympathetic Effects on Organ Systems. Summary of opposing autonomic effects on the heart, lungs, eyes, GI tract, and bladder. The sympathetic system generally promotes energy expenditure and alertness, while the parasympathetic system promotes energy conservation and digestion.Figure 18 — Adrenal Medulla. The adrenal medulla functions as a modified sympathetic ganglion. Preganglionic sympathetic neurons synapse directly on chromaffin cells, which release epinephrine (~80%) and norepinephrine (~20%) into the bloodstream, producing systemic sympathetic effects that amplify and prolong the fight-or-flight response.
Norepinephrine Synthesis & Metabolism
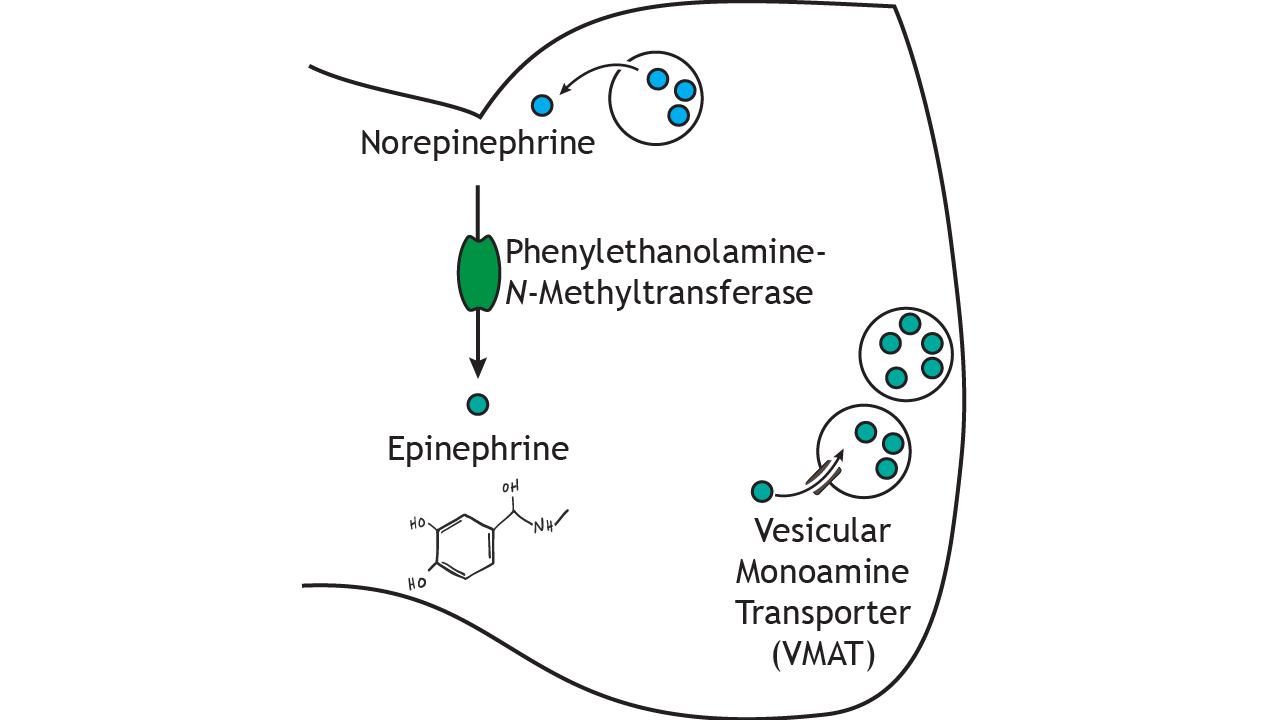
The catecholamine biosynthetic pathway: Tyrosine ⟶ (tyrosine hydroxylase, rate-limiting) DOPA ⟶ (DOPA decarboxylase) Dopamine ⟶ (dopamine β-hydroxylase, in vesicles) Norepinephrine ⟶ (PNMT, in adrenal medulla) Epinephrine. NE is removed from the synapse by: (1) reuptake-1 (into presynaptic neuron — blocked by TCAs, cocaine), (2) MAO (intraneuronally — inhibited by MAOIs), (3) COMT (extraneuronally — inhibited by entacapone). Metabolites: NE → normetanephrine (COMT) → VMA (vanillylmandelic acid). Urinary VMA and metanephrines are used to diagnose pheochromocytoma.
Figure 19 — Catecholamine Biosynthesis. The synthetic pathway: Tyrosine → DOPA (tyrosine hydroxylase, rate-limiting step) → Dopamine (DOPA decarboxylase) → Norepinephrine (dopamine β-hydroxylase, in synaptic vesicles) → Epinephrine (PNMT, in adrenal medulla only). Understanding this pathway is key to predicting the effects of drugs that inhibit or enhance specific enzymatic steps.
Acetylcholine Synthesis & Degradation
ACh is synthesized from choline + acetyl-CoA by choline acetyltransferase (ChAT) in the presynaptic terminal. After release, ACh is rapidly hydrolyzed by acetylcholinesterase (AChE) in the synaptic cleft. Choline is then recycled via a high-affinity choline transporter (blocked by hemicholinium). Vesicular ACh transport is blocked by vesamicol. ACh release from vesicles is blocked by botulinum toxin (inhibits SNARE-mediated exocytosis) and enhanced by black widow spider venom (α-latrotoxin).
Botulinum toxin blocks ACh release at the neuromuscular junction, causing flaccid paralysis. Therapeutic uses: dystonia, blepharospasm, hyperhidrosis, chronic migraine, cosmetic wrinkle reduction. Tetanus toxin blocks release of inhibitory neurotransmitters (glycine, GABA) in the spinal cord, causing spastic paralysis.
Myasthenia gravis, reversal of non-depolarizing NMJ blockade
Does not cross BBB (quaternary amine)
Pyridostigmine
Reversible (carbamate)
Myasthenia gravis (chronic treatment)
Longer-acting than neostigmine
Edrophonium
Reversible (short-acting)
Tensilon test (diagnosis of MG) — historical
Very short duration (~10 min)
Physostigmine
Reversible (carbamate)
Atropine/anticholinergic overdose, glaucoma
Crosses BBB (tertiary amine) — reverses central toxicity
Donepezil, rivastigmine, galantamine
Reversible
Alzheimer disease
Improve cholinergic transmission in CNS
Organophosphates (sarin, malathion)
Irreversible (phosphorylation)
Pesticides, nerve agents
Treat with atropine + pralidoxime (before "aging")
Neostigmine does NOT cross the BBB (quaternary amine) — use for peripheral effects. Physostigmine DOES cross the BBB (tertiary amine) — use for anticholinergic toxicity with central symptoms (delirium, seizures). This distinction is a board classic.
Muscarinic Antagonists (Anticholinergics)
Drug
Indications
Key Notes
Atropine
Bradycardia, organophosphate poisoning, mydriasis
Blocks M1–5; also used pre-operatively to reduce secretions
Ipratropium / Tiotropium
COPD, asthma (adjunct)
Inhaled — minimal systemic absorption; tiotropium is long-acting
Scopolamine
Motion sickness, preoperative antisecretory
Crosses BBB — can cause sedation, amnesia
Oxybutynin / Tolterodine
Overactive bladder, urge incontinence
Block M3 on detrusor; anticholinergic side effects
Benztropine / Trihexyphenidyl
Parkinson disease (tremor), EPS from antipsychotics
Central muscarinic blockade; caution in elderly (delirium)
Glycopyrrolate
Reduce secretions (preanesthetic), drooling
Quaternary amine; does not cross BBB
Anticholinergic Toxidrome
"Hot as a hare (hyperthermia, no sweating), Dry as a bone (dry mucous membranes, anhidrosis), Red as a beet (flushing), Blind as a bat (mydriasis, cycloplegia), Mad as a hatter (delirium, hallucinations), Full as a flask (urinary retention), Stuffed as a sausage (decreased bowel sounds)." Treatment: physostigmine for severe central symptoms; supportive care otherwise.
11 Adrenergic Agonists & Antagonists
Direct Sympathomimetics
Drug
Receptor Activity
Indications
Key Effects / Notes
Epinephrine
α1, α2, β1, β2
Anaphylaxis, cardiac arrest, asthma (acute)
Low dose: β2 vasodilation; high dose: α1 vasoconstriction
Norepinephrine
α1 > α2 > β1; minimal β2
Septic shock (first-line vasopressor)
↑SVR, ↑MAP; reflex bradycardia possible
Phenylephrine
α1 selective
Nasal decongestion, hypotension, mydriasis
Pure vasoconstriction; reflex bradycardia
Isoproterenol
β1 = β2 (non-selective β)
Refractory bradycardia, AV block
↑HR, ↑contractility, vasodilation; rarely used now
In pheochromocytoma: ALWAYS give α-blocker (phenoxybenzamine) BEFORE β-blocker. If a β-blocker is given first, unopposed α-stimulation causes hypertensive crisis. This is one of the most commonly tested pharmacology principles.
12 Antihypertensives
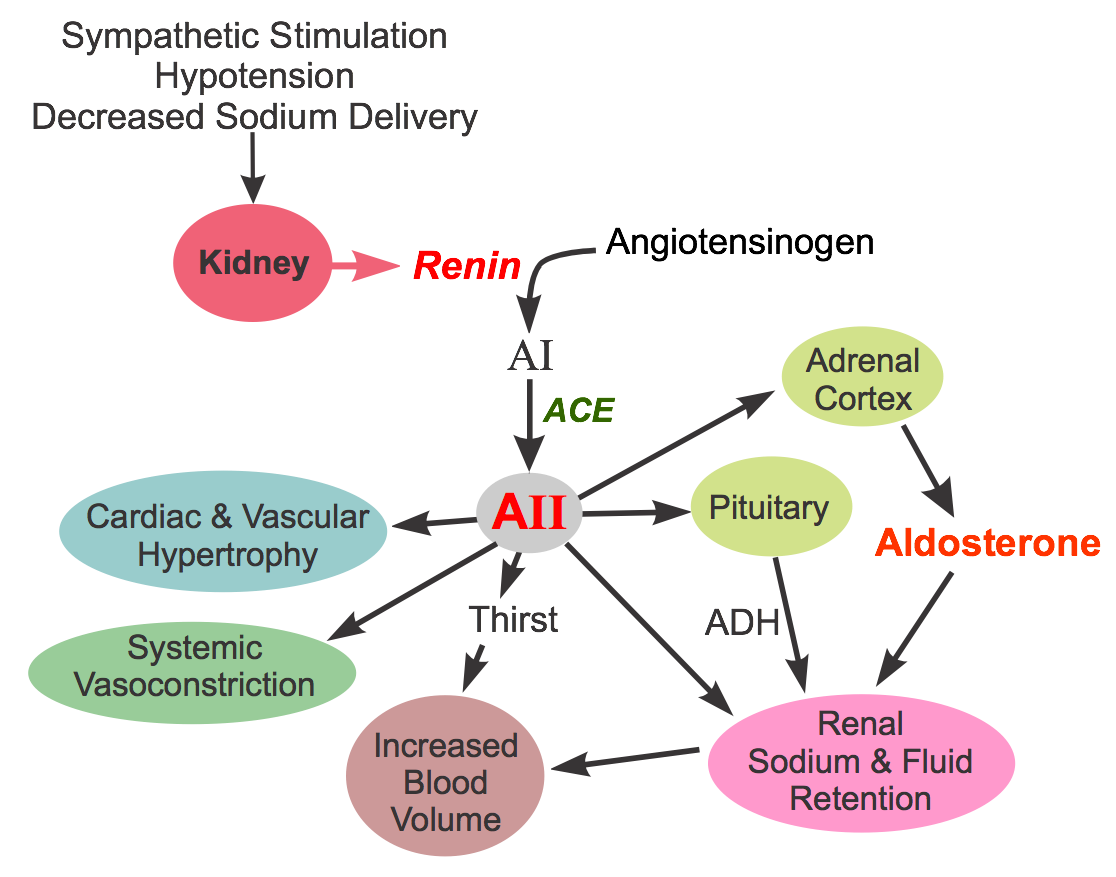
Figure 20 — Renin–Angiotensin–Aldosterone System (RAAS). Renin (released from the juxtaglomerular cells in response to decreased renal perfusion) cleaves angiotensinogen to angiotensin I, which is converted to angiotensin II by ACE. Angiotensin II causes vasoconstriction, aldosterone secretion, ADH release, and sympathetic activation. ACE inhibitors block the conversion step, while ARBs block the AT1 receptor directly.
ACE Inhibitors & ARBs
Class
Mechanism
Examples
Side Effects
Contraindications
ACE Inhibitors (-pril)
Block ACE → ↓angiotensin II, ↓aldosterone, ↑bradykinin
Constipation (verapamil), bradycardia, HF exacerbation; avoid with β-blockers
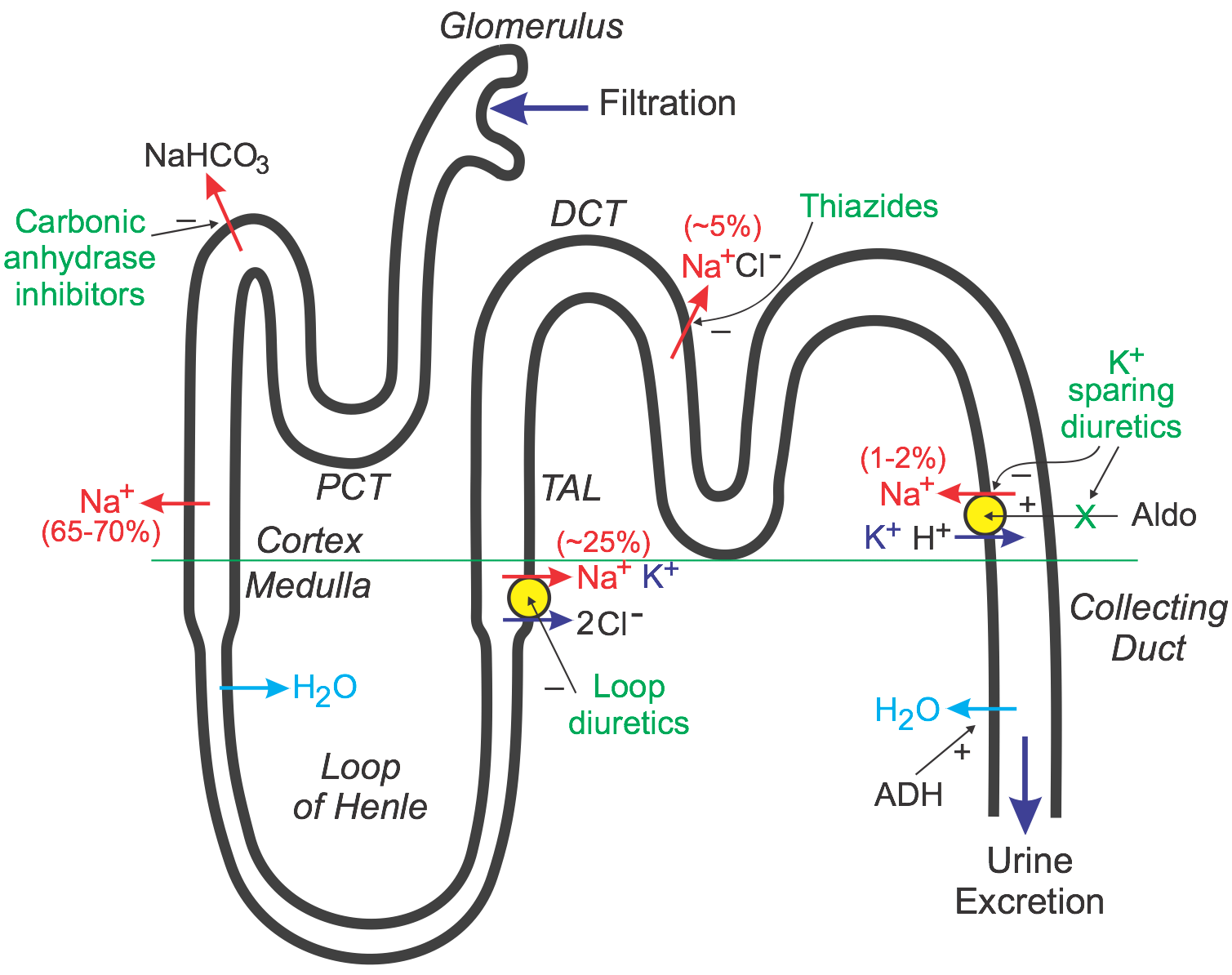
Figure 21 — Nephron Sites of Diuretic Action. Diuretics act at specific segments of the nephron. Carbonic anhydrase inhibitors (acetazolamide) act at the proximal tubule; loop diuretics (furosemide) act at the thick ascending limb of Henle; thiazides act at the distal convoluted tubule; and potassium-sparing diuretics (spironolactone, amiloride) act at the collecting duct. Osmotic diuretics (mannitol) act primarily in the proximal tubule and descending limb.
↑ICP treatment, rhabdomyolysis; contraindicated in anuria, HF
Diuretic Electrolyte Effects
Thiazides: hypokalemia + hypercalcemia (paradoxically increase Ca2+ reabsorption — useful in osteoporosis and calcium stone prevention). Loop diuretics: hypokalemia + hypocalcemia (wash out the medullary concentration gradient, lose Ca2+ — used for acute hypercalcemia). K+-sparing: hyperkalemia. Mnemonic for thiazide side effects: "HyperGLUC" — Glucose, Lipids, Uric acid, Calcium all go up.
13 Antiarrhythmics
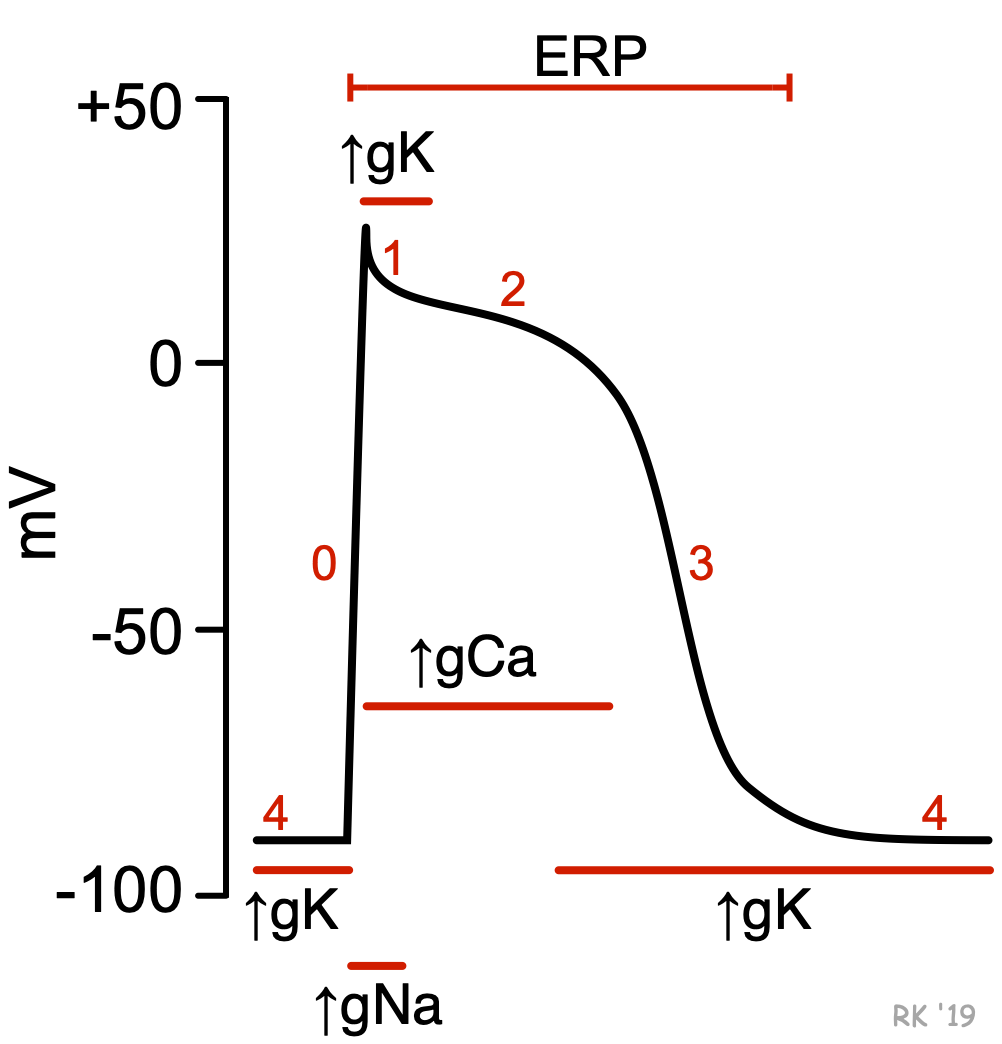
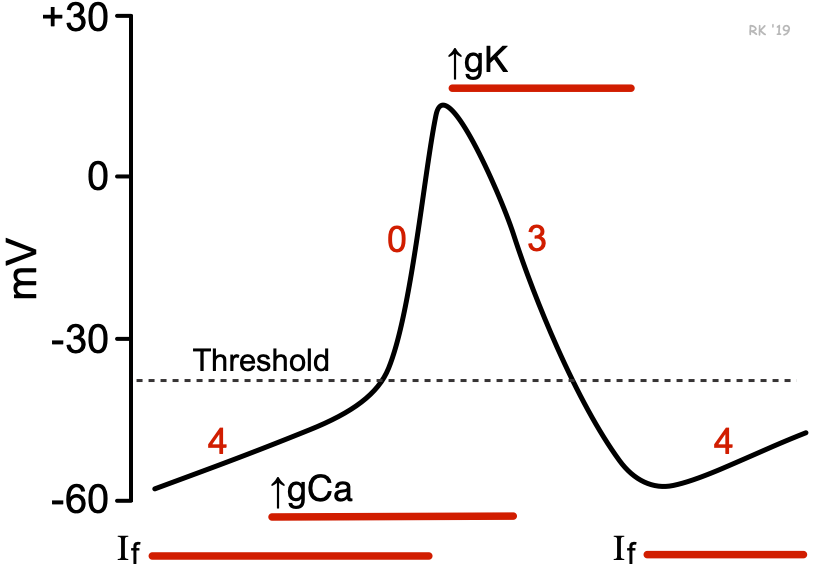
Figure 22 — Ventricular Action Potential. The ventricular (non-nodal) action potential consists of five phases: Phase 0 (rapid depolarization via Na+ influx), Phase 1 (early repolarization), Phase 2 (plateau via Ca2+ influx balanced by K+ efflux), Phase 3 (rapid repolarization via K+ efflux), and Phase 4 (resting potential). Antiarrhythmic drugs target specific ion channels in each phase: Class I blocks Na+ (Phase 0), Class III blocks K+ (Phase 3), and Class IV blocks Ca2+ (Phase 2).Figure 23 — SA Node (Pacemaker) Action Potential. Nodal cells lack a true Phase 1 and Phase 2. Phase 4 shows spontaneous depolarization driven by the funny current (If, mixed Na+/K+), Phase 0 is mediated by Ca2+ influx (slower than ventricular Phase 0), and Phase 3 is K+-mediated repolarization. Class II (β-blockers) and Class IV (CCBs) slow SA/AV node conduction. Ivabradine specifically blocks If to reduce heart rate.
Amiodarone has class I, II, III, and IV activity — it is the most broad-spectrum antiarrhythmic but also the most toxic. Remember its side effects with the mnemonic: "Amiodarone is TOO TOXIC" — Thyroid (hypo/hyper), Ocular (corneal microdeposits, optic neuropathy), Organ (pulmonary fibrosis, hepatotoxicity), Skin (blue-gray discoloration, photosensitivity), plus QT prolongation and peripheral neuropathy.
QT Prolongation
Drugs that prolong the QT interval risk torsades de pointes (polymorphic VT). Common culprits: Class IA (quinidine, procainamide), Class III (sotalol, dofetilide), macrolides, fluoroquinolones, antipsychotics (haloperidol, ziprasidone), methadone, ondansetron. Treatment of torsades: IV magnesium (first-line), overdrive pacing, isoproterenol.
14 Heart Failure & Antianginal Drugs
Heart Failure Pharmacotherapy
Drug Class
Mechanism
Mortality Benefit in HFrEF
Key Drugs
ACEi / ARB / ARNI
RAAS blockade; ARNI (sacubitril/valsartan) also ↑natriuretic peptides
The "four pillars" of guideline-directed medical therapy for HFrEF: ACEi/ARB/ARNI + β-blocker + MRA + SGLT2 inhibitor. All four reduce mortality. Initiate and titrate to target doses. Digoxin and diuretics improve symptoms but do not reduce mortality.
Antianginal Drugs
Drug
Mechanism
Effect
Notes
Nitroglycerin (sublingual, IV, patch)
Releases NO → venodilation > arterial dilation
↓Preload → ↓myocardial O2 demand
Headache, hypotension; contraindicated with PDE5 inhibitors; tolerance with continuous use
β-Blockers
↓HR, ↓contractility
↓Myocardial O2 demand
First-line chronic stable angina; avoid in Prinzmetal (variant) angina
CCBs (dihydropyridines)
Coronary vasodilation
↑O2 supply, ↓afterload
First-line for Prinzmetal angina (coronary vasospasm)
Ranolazine
Inhibits late Na+ current
↓Intracellular Ca2+ overload
Add-on for refractory angina; prolongs QT
15 Anticoagulants, Antiplatelets & Thrombolytics
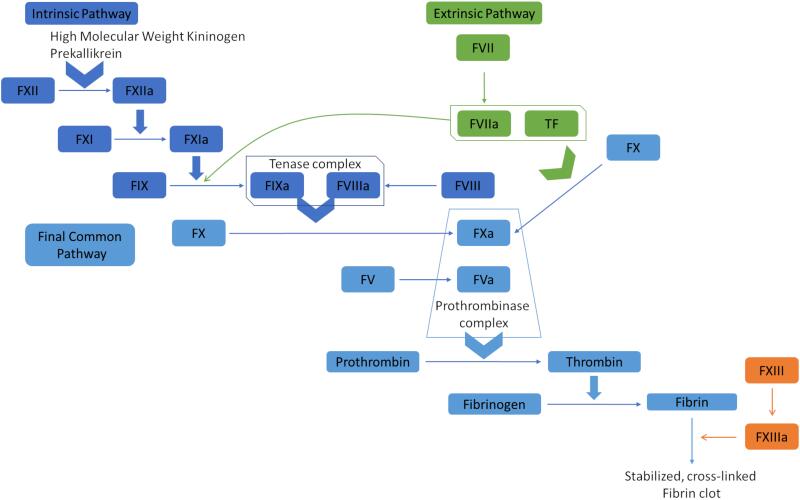
Figure 24 — Coagulation Cascade. The extrinsic pathway (tissue factor + Factor VII) and intrinsic pathway (Factors XII, XI, IX, VIII) converge at the common pathway (Factor X → prothrombin → thrombin → fibrin). Heparin (via antithrombin III) inhibits Factors IIa and Xa; warfarin inhibits synthesis of Factors II, VII, IX, and X; direct oral anticoagulants target Factor Xa (rivaroxaban, apixaban) or thrombin (dabigatran).
Anticoagulants
Drug
Mechanism
Monitoring
Reversal
Key Notes
Heparin (UFH)
Activates antithrombin III → inhibits IIa (thrombin) and Xa
aPTT
Protamine sulfate
HIT (heparin-induced thrombocytopenia) — type II is immune-mediated, causes paradoxical thrombosis
LMWH (enoxaparin)
Activates ATIII → primarily anti-Xa
Anti-Xa levels (if needed)
Protamine (partial)
More predictable PK; renal dosing needed
Warfarin
Inhibits vitamin K epoxide reductase → ↓factors II, VII, IX, X, protein C and S
PT / INR
Vitamin K, FFP, 4-factor PCC
Narrow TI; many drug/food interactions; teratogenic; initial hypercoagulable state (protein C/S t1/2 shorter)
DOACs: rivaroxaban, apixaban
Direct Xa inhibitors
Not routinely monitored
Andexanet alfa
Fewer interactions than warfarin; renal dosing for apixaban
More potent than clopidogrel; ticagrelor: dyspnea side effect; prasugrel: more bleeding
GP IIb/IIIa inhibitors (abciximab, eptifibatide, tirofiban)
Block fibrinogen binding to GP IIb/IIIa on platelets
ACS, PCI
IV only; risk of thrombocytopenia
Thrombolytics
Alteplase (tPA), reteplase, tenecteplase — activate plasminogen → plasmin → fibrin clot dissolution. Used in acute STEMI (if PCI unavailable within 120 min), acute ischemic stroke (within 4.5 hours), massive PE. Major risk: hemorrhage (including intracranial). Absolute contraindications include active internal bleeding, recent (3 months) intracranial surgery/stroke/head trauma, intracranial neoplasm, and suspected aortic dissection.
Warfarin initially creates a transient hypercoagulable state because protein C (anticoagulant, short t1/2 ~8 hrs) drops before factors II, IX, X (longer t1/2). This is why warfarin is bridged with heparin for the first 5–7 days. It also explains warfarin-induced skin necrosis (microvascular thrombosis in protein C-deficient patients).
Myopathy (esp. with statins), gallstones, hepatotoxicity
Niacin (vitamin B3)
Inhibits lipolysis in adipose → ↓VLDL synthesis
↓TG, ↓LDL, ↑↑HDL (best HDL raiser)
Niacin
Flushing (prostaglandin-mediated — pretreat with aspirin), hyperuricemia, hyperglycemia
Bile acid resins
Bind bile acids in gut → ↓enterohepatic recycling → ↑LDL receptor
↓LDL
Cholestyramine, colesevelam
GI upset, ↑TG, impair absorption of other drugs
Statins are the only lipid-lowering agents with proven mortality benefit in primary and secondary prevention of cardiovascular disease. Simvastatin and atorvastatin are CYP3A4 substrates — watch for interactions with CYP3A4 inhibitors (rhabdomyolysis risk). Pravastatin and rosuvastatin are NOT significantly CYP-metabolized and have fewer drug interactions.
Vasodilators & Other Cardiovascular Agents
Drug
Mechanism
Indication
Key Side Effects
Hydralazine
Direct arteriolar vasodilator (increases cGMP in vascular smooth muscle)
Hypotension; no mortality benefit demonstrated; rarely used now
Vasopressors for Shock
Agent
Receptor Activity
Primary Use
Key Effect
Norepinephrine
α1 > β1
Septic shock (first-line)
↑SVR, ↑MAP; some ↑CO via β1
Vasopressin
V1 receptors on vascular smooth muscle
Septic shock (adjunct to NE)
Catecholamine-independent vasoconstriction; useful in refractory septic shock
Epinephrine
α1, β1, β2
Anaphylaxis, cardiac arrest, refractory shock
↑SVR + ↑CO; may worsen splanchnic perfusion
Phenylephrine
Pure α1
Neurogenic shock, drug-induced hypotension
Pure vasoconstriction; reflex bradycardia; avoid in cardiogenic shock
Dobutamine
β1 > β2
Cardiogenic shock
↑Contractility, may ↓SVR slightly; inodilator
Dopamine
Dose-dependent: D1 → β1 → α1
Shock (second-line), symptomatic bradycardia
Low (<5): renal vasodilation; medium (5–10): cardiac; high (>10): vasoconstriction; more arrhythmogenic than NE
In septic shock, norepinephrine is the first-line vasopressor (Surviving Sepsis Campaign 2021). Vasopressin is added as a second agent if target MAP is not achieved. Epinephrine is an alternative. Dopamine is no longer recommended as first-line due to increased arrhythmia risk compared to norepinephrine. Dobutamine may be added if there is evidence of cardiac dysfunction (low CO despite adequate volume resuscitation).
17 Sedative-Hypnotics & Anxiolytics
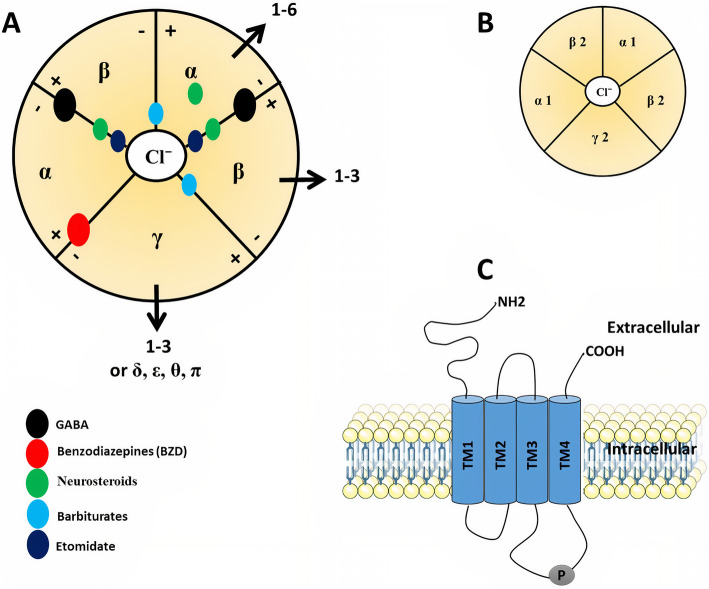
Figure 25 — GABAA Receptor Structure. The GABAA receptor is a ligand-gated chloride channel composed of five subunits (typically 2α, 2β, 1γ). GABA binds at the β/α interface to open the Cl− channel. Benzodiazepines bind at the α/γ interface (requiring a γ subunit for sensitivity), increasing the frequency of channel opening. Barbiturates bind at a separate site and increase the duration of channel opening; at high doses they can directly open the channel without GABA.
Anxiety, alcohol withdrawal seizures, muscle spasm, status epilepticus
Lorazepam
Intermediate / Intermediate
None (glucuronidation only)
Status epilepticus (first-line), anxiety, alcohol withdrawal
Midazolam
Rapid / Short
Minimal
Procedural sedation, preoperative, ICU sedation
Alprazolam
Intermediate / Short-intermediate
Minimal
Panic disorder, generalized anxiety
Chlordiazepoxide
Intermediate / Long
Yes
Alcohol withdrawal (classic choice)
Triazolam
Rapid / Ultra-short
None
Insomnia
BZD vs Barbiturate GABA Pharmacology
Benzodiazepines increase the frequency of Cl− channel opening. Barbiturates increase the duration of Cl− channel opening and at high doses can directly open the channel (without GABA). This explains why barbiturate overdose is more lethal — there is no ceiling effect. BZD reversal: flumazenil (competitive antagonist at BZD site; risk of seizures in chronic BZD users or mixed overdose).
Non-Benzodiazepine Hypnotics
Zolpidem, zaleplon, eszopiclone ("Z-drugs") — act at the α1 subunit of GABAA receptor (selective for sedation over anxiolysis/muscle relaxation). Short-acting; used for insomnia. Side effects: sleepwalking, sleep-driving, complex sleep behaviors. Suvorexant — orexin receptor antagonist for insomnia. Ramelteon — melatonin MT1/MT2 receptor agonist; no abuse potential.
18 Antidepressants & Mood Stabilizers
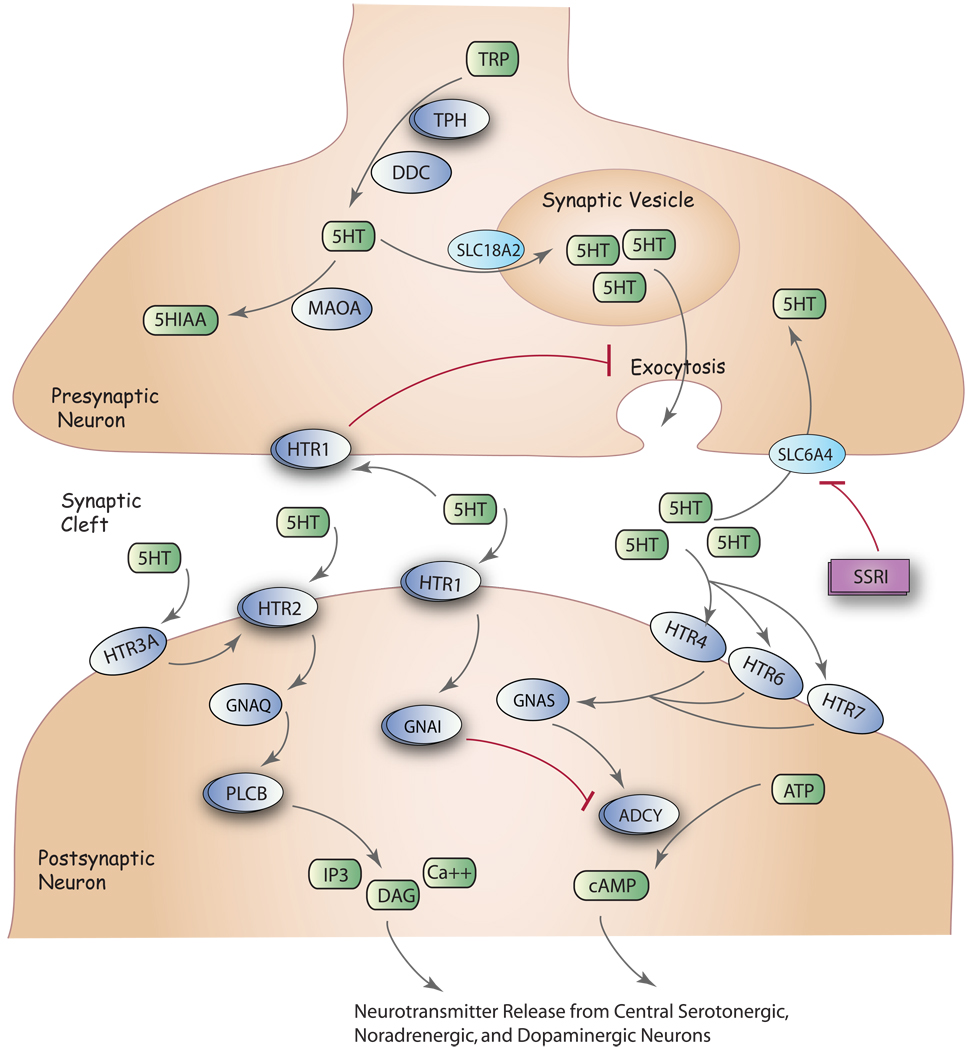
Figure 26 — SSRI Serotonin Pathway. At the serotonergic synapse, serotonin (5-HT) is synthesized from tryptophan, packaged into vesicles, and released into the synaptic cleft where it activates postsynaptic 5-HT receptors. SSRIs selectively block the serotonin reuptake transporter (SERT/5-HTT), increasing synaptic 5-HT levels and enhancing serotonergic neurotransmission. Pharmacogenomic variation in SERT, tryptophan hydroxylase, and 5-HT receptors influences individual drug response.
Bupropion: lowers seizure threshold, no sexual dysfunction, used for smoking cessation; mirtazapine: weight gain, sedation; trazodone: priapism
TCA overdose is a medical emergency: wide QRS on ECG (Na+ channel blockade), seizures, arrhythmias, and anticholinergic toxicity. Treatment: sodium bicarbonate (alkalinizes serum, increases protein binding, overcomes Na+ channel blockade) for QRS >100 ms. This is a must-know for boards and clinical practice.
Mood Stabilizers
Drug
Mechanism
Indications
Key Toxicity / Monitoring
Lithium
Not fully elucidated; inhibits IMPase, GSK-3β; modulates second messengers
Bipolar disorder (acute mania and maintenance)
Narrow TI (0.6–1.2 mEq/L); nephrotoxicity (diabetes insipidus — nephrogenic), hypothyroidism, Ebstein anomaly (teratogenic), tremor; toxicity enhanced by thiazides, NSAIDs, ACEi (all reduce renal Li clearance)
Valproate
↑GABA, blocks Na+/Ca2+ channels
Bipolar disorder, seizures, migraine
Hepatotoxicity, pancreatitis, thrombocytopenia, neural tube defects (teratogenic), weight gain
Carbamazepine
Na+ channel blockade
Bipolar disorder, trigeminal neuralgia, seizures
Agranulocytosis/aplastic anemia, SIADH, SJS (HLA-B*1502 in Asians), CYP inducer (auto-induction)
Lamotrigine
Na+ channel blockade, ↓glutamate
Bipolar depression (maintenance), seizures
SJS/TEN (slow titration required); relatively well tolerated
Serotonin Syndrome
Caused by excess serotonergic activity (e.g., MAOI + SSRI, meperidine + MAOI, linezolid + SSRI). Classic triad: (1) Altered mental status (agitation, confusion), (2) Autonomic instability (hyperthermia, tachycardia, diaphoresis, diarrhea), (3) Neuromuscular hyperactivity (myoclonus, hyperreflexia, clonus — especially lower extremity). Treatment: stop offending drug, cyproheptadine (5-HT2A antagonist), supportive care. Distinguish from NMS (lead-pipe rigidity, no clonus, caused by dopamine antagonists).
19 Antipsychotics
First-Generation (Typical) Antipsychotics
Mechanism: Block D2 receptors in the mesolimbic pathway (therapeutic effect on positive symptoms) but also block D2 in other pathways (causing side effects).
Potency
Examples
Characteristic Side Effects
High potency
Haloperidol, fluphenazine, pimozide
More EPS (dystonia, akathisia, parkinsonism, tardive dyskinesia), less sedation/anticholinergic effects
Low potency
Chlorpromazine, thioridazine
More sedation, anticholinergic effects, orthostatic hypotension; less EPS. Thioridazine: retinal deposits, QT prolongation
Second-Generation (Atypical) Antipsychotics
Drug
Key Features
Unique Side Effects
Clozapine
Most effective for treatment-resistant schizophrenia; low EPS risk
Neurotoxic metabolite (normeperidine) → seizures; avoid in renal failure and with MAOIs (serotonin syndrome)
Buprenorphine
Partial μ agonist, κ antagonist
Ceiling effect for respiratory depression; used in opioid use disorder (with naloxone = Suboxone)
Naloxone
μ, κ, δ antagonist
Opioid overdose reversal; short t1/2 (30–90 min) — may need repeat doses; precipitates withdrawal
Naltrexone
μ, κ, δ antagonist (long-acting)
Maintenance therapy for opioid and alcohol use disorders; oral or monthly IM injection
Naloxone has a shorter half-life than most opioids. After reversing an overdose, the patient must be monitored for re-sedation and respiratory depression as the naloxone wears off. Fentanyl overdose may require higher or repeated doses of naloxone due to fentanyl's high receptor affinity.
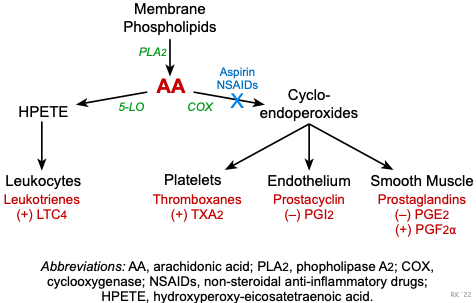
Figure 27 — Prostaglandin Pathway and NSAID Targets. Membrane phospholipids are converted to arachidonic acid by phospholipase A2. COX-1 (constitutive) and COX-2 (inducible) convert arachidonic acid to prostaglandins and thromboxane A2. Non-selective NSAIDs block both COX-1 and COX-2; selective COX-2 inhibitors (celecoxib) spare COX-1, reducing GI side effects but increasing cardiovascular risk due to unopposed TXA2 activity.
Non-Opioid Analgesics
NSAIDs (ibuprofen, naproxen, ketorolac, indomethacin): Inhibit COX-1/COX-2 → ↓prostaglandin synthesis. Side effects: GI ulceration/bleeding (COX-1), renal vasoconstriction (AKI), platelet dysfunction, cardiovascular risk (especially COX-2 selective). Acetaminophen: centrally acting analgesic/antipyretic; no anti-inflammatory effect. Hepatotoxic in overdose (NAPQI metabolite depletes glutathione) — antidote is N-acetylcysteine (NAC). Celecoxib: selective COX-2 inhibitor; less GI toxicity but increased cardiovascular risk.
NSAID Pharmacology in Detail
Drug
COX Selectivity
Key Features
Aspirin
Irreversible COX-1 > COX-2
Antiplatelet at low dose (81 mg); analgesic/anti-inflammatory at higher doses; Reye syndrome in children
Ibuprofen
Non-selective COX-1/COX-2
Most common OTC NSAID; GI, renal, CV risk; can interfere with aspirin's antiplatelet effect
Naproxen
Non-selective COX-1/COX-2
Longer t1/2 (BID dosing); possibly lower CV risk than other NSAIDs
Indomethacin
Non-selective
Potent; used for gout flares, PDA closure (neonates); highest GI risk
Ketorolac
Non-selective
IV/IM NSAID for acute pain; limit to 5 days (GI/renal toxicity)
Celecoxib
Selective COX-2
Less GI bleeding; increased CV risk (thrombotic events); sulfonamide allergy caution
COX-1 vs COX-2
COX-1 is constitutive (housekeeping): maintains gastric mucosal protection (PGE2), renal perfusion (PGI2), and platelet aggregation (TXA2). Inhibiting COX-1 causes GI ulcers, renal vasoconstriction, and antiplatelet effects. COX-2 is inducible (inflammation): mediates pain, fever, and inflammation. Selective COX-2 inhibitors spare the stomach but increase thrombotic risk (PGI2 is COX-2 dependent in endothelium; loss of PGI2 tips the balance toward TXA2-mediated platelet aggregation).
Status epilepticus (first-line), acute seizure clusters
Sedation, respiratory depression, tolerance
For status epilepticus: first-line is IV lorazepam (or IM midazolam if no IV access). If seizures persist, give IV fosphenytoin (or phenytoin, valproate, levetiracetam). If refractory, proceed to continuous infusion (midazolam, propofol, or pentobarbital) with EEG monitoring.
Parkinson Disease Drugs
Drug
Mechanism
Key Notes
Levodopa/carbidopa
Levodopa is a DA precursor; carbidopa inhibits peripheral DOPA decarboxylase (prevents peripheral conversion)
Most effective for motor symptoms; long-term: on-off phenomenon, dyskinesias, wearing off
Dopamine agonists (pramipexole, ropinirole)
Direct D2/D3 agonists
Monotherapy in early PD or adjunct; impulse control disorders, orthostatic hypotension
Selegiline, rasagiline
MAO-B inhibitors → ↓DA breakdown
Early PD monotherapy or adjunct; selegiline metabolized to amphetamine
Tremor-predominant PD; also treats drug-induced EPS; avoid in elderly (delirium)
22 Antibacterials
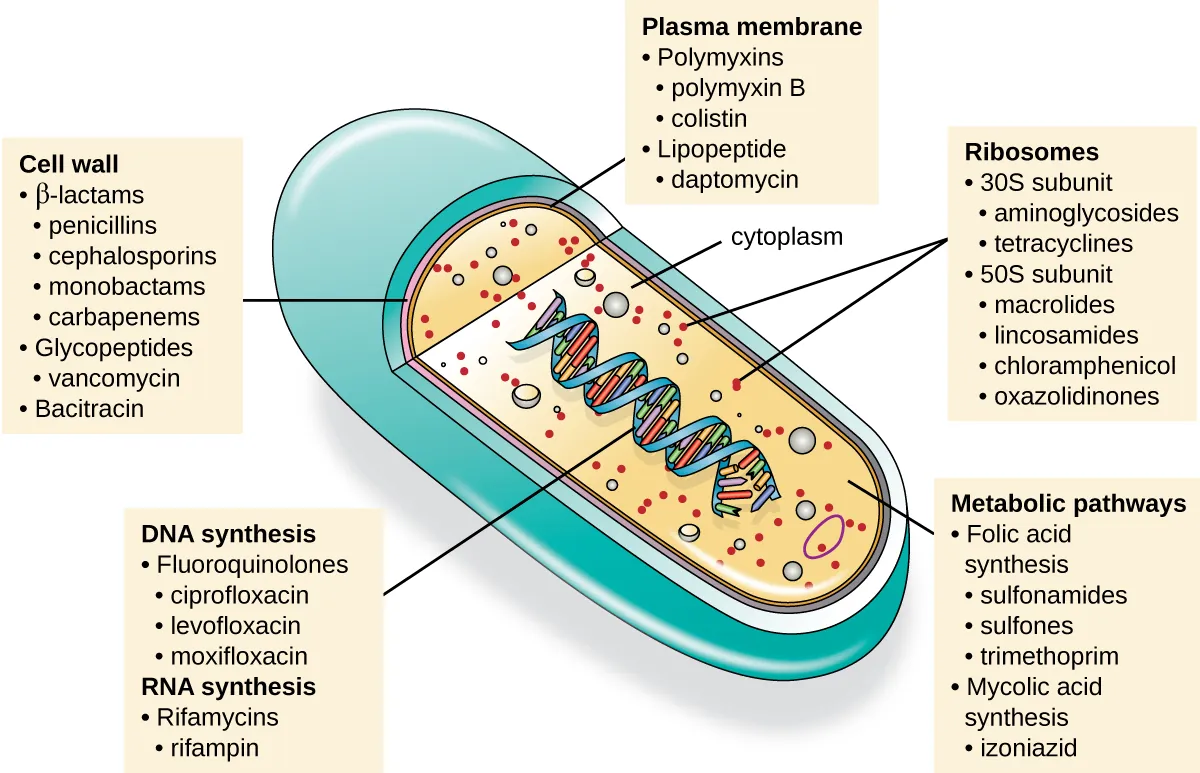
Figure 28 — Antibiotic Targets on the Bacterial Cell. Antibiotics exploit five major targets unique to or sufficiently different in bacteria: (1) cell wall synthesis (penicillins, cephalosporins, carbapenems, vancomycin), (2) cell membrane integrity (daptomycin, polymyxins), (3) protein synthesis at 30S or 50S ribosomal subunits, (4) nucleic acid synthesis (fluoroquinolones, rifampin, metronidazole), and (5) folate metabolism (sulfonamides, trimethoprim).
Cell Wall Synthesis Inhibitors
Class
Mechanism
Spectrum / Examples
Key Side Effects / Resistance
Penicillins
Bind PBPs → inhibit transpeptidation (cross-linking of peptidoglycan)
Red man syndrome (histamine release — slow infusion), nephrotoxicity, ototoxicity; VRE resistance: D-Ala-D-Lac substitution
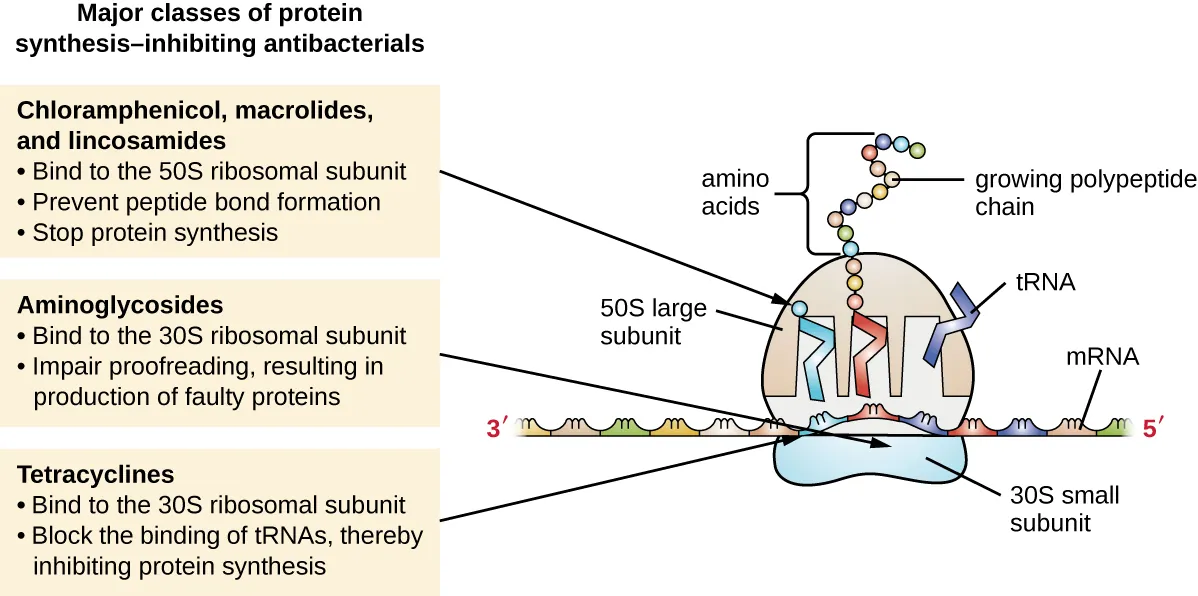
Figure 29 — Protein Synthesis Inhibitor Targets on the Bacterial Ribosome. Antibiotics target the 30S subunit (aminoglycosides cause misreading; tetracyclines block tRNA binding) or the 50S subunit (macrolides and clindamycin block translocation; chloramphenicol blocks peptidyl transferase; linezolid blocks initiation complex formation). These drugs selectively target the prokaryotic 70S ribosome, sparing the eukaryotic 80S ribosome.
UTIs, PJP prophylaxis/treatment, MRSA (CA-MRSA); hyperkalemia, bone marrow suppression, SJS, kernicterus in neonates
Metronidazole
Forms toxic free radicals damaging DNA
Metronidazole
Anaerobes (Bacteroides, C. difficile), protozoa (Giardia, Entamoeba, Trichomonas); disulfiram-like reaction with alcohol, metallic taste, peripheral neuropathy
Rifamycins
Inhibit DNA-dependent RNA polymerase
Rifampin, rifabutin
TB treatment (combination therapy); potent CYP inducer (turns body fluids orange); rifabutin: less CYP induction (used with antiretrovirals)
Daptomycin
Depolarizes cell membrane (gram+ only)
Daptomycin
MRSA bacteremia, endocarditis; inactivated by surfactant — cannot use for pneumonia; monitor CPK (myopathy)
Daptomycin is inactivated by pulmonary surfactant and must NOT be used for pneumonia. For MRSA pneumonia, use vancomycin or linezolid instead. This is a frequently tested distinction.
Porin mutations in gram-negative bacteria (carbapenem resistance in Pseudomonas)
Efflux pumps
Tetracycline resistance, multidrug-resistant Pseudomonas, P-glycoprotein in fungi
Target bypass
VRE: D-Ala-D-Lac substitution (vancomycin cannot bind); MRSA: alternative PBP2a
Bactericidal vs Bacteriostatic
Classification
Bactericidal (kill bacteria): Penicillins, cephalosporins, carbapenems, vancomycin, aminoglycosides, fluoroquinolones, metronidazole, daptomycin, isoniazid. Bacteriostatic (inhibit growth): Tetracyclines, macrolides (usually), chloramphenicol, clindamycin, TMP-SMX, linezolid. Note: bacteriostatic drugs can be bactericidal at high concentrations or against certain organisms. In immunocompromised patients and endocarditis/meningitis, bactericidal agents are generally preferred.
Antimicrobial Prophylaxis — Key Scenarios
Scenario
Prophylactic Agent
Surgical prophylaxis (clean/clean-contaminated)
Cefazolin (1st-gen cephalosporin) within 60 min of incision
Dental procedures in high-risk cardiac patients
Amoxicillin (or clindamycin if penicillin allergic)
Glucocorticoids (prednisone, prednisolone, dexamethasone, hydrocortisone) — bind intracellular receptors → modulate gene transcription → anti-inflammatory and immunosuppressive effects. Side effects (chronic use): Cushing syndrome, osteoporosis, adrenal suppression, hyperglycemia, immunosuppression, cataracts, avascular necrosis, myopathy, psychiatric effects, poor wound healing. Dexamethasone has the longest duration and highest potency (no mineralocorticoid activity). Fludrocortisone is a synthetic mineralocorticoid used for adrenal insufficiency (salt retention).
Never abruptly stop chronic glucocorticoids — the hypothalamic-pituitary-adrenal axis is suppressed and abrupt withdrawal causes adrenal crisis (hypotension, shock). Taper gradually. Patients on chronic steroids need stress-dose steroids during surgery or acute illness.
GI Pharmacology
Drug Class
Mechanism
Examples
Indications / Notes
Proton pump inhibitors (PPIs)
Irreversibly inhibit H+/K+-ATPase (proton pump) on parietal cells
Part of H. pylori triple/quadruple therapy; black tongue/stool
H. pylori eradication typically uses triple therapy: PPI + clarithromycin + amoxicillin (or metronidazole) for 14 days. Quadruple therapy (PPI + bismuth + metronidazole + tetracycline) is used in penicillin allergy or clarithromycin-resistant areas. Confirm eradication with urea breath test or stool antigen at least 4 weeks after treatment completion.
Other Endocrine Agents
Drug
Mechanism
Indication
Tamoxifen
SERM (estrogen receptor antagonist in breast, agonist in bone/endometrium)
ER+ breast cancer (adjuvant); increases risk of endometrial cancer and DVT
Raloxifene
SERM (agonist in bone, antagonist in breast/endometrium)
Osteoporosis prevention; DVT risk but no endometrial cancer risk
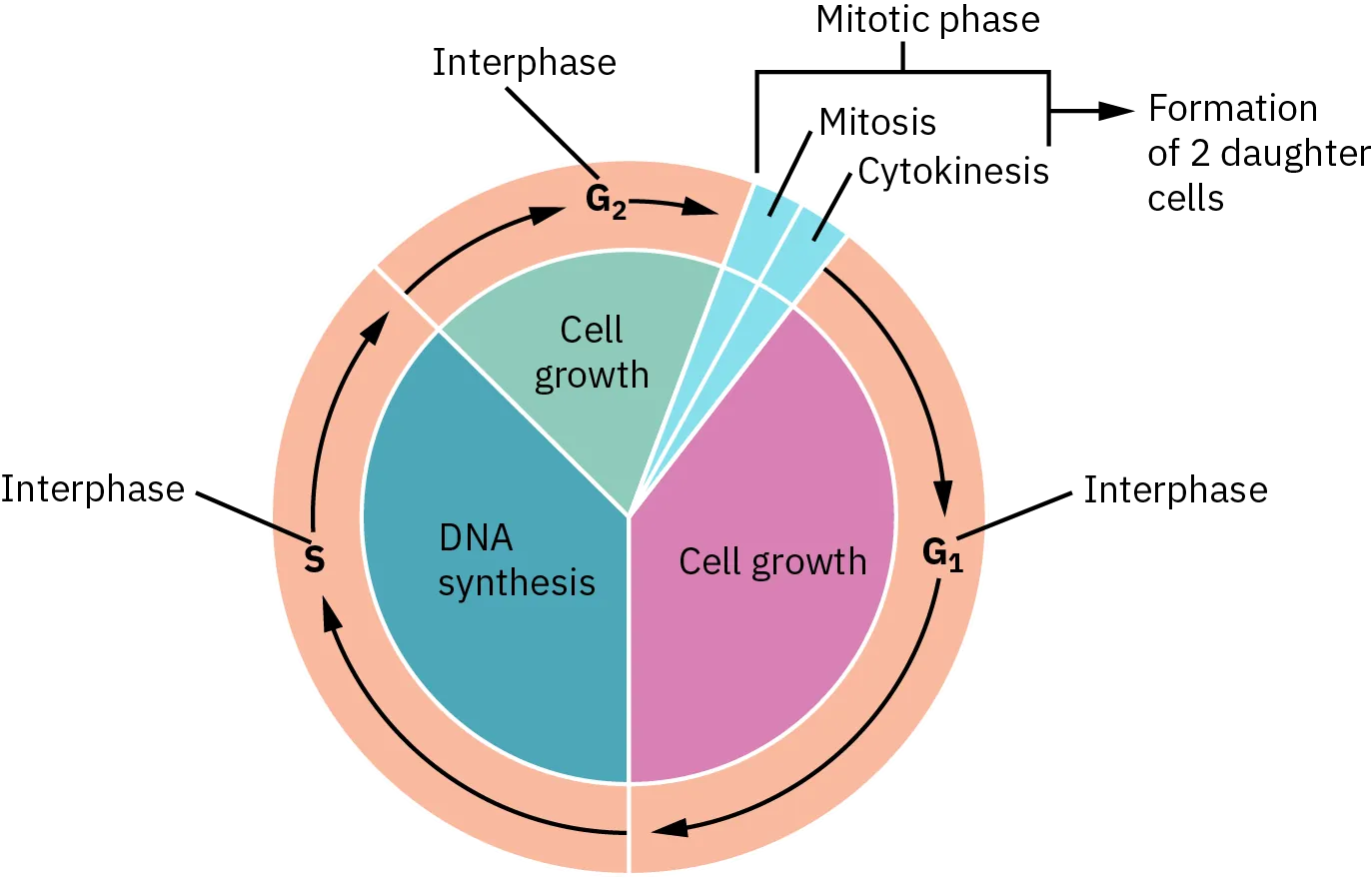
Figure 30 — Cell Cycle and Chemotherapy Drug Targets. The cell cycle consists of G1 (growth), S (DNA synthesis), G2 (preparation for mitosis), and M (mitosis) phases. Cell-cycle-specific (CCS) agents act during particular phases: antimetabolites (S phase), vinca alkaloids and taxanes (M phase). Cell-cycle-nonspecific (CCNS) agents such as alkylating agents and platinum compounds can act in any phase, including G0 resting cells.
Methotrexate: myelosuppression, hepatotoxicity, pneumonitis (rescue with leucovorin); 5-FU: myelosuppression, hand-foot syndrome; 6-MP: metabolized by XO (reduce dose with allopurinol)
Doxorubicin cardiotoxicity is irreversible and dose-dependent (dilated cardiomyopathy). Monitor LVEF serially. Dexrazoxane (iron chelator) reduces free radical damage and is cardioprotective. Bleomycin causes pulmonary fibrosis. Vincristine causes neuropathy but spares the bone marrow. These associations are board staples.
Hyperlipidemia, myelosuppression, impaired wound healing; NOT nephrotoxic (unlike calcineurin inhibitors)
Calcineurin Inhibitor vs mTOR Inhibitor
Cyclosporine and tacrolimus are calcineurin inhibitors — both cause nephrotoxicity. Sirolimus is an mTOR inhibitor that does NOT cause nephrotoxicity but causes hyperlipidemia and impairs wound healing. All three are used in transplant medicine. In drug-eluting stents, sirolimus/everolimus prevent restenosis via antiproliferative effects on smooth muscle cells.
Respiratory Pharmacology
Drug Class
Mechanism
Examples
Key Notes
Short-acting β2 agonists (SABAs)
Bronchial smooth muscle relaxation via β2 → Gs → ↑cAMP
Albuterol, levalbuterol
Rescue inhaler; tremor, tachycardia, hypokalemia
Long-acting β2 agonists (LABAs)
Same as SABA, sustained duration (12 hr)
Salmeterol, formoterol
Never use as monotherapy (black box — use with ICS); maintenance
First-line for anaphylaxis; IM into anterolateral thigh; repeat every 5–15 min if needed
Cromolyn sodium
Mast cell stabilizer → prevents degranulation
Cromolyn
Prophylaxis only (exercise-induced asthma, allergic conjunctivitis); not for acute symptoms
In anaphylaxis, epinephrine is the ONLY first-line treatment. Do not delay epinephrine for antihistamines or steroids. Antihistamines (H1 + H2 blocker) and corticosteroids are adjunctive and help prevent biphasic reactions but do not reverse the immediate life-threatening airway/hemodynamic compromise.
Displaces CO from hemoglobin; t1/2 of COHb: 5 hr room air, 1.5 hr 100% O2, 20 min hyperbaric
Methotrexate
Leucovorin (folinic acid)
Bypasses DHF reductase block; "leucovorin rescue"
For methanol or ethylene glycol poisoning, fomepizole is preferred over ethanol as an alcohol dehydrogenase inhibitor (easier to dose, fewer side effects). Dialysis is indicated for severe cases (renal failure, severe acidosis, very high levels, visual symptoms with methanol).
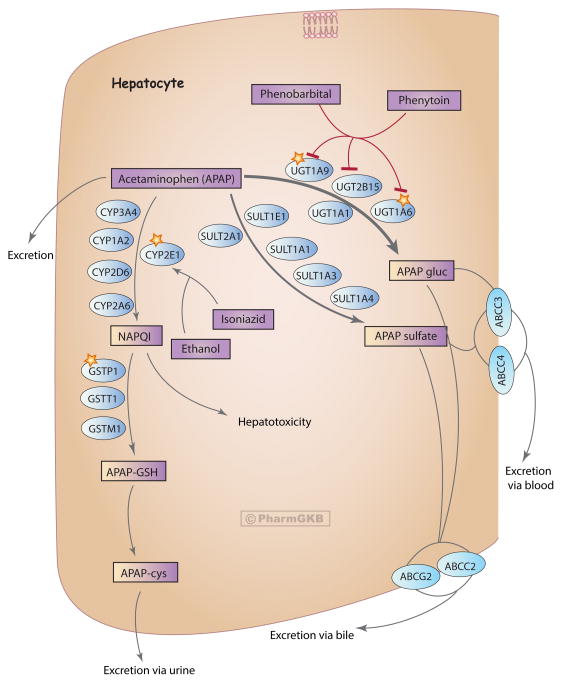
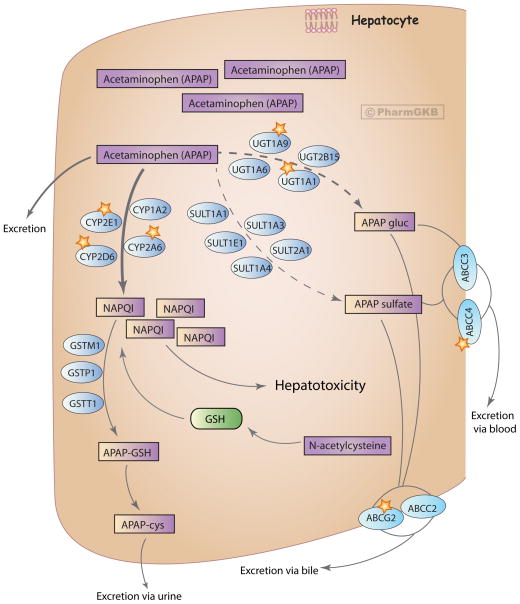
Figure 31 — Acetaminophen Metabolism at Therapeutic Doses. At normal doses, approximately 90% of acetaminophen is conjugated via glucuronidation and sulfation to inactive metabolites. Only 5–10% is oxidized by CYP2E1 to the reactive metabolite NAPQI, which is rapidly detoxified by conjugation with glutathione (GSH) and excreted as cysteine and mercapturic acid conjugates.Figure 32 — Acetaminophen Metabolism at Toxic Doses. In overdose, glucuronidation and sulfation pathways become saturated, shunting more drug through CYP2E1 oxidation. Increased NAPQI production depletes glutathione stores; once GSH falls below ~30% of normal, NAPQI accumulates and binds to hepatocellular proteins, causing centrilobular (zone 3) necrosis. N-acetylcysteine (NAC) restores glutathione and serves as a direct NAPQI scavenger.
Acetaminophen Toxicity in Detail
Acetaminophen (APAP) is the most common cause of acute liver failure in the US. At therapeutic doses, ~90% is conjugated (glucuronidation/sulfation) and 5–10% is oxidized by CYP2E1 to the toxic metabolite NAPQI, which is normally detoxified by glutathione conjugation. In overdose (>150 mg/kg or >7.5 g in adults), glutathione stores are depleted → NAPQI accumulates → hepatocellular necrosis (zone 3 / centrilobular, where CYP2E1 is most concentrated).
Phase
Timing
Features
Phase I
0–24 hours
Nausea, vomiting, malaise, normal labs (or mildly elevated transaminases)
Phase II
24–72 hours
Abdominal pain (RUQ), rising AST/ALT, ↑INR/PT; patients may feel "better"
Phase III
72–96 hours
Peak hepatotoxicity: massive AST/ALT (>10,000), coagulopathy, hepatic encephalopathy, renal failure; may progress to death
Phase IV
4 days–2 weeks
Recovery (if survived); liver regeneration
N-Acetylcysteine (NAC) is the antidote: replenishes glutathione stores, acts as a glutathione substitute, and enhances sulfation. Most effective when given within 8 hours of ingestion but still beneficial up to 24+ hours. Use the Rumack-Matthew nomogram (plot 4-hour level) to determine need for NAC. Risk factors for toxicity at lower doses: chronic alcohol use (CYP2E1 induction + glutathione depletion), malnutrition, fasting, and CYP-inducing drugs.
Chronic alcoholics are at increased risk for acetaminophen toxicity at lower doses because alcohol induces CYP2E1 (more NAPQI production) AND depletes glutathione (less detoxification). The recommended maximum daily dose should be reduced to 2 g/day in chronic alcohol users.
27 Special Populations & Drug Interactions
Pregnancy Drug Safety
The FDA replaced the old letter categories (A, B, C, D, X) with the Pregnancy and Lactation Labeling Rule (PLLR) in 2015, but letter categories remain commonly referenced. Key teratogenic drugs to know:
Fetal hydantoin syndrome (cleft lip/palate, digital hypoplasia, nail hypoplasia)
First trimester
Tetracyclines
Teeth discoloration, bone growth inhibition
Second/third trimester
Fluoroquinolones
Cartilage damage
All trimesters
Statins
Multiple congenital anomalies (contraindicated)
All trimesters
Geriatric Pharmacology
Age-related changes affecting drug handling: ↓hepatic blood flow and ↓phase I metabolism (phase II relatively preserved) → slower drug clearance. ↓GFR (~1 mL/min/year after age 40) → reduced renal clearance. ↓Total body water and ↑body fat → increased Vd for lipophilic drugs (longer t1/2), decreased Vd for hydrophilic drugs (higher peak levels). ↓Albumin → increased free fraction of protein-bound drugs. The Beers Criteria lists potentially inappropriate medications in the elderly (e.g., long-acting BZDs, anticholinergics, NSAIDs, TCAs).
Pediatric Pharmacology
Neonates have immature hepatic enzymes (especially glucuronidation — risk of chloramphenicol "gray baby syndrome" and unconjugated bilirubin toxicity), ↑total body water (larger Vd for water-soluble drugs), ↓plasma protein binding, and immature renal function. Drug dosing is typically weight-based (mg/kg) or BSA-based. Avoid certain drugs: aspirin (Reye syndrome), tetracycline (teeth/bone), fluoroquinolones (cartilage), codeine (respiratory depression in ultra-rapid metabolizers).
Major Drug Interactions
Interaction
Mechanism
Clinical Consequence
Warfarin + rifampin
CYP induction → ↑warfarin metabolism
↓INR, loss of anticoagulation
Warfarin + azole antifungals
CYP inhibition → ↓warfarin metabolism
↑INR, bleeding risk
Statins + CYP3A4 inhibitors
↓Statin metabolism → ↑statin levels
Rhabdomyolysis risk
MAOI + tyramine-rich foods
↓Tyramine breakdown → massive NE release
Hypertensive crisis
MAOI + SSRI/meperidine
Excess serotonergic activity
Serotonin syndrome
Methotrexate + NSAIDs
↓Renal MTX clearance
MTX toxicity (myelosuppression)
Lithium + thiazides/NSAIDs/ACEi
↓Renal lithium clearance
Lithium toxicity
Digoxin + amiodarone/verapamil
↓Digoxin clearance (P-gp inhibition)
Digoxin toxicity (halve the digoxin dose)
Clopidogrel + omeprazole
CYP2C19 inhibition → ↓clopidogrel activation
Reduced antiplatelet effect
Sildenafil + nitrates
Both cause cGMP-mediated vasodilation
Severe hypotension — contraindicated
Always think of drug interactions in terms of the mechanism: CYP induction (faster metabolism, lower drug levels), CYP inhibition (slower metabolism, higher drug levels), protein binding displacement, or pharmacodynamic synergy/antagonism. The most dangerous interactions involve drugs with narrow therapeutic indices.
Renal & Hepatic Impairment
Condition
Pharmacokinetic Change
Clinical Implications
Renal impairment
↓GFR → ↓renal clearance of drugs and active metabolites
↓Phase I metabolism, ↓protein synthesis (albumin), portosystemic shunting
↑Bioavailability of high-extraction drugs (propranolol, morphine); ↑free fraction of protein-bound drugs; avoid hepatotoxic drugs; use Child-Pugh score for dose adjustment
Combined renal + hepatic
Both clearance pathways impaired
Extreme caution; use drugs with extrarenal/extrahepatic clearance when possible
Therapeutic Drug Monitoring (TDM)
TDM is indicated for drugs with a narrow TI, significant interpatient PK variability, and a defined relationship between concentration and effect/toxicity. Key drugs requiring TDM:
The following topics are the most heavily tested pharmacology concepts across USMLE Step 1, Step 2, and shelf exams. Master these and you will be well prepared.
SAT For Very Annoying Skin: Sulfonamides, Amiodarone, Tetracyclines, Fluoroquinolones, Voriconazole, 5-Aminolevulinic acid, St. John's wort.
Drugs That Cause SJS / TEN
Most common: Allopurinol, sulfonamides, anticonvulsants (carbamazepine, phenytoin, lamotrigine, phenobarbital), NSAIDs (piroxicam), nevirapine. HLA-B*5801 testing recommended before allopurinol. HLA-B*1502 in East Asians before carbamazepine.
Digoxin toxicity is enhanced by hypokalemia (digoxin and K+ compete for the same binding site on Na+/K+-ATPase). Classic ECG signs: scooped ST segments ("Salvador Dali mustache"), increased PR interval, bidirectional VT. Treatment: correct K+, digoxin-specific Fab fragments.
Nitroglycerin tolerance develops with continuous exposure (24-hour patches). The mechanism involves sulfhydryl group depletion and neurohormonal activation. Prevent tolerance with a 10–12-hour nitrate-free interval daily (typically overnight). This is a board-tested concept.
Rifampin is the most potent CYP inducer and turns all body fluids orange (urine, tears, sweat). It reduces the efficacy of oral contraceptives, warfarin, HIV protease inhibitors, cyclosporine, and virtually every CYP-metabolized drug. Always screen for rifampin interactions.
Metformin should be held before iodinated contrast procedures (risk of lactic acidosis in AKI from contrast nephropathy). Resume 48 hours after the procedure if renal function is stable. This is a common clinical practice question.
Aminoglycosides exhibit concentration-dependent killing: higher peak concentrations produce greater bactericidal activity. The post-antibiotic effect (PAE) allows extended-interval dosing (once-daily gentamicin), which improves efficacy and reduces nephrotoxicity by lowering trough levels. Monitor: peak levels for efficacy, trough levels for toxicity. Synergy with cell wall agents (penicillins) is used in endocarditis treatment.
Isoniazid (INH) is the cornerstone of TB therapy. Key facts: metabolized by N-acetyltransferase (NAT2) — slow acetylators (50% of Caucasians) are at higher risk for peripheral neuropathy (pyridoxine/B6 prophylaxis required) and hepatotoxicity. INH also inhibits CYP enzymes and is a monoamine oxidase inhibitor. Drug-induced lupus occurs with chronic use (anti-histone antibodies).
Warfarin is one of the most heavily tested drugs. Key interactions: (1) CYP2C9 inhibitors increase warfarin levels (fluconazole, amiodarone, metronidazole, TMP-SMX). (2) CYP inducers decrease warfarin levels (rifampin, carbamazepine, phenytoin, barbiturates). (3) Vitamin K–rich foods (leafy greens) decrease INR. (4) Broad-spectrum antibiotics kill gut flora that produce vitamin K → increase INR. Always check INR when adding/removing interacting drugs.
Lithium is the gold standard for bipolar disorder maintenance. Its narrow therapeutic index (0.6–1.2 mEq/L) means small changes in clearance cause toxicity. Anything that reduces renal lithium clearance is dangerous: thiazide diuretics, NSAIDs, ACE inhibitors, dehydration. Signs of toxicity: coarse tremor, ataxia, confusion, seizures, nephrogenic DI. Treatment: IV saline, hemodialysis for severe toxicity.
Azathioprine and 6-mercaptopurine are metabolized by xanthine oxidase. Co-administration with allopurinol (an XO inhibitor) dramatically increases levels of these drugs, causing severe myelosuppression. Reduce the azathioprine/6-MP dose by 75% if allopurinol must be used concurrently, or switch to an alternative agent. TPMT (thiopurine methyltransferase) polymorphisms also affect 6-MP metabolism — test before initiating therapy.
Exam Strategy
For pharmacology questions: (1) Identify the drug class from the stem (mechanism clues, suffix). (2) Know the mechanism of action — this predicts both therapeutic effects and side effects. (3) Recognize toxidromes and antidotes. (4) Understand pharmacokinetic principles (first-order vs zero-order, loading dose, CYP interactions). (5) Be comfortable with receptor pharmacology (G-protein subtypes, agonist vs antagonist curves). These five skills will answer the vast majority of pharmacology questions on any exam.