Sports Medicine
Every musculoskeletal injury, concussion protocol, rehabilitation strategy, injection technique, classification system, exercise physiology concept, and return-to-play guideline in one place.
01 Musculoskeletal Anatomy Essentials
Sports medicine is the clinical discipline devoted to the prevention, diagnosis, treatment, and rehabilitation of injuries related to physical activity and sport. A thorough understanding of musculoskeletal anatomy — joints, ligaments, tendons, cartilage, and muscle — forms the foundation upon which all clinical decision-making rests.
Joint Structure
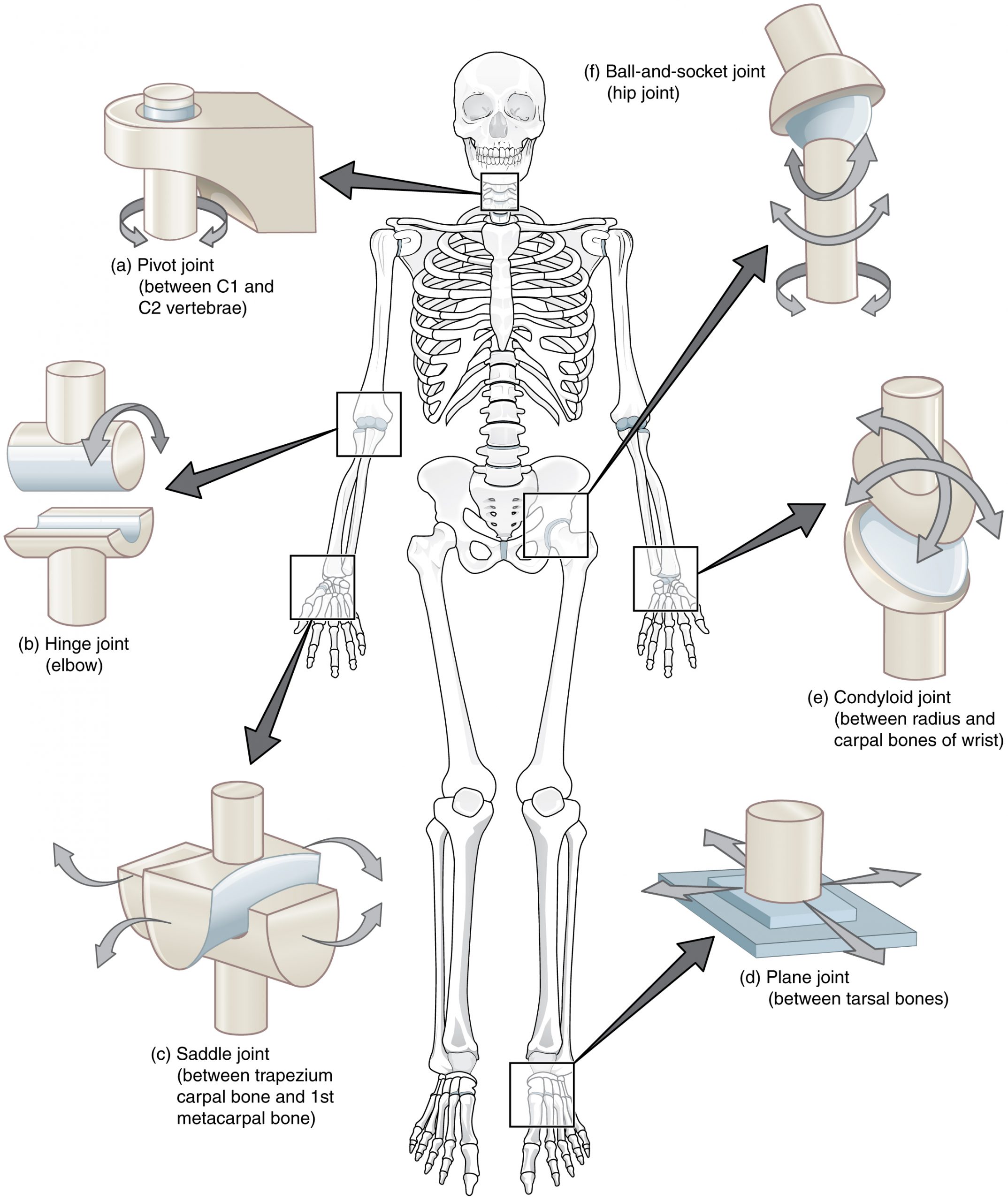
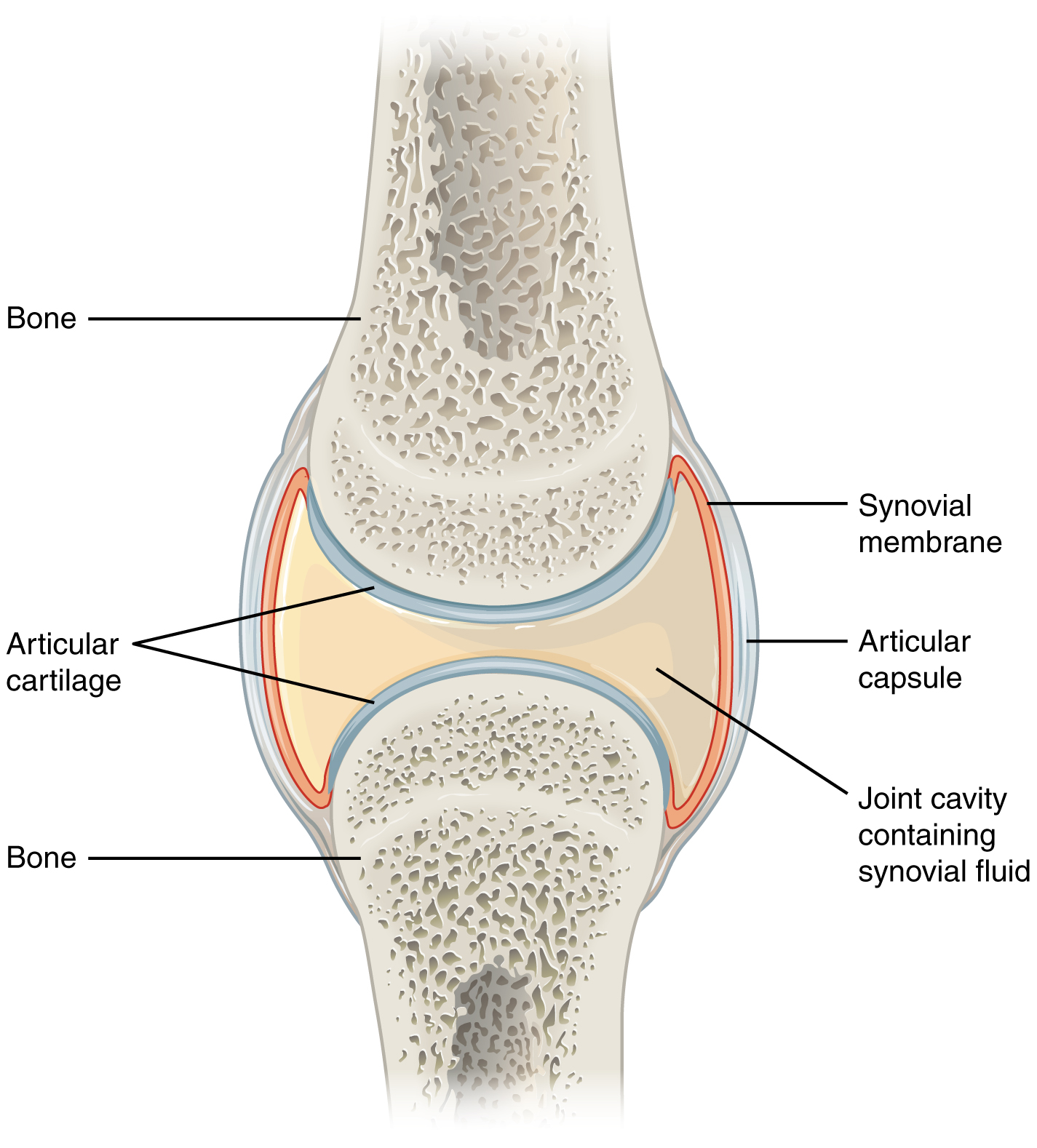
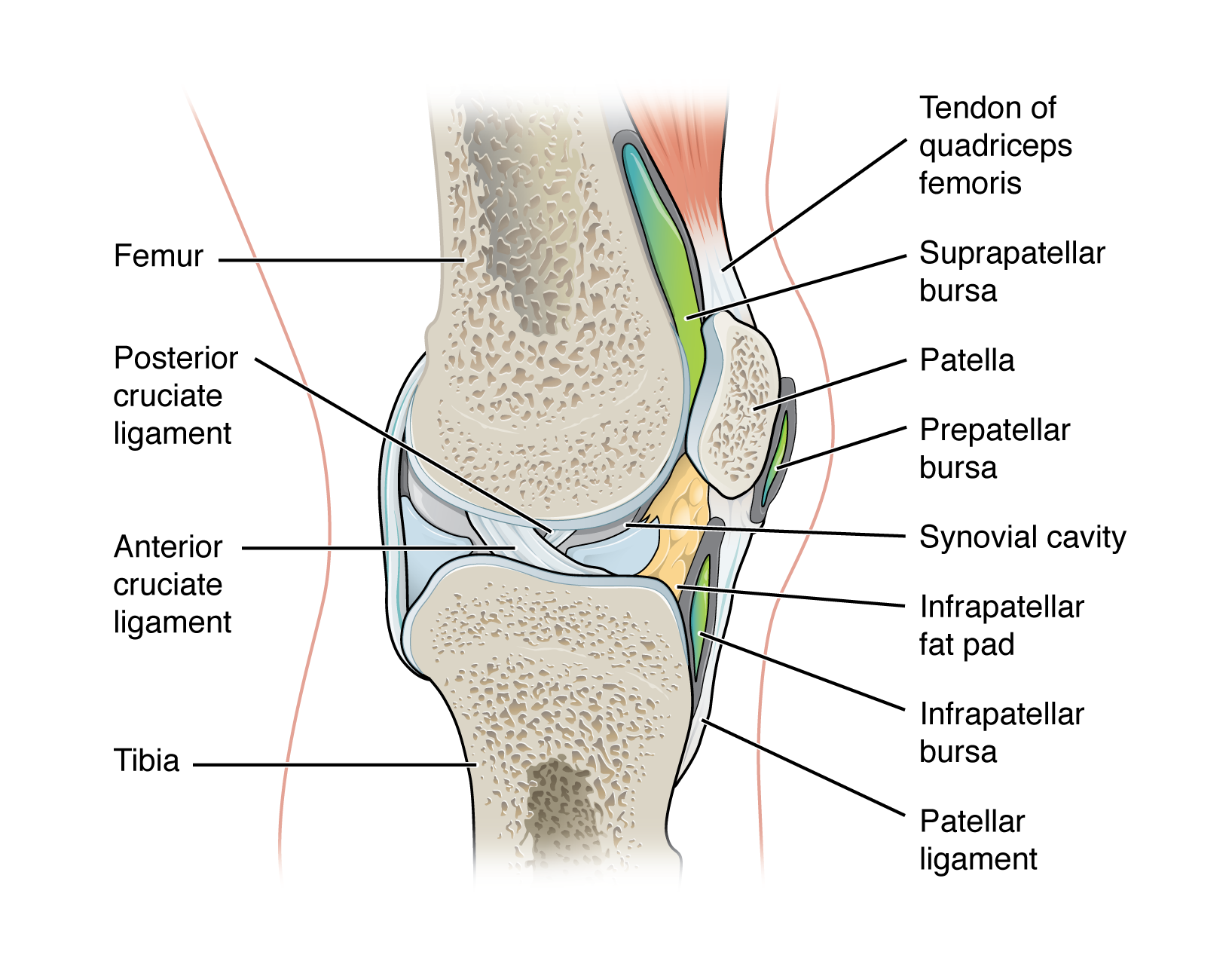
A synovial joint is the most common and most clinically relevant joint type in sports medicine. Components include: (1) articular (hyaline) cartilage — avascular, aneural tissue covering articulating bone surfaces; provides low-friction load-bearing and has very limited healing capacity; (2) synovial membrane — lines the inner joint capsule, produces synovial fluid for lubrication and nutrient delivery; (3) fibrous capsule — dense connective tissue providing structural support; (4) menisci/labra — fibrocartilaginous structures that deepen joint surfaces, distribute load, and improve stability (knee menisci, hip and shoulder labra). Types of synovial joints include hinge (knee, elbow), ball-and-socket (hip, shoulder), pivot (proximal radioulnar), saddle (1st CMC), condyloid (MCP), and plane (acromioclavicular).
Ligaments & Tendons
Ligaments connect bone to bone and provide passive joint stability. They are composed primarily of type I collagen fibers arranged in a somewhat less organized pattern than tendons, allowing slight multidirectional resistance. Key ligaments include the ACL, PCL, MCL, LCL (knee); ATFL, CFL, PTFL (ankle); UCL (elbow and thumb); and the glenohumeral ligaments (shoulder). Tendons connect muscle to bone and transmit contractile force. They are composed of densely packed, parallel type I collagen fibers with a hierarchical structure (collagen fibrils → fibers → fascicles → tendon). The enthesis is the insertion point where tendon attaches to bone — a common site of overuse injury (enthesopathy). Tendons have limited blood supply; areas of relative hypovascularity (e.g., the Achilles tendon 2–6 cm above its calcaneal insertion, the supraspinatus "critical zone") are predisposed to degenerative tendinopathy and rupture.
Cartilage Types
Hyaline cartilage covers articular surfaces, provides smooth gliding, and is primarily composed of type II collagen and proteoglycans (aggrecan). It lacks blood supply, nerve supply, and lymphatic drainage, which severely limits its capacity for self-repair. Fibrocartilage (menisci, labra, intervertebral discs) contains predominantly type I collagen, is tougher and more resistant to compressive and shearing forces, and has variable vascularity — the outer third of the meniscus ("red zone") is vascular and can heal; the inner two-thirds ("white zone") is avascular with poor healing potential. Elastic cartilage (ear, epiglottis) has minimal relevance in sports medicine.
Muscle Fiber Types
| Property | Type I (Slow Twitch) | Type IIa (Fast Oxidative) | Type IIx (Fast Glycolytic) |
|---|---|---|---|
| Contraction speed | Slow | Fast | Fastest |
| Fatigue resistance | High | Moderate | Low |
| Primary metabolism | Oxidative (aerobic) | Oxidative-glycolytic | Glycolytic (anaerobic) |
| Mitochondrial density | High | High | Low |
| Myoglobin content | High (red fibers) | Moderate | Low (white fibers) |
| Motor unit size | Small | Medium | Large |
| Force production | Low | High | Highest |
| Predominant activities | Endurance (marathon, cycling) | Middle-distance running, swimming | Sprinting, jumping, power lifting |
Bone Remodeling & Stress Response
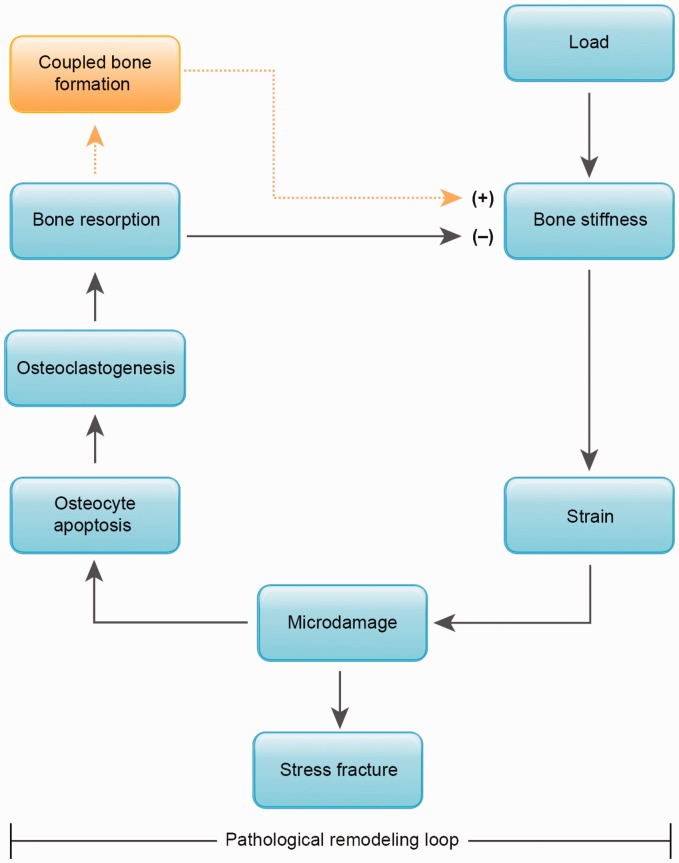
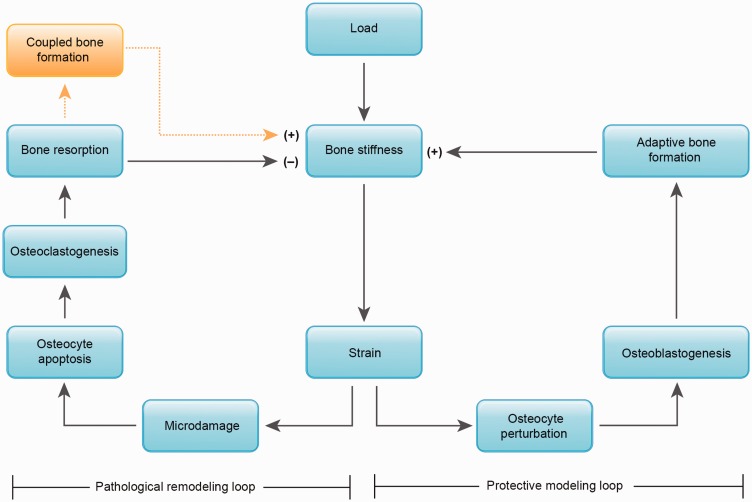
Bone is a dynamic tissue that continuously remodels in response to mechanical loading (Wolff's law). Osteoclasts resorb bone in areas of decreased stress, while osteoblasts deposit new bone where stress is applied. When loading exceeds the bone's capacity to remodel, a stress reaction occurs (periosteal edema on MRI without a fracture line), which can progress to a stress fracture (visible fracture line). The tibia, metatarsals, and navicular are the most common sites. Risk factors include rapid increases in training volume, low bone mineral density, nutritional deficiency (calcium, vitamin D), and hormonal imbalance (amenorrhea, low testosterone).
02 Exercise Physiology
Energy Systems
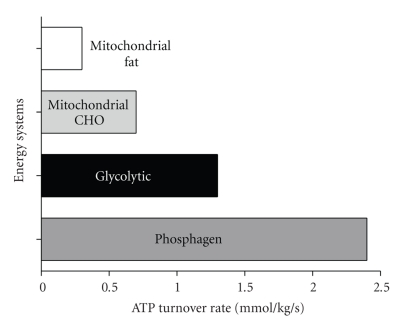
Human movement is powered by three energy systems that operate on a continuum based on exercise intensity and duration:
| Energy System | Substrate | Duration | Rate of ATP Production | Capacity | Examples |
|---|---|---|---|---|---|
| ATP-PCr (Phosphagen) | Stored ATP + phosphocreatine | 0–10 seconds | Fastest | Very limited | 100 m sprint, shot put, vertical jump |
| Anaerobic Glycolysis | Glucose/glycogen → lactate | 10 seconds–2 minutes | Fast | Limited | 400 m sprint, 100 m swim, intense intervals |
| Oxidative (Aerobic) | Carbohydrates, fats, (proteins) | >2 minutes | Slowest | Virtually unlimited | Marathon, cycling, triathlon |
VO2 Max
VO2 max (maximal oxygen consumption) represents the maximum rate at which the body can consume oxygen during maximal exercise — the gold standard measure of cardiorespiratory fitness. Normal values: untrained males ~35–45 mL/kg/min, untrained females ~27–38 mL/kg/min. Elite endurance athletes can achieve >70–85 mL/kg/min. VO2 max is determined by central factors (cardiac output = heart rate × stroke volume) and peripheral factors (arteriovenous O2 difference, muscle mitochondrial density). The Fick equation: VO2 = CO × (CaO2 − CvO2). Training can increase VO2 max by 15–25% through increased stroke volume (eccentric cardiac hypertrophy), blood volume, and mitochondrial biogenesis.
Anaerobic Threshold & Lactate Threshold
The anaerobic threshold (AT) is the exercise intensity at which lactate production begins to exceed clearance, causing blood lactate to rise exponentially. This typically occurs at ~55–65% of VO2 max in untrained individuals and ~75–90% in trained athletes. The ventilatory threshold (VT1) corresponds roughly to the AT and is identified by a nonlinear increase in minute ventilation relative to VO2. The respiratory compensation point (VT2/RCP) is a higher threshold where hyperventilation begins to compensate for metabolic acidosis. Training at or near the anaerobic threshold improves lactate clearance and shifts the threshold rightward (higher percentage of VO2 max).
Cardiac Adaptations to Training
Athlete's heart represents physiologic cardiac remodeling in response to sustained training. Endurance training (running, cycling, swimming) produces volume overload → eccentric hypertrophy (increased LV cavity size with proportional wall thickening). Resistance training (weightlifting, throwing) produces pressure overload → concentric hypertrophy (increased wall thickness with normal or mildly reduced cavity size). Key distinctions from pathologic hypertrophy (HCM): athlete's heart has normal diastolic function, regression with detraining (3–6 months), symmetric hypertrophy, wall thickness typically <13 mm (gray zone 13–15 mm), and no family history of sudden death. Resting bradycardia (40–60 bpm) is a normal finding due to increased vagal tone and stroke volume.
Thermoregulation During Exercise
During exercise, metabolic heat production can increase 15–20-fold. Heat dissipation occurs via evaporation (primary mechanism during exercise; accounts for ~80% of heat loss), convection, radiation, and conduction. When ambient temperature exceeds skin temperature (~33°C) or humidity is high (>75%), evaporative cooling becomes impaired. The wet bulb globe temperature (WBGT) integrates temperature, humidity, wind, and solar radiation — flag conditions for modified activity are typically set at WBGT ≥28°C (82°F). Heat acclimatization over 10–14 days increases plasma volume, sweat rate, sweat onset threshold, and electrolyte conservation.
03 The Sports Medicine Evaluation
Pre-Participation Physical Examination (PPE)
The PPE (also called "sports physical") is performed before athletic participation to identify conditions that may predispose to injury, illness, or sudden death. The PPE consists of: (1) medical history — the most sensitive component; includes personal history of exertional syncope, chest pain, dyspnea, palpitations, seizures, concussion, and musculoskeletal injury; family history of sudden cardiac death <50 years, cardiomyopathy, Marfan syndrome, or arrhythmia; (2) physical examination — vital signs (BP in both arms for coarctation screening), cardiac auscultation in supine and standing (to detect murmurs, especially HCM which increases with Valsalva/standing), Marfan screening (arm span > height, pectus, lens subluxation, arachnodactyly), musculoskeletal screening (90-second MSK exam or 2-minute orthopedic exam); (3) clearance determination — cleared without restriction, cleared with recommendations, or not cleared pending further evaluation.
Sideline Assessment
The sideline assessment is a rapid evaluation performed during competition to determine if an athlete can safely return to play. The approach follows a systematic protocol: (1) primary survey — ABCs (airway, breathing, circulation), cervical spine stabilization if mechanism warrants, level of consciousness; (2) secondary survey — focused history (mechanism, symptoms), inspection (deformity, swelling, ecchymosis), palpation, range of motion, neurovascular exam, special tests; (3) return-to-play decision — based on ability to perform sport-specific tasks without pain, instability, or functional limitation. Athletes with any suspicion of concussion, fracture, dislocation, neurovascular injury, or internal organ injury must be removed from play.
The 90-Second Musculoskeletal Screening Exam
| Instruction | Observation |
|---|---|
| Stand facing examiner | General habitus, symmetry, obvious deformity |
| Look at ceiling, floor, over each shoulder | Cervical spine ROM |
| Shrug shoulders against resistance | Trapezius strength (CN XI) |
| Abduct shoulders 90° against resistance | Deltoid strength |
| Full external rotation of arms | Shoulder ROM, glenohumeral pathology |
| Flex and extend elbows | Elbow ROM |
| Pronate/supinate forearms, clench fists, spread fingers | Forearm/hand function |
| Squat and duck-walk 4 steps | Hip, knee, ankle ROM and stability |
| Stand on toes, then heels | Calf strength, ankle dorsiflexion, balance |
History-Taking Framework for Sports Injuries
Use the OPQRST framework: Onset (acute traumatic vs insidious overuse), Provocation/Palliation (what worsens or improves symptoms), Quality (sharp, dull, burning, aching), Region/Radiation (location, referral patterns), Severity (0–10 pain scale, functional limitation), Timing (duration, progression, relation to activity). Also document: mechanism of injury (contact vs non-contact, position of limb), ability to bear weight or continue playing, previous injuries to the same area, prior treatments, and level of sport participation (recreational, competitive, elite).
04 Key Terminology & Abbreviations
Injury Terminology
Sprain — injury to a ligament (graded I–III). Strain — injury to a muscle or tendon (graded I–III). Tendinopathy — umbrella term for tendon pathology; preferred over "tendinitis" (which implies acute inflammation) or "tendinosis" (which implies chronic degeneration), as most tendon injuries involve a continuum. Enthesopathy — pathology at the tendon-bone insertion. Bursitis — inflammation of a bursa. Contusion — bruise; direct trauma to soft tissue. Avulsion — tearing away of a structure (tendon, ligament, or bone fragment) from its attachment. Dislocation — complete displacement of articular surfaces. Subluxation — partial/incomplete displacement with spontaneous reduction.
Grading Systems Overview
| Grade | Ligament Sprain | Muscle Strain |
|---|---|---|
| Grade I (Mild) | Microscopic ligament fiber disruption; tender, no laxity, minimal swelling | Microscopic muscle fiber disruption; mild pain, <5% strength loss |
| Grade II (Moderate) | Partial macroscopic tear; moderate pain, swelling, laxity with firm endpoint | Partial tear; moderate pain, swelling, 50% strength loss, palpable defect possible |
| Grade III (Severe) | Complete rupture; significant swelling, laxity with no endpoint (may be paradoxically less painful) | Complete rupture; severe pain (or painless), palpable defect, near-complete strength loss |
Essential Abbreviations
| Abbreviation | Meaning |
|---|---|
| ACL / PCL | Anterior / Posterior Cruciate Ligament |
| MCL / LCL | Medial / Lateral Collateral Ligament |
| ATFL / CFL / PTFL | Anterior Talofibular / Calcaneofibular / Posterior Talofibular Ligament |
| UCL | Ulnar Collateral Ligament (elbow or thumb) |
| SLAP | Superior Labrum Anterior to Posterior (tear) |
| RTC | Rotator Cuff |
| FAI | Femoroacetabular Impingement |
| OCD | Osteochondritis Dissecans |
| PFPS | Patellofemoral Pain Syndrome |
| ITBS | Iliotibial Band Syndrome |
| RTP | Return to Play |
| PPE | Pre-Participation Physical Examination |
| SCAT6 | Sport Concussion Assessment Tool, 6th edition |
| RED-S | Relative Energy Deficiency in Sport |
| WADA | World Anti-Doping Agency |
| TUE | Therapeutic Use Exemption |
| PRP | Platelet-Rich Plasma |
| MSK | Musculoskeletal |
| ROM | Range of Motion |
| RICE / POLICE | Rest-Ice-Compression-Elevation / Protection-Optimal Loading-Ice-Compression-Elevation |
| BTB | Bone-Tendon-Bone (patellar tendon autograft) |
| NSAID | Nonsteroidal Anti-Inflammatory Drug |
| CTE | Chronic Traumatic Encephalopathy |
| EIB | Exercise-Induced Bronchoconstriction |
| EAH | Exercise-Associated Hyponatremia |
| WBGT | Wet Bulb Globe Temperature |
05 ACL Injuries
The anterior cruciate ligament (ACL) is the primary restraint to anterior tibial translation and a secondary restraint to tibial rotation. It originates from the posteromedial aspect of the lateral femoral condyle and inserts on the anterior tibial spine. The ACL has two functional bundles: the anteromedial (AM) bundle (tight in flexion) and the posterolateral (PL) bundle (tight in extension).
Mechanism & Epidemiology
ACL injuries occur in approximately 200,000 patients per year in the United States. The classic non-contact mechanism involves sudden deceleration with a cutting or pivoting maneuver — the knee is in slight flexion (10–30°), valgus, and internal rotation with the foot planted. Contact mechanisms include direct lateral knee blow (valgus force). Females have 2–8× higher incidence than males in the same sport, attributed to anatomical factors (narrower intercondylar notch, greater Q-angle, increased tibial slope), hormonal factors (estrogen effects on ligament laxity), neuromuscular factors (quadriceps-dominant landing patterns, decreased hamstring activation). The classic "triad of O'Donoghue" (ACL + MCL + medial meniscus) is now recognized to more commonly involve the ACL + MCL + lateral meniscus.
Physical Examination
| Test | Technique | Positive Finding | Sensitivity / Specificity |
|---|---|---|---|
| Lachman test | Knee at 20–30° flexion; stabilize femur, translate tibia anteriorly | Increased anterior translation with soft/absent endpoint | 85–98% / 95% |
| Anterior drawer test | Knee at 90° flexion, hip at 45°; sit on foot, pull tibia forward | Increased anterior translation | 48–85% / 95% |
| Pivot shift test | Knee extended, apply valgus + internal rotation, then flex; tibia subluxates and reduces | "Clunk" as tibia reduces at ~30° flexion | 35% (awake), >95% (anesthesia) / 98% |
Imaging
Radiographs: may show a Segond fracture (lateral tibial plateau avulsion — pathognomonic for ACL tear) or deep lateral femoral notch sign (>1.5 mm sulcus). MRI is the gold standard (sensitivity 94–97%, specificity 95–100%): findings include discontinuity or abnormal signal of the ACL, bone bruise pattern on the lateral femoral condyle and posterolateral tibial plateau (pivot-shift contusion pattern), associated meniscal tears (50–70% of acute ACL tears have concomitant meniscal injury, most commonly the lateral meniscus acutely).
ACL Reconstruction
Indications for reconstruction include: young, active patients; competitive athletes planning to return to cutting/pivoting sports; combined ligamentous injuries; recurrent instability despite rehabilitation; and associated repairable meniscal tears. Graft options include:
| Graft Type | Source | Advantages | Disadvantages |
|---|---|---|---|
| BTB autograft | Bone-patellar tendon-bone (central 1/3) | Bone-to-bone healing, rigid fixation, gold standard for high-level athletes | Anterior knee pain (15–20%), kneeling pain, patellar fracture risk, donor site morbidity |
| Hamstring autograft | Semitendinosus ± gracilis tendons | Less anterior knee pain, smaller incision, less donor morbidity | Soft tissue-to-bone healing (slower), potential hamstring weakness, slightly higher re-rupture rate in some studies |
| Quadriceps tendon autograft | Central quadriceps tendon ± patellar bone block | Thick, strong graft; less anterior knee pain than BTB; versatile | Quadriceps weakness, evolving technique |
| Allograft | Cadaveric (Achilles, tibialis anterior, BTB) | No donor site morbidity, shorter operative time | Higher re-rupture rate in young athletes (<25 years), delayed incorporation, cost, disease transmission risk (extremely rare) |
Rehabilitation Timeline
Post-ACL reconstruction rehabilitation is typically criterion-based rather than purely time-based: Phase 1 (0–2 weeks) — control swelling, achieve full extension, quadriceps activation, weight-bearing as tolerated; Phase 2 (2–6 weeks) — progressive ROM (goal: 0–120° by 6 weeks), gait normalization, closed-chain strengthening; Phase 3 (6–12 weeks) — progressive strengthening, proprioception, stationary cycling; Phase 4 (3–6 months) — sport-specific drills, agility, running progression; Phase 5 (6–9+ months) — return-to-sport testing. Minimum 9 months before return to sport is generally recommended; criteria include ≥90% limb symmetry index (LSI) on isokinetic quadriceps and hamstring testing, successful completion of hop tests, and psychological readiness.
06 PCL, MCL & LCL Injuries
Posterior Cruciate Ligament (PCL)
The PCL is the strongest ligament of the knee, originating from the anterolateral medial femoral condyle and inserting on the posterior tibial sulcus. It is the primary restraint to posterior tibial translation. The most common mechanism is a dashboard injury (direct blow to the anterior proximal tibia with the knee flexed, driving the tibia posteriorly) or a fall onto a flexed knee. Isolated PCL injuries are often managed nonoperatively with quadriceps-focused rehabilitation. Surgical reconstruction is considered for combined ligamentous injuries (PCL + posterolateral corner) or grade III isolated tears with functional instability.
Posterior drawer test: patient supine, knee flexed 90°; push tibia posteriorly — increased posterior translation compared to the contralateral side. Posterior sag sign (Godfrey test): both hips and knees flexed 90°; the injured tibia sags posteriorly compared to the uninjured side. Grade I: 0–5 mm posterior translation (tibia still anterior to femoral condyles); Grade II: 5–10 mm (tibia flush with condyles); Grade III: >10 mm (tibia posterior to condyles).
Medial Collateral Ligament (MCL)
The MCL is the primary restraint to valgus stress at the knee. It consists of a superficial MCL (broad, from the medial femoral epicondyle to the proximal tibia, 5–7 cm below the joint line) and a deep MCL (thickening of the joint capsule attached to the medial meniscus). Mechanism: valgus force (lateral blow to the knee, e.g., clipping injury in football). Valgus stress testing is performed at 0° and 30° of flexion — laxity at 30° only indicates isolated MCL injury; laxity at both 0° and 30° suggests combined MCL + cruciate injury.
| MCL Grade | Laxity (Valgus Stress at 30°) | Endpoint | Management |
|---|---|---|---|
| Grade I | 0–5 mm opening | Firm | Hinged brace, early ROM, weight-bear as tolerated; RTP 1–3 weeks |
| Grade II | 5–10 mm opening | Soft but present | Hinged brace locked in extension initially, progressive ROM; RTP 3–6 weeks |
| Grade III | >10 mm opening | No endpoint | Hinged brace, evaluate for associated injuries; surgery if combined with ACL tear or persistent valgus instability; RTP 6–12 weeks |
Lateral Collateral Ligament (LCL) & Posterolateral Corner
The LCL (fibular collateral ligament) runs from the lateral femoral epicondyle to the fibular head and is the primary restraint to varus stress. It is part of the posterolateral corner (PLC), which also includes the popliteus tendon and the popliteofibular ligament. PLC injuries are less common but more likely to require surgical reconstruction, as they heal poorly. Mechanism: varus force, hyperextension, or combined rotational injury. Always assess for peroneal nerve injury (foot drop, decreased sensation in the first dorsal web space) with lateral knee injuries. Varus stress testing at 0° and 30° mirrors MCL testing logic: laxity at 30° = isolated; laxity at 0° = combined with cruciate. Dial test (increased external rotation ≥10° at 30° = PLC injury; at 30° AND 90° = PLC + PCL).
07 Meniscal Tears
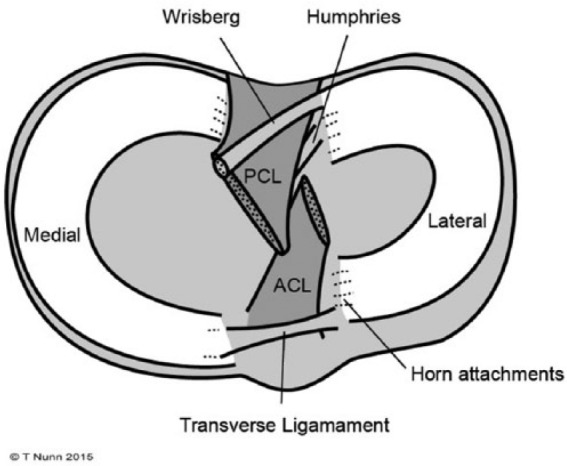
The medial and lateral menisci are C-shaped fibrocartilaginous structures that sit on the tibial plateau, deepening the articular surface, distributing load (transmitting 50% of load in extension, 85% in flexion), absorbing shock, contributing to joint stability, and aiding in lubrication and nutrition of articular cartilage. The medial meniscus is larger, more C-shaped, and firmly attached to the deep MCL and joint capsule (less mobile, more commonly torn). The lateral meniscus is smaller, more circular, and more mobile (attached to the popliteus tendon posteriorly via popliteomeniscal fascicles).
Meniscal Vascularity & Healing Potential
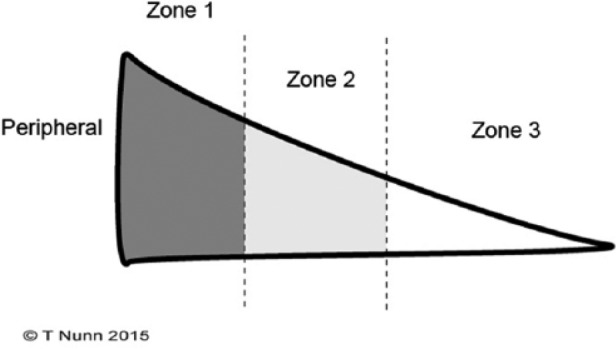
Vascularity is critical for healing: the red-red zone (peripheral 10–25%) has full vascular supply — tears here have good healing potential and are candidates for repair. The red-white zone (middle third) has partial vascularity — variable healing. The white-white zone (inner two-thirds) is avascular — tears here generally do not heal and are managed with partial meniscectomy if symptomatic.
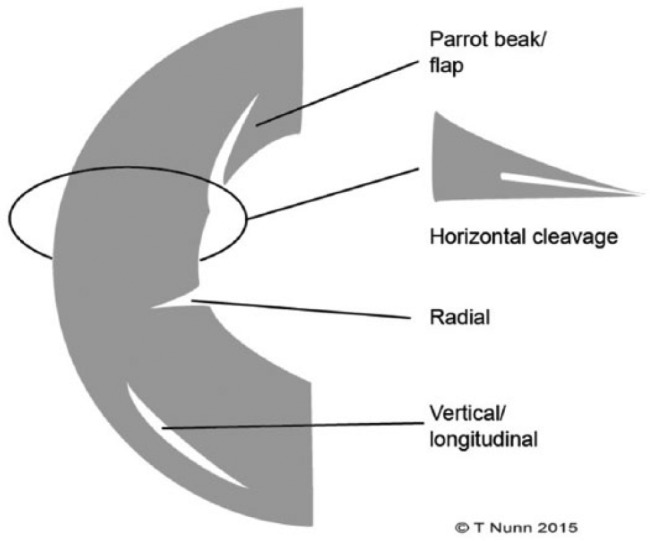
Tear Types
| Tear Type | Description | Clinical Significance |
|---|---|---|
| Longitudinal/Vertical | Runs parallel to the circumferential fibers; follows the meniscal curvature | Often in peripheral (vascular) zone; amenable to repair |
| Bucket-handle | Displaced longitudinal tear; the inner fragment flips into the intercondylar notch | Causes mechanical locking; surgical emergency if locking is present; repair preferred |
| Radial | Runs perpendicular to the circumferential fibers, from free edge toward periphery | Disrupts the meniscal hoop stress mechanism; compromises load distribution |
| Horizontal (cleavage) | Splits the meniscus into superior and inferior leaves | Common in degenerative menisci; may form parameniscal cyst |
| Complex | Combination of multiple tear patterns | Usually degenerative; often managed with partial meniscectomy |
| Root tear | Tear at the meniscal root attachment (posterior root most common) | Functionally equivalent to total meniscectomy; loss of hoop stress; consider repair |
Physical Examination
McMurray test: patient supine, knee maximally flexed; apply valgus stress + external rotation while extending (tests medial meniscus) or varus stress + internal rotation (tests lateral meniscus) — a palpable click or clunk at the joint line is positive (sensitivity 55–70%, specificity 77–97%). Joint line tenderness: palpate along the medial or lateral joint line — sensitivity ~76%, specificity ~29% (very common, non-specific). Thessaly test: patient stands on affected leg with knee flexed at 20°, rotates body — positive if medial or lateral joint line pain/clicking. Apley compression/distraction: prone, knee flexed 90°; compression + rotation = meniscal pain; distraction + rotation = ligamentous pain.
Management: Repair vs Meniscectomy
Meniscal repair is preferred whenever feasible to preserve meniscal function and prevent long-term osteoarthritis. Ideal candidates: tears in the red-red or red-white zone, longitudinal or bucket-handle pattern, <4 cm length, acute/traumatic, associated with concurrent ACL reconstruction (the hemarthrosis from ACL reconstruction promotes meniscal healing). Techniques: all-inside (suture devices), inside-out (vertical mattress sutures), outside-in (anterior horn tears). Partial meniscectomy: indicated for tears in the white-white zone, complex/degenerative tears, or failed repairs. Remove only unstable fragments, preserving as much meniscus as possible. Note: total meniscectomy leads to 3–5× increase in contact pressures and accelerated osteoarthritis — avoid whenever possible.
08 Patellofemoral & Other Knee Conditions
Patellofemoral Pain Syndrome (PFPS)
PFPS is the most common cause of anterior knee pain, especially in young, active females. It is characterized by peripatellar or retropatellar pain aggravated by activities that load the patellofemoral joint: stair climbing/descending, squatting, prolonged sitting ("theater sign"), and running. Pathophysiology is multifactorial: patellar maltracking, quadriceps weakness (especially VMO), hip abductor/external rotator weakness, excessive Q-angle, tight lateral retinaculum, foot pronation. Diagnosis is clinical — imaging is usually not necessary in typical presentations. Management is primarily conservative: VMO strengthening, hip abductor strengthening, patellar taping (McConnell technique), IT band/hamstring stretching, activity modification, NSAIDs for pain. Surgery (lateral retinacular release, tibial tubercle osteotomy) is reserved for refractory cases.
Patellar Instability & Dislocation
Acute lateral patellar dislocation typically occurs with a sudden valgus/external rotation force or direct medial blow during cutting/pivoting. The patella displaces laterally, tearing the medial patellofemoral ligament (MPFL) — the primary soft tissue restraint to lateral patellar displacement (provides ~50–60% of restraining force in early flexion). After reduction (usually spontaneous or with knee extension), assess for osteochondral fracture (present in 25–40% of first-time dislocations; MRI indicated). Risk factors for recurrence: age <18, trochlear dysplasia, patella alta, lateralized tibial tubercle (TT-TG distance >20 mm), increased Q-angle. First-time dislocation without loose body is managed conservatively (immobilization, quadriceps rehab). Recurrent instability or osteochondral fragment warrants surgery (MPFL reconstruction ± tibial tubercle osteotomy ± trochleoplasty).
Iliotibial Band Syndrome (ITBS)
ITBS is the most common cause of lateral knee pain in runners. The IT band is a thickening of the tensor fascia lata that runs from the iliac crest to Gerdy's tubercle on the proximal lateral tibia. Pain occurs at the lateral femoral epicondyle, where the IT band compresses an underlying fat pad and bursae during repetitive knee flexion-extension (the "impingement zone" at ~30° flexion). Symptoms: sharp/burning lateral knee pain, worsening with downhill running, worse at a specific distance ("mile 3 knee"). Ober's test may reveal IT band tightness. Management: activity modification, IT band stretching/foam rolling, hip abductor strengthening, gait retraining, corticosteroid injection if refractory. Surgery (IT band release/Z-plasty) is rarely needed.
Knee Osteoarthritis in Athletes
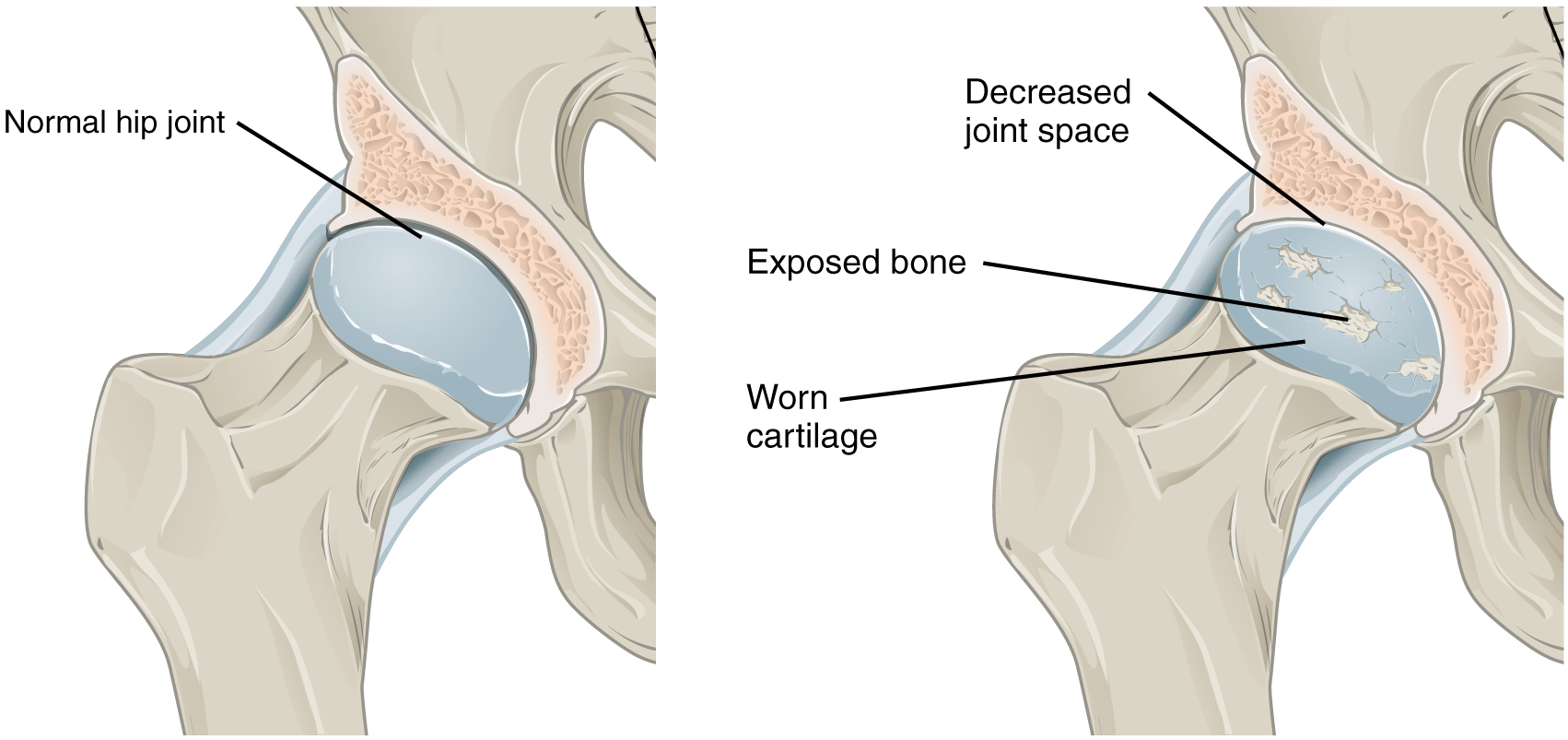
Athletes have increased risk of knee OA due to repetitive joint loading, prior meniscectomy (strongest risk factor), ACL injury, and articular cartilage damage. Prior total meniscectomy increases OA risk ~14-fold. Management in active patients emphasizes activity modification (low-impact cross-training), weight management, strengthening (quadriceps, hip), bracing (unloader brace for unicompartmental disease), intra-articular injections (corticosteroid for flares, hyaluronic acid for maintenance), and ultimately arthroplasty when conservative measures fail. Return to sport after total knee arthroplasty is possible for low-impact activities (cycling, swimming, golf) but high-impact sports are generally not recommended.
09 Rotator Cuff Pathology
The rotator cuff consists of four muscles that stabilize the glenohumeral joint and initiate shoulder motion: Supraspinatus (abduction, most commonly torn), Infraspinatus (external rotation), Teres minor (external rotation), and Subscapularis (internal rotation). Mnemonic: SITS. The supraspinatus passes beneath the coracoacromial arch (acromion, coracoacromial ligament, coracoid process), and repetitive overhead motion or acromial morphology (Type III hooked acromion per Bigliani classification) can cause impingement.

Rotator Cuff Impingement Syndrome
Subacromial impingement is the most common cause of shoulder pain in adults. It represents a spectrum from inflammation of the subacromial bursa and rotator cuff tendons to partial and eventually full-thickness tears. Neer's stages: Stage I — edema and hemorrhage (age <25, reversible); Stage II — fibrosis and tendinitis (age 25–40); Stage III — partial/complete tears, bone spur formation (age >40). External (outlet) impingement: mechanical compression by the coracoacromial arch. Internal impingement: contact between the undersurface of the posterior supraspinatus/infraspinatus and the posterosuperior glenoid rim in the abducted, externally rotated position (common in overhead athletes).
Examination
| Test | Technique | Positive Finding | Tests For |
|---|---|---|---|
| Neer's impingement sign | Passive forward flexion with scapula stabilized | Pain with full forward flexion | Subacromial impingement |
| Hawkins-Kennedy test | Forward flex shoulder 90°, internally rotate | Pain with internal rotation | Subacromial impingement |
| Empty can (Jobe) test | Arms abducted 90°, 30° forward flexion, thumbs down; resist downward force | Weakness or pain | Supraspinatus tear or tendinopathy |
| External rotation lag sign | Elbow at side, 90° flexion; passively externally rotate, release | Arm drops into internal rotation | Infraspinatus/teres minor tear |
| Lift-off test (Gerber) | Hand placed behind back; lift hand off back against resistance | Inability to lift off or weakness | Subscapularis tear |
| Belly press test | Press palm against abdomen; maintain wrist straight | Wrist flexion/inability to maintain pressure | Subscapularis tear |
| Drop arm test | Passively abduct arm to 90°, ask to slowly lower | Arm drops suddenly | Large rotator cuff tear |
Imaging & Classification
Radiographs: evaluate acromion morphology, AC joint osteophytes, superior migration of the humeral head (rotator cuff arthropathy). MRI is the gold standard: partial-thickness tear (graded by Ellman: Grade 1 <3 mm or <25% thickness; Grade 2 3–6 mm or 25–50%; Grade 3 >6 mm or >50%); full-thickness tear (classified by size: small <1 cm, medium 1–3 cm, large 3–5 cm, massive >5 cm or involving ≥2 tendons). Ultrasound is increasingly used — comparable sensitivity/specificity to MRI for full-thickness tears (95%/95%) in experienced hands.
Management
Conservative management is appropriate for impingement, partial tears, and many full-thickness tears in low-demand patients: activity modification, physical therapy (rotator cuff and periscapular strengthening, posterior capsule stretching), subacromial corticosteroid injection (limit to 3–4 per year; evidence for short-term benefit). Surgical repair indications: acute traumatic full-thickness tears in active patients, failed 3–6 months of conservative management, significant weakness (especially in external rotation), full-thickness tears >1 cm in patients <60 years with functional demands. Options: arthroscopic repair (single-row vs double-row fixation), mini-open repair. Massive irreparable tears: superior capsular reconstruction, reverse total shoulder arthroplasty.
10 Shoulder Instability
Anterior Instability (95% of Traumatic Dislocations)
The shoulder is the most commonly dislocated major joint. Anterior dislocation occurs with the arm in abduction, external rotation, and extension (e.g., tackling, throwing). The humeral head displaces anteriorly and inferiorly. Associated injuries: Bankart lesion (avulsion of the anteroinferior labrum from the glenoid rim — the "essential lesion" of anterior instability), Hill-Sachs lesion (compression fracture of the posterolateral humeral head from impaction against the glenoid), bony Bankart (glenoid rim fracture), axillary nerve injury (test deltoid sensation over the lateral arm, "regimental badge area"). Recurrence rate is age-dependent: >90% in patients <20 years, 40–60% in ages 20–30, <10% in patients >40 years (but older patients more likely to have rotator cuff tear with dislocation).
Posterior Instability (2–4%)
Posterior dislocation is rare but frequently missed (50% missed on initial presentation). Classic mechanisms: seizure, electrocution, lightning strike (internal rotators overpower external rotators). The arm is held in internal rotation and adduction; the patient cannot externally rotate. AP radiograph may show the "lightbulb sign" (internally rotated humeral head) and "rim sign" (>6 mm distance between medial humeral head and anterior glenoid rim). Axillary or Y-view radiograph confirms the posterior displacement. Reverse Hill-Sachs lesion (McLaughlin lesion) — compression fracture of the anteromedial humeral head — is the mirror image of the anterior Hill-Sachs.
Multidirectional Instability (MDI)
MDI involves symptomatic instability in more than one direction (typically inferior + anterior and/or posterior). Often bilateral, associated with generalized ligamentous laxity or hypermobility (Beighton score ≥4/9), and seen in overhead athletes (swimmers, volleyball players, gymnasts). The sulcus sign (inferior traction on the arm with the arm at the side produces a visible sulcus between the acromion and humeral head; ≥2 cm or persistence with external rotation is abnormal) is the hallmark test. Treatment is primarily conservative: prolonged rehabilitation focusing on rotator cuff and periscapular strengthening (6–12 months). Surgical intervention (arthroscopic capsular plication/shift) is reserved for failure of 6+ months of rehabilitation.
Physical Examination for Instability
| Test | Technique | Positive Finding |
|---|---|---|
| Apprehension test | Supine; arm abducted 90°, elbow flexed 90°; apply external rotation | Patient apprehension (not just pain) — sense of impending dislocation |
| Relocation test (Jobe) | After positive apprehension, apply posterior force to humeral head | Relief of apprehension |
| Release (surprise) test | After relocation, suddenly release posterior force | Return of apprehension/pain |
| Load and shift test | Seated; load humeral head into glenoid, then translate anteriorly/posteriorly | Grade I: translation to glenoid rim; Grade II: translation over rim with spontaneous reduction; Grade III: translation over rim, no reduction |
| Sulcus sign | Seated, arm at side; apply inferior traction | Visible sulcus ≥2 cm; Grade I: <1 cm; Grade II: 1–2 cm; Grade III: >2 cm |
11 SLAP Tears & Biceps Tendinopathy
SLAP Tears (Superior Labrum Anterior to Posterior)
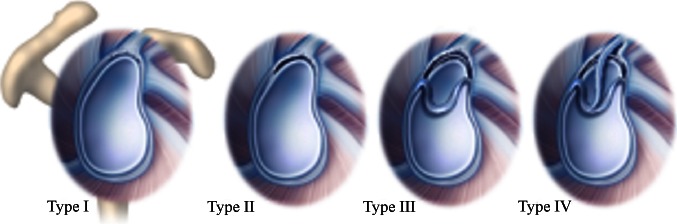
A SLAP tear involves the superior labrum at the attachment of the long head of the biceps tendon. These are common in overhead athletes (throwing, swimming, tennis) and in patients with a fall on an outstretched hand (FOOSH). The Snyder classification:
| Type | Description | Management |
|---|---|---|
| Type I | Degenerative fraying of the superior labrum; biceps anchor intact | Debridement |
| Type II | Superior labrum and biceps anchor are detached from the glenoid (most common, ~55%) | SLAP repair (suture anchors) in young athletes; biceps tenodesis in patients >35–40 years |
| Type III | Bucket-handle tear of the superior labrum; biceps anchor intact | Debridement of displaced fragment; repair if unstable |
| Type IV | Bucket-handle tear extending into the biceps tendon | If <50% biceps involved: debridement + repair; if >50%: biceps tenodesis |
SLAP Examination
O'Brien's test (active compression): arm forward flexed 90°, adducted 10–15°, internally rotated (thumb down); push down against resistance (pain = positive); then repeat in supination (thumb up) — if pain relieved in supination, suggests SLAP or AC joint pathology (deep pain = SLAP, superior/AC pain = AC joint). Biceps load test II: supine, arm abducted 120°, elbow flexed 90°, forearm supinated; ask patient to flex elbow against resistance — pain indicates SLAP tear. Crank test: arm elevated 160°, axial load applied while rotating — pain or clicking is positive.
Proximal Biceps Tendinopathy
The long head of the biceps (LHB) tendon originates from the supraglenoid tubercle and superior labrum, courses through the bicipital groove (stabilized by the transverse humeral ligament and rotator cuff interval), and is a common pain generator in anterior shoulder pain. Tenderness in the bicipital groove is the hallmark finding. Speed's test: resisted forward flexion with elbow extended and forearm supinated — pain in the bicipital groove is positive. Yergason's test: resisted supination with elbow flexed 90° — pain in the bicipital groove is positive. Management: activity modification, physical therapy, corticosteroid injection in the bicipital sheath; if refractory, biceps tenodesis (open or arthroscopic) or tenotomy (elderly/low-demand).
12 AC Joint Injuries & Other Shoulder Conditions
Acromioclavicular (AC) Joint Injuries — Rockwood Classification
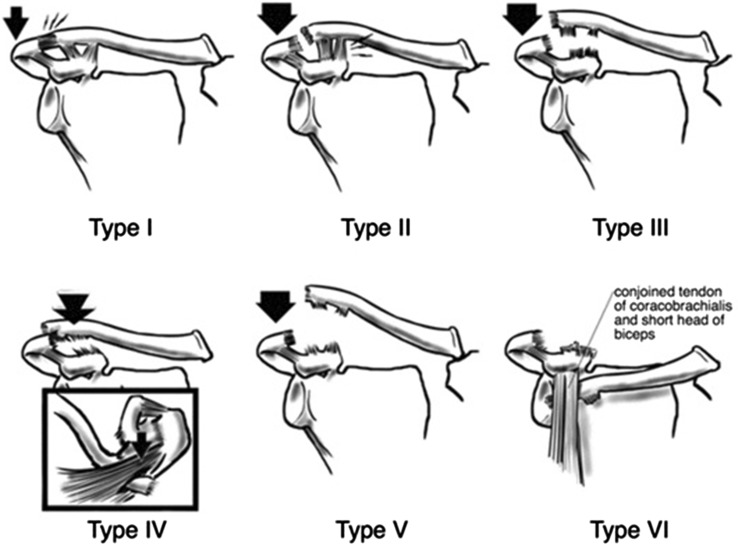
AC joint injuries ("shoulder separations") result from a direct blow to the acromion (fall on the point of the shoulder). The Rockwood classification system fully enumerates six types:
| Type | AC Ligaments | CC Ligaments | Deltotrapezial Fascia | Displacement | Management |
|---|---|---|---|---|---|
| Type I | Sprained, intact | Intact | Intact | None | Sling, ice, early ROM; RTP 1–2 weeks |
| Type II | Torn | Sprained, intact | Intact | Slight vertical (widened AC joint) | Sling, rehab; RTP 2–4 weeks |
| Type III | Torn | Torn | Detached from distal clavicle | Clavicle elevated 25–100% (CC distance increased 25–100% vs normal side) | Controversial; generally conservative for non-laborers/non-overhead athletes; surgery for high-demand overhead athletes or laborers |
| Type IV | Torn | Torn | Detached | Distal clavicle displaced posteriorly into or through the trapezius | Surgical reconstruction |
| Type V | Torn | Torn | Detached | Clavicle elevated 100–300% (gross displacement superiorly); CC distance increased >100% | Surgical reconstruction |
| Type VI | Torn | Torn (or avulsed off clavicle) | Detached | Distal clavicle displaced inferiorly, subacromial or subcoracoid | Surgical reconstruction (extremely rare) |
Adhesive Capsulitis (Frozen Shoulder)
Adhesive capsulitis is characterized by progressive, painful restriction of active AND passive shoulder ROM (unlike rotator cuff pathology, where passive ROM is typically preserved). Three phases: freezing (inflammatory) (2–9 months; gradual onset of pain, progressive loss of ROM); frozen (adhesive) (4–12 months; pain decreases, stiffness persists, ROM plateau); thawing (resolution) (5–24 months; gradual return of ROM). Total duration: 1–3 years. Risk factors: diabetes mellitus (10–20% of diabetics affected), thyroid disease, female sex, age 40–60. External rotation is the most restricted motion. Management: physical therapy (cornerstone), intra-articular corticosteroid injection, hydrodilatation (distension arthrography), manipulation under anesthesia, arthroscopic capsular release (for refractory cases).
Thoracic Outlet Syndrome (TOS)
TOS involves compression of the neurovascular bundle (brachial plexus, subclavian artery/vein) in the thoracic outlet — between the scalene muscles, first rib, and clavicle. Three types: neurogenic TOS (95%, most common; lower trunk/C8-T1 involvement = hand intrinsic weakness and medial forearm/hand numbness); venous TOS (Paget-Schroetter syndrome; upper extremity DVT, arm swelling, cyanosis, especially in overhead athletes); arterial TOS (rare, <1%; ischemic hand, cool/pale extremity). Provocation tests: Adson's test (head rotation + extension toward affected side, deep breath → diminished radial pulse); Roos test (EAST) (arms in surrender position, open/close fists for 3 minutes → reproduction of symptoms); Wright's test (hyperabduction → diminished pulse). Conservative management: physical therapy for scalene stretching, postural training. Surgery (first rib resection, scalenectomy) for refractory neurogenic TOS or vascular TOS.
13 Ankle Sprains (Lateral & Syndesmotic)
Lateral Ankle Sprain
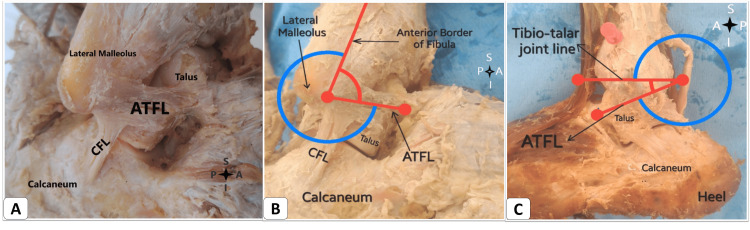
Lateral ankle sprains are the most common sports injury, accounting for ~25% of all musculoskeletal injuries. The mechanism is inversion + plantar flexion. The lateral ligament complex is injured in a predictable sequence based on severity:
| Ligament | Position | Function | Order of Injury |
|---|---|---|---|
| ATFL (Anterior Talofibular) | Anterolateral; distal fibula to talar neck | Resists anterior translation; primary restraint in plantar flexion | First (weakest, most commonly injured) |
| CFL (Calcaneofibular) | Distal fibula to calcaneus; extra-articular | Resists inversion in neutral/dorsiflexion | Second |
| PTFL (Posterior Talofibular) | Posterior fibula to posterior talus | Resists posterior translation and external rotation | Third (strongest, least commonly injured) |
Grading
| Grade | Pathology | Swelling | Weight-Bearing | Anterior Drawer/Talar Tilt | Recovery |
|---|---|---|---|---|---|
| Grade I | ATFL stretch, microscopic tears | Mild | Full weight-bearing | No laxity | 1–3 weeks |
| Grade II | ATFL partial-complete tear ± CFL stretch | Moderate, ecchymosis | Difficulty weight-bearing | Mild laxity with firm endpoint | 3–6 weeks |
| Grade III | Complete ATFL + CFL tear ± PTFL | Severe, diffuse ecchymosis | Unable to bear weight | Significant laxity, no endpoint | 6–12 weeks |
Ottawa Ankle Rules
The Ottawa ankle rules are validated clinical decision rules to determine the need for radiographs (sensitivity 97–100% for fracture, NPV ~99.6%). Ankle radiographs are indicated if there is pain in the malleolar zone AND any of: (1) bone tenderness at the posterior edge or tip of the lateral malleolus, (2) bone tenderness at the posterior edge or tip of the medial malleolus, (3) inability to bear weight both immediately and for 4 steps in the ED. Foot radiographs are indicated if there is pain in the midfoot zone AND: bone tenderness at the base of the 5th metatarsal, bone tenderness at the navicular, or inability to bear weight for 4 steps.
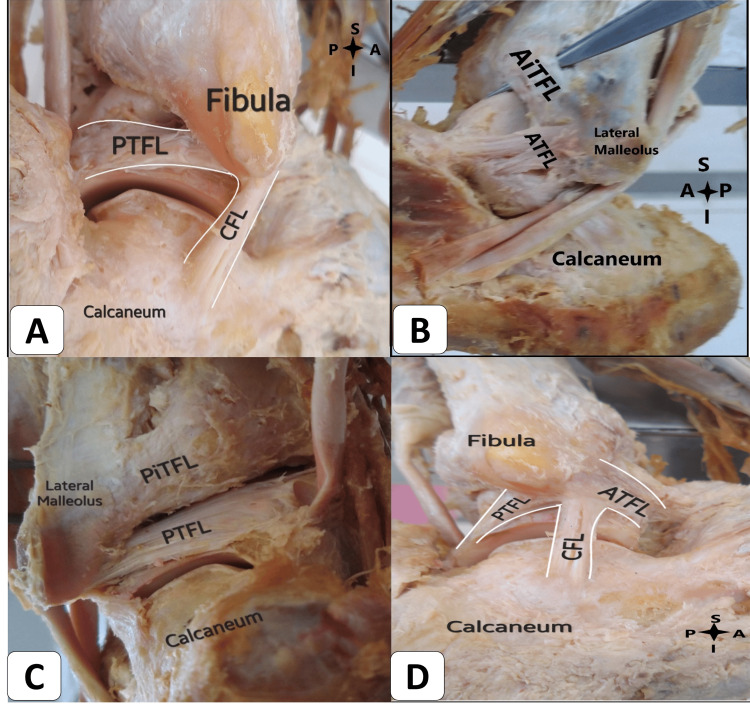
High Ankle Sprain (Syndesmotic Injury)
Syndesmotic sprains (high ankle sprains) involve the anterior inferior tibiofibular ligament (AITFL), posterior inferior tibiofibular ligament (PITFL), transverse tibiofibular ligament, and interosseous membrane. Mechanism: forced external rotation and/or dorsiflexion of the ankle. More common in football, hockey, skiing. Recovery is significantly longer than lateral sprains (6–12 weeks vs 1–6 weeks). Examination: squeeze test (compress tibia and fibula at mid-calf — pain at the syndesmosis is positive; sensitivity ~30%, specificity ~93%); external rotation stress test (stabilize leg, externally rotate the foot — pain at the syndesmosis); fibula translation test; tenderness proximal to the ankle joint along the interosseous membrane. If diastasis is present on radiographs (tibiofibular clear space >6 mm on AP, overlap <6 mm on AP or <1 mm on mortise view), surgical fixation with syndesmotic screws or suture button devices is indicated.
Return-to-Play Criteria (Ankle Sprain)
RTP requires: full pain-free ROM, ≥90% strength of the uninvolved side (especially eversion and inversion), successful completion of functional tests (hopping, cutting, figure-of-eight running), ability to perform sport-specific tasks without pain or apprehension, and adequate proprioceptive function. Bracing or taping is recommended for the first 6–12 months after return to sport. Chronic ankle instability develops in ~20–30% of patients after lateral ankle sprain and may require modified Brostrom repair (anatomic ligament reconstruction).
14 Achilles Tendinopathy & Rupture
Achilles Tendinopathy
The Achilles tendon is the thickest and strongest tendon in the body, formed by the confluence of the gastrocnemius and soleus muscles, inserting on the posterior calcaneus. Insertional tendinopathy occurs at the calcaneal insertion (associated with Haglund's deformity, retrocalcaneal bursitis, and calcific tendinopathy). Non-insertional (midsubstance) tendinopathy occurs 2–6 cm proximal to the insertion, in the "watershed zone" of relative hypovascularity. Risk factors: age >30, male sex, fluoroquinolone use, overtraining (rapid increase in volume/intensity), obesity, flat feet. Histopathology shows mucoid degeneration, neovascularization, and disorganized collagen (tendinosis, not tendinitis). Management: eccentric strengthening exercises (Alfredson protocol — 3 × 15 reps, twice daily for 12 weeks; superior to concentric exercise), load management, heel lifts, shockwave therapy (ESWT), topical nitroglycerin, PRP injection (evidence mixed). Corticosteroid injection is generally AVOIDED in and around the Achilles tendon due to increased rupture risk.
Avoid corticosteroid injection in or around the Achilles tendon. Corticosteroid injection near the Achilles tendon is associated with significantly increased risk of rupture. If pain relief is needed, consider alternatives such as peritendinous injection (not intratendinous), PRP, or shockwave therapy.
Achilles Tendon Rupture
Acute Achilles rupture typically occurs in the "weekend warrior" (male, age 30–50, intermittent high-intensity activity). Mechanism: sudden eccentric dorsiflexion force (pushing off, jumping, sprinting). The patient reports a sudden "pop" or sensation of being kicked in the back of the leg, followed by difficulty with push-off and stair climbing. Physical findings: palpable gap in the tendon (2–6 cm above calcaneus), weakness of plantar flexion (but not absent — the plantaris, tibialis posterior, and peroneals contribute to plantar flexion), positive Thompson test (squeeze the calf with the patient prone, knee flexed to 90° — absence of passive plantar flexion indicates rupture; sensitivity ~96%, specificity ~93%). Imaging: ultrasound is fast and diagnostic; MRI if clinical uncertainty exists.
Operative vs Non-Operative Management
| Factor | Operative Repair | Non-Operative (Functional Rehabilitation) |
|---|---|---|
| Re-rupture rate | 1–4% | 3–12% (with accelerated functional protocol: ~4%) |
| Return to sport | Earlier (4–6 months) | Slightly later (5–7 months) |
| Complications | Wound infection (4–10%), sural nerve injury, adhesions | Fewer wound complications |
| Strength recovery | Slightly better peak plantar flexion strength | Comparable in most studies with accelerated rehab |
| Best for | Young, active, athletes, delayed presentation | Older, sedentary, medical comorbidities; gap <1 cm on ultrasound with plantar flexion |
15 Stress Fractures, Lisfranc & Other Foot Injuries
Stress Fractures
Stress fractures result from repetitive submaximal loading that overwhelms bone's remodeling capacity. They are categorized as low-risk (compressive side of bone; tibial shaft, fibula, metatarsal shafts 2–4, calcaneus — heal well with activity modification) or high-risk (tension side or poor vascular supply; femoral neck, anterior tibial cortex "dreaded black line," navicular, 5th metatarsal, medial malleolus, sesamoids — high rate of nonunion, delayed union, or complete fracture; require more aggressive management).
5th Metatarsal Fracture Zones
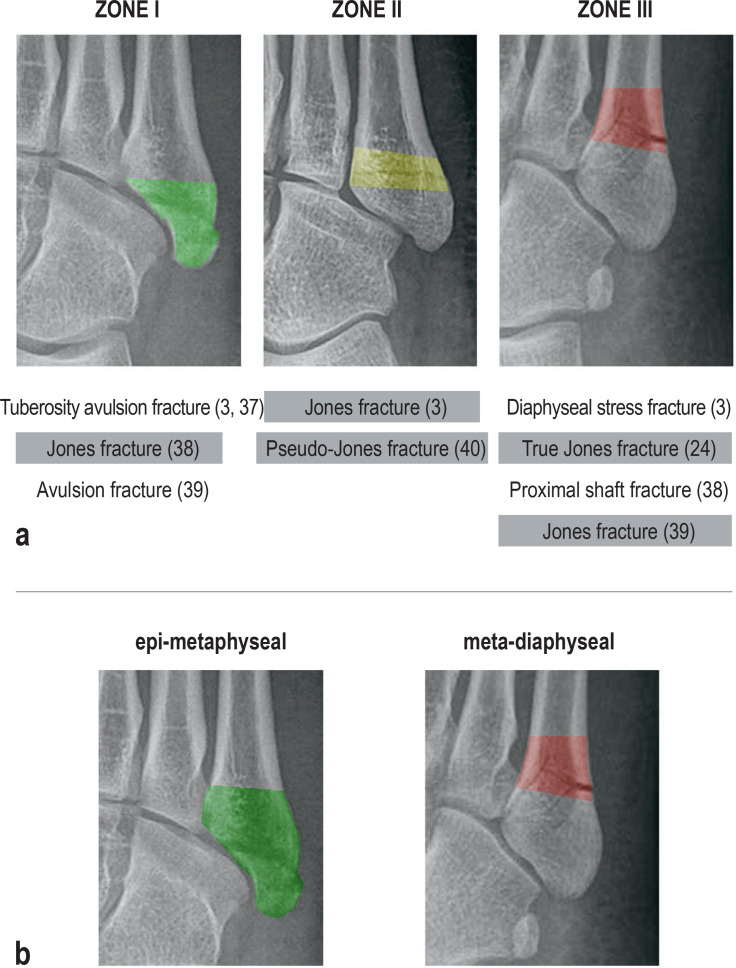
| Zone | Location | Name | Mechanism | Management |
|---|---|---|---|---|
| Zone 1 | Tuberosity (styloid process) | Avulsion fracture ("pseudo-Jones") | Inversion/plantar flexion; peroneus brevis avulsion | Hard-soled shoe or walking boot; weight-bear as tolerated; heals well (4–6 weeks) |
| Zone 2 | Metaphyseal-diaphyseal junction | Jones fracture | Acute adduction force on a plantar-flexed foot | High-risk fracture; non-weight-bearing cast 6–8 weeks OR intramedullary screw fixation (preferred in athletes for faster RTP) |
| Zone 3 | Proximal diaphysis | Diaphyseal stress fracture | Chronic repetitive loading | Highest risk of nonunion; intramedullary screw fixation recommended, especially in athletes |
Navicular Stress Fracture
The navicular stress fracture is a high-risk stress fracture that is commonly seen in sprinters, basketball players, and other explosive-sport athletes. Symptoms: vague, insidious dorsal midfoot pain with activity; point tenderness over the dorsal navicular ("N-spot"). Radiographs are often negative initially; MRI or CT is needed for diagnosis. The fracture typically occurs in the central third of the navicular (relatively avascular zone). Management: non-weight-bearing cast for 6–8 weeks with serial imaging; or internal fixation with percutaneous screw(s) for displaced fractures or athletes requiring faster return.
Fredericson MRI Stress Fracture Grading
| Grade | STIR/T2 (Periosteal Edema) | T1 (Marrow Signal) | Fracture Line |
|---|---|---|---|
| Grade 1 | Mild periosteal edema | Normal | Absent |
| Grade 2 | Moderate periosteal edema | Abnormal (bone marrow edema) | Absent |
| Grade 3 | Moderate-severe periosteal edema | Abnormal (bone marrow edema) | Absent |
| Grade 4a | Severe periosteal edema | Abnormal | Intracortical signal abnormality (visible fracture line) |
| Grade 4b | Severe periosteal edema | Abnormal | Visible fracture line on T1 and T2 |
Lisfranc Injury
The Lisfranc joint complex is the tarsometatarsal (TMT) articulation. The Lisfranc ligament connects the medial cuneiform to the base of the 2nd metatarsal (the "keystone" of the midfoot) and is the critical stabilizer. Mechanism: axial loading on a plantar-flexed foot (e.g., football player falling on another player's heel), or rotational force. The injury is commonly missed (20% missed on initial evaluation). Clinical findings: midfoot swelling, plantar ecchymosis (highly specific), pain with passive pronation-abduction of the forefoot, inability to bear weight. Radiographs: assess for loss of alignment between the medial border of the 2nd metatarsal and the medial border of the middle cuneiform on the AP view, and loss of alignment between the medial border of the 4th metatarsal and the medial border of the cuboid on the oblique view. Diastasis >2 mm between the 1st and 2nd metatarsal bases (on weight-bearing views) is diagnostic. CT for subtle injuries. Management: non-displaced, stable injuries may be treated with non-weight-bearing cast for 6–8 weeks; displaced or unstable injuries require ORIF or primary arthrodesis.
Turf Toe
Turf toe is a hyperextension sprain of the first metatarsophalangeal (MTP) joint, involving the plantar plate and sesamoid complex. Named for its association with artificial turf surfaces. Common in football linemen and dancers. Grade I: stretching of the plantar plate (play as tolerated); Grade II: partial tear, moderate swelling (2–4 weeks); Grade III: complete disruption, possible sesamoid fracture or dislocation (6–12 weeks, may require surgery if sesamoid retraction or hallux valgus deformity develops).
16 Sport-Related Concussion
Sport-related concussion (SRC) is a traumatic brain injury induced by biomechanical forces, resulting in a complex pathophysiological process affecting the brain. Key features from the Amsterdam/Berlin consensus (6th International Conference on Concussion in Sport): concussion is a functional disturbance rather than a structural injury; standard neuroimaging (CT, MRI) is typically normal; symptoms reflect a functional disturbance rather than structural damage; concussion results in a set of clinical signs and symptoms that may or may not involve loss of consciousness (LOC occurs in <10% of concussions).
Sideline Assessment (SCAT6)
The Sport Concussion Assessment Tool, 6th edition (SCAT6) is the standardized sideline assessment for athletes aged ≥13 years (Child SCAT6 for ages 5–12). Components include:
| Component | Details |
|---|---|
| Immediate assessment (on-field) | Observable signs (LOC, lying motionless, tonic posturing, motor incoordination, blank stare, facial injury); red flags requiring emergency transport (neck pain, double vision, weakness/tingling, seizure, deteriorating consciousness, vomiting) |
| Maddocks questions | Sport-specific orientation questions (not generic orientation): "What venue are we at?" "Which half is it now?" "Who scored last?" "What team did you play last?" "Did your team win the last game?" |
| Glasgow Coma Scale | Eye opening (1–4), verbal (1–5), motor (1–6); GCS <15 warrants emergency evaluation |
| Symptom evaluation | 22-item symptom checklist (headache, dizziness, fogginess, etc.) rated 0–6 severity |
| Cognitive screening | Orientation (month, date, day, year, time), immediate memory (word list recall), concentration (digits backward, months in reverse) |
| Neurological screening | Speech assessment, reading, cervical spine exam, finger-to-nose, tandem gait |
| Balance (modified BESS) | Double leg, single leg, tandem stance with eyes closed on firm surface; error counting |
| Delayed recall | Word list recall after 5–10 minutes |
Any athlete suspected of having a concussion must be immediately removed from play and must not return to play on the same day. "When in doubt, sit them out." Athletes with red flags (deteriorating LOC, seizure, vomiting, worsening headache, focal neurological deficits, neck pain) require emergency medical evaluation and cervical spine immobilization.
Concussion Pathophysiology
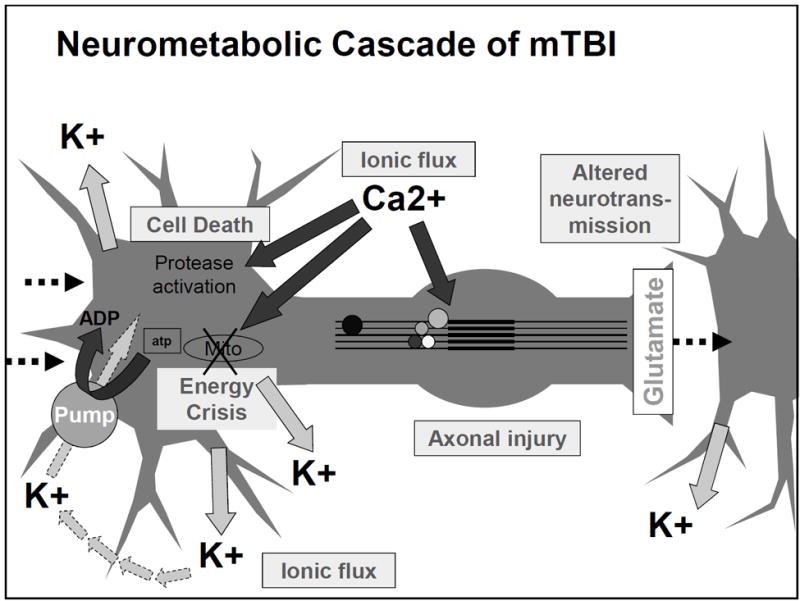
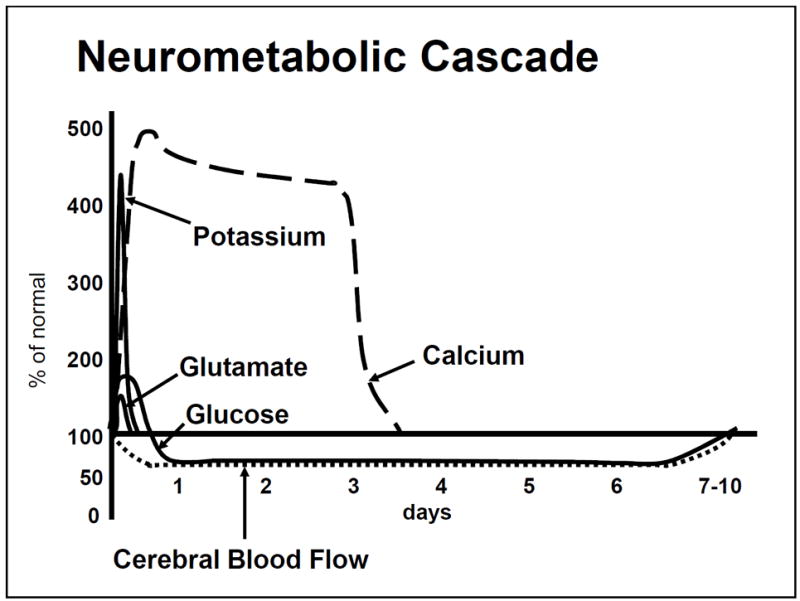
Concussion triggers a neurometabolic cascade: (1) ionic flux — indiscriminate release of excitatory neurotransmitters (glutamate) causing K+ efflux and Na+/Ca2+ influx; (2) energy crisis — Na+/K+-ATPase pump works overtime to restore ionic balance, increasing glucose demand in the setting of decreased cerebral blood flow; (3) mitochondrial dysfunction — intracellular Ca2+ accumulation impairs oxidative phosphorylation; (4) axonal injury — cytoskeletal disruption from shearing forces; (5) inflammation — microglial activation, cytokine release. This metabolic mismatch between energy supply and demand creates a "window of vulnerability" where the brain is susceptible to worsened injury from repeat trauma (basis for second impact syndrome). Resolution typically occurs over 7–14 days in most adults, though may take longer in children/adolescents.
17 Return-to-Play & Post-Concussion Syndromes

Graduated Return-to-Play Protocol (Berlin/Amsterdam Consensus)
The 6-step graduated return-to-play (RTP) protocol is criterion-based and each step takes a minimum of 24 hours. If any symptoms recur, the athlete returns to the previous asymptomatic step. The athlete must be symptom-free at rest before beginning Step 1.
| Step | Activity | Objective |
|---|---|---|
| Step 1 | Symptom-limited activity: daily activities that do not provoke symptoms (e.g., walking, light reading) | Gradual reintroduction of work/school activities |
| Step 2 | Light aerobic exercise: walking, swimming, or stationary cycling at <70% max HR; no resistance training | Increase heart rate |
| Step 3 | Sport-specific exercise: running drills, skating drills; no head-impact activities | Add movement |
| Step 4 | Non-contact training drills: progressive resistance training, complex drills; may begin sport-specific practice | Exercise, coordination, and increased thinking |
| Step 5 | Full-contact practice: following medical clearance; participate in normal training activities | Restore confidence and assess functional skills by coaching staff |
| Step 6 | Return to sport: normal game play | Full return to competition |
Post-Concussion Syndrome (PCS)
Post-concussion syndrome refers to persistent symptoms lasting >10–14 days in adults or >4 weeks in children. Symptoms include headache, dizziness, cognitive dysfunction (difficulty concentrating, memory problems), sleep disturbances, mood changes (irritability, anxiety, depression), and visual disturbances. Risk factors: female sex, prior concussions, history of migraines, psychiatric history, younger age, greater initial symptom burden. Management is multidisciplinary: cervicogenic headache treatment (manual therapy, exercise), vestibular rehabilitation (for dizziness/balance issues), vision therapy, graded aerobic exercise (sub-symptom threshold exercise training), cognitive behavioral therapy, and pharmacotherapy (amitriptyline or topiramate for post-traumatic headache; melatonin for sleep; SSRIs for mood symptoms).
Second Impact Syndrome (SIS)
Second impact syndrome occurs when an athlete sustains a second concussion before fully recovering from the first. This can cause catastrophic cerebral edema due to loss of cerebrovascular autoregulation, with mortality rates of approximately 50% and near-100% morbidity among survivors. Although rare and debated (some question whether SIS is a distinct entity vs severe diffuse cerebral swelling), it forms the basis of the universal "same-day return-to-play" prohibition and the graduated RTP protocol.
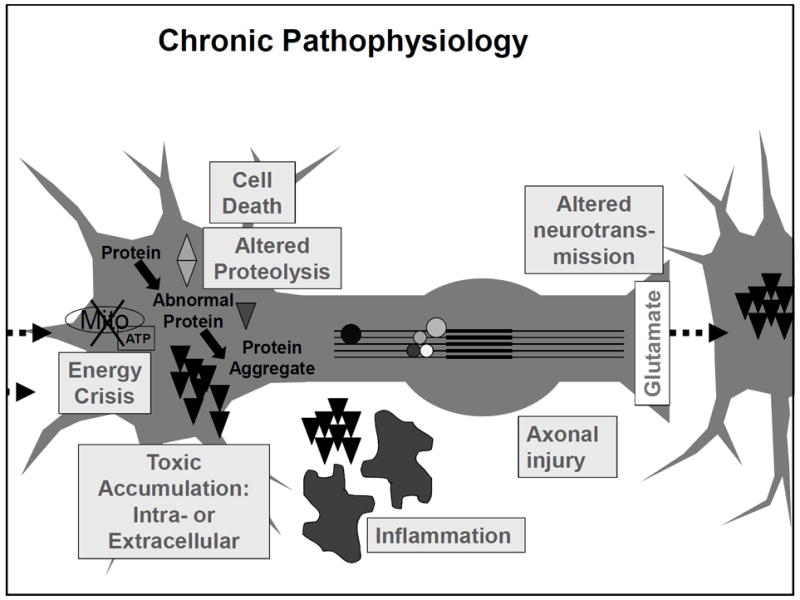
Chronic Traumatic Encephalopathy (CTE)
CTE is a progressive neurodegenerative disease associated with repetitive head trauma (both concussive and subconcussive impacts). Currently a post-mortem diagnosis only — confirmed by neuropathologic identification of perivascular accumulation of hyperphosphorylated tau protein (p-tau) in neurons at the depths of cortical sulci (pathognomonic pattern). Clinical features (in life, termed "traumatic encephalopathy syndrome" or TES): early — mood/behavioral changes (depression, impulsivity, aggression, suicidality); later — cognitive impairment (memory loss, executive dysfunction), motor symptoms (parkinsonism). Risk factors: duration of exposure to contact sports (>10 years), number of concussions, age of first exposure, APOE ε4 genotype (possible modifier). No disease-modifying treatment currently exists; management is supportive.
18 Cervical Spine Injuries & Exertional Heat Illness
Cervical Spine Injury in Sports
Any athlete with a mechanism suggesting cervical spine injury (axial loading, hyperflexion, hyperextension, significant head trauma with neck pain or neurological symptoms) requires immediate cervical spine immobilization.
On-field management: Activate EMS. Maintain cervical spine immobilization (manual in-line stabilization). If the athlete is wearing a helmet (football, hockey, lacrosse), leave the helmet AND shoulder pads in place to maintain neutral alignment. Only remove the face mask (not the helmet) to access the airway. Log-roll onto a spine board. Transport for imaging.
Canadian C-Spine Rules vs NEXUS Criteria
| Feature | Canadian C-Spine Rules | NEXUS Criteria |
|---|---|---|
| Approach | Sequential algorithm (high-risk → low-risk → ROM assessment) | 5 criteria that must ALL be met to clear |
| High-risk factors mandating imaging | Age ≥65, dangerous mechanism, paresthesias in extremities | N/A (not stratified by risk) |
| Low-risk factors permitting ROM assessment | Simple rear-end MVC, sitting in ED, ambulatory, delayed onset neck pain, no midline C-spine tenderness | N/A |
| Criteria to clear without imaging | No high-risk factors + any low-risk factor present + able to actively rotate neck 45° left and right | No posterior midline tenderness, no focal neurological deficit, normal alertness, no intoxication, no distracting injury |
| Sensitivity | 99.4% | 99.0% |
| Specificity | 45.1% (higher) | 12.9% (lower) |
Burners & Stingers
Burners/stingers are transient brachial plexus injuries, most common in football (up to 65% of college football players experience at least one). Mechanisms: (1) traction — lateral neck flexion away from the involved side with shoulder depression (stretches upper trunk C5-C6); (2) compression — lateral neck flexion toward the involved side (compresses nerve root in the foramen; more common in older athletes with cervical stenosis or foraminal stenosis). Symptoms: unilateral, transient burning pain/numbness radiating from the shoulder down the arm, with brief weakness of shoulder abduction and elbow flexion (C5-C6 distribution). Resolves within seconds to minutes (occasionally days). Bilateral symptoms, lower extremity involvement, or persistent deficits (>2 weeks) mandate cervical spine imaging (MRI) to rule out spinal cord injury, herniated disc, or spinal stenosis.
Exertional Heat Illness
| Feature | Heat Exhaustion | Exertional Heat Stroke |
|---|---|---|
| Core temperature | 37–40°C (98.6–104°F) | ≥40°C (104°F) (rectal temperature is the gold standard) |
| CNS function | Normal or mildly impaired (fatigue, lightheadedness, mild confusion) | Altered mental status (confusion, delirium, seizure, coma) — the defining feature |
| Sweating | Profuse | Variable (may or may not be sweating) |
| Skin | Pale, cool, clammy | Hot (may be dry or wet) |
| Vital signs | Tachycardia, hypotension, tachypnea | Tachycardia, hypotension, tachypnea |
| End-organ damage | Absent | Present: rhabdomyolysis, DIC, AKI, hepatic failure, ARDS |
| Management | Remove from heat, cool environment, oral rehydration, rest | Immediate cold-water immersion (most effective), target cooling to <38.9°C within 30 minutes; IV fluids; monitor for end-organ dysfunction |
| Disposition | May resume activity after full recovery and adequate rehydration | Hospital admission; mortality up to 10% with delayed treatment |
Cool first, transport second. Exertional heat stroke is a medical emergency with a 100% survival rate if cooling is initiated within 10 minutes. Cold-water immersion (CWI) to the neck is the gold standard treatment — cooling rate of ~0.2°C/min. Rectal temperature is the ONLY reliable field measure of core temperature (oral, axillary, tympanic, and temporal artery thermometry are inaccurate during exercise). Target cooling to <38.9°C (102°F).
19 Epicondylitis & UCL Injury
Lateral Epicondylitis (Tennis Elbow)
Lateral epicondylitis is the most common cause of lateral elbow pain, affecting 1–3% of the general population. Despite the name, the primary pathology is angiofibroblastic tendinosis (degenerative, not inflammatory) of the extensor carpi radialis brevis (ECRB) origin at the lateral epicondyle. It is an overuse injury common in tennis (especially with poor backhand technique), manual labor, and repetitive gripping activities. Peak incidence: age 35–50. Examination: tenderness at the lateral epicondyle, pain with resisted wrist extension (especially with the elbow extended and forearm pronated), positive Cozen's test (resisted wrist extension with elbow flexed) and Mill's test (pain on passive wrist flexion with elbow extended). Management: activity modification, counterforce (tennis elbow) strap, eccentric strengthening (wrist extension eccentrics), physical therapy, topical NSAIDs. Corticosteroid injection provides short-term relief (6–12 weeks) but may worsen long-term outcomes. PRP injection shows promising evidence. Surgical debridement (open or arthroscopic) for refractory cases (>6–12 months of conservative treatment). Natural history: ~90% improve with conservative management within 12–18 months.
Medial Epicondylitis (Golfer's Elbow)
Medial epicondylitis affects the common flexor-pronator origin (primarily flexor carpi radialis and pronator teres) at the medial epicondyle. Less common than lateral epicondylitis (ratio ~1:3–7). Common in golf (especially amateur golfers with faulty swing mechanics), throwing sports, overhead sports, and occupations requiring repetitive wrist flexion/pronation. Examination: tenderness at the medial epicondyle, pain with resisted wrist flexion and pronation. Important: evaluate the ulnar nerve (runs in the cubital tunnel posterior to the medial epicondyle) — ulnar nerve symptoms (paresthesias in the ring/small fingers) occur in 50–60% of patients with medial epicondylitis. Management is analogous to lateral epicondylitis: activity modification, counterforce strap, eccentric strengthening, physical therapy, corticosteroid injection (use caution near the ulnar nerve), and surgical debridement if conservative management fails.
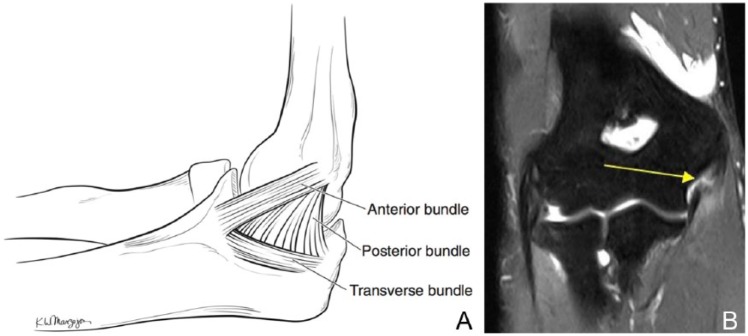
UCL Injury of the Elbow (Tommy John Injury)
The ulnar collateral ligament (UCL) of the elbow is the primary restraint to valgus stress. The anterior bundle (the most important functionally) originates from the medial epicondyle and inserts on the sublime tubercle of the ulna. UCL injury is epidemic in overhead-throwing athletes (baseball pitchers), caused by repetitive valgus stress during the late cocking and early acceleration phases of throwing. The UCL experiences near-failure tensile loads (~35 Nm) with every throw. Presentation: medial elbow pain with throwing (especially during the acceleration phase), decreased velocity and control, +/- ulnar nerve symptoms.
UCL Examination
| Test | Technique | Positive Finding |
|---|---|---|
| Valgus stress test | Elbow flexed 25–30° (to unlock the olecranon from the fossa); apply valgus force | Medial joint line opening, pain, or soft endpoint |
| Moving valgus stress test | Elbow fully flexed with valgus load applied; quickly extend the elbow while maintaining valgus stress | Reproduction of medial elbow pain at 70–120° of flexion ("shear angle"); sensitivity 100%, specificity 75% |
| Milking maneuver | Elbow flexed >90°; pull the thumb while applying valgus stress | Medial elbow pain, apprehension |
Imaging: MRI with intra-articular contrast (MR arthrogram) is the gold standard — a "T-sign" (contrast leaking beneath the UCL at the sublime tubercle) indicates undersurface tearing. Dynamic ultrasound can show medial joint space widening with valgus stress (>1 mm side-to-side difference is suggestive). Management: partial tears in non-throwing athletes may respond to PRP injection + rehabilitation (6–12 months). UCL reconstruction ("Tommy John surgery"): figure-of-eight or docking technique using palmaris longus autograft (or gracilis tendon); return to competition at pre-injury level in 80–90% of cases; typical timeline: 12–18 months to return to competitive throwing.
20 Distal Biceps, Scaphoid & Wrist Injuries
Distal Biceps Tendon Rupture
Distal biceps rupture accounts for ~3% of biceps injuries and occurs almost exclusively in men aged 30–60, during eccentric loading of a flexed elbow (e.g., catching a heavy object). Presentation: sudden "pop" in the antecubital fossa, pain, swelling, ecchymosis, weakness of forearm supination (40% loss) and elbow flexion (30% loss), and a palpable defect with a "reverse Popeye" deformity (retracted biceps muscle belly). Hook test: attempt to hook your finger under the intact biceps tendon from the lateral side with elbow flexed 90° — inability to hook the tendon is positive (sensitivity 100%, specificity 100%). MRI confirms the diagnosis. Management: surgical repair (anatomic reattachment to the radial tuberosity) is recommended for active patients — best outcomes within 2–3 weeks of injury. Delayed repair (>4 weeks) may require allograft augmentation. Non-operative management is acceptable for sedentary, elderly patients who accept strength loss.
Scaphoid Fracture
The scaphoid is the most commonly fractured carpal bone, accounting for 60–70% of carpal fractures. Mechanism: FOOSH (fall on an outstretched hand) with wrist hyperextension. Clinical examination: anatomic snuffbox tenderness (sensitivity ~90%, specificity ~40%), scaphoid tubercle tenderness (palpate volar aspect), and pain with axial compression of the thumb. Initial radiographs may be negative in up to 20% of cases — if clinical suspicion is high, treat empirically with thumb spica splint/cast and repeat imaging in 10–14 days (radiograph or MRI). MRI has near-100% sensitivity and is the imaging study of choice for occult fractures.
The scaphoid has a retrograde blood supply (enters distally, perfuses proximally via the dorsal branch of the radial artery) — proximal pole fractures have the highest risk of avascular necrosis (AVN) (up to 30–40%) and nonunion. Management: non-displaced waist fractures — thumb spica cast for 8–12 weeks; displaced fractures (>1 mm), proximal pole fractures, or athletes requiring faster return — internal fixation with a headless compression screw (Herbert screw). Return to sport with cast immobilization: 4–6 weeks post-fixation with a playing cast for contact sports.
De Quervain Tenosynovitis
De Quervain tenosynovitis is stenosing tenosynovitis of the first dorsal compartment tendons (abductor pollicis longus and extensor pollicis brevis) at the radial styloid. Common in new parents ("mommy thumb"), racquet sport athletes, and those with repetitive thumb/wrist use. The hallmark test is Finkelstein's test: the patient makes a fist over the thumb, then the examiner ulnar-deviates the wrist — sharp pain at the radial styloid is positive. Management: thumb spica splint, activity modification, NSAIDs, corticosteroid injection into the tendon sheath (80–90% cure rate with one injection; note that there may be a septum within the compartment requiring two injections), and surgical release for refractory cases.
21 Hand & Finger Injuries
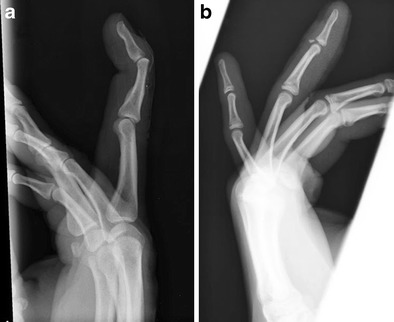
Gamekeeper's/Skier's Thumb (UCL of the Thumb)
UCL injury of the thumb MCP joint results from forced abduction/hyperextension of the thumb. Gamekeeper's thumb is chronic (repetitive stress, historically from Scottish gamekeepers breaking rabbits' necks). Skier's thumb is acute (fall on an outstretched hand with the ski pole forcing thumb abduction). The UCL of the thumb is critical for pinch grip strength. Examination: tenderness at the ulnar aspect of the thumb MCP joint, valgus stress testing at 0° and 30° flexion (laxity >30° opening or >15° side-to-side difference indicates complete tear). The Stener lesion occurs when the torn UCL displaces superficial to the adductor pollicis aponeurosis — this prevents healing and is an absolute indication for surgical repair. Stener lesion occurs in ~80% of complete UCL ruptures. MRI or ultrasound can identify a Stener lesion. Management: partial tears (stable) — thumb spica cast 4–6 weeks; complete tears or Stener lesion — surgical repair.

Mallet Finger
Mallet finger results from disruption of the terminal extensor tendon at its insertion on the distal phalanx, caused by forced flexion of an extended DIP joint (e.g., ball striking the fingertip). Presentation: inability to actively extend the DIP joint; the DIP rests in flexion. May be purely tendinous or involve a bony avulsion of the dorsal lip of the distal phalanx. Management: continuous splinting in extension (Stack splint or aluminum splint) for 6–8 weeks — the patient must NOT flex the DIP during this period, or the clock resets. Surgical fixation is indicated for bony mallet with >30% articular involvement or volar subluxation of the distal phalanx. Untreated chronic mallet finger can lead to swan-neck deformity (DIP flexion + PIP hyperextension).
Jersey Finger
Jersey finger is an avulsion of the flexor digitorum profundus (FDP) tendon from its insertion on the distal phalanx, most commonly affecting the ring finger (75% of cases). Mechanism: forced extension of a flexed DIP (e.g., grabbing an opponent's jersey in football/rugby). Presentation: inability to actively flex the DIP joint (PIP flexion is preserved via the FDS). The Leddy classification: Type I — tendon retracts to palm (no vincular blood supply; requires repair within 7–10 days); Type II — tendon retracts to PIP joint level (most common; repair within 3 months); Type III — bony avulsion, fragment caught at A4 pulley (can repair up to 6 weeks). This is a surgical emergency (especially Type I) — delayed diagnosis results in significantly worse outcomes.
22 Femoroacetabular Impingement & Labral Tears
Femoroacetabular Impingement (FAI)
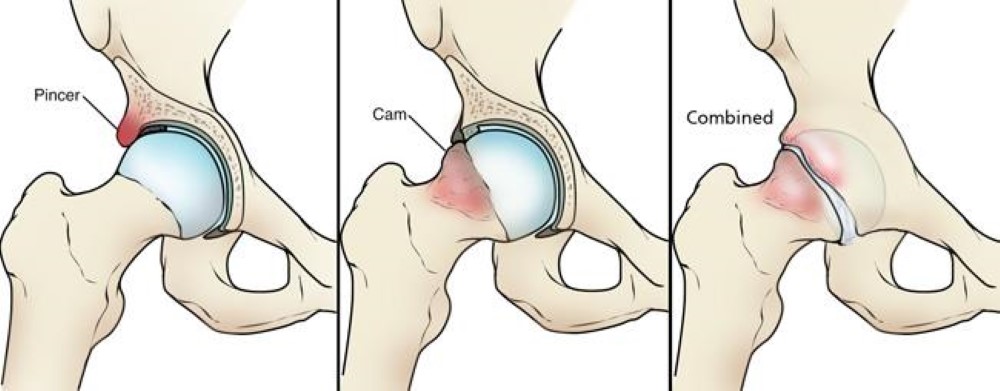
FAI is abnormal contact between the proximal femur and the acetabulum during hip motion, causing damage to the labrum and articular cartilage. Three morphologic types:
| Type | Morphology | Mechanism | Demographics |
|---|---|---|---|
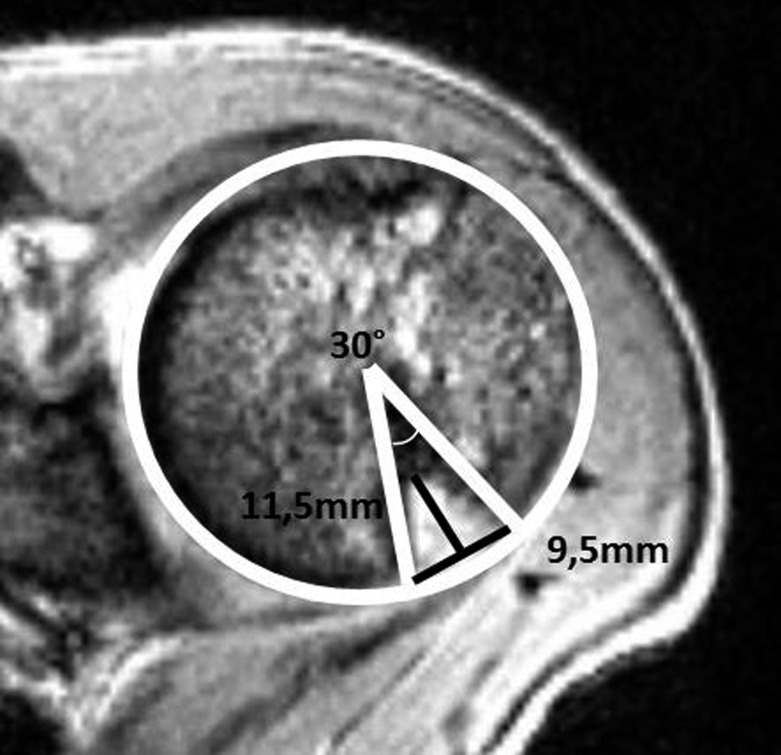
| Cam | Aspherical femoral head (osseous bump on the anterolateral femoral head-neck junction; alpha angle >55°) | Abnormal femoral head jams into the acetabulum during flexion/internal rotation; causes outside-in labral damage and adjacent cartilage delamination | More common in young males and athletes |
| Pincer | Overcoverage of the acetabulum (global = coxa profunda/protrusio; focal = acetabular retroversion = "crossover sign" on AP pelvis) | Acetabular rim contacts the femoral neck, causing labral crush injury and "contrecoup" cartilage lesion on the posteroinferior acetabulum | More common in middle-aged females |
| Combined (Mixed) | Both cam and pincer morphology | Most common presentation (~85% of FAI cases) | Variable |
Clinical Presentation & Examination
Patients present with insidious onset of groin pain (anterior hip pain), aggravated by prolonged sitting, deep flexion, stairs, and athletic activity. Pain with the "C-sign" — patient cups the hand over the anterior-lateral hip. Key examination maneuver: FADIR test (Flexion, ADduction, Internal Rotation) — supine, hip flexed to 90°, then adducted and internally rotated — reproduction of groin pain is positive (sensitivity ~94–99%, specificity ~5–8% — highly sensitive but not specific). FABER test (Flexion, ABduction, External Rotation, also called Patrick's test): supine, foot placed on contralateral knee (figure-of-4) — groin pain suggests hip pathology; posterior pain suggests SI joint dysfunction.

Hip Labral Tears
The acetabular labrum is a fibrocartilaginous ring that deepens the acetabulum by ~22%, increases joint stability, creates a suction seal (maintaining negative intra-articular pressure), and distributes contact stresses. Labral tears are frequently associated with FAI (>85% of FAI patients have labral tears). Presentation: sharp, catching groin pain with pivoting/twisting; may describe clicking or locking. MR arthrography is the gold standard for diagnosis (sensitivity 90–95%). Management: conservative treatment first (activity modification, PT, NSAIDs, intra-articular corticosteroid injection for diagnostic and therapeutic purposes); surgical intervention (hip arthroscopy with labral repair + osteoplasty to correct the underlying cam/pincer morphology) is indicated for failure of conservative treatment in patients without significant arthritis.
23 Athletic Pubalgia & Hamstring Injuries
Athletic Pubalgia (Sports Hernia / Core Muscle Injury)
Athletic pubalgia is an umbrella term for chronic groin pain in athletes caused by injury to the musculotendinous structures of the pubic region. Unlike a true inguinal hernia, there is no palpable hernia. The primary pathology involves the rectus abdominis/adductor aponeurotic plate at its attachment to the pubic symphysis. Common in sports requiring rapid acceleration, deceleration, and twisting (soccer, hockey, football). Presentation: insidious onset of unilateral lower abdominal/inguinal/adductor pain, worsening with exertion (especially sit-ups, sprinting, kicking), and improving with rest. Examination: tenderness at the pubic tubercle and conjoint tendon area, pain with resisted sit-up or resisted hip adduction. MRI shows edema at the pubic symphysis and/or rectus abdominis/adductor insertion. Management: conservative treatment (6–12 weeks of core stabilization, adductor strengthening, gradual return to sport) succeeds in ~50%; surgical repair (open or laparoscopic mesh reinforcement of the posterior inguinal wall, or adductor tenotomy for concomitant adductor pathology) has 85–95% success rate.
Hamstring Injuries
The hamstring complex consists of the biceps femoris (long and short heads), semitendinosus, and semimembranosus. The long head of the biceps femoris is the most commonly injured. Mechanism: eccentric overload during high-speed running (late swing phase, when the hamstrings decelerate knee extension); or stretching injuries (dancers, gymnasts). Risk factors: prior hamstring injury (strongest predictor; recurrence rate 12–30%), age, inadequate warm-up, fatigue, hamstring weakness, hamstring-to-quadriceps strength ratio <0.6.
Hamstring Strain Grading & Management
| Grade | Pathology | Clinical Features | MRI Findings | Return to Sport |
|---|---|---|---|---|
| Grade I | Microscopic tear, <5% fiber disruption | Mild pain, minimal swelling, full ROM with mild pain at end-range, <10% strength deficit | Muscle edema without fiber disruption | 1–3 weeks |
| Grade II | Partial tear, moderate fiber disruption | Moderate pain, swelling, ecchymosis, limited ROM, significant weakness, antalgic gait | Partial fiber disruption with edema and hemorrhage | 3–6 weeks |
| Grade III | Complete tear/avulsion | Severe pain (or painless pop), palpable defect, extensive ecchymosis, inability to bear weight | Complete disruption ± tendon retraction | 3–6 months (surgical if indicated) |
Proximal hamstring avulsion (complete tear from the ischial tuberosity) with ≥2 cm retraction is an indication for surgical repair, particularly in active patients. Other surgical indications: avulsion with ≥2 tendons involved, water skiing or similar acute stretch injuries in young patients.
Hip Flexor Strain & Piriformis Syndrome
Hip flexor (iliopsoas) strain is common in sprinters, soccer players, and martial artists. The iliopsoas is the primary hip flexor, originating from the iliacus and psoas major muscles and inserting on the lesser trochanter. Presentation: anterior hip/groin pain with resisted hip flexion, pain on passive hip extension. Management: RICE, activity modification, progressive stretching and strengthening.
Piriformis syndrome involves compression or irritation of the sciatic nerve by the piriformis muscle as it exits the greater sciatic foramen. Presentation mimics lumbar radiculopathy: buttock pain radiating down the posterior thigh. Key test: FAIR test (Flexion, Adduction, Internal Rotation — reproduces radicular symptoms). Distinguishing from lumbar radiculopathy: negative straight leg raise, no lumbar spine tenderness, normal lumbar MRI. Management: piriformis stretching, physical therapy, activity modification; botulinum toxin or corticosteroid injection for refractory cases; surgical release is rarely needed.
24 Lumbar Spine & Core Injuries in Athletes
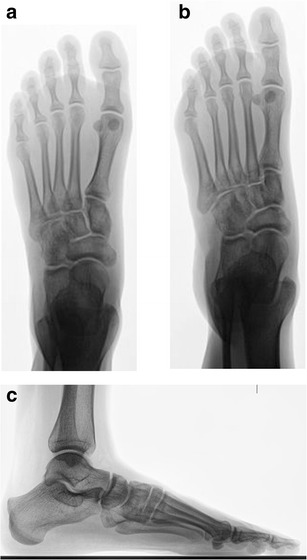
Lumbar Disc Herniation in Athletes
The intervertebral disc consists of the nucleus pulposus (gelatinous core) and the annulus fibrosus (concentric collagen lamellae). Herniation typically occurs posterolateral (at the weakest point of the annulus, where the posterior longitudinal ligament is thinnest). L4-L5 and L5-S1 are the most common levels. Athletes at increased risk: weightlifters, football linemen, gymnasts, rowers. Presentation: low back pain radiating to the lower extremity in a dermatomal pattern, worsened by flexion, Valsalva, sitting. Examination: positive straight leg raise (SLR) test (radicular pain with 30–70° of passive hip flexion with knee extended; sensitivity 91%, specificity 26%), crossed SLR (radicular pain on the affected side when raising the contralateral leg; sensitivity 29%, specificity 88%); neurological exam (assess myotomes, dermatomes, reflexes). MRI for persistent symptoms (>6 weeks) or progressive neurological deficit. Management: 90% improve with conservative treatment (physical therapy, activity modification, NSAIDs, epidural steroid injection). Surgical discectomy for: cauda equina syndrome (emergency), progressive motor weakness, or failure of 6–12 weeks of conservative management.
Spondylolysis & Spondylolisthesis
Spondylolysis is a defect (stress fracture) of the pars interarticularis, most commonly at L5 (85–95% of cases). It is the most common cause of low back pain in adolescent athletes (prevalence 6–8% in the general population, up to 47% in gymnasts, 20–30% in football linemen). Mechanism: repetitive hyperextension and rotation. On oblique radiographs, the pars defect appears as a break in the "scotty dog" sign (the collar/neck of the scotty dog). CT is the gold standard for bony detail; MRI or SPECT/CT shows active bone stress (edema = acute/active pars injury). Management: activity modification, physical therapy (core stabilization, flexion-based exercises), bracing for acute pars injuries (TLSO or Boston overlap brace for 3–6 months); surgical fusion is rarely needed unless pain is refractory or the listhesis is progressive.
Spondylolisthesis is anterior translation of one vertebra on the one below it, most commonly as a consequence of bilateral spondylolysis (isthmic spondylolisthesis). The Meyerding classification: Grade I = 0–25% slippage; Grade II = 25–50%; Grade III = 50–75%; Grade IV = 75–100%; Grade V (spondyloptosis) = complete slippage (>100%). Most athletes with Grade I–II spondylolisthesis can participate in sports without restriction after appropriate rehabilitation. Grade III+ or symptomatic progressive listhesis may require surgical stabilization.
Sacroiliac (SI) Joint Dysfunction
SI joint dysfunction accounts for 15–30% of cases of low back pain. Common in runners, dancers, and unilateral-loading sports. Presentation: unilateral buttock pain, may radiate to the posterior thigh (not below the knee), worsened by transitions (sitting to standing), prolonged sitting on one side, or single-leg activities. Diagnosis requires ≥3 positive provocative tests: FABER/Patrick's test, Gaenslen's test, thigh thrust, sacral compression, sacral distraction. Gold standard: ≥75% pain relief with fluoroscopy-guided SI joint injection (diagnostic block). Management: physical therapy (SI joint stabilization, lumbopelvic muscle strengthening), SI joint belt, intra-articular injection. Rarely requires surgical fusion.
25 Exercise-Induced Conditions
Exercise-Induced Bronchoconstriction (EIB)
EIB (previously called exercise-induced asthma) is transient airway narrowing occurring during or after vigorous exercise, affecting 5–20% of the general population and up to 90% of asthmatics. Pathophysiology: airway water loss (evaporation from high minute ventilation) → increased airway osmolarity → mast cell mediator release → bronchospasm. Symptoms peak 5–15 minutes after exercise and resolve within 30–60 minutes. Diagnosis: ≥10% fall in FEV1 from baseline during eucapnic voluntary hyperventilation (EVH) challenge, exercise challenge, or methacholine challenge. Management: pre-exercise SABA (albuterol, 2 puffs 15–20 minutes before exercise; effective in ~80%), daily ICS for frequent symptoms, LTRA (montelukast), warm-up protocol (induces "refractory period"), and environmental measures (avoid cold/dry air, wear a mask in cold weather).
Exertional Rhabdomyolysis
Exertional rhabdomyolysis is the breakdown of skeletal muscle during intense exercise, releasing intracellular contents (myoglobin, CK, potassium, phosphate) into the circulation. Risk factors: unaccustomed eccentric exercise, sickle cell trait (exertional sickling), heat, dehydration, NSAIDs, stimulants, hypokalemia. Presentation: severe muscle pain, swelling, weakness, dark (cola-colored) urine. Labs: CK >5× upper normal limit (often >10,000–100,000+ U/L); myoglobinuria (positive urine dipstick for "blood" without RBCs on microscopy). Complications: acute kidney injury (AKI from myoglobin-induced tubular injury; risk increases with CK >15,000–20,000), hyperkalemia, DIC, compartment syndrome. Management: aggressive IV normal saline (goal urine output 200–300 mL/hr), monitor renal function and electrolytes, avoid nephrotoxins. Bicarbonate alkalinization of urine is controversial.
Exercise-Associated Hyponatremia (EAH)
EAH is defined as serum Na+ <135 mEq/L during or within 24 hours of prolonged exercise. It is the leading cause of death during marathons. Pathophysiology: excessive hypotonic fluid intake (overdrinking) relative to sweat losses, combined with non-osmotic ADH secretion. Risk factors: exercise duration >4 hours, slow pace, female sex, low body weight, excessive fluid intake, NSAID use. Presentation: mild (Na+ 130–135): nausea, bloating, headache; severe (Na+ <125): confusion, seizures, pulmonary edema, coma, death. Management: mild/asymptomatic — fluid restriction, oral salt intake; severe/symptomatic (seizure, AMS) — 3% hypertonic saline IV bolus (100 mL over 10 minutes, may repeat twice). Prevention: drink to thirst (not on a schedule), avoid overdrinking, use electrolyte-containing beverages.
26 Sudden Cardiac Death & Cardiac Screening
Commotio Cordis
Commotio cordis is sudden cardiac death caused by a blunt, non-penetrating blow to the precordium, typically from a projectile (baseball, lacrosse ball, hockey puck) striking the chest during the vulnerable phase of repolarization (the upslope of the T wave, a 10–30 ms window). This triggers ventricular fibrillation in a structurally normal heart. Most victims: males under 18 years, in baseball (most common cause of sports-related sudden death in children). Survival: historically <15%, but has improved to ~60% with increased awareness and rapid access to AEDs. Management: immediate CPR and defibrillation (AED). Prevention: use of age-appropriate safety baseballs (softer) and chest protectors (though effectiveness of chest protectors is debated).
Immediate CPR and defibrillation (AED) are lifesaving. Any young athlete who collapses after a chest blow should be treated as commotio cordis until proven otherwise. Begin CPR immediately and apply an AED as soon as available. Survival is directly correlated with time to defibrillation — >90% survival if defibrillated within 3 minutes.
Sudden Cardiac Death (SCD) in Athletes
SCD in athletes has an incidence of approximately 1:40,000–1:80,000 per year in competitive athletes. The most common causes vary by age:
| Age Group | Most Common Causes |
|---|---|
| <35 years | Hypertrophic cardiomyopathy (HCM, ~36%), coronary artery anomalies (~17%), arrhythmogenic right ventricular cardiomyopathy (ARVC), myocarditis, ion channelopathies (Long QT, Brugada, CPVT, WPW), aortic dissection (Marfan syndrome), commotio cordis |
| ≥35 years | Atherosclerotic coronary artery disease (most common, >80%) |
Pre-Participation Cardiac Screening Debate
The AHA/ACC position: history and physical exam-based screening (14-element questionnaire) for all competitive athletes; ECG screening is not recommended for the general athletic population in the US due to high false-positive rate (up to 15–25%), cost, and limited evidence of mortality benefit. The ESC/IOC position: 12-lead ECG is recommended as part of routine PPE (Italian model showed significant reduction in SCD in the Veneto region after mandatory ECG screening). The international consensus criteria for ECG interpretation in athletes help distinguish physiologic adaptations from pathologic findings — normal findings in athletes include sinus bradycardia, first-degree AV block, early repolarization, and voltage criteria for LVH without other abnormalities. Abnormal findings requiring further evaluation include T-wave inversions (beyond V1–V3 in athletes <16), ST-segment depression, pathological Q waves, and prolonged QTc (>470 ms in males, >480 ms in females).
27 Overtraining Syndrome & RED-S
Overtraining Syndrome (OTS)
Overtraining syndrome is a maladaptive response to excessive training without adequate recovery, resulting in persistent performance decline despite prolonged rest. It is a diagnosis of exclusion. Distinguish from: functional overreaching (short-term performance decrement that improves with days to weeks of rest — a normal training response) and non-functional overreaching (performance decrement lasting weeks to months; stagnation). OTS features: paradoxical decrease in performance despite maintained or increased training, fatigue, mood disturbances (depression, irritability), sleep disturbances, recurrent infections, loss of appetite, hormonal changes (decreased testosterone, elevated cortisol, altered thyroid function), increased resting heart rate, decreased heart rate variability. Management: extended rest (weeks to months), gradual return to training, psychological support, nutritional optimization. Prevention: periodized training (meso/micro cycles), adequate sleep (7–9 hours), nutrition, and monitoring training load.
Relative Energy Deficiency in Sport (RED-S)
RED-S (formerly the "female athlete triad") is a syndrome resulting from relative energy deficiency — low energy availability (LEA) = energy intake minus exercise energy expenditure, relative to fat-free mass. LEA <30 kcal/kg FFM/day is considered the threshold for impaired physiological function. RED-S affects both males AND females (the concept has expanded beyond the original female athlete triad of disordered eating, amenorrhea, and osteoporosis).
RED-S Health Consequences
| System | Effects of Low Energy Availability |
|---|---|
| Reproductive | Females: functional hypothalamic amenorrhea (FHA), oligomenorrhea, anovulation, delayed menarche; Males: decreased testosterone, low libido, erectile dysfunction |
| Bone | Decreased bone mineral density, increased stress fracture risk, premature osteoporosis, failure to achieve peak bone mass in adolescents |
| Metabolic | Decreased resting metabolic rate, altered thyroid function (low T3), insulin resistance |
| Cardiovascular | Lipid abnormalities, endothelial dysfunction, bradycardia (pathologic) |
| Hematologic | Iron deficiency anemia |
| Psychological | Depression, anxiety, disordered eating / eating disorders (anorexia nervosa, bulimia, EDNOS) |
| Immunologic | Increased susceptibility to infection |
| Growth & Development | Growth retardation and delayed puberty in adolescent athletes |
| Performance | Decreased muscle strength, endurance, concentration, coordination, training response |
Management: increase energy availability to >45 kcal/kg FFM/day, address disordered eating with multidisciplinary team (physician, dietitian, psychologist), calcium (1500 mg/day) + vitamin D (600–1000 IU/day) supplementation, hormone replacement if amenorrhea >6 months and nutritional strategies fail (transdermal estradiol preferred over OCP for bone health), weight-bearing exercise modification. Return-to-play: criterion-based, requires adequate energy intake, menstrual function restoration (or documented recovery of hormonal markers in males), and bone health stabilization.
28 Anti-Doping & PRP/Regenerative Medicine
World Anti-Doping Agency (WADA) Prohibited List
The WADA Code governs anti-doping in all Olympic sports and most professional leagues worldwide. The WADA Prohibited List is updated annually (effective January 1 each year) and includes:
| Category | Substances/Methods | Prohibited Status |
|---|---|---|
| S0: Non-approved substances | Any pharmacological substance not addressed by other sections with no current approval for human therapeutic use | At all times |
| S1: Anabolic agents | Anabolic androgenic steroids (testosterone, nandrolone, stanozolol), other anabolic agents (SARMs, clenbuterol) | At all times |
| S2: Peptide hormones & growth factors | EPO, HGH, IGF-1, hCG (males) | At all times |
| S3: Beta-2 agonists | All beta-2 agonists EXCEPT inhaled salbutamol (≤1600 mcg/24h), formoterol (≤54 mcg/24h), salmeterol (inhaled per manufacturer's dosing) | At all times (with exceptions noted) |
| S4: Hormone & metabolic modulators | Aromatase inhibitors, SERMs (tamoxifen), insulin (non-diabetics), meldonium | At all times |
| S5: Diuretics & masking agents | All diuretics, probenecid, plasma expanders, desmopressin | At all times |
| S6: Stimulants | Amphetamines, ephedrine (>10 mcg/mL), methylphenidate, cocaine | In-competition only |
| S7: Narcotics | Morphine, oxycodone, fentanyl (note: tramadol was added to monitoring program and is prohibited as of 2024) | In-competition only |
| S8: Cannabinoids | THC, synthetic cannabinoids | In-competition only |
| S9: Glucocorticoids | All glucocorticoids by injection, oral, or rectal routes | In-competition only (systemic routes); topical/dermatological, ophthalmic, ear, nasal, buccal, and perianal are permitted |
| M1-M3: Prohibited methods | M1: Manipulation of blood (blood transfusion, RBCT); M2: Chemical/physical manipulation (IV infusions >100 mL/12h outside hospital); M3: Gene and cell doping | At all times |
Therapeutic Use Exemption (TUE)
The TUE process allows athletes with legitimate medical conditions to use otherwise-prohibited substances. Criteria: (1) the substance is necessary to treat a diagnosed condition; (2) withholding would cause significant health impairment; (3) no reasonable therapeutic alternative exists; (4) the substance will not produce additional performance enhancement beyond returning to normal health. Common TUE examples: insulin for type 1 diabetes, testosterone for documented hypogonadism, stimulants for ADHD, inhaled beta-2 agonists for asthma (though salbutamol and formoterol at therapeutic doses no longer require TUE).
PRP & Regenerative Medicine
Platelet-rich plasma (PRP) is an autologous blood product with a platelet concentration above baseline (~3–5x). Platelets release growth factors (PDGF, TGF-beta, VEGF, EGF, IGF-1) that promote tissue healing. PRP preparation: venipuncture (15–60 mL whole blood), centrifuge (single or double spin), isolate platelet-rich layer. Classified by leukocyte content (leukocyte-rich PRP [LR-PRP] vs leukocyte-poor PRP [LP-PRP]) and by platelet concentration. WADA status: PRP injections are currently PERMITTED (removed from the prohibited list in 2011). Evidence: best for lateral epicondylitis (superior to corticosteroid at 6–12 months), promising for patellar tendinopathy, gluteal tendinopathy, and partial muscle injuries; evidence mixed or insufficient for rotator cuff, ACL healing, osteoarthritis. Other regenerative options: stem cell therapy (mesenchymal stem cells, bone marrow aspirate concentrate [BMAC]) — limited high-quality evidence; prolotherapy (hypertonic dextrose injection to stimulate healing); amniotic membrane/growth factor injections — insufficient evidence for most applications.
29 Joint & Bursa Injections
General Principles
Joint and soft tissue injections are among the most common procedures in sports medicine. Indications include diagnostic (confirm pain generator via anesthetic block) and therapeutic (pain relief, anti-inflammatory). Contraindications: overlying skin infection (absolute), bacteremia, prosthetic joint (relative), coagulopathy (relative), allergy to injectate. Technique: sterile preparation, identify landmarks (anatomic or ultrasound-guided), aspirate before injecting (confirm intra-articular placement, rule out septic joint), inject medication.
Corticosteroid Injection Medications
| Corticosteroid | Relative Potency | Solubility | Duration | Common Doses (Large Joint / Small Joint) |
|---|---|---|---|---|
| Triamcinolone acetonide (Kenalog) | 5 | Low (microcrystalline) | Long (weeks) | 40 mg / 10–20 mg |
| Methylprednisolone acetate (Depo-Medrol) | 5 | Low | Long | 40–80 mg / 10–20 mg |
| Betamethasone (Celestone) | 25 | Mixed (crystalline + soluble) | Medium-long | 6 mg (1 mL) / 3 mg (0.5 mL) |
| Dexamethasone sodium phosphate | 25 | High (soluble) | Short (days) | 4 mg / 1–2 mg |
General guidelines: limit corticosteroid injections to 3–4 per joint per year (minimum 3-month intervals). More soluble preparations (dexamethasone) cause less post-injection flare but shorter duration. Less soluble preparations (triamcinolone) have longer-lasting effects but higher risk of soft tissue atrophy, skin depigmentation, and post-injection flare. Mix with local anesthetic (1% lidocaine for immediate effect, 0.25% bupivacaine for longer duration).
Common Injection Sites & Landmarks
| Site | Landmark | Needle Size | Volume |
|---|---|---|---|
| Knee (intra-articular) | Superolateral approach: 1 cm superior and 1 cm lateral to superolateral patella; direct needle at 45° toward intercondylar notch | 22G, 1.5-inch | 5–10 mL (1 mL steroid + anesthetic) |
| Subacromial space | Posterior approach: 2 cm inferior and 2 cm medial to posterolateral corner of acromion; direct anteriorly and slightly superiorly | 22G, 1.5-inch | 5–8 mL |
| Glenohumeral joint | Posterior approach: 2 cm inferior and 2 cm medial to posterolateral corner of acromion; direct toward coracoid process | 22G, 1.5-inch | 3–5 mL |
| Greater trochanteric bursa | Point of maximal tenderness over greater trochanter; perpendicular to skin down to bone | 22G, 1.5–3.5-inch | 3–5 mL |
| Lateral epicondyle (tennis elbow) | Point of maximal tenderness at lateral epicondyle; peritendinous (not intratendinous) | 25G, 1-inch | 1–2 mL |
| De Quervain (1st dorsal compartment) | 1 cm proximal to radial styloid; tangential to the skin along the tendon sheath | 25G, 5/8-inch | 0.5–1 mL |
| Plantar fascia | Medial approach: medial aspect of calcaneus at the plantar fascia origin; medial-to-lateral | 25G, 1-inch | 1–2 mL |
Hyaluronic Acid (Viscosupplementation)
Hyaluronic acid (HA) injection (viscosupplementation) is used for knee osteoarthritis. Products: Synvisc (hylan G-F 20, single injection, 6 mL), Euflexxa (sodium hyaluronate, 3 weekly injections, 2 mL each), Supartz (5 weekly injections, 2.5 mL each), Gel-One (single injection, 3 mL). Mechanism: restores viscoelastic properties of synovial fluid, may have anti-inflammatory effects. Evidence is mixed — AAOS guidelines do not recommend HA injection (weak evidence of modest benefit), but it remains widely used. Best candidates: mild-moderate OA (Kellgren-Lawrence grade 2–3), patients who have failed or cannot take oral NSAIDs, and those who wish to delay joint replacement.
30 PRP & Musculoskeletal Ultrasound
PRP Injection Technique
Preparation: draw 15–60 mL whole blood into ACD-A or sodium citrate tubes; centrifuge (single spin: 1,500 rpm for 5–10 min to separate RBCs from platelet-rich plasma; double spin: additional centrifugation to concentrate platelets further). Yield: 3–7 mL of PRP with platelet concentration 3–8× baseline. Activation: calcium chloride or thrombin can be added (optional; some prefer non-activated PRP for injection). Inject under ultrasound guidance for tendon, ligament, and joint applications. Post-injection: avoid NSAIDs for 2–4 weeks (may inhibit platelet-mediated healing), relative rest for 48–72 hours, gradual return to activity over 2–6 weeks. PRP is generally well-tolerated; the most common side effect is post-injection pain/flare (24–72 hours).
Musculoskeletal Ultrasound (MSK US)
MSK ultrasound has become an essential tool in sports medicine for both diagnosis and procedural guidance. Advantages over MRI: real-time imaging, dynamic assessment (evaluate structures during movement), portability (point-of-care), no radiation, lower cost, allows contralateral comparison, and procedural guidance.
MSK Ultrasound Applications
| Application | Details |
|---|---|
| Tendon pathology | Tendinopathy (thickening, hypoechogenicity, neovascularity on Doppler), partial/complete tears, calcific deposits |
| Ligament assessment | UCL of the elbow (dynamic valgus stress), lateral ankle ligaments, MCL of the knee |
| Muscle injury | Strain grading, hematoma, muscle herniation |
| Joint effusion | Rapid detection; guides aspiration |
| Fracture | Cortical irregularity (rib, metatarsal, stress fractures not yet visible on radiograph) |
| Guided injection | Joint injection (shoulder, knee, hip), tendon sheath injection, bursa injection, PRP delivery, nerve blocks |
| Nerve assessment | Carpal tunnel (median nerve cross-sectional area >10 mm²), cubital tunnel (ulnar nerve) |
| Foreign body | Detection and guided removal of splinters, glass, other foreign bodies |
Key artifacts and technique: anisotropy — tendons appear artifactually hypoechoic when the ultrasound beam is not perpendicular to the tendon fibers; correct by adjusting the transducer angle ("heel-toe" maneuver). Normal tendon appears hyperechoic (bright) with a fibrillar pattern. Tendinopathy appears as focal hypoechogenicity with loss of fibrillar pattern, tendon thickening, and neovascularity on power Doppler.
31 Arthrocentesis & Fracture/Dislocation Reduction
Arthrocentesis
Arthrocentesis (joint aspiration) is performed for diagnostic and/or therapeutic purposes. Indications: suspected septic arthritis (emergency), crystal arthropathy, hemarthrosis, tense effusion causing pain/immobility. Analysis of aspirated fluid:
| Characteristic | Normal | Non-inflammatory (OA) | Inflammatory (RA, gout) | Septic |
|---|---|---|---|---|
| Appearance | Clear, colorless | Clear, yellow | Cloudy, yellow-green | Turbid, purulent |
| Viscosity | High | High | Low | Low |
| WBC count (/μL) | <200 | <2,000 | 2,000–50,000 | >50,000 (often >100,000) |
| PMN % | <25% | <25% | >50% | >75% |
| Crystals | None | None | MSU (gout) or CPPD (pseudogout) | None (but may coexist) |
| Culture | Negative | Negative | Negative | Positive (60–80%) |
Shoulder Dislocation Reduction
Multiple techniques exist for closed reduction of anterior shoulder dislocation. Pre-reduction radiographs (AP and axillary/Y-view) are recommended to confirm direction and rule out associated fracture. Adequate sedation and analgesia (procedural sedation or intra-articular lidocaine) improve success and patient comfort.
| Technique | Description | Notes |
|---|---|---|
| External rotation (Hennepin) | Elbow at 90°, slowly externally rotate the arm; gravity and muscle relaxation allow reduction | Gentle, low force; high success rate with sedation |
| Cunningham technique | Patient seated; massage biceps, deltoid, and trapezius muscles while patient shrugs; arm adducted at side | No traction, no sedation required; relies on muscle relaxation |
| Stimson technique | Patient prone on elevated stretcher; affected arm hangs over the side with 5–10 lbs of weight | Gravity-assisted; takes 15–30 min; minimal force |
| Traction-countertraction | Axial traction on the arm with a sheet around the patient's torso for countertraction | Reliable; may require more sedation |
| Milch technique | Slowly abduct the arm overhead, then apply gentle traction and external rotation; push the humeral head over the glenoid rim | Well-tolerated, often successful without sedation |
Post-reduction: obtain radiographs to confirm reduction, assess neurovascular status (axillary nerve), immobilize in sling (internal rotation in traditional approach; some evidence supports external rotation immobilization in young patients to reduce recurrence). Refer for MRI and orthopedic follow-up.
Finger Dislocation Reduction
Dorsal PIP dislocation (most common finger dislocation): digital nerve block (1% lidocaine without epinephrine, at the base of the finger), hyperextend then apply longitudinal traction and volar-directed pressure to the base of the middle phalanx. Post-reduction: assess collateral ligament stability, obtain postreduction radiograph, buddy tape to adjacent finger, early ROM. Refer if irreducible, unstable, or associated with fracture involving >30% of the articular surface.
32 Taping, Bracing & Rehabilitation Principles
Taping & Bracing
| Application | Type | Purpose |
|---|---|---|
| Ankle prophylactic taping | Stirrup and figure-of-8 with athletic tape | Prevent lateral ankle sprain recurrence; most effective in athletes with prior ankle sprain |
| Ankle brace (lace-up or semi-rigid) | Active Ankle, ASO brace | Alternative to taping; easier application, similar effectiveness; may be more cost-effective |
| Patellar taping (McConnell) | Rigid tape to medialize the patella | Reduce patellofemoral pain; correct patellar maltracking |
| Kinesiology tape (KT tape) | Elastic adhesive tape applied along muscle/tendon | Proprioceptive feedback, pain relief; limited evidence for structural support |
| Knee brace (functional ACL) | Custom or off-the-shelf hinged brace | Post-ACL reconstruction RTP; evidence for preventing re-injury is limited |
| Knee brace (unloader) | Valgus or varus unloading brace | Unicompartmental knee OA; redistributes load away from affected compartment |
| Counterforce strap | Forearm band worn 2–3 cm distal to epicondyle | Lateral/medial epicondylitis; reduces tendon load at insertion |
| Thumb spica brace/splint | Rigid or semi-rigid splint immobilizing thumb MCP and wrist | Scaphoid fracture, de Quervain, gamekeeper's thumb |
Rehabilitation Principles
Sports medicine rehabilitation follows a criterion-based progression (not strictly time-based) through phases:
| Phase | Goals | Activities | Criteria to Progress |
|---|---|---|---|
| Phase 1: Acute (Protection) | Control pain, swelling, inflammation; protect healing tissue | POLICE (Protection, Optimal Loading, Ice, Compression, Elevation), gentle ROM, isometrics, crutches/brace as needed | Minimal swelling, pain-free passive ROM, adequate pain control |
| Phase 2: Subacute (Controlled Motion) | Restore full ROM, begin strengthening, normalize gait | Progressive ROM exercises, isotonic strengthening (open and closed chain), proprioception training, aquatic therapy, stationary cycling | Full pain-free ROM, manual muscle testing ≥4/5, normal gait |
| Phase 3: Strengthening | Restore full strength, power, endurance, neuromuscular control | Progressive resistance exercise, sport-specific movement patterns, plyometrics (initially low-level), balance/proprioception | ≥80% LSI on strength testing, functional movement screening without compensatory patterns |
| Phase 4: Return to Sport | Sport-specific conditioning, confidence, full performance | Agility drills, sport-specific drills, full-speed running, contact progression (if applicable), psychological readiness | ≥90% LSI on strength and functional testing (hop tests), sport-specific tasks pain-free, cleared by physician |
33 Imaging & Diagnostics
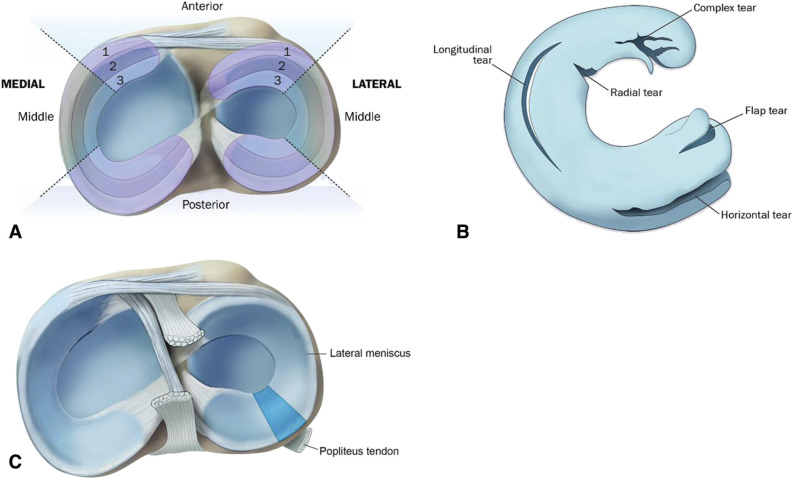
Imaging Modality Selection
| Modality | Best For | Limitations |
|---|---|---|
| Radiograph (X-ray) | First-line for fractures, dislocations, arthritis, bony alignment, foreign bodies; weight-bearing views for joint space narrowing (OA), stress fractures (late), Lisfranc diastasis | Limited soft tissue detail; early stress fractures often negative; cannot visualize tendons, ligaments, cartilage |
| MRI | Gold standard for soft tissue: ligaments (ACL, UCL), menisci, tendons (rotator cuff), labrum, cartilage, bone marrow edema, stress fractures (early); no radiation | Cost, time, availability; metal contraindications; motion artifact; may overdetect asymptomatic pathology |
| MR Arthrography | Superior for labral tears (shoulder, hip), SLAP lesions, partial-thickness rotator cuff tears, intra-articular loose bodies | Invasive (intra-articular contrast injection); all MRI limitations |
| CT | Complex fractures, bony detail (pars defect in spondylolysis, osteochondral lesions, glenoid bone loss quantification), 3D reconstruction for surgical planning | Radiation; limited soft tissue assessment |
| Ultrasound | Real-time, dynamic tendon/ligament assessment, muscle injuries, effusions, guided injections/aspirations, nerve assessment; no radiation; portable | Operator-dependent; limited by acoustic windows; cannot visualize bone marrow or deep structures; steep learning curve |
| Bone scan (scintigraphy) | Stress fractures (high sensitivity, low specificity), avascular necrosis; whole-body assessment for multifocal disease | Low specificity; radiation; being replaced by MRI for most indications |
Key Radiographic Findings
| Finding | Significance |
|---|---|
| Segond fracture | Lateral tibial plateau avulsion — pathognomonic for ACL tear |
| Arcuate sign | Fibular head/styloid avulsion — associated with posterolateral corner injury |
| Lightbulb sign | Internally rotated humeral head on AP shoulder — posterior shoulder dislocation |
| Hill-Sachs lesion | Posterolateral humeral head compression fracture — anterior shoulder dislocation |
| Scotty dog collar fracture | Pars interarticularis defect on oblique lumbar X-ray — spondylolysis |
| Crossover sign | Figure-of-8 pattern of anterior and posterior acetabular walls on AP pelvis — acetabular retroversion (pincer FAI) |
| Lipohemarthrosis (on lateral knee X-ray) | Fat-fluid level in suprapatellar pouch — intra-articular fracture |
| Fleck sign | Small bony fragment between 1st and 2nd metatarsal bases — Lisfranc ligament avulsion |
34 Classification Systems (All)
Ligament Sprain Grading (Universal)
| Grade | Description | Laxity | Function |
|---|---|---|---|
| Grade I | Microscopic fiber disruption; ligament intact | No laxity | Minimal functional loss |
| Grade II | Partial macroscopic tear | Increased laxity with firm endpoint | Moderate functional loss |
| Grade III | Complete rupture | Gross laxity, no endpoint | Severe functional loss |
Muscle Strain Grading
| Grade | Pathology | Strength Deficit | ROM Deficit | Estimated RTP |
|---|---|---|---|---|
| Grade I | Microscopic fiber disruption | <10% | Minimal | 1–3 weeks |
| Grade II | Partial tear, moderate fiber disruption | Up to 50% | Moderate | 3–6 weeks |
| Grade III | Complete tear or avulsion | >50% | Severe | 3–6 months |
Rockwood AC Joint Classification (I–VI)
| Type | AC Ligaments | CC Ligaments | Displacement | Treatment |
|---|---|---|---|---|
| I | Sprain | Intact | None | Conservative |
| II | Torn | Sprain | Slight vertical | Conservative |
| III | Torn | Torn | 25–100% CC distance increase | Controversial (conservative vs surgical) |
| IV | Torn | Torn | Posterior into trapezius | Surgical |
| V | Torn | Torn | 100–300% CC distance increase | Surgical |
| VI | Torn | Torn | Inferior (subacromial/subcoracoid) | Surgical |
Ankle Sprain Grading
| Grade | Ligament Injury | Laxity | Weight-Bearing | Recovery |
|---|---|---|---|---|
| I | ATFL stretch/microscopic tear | None | Full | 1–3 weeks |
| II | ATFL partial-complete tear ± CFL | Mild-moderate | Difficulty | 3–6 weeks |
| III | Complete ATFL + CFL ± PTFL | Significant | Unable | 6–12 weeks |
Fredericson MRI Stress Fracture Grading
| Grade | Periosteal Edema (T2/STIR) | Marrow Edema (T1) | Fracture Line |
|---|---|---|---|
| 1 | Mild periosteal edema | Normal | No |
| 2 | Moderate periosteal edema | Present | No |
| 3 | Moderate-severe | Present | No |
| 4a | Severe | Present | Intracortical signal change |
| 4b | Severe | Present | Visible on T1 and T2 |
Brighton Criteria for Joint Hypermobility Syndrome
Major criteria: (1) Beighton score ≥4/9 (currently or historically); (2) Arthralgia >3 months in ≥4 joints. Minor criteria: (1) Beighton score 1–3/9; (2) Arthralgia in 1–3 joints or back pain ≥3 months or spondylolysis/spondylolisthesis; (3) Dislocation/subluxation in >1 joint or in 1 joint on >1 occasion; (4) Soft tissue rheumatism ≥3 lesions; (5) Marfanoid habitus; (6) Abnormal skin (striae, hyperextensibility, thin skin, papyraceous scarring); (7) Eye signs (drooping eyelids, myopia, antimongoloid slant). Diagnosis requires: 2 major criteria, OR 1 major + 2 minor, OR 4 minor, OR 2 minor if unequivocally affected first-degree relative.
Beighton Hypermobility Score (0–9)
| Maneuver | Points (each side) |
|---|---|
| Passive dorsiflexion of 5th MCP joint >90° | 1 (left) + 1 (right) = 2 |
| Passive apposition of thumb to volar forearm | 1 (left) + 1 (right) = 2 |
| Hyperextension of elbow >10° | 1 (left) + 1 (right) = 2 |
| Hyperextension of knee >10° (genu recurvatum) | 1 (left) + 1 (right) = 2 |
| Forward flexion with palms flat on floor (knees locked) | 1 (bilateral) = 1 |
| Total possible: 9 points. Score ≥4 indicates generalized joint hypermobility. | |
Meyerding Spondylolisthesis Classification
| Grade | Percent Slippage |
|---|---|
| Grade I | 0–25% |
| Grade II | 25–50% |
| Grade III | 50–75% |
| Grade IV | 75–100% |
| Grade V (Spondyloptosis) | >100% (complete displacement) |
Snyder SLAP Tear Classification (I–IV)
| Type | Description |
|---|---|
| I | Degenerative fraying; biceps anchor intact |
| II | Labrum and biceps anchor detached from glenoid (most common) |
| III | Bucket-handle tear; biceps anchor intact |
| IV | Bucket-handle tear extending into biceps tendon |
Neer Impingement Stages
| Stage | Pathology | Age | Reversibility |
|---|---|---|---|
| I | Edema, hemorrhage of bursa and rotator cuff | <25 years | Reversible |
| II | Fibrosis, tendinitis of rotator cuff | 25–40 years | Partially reversible |
| III | Rotator cuff tears, bone spur formation | >40 years | Irreversible |
Concussion Severity (Traditional — Historical Reference)
Note: Modern concussion management does not use severity grading for return-to-play decisions (replaced by the symptom-based graduated RTP protocol). Historical systems included: Cantu grading (Grade 1: no LOC, PTA <30 min; Grade 2: LOC <5 min or PTA 30 min–24 hr; Grade 3: LOC >5 min or PTA >24 hr) and the AAN 1997 practice parameter (Grade 1: transient confusion, no LOC, symptoms resolve <15 min; Grade 2: symptoms >15 min, no LOC; Grade 3: any LOC). These systems are no longer recommended by current consensus statements.
Ellman Partial-Thickness Rotator Cuff Tear Grading
| Grade | Depth of Tendon Involvement |
|---|---|
| Grade 1 | <3 mm or <25% thickness |
| Grade 2 | 3–6 mm or 25–50% thickness |
| Grade 3 | >6 mm or >50% thickness |
Leddy Jersey Finger Classification
| Type | Tendon Retraction | Timing of Repair |
|---|---|---|
| I | Retracted to palm (no vincular blood supply) | Within 7–10 days (urgent) |
| II | Retracted to PIP joint level (most common) | Within 3 months |
| III | Bony avulsion at A4 pulley level | Within 6 weeks |
35 Medications Master Table
NSAIDs
| Drug | Dose | Route | Key Notes | WADA Status |
|---|---|---|---|---|
| Ibuprofen | 200–800 mg q6–8h (max 3200 mg/day) | PO | OTC; GI side effects; renal risk | Permitted |
| Naproxen | 250–500 mg q12h (max 1250 mg/day) | PO | Longer half-life; CV safety profile may be best among NSAIDs | Permitted |
| Meloxicam | 7.5–15 mg daily | PO | COX-2 preferential; once daily dosing; lower GI risk than nonselective NSAIDs | Permitted |
| Celecoxib | 100–200 mg q12–24h | PO | Selective COX-2 inhibitor; lowest GI risk; sulfonamide allergy caution | Permitted |
| Ketorolac | 10 mg PO q4–6h (max 5 days) or 15–30 mg IV/IM | PO/IM/IV | Most potent analgesic NSAID; limit to 5 days; high renal/GI risk | Permitted |
| Diclofenac (topical) | 1% gel, apply 4 g to affected area QID | Topical | Local effect, minimal systemic absorption; good for superficial soft tissue | Permitted |
| Indomethacin | 25–50 mg q8h | PO | Used for heterotopic ossification prophylaxis and acute gout | Permitted |
Corticosteroid Injections
| Agent | Typical Dose (Large Joint) | Duration of Effect | WADA Status |
|---|---|---|---|
| Triamcinolone acetonide | 40 mg | 4–6 weeks | Prohibited in-competition (systemic: injection/oral/rectal); permitted topical/local* |
| Methylprednisolone acetate | 40–80 mg | 4–6 weeks | Same as above |
| Betamethasone | 6 mg (1 mL) | 3–4 weeks | Same as above |
| Dexamethasone | 4 mg | 1–2 weeks | Same as above |
*Note: WADA considers injectable glucocorticoids (intra-articular, periarticular, peritendinous) as prohibited in-competition by all systemic routes. Local injections may result in systemic absorption and positive testing. Athletes should declare injections and may need a washout period of up to several weeks before competition.
Muscle Relaxants
| Drug | Dose | Mechanism | Key Notes |
|---|---|---|---|
| Cyclobenzaprine (Flexeril) | 5–10 mg TID (or 15–30 mg ER daily) | Central acting; structurally related to TCAs | Sedation; avoid in elderly; short-term use (≤2–3 weeks); no WADA concern |
| Methocarbamol (Robaxin) | 500–1500 mg QID | Central acting | Less sedating than cyclobenzaprine; OTC in some countries |
| Tizanidine (Zanaflex) | 2–8 mg q6–8h (max 36 mg/day) | Alpha-2 agonist | Monitor LFTs; hypotension risk; sedation |
| Baclofen | 5–20 mg TID | GABA-B agonist | More commonly used for spasticity; withdrawal risk with abrupt discontinuation |
Topical Agents
| Agent | Application | Mechanism | Notes |
|---|---|---|---|
| Diclofenac 1% gel (Voltaren) | 4 g to affected area QID | Topical NSAID | OTC; minimal systemic effects; good for superficial joints/tendons |
| Lidocaine 5% patch (Lidoderm) | Apply to painful area for 12 hours on/12 hours off | Sodium channel blockade | Localized analgesia; minimal systemic absorption |
| Capsaicin 0.025–0.075% cream | Apply TID-QID | Substance P depletion | Burning sensation initially; takes 2–4 weeks for effect |
| Menthol/methyl salicylate (Biofreeze, Icy Hot) | Apply PRN | Counterirritant | Temporary pain relief; avoid with heating pads |
Other Important Medications
| Drug | Indication | Dose | WADA Status |
|---|---|---|---|
| Acetaminophen | Pain, mild-moderate | 500–1000 mg q6h (max 3000–4000 mg/day) | Permitted |
| Albuterol (inhaled) | EIB prophylaxis/treatment | 2 puffs (180 mcg) 15–20 min before exercise | Permitted (≤1600 mcg/24h inhaled) |
| Montelukast | EIB prophylaxis | 10 mg daily (taken 2 hours before exercise) | Permitted |
| Amitriptyline | Post-concussion headache, chronic pain | 10–25 mg at bedtime | Permitted |
| Melatonin | Post-concussion sleep disturbance | 0.5–5 mg at bedtime | Permitted |
36 Abbreviations Master List
| Abbreviation | Full Term |
|---|---|
| ACL | Anterior Cruciate Ligament |
| AITFL | Anterior Inferior Tibiofibular Ligament |
| AKI | Acute Kidney Injury |
| AM / PL | Anteromedial / Posterolateral (ACL bundles) |
| ARVC | Arrhythmogenic Right Ventricular Cardiomyopathy |
| ATFL | Anterior Talofibular Ligament |
| BMAC | Bone Marrow Aspirate Concentrate |
| BTB | Bone-Tendon-Bone (patellar tendon graft) |
| CC | Coracoclavicular (ligament/distance) |
| CFL | Calcaneofibular Ligament |
| CK | Creatine Kinase |
| CMC | Carpometacarpal (joint) |
| CTE | Chronic Traumatic Encephalopathy |
| DIC | Disseminated Intravascular Coagulation |
| DIP / PIP / MCP / MTP | Distal / Proximal Interphalangeal, Metacarpophalangeal, Metatarsophalangeal |
| DVT | Deep Vein Thrombosis |
| EAH | Exercise-Associated Hyponatremia |
| ECRB | Extensor Carpi Radialis Brevis |
| EIB | Exercise-Induced Bronchoconstriction |
| EPO | Erythropoietin |
| ESWT | Extracorporeal Shockwave Therapy |
| EVH | Eucapnic Voluntary Hyperventilation |
| FADIR | Flexion, Adduction, Internal Rotation (test) |
| FAI | Femoroacetabular Impingement |
| FDP / FDS | Flexor Digitorum Profundus / Superficialis |
| FEV1 | Forced Expiratory Volume in 1 second |
| FFM | Fat-Free Mass |
| FHA | Functional Hypothalamic Amenorrhea |
| FOOSH | Fall on Outstretched Hand |
| GCS | Glasgow Coma Scale |
| HA | Hyaluronic Acid |
| HCM | Hypertrophic Cardiomyopathy |
| HGH | Human Growth Hormone |
| ITBS | Iliotibial Band Syndrome |
| LCL | Lateral Collateral Ligament |
| LEA | Low Energy Availability |
| LHB | Long Head of Biceps |
| LOC | Loss of Consciousness |
| LP-PRP / LR-PRP | Leukocyte-Poor / Leukocyte-Rich Platelet-Rich Plasma |
| LSI | Limb Symmetry Index |
| LTRA | Leukotriene Receptor Antagonist |
| MCL | Medial Collateral Ligament |
| MDI | Multidirectional Instability |
| MPFL | Medial Patellofemoral Ligament |
| MSK | Musculoskeletal |
| NEXUS | National Emergency X-Radiography Utilization Study |
| OA | Osteoarthritis |
| OCD | Osteochondritis Dissecans |
| ORIF | Open Reduction and Internal Fixation |
| OTS | Overtraining Syndrome |
| PCL | Posterior Cruciate Ligament |
| PCS | Post-Concussion Syndrome |
| PFPS | Patellofemoral Pain Syndrome |
| PITFL | Posterior Inferior Tibiofibular Ligament |
| PLC | Posterolateral Corner |
| POLICE | Protection, Optimal Loading, Ice, Compression, Elevation |
| PPE | Pre-Participation Physical Examination |
| PRP | Platelet-Rich Plasma |
| PTFL | Posterior Talofibular Ligament |
| RED-S | Relative Energy Deficiency in Sport |
| ROM | Range of Motion |
| RTC | Rotator Cuff |
| RTP | Return to Play |
| SABA | Short-Acting Beta-2 Agonist |
| SARMs | Selective Androgen Receptor Modulators |
| SCAT6 | Sport Concussion Assessment Tool, 6th edition |
| SCD | Sudden Cardiac Death |
| SI | Sacroiliac (joint) |
| SIS | Second Impact Syndrome |
| SLAP | Superior Labrum Anterior to Posterior |
| SLR | Straight Leg Raise |
| TES | Traumatic Encephalopathy Syndrome |
| TLSO | Thoracolumbosacral Orthosis |
| TMT | Tarsometatarsal (joint) |
| TOS | Thoracic Outlet Syndrome |
| TUE | Therapeutic Use Exemption |
| UCL | Ulnar Collateral Ligament |
| VMO | Vastus Medialis Oblique |
| VO2 max | Maximal Oxygen Consumption |
| WADA | World Anti-Doping Agency |
| WBGT | Wet Bulb Globe Temperature |
37 Risk Factors & Injury Prevention
Modifiable Risk Factors for Sports Injury
| Risk Factor | Injuries Associated | Intervention |
|---|---|---|
| Inadequate warm-up | Muscle strains, ligament sprains | Dynamic warm-up (10–15 min): jogging, high knees, butt kicks, lunges, sport-specific movements |
| Muscle weakness/imbalance | ACL tears (hamstring/quadriceps imbalance), rotator cuff tears, PFPS | Targeted strengthening; neuromuscular training programs (FIFA 11+, PEP program) |
| Poor flexibility | Hamstring strains, Achilles tendinopathy, hip flexor strains | Regular stretching program (dynamic before activity, static after) |
| Rapid training load increase | Stress fractures, tendinopathy, overtraining syndrome | 10% rule (increase weekly training volume by no more than 10%); periodization |
| Faulty biomechanics | ACL tears (knee valgus on landing), PFPS, ITBS, plantar fasciitis | Movement assessment and correction; gait analysis; proper technique coaching |
| Inadequate nutrition/hydration | Stress fractures (calcium/vitamin D deficiency), muscle cramps, heat illness, RED-S | Adequate caloric intake, calcium (1000–1500 mg/day), vitamin D (600–2000 IU/day), hydration to thirst |
| Poor equipment/surface | Ankle sprains (uneven terrain), turf toe (artificial turf), concussion (inadequate helmet) | Proper footwear, maintained playing surfaces, certified protective equipment |
| Previous injury | Recurrent ankle sprain, hamstring re-tear, ACL re-tear | Complete rehabilitation before return to sport; prophylactic bracing/taping; sport-specific reconditioning |
ACL Injury Prevention Programs
Neuromuscular training programs have been shown to reduce ACL injury rates by 50–70%, especially in female athletes. Key programs:
| Program | Components | Evidence |
|---|---|---|
| FIFA 11+ | Structured warm-up: running exercises, strength/balance/plyometric exercises, advanced running; 20 min, 2–3x/week | Reduces overall injuries by 30–50% and ACL injuries by 50% in soccer players |
| PEP (Prevent Injury Enhance Performance) | Warm-up, stretching, strengthening, plyometrics, sport-specific agility; emphasis on proper landing mechanics (knee over toe, soft landings, avoid valgus collapse) | Reduces ACL injuries by 70–88% in female soccer players |
| Sportsmetrics | 3-phase plyometric training program over 6 weeks; jump training, flexibility, weight training | Reduces landing forces; improves hamstring/quadriceps strength ratio; reduces knee injuries |
Non-Modifiable Risk Factors
Age (adolescents: growth plate vulnerability, apophysitis; older athletes: degenerative changes, slower healing), sex (females: higher ACL tear rate, stress fracture rate, patellofemoral issues; males: higher overall injury rate in contact sports), genetics (collagen gene variants, muscle fiber type distribution, joint morphology), anatomical factors (narrow intercondylar notch, increased tibial slope, genu valgum, excessive Q-angle, trochlear dysplasia, cam morphology), prior concussion (increases risk of subsequent concussion by 2–6×).
Amsterdam/Berlin Consensus on Concussion in Sport (2023) AAOS Clinical Practice Guideline: ACL Injuries (2022) IOC Consensus Statement: RED-S (2018) WADA Prohibited List (2025) JOSPT Clinical Practice Guideline: Ankle Sprains (2017) ACSM Position Stand: Exertional Heat Illness (2007)