Critical Care / ICU
Every diagnosis, procedure, ventilator mode, vasoactive drug, and documentation framework you need to survive week one in the ICU and beyond.
All diagrams on this page are sourced from published educational or institutional materials rather than AI generation. Each figure caption links to the original source, and the full diagram and guideline citations are collected in the references section at the bottom.
01 ICU Principles & Organ-System Foundations
The intensive care unit is where physiology that is normally invisible becomes the story of the chart. Every ICU patient is defined by which of their organ systems is failing and which are at risk of failing next. A competent ICU scribe learns to think in systems — neurologic, cardiovascular, pulmonary, renal, hepatic/GI, hematologic/ID, endocrine — because this is exactly how the critical care team rounds, dictates, and writes progress notes.
The Oxygen Delivery Equation
Nearly every ICU decision comes back to oxygen delivery. DO2 (oxygen delivery) = cardiac output × arterial oxygen content = (HR × SV) × (1.34 × Hgb × SaO2 + 0.003 × PaO2). When the ICU team adjusts a ventilator, gives a transfusion, starts norepinephrine, or begins dobutamine, the underlying question is always: is this patient delivering enough oxygen to their tissues? Lactate, ScvO2 (central venous oxygen saturation), mixed venous saturation, and capillary refill time are the surrogate markers the team uses to answer that question.
Cardiopulmonary Anatomy Refresher
Deoxygenated blood returns through the SVC and IVC to the right atrium, crosses the tricuspid valve into the right ventricle, and is pumped through the pulmonary valve into the pulmonary arteries for gas exchange at the alveolar-capillary membrane. Oxygenated blood returns through pulmonary veins to the left atrium, crosses the mitral valve into the left ventricle, and is ejected through the aortic valve to the systemic circulation. This loop matters because ICU shock states almost always localize to one of four places: the pump (cardiogenic), the tank (hypovolemia), the pipes (distributive), or a physical obstruction (tamponade, tension pneumothorax, massive PE).
Pulmonary Physiology for Scribes
Gas exchange occurs at the alveolus. PaO2 is the partial pressure of oxygen dissolved in arterial blood (normal 80–100 mmHg on room air). SaO2 is the percentage of hemoglobin saturated with oxygen (normal > 95%). PaCO2 reflects alveolar ventilation (normal 35–45 mmHg). The P/F ratio (PaO2 divided by FiO2) is the single most important number in ARDS documentation — a patient on 100% oxygen with a PaO2 of 80 has a P/F of 80, which is severe ARDS.
You will hear the team say "P/F of 150" or "she has a pressure-support trial going" — learn to translate these immediately into chart language. Document the FiO2, PEEP, and most recent ABG at the start of every progress note. The intensivist will thank you.
Renal, Hepatic & Hematologic Foundations
Kidneys regulate volume, electrolytes, and acid-base; the liver clears drugs and synthesizes clotting factors; bone marrow produces the cells that fight infection and carry oxygen. ICU patients frequently have all three under stress simultaneously — this is what multi-organ dysfunction syndrome (MODS) looks like in real time.
Acid-Base in the ICU
ABG interpretation is a daily scribe task. The four primary disorders are metabolic acidosis (low HCO3, often with an anion gap from lactate, ketones, or uremia), metabolic alkalosis (high HCO3, from vomiting, NG suction, diuretics), respiratory acidosis (high PaCO2, from hypoventilation), and respiratory alkalosis (low PaCO2, from hyperventilation, sepsis, PE). Always calculate the anion gap (Na − Cl − HCO3, normal 8–12) and check for mixed disorders using Winter's formula (expected PaCO2 = 1.5 × HCO3 + 8 ± 2). Scribes should document the primary disorder and any compensation when the attending interprets an ABG at the bedside.
Fluids & Resuscitation
Crystalloids (normal saline, lactated Ringer's, Plasma-Lyte) are first-line in most resuscitation scenarios. The SMART trial suggested balanced crystalloids (LR, Plasma-Lyte) reduce major adverse kidney events compared with saline. Albumin (5% or 25%) is used in specific scenarios: large-volume paracentesis, hepatorenal syndrome, SBP. Blood products are reserved for active bleeding or Hgb < 7 in most ICU patients.
02 Scribe Documentation Framework (ICU Note Structure)
ICU progress notes differ from outpatient SOAP notes in one critical way: they are written by system, not by problem. A typical ICU attending will round at the bedside and dictate a note that reads: "Neuro — intubated, sedated on propofol, RASS −2, CAM-ICU negative. CV — on norepinephrine 0.15, MAP > 65, lactate down to 2.1. Pulm — AC/VC, TV 400, PEEP 10, FiO2 50%, P/F 180. Renal — oliguric, Cr up to 2.3, started CRRT. GI — NPO, tube feeds held. Heme/ID — WBC 18, on vanc/zosyn day 3. Endo — on insulin drip." Your job as a scribe is to capture this rapid systems-based dictation accurately.
Neuro: Mental status, sedation (drug, dose, RASS target and actual), delirium screen (CAM-ICU), pain (CPOT), seizure activity, any focal deficits, GCS if applicable.
CV: Hemodynamics (BP, HR, MAP, CVP if available), rhythm, pressors/inotropes with doses, lactate trend, fluid balance (I/O for prior 24 h), weight change, echo findings if new.
Pulm: Ventilator mode and settings (FiO2, PEEP, TV, RR, plateau pressure, peak pressure), most recent ABG, P/F ratio, secretions, chest X-ray findings, plan for weaning/extubation.
Renal/FEN: Creatinine trend, UOP (mL/kg/hr), electrolytes (K, Mg, Phos), acid-base, dialysis/CRRT status, IVF type and rate, nutrition (TPN vs enteral).
GI/Hepatic: Diet, tube feeds (rate, residuals), LFTs, bilirubin, ascites, last BM, stress ulcer prophylaxis.
Heme: Hgb/Hct, platelets, INR/PTT, transfusion history, DVT prophylaxis.
ID: Tmax, WBC, cultures (blood, urine, sputum, CSF) with days pending or results, current antibiotics with day number, source control, lines and duration.
Endo: Glucose control (insulin drip vs sliding scale), cortisol if applicable, TFTs if concern.
Lines/Tubes/Drains: Endotracheal tube (size, depth at lip), central line (site, day), arterial line, Foley, NG/OG, chest tubes, surgical drains.
The plan is written as a bulleted list of active problems. Every ICU patient has a "problem list" at the top of the note: "1) Septic shock from pneumonia 2) ARDS 3) AKI 4) DM 5) Atrial fibrillation." Each problem gets a brief plan. This is sometimes called the FASTHUG BID mnemonic: Feeding, Analgesia, Sedation, Thromboprophylaxis, Head of bed elevated, Ulcer prophylaxis, Glucose control, Bowel regimen, Indwelling catheter review, De-escalation of antibiotics.
Always pre-populate vitals, vent settings, drip rates, and most recent labs before rounds start. When the attending walks into the room, your cursor should already be in the A&P box. This is the single biggest efficiency gain you can make as an ICU scribe.
03 Shock — Overview & Classification
Shock is a state of inadequate tissue oxygen delivery leading to cellular dysfunction and, if untreated, death. Shock is not defined by a specific blood pressure — a patient with a MAP of 70 who is oliguric, obtunded, and lactic is in shock. Clinically, ICU teams classify shock into four physiologic categories.
| Type | Mechanism | CO | SVR | CVP/PCWP | Examples |
|---|---|---|---|---|---|
| Hypovolemic | Loss of intravascular volume | ↓ | ↑ | ↓ | Hemorrhage, severe dehydration, burns |
| Cardiogenic | Pump failure | ↓ | ↑ | ↑ | MI, acute HF, myocarditis, valvular |
| Obstructive | Mechanical obstruction to flow | ↓ | ↑ | ↑ | Tamponade, tension PTX, massive PE |
| Distributive | Loss of vascular tone | ↑ or normal | ↓ | ↓ or normal | Sepsis, anaphylaxis, neurogenic, adrenal |
The most useful single bedside metric for shock severity is the Shock Index = HR/SBP. A shock index > 0.9 suggests significant hemodynamic compromise; > 1.4 portends high mortality. Add this to every unstable patient's note.
Cool, mottled extremities; delayed capillary refill > 3 seconds; altered mental status; oliguria (< 0.5 mL/kg/hr); lactate > 2 mmol/L and rising; narrowing pulse pressure; base deficit on ABG. Any of these should trigger a rapid bedside assessment for cause.
04 Sepsis & Septic Shock INFECTIOUS
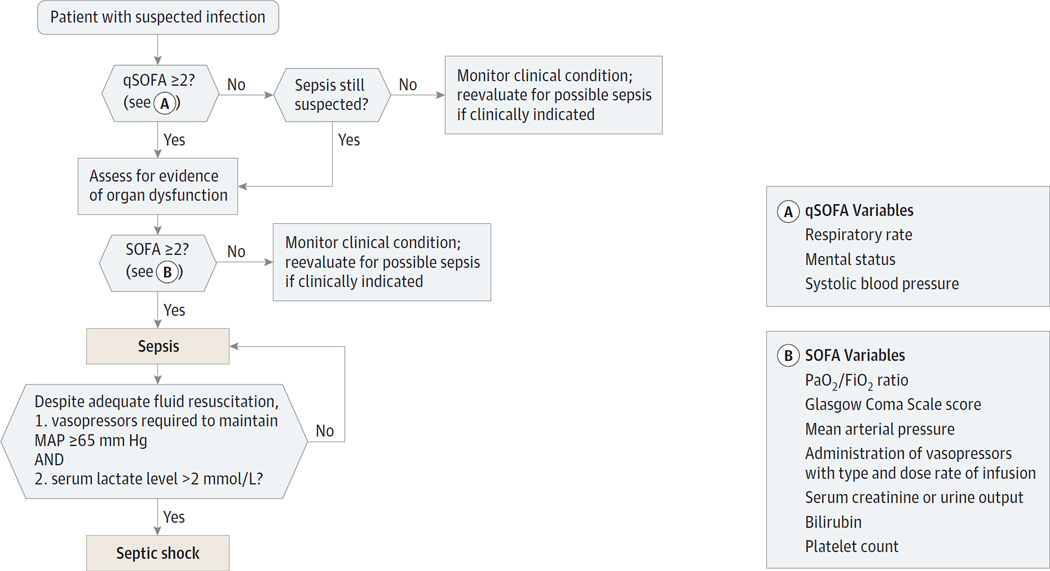
Sepsis (Sepsis-3 definition) is life-threatening organ dysfunction caused by a dysregulated host response to infection, identified clinically by a rise in the SOFA score of 2 or more points. Septic shock is sepsis plus persistent hypotension requiring vasopressors to maintain MAP ≥ 65 mmHg AND a lactate > 2 mmol/L despite adequate volume resuscitation. Hospital mortality for septic shock remains 30–40%.
Pathophysiology
A pathogen triggers a cytokine storm (TNF-α, IL-1, IL-6). The endothelium becomes leaky, nitric oxide is overproduced, vascular tone collapses (distributive shock), microcirculation is compromised, and cells cannot extract oxygen even when it is delivered. The result is high cardiac output with low SVR, warm peripheries early ("warm shock") progressing to cold, mottled peripheries late ("cold shock") as cardiac function fails.
Clinical Presentation
Fever or hypothermia, tachycardia, tachypnea, altered mental status, oliguria, hypotension, and often a identifiable source: pneumonia (most common), urinary tract, intra-abdominal, skin/soft tissue, meningitis, or line infection. Petechiae and purpura fulminans should raise concern for meningococcemia or DIC.
Diagnostic Workup
Blood cultures × 2 before antibiotics (if no delay), lactate, CBC with differential, BMP, LFTs, coags, urinalysis and urine culture, imaging of suspected source (CXR, CT abd/pelvis), sputum culture if intubated, lumbar puncture if CNS source suspected. Procalcitonin is sometimes trended.
qSOFA (bedside screen): RR ≥ 22, altered mental status (GCS < 15), SBP ≤ 100. Score 2+ = high risk.
SOFA (ICU): Scores 0–4 in each of 6 systems: Respiratory (PaO2/FiO2), Coagulation (platelets), Liver (bilirubin), Cardiovascular (MAP / pressor dose), CNS (GCS), Renal (creatinine / UOP). ΔSOFA ≥ 2 defines sepsis.
Management — The Sepsis Bundle
The Surviving Sepsis Campaign 2021 guidelines define the "Hour-1 Bundle": measure lactate, obtain blood cultures, administer broad-spectrum antibiotics, begin 30 mL/kg crystalloid for hypotension or lactate ≥ 4, and apply vasopressors if hypotension persists after fluids (target MAP ≥ 65). Norepinephrine is the first-line vasopressor. Add vasopressin 0.03 U/min as a second agent. Consider hydrocortisone 200 mg/day in refractory septic shock.
Community-acquired: ceftriaxone + azithromycin (pneumonia), or piperacillin-tazobactam for broader coverage. Hospital-acquired/immunocompromised: vancomycin + cefepime or meropenem + consideration of antifungal. Suspected MRSA: add vancomycin or linezolid. Source and local antibiogram drive selection. IDSA HAP/VAP guidelines are the reference for hospital-acquired pneumonia coverage.
When the team says "start the sepsis bundle," document the time each bundle element was completed: time of lactate draw, time cultures sent, time antibiotics infused, volume of fluids given. Sepsis bundle compliance is a quality metric tracked by hospitals — your timestamps matter.
05 Cardiogenic Shock & Acute Heart Failure CARDIAC
Cardiogenic shock is low cardiac output shock from pump failure. SBP < 90 for > 30 min or requiring pressors to maintain, cardiac index < 2.2 L/min/m², and elevated filling pressures (PCWP > 15). The most common cause is acute MI with LV dysfunction; others include decompensated HFrEF, myocarditis, acute valvular pathology (papillary muscle rupture, flail leaflet), and post-cardiotomy.
Clinical Presentation & Hemodynamics
Cool extremities, diaphoresis, altered mental status, oliguria, elevated JVD, pulmonary edema/rales, S3 gallop, hypotension with narrow pulse pressure. The classic Forrester/Killip patterns identify "cold and wet" patients.
| Class | Findings | Mortality |
|---|---|---|
| I | No clinical signs of HF | ~6% |
| II | Rales < 50% lung fields, S3, elevated JVP | ~17% |
| III | Frank pulmonary edema, rales > 50% | ~38% |
| IV | Cardiogenic shock (SBP < 90, hypoperfusion) | ~67% |
Management
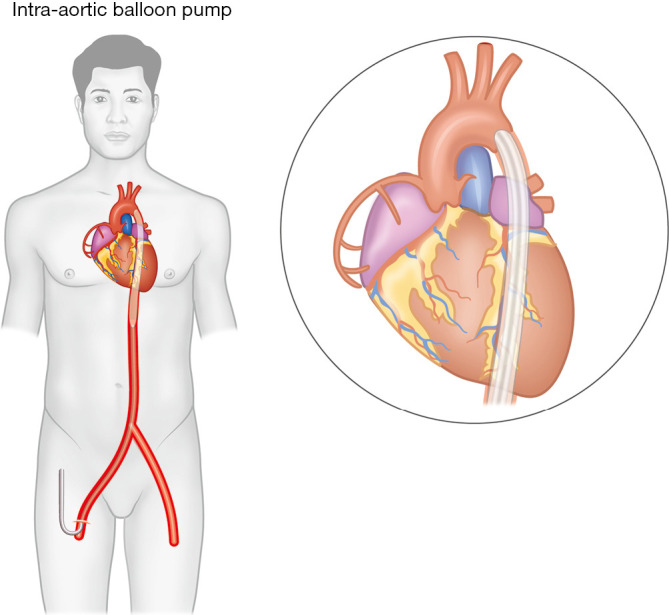
Emergent revascularization for MI-related shock (2021 ACC/AHA coronary revascularization guideline). Hemodynamic support with dobutamine (inotrope, β1 agonist), milrinone (PDE-3 inhibitor, inodilator), or norepinephrine for BP. Mechanical circulatory support escalates from IABP (intra-aortic balloon pump) to Impella (axial-flow LV assist) to VA-ECMO in refractory cases. Diuresis with IV furosemide for volume overload once perfusion stabilized. Avoid beta-blockers acutely.
06 Hypovolemic, Obstructive & Distributive Shock CIRCULATORY
Hypovolemic Shock
Volume loss — hemorrhage (trauma, GI bleed, ruptured AAA, ectopic pregnancy, post-partum) or fluid losses (severe diarrhea, DKA, burns). Classic physiology: low CVP, low CO, high SVR, narrow pulse pressure, orthostatic vitals, cool peripheries. Management is volume: crystalloid for non-hemorrhagic losses, massive transfusion protocol (MTP, 1:1:1 ratio of pRBC:FFP:platelets) for hemorrhagic shock, source control, permissive hypotension in trauma until definitive bleeding control.
Obstructive Shock
Mechanical barrier to forward flow. The big three:
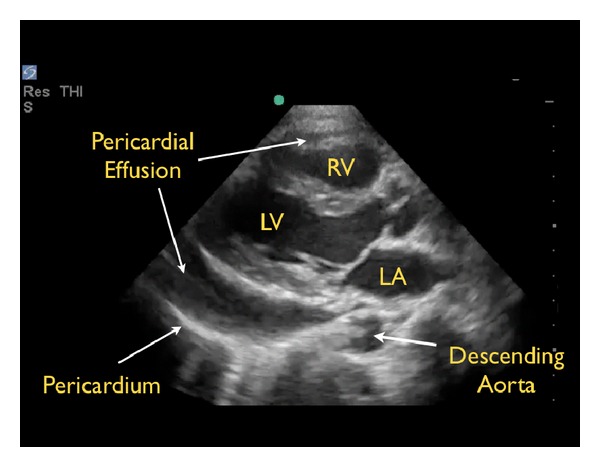
- Cardiac tamponade — pericardial effusion compressing the heart. Beck's triad: hypotension, muffled heart sounds, elevated JVD. Pulsus paradoxus > 10 mmHg. Bedside echo shows diastolic RV collapse. Treat with emergent pericardiocentesis.
- Tension pneumothorax — absent breath sounds unilaterally, tracheal deviation away, hypotension, JVD, hyperresonance to percussion. Do not wait for CXR. Needle decompression (2nd intercostal, midclavicular) followed by chest tube.
- Massive PE — sudden hypoxia, hypotension, RV strain on ECG (S1Q3T3), elevated troponin/BNP, RV dilation on echo. Systemic thrombolytics or catheter-directed therapy.
Distributive Shock (Non-Septic)
Anaphylaxis: IgE-mediated, with hypotension, urticaria, bronchospasm, angioedema after exposure to allergen. Treat with IM epinephrine 0.3–0.5 mg (first and most important), IV fluids, H1/H2 blockers, steroids, bronchodilators. Neurogenic shock: spinal cord injury above T6, loss of sympathetic outflow → bradycardia + hypotension. Treat with fluids, phenylephrine, atropine for bradycardia. Adrenal crisis: cortisol deficiency, refractory shock — treat with hydrocortisone 100 mg IV.
07 Acute Respiratory Failure & ARDS PULMONARY
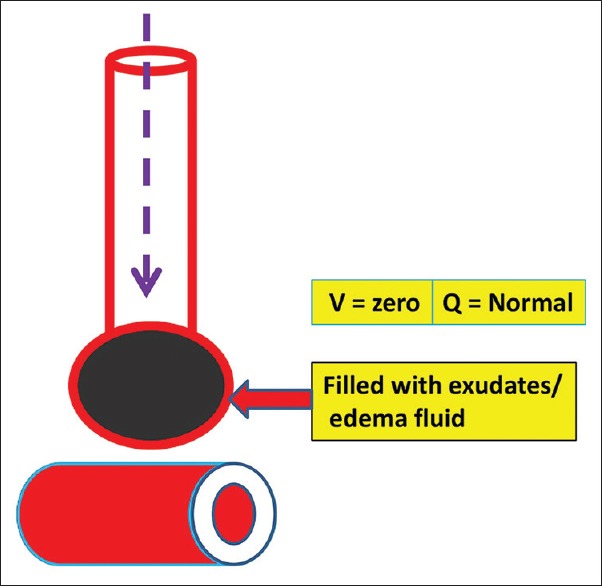
Acute respiratory failure is classified as Type 1 (hypoxemic, PaO2 < 60) or Type 2 (hypercapnic, PaCO2 > 50 with acidosis). Type 1 reflects a problem with oxygenation (V/Q mismatch, shunt, diffusion impairment). Type 2 reflects ventilation failure (airway obstruction, respiratory muscle weakness, depressed drive).
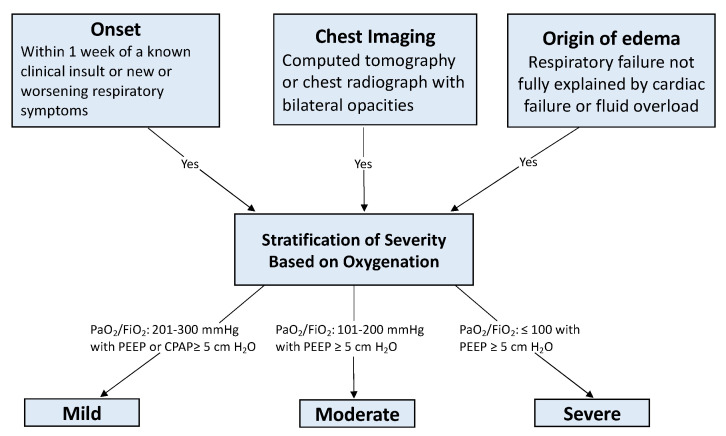
ARDS — Berlin Definition
Acute Respiratory Distress Syndrome (ARDS) is non-cardiogenic pulmonary edema from diffuse alveolar injury. The Berlin Definition requires: onset within 1 week of a known insult, bilateral opacities on imaging, respiratory failure not fully explained by cardiac failure or fluid overload, and impaired oxygenation graded by P/F ratio.
| Severity | P/F Ratio | Mortality |
|---|---|---|
| Mild | 201–300 | ~27% |
| Moderate | 101–200 | ~32% |
| Severe | ≤ 100 | ~45% |
Management — Lung Protective Ventilation
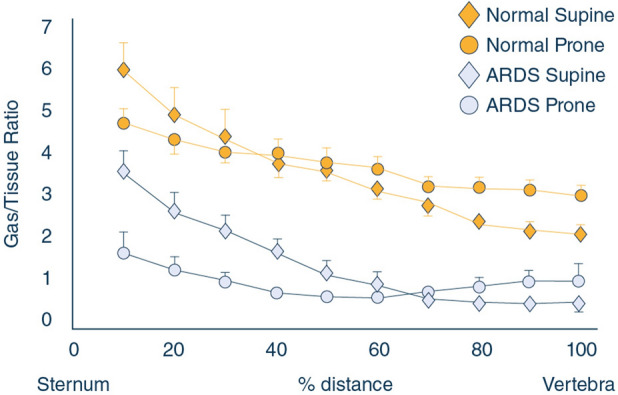
The landmark ARDSNet ARMA trial established low tidal volume ventilation (6 mL/kg predicted body weight, plateau pressure < 30 cmH2O) as the standard of care. Higher PEEP, conservative fluid strategy, and deep sedation are added as severity worsens. For severe ARDS with P/F < 150, PROSEVA trial demonstrated mortality benefit with prone positioning > 16 hours/day. Neuromuscular blockade (cisatracurium) can be used in the first 48 hours. Refractory hypoxemia escalates to inhaled pulmonary vasodilators (nitric oxide, epoprostenol) or VV-ECMO.
Always document the FiO2 and PEEP when recording a P/F ratio. "P/F 120" means nothing without knowing the ventilator settings that produced it. The correct chart entry is "PaO2 72 on FiO2 0.6, PEEP 12, P/F 120, moderate ARDS."
08 Mechanical Ventilation — Modes, Settings & Weaning PULMONARY
The ventilator is the most important piece of equipment in the ICU. Scribes must learn to read and document ventilator settings with the same fluency as vital signs.
Core Ventilator Modes
| Mode | What It Delivers | When Used |
|---|---|---|
| AC/VC (Assist Control, Volume Control) | Fixed tidal volume with every breath | Default for sick/sedated patients, ARDS |
| AC/PC (Assist Control, Pressure Control) | Fixed inspiratory pressure, variable volume | Severe ARDS, high peak pressures |
| SIMV | Set mandatory breaths + patient-triggered | Weaning (historically; now less used) |
| PSV / PS | Patient-triggered with pressure support | Weaning / spontaneous breathing trials |
| CPAP | Continuous positive pressure, no mandatory breaths | Weaning, OSA, NIV |
| APRV | Airway pressure release ventilation | Refractory hypoxemia, open lung |
FiO2: Inspired O2 fraction (0.21–1.0). PEEP: Positive end-expiratory pressure (cmH2O). TV (Vt): Tidal volume (mL, or mL/kg PBW). RR: Set rate and total (patient + vent) rate. Pplat: Plateau pressure (target < 30). Ppeak: Peak inspiratory pressure. I:E ratio: Inspiratory to expiratory time. Minute ventilation (Ve): TV × RR.
Troubleshooting: High peak + normal plateau = airway resistance issue (kink, mucus, bronchospasm). High peak + high plateau = compliance issue (ARDS progression, PTX, mainstem intubation).
Weaning & Extubation
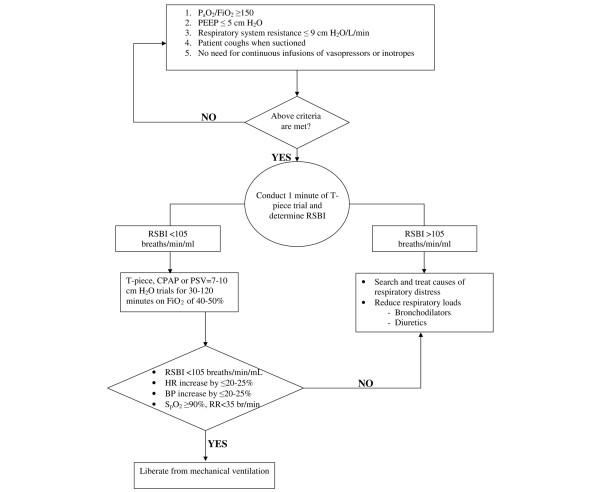
Daily spontaneous awakening trial (SAT) + spontaneous breathing trial (SBT) is the standard. SBT = 30–120 min on PS 5/PEEP 5 or T-piece. RSBI (rapid shallow breathing index) = RR/TV(L); < 105 predicts successful extubation. Also required: adequate oxygenation (FiO2 ≤ 0.4, PEEP ≤ 5), hemodynamic stability, cough/gag, manageable secretions, appropriate mental status.
Ventilator-Associated Pneumonia (VAP)
New infiltrate + fever + leukocytosis + purulent secretions > 48 h after intubation. Prevention bundle: head of bed 30°, oral care with chlorhexidine, daily sedation interruption, DVT/stress ulcer prophylaxis, subglottic suction. Treatment per IDSA/ATS HAP/VAP guidelines: vancomycin + antipseudomonal beta-lactam (cefepime, pip-tazo, or meropenem).
09 Status Asthmaticus & COPD Exacerbation PULMONARY
Status asthmaticus is a severe asthma exacerbation unresponsive to initial bronchodilators, progressing toward respiratory failure. Clinical features: severe dyspnea, accessory muscle use, silent chest (ominous), tachycardia, pulsus paradoxus, altered mental status. ABG may show normalizing PaCO2 — a bad sign indicating respiratory muscle fatigue.
Management: continuous nebulized albuterol/ipratropium, IV methylprednisolone (80–125 mg), magnesium sulfate 2 g IV, epinephrine IM if no IV access, consider heliox. Intubation is high-risk due to auto-PEEP and breath-stacking — use ketamine (bronchodilator) for induction, low RR (6–10), long expiratory time, permissive hypercapnia, and tolerate high plateau pressures to avoid barotrauma.
COPD exacerbation with hypercapnic respiratory failure is a classic NIV (non-invasive ventilation, BiPAP) indication. BiPAP reduces intubation rates and mortality. Settings typically start at IPAP 10 / EPAP 5 and titrate. Steroids (prednisone 40 mg × 5 days) and antibiotics (azithromycin, doxycycline) are standard. If NIV fails (worsening acidosis, mental status), intubate.
10 Cardiac Arrest, Post-Arrest Care & TTM CARDIAC
Cardiac arrest care follows the AHA 2020 ACLS guidelines. Shockable rhythms (VF/pulseless VT) are treated with immediate defibrillation, high-quality CPR (100–120/min, depth ≥ 2 inches), epinephrine 1 mg every 3–5 min, amiodarone 300 mg after 3 shocks. Non-shockable rhythms (PEA/asystole) get CPR + epinephrine + reversible cause search (H's and T's).
H's: Hypoxia, Hypovolemia, Hydrogen ion (acidosis), Hypo/hyperkalemia, Hypothermia, Hypoglycemia.
T's: Toxins, Tamponade, Tension pneumothorax, Thrombosis (pulmonary), Thrombosis (coronary), Trauma.
Post-Arrest Care
After ROSC: airway/ventilation (avoid hyperoxia, target SpO2 92–98%, normocapnia), hemodynamic support (MAP ≥ 65, often requires pressors), 12-lead ECG (STEMI → cath), and targeted temperature management (TTM). Current evidence supports targeted normothermia (36°C) or mild hypothermia (33–36°C) for 24 hours in comatose post-arrest patients. Neurologic prognostication is delayed at least 72 hours off sedation.
11 STEMI, Malignant Arrhythmias & ECMO CARDIAC
STEMI (ST-elevation MI) requires emergent reperfusion: primary PCI within 90 minutes (door-to-balloon), thrombolytics if PCI unavailable. Standard meds: aspirin 325 mg chewed, P2Y12 inhibitor (ticagrelor, prasugrel, or clopidogrel), anticoagulation (heparin or bivalirudin), high-intensity statin, beta-blocker if hemodynamically stable, ACEi within 24 hours.
Malignant arrhythmias: VT (monomorphic) — synchronized cardioversion if unstable, amiodarone or procainamide if stable. VF / pulseless VT — unsynchronized defibrillation. Torsades de pointes — magnesium 2 g IV, overdrive pacing. Atrial fibrillation with RVR and instability — synchronized cardioversion (100–200 J). Stable — diltiazem, metoprolol, amiodarone.
ECMO Indications
VV-ECMO (veno-venous) supports oxygenation in refractory respiratory failure: severe ARDS with P/F < 80 despite optimized ventilation, Murray score ≥ 3, failure of prone/paralysis. VA-ECMO (veno-arterial) supports both heart and lungs: refractory cardiogenic shock, post-arrest, massive PE. Cannulation is typically femoral-femoral (VA) or femoral-internal jugular (VV).
12 AKI, CRRT & Electrolyte Emergencies RENAL
Acute kidney injury (AKI) is defined by the KDIGO criteria: rise in creatinine ≥ 0.3 mg/dL within 48 h, or 1.5× baseline within 7 days, or UOP < 0.5 mL/kg/hr × 6 h. Three physiologic categories: prerenal (hypovolemia, sepsis, cardiorenal — FeNa < 1%), intrinsic (ATN, AIN, glomerular, contrast — FeNa > 2%), postrenal (obstruction — ultrasound for hydronephrosis).
| Stage | Creatinine | Urine Output |
|---|---|---|
| 1 (Risk) | 1.5–1.9× baseline, or ≥ 0.3 rise | < 0.5 mL/kg/hr × 6–12 h |
| 2 (Injury) | 2.0–2.9× baseline | < 0.5 mL/kg/hr × ≥ 12 h |
| 3 (Failure) | ≥ 3.0× baseline, or Cr ≥ 4, or RRT | < 0.3 mL/kg/hr × 24 h, or anuria × 12 h |
CRRT & Dialysis
Indications for RRT (AEIOU): Acidosis refractory, Electrolyte (K > 6.5 refractory), Ingestion (dialyzable toxin), Overload (refractory pulmonary edema), Uremia (pericarditis, encephalopathy). CRRT (continuous renal replacement therapy) runs 24 h/day and is preferred in hemodynamically unstable ICU patients. Modalities: CVVH (convection), CVVHD (diffusion), CVVHDF (combined). Document access site, mode, blood flow rate, effluent rate, anticoagulation (citrate vs heparin), and fluid removal goal.
Electrolyte Emergencies
Hyperkalemia: K > 6.5 with ECG changes (peaked T waves, widened QRS, sine wave). Treat in order: (1) calcium gluconate 1 g IV for membrane stabilization, (2) insulin + D50 and beta-agonist to shift K intracellular, (3) remove K with loop diuretics, kayexalate, or dialysis. Hyponatremia: severe symptomatic (seizures, coma, Na < 120) — 3% saline 100 mL bolus × up to 3, correct no faster than 8–10 mEq/24 h to avoid osmotic demyelination. Hypocalcemia, hypomagnesemia, hypophosphatemia: replace aggressively in the ICU, particularly in CRRT/refeeding patients.
13 DKA, HHS & Endocrine Emergencies ENDOCRINE
DKA
Diabetic ketoacidosis: glucose > 250, anion gap acidosis (pH < 7.3, HCO3 < 18), ketonemia/ketonuria. Presents with Kussmaul breathing, fruity breath, abdominal pain, altered mental status. Management: IV fluids (normal saline 1–2 L bolus, then maintenance), insulin drip 0.1 U/kg/hr (hold if K < 3.3, replete first), K replacement (DKA patients are total-body K depleted despite normal serum K), monitor anion gap q2–4h, transition to subcutaneous insulin when gap closes and patient eating.
HHS
Hyperosmolar hyperglycemic state: glucose often > 600, effective osmolality > 320, minimal ketosis, profound dehydration, altered mental status. Mortality higher than DKA. Management focuses on aggressive volume replacement, slower glucose correction, cautious insulin, correction of underlying precipitant.
Adrenal Crisis, Thyroid Storm, Myxedema Coma
Adrenal crisis: refractory hypotension, hypoglycemia, hyponatremia, hyperkalemia in adrenal insufficient patient under stress. Hydrocortisone 100 mg IV bolus + 200 mg/24 h infusion. Thyroid storm: hyperthermia, tachyarrhythmia, agitation, GI symptoms. Treat with beta-blockers (propranolol), PTU or methimazole, iodine (Lugol's) ≥ 1 hour after thionamide, hydrocortisone. Myxedema coma: hypothermia, bradycardia, hypoventilation, altered mental status, hyponatremia. IV levothyroxine 200–400 mcg loading, hydrocortisone, supportive care.
14 GI Bleeding & Hepatic Emergencies GI/HEPATIC
Upper GI bleed: hematemesis, melena, coffee-ground emesis. Causes: peptic ulcer (most common), variceal bleeding (cirrhosis), Mallory-Weiss tear, gastritis, AVMs, malignancy. Management: 2 large-bore IVs, type and cross, resuscitate (crystalloid then blood), PPI drip (pantoprazole 80 mg bolus then 8 mg/hr), octreotide 50 mcg bolus + 50 mcg/hr if variceal suspected, ceftriaxone for SBP prophylaxis in cirrhotic patients, emergent EGD within 12–24 hours. Massive/refractory: balloon tamponade (Blakemore/Minnesota), TIPS, embolization, surgery.
Massive transfusion protocol triggered by hemorrhagic shock: 1:1:1 ratio pRBC/FFP/platelets, consider TXA within 3 hours of trauma, monitor for hypothermia / acidosis / coagulopathy ("lethal triad"). Target Hgb > 7 (restrictive strategy) per TRICC trial and subsequent studies, except active ACS or active bleeding.
Acute liver failure / hepatic encephalopathy: lactulose (target 2–3 soft BMs/day), rifaximin, correction of precipitants (infection, GI bleed, electrolytes), N-acetylcysteine if acetaminophen-induced.
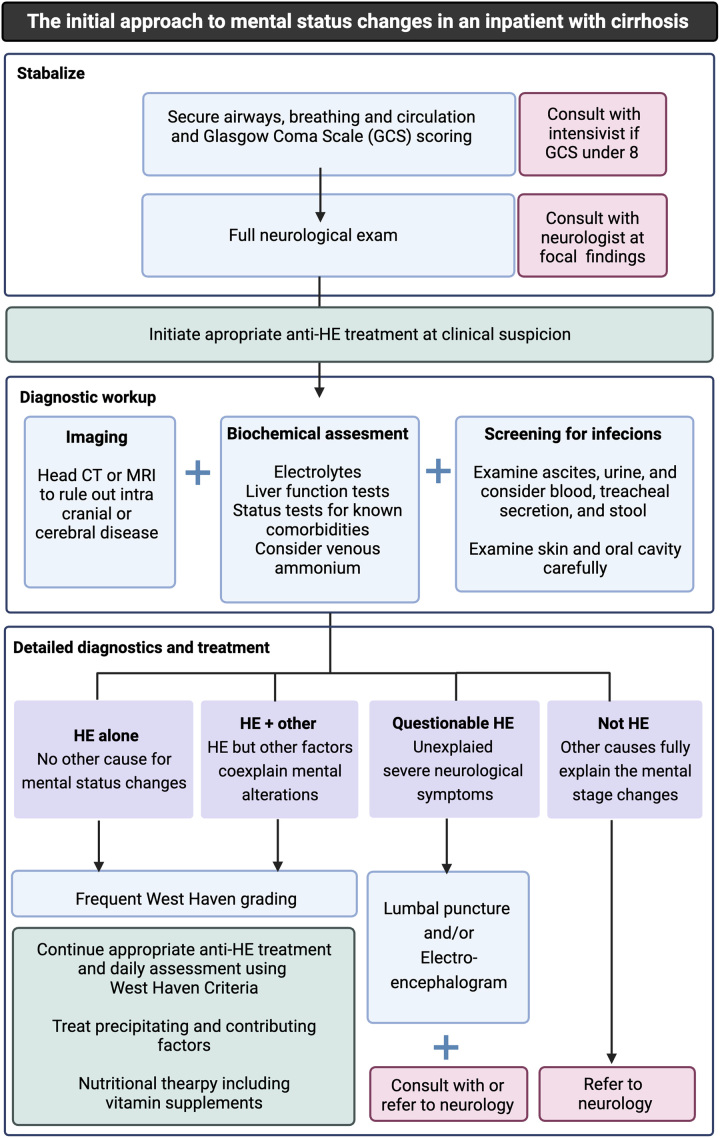
15 Neurologic Emergencies NEURO
Intracerebral Hemorrhage (ICH)
Spontaneous bleed (often hypertensive) or secondary (AVM, aneurysm, tumor, anticoagulant). Treatment: aggressive BP control (target SBP 140 per INTERACT-2), reverse anticoagulation (PCC for warfarin, idarucizumab for dabigatran, andexanet or PCC for factor Xa inhibitors), neurosurgical consult for evacuation if indicated, ICP management (head elevation, hypertonic saline, mannitol, seizure prophylaxis).
Cushing's triad (hypertension, bradycardia, irregular respirations) is a late sign of increased intracranial pressure and impending herniation.
Ischemic Stroke
tPA within 4.5 hours of onset (with criteria); thrombectomy within 6–24 h for large vessel occlusion. BP parameters differ: permissive HTN (< 220/120) if not treating with tPA, < 185/110 if treating. Document NIH Stroke Scale.
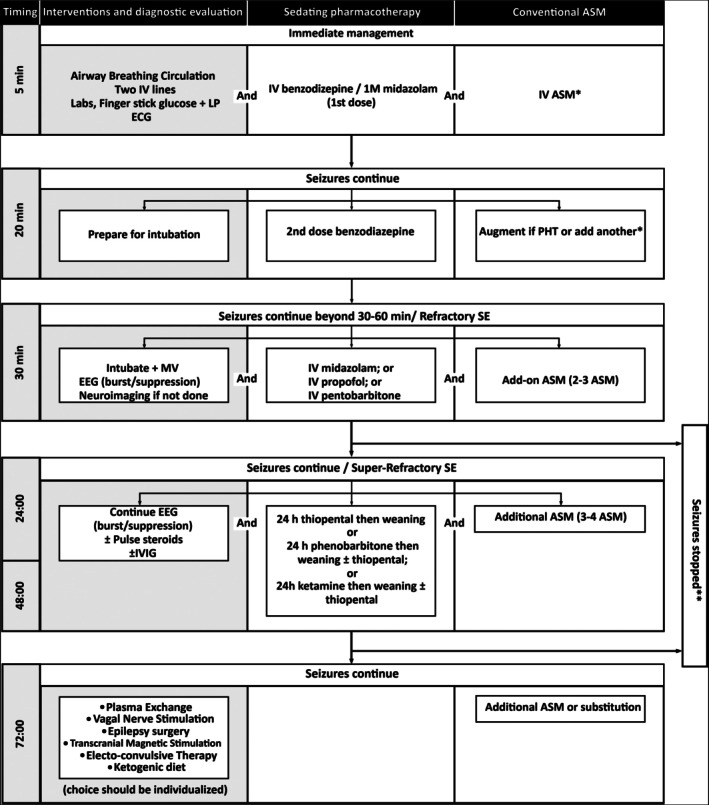
Status Epilepticus
Seizure > 5 minutes or recurrent without recovery. First-line: IV benzodiazepine (lorazepam 4 mg IV, midazolam 10 mg IM). Second-line: levetiracetam 60 mg/kg, fosphenytoin 20 mg PE/kg, or valproate. Refractory: propofol or midazolam infusion, intubation, continuous EEG monitoring.
16 Toxicology — Overdose & Withdrawal TOX
Acetaminophen overdose: stages I (6–24 h, nonspecific), II (24–72 h, RUQ pain, LFTs rising), III (72–96 h, fulminant hepatic failure), IV (recovery or transplant/death). Rumack-Matthew nomogram guides treatment. N-acetylcysteine (NAC) IV 150 mg/kg loading, or PO, maximally effective within 8 hours but beneficial even late.
Opioid overdose: triad of miosis, respiratory depression, altered mental status. Naloxone 0.04–2 mg titrated; long-acting opioids require naloxone drip.
Alcohol withdrawal & DT: tremor/anxiety 6–12 h, seizures 12–48 h, hallucinosis 12–48 h, delirium tremens 48–96 h (tachycardia, hyperthermia, severe agitation, mortality up to 15%). Treat with symptom-triggered benzodiazepines (CIWA protocol), thiamine BEFORE glucose, folate, fluids. Severe: propofol or phenobarbital, dexmedetomidine adjunct.
Benzodiazepine overdose: supportive; flumazenil rarely used due to seizure risk. Beta-blocker / calcium channel blocker overdose: IV fluids, calcium, glucagon, high-dose insulin euglycemia, lipid emulsion, pressors. TCA overdose: sodium bicarbonate for QRS widening > 100 ms.
17 Toxidromes & Temperature Emergencies TOX
| Syndrome | Cause | Features | Treatment |
|---|---|---|---|
| NMS | Neuroleptics (antipsychotics) | Hyperthermia, lead-pipe rigidity, AMS, autonomic instability, ↑CK | Stop agent, cooling, dantrolene, bromocriptine |
| Serotonin syndrome | SSRIs, MAOIs, linezolid, tramadol | Clonus, hyperreflexia, hyperthermia, agitation | Stop agent, cyproheptadine, benzos |
| Malignant hyperthermia | Volatile anesthetics, succinylcholine | Muscle rigidity, hyperthermia, acidosis, hyperkalemia | Dantrolene, cooling, supportive |
| Anticholinergic | Antihistamines, TCAs, atropine | Hot, dry, red, mad, blind (mydriasis), urinary retention | Physostigmine if severe |
| Cholinergic | Organophosphates, carbamates | SLUDGE: salivation, lacrimation, urination, defecation, GI, emesis | Atropine, pralidoxime |
| Sympathomimetic | Cocaine, amphetamines | Tachycardia, HTN, mydriasis, diaphoresis, agitation | Benzodiazepines |
Severe hypothermia: < 28°C → warm central fluids, warmed humidified O2, bladder/peritoneal lavage, ECMO for refractory. Don't call death until warm (> 32°C). Heat stroke: core temp > 40°C with CNS dysfunction → aggressive cooling (cold water immersion, evaporative), IV fluids, monitor for rhabdo/DIC/AKI.
18 ICU Procedures — Airway, Access & Bedside
| Procedure | Indication | Scribe Documentation Elements |
|---|---|---|
| Endotracheal intubation / RSI | Respiratory failure, airway protection | Pre-oxygenation, induction (etomidate/ketamine/propofol), paralytic (rocuronium/succinylcholine), Mallampati, Cormack-Lehane grade, ETT size, depth at lip, confirmation (EtCO2, bilateral breath sounds, CXR) |
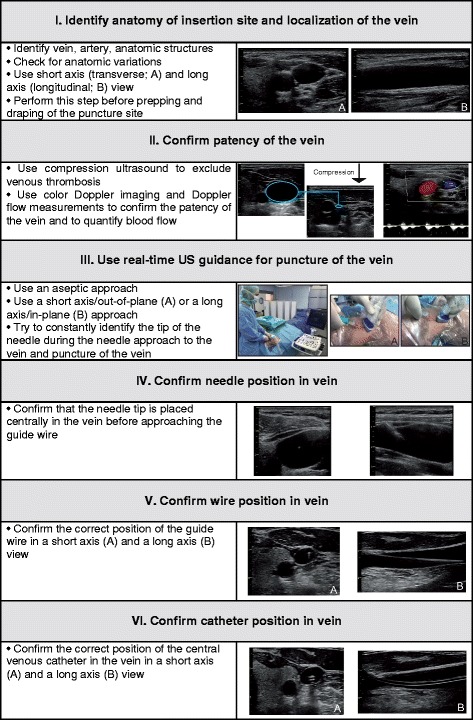
| Central line (IJ, subclavian, femoral) | Pressors, CVP, poor peripheral access | Site, US guidance, consent, sterile technique, # attempts, complications (PTX, hematoma, arterial puncture), confirmation CXR, catheter type (triple-lumen, Cordis, Shiley) |
| Arterial line | Continuous BP, frequent ABGs | Site (radial, femoral), Allen test, waveform, complications |
| Thoracentesis | Pleural effusion diagnostic/therapeutic | Side, volume, appearance, labs (Light's criteria), complications (PTX) |
| Paracentesis | Ascites — diagnostic (SBP) or therapeutic | Volume, SAAG, cell count, albumin replacement if > 5 L |
| Lumbar puncture | Suspected meningitis, SAH, CNS eval | Opening pressure, tube labels (cell count, protein, glucose, culture, special), appearance, complications |
| Chest tube | PTX, hemothorax, empyema, large effusion | Size (28–36 Fr), site, output (initial and ongoing), suction vs water seal, air leak |
| Bronchoscopy | BAL, secretion clearance, airway evaluation | Findings, BAL samples, complications |
| Cardioversion / defibrillation | Unstable VT/VF/AF with RVR | Sync vs unsync, joules, outcome, sedation used |
| Pericardiocentesis | Tamponade | Approach, fluid appearance and volume, hemodynamic response |
| ECMO cannulation | Refractory respiratory/circulatory failure | Configuration (VV/VA), cannula sizes and sites, flows, circuit parameters |
For every procedure you document: timestamp of start and stop, who performed, consent (emergent or informed), sterile prep, local anesthetic, ultrasound guidance if used, number of attempts, immediate complications, and post-procedure imaging (especially post-line CXR). Missing any of these is a common billing/compliance failure.
19 Hemodynamic Monitoring & POCUS
Arterial line waveform: dicrotic notch reflects aortic valve closure. Underdamped (whip) = overestimates SBP; overdamped = underestimates SBP. MAP is the most reliable number.
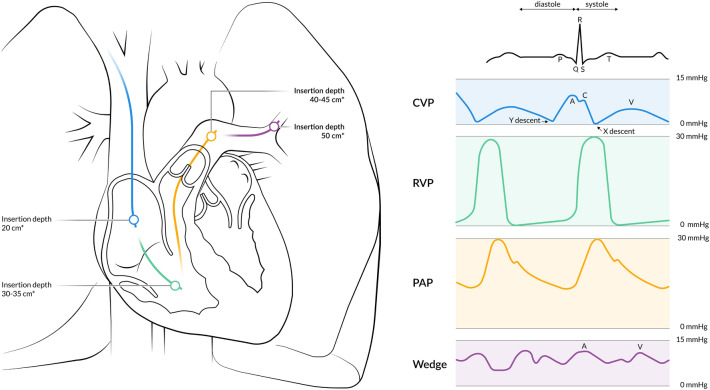
CVP: central venous pressure (normal 2–8 mmHg). Single values are unreliable for volume assessment; trends with fluid challenges are more useful.
PA catheter (Swan-Ganz): provides PCWP, CO, SVR, mixed venous O2 saturation. Largely replaced by less invasive methods but still used in complex shock.
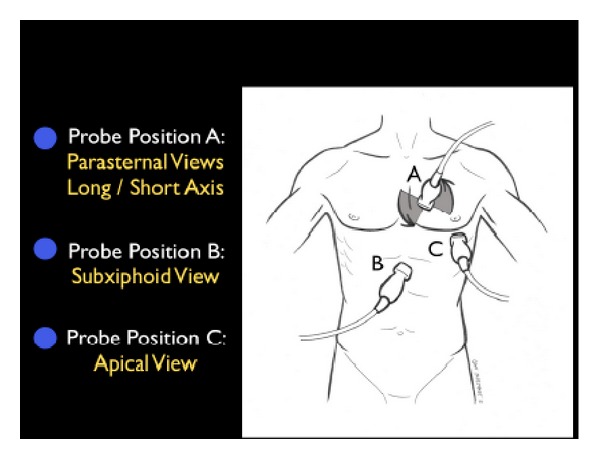
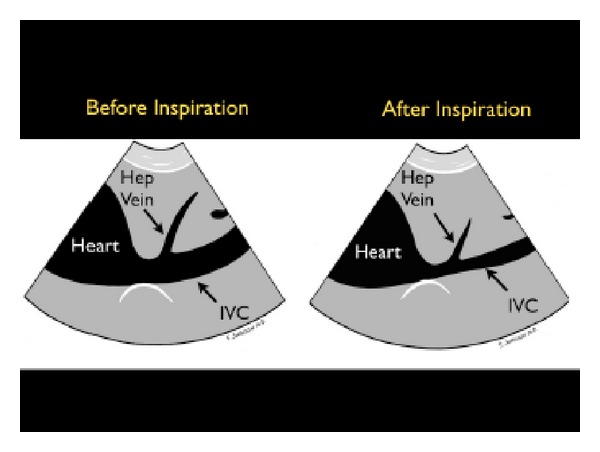
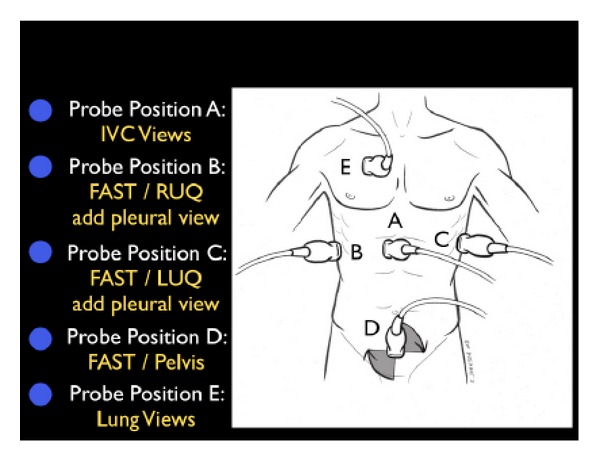
Point-of-care ultrasound (POCUS): the modern ICU "stethoscope." Cardiac (RV/LV function, effusion, IVC collapsibility for volume status), pulmonary (B-lines for edema, sliding for PTX), abdominal (FAST for free fluid), vascular (DVT, central line guidance).
Dynamic volume assessment: static measures like CVP are unreliable. Preferred dynamic indicators include pulse pressure variation (PPV > 13% suggests fluid responsiveness in mechanically ventilated patients with controlled breaths), stroke volume variation (SVV), IVC collapsibility on POCUS, and passive leg raise with real-time cardiac output assessment. Scribes document which method the team used and the inferred fluid strategy.
CBC with diff, BMP, magnesium, phosphate, LFTs, lactate, troponin (if cardiac concern), BNP, coagulation (PT/INR/PTT), ABG with lactate, cultures pending, procalcitonin (sometimes). Note trends, not just single values.
20 ICU Medications — Sedation, Pressors & Prophylaxis
Sedation & Analgesia
| Drug | Class | Key Notes |
|---|---|---|
| Propofol (Diprivan) | GABA-A | Fast on/off, hypotension, PRIS (propofol infusion syndrome) with high doses > 48 h, lipid load |
| Midazolam (Versed) | Benzodiazepine | Accumulates with prolonged use, active metabolites, delirium risk |
| Dexmedetomidine (Precedex) | α2 agonist | Light sedation, bradycardia/hypotension, less delirium, no respiratory depression |
| Ketamine | NMDA antagonist | Maintains BP, bronchodilator, good for status asthmaticus intubation |
| Fentanyl | Opioid | First-line analgesia, short acting, chest wall rigidity at high doses |
| Hydromorphone (Dilaudid) | Opioid | Longer acting, boluses common |
| Morphine | Opioid | Histamine release, avoid in AKI |
Neuromuscular Blockade (Paralytics)
| Drug | Class | Use |
|---|---|---|
| Succinylcholine | Depolarizing | RSI; avoid in hyperkalemia, crush, burns > 24 h |
| Rocuronium | Non-depolarizing | RSI alternative, reversible with sugammadex |
| Vecuronium | Non-depolarizing | Longer procedures |
| Cisatracurium | Non-depolarizing | Hofmann elimination, preferred in organ failure and severe ARDS |
Vasopressors & Inotropes
| Drug | Receptors | Primary Use |
|---|---|---|
| Norepinephrine (Levophed) | α1 >> β1 | First-line for septic shock |
| Vasopressin | V1 | Adjunct in septic shock, refractory hypotension |
| Epinephrine | α1, β1, β2 | Anaphylaxis, cardiac arrest, refractory shock |
| Phenylephrine | α1 | Pure vasoconstrictor, bradycardic hypotension |
| Dopamine | Dose dependent | Largely replaced; bradycardic shock |
| Dobutamine | β1 (β2) | Inotrope for cardiogenic shock |
| Milrinone | PDE-3 inhibitor | Inodilator, cardiogenic shock, pulmonary HTN |
Prophylaxis & Supportive
DVT prophylaxis: enoxaparin 40 mg SQ daily or heparin 5000 U SQ q8h; mechanical (SCDs) if contraindicated. Stress ulcer prophylaxis: PPI (pantoprazole) or H2 blocker in mechanically ventilated, coagulopathic, or high-risk patients. Glycemic control: insulin drip targeting 140–180 mg/dL per NICE-SUGAR trial. Electrolytes: K > 4, Mg > 2 in cardiac patients; replete phosphate in refeeding.
21 Classification Systems & Scoring
| Component | Score | Finding |
|---|---|---|
| Eye | 4 | Spontaneous |
| 3 | To voice | |
| 2 | To pain | |
| 1 | None | |
| Verbal | 5 | Oriented |
| 4 | Confused | |
| 3 | Inappropriate words | |
| 2 | Incomprehensible sounds | |
| 1 | None | |
| Motor | 6 | Obeys commands |
| 5 | Localizes pain | |
| 4 | Withdraws from pain | |
| 3 | Flexion (decorticate) | |
| 2 | Extension (decerebrate) | |
| 1 | None |
| Score | Term | Description |
|---|---|---|
| +4 | Combative | Violent, immediate danger |
| +3 | Very agitated | Pulls tubes, aggressive |
| +2 | Agitated | Frequent nonpurposeful movement |
| +1 | Restless | Anxious, no aggressive movements |
| 0 | Alert and calm | |
| −1 | Drowsy | > 10 sec awakening to voice |
| −2 | Light sedation | < 10 sec awakening to voice |
| −3 | Moderate sedation | Movement to voice, no eye contact |
| −4 | Deep sedation | Movement to physical stimulation |
| −5 | Unarousable | No response |
Six organ systems each scored 0–4 (maximum total 24):
- Respiration: PaO2/FiO2 (>400 / 301–400 / 201–300 / 101–200 / ≤100)
- Coagulation: Platelets (>150 / 101–150 / 51–100 / 21–50 / ≤20 ×10^9/L)
- Liver: Bilirubin (<1.2 / 1.2–1.9 / 2.0–5.9 / 6.0–11.9 / ≥12)
- Cardiovascular: MAP ≥70 / MAP <70 / dopamine ≤5 or dobutamine / dopamine >5 or NE ≤0.1 / dopamine >15 or NE >0.1
- CNS: GCS 15 / 13–14 / 10–12 / 6–9 / <6
- Renal: Creatinine (<1.2 / 1.2–1.9 / 2.0–3.4 / 3.5–4.9 / ≥5) or UOP
The APACHE II score is a more comprehensive 12-variable severity score used for ICU benchmarking. NUTRIC identifies patients who benefit from aggressive nutrition support. CAM-ICU is the bedside delirium screen. Shock Index = HR/SBP (> 0.9 abnormal).
22 Physical Exam & Daily ICU Rounds
The ICU exam is focused and repetitive: you document the same elements every day, looking for interval change. General appearance: sedated, awake, in distress, comfortable. HEENT: pupils (size, reactivity), ETT position, NG tube. Neck: central line, tracheostomy, JVD. Cardiac: rate, rhythm, murmurs, rubs, S3/S4. Pulmonary: breath sounds (bilateral, clear, crackles, rhonchi, wheezes, diminished), symmetric chest rise, ventilator synchrony. Abdomen: soft, distended, tender, bowel sounds, ostomy/drains. Extremities: edema, pulses, warmth, capillary refill, mottling. Neuro: following commands, moving all extremities, pupillary response, cough/gag if intubated.
Rounds move fast. The attending examines the patient in 60 seconds and dictates findings while walking to the next room. Learn the shorthand: "Lungs coarse bilaterally, soft abd, trace edema, moves all four, pupils 3/3 reactive" becomes a complete documented exam when typed accurately.
23 Abbreviations Master List
Organ Systems & Syndromes
Procedures, Lines & Equipment
Ventilation & Hemodynamics
Scores & Scales
24 Sample HPI Templates & References
These sample HPIs represent the kinds of admissions and progress notes you will draft in the ICU. Internalize the rhythm: one-sentence identification, presenting event, objective data at presentation, interventions, and current status.
"Mr. [Name] is a 71-year-old male with a history of COPD, type 2 diabetes, and hypertension who was admitted to the MICU from the emergency department for septic shock secondary to right lower lobe pneumonia. He presented with 3 days of productive cough, fever to 39.4°C, progressive dyspnea, and confusion. In the ED, initial vitals showed BP 78/42, HR 128, RR 32, SpO2 84% on room air, T 39.6. Lactate was 5.2, WBC 22.4 with 18% bands, procalcitonin 14. He received 30 mL/kg lactated Ringer's, ceftriaxone and azithromycin, and was started on norepinephrine with vasopressin adjunct. He was intubated for hypoxemic respiratory failure (P/F 110). On arrival to the ICU, he is on AC/VC, FiO2 0.6, PEEP 10, TV 400, RASS −2 on fentanyl and propofol, norepinephrine 0.25 mcg/kg/min, MAP 67, repeat lactate 3.4."
"Ms. [Name] is a 58-year-old female with a history of RA on methotrexate, admitted 3 days ago with bilateral community-acquired pneumonia and severe ARDS. Intubated in the ED, now on AC/VC with FiO2 0.7, PEEP 14, TV 340 (6 mL/kg PBW), RR 26, Pplat 28. Most recent ABG 7.28/52/68/24, P/F 97 (severe ARDS). She was proned yesterday for 18 hours with improvement in oxygenation. She is on cisatracurium infusion for ventilator dyssynchrony, fentanyl, and midazolam. Hemodynamics: NE 0.08, MAP 68. Cultures growing strep pneumoniae from sputum and blood, day 3 of ceftriaxone. AKI stage 2 with Cr up from 0.9 to 2.1, oliguric."
"Mr. [Name] is a 62-year-old male with a history of CAD s/p CABG and ischemic cardiomyopathy (LVEF 25%) who suffered an out-of-hospital cardiac arrest witnessed by his wife. Bystander CPR initiated; initial rhythm on EMS arrival was VF. He received 3 shocks, epinephrine × 3, amiodarone 300 mg, and achieved ROSC after approximately 18 minutes of downtime. In the ED, ECG showed anterior STEMI; taken emergently to cath lab with PCI to proximal LAD (100% thrombotic occlusion, drug-eluting stent placed). On arrival to CICU, he is intubated, comatose, on norepinephrine 0.12 and dobutamine 5, IABP at 1:1. Targeted normothermia (36°C) initiated for 24 hours. Neurologic exam: GCS 3T, pupils 3 mm reactive, no spontaneous movements off sedation."
"Mr. [Name] is a 59-year-old male with a history of alcoholic cirrhosis (Child-Pugh C, MELD 22), known esophageal varices, and prior variceal banding, who presented with two episodes of large-volume hematemesis and hemodynamic instability. Initial vitals BP 82/40, HR 132, Hgb 6.1, INR 2.3, platelets 68. MTP activated, received 4 units pRBC, 2 units FFP, 1 unit platelets. Started on octreotide and pantoprazole drips, ceftriaxone for SBP prophylaxis. Emergent EGD revealed grade III esophageal varices with active bleeding; band ligation performed. Post-procedure, he is intubated for airway protection, hemodynamically improved on vasopressin 0.04, MAP 70, repeat Hgb 8.4. Plan: ICU monitoring, beta-blocker once stabilized, TIPS evaluation if re-bleeds."
"Ms. [Name] is a 34-year-old female with a known seizure disorder on levetiracetam who was brought in by EMS after witnessed generalized tonic-clonic seizure activity lasting over 20 minutes. She received 10 mg IM midazolam by EMS and an additional 4 mg IV lorazepam on arrival without resolution. Loading dose of fosphenytoin 20 mg PE/kg administered, followed by levetiracetam 60 mg/kg, without cessation. Intubated for airway protection and started on midazolam continuous infusion titrated to burst suppression on continuous EEG. Workup: negative CT head, LP unremarkable, labs notable for levetiracetam sub-therapeutic at 4. Currently on midazolam 0.2 mg/kg/hr, seizure-free on EEG for 6 hours."
"Mrs. [Name] is a 74-year-old female admitted 8 days ago with perforated diverticulitis s/p exploratory laparotomy with sigmoid resection and Hartmann's procedure, course complicated by septic shock, ARDS, AKI requiring CRRT, and new onset atrial fibrillation with RVR. Currently: intubated AC/VC FiO2 0.55, PEEP 12, P/F 165; NE 0.2, vasopressin 0.04, MAP 66; CRRT day 4, fluid removal 1.5 L/day, Cr 3.8; amiodarone drip for rate control; TPN (inability to tolerate tube feeds due to ileus); day 8 meropenem, day 6 micafungin for candidemia; Hgb 7.8, platelets 62 (heparin stopped, HIT workup pending). SOFA score today: 12. Family meeting scheduled for goals of care discussion."
References & Sources
Clinical Practice Guidelines
KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl. 2012.
Panchal AR et al. 2020 AHA Guidelines for CPR and Emergency Cardiovascular Care. Circulation. 2020.
ARDS Definition Task Force. Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA. 2012.
Landmark Clinical Trials
ARDSNet (ARMA). Ventilation with lower tidal volumes for acute lung injury and ARDS. NEJM. 2000.
Guérin C et al. (PROSEVA). Prone positioning in severe ARDS. NEJM. 2013.
Villanueva C et al. Transfusion strategies for acute upper gastrointestinal bleeding. NEJM. 2013.
Semler MW et al. (SMART). Balanced crystalloids versus saline in critically ill adults. NEJM. 2018.
Diagram & Figure Sources
Figure 1: Cardiac Conduction System. OpenStax College. CC BY 3.0.
Figure 2: Major Respiratory Organs. OpenStax College. CC BY 3.0.
Figure 3: ICU Mechanical Ventilator. Wikimedia Commons. Public domain.
Figure 4: Central Venous Catheter. Wikimedia Commons. Public domain.
The best ICU scribes think in systems. When the attending says "she's in septic shock from a pneumonia with ARDS and AKI on CRRT," a great scribe immediately knows the note will have a Pulm section documenting the ventilator and P/F, a CV section with the pressor doses and lactate trend, a Renal section with the CRRT parameters, and an ID section with cultures and antibiotic day counts. When the intensivist says "she's MAP 58, bump the Levo, give 500 of LR, and get a lactate," the scribe documents the intervention, the rationale, and the response within seconds.
Be fast. Be accurate. Pre-populate. Learn the drugs by both name and typical dose range. Anticipate the systems-based note. Track trends, not isolated numbers. Know when a number is critical (a Pplat of 34, a K of 6.8, a lactate rising from 2 to 5). Understand that the ICU is a symphony of small decisions made many times a day, and your notes are the written record of every one of them.
Welcome to critical care. It is the most intellectually dense specialty in medicine — and the most rewarding place a scribe can learn.