Dermatology
Every diagnosis, lesion morphology, procedure, biologic, and documentation framework you need to succeed on day one and beyond in a dermatology clinic.
All diagrams on this page are sourced from published educational or institutional materials rather than AI generation. Each figure caption links to the original source, and the full diagram and guideline citations are collected in the references section at the bottom.
01 The Skin — Anatomy & Physiology Essentials
Dermatology is the study and treatment of the skin, hair, and nails. The skin is the largest organ of the body, weighing roughly 16% of total body weight and covering approximately 1.5 to 2 square meters in adults. It is simultaneously a mechanical barrier, an immune organ, a thermoregulatory system, a sensory structure, and a synthesis site for vitamin D. Understanding its layered architecture is the prerequisite to understanding every disease and procedure in the guide below.
The Three Layers of the Skin
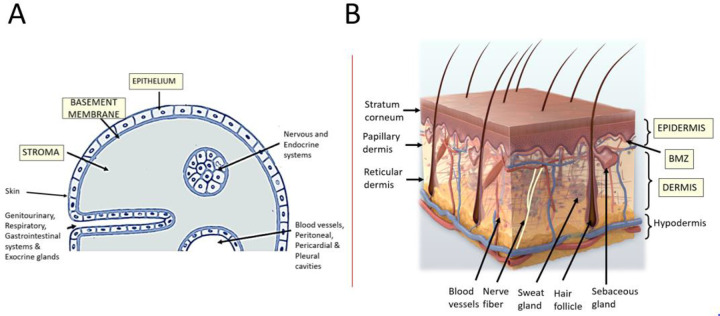
The skin is organized into three distinct layers. The outermost is the epidermis, a stratified squamous epithelium that is avascular and relies on diffusion from the underlying dermis for nutrition. Beneath it lies the dermis, a collagen- and elastin-rich connective tissue layer that houses blood vessels, lymphatics, nerves, sebaceous glands, eccrine and apocrine sweat glands, and the hair follicle apparatus. Deepest is the subcutis (also called the hypodermis or panniculus), a layer of fat lobules separated by fibrous septa that insulates, cushions, and stores energy.
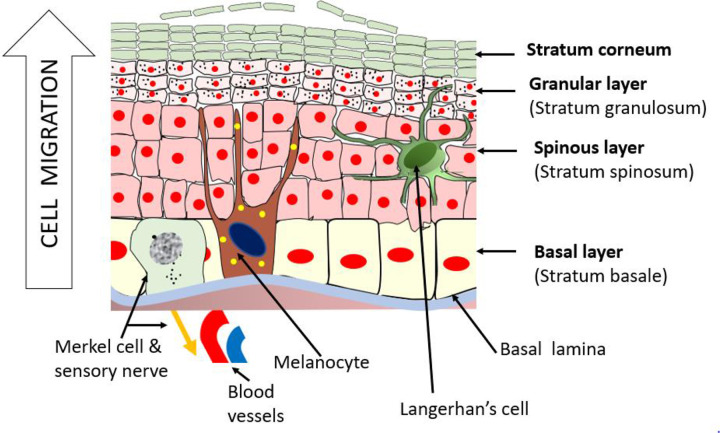
Within the epidermis itself, there are four to five sublayers moving from deep to superficial: the stratum basale (basal cell layer, where keratinocytes divide and where melanocytes sit), the stratum spinosum (spinous or prickle cell layer, where desmosomal connections create a "spiny" appearance), the stratum granulosum (granular layer, where keratohyalin granules form), the stratum lucidum (present only in thick skin of palms and soles), and the stratum corneum (the outer "brick and mortar" layer of anucleate corneocytes embedded in a lipid matrix, which forms the primary mechanical and water barrier). Pathology at each level produces characteristic diseases: psoriasis involves hyperproliferation of basal keratinocytes and parakeratosis of the stratum corneum, pemphigus vulgaris destroys desmosomes within the stratum spinosum, and bullous pemphigoid splits the dermoepidermal junction below the basal layer.
Cells You Must Know
Five cell populations dominate skin pathology. Keratinocytes (≈ 95% of epidermal cells) produce keratin and form the structural scaffold; their dysregulation drives psoriasis, eczema, and skin cancers. Melanocytes (in the basal layer) produce melanin packaged into melanosomes and transferred to neighboring keratinocytes; their malignant transformation produces melanoma. Langerhans cells are dendritic antigen-presenting cells that sample the epidermis for pathogens and drive allergic contact dermatitis. Merkel cells are mechanoreceptors in the basal layer that can give rise to the aggressive Merkel cell carcinoma. In the dermis, fibroblasts synthesize collagen and elastin and are central to wound healing and scleroderma pathophysiology.
Adnexal Structures
Hair follicles, sebaceous glands, and sweat glands ("skin appendages" or adnexae) are epidermal derivatives that extend into the dermis. The pilosebaceous unit (hair follicle + sebaceous gland + arrector pili muscle) is the anatomic home of acne, rosacea, and folliculitis. Eccrine sweat glands are distributed almost everywhere on the body and mediate thermoregulation; apocrine sweat glands open into hair follicles in the axillae and anogenital region and are the origin of hidradenitis suppurativa. Nail units consist of the matrix (where nail plate is generated), nail bed, proximal and lateral nail folds, and cuticle.
Know the anatomy cold. When the attending dictates "excisional biopsy to the subcutis with 2 mm margins" or "lesion extends into the reticular dermis" or "shave biopsy staying in the papillary dermis," you need to chart these depth qualifiers without hesitation. The dermis itself is divided into a superficial papillary dermis (loose collagen, contains the dermal papillae that interdigitate with the rete ridges of the epidermis) and a deeper reticular dermis (dense collagen, where most adnexal structures live).
02 Scribe Documentation Framework
The Dermatology SOAP Note
Dermatology notes are highly visual and morphology-driven. Where an internist describes a symptom, a dermatologist describes a lesion: its type, color, shape, border, distribution, and change over time. A scribe who cannot translate the attending's spoken morphology into written shorthand will fall behind immediately.
Chief Complaint: A single phrase — "full body skin exam," "new mole right back," "rash both hands," "follow-up psoriasis on biologic."
HPI: Use the modified OLDCARTS adapted to skin disease. Always capture: onset and duration (days, weeks, months, years), distribution (localized vs generalized, symmetric vs asymmetric, photo-exposed vs covered), associated symptoms (pruritus, pain, burning, bleeding), exacerbating factors (sun, heat, stress, detergents, new medications, occupational exposures), prior treatments tried and their effect (OTC steroids, moisturizers, prior prescriptions), and for suspicious lesions the ABCDE change history (Asymmetry, Border, Color, Diameter, Evolution).
Past Dermatologic History: Prior skin cancers (type, location, year, treatment — Mohs vs excision vs ED&C), history of atypical nevi, family history of melanoma, history of eczema/psoriasis, phototherapy, biologic or systemic therapy history, and radiation.
Social / Exposure History: Sun exposure patterns, tanning bed use, occupational exposures (mechanics, hairdressers, healthcare workers, construction), hobbies, pets, travel, new soaps/cosmetics, and Fitzpatrick skin type self-assessment.
General: Fitzpatrick skin type I–VI, overall photodamage grade, presence of scattered lentigines or actinic keratoses.
Lesion description format: Location → size (mm) → primary morphology → secondary changes → color → border → configuration. Example: "Left dorsal forearm, 6 mm, well-demarcated erythematous scaly papule with central erosion, irregular border."
Total body skin exam (TBSE): Document scalp, face, ears, neck, anterior and posterior trunk, upper extremities including axillae, lower extremities including soles and interdigital spaces, and genitalia when appropriate. A common shorthand: "TBSE performed, no concerning pigmented or non-pigmented lesions identified aside from those described above."
Each lesion or diagnosis is listed separately with its plan: biopsy type, cryotherapy site, topical prescription with strength and vehicle, systemic therapy, return-to-clinic interval, and counseling (sun protection, moisturizer technique, trigger avoidance). In a skin cancer clinic, the plan section frequently includes referral to Mohs surgery and pathology follow-up instructions.
Dermatologists speak in a staccato rhythm during skin exams. Expect the attending to walk the room and say "scalp clear, face has a few AKs right temple frozen, right cheek 4 mm pearly papule — biopsy, chest clear, left back 8 mm asymmetric pigmented macule — shave biopsy." You must keep up. A helpful habit is to pre-build a "biopsies today" running list at the top of your note so you can drop each site in as it is called out and re-populate the full description later.
03 Primary & Secondary Lesion Morphology Foundation
Morphology is the language of dermatology. Every encounter begins with the attending naming a primary lesion type, optionally layering on secondary changes, and then describing color, configuration, and distribution. You must memorize these terms cold — they are used every minute of every clinic day.
| Term | Definition | Example |
|---|---|---|
| Macule | Flat, circumscribed color change, < 1 cm | Freckle, lentigo, petechia |
| Patch | Flat color change, ≥ 1 cm | Vitiligo, café-au-lait |
| Papule | Raised, solid lesion, < 1 cm | Molluscum, nevus, acne comedo |
| Plaque | Raised, flat-topped lesion, ≥ 1 cm | Psoriasis plaque, lichen planus |
| Nodule | Raised, solid, ≥ 1 cm with depth into dermis/subcutis | Lipoma, epidermoid cyst, SCC |
| Tumor | Nodule > 2 cm | Large BCC, soft-tissue sarcoma |
| Vesicle | Fluid-filled, < 1 cm | HSV, varicella, dyshidrotic eczema |
| Bulla | Fluid-filled, ≥ 1 cm | Bullous pemphigoid, burn |
| Pustule | Pus-filled raised lesion | Acne pustule, folliculitis, pustular psoriasis |
| Wheal (hive) | Transient edematous papule/plaque | Urticaria |
| Cyst | Encapsulated sac with fluid or semisolid contents | Epidermoid cyst, pilar cyst |
| Term | Definition |
|---|---|
| Scale | Flakes of stratum corneum (psoriasis silvery scale, seborrheic yellow greasy scale) |
| Crust | Dried serum, blood, or pus on the skin surface (impetigo's honey crust) |
| Erosion | Loss of epidermis only — heals without scarring |
| Ulcer | Loss of epidermis + dermis — heals with scarring |
| Fissure | Linear crack through epidermis into dermis |
| Lichenification | Thickened skin with exaggerated skin markings from chronic rubbing |
| Excoriation | Linear erosion from scratching |
| Atrophy | Thinning of the epidermis or dermis |
| Scar | Replacement of normal tissue with fibrous tissue after injury |
Configuration and distribution terms round out the vocabulary. Annular (ring-shaped, as in tinea corporis or granuloma annulare), linear (as in lichen striatus or poison ivy), grouped or herpetiform (as in HSV), reticulated (net-like, as in livedo reticularis), serpiginous (snake-like, as in cutaneous larva migrans), dermatomal (following a nerve root, as in herpes zoster), photodistributed (sun-exposed areas only), intertriginous (in skin folds, as in inverse psoriasis or candidal intertrigo), and acral (hands/feet) are all terms you will hear routinely.
04 Acne Vulgaris Inflammatory
Acne vulgaris is the most common dermatologic diagnosis worldwide, affecting up to 85% of adolescents and a significant minority of adults, especially women in their 20s and 30s. It is a chronic inflammatory disease of the pilosebaceous unit driven by four interacting factors: increased sebum production under androgen influence, follicular hyperkeratinization (plugging of the follicular opening), colonization by Cutibacterium acnes (formerly Propionibacterium acnes), and inflammatory cytokine release.

Clinical Presentation
Acne lesions are classified as non-inflammatory (open comedones = blackheads, closed comedones = whiteheads) or inflammatory (papules, pustules, nodules, cysts). Distribution is typically the T-zone (forehead, nose, chin), cheeks, upper back, chest, and shoulders — all sebaceous-rich areas. Severity is graded as mild (comedonal ± few inflammatory lesions), moderate (numerous papules/pustules), or severe/nodulocystic (deep nodules, cysts, risk of scarring). The attending may also describe post-inflammatory hyperpigmentation (PIH) in darker skin types or post-inflammatory erythema (PIE) in lighter skin.
Management
The 2024 AAD Guidelines of Care for Acne Vulgaris recommend a stepwise combination approach. Mild: topical retinoid (tretinoin, adapalene, tazarotene) + benzoyl peroxide ± topical antibiotic (clindamycin) — never topical antibiotic monotherapy due to resistance. Moderate: add oral antibiotic (doxycycline or minocycline) for 3–4 months, or combined oral contraceptive/spironolactone in females. Severe / nodulocystic / scarring: oral isotretinoin (Accutane), typically 0.5–1 mg/kg/day to a cumulative dose of 120–150 mg/kg.
Isotretinoin requires enrollment in the iPLEDGE REMS program, monthly pregnancy testing in females of childbearing potential, two forms of contraception, and monthly labs (LFTs, lipids, CBC). You will document iPLEDGE counseling at every visit for isotretinoin patients. Hormonal therapy (combined OCPs, spironolactone 50–200 mg/day) is particularly effective for adult female acne with jawline distribution and premenstrual flare.
For every acne visit, document lesion counts in general terms ("approximately 15 inflammatory papules and 6 closed comedones on the cheeks and forehead, no nodules or cysts, no active scarring"), mention PIH/PIE if present, document current regimen and compliance, and capture any recent tolerability issues (dryness, irritation, photosensitivity). The IGA (Investigator Global Assessment) 0–4 scale is frequently used: 0 clear, 1 almost clear, 2 mild, 3 moderate, 4 severe.
05 Rosacea Inflammatory
Rosacea is a chronic inflammatory facial dermatosis characterized by persistent central facial erythema, flushing, telangiectasias, and inflammatory papules/pustules. It overwhelmingly affects fair-skinned adults (Fitzpatrick I–II), peaks between ages 30 and 60, and is more common in women (though phymatous changes are more common in men). Classic triggers include sun exposure, heat, spicy foods, alcohol (especially red wine), hot beverages, stress, and exercise.
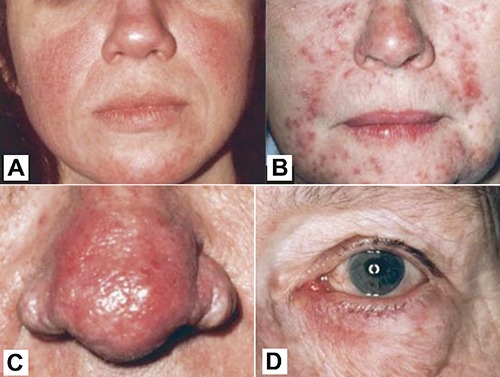
Four phenotypes are recognized: erythematotelangiectatic (persistent central facial erythema and telangiectasias, prominent flushing), papulopustular (acneiform papules and pustules without comedones — the key distinguishing feature from acne), phymatous (thickened, bulbous sebaceous hyperplasia, most commonly affecting the nose = rhinophyma), and ocular rosacea (blepharitis, conjunctivitis, gritty or burning eyes — easy to miss without asking).
Topical: metronidazole 0.75–1%, azelaic acid 15%, ivermectin 1% cream, brimonidine 0.33% gel (for erythema), oxymetazoline 1% cream. Oral: low-dose doxycycline (40 mg modified-release, sub-antimicrobial dose) for papulopustular rosacea. Procedural: pulsed-dye laser or IPL for telangiectasias and erythema; ablative CO2 laser or electrosurgery for rhinophyma. Sun protection, trigger avoidance, and gentle skin care are universally recommended.
06 Atopic Dermatitis (Eczema) Inflammatory
Atopic dermatitis (AD) is a chronic, relapsing, intensely pruritic inflammatory skin disease driven by a combination of epidermal barrier dysfunction (notably filaggrin gene mutations) and Th2-skewed immune response (IL-4, IL-13, IL-31). It is the most common chronic skin disease in children, affecting up to 20% of pediatric patients and 3% of adults, and it is often the first manifestation of the "atopic march" that includes allergic rhinitis, asthma, and food allergy.
Clinical Presentation by Age
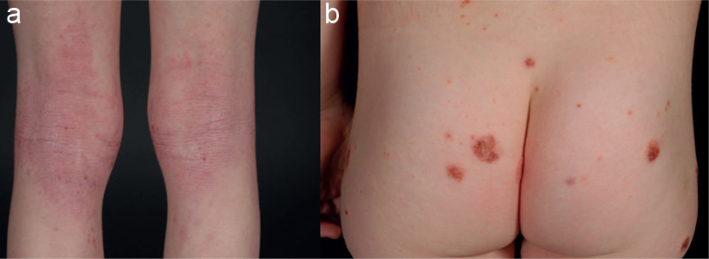
Infantile (0–2 years): erythematous, weeping, crusted patches on the cheeks, scalp, and extensor surfaces; diaper area typically spared. Childhood (2–12 years): flexural involvement (antecubital and popliteal fossae), neck, wrists, ankles; lichenification from chronic scratching. Adolescent/adult: flexural lichenification, hand dermatitis, eyelid involvement, chronic hand eczema. The cardinal symptom at every age is intense pruritus — "the itch that rashes."
Management
The 2023 AAD Guidelines on Topical Therapy for AD emphasize a foundation of daily emollients, lukewarm bathing, and trigger avoidance, layered with topical anti-inflammatories. First-line topicals include topical corticosteroids (potency matched to body region — low-potency on face/folds, mid-potency on body, high-potency on palms/soles and thick plaques), topical calcineurin inhibitors (tacrolimus 0.03/0.1% ointment, pimecrolimus 1% cream — steroid-sparing, safe on face/eyelids), crisaborole 2% ointment (PDE-4 inhibitor), and ruxolitinib 1.5% cream (topical JAK inhibitor).
For moderate-to-severe disease unresponsive to topicals, systemic therapy per the 2024 AAD systemic AD guideline includes dupilumab (IL-4Rα antibody, FDA-approved down to age 6 months), tralokinumab (anti-IL-13), lebrikizumab (anti-IL-13), and oral JAK inhibitors (upadacitinib, abrocitinib) with boxed warnings for thrombosis, malignancy, and cardiovascular events. Phototherapy (NB-UVB) remains a useful option.
07 Contact Dermatitis & Hand Dermatitis Inflammatory
Contact dermatitis divides into irritant contact dermatitis (ICD) — a direct cytotoxic reaction to a substance that requires no prior sensitization and affects anyone exposed at sufficient dose (80% of cases) — and allergic contact dermatitis (ACD) — a type IV delayed hypersensitivity requiring prior sensitization and a second exposure to elicit the reaction (20% of cases). Both produce erythematous, pruritic, vesicular plaques in the distribution of exposure, but ACD tends to have sharper margins that echo the shape of the contactant.

Common ICD triggers include soaps, detergents, solvents, cement, and water (wet work in healthcare and hairdressing). Common ACD allergens include nickel (jewelry, belt buckles, phone cases), fragrance mix, balsam of Peru, preservatives (methylisothiazolinone, formaldehyde releasers), neomycin, bacitracin, rubber accelerators (thiurams, carbamates — gloves), and poison ivy/oak/sumac (urushiol). Diagnosis of ACD is confirmed with patch testing, typically using the T.R.U.E. test or a comprehensive panel (North American 80 Comprehensive Series) applied to the back for 48 hours with readings at days 2, 4, and 7.
Management includes identification and strict avoidance of the culprit, topical corticosteroids (potency matched to body site), oral prednisone tapers for severe widespread cases (poison ivy involving > 10% BSA classically warrants 2–3 week taper), cool compresses, and barrier repair emollients.
08 Psoriasis Inflammatory
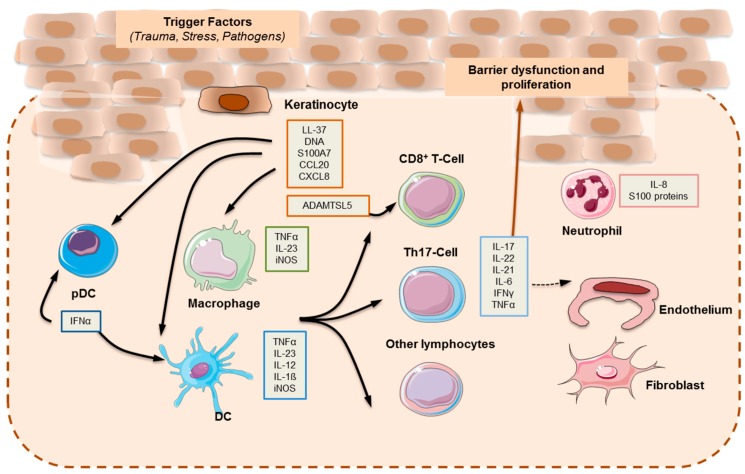
Psoriasis is a chronic, immune-mediated, inflammatory disease of the skin and joints driven by a dysregulated IL-23/Th17 axis. Affected keratinocytes proliferate at roughly 7 times the normal rate, producing the characteristic thick silvery scale on an erythematous base. It affects approximately 2–3% of the US population and is strongly associated with cardiometabolic comorbidity, depression, inflammatory bowel disease, and up to 30% risk of psoriatic arthritis.
Clinical Variants
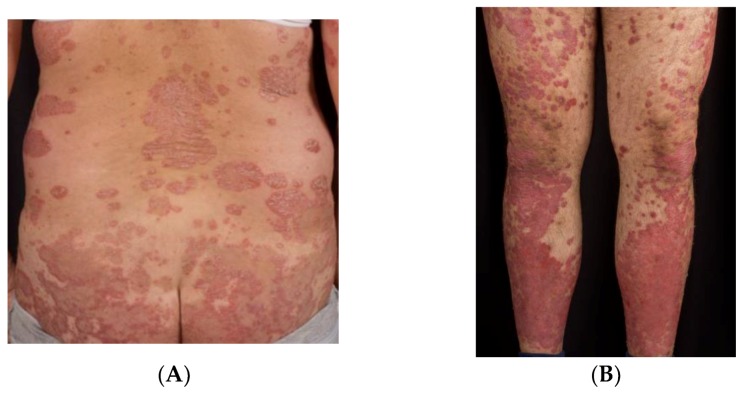
Chronic plaque psoriasis (80–90%) — well-demarcated, symmetric erythematous plaques with silvery scale on scalp, extensor elbows/knees, lumbosacral back, and umbilicus. Guttate psoriasis — small "drop-like" papules, often post-streptococcal in children/young adults. Inverse psoriasis — smooth, shiny, erythematous plaques without scale in skin folds (axillae, groin, inframammary). Pustular psoriasis — sterile pustules on erythematous base (generalized GPP or palmoplantar PPP). Erythrodermic psoriasis — > 90% BSA erythema, dermatologic emergency with risk of hypothermia, high-output heart failure, and infection. Nail psoriasis — pitting, oil drops, subungual hyperkeratosis, onycholysis. Psoriatic arthritis — inflammatory arthritis with dactylitis, enthesitis, DIP involvement.
Management
Limited disease (< 5% BSA): topical corticosteroids, vitamin D analogs (calcipotriene), topical retinoids (tazarotene), calcineurin inhibitors for face/folds, combination calcipotriene/betamethasone, coal tar, anthralin. Moderate-to-severe (≥ 5–10% BSA or functional impairment): phototherapy (NB-UVB, PUVA), systemic agents, or biologics.
The AAD/NPF guidelines on biologics for psoriasis stratify by target: TNF-α inhibitors (adalimumab, etanercept, infliximab, certolizumab), IL-12/23 inhibitor (ustekinumab), IL-17 inhibitors (secukinumab, ixekizumab, brodalumab, bimekizumab), and IL-23 inhibitors (guselkumab, risankizumab, tildrakizumab). Oral systemics include methotrexate, cyclosporine (short-term rescue), acitretin, apremilast (PDE-4), and deucravacitinib (TYK2).
Severity is measured with BSA (body surface area, palm = 1%), the PASI (Psoriasis Area and Severity Index, 0–72, based on erythema, induration, scale × BSA in 4 body regions), the IGA (0–4 Investigator Global Assessment), and DLQI (Dermatology Life Quality Index, 0–30, patient-reported).
09 Seborrheic Dermatitis Inflammatory
Seborrheic dermatitis is a chronic, relapsing eruption characterized by erythematous patches with greasy yellow scale in sebum-rich areas: scalp (dandruff), eyebrows, nasolabial folds, ears, central chest, and intertriginous zones. It is driven by an inflammatory response to Malassezia yeast. It is more common and more severe in Parkinson's disease, HIV/AIDS (often the first cutaneous sign), and stroke patients. Infantile "cradle cap" is the pediatric form.
Management: antifungal shampoos and creams (ketoconazole 2%, selenium sulfide, zinc pyrithione, ciclopirox), low-potency topical steroids for flares, topical calcineurin inhibitors for facial involvement (steroid-sparing for chronic use). Counsel patients that this is chronic and relapsing, not curable.
10 Hidradenitis Suppurativa & Urticaria Inflammatory
Hidradenitis Suppurativa (HS)
HS is a chronic, recurrent, debilitating inflammatory disease of terminal hair follicles in apocrine-bearing skin (axillae, groin, inframammary, gluteal folds). Lesions progress from painful inflammatory nodules to abscesses, draining sinus tracts, and hypertrophic scarring. Severity is graded with Hurley staging: Stage I — isolated nodules/abscesses without sinus tracts or scarring; Stage II — recurrent abscesses with sinus tracts and scarring, single or multiple lesions separated by normal skin; Stage III — diffuse involvement with multiple interconnected sinus tracts and abscesses across an entire area, no normal skin between lesions. Treatment includes topical clindamycin, oral tetracyclines, clindamycin + rifampin combination, adalimumab (FDA-approved for moderate-to-severe HS), secukinumab (FDA-approved 2023), hormonal therapy in women, and surgical deroofing or wide excision for Hurley III.

Urticaria (Hives)
Urticaria is characterized by transient wheals (edematous papules/plaques) that individually resolve within 24 hours without residual marks, often accompanied by angioedema. Acute urticaria (< 6 weeks) is usually infection-, medication-, or food-triggered; chronic urticaria (≥ 6 weeks) is most often idiopathic (CSU, chronic spontaneous urticaria). Treatment is second-generation H1 antihistamines (cetirizine, loratadine, fexofenadine, levocetirizine) at standard dose, escalating up to 4× dose, then adding H2 blockers, leukotriene antagonists, and finally omalizumab (anti-IgE) for refractory CSU. Never dismiss hives with throat swelling or respiratory symptoms — that is anaphylaxis and requires epinephrine.
11 Drug Eruptions, SJS/TEN & DRESS Emergency
Cutaneous drug reactions range from trivial to life-threatening. The morbilliform (maculopapular) drug eruption is by far the most common, appearing 7–14 days after a new medication as a symmetric, pruritic, blanching erythematous eruption on the trunk that spreads centrifugally. Usually self-limited on withdrawal.

Stevens-Johnson Syndrome (SJS) / Toxic Epidermal Necrolysis (TEN): A spectrum of full-thickness epidermal necrosis with mucosal involvement (oral, ocular, genital). SJS = < 10% BSA detachment, SJS/TEN overlap = 10–30%, TEN = > 30%. Classic culprits: allopurinol, lamotrigine, carbamazepine, phenytoin, sulfonamides, nevirapine, NSAIDs (oxicams). Patients present with flu-like prodrome, then painful erythema with targetoid lesions that evolve into flaccid bullae and sheet-like epidermal detachment. Nikolsky sign positive. Mortality correlates with SCORTEN score (age > 40, malignancy, HR > 120, BSA > 10%, BUN > 28, glucose > 252, bicarbonate < 20). Management: ICU or burn unit, immediate withdrawal of culprit, supportive care, wound care, ophthalmology consultation.
DRESS (Drug Reaction with Eosinophilia and Systemic Symptoms): Delayed 2–8 weeks after drug start. Presents with diffuse morbilliform eruption, fever, facial edema, lymphadenopathy, eosinophilia, atypical lymphocytes, and internal organ involvement (hepatitis most common, also nephritis, myocarditis, pneumonitis). Classic culprits: allopurinol, anticonvulsants, sulfonamides, vancomycin, minocycline. Management: withdraw drug, systemic corticosteroids, monitor for reactivation and late thyroiditis.
12 Melanoma Neoplastic
Melanoma is a malignant tumor arising from melanocytes, responsible for the majority of skin cancer mortality despite representing only about 1% of cutaneous malignancies. Early detection is life-saving: thin melanomas (< 1 mm Breslow depth) have > 95% 5-year survival, while thick metastatic disease has historically had single-digit survival (though checkpoint inhibitors have dramatically improved outcomes).

Subtypes
Superficial spreading melanoma (≈ 70%, radial growth phase, trunk in men and legs in women), nodular melanoma (≈ 15%, vertical growth from the start, often amelanotic, worst prognosis for thickness at diagnosis), lentigo maligna melanoma (chronically sun-damaged skin of the head and neck in older adults, slow horizontal growth), acral lentiginous melanoma (palms, soles, subungual — most common subtype in Black, Asian, and Hispanic patients; not related to sun exposure), and rare variants (desmoplastic, mucosal, uveal).
A — Asymmetry: one half does not mirror the other. B — Border irregularity: scalloped, notched, or poorly defined. C — Color variegation: multiple shades of brown, black, red, white, or blue. D — Diameter: > 6 mm (the size of a pencil eraser), though smaller melanomas exist. E — Evolution: any change in size, shape, color, symptoms (itch, bleed, pain).
The "ugly duckling" sign — a lesion that looks different from all the patient's other moles — is sometimes more sensitive than ABCDE, especially in patients with many atypical nevi.
Tumor thickness (Breslow depth) measured in millimeters from the top of the granular layer to the deepest tumor cell is the single most important prognostic factor. T-stage thresholds per AJCC 8th edition melanoma staging:
| T stage | Thickness | Ulceration |
|---|---|---|
| Tis | Melanoma in situ (confined to epidermis) | N/A |
| T1a | < 0.8 mm | Without ulceration |
| T1b | < 0.8 mm with ulceration, or 0.8–1.0 mm | ± Ulceration |
| T2 | > 1.0–2.0 mm | a without / b with ulceration |
| T3 | > 2.0–4.0 mm | a without / b with ulceration |
| T4 | > 4.0 mm | a without / b with ulceration |
Historical Clark levels (I epidermis only, II into papillary dermis, III filling papillary dermis, IV into reticular dermis, V into subcutis) are largely supplanted by Breslow depth but still appear on older path reports.
Management
Initial biopsy should be full-thickness (excisional or broad shave to subcutis) to ensure accurate Breslow measurement — never a partial or superficial shave on a suspected melanoma. Definitive treatment after diagnosis follows AAD melanoma guidelines and NCCN melanoma guidelines: wide local excision with margins based on Breslow (in situ 0.5–1.0 cm, < 1 mm → 1 cm, 1–2 mm → 1–2 cm, > 2 mm → 2 cm). Sentinel lymph node biopsy is offered for T1b and above. Systemic therapy for advanced disease includes immune checkpoint inhibitors (nivolumab, pembrolizumab, ipilimumab/nivolumab combination, relatlimab) and targeted therapy for BRAF V600-mutant disease (dabrafenib/trametinib, encorafenib/binimetinib).
13 Basal Cell Carcinoma (BCC) Neoplastic
BCC is the most common human cancer, arising from the basal layer of the epidermis and driven by chronic UV exposure and mutations in the Hedgehog signaling pathway (PTCH1, SMO). It rarely metastasizes but can be locally aggressive and destructive, especially in high-risk anatomic sites.

Subtypes
Nodular BCC (60%) — pearly papule with rolled borders, central ulceration ("rodent ulcer"), arborizing telangiectasias; face. Superficial BCC — erythematous scaly patch often mistaken for eczema; trunk. Morpheaform (sclerosing/infiltrative) BCC — scar-like indurated plaque, ill-defined borders, aggressive subclinical extension; Mohs is the treatment of choice. Pigmented BCC — more common in darker skin types; can mimic melanoma. Basosquamous — hybrid with more aggressive behavior.
Treatment per the AAD BCC guidelines depends on subtype, size, location, and patient factors. Options: standard excision with 4 mm margins (low-risk), Mohs micrographic surgery (high-risk lesions, face/ears/H-zone, recurrent, aggressive histology, > 2 cm trunk/extremity), electrodesiccation and curettage (ED&C) for small superficial/nodular on trunk/extremities (not on terminal-hair-bearing areas), cryotherapy, topical 5-FU or imiquimod for superficial BCC, photodynamic therapy, and radiation for non-surgical candidates. Advanced/metastatic BCC can be treated with hedgehog pathway inhibitors (vismodegib, sonidegib) and PD-1 inhibitors (cemiplimab).
14 Squamous Cell Carcinoma (SCC) & Actinic Keratosis Neoplastic
Actinic Keratosis (AK)
AKs are precancerous proliferations of atypical keratinocytes on chronically sun-damaged skin, presenting as rough, scaly, pink or skin-colored macules/papules on the face, scalp, dorsal hands, forearms, and ears. Often better felt than seen ("sandpaper" quality). Approximately 0.1–10% per lesion per year progress to invasive SCC, but the cumulative field risk is the concern. Treatment: cryotherapy (lesion-directed), field therapy with topical 5-fluorouracil, imiquimod, tirbanibulin, diclofenac, or photodynamic therapy.
Squamous Cell Carcinoma
Invasive SCC arises from full-thickness atypical keratinocytes and has real (though low in most cases) metastatic potential. SCC in situ (Bowen's disease) is a well-demarcated erythematous scaly plaque confined to the epidermis. Invasive SCC presents as indurated, hyperkeratotic, friable, tender papules or nodules on sun-exposed skin; ulceration is common. Keratoacanthoma is a rapidly growing dome-shaped nodule with central keratin plug, now generally considered a well-differentiated SCC variant.
Factors that define high-risk SCC per AAD SCC guidelines: diameter ≥ 2 cm, depth > 2 mm or beyond subcutaneous fat, location on ear/lip/temple/genitalia, poor differentiation, perineural invasion (≥ 0.1 mm nerves), lymphovascular invasion, recurrent tumor, immunosuppression (organ transplant recipients have 65–250× increased SCC risk), and arising in scar/chronic wound (Marjolin ulcer).
Treatment mirrors BCC: standard excision 4–6 mm margins for low-risk, Mohs for high-risk or cosmetically sensitive, ED&C for small low-risk lesions, radiation for non-surgical candidates. Locally advanced or metastatic cutaneous SCC is treated with PD-1 inhibitors (cemiplimab, pembrolizumab). Screening: USPSTF 2023 skin cancer screening recommendations concluded current evidence is insufficient (I statement) to recommend for or against routine visual skin exam in asymptomatic adults.
15 Benign Neoplasms & Dysplastic Nevi Neoplastic
Dermatologists spend a significant portion of every clinic reassuring patients about benign lesions and distinguishing them from malignancies. A working vocabulary is essential.
| Lesion | Description |
|---|---|
| Seborrheic keratosis | "Stuck-on" waxy brown papule, warty surface; very common after age 40; benign |
| Melanocytic nevus (mole) | Junctional (flat), compound (slightly raised), or intradermal (dome-shaped); symmetric and stable |
| Dysplastic (atypical) nevus | Features overlapping with melanoma; marker of increased melanoma risk; monitored or biopsied |
| Halo nevus | Nevus with surrounding hypopigmentation from immune response |
| Blue nevus | Dermal dendritic melanocytes producing a blue hue from Tyndall effect |
| Dermatofibroma | Firm pink-brown papule, "dimple sign" on lateral compression; benign |
| Cherry angioma | Bright red dome papule, vascular, benign |
| Skin tag (acrochordon) | Pedunculated soft flesh-colored papule in skin folds |
| Lipoma | Soft mobile subcutaneous nodule of mature adipocytes |
| Epidermoid cyst | Dome-shaped cyst with central punctum, contains keratin; "sebaceous cyst" is a misnomer |
| Pyogenic granuloma | Rapidly growing friable red papule, bleeds easily; lobular capillary hemangioma |
| Lentigo | Flat brown macule from chronic sun exposure ("age spot", "liver spot") |
Dysplastic nevus syndrome (familial atypical multiple mole melanoma, FAMMM) describes patients with > 50 nevi, several atypical, and a family history of melanoma. These patients warrant dermoscopy-guided surveillance every 3–12 months and often total body photography for change detection.
16 Alopecia (AGA, Areata, Scarring) Hair/Nails
Androgenetic alopecia (AGA) is the most common cause of hair loss, driven by sensitivity of scalp hair follicles to dihydrotestosterone (DHT). Male pattern: bitemporal recession and vertex thinning (Norwood-Hamilton scale I–VII). Female pattern: diffuse central thinning with preserved frontal hairline (Ludwig I–III). Treatment: topical minoxidil 2–5%, oral finasteride 1 mg (men), oral dutasteride, oral minoxidil low-dose, spironolactone (women), PRP injections, hair transplant.
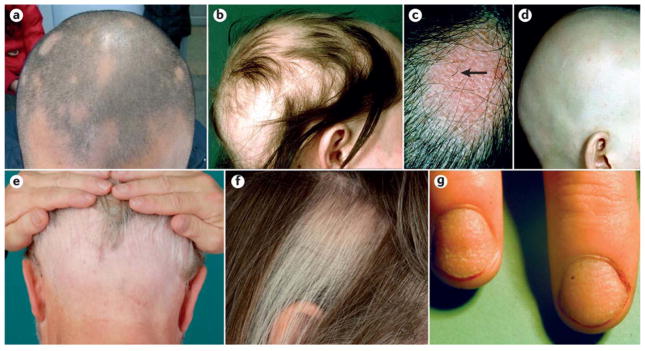
Alopecia areata is an autoimmune, non-scarring hair loss producing smooth round patches of complete hair loss with "exclamation point hairs" at the margins. Can progress to alopecia totalis (entire scalp) or alopecia universalis (entire body). Treatment: intralesional triamcinolone (first-line for patchy disease), topical/oral steroids, topical minoxidil, topical immunotherapy (squaric acid), and FDA-approved oral JAK inhibitors (baricitinib, ritlecitinib, deuruxolitinib).
Telogen effluvium is diffuse non-scarring shedding 2–3 months after a trigger (childbirth, severe illness, surgery, crash diet, new medication, thyroid disease); typically self-resolves.
Scarring (cicatricial) alopecia destroys the follicle permanently. Subtypes include central centrifugal cicatricial alopecia (CCCA, common in Black women), frontal fibrosing alopecia (postmenopausal women, frontal hairline and eyebrows), lichen planopilaris, and discoid lupus erythematosus. These are dermatologic urgencies in the sense that early treatment can arrest progression but cannot restore lost follicles.
17 Bullous Diseases & Connective Tissue Disease Autoimmune
Bullous Diseases
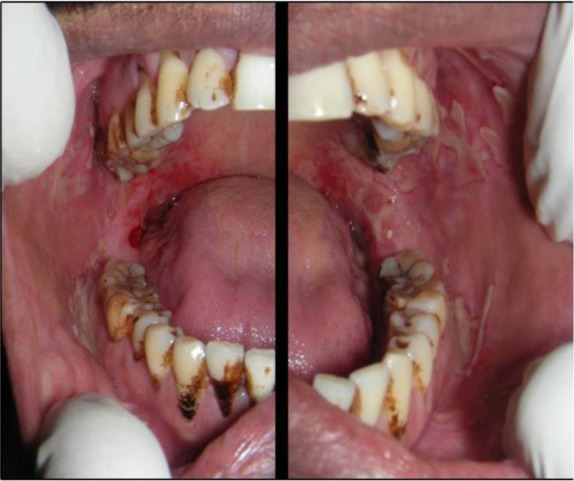
Pemphigus vulgaris — autoantibodies (IgG) against desmoglein 3 (and sometimes 1) cause intraepidermal acantholysis, producing flaccid bullae and painful erosions with prominent oral mucosal involvement. Nikolsky sign positive. Direct immunofluorescence (DIF) shows intercellular "chicken wire" IgG deposition. Treatment: high-dose corticosteroids, rituximab (now first-line), azathioprine, mycophenolate. Untreated mortality is high.
Bullous pemphigoid — autoantibodies against BP180 and BP230 hemidesmosomal proteins cause subepidermal split, producing tense bullae on erythematous or urticarial base, typically in elderly patients. Less mucosal involvement. DIF shows linear IgG and C3 at the basement membrane zone. Treatment: topical clobetasol, oral steroids, doxycycline + niacinamide, rituximab, dupilumab (emerging).

Dermatitis herpetiformis — intensely pruritic grouped vesicles on extensor surfaces (elbows, knees, buttocks) associated with celiac disease. IgA deposition at dermal papillae. Treatment: gluten-free diet and dapsone.
Connective Tissue Disease in Skin
Cutaneous lupus erythematosus has three major subtypes: acute CLE (malar "butterfly" rash of SLE, photosensitive), subacute CLE (annular or psoriasiform plaques on sun-exposed skin, strong Ro/SSA association), and chronic CLE / discoid LE (scarring plaques with follicular plugging, dyspigmentation, atrophy, scarring alopecia). Treatment: sun protection, topical steroids, topical calcineurin inhibitors, antimalarials (hydroxychloroquine), immunosuppressants.

Dermatomyositis — heliotrope rash (violaceous eyelid discoloration), Gottron papules (violaceous papules over DIP/PIP/MCP joints), shawl sign, V-sign, holster sign, mechanic's hands, nailfold telangiectasias + proximal muscle weakness. Screen for underlying malignancy in adults.
Systemic sclerosis (scleroderma) — skin thickening, Raynaud phenomenon, digital ulcers, sclerodactyly, telangiectasias, calcinosis cutis. Limited (CREST) vs diffuse subtypes with distinct antibody profiles.
18 Cutaneous Infections & Infestations Infectious
Viral
Warts (HPV): common (verruca vulgaris), plantar, flat, and anogenital (condyloma acuminatum). Treatment: cryotherapy, salicylic acid, imiquimod, cantharidin, intralesional candida antigen, laser. Molluscum contagiosum: pox virus producing umbilicated pearly papules, common in children and immunocompromised. Treatment: cantharidin, curettage, cryotherapy, or watchful waiting. HSV: grouped vesicles on erythematous base (HSV-1 orolabial, HSV-2 genital). Tzanck smear shows multinucleated giant cells. Treatment: acyclovir, valacyclovir, famciclovir. Varicella-zoster (shingles): dermatomal vesicular eruption. Treatment within 72 hours with valacyclovir 1 g TID × 7 days. Shingrix vaccine reduces incidence and postherpetic neuralgia.

Fungal
Tinea (dermatophytosis) — capitis, corporis, cruris, pedis, unguium (onychomycosis), manuum, barbae. KOH preparation shows septate branching hyphae. Topical antifungals (terbinafine, clotrimazole, ketoconazole) for limited disease; oral terbinafine or itraconazole for tinea capitis, extensive disease, or onychomycosis. Tinea versicolor (Malassezia) — hypo- or hyperpigmented scaly patches on trunk; "spaghetti and meatballs" on KOH. Topical selenium sulfide, ketoconazole, or oral fluconazole. Candidiasis — intertriginous, diaper, oral thrush. Topical nystatin, clotrimazole, or oral fluconazole.

Bacterial
Impetigo — honey-crusted erosions, most commonly S. aureus or S. pyogenes; topical mupirocin or oral cephalexin. Cellulitis / erysipelas — warm, erythematous, tender, ill-defined plaques (cellulitis) or sharply demarcated plaques with raised border (erysipelas). Folliculitis — follicle-based pustules; hot tub (Pseudomonas), bacterial (S. aureus), pityrosporum. Abscess / furuncle / carbuncle — incision and drainage is primary treatment.
Infestations
Scabies — intensely pruritic eruption (worse at night) with burrows in interdigital webs, wrists, axillae, waist, genitalia. Permethrin 5% cream (overnight, repeat in 1 week) or oral ivermectin. Treat household contacts and wash bedding. Pediculosis (head, body, pubic lice) — permethrin, malathion, spinosad, oral ivermectin. Bed bugs — linear "breakfast, lunch, dinner" bites; environmental eradication.
19 Dermatologic Procedures — A to Z Procedures
Procedures are the backbone of a dermatology clinic day. A typical half-day may involve a dozen biopsies, several cryotherapy treatments, a Mohs case, and injections. Know the procedural vocabulary cold.
| Procedure | Description & Indication |
|---|---|
| Shave biopsy | Flexible blade removes epidermis and variable dermis; for exophytic or superficial lesions (BCC, SCC, AK, seborrheic keratosis). Not for suspected melanoma if depth matters. |
| Saucerization (deep shave) | Deep saucer-shaped shave through dermis; used for pigmented lesions to capture full depth. |
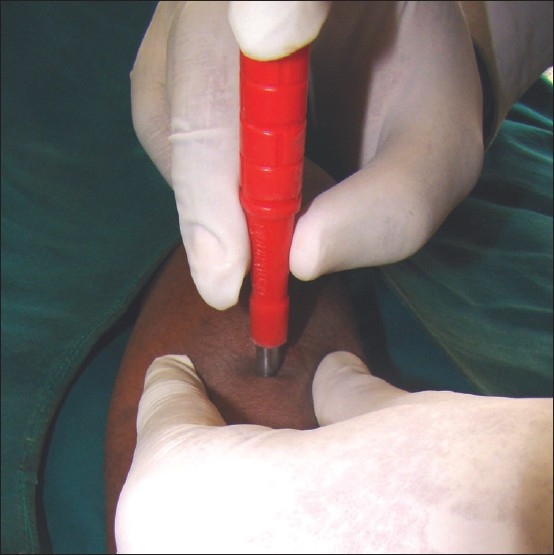
| Punch biopsy | Cylindrical blade (2–8 mm) takes full-thickness cylinder of skin through subcutis. For inflammatory dermatoses, DIF, full-thickness sampling. Closed with single suture or second-intention. |
| Excisional biopsy | Elliptical full-thickness excision with defined margins; 3:1 length-to-width ratio for primary closure. For suspected melanoma, complete removal. |
| Incisional biopsy | Partial full-thickness sample of a large lesion when excisional biopsy is impractical. |
| Electrodesiccation & curettage (ED&C) | Scrape friable tumor with curette, desiccate with hyfrecator; 2–3 cycles. Low-risk superficial/nodular BCC and small SCC on trunk/extremities. Leaves hypopigmented scar. |
| Cryotherapy | Liquid nitrogen (-196 °C) freeze via spray or cotton-tip. AKs, warts, SKs, molluscum, superficial BCC. Freeze times 5–30 seconds depending on target. |
| Mohs micrographic surgery | Tissue-sparing excision with real-time frozen-section margin evaluation by the Mohs surgeon. Highest cure rates (> 98% for primary BCC/SCC). Indicated for high-risk anatomic sites, aggressive histology, recurrent tumors, large lesions, and immunosuppressed patients per AUC Mohs appropriate use criteria. |
| Intralesional triamcinolone | Kenalog 2.5–40 mg/mL injected into alopecia areata patches, keloids, hypertrophic scars, cystic acne, granuloma annulare, lichen planus. |
| Phototherapy | NB-UVB (311 nm) or PUVA (psoralen + UVA) for psoriasis, AD, vitiligo, CTCL, pruritus. Booth-based; 2–3 sessions/week. |
| Photodynamic therapy (PDT) | Topical photosensitizer (5-ALA or MAL) activated by blue or red light. Field therapy for AKs and superficial BCC. |
| Laser | PDL (vascular — telangiectasias, PWS, rosacea), IPL, Nd:YAG (deep vascular, hair), CO₂ (ablative resurfacing, rhinophyma), fractional resurfacing, Q-switched (tattoo, pigment), ruby/alexandrite (hair removal). |
| Chemical peels | Superficial (glycolic, salicylic, Jessner's), medium (TCA 35%), deep (phenol) — for photodamage, melasma, AKs, acne. |
| Patch testing | Allergens applied to back under occlusion × 48 h, read at days 2, 4, 7. For suspected allergic contact dermatitis. |
| Wood's lamp | 365 nm UV — highlights vitiligo, tinea versicolor (yellow fluorescence), tinea capitis (certain species), porphyria cutanea tarda urine (coral red), erythrasma (coral red). |
For every biopsy, your note must capture: site (specific anatomic location), size (mm), type of biopsy, anesthetic (lidocaine 1% with epi, volume), specimen sent to pathology, hemostasis (aluminum chloride, electrocautery, pressure), closure (none / suture type and number), and post-procedure instructions. A common running template: "Site marked, photographed, consented. Cleansed with chlorhexidine. Local anesthesia with 1% lidocaine with epinephrine. Shave biopsy performed with DermaBlade. Hemostasis achieved with aluminum chloride. Specimen to dermpath. Wound care instructions given."
20 Biopsy Interpretation & Pathology Reports Diagnostics
Dermpath reports arrive 3–10 days after biopsy and are reviewed by the attending at every follow-up. You will document the path result in the assessment and plan, and you must be able to recognize the vocabulary.
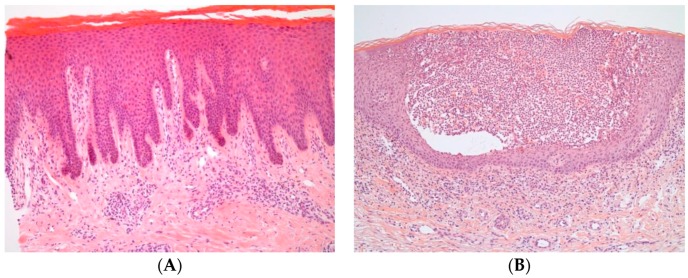
Acanthosis — thickening of the stratum spinosum (psoriasis, chronic eczema). Hyperkeratosis — thickening of the stratum corneum. Parakeratosis — retained nuclei in stratum corneum (psoriasis). Spongiosis — intercellular edema of the epidermis (eczema). Acantholysis — loss of keratinocyte-keratinocyte adhesion (pemphigus). Atypia — abnormal cellular morphology. Dysplasia — disordered growth, graded mild/moderate/severe. Perineural invasion (PNI) — tumor along nerves, adverse feature in SCC. Ulceration — loss of epidermis over tumor, upstages melanoma and SCC. Solar elastosis — background sun damage in dermis. Lichenoid infiltrate — band-like lymphocytic infiltrate at DEJ (lichen planus, lupus). Granulomatous — macrophage aggregates (granuloma annulare, sarcoid).
Melanoma pathology reports specifically include: Breslow depth (mm), Clark level, ulceration status, mitotic rate (per mm²), lymphovascular invasion, perineural invasion, microsatellites, regression, tumor-infiltrating lymphocytes, and margin status. Every one of these is relevant to staging and treatment decisions.
For non-melanoma skin cancer path, document: histologic subtype (e.g., "superficial BCC," "infiltrative BCC," "moderately differentiated SCC"), depth of invasion, PNI, LVI, and peripheral and deep margin status (clear, positive, close).
21 Medications You Must Know Medications
Topical Corticosteroid Potency Classes
| Class | Potency | Examples |
|---|---|---|
| I | Super-potent | Clobetasol 0.05%, halobetasol 0.05%, betamethasone dipropionate 0.05% (augmented) |
| II | High | Fluocinonide 0.05%, mometasone furoate 0.1% ointment, desoximetasone 0.25% |
| III | High–mid | Triamcinolone acetonide 0.5%, betamethasone valerate 0.1% ointment |
| IV | Mid | Triamcinolone acetonide 0.1%, mometasone furoate cream, fluocinolone 0.025% |
| V | Mid–low | Hydrocortisone valerate 0.2%, betamethasone valerate 0.1% cream |
| VI | Low | Desonide 0.05%, alclometasone 0.05%, fluocinolone 0.01% |
| VII | Least potent | Hydrocortisone 1%, 2.5% (OTC / face-safe) |
Vehicle matters: ointments are most potent (occlusive), creams mid-potency, lotions/solutions/foams best for scalp and hair-bearing areas. Never use Class I on face, eyelids, or intertriginous zones for more than a few days due to atrophy, telangiectasia, striae, and HPA axis suppression.
Key Medication Classes
| Class | Agents | Use |
|---|---|---|
| Topical retinoids | Tretinoin, adapalene, tazarotene, trifarotene | Acne, AKs, photodamage, psoriasis |
| Systemic retinoids | Isotretinoin, acitretin | Severe acne (iso), psoriasis (acitretin); both teratogenic |
| Calcineurin inhibitors | Tacrolimus ointment, pimecrolimus cream | AD, vitiligo, facial steroid-sparing |
| PDE-4 inhibitors | Crisaborole (topical), apremilast (oral), roflumilast (topical) | AD, psoriasis |
| JAK inhibitors (topical) | Ruxolitinib cream, topical tofacitinib | AD, vitiligo |
| JAK inhibitors (oral) | Upadacitinib, abrocitinib, baricitinib, deuruxolitinib, ritlecitinib | AD, alopecia areata, vitiligo — boxed warnings |
| TNF-α biologics | Adalimumab, etanercept, infliximab, certolizumab | Psoriasis, HS, PsA |
| IL-17 biologics | Secukinumab, ixekizumab, brodalumab, bimekizumab | Psoriasis, PsA, HS |
| IL-23 biologics | Guselkumab, risankizumab, tildrakizumab | Psoriasis, PsA |
| IL-12/23 | Ustekinumab | Psoriasis, PsA, IBD |
| IL-4/13 biologics | Dupilumab (anti-IL-4Rα), tralokinumab, lebrikizumab (anti-IL-13) | AD, asthma, nasal polyps, EoE |
| Antifungals | Terbinafine, itraconazole, fluconazole, griseofulvin; topical clotrimazole, ketoconazole, ciclopirox | Dermatophytes, yeast, onychomycosis |
| Antivirals | Acyclovir, valacyclovir, famciclovir | HSV, VZV |
| Antibiotics (derm) | Doxycycline, minocycline, cephalexin, clindamycin, TMP-SMX, mupirocin | Acne, rosacea, cellulitis, impetigo |
| Antihistamines | Cetirizine, loratadine, fexofenadine, hydroxyzine, diphenhydramine, doxepin | Urticaria, pruritus |
| Immunosuppressants | Methotrexate, cyclosporine, mycophenolate, azathioprine, rituximab | Autoimmune/bullous disease, severe inflammatory disease |
22 Classification Systems & Fitzpatrick Scale Classification
| Type | Description | Sunburn / Tan Response |
|---|---|---|
| I | Pale white skin, red/blond hair, blue eyes, freckles | Always burns, never tans |
| II | White skin, fair-haired, blue/green/hazel eyes | Burns easily, tans poorly |
| III | Cream-white / light brown | Burns sometimes, tans gradually |
| IV | Moderate brown (Mediterranean) | Burns minimally, tans easily |
| V | Dark brown | Rarely burns, tans darkly |
| VI | Deeply pigmented dark brown/black | Never burns, deeply pigmented |
Scored 0–72. Four body regions (head, upper extremities, trunk, lower extremities) each scored 0–4 for erythema, induration, and scale, then weighted by area involvement (0 = none to 6 = 90–100%) and regional multiplier (head 0.1, UE 0.2, trunk 0.3, LE 0.4). A "PASI 75" response (75% reduction from baseline) has historically been the benchmark for clinical trial success; PASI 90 and PASI 100 are now standard with modern biologics.
EASI (Eczema Area and Severity Index): 0–72, modeled after PASI with four regions scored for erythema, induration/edema, excoriation, and lichenification. IGA (Investigator Global Assessment): 0 clear, 1 almost clear, 2 mild, 3 moderate, 4 severe — used across psoriasis, AD, acne, and rosacea trials. SCORAD combines extent, intensity, and subjective symptoms. POEM is the patient-reported outcome.
Hurley staging for HS (I–III, see Section 10). Norwood-Hamilton for male AGA (I–VII). Ludwig for female AGA (I–III). SALT score for alopecia areata (Severity of Alopecia Tool, 0–100% scalp hair loss). SCORTEN for SJS/TEN mortality. AJCC TNM for melanoma and non-melanoma skin cancer. BWH (Brigham & Women's) staging for cutaneous SCC. CEAP for chronic venous disease (overlap with vascular). Clark levels I–V for melanoma (historical). Breslow depth categories (see Section 12).
22b Physical Exam & Dermoscopy Essentials Exam
The dermatologic physical exam is equal parts pattern recognition and systematic technique. Every new patient should have a baseline TBSE offered; every established patient gets a focused exam with TBSE updated annually or more often for high-risk patients (personal melanoma history, multiple atypical nevi, organ transplant, CLL, xeroderma pigmentosum).
Fitzpatrick skin type: ___ Photodamage: mild/moderate/severe
Scalp: _____ Face/ears: _____
Neck/chest: _____ Abdomen/back: _____
Upper extremities (incl. axillae, palms): _____
Lower extremities (incl. soles, interdigital): _____
Genitalia / gluteal cleft: offered / examined / deferred
Nails / mucous membranes: _____
Hair: density, pattern, pull test
Lesions of concern: [list with site, size, morphology, plan]
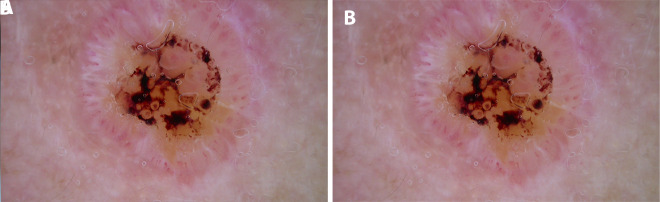
Dermoscopy (a handheld polarized magnifier, often 10×) is now standard of care for pigmented lesion evaluation and is increasingly used for non-pigmented lesions, hair, nails, and inflammatory dermatoses. Features you may hear dictated: pigment network (regular honeycomb = benign; atypical/irregular = concerning), globules, streaks, blue-white veil (regression), negative network, chrysalis structures, milia-like cysts and comedo-like openings (seborrheic keratosis), arborizing vessels (BCC), strawberry pattern (facial AK), parallel ridge pattern (acral melanoma), and the 7-point checklist or 3-point checklist for pigmented lesion scoring.

You will often hear the attending narrate dermoscopy findings out loud: "atypical pigment network, focal blue-white veil, irregular dots and globules at the periphery, positive for at least 3 of the 7-point checklist — biopsy." Capture these verbatim when possible; they belong in the procedure indication and the path requisition.
23 Abbreviations Master List Reference
Diagnoses & Conditions
Procedures & Exam
Medications
23b Risk Factors & Comorbidities Risk
Dermatology diagnoses rarely exist in isolation. Skin cancer is driven by cumulative UV exposure, immunosuppression, and genetics; inflammatory dermatoses are tightly linked to systemic disease. Capturing risk factors is a core scribe responsibility.
UV exposure history: Lifetime sunburns (especially blistering in childhood), outdoor occupation, tanning bed use (number of sessions, age of first use — each session < age 35 raises melanoma risk), sunscreen habits, protective clothing.
Phototype & genetic factors: Fitzpatrick I–II, red/blond hair, blue/green eyes, freckling, family history of melanoma or non-melanoma skin cancer, personal history of skin cancer, xeroderma pigmentosum, Gorlin (basal cell nevus) syndrome, albinism, dysplastic nevus syndrome.
Immunosuppression: Organ transplant (SCC risk 65–250×, BCC 10×, melanoma 2–4×), chronic CLL/lymphoma, HIV, long-term systemic steroids, TNF and IL-23 inhibitors (minor increase), azathioprine (photocarcinogenic metabolite).
Psoriasis/PsA comorbidities: Cardiometabolic disease (MI, stroke, metabolic syndrome), obesity, NAFLD, inflammatory bowel disease, uveitis, depression, alcohol use disorder.
Atopic dermatitis comorbidities: Asthma, allergic rhinitis, food allergy, EoE, anxiety/depression, increased skin infection risk.
HS comorbidities: Obesity, smoking, metabolic syndrome, PCOS, IBD, spondyloarthropathy, depression.
Dermatomyositis: Screen for underlying internal malignancy (ovarian, gastric, lung, colorectal, NHL) in adults, especially at diagnosis and for 3 years after.
24 Sample HPI Templates & References Templates
These templates show the kind of documentation expected in a dermatology clinic note. Use them as frameworks to internalize the rhythm and content of a good derm HPI.
"Ms. [Name] is a 24-year-old female with Fitzpatrick type IV skin presenting for evaluation of adult-onset acne. She reports a 2-year history of inflammatory papules and pustules predominantly involving the jawline, chin, and lower cheeks, with premenstrual flaring. She denies scalp involvement or scarring but endorses post-inflammatory hyperpigmentation. Prior treatments include OTC salicylic acid wash and adapalene 0.1% gel with minimal improvement. No prior oral antibiotics or isotretinoin. Menstrual cycles are regular; she is on no contraceptive currently. Denies hirsutism, alopecia, or galactorrhea. PCOS has not been evaluated. On exam, approximately 12 inflammatory papules and 4 deep tender nodules distributed along the jawline bilaterally, scattered closed comedones on the forehead, and multiple PIH macules. IGA 3 (moderate)."
"Mr. [Name] is a 58-year-old male with Fitzpatrick type II skin, personal history of 30+ lifetime sunburns, recreational boating, and a family history of melanoma (father) who presents for evaluation of a changing mole on the left upper back noted by his wife 3 months ago. He reports the lesion has grown from the size of a pencil eraser to approximately 9 mm, has darkened unevenly, and occasionally itches but does not bleed. On dermoscopy-assisted exam, there is a 9 mm asymmetric pigmented macule with irregular notched borders, variegated brown-to-black pigmentation with a small area of blue-gray regression, and an atypical pigment network. Ugly duckling sign positive compared to his other nevi. TBSE otherwise reveals 14 banal compound nevi and scattered solar lentigines. Plan: broad shave (saucerization) biopsy of the left upper back lesion today."
"Mrs. [Name] is a 36-year-old woman with a lifelong history of atopic dermatitis, asthma, and allergic rhinitis (the full atopic triad) presenting with a 3-week flare of generalized pruritic eczematous dermatitis. Flare began during a period of work stress and coincided with switching to a new laundry detergent. She reports intense nocturnal itching disrupting sleep 5 nights per week, EASI pre-visit estimated at 18, BSA approximately 25%. Current regimen: triamcinolone 0.1% ointment BID to body (used daily for 3 weeks), hydrocortisone 2.5% to face, CeraVe cream twice daily. She is not currently on systemic therapy, has not tried dupilumab, and has no prior phototherapy. No recent infections, no fever. On exam, lichenified and excoriated erythematous patches in antecubital and popliteal fossae, diffuse xerosis, eyelid involvement with Dennie-Morgan lines, and scattered excoriations on the trunk. No honey crusts or pustules."
"Mr. [Name] is a 45-year-old man with moderate-to-severe chronic plaque psoriasis, psoriatic arthritis, and metabolic syndrome, established on risankizumab 150 mg SQ every 12 weeks since January 2025. He is here for routine 3-month follow-up. He reports near-complete clearance of his previously extensive plaques (baseline BSA 22%, PASI 16; today BSA < 1%, PASI 1), resolved scalp involvement, and significant improvement in joint symptoms (previously DIP swelling and enthesitis). No adverse events, no infections, no injection site reactions. Latest labs: TB screen negative, hepatitis panel non-reactive, CBC and CMP within normal limits. PHQ-2 negative. On exam, faint post-inflammatory erythema at prior plaque sites on bilateral elbows and lumbosacral back; scalp, nails, and intertriginous areas clear. IGA 1 (almost clear). DLQI 2."
"Ms. [Name] is a 62-year-old woman referred urgently from primary care for evaluation of a new rash. She was started on allopurinol 300 mg daily 18 days ago for asymptomatic hyperuricemia. Eight days ago she developed a pruritic eruption on the trunk that has spread to involve the extremities and now the face, accompanied by subjective fevers to 100.8 °F, facial swelling, and general malaise. She denies oral ulcers, eye pain, dysphagia, or skin pain. On exam, diffuse morbilliform erythematous eruption covering approximately 60% BSA, facial edema (especially periorbital), cervical lymphadenopathy, no bullae, no mucosal involvement, Nikolsky sign negative. Labs obtained today: eosinophilia 1,800/μL, AST 145, ALT 180, creatinine 1.2 (baseline 0.8). Assessment: probable DRESS syndrome secondary to allopurinol. Plan: immediate discontinuation of allopurinol, systemic prednisone 1 mg/kg, admission to medicine for monitoring, hepatology and nephrology consultation, counsel patient on lifelong avoidance of allopurinol and cross-reactive agents."
References & Sources
NCCN Clinical Practice Guidelines in Oncology: Melanoma: Cutaneous. 2023.
Figure 1: Structure of the skin. OpenStax College. CC BY 3.0.
Figure 2: Detailed skin anatomy. BruceBlaus / Blausen Medical. CC BY 3.0.
Figure 3: Acne vulgaris. Roshu Bangal via Wikimedia Commons. CC BY-SA 4.0.
Figure 4: Plaque psoriasis on back. Bobjgalindo via Wikimedia Commons. CC BY-SA 4.0.
Figure 5: Cutaneous melanoma. National Cancer Institute. Public domain.
Figure 6: Nodular basal cell carcinoma. Klaus D. Peter via Wikimedia Commons. CC BY 3.0 DE.
The best dermatology scribes are fluent in morphology. When the attending dictates "6 mm asymmetric pigmented macule with variegated color and irregular borders on the left upper back," a great scribe immediately knows this is a melanoma-rule-out that will get a saucerization biopsy, already has the pathology follow-up in mind, and knows to capture the ABCDE features in the note. When the attending says "moderate plaque psoriasis, BSA 12%, PASI 14, failed topicals, start risankizumab," the scribe understands the biologic class, the dosing schedule, the baseline labs needed (TB screen, hepatitis panel, CBC, CMP), and the counseling points to document.
Dermatology moves fast — a high-volume clinic can see 40–60 patients per day with multiple procedures woven between visits. Efficiency is built on pre-charting prior biopsies and pathology results, on pattern recognition for the common conditions, on procedural templates you can drop and customize in seconds, and on a true understanding of the medicine so you can anticipate rather than react.
Read the pathology reports before the attending walks in. Pre-populate biopsy notes with site, size, and technique templates. Know the biologics by brand name and dose interval because patients will ask. Learn the difference between a Mohs candidate and a standard excision candidate so you can stage the note appropriately.
Welcome to dermatology. The visual learning curve is steep but the rhythm is deeply satisfying once you internalize it.