Every pathogen, syndrome, antimicrobial agent, resistance pattern, empiric regimen, prophylaxis strategy, and management algorithm in one place.
01 Microbiology Fundamentals
Infectious disease medicine rests on a foundation of microbiology — understanding how organisms are classified, how they cause disease, and how they evade host defenses and antimicrobial therapy. The Gram stain remains the single most important rapid diagnostic test in clinical microbiology, dividing bacteria into two major groups based on cell wall structure. Virulence factors determine pathogenicity, while resistance mechanisms dictate treatment choices. Mastery of these fundamentals is essential for rational empiric therapy and antimicrobial stewardship.
Gram Stain Classification
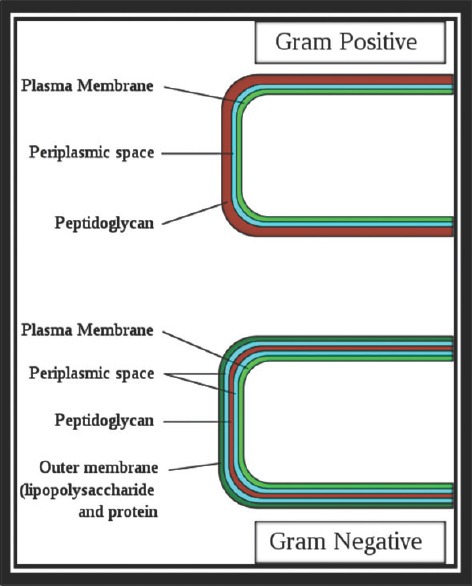
The Gram stain differentiates bacteria by cell wall composition. Gram-positive organisms retain the crystal violet–iodine complex due to a thick peptidoglycan layer (20–80 nm), appearing purple/blue. Gram-negative organisms have a thin peptidoglycan layer (1–3 nm) surrounded by an outer membrane containing lipopolysaccharide (LPS/endotoxin), and stain pink/red with the safranin counterstain.
Figure 1 — Bacterial Cell Envelope Structure. Comparison of Gram-positive and Gram-negative bacterial cell wall architecture, highlighting the thick peptidoglycan layer in Gram-positive organisms and the outer membrane with lipopolysaccharide in Gram-negative organisms.
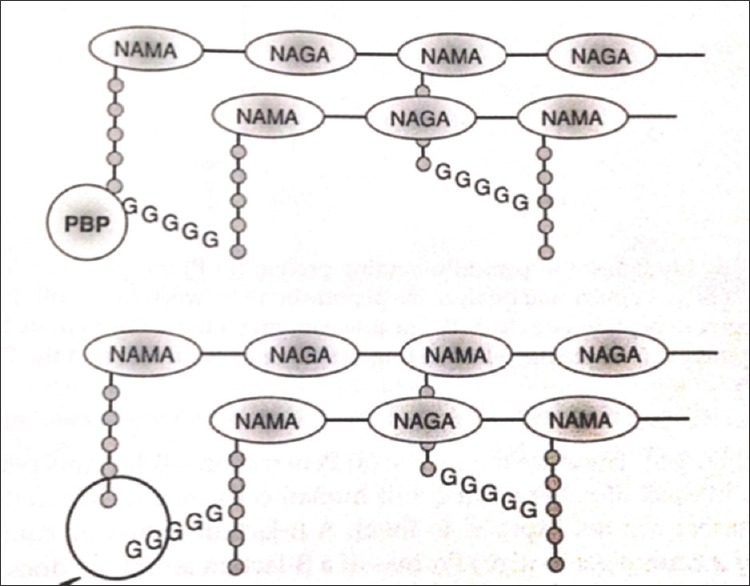
The cell wall is the primary target of many antibiotics. Peptidoglycan (murein) is the structural scaffold; beta-lactams inhibit its synthesis by binding penicillin-binding proteins (PBPs). Key virulence factors include:
Virulence Factor
Mechanism
Example Organisms
Endotoxin (LPS)
Lipid A triggers TLR4 → cytokine storm → septic shock
All Gram-negative bacteria
Exotoxins
Secreted proteins causing tissue damage
TSST-1 (S. aureus), Shiga toxin (EHEC), tetanospasmin (C. tetani)
Capsule
Antiphagocytic polysaccharide
S. pneumoniae, N. meningitidis, Klebsiella, H. influenzae type b
Biofilm
Sessile community on surfaces; 1000× increased antibiotic resistance
S. epidermidis (prosthetic devices), P. aeruginosa (CF lungs)
Protein A
Binds Fc portion of IgG → prevents opsonization
S. aureus
IgA protease
Cleaves mucosal IgA
N. meningitidis, N. gonorrhoeae, S. pneumoniae, H. influenzae
Pili/fimbriae
Adhesion to mucosal epithelium
E. coli (P fimbriae → pyelonephritis), N. gonorrhoeae
Figure 2 — Beta-Lactam Antibiotic Mechanism of Action. Diagram illustrating how beta-lactam antibiotics inhibit bacterial cell wall synthesis by binding penicillin-binding proteins (PBPs) and disrupting peptidoglycan cross-linking.
Antimicrobial Resistance Mechanisms
Mechanism
Description
Clinical Examples
Enzymatic inactivation
Bacteria produce enzymes that destroy/modify the antibiotic
PBP2a in MRSA (mecA gene), vanA/vanB in VRE, 23S rRNA methylation (macrolide resistance)
Efflux pumps
Active removal of antibiotic from cell
Tetracycline resistance, fluoroquinolone resistance in P. aeruginosa
Decreased permeability
Loss of outer membrane porins
Carbapenem resistance in P. aeruginosa (OprD loss), Acinetobacter
Target bypass
Alternative metabolic pathway circumvents inhibited step
Vancomycin resistance (D-Ala-D-Lac replaces D-Ala-D-Ala in VRE)
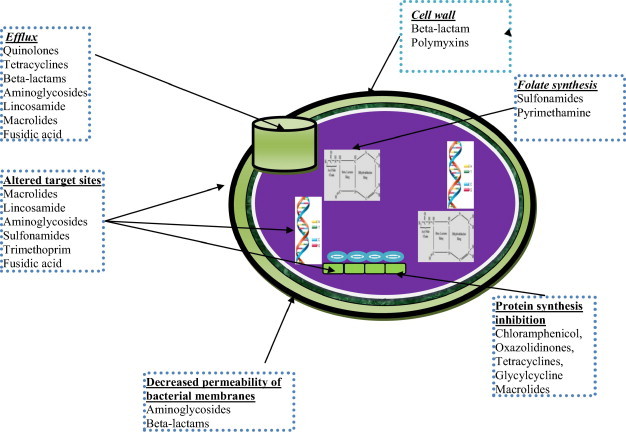
Figure 3 — Antimicrobial Resistance Mechanisms. Overview of how bacteria develop resistance to antibiotics, including enzymatic inactivation, target modification, efflux pumps, and decreased permeability.
The "ESKAPE" pathogens — Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, Enterobacter spp. — are the leading causes of nosocomial infections and are increasingly multidrug-resistant. These organisms "escape" the effects of commonly used antibiotics.
When Gram stain shows Gram-negative diplococci in CSF, treat for N. meningitidis immediately. When it shows Gram-positive diplococci, think S. pneumoniae. Gram-positive rods in blood cultures from an elderly or immunocompromised patient should prompt concern for Listeria monocytogenes.
02 The Infectious Disease Assessment
The systematic evaluation of a patient with suspected infection involves identifying the source, the likely pathogen, and the severity of illness. The fever workup, blood culture interpretation, and sepsis screening tools are the cornerstones of ID assessment.
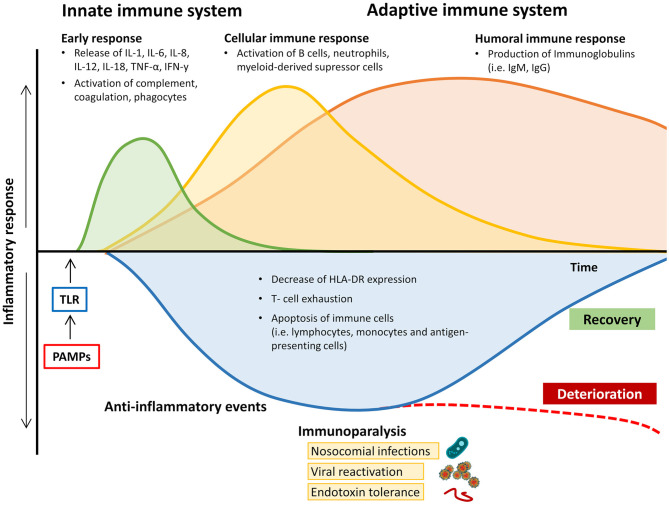
Figure 33 — Inflammatory Response Trajectory in Sepsis. The dynamic balance between pro-inflammatory and anti-inflammatory immune responses during sepsis progression, from the initial hyperinflammatory phase through the immunosuppressive phase, illustrating why timely assessment and intervention are critical.
Fever Workup
Fever is defined as a core body temperature ≥38.0°C (100.4°F). In elderly and immunocompromised patients, fever may be absent despite serious infection (hypothermia <36°C may indicate sepsis). A systematic approach to fever includes:
Step
Action
Details
1. History
Characterize the fever
Onset, duration, pattern (continuous, intermittent, relapsing), associated symptoms, travel, exposures, sexual history, IV drug use, immunosuppression
2. Physical exam
Source identification
Skin (rash, wounds, IV sites), lungs (crackles, consolidation), heart (new murmur), abdomen (tenderness, peritonitis), joints, meninges (nuchal rigidity)
3. Basic labs
CBC, CMP, lactate, procalcitonin
Leukocytosis (or leukopenia in sepsis), left shift, thrombocytopenia, elevated lactate, AKI
4. Cultures
Blood cultures (2 sets from separate sites), urine culture, sputum culture
Repeat cultures; if clinical concern, treat and investigate (line infection)
2/2 bottles positive for CoNS
More likely true infection, especially with central line
Treat as line infection; consider line removal
Any bottle positive for S. aureus, S. lugdunensis, or Candida
Always true pathogen
Full workup: repeat cultures, echocardiography, source control
Polymicrobial (GNR + anaerobes)
Suggests GI source (perforation, abscess)
CT abdomen/pelvis, surgical consultation
S. aureus bacteremia (SAB) is never a contaminant. Every patient with SAB requires: (1) repeat blood cultures every 48 hours until clearance, (2) echocardiography (TEE preferred), (3) evaluation for metastatic foci, and (4) a minimum of 2 weeks IV therapy for uncomplicated SAB, 4–6 weeks if complicated (endocarditis, osteomyelitis, deep-seated focus). ID consultation for SAB reduces mortality.
Sepsis Screening — qSOFA
The quick SOFA (qSOFA) is a bedside screening tool for patients with suspected infection outside the ICU. A score ≥2 identifies patients at risk for poor outcomes:
Criterion
Points
Respiratory rate ≥22/min
1
Altered mentation (GCS <15)
1
Systolic blood pressure ≤100 mmHg
1
qSOFA ≥2 has a specificity of ~70% for in-hospital mortality in non-ICU patients with suspected infection. It is a screening tool — the full SOFA score is required for the formal Sepsis-3 definition.
LP (if no contraindication), blood cultures, CT head first if focal deficits
Erythema/warmth around catheter site
Catheter-related BSI
Paired peripheral and catheter cultures, differential time to positivity
Abdominal pain with peritoneal signs
Intra-abdominal abscess/peritonitis
CT abdomen/pelvis with contrast
03 Key Terminology & Abbreviations
Term
Definition
Bacteremia
Presence of viable bacteria in the bloodstream, confirmed by positive blood culture
Sepsis (Sepsis-3)
Life-threatening organ dysfunction caused by dysregulated host response to infection; SOFA score ≥2
Septic shock
Subset of sepsis with vasopressor requirement to maintain MAP ≥65 AND lactate >2 mmol/L despite adequate fluid resuscitation
Empiric therapy
Initial antibiotic regimen chosen before organism identification, based on suspected source and local resistance patterns
De-escalation
Narrowing antibiotic spectrum once culture and sensitivity results are available
MIC
Minimum inhibitory concentration — lowest concentration of antibiotic that prevents visible bacterial growth
Bactericidal
Antibiotic that kills bacteria (MBC/MIC ratio ≤4); required for endocarditis, meningitis, neutropenic fever
Bacteriostatic
Antibiotic that inhibits bacterial growth without killing; host immune system completes eradication
MDR
Multidrug-resistant — resistant to ≥1 agent in ≥3 antimicrobial categories
ESBL
Extended-spectrum beta-lactamase — enzyme conferring resistance to 3rd-generation cephalosporins; treat with carbapenems
CRE
Carbapenem-resistant Enterobacterales — resistant to carbapenems via carbapenemases (KPC, NDM, OXA-48)
ABxAntibioticsAMSAltered mental statusARTAntiretroviral therapyBCxBlood cultureBSIBloodstream infectionCAPCommunity-acquired pneumoniaCDIClostridioides difficile infectionCMVCytomegalovirusCNSCentral nervous systemCoNSCoagulase-negative staphylococciCRBSICatheter-related bloodstream infectionCRECarbapenem-resistant EnterobacteralesCSFCerebrospinal fluidDOTDirectly observed therapyESBLExtended-spectrum beta-lactamaseFMTFecal microbiota transplantationFUOFever of unknown originGASGroup A StreptococcusGBSGroup B StreptococcusHAPHospital-acquired pneumoniaHSVHerpes simplex virusIDInfectious diseaseIGRAInterferon-gamma release assayINSTIIntegrase strand transfer inhibitorLPLumbar punctureMACMycobacterium avium complexMDRMultidrug-resistantMICMinimum inhibitory concentrationMRSAMethicillin-resistant S. aureusMSSAMethicillin-susceptible S. aureusOIOpportunistic infectionPCP/PJPPneumocystis jirovecii pneumoniaPEPPost-exposure prophylaxisPrEPPre-exposure prophylaxisRIPERifampin, Isoniazid, Pyrazinamide, EthambutolSABS. aureus bacteremiaSOFASequential Organ Failure AssessmentSSTISkin and soft tissue infectionTBTuberculosisTDMTherapeutic drug monitoringTEETransesophageal echocardiographyTMP-SMXTrimethoprim-sulfamethoxazoleVAPVentilator-associated pneumoniaVREVancomycin-resistant Enterococcus
04 Sepsis & Septic Shock
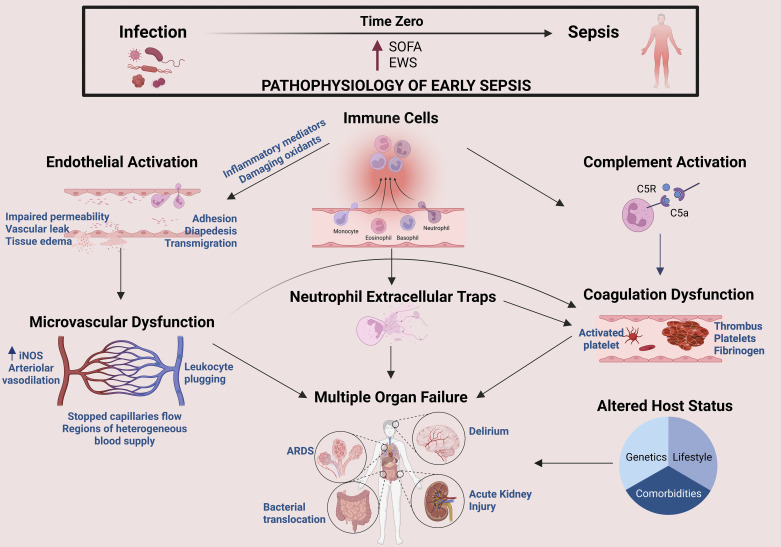
Sepsis is a medical emergency defined by the Sepsis-3 consensus (2016) as life-threatening organ dysfunction caused by a dysregulated host response to infection. It affects over 1.7 million adults annually in the United States, with a mortality rate of 15–30% for sepsis and 40–50% for septic shock.
Figure 4 — Sepsis Pathophysiology. The critical transition from infection to sepsis at the molecular level, depicting how host-defense mediators trigger immune responses affecting the complement system, endothelium, and microvasculature, leading to organ dysfunction.
All elements should be initiated within 1 hour of sepsis recognition:
1. Measure lactate — remeasure if initial lactate >2 mmol/L
2. Obtain blood cultures before antibiotics (do not delay ABx if cultures cannot be obtained promptly)
3. Administer broad-spectrum antibiotics — each hour of delay increases mortality by ~4%
4. Begin rapid fluid resuscitation — 30 mL/kg crystalloid for hypotension or lactate ≥4 mmol/L
5. Start vasopressors if hypotension persists during or after fluid resuscitation — target MAP ≥65 mmHg
Sepsis-3 Definitions
Term
Definition
Criteria
Sepsis
Infection + organ dysfunction
Suspected or documented infection with acute change in SOFA score ≥2 points
Septic shock
Subset of sepsis with circulatory and metabolic failure
Sepsis + vasopressor requirement to maintain MAP ≥65 mmHg AND serum lactate >2 mmol/L despite adequate volume resuscitation
SOFA Score (Sequential Organ Failure Assessment)
Organ System
0
1
2
3
4
Respiration (PaO2/FiO2)
≥400
<400
<300
<200 with ventilatory support
<100 with ventilatory support
Coagulation (platelets ×10³/µL)
≥150
<150
<100
<50
<20
Liver (bilirubin, mg/dL)
<1.2
1.2–1.9
2.0–5.9
6.0–11.9
>12
Cardiovascular (MAP/vasopressors)
MAP ≥70
MAP <70
Dopamine ≤5 or dobutamine any dose
Dopamine >5 or epi/norepi ≤0.1
Dopamine >15 or epi/norepi >0.1
CNS (GCS)
15
13–14
10–12
6–9
<6
Renal (creatinine mg/dL or UOP)
<1.2
1.2–1.9
2.0–3.4
3.5–4.9 or UOP <500 mL/d
>5.0 or UOP <200 mL/d
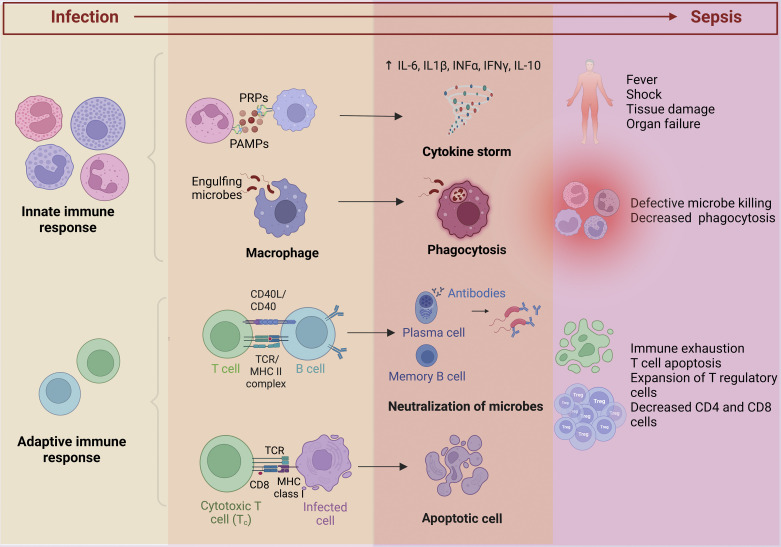
Figure 5 — Immune Activation and Suppression in Sepsis. Dual immune response in sepsis: systemic immune activation producing a cytokine storm (leading to fever, shock, and organ dysfunction) alongside sepsis-induced immunosuppression with apoptotic depletion and immune cell exhaustion.
Vasopressor Selection in Septic Shock
Agent
Receptor
Role
Dose Range
Norepinephrine
α1 >> β1
First-line vasopressor
0.01–3 µg/kg/min
Vasopressin
V1
Second-line, added to norepinephrine (catecholamine-sparing)
0.03–0.04 units/min (fixed dose)
Epinephrine
α1, β1, β2
Second/third-line; also for anaphylactic shock
0.01–0.5 µg/kg/min
Phenylephrine
Pure α1
Alternative if tachyarrhythmia limits norepinephrine use
0.5–6 µg/kg/min
Angiotensin II
AT1 receptor
Refractory vasodilatory shock
20–200 ng/kg/min
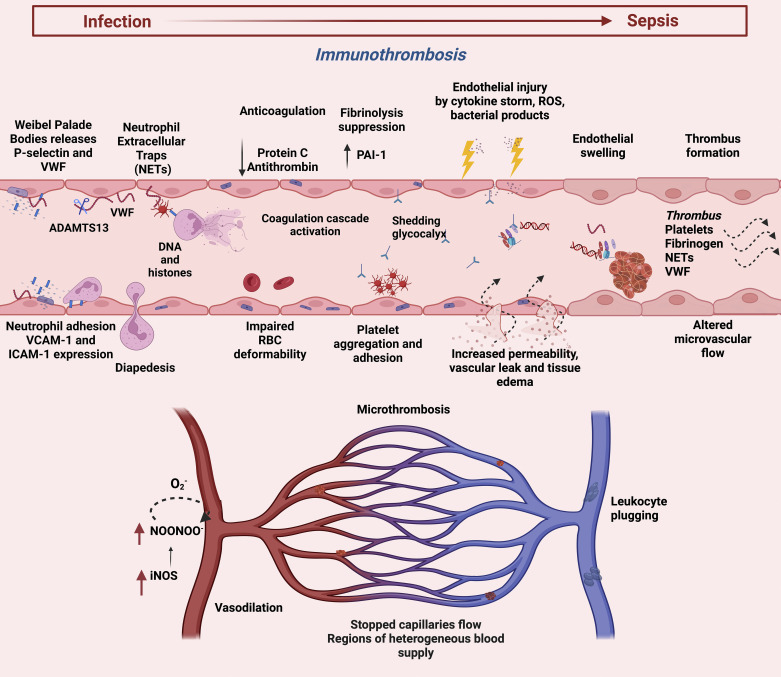
Figure 6 — Endothelial and Coagulation Dysfunction in Sepsis. Endothelial activation in sepsis showing Weibel-Palade body release, platelet-neutrophil interactions, neutrophil extracellular trap (NET) formation, and the cascade leading to increased vascular permeability and microthrombosis.
Lactate-Guided Resuscitation
Serum lactate reflects tissue hypoperfusion and anaerobic metabolism. A target of lactate clearance ≥20% every 2 hours (or normalization <2 mmol/L) guides adequacy of resuscitation. Persistently elevated lactate despite resuscitation suggests ongoing tissue hypoperfusion, mesenteric ischemia, hepatic dysfunction, or catecholamine excess.
Do not delay antibiotics for imaging or procedures. In septic shock, every hour of delayed antibiotic administration increases mortality by approximately 4–8%. Draw blood cultures first, but if venipuncture will take time, start antibiotics immediately and draw cultures as soon as possible thereafter.
Corticosteroids in Septic Shock
The Surviving Sepsis Campaign (2021) suggests IV hydrocortisone 200 mg/day (50 mg q6h or continuous infusion) for patients with septic shock who remain vasopressor-dependent despite adequate fluid resuscitation. The ADRENAL and APROCCHSS trials showed modest reduction in time to shock reversal but inconsistent mortality benefit. Consider initiating when norepinephrine dose reaches ≥0.25 µg/kg/min.
05 Bloodstream Infections & Bacteremia
Catheter-Related Bloodstream Infections (CRBSI)
Central venous catheters account for ~250,000 BSIs annually in the U.S. Diagnosis requires differential time to positivity (DTP) — blood cultures drawn through the catheter turn positive ≥2 hours before peripheral cultures, suggesting the catheter as the source.
Pathogen
Frequency
Line Removal?
Treatment
CoNS
~35%
Try salvage with lock therapy if uncomplicated
Vancomycin 7–14 days
S. aureus
~15%
Always remove the line
Nafcillin/cefazolin (MSSA) or vancomycin (MRSA) × 4–6 weeks
Enterococcus
~10%
Remove if possible
Ampicillin (if susceptible) or vancomycin × 7–14 days
Gram-negative rods
~20%
Remove if possible
Directed therapy × 7–14 days
Candida spp.
~10%
Always remove the line
Echinocandin × 14 days after first negative BCx + ophthalmologic exam
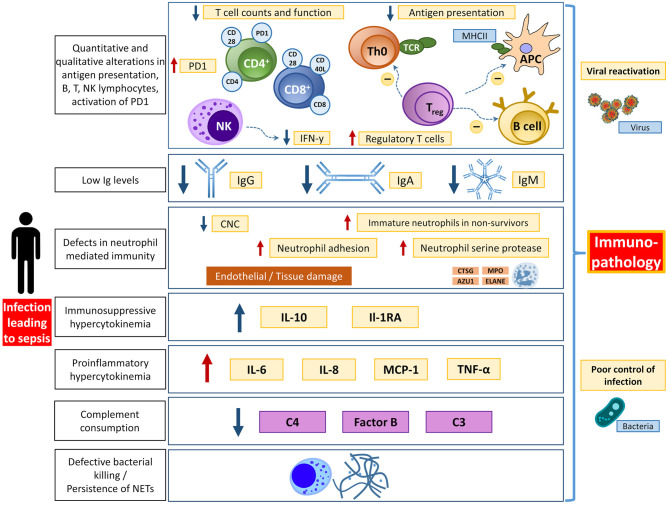
Figure 34 — Immunological Dysfunction in Sepsis. Comprehensive overview of the different aspects of immunological dysfunction during sepsis, including complement activation, coagulation cascade derangements, endothelial injury, and cellular immune suppression that collectively drive multi-organ failure.
Candidemia
Candida in blood cultures is never a contaminant. Management: (1) remove all central venous catheters, (2) start echinocandin empirically (micafungin 100 mg IV daily or caspofungin 70 mg load then 50 mg daily), (3) obtain ophthalmologic exam to evaluate for endophthalmitis, (4) repeat blood cultures daily until clearance, (5) treat for 14 days after first negative blood culture. Fluconazole can be used for step-down if the species is susceptible (C. albicans, C. parapsilosis) and the patient is clinically stable.
C. auris is an emerging multidrug-resistant Candida species that is often resistant to fluconazole, variably resistant to amphotericin B, and occasionally resistant to echinocandins. It persists on surfaces and skin, causing nosocomial outbreaks. Contact precautions and aggressive environmental cleaning are essential.
S. aureus Bacteremia — Mandatory Workup
Component
Details
Repeat blood cultures
Every 48 hours until negative; duration of therapy starts from first negative culture
Echocardiography
TEE preferred (sensitivity 90–95% vs TTE 50–70% for vegetations); TTE acceptable if low-risk
Source investigation
CT/MRI for metastatic foci (vertebral osteomyelitis, epidural abscess, splenic abscess)
ID consultation
Shown to reduce mortality by 50% and improve adherence to evidence-based care
Uncomplicated SAB
Removable focus + negative TEE + negative follow-up cultures at 48–72h + no metastatic infection + no prosthetic material → 2 weeks IV therapy
Complicated SAB
Any of: positive follow-up cultures at 72h, endocarditis, metastatic infection, prosthetic material → 4–6 weeks IV therapy
06 Fever of Unknown Origin
Fever of unknown origin (FUO) was classically defined by Petersdorf and Beeson (1961) as fever >38.3°C on multiple occasions, lasting >3 weeks, with no diagnosis after 1 week of inpatient evaluation. Modern definitions allow outpatient workup. The etiology falls into four major categories: infections (~30%), malignancy (~20%), autoimmune/inflammatory (~15%), and undiagnosed (~25%).
FUO Categories
Type
Definition
Common Etiologies
Classic FUO
Fever >3 weeks, no diagnosis after appropriate workup
TB, endocarditis, intra-abdominal abscess, lymphoma, adult Still disease, temporal arteritis
Nosocomial FUO
Hospitalized ≥24h, fever developing after admission, no infection at admission
C. difficile, catheter-related infection, drug fever, DVT/PE, sinusitis (intubated), acalculous cholecystitis
Neutropenic FUO
ANC <500/µL with fever ≥38.3°C, no identifiable source after 3 days
HIV-positive with fever >4 weeks (outpatient) or >3 days (inpatient)
MAC (CD4 <50), CMV, PJP, lymphoma, TB, histoplasmosis
Diagnostic Approach to Classic FUO
Phase
Investigations
Initial
CBC with differential, CMP, ESR, CRP, LDH, ferritin, blood cultures ×3, urinalysis/culture, CXR, HIV test, ANA, RF
Directed
CT chest/abdomen/pelvis, TTE/TEE (if murmur or risk factors), peripheral smear, serum protein electrophoresis
Advanced
FDG-PET/CT (excellent for localizing occult infection or malignancy), bone marrow biopsy, temporal artery biopsy (if age >55 with elevated ESR), liver biopsy
FDG-PET/CT has become a valuable tool in FUO workup, with a diagnostic yield of 40–70% in identifying the source when conventional imaging is negative. It is particularly useful for detecting large-vessel vasculitis, occult abscesses, and lymphoma.
Drug fever should always be considered in hospitalized patients with FUO. Classic culprits include beta-lactams, sulfonamides, anticonvulsants, and allopurinol. The patient may appear "inappropriately well" with relative bradycardia and eosinophilia. The fever typically resolves within 48–72 hours of drug discontinuation.
07 Community-Acquired Pneumonia
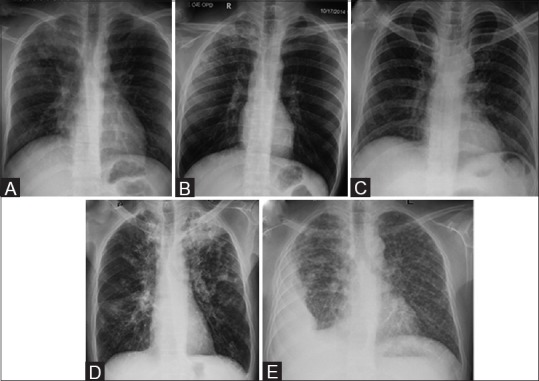
Community-acquired pneumonia (CAP) is the leading infectious cause of death worldwide. The 2019 ATS/IDSA guidelines emphasize severity-based empiric therapy, covering typical and atypical pathogens, with risk stratification using validated scoring systems.
Figure 7 — Chest Radiograph Findings in Pulmonary Infection. Representative chest radiographs demonstrating lobar consolidation, air bronchograms, and other characteristic findings of bacterial pneumonia that guide initial clinical assessment and management.
Beta-lactam (ampicillin-sulbactam 3 g q6h, ceftriaxone 1–2 g q24h, or cefotaxime) PLUS macrolide (azithromycin 500 mg daily); OR respiratory FQ alone
Duration 5–7 days
ICU (severe CAP)
Beta-lactam (ceftriaxone or ampicillin-sulbactam) PLUS macrolide; OR beta-lactam PLUS respiratory FQ
Add vancomycin + piperacillin-tazobactam if MRSA/Pseudomonas risk factors
ATS/IDSA 2019 no longer recommends routine MRSA or Pseudomonas coverage for CAP unless the patient has risk factors (prior respiratory isolation of these organisms, recent hospitalization with parenteral antibiotics). Always obtain cultures and procalcitonin before starting antibiotics when possible.
Hospital-acquired pneumonia (HAP) develops ≥48 hours after hospital admission and was not incubating at the time of admission. Ventilator-associated pneumonia (VAP) develops ≥48 hours after endotracheal intubation. Both carry mortality rates of 20–50%.
Figure 35 — Genetic and Biochemical Basis of Antibiotic Resistance. Diagram illustrating the biochemical and genetic mechanisms underlying antibiotic resistance, including plasmid-mediated transfer of resistance genes, beta-lactamase production, and efflux pump overexpression — key factors driving MDR HAP/VAP pathogens.
Risk Factors for MDR Pathogens
MRSA Risk Factors
Pseudomonas Risk Factors
Prior MRSA isolation
Prior Pseudomonas isolation
IV antibiotic use within 90 days
IV antibiotic use within 90 days
High MRSA prevalence unit (>20%)
Structural lung disease (bronchiectasis, CF)
Hemodialysis
Prolonged mechanical ventilation
Empiric Therapy (ATS/IDSA 2016)
Risk Category
Regimen
HAP/VAP, no MDR risk, low mortality risk
Piperacillin-tazobactam 4.5 g q6h OR cefepime 2 g q8h OR meropenem 1 g q8h
HAP/VAP with MRSA risk
Above PLUS vancomycin (trough 15–20 µg/mL or AUC/MIC 400–600) OR linezolid 600 mg q12h
HAP/VAP with Pseudomonas risk
2 anti-pseudomonal agents from different classes (e.g., pip-tazo + tobramycin, or cefepime + ciprofloxacin)
HAP/VAP with both MRSA + Pseudomonas risk
Anti-pseudomonal beta-lactam + anti-pseudomonal agent from 2nd class + MRSA coverage
VAP prevention bundle: head-of-bed elevation 30–45°, daily sedation vacation and spontaneous breathing trial, oral chlorhexidine, DVT and stress ulcer prophylaxis, daily assessment for extubation readiness. These measures together reduce VAP rates by 40–70%.
VAP Diagnostic Criteria
Clinical diagnosis: new or progressive infiltrate on CXR plus ≥2 of: fever >38°C, leukocytosis (>12,000) or leukopenia (<4,000), purulent secretions. The Clinical Pulmonary Infection Score (CPIS) ≥6 suggests VAP. Obtain lower respiratory tract cultures (endotracheal aspirate with semi-quantitative culture or BAL with quantitative culture ≥10&sup4; CFU/mL) before changing antibiotics.
09 Tuberculosis
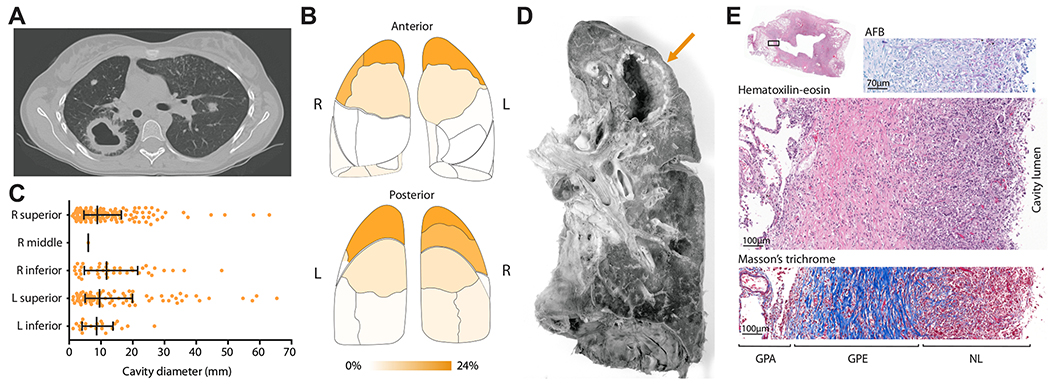
Tuberculosis (TB), caused by Mycobacterium tuberculosis, remains a leading infectious killer globally, with ~10 million new cases and 1.5 million deaths annually. One-quarter of the world's population is latently infected. In the United States, TB disproportionately affects foreign-born individuals, people experiencing homelessness, and the immunocompromised.
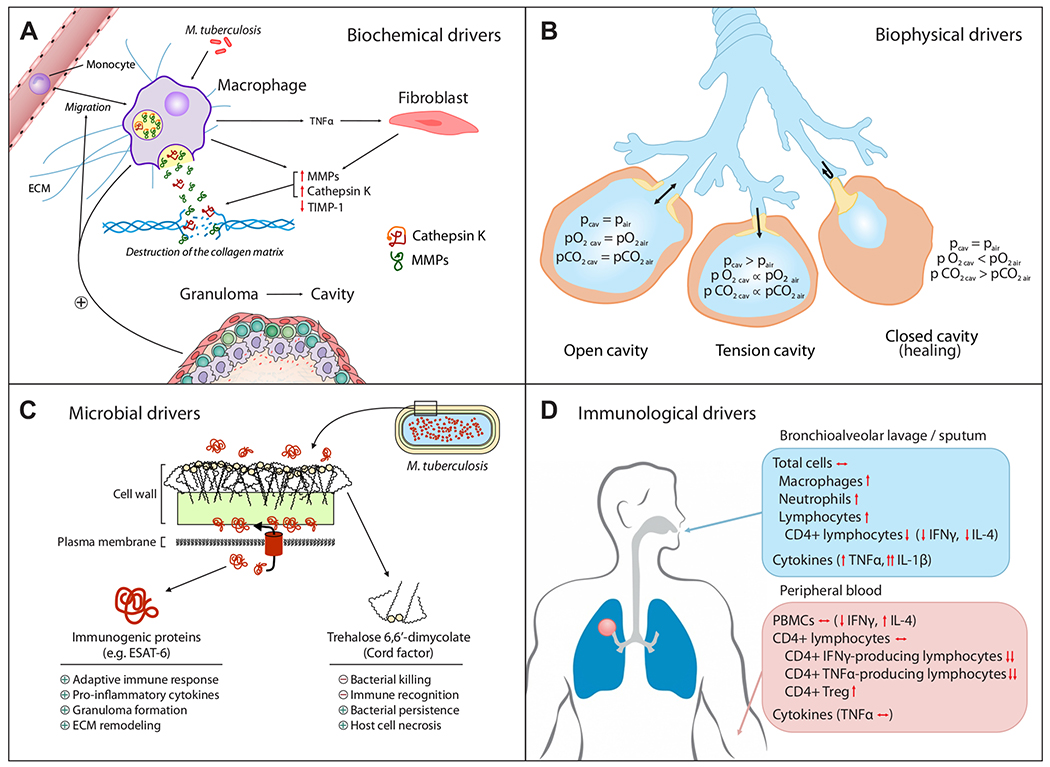
Figure 8 — Architecture of Tuberculosis Cavities. CT-scan reconstruction and histological cross-section of TB cavity wall, showing cavity location, size distribution across bronchopulmonary segments, and the structural features that make cavitary TB difficult to treat.
Latent TB Infection (LTBI) vs Active TB
Feature
Latent TB (LTBI)
Active TB
Symptoms
None
Cough >2–3 weeks, hemoptysis, night sweats, weight loss, fever
Usually positive (may be negative if severely immunosuppressed)
Treatment goal
Prevent reactivation
Cure infection, prevent transmission
Screening: TST vs IGRA
Test
Mechanism
Advantages
Limitations
TST (Mantoux/PPD)
Intradermal injection of purified protein derivative; read at 48–72 hours
Inexpensive, widely available
Cross-reacts with BCG and NTM; requires return visit; reader variability
IGRA (QuantiFERON, T-SPOT)
Measures interferon-gamma release from T cells stimulated by TB-specific antigens (ESAT-6, CFP-10)
Single blood draw; not affected by BCG; more specific
More expensive; may have indeterminate results in immunosuppressed
TST interpretation (induration cutoffs): ≥5 mm = positive in HIV, close contacts, immunosuppressed, CXR with old TB. ≥10 mm = recent immigrants, IVDU, healthcare workers, high-risk congregate settings. ≥15 mm = no known risk factors.
Active TB Treatment — Standard 4-Drug RIPE Regimen
Hepatotoxicity (#1 cause of drug-induced liver injury), peripheral neuropathy (give pyridoxine/B6 25–50 mg daily)
Pyrazinamide
Z
25 mg/kg (max 2 g)
First 2 months only
Hepatotoxicity, hyperuricemia/gout, arthralgias
Ethambutol
E
15–20 mg/kg
First 2 months only (or until susceptibilities confirmed)
Optic neuritis (red-green color discrimination — baseline and monthly visual acuity testing)
Standard regimen: 2 months RIPE (intensive phase) → 4 months RI (continuation phase) = 6 months total. Extend to 9 months if cavitary disease AND positive 2-month sputum culture.
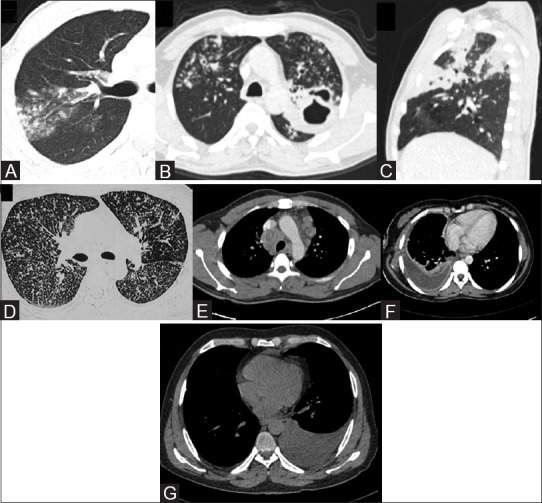
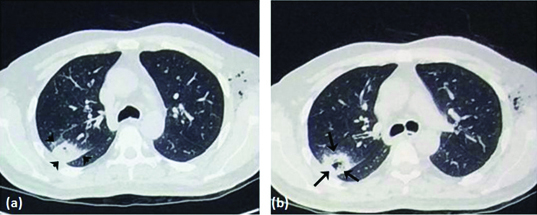
Figure 9 — CT Findings in Active Pulmonary Tuberculosis. High-resolution CT imaging demonstrating characteristic findings of active TB including upper lobe infiltrates, cavitation, tree-in-bud pattern, and centrilobular nodules that distinguish active from latent disease.
All patients with active TB should be on respiratory isolation (airborne precautions: negative-pressure room, N95 respirator for healthcare workers). Isolation can be discontinued after clinical improvement, 3 consecutive negative AFB sputum smears collected 8–24 hours apart, and a reliable treatment plan in place.
LTBI Treatment Regimens
Regimen
Duration
Dosing
Notes
3HP (preferred)
3 months (12 doses)
Isoniazid + rifapentine weekly (DOT)
Highest completion rates; not for HIV on PIs or children <2y
4R
4 months
Rifampin daily
Good alternative; fewer hepatotoxicity than 9H
9H
9 months
Isoniazid daily
Older standard; low completion rates
Figure 10 — Drivers of Pulmonary Cavitation in TB. Overview of the biochemical, biophysical, microbial, and immunological processes that drive cavity formation in tuberculosis, a key factor in disease transmission and treatment challenges.
MDR-TB & XDR-TB
MDR-TB: resistant to at least isoniazid + rifampin. XDR-TB: MDR-TB + resistance to a fluoroquinolone + at least one injectable agent (or bedaquiline/linezolid). Treatment requires 4–6 drugs for 18–20 months (newer regimens with bedaquiline, pretomanid, and linezolid [BPaL] allow shorter 6–9 month courses). ID and public health involvement is mandatory.
10 Fungal Pneumonia & Opportunistic Infections
Pneumocystis jirovecii Pneumonia (PJP)
PJP occurs in severely immunocompromised patients, classically HIV with CD4 <200 cells/µL. Presentation: gradual-onset dyspnea, dry cough, fever, bilateral ground-glass opacities on CT. Elevated LDH and (1,3)-beta-D-glucan support diagnosis. Confirmed by silver stain or DFA of induced sputum or BAL.
Severity
Treatment
Adjunctive Therapy
Mild-moderate (PaO2 >70, A-a gradient <35)
TMP-SMX 15–20 mg/kg/day (TMP component) PO divided q8h × 21 days
None required
Moderate-severe (PaO2 ≤70 or A-a gradient ≥35)
TMP-SMX 15–20 mg/kg/day IV divided q6–8h × 21 days
Prednisone 40 mg BID × 5d, then 40 mg daily × 5d, then 20 mg daily × 11d (reduces mortality if started within 72h)
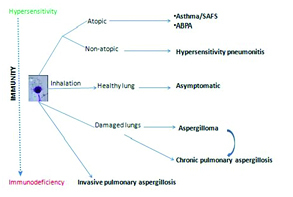
Figure 11 — Spectrum of Pulmonary Aspergillosis. Schematic diagram showing the range of pulmonary aspergillosis presentations from allergic bronchopulmonary aspergillosis (ABPA) to invasive disease, correlated with host immune status from immunocompetent to severely immunosuppressed.
Invasive Aspergillosis
Occurs in prolonged neutropenia (ANC <500 for >10 days), solid organ/stem cell transplant, high-dose corticosteroids. Classic CT finding: halo sign (early) and air crescent sign (recovery phase, ~2–3 weeks). Diagnose with serum/BAL galactomannan antigen and culture. Treatment: voriconazole 6 mg/kg IV q12h × 2 doses, then 4 mg/kg IV q12h (target trough 2–5.5 µg/mL). Alternative: isavuconazole or liposomal amphotericin B.
Figure 12 — Halo Sign and Air Crescent Sign in Invasive Aspergillosis. Chronological CT findings of angioinvasive aspergillosis: the early halo sign (ground-glass attenuation surrounding a dense nodule representing hemorrhage) progressing to the air crescent sign during neutrophil recovery, a hallmark of this fungal infection.
In HIV patients with cryptococcal meningitis, elevated intracranial pressure is the primary cause of early mortality. Therapeutic lumbar punctures should be performed daily to maintain opening pressure <20 cm H2O. Serial large-volume (20–30 mL) LPs or a lumbar drain may be necessary. Do NOT start ART immediately — wait 4–6 weeks to reduce risk of immune reconstitution inflammatory syndrome (IRIS).
11 Bacterial Meningitis
Emergency — Bacterial Meningitis
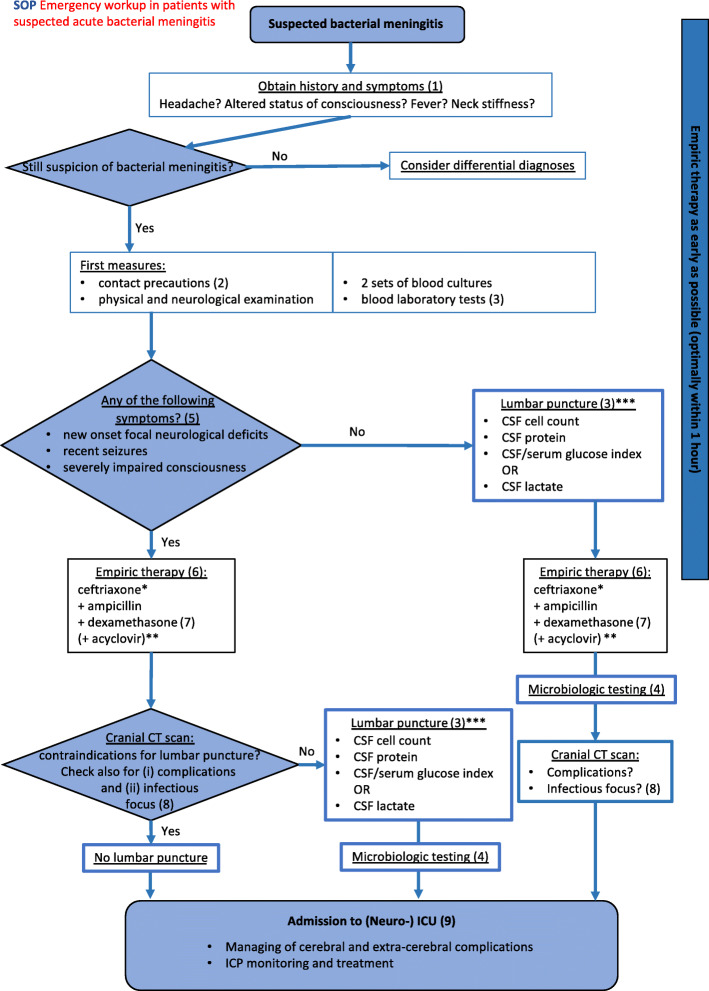
Bacterial meningitis is a medical emergency with mortality of 15–25% and neurologic sequelae in 30–50% of survivors. If suspected: blood cultures → empiric antibiotics + dexamethasone → lumbar puncture (in that order). Do NOT delay antibiotics for LP or CT. CT head before LP only if: immunocompromised, history of CNS disease, new-onset seizure, papilledema, altered consciousness, or focal neurologic deficit.
Figure 13 — Clinical Pathway for Suspected Bacterial Meningitis. Emergency department algorithm for the workup and management of suspected bacterial meningitis, including decision points for CT before lumbar puncture, empiric antibiotic timing, and dexamethasone administration.
CSF Analysis in Meningitis
Parameter
Normal
Bacterial
Viral
TB/Fungal
Opening pressure
10–20 cm H2O
>25 (often >30)
Normal or mildly elevated
Elevated
WBC (/µL)
<5
1,000–10,000+ (neutrophil predominant)
50–1,000 (lymphocyte predominant)
50–500 (lymphocyte predominant)
Glucose (mg/dL)
45–80 (CSF/serum ratio ≥0.6)
<40 (ratio <0.4)
Normal
Low
Protein (mg/dL)
15–45
>250
50–200
100–500
Gram stain
No organisms
Positive in 60–90%
Negative
AFB smear sensitivity ~10–40% (TB); India ink ~50% (Crypto)
Empiric Antibiotic Therapy by Age Group
Age Group
Common Pathogens
Empiric Regimen
Neonates (<1 month)
GBS, E. coli, Listeria
Ampicillin + gentamicin (or cefotaxime)
Infants/children (1 mo–18 y)
S. pneumoniae, N. meningitidis, H. influenzae type b
Dexamethasone 0.15 mg/kg IV q6h × 4 days, given 15–20 minutes BEFORE or with the first dose of antibiotics. Proven to reduce mortality and hearing loss in S. pneumoniae meningitis in adults (de Gans trial, NEJM 2002). Continue only if Gram stain or culture confirms pneumococcal meningitis. Discontinue if another organism is identified.
N. meningitidis Chemoprophylaxis
Close contacts of patients with meningococcal meningitis require prophylaxis within 24 hours:
Agent
Dose
Notes
Rifampin
600 mg PO q12h × 2 days
Not for pregnant women
Ciprofloxacin (preferred for adults)
500 mg PO × 1 dose
Single dose, most convenient
Ceftriaxone
250 mg IM × 1 dose
Preferred in pregnancy and children
The index patient treated with ceftriaxone does NOT need additional chemoprophylaxis (ceftriaxone eradicates nasopharyngeal carriage). If treated with penicillin, the patient should also receive chemoprophylaxis before discharge.
12 Viral Encephalitis
HSV Encephalitis
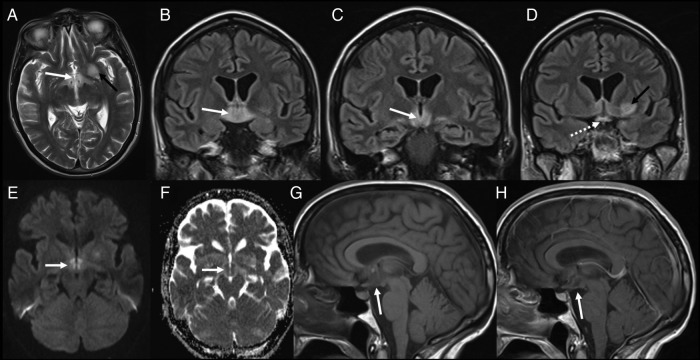
HSV-1 encephalitis is the most common cause of sporadic fatal encephalitis in the United States. It classically involves the temporal lobes (bilateral but asymmetric). Presentation: acute onset fever, headache, altered mental status, seizures, focal neurologic deficits, personality changes.
Figure 14 — MRI Findings in HSV Encephalitis. T2/FLAIR, DWI, and ADC MRI sequences demonstrating characteristic temporal lobe involvement in herpes simplex encephalitis, with signal abnormality, restricted diffusion, and gyral swelling — key findings that support early clinical diagnosis.
Emergency — HSV Encephalitis
Start IV acyclovir 10 mg/kg q8h immediately upon clinical suspicion — do not wait for LP or MRI results. Untreated mortality is ~70%; with early acyclovir, mortality drops to 20–30%. Continue for 14–21 days.
Diagnostic Test
Finding
CSF analysis
Lymphocytic pleocytosis (10–500 WBC), elevated protein, normal glucose, RBCs may be present (hemorrhagic necrosis)
CSF HSV PCR
Gold standard; sensitivity ~98%, specificity ~99%. May be negative in first 24–72 hours — if high suspicion, repeat LP in 3–7 days
MRI brain
T2/FLAIR hyperintensity in medial temporal lobes (bilateral but asymmetric), insular cortex, orbitofrontal regions; may show hemorrhage
EEG
Periodic lateralized epileptiform discharges (PLEDs) in temporal region
Summer/fall; children; aseptic meningitis more than encephalitis
CSF enterovirus PCR
Supportive
VZV
Immunocompromised; may occur without rash; vasculopathy, cerebellitis
CSF VZV PCR, VZV IgG
IV acyclovir 10–15 mg/kg q8h
CMV
HIV with CD4 <50; ventriculoencephalitis
CSF CMV PCR
Ganciclovir + foscarnet
Rabies
Animal bite exposure; hydrophobia, aerophobia, encephalitic or paralytic form; almost uniformly fatal once symptomatic
Nuchal skin biopsy (DFA), saliva PCR
Post-exposure prophylaxis (PEP): wound care + rabies immunoglobulin + vaccine series
13 Brain Abscess & Epidural Abscess
Brain Abscess
Brain abscess arises from contiguous spread (sinusitis, otitis, dental infection), hematogenous dissemination (endocarditis, lung abscess, IVDU), or post-neurosurgical/trauma. Classic triad (present in <50%): headache, fever, focal neurologic deficit. Organisms depend on source: contiguous — Streptococcus, anaerobes; hematogenous — S. aureus, Streptococcus; immunocompromised — Toxoplasma, Nocardia, Aspergillus.
Feature
Details
Imaging
MRI with contrast (gold standard): ring-enhancing lesion with restricted diffusion on DWI (differentiates from tumor)
Empiric therapy
Ceftriaxone 2 g IV q12h + metronidazole 500 mg IV q8h ± vancomycin (if post-surgical or MRSA risk). Duration: 6–8 weeks IV
Surgical drainage
Indicated if abscess >2.5 cm, mass effect, intraventricular rupture, or no improvement on antibiotics
LP
Contraindicated — risk of herniation. Diagnosis is imaging-based.
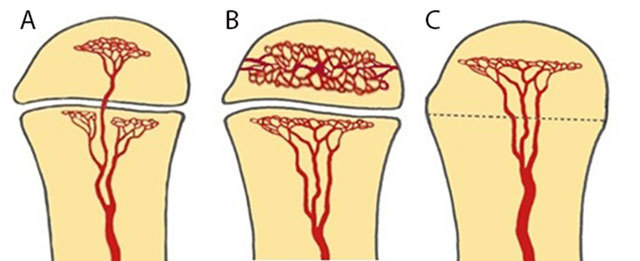
Figure 36 — Bone Vascularization and Hematogenous Spread. Schematic showing vascularization patterns in long bones across age groups (infant, child, adult), explaining why hematogenous osteomyelitis and brain abscess from hematogenous sources differ in their anatomic predilection based on blood supply patterns.
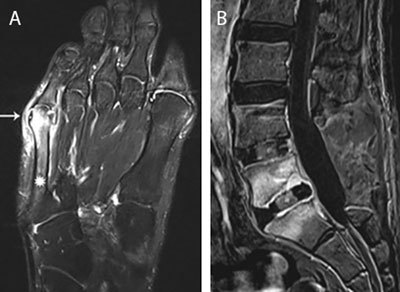
Spinal Epidural Abscess
A neurosurgical emergency. Risk factors: IVDU, epidural catheter, spinal procedures, diabetes, immunosuppression. Classic triad: back pain, fever, neurologic deficit (progressive weakness, sensory level, bowel/bladder dysfunction). Most common organism: S. aureus (~65%).
Component
Details
Imaging
MRI with gadolinium of entire spine (gold standard); sensitivity >90%
Treatment
Emergent surgical decompression + drainage + IV antibiotics (vancomycin + ceftriaxone). Medical management alone only if: no neurologic deficit, stable imaging, organism identified, and close follow-up
Duration
4–6 weeks IV antibiotics minimum; 6–8 weeks if associated osteomyelitis/discitis
The key to outcome in spinal epidural abscess is early diagnosis. Once paralysis develops, it is often irreversible. Any patient with fever + back pain + risk factors (IVDU, DM, recent spinal procedure) should receive an urgent MRI of the entire spine, not just the symptomatic region — skip lesions occur in up to 15% of cases.
14 Infective Endocarditis
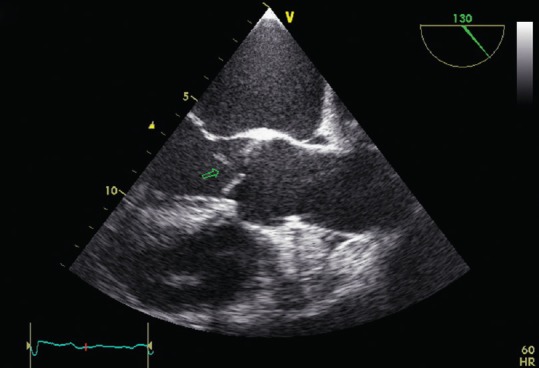
Infective endocarditis (IE) is an infection of the endocardial surface of the heart, usually involving one or more heart valves. The diagnosis relies on the modified Duke criteria (2023 update), integrating clinical, microbiologic, imaging, and pathologic data.
Figure 15 — Aortic Valve Vegetation on Transesophageal Echocardiography. TEE long-axis view demonstrating a mobile echogenic vegetation attached to the aortic valve, the hallmark finding in infective endocarditis imaging and a major criterion in the modified Duke diagnostic criteria.
Modified Duke Criteria (2023 Update)
Major Criteria
Definition
Blood cultures
Typical organism from ≥2 separate cultures (viridans streptococci, S. bovis, HACEK, S. aureus, Enterococcus without a primary focus); OR persistently positive cultures (≥2 positive >12 hours apart, or 3/3 or majority of ≥4 cultures positive)
Imaging
Vegetation, abscess, pseudoaneurysm, or new dehiscence on echocardiography; OR abnormal activity on FDG-PET/CT or radiolabeled leukocyte SPECT/CT (prosthetic valve, implanted device)
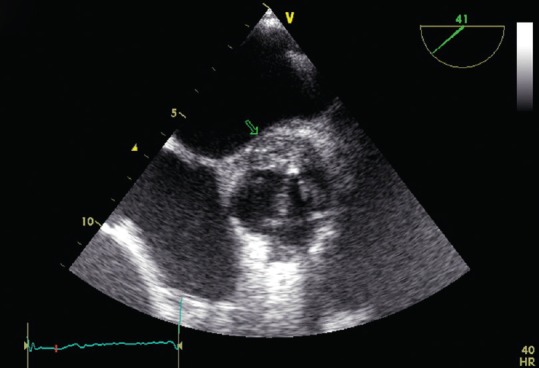
Figure 16 — Perivalvular Abscess in Infective Endocarditis. TEE imaging demonstrating a perivalvular aortic abscess, a serious complication of infective endocarditis that often necessitates urgent surgical intervention due to risk of septic embolization and hemodynamic instability.
Large vegetation (>10 mm) with embolic event or high embolic risk
Urgent
Prosthetic valve endocarditis with dehiscence or obstruction
Urgent
Fungal or highly resistant organism
Urgent
The POET trial (NEJM 2019) demonstrated that in clinically stable patients with left-sided endocarditis, switching from IV to oral antibiotics after at least 10 days of IV therapy is non-inferior to completing the full IV course. This applies only to streptococcal, enterococcal, S. aureus, or CoNS endocarditis with documented clinical response and no abscess.
15 Osteomyelitis
Osteomyelitis is infection of bone, classified by mechanism: hematogenous (bacteremia seeding bone, common in children and vertebral bodies in adults), contiguous (direct spread from adjacent soft tissue, trauma, or surgery), and vascular insufficiency (diabetic foot). The most common pathogen across all types is S. aureus.
Figure 17 — Routes of Infectious Spread in Osteomyelitis. The three main pathways by which bone infection develops: hematogenous seeding via the bloodstream, contiguous spread from adjacent soft tissue or surgical sites, and direct inoculation from trauma or open fractures.
Classification by Mechanism
Type
Typical Location
Common Organisms
Key Features
Hematogenous
Vertebral bodies (adults); metaphysis of long bones (children)
S. aureus, coagulase-negative Staphylococci, Streptococcus; GNR (IVDU, UTI source); Salmonella (sickle cell disease)
Insidious back pain with elevated ESR/CRP; children: limp, refusal to bear weight
Polymicrobial: S. aureus, Streptococcus, Enterococcus, GNR, anaerobes
Chronic non-healing ulcer overlying bone
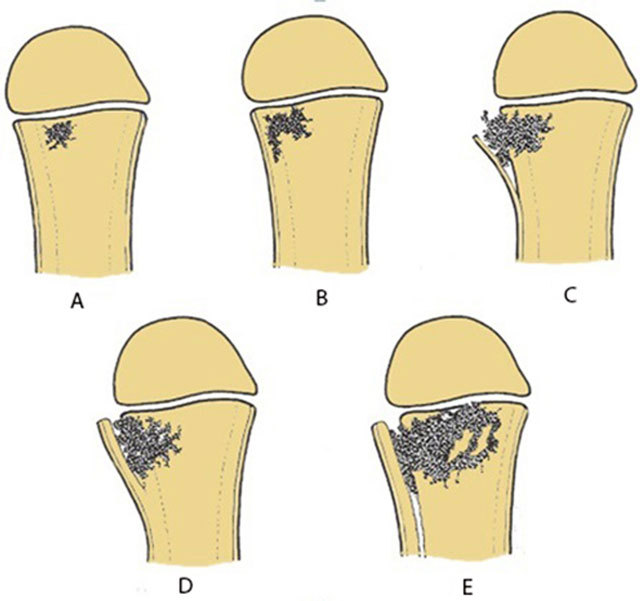
Figure 18 — Pathological Progression of Acute Osteomyelitis. Schematic illustrating the consecutive events in acute osteomyelitis from initial bacterial seeding through periosteal elevation, abscess formation, sequestrum development, and involucrum formation in chronic disease.
Diagnosis
Modality
Sensitivity/Specificity
Role
Plain radiographs
Low sensitivity early (<40% at 2 weeks)
May show periosteal elevation, cortical destruction, sequestrum (late findings)
MRI
Sensitivity 90–100%, specificity 80–90%
Gold standard imaging; shows bone marrow edema, soft tissue extent, abscess
Bone biopsy + culture
Gold standard for organism identification
Required before prolonged antibiotic therapy; avoid swab cultures of wound surface (unreliable)
If sterile metal probe reaches bone through ulcer, osteomyelitis is likely
ESR/CRP
Elevated in >90%
Useful for monitoring treatment response (CRP normalizes faster than ESR)
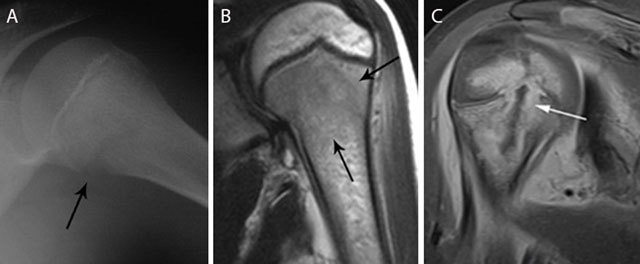
Figure 19 — MRI of Acute Osteomyelitis. MRI demonstrating the characteristic findings of acute osteomyelitis including bone marrow edema (T1 hypointensity, T2/STIR hyperintensity), periosteal reaction, and adjacent soft tissue inflammation — MRI is the gold standard imaging modality with 90–100% sensitivity.
Treatment
Scenario
Antibiotic
Duration
Native vertebral osteomyelitis (MSSA)
Nafcillin/oxacillin 2 g IV q4h or cefazolin 2 g IV q8h
6 weeks IV
Native vertebral osteomyelitis (MRSA)
Vancomycin (AUC/MIC 400–600)
6 weeks IV
Contiguous osteomyelitis with debridement
Culture-directed IV therapy
4–6 weeks (from last debridement)
Prosthetic joint infection with DAIR
IV pathogen-directed + rifampin (after wound closure)
6 weeks IV, then oral suppressive therapy × 3–6 months
Diabetic foot osteomyelitis
Culture-directed therapy; consider ampicillin-sulbactam or ertapenem for polymicrobial
6 weeks if no amputation; shorter if all infected bone resected
16 Septic Arthritis
Septic arthritis is a joint space infection that constitutes an orthopedic emergency — delayed treatment leads to irreversible cartilage destruction. The most common organism is S. aureus in adults and N. gonorrhoeae in sexually active young adults.
Repeated arthrocentesis or surgical drainage; surgical washout for hip joint (cannot aspirate easily), prosthetic joint, or failure to improve
Always send synovial fluid for crystal analysis (polarized microscopy) in addition to Gram stain and culture. Gout and pseudogout can mimic septic arthritis, but the two can coexist — crystals do not exclude infection. If the clinical picture is concerning for sepsis, treat empirically even if crystals are present.
17 C. difficile Infection
Clostridioides difficile infection (CDI) is the most common cause of healthcare-associated diarrhea. Risk factors: antibiotic exposure (especially fluoroquinolones, clindamycin, broad-spectrum cephalosporins), age >65, hospitalization, PPI use, immunosuppression.
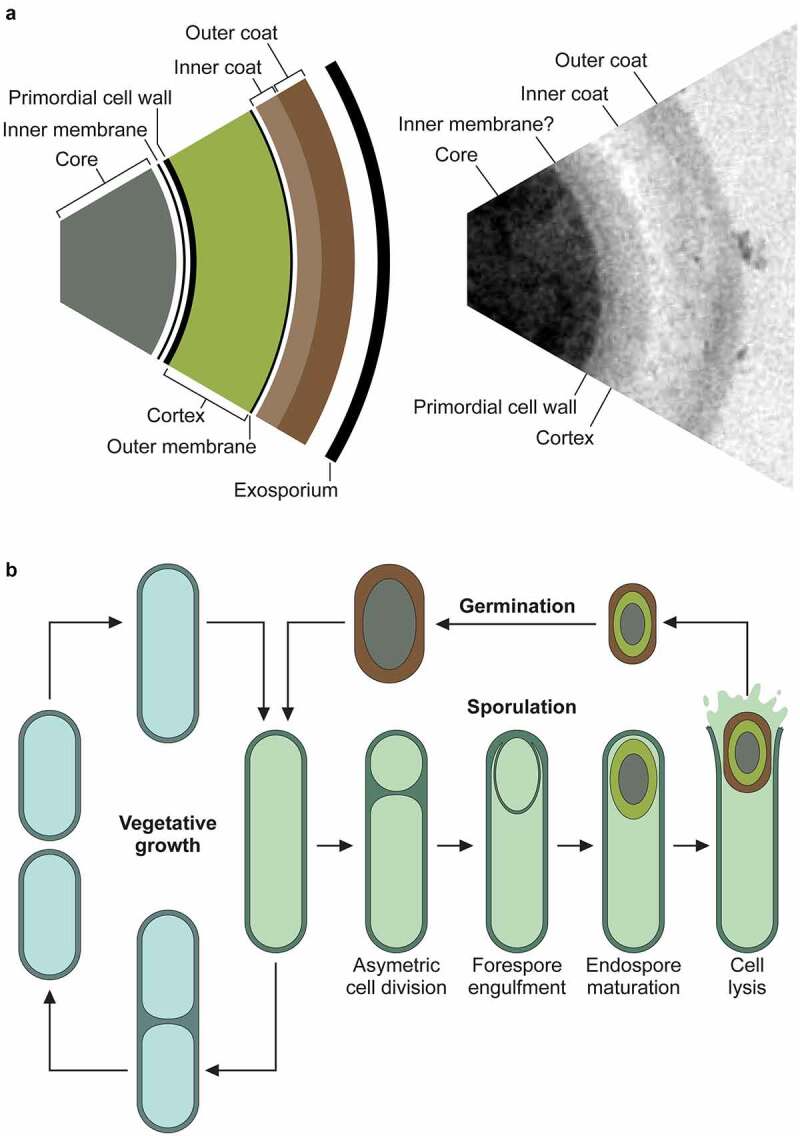
Figure 20 — C. difficile Spore Structure and Lifecycle. The multi-layered spore structure and sporulation/germination cycle of Clostridioides difficile, illustrating how spores survive environmental stresses and antibiotic exposure, enabling persistence and transmission in healthcare settings.
Diagnosis
Test only formed stool specimens from patients with ≥3 unformed stools in 24 hours. The preferred approach is a two-step algorithm: (1) GDH (glutamate dehydrogenase) antigen screen or NAAT, then (2) toxin A/B EIA if NAAT is positive. Alternatively, NAAT alone (high sensitivity but may detect colonization rather than active disease).
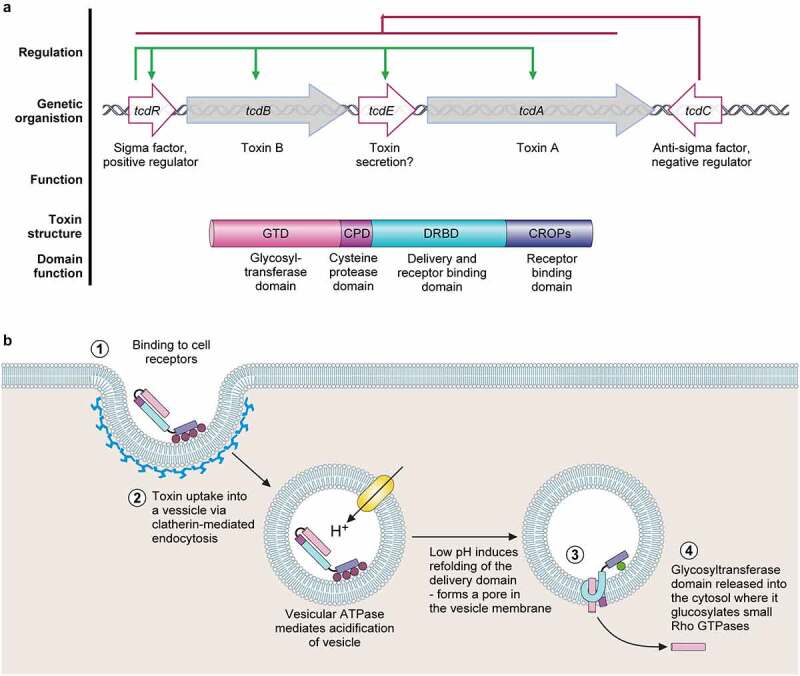
Figure 21 — C. difficile Toxin Pathogenesis. The pathogenicity locus (PaLoc) organization and the ABCD model of toxin action, showing how toxins A (TcdA) and B (TcdB) bind to host cell receptors, undergo endocytosis, and glucosylate Rho GTPases to cause epithelial damage, inflammation, and diarrhea.
Fidaxomicin 200 mg PO BID × 10 days (preferred) OR vancomycin 125 mg PO QID × 10 days
Severe
WBC ≥15,000 OR Cr ≥1.5 mg/dL
Fidaxomicin 200 mg PO BID × 10 days OR vancomycin 125 mg PO QID × 10 days
Fulminant
Hypotension, shock, ileus, megacolon
Vancomycin 500 mg PO/NG QID + vancomycin 500 mg per rectum q6h (if ileus) + metronidazole 500 mg IV q8h. Surgical consultation for colectomy
First recurrence
Recurrence within 2–8 weeks of completing therapy
Fidaxomicin 200 mg BID × 10 days, then every other day × 20 days (extended-pulsed regimen); OR vancomycin taper/pulse
Second or subsequent recurrence
Multiple recurrences
Vancomycin taper/pulse, then fecal microbiota transplantation (FMT) after completing antibiotic course; or bezlotoxumab (anti-toxin B monoclonal antibody) as adjunct
Fidaxomicin is now preferred over oral vancomycin for initial and recurrent CDI because it has a narrower spectrum (less disruption of normal flora), lower recurrence rates (~13% vs ~27% with vancomycin), and achieves high fecal concentrations. The main limitation is cost.
Do NOT test for cure. A positive NAAT can persist for weeks after successful treatment. Repeat testing should only be done if symptoms recur. Also, do NOT use anti-motility agents (loperamide) in CDI as they may precipitate toxic megacolon.
18 Intra-Abdominal Infections
Classification
Type
Examples
Microbiology
Primary peritonitis (SBP)
Spontaneous bacterial peritonitis in cirrhotic ascites
E. coli, Klebsiella, S. pneumoniae (monomicrobial)
Persistent/recurrent infection after adequate treatment of secondary peritonitis
Resistant organisms: VRE, Candida, Pseudomonas
Intra-abdominal abscess
Hepatic, splenic, pancreatic, tubo-ovarian, psoas
Polymicrobial; amoebic liver abscess (E. histolytica)
Spontaneous Bacterial Peritonitis (SBP)
Diagnose by paracentesis: ascitic fluid PMN count ≥250 cells/µL = SBP (culture may be negative in ~40%). Treatment: ceftriaxone 2 g IV daily × 5 days. Albumin 1.5 g/kg at diagnosis and 1 g/kg on day 3 reduces mortality in patients with Cr >1, BUN >30, or bilirubin >4. Prophylaxis: norfloxacin 400 mg daily or TMP-SMX for patients with prior SBP, GI hemorrhage, or ascitic fluid protein <1.5 g/dL with advanced liver disease.
Ceftriaxone + metronidazole; OR ertapenem 1 g IV daily; OR ampicillin-sulbactam 3 g IV q6h
Severe (healthcare-associated, post-operative)
Piperacillin-tazobactam 4.5 g IV q6h; OR meropenem 1 g IV q8h; OR cefepime + metronidazole ± vancomycin (if Enterococcus risk)
Source control (surgical repair of perforation, drainage of abscess) is the cornerstone of managing secondary peritonitis. Antibiotics alone are insufficient without adequate source control. CT-guided percutaneous drainage has replaced open surgery for most abscesses.
19 Infectious Diarrhea
Etiology by Mechanism
Type
Organisms
Key Features
Inflammatory (bloody/dysentery)
Shigella, Salmonella, Campylobacter, EHEC (O157:H7), C. difficile, Entamoeba
Empiric antibiotics for community-acquired bloody diarrhea are generally NOT recommended until EHEC is excluded (stool culture, Shiga toxin testing). However, if the patient is severely ill with dysentery (fever, toxicity), azithromycin is the safest empiric choice while awaiting stool studies, as it covers Shigella and Campylobacter without the theoretical risk of HUS associated with fluoroquinolones in EHEC.
20 UTI & Pyelonephritis
Classification
Type
Definition
Common Pathogens
Uncomplicated cystitis
Lower UTI in non-pregnant, premenopausal woman with normal urinary tract
E. coli (~80%), S. saprophyticus, Klebsiella, Proteus
Complicated UTI
UTI with structural/functional abnormality, pregnancy, male sex, catheter, renal transplant, obstruction
E. coli, Klebsiella, Proteus, Enterococcus, Pseudomonas
Pyelonephritis
Upper UTI with flank pain, fever, CVA tenderness
E. coli, Klebsiella, Proteus; consider MRSA if hematogenous
Catheter-associated UTI (CAUTI)
Symptoms + ≥10³ CFU/mL from catheterized specimen (or new catheter specimen after removal)
E. coli, Enterococcus, Candida, Pseudomonas, Klebsiella
Treatment
Condition
First-Line
Alternatives
Duration
Uncomplicated cystitis
Nitrofurantoin 100 mg BID × 5 days or TMP-SMX DS BID × 3 days (if local resistance <20%)
Fosfomycin 3 g PO × 1 dose
3–5 days
Complicated cystitis
Fluoroquinolone (ciprofloxacin 500 mg BID or levofloxacin 750 mg daily) or TMP-SMX
IV if unable to tolerate PO
7–14 days
Uncomplicated pyelonephritis (outpatient)
Ciprofloxacin 500 mg BID × 7 days or TMP-SMX DS BID × 14 days
Ceftriaxone 1 g IM × 1 dose as bridge
7–14 days
Complicated pyelonephritis / urosepsis
Ceftriaxone 1–2 g IV daily, piperacillin-tazobactam, or meropenem (if ESBL risk)
Add vancomycin if Gram-positive cocci in clusters
10–14 days
CAUTI
Remove or replace catheter + culture-directed therapy
Empiric ceftriaxone or fluoroquinolone
7 days (if prompt response); 10–14 days (if delayed response)
Asymptomatic bacteriuria (ASB) should only be treated in two populations: pregnant women (risk of pyelonephritis and preterm labor) and patients undergoing urologic procedures with anticipated mucosal bleeding. Do NOT treat ASB in elderly patients, catheterized patients, or diabetics — treatment does not improve outcomes and promotes resistance.
21 Sexually Transmitted Infections
Gonorrhea & Chlamydia
Feature
Gonorrhea (N. gonorrhoeae)
Chlamydia (C. trachomatis)
Presentation (male)
Purulent urethral discharge, dysuria (2–5 day incubation)
Mucoid/watery discharge, dysuria (7–21 day incubation); often asymptomatic
Presentation (female)
Cervicitis, PID; often asymptomatic
Cervicitis, PID; most common bacterial STI; often asymptomatic
Diagnosis
NAAT (urine or swab) — test of choice; culture for susceptibility if treatment failure
NAAT (urine or swab) — test of choice
Treatment
Ceftriaxone 500 mg IM × 1 dose (1 g if ≥150 kg). If chlamydia not excluded, add doxycycline 100 mg BID × 7 days
Doxycycline 100 mg PO BID × 7 days (preferred over azithromycin per 2021 CDC STI guidelines)
Partner notification
All sexual partners within 60 days; expedited partner therapy (EPT) where legal
All partners within 60 days; EPT
Syphilis (Treponema pallidum)
Stage
Presentation
Treatment
Primary
Painless chancre (clean-based ulcer) at inoculation site, 10–90 days post-exposure; painless lymphadenopathy
Benzathine penicillin G 2.4 million units IM × 1 dose
Secondary
Diffuse maculopapular rash (including palms and soles), condylomata lata, mucous patches, fever, lymphadenopathy; 6–12 weeks after primary
Benzathine penicillin G 2.4 million units IM × 1 dose
Latent (early <1 yr)
Asymptomatic, positive serology
Benzathine penicillin G 2.4 million units IM × 1 dose
Latent (late >1 yr or unknown duration)
Asymptomatic, positive serology
Benzathine penicillin G 2.4 million units IM weekly × 3 doses
Tertiary
Gummas, aortitis (ascending aortic aneurysm), tabes dorsalis, general paresis
Benzathine penicillin G 2.4 million units IM weekly × 3 doses
IV penicillin G 3–4 million units q4h × 10–14 days
Figure 22 — Secondary Syphilis — Palmar and Plantar Lesions. Clinical photograph demonstrating the characteristic maculopapular rash of secondary syphilis involving the palms and soles, a hallmark finding that distinguishes syphilis from most other dermatologic conditions and should prompt serologic testing.
Serologic testing: Screen with non-treponemal test (RPR or VDRL) → confirm with treponemal test (FTA-ABS or TP-PA). Many labs now use reverse algorithm: treponemal screen → reflex RPR. Non-treponemal titers correlate with disease activity and are used to monitor treatment response (4-fold decline = adequate response). The Jarisch-Herxheimer reaction (fever, rigors, hypotension within 24h of treatment) is common in early syphilis and is self-limited.
Genital Herpes (HSV-1 & HSV-2)
Feature
Details
Presentation
Painful vesicles/ulcers on erythematous base; inguinal lymphadenopathy; primary episode is most severe
Diagnosis
HSV PCR (preferred) or viral culture of lesion; type-specific serology (HSV-1 IgG, HSV-2 IgG)
First episode
Valacyclovir 1 g PO BID × 7–10 days or acyclovir 400 mg TID × 7–10 days
Recurrent episodes
Valacyclovir 500 mg BID × 3 days or 1 g daily × 5 days
Suppressive therapy
Valacyclovir 500 mg–1 g PO daily (reduces outbreaks by 70–80% and transmission by 50%)
22 PID & Tubo-ovarian Abscess
Pelvic inflammatory disease (PID) is an ascending infection of the upper female genital tract (endometritis, salpingitis, peritonitis, tubo-ovarian abscess). It is primarily caused by N. gonorrhoeae and C. trachomatis, but is often polymicrobial (anaerobes, GNR, Mycoplasma genitalium).
Diagnosis
Clinical diagnosis: pelvic/lower abdominal pain + one or more of: cervical motion tenderness, uterine tenderness, adnexal tenderness. Additional criteria supporting diagnosis: fever >38.3°C, cervical mucopurulent discharge, elevated WBC, elevated ESR/CRP, laboratory documentation of GC/CT.
Treatment (CDC 2021)
Setting
Regimen
Outpatient (mild-moderate)
Ceftriaxone 500 mg IM × 1 dose + doxycycline 100 mg PO BID × 14 days ± metronidazole 500 mg PO BID × 14 days
Inpatient
Cefotetan 2 g IV q12h + doxycycline 100 mg PO/IV q12h; OR cefoxitin 2 g IV q6h + doxycycline 100 mg PO/IV q12h; OR clindamycin 900 mg IV q8h + gentamicin (loading + maintenance)
Tubo-ovarian Abscess (TOA)
Diagnosed by pelvic ultrasound or CT. Treatment: IV antibiotics (as above for inpatient PID) + image-guided drainage if abscess ≥3 cm or failure to improve in 48–72 hours. Surgical intervention if ruptured (surgical emergency) or unresponsive to medical therapy.
Low threshold to diagnose and treat PID — untreated PID leads to infertility (~15% after one episode, ~35% after two), ectopic pregnancy, and chronic pelvic pain. The clinical diagnosis has low sensitivity and specificity, but the consequences of delayed treatment outweigh the risks of overtreatment. Test all PID patients for HIV and syphilis.
23 HIV Pathophysiology & Natural History
Human immunodeficiency virus (HIV) is a retrovirus that targets CD4+ T lymphocytes, leading to progressive immune deficiency. Without treatment, HIV progresses through well-defined stages over 8–10 years from acute infection to AIDS (CD4 <200 cells/µL or AIDS-defining illness).
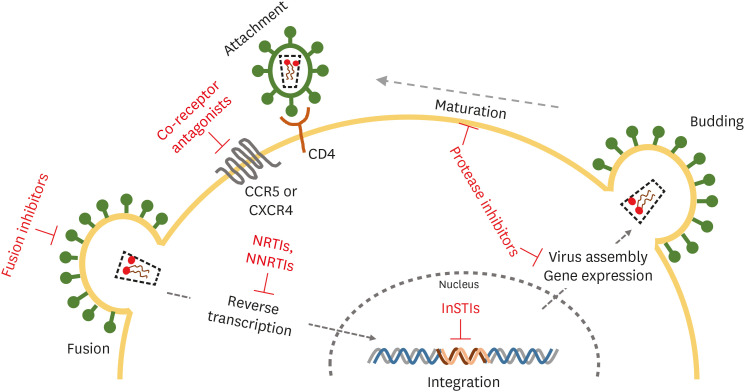
Figure 23 — HIV-1 Lifecycle and Antiretroviral Drug Targets. Comprehensive diagram of the HIV-1 replication cycle from viral attachment and entry through reverse transcription, integration, assembly, and maturation, with each step labeled alongside the corresponding antiretroviral drug classes that target it.
Usually asymptomatic; persistent generalized lymphadenopathy
Symptomatic HIV / AIDS
Variable
<200 cells/µL
Rising
Opportunistic infections, wasting, malignancies, death within 2–3 years without ART
Without treatment, median time from HIV infection to AIDS is ~10 years, and median survival after AIDS diagnosis is ~2 years. With modern ART, life expectancy approaches that of the general population when treatment is initiated early and consistently maintained.
24 HIV Testing & Diagnosis
Recommended Testing Algorithm (CDC 2014)
Step
Test
Window Period
Notes
1. Initial screen
4th-generation HIV-1/2 Ag/Ab combo assay
~2 weeks (detects p24 Ag)
Detects both HIV-1/2 antibodies and p24 antigen; replaces older Ab-only tests
2. Confirmatory
HIV-1/HIV-2 antibody differentiation immunoassay
—
Distinguishes HIV-1 from HIV-2
3. If discordant
HIV-1 RNA (viral load/NAAT)
~10–14 days
Detects acute HIV before antibody seroconversion; resolves indeterminate results
Baseline Laboratory Workup (Newly Diagnosed HIV)
Test
Purpose
CD4 count (absolute and %)
Determines immunologic status and need for OI prophylaxis
HIV RNA viral load
Baseline for monitoring ART response; goal is undetectable (<20–50 copies/mL)
HIV genotype (resistance testing)
Guide ART selection; perform before initiating therapy
HLA-B*5701
Screen before abacavir use — if positive, do NOT use abacavir (risk of hypersensitivity reaction)
CBC, CMP, lipid panel, HbA1c
Baseline metabolic assessment; ART metabolic monitoring
Hepatitis B (HBsAg, anti-HBs, anti-HBc), Hepatitis C Ab
Coinfection management; tenofovir-containing regimens treat both HIV and HBV
RPR/VDRL, GC/CT NAAT, Trichomonas
STI screening
TB screening (IGRA or PPD)
Latent TB treatment if positive
Toxoplasma IgG
If positive and CD4 <100, prophylaxis required
G6PD level
Before dapsone or primaquine use
25 Antiretroviral Therapy
ART is recommended for all persons with HIV regardless of CD4 count (treat early). The goal is durable viral suppression (HIV RNA <50 copies/mL), immune reconstitution, reduced transmission, and improved survival. Modern regimens are once-daily, well-tolerated, and highly effective.
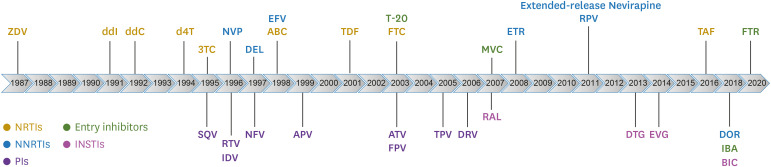
Figure 24 — Timeline of FDA-Approved Antiretroviral Drugs. Historical timeline showing the development and FDA approval of antiretroviral medications by drug class, from the first NRTI (zidovudine, 1987) through modern integrase inhibitors and long-acting injectable formulations.
Preferred Initial ART Regimens (DHHS 2023)
Regimen
Components
Key Considerations
Bictegravir/emtricitabine/TAF (Biktarvy)
INSTI + 2 NRTIs (single tablet)
High barrier to resistance, minimal drug interactions, once daily. Cannot use if CrCl <30 or with rifampin
Dolutegravir/lamivudine (Dovato)
INSTI + 1 NRTI (2-drug regimen, single tablet)
Only if HBV negative, HIV RNA <500,000, no resistance to either component; once daily
Dolutegravir + emtricitabine/TAF (or TDF)
INSTI + 2 NRTIs
Flexible backbone; dolutegravir has high barrier to resistance
Cabotegravir + rilpivirine (Cabenuva)
Long-acting injectable INSTI + NNRTI
IM injections every 1–2 months; for virally suppressed patients (switch strategy); NOT for initial therapy
Pre-Exposure Prophylaxis (PrEP)
Regimen
Population
Monitoring
Emtricitabine/TDF (Truvada) daily
All at-risk populations
HIV test q3 months, renal function q6–12 months, STI screen q3–6 months
Emtricitabine/TAF (Descovy) daily
MSM, transgender women (≥35 kg); NOT approved for receptive vaginal sex
Same as above; less renal/bone toxicity than TDF
Cabotegravir (Apretude) IM q2 months
All at-risk populations
Superior efficacy to daily oral PrEP in trials; long-acting injectable
Post-Exposure Prophylaxis (PEP)
Initiate within 72 hours of exposure (sooner is better; ideally within 2 hours). Standard regimen: emtricitabine/TDF + dolutegravir (or raltegravir) × 28 days. Test source patient and exposed individual for HIV at baseline, 4–6 weeks, and 12 weeks.
Immune reconstitution inflammatory syndrome (IRIS) can occur within weeks to months of ART initiation, as the recovering immune system mounts an exaggerated inflammatory response against pre-existing opportunistic infections (paradoxical IRIS) or uncovers subclinical infections (unmasking IRIS). Common in patients starting ART with CD4 <50 and high viral load. Treatment: continue ART, treat the underlying OI, add corticosteroids for severe cases. For this reason, in cryptococcal meningitis and TB meningitis, ART initiation should be delayed 4–6 weeks and 2–8 weeks, respectively.
26 Opportunistic Infections in HIV
CD4-Based Risk & Prophylaxis
CD4 Threshold
Opportunistic Infection
Prophylaxis
When to Stop Prophylaxis
<200
Pneumocystis jirovecii (PJP)
TMP-SMX DS daily (also covers Toxoplasma)
CD4 >200 for ≥3 months on ART
<100
Toxoplasma gondii (if IgG positive)
TMP-SMX DS daily
CD4 >200 for ≥3 months on ART
<50
Mycobacterium avium complex (MAC)
Azithromycin 1200 mg weekly (if unable to start ART promptly)
CD4 >100 for ≥3 months on ART; not required if starting ART immediately
<50
CMV retinitis
No primary prophylaxis; regular fundoscopic exams
—
Any CD4
TB (if LTBI positive)
LTBI treatment (3HP, 4R, or 9H)
After completing course
Figure 25 — Kaposi Sarcoma in HIV/AIDS. Clinical photograph demonstrating the characteristic violaceous (purple) plaques of Kaposi sarcoma on the face and ear of an HIV-positive patient. KS is the most common neoplasm in AIDS and is caused by human herpesvirus 8 (HHV-8).
ART (may regress with immune reconstitution); chemotherapy for advanced (liposomal doxorubicin)
Toxoplasma ring-enhancing brain lesions in HIV must be differentiated from primary CNS lymphoma (typically single lesion, EBV PCR in CSF, thallium SPECT/PET uptake). Empiric treatment for toxoplasmosis with clinical and radiographic reassessment at 2 weeks is the standard approach — biopsy is reserved for patients who do not respond or are Toxoplasma IgG negative.
27 Cellulitis, Abscess & Necrotizing Fasciitis
Purulent vs Non-Purulent SSTI
Type
Organisms
Treatment
Non-purulent cellulitis (no abscess/drainage)
Beta-hemolytic Streptococcus (GAS) most common; MSSA
Cephalexin 500 mg QID, dicloxacillin 500 mg QID, or clindamycin 300–450 mg TID × 5–7 days. Add MRSA coverage only if: penetrating trauma, IVDU, MRSA risk factors, failure of beta-lactam
I&D is primary treatment for abscess; add TMP-SMX DS BID or doxycycline 100 mg BID if: abscess >2 cm, multiple lesions, surrounding cellulitis, immunocompromised, systemic symptoms
Severe (failed oral, rapid progression, systemic toxicity)
S. aureus (including MRSA), Streptococcus
Vancomycin 15–20 mg/kg IV q8–12h + piperacillin-tazobactam (if polymicrobial concern); OR vancomycin + ceftriaxone
Figure 26 — CT Findings in Necrotizing Fasciitis. CT imaging demonstrating extensive streaky soft-tissue gas tracking along fascial planes of the thigh, a characteristic finding of necrotizing fasciitis. While CT can support the diagnosis, clinical suspicion alone warrants emergent surgical exploration.
Necrotizing Fasciitis
Emergency — Necrotizing Fasciitis
Necrotizing fasciitis is a surgical emergency with mortality of 25–35% (higher if delayed surgery). Clinical features: severe pain out of proportion to exam findings, rapidly spreading erythema, crepitus, bullae/hemorrhagic blisters, skin necrosis, septic shock. Do NOT wait for imaging if clinical suspicion is high. Treatment: emergent surgical debridement + broad-spectrum antibiotics (vancomycin + piperacillin-tazobactam + clindamycin). Clindamycin inhibits toxin production. Serial debridements are typically required.
Liver disease, raw shellfish consumption, wound exposure to water
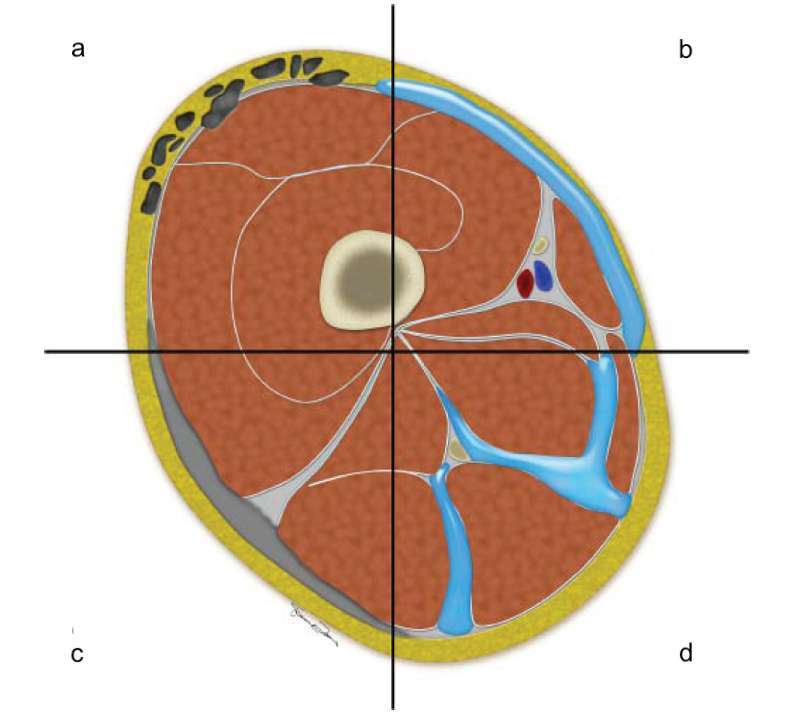
Figure 27 — Cross-Sectional Anatomy of Necrotizing Fasciitis. Schematic diagram illustrating the cross-sectional anatomy of the thigh with the spectrum of imaging findings in necrotizing fasciitis, including fascial thickening, subcutaneous gas, subfascial fluid collections, and myonecrosis.
LRINEC Score (Laboratory Risk Indicator for Necrotizing Fasciitis)
Variable
Score
CRP ≥150 mg/L
4
WBC 15,000–25,000
1; >25,000 = 2
Hemoglobin 11–13.5 g/dL
1; <11 = 2
Sodium <135 mEq/L
2
Creatinine >1.6 mg/dL
2
Glucose >180 mg/dL
1
Score ≥6 suggests necrotizing fasciitis (PPV ~92%). However, a low score does NOT exclude the diagnosis — clinical suspicion should override the score. If in doubt, take the patient to the operating room.
28 Diabetic Foot Infections
Diabetic foot infections (DFI) occur in ~25% of diabetics over their lifetime, and are the leading cause of non-traumatic lower extremity amputation. Classification guides management.
Figure 37 — Radiographic Findings of Diabetic Foot Osteomyelitis. Plain radiograph demonstrating destruction of the first metatarsal head from osteomyelitis in a diabetic foot. While plain films have limited early sensitivity, they may reveal cortical destruction, periosteal reaction, and soft tissue gas in advanced cases.
IWGDF/IDSA Severity Classification
Grade
Severity
Clinical Features
Treatment
1
Uninfected
Wound without signs of infection
Wound care, offloading
2
Mild
Infection limited to skin/subcutaneous tissue, erythema ≤2 cm around ulcer, no systemic signs
Oral antibiotics: cephalexin, amoxicillin-clavulanate, or TMP-SMX + amoxicillin-clavulanate
3
Moderate
Erythema >2 cm, or involving deeper structures (abscess, osteomyelitis, septic arthritis), no SIRS
IV antibiotics: ampicillin-sulbactam, piperacillin-tazobactam, or ertapenem. Consider MRSA coverage
4
Severe
Any foot infection with SIRS/sepsis
Broad-spectrum IV: vancomycin + piperacillin-tazobactam or meropenem. Emergent surgical evaluation
Figure 28 — Probe-to-Bone Test in Diabetic Foot Infection. Clinical photograph of a positive probe-to-bone test at the first metatarsal head, where a sterile blunt metal probe reaches bone through the ulcer — a bedside test with approximately 89% sensitivity for osteomyelitis in high-risk patients.
Osteomyelitis in Diabetic Foot
The probe-to-bone (PTB) test is performed by inserting a sterile blunt metal probe through the ulcer: if bone is palpable, osteomyelitis is likely (sensitivity ~89% in patients with high pretest probability). ESR >70 mm/hr has high specificity for osteomyelitis. MRI is the gold standard imaging modality. Bone biopsy with culture provides definitive diagnosis and guides antibiotic therapy — always preferred over wound swab cultures.
Figure 29 — MRI of Diabetic Foot Osteomyelitis. MRI demonstrating osteomyelitis involving the distal phalanx in a diabetic foot, showing bone marrow signal changes with T1 hypointensity and T2 hyperintensity — MRI is the gold standard imaging modality for confirming osteomyelitis in diabetic foot infections.
Multidisciplinary management (ID, vascular surgery, podiatry, wound care, endocrinology) significantly reduces amputation rates. Always assess peripheral arterial disease (ABI, pulse examination) as revascularization may be needed before infection can heal. Optimize glycemic control concurrently.
29 Antibiotic Spectrum & Selection
Beta-Lactam Antibiotics
Class
Examples
Spectrum
Key Notes
Natural penicillins
Penicillin G, Penicillin V
Streptococcus, Treponema pallidum, Actinomyces
Drug of choice for syphilis; narrow spectrum
Anti-staphylococcal penicillins
Nafcillin, oxacillin, dicloxacillin
MSSA (beta-lactamase stable)
Drug of choice for MSSA; does NOT cover MRSA
Aminopenicillins
Amoxicillin, ampicillin
Streptococcus, Enterococcus, Listeria, some GNR
Ampicillin for Listeria and Enterococcus; susceptible to beta-lactamases
Broad GNR + Pseudomonas, stable to AmpC beta-lactamases
Better against Enterobacter than 3rd-gen (AmpC stable)
5th-gen cephalosporins
Ceftaroline
MRSA + Gram-negative (not Pseudomonas)
Only cephalosporin active against MRSA
Carbapenems
Meropenem, imipenem, ertapenem, doripenem
Broadest beta-lactam spectrum: GPC, GNR, anaerobes. Ertapenem does NOT cover Pseudomonas or Acinetobacter
Reserve for ESBL, serious polymicrobial infections; imipenem lowers seizure threshold
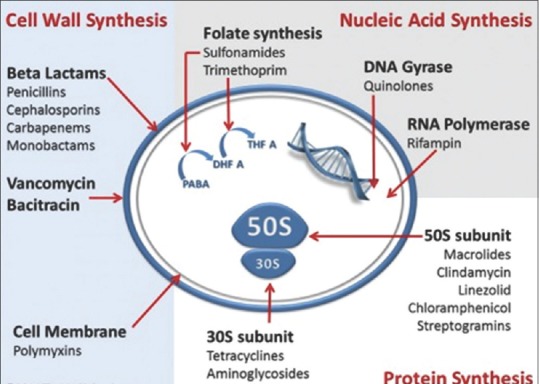
Figure 30 — Mechanisms of Action of Major Antibiotic Classes. Comprehensive overview of antibiotic targets including cell wall synthesis (beta-lactams, glycopeptides), protein synthesis (aminoglycosides, macrolides, tetracyclines), DNA replication (fluoroquinolones), and folate metabolism (TMP-SMX), showing how each class disrupts essential bacterial processes.
Non-Beta-Lactam Antibiotics
Agent
Spectrum
Key Uses
Major Toxicities
Vancomycin
MRSA, CoNS, Enterococcus (not VRE vanA), C. difficile (PO only)
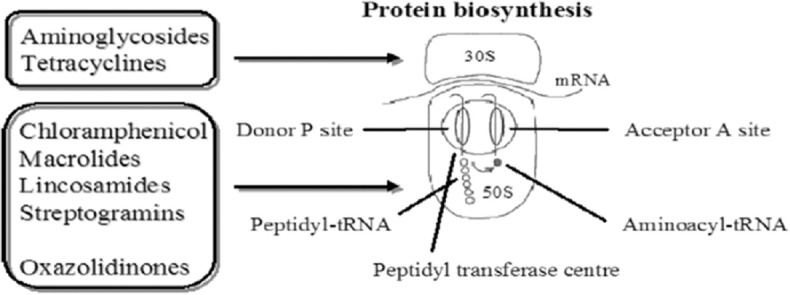
Figure 31 — Protein Synthesis Inhibitors — Ribosomal Targets. Diagram of the bacterial ribosome showing sites of action of protein synthesis inhibitors: aminoglycosides and tetracyclines on the 30S subunit, macrolides and lincosamides on the 50S subunit, and oxazolidinones (linezolid) on the 23S rRNA of the 50S subunit.
"Cidal vs static" matters in specific clinical scenarios. Bactericidal agents are required for meningitis (poor immune penetration to CNS), endocarditis (bacteria within vegetations are shielded), and neutropenic fever (no functioning immune system). Linezolid is bacteriostatic against Enterococcus and Staphylococcus but bactericidal against Streptococcus.
Cryptococcus, some Candida; always used in combination (synergy with amphotericin B)
Myelosuppression (dose-dependent), hepatotoxicity, GI toxicity
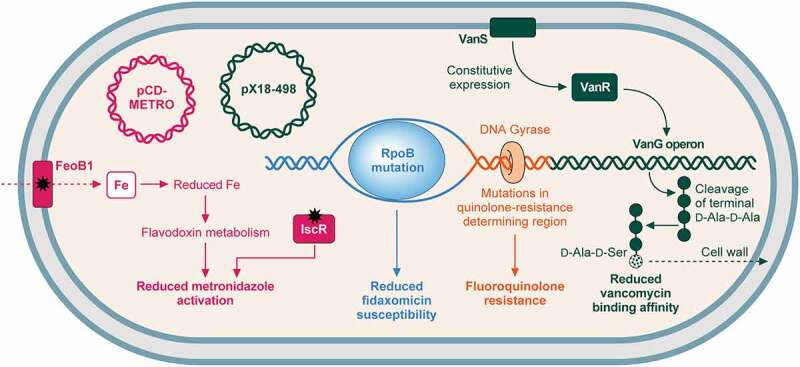
Figure 38 — Antimicrobial Resistance in C. difficile. Resistance pathways for the key antibiotics used to treat C. difficile infection (metronidazole, fidaxomicin, vancomycin, and fluoroquinolones), highlighting the molecular mechanisms that contribute to treatment failure and recurrence.
Mucormycosis (Rhizopus, Mucor) is treated with liposomal amphotericin B + surgical debridement. Risk factors: uncontrolled diabetes (especially DKA), iron overload, deferoxamine therapy, hematologic malignancy. Azoles and echinocandins have NO activity against Mucor (except isavuconazole, which has approval for mucormycosis). Posaconazole is used for step-down therapy.
31 Antiviral Agents
Agent
Mechanism
Indications
Key Notes
Acyclovir / Valacyclovir
Guanosine analog; requires viral thymidine kinase for activation → inhibits viral DNA polymerase
Use serum procalcitonin to guide antibiotic initiation and duration in respiratory infections and sepsis
Procalcitonin <0.25 ng/mL: bacterial infection unlikely; <0.5 or declining by ≥80%: consider stopping antibiotics. Reduces antibiotic exposure by 2–3 days
Therapeutic drug monitoring (TDM)
Measuring drug levels to optimize efficacy and minimize toxicity
CAP: 5 days. UTI (uncomplicated): 3–5 days. Intra-abdominal (source controlled): 4 days. Cellulitis: 5–6 days. Bacteremia (GNR uncomplicated): 7 days
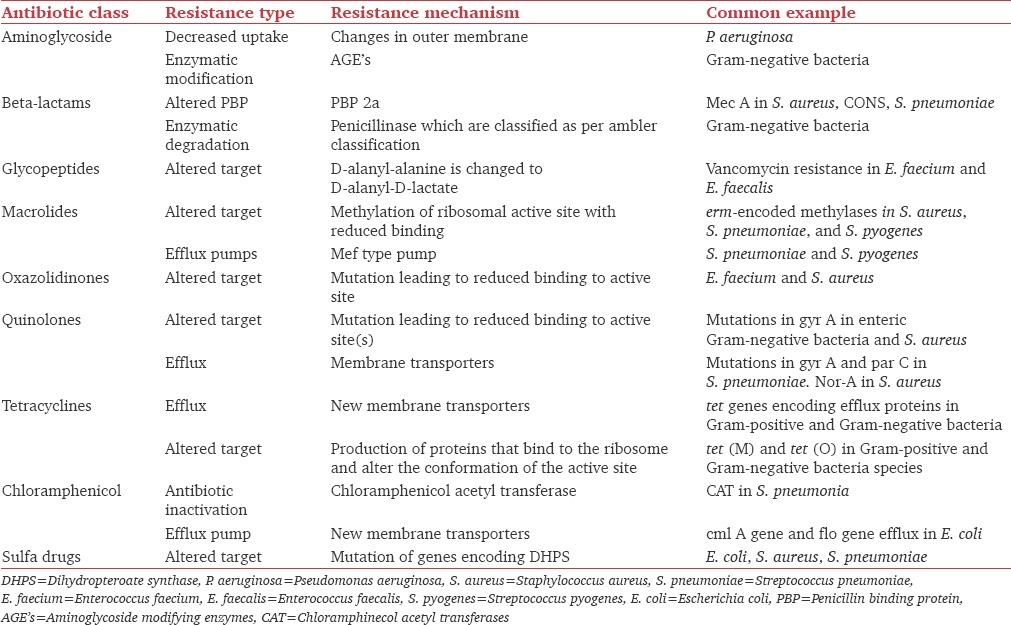
Figure 32 — Antibiotic Resistance Mechanisms by Drug Class. Comprehensive reference showing the specific resistance mechanisms (enzymatic degradation, target modification, efflux, permeability changes) for each major class of antibiotics, essential knowledge for antimicrobial stewardship and empiric therapy selection.
The IDSA recommends that all hospitals implement an antimicrobial stewardship program. Key elements: physician and pharmacist co-leadership, hospital administration support, real-time access to antibiograms, integration with infection prevention, education, and tracking/reporting of antibiotic use metrics (DOT per 1,000 patient-days).
Antibiotic-associated C. difficile risk (highest to lowest): fluoroquinolones, clindamycin, broad-spectrum cephalosporins, carbapenems, penicillins. Every unnecessary day of broad-spectrum antibiotics increases CDI risk.
33 Imaging in Infectious Disease
Clinical Scenario
Imaging Modality
Key Findings
Community-acquired pneumonia
CXR (PA and lateral)
Lobar consolidation, air bronchograms, pleural effusion; CT if CXR negative but high suspicion
Lung abscess
CT chest with contrast
Thick-walled cavitary lesion with air-fluid level; dependent segments (aspiration)
Fascial thickening, fat stranding, gas tracking along fascial planes; MRI more sensitive but takes longer
FUO workup
FDG-PET/CT
Detects occult infection, inflammation, or malignancy with 40–70% diagnostic yield
34 Classification Systems
Sepsis-3 (2016 Third International Consensus Definitions)
Term
Definition
Sepsis
Life-threatening organ dysfunction caused by a dysregulated host response to infection. Operationalized as suspected infection + acute SOFA score increase ≥2
Septic shock
Sepsis requiring vasopressors to maintain MAP ≥65 mmHg AND lactate >2 mmol/L after adequate volume resuscitation. Hospital mortality >40%
Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):801–810.
Evans L, Rhodes A, Alhazzani W, et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Intensive Care Med. 2021;47(11):1181–1247.
Metlay JP, Waterer GW, Long AC, et al. Diagnosis and Treatment of Adults with Community-acquired Pneumonia. ATS/IDSA 2019 Guidelines. Am J Respir Crit Care Med. 2019;200(7):e45–e67.
Kalil AC, Metersky ML, Klompas M, et al. Management of Adults with Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines. Clin Infect Dis. 2016;63(5):e61–e111.
Nahid P, Dorman SE, Alipanah N, et al. Official ATS/CDC/IDSA Clinical Practice Guideline: Treatment of Drug-Susceptible Tuberculosis. Clin Infect Dis. 2016;63(7):e147–e195.
Tunkel AR, Hartman BJ, Kaplan SL, et al. Practice Guidelines for the Management of Bacterial Meningitis. Clin Infect Dis. 2004;39(9):1267–1284.
de Gans J, van de Beek D. Dexamethasone in adults with bacterial meningitis. N Engl J Med. 2002;347(20):1549–1556.
Baddour LM, Wilson WR, Bayer AS, et al. Infective Endocarditis in Adults: Diagnosis, Antimicrobial Therapy, and Management of Complications (AHA 2015 Update). Circulation. 2015;132(15):1435–1486.
Fowler VG, Durack DT, Selton-Suty C, et al. The 2023 Duke-ISCVID Criteria for Infective Endocarditis. Clin Infect Dis. 2023;77(4):518–526.
Iversen K, Ihlemann N, Gill SU, et al. Partial oral versus intravenous antibiotic treatment of endocarditis (POET trial). N Engl J Med. 2019;380(5):415–424.
Berbari EF, Kanj SS, Kowalski TJ, et al. IDSA Clinical Practice Guidelines for the Diagnosis and Treatment of Native Vertebral Osteomyelitis. Clin Infect Dis. 2015;61(6):e26–e46.
McDonald LC, Gerding DN, Johnson S, et al. Clinical Practice Guidelines for Clostridioides difficile Infection in Adults and Children: 2017 Update by IDSA/SHEA. Clin Infect Dis. 2018;66(7):e1–e48.
Johnson S, Lavergne V, Skinner AM, et al. Clinical Practice Guideline by the IDSA/SHEA: 2021 Focused Update on Management of CDI in Adults. Clin Infect Dis. 2021;73(5):e1029–e1044.
Gupta K, Hooton TM, Naber KG, et al. International Clinical Practice Guidelines for the Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in Women: IDSA/ESMID 2011. Clin Infect Dis. 2011;52(5):e103–e120.
Workowski KA, Bachmann LH, Chan PA, et al. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep. 2021;70(4):1–187.
Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents with HIV. Department of Health and Human Services (DHHS). Updated 2023.
Panel on Opportunistic Infections in Adults and Adolescents with HIV. Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV. NIH/CDC/IDSA. Updated 2023.
Stevens DL, Bisno AL, Chambers HF, et al. Practice Guidelines for the Diagnosis and Management of Skin and Soft Tissue Infections: 2014 Update by IDSA. Clin Infect Dis. 2014;59(2):e10–e52.
Lipsky BA, Berendt AR, Deery HG, et al. IDSA Clinical Practice Guideline for the Diagnosis and Treatment of Diabetic Foot Infections. Clin Infect Dis. 2012;54(12):e132–e173.
Barlam TF, Cosgrove SE, Abbo LM, et al. Implementing an Antibiotic Stewardship Program: Guidelines by IDSA and SHEA. Clin Infect Dis. 2016;62(10):e51–e77.