Family Medicine
Every diagnosis, screening guideline, medication, procedure, classification system, immunization schedule, and management strategy across the full lifespan — in one place.
01 Scope of Family Medicine
Family medicine is the only specialty defined by breadth rather than organ system, disease category, or patient age. A family physician manages undifferentiated illness across the entire lifespan — newborn through geriatric — in ambulatory, inpatient, and procedural settings. The scope includes preventive care and screening, chronic disease management (hypertension, diabetes, dyslipidemia, COPD, heart failure), acute care (infections, injuries, abdominal pain), mental and behavioral health (depression, anxiety, ADHD, substance use), musculoskeletal medicine, women's health (contraception, prenatal, menopause), pediatrics, geriatrics, dermatology, and office-based procedures. Family physicians provide approximately 200 million office visits annually in the United States — more than any other specialty.
The intellectual core of the specialty is the biopsychosocial model: disease is never purely biomedical. Social determinants (housing, food security, employment, insurance status), behavioral factors (tobacco, alcohol, physical activity, sleep), and psychological context (stress, trauma, family dynamics) are as clinically relevant as lab values. A comprehensive family medicine encounter integrates all three domains into every clinical decision.
The Four Pillars of Family Medicine Practice
| Pillar | Scope | Key Activities |
|---|---|---|
| Preventive Care | All ages — birth to death | Immunizations, cancer screening (USPSTF), cardiovascular risk assessment (ASCVD), well-child visits, annual wellness visits, counseling |
| Chronic Disease | Primarily adult, increasing in adolescents | Hypertension, DM2, dyslipidemia, COPD, asthma, CHF, CKD, thyroid disease, obesity — titrating medications, monitoring targets, preventing complications |
| Acute/Episodic Care | All ages | URI, UTI, otitis, pharyngitis, skin infections, lacerations, fractures, abdominal pain triage, chest pain risk stratification |
| Behavioral Health | All ages | Depression, anxiety, ADHD, insomnia, substance use disorders, motivational interviewing, medication management, brief counseling |
02 The Comprehensive Physical Exam
The family medicine physical exam adapts to context — a focused exam for an acute sore throat is fundamentally different from a comprehensive annual wellness exam. However, every family physician must be able to perform a complete head-to-toe examination and know the specific findings that trigger further workup or referral.
Vital Signs — The Fifth Vital Sign
| Vital Sign | Normal Adult Range | Critical Thresholds | Clinical Pearl |
|---|---|---|---|
| Blood Pressure | < 120/80 mmHg | Elevated: 120-129/<80; Stage 1 HTN: 130-139/80-89; Stage 2: ≥140/90; Crisis: >180/120 | Confirm with repeated measurements on 2 separate occasions; use correct cuff size (bladder covers 80% of arm circumference) |
| Heart Rate | 60-100 bpm | Bradycardia <60; tachycardia >100; concern >150 at rest | Irregularly irregular = atrial fibrillation until proven otherwise |
| Respiratory Rate | 12-20/min | Tachypnea >20; bradypnea <12 | Count for a full 30 seconds; most commonly miscounted vital sign |
| Temperature | 36.1-37.2 °C (97-99 °F) | Fever ≥38.0 °C (100.4 °F); hypothermia <35 °C | Elderly patients may be afebrile despite serious infection |
| O2 Saturation | 95-100% | <92% on room air warrants urgent evaluation; COPD patients may have lower baselines (88-92%) | Falsely normal in CO poisoning; falsely low with nail polish, poor perfusion, or dark skin pigmentation |
| Pain (0-10) | 0 | Functional impairment threshold varies; trend matters more than single number | Use age-appropriate scales: Wong-Baker FACES for children 3-7, numeric for adults |
BMI Classification
| BMI (kg/m²) | Category | Clinical Implication |
|---|---|---|
| < 18.5 | Underweight | Screen for eating disorders, malnutrition, malignancy, hyperthyroidism |
| 18.5-24.9 | Normal | Standard risk |
| 25.0-29.9 | Overweight | Lifestyle counseling; screen for metabolic syndrome |
| 30.0-34.9 | Obesity Class I | Intensive behavioral intervention; consider pharmacotherapy |
| 35.0-39.9 | Obesity Class II | Pharmacotherapy + behavioral; bariatric surgery if comorbidities present |
| ≥ 40.0 | Obesity Class III (severe) | Bariatric surgery evaluation; high risk for OSA, DM2, CVD |
Exam by System — Key Findings That Change Management
HEENT: Conjunctival pallor (anemia), scleral icterus (liver disease), thyromegaly or nodules (palpate with patient swallowing water — nodules >1 cm need ultrasound), tympanic membrane (red/bulging = AOM; retracted/dull = effusion; perforation), oropharynx (tonsillar exudate + fever + anterior cervical LAD + absence of cough = Centor 3-4, consider rapid strep).
Cardiovascular: Murmur grading (I-VI scale; grade III+ or any diastolic murmur warrants echocardiogram), irregular rhythm (ECG to rule out AFib), JVD (right heart failure), carotid bruits (consider duplex ultrasound if symptomatic or high cardiovascular risk), peripheral edema grading (1+ to 4+).
Pulmonary: Wheezes (asthma, COPD, heart failure), crackles (pneumonia, pulmonary fibrosis, CHF), decreased breath sounds (effusion, pneumothorax), prolonged expiratory phase (obstruction). Assess respiratory effort, accessory muscle use, and ability to speak in full sentences.
Abdomen: Auscultate before palpation. Rebound tenderness and involuntary guarding = peritoneal irritation, requires urgent imaging. Murphy's sign (RUQ pain with inspiration during palpation = cholecystitis). McBurney's point tenderness (RLQ = appendicitis). Costovertebral angle tenderness (pyelonephritis). Hepatosplenomegaly requires workup.
Musculoskeletal: Range of motion testing (active then passive — pain with active but not passive = soft tissue; pain with both = intra-articular). Straight leg raise (radiculopathy: positive if reproduces leg pain at <60°). Drawer tests (ACL/PCL), McMurray's (meniscus), Phalen's/Tinel's (carpal tunnel).
Neurological: Cranial nerves II-XII, strength (0-5 scale), sensation (light touch, pinprick), deep tendon reflexes (0-4+ scale; 2+ = normal), cerebellar function (finger-to-nose, heel-to-shin, Romberg). Mini-Mental State Exam (MMSE) or Montreal Cognitive Assessment (MoCA) for cognitive screening in geriatric patients.
03 Preventive Medicine Framework
Preventive care is the defining activity of family medicine. The US Preventive Services Task Force (USPSTF) issues evidence-graded recommendations (A, B, C, D, I) that drive screening and counseling decisions. Grade A/B recommendations are standard of care — most insurers cover them with no patient cost-sharing under the ACA. The USPSTF recommendation framework uses net benefit analysis: benefits of the intervention minus harms (false positives, overdiagnosis, procedural complications).
Core Screening Schedule — Adults
| Condition | Test | Population | Frequency | USPSTF Grade |
|---|---|---|---|---|
| Hypertension | Office BP measurement | Adults ≥18 | Annual (or every 3-5 years if normal and <40) | A |
| Diabetes (Type 2) | Fasting glucose, A1C, or OGTT | Adults 35-70 with overweight/obesity | Every 3 years if normal | B |
| Dyslipidemia | Lipid panel | Men ≥35, women ≥45 (earlier if risk factors) | Every 5 years; more often if borderline or on therapy | A/B |
| Colorectal cancer | Colonoscopy, FIT, Cologuard, flex sig, CT colonography | Adults 45-75 | Colonoscopy q10yr, FIT annually, Cologuard q1-3yr | A |
| Breast cancer | Mammography | Women 40-74 | Biennial (may be annual based on shared decision-making) | B |
| Cervical cancer | Pap smear ± HPV co-testing | Women 21-65 | Pap q3yr (21-29); Pap+HPV q5yr or Pap q3yr (30-65) | A |
| Lung cancer | Low-dose CT chest | Adults 50-80 with ≥20 pack-year hx, current or quit <15yr | Annual | B |
| AAA | Abdominal ultrasound | Men 65-75 who ever smoked | One-time screening | B |
| Osteoporosis | DEXA scan | Women ≥65; postmenopausal <65 with risk factors | Every 2 years if on therapy or high risk | B |
| Depression | PHQ-2/PHQ-9 | All adults ≥18 | Annual or as indicated | B |
| Hepatitis C | Anti-HCV antibody | All adults 18-79 | One-time screening | B |
| HIV | HIV 1/2 Ag/Ab | All adults 15-65 | At least once; more if high risk | A |
Cardiovascular Risk Assessment
The Pooled Cohort Equations (PCE) estimate 10-year ASCVD risk using age, sex, race, total cholesterol, HDL, systolic BP, BP treatment status, diabetes, and smoking. Risk categories: low (<5%), borderline (5-7.4%), intermediate (7.5-19.9%), high (≥20%). The PCE drives statin initiation decisions per 2018 AHA/ACC cholesterol guidelines: high-intensity statin for ASCVD risk ≥20% or known ASCVD; moderate-intensity statin for 7.5-19.9% with risk enhancers; shared decision-making for 5-7.4%.
04 Hypertension Chronic
Hypertension affects 47% of US adults (~116 million) and is the leading modifiable risk factor for stroke, MI, heart failure, CKD, and aortic dissection. The 2017 ACC/AHA guidelines lowered the diagnostic threshold from 140/90 to 130/80 mmHg, instantly reclassifying ~31 million Americans as hypertensive.
Classification (2017 ACC/AHA)
| Category | Systolic (mmHg) | Diastolic (mmHg) | Management |
|---|---|---|---|
| Normal | <120 | <80 | Reassess annually |
| Elevated | 120-129 | <80 | Lifestyle modification; reassess in 3-6 months |
| Stage 1 HTN | 130-139 | 80-89 | Lifestyle + pharmacotherapy if 10-yr ASCVD risk ≥10% or known CVD/DM/CKD |
| Stage 2 HTN | ≥140 | ≥90 | Lifestyle + pharmacotherapy (two-drug combination if BP ≥20/10 above goal) |
| Hypertensive Crisis | >180 | >120 | Urgency (no end-organ damage): oral meds, recheck in hours. Emergency (end-organ damage): IV meds, ICU |
First-Line Antihypertensives
| Class | Examples (Generic/Brand) | Mechanism | Preferred When | Pearl |
|---|---|---|---|---|
| ACE Inhibitor | Lisinopril (Prinivil, Zestril), enalapril (Vasotec), ramipril (Altace) | Blocks ACE → ↓ angiotensin II → vasodilation + ↓ aldosterone | DM with proteinuria, CKD, HF with reduced EF, post-MI | Dry cough in 10-20%; angioedema rare but life-threatening; check K+ and Cr at 1-2 weeks; contraindicated in pregnancy |
| ARB | Losartan (Cozaar), valsartan (Diovan), olmesartan (Benicar) | Blocks AT1 receptor → same downstream effects as ACEI without cough | ACEI-intolerant (cough), same indications as ACEI | Never combine ARB + ACEI (ONTARGET trial: no benefit, more harm); check K+ and Cr |
| CCB (dihydropyridine) | Amlodipine (Norvasc), nifedipine ER (Procardia XL) | Blocks L-type Ca2+ channels in vascular smooth muscle → vasodilation | Black patients, elderly, angina, Raynaud's; no metabolic effects | Peripheral edema is dose-dependent (up to 30% at 10 mg); adding ACEI/ARB reduces edema |
| Thiazide/Thiazide-like | Chlorthalidone 12.5-25 mg, hydrochlorothiazide (HCTZ) 25 mg, indapamide 1.25-2.5 mg | Inhibits NaCl cotransporter in DCT → ↓ intravascular volume, then sustained vasodilation | Black patients, elderly, osteoporosis (preserves bone Ca2+); first-line per ALLHAT | Chlorthalidone is more potent and longer-acting than HCTZ; monitor K+, Na+, uric acid, glucose |
Resistant Hypertension
Defined as BP above goal despite 3 optimally dosed antihypertensives from different classes, one of which is a diuretic — or BP controlled on 4+ drugs. Prevalence: 10-15% of treated hypertensives. Workup: confirm adherence (pill counts, pharmacy fills), rule out white-coat HTN (24-hr ABPM or home BP monitoring), evaluate for secondary causes: primary aldosteronism (aldosterone/renin ratio >30 with aldosterone >15 ng/dL), renal artery stenosis (renal duplex or CTA), pheochromocytoma (24-hr urine metanephrines/catecholamines), obstructive sleep apnea (most common secondary cause — screen with Epworth or STOP-BANG), Cushing's syndrome (24-hr urine cortisol, overnight dexamethasone suppression). Fourth-line agent: spironolactone 25-50 mg daily (PATHWAY-2 trial: most effective add-on for resistant HTN).
05 Diabetes Mellitus Chronic
Type 2 diabetes mellitus (T2DM) affects 37 million Americans (~11% of the population). It is the leading cause of CKD, non-traumatic lower extremity amputation, and adult-onset blindness. Family physicians manage the majority of T2DM in the US. The ADA Standards of Care (2024) define diagnosis and management targets.
Diagnostic Criteria
| Test | Normal | Prediabetes | Diabetes |
|---|---|---|---|
| Fasting Plasma Glucose | <100 mg/dL | 100-125 mg/dL (IFG) | ≥126 mg/dL |
| 2-hr OGTT (75g) | <140 mg/dL | 140-199 mg/dL (IGT) | ≥200 mg/dL |
| A1C | <5.7% | 5.7-6.4% | ≥6.5% |
| Random Glucose + Symptoms | — | — | ≥200 mg/dL with polyuria, polydipsia, weight loss |
Two abnormal tests are required for diagnosis in asymptomatic patients. A random glucose ≥200 with classic symptoms is diagnostic on a single test.
Pharmacotherapy — Stepwise Approach
| Agent (Generic/Brand) | Mechanism | A1C Reduction | Key Benefit | Pearl |
|---|---|---|---|---|
| Metformin (Glucophage) 500-2000 mg/day | Decreases hepatic glucose production, increases insulin sensitivity | 1.0-1.5% | First-line; weight-neutral; inexpensive; possible CV benefit | Hold if eGFR <30; risk of lactic acidosis overstated; GI side effects minimized with ER formulation; hold 48hr before iodinated contrast if eGFR <45 |
| GLP-1 RA: semaglutide (Ozempic 0.25-2 mg/wk, Wegovy), liraglutide (Victoza 0.6-1.8 mg/day), dulaglutide (Trulicity) | Incretin mimetic → glucose-dependent insulin secretion, ↓ glucagon, delays gastric emptying, ↓ appetite | 1.0-1.8% | Weight loss (5-15%), CV mortality reduction (LEADER, SUSTAIN-6, SELECT trials) | Contraindicated with personal/family hx of medullary thyroid cancer or MEN2; nausea common at initiation — start low, titrate slowly |
| SGLT2i: empagliflozin (Jardiance 10-25 mg), dapagliflozin (Farxiga 5-10 mg), canagliflozin (Invokana) | Blocks glucose reabsorption in proximal tubule → glycosuria, natriuresis | 0.5-0.9% | CV death reduction (EMPA-REG), HF hospitalization reduction, CKD progression slowed (CREDENCE, DAPA-CKD) | Risk of genital mycotic infections (candidal); euglycemic DKA (rare, suspect in ill patient on SGLT2i); hold perioperatively |
| Sulfonylureas: glipizide (Glucotrol 5-20 mg), glimepiride (Amaryl 1-4 mg) | Stimulates pancreatic beta-cell insulin secretion (ATP-sensitive K+ channels) | 1.0-1.5% | Rapid onset, inexpensive | Hypoglycemia risk (especially glyburide — avoid); weight gain; avoid in CKD (accumulation) |
| DPP-4i: sitagliptin (Januvia 100 mg), linagliptin (Tradjenta 5 mg) | Inhibits DPP-4 → prolongs endogenous GLP-1/GIP | 0.5-0.8% | Weight-neutral, well-tolerated, oral | No CV benefit; less effective than GLP-1 RA; do not combine with GLP-1 RA (redundant mechanism) |
| Insulin: basal (glargine/Lantus, detemir/Levemir, degludec/Tresiba), prandial (lispro/Humalog, aspart/NovoLog) | Exogenous insulin replacement | 1.5-3.5% | Most potent glucose lowering; essential for T1DM and late-stage T2DM | Start basal 10 units or 0.1-0.2 U/kg/day; titrate by 2 units q3 days to fasting glucose target; hypoglycemia and weight gain are dose-limiting |
Step 1: Metformin + lifestyle for all T2DM. Step 2: If established ASCVD or high CV risk → add GLP-1 RA (with proven CV benefit) or SGLT2i. If HF or CKD → add SGLT2i (preferred) or GLP-1 RA. If neither → add agent based on need to minimize hypoglycemia (GLP-1 RA, SGLT2i, DPP-4i), need for weight loss (GLP-1 RA, SGLT2i), or cost (sulfonylurea, TZD). Step 3: Add basal insulin if A1C remains above target after dual/triple oral/injectable therapy. A1C target: <7% for most adults; <6.5% if safe and achievable for younger patients; <8% for frail elderly, limited life expectancy, or history of severe hypoglycemia.
Monitoring & Complications Screening
A1C: Every 3 months if not at goal, every 6 months if stable. Annual foot exam: Semmes-Weinstein 10g monofilament + vibration (128 Hz tuning fork) to screen for peripheral neuropathy; inspect for ulcers, deformity, calluses. Annual eye exam: Dilated fundoscopy or retinal photography for diabetic retinopathy (DR stages: none, mild NPDR, moderate NPDR, severe NPDR, PDR). Urine albumin-to-creatinine ratio (UACR): Annual; microalbuminuria = 30-300 mg/g, macroalbuminuria >300 mg/g — start ACEi/ARB. Lipids: High-intensity statin for all diabetics 40-75; moderate-intensity for <40 with risk factors.
06 Dyslipidemia Chronic
Dyslipidemia — elevated LDL-C, low HDL-C, or elevated triglycerides — is a primary driver of atherosclerotic cardiovascular disease. LDL-C is the primary therapeutic target. The 2018 AHA/ACC cholesterol guidelines shifted management from treating to a numeric LDL target toward a risk-based statin intensity approach, though LDL thresholds still guide escalation.
Statin Intensity
| Intensity | Expected LDL Reduction | Agents |
|---|---|---|
| High | ≥50% | Atorvastatin 40-80 mg; rosuvastatin 20-40 mg |
| Moderate | 30-49% | Atorvastatin 10-20 mg; rosuvastatin 5-10 mg; simvastatin 20-40 mg; pravastatin 40-80 mg |
| Low | <30% | Simvastatin 10 mg; pravastatin 10-20 mg; lovastatin 20 mg |
Who Gets a Statin?
Four statin benefit groups: (1) Clinical ASCVD (MI, stroke, PAD) → high-intensity. (2) LDL ≥190 mg/dL (familial hypercholesterolemia) → high-intensity. (3) Diabetes age 40-75 → moderate-intensity; high-intensity if multiple risk factors or 10-yr ASCVD ≥20%. (4) 10-yr ASCVD risk ≥7.5% age 40-75 → moderate-to-high intensity. For ASCVD patients not at LDL goal (<70 mg/dL), add ezetimibe (Zetia) 10 mg, then PCSK9 inhibitor (evolocumab/Repatha 140 mg q2wk or alirocumab/Praluent 75-150 mg q2wk) if still above target.
Hypertriglyceridemia
Triglycerides ≥500 mg/dL carry risk of acute pancreatitis — treat with fibrate (fenofibrate/Tricor 145 mg daily), omega-3 fatty acids (icosapent ethyl/Vascepa 2g BID — the REDUCE-IT trial showed 25% CV risk reduction), or niacin. For moderate hypertriglyceridemia (150-499), optimize lifestyle (weight loss, reduce refined carbs/alcohol, exercise) and treat underlying causes (uncontrolled DM, hypothyroidism, medications like thiazides, beta-blockers, estrogens, retinoids).
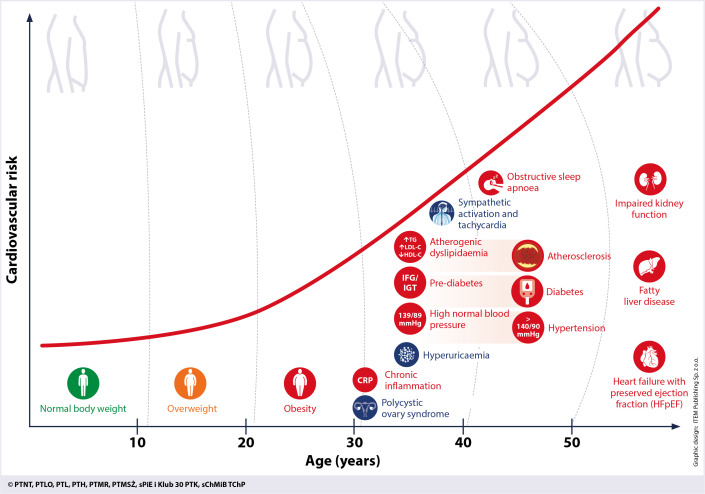
07 Obesity & Metabolic Syndrome Chronic
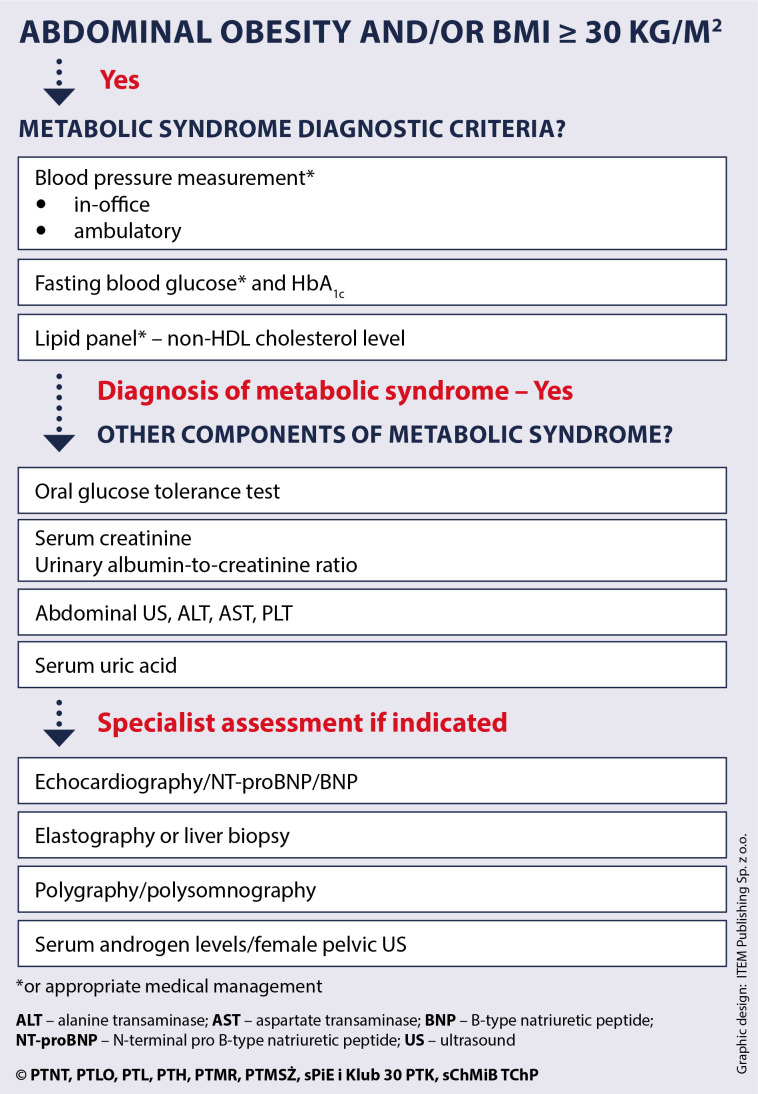
Obesity (BMI ≥30) affects 42% of US adults and is the strongest modifiable risk factor for T2DM, OSA, NAFLD, OA, and multiple cancers (endometrial, breast, colon). Metabolic syndrome — a cluster of insulin resistance-driven findings — is present in ~35% of adults.
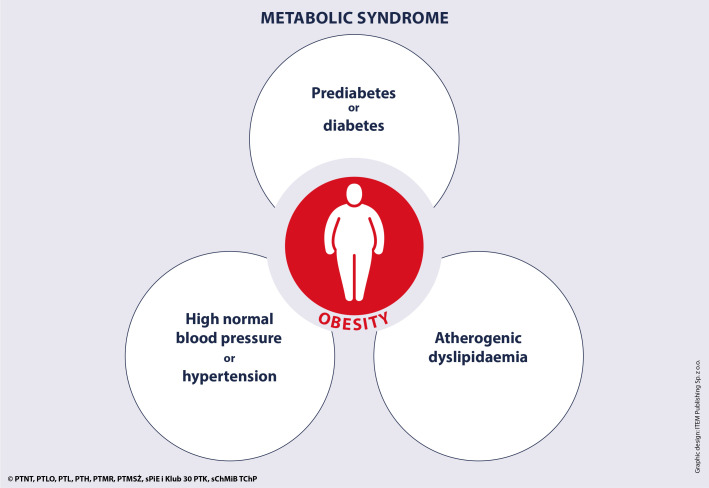
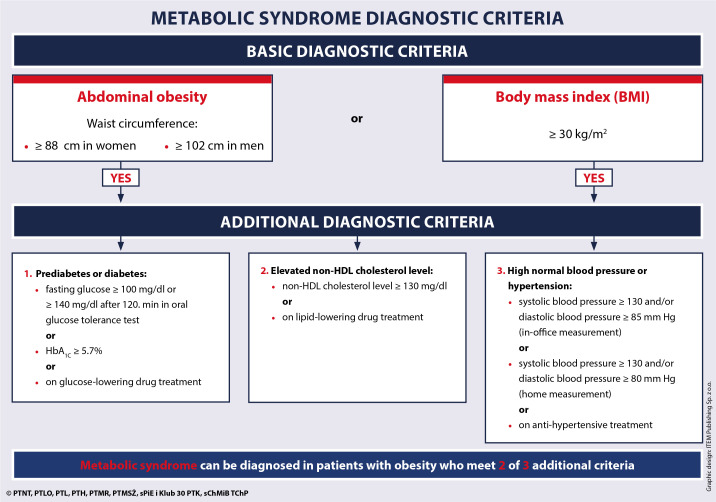
Metabolic Syndrome Criteria (ATP III / IDF Harmonized)
Three of five required: (1) Waist circumference ≥102 cm (40 in) in men or ≥88 cm (35 in) in women. (2) Triglycerides ≥150 mg/dL or on treatment. (3) HDL <40 mg/dL in men or <50 mg/dL in women. (4) BP ≥130/85 or on treatment. (5) Fasting glucose ≥100 mg/dL or on treatment. Metabolic syndrome doubles the risk of CVD and quintuples the risk of T2DM.
Anti-Obesity Medications
| Agent (Generic/Brand) | Mechanism | Expected Weight Loss | Key Considerations |
|---|---|---|---|
| Semaglutide 2.4 mg/wk (Wegovy) | GLP-1 RA → appetite suppression, delayed gastric emptying | ~15% total body weight (STEP trials) | Nausea, vomiting at initiation; titrate over 16 weeks; pancreatitis risk; CI in MTC/MEN2 |
| Tirzepatide 5-15 mg/wk (Zepbound) | Dual GIP/GLP-1 RA | ~20% total body weight (SURMOUNT trials) | Currently highest efficacy; similar GI side effects; titrate over 20 weeks |
| Phentermine-topiramate ER (Qsymia) | Sympathomimetic + anticonvulsant → appetite suppression | ~10% | Contraindicated in pregnancy (topiramate is teratogenic), uncontrolled HTN, hyperthyroidism, glaucoma |
| Naltrexone-bupropion (Contrave) | Opioid antagonist + dopamine/NE reuptake inhibitor → hypothalamic appetite regulation | ~5-6% | Useful if concurrent depression or tobacco use; CI with opioid use, seizure history |
| Orlistat (Xenical/Alli OTC) | Pancreatic lipase inhibitor → ↓ fat absorption by 30% | ~3-5% | GI side effects (steatorrhea, fecal urgency); supplement fat-soluble vitamins (A, D, E, K) |
Bariatric surgery: Indicated for BMI ≥40, or BMI ≥35 with obesity-related comorbidities (DM2, OSA, HTN). Options: Roux-en-Y gastric bypass (RYGB, 25-30% weight loss, best DM2 remission), sleeve gastrectomy (most common, 20-25% weight loss), adjustable gastric banding (declining due to complications). Long-term nutritional monitoring required: B12, iron, calcium, vitamin D, folate.
08 Chronic Pain Management Chronic
Chronic pain (lasting >3 months) affects ~50 million US adults. Family physicians prescribe the majority of chronic pain medications and must balance adequate analgesia with opioid risk. The CDC Clinical Practice Guideline for Prescribing Opioids (2022) updated the 2016 guideline with more flexible language but maintained the principle: non-opioid therapy is preferred for chronic non-cancer pain.
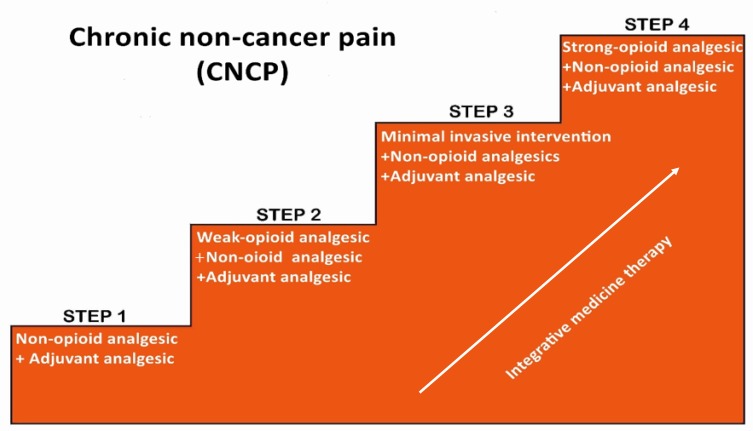
WHO Analgesic Ladder (Adapted for Primary Care)
| Step | Agent | Indication | Pearl |
|---|---|---|---|
| 1 — Non-opioid | Acetaminophen (Tylenol) 500-1000 mg q6-8h (max 3g/day); NSAIDs: ibuprofen 400-800 mg q6-8h, naproxen 250-500 mg q12h, meloxicam 7.5-15 mg daily | Mild-moderate pain; OA, headache, musculoskeletal | NSAIDs: GI bleed risk (add PPI if >65, on ASA, or hx of GI bleed); renal toxicity with chronic use; CV risk with long-term use. Acetaminophen: hepatotoxicity >3g/day |
| 2 — Adjuvant | Duloxetine (Cymbalta) 30-60 mg/day; gabapentin 300-3600 mg/day; pregabalin (Lyrica) 75-300 mg BID; TCAs: amitriptyline 10-75 mg qhs, nortriptyline 10-75 mg qhs | Neuropathic pain, fibromyalgia, chronic musculoskeletal pain | Duloxetine is FDA-approved for DPN, fibromyalgia, chronic musculoskeletal pain, and depression — treats pain + mood. Gabapentin: sedation, dizziness; taper to discontinue |
| 3 — Weak opioid | Tramadol (Ultram) 50-100 mg q4-6h (max 400 mg/day) | Moderate pain refractory to steps 1-2 | Seizure risk (especially with SSRIs/SNRIs — serotonin syndrome); lowers seizure threshold; still carries opioid risks (dependence, respiratory depression) |
| 4 — Strong opioid | Oxycodone, hydrocodone, morphine — lowest effective dose for shortest duration | Severe pain or pain refractory to non-opioid approaches after shared decision-making | Check PDMP before every prescription; urine drug screen at baseline and periodically; naloxone co-prescribing if ≥50 MME/day or concurrent benzodiazepines |
For patients on chronic opioid therapy: (1) Written treatment agreement/informed consent. (2) Check state PDMP at each refill. (3) Urine drug screen at baseline, then at least annually. (4) Calculate morphine milligram equivalents (MME): ≥50 MME/day = increased overdose risk; ≥90 MME/day = avoid or justify carefully. (5) Co-prescribe naloxone (Narcan) 4 mg nasal spray if ≥50 MME, concurrent benzodiazepines, hx of overdose, or substance use disorder. (6) Avoid concurrent benzodiazepines — combination increases overdose death risk 10-fold. (7) Reassess function, not just pain score — is the patient doing more, not just hurting less?
09 Upper Respiratory Infections & Sinusitis Acute
URIs are the most common reason for ambulatory visits in the US (~500 million/year). The vast majority are viral (rhinovirus, coronavirus, RSV, influenza, parainfluenza, adenovirus). Inappropriate antibiotic prescribing for viral URIs is the single largest driver of antibiotic resistance in the community. Only 0.5-2% of URIs are complicated by bacterial sinusitis.
Acute Bacterial Rhinosinusitis — Diagnostic Criteria
Antibiotics are appropriate ONLY when clinical criteria suggest bacterial infection. Three patterns qualify: (1) Persistent symptoms ≥10 days without improvement (nasal discharge, facial pain/pressure, cough). (2) Severe onset: high fever (≥39°C/102°F) + purulent nasal discharge for ≥3 consecutive days. (3) Double-worsening: symptoms initially improve then worsen again (new fever, increased discharge, headache) around day 5-6. Imaging is NOT recommended for uncomplicated acute sinusitis — clinical diagnosis only.
Treatment
Viral URI: Supportive only — analgesics (acetaminophen, ibuprofen), nasal saline irrigation, honey for cough (age >1 year), dextromethorphan (minimal evidence but commonly used), pseudoephedrine or oxymetazoline nasal spray ≤3 days (rhinitis medicamentosa risk with prolonged use). Antibiotics provide zero benefit and should NOT be prescribed.
Acute bacterial sinusitis (first-line): Amoxicillin-clavulanate (Augmentin) 875/125 mg BID × 5-7 days (standard) or 2000/125 mg BID if risk factors for resistance (recent antibiotics, daycare, region with >10% PRP). Alternatives for penicillin allergy: doxycycline 100 mg BID × 5-7 days, or respiratory fluoroquinolone (levofloxacin 500 mg daily — reserve for true beta-lactam allergy). Watchful waiting for 7 days with analgesics is a valid option for mild bacterial sinusitis per IDSA guidelines.
10 Otitis & Pharyngitis Acute
Acute Otitis Media (AOM)
Most common bacterial infection in children. Diagnosis requires: (1) acute onset of symptoms (ear pain, irritability, fever), (2) middle ear effusion (bulging TM, limited mobility on pneumatic otoscopy, air-fluid level), AND (3) signs of middle ear inflammation (erythema of TM, otalgia). A red TM alone is NOT diagnostic — crying makes the TM red.
| Scenario | Management |
|---|---|
| Age ≥2, unilateral, non-severe | Observation option: analgesics × 48-72 hr; prescribe antibiotics if no improvement (safety-net prescription) |
| Age ≥2, bilateral or severe (fever ≥39°C, severe otalgia, >48 hr symptoms) | Amoxicillin 80-90 mg/kg/day divided BID × 10 days (age <2) or 5-7 days (age ≥2) |
| Age 6-23 months, unilateral, non-severe | May observe with close follow-up OR treat |
| Age <6 months | Always treat: amoxicillin 80-90 mg/kg/day |
| Treatment failure at 48-72 hr | Amoxicillin-clavulanate 90/6.4 mg/kg/day; or ceftriaxone 50 mg/kg IM × 3 days |
Pharyngitis — Centor / McIsaac Criteria
| Criterion | Points |
|---|---|
| Tonsillar exudate or swelling | +1 |
| Tender anterior cervical lymphadenopathy | +1 |
| Fever (subjective or ≥38°C) | +1 |
| Absence of cough | +1 |
| Age 3-14 | +1 |
| Age 15-44 | 0 |
| Age ≥45 | −1 |
Score 0-1: No testing needed, symptomatic care. Score 2-3: Rapid antigen detection test (RADT); treat if positive. Score 4-5: RADT or empiric treatment. For children/adolescents, a negative RADT should be confirmed with throat culture (RADT sensitivity ~85-90%, culture is gold standard). Treatment: penicillin V 500 mg BID × 10 days or amoxicillin 500 mg BID × 10 days; single-dose IM benzathine penicillin G 1.2 million units if adherence is a concern. Goal: prevent acute rheumatic fever (requires treatment within 9 days of symptom onset).
11 Urinary Tract Infections Acute
UTIs are the second most common infection seen in primary care. Uncomplicated cystitis occurs almost exclusively in premenopausal, non-pregnant women. Complicated UTI includes: male patients, pregnant patients, catheterized patients, anatomic abnormalities, immunosuppression, and concurrent pyelonephritis.
Uncomplicated Cystitis — Treatment
| Agent | Dose | Duration | Notes |
|---|---|---|---|
| Nitrofurantoin (Macrobid) | 100 mg BID | 5 days | First-line; avoid if eGFR <30; covers E. coli but NOT Proteus or Pseudomonas |
| TMP-SMX (Bactrim DS) | 160/800 mg BID | 3 days | First-line if local resistance <20%; avoid in third trimester (kernicterus risk); check sulfa allergy |
| Fosfomycin (Monurol) | 3 g single dose | 1 dose | Convenient but slightly less effective; useful for ESBL-producing organisms |
| Fluoroquinolone (ciprofloxacin, levofloxacin) | 250-500 mg BID / 250-500 mg daily | 3 days | Reserve for complicated UTI or pyelonephritis; FDA black box: tendon rupture, aortic dissection, neuropathy |

Pyelonephritis: Presents with fever, flank pain, CVA tenderness ± nausea/vomiting. Labs: UA with pyuria/bacteriuria, CBC (leukocytosis), blood cultures if febrile. Outpatient treatment (mild): ciprofloxacin 500 mg BID × 7 days or TMP-SMX DS BID × 14 days + single dose ceftriaxone 1g IM. Inpatient criteria: sepsis, vomiting preventing oral intake, pregnancy, obstruction suspected.
12 Skin & Soft Tissue Infections Acute
Skin and soft tissue infections (SSTIs) range from simple cellulitis to necrotizing fasciitis. The primary clinical decision: purulent (abscess likely — I&D is the primary treatment) vs non-purulent (cellulitis/erysipelas — antibiotics are the primary treatment).
SSTI Classification & Management
| Type | Presentation | Pathogen | Treatment |
|---|---|---|---|
| Simple abscess | Fluctuant, tender, erythematous nodule ± pustule | MRSA (most common community cause), S. aureus | I&D is sufficient for most; antibiotics added if: cellulitis >5 cm surrounding, immunocompromised, multiple abscesses, indwelling device. TMP-SMX DS BID or doxycycline 100 mg BID × 7-10 days |
| Non-purulent cellulitis | Spreading erythema, warmth, tenderness, no drainable collection | Group A Strep (most common), MSSA | Cephalexin 500 mg QID or dicloxacillin 500 mg QID × 5-7 days. If MRSA concern: add TMP-SMX or doxycycline |
| Erysipelas | Sharply demarcated, raised, bright red plaque; face or lower extremity | Group A Strep | Penicillin VK 500 mg QID × 5 days; amoxicillin 500 mg TID alternative |
| Necrotizing fasciitis | EMERGENCY — pain out of proportion to exam, rapid spread, crepitus, dusky/necrotic skin, sepsis, bullae | Type I (polymicrobial), Type II (GAS), Type III (Vibrio — saltwater/raw seafood) | Emergent surgical debridement + broad-spectrum IV antibiotics (vancomycin + piperacillin-tazobactam + clindamycin). Mortality 20-40% even with treatment |
Pain out of proportion to exam findings is the earliest and most important sign. Other red flags: rapidly progressing erythema (mark borders with pen — if spreading visibly over hours, suspect NF), bullae or skin necrosis, crepitus on palpation (gas in tissue), systemic toxicity (fever, tachycardia, hypotension), WBC >15,000 or Na <135. The LRINEC score (Lab Risk Indicator for Necrotizing Fasciitis) uses CRP, WBC, hemoglobin, sodium, creatinine, and glucose to risk-stratify — score ≥6 raises suspicion, ≥8 is strongly suggestive. CT showing gas in soft tissue is diagnostic but do NOT delay surgical consultation waiting for imaging.
13 Acute Low Back Pain Acute
Low back pain is the leading cause of disability worldwide and the second most common reason for primary care visits. ~90% of acute low back pain is nonspecific mechanical pain — no identifiable structural pathology, self-limited within 4-6 weeks. The critical task in primary care is identifying the 1-5% of patients with serious underlying pathology requiring urgent evaluation.
Red Flags — When to Image or Urgently Refer
| Red Flag | Concern | Action |
|---|---|---|
| Saddle anesthesia, urinary retention/incontinence, fecal incontinence, bilateral leg weakness | Cauda equina syndrome | EMERGENT MRI + surgical consult within hours |
| History of cancer + new back pain, unexplained weight loss, age >50 with new LBP | Spinal metastasis | MRI with contrast |
| Fever + back pain, IV drug use, recent spinal procedure, immunosuppression | Spinal epidural abscess / osteomyelitis | MRI with contrast + ESR/CRP + blood cultures |
| Significant trauma (fall, MVC) or minor trauma in osteoporotic patient | Compression fracture | X-ray first; MRI if neurologic symptoms |
| Progressive neurologic deficit (foot drop, ascending weakness) | Compressive myelopathy or severe radiculopathy | Urgent MRI |

Management of nonspecific acute LBP: Reassurance (expected to improve in 2-4 weeks), stay active (bed rest worsens outcomes), NSAIDs first-line (ibuprofen 400-600 mg TID or naproxen 500 mg BID), topical heat. Second-line: skeletal muscle relaxant for spasm (cyclobenzaprine 5-10 mg TID × 7-10 days — sedation is common and can be used therapeutically at bedtime). Avoid imaging in the first 6 weeks unless red flags are present — early MRI increases surgery rates without improving outcomes. Avoid opioids as first-line.
14 Acute Abdomen Triage Acute
The family physician's role in acute abdominal pain is pattern recognition and triage — determining who needs emergent surgical evaluation, who needs urgent workup, and who can be managed conservatively. Location of pain is the most useful initial discriminator.
Abdominal Pain by Location — Differential Diagnosis
| Location | Common Causes | Key Tests |
|---|---|---|
| RUQ | Cholecystitis (Murphy's sign), hepatitis, liver abscess, right-sided pneumonia, Fitz-Hugh-Curtis (PID-associated perihepatitis) | RUQ ultrasound, LFTs, lipase |
| Epigastric | Peptic ulcer disease, gastritis, pancreatitis, GERD, MI (inferior wall), aortic dissection | Lipase, ECG, CXR if free air suspected |
| LUQ | Splenic infarct/rupture, pancreatitis (tail), left lower lobe pneumonia | CT abdomen, CBC |
| RLQ | Appendicitis (McBurney's point), ovarian torsion/cyst, ectopic pregnancy, Meckel's diverticulum, mesenteric adenitis (children) | CT abdomen/pelvis (adults), US (pediatric/pregnant), beta-hCG in reproductive-age women |
| LLQ | Diverticulitis, ovarian pathology, sigmoid volvulus, IBD flare | CT abdomen/pelvis |
| Suprapubic | UTI/cystitis, urinary retention, PID, ectopic pregnancy | UA, beta-hCG, pelvic ultrasound |
| Diffuse | SBO, mesenteric ischemia, DKA, peritonitis, gastroenteritis, IBD | CT with IV contrast, lactate, CBC, BMP |
Involuntary guarding + rigidity = peritonitis until proven otherwise. Upright CXR or CT showing free intraperitoneal air = perforated viscus → emergent surgery. Pain out of proportion to exam with metabolic acidosis and lactate elevation → mesenteric ischemia until proven otherwise (mortality >50% if delayed). Testicular pain in males <25 with high-riding testis and absent cremasteric reflex = testicular torsion → 6-hour window for detorsion. All reproductive-age women with acute abdominal/pelvic pain need a beta-hCG — ruptured ectopic pregnancy kills.
15 Osteoarthritis MSK
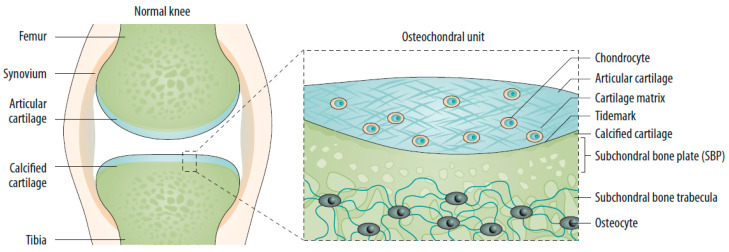
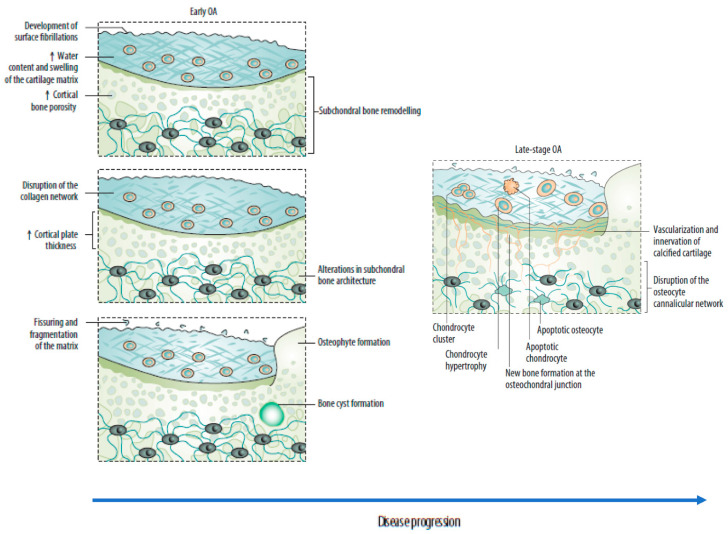
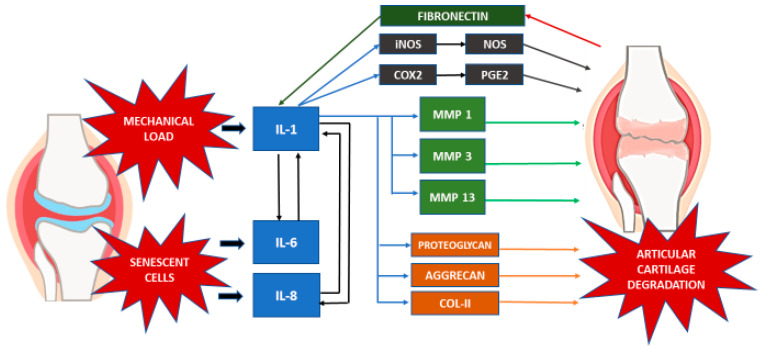
Osteoarthritis (OA) is the most common joint disease — affecting >32 million US adults. It is a disease of the entire joint, not just "worn cartilage": cartilage degradation, subchondral bone remodeling, osteophyte formation, synovial inflammation, and ligament/meniscal degeneration all contribute. Most commonly affected joints: knees, hips, hands (DIP > PIP; spares MCPs — this pattern differentiates OA from RA), and spine (facet joints, disc degeneration).
Diagnosis
Clinical diagnosis — imaging is confirmatory, not required. Classic features: joint pain that worsens with activity and improves with rest, morning stiffness <30 minutes (vs RA: >60 minutes), crepitus, bony enlargement (Heberden's nodes = DIP, Bouchard's nodes = PIP), reduced ROM. X-ray findings: Joint space narrowing, osteophytes, subchondral sclerosis, subchondral cysts. Kellgren-Lawrence grading (0-4) quantifies radiographic severity.
Kellgren-Lawrence Classification
| Grade | Radiographic Findings | Clinical Correlation |
|---|---|---|
| 0 | Normal | No radiographic OA |
| 1 | Doubtful — possible osteophytes, no joint space narrowing | Symptoms may or may not be present |
| 2 | Mild — definite osteophytes, possible joint space narrowing | Intermittent pain with activity |
| 3 | Moderate — moderate osteophytes, definite narrowing, some sclerosis | Regular pain, functional limitation |
| 4 | Severe — large osteophytes, marked narrowing, severe sclerosis, bone deformity | Constant pain, significant disability; joint replacement candidate |
Management
Non-pharmacologic (first-line for all): Weight loss (every 1 lb lost = 4 lbs of pressure off the knee), low-impact exercise (swimming, cycling, walking), physical therapy for strengthening and ROM, knee bracing/orthotics, assistive devices. Pharmacologic: Topical NSAIDs (diclofenac gel — fewer systemic side effects), oral NSAIDs (shortest duration, lowest dose), topical capsaicin, duloxetine 60 mg daily (FDA-approved for OA pain). Intra-articular: Corticosteroid injection (triamcinolone 40 mg for knee — provides 4-8 weeks of relief; limit to 3-4/year per joint). Hyaluronic acid injections have modest evidence. Surgical: Total joint arthroplasty for refractory KL grade 3-4 with failure of conservative management.
16 Tendinopathies & Overuse Injuries MSK
Tendinopathy (formerly "tendinitis") is the preferred term because histology shows collagen degeneration and failed healing, not acute inflammation. Common sites encountered in family medicine:
| Condition | Location | Exam Finding | First-Line Treatment |
|---|---|---|---|
| Lateral epicondylitis ("tennis elbow") | Common extensor tendon at lateral epicondyle | Pain with resisted wrist extension and grip; tenderness over lateral epicondyle | Relative rest, counterforce brace, eccentric wrist extension exercises, topical NSAID |
| Medial epicondylitis ("golfer's elbow") | Common flexor tendon at medial epicondyle | Pain with resisted wrist flexion and forearm pronation | Same principles as lateral; less common |
| Rotator cuff tendinopathy | Supraspinatus (most common), infraspinatus | Painful arc (60-120° abduction), positive Neer's and Hawkins impingement tests, weakness with external rotation (infraspinatus) | PT (rotator cuff strengthening, scapular stabilization), subacromial corticosteroid injection if refractory |
| De Quervain's tenosynovitis | 1st dorsal compartment (APL, EPB tendons) | Positive Finkelstein's test (ulnar deviation of wrist with thumb in fist → pain over radial styloid) | Thumb spica splint, corticosteroid injection into 1st dorsal compartment (cure rate ~80%) |
| Plantar fasciitis | Plantar fascia at calcaneal insertion | First-step morning pain, tenderness at medial calcaneal tubercle | Calf/plantar stretching, supportive footwear, night splint, NSAIDs; corticosteroid injection if >6 weeks refractory (risk of fat pad atrophy) |
| Achilles tendinopathy | Achilles tendon (mid-substance or insertional) | Pain with palpation 2-6 cm above calcaneus (mid-substance); pain at insertion (insertional); positive Thompson test rules out rupture | Eccentric heel drop exercises (Alfredson protocol), heel lifts, avoid fluoroquinolones (tendon rupture risk) |
17 Chronic Low Back Pain MSK
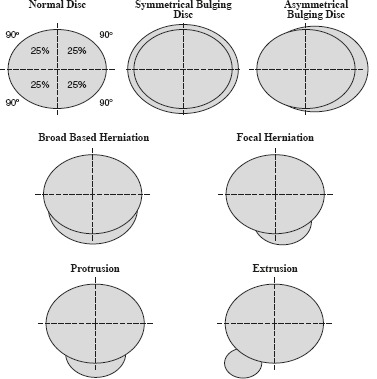
Chronic LBP persists beyond 12 weeks. Unlike acute LBP, chronic LBP is a biopsychosocial condition: psychosocial factors (depression, catastrophizing, job dissatisfaction, fear-avoidance behavior) are stronger predictors of chronicity than MRI findings. Up to 60% of asymptomatic adults have disc bulges on MRI — imaging findings often do not correlate with symptoms.

Management Hierarchy
First-line: Exercise therapy (core stabilization, yoga, tai chi — all have Level A evidence), cognitive behavioral therapy (CBT), interdisciplinary rehabilitation. Second-line: Duloxetine 60 mg daily (FDA-approved for chronic musculoskeletal pain), NSAIDs for flares, spinal manipulation (modest short-term benefit). Third-line: Gabapentin/pregabalin if radicular component; tramadol only if non-opioid approaches have failed. Avoid: Chronic opioids (no evidence of long-term benefit for CLBP and substantial harm), passive modalities (ultrasound, TENS — minimal evidence), repeat imaging without new red flags, surgery for nonspecific LBP.
When to refer for surgery: Cauda equina syndrome (emergent). Progressive motor deficit (urgent). Radiculopathy with concordant MRI findings refractory to 6-8 weeks of conservative care. Spinal stenosis with neurogenic claudication limiting function despite physical therapy.
18 Osteoporosis MSK
Osteoporosis is a systemic skeletal disease characterized by low bone mass and microarchitectural deterioration → increased fracture risk. Affects 10 million Americans (80% women). Hip fractures carry 20-30% one-year mortality in elderly patients. The USPSTF recommends DEXA screening for all women ≥65 and postmenopausal women <65 with risk factors (FRAX tool).
T-Score Classification (WHO)
| T-Score | Classification | Clinical Action |
|---|---|---|
| ≥ −1.0 | Normal | Rescreen based on risk factors |
| −1.0 to −2.5 | Osteopenia | FRAX assessment; treat if 10-yr hip fracture risk ≥3% or major osteoporotic fracture ≥20% |
| ≤ −2.5 | Osteoporosis | Pharmacotherapy + calcium/vitamin D + fall prevention |
| ≤ −2.5 with fragility fracture | Severe osteoporosis | Aggressive treatment; consider anabolic agent first |
Pharmacotherapy
| Agent | Mechanism | Dosing | Pearl |
|---|---|---|---|
| Alendronate (Fosamax) | Bisphosphonate — inhibits osteoclast resorption | 70 mg PO weekly | Take on empty stomach with full glass of water, remain upright 30 min (esophageal erosion risk); drug holiday after 5 yr PO or 3 yr IV |
| Risedronate (Actonel) | Bisphosphonate | 35 mg PO weekly or 150 mg monthly | Same precautions as alendronate |
| Zoledronic acid (Reclast) | IV bisphosphonate | 5 mg IV annually | Best adherence; flu-like reaction common after first infusion; check vitamin D and renal function before |
| Denosumab (Prolia) | RANKL inhibitor → decreases osteoclast formation | 60 mg SubQ q6months | No renal dose adjustment; rebound vertebral fractures if discontinued — must transition to bisphosphonate |
| Teriparatide (Forteo) | PTH analog — anabolic (stimulates osteoblasts) | 20 mcg SubQ daily × 2 years | For severe osteoporosis or fracture despite bisphosphonate; must follow with antiresorptive agent; black box: osteosarcoma in rats |
| Romosozumab (Evenity) | Sclerostin inhibitor — anabolic + antiresorptive | 210 mg SubQ monthly × 12 months | Most potent for BMD gain; black box: CV risk (avoid within 1 yr of MI/stroke); follow with bisphosphonate or denosumab |
Supplementation baseline: Calcium 1000-1200 mg/day (dietary + supplement if needed), vitamin D 800-1000 IU/day (target 25-OH vitamin D ≥30 ng/mL). Weight-bearing exercise and fall prevention are essential non-pharmacologic components.
19 Depression & Anxiety Behavioral
Depression and anxiety are the two most common mental health conditions in primary care. Family physicians manage the majority of depression and anxiety in the US — only ~20% of patients are referred to psychiatry. The PHQ-9 (depression) and GAD-7 (anxiety) are validated screening and monitoring instruments used at nearly every primary care encounter.
PHQ-9 Scoring
| Score | Severity | Management |
|---|---|---|
| 0-4 | Minimal | No treatment; reassess if clinically indicated |
| 5-9 | Mild | Watchful waiting, lifestyle modifications, consider therapy (CBT) |
| 10-14 | Moderate | Antidepressant OR psychotherapy; combination preferred if available |
| 15-19 | Moderately severe | Antidepressant + psychotherapy strongly recommended |
| 20-27 | Severe | Antidepressant + psychotherapy; consider psychiatry referral |
Antidepressant Selection
| Class / Agent | Dose Range | Key Feature | Side Effects / Pearl |
|---|---|---|---|
| SSRI — sertraline (Zoloft) | 50-200 mg/day | First-line for MDD and most anxiety disorders; safe in cardiac patients | GI side effects (nausea, diarrhea); sexual dysfunction 30-50%; avoid abrupt discontinuation |
| SSRI — escitalopram (Lexapro) | 10-20 mg/day | Best tolerated SSRI; fewest drug interactions | QTc prolongation at 20 mg — ECG if >65 or cardiac hx; max 10 mg if >65 |
| SSRI — fluoxetine (Prozac) | 20-80 mg/day | Long half-life (5 days) — no discontinuation syndrome; preferred in non-adherent patients | Most activating SSRI; CYP2D6 inhibitor (drug interactions) |
| SNRI — duloxetine (Cymbalta) | 30-120 mg/day | Depression + chronic pain + fibromyalgia + DPN | Hepatotoxicity with heavy alcohol use; nausea; BP elevation at higher doses |
| SNRI — venlafaxine XR (Effexor XR) | 75-225 mg/day | Effective for treatment-resistant depression; GAD approved | Dose-dependent hypertension; worst discontinuation syndrome of all antidepressants; taper very slowly |
| Bupropion (Wellbutrin XL) | 150-450 mg/day | No sexual dysfunction, no weight gain; helps with smoking cessation; activating | Contraindicated in seizure disorders, eating disorders; lower seizure threshold; not effective for anxiety |
| Mirtazapine (Remeron) | 15-45 mg/day | Sedating, appetite-stimulating — good for depressed elderly with insomnia and weight loss | Weight gain, sedation (paradoxically more sedating at 15 mg than 45 mg); no sexual dysfunction |
GAD-7 and Anxiety Management
GAD-7 scoring: 0-4 minimal, 5-9 mild, 10-14 moderate, 15-21 severe. First-line pharmacotherapy for generalized anxiety disorder: SSRIs (sertraline, escitalopram) or SNRIs (duloxetine, venlafaxine). Buspirone (BuSpar) 10-30 mg/day in divided doses is a non-addictive anxiolytic — takes 2-4 weeks for full effect. Benzodiazepines (lorazepam, alprazolam) for short-term use ONLY (<2-4 weeks) — high addiction potential, cognitive impairment, fall risk in elderly, rebound anxiety. CBT is equally effective as medication for mild-moderate anxiety and should be offered to all patients.
20 ADHD Behavioral
Attention-deficit/hyperactivity disorder (ADHD) affects 5-7% of children and 2.5-4% of adults. Family physicians diagnose and manage the majority of pediatric ADHD. DSM-5 requires 6+ symptoms of inattention and/or hyperactivity-impulsivity persisting ≥6 months, present before age 12, in ≥2 settings (home + school/work), with functional impairment.
Pharmacotherapy
| Agent (Generic/Brand) | Class | Dosing | Duration | Pearl |
|---|---|---|---|---|
| Methylphenidate IR (Ritalin) | Stimulant (dopamine/NE reuptake inhibitor) | 5-60 mg/day divided BID-TID | 3-4 hours | Start low, titrate weekly; first-line in children ≥6 |
| Methylphenidate ER (Concerta) | Stimulant | 18-72 mg daily | 10-12 hours | OROS delivery; cannot crush; avoids noon dose at school |
| Amphetamine mixed salts (Adderall XR) | Stimulant (dopamine/NE release + reuptake inhibition) | 5-30 mg daily | 10-12 hours | May be more effective if methylphenidate fails; higher abuse potential |
| Lisdexamfetamine (Vyvanse) | Prodrug stimulant | 20-70 mg daily | 12-14 hours | Requires enzymatic conversion — lower abuse potential; also FDA-approved for binge eating disorder |
| Atomoxetine (Strattera) | Non-stimulant (NE reuptake inhibitor) | 40-100 mg daily (adults) | 24 hours | No abuse potential; takes 4-6 weeks for full effect; useful if tics, anxiety, or substance use concerns |
| Guanfacine ER (Intuniv) | Non-stimulant (alpha-2 agonist) | 1-4 mg daily | 24 hours | Sedation, hypotension; helpful for hyperactivity/impulsivity predominant; can augment stimulants |
AAP guidelines for children: Age 4-5: behavioral therapy first, methylphenidate if inadequate response. Age 6-11: stimulant medication + behavioral therapy (combined is superior). Age ≥12: stimulant medication with or without behavioral therapy. Monitor: height, weight (growth charts — stimulants can suppress appetite/growth), heart rate, blood pressure, tics, sleep, mood.
21 Substance Use Disorders Behavioral
Substance use disorders (SUDs) are among the most under-recognized and undertreated conditions in primary care. Family physicians are uniquely positioned to screen (SBIRT: Screening, Brief Intervention, Referral to Treatment), initiate medication-assisted treatment (MAT), and provide longitudinal care. Alcohol use disorder (AUD) and opioid use disorder (OUD) are the two SUDs most commonly managed in the primary care setting.
Alcohol Use Disorder
Screening: AUDIT-C (3 questions, score ≥4 men / ≥3 women = positive screen) or CAGE (2+ positive = concerning). DSM-5 AUD: ≥2 of 11 criteria in a 12-month period (mild: 2-3; moderate: 4-5; severe: 6+).
Pharmacotherapy for AUD:
| Agent | Mechanism | Dose | Pearl |
|---|---|---|---|
| Naltrexone (ReVia, Vivitrol) | Opioid antagonist → reduces reward from drinking | 50 mg PO daily or 380 mg IM monthly | Most effective for reducing heavy drinking days; contraindicated if on opioids; check LFTs |
| Acamprosate (Campral) | Glutamate modulator → reduces craving in abstinence | 666 mg TID | Works best after detox in abstinent patients; dose-adjust for renal impairment; no hepatotoxicity (advantage over naltrexone) |
| Disulfiram (Antabuse) | Aldehyde dehydrogenase inhibitor → aversive reaction with alcohol | 250-500 mg daily | Causes nausea, vomiting, flushing, headache if alcohol consumed; requires high motivation; hepatotoxicity risk |
Opioid Use Disorder
Buprenorphine-naloxone (Suboxone): Partial mu-opioid agonist. Family physicians can prescribe buprenorphine — the X-waiver requirement was eliminated in 2023. Induction: patient must be in moderate withdrawal (COWS score ≥8-12); start 2-4 mg SL, may repeat in 1-2 hours, typical day-1 dose 8-16 mg. Maintenance: 16-24 mg/day. Has a ceiling effect for respiratory depression — much safer than methadone. Common induction pitfall: starting too early precipitates withdrawal (buprenorphine displaces full agonists from receptors).
Naltrexone (Vivitrol) 380 mg IM monthly: Full opioid antagonist. Patient must be opioid-free for 7-10 days before starting (precipitated withdrawal risk). Best for highly motivated patients or those in controlled environments (drug court, sober living).
22 Insomnia Behavioral
Chronic insomnia (difficulty initiating or maintaining sleep ≥3 nights/week for ≥3 months) affects 10-15% of adults. First-line treatment is NOT medication — it is cognitive behavioral therapy for insomnia (CBT-I), which has better long-term efficacy than any pharmacotherapy and no side effects.
CBT-I Components
Sleep restriction: Limit time in bed to actual sleep time (e.g., if sleeping 5 hr but in bed 8 hr, restrict to 5 hr; gradually increase by 15-30 min as efficiency improves; target sleep efficiency ≥85%). Stimulus control: Bed is for sleep and sex only; leave bed if awake >20 minutes. Sleep hygiene: Consistent wake time, dark/cool room, no screens 1 hr before bed, limit caffeine after noon, avoid alcohol. Cognitive restructuring: Address catastrophic beliefs about sleep consequences.
Pharmacotherapy (Second-Line)
| Agent | Mechanism | Dose | Pearl |
|---|---|---|---|
| Melatonin | MT1/MT2 receptor agonist | 0.5-5 mg 1-2 hr before bed | Most evidence for circadian rhythm disorders and jet lag; minimal evidence for chronic insomnia; OTC; low risk |
| Trazodone | 5-HT2A antagonist + weak SERT inhibitor | 25-100 mg qhs | Most commonly prescribed off-label sleep aid; not FDA-approved for insomnia; priapism (rare); minimal dependence |
| Suvorexant (Belsomra) | Dual orexin receptor antagonist (DORA) | 10-20 mg qhs | FDA-approved; no rebound insomnia; avoid with strong CYP3A4 inhibitors; expensive |
| Lemborexant (DayVigo) | DORA | 5-10 mg qhs | Similar to suvorexant; may have slight advantage for sleep maintenance |
| Zolpidem (Ambien) | Non-benzodiazepine GABA-A agonist | 5 mg (women) / 5-10 mg (men) qhs | FDA lowered female dose due to next-morning impairment; sleepwalking, sleep-driving risk; short-term only (<4 weeks) |
| Doxepin (Silenor) | H1 antihistamine at low dose | 3-6 mg qhs | FDA-approved for sleep maintenance insomnia; safe in elderly (minimal anticholinergic at this dose) |
23 Contraception Women's Health
Family physicians provide the majority of contraceptive care in the US. Contraceptive counseling should be patient-centered, using the tiered-effectiveness model (LARC → hormonal → barrier) while respecting patient autonomy.
Contraceptive Methods by Effectiveness
| Method | Typical-Use Failure Rate | Mechanism | Duration | Key Consideration |
|---|---|---|---|---|
| Copper IUD (Paragard) | 0.8% | Spermicidal Cu2+ ions; inflammatory reaction prevents implantation | 10-12 years | Non-hormonal; heavier periods; can serve as emergency contraception (within 5 days) |
| LNG-IUD (Mirena, Kyleena, Liletta) | 0.1-0.4% | Local progestin → thins endometrium, thickens cervical mucus | 3-8 years (device-dependent) | Reduces menstrual bleeding (treats menorrhagia); Mirena FDA-approved for heavy periods |
| Etonogestrel implant (Nexplanon) | 0.1% | Progestin → suppresses ovulation, thickens mucus | 3-5 years | Most effective reversible contraceptive; irregular bleeding most common reason for discontinuation |
| DMPA injection (Depo-Provera) | 4% | Progestin → suppresses ovulation | Every 3 months | Weight gain, bone density loss (reversible); delayed return to fertility (up to 10 months) |
| Combined OCP (various) | 7% | Estrogen + progestin → suppress ovulation, thin endometrium, thicken mucus | Daily pill | Contraindicated in smokers ≥35, migraine with aura, VTE history, breast cancer (use CDC MEC categories) |
| Progestin-only pill (Norethindrone 0.35 mg) | 7% | Thickens mucus; inconsistently suppresses ovulation | Daily pill (3-hour window) | Safe for breastfeeding, smokers ≥35, migraine with aura; new POP: norgestrel (Opill) available OTC 2024 |
| Patch (Xulane) / Ring (NuvaRing) | 7% | Combined hormonal — transdermal/vaginal absorption | Weekly patch / monthly ring | Same contraindications as OCP; patch less effective in women >90 kg |
| Male condom | 13% | Barrier | Per use | Only method that prevents STIs (dual method recommended with hormonal) |
CDC Medical Eligibility Criteria (MEC) — Key Category 4 Contraindications
Category 4 = unacceptable health risk: Combined hormonal contraceptives (CHC) are Category 4 with: current or hx of VTE/PE, ischemic heart disease, stroke, migraine with aura, breast cancer, smoker ≥35 (if ≥15 cigarettes/day), <3 weeks postpartum, hepatocellular adenoma, severe cirrhosis, SLE with antiphospholipid antibodies. The progestin-only methods (IUD, implant, DMPA, POP) have very few Category 4 contraindications and are safe in nearly all patients.
24 Prenatal Care Women's Health
Family physicians deliver ~20% of babies in the US and provide the majority of prenatal care in rural settings. Standard prenatal visit schedule: monthly through 28 weeks, biweekly 28-36 weeks, weekly 36 weeks to delivery. First visit ideally at 8-10 weeks.
Prenatal Visit Laboratory Schedule
| Timing | Labs & Tests |
|---|---|
| Initial visit (8-10 wk) | CBC, blood type/Rh/antibody screen, rubella immunity, hepatitis B surface antigen, HIV, RPR/VDRL, UA + culture, Pap if due, chlamydia/gonorrhea (NAAT), urine hCG confirmation |
| 11-14 weeks | First trimester screen (NT ultrasound + PAPP-A + free beta-hCG) or cell-free DNA (NIPT) for aneuploidy |
| 15-20 weeks | Quad screen (if no first-trimester screen), AFP for neural tube defects, anatomy ultrasound at 18-22 weeks |
| 24-28 weeks | 1-hr glucose challenge test (50g GCT; ≥140 → 3-hr 100g OGTT for GDM), CBC (screen for anemia), Rh antibody screen (if Rh-negative: give RhoGAM 300 mcg IM at 28 wk) |
| 35-37 weeks | Group B Strep (GBS) vaginal-rectal culture; if positive, intrapartum penicillin G prophylaxis |
| 36+ weeks | Confirm fetal presentation (Leopold's maneuvers/ultrasound); discuss labor plan; screen for preeclampsia (BP, proteinuria) |
Common Prenatal Complications
Gestational diabetes (GDM): Diagnosed when 2+ of 4 values on 3-hr OGTT are abnormal (fasting ≥95, 1-hr ≥180, 2-hr ≥155, 3-hr ≥140 mg/dL). Management: dietary modification + glucose monitoring (fasting <95, 1-hr postprandial <140, 2-hr <120); insulin is first-line pharmacotherapy if diet fails (metformin and glyburide used but NOT FDA-approved for pregnancy).
Preeclampsia: New-onset hypertension (≥140/90 on 2 occasions ≥4 hours apart) after 20 weeks with proteinuria (≥300 mg/24hr or protein/creatinine ratio ≥0.3) or end-organ dysfunction (platelets <100K, Cr >1.1, elevated LFTs, pulmonary edema, cerebral/visual symptoms). Severe features: SBP ≥160 or DBP ≥110, thrombocytopenia, renal insufficiency, liver dysfunction, or symptoms. Definitive treatment: delivery. Magnesium sulfate for seizure prophylaxis (eclampsia prevention). Low-dose aspirin (81 mg starting 12-16 weeks) is recommended for high-risk women to prevent preeclampsia.
25 Menopause Women's Health
Menopause is defined as 12 consecutive months of amenorrhea without other cause, reflecting ovarian follicular depletion. Average age: 51 years. Perimenopause (the transition) begins 4-8 years before final menstrual period and is characterized by irregular cycles, vasomotor symptoms, and hormone fluctuations. Diagnosis is clinical — FSH testing is rarely needed (and unreliable during perimenopause due to fluctuations).
Vasomotor Symptoms — Management
Hormone therapy (HT): Most effective treatment for hot flashes and vaginal atrophy. Estrogen alone (for women without a uterus) or combined estrogen + progestogen (for women with a uterus — progestogen prevents endometrial hyperplasia/cancer). Standard: conjugated equine estrogens (CEE/Premarin) 0.3-0.625 mg/day or transdermal estradiol patch 0.025-0.05 mg/day + medroxyprogesterone acetate (MPA) 2.5 mg daily or micronized progesterone 100-200 mg daily. Initiate within 10 years of menopause or age <60 for best risk-benefit ratio (WHI "timing hypothesis"). Contraindicated in: breast cancer, VTE, stroke, MI, active liver disease.
Non-hormonal options: Fezolinetant (Veozah) 45 mg daily — first NK3 receptor antagonist, FDA-approved 2023, reduces hot flashes ~60%. Paroxetine 7.5 mg (Brisdelle) — only FDA-approved SSRI for vasomotor symptoms. Venlafaxine 37.5-75 mg, gabapentin 300-900 mg qhs (off-label but effective). CBT also reduces vasomotor symptom severity.
Genitourinary syndrome of menopause (GSM): Vaginal dryness, dyspareunia, urinary frequency/urgency. First-line: vaginal moisturizers (Replens) + lubricants. If insufficient: low-dose vaginal estrogen (estradiol cream 0.5g 2×/wk, estradiol ring/Estring, estradiol vaginal tablet) — minimal systemic absorption, safe even in many breast cancer survivors (discuss with oncologist). Ospemifene (Osphena) 60 mg PO daily is an oral SERM alternative.
26 Cervical & Breast Cancer Screening Women's Health
Cervical Cancer Screening
| Age Group | Recommended Screening | Frequency |
|---|---|---|
| <21 | No screening (regardless of sexual activity) | — |
| 21-29 | Cytology (Pap) alone | Every 3 years |
| 30-65 | Pap + hrHPV co-testing (preferred) OR hrHPV alone OR Pap alone | Co-testing q5yr; hrHPV alone q5yr; Pap alone q3yr |
| >65 | Stop if adequate prior negative screening (3 consecutive negative Paps or 2 negative co-tests in prior 10 years) | — |
| Post-hysterectomy (supracervical → continue; total with cervix removed for benign disease and no CIN2+ history) | Stop | — |
Abnormal Pap management (ASCCP 2019): Risk-based approach using current and prior results. LSIL with negative HPV → repeat in 1 year. LSIL or ASC-US with positive HPV → colposcopy. HSIL → expedited treatment (LEEP) or colposcopy with biopsy. CIN1 → surveillance. CIN2/3 → excisional treatment (LEEP/cold knife cone).
Breast Cancer Screening
USPSTF (2024): Biennial mammography for all women aged 40-74. ACS: Annual mammography starting at 45 (may start at 40 with shared decision-making); biennial at 55+. For high-risk women (BRCA carriers, ≥20% lifetime risk by models, chest radiation 10-30): annual mammography + breast MRI starting at 25-30. Clinical breast exam: no longer specifically recommended by USPSTF but still performed in practice.
BI-RADS Classification:
| Category | Assessment | Action |
|---|---|---|
| 0 | Incomplete — needs additional imaging | Callback for diagnostic mammogram, ultrasound, or MRI |
| 1 | Negative | Routine screening |
| 2 | Benign finding | Routine screening |
| 3 | Probably benign (<2% malignancy risk) | Short-interval follow-up at 6 months |
| 4 | Suspicious (2-95% malignancy risk) | Tissue diagnosis (biopsy) |
| 5 | Highly suggestive of malignancy (≥95%) | Tissue diagnosis (biopsy) |
| 6 | Known biopsy-proven malignancy | Surgical management |
27 Well-Child Visits & Milestones Pediatric
The AAP Bright Futures schedule defines well-child visit timing: newborn, 1 month, 2, 4, 6, 9, 12, 15, 18, 24, 30 months, then annually 3-21 years. Each visit includes growth assessment (plotted on CDC growth charts — weight, length/height, head circumference through 24 months, BMI starting at age 2), developmental screening, immunizations, and anticipatory guidance.
Key Developmental Milestones
| Age | Gross Motor | Fine Motor | Language | Social |
|---|---|---|---|---|
| 2 months | Lifts head prone | Hands open 50% | Coos, social smile | Recognizes parent |
| 4 months | Rolls front to back | Reaches, grasps rattle | Laughs, squeals | Enjoys social play |
| 6 months | Sits with support, rolls both ways | Transfers objects hand to hand | Babbles consonants (ba, da) | Stranger anxiety begins |
| 9 months | Pulls to stand, crawls | Pincer grasp developing | Mama/dada (nonspecific) | Separation anxiety, object permanence |
| 12 months | Cruises, may walk independently | Mature pincer grasp | 1-3 words, follows simple commands | Points to show interest, waves bye |
| 18 months | Walks well, climbs stairs with hand held | Stacks 2-4 blocks, scribbles | 10-25 words, points to body parts | Parallel play, imitates |
| 2 years | Runs, kicks ball, climbs | Stacks 6 blocks, turns pages | 2-word phrases ("want milk"), 50+ words | Parallel play, follows 2-step commands |
| 3 years | Pedals tricycle, balances briefly on one foot | Draws circle, uses scissors | 3-word sentences, 75% intelligible to strangers | Interactive play, takes turns |
| 4 years | Hops on one foot, climbs stairs alternating feet | Draws square, dresses self | Complex sentences, tells stories, 100% intelligible | Cooperative play, imaginary friends |
| 5 years | Skips, catches ball | Draws triangle, ties shoes (by 6) | Counts to 10, knows colors, follows 3-step commands | Understands rules, plays organized games |
28 Immunization Schedule Pediatric
The CDC/ACIP immunization schedule is the most frequently referenced guideline in family medicine. Keeping children on schedule prevents an estimated 42,000 deaths per year in the US. The schedule is updated annually; the core childhood series:
Childhood Immunization Schedule (Birth-6 Years)
| Vaccine | Doses | Schedule | Pearl |
|---|---|---|---|
| Hepatitis B (HepB) | 3 | Birth, 1 month, 6 months | First dose within 24 hours of birth; if mother HBsAg+: HBIG + vaccine within 12 hours |
| Rotavirus (RV) | 2-3 | 2, 4 months (Rotarix/2-dose) or 2, 4, 6 months (RotaTeq/3-dose) | Oral live vaccine; do not start after 15 weeks; must complete by 8 months |
| DTaP (diphtheria, tetanus, acellular pertussis) | 5 | 2, 4, 6, 15-18 months, 4-6 years | Switch to Tdap at age 11-12; then Td or Tdap q10 years |
| Hib (H. influenzae type b) | 3-4 | 2, 4, 6 (PRP-T), 12-15 months | Dramatically reduced epiglottitis and bacterial meningitis |
| PCV15 or PCV20 (pneumococcal) | 3-4 | 2, 4, 6, 12-15 months | PCV15 may need PPSV23 follow-up in high-risk children |
| IPV (inactivated polio) | 4 | 2, 4, 6-18 months, 4-6 years | No oral polio (OPV) used in US since 2000 |
| MMR (measles, mumps, rubella) | 2 | 12-15 months, 4-6 years | Live vaccine; contraindicated in pregnancy and severe immunodeficiency; NO causal link to autism |
| Varicella | 2 | 12-15 months, 4-6 years | Live vaccine; avoid in immunocompromised; if ≥13 years and not immune: 2 doses 4-8 weeks apart |
| Hepatitis A (HepA) | 2 | 12 months, 18 months (6-18 months apart) | Universal childhood vaccination since 2006 |
| Influenza | Annual | ≥6 months annually | First-ever flu vaccine in children <9 years: 2 doses 4 weeks apart |
29 Common Pediatric Conditions Pediatric
Croup (Laryngotracheobronchitis)
Peak age 6 months - 3 years. Cause: parainfluenza virus (75%). Classic presentation: barky/seal-like cough, inspiratory stridor, hoarse voice, preceded by URI prodrome. Steeple sign on AP neck X-ray (subglottic narrowing — but X-ray rarely needed). Management: mild (no stridor at rest) → single dose dexamethasone 0.6 mg/kg PO/IM (max 10 mg). Moderate-severe (stridor at rest) → dexamethasone + nebulized racemic epinephrine 0.5 mL of 2.25% in 3 mL NS (observe 2-4 hours for rebound). Red flag: drooling + tripod positioning + toxic appearance = think epiglottitis (now rare post-Hib vaccine).
Pediatric Asthma
Most common chronic disease of childhood. Diagnosis in children ≥5: spirometry showing reversible obstruction (FEV1 improvement ≥12% after bronchodilator). In children <5: clinical diagnosis based on recurrent wheezing (≥3 episodes), symptom pattern, and response to therapy.
| Severity (age ≥5) | Symptoms | Nighttime Awakenings | FEV1 | Step Therapy |
|---|---|---|---|---|
| Intermittent | ≤2 days/week | ≤2×/month | >80% | Step 1: SABA PRN (albuterol) |
| Mild persistent | >2 days/week but not daily | 3-4×/month | ≥80% | Step 2: Low-dose ICS (fluticasone 44-88 mcg BID) or PRN ICS-formoterol |
| Moderate persistent | Daily | >1×/week | 60-80% | Step 3: Low-dose ICS + LABA (fluticasone/salmeterol) or medium-dose ICS |
| Severe persistent | Throughout day | Nightly | <60% | Step 4-5: Medium/high-dose ICS + LABA; consider add-on (LAMA, biologic, oral steroids) |
Acute Otitis Media (Pediatric) — see also Section 10
Most common bacterial infection in children. Risk factors: age <2, daycare attendance, second-hand smoke, bottle-propping, pacifier use after 6 months. Pathogens: S. pneumoniae, non-typeable H. influenzae, M. catarrhalis. Prevention: pneumococcal vaccine, influenza vaccine, breastfeeding.
Febrile Seizures
Occur in 2-5% of children ages 6 months to 5 years. Simple febrile seizure: generalized tonic-clonic, <15 minutes, does not recur within 24 hours. Management: parental reassurance, treat underlying fever source; no antiepileptic drugs, no neuroimaging, no EEG needed. Complex febrile seizure: focal, >15 minutes, or recurrent within 24 hours → consider EEG and workup for other causes. Simple febrile seizures do NOT increase epilepsy risk significantly (2% vs 1% baseline).
30 Adolescent Health Pediatric
Adolescent visits (11-21 years) require a unique approach: confidential screening for high-risk behaviors, STI screening, contraception counseling, and mental health assessment. The HEEADSSS psychosocial assessment framework: Home, Education/Employment, Eating, Activities, Drugs, Sexuality, Suicide/depression, Safety.
Adolescent-Specific Screening & Vaccines
| Item | Age | Details |
|---|---|---|
| HPV vaccine (Gardasil 9) | 11-12 (routine); catch-up through 26 | 2 doses if started <15 (0, 6-12 months); 3 doses if started ≥15 (0, 1-2, 6 months); prevents cervical, anal, oropharyngeal cancers + genital warts |
| Tdap booster | 11-12 | Single dose replacing Td; then Td or Tdap q10 years |
| Meningococcal ACWY (MenACWY) | 11-12, booster at 16 | Quadrivalent; booster at 16 provides coverage through college |
| Meningococcal B (MenB) | 16-23 (shared decision-making) | Not routinely recommended; 2-3 dose series |
| Depression screening | ≥12 annually | PHQ-A (adolescent-modified); Columbia Suicide Severity Rating Scale if positive |
| STI screening | Sexually active: chlamydia/gonorrhea annually (women <25, MSM); HIV at least once ≥15 | NAAT urine or vaginal/cervical swab |
31 Polypharmacy & Deprescribing Geriatric
Polypharmacy (typically defined as ≥5 concurrent medications) affects >40% of adults ≥65. It is a direct cause of adverse drug events (ADEs), falls, cognitive impairment, hospitalization, and mortality. The family physician manages the medication list longitudinally and is best positioned to deprescribe — the systematic process of reducing or stopping medications that are no longer beneficial or are potentially harmful.
Beers Criteria — High-Risk Medications in Elderly (Selected)
| Drug / Class | Risk in Elderly | Alternative |
|---|---|---|
| Benzodiazepines (diazepam, lorazepam, alprazolam) | Falls, fractures, cognitive impairment, dependence | CBT-I for insomnia; SSRI/buspirone for anxiety |
| Anticholinergics (diphenhydramine, hydroxyzine, oxybutynin, TCAs at high dose) | Confusion, delirium, dry mouth, urinary retention, constipation, tachycardia | Loratadine/cetirizine for allergies; mirabegron for OAB; trazodone/melatonin for sleep |
| NSAIDs (chronic use) | GI bleed, renal impairment, HTN, HF exacerbation | Topical NSAIDs, acetaminophen, duloxetine, non-pharmacologic pain management |
| Proton pump inhibitors (chronic >8 weeks without indication) | C. difficile, pneumonia, hypomagnesemia, osteoporotic fractures, CKD | H2 blocker (famotidine), step-down and discontinue if no ongoing indication |
| Sulfonylureas (glyburide especially) | Prolonged hypoglycemia (long half-life, renal clearance) | Glipizide (shorter acting), DPP-4i, or relaxed A1C targets |
| Skeletal muscle relaxants (cyclobenzaprine, methocarbamol) | Sedation, anticholinergic effects, fall risk | PT, topical agents, non-pharmacologic |
Deprescribing Process
Step 1: Reconcile the complete medication list (include OTC, supplements, herbals). Step 2: Identify potentially inappropriate medications (PIMs) using Beers Criteria, STOPP/START criteria, or deprescribing algorithms (deprescribing.org). Step 3: Prioritize — target drugs with highest harm potential and lowest current benefit. Step 4: Taper (do not abruptly stop benzodiazepines, opioids, beta-blockers, corticosteroids, or antidepressants). Step 5: Monitor for withdrawal or return of original condition. Step 6: Repeat at each visit. Deprescribe one medication at a time to attribute any changes.
32 Dementia & Cognitive Decline Geriatric
Dementia affects ~6.7 million Americans ≥65. Alzheimer's disease accounts for 60-80% of cases, followed by vascular dementia (10-20%), Lewy body dementia (5-15%), and frontotemporal dementia (5-10%). Family physicians are typically the first to identify cognitive decline and initiate the diagnostic workup.
Screening & Diagnosis
MoCA (Montreal Cognitive Assessment): 30-point test covering visuospatial, naming, attention, language, abstraction, delayed recall, and orientation. Score ≤25 suggests cognitive impairment (sensitivity 90%, specificity 87% for MCI). MMSE (Mini-Mental State Exam): 30-point test; ≤23 suggests dementia; less sensitive for MCI than MoCA. Mini-Cog: 3-word recall + clock draw — rapid, effective screen for office use.
Reversible Causes to Exclude
Before diagnosing dementia, rule out: hypothyroidism (TSH), B12 deficiency (serum B12 + methylmalonic acid), depression (pseudodementia) (PHQ-9 — treat depression first and reassess), normal pressure hydrocephalus (triad: magnetic gait, urinary incontinence, dementia — MRI shows ventriculomegaly out of proportion to atrophy), medication effects (anticholinergics, benzodiazepines, opioids), sleep disorders (OSA), syphilis (RPR if risk factors). Standard labs: CBC, CMP, TSH, B12, folate, RPR, urinalysis. MRI brain without contrast to assess for structural causes, vascular changes, and atrophy pattern.
Pharmacotherapy
| Agent | Mechanism | Indication | Pearl |
|---|---|---|---|
| Donepezil (Aricept) 5-10 mg qhs | Cholinesterase inhibitor | Mild-moderate Alzheimer's | Most commonly used; GI side effects, bradycardia; check HR before starting |
| Rivastigmine (Exelon) patch 4.6-13.3 mg/24hr | Cholinesterase inhibitor | Mild-moderate Alzheimer's; Parkinson's disease dementia | Patch formulation reduces GI side effects |
| Memantine (Namenda) 5-20 mg/day | NMDA receptor antagonist | Moderate-severe Alzheimer's (often added to donepezil) | Better tolerated than ChEIs; may combine with donepezil (Namzaric = combination) |
| Lecanemab (Leqembi) | Anti-amyloid monoclonal antibody | Early Alzheimer's with confirmed amyloid pathology | 27% slowing of cognitive decline; ARIA (amyloid-related imaging abnormalities) risk — requires MRI monitoring; IV infusion q2 weeks |
Non-pharmacologic management (often more impactful): Structured daily routines, caregiver education and support, safety assessments (driving, wandering, firearms), advance care planning, adult day programs, occupational therapy, music/art therapy, exercise (30+ min walking has cognitive benefits), management of behavioral symptoms (redirect, validate, minimize triggers before using antipsychotics — which carry a black box warning for increased mortality in elderly with dementia).
33 Falls Prevention Geriatric
Falls are the leading cause of injury-related death in adults ≥65 (36,000 deaths/year in the US). One in four older adults falls each year, and falls are the most common cause of traumatic brain injury and hip fracture in this population. The USPSTF recommends exercise interventions to prevent falls in community-dwelling adults ≥65 at increased fall risk (Grade B).
Fall Risk Assessment — Key Components
Screening: Ask every patient ≥65 at annual visit: "Have you fallen in the past year? Do you feel unsteady when standing or walking?" If yes to either → comprehensive fall risk assessment.
Assessment: (1) Gait and balance testing: Timed Up and Go (TUG) — >12 seconds = increased fall risk; 30-second Chair Stand Test. (2) Medication review: target benzodiazepines, opioids, anticholinergics, antihypertensives (orthostatic hypotension), antihistamines. (3) Orthostatic vitals: BP lying → standing at 1 and 3 minutes; drop ≥20 systolic or ≥10 diastolic = orthostatic hypotension. (4) Vision: visual acuity, cataract evaluation. (5) Footwear and home safety: grab bars, remove throw rugs, adequate lighting, non-slip mats. (6) Vitamin D: supplement 800-1000 IU daily (prevents falls via improved muscle strength and neuromuscular function).
Exercise interventions: Tai chi (strongest evidence — reduces falls by 20-30%), balance training, strength training (especially lower extremity), and gait training. Referral to physical therapy for individualized fall prevention program.
34 Advanced Care Planning Geriatric
Advanced care planning (ACP) is the process of discussing and documenting a patient's values, goals, and preferences for future medical care in the event they cannot speak for themselves. Every adult — especially those ≥65 or with serious illness — should have ACP documented. Family physicians are the ideal provider for these conversations because of the longitudinal patient relationship.
Key ACP Documents
| Document | Function | Key Points |
|---|---|---|
| Advance Directive (Living Will) | Specifies what treatments the patient does or does not want | CPR, intubation/mechanical ventilation, artificial nutrition/hydration, dialysis; should specify under what conditions (e.g., "if permanently unconscious") |
| Durable Power of Attorney for Healthcare (Healthcare Proxy) | Designates a person to make medical decisions if the patient cannot | The most important ACP document — a named decision-maker who knows the patient's values can address unforeseen scenarios that a living will cannot anticipate |
| POLST/MOLST | Physician/Medical Orders for Life-Sustaining Treatment | Actionable medical orders (not just patient preferences); signed by physician; honored by EMS; covers CPR, intubation, hospital transfer, IV fluids, antibiotics |
| DNR/DNI | Do Not Resuscitate / Do Not Intubate orders | Specific medical orders; patients often conflate DNR with "do nothing" — clarify that DNR means no CPR/defibrillation but all other care continues |
35 Common Rashes — Eczema, Psoriasis, Fungal Derm
Atopic Dermatitis (Eczema)
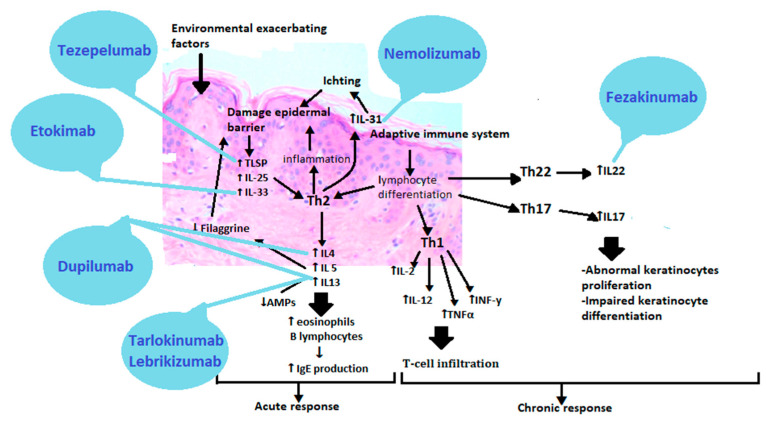
Chronic, relapsing, intensely pruritic dermatitis. Affects 10-20% of children and 1-3% of adults. Distribution varies by age: infants (face, extensor surfaces), children/adults (flexural areas — antecubital fossa, popliteal fossa, neck). Part of the atopic triad (eczema, asthma, allergic rhinitis). Pathophysiology: filaggrin gene mutations lead to epidermal barrier dysfunction + Th2-mediated inflammation.
Management: (1) Restore skin barrier: liberal emollient application (CeraVe, Vanicream, Aquaphor — apply within 3 minutes of bathing). (2) Mild: low-potency topical corticosteroid (hydrocortisone 2.5% for face/folds). (3) Moderate: medium-potency (triamcinolone 0.1% for body). (4) Severe or steroid-sparing: topical calcineurin inhibitors (tacrolimus 0.03-0.1%, pimecrolimus 1%) — no skin atrophy risk. (5) Refractory: dupilumab (Dupixent) — IL-4/IL-13 monoclonal antibody, SC q2wk, approved for ≥6 months. Avoid triggers: fragrances, harsh soaps, wool, dust mites, pet dander. Bleach baths (1/4 cup per full tub, 10 min, 2-3x/week) reduce skin Staph colonization.
Psoriasis
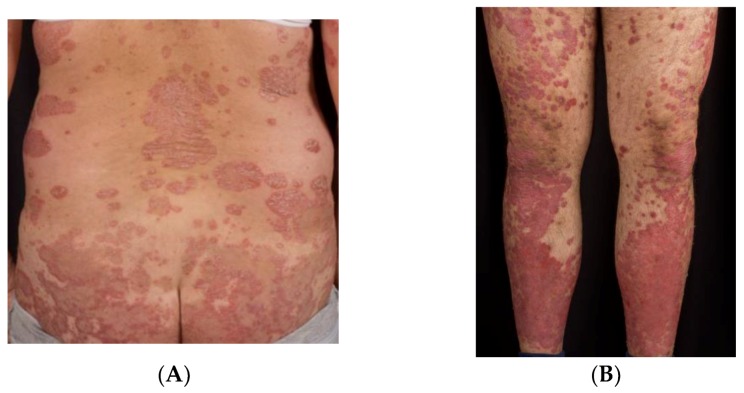
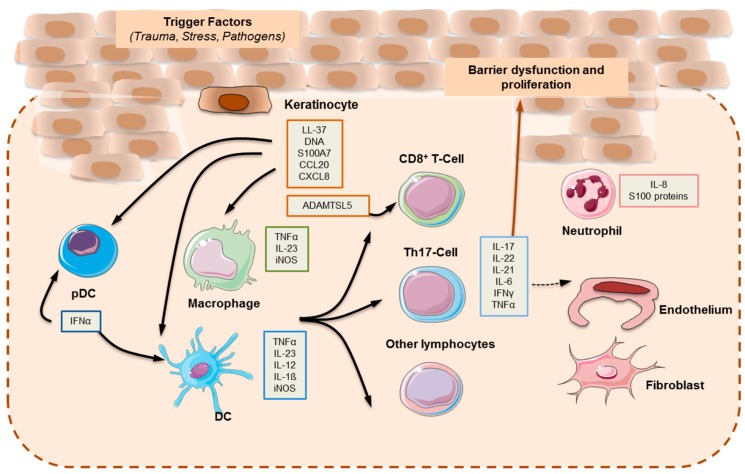
Chronic autoimmune disease affecting 2-3% of the global population. Classic presentation: well-demarcated, salmon-pink plaques with silvery-white scale on extensor surfaces (elbows, knees), scalp, and lumbosacral area. Auspitz sign (pinpoint bleeding when scale is removed). Associated with: psoriatic arthritis (up to 30% of psoriasis patients), metabolic syndrome, depression, cardiovascular disease.
Management by severity: Mild (<3% BSA): topical corticosteroids (betamethasone 0.05% ointment), topical vitamin D analogs (calcipotriene), combination calcipotriene/betamethasone (Enstilar foam). Moderate-severe (>3% BSA or refractory): phototherapy (narrowband UVB), or systemic agents: methotrexate 7.5-25 mg/week (monitor LFTs, CBC; avoid in liver disease/pregnancy), apremilast (Otezla — PDE4 inhibitor), or biologics (adalimumab/Humira, secukinumab/Cosentyx, risankizumab/Skyrizi, guselkumab/Tremfya). Screen for psoriatic arthritis (morning stiffness, dactylitis, nail pitting) at every visit.
Dermatophyte Infections (Tinea)
| Type | Location | Appearance | Treatment |
|---|---|---|---|
| Tinea corporis (ringworm) | Body/trunk | Annular, erythematous, scaly plaque with central clearing | Topical: terbinafine 1% BID or clotrimazole 1% BID × 2-4 weeks |
| Tinea pedis (athlete's foot) | Feet (interdigital, moccasin, vesicular) | Scaling, maceration, fissuring between toes; or diffuse scaling of sole | Topical antifungal × 4 weeks; keep feet dry |
| Tinea cruris (jock itch) | Groin, inner thigh | Erythematous, scaly plaques with raised border; spares scrotum (unlike candida) | Topical antifungal × 2-4 weeks; powder to reduce moisture |
| Tinea capitis | Scalp (children) | Scaly patches with hair loss, "black dot" tinea, kerion (boggy, inflammatory mass) | SYSTEMIC required (topicals don't penetrate hair follicle): griseofulvin 20-25 mg/kg/day × 6-8 weeks or terbinafine 250 mg/day × 4-6 weeks (adults/older children) |
| Tinea unguium (onychomycosis) | Nails (toenails > fingernails) | Thickened, yellow, brittle, dystrophic nails; subungual debris | Terbinafine (Lamisil) 250 mg daily × 6 weeks (fingernails) or 12 weeks (toenails); check LFTs; topical efinaconazole (Jublia) for mild cases |
36 Skin Cancer Screening (ABCDE) Derm
Melanoma accounts for only 1% of skin cancers but causes the majority of skin cancer deaths (~8,000/year in the US). Family physicians perform opportunistic skin cancer screening during physical exams — the USPSTF has an I (insufficient evidence) rating for routine whole-body screening in asymptomatic average-risk adults, but clinical vigilance remains essential.
ABCDE Criteria for Melanoma
| Criterion | Feature | Detail |
|---|---|---|
| A — Asymmetry | One half unlike the other | Benign nevi are symmetric |
| B — Border | Irregular, ragged, notched, or blurred edges | Benign nevi have smooth, even borders |
| C — Color | Varied (brown, black, red, white, blue within one lesion) | Benign nevi are usually one shade of brown |
| D — Diameter | >6 mm (pencil eraser) | Though melanomas can be smaller; diameter alone is not sensitive |
| E — Evolving | Changing in size, shape, color, or new symptoms (bleeding, itching) | Most important criterion; any changing mole in an adult warrants evaluation |
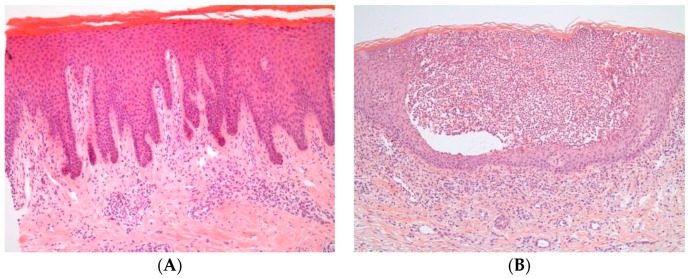
The "ugly duckling" sign: A mole that looks different from all other moles on the patient's body — even if it doesn't meet ABCDE criteria — warrants biopsy. This is often how nodular melanoma (which may be symmetric and uniform) is caught.
Non-Melanoma Skin Cancers
Basal cell carcinoma (BCC): Most common cancer in humans. Pearly, translucent papule/nodule with telangiectasia and rolled borders; may have central ulceration ("rodent ulcer"). Sun-exposed areas. Locally invasive but almost never metastasizes. Treatment: excision, Mohs surgery (face/high-risk), ED&C, topical imiquimod (superficial BCC).
Squamous cell carcinoma (SCC): Keratotic papule/plaque, may be ulcerated, on sun-exposed skin (especially scalp, ears, lower lip, dorsal hands). Can metastasize (2-6% risk, higher on lip/ear, immunosuppressed patients). Precursor: actinic keratosis (scaly, rough papule on sun-damaged skin — treat with cryotherapy, topical 5-FU, or imiquimod). SCC treatment: excision with margins, Mohs for high-risk.
37 Acne Derm
Acne vulgaris affects 85% of adolescents and can persist into adulthood. Pathophysiology involves four mechanisms: (1) follicular hyperkeratinization (plugging), (2) excess sebum production (androgen-driven), (3) Cutibacterium acnes (formerly Propionibacterium acnes) proliferation, (4) inflammation. Classification: comedonal (whiteheads/blackheads), inflammatory (papules, pustules), nodulocystic (deep, painful nodules/cysts — highest scarring risk).
Treatment by Severity
| Severity | First-Line | Add-On / Second-Line | Pearl |
|---|---|---|---|
| Mild comedonal | Topical retinoid (adapalene 0.1% / Differin — OTC, tretinoin 0.025-0.1%) | Benzoyl peroxide (BP) 2.5-5% — antibacterial | Retinoids are the backbone of ALL acne regimens — they normalize follicular keratinization |
| Mild-moderate inflammatory | Topical retinoid + topical BP ± topical antibiotic (clindamycin 1%) | Combination products: adapalene/BP (Epiduo), clindamycin/BP (Duac) | NEVER use topical antibiotics as monotherapy (resistance); always combine with BP |
| Moderate-severe inflammatory | Oral antibiotic (doxycycline 100 mg daily or minocycline 100 mg daily) + topical retinoid + BP | Oral antibiotics × 3 months max then discontinue (maintain with topicals); spironolactone 50-200 mg daily in women (anti-androgen) | Limit oral antibiotic duration to prevent resistance; combine with topical regimen always |
| Severe nodulocystic or refractory | Isotretinoin (Accutane) 0.5-1 mg/kg/day × 15-20 weeks (cumulative dose 120-150 mg/kg) | — | iPLEDGE program required (teratogenicity — pregnancy test monthly, 2 forms of contraception); monitor LFTs, lipids monthly; dry skin/lips universal; depression monitoring (causal link debated) |
38 Joint Injections Procedure
Corticosteroid injections are among the most commonly performed office procedures in family medicine. Indications: inflammatory or degenerative joint pain refractory to oral management, bursitis, trigger finger, de Quervain's tenosynovitis, plantar fasciitis.
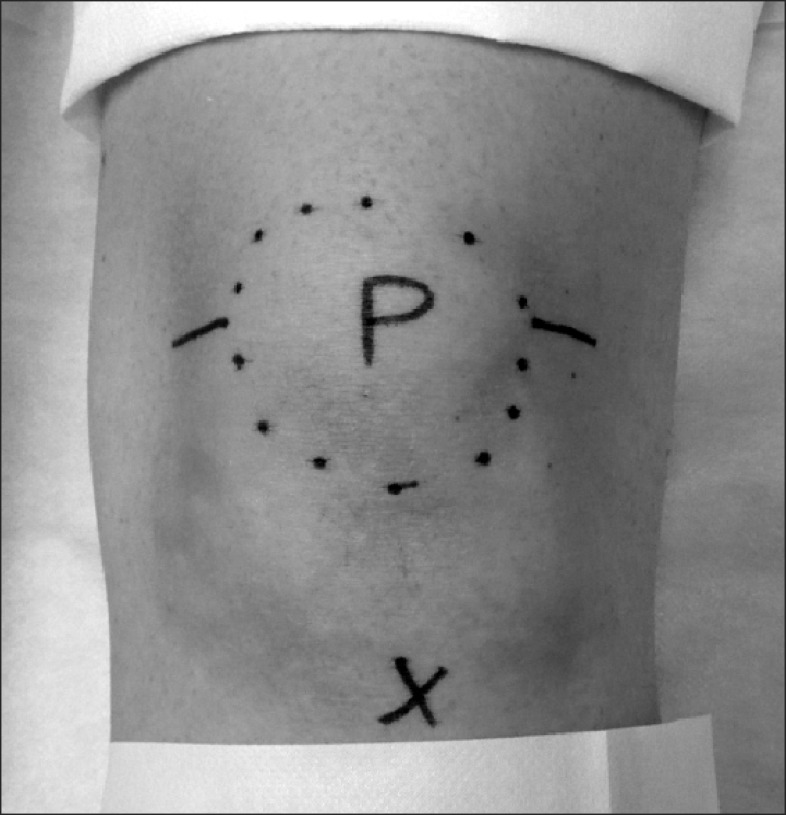
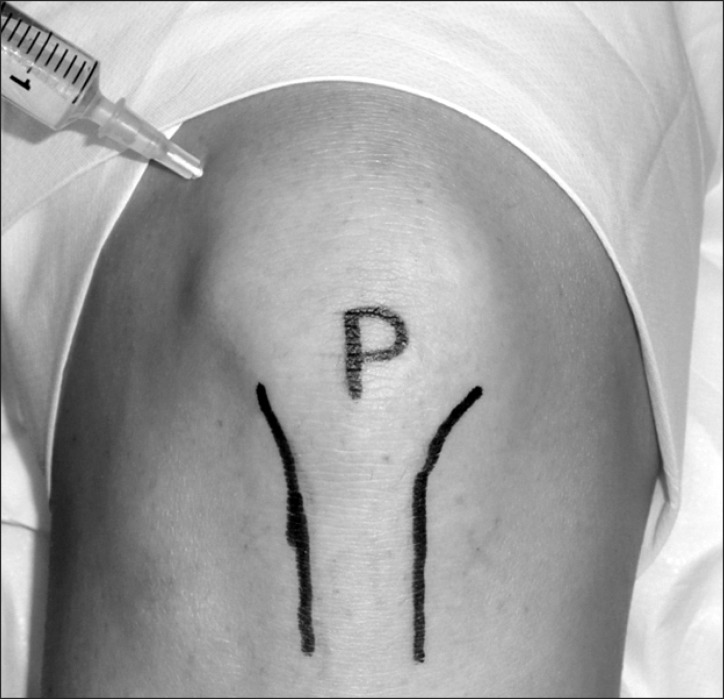
Common Injection Sites & Technique
| Joint/Site | Approach | Steroid / Dose | Pearl |
|---|---|---|---|
| Knee | Superolateral (most common): patient supine, knee extended, insert needle at superolateral patellar border directed under patella | Triamcinolone 40 mg + 3-5 mL lidocaine 1% | Aspirate effusion first (send for cell count, crystals, culture if infection suspected); limit to 3-4 injections/year |
| Shoulder (subacromial) | Posterior approach: 2 cm inferior and medial to posterolateral acromion corner; direct needle anteriorly and slightly superiorly into subacromial space | Triamcinolone 40 mg + 3-5 mL lidocaine 1% | Pain relief confirms impingement diagnosis (diagnostic + therapeutic) |
| Trigger finger (A1 pulley) | Insert needle at palmar MCP crease, tangential to tendon, into tendon sheath | Triamcinolone 10 mg + 0.5 mL lidocaine 1% | Single injection resolves ~60-70% of trigger fingers; may repeat once before surgical referral |
| Lateral epicondyle (tennis elbow) | Palpate maximally tender point at lateral epicondyle; insert perpendicular to skin | Triamcinolone 10-20 mg + 1 mL lidocaine 1% | Short-term relief but may worsen long-term outcomes vs PT alone; use judiciously |
| Greater trochanteric bursa | Lateral decubitus; palpate maximal tenderness over greater trochanter; insert perpendicular | Triamcinolone 40 mg + 3-5 mL lidocaine 1% | Combined injection + PT has best outcomes |
39 Skin Biopsy & Excision Procedure
Family physicians perform the majority of skin biopsies in the US. The three main biopsy types serve different diagnostic purposes:
| Technique | Method | Best For | Pearl |
|---|---|---|---|
| Shave biopsy | Tangential excision with blade or DermaBlade parallel to skin surface | Raised lesions, superficial lesions; when melanoma is NOT suspected | Fastest, minimal scarring; does NOT provide depth — never use for pigmented lesions suspicious for melanoma |
| Punch biopsy | Circular blade (2-6 mm) through full thickness of skin | Inflammatory rashes (need epidermis + dermis for path), alopecia, small lesions; can be diagnostic or excisional if ≤4 mm | Standard: 4 mm punch for most indications; 1-2 sutures to close; orient punch along relaxed skin tension lines (RSTL) for best cosmetic result |
| Excisional biopsy | Elliptical excision with scalpel, full thickness including subcutaneous fat | Suspected melanoma (need full depth + margins), lipomas, cysts, any lesion requiring complete removal | 3:1 length-to-width ellipse ratio; orient along RSTL; for suspected melanoma: 1-3 mm clinical margins at biopsy; definitive wide excision with margins based on Breslow depth after pathology |
Local anesthesia: Lidocaine 1% (max dose 4.5 mg/kg without epi, 7 mg/kg with epi). Buffer with sodium bicarbonate (1 mL bicarb per 9 mL lidocaine) to reduce injection pain. Inject slowly, use small-gauge needle (27-30G). Avoid epinephrine on digits (historic teaching, now debated — low-dose epinephrine on fingers is increasingly considered safe).
40 Spirometry Procedure
Spirometry is the office-based pulmonary function test used to diagnose and monitor obstructive lung diseases (asthma, COPD). Every family medicine office should have the capability to perform spirometry.
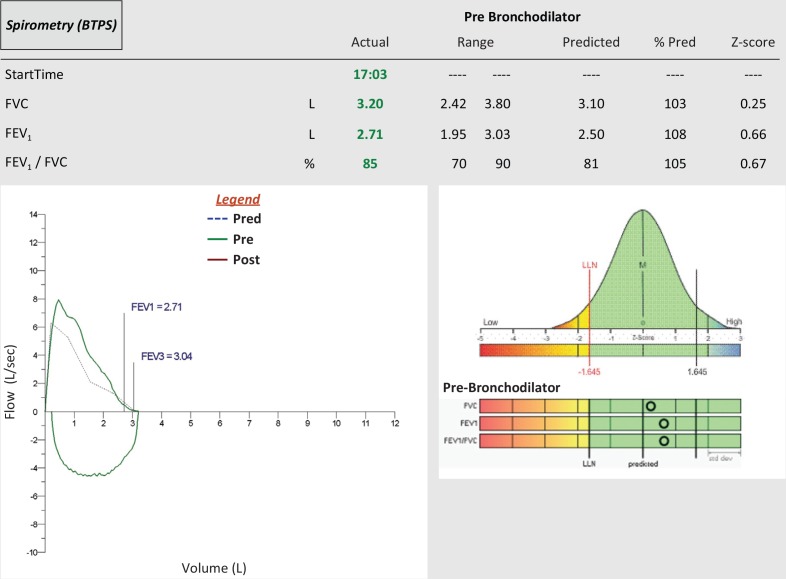
Key Spirometry Values
| Measure | Definition | Clinical Significance |
|---|---|---|
| FEV1 | Forced expiratory volume in 1 second | Most reproducible measure; used to grade COPD severity and assess asthma control |
| FVC | Forced vital capacity — total volume exhaled after maximal inspiration | Reduced in restrictive disease; may be reduced in severe obstruction (air trapping) |
| FEV1/FVC ratio | Proportion of FVC exhaled in first second | <0.70 = obstruction (GOLD criteria for COPD). Normal for age needed — ratio naturally decreases with age |
| Bronchodilator response | Repeat spirometry 15-20 min after 400 mcg albuterol | ≥12% AND ≥200 mL improvement in FEV1 = positive (reversible obstruction — suggests asthma) |
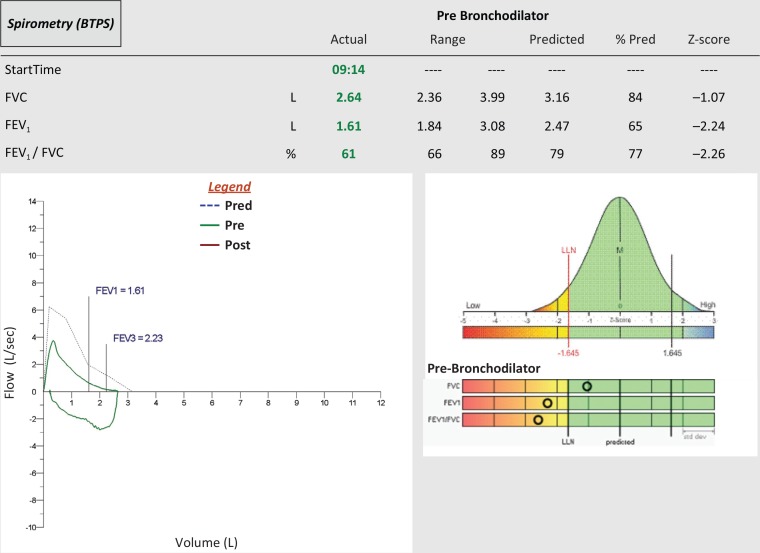
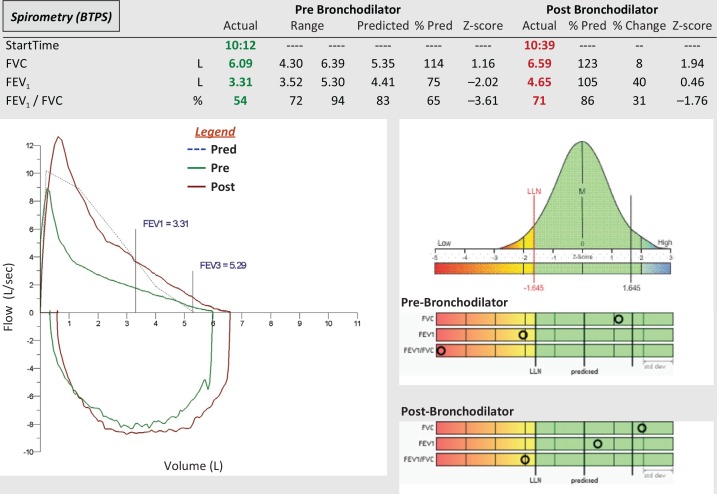
GOLD COPD Staging by FEV1 (Post-Bronchodilator)
| Stage | FEV1 (% predicted) | Severity |
|---|---|---|
| GOLD 1 | ≥80% | Mild |
| GOLD 2 | 50-79% | Moderate |
| GOLD 3 | 30-49% | Severe |
| GOLD 4 | <30% | Very severe |
COPD maintenance therapy (GOLD 2024): All: smoking cessation + influenza/pneumococcal/COVID vaccination + pulmonary rehab. Group A (few symptoms, low exacerbation risk): SABA or SAMA PRN. Group B (more symptoms): LABA or LAMA (tiotropium/Spiriva is most studied LAMA). Group E (exacerbations): LABA + LAMA; if eosinophils ≥300: LABA + LAMA + ICS (triple therapy — ETHOS and IMPACT trials showed mortality benefit).
41 Wound Care Procedure
Laceration repair and wound management are core family medicine procedures. The two critical decisions: (1) Does this wound need closure? (2) Primary (sutures/staples now), delayed primary (close in 3-5 days if contaminated), or secondary intention (leave open to heal by granulation)?
Wound Closure Guidelines
| Factor | Primary Closure Appropriate | Delayed or Secondary Closure |
|---|---|---|
| Time since injury | <6-8 hours (body), <12-24 hours (face — rich blood supply) | >24 hours, or grossly contaminated |
| Contamination | Clean or minimally contaminated | Heavy contamination, bite wounds (except face), soil/organic matter |
| Mechanism | Sharp/clean laceration | Crush injury, stellate laceration, high-velocity projectile |
Suture selection: Face: 5-0 or 6-0 non-absorbable (nylon), remove in 5 days. Scalp: staples (fast, effective) or 3-0 nylon, remove in 7-10 days. Extremity: 4-0 nylon, remove in 10-14 days. Deep layer (dermal): absorbable (Vicryl 4-0 or 5-0) for tension reduction — buried knot. Tissue adhesive (Dermabond): appropriate for clean, low-tension lacerations, especially in children.
Tetanus prophylaxis: Clean minor wound: Tdap/Td if >10 years since last dose. All other wounds (contaminated, puncture, crush, burns, frostbite): Tdap/Td if >5 years since last dose. If unknown or <3 prior doses: give Tdap + TIG (tetanus immune globulin) for non-clean wounds.
42 Splinting & Fracture Management Procedure
Family physicians diagnose and initially manage the majority of non-displaced fractures. Proper splinting immobilizes the injured area, reduces pain, and prevents further injury during the healing process.
Splinting Principles
Immobilize one joint above and one joint below the fracture. Apply over appropriate padding (stockinette + cotton roll/Webril). Check and document neurovascular status (sensation, capillary refill, pulses) before AND after splint application. Common splints:
| Splint Type | Indication | Position |
|---|---|---|
| Sugar-tong forearm | Distal radius fractures (Colles', Smith's) | Elbow 90° flexion, wrist neutral to slight extension |
| Ulnar gutter | 4th/5th metacarpal fractures (Boxer's fracture) | Wrist 20-30° extension, MCP 70-90° flexion, IP joints slightly flexed |
| Thumb spica | Scaphoid fracture (snuffbox tenderness), De Quervain's, thumb UCL injury (gamekeeper's) | Wrist neutral, thumb in abduction (glass-holding position) |
| Posterior ankle | Ankle fractures (non-displaced), severe sprains | Ankle 90° (neutral dorsiflexion), toes free |
| Buddy taping | Non-displaced phalangeal fractures, finger sprains | Tape injured finger to adjacent finger with gauze between; allows some ROM |
Ottawa Ankle Rules: X-ray only if: bone tenderness at posterior edge or tip of lateral or medial malleolus, OR inability to bear weight immediately and in the ED (4 steps). These rules have ~98% sensitivity for fracture and reduce unnecessary X-rays by 30-40%. Similar rules exist for knee (Ottawa Knee Rules) and foot (Ottawa Foot Rules for midfoot fractures).
43 USPSTF Screening Guidelines — Consolidated
| Condition | Population | Screening Method | Interval | Grade |
|---|---|---|---|---|
| Hypertension | Adults ≥18 | Office BP | Annual; q3-5yr if normal <40 | A |
| Type 2 Diabetes | Adults 35-70 with overweight/obesity | FPG, A1C, or OGTT | Every 3 years | B |
| Dyslipidemia | Men ≥35; women ≥45 | Lipid panel | Every 5 years | A/B |
| Colorectal Cancer | Adults 45-75 | Colonoscopy, FIT, Cologuard | Depends on modality | A |
| Breast Cancer | Women 40-74 | Mammography | Biennial | B |
| Cervical Cancer | Women 21-65 | Pap ± hrHPV | q3-5yr depending on test | A |
| Lung Cancer | Adults 50-80, ≥20 pack-year hx | Low-dose CT | Annual | B |
| AAA | Men 65-75 who ever smoked | Abdominal US | One-time | B |
| Osteoporosis | Women ≥65; postmenopausal <65 with risk | DEXA | Per risk | B |
| Depression | All adults ≥18 | PHQ-2/PHQ-9 | Annual | B |
| Hepatitis C | Adults 18-79 | Anti-HCV Ab | One-time | B |
| HIV | Adults 15-65 | HIV Ag/Ab | At least once | A |
| Hepatitis B | Adolescents/adults at increased risk | HBsAg, anti-HBs, anti-HBc | Per risk | B |
| STIs (Chlamydia/Gonorrhea) | Sexually active women <25, others at risk | NAAT | Annual | B |
| Prediabetes/DM (pregnancy) | Pregnant women 24-28 wk | GCT/OGTT | 24-28 weeks | B |
| Unhealthy Alcohol Use | Adults ≥18 | AUDIT-C | Annual | B |
| Tobacco Use | All adults | Ask + advise cessation | Every visit | A |
| Obesity | Adults ≥18 | BMI calculation | Annual | B |
| Anxiety | Adults <65 | GAD-7 | Per clinical judgment | B |
44 Classification Systems
| System | Application | Key Features |
|---|---|---|
| JNC 8 / 2017 ACC/AHA BP Classification | Hypertension staging | Normal, Elevated, Stage 1 (130-139/80-89), Stage 2 (≥140/90), Crisis (>180/120) |
| ADA Diabetes Criteria | Diabetes diagnosis | FPG ≥126, 2-hr OGTT ≥200, A1C ≥6.5%, random glucose ≥200 + symptoms |
| BMI Classification (WHO) | Obesity staging | Underweight <18.5, Normal 18.5-24.9, Overweight 25-29.9, Obesity I/II/III: 30/35/40+ |
| Centor / McIsaac Score | Pharyngitis — strep likelihood | 5 criteria (exudate, LAD, fever, no cough, age); guides testing/treatment |
| CURB-65 | Pneumonia severity | Confusion, Urea >7, RR ≥30, BP <90/60, age ≥65; 0-1 outpatient, 2 consider admit, 3+ ICU |
| PHQ-9 | Depression severity | 0-4 minimal, 5-9 mild, 10-14 moderate, 15-19 mod-severe, 20-27 severe |
| GAD-7 | Anxiety severity | 0-4 minimal, 5-9 mild, 10-14 moderate, 15-21 severe |
| AUDIT / AUDIT-C | Alcohol use screening | AUDIT-C ≥4 (men) / ≥3 (women) = positive screen |
| Kellgren-Lawrence | OA radiographic severity | Grades 0-4: normal to severe (osteophytes, narrowing, sclerosis, deformity) |
| T-Score (WHO) | Bone density | Normal ≥−1.0, Osteopenia −1.0 to −2.5, Osteoporosis ≤−2.5 |
| BI-RADS | Mammography assessment | Categories 0-6: incomplete to known malignancy |
| Bethesda System | Pap smear cytology | NILM, ASC-US, ASC-H, LSIL, HSIL, AGC, carcinoma |
| GOLD Staging | COPD severity | 1-4 by FEV1 % predicted: ≥80, 50-79, 30-49, <30 |
| NYHA Functional Class | Heart failure severity | I (no limitation), II (slight), III (marked), IV (symptoms at rest) |
| CKD Staging (KDIGO) | Chronic kidney disease | Stages 1-5 by eGFR: ≥90, 60-89, 30-59, 15-29, <15 |
| ASCVD Risk (PCE) | 10-year CV risk | Low <5%, Borderline 5-7.4%, Intermediate 7.5-19.9%, High ≥20% |
| Ottawa Rules | Ankle/knee/foot X-ray decision | Clinical criteria to rule out fracture without imaging; ~98% sensitivity |
| Beers Criteria (AGS) | Potentially inappropriate medications in elderly | Updated every 3 years; categorizes drugs to avoid, use with caution, or avoid in specific conditions |
45 Medications Master Table
Antihypertensives
| Generic (Brand) | Class | Typical Dose | Mechanism | Key Pearl |
|---|---|---|---|---|
| Lisinopril (Zestril) | ACEi | 10-40 mg daily | ↓ Angiotensin II | Cough 10-20%; angioedema; monitor K+/Cr; CI in pregnancy |
| Losartan (Cozaar) | ARB | 50-100 mg daily | AT1 receptor blockade | No cough; uricosuric effect (lowers uric acid) |
| Amlodipine (Norvasc) | DHP-CCB | 5-10 mg daily | Vascular smooth muscle relaxation | Peripheral edema; long half-life; safe in pregnancy (category C) |
| Chlorthalidone | Thiazide-like | 12.5-25 mg daily | ↓ NaCl reabsorption in DCT | More potent than HCTZ; hypokalemia, hyponatremia, hyperuricemia |
| Metoprolol succinate (Toprol XL) | Beta-1 selective blocker | 25-200 mg daily | ↓ HR and contractility | Also for HFrEF; avoid abrupt discontinuation; mask hypoglycemia in diabetics |
| Spironolactone (Aldactone) | MRA | 25-50 mg daily | Aldosterone antagonism | Best 4th-line for resistant HTN; hyperkalemia; gynecomastia in men |
Diabetes Agents
| Generic (Brand) | Class | Typical Dose | A1C Reduction | Key Pearl |
|---|---|---|---|---|
| Metformin (Glucophage) | Biguanide | 500-2000 mg daily | 1.0-1.5% | First-line; hold if eGFR <30; GI side effects → use ER |
| Semaglutide (Ozempic) | GLP-1 RA | 0.25-2 mg SC weekly | 1.0-1.8% | CV benefit; weight loss; nausea; CI with MTC/MEN2 |
| Empagliflozin (Jardiance) | SGLT2i | 10-25 mg daily | 0.5-0.9% | CV + renal + HF benefit; genital mycotic infections; euglycemic DKA |
| Glipizide (Glucotrol) | Sulfonylurea | 5-20 mg daily | 1.0-1.5% | Cheap; hypoglycemia risk; weight gain |
| Sitagliptin (Januvia) | DPP-4i | 100 mg daily | 0.5-0.8% | Weight-neutral; dose adjust for CKD; no CV benefit |
| Insulin glargine (Lantus) | Basal insulin | 10 U → titrate | 1.5-3.5% | Start 10 U or 0.1-0.2 U/kg; titrate by 2 U q3d to fasting target |
Lipid Agents
| Generic (Brand) | Class | Typical Dose | LDL Reduction | Key Pearl |
|---|---|---|---|---|
| Atorvastatin (Lipitor) | HMG-CoA reductase inhibitor | 10-80 mg daily | 30-50%+ (dose-dependent) | High-intensity at 40-80 mg; myalgias 5-10%; hepatotoxicity rare; check baseline LFTs |
| Rosuvastatin (Crestor) | Statin | 5-40 mg daily | 30-50%+ | Most potent statin per mg; high-intensity at 20-40 mg; CKD dose adjustment |
| Ezetimibe (Zetia) | Cholesterol absorption inhibitor | 10 mg daily | ~18% | Add-on to statin; IMPROVE-IT trial: benefit in ACS patients |
| Icosapent ethyl (Vascepa) | Omega-3 (EPA) | 2 g BID | TG reduction; CV risk reduction | REDUCE-IT: 25% CV event reduction; use with statin; AFib risk |
| Evolocumab (Repatha) | PCSK9 inhibitor | 140 mg SC q2wk | ~60% | For ASCVD patients not at LDL goal on max statin + ezetimibe; expensive |
Antibiotics (Common Primary Care)
| Generic (Brand) | Class | Common Use | Key Pearl |
|---|---|---|---|
| Amoxicillin | Aminopenicillin | Strep pharyngitis, AOM, sinusitis | First-line for many pediatric infections; 80-90 mg/kg/day for AOM |
| Amoxicillin-clavulanate (Augmentin) | Beta-lactam + BLI | Sinusitis, AOM (2nd-line), bite wounds | Covers beta-lactamase producers; diarrhea common |
| Azithromycin (Zithromax) | Macrolide | CAP, chlamydia, pertussis | 5-day Z-pack; QTc prolongation; increasing resistance in S. pneumoniae |
| Doxycycline | Tetracycline | Sinusitis (alt), cellulitis (MRSA), Lyme, chlamydia, acne | Photosensitivity; esophageal erosion (take with water, upright); avoid in children <8 and pregnancy |
| Cephalexin (Keflex) | 1st gen cephalosporin | Cellulitis (non-purulent), UTI (pregnancy) | MSSA coverage; does not cover MRSA |
| TMP-SMX (Bactrim DS) | Folate antagonist | UTI, MRSA skin infections | Check sulfa allergy; hyperkalemia; avoid in 3rd trimester |
| Nitrofurantoin (Macrobid) | Nitrofuran | Uncomplicated cystitis | First-line UTI; avoid if eGFR <30; does not treat pyelonephritis |
| Ciprofloxacin (Cipro) | Fluoroquinolone | Pyelonephritis, complicated UTI | FDA black box: tendon rupture, aortic dissection, neuropathy; reserve for serious infections |
Mental Health Medications
| Generic (Brand) | Class | Typical Dose | Key Pearl |
|---|---|---|---|
| Sertraline (Zoloft) | SSRI | 50-200 mg daily | First-line MDD/GAD/PTSD/OCD/panic; safest in cardiac patients |
| Escitalopram (Lexapro) | SSRI | 10-20 mg daily | Best tolerated; fewest interactions; QTc at 20 mg |
| Bupropion XL (Wellbutrin) | NDRI | 150-450 mg daily | No sexual dysfunction/weight gain; CI in seizures/eating disorders |
| Duloxetine (Cymbalta) | SNRI | 30-120 mg daily | MDD + pain; hepatotoxicity with alcohol; nausea |
| Buspirone (BuSpar) | 5-HT1A agonist | 10-30 mg BID-TID | Non-addictive anxiolytic; 2-4 week onset; no CNS depression |
| Methylphenidate ER (Concerta) | Stimulant | 18-72 mg daily | ADHD first-line; monitor growth, HR, BP; Schedule II |
| Naltrexone (Vivitrol) | Opioid antagonist | 50 mg PO or 380 mg IM monthly | AUD and OUD; patient must be opioid-free 7-10 days |
| Buprenorphine-naloxone (Suboxone) | Partial mu agonist | 8-24 mg SL daily | OUD maintenance; X-waiver eliminated 2023; ceiling on respiratory depression |
46 Abbreviations Master List
Diagnoses
Screening & Assessment Tools
Procedures & Imaging
Medications & Labs
Organizations & Guidelines
47 Immunization Schedules (Adult & Pediatric)
Adult Immunization Schedule (CDC/ACIP)
| Vaccine | Indication | Schedule | Pearl |
|---|---|---|---|
| Influenza | All adults annually | 1 dose annually (fall) | Egg allergy no longer a contraindication (even with anaphylaxis); high-dose (Fluzone HD) or adjuvanted (Fluad) for ≥65 |
| Td/Tdap | All adults | Tdap once (if not received), then Td or Tdap q10 years | Tdap during each pregnancy (27-36 weeks) regardless of prior vaccination |
| COVID-19 | All adults | Per current CDC recommendations (updated annually) | Updated formulations target circulating variants; coadministration with other vaccines is acceptable |
| Shingles (Shingrix) | Adults ≥50 | 2 doses, 2-6 months apart | Recombinant (not live); 90%+ efficacy; give even if prior Zostavax or prior shingles episode |
| Pneumococcal (PCV20 or PCV15+PPSV23) | Adults ≥65, or 19-64 with risk factors | PCV20 single dose (preferred); or PCV15 → PPSV23 ≥1 year later | Risk factors: chronic heart/lung/liver/kidney disease, diabetes, alcoholism, smoking, immunocompromised, CSF leak, cochlear implant |
| Hepatitis B | Adults 19-59 (all); ≥60 with risk factors | 3-dose (Engerix-B: 0, 1, 6 months) or 2-dose (Heplisav-B: 0, 1 month) | Heplisav-B preferred for rapid completion; check anti-HBs 1-2 months after completion in healthcare workers and dialysis patients |
| HPV (Gardasil 9) | Through age 26 (routine); 27-45 shared decision-making | 2 doses (if started <15) or 3 doses | Catch-up through 26; most effective before sexual debut; prevents 6 cancer types |
| MMR | Adults born after 1957 without evidence of immunity | 1 or 2 doses depending on risk (healthcare workers, international travel: 2 doses) | Live vaccine; CI in pregnancy and severe immunodeficiency |
| Varicella | Adults without evidence of immunity | 2 doses, 4-8 weeks apart | Live vaccine; CI in pregnancy; evidence of immunity = US-born before 1980, documented doses, positive titer, or provider-diagnosed disease |
| RSV (Abrysvo or Arexvy) | Adults ≥60 (shared decision-making); pregnant persons 32-36 weeks (Abrysvo) | Single dose | New (2023); seasonal (fall); maternal vaccination protects newborns from RSV bronchiolitis |
References & Figure Sources
Figures
- Figure 1 — Cardiovascular and Metabolic Risk Factors. Galicia-Garcia U, et al. PMC7503727. Licensed under CC BY 4.0.
- Figure 2 — Vascular Flow Dynamics and Atherosclerosis. Jebari-Benslaiman S, et al. PMC8954705. Licensed under CC BY 4.0.
- Figure 3 — Atherosclerotic Plaque Formation. Jebari-Benslaiman S, et al. PMC8954705. Licensed under CC BY 4.0.
- Figure 4 — The RAAS. Patel S, et al. PMC8547789. Licensed under CC BY 4.0.
- Figure 5 — Pancreatic Beta-Cell Insulin Secretion. Galicia-Garcia U, et al. PMC7503727. Licensed under CC BY 4.0.
- Figure 6 — T2DM Pathophysiology. Galicia-Garcia U, et al. PMC7503727. Licensed under CC BY 4.0.
- Figure 7 — Insulin Effects on Adipose Tissue. Galicia-Garcia U, et al. PMC7503727. Licensed under CC BY 4.0.
- Figure 8 — Diabetic Dyslipidemia. Galicia-Garcia U, et al. PMC7503727. Licensed under CC BY 4.0.
- Figure 9 — Metabolic Syndrome Components. Sliwinska A, et al. PMC9479724. Licensed under CC BY-NC-ND 4.0.
- Figure 10 — Metabolic Syndrome Criteria. Sliwinska A, et al. PMC9479724. Licensed under CC BY-NC-ND 4.0.
- Figure 11 — Obesity and CV Risk Progression. Sliwinska A, et al. PMC9479724. Licensed under CC BY-NC-ND 4.0.
- Figure 12 — Modified WHO Analgesic Ladder. Pergolizzi JV, et al. PMC7038776. Licensed under CC BY-NC 3.0.
- Figure 13 — Disc Extrusion on MRI. Fairbank J, et al. PMC3756868. Licensed under CC BY 4.0.
- Figure 14 — Lumbar Disc Herniation Types. Fairbank J, et al. PMC3756868. Licensed under CC BY 4.0.
- Figure 15 — Lumbar Disc Herniation on MRI. Fairbank J, et al. PMC3756868. Licensed under CC BY 4.0.
- Figure 16 — Normal Knee Joint Anatomy. Latourte A, et al. PMC9604603. Licensed under CC BY 4.0.
- Figure 17 — Osteoarthritis Progression. Latourte A, et al. PMC9604603. Licensed under CC BY 4.0.
- Figure 18 — Lumbar Spinal Stenosis on MRI. Fairbank J, et al. PMC3756868. Licensed under CC BY 4.0.
- Figure 19 — Inflammatory Mediators in MSK Disease. Guszczyn T, et al. PMC7696673. Licensed under CC BY 4.0.
- Figure 20 — Treatment Algorithm. Sliwinska A, et al. PMC9479724. Licensed under CC BY-NC-ND 4.0.
- Figure 21 — Progressive Hippocampal Atrophy. Johnson KA, et al. PMC3312396. Licensed under CC BY 4.0.
- Figure 22 — FDG-PET Brain Imaging in AD. Johnson KA, et al. PMC3312396. Licensed under CC BY 4.0.
- Figure 23 — Immunopathogenesis of Atopic Dermatitis. Sroka-Tomaszewska J, et al. PMC8074061. Licensed under CC BY 4.0.
- Figure 24 — Targeted AD Therapies. Sroka-Tomaszewska J, et al. PMC8074061. Licensed under CC BY 4.0.
- Figure 25 — Clinical Manifestations of Psoriasis. Rendon A, Schakel K. PMC6471628. Licensed under CC BY 4.0.
- Figure 26 — Psoriasis Immunopathogenesis. Rendon A, Schakel K. PMC6471628. Licensed under CC BY 4.0.
- Figure 27 — Histopathology of Psoriasis. Rendon A, Schakel K. PMC6471628. Licensed under CC BY 4.0.
- Figure 28 — Knee Injection Landmarks. Choi YJ, et al. PMC3953519. Licensed under CC BY-NC 4.0.
- Figure 29 — Superolateral Knee Injection. Choi YJ, et al. PMC3953519. Licensed under CC BY-NC 4.0.
- Figure 30 — Normal Spirometry. Ruppel GL, et al. PMC6516140. Licensed under CC BY 4.0.
- Figure 31 — Obstructive Pattern on Spirometry. Ruppel GL, et al. PMC6516140. Licensed under CC BY 4.0.
- Figure 32 — Bronchodilator Reversibility. Ruppel GL, et al. PMC6516140. Licensed under CC BY 4.0.
Key Guidelines & Trials
- Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults. J Am Coll Cardiol. 2018;71(19):e127-e248. PMID: 29133356
- SPRINT Research Group. A Randomized Trial of Intensive versus Standard Blood-Pressure Control. N Engl J Med. 2015;373(22):2103-2116. PMID: 26551272
- American Diabetes Association Professional Practice Committee. Standards of Care in Diabetes — 2024. Diabetes Care. 2024;47(Suppl 1). PMID: 36507645
- Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol. Circulation. 2019;139(25):e1082-e1143. PMID: 30586774
- Bhatt DL, Steg PG, Miller M, et al. Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia (REDUCE-IT). N Engl J Med. 2019;380(1):11-22. PMID: 30415628
- Dowell D, Ragan KR, Jones CM, et al. CDC Clinical Practice Guideline for Prescribing Opioids for Pain — United States, 2022. MMWR Recomm Rep. 2022;71(3):1-95. PMID: 36327391
- US Preventive Services Task Force. Screening for Prediabetes and Type 2 Diabetes: US Preventive Services Task Force Recommendation Statement. JAMA. 2021;326(8):736-743. PMID: 30763518
- Jaddoe VWV, et al. Global Vascular Guidelines reference. Used for ASCVD risk framework. PMID: 31159978
- Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes (EMPA-REG OUTCOME). N Engl J Med. 2015;373(22):2117-2128. PMID: 26378978
- Marso SP, Daniels GH, Poulter NR, et al. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes (LEADER). N Engl J Med. 2016;375(4):311-322. PMID: 27295427
- Williams B, MacDonald TM, Morant SV, et al. Spironolactone versus placebo, bisoprolol, and doxazosin to determine the optimal treatment for drug-resistant hypertension (PATHWAY-2). Lancet. 2015;386(10008):2059-2068. PMID: 26414968
Textbooks & Reference Works
- Rakel's Textbook of Family Medicine. 10th ed. Rakel RE, Rakel DP, eds. Elsevier; 2021.
- Current Medical Diagnosis & Treatment (CMDT). Papadakis MA, McPhee SJ, eds. McGraw-Hill. Updated annually.
- Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents. 4th ed. Hagan JF, Shaw JS, Duncan PM, eds. AAP; 2017.
- Pfenninger and Fowler's Procedures for Primary Care. 4th ed. Pfenninger JL, Fowler GC, eds. Elsevier; 2019.