Allergy & Immunology
Every diagnosis, procedure, medication, classification, and documentation framework you need to function confidently in an allergy/immunology clinic.
All diagrams on this page are sourced from published educational or institutional materials rather than AI generation. Each figure caption links to its original source, and the full diagram and guideline citations are collected in the references section at the bottom.
01 The Immune System — Essentials
Allergy and immunology sits at the intersection of two problems that look opposite but share the same machinery: an immune system that reacts to things it should tolerate (allergy, hypersensitivity, autoimmunity), and an immune system that fails to respond to things it should fight (immunodeficiency). Understanding how the immune system is supposed to work is the foundation for every note you will write in this clinic.
Innate vs Adaptive Immunity
The innate immune system is the first responder: neutrophils, macrophages, natural killer (NK) cells, dendritic cells, complement proteins, and the physical barriers of skin and mucosa. It reacts within minutes to hours using pattern recognition receptors (toll-like receptors, NOD-like receptors) that identify conserved microbial signatures. The adaptive immune system is slower (days to weeks) but specific and memory-forming: B cells produce antibodies, T cells recognize peptide antigens presented by MHC molecules. Most immunologic disease in the clinic involves dysregulation of one or both arms.
T Cells, B Cells, and Antibodies
T cells mature in the thymus and are classified by surface markers and function: CD4+ helper T cells (Th1 drives intracellular infection response and IFN-γ, Th2 drives allergy and IL-4/IL-5/IL-13, Th17 drives extracellular bacteria/fungi and IL-17, Treg suppresses), and CD8+ cytotoxic T cells that kill virally infected or malignant cells. B cells mature in the bone marrow, recognize antigen through surface immunoglobulin, and after activation differentiate into plasma cells that secrete antibodies. The five immunoglobulin isotypes — IgG (dominant serum antibody, crosses placenta), IgA (mucosal), IgM (first antibody produced), IgE (allergy, parasites), and IgD (B cell receptor) — each have distinct roles you will document repeatedly.
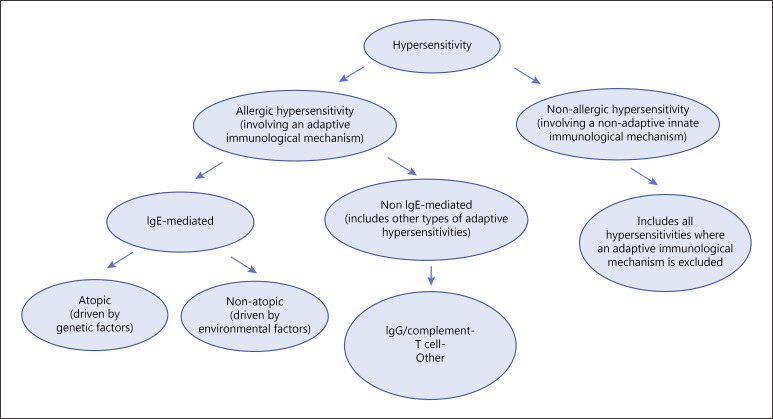
The Gell & Coombs Hypersensitivity Framework
Almost every allergic disease you will document maps to one of four classical hypersensitivity mechanisms, and the physician will frequently reference them by number:
| Type | Mechanism | Timing | Examples |
|---|---|---|---|
| I | IgE-mediated; mast cell and basophil degranulation releasing histamine, tryptase, leukotrienes | Minutes | Anaphylaxis, allergic rhinitis, food allergy, acute urticaria, asthma exacerbation from allergen |
| II | IgG/IgM antibody binding to cell-surface antigen, leading to complement activation or opsonization | Minutes to hours | Hemolytic transfusion reaction, autoimmune hemolytic anemia, drug-induced thrombocytopenia |
| III | Immune complex deposition activating complement and neutrophils | Hours to days | Serum sickness, post-streptococcal glomerulonephritis, hypersensitivity vasculitis |
| IV | T-cell mediated, delayed-type hypersensitivity (DTH) | 48–72 hours (or longer) | Contact dermatitis, tuberculin reaction, DRESS, SJS/TEN, chronic transplant rejection |
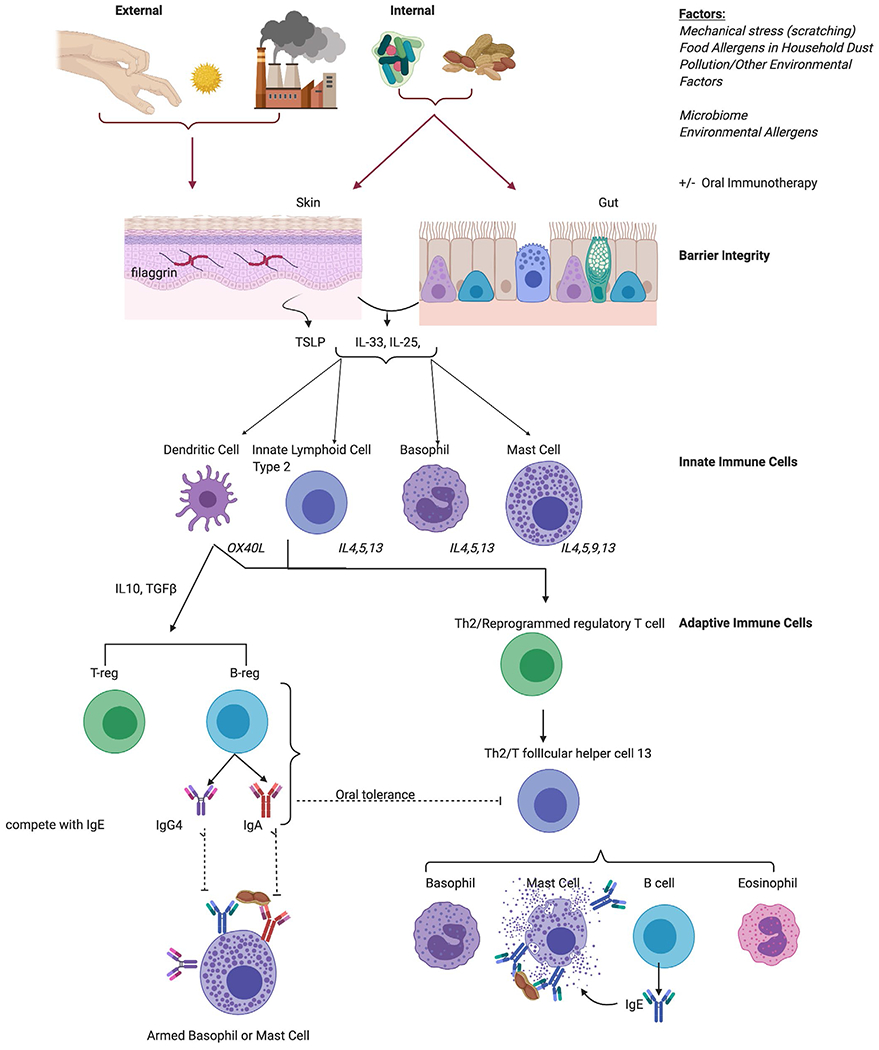
The Atopic March
A scribe will frequently hear the phrase atopic march: the tendency of atopic disease to progress through childhood in a predictable sequence — atopic dermatitis in infancy, food allergy in early childhood, allergic rhinitis in mid-childhood, and asthma later. A positive family history of atopy and early-onset severe eczema are the strongest predictors. Document atopy carefully because it shapes risk assessment and therapy decisions.
When the attending says "Type I reaction," they mean IgE-mediated and treat with antihistamines ± epinephrine. When they say "Type IV," they mean delayed/contact and treat with topical steroids. You should never confuse these two in documentation — they drive completely different workups and billing codes.
02 Scribe Documentation Framework
Allergy/immunology encounters come in a few distinct flavors, and each has its own documentation rhythm. You need to recognize the visit type within the first minute and start pre-populating the correct template.
Encounter Types
- New consult — the most common. A patient is referred for suspected allergy, unexplained anaphylaxis, recurrent infections, chronic urticaria, or drug reaction. Expect a long, detailed HPI and a full review of prior testing and trigger exposures.
- Follow-up — monitoring symptom control, biologic response, immunotherapy progress, or lab trends in a known immunodeficiency.
- Skin test visit — focused around a procedure (prick, intradermal, patch). Document the panel, reaction sizes, controls, and interpretation.
- Drug challenge / desensitization — procedure-based visit documented with incremental doses, vitals, and any reactions.
- Immunotherapy build-up / maintenance — weekly or monthly shot visits.
- Biologic infusion / injection — omalizumab, mepolizumab, dupilumab, etc. Documented with dose, site, pre/post vitals, tolerance.
The Allergy HPI
A high-quality allergy HPI differs from a generic HPI because the diagnosis often hinges on timing, exposure, and pattern. Document these elements for every reaction:
- Trigger & timing — What was consumed, applied, inhaled, or injected? How long after exposure did symptoms start? (Minutes favor IgE, hours-to-days favor Type IV or non-IgE.)
- Symptoms by system — cutaneous (hives, angioedema, flushing, pruritus), respiratory (rhinorrhea, wheeze, stridor, dyspnea), GI (nausea, vomiting, diarrhea, abdominal pain), cardiovascular (presyncope, hypotension, tachycardia), neurologic (sense of doom).
- Duration & resolution — Self-limited? Required ED, epinephrine, steroids, antihistamines? Biphasic recurrence?
- Cofactors — exercise, alcohol, NSAIDs, menstruation, infection, recent immunization. Food-dependent exercise-induced anaphylaxis is a classic scenario the physician will probe for.
- Prior reactions & trend — Number, severity progression, worst reaction, time since last reaction.
- Environmental & atopic context — pets, dust, mold exposure, seasonal pattern, family history of atopy, comorbid eczema/asthma/rhinitis.
PID HPI — The Infection History
For primary immunodeficiency consults, the HPI is effectively an infection catalog. Capture frequency, severity, organism (when cultured), sites (sinopulmonary, GI, skin, deep/visceral), hospitalizations, IV antibiotic courses, and unusual organisms (Pneumocystis, atypical mycobacteria, invasive candida, opportunists). Document whether infections respond normally to antibiotics or recur promptly after stopping.
Two habits separate average scribes from great ones in allergy: (1) write exact minutes, not "a few minutes," because IgE reactions typically start <30 min after exposure and that number drives the diagnosis; and (2) always chart the route of exposure (ingested, injected, inhaled, contact) because desensitization and testing protocols depend on it.
03 Allergic Rhinitis & Conjunctivitis Upper Airway
Allergic rhinitis (AR) is the highest-volume diagnosis in most allergy clinics, affecting 10–30% of adults and up to 40% of children. It is IgE-mediated inflammation of the nasal mucosa triggered by aeroallergens (pollens, dust mites, pet dander, molds, cockroach). Though often dismissed as trivial, uncontrolled AR drives sinusitis, otitis media with effusion, worsens asthma, and causes enormous productivity loss.
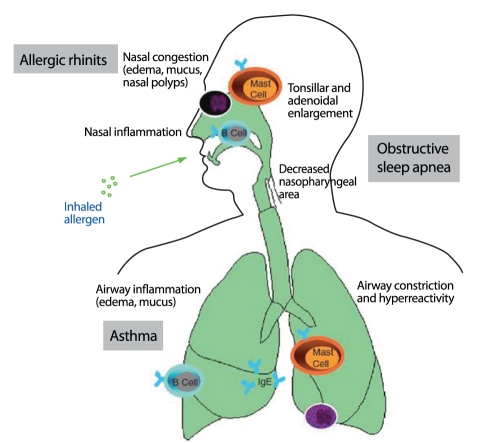
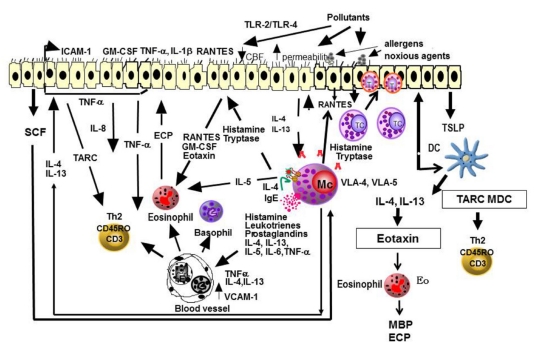
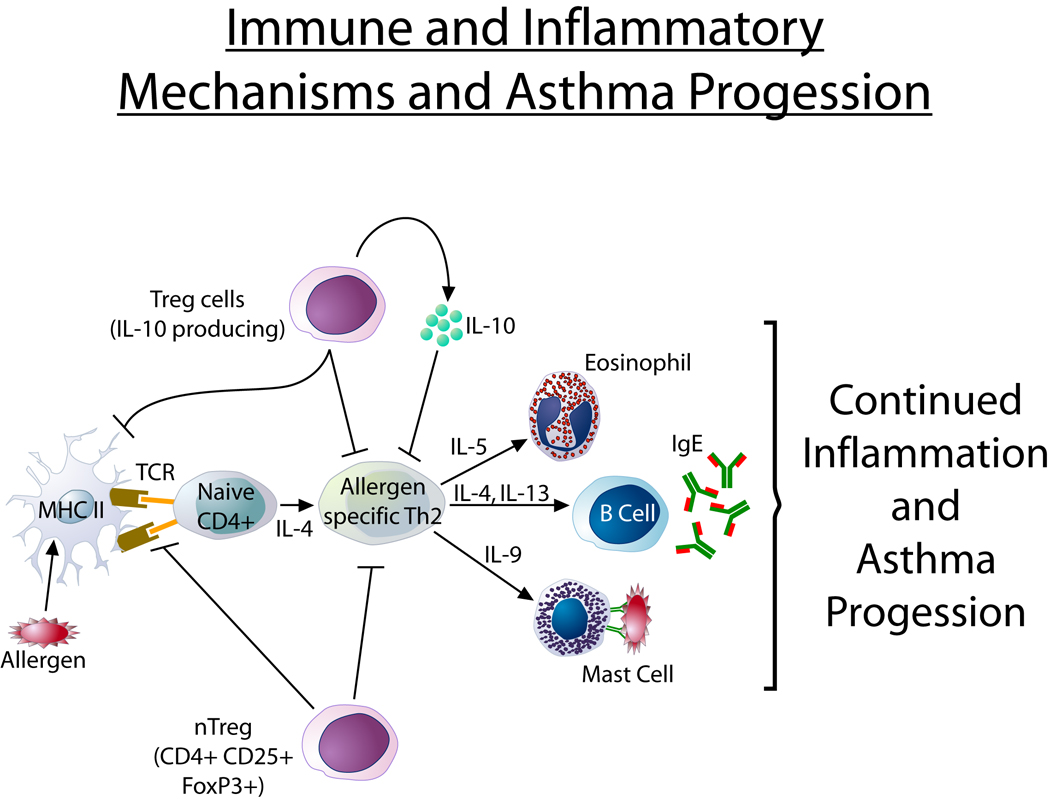
Pathophysiology
Sensitization occurs when inhaled allergen is processed by dendritic cells, presented to Th2 cells, and drives IgE production. On re-exposure, allergen cross-links mast cell surface IgE, releasing histamine, tryptase, leukotrienes, and prostaglandins — causing the early phase (minutes: sneezing, itching, rhinorrhea). Cytokine-driven recruitment of eosinophils and basophils produces a late phase (4–8 hours later: congestion, persistent symptoms).
Clinical Presentation
The classic tetrad: sneezing, rhinorrhea, nasal itching, and congestion, often with ocular itching, tearing, redness (allergic conjunctivitis), and postnasal drip. Physical findings include pale or violaceous boggy turbinates, clear rhinorrhea, allergic shiners (infraorbital darkening), the allergic salute (transverse nasal crease from rubbing), and cobblestoning of the posterior pharynx. Seasonal AR is driven by pollens (tree in spring, grass in early summer, ragweed/weed in fall). Perennial AR is driven by indoor allergens (dust mite, pet, cockroach, mold).
Classification (ARIA)
| Axis | Category | Definition |
|---|---|---|
| Frequency | Intermittent | <4 days/week or <4 consecutive weeks |
| Persistent | ≥4 days/week and ≥4 consecutive weeks | |
| Severity | Mild | Normal sleep, normal activities, no troublesome symptoms |
| Moderate/Severe | Any of: abnormal sleep, impaired activities, troublesome symptoms |
Diagnostic Workup
Diagnosis is clinical but confirmed with specific IgE testing — either skin prick testing or serum specific IgE (ImmunoCAP) to the suspected aeroallergens. A panel usually includes regional trees, grasses, weeds, dust mite (Dermatophagoides pteronyssinus and D. farinae), cat, dog, cockroach, and relevant molds (Alternaria, Cladosporium, Aspergillus, Penicillium).
Management
Stepwise therapy per the Joint Task Force 2017 Rhinitis Practice Parameter: allergen avoidance, intranasal corticosteroids (the most effective monotherapy), oral or intranasal second-generation antihistamines, intranasal antihistamines, leukotriene receptor antagonists (with a boxed warning on montelukast for neuropsychiatric effects), and allergen immunotherapy (SCIT or SLIT) for moderate/severe disease unresponsive to pharmacotherapy or as disease-modifying therapy. Intranasal ipratropium helps rhinorrhea; saline irrigation is cheap and effective adjunctive therapy.
The attending will often say "give them a step-up to combination INCS + intranasal antihistamine" — this is azelastine/fluticasone (Dymista). Document the brand because the pharmacy will substitute components and the patient will lose the benefit.
04 Asthma (Allergy Perspective) Lower Airway
Asthma is co-managed by allergy and pulmonology. Allergy clinics see asthma primarily when it is allergic-phenotype, uncontrolled on step-up therapy, or a candidate for biologics. GINA 2024 guidelines are the current standard.
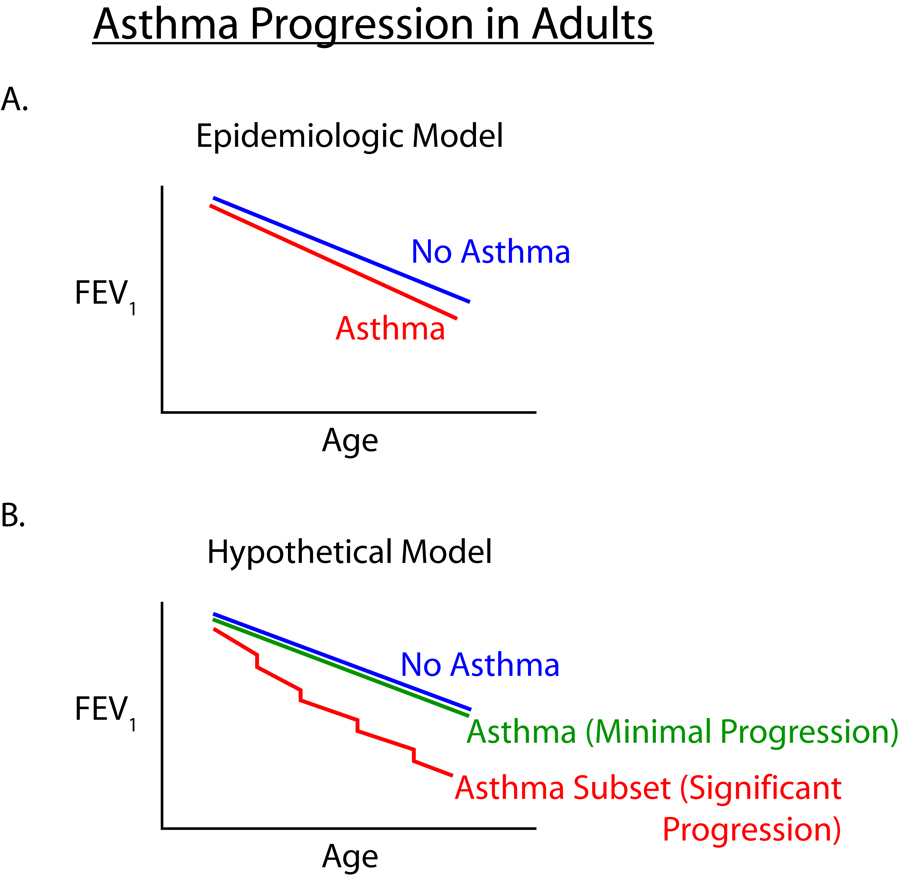
Pathophysiology & Phenotypes
Chronic airway inflammation drives bronchial hyperresponsiveness, reversible bronchoconstriction, mucus hypersecretion, and airway remodeling. The two broad phenotypes are Type 2-high (eosinophilic, IgE-driven, allergic, often atopic, biologic-responsive) and Type 2-low (neutrophilic or paucigranulocytic, often obesity-associated, less biologic-responsive).
Severity & Control
Score 1 point for each: (1) daytime symptoms >2×/week, (2) any night waking from asthma, (3) reliever use >2×/week, (4) any activity limitation.
| Level | Criteria |
|---|---|
| Well controlled | None of the above |
| Partly controlled | 1–2 of the above |
| Uncontrolled | 3–4 of the above |
Workup & Management
Diagnosis is confirmed by spirometry showing reversible obstruction (FEV1 increase ≥12% and ≥200 mL post-bronchodilator). Allergy clinic specifics: FeNO (fractional exhaled nitric oxide, >25 ppb suggests Type 2 inflammation, >50 ppb strongly so), peripheral eosinophil count, total and specific IgE, and aeroallergen skin testing. Management follows GINA steps 1–5; severe asthma uncontrolled on medium-high dose ICS-LABA triggers biologic consideration (see Section 17).
05 Atopic Dermatitis Cutaneous
Atopic dermatitis (AD, eczema) is a chronic relapsing inflammatory skin disease — the first step on the atopic march. Allergy is often consulted for moderate-severe AD to evaluate allergic triggers, consider systemic therapy, and differentiate allergic from non-allergic skin disease.
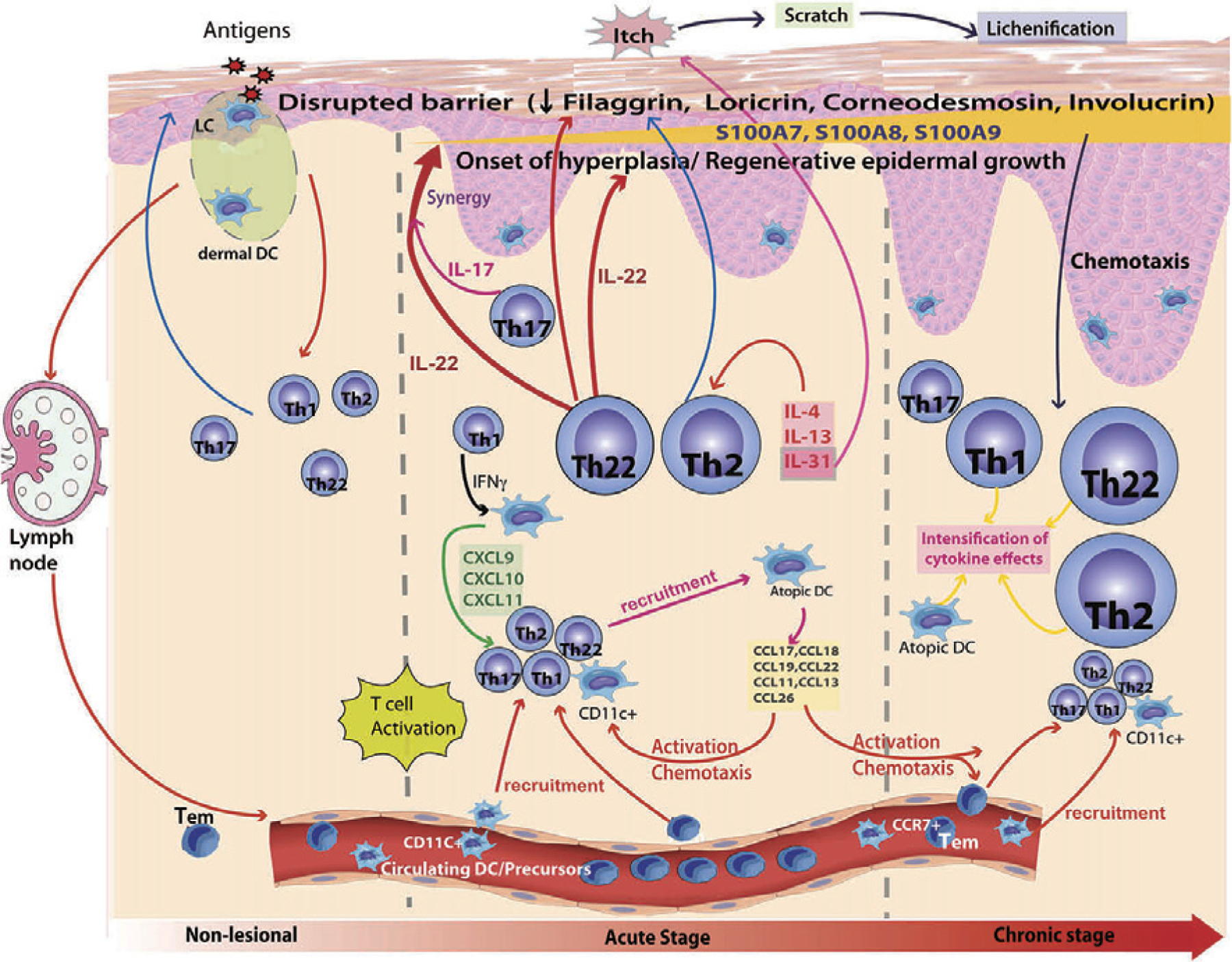
Pathophysiology
Dual defect: a compromised skin barrier (often filaggrin loss-of-function mutations, reduced ceramides) and Th2-skewed inflammation (IL-4, IL-13, IL-31 — the itch cytokine). The barrier defect allows allergen and microbe penetration, triggering immune activation; the inflammation worsens the barrier, creating a vicious cycle.
Clinical Presentation
Infants: facial and extensor surface erythematous, weeping plaques. Children and adults: flexural (antecubital, popliteal, neck, wrists, ankles) lichenified plaques with excoriation. Intense pruritus is the defining symptom. Complications include impetiginization (S. aureus), eczema herpeticum (disseminated HSV, a dermatologic emergency), and molluscum.
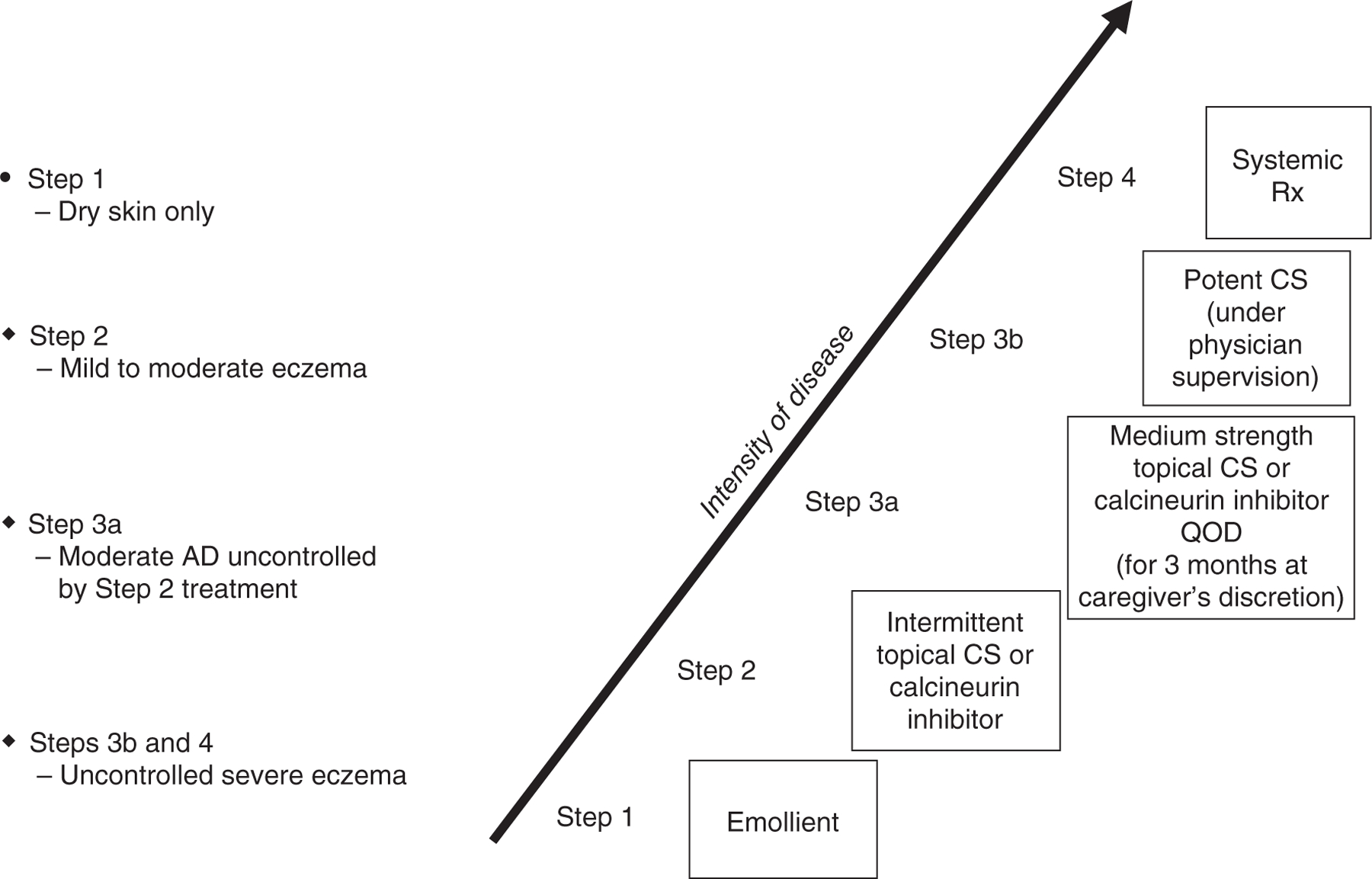
Management
Trigger avoidance, daily emollients, topical corticosteroids (appropriate potency for body site), topical calcineurin inhibitors (tacrolimus, pimecrolimus), topical PDE4 inhibitor (crisaborole), topical JAK inhibitor (ruxolitinib). For moderate-to-severe disease unresponsive to topicals, systemic options include dupilumab (anti-IL-4Rα, approved down to age 6 months), tralokinumab (anti-IL-13), lebrikizumab, and oral JAK inhibitors (abrocitinib, upadacitinib) per the 2023 AAAAI/ACAAI JTF Atopic Dermatitis Guidelines.
06 Urticaria & Angioedema Cutaneous/Mucosal
Urticaria (hives) and angioedema frequently coexist but have distinct differential diagnoses and management. Getting the subtype right is critical because it drives whether the physician orders C1 esterase inhibitor levels, pursues autoimmune workup, or starts omalizumab.

Urticaria Subtypes
| Subtype | Definition | Key Features |
|---|---|---|
| Acute | <6 weeks | Often infection-triggered, food, drug; usually self-limited |
| Chronic Spontaneous (CSU) | ≥6 weeks, no external trigger | ~50% autoimmune (anti-FcεRI or anti-IgE autoantibodies); ASST+ |
| Chronic Inducible (CIndU) | Reproducibly triggered by a specific stimulus | Dermatographism, cold, heat, pressure (delayed), solar, cholinergic, aquagenic, vibratory |
Individual wheals last <24 hours; lesions lasting >24 hours or leaving bruising suggest urticarial vasculitis and require biopsy.
Angioedema Subtypes
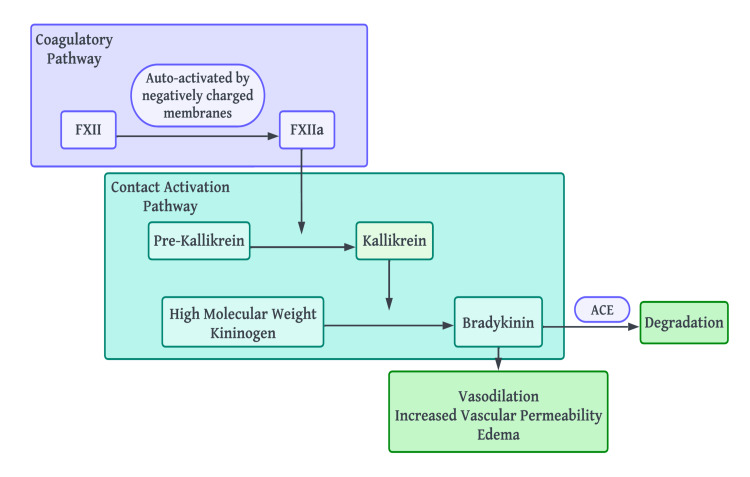
Histaminergic (mast cell mediated, usually with urticaria): responds to antihistamines and epinephrine. Bradykinin-mediated (isolated, no urticaria, often laryngeal or GI, poorly responsive to epinephrine): includes hereditary angioedema (HAE) and ACE inhibitor-induced angioedema. HAE is caused by C1 inhibitor deficiency (Type I: low quantity) or dysfunction (Type II: normal quantity, low function), or is HAE with normal C1-INH (Type III, often F12 mutations).
Workup
CSU: CBC with differential, ESR/CRP, TSH and thyroid antibodies, basic chemistries; escalate only if history suggests secondary cause. Isolated angioedema: C4 (low in all HAE types during and between attacks), C1 esterase inhibitor antigenic level, C1 esterase inhibitor functional level, C1q (low in acquired C1-INH deficiency).
Management
CSU follows the EAACI/GA²LEN Urticaria Guideline stepwise approach: second-generation H1 antihistamine at standard dose, up-dose to 4× standard, add omalizumab, then consider cyclosporine. Avoid chronic systemic steroids. HAE on-demand therapy includes C1 esterase inhibitor concentrates (Berinert, Cinryze, Ruconest), icatibant (bradykinin B2 receptor antagonist), and ecallantide. Long-term prophylaxis: lanadelumab (anti-kallikrein mAb), berotralstat (oral kallikrein inhibitor), or C1-INH replacement.
07 Anaphylaxis Emergency
Anaphylaxis is the highest-acuity allergy diagnosis and the one the attending will care most about documenting precisely. Miss an anaphylaxis diagnosis and the patient does not get epinephrine auto-injectors, an action plan, or proper follow-up — decisions with life-or-death consequences.
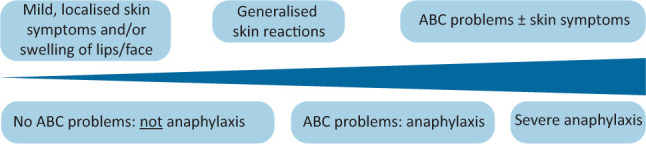
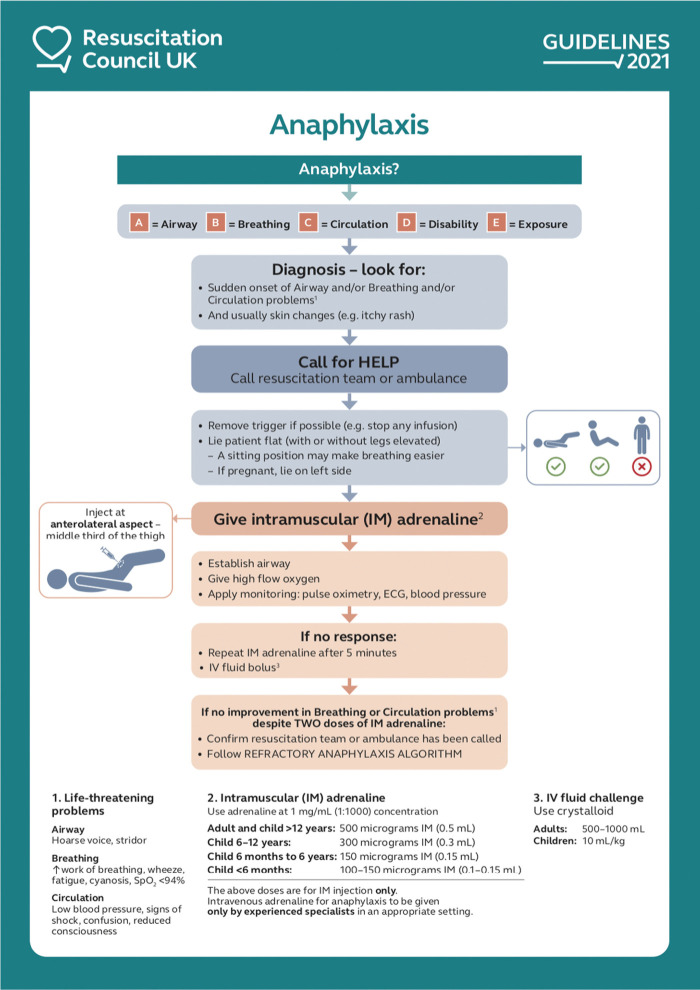
Definition — WAO 2020 Criteria
Anaphylaxis is highly likely when any one of the following criteria is fulfilled per the World Allergy Organization 2020 Anaphylaxis Guidance:
Criterion 1: Acute onset (minutes to several hours) of an illness with simultaneous involvement of skin and/or mucosal tissue (generalized hives, pruritus, flushing, swollen lips/tongue/uvula) AND at least one of:
(a) respiratory compromise (dyspnea, wheeze, stridor, reduced PEF, hypoxemia)
(b) reduced BP or end-organ dysfunction (hypotonia, syncope, incontinence)
(c) severe GI symptoms (severe crampy abdominal pain, repetitive vomiting), especially after non-food allergen exposure.
Criterion 2: Acute onset of hypotension, bronchospasm, or laryngeal involvement after exposure to a known or highly probable allergen, even without skin involvement.
Hypotension in adults = SBP <90 or >30% decrease from baseline; in children = age-adjusted low SBP or >30% decrease.
Ring & Messmer Severity Grading
| Grade | Skin | GI | Respiratory | Cardiovascular |
|---|---|---|---|---|
| I | Generalized skin symptoms (erythema, urticaria, angioedema) | — | — | — |
| II | May be present | Nausea, cramping | Rhinorrhea, hoarseness, dyspnea | Tachycardia (>20/min), hypotension (>20 mmHg), arrhythmia |
| III | May be present | Vomiting, defecation | Laryngeal edema, bronchospasm, cyanosis | Shock |
| IV | May be present | — | Respiratory arrest | Cardiac arrest |
The Brighton Collaboration case definition provides a 3-level diagnostic certainty framework (Levels 1–3) used in vaccine safety surveillance and research.
Management
Intramuscular epinephrine 0.01 mg/kg (max 0.5 mg adult, 0.3 mg pediatric) into the anterolateral thigh is the first and only life-saving drug — antihistamines and steroids are adjuncts. Supine positioning with legs elevated (unless respiratory compromise dictates otherwise), IV fluids, oxygen, H1 and H2 antihistamines, bronchodilators for wheezing, and glucagon for patients on beta-blockers. Observation period: 2020 AAAAI/ACAAI JTF Anaphylaxis Practice Parameter Update recommends individualized observation (minimum 1 hour for mild, longer for severe, biphasic-risk, or multiple epinephrine doses). Biphasic reactions occur in up to 5% within 1–72 hours.
- Two epinephrine auto-injectors prescribed
- Written anaphylaxis action plan
- Referral to allergy/immunology
- Trigger avoidance counseling
- MedicAlert identification recommendation
Scribe Documentation Tips
When documenting the ED or clinic anaphylaxis note, explicitly list which WAO criterion was met. Do not write "possible anaphylaxis" — the physician wants either "meets criteria for anaphylaxis per WAO criterion X" or "does not meet criteria." Also document the exact number of epinephrine doses, the time each was administered, the route (IM thigh vs IV), and the clinical response after each dose. Order a serum tryptase ideally between 15 minutes and 3 hours after symptom onset; baseline tryptase is drawn >24 hours later.
08 Food Allergy & Food Intolerance Immunologic
Food allergy affects ~8% of children and ~10% of adults. The NIAID Expert Panel Food Allergy Guidelines (Sampson criteria) and the AAAAI/ACAAI JTF Food Allergy Practice Parameter are the standard references.
Categories of Adverse Food Reactions
- IgE-mediated food allergy — immediate hypersensitivity (minutes to 2 hours). Top 9 allergens: milk, egg, wheat, soy, peanut, tree nut, fish, shellfish, sesame.
- Non-IgE cell-mediated — food protein-induced enterocolitis syndrome (FPIES, delayed profuse vomiting 1–4 hours after trigger, often with pallor and lethargy), food protein-induced proctocolitis, celiac disease.
- Mixed — eosinophilic esophagitis (EoE), atopic dermatitis with food triggers.
- Oral allergy syndrome (pollen-food allergy syndrome) — cross-reactive IgE between pollen proteins and labile fruit/vegetable proteins (e.g., birch-apple, ragweed-melon). Symptoms are limited to oral pruritus and mild lip swelling and rarely progress to anaphylaxis.
- Alpha-gal syndrome — delayed (3–6 hours) anaphylaxis to mammalian meat after tick bite sensitization to galactose-α-1,3-galactose.
- Non-immunologic intolerance — lactose intolerance, food additive reactions, scombroid poisoning.
Workup
History is primary. Skin prick testing and specific IgE provide sensitization data but not clinical reactivity; test only for foods suggested by history. Component-resolved diagnostics (e.g., Ara h 2 for peanut, Cor a 14 for hazelnut, Ana o 3 for cashew) improve specificity. Oral food challenge remains the gold standard. Basal tryptase if systemic reaction. For FPIES: no IgE testing; diagnosis is clinical per the International FPIES Consensus Guidelines.
Management
Strict avoidance, epinephrine auto-injectors for IgE-mediated, emergency action plan, nutrition referral. Peanut oral immunotherapy (Palforzia) is FDA-approved for ages 4–17 to reduce the severity of reactions from accidental exposure. Early peanut introduction per LEAP trial has changed pediatric prevention.
09 Drug Hypersensitivity Immunologic
Drug reactions span all four Gell & Coombs types. The most common clinic scenarios are penicillin allergy evaluation (often delabeling), NSAID reactions, sulfa allergy evaluation, perioperative anaphylaxis workup, and delayed cutaneous reactions. The 2022 AAAAI/ACAAI JTF Drug Allergy Practice Parameter is the current standard.
Penicillin Allergy
Approximately 10% of Americans carry a penicillin allergy label, but >90% of them are not truly allergic on formal testing. Delabeling improves antibiotic selection, reduces C. difficile, MRSA, and hospital costs. Evaluation uses history stratification (high-risk features include anaphylaxis, SJS/TEN, DRESS, interstitial nephritis, hemolytic anemia), skin prick and intradermal testing with major (PPL — benzylpenicilloyl polylysine, Pre-Pen) and minor (penicillin G) determinants, followed by oral amoxicillin challenge if skin testing is negative. Low-risk patients with distant reactions can often proceed directly to direct oral amoxicillin challenge.
NSAID Hypersensitivity
Multiple mechanisms: COX-1 inhibition causing leukotriene shunting (NERD — NSAID-exacerbated respiratory disease, the Samter's triad of asthma, nasal polyps, and NSAID-induced respiratory reactions); cross-reactive urticaria/angioedema (NIUA); single NSAID IgE-mediated reactions; delayed T-cell reactions. Documentation must specify the drug, dose, timing, and reaction phenotype.
Severe Cutaneous Adverse Reactions (SCARs)
DRESS (drug reaction with eosinophilia and systemic symptoms — latency 2–8 weeks, fever, rash, eosinophilia, hepatitis, lymphadenopathy), SJS/TEN (Stevens-Johnson syndrome/toxic epidermal necrolysis — mucocutaneous blistering with skin detachment), AGEP (acute generalized exanthematous pustulosis). These are Type IV reactions; skin testing and challenge are contraindicated. Drug provocation testing is absolutely contraindicated in SCAR history.
Perioperative Anaphylaxis
Most commonly caused by neuromuscular blocking agents (rocuronium, succinylcholine), antibiotics, chlorhexidine, latex, blue dyes (isosulfan blue), and less commonly induction agents or opioids. Workup includes tryptase at the event, repeat at 1–2 hours and >24 hours, then comprehensive skin testing 4–6 weeks later. Desensitization is performed for essential drugs when no alternative exists — documentation must include incremental doses, vital signs at each step, and any breakthrough symptoms.
10 Insect Sting (Venom) Allergy Immunologic
Stinging Hymenoptera include honeybee, yellow jacket, wasp, hornet, and fire ant. Reactions range from normal local swelling to large local reactions to systemic anaphylaxis. Systemic reactions carry a ~30–60% risk of recurrence without treatment, dropping to <5% with venom immunotherapy.
Mueller Grading of Systemic Sting Reactions
| Grade | Findings |
|---|---|
| I | Generalized urticaria, itching, malaise, anxiety |
| II | Grade I plus 2 or more of: angioedema, chest tightness, nausea/vomiting, diarrhea, abdominal pain, dizziness |
| III | Grade II plus 2 or more of: dyspnea, wheezing, stridor, dysarthria, hoarseness, confusion, sense of impending doom |
| IV | Grade III plus 2 or more of: hypotension, collapse, loss of consciousness, incontinence, cyanosis |
Workup & Management
Skin testing to venom extracts (honeybee, yellow jacket, yellow hornet, white-faced hornet, wasp — fire ant uses whole-body extract) 4–6 weeks after the reaction; if negative, specific IgE and a repeat in 4–6 weeks. Baseline tryptase is mandatory because elevated tryptase suggests underlying mast cell disease and indicates lifelong VIT. Venom immunotherapy (VIT) is indicated for patients with systemic reactions and positive testing; protocols include conventional (15–20 weekly build-up visits), cluster, and rush protocols. Maintenance is typically 5 years, longer if high risk.
11 Latex & Contact Allergies Cutaneous
Latex allergy is IgE-mediated hypersensitivity to natural rubber latex proteins; high-risk groups include healthcare workers, children with spina bifida (repeated surgical exposure), and workers with occupational latex exposure. Symptoms range from contact urticaria to anaphylaxis. Management is strict latex avoidance (latex-free gloves, operating environments) and cross-reactive food avoidance (banana, avocado, kiwi, chestnut — the latex-fruit syndrome).
Allergic contact dermatitis is a Type IV reaction. Common culprits: nickel, fragrance mix, balsam of Peru, neomycin, bacitracin, formaldehyde, rubber accelerators (thiurams, carbamates), para-phenylenediamine (PPD, hair dye), methylisothiazolinone (MI, cosmetics). Diagnosis is by patch testing with standardized allergen panels (T.R.U.E. Test, NACDG panel); readings at 48 and 96 hours (and sometimes day 7). Management is identification and strict avoidance, topical steroids for flares, and a Contact Allergen Management Program (CAMP) list of safe products.
12 Eosinophilic Disorders Inflammatory
Eosinophilic Esophagitis (EoE)
Chronic, immune-mediated esophageal disease with eosinophil-predominant inflammation causing dysphagia, food impaction, chest pain, GERD-like symptoms, and in children feeding difficulties. Diagnosis: endoscopy with biopsy showing ≥15 eosinophils/HPF after excluding other causes. Allergy involvement includes food allergy evaluation; although skin testing and specific IgE have poor predictive value, empiric elimination diets (6-food, 4-food, or 2-food) are a core management strategy alongside PPIs, swallowed topical steroids (budesonide oral suspension, fluticasone), and dupilumab (FDA-approved for EoE).
Hypereosinophilic Syndrome (HES)
Persistent eosinophilia >1,500/µL with end-organ involvement. Variants include myeloproliferative (FIP1L1-PDGFRA fusion, imatinib-responsive), lymphocytic, familial, idiopathic, and overlap with EGPA. Workup includes peripheral smear, flow cytometry, tryptase, B12, vitamin B12, cardiac eval (echo, troponin), skin/tissue biopsy, and molecular studies.
EGPA (Churg-Strauss)
Eosinophilic granulomatosis with polyangiitis: asthma + eosinophilia >10% + systemic vasculitis affecting sinuses, lung, heart, skin (palpable purpura), GI, peripheral nerves (mononeuritis multiplex). ANCA-positive in ~40% (p-ANCA/MPO). Treated with systemic steroids, mepolizumab (anti-IL-5, FDA-approved for EGPA), and in severe disease cyclophosphamide or rituximab.
13 Mast Cell Disorders Inflammatory
Mastocytosis
Clonal mast cell proliferation. Cutaneous mastocytosis: skin-limited, most common in children, includes urticaria pigmentosa (maculopapular cutaneous mastocytosis) and mastocytoma. Systemic mastocytosis: bone marrow and other organ involvement, almost always harbors a KIT D816V mutation; subtypes include indolent SM, smoldering SM, SM with associated hematologic neoplasm (SM-AHN), aggressive SM, and mast cell leukemia. WHO criteria require 1 major (multifocal dense mast cell infiltrates) plus 1 minor, or 3 minor criteria (atypical morphology, KIT D816V, aberrant CD25/CD2/CD30, persistent tryptase >20 ng/mL excluding AHN).
Mast Cell Activation Syndrome (MCAS)
Consensus criteria (Valent): (1) typical episodic multisystem symptoms consistent with mast cell mediator release, (2) objective evidence of mast cell activation (rise in tryptase ≥20% above baseline plus 2 ng/mL within 4 hours of symptoms), and (3) response to mast cell-targeted therapy. Management: trigger avoidance, H1 and H2 antihistamines, leukotriene modifiers, cromolyn, and in select cases omalizumab or avapritinib (KIT inhibitor).
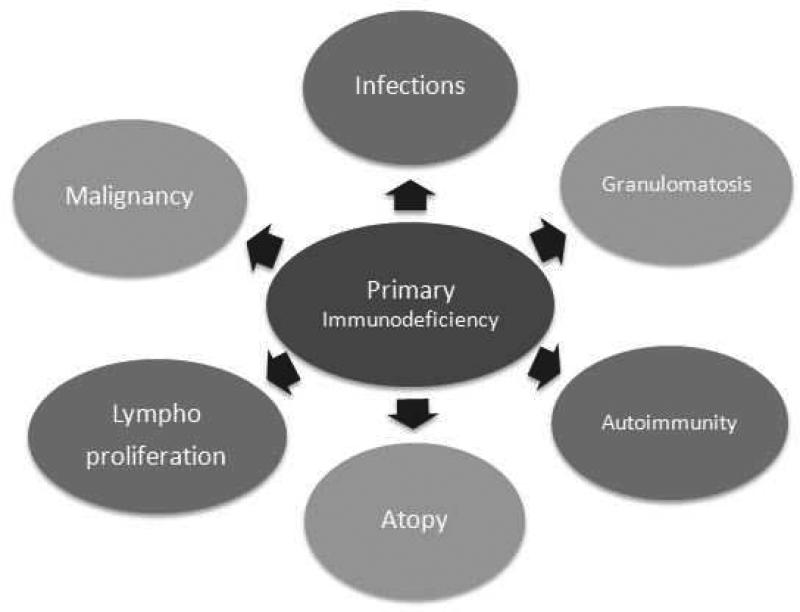
14 Primary Immunodeficiency Diseases Immunodeficiency
More than 450 inborn errors of immunity are now recognized. The clinic sees a handful frequently: CVID, selective IgA deficiency, specific antibody deficiency, X-linked agammaglobulinemia (XLA), chronic granulomatous disease (CGD), complement deficiencies, and in pediatric practice SCID and DiGeorge.
Common Variable Immunodeficiency (CVID)
Most common symptomatic primary antibody deficiency in adults. Recurrent sinopulmonary infections, bronchiectasis, GI disease (nodular lymphoid hyperplasia, chronic diarrhea, giardia), autoimmunity (ITP, AIHA), granulomatous disease, and increased malignancy risk (lymphoma, gastric cancer).
All of:
- Marked decrease of IgG and marked decrease of at least one of IgA or IgM
- Poor response to vaccines (and/or absent isohemagglutinins)
- Secondary hypogammaglobulinemia excluded
- Diagnosis after age 4
- No profound T-cell deficiency
Selective IgA Deficiency
Serum IgA <7 mg/dL with normal IgG and IgM; the most common PID (~1:600). Most are asymptomatic; a subset has recurrent sinopulmonary infection, autoimmunity, atopy, or anti-IgA antibodies that predispose to anaphylaxis with blood products. No specific treatment for the deficiency itself.
X-Linked Agammaglobulinemia (Bruton)
BTK mutation, absent B cells, very low all immunoglobulin classes. Boys present after 6 months as maternal IgG wanes, with severe encapsulated bacterial infections and enteroviral disease. Treat with lifelong Ig replacement.
SCID
Severe combined immunodeficiency — profound T-cell (± B, ± NK) deficiency. Presents in infancy with failure to thrive, persistent diarrhea, thrush, opportunistic infection. SCID is on the universal newborn screen via TREC (T-cell receptor excision circles). Treatment is hematopoietic stem cell transplant (the earlier, the better), gene therapy for selected subtypes, and PEG-ADA for ADA-SCID. Avoid live vaccines and irradiate/CMV-negative blood products.
Chronic Granulomatous Disease (CGD)
Defect in NADPH oxidase (most commonly X-linked gp91phox). Neutrophils phagocytose but cannot kill catalase-positive organisms (Staph aureus, Serratia, Burkholderia cepacia, Nocardia, Aspergillus). Patients develop recurrent abscesses, lymphadenitis, pneumonia, osteomyelitis, and granulomatous inflammation. Dihydrorhodamine (DHR) flow cytometry is the diagnostic test. Treat with antibacterial prophylaxis (TMP-SMX), antifungal prophylaxis (itraconazole), IFN-γ, and HSCT.
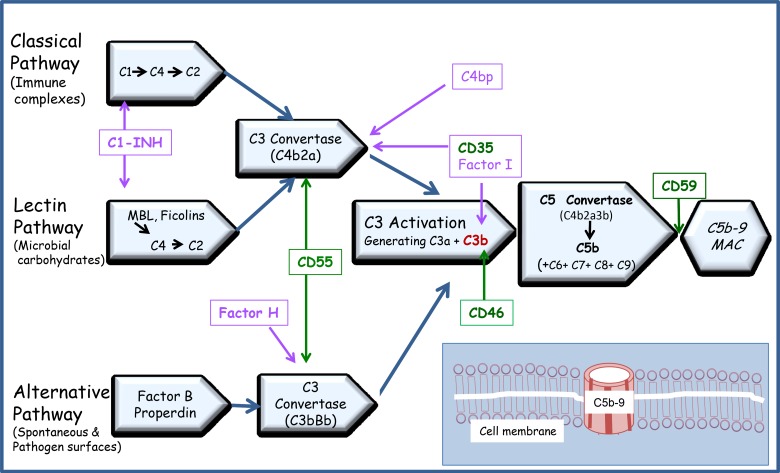
Complement Deficiencies
Early complement deficiencies (C1, C2, C4) associate with lupus-like autoimmunity. Late complement deficiencies (C5–C9, properdin, factor D) associate with recurrent Neisseria infections. Screen with CH50 (classical pathway) and AH50 (alternative pathway).
DiGeorge (22q11.2 Deletion)
CATCH-22: Cardiac anomalies, Abnormal facies, Thymic hypoplasia, Cleft palate, Hypocalcemia. T-cell deficiency severity varies from partial (mild) to complete DiGeorge (SCID-like, requiring thymic or HSCT transplantation).
15 Secondary Immunodeficiency & ALPS Immunodeficiency
Secondary immunodeficiency is far more common than PID. Causes include medications (rituximab, steroids, chemotherapy, anti-seizure drugs), protein loss (nephrotic syndrome, protein-losing enteropathy), malignancy (CLL, multiple myeloma, lymphoma), infection (HIV), malnutrition, and post-transplant immunosuppression. Workup mirrors PID (quantitative immunoglobulins, lymphocyte subsets, vaccine response) but management focuses on reversing the underlying cause and providing Ig replacement or prophylactic antibiotics as indicated.
Autoimmune lymphoproliferative syndrome (ALPS) is a FAS pathway disorder characterized by chronic nonmalignant lymphadenopathy, splenomegaly, autoimmune cytopenias, elevated double-negative T cells (CD3+CD4-CD8-TCRαβ+), and increased lymphoma risk. Treated with immunosuppression (sirolimus, mycophenolate) and splenectomy avoided when possible due to sepsis risk.
16 Allergy/Immunology Procedures Procedures
Skin Prick Testing (SPT)
A drop of standardized allergen extract is placed on the skin (volar forearm or back) and a lancet introduces the allergen into the epidermis. Positive control = histamine; negative control = saline/glycerin. Read at 15–20 minutes. A wheal ≥3 mm larger than saline is considered positive. Antihistamines must be held 5–7 days prior. Document the panel, wheal/flare sizes for each allergen, positive and negative control results, any systemic reactions, and the interpretation.

Intradermal Testing
A small volume (0.02–0.05 mL) of diluted allergen (typically 100–1,000× more dilute than SPT concentrate) is injected intradermally. More sensitive but less specific than SPT; used primarily for venom and drug allergy evaluation, not aeroallergens (high false-positive rate).
Patch Testing
Standardized allergen panels (T.R.U.E. Test 36 allergens, NACDG 80 allergens, or custom series) are applied to the upper back under occlusive chambers. Patches remain in place for 48 hours, then are removed and read at 48 and 96 hours (some allergens require day 7 reading). Reactions are graded: +/- (doubtful), + (weak, erythema, non-vesicular), ++ (strong, edema, vesicles), +++ (extreme, bullous), IR (irritant).
Drug Challenges & Desensitization
Graded drug challenge is the gold standard to rule out drug allergy in low-risk patients: typically 1/10 then full dose with 30-minute observation. Desensitization (temporary tolerance induction) is used when the drug is essential and allergy confirmed; protocols involve 12–16 incremental doubling doses over hours with close monitoring. Document every dose, time, and vital signs.
Oral Food Challenge
The gold standard for diagnosing or excluding food allergy. Performed in a monitored setting with graded doses (typically eighths of a full serving every 15–20 minutes), observation for 2 hours after the final dose. Document dose, time, cumulative amount, symptoms, vitals, treatment, and interpretation.
Venom & Aeroallergen Immunotherapy
See Section 17. Procedural documentation includes extract, vial number/color, dose volume, concentration, injection site, pre/post vital signs, local and systemic reaction.
Skin Biopsy
Performed for urticarial vasculitis (lesions lasting >24 hours, bruising, pain), suspected mastocytosis (stain for tryptase, CD25, CD117), and unclear cutaneous eruptions. Punch biopsy (3–4 mm) is the typical technique.
| Procedure | Purpose | Typical Read Time |
|---|---|---|
| Skin prick test | IgE aeroallergen, food, drug, venom | 15–20 min |
| Intradermal test | Venom, drug, select aeroallergens | 15–20 min |
| Patch test | Allergic contact dermatitis | 48 & 96 h |
| Drug challenge | Confirm/exclude drug allergy | 1–4 h observation |
| Oral food challenge | Confirm/exclude food allergy | 2–4 h |
| Desensitization | Temporary tolerance | 4–8 h |
| Venom immunotherapy | Disease modification | 30-min post-dose obs |
| Skin biopsy | Diagnostic tissue | N/A |
Always chart the vial concentration and dilution step in immunotherapy and desensitization notes — "vial 4 red 0.3 mL" is not interchangeable with "vial 3 blue 0.3 mL" and an error can trigger anaphylaxis. When in doubt, confirm with the nurse before documenting.
17 Immunotherapy & Biologics Treatment
Subcutaneous Immunotherapy (SCIT) & Sublingual Immunotherapy (SLIT)
Allergen-specific immunotherapy is the only disease-modifying treatment for allergic rhinitis, allergic asthma, and stinging insect allergy. SCIT involves a build-up phase (weekly for 3–6 months, escalating concentration and volume) and a maintenance phase (every 2–4 weeks for 3–5 years). SLIT uses FDA-approved tablets (grass: Grastek, Oralair; ragweed: Ragwitek; dust mite: Odactra) taken daily. The 2011 AAAAI/ACAAI Immunotherapy Practice Parameter is the current standard.
Biologics in Allergy & Immunology
| Drug | Target | Approved Indications |
|---|---|---|
| Omalizumab (Xolair) | IgE | Moderate-severe allergic asthma, CSU, nasal polyps, food allergy (reduce reaction severity) |
| Mepolizumab (Nucala) | IL-5 | Severe eosinophilic asthma, EGPA, HES, CRSwNP |
| Reslizumab (Cinqair) | IL-5 | Severe eosinophilic asthma |
| Benralizumab (Fasenra) | IL-5 receptor α | Severe eosinophilic asthma, EGPA |
| Dupilumab (Dupixent) | IL-4Rα (blocks IL-4/IL-13) | Atopic dermatitis, asthma, CRSwNP, EoE, prurigo nodularis, COPD with Type 2 inflammation |
| Tezepelumab (Tezspire) | TSLP | Severe asthma (any phenotype) |
| Tralokinumab (Adbry) | IL-13 | Atopic dermatitis |
| Lebrikizumab (Ebglyss) | IL-13 | Atopic dermatitis |
Hereditary Angioedema Agents
- C1 esterase inhibitor concentrates — Berinert (IV, on-demand), Cinryze (IV, prophylaxis), Ruconest (recombinant, IV, on-demand), Haegarda (SC, prophylaxis).
- Icatibant (Firazyr) — bradykinin B2 receptor antagonist, SC on-demand.
- Ecallantide (Kalbitor) — kallikrein inhibitor, SC on-demand.
- Lanadelumab (Takhzyro) — anti-kallikrein mAb, SC prophylaxis every 2 weeks.
- Berotralstat (Orladeyo) — oral kallikrein inhibitor, daily prophylaxis.
- Antifibrinolytics (tranexamic acid, epsilon-aminocaproic acid) — older prophylaxis option.
Immunoglobulin Replacement (IVIG / SCIG)
For antibody deficiencies (CVID, XLA, specific antibody deficiency, secondary hypogammaglobulinemia with infections). IVIG is given every 3–4 weeks at 400–600 mg/kg; SCIG is given weekly at ~100–150 mg/kg. Document product, dose, infusion rate, pre-medication, vital signs, and any adverse reactions (headache, flushing, rigors, aseptic meningitis with IVIG).
18 Laboratory Testing & Imaging Diagnostics
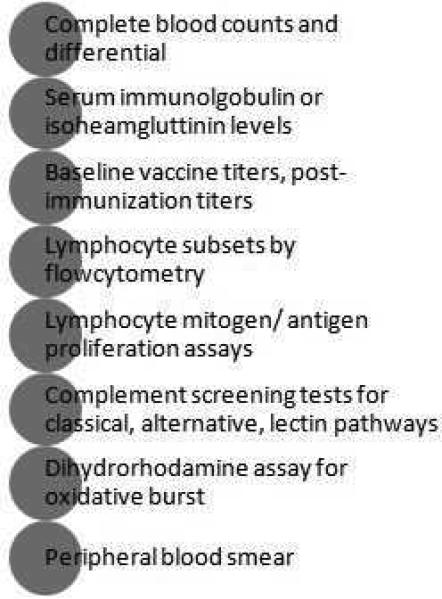
Immunologic Labs You Will See
- Total IgE — elevated in atopy, parasites, ABPA, HES, IgE myeloma, hyper-IgE syndrome.
- Specific IgE (ImmunoCAP) — quantitative allergen-specific antibody, reported in kUA/L; class 0 (<0.35) to class 6 (>100).
- Tryptase — total tryptase >11.4 ng/mL is elevated; baseline >20 supports mast cell disease; peak during anaphylaxis is most useful 15 min–3 h after symptom onset.
- Quantitative immunoglobulins — IgG, IgA, IgM, and IgG subclasses (IgG1–4) for PID workup.
- Vaccine titers — tetanus (protein antigen) and pneumococcal serotype titers (polysaccharide antigen) pre- and post-Pneumovax.
- Lymphocyte subsets — CD3, CD4, CD8, CD19, CD16/56 by flow cytometry.
- Complement — C3, C4, CH50, AH50, C1-INH antigenic and functional levels.
- DHR — dihydrorhodamine flow assay for CGD.
- T-cell function — mitogen (PHA, ConA) and antigen (candida, tetanus) proliferation assays.
- Newborn screen — TREC for SCID, KREC for B-cell deficiencies (select states).
Imaging in the Allergy Clinic
Less imaging-heavy than other specialties, but you will see: sinus CT (chronic rhinosinusitis, nasal polyps, AFRS), chest CT (bronchiectasis in PID or ABPA, ground-glass in HP, nodules in EGPA), high-resolution CT for hypersensitivity pneumonitis, and occasional MRI for complications.
19 Medications You Must Know Pharmacology
| Generic | Brand | Class / Generation | Notes |
|---|---|---|---|
| Diphenhydramine | Benadryl | 1st gen H1 | Sedating; anticholinergic; IV/PO; short-acting |
| Hydroxyzine | Atarax, Vistaril | 1st gen H1 | Sedating; antipruritic |
| Cetirizine | Zyrtec | 2nd gen H1 | Minimally sedating; once daily |
| Levocetirizine | Xyzal | 2nd gen H1 | Active enantiomer of cetirizine |
| Loratadine | Claritin | 2nd gen H1 | Non-sedating |
| Desloratadine | Clarinex | 2nd gen H1 | Active metabolite of loratadine |
| Fexofenadine | Allegra | 2nd gen H1 | Non-sedating; take apart from fruit juice |
| Famotidine | Pepcid | H2 blocker | Adjunct in anaphylaxis, urticaria, MCAS |
| Ranitidine | Zantac | H2 blocker | Withdrawn 2020 (NDMA); historical relevance |
| Generic | Brand | Class |
|---|---|---|
| Fluticasone propionate | Flonase | INCS |
| Fluticasone furoate | Flonase Sensimist, Veramyst | INCS |
| Mometasone | Nasonex | INCS |
| Budesonide | Rhinocort | INCS |
| Triamcinolone | Nasacort | INCS |
| Azelastine | Astelin, Astepro | Intranasal antihistamine |
| Olopatadine | Patanase | Intranasal antihistamine |
| Azelastine/fluticasone | Dymista | Combination INAH + INCS |
| Ipratropium | Atrovent nasal | Anticholinergic (rhinorrhea) |
| Cromolyn sodium | NasalCrom | Mast cell stabilizer |
| Generic | Brand | Class |
|---|---|---|
| Montelukast | Singulair | LTRA — boxed warning for neuropsych effects |
| Zafirlukast | Accolate | LTRA |
| Zileuton | Zyflo | 5-lipoxygenase inhibitor |
| Fluticasone/salmeterol | Advair | ICS/LABA |
| Budesonide/formoterol | Symbicort | ICS/LABA — MART/SMART therapy |
| Fluticasone/umeclidinium/vilanterol | Trelegy | ICS/LAMA/LABA |
| Albuterol | ProAir, Ventolin, Proventil | SABA |
| Drug | Dose/Form | Notes |
|---|---|---|
| Epinephrine IM | 0.3 mg adult / 0.15 mg peds auto-injector; 0.01 mg/kg | First-line; repeat q5–15 min PRN |
| EpiPen, Auvi-Q, Adrenaclick, Neffy | Auto-injectors (Neffy is intranasal) | Prescribe 2 devices |
| Methylprednisolone | 1–2 mg/kg IV | Adjunct, not first-line |
| Prednisone | 40–60 mg PO taper | Post-anaphylaxis, severe urticaria |
| Glucagon | 1–5 mg IV | Beta-blocked patients with refractory anaphylaxis |
20 Classification Systems Reference
Several systems beyond those already enumerated in disease sections appear in allergy notes. Document the named system whenever the attending references it.
- NIAID/FAAN 2006 Anaphylaxis Criteria — the predecessor to the WAO 2020 criteria; still referenced.
- SCORAD / EASI / IGA — atopic dermatitis severity scores (SCORing Atopic Dermatitis, Eczema Area and Severity Index, Investigator Global Assessment).
- UAS7 — Urticaria Activity Score over 7 days (0–42); guides chronic urticaria therapy escalation.
- ACT / C-ACT — Asthma Control Test (ages 12+) / Childhood ACT (ages 4–11).
- TNSS / RQLQ — Total Nasal Symptom Score / Rhinoconjunctivitis Quality of Life Questionnaire.
- GINA steps 1–5 — asthma treatment ladder.
- Lund-Mackay — sinus CT scoring for chronic rhinosinusitis.
- Samter's triad — aspirin sensitivity + nasal polyps + asthma (NERD/AERD).
21 Physical Exam — The Allergy Exam
Allergy exams are focused but systematic. Document these elements by system.
Gen: well-appearing, NAD
HEENT:
Eyes — conjunctivae clear/injected, no chemosis, allergic shiners absent/present
Ears — TMs clear bilaterally, no effusion
Nose — turbinates pale/boggy/erythematous, clear rhinorrhea absent/present, septum midline, no polyps
Oropharynx — cobblestoning absent/present, no tonsillar enlargement, uvula midline
Neck: supple, no lymphadenopathy, no thyromegaly
Lungs: CTA bilat, no wheeze/rhonchi/rales, good air movement
CV: RRR, no m/r/g
Abd: soft, nontender, no HSM
Skin: no rash, no wheals, no dermatographism; [describe lesions — distribution, morphology, scaling, lichenification]
Extremities: no edema, no clubbing
Neuro: A&Ox3, grossly intact
Mental status, gait, and cranial nerve exam are added for complex immunodeficiency or vasculitis consults. For atopic dermatitis visits, document body surface area (BSA) affected, EASI score components, lichenification, excoriation, and any signs of secondary infection.
22 Abbreviations Master List Reference
Diagnoses & Conditions
Procedures, Testing & Therapies
Labs & Diagnostics
23 Sample HPI Templates
These templates show the kind of documentation expected in an allergy/immunology clinic note. Use them as frameworks to internalize the rhythm and content of a good allergy HPI.
"Ms. [Name] is a 32-year-old female with a history of childhood eczema and mild intermittent asthma who presents for evaluation of year-round nasal symptoms worsening over the past 2 years. She reports daily sneezing paroxysms, clear rhinorrhea, bilateral nasal congestion, and itchy watery eyes. Symptoms are worst in the morning and when vacuuming, and are significantly exacerbated in spring (March–May) and fall (September). She has two indoor cats and a dog; symptoms improve on vacation away from home. She denies epistaxis, facial pain, anosmia, or asthma exacerbations. Current medications: cetirizine 10 mg PRN with partial relief, fluticasone nasal spray used inconsistently. She has not tried allergen avoidance measures and has no prior skin or blood allergy testing. Impact: sleep is disrupted 3–4 nights/week and she has missed work twice this month. On exam, turbinates are pale and boggy bilaterally with clear rhinorrhea, bilateral allergic shiners, cobblestoning of posterior pharynx, lungs clear."
"Mr. [Name] is a 45-year-old male with no known prior food allergies referred from the ED for evaluation of anaphylaxis 4 days ago. At approximately 7:30 PM, 20 minutes after finishing a restaurant meal containing shrimp scampi (first known shrimp exposure), he developed generalized pruritus and urticaria, lip and tongue swelling, throat tightness, dyspnea with wheezing, two episodes of vomiting, and presyncope. Wife called 911. EMS administered IM epinephrine 0.3 mg at 8:05 PM with partial improvement. On ED arrival at 8:20 PM: BP 82/50, HR 125, SpO2 92% on RA. Received a second IM epinephrine 0.3 mg, IV methylprednisolone 125 mg, diphenhydramine 50 mg, famotidine 20 mg, 1 L NS bolus, and albuterol nebulizer. Symptoms resolved over 90 minutes. Observed for 6 hours without biphasic reaction and discharged with EpiPen 2-pack, prednisone 40 mg PO × 3 days, and allergy referral. He denies prior shellfish reactions (had not eaten shrimp before). Reports tolerating crab and lobster occasionally without issue. No NSAIDs, alcohol, or exercise surrounding the meal. No history of mastocytosis symptoms or unprovoked anaphylaxis. Plan includes skin prick and specific IgE to shellfish panel, baseline tryptase."
"Mrs. [Name] is a 38-year-old female presenting with 11 months of daily itchy wheals without identifiable trigger. Lesions appear on the trunk, arms, and thighs, last 6–12 hours (never >24 hours), resolve without bruising or scarring. Intermittent lip and periorbital angioedema 2–3 times per month; no tongue or laryngeal involvement, no GI symptoms, no hemodynamic instability. Triggers not identified: no correlation with foods, medications, cold, heat, pressure, exercise, or menses. She has tried cetirizine 10 mg daily without relief, then fexofenadine 180 mg BID and loratadine 10 mg QHS added with minimal improvement. No NSAIDs, ACE inhibitors, or recent infections. Past medical history includes hypothyroidism on levothyroxine. Family history negative for HAE. UAS7 score today: 28 (moderate-to-severe). Workup ordered: CBC, CMP, TSH, anti-TPO, ESR, CRP, total IgE. Plan: up-dose to 4× standard second-generation antihistamine, add famotidine 20 mg BID, discuss omalizumab if inadequate response in 4 weeks."
"Mr. [Name] is a 52-year-old male with a PCN allergy label dating to age 7 who presents for delabeling prior to upcoming dental implant surgery. He recalls developing a generalized maculopapular rash approximately 5 days into a course of amoxicillin for otitis media. No hives, angioedema, wheeze, hypotension, mucosal involvement, or skin detachment reported. Rash resolved within 1 week of stopping. No subsequent exposures to any β-lactams since childhood (he has avoided them entirely). He has taken cephalexin twice without issue in the past decade. No personal or family history of SJS, TEN, DRESS, or serum sickness. Reaction classified as low-risk childhood exanthem. Plan: after obtaining consent and confirming no antihistamine use in past 5 days, proceed with penicillin skin testing (Pre-Pen, penicillin G major and minor determinants, positive and negative controls) followed by oral amoxicillin 250 mg graded challenge with 1-hour observation if testing negative."
"Ms. [Name] is a 28-year-old female referred for recurrent sinopulmonary infections over the past 6 years. She reports 5–7 sinus infections annually requiring oral antibiotics, 3 episodes of pneumonia (2 requiring hospitalization, one with Streptococcus pneumoniae bacteremia), chronic productive cough, and sinus CT showing chronic pansinusitis. She has also had 2 episodes of bacterial gastroenteritis and chronic intermittent diarrhea with confirmed Giardia last year. Denies opportunistic infections, deep-seated abscesses, or unusual organisms. Immunizations up to date. Past medical history: ITP at age 24 (resolved with steroids), mild splenomegaly on recent ultrasound. Family history: sister with recurrent sinus infections and ITP. Prior workup (outside): IgG 410 mg/dL (low), IgA 32 mg/dL (low), IgM 48 mg/dL (low-normal), poor response to Pneumovax post-immunization (protective titers to 3 of 14 serotypes). HIV negative. Plan: repeat quantitative immunoglobulins, lymphocyte subsets, IgG subclasses, tetanus titer, and evaluate for CVID per ESID criteria; if confirmed, initiate Ig replacement therapy."
"Patient is a 3-year-old male brought in by mother for evaluation of suspected peanut allergy. At 14 months, within 5 minutes of eating peanut butter for the first time, he developed perioral hives, facial swelling, and 2 episodes of vomiting. No respiratory or cardiovascular symptoms. Mother gave diphenhydramine; symptoms resolved over 1 hour. Strict peanut avoidance since, including other tree nuts out of precaution. He tolerates all other allergens including egg, milk, wheat, soy, fish, shellfish, and sesame. Past medical history: severe infantile eczema (now well-controlled), mild intermittent wheezing with viral URIs. Family history: older sister with allergic rhinitis, father with asthma. No prior formal testing. Plan: skin prick testing to peanut and tree nut panel, Ara h 2 component IgE, discuss risk stratification, epinephrine auto-injector training, and potential for future oral food challenge or oral immunotherapy."
The best allergy/immunology scribes are detail obsessives. When the attending says "the reaction was about 20 minutes after the bite of shrimp," you write "20 minutes after ingestion of shrimp" — precision matters because it determines whether this is IgE-mediated, alpha-gal, FPIES, or scombroid. When the attending mentions "omalizumab 300 mg every 4 weeks," you already know the indication (allergic asthma, CSU, CRSwNP, or food allergy), the IgE-based dosing table, and to document the pre/post vitals and observation period.
Listen for the named classifications — WAO, Ring & Messmer, Mueller, ARIA, GINA, ESID, Gell & Coombs — and write them into the assessment exactly as the attending references them. Always chart route, dose, time, and specific agents in exact detail. Pre-populate labs and imaging before the patient arrives. Know your biologics by brand, generic, and target. Keep a mental map of which reactions absolutely preclude testing or challenge (SJS/TEN, DRESS, AGEP, hemolysis, interstitial nephritis).
Allergy/immunology rewards scribes who love precision and understand that a few extra words in the HPI can change a diagnosis. Welcome to the specialty.
24 References & Sources
Clinical Practice Guidelines
Cardona V, et al. World Allergy Organization Anaphylaxis Guidance 2020. World Allergy Organ J. 2020.
Dykewicz MS, et al. Rhinitis 2020: A practice parameter update. J Allergy Clin Immunol. 2020.
Global Initiative for Asthma. GINA Main Report 2024.
Khan DA, et al. Drug allergy: A 2022 practice parameter update. J Allergy Clin Immunol. 2022.
ESID Registry — Working Definitions for Clinical Diagnosis of Primary Immunodeficiency.
U.S. Preventive Services Task Force (USPSTF) recommendations — relevant to asthma screening, atopic comorbidity, and preventive services.
Landmark Trials & Key Studies
Diagram & Figure Sources
Figure 1: Immune System Cell Migration. OpenStax College, Anatomy & Physiology. CC BY 3.0.
Figure 2: Anatomy of the Lymphatic System. OpenStax College, Anatomy & Physiology. CC BY 3.0.
Figure 3: Signs and Symptoms of Anaphylaxis. Mikael Häggström, Wikimedia Commons. Public domain.
Figure 4: Allergy Skin Testing. Wolfgang Ihloff, Wikimedia Commons. CC BY-SA 3.0.