Emergency Medicine
Every critical presentation, resuscitation protocol, acute diagnosis, procedure, disposition decision, and management strategy in one place.
01 The Emergency Medicine Approach
Emergency medicine is the only specialty defined not by an organ system or patient demographic but by acuity and undifferentiated presentation. The ED physician sees every chief complaint, from cardiac arrest to laceration repair, and must risk-stratify within minutes. The central question is never "what is the complete diagnosis?" but rather "does this patient have a life-threatening condition that I must identify and treat right now?"
Triage — Emergency Severity Index (ESI)
ESI is the standard 5-level triage system used in US emergency departments. It combines acuity with expected resource utilization to prioritize patient flow.
| ESI Level | Description | Clinical Example | Expected Resources |
|---|---|---|---|
| 1 | Immediate life-saving intervention required | Cardiac arrest, respiratory failure, active massive hemorrhage | Resuscitation bay |
| 2 | High-risk situation, confused/lethargic, severe pain/distress | Chest pain with ECG changes, stroke symptoms, unstable vital signs | Immediate bedside evaluation |
| 3 | Stable but likely needs multiple resources (labs, imaging, IV meds) | Abdominal pain needing CT, renal colic, pneumonia | 2+ resources |
| 4 | Stable, needs 1 resource | Simple laceration, UTI needing UA, ankle sprain needing X-ray | 1 resource |
| 5 | Stable, needs 0 resources (exam only) | Prescription refill, suture removal, medication question | 0 resources |
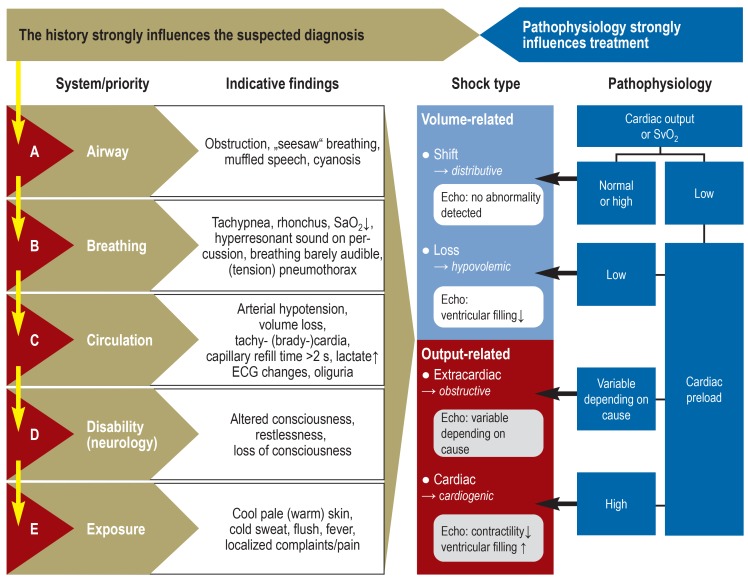
Primary Survey — ABCDE
The primary survey is performed on every critically ill or injured patient. It is a systematic, sequential assessment that identifies and treats life threats in the order they will kill the patient fastest.
| Step | Assessment | Immediate Interventions |
|---|---|---|
| A — Airway | Is the airway patent? Look for stridor, gurgling, obstruction, facial trauma, angioedema | Jaw thrust, suction, OPA/NPA, intubation, surgical airway |
| B — Breathing | RR, SpO2, breath sounds bilateral? Chest wall excursion symmetric? Trachea midline? | O2, BVM, needle decompression for tension PTX, chest tube, intubation |
| C — Circulation | HR, BP, skin (cool/clammy = shock), active bleeding? Pulse quality? | 2 large-bore IVs, fluid bolus, blood products, pressors, tourniquet, direct pressure |
| D — Disability | GCS, pupils (size, reactivity, symmetry), gross motor exam, glucose | Dextrose for hypoglycemia, naloxone for opioid overdose, mannitol/hypertonic saline for herniation |
| E — Exposure/Environment | Fully undress patient, log-roll, temperature | Warm blankets (prevent hypothermia), identify posterior wounds, rectal exam in trauma if indicated |
Secondary Survey
Performed only after the primary survey is complete and life threats are addressed. This is the comprehensive head-to-toe physical exam: HEENT (pupil response, TMs, oropharynx), neck (JVD, tracheal deviation, c-spine tenderness), chest (heart sounds, lung fields), abdomen (tenderness, guarding, rigidity, peritoneal signs), pelvis (stability), extremities (pulses, deformity, compartments), neuro (cranial nerves, strength, sensation, reflexes, cerebellar), skin (rashes, wounds, track marks), and a detailed history (SAMPLE: Signs/symptoms, Allergies, Medications, Past medical history, Last meal, Events preceding).
02 Resuscitation Fundamentals
ACLS — Cardiac Arrest Algorithms
The 2020 AHA Guidelines define two pathways based on initial rhythm:
| Shockable (VF/pVT) | Non-Shockable (Asystole/PEA) |
|---|---|
| Defibrillate immediately (biphasic 120–200 J, mono 360 J) | CPR × 2 min, then rhythm check |
| Resume CPR × 2 min, rhythm check | Epinephrine 1 mg IV/IO q3–5 min (give ASAP) |
| Epinephrine 1 mg IV/IO q3–5 min (after 2nd shock) | Identify and treat reversible causes (H's and T's) |
| Amiodarone 300 mg IV (first dose), then 150 mg (second dose) | Continue CPR with rhythm checks q2min |
The H's and T's — reversible causes of cardiac arrest: Hypovolemia, Hypoxia, Hydrogen ion (acidosis), Hypo/hyperkalemia, Hypothermia, Tension pneumothorax, Tamponade (cardiac), Toxins, Thrombosis (coronary/pulmonary). High-quality CPR is the single most important intervention: rate 100–120/min, depth 2–2.4 inches (5–6 cm), full chest recoil, minimize interruptions (< 10 sec for rhythm checks).
Airway Management Hierarchy
Airway interventions escalate in invasiveness: positioning (head tilt–chin lift, jaw thrust in trauma) → basic adjuncts (OPA in unconscious without gag, NPA if gag intact) → bag-valve-mask (BVM) → supraglottic airway (LMA, King tube — rescue device or prehospital) → endotracheal intubation (RSI is the ED standard) → surgical airway (cricothyrotomy — "can't intubate, can't oxygenate" scenario).
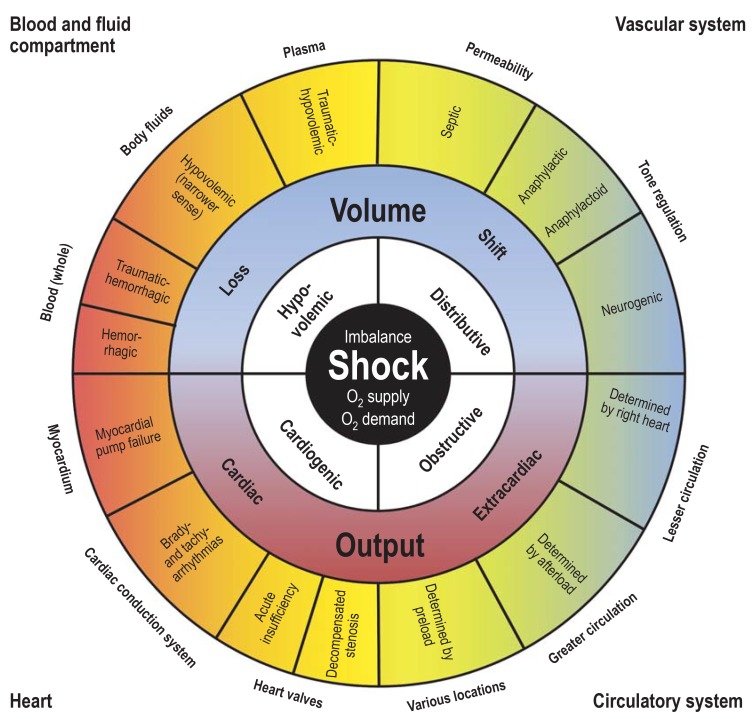
Shock Recognition & Classification
| Type | Mechanism | Classic Findings | Examples | Initial Treatment |
|---|---|---|---|---|
| Hypovolemic | Decreased preload (volume loss) | Tachycardia, hypotension, flat neck veins, cool extremities | Hemorrhage, dehydration, burns | IV fluids, blood products, control hemorrhage |
| Cardiogenic | Pump failure | Hypotension, JVD, pulmonary edema, cool extremities | MI, cardiomyopathy, myocarditis, valvular catastrophe | Vasopressors (norepinephrine), inotropes (dobutamine), mechanical support |
| Distributive | Vasodilation (decreased SVR) | Hypotension, warm extremities (early), tachycardia, wide pulse pressure | Sepsis, anaphylaxis, neurogenic, adrenal crisis | Fluids + vasopressors (norepinephrine), treat cause |
| Obstructive | Mechanical obstruction to flow | Hypotension, JVD, muffled heart sounds (tamponade) or absent breath sounds (tension PTX) | Tension PTX, cardiac tamponade, massive PE | Needle decompression, pericardiocentesis, thrombolytics |
Hemorrhagic Shock Staging (ATLS)
| Class | Blood Loss | HR | BP | RR | Mental Status | Fluid Replacement |
|---|---|---|---|---|---|---|
| I | < 750 mL (< 15%) | < 100 | Normal | 14–20 | Slightly anxious | Crystalloid |
| II | 750–1500 mL (15–30%) | 100–120 | Normal | 20–30 | Anxious | Crystalloid |
| III | 1500–2000 mL (30–40%) | 120–140 | Decreased | 30–40 | Confused | Crystalloid + blood |
| IV | > 2000 mL (> 40%) | > 140 | Very low | > 35 | Lethargic/obtunded | Massive transfusion protocol |
Activated for anticipated need of ≥10 units pRBCs in 24 hours or ≥4 units in 1 hour. Target ratio: 1:1:1 (pRBC : FFP : platelets). Tranexamic acid (TXA) 1 g IV over 10 min within 3 hours of injury (CRASH-2 trial). Monitor: calcium (citrate in blood products chelates Ca → hypocalcemia → give calcium chloride 1 g IV or calcium gluconate 3 g IV), temperature (hypothermia worsens coagulopathy), potassium, ionized calcium, fibrinogen (target > 150 mg/dL — give cryoprecipitate if low). The lethal triad of trauma: hypothermia + acidosis + coagulopathy.
03 Key Terminology & Abbreviations
Emergency medicine uses a dense layer of abbreviations across triage, resuscitation, trauma, and disposition. A comprehensive list is provided in Section 50. Below are the foundational terms every EM reference requires:
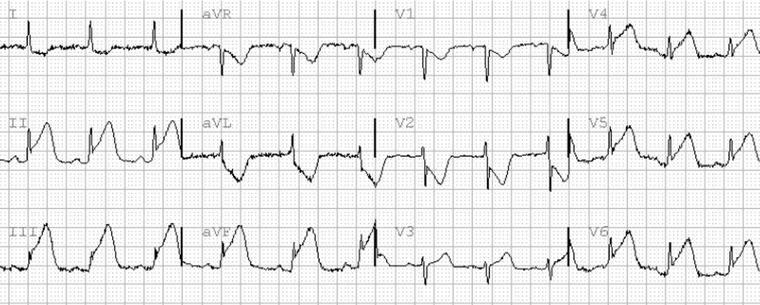
04 Acute Coronary Syndromes CV
ACS is a spectrum of acute myocardial ischemia ranging from unstable angina (UA) to non-ST-elevation MI (NSTEMI) to ST-elevation MI (STEMI). ACS is the leading cause of death worldwide and the most common high-acuity cardiac presentation in the ED. The critical ED task is rapid ECG interpretation (< 10 minutes from arrival) to identify STEMI, which requires emergent reperfusion.
ACS Spectrum
| Entity | ECG | Troponin | Pathology | Urgency |
|---|---|---|---|---|
| Unstable Angina | Normal or ST depression/T-wave changes | Negative | Partial coronary occlusion, no necrosis | Admit, serial troponins, risk stratify |
| NSTEMI | ST depression, T-wave inversion, or non-specific changes | Elevated | Partial occlusion with myocardial necrosis | Admit, anticoagulate, cardiology consult, cath within 24–72 hrs |
| STEMI | ≥1 mm ST elevation in ≥2 contiguous leads (or new LBBB) | Elevated (may be initially negative) | Complete coronary occlusion | Emergent PCI (door-to-balloon < 90 min) or thrombolytics (door-to-needle < 30 min) |
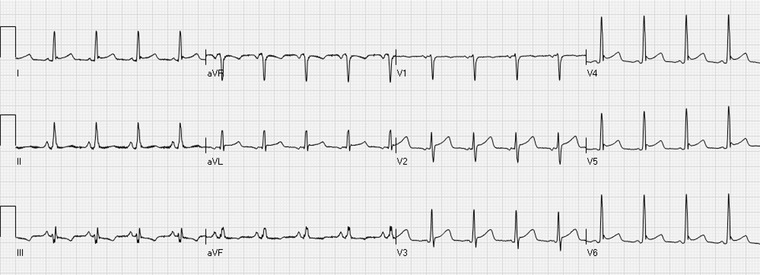
STEMI Localization by ECG
| Leads with ST Elevation | Territory | Culprit Artery | Watch For |
|---|---|---|---|
| V1–V4 | Anterior/LAD | LAD | Large territory → cardiogenic shock, VT/VF |
| II, III, aVF | Inferior | RCA (85%) or LCx | Right ventricular involvement (get V4R), bradycardia, avoid nitrates if RV infarct |
| I, aVL, V5–V6 | Lateral | LCx | Often with inferior or anterior MI |
| V7–V9 (posterior leads) | Posterior | RCA or LCx | Suspect if prominent R wave + ST depression V1–V3 (mirror image) |

Initial ED Management of ACS
MONA (Morphine, Oxygen, Nitroglycerin, Aspirin) is the classic mnemonic but has evolved: Aspirin 325 mg chewed (non-enteric coated, immediate), Nitroglycerin 0.4 mg SL q5min × 3 (hold if SBP < 90, RV infarct, or PDE5 inhibitor within 24–48 hrs), heparin (UFH 60 U/kg bolus max 4000 U, then 12 U/kg/hr infusion; or enoxaparin 1 mg/kg SQ), P2Y12 inhibitor (clopidogrel 600 mg load or ticagrelor 180 mg load — check with interventional cardiologist before cath as some prefer to load in the lab). Oxygen only if SpO2 < 94%. Morphine with caution — may increase mortality in NSTEMI.
05 Acute Heart Failure & Pulmonary Edema CV
Acute decompensated heart failure (ADHF) presents as sudden or worsening dyspnea, orthopnea, and hypoxia from pulmonary venous congestion. The ED must rapidly distinguish cardiogenic pulmonary edema from pneumonia, COPD, and PE. BNP > 400 pg/mL (or NT-proBNP > 900 pg/mL) strongly supports HF; < 100 (< 300) makes it unlikely. CXR shows cephalization of vessels, Kerley B lines, bilateral pleural effusions, and perihilar edema ("butterfly" or "bat wing" pattern).
Acute Management
The mainstay is preload and afterload reduction, NOT fluid boluses. Nitroglycerin 400 mcg SL, then IV infusion 10–200 mcg/min (titrate to symptom relief and SBP > 100). Furosemide (Lasix) 40–80 mg IV (if on chronic diuretics, give ≥ home dose IV). BiPAP (CPAP 10–12 cmH2O or BiPAP 10/5) dramatically reduces work of breathing and intubation rates — start immediately in moderate-to-severe respiratory distress. For flash pulmonary edema with hypertension: aggressive nitroglycerin (high-dose bolus 2 mg IV followed by infusion) is highly effective.
When ADHF progresses to cardiogenic shock (SBP < 90, signs of end-organ hypoperfusion, CI < 2.2 L/min/m²): start norepinephrine (first-line vasopressor per SOAP II trial) and dobutamine (5–20 mcg/kg/min for inotropy). Avoid fluids unless clear hypovolemia. Emergent cardiology consult for mechanical circulatory support (Impella, IABP, ECMO). Mortality exceeds 40%.
06 Aortic Dissection & Aortic Emergencies CV
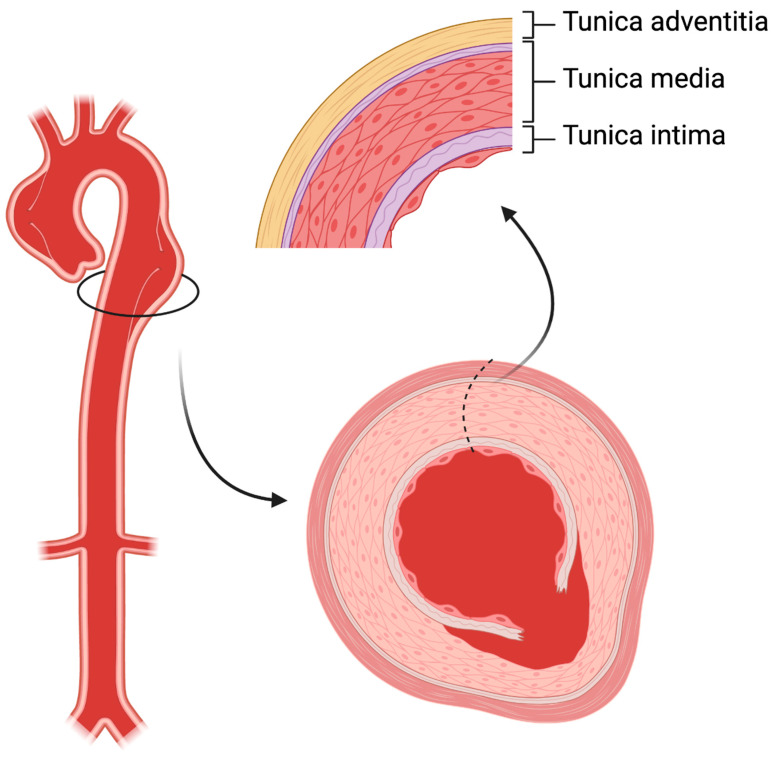
Aortic dissection is a tear in the aortic intima allowing blood to enter the media, creating a false lumen. Mortality increases 1–2% per hour if untreated. Classic presentation: sudden-onset "tearing" or "ripping" chest/back pain that is maximal at onset, radiating to the back (descending) or anterior chest (ascending). Risk factors: uncontrolled hypertension, Marfan syndrome, bicuspid aortic valve, prior cardiac surgery, cocaine use.
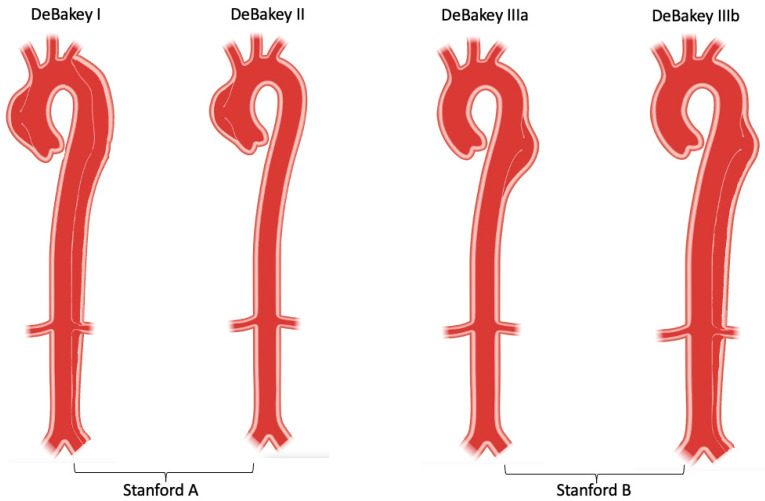
Stanford Classification
| Type | Involvement | Management | Mortality (untreated) |
|---|---|---|---|
| A | Ascending aorta involved (regardless of distal extent) | Emergent open surgical repair | ~1–2% per hour for 48 hrs |
| B | Descending aorta only (distal to left subclavian) | Medical management (anti-impulse therapy); TEVAR if complicated | ~10% at 30 days with medical management |
ED Management
Anti-impulse therapy: target HR < 60 bpm and SBP 100–120 mmHg. Start IV esmolol (500 mcg/kg bolus, then 50–200 mcg/kg/min) or labetalol (20 mg IV bolus, then 1–2 mg/min infusion). Beta-blocker FIRST — do not give vasodilators (nitroprusside, nicardipine) without beta-blockade, as reflex tachycardia increases aortic shear stress. Add nitroprusside (0.25–10 mcg/kg/min) only after HR is controlled. CTA chest/abdomen/pelvis is the gold-standard diagnostic study (sensitivity > 95%).
07 Cardiac Arrest & Post-Arrest Care CV
Cardiac arrest survival depends on the chain of survival: early recognition, early CPR, early defibrillation, and advanced resuscitation. Out-of-hospital cardiac arrest (OHCA) survival to discharge averages 10–12% nationally; in-hospital cardiac arrest (IHCA) survival is approximately 25%. Shockable rhythms (VF/pVT) carry significantly better prognosis than non-shockable (asystole/PEA).
Post-Arrest Care
After ROSC, immediate priorities: 12-lead ECG (emergent cath if STEMI or high suspicion of coronary occlusion), targeted temperature management (TTM) — the TTM2 trial (2021) found no benefit of 33°C vs. 36°C, and current guidelines recommend maintaining temperature ≤ 37.5°C and actively preventing fever. Hemodynamic optimization: MAP > 65 mmHg (vasopressors as needed), avoid hypotension and hypoxia (target SpO2 94–98%, avoid hyperoxia). Neuroprognostication should be delayed ≥ 72 hours after rewarming — never withdraw care based on exam alone within the first 72 hours.
08 Arrhythmia Management CV
Tachyarrhythmias
| Rhythm | ECG Features | Stable Management | Unstable Management |
|---|---|---|---|
| SVT (AVNRT/AVRT) | Narrow complex, regular, rate 150–250, no visible P waves | Vagal maneuvers (modified Valsalva) → Adenosine 6 mg rapid IV push (may repeat 12 mg × 2) | Synchronized cardioversion 50–100 J |
| AFib with RVR | Irregularly irregular, narrow complex, no distinct P waves, rate > 100 | Rate control: diltiazem 0.25 mg/kg IV (15–20 mg) over 2 min, then 5–15 mg/hr infusion; or metoprolol 5 mg IV q5min × 3 | Synchronized cardioversion 120–200 J (biphasic) |
| AFlutter | Sawtooth pattern (leads II, III, aVF), rate usually 150 (2:1 block) or 75 (4:1) | Rate control same as AFib; cardioversion very effective at low energy | Synchronized cardioversion 50–100 J |
| Monomorphic VT | Wide complex, regular, rate > 100, AV dissociation | Amiodarone 150 mg IV over 10 min, then 1 mg/min × 6 hrs; or procainamide 20–50 mg/min until arrhythmia resolves (max 17 mg/kg) | Synchronized cardioversion 100 J |
| Polymorphic VT (Torsades) | Wide complex, undulating axis, often preceded by long QT | Magnesium sulfate 2 g IV over 10 min; isoproterenol or overdrive pacing | Defibrillation (unsynchronized) 120–200 J |
Bradyarrhythmias
Symptomatic bradycardia (HR < 50 with hypotension, AMS, chest pain, or acute HF): Atropine 1 mg IV q3–5 min (max 3 mg) — will not work in Mobitz II or third-degree block (infranodal). If atropine fails: transcutaneous pacing (start at 60 mA, increase until capture, then add 10 mA safety margin; sedate the patient with fentanyl/midazolam). Dopamine infusion (5–20 mcg/kg/min) or epinephrine infusion (2–10 mcg/min) as bridge to transvenous pacing.
09 Hypertensive Emergencies CV
A hypertensive emergency is severely elevated BP (often > 180/120) with acute end-organ damage: encephalopathy, acute stroke, aortic dissection, acute MI, pulmonary edema, eclampsia, acute renal failure, or retinal hemorrhage. Hypertensive urgency is severely elevated BP without end-organ damage — manage with oral agents and outpatient follow-up; aggressive IV reduction is not indicated and may cause harm.
Treatment by End-Organ
| Scenario | Agent of Choice | BP Target |
|---|---|---|
| Aortic dissection | Esmolol or labetalol (beta-blocker first) | SBP 100–120, HR < 60 within 20 min |
| Acute pulmonary edema | Nitroglycerin infusion + furosemide | 25% reduction in MAP over 1 hr |
| Acute ischemic stroke | Nicardipine or labetalol | < 185/110 if thrombolytic candidate; otherwise < 220/120 |
| Hemorrhagic stroke (ICH) | Nicardipine or clevidipine | SBP < 140 (per INTERACT2) |
| Eclampsia | Magnesium sulfate (seizure prevention) + labetalol or hydralazine | SBP < 160, DBP < 110 |
| Sympathomimetic crisis (cocaine) | Benzodiazepines first, then nitroglycerin/phentolamine — avoid beta-blockers | Symptom-guided |
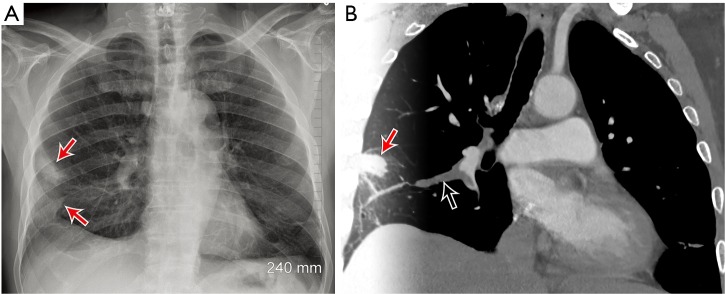
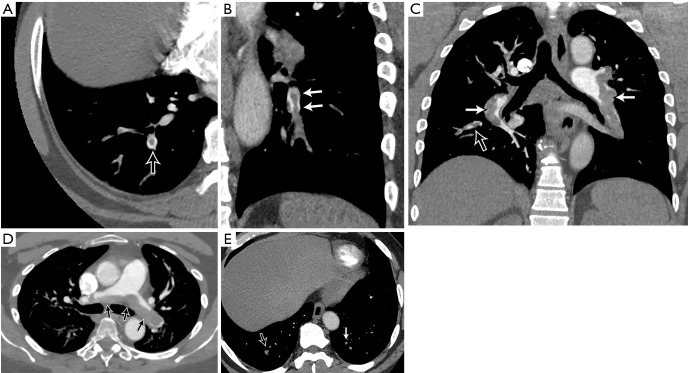
10 Pulmonary Embolism CV
PE is the third leading cause of cardiovascular death. The ED challenge is identifying PE among the high volume of patients with chest pain and dyspnea while avoiding unnecessary CT angiography. Risk stratification begins with clinical probability assessment.
Wells Score for PE
| Criterion | Points |
|---|---|
| Clinical signs/symptoms of DVT | 3.0 |
| PE is #1 or equally likely diagnosis | 3.0 |
| Heart rate > 100 | 1.5 |
| Immobilization (≥3 days) or surgery in prior 4 weeks | 1.5 |
| Previous DVT/PE | 1.5 |
| Hemoptysis | 1.0 |
| Active cancer (treatment within 6 months or palliative) | 1.0 |
Score ≤4: PE unlikely → check D-dimer (if < 500 ng/mL, PE excluded). Score >4: PE likely → proceed to CTA. PERC rule: if clinical gestalt is "PE unlikely" AND all 8 PERC criteria are negative (age < 50, HR < 100, SpO2 ≥ 95%, no hemoptysis, no estrogen use, no prior DVT/PE, no unilateral leg swelling, no surgery/trauma requiring hospitalization in past 4 weeks), D-dimer is unnecessary — PE is effectively excluded.
Management by Severity
| Category | Hemodynamics | RV Strain | Treatment |
|---|---|---|---|
| Low-risk | Stable | No | Anticoagulation (heparin → DOAC). Some qualify for outpatient treatment (Hestia criteria) |
| Submassive (intermediate-risk) | Stable | Yes (RV dilation on CT/echo, elevated troponin/BNP) | Anticoagulation + close monitoring in ICU; consider catheter-directed therapy if decompensating |
| Massive | Hemodynamically unstable (SBP < 90) | Yes | Systemic thrombolytics (alteplase 100 mg IV over 2 hrs), surgical embolectomy, or catheter-directed therapy. Bolus fluids cautiously (250–500 mL — excessive fluids worsen RV) |
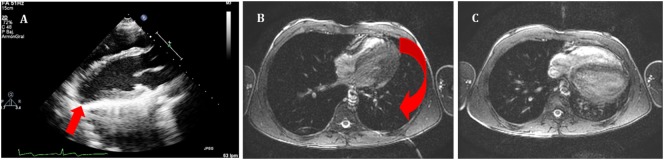
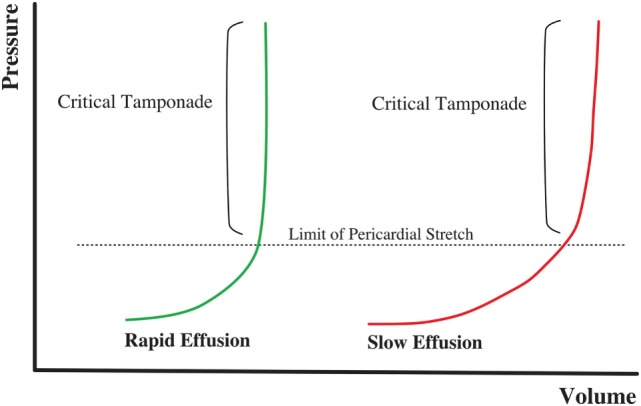
11 Cardiac Tamponade CV
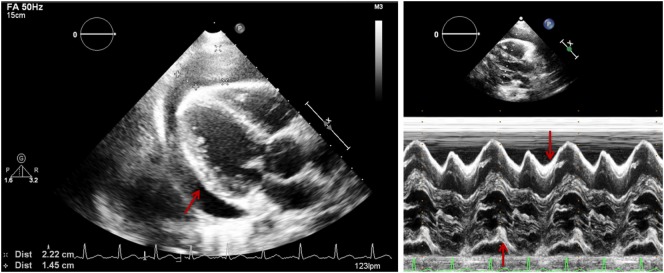
Pericardial fluid accumulation compressing the heart, impairing diastolic filling. The physiologic consequence is obstructive shock — reduced cardiac output despite adequate volume. Causes: malignancy (most common cause of large effusions), uremia, post-MI (Dressler syndrome), trauma (hemopericardium), aortic dissection (rupture into pericardium), infection (TB, viral). Beck's triad: hypotension, muffled heart sounds, JVD. Pulsus paradoxus > 10 mmHg (SBP drop with inspiration) is a key sign. Electrical alternans on ECG (beat-to-beat alternation in QRS amplitude) is specific but not sensitive.
Bedside echo is the diagnostic study of choice — pericardial effusion with RV diastolic collapse (earliest sign of tamponade physiology) and RA systolic collapse. Treatment: emergent pericardiocentesis (subxiphoid approach, ultrasound-guided, advance 18-gauge needle at 30–45° toward the left shoulder). Even removing 20–50 mL can dramatically improve hemodynamics. IV fluid bolus (500–1000 mL) as temporizing measure to increase preload. Traumatic tamponade often requires emergent thoracotomy rather than pericardiocentesis.
12 Acute Asthma & Status Asthmaticus Resp
Asthma exacerbation severity drives treatment intensity. Mild-moderate: speaks in sentences, RR < 30, SpO2 ≥ 90%, PEF > 50% predicted. Severe: speaks in words, RR > 30, accessory muscle use, SpO2 < 90%, PEF < 50%. Status asthmaticus: severe exacerbation refractory to initial bronchodilator therapy, representing a life-threatening emergency.
Stepwise ED Management
First-line: continuous nebulized albuterol (10–15 mg/hr) + ipratropium 0.5 mg nebulized q20min × 3. Corticosteroids early: prednisone 60 mg PO or methylprednisolone 125 mg IV (onset 4–6 hrs, but give early). Magnesium sulfate 2 g IV over 20 min for severe exacerbation (NNT = 4 for preventing admission). Epinephrine 0.3–0.5 mg IM for impending respiratory failure. For patients failing NIV: intubation is dangerous in status asthmaticus (post-intubation hypotension from air trapping — use ketamine for induction, permissive hypercapnia strategy, low RR 8–10, long expiratory time, I:E 1:4–1:5).
13 COPD Exacerbation Resp
Acute worsening of respiratory symptoms (dyspnea, cough, sputum volume/purulence) beyond normal day-to-day variation requiring a change in medication. Most common triggers: viral/bacterial infection (60–80%), air pollution, PE, and pneumothorax. COPD patients live with chronic CO2 retention; their respiratory drive may be hypoxic rather than hypercarbic. Target SpO2 88–92% — excessive oxygen can worsen hypercapnia through the Haldane effect and V/Q mismatch redistribution.
Treatment
Bronchodilators: albuterol + ipratropium nebulized. Systemic corticosteroids: prednisone 40 mg PO × 5 days (or methylprednisolone IV). Antibiotics if purulent sputum or requiring mechanical ventilation: azithromycin 500 mg × 1 day then 250 mg × 4 days, or doxycycline 100 mg BID, or amoxicillin-clavulanate. BiPAP (IPAP 10–15 cmH2O, EPAP 5 cmH2O) is first-line for COPD exacerbation with respiratory acidosis (pH < 7.35, pCO2 > 45) — reduces intubation rate by 60% and mortality by 50% (Cochrane review).
14 Pneumonia (CAP, HAP, Aspiration) Resp
Community-acquired pneumonia (CAP) is the most common infectious cause of death in the US. Typical pathogens: S. pneumoniae (most common), H. influenzae, M. catarrhalis. Atypical: Mycoplasma, Chlamydophila, Legionella. Viral: influenza, RSV, SARS-CoV-2.
Severity & Disposition — CURB-65
| Criterion | Definition | Points |
|---|---|---|
| Confusion | New mental confusion | 1 |
| Urea | BUN > 20 mg/dL | 1 |
| Respiratory rate | ≥ 30 breaths/min | 1 |
| Blood pressure | SBP < 90 or DBP ≤ 60 | 1 |
| Age | ≥ 65 years | 1 |
Score 0–1: outpatient. 2: consider short hospitalization. 3–5: admit, 4–5 consider ICU.
Empiric Antibiotic Regimens
| Setting | Empiric Regimen |
|---|---|
| Outpatient (healthy, no comorbidities) | Amoxicillin 1 g TID × 5 days; OR doxycycline 100 mg BID; OR azithromycin 500 mg day 1, then 250 mg × 4 days |
| Outpatient (comorbidities: DM, CKD, COPD, CHF) | Amoxicillin-clavulanate 875/125 BID + azithromycin; OR respiratory fluoroquinolone (levofloxacin 750 mg daily) |
| Inpatient (non-ICU) | Ceftriaxone 1–2 g IV daily + azithromycin 500 mg IV daily; OR levofloxacin 750 mg IV daily |
| Inpatient (ICU) | Ceftriaxone 2 g IV + azithromycin 500 mg IV; add vancomycin + piperacillin-tazobactam if MRSA/Pseudomonas risk factors |
| Aspiration pneumonia | Ampicillin-sulbactam 3 g IV q6h; OR clindamycin 600 mg IV q8h + ceftriaxone (if community-acquired) |
15 Pneumothorax Resp
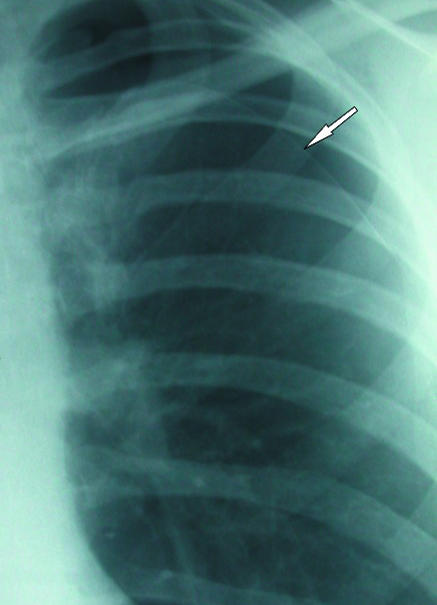
Types
| Type | Mechanism | Presentation | Management |
|---|---|---|---|
| Simple spontaneous (primary) | Rupture of apical bleb; tall, thin young males | Acute pleuritic chest pain, dyspnea, decreased breath sounds unilaterally | Small (< 2 cm apex-to-cupola): observe, supplemental O2. Large or symptomatic: aspiration or chest tube (pigtail 14 Fr or standard 20–24 Fr) |
| Secondary spontaneous | Underlying lung disease (COPD, CF, Marfan) | More symptomatic due to reduced reserve | Lower threshold for chest tube; higher risk of recurrence |
| Tension | One-way valve mechanism; air accumulates under pressure | Hypotension, tracheal deviation (away), JVD, absent breath sounds, cardiac arrest (PEA) | Immediate needle decompression (14-gauge needle, 2nd ICS midclavicular line or 5th ICS anterior axillary line) followed by chest tube |
| Open ("sucking chest wound") | Penetrating trauma with persistent chest wall defect | Air sucked in/out of wound with respiration | Three-sided occlusive dressing (allows air out but not in) → chest tube remote from wound |
16 Acute Respiratory Failure & Mechanical Ventilation Resp
Type I (hypoxemic): PaO2 < 60 mmHg on room air. Caused by V/Q mismatch, shunt, diffusion impairment (pneumonia, ARDS, PE, pulmonary edema). Type II (hypercapnic): PaCO2 > 50 mmHg with respiratory acidosis. Caused by alveolar hypoventilation (COPD, neuromuscular disease, drug overdose, obesity hypoventilation).
Initial Ventilator Settings (Post-Intubation)
| Parameter | ARDS / Lung-Protective | Obstructive (COPD/Asthma) |
|---|---|---|
| Mode | Volume control (AC/VC) | Volume control |
| Tidal Volume | 6–8 mL/kg ideal body weight | 6–8 mL/kg IBW |
| Rate | 14–20 | 8–12 (lower to allow exhalation) |
| FiO2 | Start 100%, wean to SpO2 92–96% | Titrate to SpO2 88–92% |
| PEEP | Start 5–10 cmH2O, titrate per ARDSNet PEEP/FiO2 table | Low (3–5 cmH2O, match auto-PEEP) |
| Plateau Pressure Goal | < 30 cmH2O | < 30 cmH2O; watch for auto-PEEP |
ARDSNet protocol (ARMA trial, NEJM 2000): low tidal volume ventilation (6 mL/kg IBW) reduces mortality by 22% in ARDS. Target plateau pressure < 30 cmH2O. Permissive hypercapnia acceptable (pH ≥ 7.20). Prone positioning for 16+ hrs/day in moderate-severe ARDS (P/F < 150) reduces mortality (PROSEVA trial).
17 Acute Ischemic Stroke Neuro
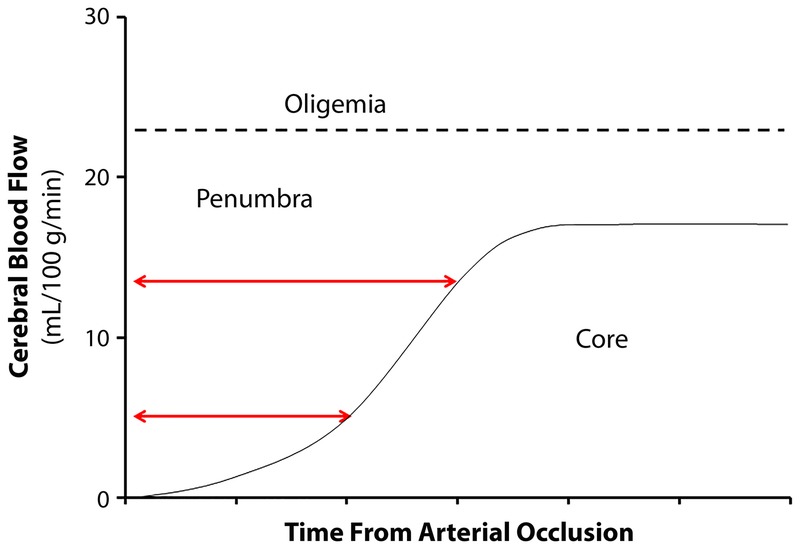
Stroke is a time-critical emergency — "time is brain." Approximately 1.9 million neurons are lost per minute during a large-vessel occlusion. The ED role is rapid recognition (NIHSS assessment), immediate CT to exclude hemorrhage, and initiation of reperfusion therapy within the time window.
Reperfusion Windows
| Therapy | Time Window | Eligibility | Key Details |
|---|---|---|---|
| IV alteplase (tPA) | ≤ 4.5 hours from last known well | Age ≥18, disabling deficit, no hemorrhage on CT | Dose: 0.9 mg/kg (max 90 mg), 10% bolus over 1 min, remainder over 60 min. BP must be < 185/110 before and < 180/105 for 24 hrs after. Exclusion: recent surgery, active bleeding, platelets < 100K, INR > 1.7 |
| IV tenecteplase | ≤ 4.5 hours | Emerging as alternative to alteplase | 0.25 mg/kg single bolus (max 25 mg); easier administration, gaining guideline support |
| Mechanical thrombectomy | ≤ 24 hours (with imaging selection) | Large-vessel occlusion (ICA, M1, M2 MCA), NIHSS ≥ 6, salvageable penumbra on CT perfusion/MRI | Extended to 24 hrs by DAWN and DEFUSE-3 trials. NNT = 2.8 for functional independence |
Common mimics: hypoglycemia (always check glucose before CT), Todd's paralysis (post-ictal), complex migraine, conversion disorder, brain tumor. CT head without contrast is the initial study — its primary role is to exclude hemorrhage, not to "see the stroke." Early ischemic changes are subtle (loss of gray-white differentiation, sulcal effacement, hyperdense vessel sign). CTA head and neck should be obtained simultaneously to identify large-vessel occlusion for thrombectomy candidacy.
18 Hemorrhagic Stroke (ICH & SAH) Neuro
Intracerebral Hemorrhage (ICH)
Spontaneous ICH accounts for 10–15% of all strokes but carries 40–50% 30-day mortality. Most common cause: hypertensive arteriopathy (deep structures: basal ganglia, thalamus, pons, cerebellum). Other causes: cerebral amyloid angiopathy (lobar hemorrhages in elderly), anticoagulant use, vascular malformations, hemorrhagic conversion of ischemic stroke. CT head shows hyperdense (bright white) intraparenchymal blood.
Management: aggressive BP control (SBP target < 140 mmHg within 1 hr — INTERACT2; use nicardipine infusion). Reverse anticoagulation immediately if applicable (warfarin → 4-factor PCC + vitamin K 10 mg IV; DOAC → idarucizumab for dabigatran, andexanet alfa for Xa inhibitors, or 4-factor PCC if specific reversal unavailable). Neurosurgery consult for cerebellar hemorrhage > 3 cm (may need emergent evacuation) or hydrocephalus (EVD placement).
Subarachnoid Hemorrhage (SAH)
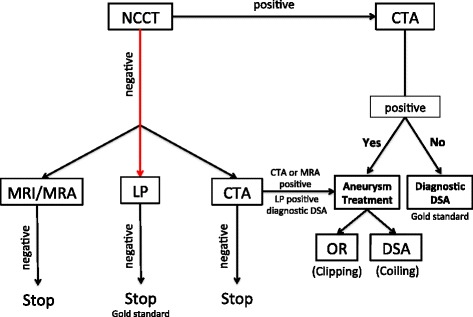
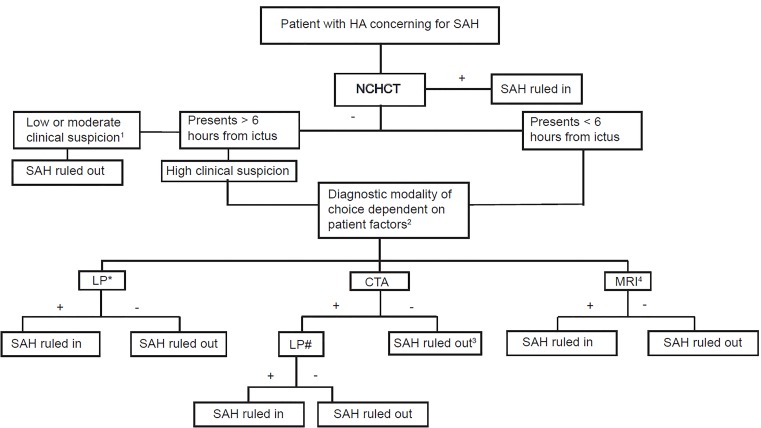
85% from ruptured cerebral aneurysm. Classic presentation: "worst headache of my life," sudden onset, maximal intensity at onset ("thunderclap headache"), with or without neck stiffness, photophobia, vomiting, syncope, or coma. CT head sensitivity: 95–100% within 6 hours, drops to ~85% at 24 hours and further with time. If CT is negative and clinical suspicion remains: lumbar puncture looking for xanthochromia (yellow discoloration of CSF from bilirubin, most reliable at 12+ hours after onset) or elevated RBCs that do not clear with sequential tubes.
After SAH diagnosis: CTA to locate the aneurysm, neurosurgery/neurointerventional consult for definitive treatment (endovascular coiling preferred over surgical clipping for most aneurysms per ISAT trial). Nimodipine 60 mg PO q4h × 21 days (prevents vasospasm-related delayed cerebral ischemia — the only medication proven to improve outcomes in SAH). Keep SBP < 160 until aneurysm secured.
19 Status Epilepticus Neuro
Defined as continuous seizure activity lasting ≥ 5 minutes or ≥ 2 seizures without return to baseline. A true time-critical neurological emergency — prolonged seizure activity causes excitotoxic neuronal injury, rhabdomyolysis, hyperthermia, and systemic acidosis. Mortality approaches 20% and increases with duration of seizure.
Stepwise Treatment Protocol
| Stage | Timing | Intervention |
|---|---|---|
| 1st line | 0–5 min | Benzodiazepines: lorazepam 0.1 mg/kg IV (max 4 mg, may repeat ×1) OR midazolam 10 mg IM (if no IV). Prehospital: diazepam 20 mg rectal or midazolam 10 mg IM/intranasal |
| 2nd line | 5–20 min | If seizures persist after 2 doses of benzodiazepine: fosphenytoin 20 mg PE/kg IV (rate ≤ 150 mg PE/min); OR levetiracetam (Keppra) 60 mg/kg IV (max 4500 mg) over 15 min; OR valproic acid 40 mg/kg IV (max 3000 mg) over 10 min |
| Refractory | > 20 min | Intubation + continuous IV infusion: propofol (1–2 mg/kg bolus, 20–80 mcg/kg/min), midazolam (0.2 mg/kg bolus, 0.1–2 mg/kg/hr), or pentobarbital (5 mg/kg load, 1–5 mg/kg/hr). Continuous EEG monitoring required |
20 Meningitis & Encephalitis Neuro
Bacterial meningitis carries 20–25% mortality even with treatment and requires emergent antibiotics — do not delay for LP or imaging. Classic triad: fever, nuchal rigidity, altered mental status (present in only ~44% of bacterial meningitis). Kernig's sign (pain with knee extension when hip flexed) and Brudzinski's sign (involuntary hip flexion with passive neck flexion) have low sensitivity but moderate specificity.
Empiric Antibiotics by Age
| Age Group | Common Pathogens | Empiric Regimen |
|---|---|---|
| < 1 month | GBS, E. coli, Listeria | Ampicillin + cefotaxime (or gentamicin) |
| 1–23 months | S. pneumoniae, N. meningitidis, GBS | Vancomycin + ceftriaxone (or cefotaxime) |
| 2–50 years | S. pneumoniae, N. meningitidis | Vancomycin + ceftriaxone |
| > 50 years or immunocompromised | S. pneumoniae, N. meningitidis, Listeria | Vancomycin + ceftriaxone + ampicillin (Listeria coverage) |
Dexamethasone 0.15 mg/kg IV q6h × 4 days — give with or just before the first antibiotic dose. Reduces mortality and neurological sequelae in pneumococcal meningitis (de Gans et al., NEJM 2002).
LP Interpretation
| Parameter | Bacterial | Viral | TB/Fungal |
|---|---|---|---|
| Opening pressure | Elevated (> 25 cmH2O) | Normal to mildly elevated | Elevated |
| WBC | 1000–10,000+ (PMN predominant) | 10–500 (lymphocyte predominant) | 100–500 (lymphocyte predominant) |
| Glucose | Low (< 40 or CSF:serum < 0.4) | Normal | Low |
| Protein | High (> 250 mg/dL) | Normal to mildly elevated | High |
| Gram stain | Positive in 60–90% | Negative | AFB smear (low sensitivity) |
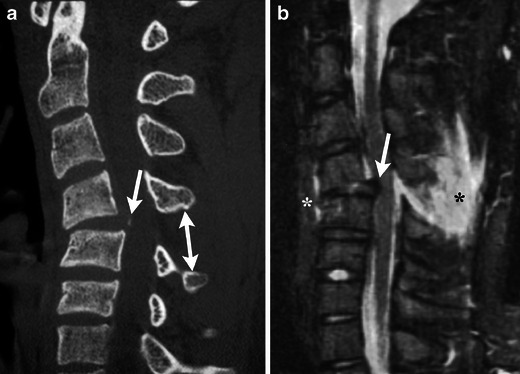
21 Spinal Cord Compression Neuro
Acute spinal cord compression is a neurosurgical/oncologic emergency. Most common cause: metastatic disease (breast, lung, prostate account for >50%). Other causes: epidural abscess, disk herniation, epidural hematoma. Presentation: progressive back pain (often the first symptom, present for weeks before neurological deficits), bilateral leg weakness, sensory level, urinary retention or incontinence. A sensory level (loss of sensation below a dermatomal line) is highly specific for cord compression.
Diagnosis: MRI of the entire spine (urgent, within hours). Treatment: dexamethasone 10 mg IV bolus followed by 4 mg IV q6h (reduces cord edema). Urgent neurosurgery or radiation oncology consult for surgical decompression vs. radiation therapy. Functional outcomes correlate directly with neurological status at the time of treatment — ambulatory patients have >80% chance of remaining ambulatory; paraplegic patients have <10% chance of walking again.
22 Traumatic Brain Injury Trauma
Glasgow Coma Scale (GCS)
| Component | Response | Score |
|---|---|---|
| Eye Opening (E) | Spontaneous | 4 |
| To voice | 3 | |
| To pain | 2 | |
| None | 1 | |
| Verbal (V) | Oriented | 5 |
| Confused | 4 | |
| Inappropriate words | 3 | |
| Incomprehensible sounds | 2 | |
| None | 1 | |
| Motor (M) | Obeys commands | 6 |
| Localizes pain | 5 | |
| Withdrawal (flexion) | 4 | |
| Abnormal flexion (decorticate) | 3 | |
| Extension (decerebrate) | 2 | |
| None | 1 |
GCS 13–15: mild TBI; 9–12: moderate; 3–8: severe (intubate for airway protection). The motor score is the single most predictive component.
Herniation Syndromes
Signs of herniation: unilateral fixed, dilated pupil (CN III compression from uncal herniation), Cushing's triad (hypertension, bradycardia, irregular respirations — a late and ominous sign), decerebrate posturing. Emergency management of herniation: elevate HOB 30°, mannitol 1–1.5 g/kg IV (osmotic diuresis) or hypertonic saline 3% 250 mL or 23.4% 30 mL IV over 15 min, hyperventilation to pCO2 30–35 mmHg (temporizing only — causes vasoconstriction reducing ICP but also reducing cerebral perfusion), emergent neurosurgery consult for decompressive craniectomy.

Canadian CT Head Rule
For minor head injury (GCS 13–15) — CT is required if ANY of the following are present:
| High Risk (for neurosurgical intervention) | Medium Risk (for brain injury on CT) |
|---|---|
| GCS < 15 at 2 hours post-injury | Retrograde amnesia > 30 min before impact |
| Suspected open or depressed skull fracture | Dangerous mechanism (pedestrian struck, ejected from vehicle, fall > 3 feet / 5 stairs) |
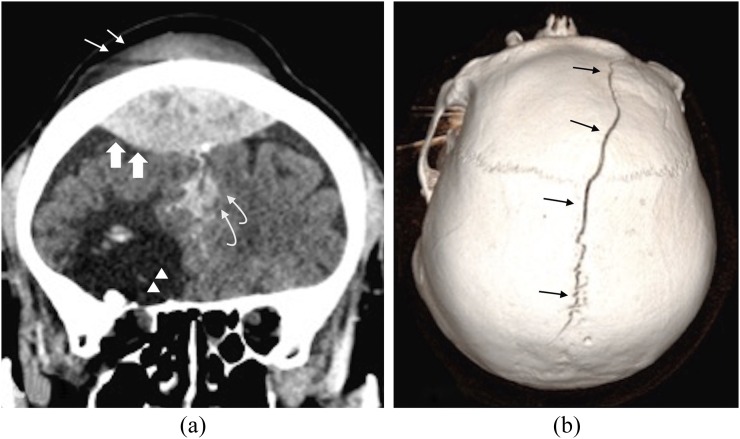
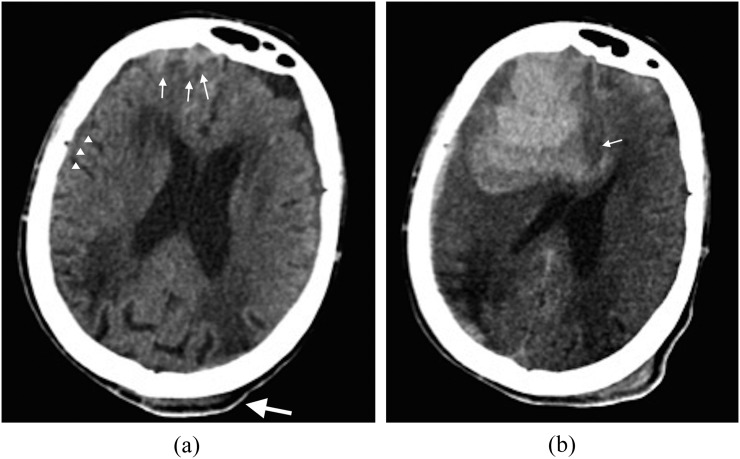
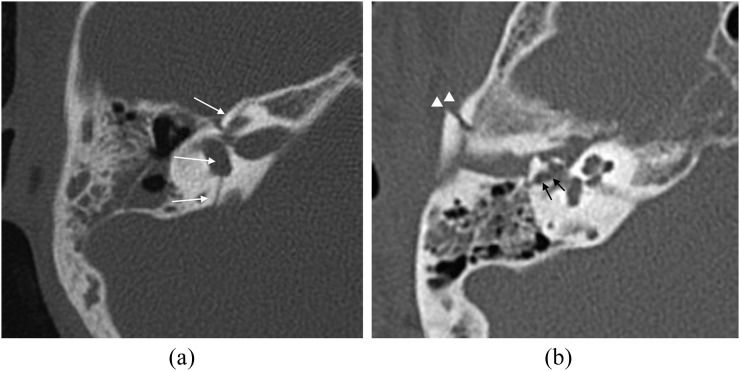
| Any sign of basal skull fracture (hemotympanum, raccoon eyes, Battle's sign, CSF otorrhea/rhinorrhea) | — |
| ≥ 2 episodes of vomiting | — |
| Age ≥ 65 | — |
23 Cervical Spine Injury Trauma
The ED must identify or confidently exclude c-spine injury in every trauma patient. Clinical decision rules allow safe clearance without imaging in low-risk patients.
NEXUS Criteria & Canadian C-Spine Rule
NEXUS: C-spine imaging NOT needed if ALL 5 criteria met: no posterior midline tenderness, no focal neurological deficit, normal alertness, no intoxication, no distracting injury. Canadian C-Spine Rule (more sensitive than NEXUS): Step 1 — any high-risk factor mandating imaging? (age ≥ 65, dangerous mechanism, paresthesias in extremities). If yes → image. Step 2 — any low-risk factor allowing safe ROM assessment? (simple rear-end MVC, sitting in ED, ambulatory at any time, delayed onset neck pain, no midline tenderness). If yes → Step 3: can patient actively rotate neck 45° left and right? If yes → no imaging needed.
High-Yield C-Spine Injuries
| Injury | Mechanism | Level | Key Point |
|---|---|---|---|
| Atlas (C1) fracture (Jefferson) | Axial loading (diving) | C1 | Lateral mass spread on open-mouth view; usually stable |
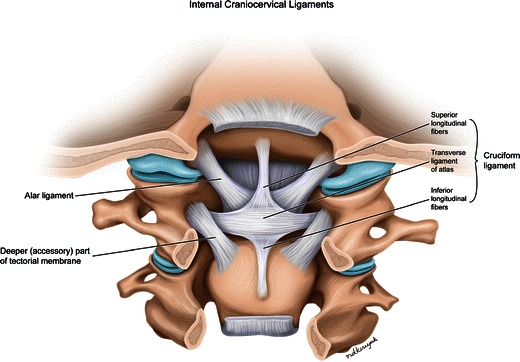
| Odontoid (dens) fracture | Flexion/extension | C2 | Type II (base of dens) most common and most unstable; common in elderly falls |
| Hangman's fracture | Hyperextension + axial load | C2 pedicles | Bilateral pars fracture; often paradoxically stable (spinal canal widened) |
| Facet dislocation | Flexion-rotation | Subaxial (C3–C7) | Unilateral: 25% subluxation; Bilateral: 50% subluxation with high SCI risk |
| SCIWORA | Flexion/extension in children | Any | Spinal cord injury without radiographic abnormality; MRI required. More common in pediatric patients due to ligamentous laxity |
24 Chest Trauma Trauma
Chest trauma is responsible for 25% of trauma deaths. Most life-threatening injuries can be identified on primary survey and CXR. The "deadly dozen" includes tension PTX, open PTX, massive hemothorax, flail chest, cardiac tamponade, and tracheobronchial disruption (identified during primary survey), plus aortic injury, diaphragmatic rupture, esophageal perforation, pulmonary contusion, myocardial contusion, and simple PTX/hemothorax (identified during secondary survey).
Key Chest Trauma Entities
| Injury | Diagnosis | Management |
|---|---|---|
| Massive hemothorax (>1500 mL initial or >200 mL/hr × 2–4 hrs) | CXR: opacification of hemithorax; absent breath sounds, dullness to percussion, hypotension | Chest tube (36–40 Fr) + autotransfusion; if criteria met → emergent thoracotomy |
| Flail chest (≥3 consecutive ribs fractured in ≥2 places) | Paradoxical chest wall movement, crepitus, severe pain | Pain control (epidural or intercostal nerve block), positive-pressure ventilation if respiratory failure; underlying pulmonary contusion is the real threat |
| Blunt cardiac injury (BCI) | Sternal fracture, ECG changes (new RBBB, ST changes), elevated troponin | Monitoring, treat arrhythmias; echocardiography if hemodynamically significant; rarely causes tamponade |
| Traumatic aortic injury | Widened mediastinum on CXR; confirmed by CTA (intimal flap at aortic isthmus distal to left subclavian) | HR/BP control (same as dissection), emergent TEVAR or open repair. 85% die at scene; of survivors, 50% die within 24 hrs without repair |
25 Abdominal Trauma & FAST Exam Trauma
Blunt abdominal trauma: spleen is the most commonly injured solid organ (left-sided mechanism), followed by liver (right-sided). In penetrating trauma, liver is most commonly injured (stab wounds), followed by small bowel (gunshot wounds). The FAST exam (Focused Assessment with Sonography for Trauma) is performed in the resuscitation bay to detect free fluid (blood) in four windows: RUQ (Morison's pouch — most sensitive for free fluid), LUQ (splenorenal recess), suprapubic (pelvis), and subxiphoid (pericardial). FAST is 85–95% sensitive for significant hemoperitoneum.
Management Algorithm
Hemodynamically unstable + positive FAST: emergent exploratory laparotomy. Hemodynamically stable + positive FAST or high-energy mechanism: CT abdomen/pelvis with IV contrast for injury grading. FAST negative + stable: serial exams; CT if clinical concern persists (FAST misses retroperitoneal, hollow viscus, and diaphragm injuries).
Splenic Injury Grading (AAST)
| Grade | Injury | Management |
|---|---|---|
| I | Subcapsular hematoma < 10% surface; capsular laceration < 1 cm | Non-operative (observation, serial exams, Hgb q6h) |
| II | Subcapsular 10–50%; intraparenchymal < 5 cm; laceration 1–3 cm | Non-operative in most stable patients |
| III | Subcapsular > 50% or expanding; intraparenchymal > 5 cm; laceration > 3 cm | Non-operative with angioembolization vs. operative (patient-dependent) |
| IV | Laceration involving segmental or hilar vessels; >25% devascularized | Angioembolization or splenectomy |
| V | Shattered spleen or hilar vascular injury with complete devascularization | Splenectomy |
26 Pelvic Fracture & Hemorrhage Trauma
Unstable pelvic fractures (open-book, vertical shear) can cause massive hemorrhage from the presacral venous plexus and pelvic arterial branches, with blood loss exceeding 3–5 liters. Mechanism: high-energy (MVC, motorcycle, pedestrian struck, fall from height). Exam: pelvic instability on gentle AP compression (perform ONCE — repeated rocking worsens hemorrhage). Do NOT perform a rocking exam if instability is obvious or if a pelvic binder is already in place.
Management: pelvic binder (commercially available or bedsheet wrapped tightly at the level of the greater trochanters) to reduce pelvic volume and tamponade hemorrhage. Activate MTP. If hemodynamically unstable despite binder + MTP: angioembolization (if CTA shows arterial blush) or preperitoneal pelvic packing (direct surgical packing of the pelvic space). REBOA (Resuscitative Endovascular Balloon Occlusion of the Aorta) in Zone III (infrarenal) is an emerging temporizing measure.
27 Orthopedic Emergencies Trauma
Open Fractures — Gustilo-Anderson Classification
| Type | Wound Size | Soft Tissue Injury | Contamination | Antibiotic |
|---|---|---|---|---|
| I | < 1 cm | Minimal | Clean | Cefazolin 2 g IV |
| II | 1–10 cm | Moderate | Moderate | Cefazolin 2 g IV |
| IIIA | > 10 cm | Extensive, adequate coverage | High | Cefazolin + gentamicin |
| IIIB | > 10 cm | Extensive, requires flap coverage | High | Cefazolin + gentamicin |
| IIIC | Any | Vascular injury requiring repair | Any | Cefazolin + gentamicin + PCN if soil contamination |
All open fractures need: tetanus prophylaxis, IV antibiotics within 1 hour, irrigation and debridement in the OR (ideally within 6–24 hours), and orthopedic consult.

Compartment Syndrome
Elevated pressure within a closed fascial compartment compromising perfusion. Most common after tibial fractures, crush injuries, and reperfusion after vascular repair. The 6 P's (Pain out of proportion, Pain with passive stretch — the earliest and most reliable sign, Paresthesias, Pressure/tense compartment, Pallor, Pulselessness — a LATE finding). Normal compartment pressure: 0–8 mmHg. Delta pressure (diastolic BP minus compartment pressure) < 30 mmHg = fasciotomy indicated. Treatment: emergent fasciotomy. Delay beyond 6–8 hours causes irreversible muscle necrosis and Volkmann's contracture.
High-Risk Dislocations
| Joint | Direction | Neurovascular Risk | Urgency |
|---|---|---|---|
| Shoulder (anterior, 95%) | Anterior-inferior | Axillary nerve (deltoid weakness, lateral shoulder numbness) | Reduce promptly; pre/post reduction neurovascular exam mandatory |
| Hip (posterior, 90%) | Posterior | Sciatic nerve; AVN risk increases after 6 hrs | Reduce within 6 hours to prevent femoral head AVN |
| Knee | Anterior or posterior | Popliteal artery injury in 30–40%; peroneal nerve | Vascular emergency: reduce immediately, ABI, CTA if any concern for vascular injury |
| Lunate/perilunate (wrist) | Volar (lunate) or dorsal (perilunate) | Median nerve (carpal tunnel) | Often missed on initial X-ray; look for "spilled teacup" sign on lateral |
28 Acute Abdomen & Imaging Approach GI
The "acute abdomen" is not a diagnosis but a clinical presentation: acute abdominal pain requiring urgent evaluation and often intervention. The ED approach centers on identifying surgical emergencies (appendicitis, perforated viscus, bowel obstruction, mesenteric ischemia, ruptured AAA, ectopic pregnancy) and time-critical medical conditions (DKA, ACS with epigastric pain, adrenal crisis).
Abdominal Pain Differential by Location
| Location | Key Diagnoses |
|---|---|
| RUQ | Cholecystitis, hepatitis, Fitz-Hugh-Curtis, hepatic abscess, RLL pneumonia, nephrolithiasis |
| LUQ | Splenic pathology (infarct, rupture), gastric ulcer, pancreatitis (tail), LLL pneumonia |
| RLQ | Appendicitis, ovarian torsion/cyst, ectopic pregnancy, Meckel's, inguinal hernia, mesenteric adenitis |
| LLQ | Diverticulitis, ovarian torsion/cyst, ectopic pregnancy, sigmoid volvulus, inguinal hernia |
| Epigastric | Peptic ulcer, pancreatitis, ACS (inferior MI), AAA, gastritis, biliary disease |
| Periumbilical | Early appendicitis (visceral pain), SBO, mesenteric ischemia, AAA |
| Suprapubic | UTI, urinary retention, ovarian torsion, ectopic pregnancy, PID |
| Diffuse | Peritonitis (any cause), DKA, mesenteric ischemia, SBO, IBD flare |
29 Appendicitis & Cholecystitis GI
Appendicitis
Lifetime incidence 7–8%. Classic presentation: periumbilical pain migrating to RLQ (visceral → somatic pain as inflammation reaches the parietal peritoneum), anorexia, nausea/vomiting, low-grade fever. McBurney's point tenderness (1/3 of the distance from ASIS to umbilicus). Special signs: Rovsing's (RLQ pain with LLQ palpation), psoas sign (pain with right hip extension — retrocecal appendix), obturator sign (pain with internal rotation of flexed right hip — pelvic appendix).
Diagnosis: CT abdomen/pelvis with IV contrast is the gold standard (sensitivity 98%). Ultrasound is first-line in pregnant patients and children. Alvarado (MANTRELS) score: Migration, Anorexia, Nausea, Tenderness (RLQ), Rebound, Elevation of temperature, Leukocytosis, Shift to left; score ≥7 strongly suggests appendicitis. Treatment: appendectomy (laparoscopic preferred). Antibiotics alone are an option for uncomplicated appendicitis in selected patients (CODA trial), though recurrence rate is ~30% at 2 years.
Acute Cholecystitis
Gallstone impacted in the cystic duct causing gallbladder inflammation. Presentation: persistent RUQ pain (>4–6 hrs, distinguishing it from biliary colic which resolves), fever, Murphy's sign (inspiratory arrest during RUQ palpation). Diagnosis: RUQ ultrasound showing gallstones + gallbladder wall thickening > 3 mm + pericholecystic fluid + sonographic Murphy's sign. HIDA scan if ultrasound equivocal (non-filling of gallbladder = cystic duct obstruction). Treatment: NPO, IV fluids, antibiotics (piperacillin-tazobactam or ceftriaxone + metronidazole), surgical consult for cholecystectomy (ideally within 72 hours of admission).
30 Bowel Obstruction & Mesenteric Ischemia GI
Small Bowel Obstruction (SBO)
Causes: adhesions from prior surgery (75%), hernias (15%), malignancy, Crohn's disease, volvulus. Presentation: crampy abdominal pain, nausea/vomiting (earlier and more profuse in proximal obstruction), obstipation/constipation, distension. X-ray: dilated small bowel loops (> 3 cm), air-fluid levels, decompressed colon. CT with IV and oral contrast is the definitive study — identifies transition point, closed-loop obstruction, and signs of strangulation (mesenteric haziness, wall thickening, reduced enhancement, pneumatosis).
Treatment: NGT decompression (Salem sump), IV fluids, NPO, electrolyte correction. Surgery if: signs of strangulation/ischemia, closed-loop obstruction, peritonitis, complete obstruction without improvement in 48–72 hours, or incarcerated hernia.
Mesenteric Ischemia
Acute mesenteric ischemia is a surgical emergency with 60–80% mortality. The hallmark: "pain out of proportion to exam" — severe abdominal pain with a benign abdominal examination (early). As bowel infarction develops: peritoneal signs, bloody stool, lactic acidosis. Causes: SMA embolism (~50%), SMA thrombosis (~25%), NOMI (~15%), mesenteric venous thrombosis (~10%). CTA is diagnostic (filling defects, bowel wall changes). Treatment: heparin, emergent surgical embolectomy or revascularization, bowel resection if necrotic; second-look laparotomy at 24–48 hours.
31 GI Hemorrhage GI
Upper GI Bleeding (UGIB)
Source proximal to the ligament of Treitz. Presentation: hematemesis (bright red or coffee-ground emesis), melena (black tarry stool), or hematochezia (if massive). Most common causes: peptic ulcer disease (35–50%), esophageal/gastric varices (10–20%), Mallory-Weiss tear, erosive gastritis/esophagitis. Glasgow-Blatchford Score (GBS): BUN, hemoglobin, SBP, HR, melena, syncope, hepatic disease, heart failure. Score 0–1: safe for outpatient management. Score ≥6: high risk, needs intervention.
Management: 2 large-bore IVs, fluid resuscitation, type and cross. Restrictive transfusion (Hgb target ≥ 7 g/dL, ≥ 8 if active CAD per Villanueva et al., NEJM 2013). PPI: pantoprazole 80 mg IV bolus, then 8 mg/hr infusion for suspected ulcer bleeding. EGD within 24 hours (12 hours if high-risk features). Variceal bleed: octreotide 50 mcg IV bolus then 50 mcg/hr, antibiotics (ceftriaxone 1 g IV), urgent EGD for band ligation. If uncontrolled variceal bleeding: Blakemore/Minnesota tube or TIPS.
Lower GI Bleeding (LGIB)
Source distal to ligament of Treitz. Presentation: hematochezia (bright red blood per rectum). Common causes: diverticular bleeding (most common cause of massive LGIB), hemorrhoids, AV malformations, colitis (IBD, ischemic, infectious), colorectal cancer. Most LGIB stops spontaneously (80–85%). Hemodynamically significant LGIB: resuscitate, CTA if unstable (identifies active extravasation/source), colonoscopy within 24 hours if stabilized.
32 Pancreatitis GI
Diagnosis requires 2 of 3: (1) characteristic abdominal pain (epigastric, radiating to back, worse after eating), (2) serum lipase ≥ 3× upper limit of normal, (3) imaging findings (CT showing pancreatic edema/necrosis/peripancreatic stranding). Lipase is preferred over amylase (more sensitive and specific, stays elevated longer). Most common causes: gallstones (40%) and alcohol (30%). Other: hypertriglyceridemia (> 1000 mg/dL), post-ERCP, medications (valproic acid, azathioprine), autoimmune.
Management: aggressive IV fluid resuscitation (LR preferred, 1.5 mL/kg/hr for 24 hrs per WATERFALL trial — though subsequent evidence favors moderate resuscitation), pain control (IV opioids, NSAIDs), early enteral nutrition (within 24 hrs if tolerated — no need to wait for pain resolution). CT is NOT needed at presentation unless the diagnosis is uncertain or complications are suspected. CT should be obtained at 48–72 hours if not improving to assess for necrosis. Ranson's criteria and BISAP score predict severity. Gallstone pancreatitis requires cholecystectomy during the same admission (to prevent recurrence).
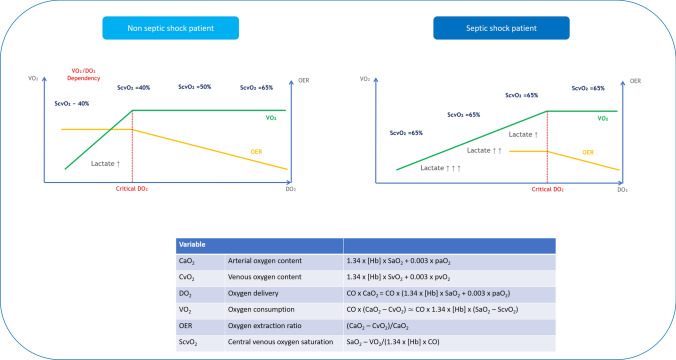
33 Sepsis & Septic Shock Infxn
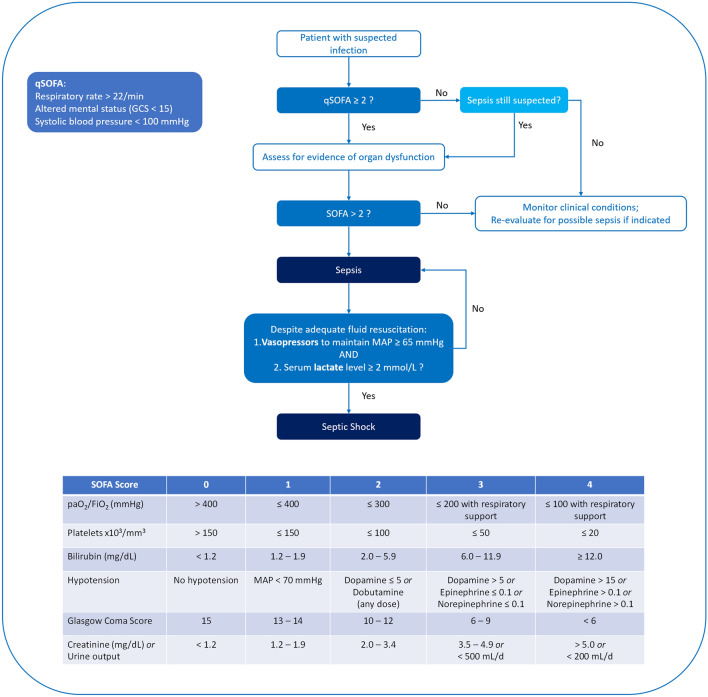
Sepsis is life-threatening organ dysfunction caused by a dysregulated host response to infection. The Sepsis-3 (2016) definition requires suspected infection + acute change in SOFA score ≥ 2 points. qSOFA (quick bedside screen): RR ≥ 22, altered mentation, SBP ≤ 100. Two or more qSOFA criteria should prompt further evaluation. Septic shock: sepsis + vasopressor requirement to maintain MAP ≥ 65 + lactate > 2 mmol/L despite adequate fluid resuscitation. Septic shock mortality: 30–40%.
Hour-1 Bundle (Surviving Sepsis Campaign 2021)
| Intervention | Details |
|---|---|
| Measure lactate | If lactate > 2 mmol/L, remeasure within 2–4 hours to guide resuscitation |
| Blood cultures before antibiotics | At least 2 sets (aerobic + anaerobic) from different sites; do NOT delay antibiotics for cultures |
| Broad-spectrum antibiotics | Within 1 hour of sepsis recognition. Common regimens: vancomycin + piperacillin-tazobactam; or vancomycin + cefepime; or meropenem for critically ill |
| IV fluids | 30 mL/kg crystalloid (LR preferred over NS) for hypotension or lactate ≥ 4 mmol/L. Reassess after each bolus; do NOT give all 30 mL/kg blindly if patient develops volume overload |
| Vasopressors | If hypotension persists after initial fluid resuscitation: norepinephrine is first-line (start 5–10 mcg/min, titrate to MAP ≥ 65). Add vasopressin 0.04 units/min as second-line. Consider hydrocortisone 200 mg/day IV if shock refractory to vasopressors |
34 Skin & Soft Tissue Infections Infxn

Spectrum of SSTIs
| Entity | Description | Treatment |
|---|---|---|
| Cellulitis (non-purulent) | Spreading erythema, warmth, tenderness without drainable collection; typically beta-hemolytic strep | Mild: cephalexin 500 mg QID or amoxicillin-clavulanate. Moderate/severe: cefazolin 1–2 g IV q8h or ceftriaxone 1 g IV daily. Mark borders with pen to track progression |
| Abscess (purulent) | Fluctuant, tender collection; often CA-MRSA | I&D is the primary treatment. Antibiotics for surrounding cellulitis, systemic symptoms, or high-risk patients: TMP-SMX DS BID or doxycycline 100 mg BID × 7–10 days |
| Necrotizing fasciitis | Rapidly progressive deep infection destroying fascia and subcutaneous tissue. Pain out of proportion, crepitus, skin necrosis, bullae, "dishwater" gray drainage, systemic toxicity | Emergent surgical debridement + broad-spectrum antibiotics (vancomycin + piperacillin-tazobactam + clindamycin for toxin suppression). CT showing gas in soft tissue is specific but not sensitive. LRINEC score ≥6 suggests necrotizing infection |
Pain out of proportion to visible findings, rapid progression despite antibiotics, bullae/skin necrosis, crepitus on palpation, systemic toxicity (fever, tachycardia, hypotension), WBC > 15,000 or < 4,000, elevated CK. If suspected, do NOT delay surgical consult for imaging. Mortality exceeds 30% even with treatment; approaches 100% without surgery.
35 Toxidrome Recognition & General Approach Tox
A toxidrome is a constellation of signs and symptoms that suggests a particular class of poisoning. Recognizing the toxidrome narrows the differential immediately and guides empiric treatment before confirmatory labs return.
| Toxidrome | Vital Signs | Pupils | Key Findings | Agents | Antidote |
|---|---|---|---|---|---|
| Sympathomimetic | Hypertension, tachycardia, hyperthermia | Mydriasis | Agitation, diaphoresis, tremor, seizures | Cocaine, amphetamines, MDMA, synthetic cathinones | Benzodiazepines (primary treatment); avoid beta-blockers with cocaine |
| Anticholinergic | Tachycardia, hyperthermia, hypertension | Mydriasis | "Hot as a hare, dry as a bone, red as a beet, blind as a bat, mad as a hatter." Dry skin, urinary retention, ileus, delirium | Diphenhydramine, TCAs, atropine, jimsonweed, scopolamine | Physostigmine 1–2 mg IV slow push (for pure anticholinergic; avoid in TCA overdose) |
| Cholinergic | Bradycardia, hypotension | Miosis | DUMBBBELS: Diarrhea, Urination, Miosis, Bronchospasm/Bradycardia, Emesis, Lacrimation, Salivation | Organophosphates, nerve agents, carbamates | Atropine (high doses, 2–4 mg IV, double q5min until secretions dry) + pralidoxime (2-PAM) |
| Opioid | Bradypnea, hypotension, bradycardia | Miosis (pinpoint) | CNS depression, respiratory depression, decreased bowel sounds | Heroin, fentanyl, morphine, oxycodone, methadone | Naloxone 0.04–2 mg IV/IM/IN (start low, titrate to respiratory effort, not alertness) |
| Sedative-Hypnotic | Bradypnea, hypotension | Normal or miosis | CNS depression, normal pupils (distinguishes from opioid) | Benzodiazepines, barbiturates, GHB, zolpidem | Flumazenil 0.2 mg IV (rarely used — seizure risk in chronic benzodiazepine users or co-ingestion with seizure-threshold-lowering drugs) |
| Serotonin Syndrome | Tachycardia, hypertension, hyperthermia | Mydriasis | Clonus (spontaneous, inducible, ocular), hyperreflexia, agitation, diaphoresis, diarrhea | SSRIs + MAOIs, tramadol, linezolid, dextromethorphan, MDMA | Cyproheptadine 12 mg PO load, then 4 mg q6h; benzodiazepines for agitation; avoid paralysis (masks clonus) |
36 Acetaminophen & Salicylate Toxicity Tox
Acetaminophen (APAP) Overdose
The most common cause of acute liver failure in the US. Toxic dose: > 150 mg/kg or > 7.5 g in adults. Metabolism: at therapeutic doses, APAP is metabolized via glucuronidation/sulfation. In overdose, these pathways saturate, and CYP2E1 converts APAP to NAPQI, a toxic metabolite that depletes glutathione and causes hepatocellular necrosis. Stages: (1) 0–24 hrs: nausea, vomiting, normal labs; (2) 24–72 hrs: RUQ pain, rising AST/ALT; (3) 72–96 hrs: peak hepatotoxicity (AST/ALT > 10,000, coagulopathy, renal failure, encephalopathy); (4) Recovery or death.
Rumack-Matthew Nomogram: Plot the 4-hour post-ingestion APAP level on the nomogram. Treatment line starts at 150 mcg/mL at 4 hours. If level is above the line: N-acetylcysteine (NAC) — IV protocol: 150 mg/kg over 1 hour, then 50 mg/kg over 4 hours, then 100 mg/kg over 16 hours (total 21 hours). Oral: 140 mg/kg load, then 70 mg/kg q4h × 17 additional doses. NAC is most effective within 8 hours but should be given at ANY time if clinical concern for toxicity. Always check an APAP level on every overdose patient regardless of reported ingestion.
Salicylate Toxicity
Acute ingestion > 150 mg/kg is toxic; > 500 mg/kg is potentially lethal. Chronic salicylism occurs at lower levels in elderly patients on aspirin. Pathophysiology: uncouples oxidative phosphorylation, stimulates respiratory center, causes metabolic acidosis. Classic ABG: mixed respiratory alkalosis + metabolic acidosis (early: respiratory alkalosis from central stimulation; late: AG metabolic acidosis predominates). Symptoms: tinnitus, nausea, vomiting, hyperpnea, diaphoresis, altered mental status, seizures.
Treatment: sodium bicarbonate infusion (150 mEq in 1 L D5W at 1.5–2× maintenance) targeting urine pH 7.5–8.0 (alkalinize the urine to trap salicylate in its ionized form for renal excretion). Monitor K+ closely (hypokalemia prevents urine alkalinization). Hemodialysis indications: salicylate level > 90 mg/dL (acute) or > 60 mg/dL (chronic), altered mental status, renal failure, pulmonary edema, refractory acidosis. Do NOT intubate salicylate patients unless absolutely necessary — their compensatory hyperventilation is maintaining acid-base balance; matching their minute ventilation post-intubation is extremely difficult, and loss of respiratory compensation leads to rapid acidemia, cardiovascular collapse, and death.
37 Alcohol Withdrawal & Sedative-Hypnotic Toxicity Tox
Alcohol withdrawal is a spectrum from mild (tremor, anxiety, insomnia, 6–24 hrs after last drink) to moderate (hallucinations, 12–48 hrs) to seizures (12–48 hrs) to delirium tremens (48–96 hrs: confusion, agitation, autonomic instability, hyperthermia, seizures — mortality 5–15% without treatment, up to 35% untreated). Use the CIWA-Ar score (Clinical Institute Withdrawal Assessment for Alcohol, Revised) to guide benzodiazepine dosing: 10 parameters scored 0–7 each (max 67). CIWA < 10: mild, monitoring. 10–18: moderate, treat. > 18: severe, aggressive treatment.
Treatment: benzodiazepines are the mainstay. Symptom-triggered dosing (CIWA-guided) is preferred over fixed-schedule. Diazepam 10–20 mg IV q10–15 min (active metabolites provide smooth taper) or lorazepam 2–4 mg IV q15–30 min (preferred in liver failure — no active metabolites). For refractory DTs: phenobarbital 130–260 mg IV, propofol infusion, or dexmedetomidine adjunct. IV thiamine 500 mg before glucose (prevent Wernicke's encephalopathy), IV magnesium, folate, multivitamins.
38 Anaphylaxis Tox
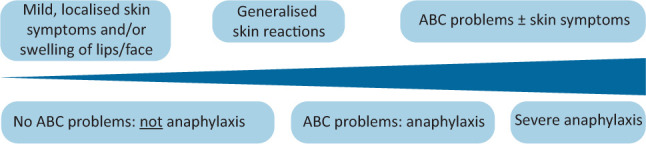
Anaphylaxis is a severe, life-threatening systemic allergic reaction involving ≥2 organ systems (skin/mucosal, respiratory, cardiovascular, GI). Triggers: foods (peanuts, tree nuts, shellfish), medications (antibiotics, NSAIDs), insect stings, latex. Can occur within seconds to minutes of exposure. Presentation: urticaria/angioedema (90%), bronchospasm/stridor, hypotension/tachycardia, nausea/vomiting/cramping.
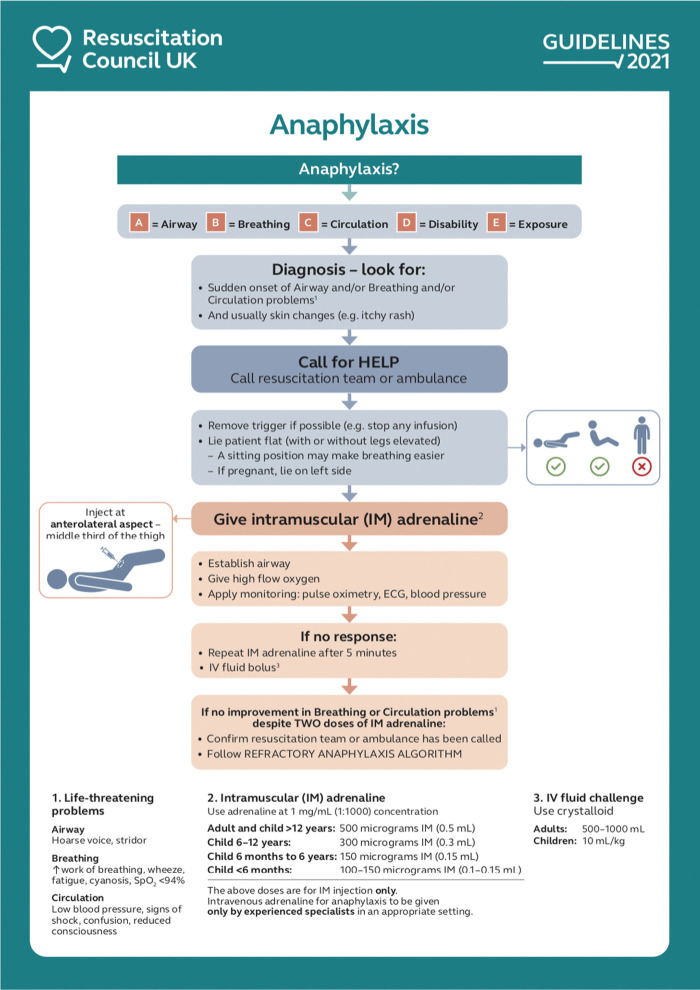
Epinephrine is the ONLY first-line treatment: 0.3–0.5 mg IM (1:1000 concentration) in the anterolateral thigh. May repeat q5–15 min. IV epinephrine (1:10,000, 0.1 mg boluses or infusion 1–10 mcg/min) for refractory shock. Adjuncts: IV fluids (1–2 L bolus for hypotension), albuterol nebulized (bronchospasm), diphenhydramine 50 mg IV (H1 blocker), famotidine 20 mg IV (H2 blocker), methylprednisolone 125 mg IV (prevents biphasic reaction — occurs in 5–20% at 1–72 hours). Observe 4–6 hours post-treatment; prescribe EpiPen and refer to allergist on discharge.
39 Environmental Emergencies Tox
Heat Emergencies
| Entity | Core Temp | Key Features | Treatment |
|---|---|---|---|
| Heat exhaustion | < 40°C (104°F) | Heavy sweating, weakness, headache, nausea, normal mentation | Rest, cool environment, oral/IV rehydration |
| Heat stroke | ≥ 40°C (104°F) | Altered mental status (confusion, seizures, coma) + hot skin (may be dry or sweaty) | Aggressive cooling: cold water immersion (most effective, target < 39°C within 30 min), evaporative cooling (mist + fans), ice packs to axillae/groin/neck. Stop cooling at 38.5°C. Intubate if needed, IV fluids, treat rhabdomyolysis |
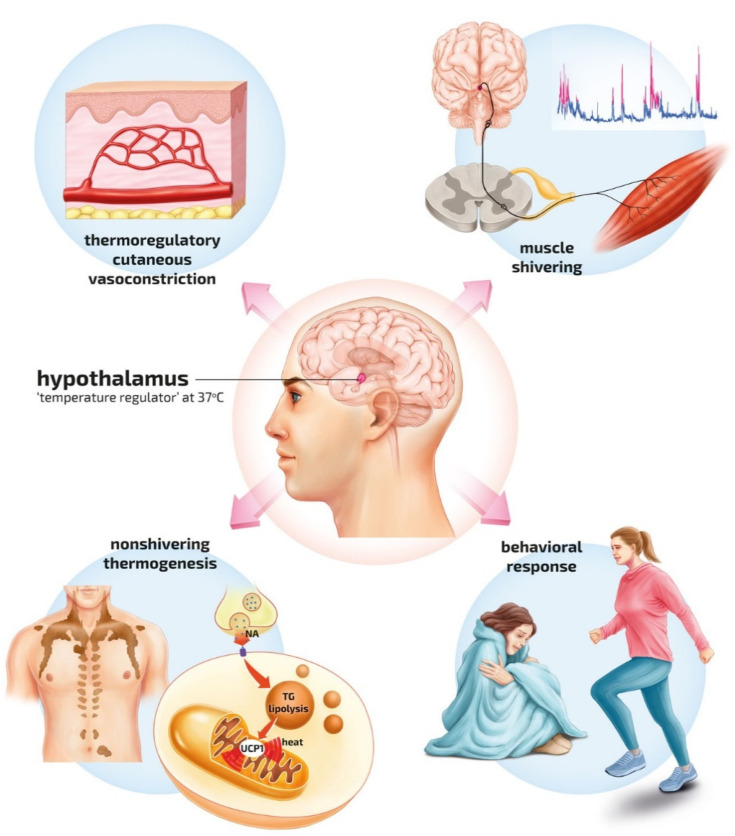
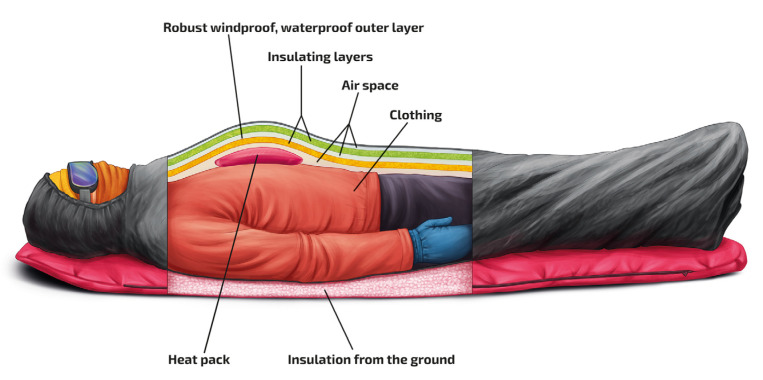
Hypothermia
| Severity | Core Temp | Signs | Treatment |
|---|---|---|---|
| Mild | 32–35°C (90–95°F) | Shivering, confusion, tachycardia | Passive external rewarming (warm blankets, warm environment) |
| Moderate | 28–32°C (82–90°F) | Shivering stops, paradoxical undressing, atrial fibrillation, decreased LOC | Active external rewarming (forced warm air, warm blankets) + warm IV fluids (40–42°C) |
| Severe | < 28°C (82°F) | Unresponsive, VF risk, fixed dilated pupils (do not pronounce dead until warm and dead) | Active internal rewarming: warm IV fluids, warm humidified O2, peritoneal/pleural lavage with warm saline, ECMO for cardiac arrest |
Drowning
Leading cause of unintentional death in children 1–4 years. Primary insult is hypoxia from water aspiration and laryngospasm. All drowning patients who are symptomatic or have any submersion > 1 minute require ED evaluation. Treatment is supportive: supplemental O2, positive-pressure ventilation if needed, intubation for respiratory failure. Monitor for ARDS (may develop 6–24 hours post-submersion). Hypothermia from cold-water submersion may be neuroprotective and is not a reason to terminate resuscitation early. Cervical spine precautions if diving mechanism.
40 Pediatric Emergencies Peds
Febrile Seizures
Most common seizure type in children (2–5% of children aged 6 months to 5 years). Simple febrile seizure: generalized, < 15 minutes, does not recur within 24 hours. Complex: focal, > 15 minutes, or recurrent within 24 hours. Simple febrile seizures are benign — no increased epilepsy risk, no need for LP or EEG in well-appearing children ≥ 12 months with first simple febrile seizure. Treat the fever and reassure parents.
Croup (Laryngotracheobronchitis)
Viral (parainfluenza most common), ages 6 months to 3 years. Presentation: barking "seal-like" cough, inspiratory stridor, hoarseness, worse at night. "Steeple sign" on AP neck X-ray (subglottic narrowing). Treatment: mild (stridor at rest) → dexamethasone 0.6 mg/kg PO/IM (single dose); moderate-severe → nebulized racemic epinephrine (0.5 mL of 2.25% in 3 mL NS) + dexamethasone. Observe ≥ 3–4 hours after racemic epi for rebound.
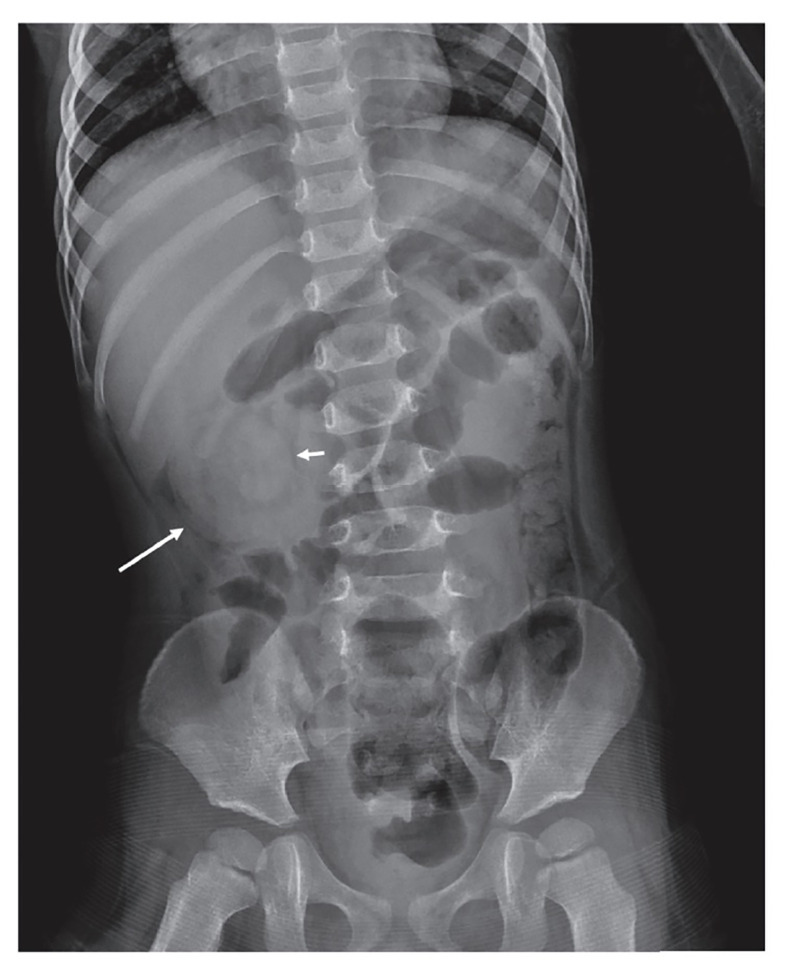
Intussusception
Telescoping of proximal bowel into distal segment. Peak incidence: 6–36 months. Most common cause of bowel obstruction in infants. Classic triad: colicky abdominal pain (intermittent, severe, with drawing up of legs), vomiting, and "currant jelly" stool (bloody mucus — a LATE sign). Palpable "sausage-shaped" mass in RUQ. Diagnosis: ultrasound showing "target sign" or "pseudokidney sign." Treatment: air-contrast or hydrostatic enema (both diagnostic and therapeutic, 80–95% success for reduction). Surgery if enema fails, peritonitis, or perforation.
Non-Accidental Trauma (NAT)
Suspect when: injury inconsistent with developmental stage, changing history, delay in seeking care, multiple injuries at different stages of healing, specific injury patterns (posterior rib fractures, metaphyseal "corner" or "bucket handle" fractures, retinal hemorrhages, patterned bruising/burns). Mandatory reporting is required in all US states when NAT is suspected. Workup: skeletal survey (children < 2 years), head CT, ophthalmologic exam, labs (CBC, CMP, coags, lipase, UA for hematuria).
41 Obstetric Emergencies OB
Ectopic Pregnancy
Implantation outside the uterine cavity (95% in fallopian tube). Risk factors: prior ectopic, PID, tubal surgery, IUD. Presentation: abdominal/pelvic pain + vaginal bleeding + positive pregnancy test. Ruptured ectopic causes acute abdomen with hemoperitoneal shock. Diagnosis: transvaginal ultrasound (absence of IUP with beta-hCG above discriminatory zone, typically ≥1500–2000 mIU/mL) + adnexal mass or free fluid. Treatment: hemodynamically stable + unruptured → methotrexate (50 mg/m² IM single dose) if criteria met (no fetal cardiac activity, mass < 4 cm, beta-hCG < 5000). Ruptured or hemodynamically unstable → emergent salpingectomy.
Eclampsia & Severe Preeclampsia
Preeclampsia: new-onset hypertension (≥140/90 after 20 weeks) + proteinuria or end-organ dysfunction. Severe features: SBP ≥ 160 or DBP ≥ 110, platelets < 100K, elevated liver enzymes (2× normal), renal insufficiency (Cr > 1.1), pulmonary edema, headache/visual disturbances. Eclampsia: seizures in preeclamptic patient. Treatment: magnesium sulfate 4–6 g IV over 20 min (seizure prophylaxis and treatment), then 1–2 g/hr maintenance; antihypertensives (IV labetalol or hydralazine); definitive treatment is delivery.
Perimortem Cesarean Delivery
If a pregnant patient (fundus at or above the umbilicus, roughly ≥ 20 weeks) suffers cardiac arrest and does not have ROSC within 4 minutes of CPR, perimortem C-section should be performed at the bedside. The goal is delivery within 5 minutes of arrest (the "4-minute rule" — decision at 4 min, delivery by 5 min). This is performed to improve maternal resuscitation (relieving aortocaval compression) as much as for fetal survival. The procedure is performed at the patient's current location — do not move to the OR.
42 Psychiatric Emergencies Psych
Suicidal Patient
Risk assessment: SAD PERSONS (Sex, Age, Depression, Previous attempt, Ethanol abuse, Rational thinking loss, Social supports lacking, Organized plan, No spouse, Sickness). High-risk features: specific plan, access to means (especially firearms), active psychosis, recent discharge from psychiatric facility, male > 45, history of prior attempts. Columbia Suicide Severity Rating Scale (C-SSRS) is the standard structured assessment. All patients with active suicidal ideation with plan or intent require psychiatric evaluation and safety precautions (1:1 observation, search for sharps, remove cords/ligatures from room).
Acute Agitation Management
| Approach | Details |
|---|---|
| Verbal de-escalation | First-line always. Calm tone, validate feelings, offer choices, maintain safe distance |
| PO medications (cooperative patient) | Olanzapine 5–10 mg ODT or risperidone 2 mg + lorazepam 2 mg PO |
| IM medications (uncooperative) | "B52": haloperidol 5 mg + lorazepam 2 mg + diphenhydramine 50 mg IM. Alternative: olanzapine 10 mg IM (do NOT combine IM olanzapine with IM benzodiazepine — respiratory depression risk). Ketamine 4 mg/kg IM for severe agitation/excited delirium |
| Physical restraints | Last resort. 4-point leather restraints. Requires physician order, Q15 min checks, neurovascular assessment, offer food/water/toileting q2h. Document ongoing need |
43 Geriatric Emergencies Geri
Elderly patients (≥ 65 years) present atypically: MI without chest pain (dyspnea, confusion), sepsis without fever (hypothermia is a worse prognostic sign), UTI presenting as altered mental status, appendicitis without peritoneal signs. Falls are the leading cause of injury-related death in the elderly. Always consider: medication effects (polypharmacy, anticoagulants), baseline cognitive function (delirium vs. dementia), occult fractures, and disposition challenges (can the patient safely return home?).
Occult Fractures in the Elderly
| Fracture | Presentation | Imaging Pitfall | Next Step |
|---|---|---|---|
| Hip fracture (femoral neck) | Pain with weight bearing, shortened/externally rotated leg | X-ray negative in 2–10% of occult hip fractures | MRI (gold standard) or CT if MRI unavailable |
| C2 (odontoid) fracture | Neck pain after fall, especially if on anticoagulants | Often missed on lateral c-spine X-ray | CT c-spine (not plain films) for elderly trauma patients |
| Vertebral compression fracture | Back pain after fall or spontaneous (osteoporosis) | May be subtle on X-ray | MRI to assess acuity if treatment decisions hinge on it |
| Pelvic rami fractures | Groin/hip pain, difficulty ambulating | Can be subtle on AP pelvis X-ray | CT pelvis for definitive evaluation |
Any elderly patient on anticoagulation (warfarin, DOACs) who falls and strikes their head requires a CT head even if asymptomatic and GCS 15. Delayed intracranial hemorrhage can occur hours later. Consider observation for 6–24 hours or reliable return precautions. Check INR for warfarin patients; reverse anticoagulation if intracranial hemorrhage is identified.
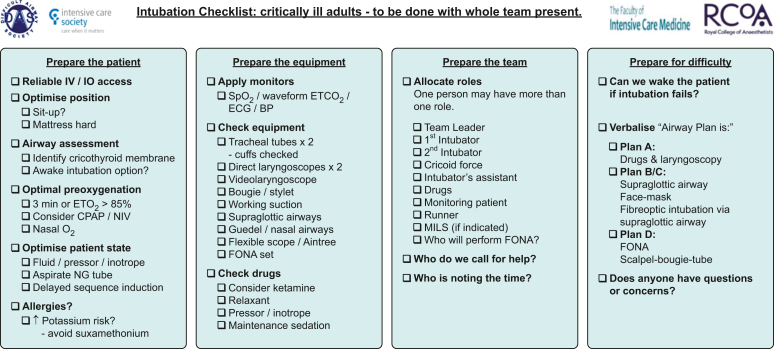
44 Airway Management & RSI Procedures
Rapid Sequence Intubation (RSI)
RSI is the standard of care for emergency intubation in the ED. It involves simultaneous administration of a sedative and neuromuscular blocking agent to facilitate endotracheal intubation while minimizing aspiration risk.
| Phase | Action | Details |
|---|---|---|
| Preparation | Equipment, positioning, preoxygenation | SOAP-ME: Suction, Oxygen, Airway equipment, Pharmacy, Monitoring/End-tidal CO2. Preoxygenate with 100% O2 × 3 min or 8 vital capacity breaths. Position: sniffing/ramped. Apneic oxygenation: 15 L/min NC during attempt |
| Induction | Push sedative | Etomidate 0.3 mg/kg IV (hemodynamically neutral; avoid in sepsis/adrenal insufficiency). Ketamine 1.5–2 mg/kg IV (preferred in hypotension/asthma; does NOT raise ICP in ventilated patients). Propofol 1.5 mg/kg IV (hypotension risk). Midazolam 0.1–0.3 mg/kg (avoid in hypotension) |
| Paralysis | Push neuromuscular blocker | Succinylcholine 1.5 mg/kg IV (onset 45 sec, duration 6–10 min; contraindicated in hyperkalemia, burns >24 hrs, crush >72 hrs, denervation injuries, malignant hyperthermia history). Rocuronium 1.2 mg/kg IV (onset 60 sec, duration 45–60 min; reversible with sugammadex 16 mg/kg) |
| Placement | Intubate | Video laryngoscopy (preferred in most EDs) or direct laryngoscopy. Confirm with continuous waveform capnography (ETCO2) — the gold standard for tube confirmation. Also: bilateral breath sounds, condensation in tube, chest rise, SpO2 |
| Post-intubation | Secure, ventilate, sedate | Secure ETT (tape or commercial holder), CXR for depth (2–4 cm above carina), start sedation (propofol or ketamine infusion + fentanyl) and long-acting paralytic if needed |
Surgical Airway (Cricothyrotomy)
Indicated when intubation and ventilation both fail ("can't intubate, can't oxygenate"). Technique: identify cricothyroid membrane (between thyroid and cricoid cartilages), vertical skin incision, horizontal stab through membrane, insert bougie, railroad a 6.0 cuffed ETT or tracheostomy tube over bougie. Contraindicated in children < 8–10 years (needle cricothyrotomy with jet ventilation instead due to small anatomy).
Non-Invasive Ventilation & High-Flow Nasal Cannula
| Modality | Settings | Best Indications | Contraindications |
|---|---|---|---|
| HFNC (High-Flow Nasal Cannula) | 40–60 L/min, FiO2 titrated, heated/humidified | Hypoxemic respiratory failure, bridge during RSI preoxygenation, post-extubation | Severe facial trauma, complete upper airway obstruction |
| CPAP | 5–15 cmH2O continuous | Pulmonary edema (cardiogenic), obstructive sleep apnea | Vomiting, AMS (aspiration risk), pneumothorax |
| BiPAP | IPAP 10–20 / EPAP 5–10 cmH2O | COPD exacerbation, CHF, obesity hypoventilation, bridge to intubation | Same as CPAP; facial trauma making mask seal impossible |
45 Vascular Access & Chest Procedures Procedures
Vascular Access Hierarchy
| Access Type | Gauge/Size | Flow Rate | When to Use |
|---|---|---|---|
| Peripheral IV (PIV) | 18G (green) or 16G (gray) | ~200–350 mL/min (16G with pressure bag) | First-line; 2 large-bore IVs for trauma/resuscitation |
| Intraosseous (IO) | 15G (EZ-IO drill) | ~80–125 mL/min (pressure infusion) | If IV not obtained within 60–90 sec in critical patient. Sites: proximal tibia (preferred in adults), proximal humerus, distal tibia (pediatric). Can give any medication or fluid including blood products |
| Central venous catheter (CVC) | Triple-lumen 7 Fr | ~70–100 mL/min (distal port) | Vasopressor administration, no peripheral access, CVP monitoring. Sites: IJ (preferred, US-guided), subclavian, femoral. IJ and subclavian carry pneumothorax risk; femoral has highest infection rate |
| Introducer sheath (Cordis) | 8.5 Fr | ~300–500 mL/min | Rapid volume resuscitation (massive hemorrhage); PA catheter introduction |
Chest Tube Insertion
Indications: pneumothorax (traumatic, large spontaneous), hemothorax, empyema, large symptomatic pleural effusion. Technique: safe triangle (bordered by anterior border of latissimus dorsi, lateral border of pectoralis major, line of the 5th intercostal space, apex of the axilla). Position: 4th–5th ICS, anterior to mid-axillary line. Incise skin, blunt dissect through intercostal muscles ABOVE the rib (neurovascular bundle runs below each rib), enter pleural space, finger sweep, insert tube directed posteriorly-superiorly for air or posteriorly-inferiorly for fluid. Tube size: 28–36 Fr for hemothorax, 20–24 Fr for pneumothorax. Connect to closed drainage system (Pleur-Evac) with 20 cmH2O suction. Confirm with CXR.

Needle Decompression
For tension pneumothorax when clinical diagnosis is made (do NOT wait for imaging). Site: 5th ICS, anterior axillary line (preferred over the traditional 2nd ICS midclavicular line due to greater chest wall thickness at the 2nd ICS). Use a 14-gauge angiocatheter, at least 8 cm long. Insert perpendicular to chest wall, above the rib. Rush of air confirms decompression. This is a temporizing measure — follow immediately with chest tube.
46 Wound Management & Procedural Sedation Procedures
Laceration Repair
Assessment: mechanism, contamination, depth (tendon/nerve/vessel/joint involvement?), foreign body, neurovascular status distal to wound, time since injury. Anesthesia: local infiltration with lidocaine 1% (max 4.5 mg/kg without epi, 7 mg/kg with epi) or bupivacaine 0.25% (longer duration). LET gel (lidocaine-epinephrine-tetracaine) for pediatric face/scalp lacerations. Closure: simple interrupted sutures (nylon for skin, absorbable for deep layers), running sutures (rapid closure of clean linear wounds), deep dermal sutures (Vicryl for dead space closure), wound adhesive (2-octyl cyanoacrylate / Dermabond) for clean superficial lacerations, staples for scalp. Suture removal timing: face 3–5 days, scalp 7–10 days, trunk 7–10 days, extremities 10–14 days, joints 14 days.
Procedural Sedation
| Agent | Dose | Onset/Duration | Pros | Cons |
|---|---|---|---|---|
| Propofol | 0.5–1 mg/kg IV, titrate with 0.25–0.5 mg/kg boluses q30–60 sec | 30 sec / 5–10 min | Ultra-short acting, reliable, rapid recovery | Apnea, hypotension, no analgesia (combine with fentanyl) |
| Ketamine | 1–2 mg/kg IV or 4 mg/kg IM | IV: 1 min / 15–30 min; IM: 5 min / 30–60 min | Maintains airway reflexes, bronchodilation, analgesia, hemodynamically stable | Emergence reactions (adults > children; pretreat with midazolam 0.05 mg/kg), laryngospasm (rare), vomiting |
| Etomidate | 0.1–0.15 mg/kg IV | 30 sec / 5–10 min | Hemodynamically neutral | Myoclonus, no analgesia, adrenal suppression |
| Midazolam + Fentanyl | Midazolam 0.05 mg/kg + Fentanyl 1 mcg/kg IV | 2–5 min / 30–60 min | Titratable, reversible (flumazenil/naloxone) | Slower onset/recovery, respiratory depression with combination |
47 Reduction Techniques & Bedside Ultrasound Procedures
Shoulder Dislocation Reduction
Multiple techniques exist; selection depends on patient body habitus, cooperation, and provider experience. External rotation method: patient supine, elbow at 90°, slowly externally rotate the arm (adducted) until relocates. Cunningham technique: patient seated, provider massages biceps, deltoid, and trapezius muscles (no traction). Stimson technique: patient prone, arm hanging off stretcher with 5–10 lb weight; gravity reduces. Traction-countertraction: sheet around patient's chest for countertraction, steady traction on the arm. Pre-reduction X-ray to confirm dislocation and rule out fracture. Post-reduction: neurovascular exam (check axillary nerve), X-ray to confirm reduction, sling × 2–3 weeks, orthopedic follow-up.
Emergency Bedside Ultrasound Applications
| Application | Probe | What You're Looking For |
|---|---|---|
| FAST exam | Curvilinear | Free fluid in RUQ (Morison's), LUQ (splenorenal), pelvis, pericardium |
| Cardiac (focused echo) | Phased array | Pericardial effusion, RV dilation (PE), global LV function, tamponade physiology |
| Lung ultrasound | Linear or curvilinear | Lung sliding (rules out PTX if present), B-lines (pulmonary edema), consolidation (pneumonia), pleural effusion |
| Aorta | Curvilinear | AAA (≥ 3 cm diameter), dissection flap |
| IVC assessment | Curvilinear/phased array | IVC diameter and collapsibility (estimates volume status; IVC < 1 cm with complete collapse = low CVP) |
| Vascular access guidance | Linear | Vessel identification, real-time needle guidance for IJ CVC, peripheral IV, arterial line |
| Soft tissue | Linear | Abscess vs. cellulitis, foreign body, tendon injury |
| Renal/biliary | Curvilinear | Hydronephrosis (renal colic), gallstones, gallbladder wall thickening |
| DVT | Linear | 2-point compression: CFV and popliteal vein. Non-compressible vein = DVT |
| First-trimester pregnancy | Curvilinear (transabdominal) or endocavitary | IUP vs. ectopic; fetal heart rate; free fluid (ruptured ectopic) |
48 Clinical Decision Rules & Scoring Systems
| Rule/Score | Application | Key Thresholds |
|---|---|---|
| HEART Score | Chest pain risk stratification | 0–3: low risk (safe for discharge); 4–6: moderate; 7–10: high (early invasive) |
| Wells PE | PE probability | ≤4: unlikely (D-dimer to rule out); >4: likely (CTA) |
| Wells DVT | DVT probability | ≤1: unlikely (D-dimer); ≥2: likely (compression US) |
| PERC Rule | PE exclusion without D-dimer | All 8 criteria negative in low-risk = PE excluded |
| Ottawa Ankle Rules | Ankle X-ray necessity | X-ray if: unable to bear weight (4 steps) OR bone tenderness at posterior edge/tip of lateral or medial malleolus |
| Ottawa Knee Rules | Knee X-ray necessity | X-ray if: age ≥55, isolated patellar tenderness, fibular head tenderness, inability to flex 90°, inability to bear weight (4 steps) |
| Canadian C-Spine Rule | C-spine imaging | 3-step algorithm as described in Section 23 |
| Canadian CT Head Rule | CT head for minor head injury | High-risk and medium-risk criteria as described in Section 22 |
| GCS | Consciousness level | 13–15: mild; 9–12: moderate; 3–8: severe TBI (intubate) |
| NIHSS | Stroke severity | 0: no deficit; 1–4: minor; 5–15: moderate; 16–20: moderate-severe; 21–42: severe |
| CURB-65 | Pneumonia severity/disposition | 0–1: outpatient; 2: consider admission; 3–5: admit/ICU |
| qSOFA | Sepsis bedside screen | ≥2 of: RR ≥22, AMS, SBP ≤100 |
| Glasgow-Blatchford | UGIB risk | 0–1: outpatient management; ≥6: high risk, likely intervention needed |
| CIWA-Ar | Alcohol withdrawal severity | <10: mild; 10–18: moderate; >18: severe (aggressive treatment) |
| Alvarado (MANTRELS) | Appendicitis probability | ≤4: unlikely; 5–6: equivocal; ≥7: probable |
| Centor/McIsaac | Strep pharyngitis | 0–1: no testing; 2–3: rapid antigen test; 4–5: empiric antibiotics or test |
| PECARN | Pediatric head CT decision | Identifies very low-risk children (<2% bleed risk) who can safely avoid CT |
| Ranson's Criteria | Pancreatitis severity | ≥3 criteria: severe (predicted mortality 15–40%) |
| BISAP | Pancreatitis mortality prediction | ≥3: >20% mortality |
| CHA₂DS₂-VASc | AFib stroke risk (for anticoagulation decision) | ≥2 (men), ≥3 (women): anticoagulate |
| HAS-BLED | Bleeding risk on anticoagulation | ≥3: high risk (does not contraindicate, but requires monitoring) |
49 Medications Master Table Meds
RSI & Airway Medications
| Drug (Brand) | Mechanism | Dose | Indication | Critical Pearl |
|---|---|---|---|---|
| Etomidate (Amidate) | GABA-A agonist | 0.3 mg/kg IV | RSI induction | Hemodynamically neutral; single-dose adrenal suppression clinically insignificant |
| Ketamine (Ketalar) | NMDA antagonist | 1.5–2 mg/kg IV | RSI induction | Preferred in hypotension and asthma; sympathomimetic effect supports BP |
| Propofol (Diprivan) | GABA-A agonist | 1.5 mg/kg IV | RSI induction, sedation | Causes hypotension; use lower doses in elderly/hypovolemic |
| Succinylcholine (Anectine) | Depolarizing NMB | 1.5 mg/kg IV | RSI paralysis | CI: hyperkalemia, burns >24h, denervation, MH history. Fastest onset (45 sec) |
| Rocuronium (Zemuron) | Non-depolarizing NMB | 1.2 mg/kg IV | RSI paralysis | Onset 60 sec at intubating dose. Reversible with sugammadex 16 mg/kg |
Vasopressors & Inotropes
| Drug | Mechanism | Dose Range | Primary Use | Critical Pearl |
|---|---|---|---|---|
| Norepinephrine (Levophed) | α1 >> β1 | 5–50 mcg/min | First-line for septic shock, cardiogenic shock | Central line preferred but can run peripherally short-term via large PIV; titrate to MAP ≥ 65 |
| Epinephrine (Adrenalin) | α1 + β1 + β2 | 1–20 mcg/min | Anaphylaxis, cardiac arrest, refractory septic shock | Increases HR, contractility, and SVR; may cause lactic acidosis at high doses |
| Vasopressin (Pitressin) | V1 receptor agonist | 0.04 units/min (fixed) | Second-line in septic shock | Not titrated; add to norepinephrine, not as replacement |
| Dobutamine (Dobutrex) | β1 > β2 | 5–20 mcg/kg/min | Cardiogenic shock (inotropy) | Can cause hypotension (vasodilation); usually combined with vasopressor |
| Phenylephrine (Neo-Synephrine) | Pure α1 | 40–360 mcg/min | Neurogenic shock, SVT-related hypotension | Pure vasoconstrictor; avoid in cardiogenic shock (increases afterload) |
| Dopamine | Dose-dependent: D1 → β1 → α1 | 5–20 mcg/kg/min | Bradycardia-related hypotension (alternative to transcutaneous pacing) | Higher arrhythmia risk than norepinephrine in septic shock; largely replaced |
Antidotes
| Poison | Antidote | Dose | Key Note |
|---|---|---|---|
| Acetaminophen | N-acetylcysteine (NAC / Acetadote) | 150 mg/kg over 1 hr → 50 mg/kg over 4 hr → 100 mg/kg over 16 hr (IV) | Most effective within 8 hrs; give at any time if indicated |
| Opioids | Naloxone (Narcan) | 0.04–2 mg IV/IM/IN | Start low, titrate to respiratory effort; duration shorter than most opioids → resedation risk |
| Benzodiazepines | Flumazenil (Romazicon) | 0.2 mg IV q1min (max 3 mg) | Rarely used; risk of seizures in chronic benzo users; contraindicated with TCA co-ingestion |
| Organophosphates | Atropine + pralidoxime | Atropine 2–4 mg IV q5min; pralidoxime 1–2 g IV over 30 min | Titrate atropine to drying of secretions; no maximum dose |
| Warfarin (life-threatening bleed) | 4-factor PCC (Kcentra) + Vitamin K | PCC: 25–50 units/kg IV; Vit K 10 mg IV over 10 min | PCC reverses INR within minutes; Vitamin K sustains reversal |
| Dabigatran | Idarucizumab (Praxbind) | 5 g IV (two 2.5 g boluses) | Complete reversal within minutes |
| Xa inhibitors (rivaroxaban, apixaban) | Andexanet alfa (Andexxa) | 400–800 mg IV bolus, then infusion | Expensive; 4-factor PCC 50 units/kg is the practical alternative |
| Beta-blockers / CCBs | Glucagon, high-dose insulin euglycemia (HIE) | Glucagon 3–10 mg IV; Insulin 1 unit/kg bolus + 1 unit/kg/hr + D10W | HIE is first-line for CCB overdose; give with dextrose, monitor glucose and K+ |
| Digoxin | Digoxin-specific Fab (DigiFab) | Based on ingested dose or serum level; empiric 10–20 vials for acute toxicity | For life-threatening arrhythmia or K+ > 5.0 in digoxin toxicity |
| Methanol / Ethylene glycol | Fomepizole (Antizol) | 15 mg/kg IV load, then 10 mg/kg q12h | Blocks alcohol dehydrogenase; also hemodialysis if severe acidosis or level > 50 mg/dL |
| Cyanide | Hydroxocobalamin (Cyanokit) | 5 g IV over 15 min | Suspect in fire/smoke inhalation victims with lactic acidosis + normal SpO2 |
| Carbon monoxide | 100% O2 (hyperbaric if severe) | High-flow 100% O2 via NRB mask | Pulse ox is unreliable (reads falsely normal). Use co-oximetry for COHb level |
Analgesics & Sedatives
| Drug (Brand) | Dose | Route | Duration | Pearl |
|---|---|---|---|---|
| Fentanyl | 0.5–1 mcg/kg | IV | 30–60 min | Preferred in hemodynamic instability; no histamine release |
| Morphine | 0.1 mg/kg (4–8 mg) | IV | 3–4 hrs | Histamine release → hypotension; use with caution in ACS |
| Ketorolac (Toradol) | 15–30 mg | IV/IM | 4–6 hrs | NSAID; avoid in renal impairment, GI bleed risk, anticoagulation |
| Acetaminophen (Ofirmev) | 1 g | IV | 4–6 hrs | Excellent adjunct; reduces opioid requirement by 30% |
| Ketamine (subdissociative) | 0.1–0.3 mg/kg IV or 0.5 mg/kg IN | IV/IN | 15–30 min | Effective for pain; opioid-sparing; minimal respiratory depression |
Common EM Antibiotics
| Drug (Brand) | Dose | Common EM Indication | Key Note |
|---|---|---|---|
| Ceftriaxone (Rocephin) | 1–2 g IV daily | Pneumonia, UTI, meningitis, gonorrhea | Broad gram-negative coverage; do not mix with calcium-containing solutions in neonates |
| Piperacillin-tazobactam (Zosyn) | 3.375–4.5 g IV q6–8h | Sepsis, necrotizing fasciitis, intra-abdominal infection | Broad-spectrum including Pseudomonas and anaerobes |
| Vancomycin | 15–20 mg/kg IV (based on actual body weight) | Sepsis (MRSA), meningitis, severe SSTI | Load with 25–30 mg/kg for critically ill; monitor troughs or AUC/MIC |
| Metronidazole (Flagyl) | 500 mg IV/PO q8h | Intra-abdominal infection (anaerobic), C. diff | Avoid alcohol (disulfiram reaction) |
| Azithromycin (Zithromax) | 500 mg IV/PO × 1 day, then 250 mg × 4 | CAP atypical coverage, STI | QT prolongation risk |
| TMP-SMX (Bactrim DS) | 1–2 DS tabs PO BID | Uncomplicated UTI, MRSA SSTI | Hyperkalemia risk; avoid in pregnancy (folate antagonist) |
50 Abbreviations Master List
General & Resuscitation
Diagnoses
Procedures & Imaging
Medications & Labs
Scoring & Decision Rules
51 Disposition Decision Framework & References
Disposition Decision Framework
Every ED patient requires a disposition decision: discharge home, observe (observation unit), admit to the floor, or admit to the ICU. This decision integrates acuity, diagnosis, clinical trajectory, and patient factors.
| Disposition | Criteria | Examples |
|---|---|---|
| Discharge | Diagnosis benign or treatable as outpatient; vital signs stable; pain controlled; able to tolerate PO; reliable follow-up; safe home environment | Simple laceration, sprained ankle, uncomplicated UTI, low-risk chest pain (HEART 0–3) |
| Observation (23-hr) | Diagnosis uncertain; need serial assessments or short-interval testing; not clearly requiring inpatient admission | Chest pain rule-out (serial troponins), TIA workup, syncope with moderate-risk features, mild CHF responding to diuretics |
| Floor admission | Diagnosis requiring inpatient treatment; IV medications, serial monitoring, or procedures needed | Pneumonia requiring IV antibiotics, SBO with NGT, pyelonephritis, new AFib requiring rate control |
| ICU admission | Hemodynamic instability, respiratory failure, continuous infusions (vasopressors, antiarrhythmics), need for invasive monitoring, high risk for rapid deterioration | Septic shock, intubated patients, STEMI post-cath, massive PE, status epilepticus, DKA with pH < 7.1 |