Child & Adolescent Psychiatry
Every diagnosis, developmental milestone, rating scale, medication, abbreviation, and documentation framework you need to scribe in child & adolescent psychiatry.
All diagrams on this page are sourced from published educational or institutional materials rather than AI generation. Each figure caption links to the original source, and the full diagram and guideline citations are collected in the references section at the bottom.
01 Child Psychiatry Foundations & Normal Development
Child and adolescent psychiatry is the medical specialty that evaluates and treats mental, emotional, developmental, and behavioral disorders in patients from infancy through young adulthood (roughly 0–21, though some clinics extend to 25 for transition-age youth). Unlike adult psychiatry, every diagnosis must be interpreted through the lens of normal development. A behavior that is pathological at age 10 may be developmentally expected at age 3. The scribe must understand both the disease framework (DSM-5-TR) and the developmental framework (milestones, temperament, attachment, adolescence) to chart accurately.
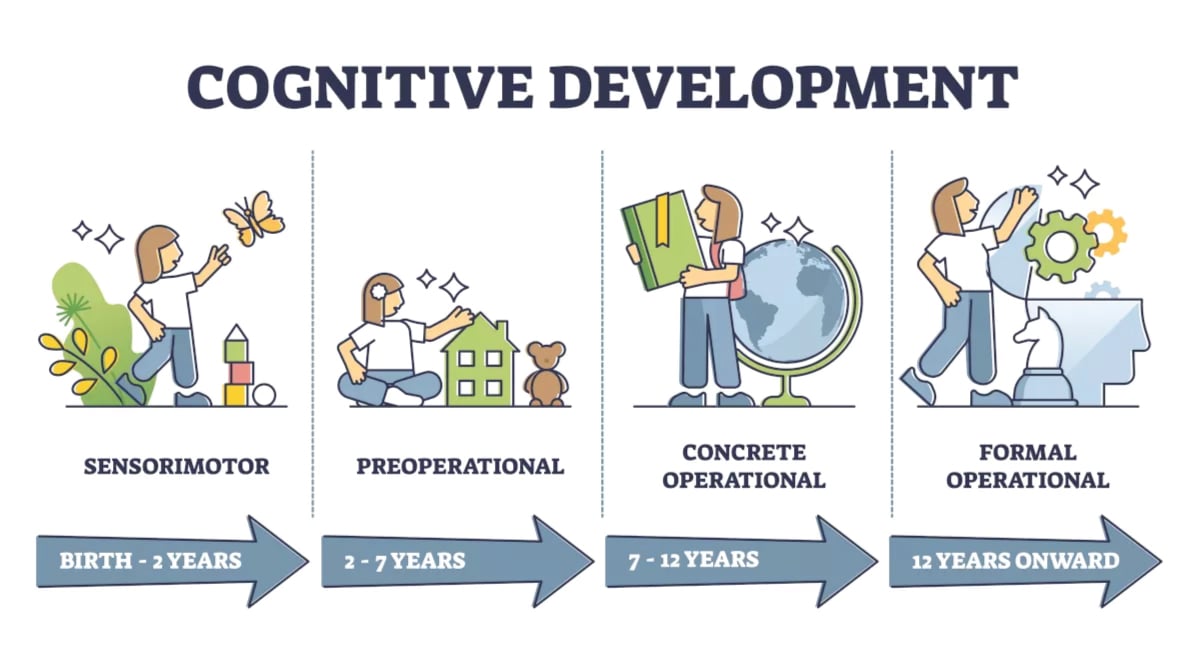
Developmental Framework
Clinicians continuously ask themselves whether a presenting concern represents developmental variation, developmental delay, or a psychiatric disorder. Developmental domains evaluated at every encounter include gross motor, fine motor, language (receptive and expressive), cognitive, social-emotional, and adaptive (self-care) skills. A delay in one domain is a red flag; delay in two or more is called global developmental delay and almost always prompts a workup.
Key Developmental Milestones
| Age | Gross Motor | Language | Social-Emotional |
|---|---|---|---|
| 2 months | Lifts head prone | Coos, turns to voice | Social smile |
| 6 months | Rolls, sits with support | Babbles | Recognizes caregivers, stranger awareness emerging |
| 12 months | Cruises, first steps | First words, follows simple commands | Waves, plays pat-a-cake, separation anxiety |
| 18 months | Walks well, runs | 10–25 words, points to objects | Parallel play, imitates |
| 2 years | Kicks ball, walks stairs | 2-word phrases, 50+ words, 50% intelligible | Tantrums normal, pretend play begins |
| 3 years | Tricycle, jumps | 3-word sentences, 75% intelligible | Shares briefly, toilet trained (most) |
| 4 years | Hops on one foot | 100% intelligible to strangers, tells stories | Cooperative play, imaginative friends |
| 5 years | Skips | Complex sentences, counts, names colors | Follows rules in games, dresses independently |
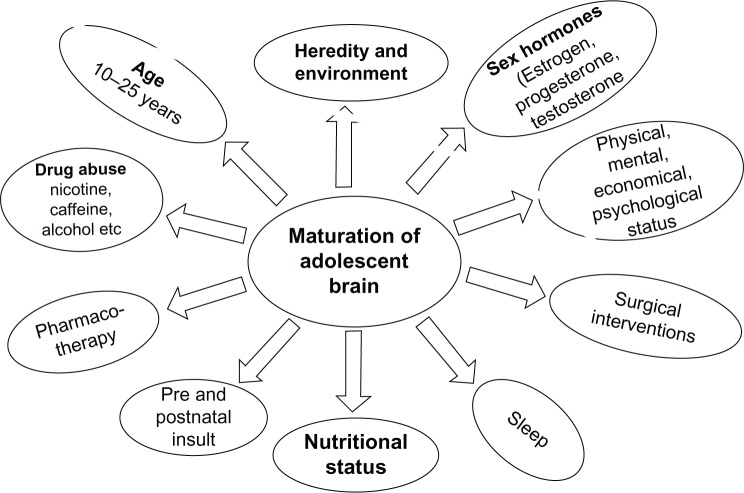
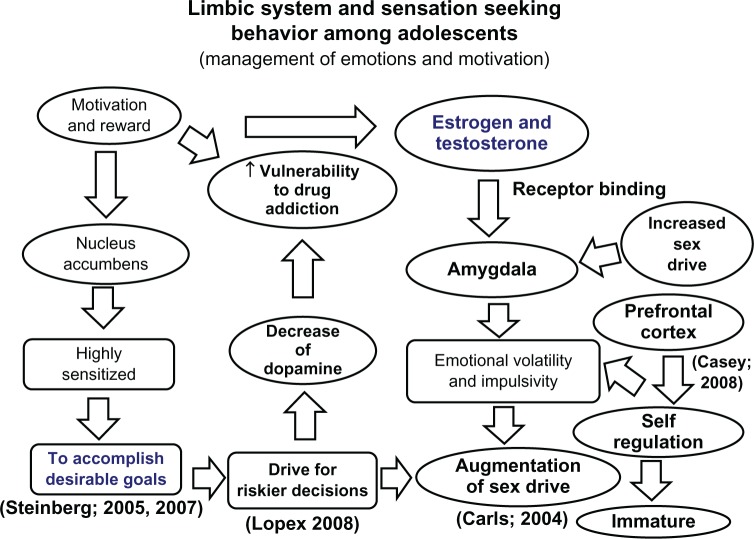
Adolescent Development
Adolescence (roughly 11–21) is marked by puberty, identity formation, abstract cognition, and the peak onset of most psychiatric disorders. The prefrontal cortex is the last brain region to fully mature (~age 25), explaining why risk-taking, poor impulse control, and emotional volatility are developmentally normative. Most psychiatric disorders — mood, anxiety, psychosis, eating disorders, substance use — have their first presentation during this window, which is why adolescence is the single highest-yield period for early intervention.
Always chart age in years and months for children under 5 (e.g., "3y 4m") and note the developmental domain when a concern is raised. The attending will constantly reference milestones; if the parent says "he still isn't saying two-word phrases at 2.5 years," that is a language delay and must be in the HPI verbatim.
02 Scribe Documentation Framework (SOAP, HPI, MSE)
Child psychiatry notes have three peculiarities: (1) the history is obtained from multiple informants (parent, child, teacher, prior therapist, pediatrician); (2) the mental status exam replaces the physical exam as the central objective finding; and (3) every note must contain a safety assessment (suicidality, self-injury, homicidality, access to means).
Chief Complaint: State who brought the child, why, and in whose words. Example: "7-year-old male brought by mother for evaluation of 'inability to pay attention in school and frequent meltdowns.'"
HPI: Document onset, duration, frequency, severity, setting (home/school/peers), triggers, and course of symptoms. Always note pervasiveness (do symptoms cross settings?) and impairment (academic, social, family functioning). Capture collateral: teacher reports, prior Vanderbilt/SNAP scores, pediatrician's referral concerns.
Developmental History: Pregnancy (prenatal exposures, complications), birth (gestational age, NICU stay), milestones (motor, language, toileting), early temperament.
Past Psychiatric History: Prior diagnoses, psychiatric hospitalizations, prior medication trials (drug, max dose, duration, response, side effects), prior therapists, suicide attempts, self-injury.
Past Medical History: Seizures, head injury, thyroid disease, asthma, allergies, prematurity, growth parameters.
Family History: First-degree relatives with ADHD, depression, bipolar, anxiety, OCD, psychosis, substance use, suicide, tics, autism, learning disorders.
Social History: Household composition, custody arrangement, stressors, moves, school (grade, IEP/504, bullying, academic performance), screen time, sleep, diet, exercise, trauma screen (ACEs), firearms in home.
Safety: Suicidal ideation (passive/active, plan, intent, means), homicidal ideation, non-suicidal self-injury (NSSI), access to firearms/medications, and any prior attempts. This must be in every note.
The MSE replaces the physical exam as the central objective finding. See Section 21 for the full pediatric MSE template. Also document vitals (HR, BP, weight, height, BMI percentile) because stimulants and antipsychotics require growth and cardiovascular monitoring.
Diagnoses using DSM-5-TR terminology with ICD-10 codes, differential, formulation (biopsychosocial), and plan: therapy modality, medication changes (with indication and dosing rationale), labs, collateral contacts (school, PCP), next appointment, and explicit safety plan.
You will hear the attending say "developmentally appropriate" or "age-inconsistent" — these phrases are your cue to match symptoms to the developmental framework. Never chart a toddler's tantrum as pathological without context. Also: always document the informant next to each piece of history ("per mother," "per patient," "per teacher form").
03 Attention-Deficit/Hyperactivity Disorder (ADHD) Neurodevelopmental
ADHD is the single most common diagnosis in child psychiatry, affecting ~9% of children in the US. It is a neurodevelopmental disorder of inattention, hyperactivity, and impulsivity that begins before age 12, persists >6 months, is present in 2+ settings, and causes functional impairment.
Pathophysiology
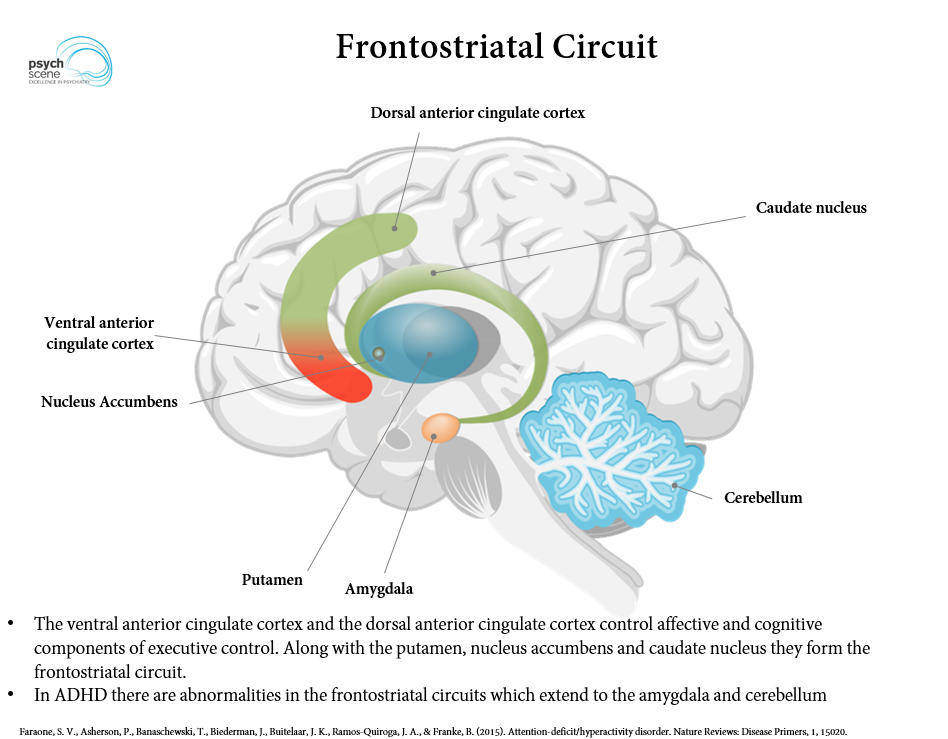
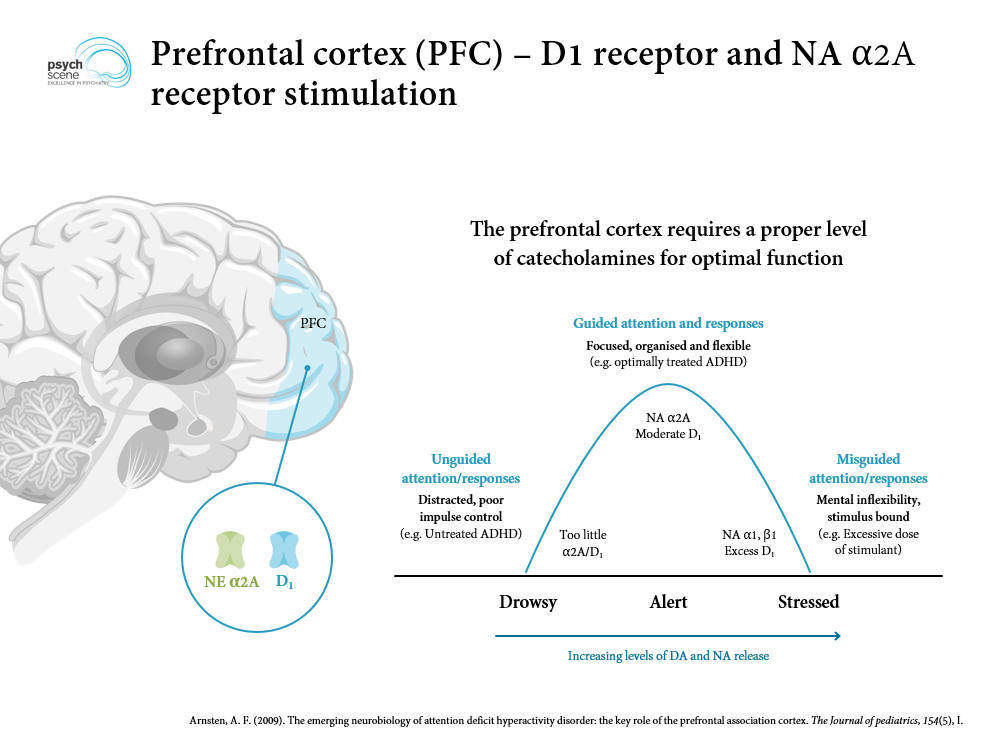
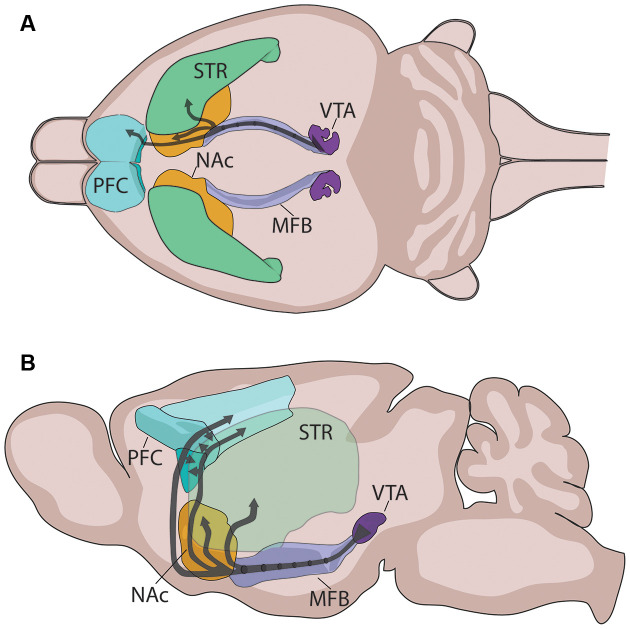
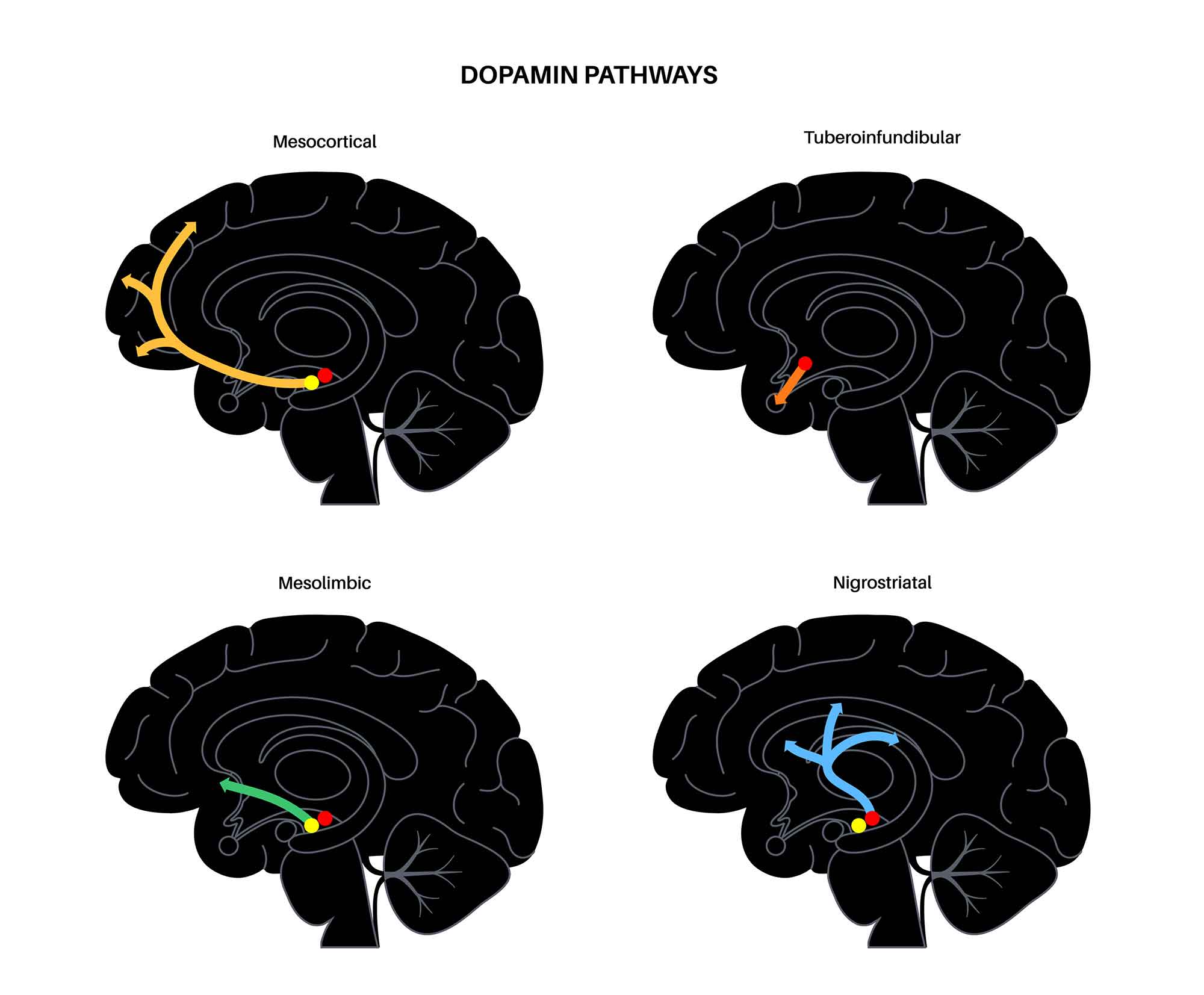
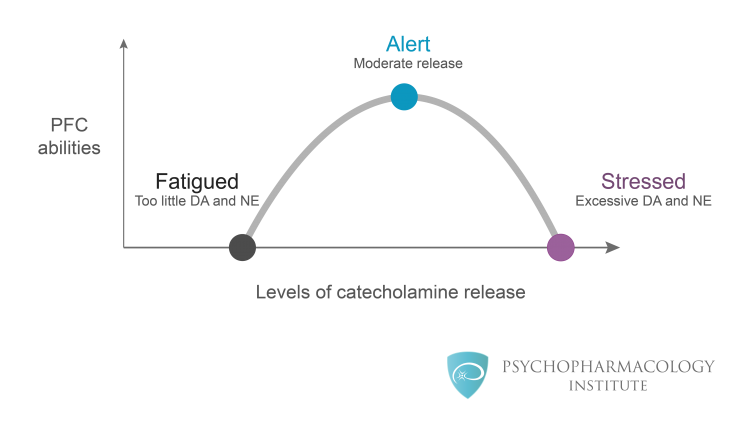
ADHD involves dysfunction of fronto-striatal and fronto-cerebellar circuits mediated by dopamine and norepinephrine. Delayed cortical maturation (especially prefrontal cortex) and reduced activation of executive-function networks underlie symptoms. Strongly heritable (h² ~0.75) — family history is often the first clue.
Inattention (6+ symptoms for children, 5+ for age 17+):
- Fails to give close attention to details or makes careless mistakes
- Difficulty sustaining attention in tasks/play
- Does not seem to listen when spoken to directly
- Does not follow through on instructions, fails to finish tasks
- Difficulty organizing tasks and activities
- Avoids tasks requiring sustained mental effort
- Loses things necessary for tasks
- Easily distracted by extraneous stimuli
- Forgetful in daily activities
Hyperactivity/Impulsivity (6+ symptoms for children, 5+ for age 17+):
- Fidgets, taps hands/feet, squirms
- Leaves seat when remaining seated is expected
- Runs/climbs inappropriately (restlessness in adolescents)
- Unable to play quietly
- "On the go" / "driven by a motor"
- Talks excessively
- Blurts out answers before question completed
- Difficulty waiting turn
- Interrupts or intrudes on others
Required for diagnosis: symptoms present before age 12, in ≥2 settings, causing impairment, not better explained by another disorder.
Presentations & Subtypes
| Presentation | Criteria Met | Classic Picture |
|---|---|---|
| Combined | 6+ inattentive AND 6+ hyperactive/impulsive | Most common in elementary-school boys |
| Predominantly Inattentive | 6+ inattentive only | "Daydreamer"; often missed in girls; academic underachievement |
| Predominantly Hyperactive-Impulsive | 6+ hyperactive/impulsive only | Younger children; may evolve into combined type |
Severity is rated mild, moderate, or severe based on symptom count beyond threshold and functional impairment.
Diagnostic Workup
Diagnosis is clinical and requires multi-informant rating scales. The Vanderbilt ADHD Diagnostic Rating Scale is the most widely used in primary care and pediatric psychiatry and is available in parent and teacher versions. Scoring: a symptom counts as "present" if rated 2 (often) or 3 (very often). The parent scale screens for ODD, conduct disorder, anxiety/depression, and performance impairment. Alternatives include the SNAP-IV and Conners-3. Rule out medical mimics: hearing/vision impairment, OSA, iron deficiency, thyroid dysfunction, absence seizures, trauma, learning disorder.
Management
The AAP 2019 ADHD clinical practice guideline and AACAP ADHD practice parameter structure treatment by age. Preschool (4–5): parent training in behavior management (PCIT, Triple P) first-line; methylphenidate if severe, refractory. Elementary (6–12): combination of FDA-approved medication and behavioral therapy + school accommodations (IEP/504). Adolescent (12–17): medication + behavior therapy, with adolescent assent. Stimulants (methylphenidate, amphetamine) are first-line (70–80% response). Non-stimulants (atomoxetine, guanfacine ER, clonidine ER, viloxazine) are alternatives for poor responders, substance risk, tics, or side effects.
You will chart Vanderbilt and SNAP-IV scores constantly. Always document the informant ("parent Vanderbilt" vs "teacher Vanderbilt") and the specific subscale totals. At medication visits, capture current dose, schedule, duration of effect, appetite, sleep, mood, rebound, tics, and growth (weight/height percentiles).
04 Autism Spectrum Disorder (ASD) Neurodevelopmental
Autism spectrum disorder is a neurodevelopmental disorder characterized by persistent deficits in social communication and restricted, repetitive behaviors. Prevalence is ~1 in 36 per the CDC's ADDM network. DSM-5-TR eliminated prior subtypes (Asperger, PDD-NOS) in favor of a single spectrum diagnosis with severity levels.
DSM-5-TR Core Criteria
- Persistent deficits in social communication/interaction across multiple contexts: (a) social-emotional reciprocity, (b) nonverbal communication (eye contact, gestures, facial expression), (c) developing/maintaining relationships.
- Restricted, repetitive patterns of behavior/interests/activities (2 of 4): (a) stereotyped/repetitive movements or speech, (b) insistence on sameness/routines, (c) highly restricted fixated interests, (d) hyper- or hyporeactivity to sensory input.
- Symptoms present in early developmental period (though may not fully manifest until social demands exceed capacity).
- Cause clinically significant impairment.
- Not better explained by intellectual disability or global developmental delay.
Severity Levels — Full Enumeration
| Level | Social Communication | Restricted/Repetitive | Support Needed |
|---|---|---|---|
| Level 1 | Noticeable deficits without supports; difficulty initiating; atypical responses | Inflexibility interferes with functioning; difficulty switching activities | Requiring support |
| Level 2 | Marked deficits; limited initiation; reduced/abnormal response to others | Frequent RRBs obvious to casual observer; distress changing focus | Requiring substantial support |
| Level 3 | Severe deficits; very limited initiation; minimal response | Extreme inflexibility; RRBs markedly interfere with all functioning | Requiring very substantial support |
Screening & Diagnosis
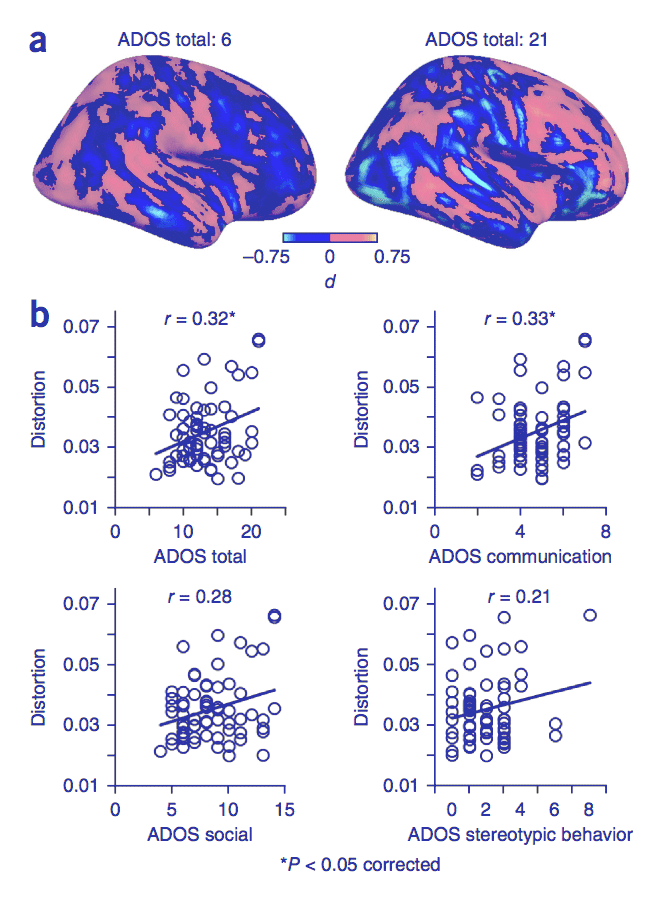
The AAP autism identification guideline recommends universal autism-specific screening at 18 and 24 months using the M-CHAT-R/F. Scoring: total score 0–2 = low risk; 3–7 = medium (follow-up interview); 8–20 = high risk (refer for diagnostic evaluation). Definitive diagnosis uses the ADOS-2 (Autism Diagnostic Observation Schedule) and ADI-R (Autism Diagnostic Interview-Revised), typically administered by developmental psychologists.
Management
The AACAP ASD practice parameter emphasizes early intensive behavioral intervention, particularly applied behavior analysis (ABA), speech-language therapy, occupational therapy, and parent training. No medication treats core autism symptoms; however, risperidone and aripiprazole are FDA-approved for irritability and aggression in autism. SSRIs may target comorbid anxiety or OCD-like rigidity. Stimulants are used cautiously for comorbid ADHD. Screen for seizures, sleep disturbance, GI issues, and genetic syndromes (Fragile X, Rett, tuberous sclerosis).
05 Intellectual, Learning & Communication Disorders Neurodevelopmental
Intellectual Developmental Disorder (Intellectual Disability)
Defined by deficits in both intellectual functioning (reasoning, problem-solving, abstract thinking) and adaptive functioning (conceptual, social, practical) with onset during the developmental period. Severity (mild, moderate, severe, profound) is based on adaptive functioning rather than IQ alone, though IQ <70 is typical. Etiologies: genetic syndromes (Down, Fragile X, Williams, Prader-Willi), prenatal (fetal alcohol, infection), perinatal (hypoxic-ischemic injury), postnatal (meningitis, TBI), idiopathic. Workup for unexplained ID includes chromosomal microarray, Fragile X testing, metabolic studies, and brain MRI when indicated.
Global Developmental Delay
Used for children <5 years who cannot reliably complete IQ testing but demonstrate delays in 2+ developmental domains. Reassessed as the child ages.
Specific Learning Disorder (SLD)
Difficulty learning and using academic skills with symptoms ≥6 months despite interventions, affecting reading (dyslexia), written expression (dysgraphia), or mathematics (dyscalculia). Performance is substantially below age expectations and causes impairment. Requires normal intelligence and no other sensory/neurological cause. Documented via psychoeducational testing and addressed via IEP/504 plans.
Communication Disorders
- Language Disorder: persistent difficulty acquiring and using language (reduced vocabulary, limited sentence structure, impaired discourse).
- Speech Sound Disorder: difficulty with speech production (articulation) interfering with intelligibility.
- Childhood-Onset Fluency Disorder (Stuttering): disturbance in normal fluency and time patterning.
- Social (Pragmatic) Communication Disorder: persistent difficulty with social use of verbal and nonverbal communication without the restricted repetitive behaviors that would make it autism.
Management is speech-language therapy, IEP services, and classroom accommodations.
06 Motor & Tic Disorders Neurodevelopmental
Developmental Coordination Disorder (DCD)
Acquisition and execution of coordinated motor skills substantially below expectation for age (clumsy, slow, inaccurate motor performance), interfering with ADLs and academics. Onset in early developmental period. Managed with OT.
Stereotypic Movement Disorder
Repetitive, seemingly driven, purposeless motor behavior (hand flapping, body rocking, self-biting, head banging). May occur with or without self-injurious behavior and is commonly seen in intellectual disability and autism.
Tic Disorders
- Provisional Tic Disorder: single/multiple motor and/or vocal tics, <1 year duration.
- Persistent (Chronic) Motor OR Vocal Tic Disorder: single or multiple motor OR vocal tics (not both), >1 year, onset before 18.
- Tourette's Disorder: both multiple motor AND one or more vocal tics (not necessarily concurrent), >1 year, onset before 18.
Tics wax and wane, worsen with stress/fatigue, and are often preceded by a premonitory urge. ~85% of Tourette patients have comorbid ADHD or OCD. Management: psychoeducation first, Comprehensive Behavioral Intervention for Tics (CBIT) as first-line behavioral treatment. Medications (alpha-2 agonists guanfacine/clonidine first-line; antipsychotics like aripiprazole, risperidone, or pimozide for severe cases) per the AACAP tic disorders practice parameter.
07 Disruptive, Impulse-Control & Conduct Disorders Externalizing
Oppositional Defiant Disorder (ODD)
Pattern of angry/irritable mood, argumentative/defiant behavior, or vindictiveness lasting ≥6 months and involving ≥4 symptoms from these categories (for children <5: on most days; ≥5: at least weekly). Symptoms include losing temper, easily annoyed, angry/resentful, arguing with authority, actively defying rules, deliberately annoying others, blaming others, spiteful or vindictive twice in 6 months. Must cause impairment and not occur exclusively during a mood/psychotic disorder.
Conduct Disorder (CD)
Repetitive, persistent pattern of behavior violating basic rights of others or major societal norms: aggression to people/animals, destruction of property, deceitfulness/theft, serious violations of rules. ≥3 criteria in the past 12 months with at least 1 in past 6 months. Specifiers: childhood-onset (before 10), adolescent-onset, with limited prosocial emotions ("callous-unemotional"). Strong risk factor for antisocial personality disorder in adulthood.
Disruptive Mood Dysregulation Disorder (DMDD)
Severe recurrent temper outbursts (verbal or behavioral) grossly out of proportion, ≥3 times/week, with persistently irritable/angry mood between outbursts, present for ≥12 months in ≥2 settings. Age of onset before 10, diagnosis between 6 and 18. Created to reduce over-diagnosis of pediatric bipolar disorder.
Intermittent Explosive Disorder (IED)
Recurrent behavioral outbursts representing failure to control aggressive impulses (verbal aggression twice weekly for 3 months, OR 3 behavioral outbursts involving damage/assault in 12 months). Minimum age 6.
Management of externalizing disorders emphasizes parent management training (PMT), Parent-Child Interaction Therapy (PCIT) for young children, multi-systemic therapy for older adolescents, treating comorbid ADHD aggressively, and SSRIs or atypical antipsychotics as adjuncts when irritability or aggression is severe.
08 Mood Disorders in Children & Adolescents Internalizing
Major Depressive Disorder (MDD)
DSM-5-TR criteria in youth mirror adults but with key differences: in children and adolescents, mood may be irritable rather than sad, and failure to make expected weight gain can substitute for weight loss. ≥5 of 9 SIGECAPS symptoms (depressed/irritable mood, anhedonia, sleep disturbance, interest loss, guilt/worthlessness, energy loss, concentration, appetite/weight, psychomotor change, suicidal ideation) for ≥2 weeks with impairment.
Screening: PHQ-A (adolescent modification) and PHQ-9 modified for adolescents. The Mood and Feelings Questionnaire (MFQ) is the most widely used child depression scale. Per USPSTF 2022 guidance, screen adolescents aged 12–18 for MDD routinely.
Management follows the AACAP depression practice parameter: mild depression → psychotherapy (CBT, IPT-A); moderate-severe → SSRI + CBT (combination superior per the TADS trial). Fluoxetine is FDA-approved for MDD ages 8+; escitalopram for ages 12+. All antidepressants carry a black box warning for increased suicidal ideation in patients <25; weekly follow-up is recommended for the first 4 weeks.
Persistent Depressive Disorder (Dysthymia)
Depressed or irritable mood most days for ≥1 year in children/adolescents (vs 2 years in adults) plus 2+ symptoms (appetite, sleep, energy, self-esteem, concentration, hopelessness).
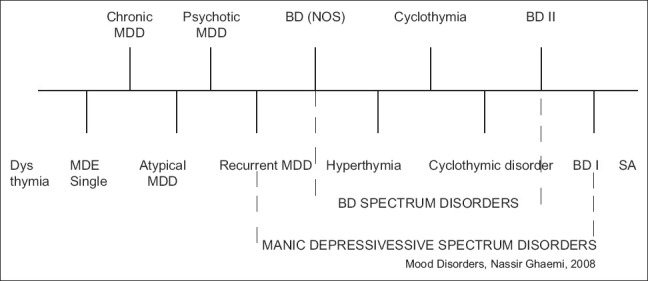
Bipolar Disorder in Pediatrics
Classical Bipolar I requires a manic episode (distinct period of abnormally elevated/irritable mood with ≥3 symptoms DIGFAST — distractibility, indiscretion, grandiosity, flight of ideas, activity increase, sleep decrease, talkativeness — lasting ≥7 days or requiring hospitalization). Pediatric bipolar is controversial and over-diagnosed; rigid application of criteria is essential. Treatment: lithium (FDA approved age 7+), risperidone, aripiprazole, quetiapine, olanzapine, lurasidone; valproate and lamotrigine are used off-label. Per the AACAP bipolar practice parameter.
09 Anxiety Disorders in Youth Internalizing
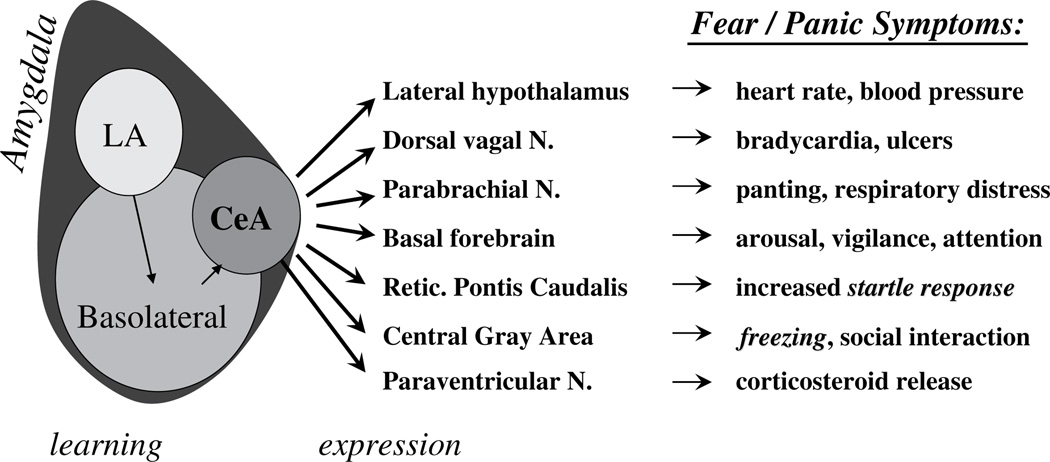
Anxiety disorders are the most common psychiatric disorders in children (~1 in 12). They share a pattern of developmentally inappropriate, persistent, impairing anxiety.
Separation Anxiety Disorder
Developmentally inappropriate and excessive fear concerning separation from attachment figures (≥3 of 8 symptoms including distress on separation, worry about harm to caregivers, refusal to leave home, nightmares of separation, physical complaints). Duration ≥4 weeks in children.
Selective Mutism
Consistent failure to speak in specific social situations where speaking is expected (e.g., school) despite speaking in others. Lasts ≥1 month (beyond first month of school). Interferes with achievement or communication.
Specific Phobia, Social Anxiety Disorder, Generalized Anxiety Disorder, Panic Disorder
GAD in children requires only 1 associated symptom (vs 3 in adults) from restlessness, fatigue, concentration, irritability, muscle tension, sleep disturbance. Social anxiety in children must occur in peer settings, not only with adults. School refusal is not a DSM diagnosis but a presenting problem frequently driven by separation anxiety, social anxiety, depression, bullying, or learning disorders.
Screening: the SCARED (Screen for Child Anxiety Related Disorders, 41 items, 5 subscales, cutoff ≥25 suggests anxiety disorder) and GAD-7 for adolescents, and the RCADS (Revised Child Anxiety and Depression Scale) are workhorses. Management per the AACAP anxiety practice parameter: CBT with exposure is first-line; SSRIs (fluoxetine, sertraline, escitalopram) are effective; the CAMS trial showed combination CBT + sertraline is superior to either alone.
10 OCD & Related Disorders in Youth Internalizing
OCD affects ~1–3% of children; onset is bimodal with peaks around ages 10 and early 20s. Obsessions are intrusive, unwanted thoughts/urges/images causing distress; compulsions are repetitive behaviors/mental acts performed to reduce distress. Symptoms must consume >1 hour/day or cause marked impairment.
Related disorders include body dysmorphic disorder, hoarding disorder (rare in childhood), trichotillomania (hair-pulling), and excoriation (skin-picking) disorder. Pediatric acute-onset neuropsychiatric syndrome (PANS/PANDAS) presents with abrupt OCD and/or tics, sometimes post-streptococcal.
Severity is measured with the CY-BOCS (Children's Yale-Brown Obsessive Compulsive Scale). Per the AACAP OCD practice parameter: CBT with exposure and response prevention (ERP) is first-line; combination CBT + SSRI is most effective per POTS trial. FDA-approved SSRIs for pediatric OCD: fluoxetine (age 7+), sertraline (age 6+), fluvoxamine (age 8+), clomipramine (age 10+).
11 Trauma, Stress & Attachment Disorders Trauma
PTSD in Children & Adolescents
Exposure to actual/threatened death, serious injury, or sexual violence (directly, witnessed, learned about a loved one, or repeated exposure). Symptoms: intrusion (memories, nightmares, flashbacks, dissociation, distress at cues), avoidance, negative alterations in cognition/mood, and hyperarousal (irritability, recklessness, hypervigilance, startle, concentration, sleep). DSM-5-TR has a separate criteria set for children 6 and younger (fewer symptoms required; trauma may manifest as re-enactment play, generalized fears, and social withdrawal).
Acute Stress Disorder
Same trauma exposure; symptoms last 3 days to 1 month.
Adjustment Disorders
Emotional or behavioral symptoms in response to an identifiable stressor occurring within 3 months, not meeting criteria for another disorder, resolving within 6 months of stressor cessation.
Reactive Attachment Disorder (RAD) & Disinhibited Social Engagement Disorder (DSED)
Both result from pathogenic care (neglect, repeated caregiver changes, institutional rearing). RAD: consistently inhibited, emotionally withdrawn behavior toward caregivers. DSED: culturally inappropriate, overly familiar behavior with unfamiliar adults. Both require a developmental age ≥9 months and onset before age 5.
Screening: UCLA PTSD-RI, TSCC (Trauma Symptom Checklist for Children), and pediatric ACEs screening. Management: Trauma-Focused CBT (TF-CBT) is the most evidence-based treatment. Per the AACAP PTSD practice parameter, SSRIs are second-line; prazosin for trauma-related nightmares.
12 Feeding & Eating Disorders Eating
Eating disorders in youth are high-mortality psychiatric conditions and must be caught early. The pediatric psychiatrist works closely with adolescent medicine, nutrition, and medical stabilization teams.
- Anorexia Nervosa: restriction of intake → significantly low body weight; intense fear of gaining weight; disturbed body image. Subtypes: restricting vs binge-purge.
- Bulimia Nervosa: recurrent binges + inappropriate compensatory behaviors (vomiting, laxatives, fasting, exercise) ≥1×/week for 3 months.
- Binge-Eating Disorder: recurrent binges without compensation, ≥1×/week for 3 months.
- Avoidant/Restrictive Food Intake Disorder (ARFID): avoidance/restriction without body image disturbance (sensory-based, fear of aversive consequences, or lack of interest).
- Pica: eating non-nutritive, non-food substances for ≥1 month.
- Rumination Disorder: repeated regurgitation of food.
- Other Specified Feeding or Eating Disorder (OSFED): including atypical anorexia and purging disorder.
Red flags requiring medical admission: HR <50 bpm (daytime), orthostatic vital changes, hypokalemia, hypophosphatemia, <75% expected body weight, refusal to eat, arrhythmia. Refeeding syndrome (hypophosphatemia, hypomagnesemia, hypokalemia, fluid shifts) is the most dangerous early complication.
Screening: SCOFF questionnaire (Sick, Control, One stone, Fat, Food — score ≥2 positive), EDE-Q, and growth curve review. Management: Family-Based Treatment (FBT / Maudsley) is first-line for adolescent anorexia per the AACAP eating disorders practice parameter. Fluoxetine is evidence-based for bulimia in adolescents. Lisdexamfetamine is FDA-approved for BED in adults (not children).
13 Elimination & Pediatric Sleep-Wake Disorders Other
Enuresis
Repeated involuntary voiding (age ≥5 or developmental equivalent), ≥2×/week for 3 months. Subtypes: nocturnal only (most common), diurnal, both. Rule out UTI, diabetes, structural abnormalities. Treatment: bedwetting alarms first-line; desmopressin (DDAVP) for short-term control.
Encopresis
Repeated passage of feces into inappropriate places, age ≥4, ≥1×/month for 3 months. With or without constipation/overflow incontinence. Treat constipation aggressively (polyethylene glycol), behavioral toileting program, treat comorbid shame.
Pediatric Sleep-Wake Disorders
Include insomnia, delayed sleep-wake phase disorder (common in adolescents), night terrors, nightmares, sleepwalking, restless leg syndrome, and OSA. Document sleep hygiene, bedtime, latency, nocturnal awakenings, screen use, caffeine. Melatonin (0.5–5 mg) is widely used though not FDA approved for pediatric insomnia; clonidine and guanfacine are used off-label, especially in ADHD/autism populations.
14 Gender Dysphoria & Somatic Symptom Disorders Other
Gender Dysphoria in Children & Adolescents
Marked incongruence between experienced/expressed gender and assigned gender, associated with clinically significant distress/impairment, lasting ≥6 months. Children's criteria emphasize strong desire to be another gender and preferences in play, clothing, and peers. Adolescents' criteria emphasize incongruence with primary/secondary sex characteristics. Management involves multidisciplinary gender clinics; the psychiatrist's role is mental health assessment and treatment of comorbidities.
Somatic Symptom Disorder
Somatic symptoms causing distress or disruption, with excessive thoughts/feelings/behaviors about those symptoms for ≥6 months.
Functional Neurological Symptom Disorder (Conversion Disorder)
Altered voluntary motor or sensory function (weakness, tremor, non-epileptic seizures, abnormal movements, sensory loss) with incompatibility between symptoms and recognized neurological disease.
Factitious Disorder Imposed on Another (Medical Child Abuse)
Falsification of physical/psychological signs in another (historically Munchausen by proxy). A form of child abuse — mandatory reporting required.
15 Early-Onset Psychosis & Adolescent Substance Use Psychosis/SUD
Early-Onset Schizophrenia
Schizophrenia with onset before age 18 (childhood-onset: before 13). Criteria are identical to adult schizophrenia: ≥2 of 5 symptoms (delusions, hallucinations, disorganized speech, grossly disorganized/catatonic behavior, negative symptoms) for ≥1 month with ≥6 months total disturbance. Clinical high-risk / prodromal phase involves attenuated positive symptoms, decline in function, and genetic risk. Per the AACAP schizophrenia practice parameter: early antipsychotic treatment (risperidone, aripiprazole, olanzapine, paliperidone, lurasidone are FDA-approved for adolescent schizophrenia) combined with psychosocial rehabilitation.
Adolescent Substance Use
Alcohol, cannabis, nicotine/vaping, opioids, and stimulants are the most common. DSM-5-TR Substance Use Disorder criteria apply: mild (2–3), moderate (4–5), severe (≥6 symptoms). Screen with the CRAFFT (Car, Relax, Alone, Forget, Friends, Trouble; score ≥2 positive). Motivational interviewing, family therapy, and medication-assisted treatment (naltrexone, buprenorphine for opioid use in adolescents ≥16) when indicated.
16 Suicidality, Self-Injury & Safety Assessment Safety
Suicide is a leading cause of death in adolescents. Every child psychiatry note must contain a documented suicide risk assessment. NSSI (non-suicidal self-injury) — cutting, burning, scratching — is distinct from suicidal behavior but is a risk factor for future attempts.
- Wish to be dead: "Have you wished you were dead or wished you could go to sleep and not wake up?"
- Non-specific active SI: "Have you actually had any thoughts of killing yourself?"
- Active SI with method (no plan, no intent): "Have you thought about how you might do this?"
- Active SI with some intent (no specific plan): "Have you had these thoughts and had some intention of acting on them?"
- Active SI with plan and intent: "Have you started to work out or worked out the details of how to kill yourself? Do you intend to carry out this plan?"
Any "yes" to 4 or 5, or recent suicidal behavior, triggers immediate safety intervention.
Ask Suicide-Screening Questions (ASQ): 4-item NIMH-validated tool for ED and clinic use — past wish to be dead, past thoughts of killing oneself, current thoughts, past attempt; any "yes" prompts an acute suicide risk assessment. Per the AACAP suicidal behavior practice parameter, safety planning, means restriction counseling (especially firearms), and linkage to care are core interventions. Lethal means counseling about securing firearms and medications should be documented at every safety assessment.
Every note ends with a safety statement. Standard template: "Patient denies SI, HI, plan, intent, and access to means. No recent NSSI. Contracts safety. Parent reports firearms secured." Document exactly what was asked and what the patient and parent said. Copy-paste safety language is a malpractice risk — chart the actual assessment.
17 Screening Tools & Rating Scales
| Scale | Purpose | Age | Key Cutoff/Notes |
|---|---|---|---|
| ASQ-3 / SWYC | Developmental screen | 1 mo–5.5 y | Used at well-child visits; <cutoff triggers referral |
| M-CHAT-R/F | Autism screen | 16–30 mo | 0–2 low, 3–7 medium, 8–20 high |
| ADOS-2 / ADI-R | Autism diagnostic | Toddler–adult | Gold standard; psychologist-administered |
| Vanderbilt | ADHD + comorbid | 6–12 y | Parent & teacher; 6+ items scored 2 or 3 |
| SNAP-IV | ADHD, ODD | School-age | 26-item short form widely used |
| Conners-3 | ADHD comprehensive | 6–18 y | T-scores by age/sex |
| PHQ-A / PHQ-9-A | Depression | 11–17 y | 0–4 none, 5–9 mild, 10–14 mod, 15–19 mod-sev, 20–27 severe |
| MFQ | Depression | 6–17 y | Long 33-item, short 13-item; cutoff ≥12 short |
| CDI-2 | Depression | 7–17 y | Self-report; T-scores |
| SCARED | Anxiety | 8–18 y | Total ≥25 suggests anxiety disorder |
| RCADS | Anxiety + depression | 8–18 y | Multi-subscale |
| GAD-7 | Generalized anxiety | 12+ | 5/10/15 cutoffs mild/mod/severe |
| CY-BOCS | OCD severity | 6–17 y | 0–40; 16–23 moderate; ≥24 severe |
| UCLA PTSD-RI | PTSD | 7–18 y | DSM-5 version available |
| TSCC | Trauma symptoms | 8–16 y | Multi-scale |
| SCOFF | Eating disorder screen | Adolescents | ≥2 positive |
| EDE-Q(A) | Eating disorder severity | Adolescents | Self-report global score |
| CRAFFT | Substance use | 12–21 y | ≥2 positive → further assessment |
| ASQ (suicide) | Suicide screen | ≥10 y | Any "yes" triggers full assessment |
| C-SSRS | Suicide severity | All ages | 5-level ideation ladder + behavior |
18 Therapeutic Procedures & Interventions
Child psychiatry "procedures" are psychotherapy modalities, system-level interventions, and medication management visits. The scribe must recognize each by name and know its evidence base and target diagnosis.
| Intervention | Description | Target Conditions |
|---|---|---|
| PCIT (Parent-Child Interaction Therapy) | Coached live parent-child play; child-directed and parent-directed phases | ODD, disruptive behavior, ages 2–7 |
| PMT (Parent Management Training) | Structured parent training in behavioral principles | ODD, CD, ADHD |
| Triple P | Positive parenting program (tiered) | Behavior problems |
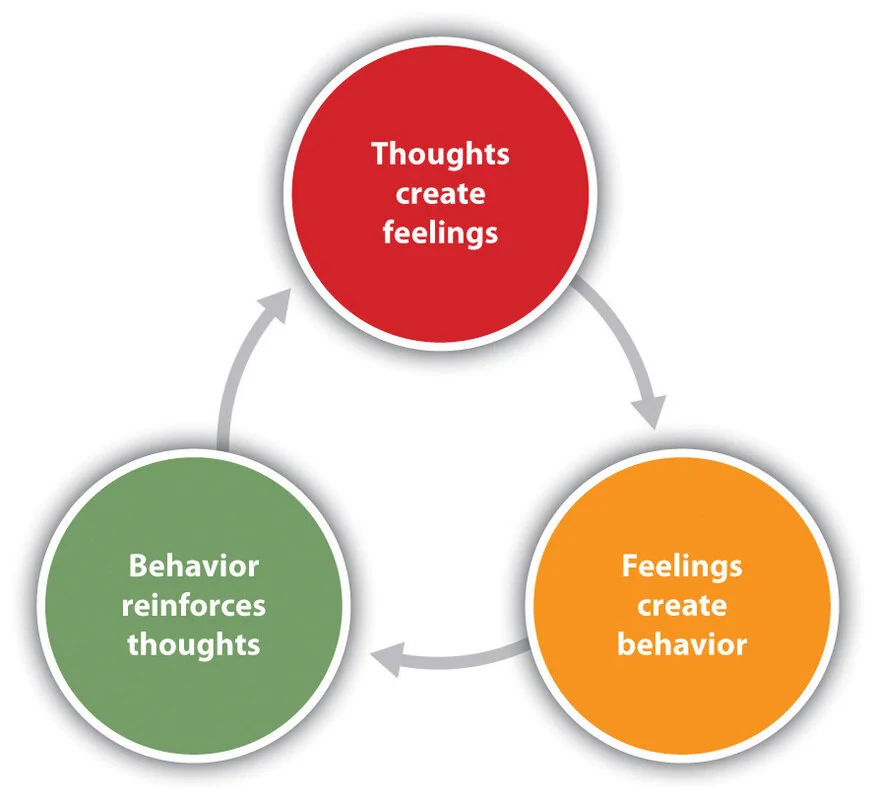
| CBT (Cognitive Behavioral Therapy) | Thought-feeling-behavior model; homework; exposure | Anxiety, depression, OCD |
| ERP (Exposure & Response Prevention) | CBT variant with graded exposure | OCD, phobias |
| TF-CBT (Trauma-Focused CBT) | Manualized 12–16 session trauma protocol | PTSD, trauma exposure |
| DBT-A (Adolescent DBT) | Mindfulness, distress tolerance, emotion regulation, interpersonal effectiveness; multifamily skills group | NSSI, BPD traits, suicidality, DMDD |
| IPT-A | Interpersonal therapy adapted for adolescents | Depression |
| Family-Based Treatment (Maudsley) | Parents take charge of refeeding | Adolescent anorexia |
| Play Therapy | Developmentally appropriate expression through play | Young children with trauma/anxiety |
| ABA | Intensive behavioral intervention for skill building | Autism |
| CBIT | Habit reversal for tics | Tourette/tic disorders |
| IEP / 504 plan | School-based special education supports | All diagnoses affecting learning |
| Medication Management | Titration, monitoring, labs, growth/vitals, side effects | All pharmacologically treated conditions |
| School Consultation | Letter to school, IEP attendance, behavior plan | ADHD, autism, mood, anxiety |
When a clinician says "we'll start TF-CBT" or "refer for PCIT," document the exact modality, the referral target (therapist/agency), and the indication. These acronyms matter for insurance authorization and continuity of care.
19 Pediatric Psychopharmacology
Pediatric psychopharmacology is dose- and weight-sensitive, requires baseline and follow-up monitoring, and carries unique safety concerns (growth suppression, metabolic syndrome, suicidality, extrapyramidal symptoms). Always document weight, height, BMI percentile, and vital signs at medication visits.
Stimulants (First-Line ADHD)
| Generic | Brand | Class | Duration |
|---|---|---|---|
| Methylphenidate IR | Ritalin | MPH | 3–5 h |
| Methylphenidate ER | Concerta, Metadate CD, Ritalin LA | MPH | 8–12 h |
| Dexmethylphenidate | Focalin, Focalin XR | MPH (d-isomer) | 4–12 h |
| Mixed amphetamine salts | Adderall, Adderall XR | AMP | 4–12 h |
| Lisdexamfetamine | Vyvanse | AMP prodrug | 10–13 h |
| Dextroamphetamine | Dexedrine | AMP | 4–6 h |
Common side effects: decreased appetite, weight loss, insomnia, headache, irritability, rebound, tics (rare), mild BP/HR elevation. Screen for cardiac history and family history of sudden death; EKG only if concerning history.
Non-Stimulants
- Atomoxetine (Strattera): SNRI; 1–2 week onset; FDA ADHD age 6+. Warnings: suicidal ideation, hepatotoxicity (rare).
- Guanfacine ER (Intuniv): alpha-2A agonist; FDA ADHD age 6+. Side effects: sedation, dry mouth, hypotension.
- Clonidine ER (Kapvay): alpha-2 agonist; FDA ADHD age 6+; also used for sleep, tics, aggression.
- Viloxazine ER (Qelbree): newer SNRI; FDA ADHD age 6+.
SSRIs (Anxiety, Depression, OCD)
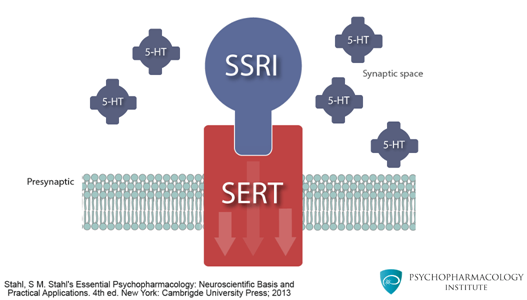
- Fluoxetine (Prozac): FDA MDD age 8+, OCD age 7+; longest half-life, good for non-adherent teens.
- Sertraline (Zoloft): FDA OCD age 6+; widely used in pediatric anxiety off-label.
- Escitalopram (Lexapro): FDA MDD age 12+, GAD age 7+.
- Fluvoxamine (Luvox): FDA OCD age 8+.
All SSRIs carry a black box warning for increased suicidal ideation in patients <25. Start low, go slow, monitor weekly for the first 4 weeks. Screen for activation, agitation, mania (can unmask bipolar disorder).
Antipsychotics
- Risperidone (Risperdal): FDA autism irritability age 5+, bipolar mania age 10+, schizophrenia age 13+. Watch prolactin, weight, metabolic.
- Aripiprazole (Abilify): FDA autism irritability age 6+, bipolar age 10+, schizophrenia age 13+, Tourette age 6+. Better metabolic profile; akathisia common.
- Olanzapine, Quetiapine, Lurasidone, Paliperidone, Asenapine: FDA-approved for pediatric bipolar/schizophrenia.
Baseline and ongoing metabolic monitoring is mandatory: weight, BMI, waist, fasting glucose, A1C, lipids, LFTs, prolactin (risperidone), EKG for QT concerns, AIMS for tardive dyskinesia.
Mood Stabilizers
- Lithium: FDA bipolar age 7+; monitor levels (0.6–1.2 mEq/L), TSH, Cr, Ca, weight.
- Valproate (Depakote): off-label pediatric bipolar; hepatotoxicity, pancreatitis, teratogenicity, thrombocytopenia.
- Lamotrigine (Lamictal): maintenance bipolar; slow titration due to SJS/TEN risk.
Other
- Melatonin: 0.5–5 mg for sleep onset.
- Prazosin: off-label for PTSD nightmares.
- Benzodiazepines: used sparingly in pediatrics (paradoxical disinhibition, dependence, cognitive effects); short-term, acute distress only.
- Naltrexone: adolescent alcohol/opioid use disorder (≥18 typically; off-label younger).
- Buprenorphine: FDA age 16+ for OUD.
20 Classification Systems & Developmental Benchmarks
DSM-5-TR Diagnostic Categories Relevant to Youth
- Neurodevelopmental Disorders (ADHD, ASD, ID, SLD, communication, motor/tic)
- Schizophrenia Spectrum and Other Psychotic Disorders
- Bipolar and Related Disorders
- Depressive Disorders (incl. DMDD)
- Anxiety Disorders (incl. separation anxiety, selective mutism)
- OCD and Related Disorders
- Trauma- and Stressor-Related Disorders (RAD, DSED, PTSD, acute stress, adjustment)
- Feeding and Eating Disorders
- Elimination Disorders
- Sleep-Wake Disorders
- Disruptive, Impulse-Control, and Conduct Disorders (ODD, CD, IED)
- Substance-Related and Addictive Disorders
- Gender Dysphoria
- Somatic Symptom and Related Disorders
Growth Chart Percentiles to Know
| Percentile | Meaning | Clinical Action |
|---|---|---|
| < 3rd | Underweight/short stature | Growth concern; ED workup; stimulant reassessment |
| 3rd–15th | Low end of normal | Monitor trajectory |
| 15th–85th | Normal | Continue routine monitoring |
| 85th–95th | Overweight | Lifestyle counseling; antipsychotic metabolic review |
| > 95th | Obesity | Metabolic workup; medication choice reconsideration |
A drop of >2 percentile bands on a stimulant warrants dose reduction, medication holiday, or switch.
ADHD Severity (DSM-5-TR)
| Severity | Criteria |
|---|---|
| Mild | Few symptoms beyond diagnostic threshold; minor impairment |
| Moderate | Symptoms or impairment between mild and severe |
| Severe | Many symptoms beyond threshold; severe impairment |
Tanner Staging (Pubertal Development)
Tanner 1 (prepubertal) through Tanner 5 (adult) — referenced when pubertal blockers, hormonal therapy, or eating disorder presentation are discussed.
21 Mental Status Exam in Children
The pediatric MSE replaces the physical exam as the primary objective assessment. It must be developmentally calibrated — you do not expect the same organized, goal-directed speech from a 4-year-old as from a 16-year-old.
Appearance: age-appropriate, grooming, dress, any dysmorphic features, growth parameters.
Behavior/Attitude: cooperative, engaged, avoidant, hyperactive, aggressive, shy; interaction with parent; separation tolerance; play behavior.
Speech: rate, rhythm, volume, articulation, fluency; age-appropriate vocabulary and grammar.
Language: receptive (follows commands) and expressive (spontaneous, prompted).
Motor: activity level, coordination, tics, stereotypies, mannerisms.
Mood: patient's own word ("I feel sad/mad/okay"); for young children, use picture scales.
Affect: observed emotion — range (full, restricted, flat), appropriateness, congruence, lability.
Thought Process: goal-directed, circumstantial, tangential, loose; developmentally calibrated.
Thought Content: preoccupations, obsessions, delusions, paranoia, suicidality, homicidality, hallucinations (visual common in young children; cross-check for developmental fantasy).
Perceptions: hallucinations — type, command, content.
Cognition: alert, oriented (age-appropriate), attention (digit span, serial tasks), memory, fund of knowledge.
Insight/Judgment: limited by developmental stage; compare to age peers.
Interaction with Parent/Caregiver: attachment behavior, eye contact, responsiveness, boundary testing.
22 Abbreviations Master List
Diagnoses
Assessments & Scales
Interventions & Workflow
Medications & Labs
23 Sample HPI Templates
These templates show the kind of documentation expected in a child & adolescent psychiatry clinic note. Use them as frameworks to internalize the rhythm of a good pediatric psychiatric HPI.
"Ethan is an 8y 3m old male brought by his mother for evaluation of inattention and hyperactivity. Mother reports concerns since kindergarten, worsening in 2nd grade: 'he can't sit still, forgets assignments daily, loses his homework, interrupts constantly, and needs 20 reminders to finish a task.' Teacher Vanderbilt completed last week: 7/9 inattentive and 6/9 hyperactive/impulsive items scored 2 or 3, with performance impairment in reading and math. Parent Vanderbilt: 8/9 inattentive, 7/9 hyperactive. Symptoms present before age 12, in both school and home settings, with academic and social impairment. Denies depressed/irritable mood, trauma, sleep disturbance, tics, or hallucinations. Developmental milestones on time. Birth and medical history unremarkable. Family history notable for father with ADHD. No prior psychiatric treatment. Sleep 9 h/night. No tics. Height 50th %ile, weight 45th %ile. Meets DSM-5-TR criteria for ADHD, combined presentation, moderate."
"Mia is a 2y 8m old female referred by her pediatrician after a positive M-CHAT-R screen (score 9, high risk) at her 24-month well-child visit. Parents report limited eye contact since infancy, only 5 spoken words, no pointing to share interest, no pretend play, and distress with changes in routine. She lines up toys, flaps her hands when excited, and is highly sensitive to loud sounds and clothing tags. Social-emotional: does not respond to name consistently, prefers solo play, minimal reciprocal interaction. No regression. Pregnancy and birth uncomplicated. Gross motor on time. Hearing tested and normal. Family history: maternal cousin with ASD. Referred for ADOS-2 through developmental psychology, audiology re-evaluation, early intervention enrollment, and speech-language therapy. Genetic testing (chromosomal microarray, Fragile X) ordered."
"Jordan is a 15-year-old female brought by mother for worsening depression and passive suicidal ideation over 6 weeks. She reports depressed mood daily, anhedonia (quit soccer, no longer sees friends), initial and terminal insomnia, decreased appetite with 7-lb weight loss, fatigue, poor concentration with falling grades, and feelings of worthlessness. PHQ-A score 18 (moderately severe). She endorses passive SI ('wishing I wouldn't wake up') daily for 2 weeks, denies active SI, plan, intent, or NSSI, though mother reports finding a razor in her room. Denies substance use (CRAFFT 0). Trauma history: parental divorce last year, recent peer conflict at school. No prior psychiatric treatment. Family history: maternal MDD, maternal grandmother completed suicide. Firearms not in home; mother agrees to lock away medications. C-SSRS ideation level 1–2, no behavior. Safety plan reviewed with patient and mother; start fluoxetine 10 mg daily with weekly follow-up; referral for CBT; mother contacted school counselor."
"Lucas is a 10y 2m old male with a 3-week history of school refusal. Mother reports that since returning from winter break, Lucas complains of stomachaches every weekday morning and has missed 12 days of school. Symptoms resolve once he stays home. Denies medical cause (pediatrician workup negative). On detailed history, he reports fear of being called on in class, worry that something 'bad will happen to mom' while he is away, and recent teasing by a classmate about his glasses. SCARED score 38, elevated on separation anxiety, generalized anxiety, and social anxiety subscales. Sleep, appetite preserved. No depression. No SI. School attendance was 100% in previous years. Academically above grade level. Plan: CBT with graded exposure and gradual school reentry; coordinate with school counselor for 504; parents to resist reinforcement of avoidance; consider SSRI if behavioral plan insufficient at 4 weeks."
"Ava is a 14-year-old female brought by her parents for evaluation of 6 months of restrictive eating and weight loss. Weight has decreased from 52 kg (50th %ile BMI) to 41 kg (<3rd %ile BMI) over 6 months. She reports counting calories (~700/day), excessive exercise (2+ hours daily), amenorrhea ×4 months, intense fear of weight gain, and body image disturbance (describes self as 'fat' despite visible emaciation). Denies bingeing or purging. SCOFF 4/5. Vitals: HR 46, BP 92/58, orthostatic positive. Labs pending: CMP, phosphorus, magnesium, TSH, EKG. Denies SI. No prior psychiatric treatment. Family history: maternal aunt with anorexia. Meets DSM-5-TR criteria for anorexia nervosa, restricting type. Medically unstable (bradycardia, orthostatic) — referral to adolescent medicine for admission and refeeding; Family-Based Treatment to follow; safety plan reviewed."
"Caleb is a 6y 5m old male brought by both parents for escalating oppositional and aggressive behavior over 9 months. Parents report daily tantrums lasting 30–60 minutes triggered by transitions and limit-setting, verbal defiance ('no,' 'you can't make me'), hitting younger sibling 3–4 times/week, and spiteful behavior (purposely breaks sibling's toys). Behaviors occur primarily at home; kindergarten teacher reports mild defiance but no aggression. No cruelty to animals, fire-setting, or stealing. Parent Vanderbilt negative for ADHD (3/9 inattentive, 2/9 hyperactive). No mood symptoms. No trauma history. Sleep good. No medical issues. Meets DSM-5-TR criteria for oppositional defiant disorder, mild. Plan: refer family for Parent-Child Interaction Therapy (PCIT); psychoeducation on behavioral principles provided; follow-up in 6 weeks to reassess."
The best child psychiatry scribes hold two frameworks simultaneously: the DSM-5-TR diagnostic system and the normal developmental timeline. When a parent says "he isn't talking at two," you already know that is a language delay and anticipate a speech referral. When the attending says "Vanderbilt positive, combined presentation, impairment across settings," you are already structuring the assessment with DSM criteria in mind. You recognize that a 4-year-old's flat affect during a stranger's interview is not the same as a 14-year-old's flat affect during an interview about her mood.
Always capture the informant ("per mother," "per teacher form," "per patient"). Always document the safety assessment in every note — not with boilerplate but with what was actually asked and said. Always track weight, height, BMI, and BP on medication-managed patients. Learn the rating scale cutoffs cold so you can chart "PHQ-A 18, moderately severe" without looking it up.
Welcome to child & adolescent psychiatry. These are the highest-stakes, highest-reward conversations in medicine — catching a problem early can change a trajectory for a lifetime.
24 References & Sources
Clinical Practice Guidelines
AACAP Practice Parameter for the Assessment and Treatment of ADHD. JAACAP. 2007.
USPSTF. Screening for Depression and Suicide Risk in Children and Adolescents. JAMA. 2022.
Landmark Clinical Trials
CAMS: Child/Adolescent Anxiety Multimodal Study — CBT, sertraline, or combination. NEJM. 2008.
POTS: Pediatric OCD Treatment Study — CBT, sertraline, and their combination. JAMA. 2004.
MTA: Multimodal Treatment Study of ADHD. Arch Gen Psychiatry. 1999.
Diagram & Figure Sources
Figure 1: The Brain. OpenStax Anatomy & Physiology. CC BY 3.0.
Figure 2: CDC Pediatric Growth Chart. CDC/NCHS. Public domain.
Figure 3: M-CHAT-R/F Screening Instrument. Robins DL et al. Public domain/author release.