Emergency Medicine
Every chief complaint, diagnosis, procedure, medication, score, and documentation framework you need to survive your first ED shift and thrive beyond it.
All diagrams on this page are sourced from published educational or institutional materials rather than AI generation. Each figure caption links to the original source, and the full diagram and guideline citations are collected in the references section at the bottom.
01 ED Flow, Triage & Core Principles
The emergency department is unlike any other clinical environment. Patients arrive undifferentiated, acuity ranges from life-threatening to trivial within the same hallway, and documentation must capture a rapidly changing clinical picture in real time. Every ED encounter begins with a single organizing question: Is this patient sick or not sick? Everything downstream — triage level, room assignment, workup tempo, disposition — flows from that judgment.
The ED Encounter Flow
A typical ED visit proceeds through predictable stages. At arrival, the patient is triaged by a nurse who assigns an acuity level, captures vital signs, and performs a focused chief-complaint assessment. The patient is then placed in a room (or the hallway during surge) and seen by the clinician (physician, PA, or NP). A history and physical is performed, initial orders are placed (labs, imaging, medications), and reassessments occur as results return. The encounter ends in a disposition decision: discharge home, admit to an inpatient service, transfer to a higher level of care, observe in an ED observation unit, leave against medical advice, or — rarely — expire in the department.
The Emergency Severity Index (ESI)
US emergency departments overwhelmingly use the five-level Emergency Severity Index for triage. The ESI is a rapid sorting algorithm based on acuity and anticipated resource use.
| Level | Acuity | Examples |
|---|---|---|
| ESI 1 | Requires immediate life-saving intervention | Cardiac arrest, unresponsive, severe respiratory distress, major trauma in shock |
| ESI 2 | High risk, confused/lethargic, severe pain/distress, or abnormal vitals in the danger zone | Chest pain concerning for ACS, stroke symptoms, sepsis, suicidal ideation with plan |
| ESI 3 | Stable but requires many resources (≥ 2) | Abdominal pain needing labs + imaging, moderate asthma needing nebs + CXR |
| ESI 4 | Stable, one resource needed | Simple laceration needing sutures, UTI needing urinalysis + antibiotics |
| ESI 5 | Stable, no resources needed | Medication refill, suture removal, simple rash |
A "resource" in ESI terms is anything beyond history, physical exam, and point-of-care testing — labs, imaging, IV fluids, IV medications, specialty consultation, and procedures all count. ESI 2 patients deserve immediate bedding and physician evaluation; ESI 1 patients bypass normal triage entirely and go straight to the resuscitation bay. Scribes do not assign ESI levels, but understanding them is essential to anticipating the tempo of a case (AHRQ ESI Implementation Handbook).
ABCs and the Primary Survey
Every acutely ill patient is first assessed by ABCDE: Airway (patent? protected? at risk?), Breathing (rate, effort, oxygenation, breath sounds), Circulation (pulse, BP, perfusion, bleeding control), Disability (GCS, pupils, gross neuro), Exposure (fully undress, check for occult injury, prevent hypothermia). This is the core framework for both medical resuscitation and trauma. You will hear the team move through it out loud during every trauma activation and code.
In the ED, every resuscitation note should document the ABCDE survey even if some components are grossly normal. "Airway: patent, self-protecting. Breathing: RR 18, sats 99% on room air, clear bilaterally. Circulation: strong radial pulse, warm well-perfused, no external bleeding. Disability: GCS 15. Exposure: fully examined, no additional injuries." That single paragraph shows medical decision-making and is far more valuable than a sparse vitals block.
02 Scribe Documentation Framework
The ED Note Structure
ED notes resemble SOAP but are heavily weighted toward the HPI, medical decision-making (MDM), and the course/reassessment sections. The note must show that the clinician considered life-threatening diagnoses, ruled in or ruled out each by history, exam, labs, and imaging, and justified the disposition.
Chief Complaint: The single presenting problem in the patient's words or a short medical phrase. "Chest pain," "fell from ladder," "shortness of breath."
HPI: Use OPQRST — Onset, Provocation/palliation, Quality, Radiation, Severity, Timing. Then add the complaint-specific high-yield elements (e.g., for chest pain: exertional component, associated dyspnea/diaphoresis/nausea; for headache: thunderclap quality, neck stiffness, fever; for abdominal pain: migration, bilious vomiting, BRBPR).
Pertinent positives and negatives: An ED HPI explicitly documents the absence of red flags. "Denies back pain, lower-extremity weakness, saddle anesthesia, urinary retention, or bowel incontinence" is the right way to close out a back-pain HPI.
PMH/PSH/Meds/Allergies/Social/Family: Captured briefly but must include anticoagulants, antiplatelets, immunosuppression, prior cardiac/vascular/neurologic disease, substance use, and any prior similar presentations.
Vitals: Initial vitals, worst vitals, and final vitals. Always flag abnormal values. Repeat vitals after any intervention.
Physical exam: Focused but complete for the complaint. Every trauma patient gets a full head-to-toe. Every abdominal pain patient gets a complete abdominal exam plus rectal if indicated. Every stroke alert gets a NIHSS.
Results: Document specific numeric values (troponin, lactate, creatinine, hemoglobin, WBC, INR, HCG, pH, lactate) and imaging findings verbatim from the radiology read. Note whether reads are preliminary or final.
The MDM is the heart of the ED note. It lists the differential diagnoses considered, what was done to evaluate each, the rationale for the working diagnosis, and the disposition. Under 2023 E/M guidelines, the MDM (not the bullet count) drives the level of service. A strong MDM explicitly names the "can't miss" diagnoses, risk stratification tools used (HEART score, Wells, PERC, PECARN, qSOFA), and the reasoning that led to disposition.
The phrase "shared decision-making" is a magic one in ED charting. If the attending discusses risks, benefits, and alternatives with the patient and the patient participates in the disposition choice (e.g., declining admission for low-risk chest pain), always document it explicitly. It protects the physician and reflects modern ED practice.
03 Chest Pain & Cardiovascular Emergencies Cardiovascular
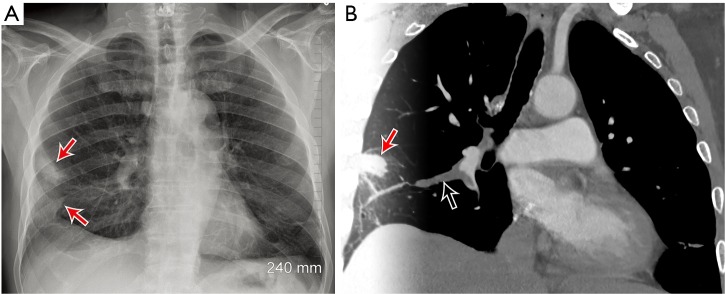
Chest pain is one of the highest-volume and highest-liability complaints in the ED. The scribe must anticipate documentation of six "can't miss" diagnoses: acute coronary syndrome (ACS), pulmonary embolism (PE), aortic dissection, tension pneumothorax, cardiac tamponade, and esophageal rupture (Boerhaave).
Acute Coronary Syndrome (ACS)
ACS is a spectrum ranging from unstable angina to NSTEMI (non-ST-elevation MI) to STEMI (ST-elevation MI). The pathophysiology is atherosclerotic plaque rupture with thrombus formation in a coronary artery, producing downstream myocardial ischemia or infarction. Classic presentation is substernal pressure radiating to the left arm or jaw, with diaphoresis, nausea, and dyspnea. Atypical presentations are common in women, diabetics, and the elderly — isolated dyspnea, fatigue, or epigastric discomfort. The ED workup is a 12-lead EKG within 10 minutes of arrival, serial high-sensitivity troponins, CXR, and risk stratification.
STEMI is defined by new ST elevation ≥ 1 mm in two contiguous limb leads or ≥ 2 mm in contiguous precordial leads (or a new LBBB with Sgarbossa criteria). STEMI triggers emergent cath lab activation with a door-to-balloon goal of ≤ 90 minutes. NSTEMI and unstable angina are managed with dual antiplatelet therapy (aspirin + a P2Y12 inhibitor), anticoagulation (heparin), nitrates, beta-blockers, and high-intensity statin, with risk-stratified timing of cardiac catheterization (2021 ACC/AHA Chest Pain Evaluation Guideline).
The HEART score is the dominant risk-stratification tool for ED chest pain. It incorporates History, EKG, Age, Risk factors, and Troponin, each scored 0–2, for a total of 0–10. Low score (0–3) predicts < 2% 30-day MACE and supports discharge; moderate (4–6) warrants observation; high (≥ 7) warrants admission and early invasive workup.
Pulmonary Embolism (PE)
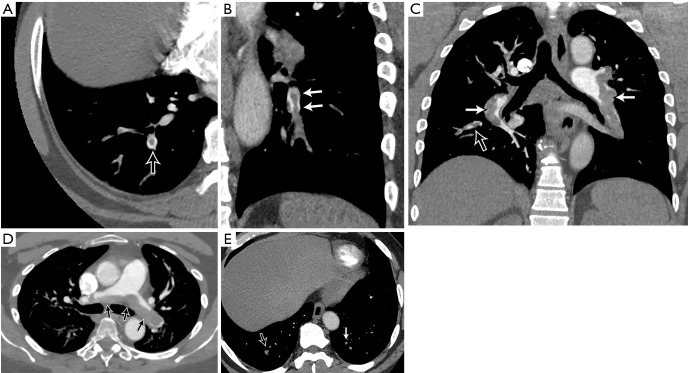
PE is thrombus (usually from a DVT) that embolizes to the pulmonary arteries, producing V/Q mismatch, hypoxemia, and, when large, right heart strain and obstructive shock. Classic presentation is pleuritic chest pain, dyspnea, tachycardia, hypoxia, and leg swelling — but the "classic" tetrad is rarely all present. The ED uses the Wells score and PERC rule to stratify pre-test probability. Low pre-test probability + PERC-negative rules out PE without testing; otherwise, D-dimer (with age-adjusted cutoff) or CT pulmonary angiogram (CTPA) is used. Massive PE with shock is treated with systemic thrombolytics (tPA) or thrombectomy; submassive and stable PE are treated with anticoagulation (heparin, LMWH, or a DOAC) (2019 ESC PE Guidelines).
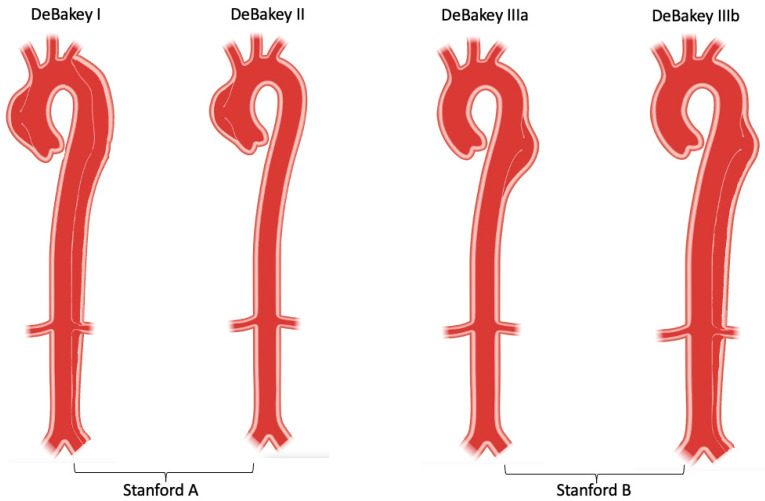
Aortic Dissection
Dissection is a tear in the aortic intima allowing blood to propagate through a false lumen within the aortic wall. The Stanford classification divides dissections into Type A (involves the ascending aorta — surgical emergency) and Type B (descending aorta only — medical management with impulse control). Classic presentation is sudden, tearing, maximal-at-onset chest or back pain with a BP differential between arms, widened mediastinum on CXR, and sometimes neurologic or limb ischemic findings. Diagnosis is by CT angiogram of the chest/abdomen/pelvis. Medical management focuses on aggressive BP and heart rate control with IV beta-blockers (esmolol, labetalol), targeting SBP 100–120 and HR < 60.
Cardiac Arrest & ACLS
Cardiac arrest management follows the AHA ACLS algorithm (2020 AHA Guidelines for CPR and ECC): high-quality chest compressions (100–120/min, depth 2–2.4 inches, full recoil, minimal interruptions), early defibrillation for shockable rhythms (VF/pulseless VT), airway management, IV/IO access, and pharmacologic therapy. Epinephrine 1 mg IV/IO every 3–5 minutes is given for all arrests. Amiodarone 300 mg (then 150 mg) or lidocaine is added for refractory VF/VT. Reversible causes are addressed via the "Hs and Ts": Hypovolemia, Hypoxia, Hydrogen ion (acidosis), Hypo/hyperkalemia, Hypothermia, Tension pneumothorax, Tamponade, Toxins, Thrombosis (pulmonary), Thrombosis (coronary). ROSC (return of spontaneous circulation) triggers post-arrest care: targeted temperature management, advanced hemodynamic support, and identification of the underlying etiology.
Arrhythmias
Unstable tachycardia (hypotension, altered mental status, chest pain, signs of shock) is treated with synchronized cardioversion. Stable SVT is treated with vagal maneuvers followed by adenosine 6 mg IV push (then 12 mg). Atrial fibrillation with RVR is managed with rate control (diltiazem, metoprolol) or rhythm control depending on duration and stability. Stable VT is treated with amiodarone, procainamide, or lidocaine. Unstable bradycardia is treated with atropine 1 mg IV, then transcutaneous pacing, then dopamine or epinephrine infusion.
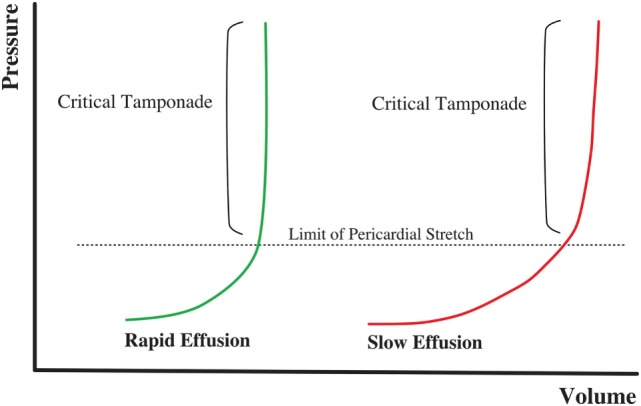
Tension Pneumothorax & Tamponade
Tension pneumothorax is a clinical diagnosis: hypotension, tracheal deviation, absent breath sounds, JVD, respiratory distress. Treatment is immediate needle decompression in the 2nd intercostal space at the midclavicular line (or 4th/5th at the anterior axillary line per ATLS 10th edition) followed by tube thoracostomy. Cardiac tamponade classically presents with Beck's triad (hypotension, JVD, muffled heart sounds); POCUS shows a pericardial effusion with RV diastolic collapse. Treatment is emergent pericardiocentesis.
Sudden/tearing onset, maximum severity at onset, radiation to back, BP differential between arms, syncope, exertional component, hemoptysis, diaphoresis, new murmur, pulsus paradoxus, hypoxia, tachycardia out of proportion to vitals, unilateral leg swelling, recent surgery or immobilization, active cancer, pregnancy, known clotting disorder.
04 Dyspnea & Respiratory Emergencies Pulmonary
Dyspnea is the complaint — the underlying diagnosis could be cardiac, pulmonary, metabolic, toxicologic, or neuromuscular. The ED differential focuses on CHF exacerbation, COPD exacerbation, asthma, pneumonia, PE, pneumothorax, and, increasingly, COVID-19.
Acute Decompensated Heart Failure (CHF)
Classic presentation is orthopnea, paroxysmal nocturnal dyspnea, bibasilar crackles, elevated JVP, peripheral edema, and a positive BNP. CXR shows cephalization, Kerley B lines, perihilar infiltrates, and possibly pleural effusions. POCUS shows B-lines and a plethoric IVC. Treatment is preload reduction with IV loop diuretics (furosemide), afterload reduction with nitroglycerin, non-invasive ventilation (BiPAP) for respiratory distress, and treatment of the precipitant (ischemia, dysrhythmia, dietary indiscretion, medication non-adherence).
COPD & Asthma Exacerbations
COPD exacerbations present with increased dyspnea, cough, and sputum production in a patient with known COPD. Treatment is bronchodilators (albuterol + ipratropium nebs), systemic steroids (prednisone 40 mg PO or methylprednisolone IV), antibiotics if Anthonisen criteria met, and non-invasive ventilation for hypercapnic respiratory failure. Asthma exacerbations are treated with continuous albuterol, ipratropium, IV/IM epinephrine or terbutaline in severe cases, magnesium sulfate IV (2 g over 20 min), systemic steroids, and NIV or intubation if failing. Peak flow measurements guide severity and response.
Pneumonia
Community-acquired pneumonia (CAP) presents with fever, cough, sputum, pleuritic chest pain, and focal lung findings. CXR shows lobar or multifocal infiltrates. CURB-65 and PSI scores guide disposition. Empiric therapy per IDSA guidelines: outpatient healthy patients get amoxicillin or doxycycline; inpatient non-ICU gets a beta-lactam + macrolide or respiratory fluoroquinolone; ICU patients get beta-lactam + macrolide or fluoroquinolone, with MRSA and Pseudomonas coverage added for specific risk factors (2019 ATS/IDSA CAP Guidelines).
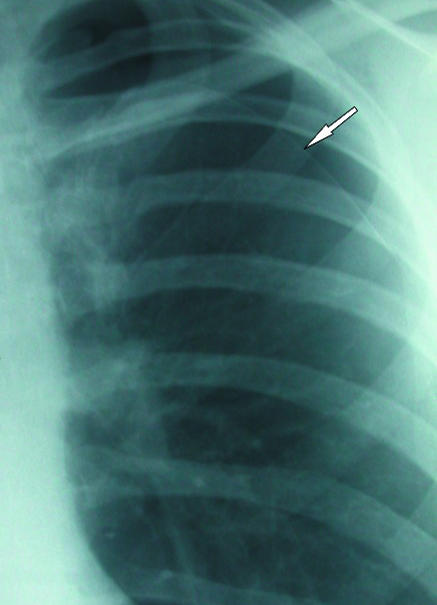
Pneumothorax
Spontaneous pneumothorax occurs in tall, thin young males or patients with underlying lung disease (COPD bullae). Presents with sudden pleuritic chest pain and dyspnea, decreased breath sounds, hyperresonance. Diagnosis is by CXR or POCUS (absent lung sliding). Small, stable primary pneumothoraces may be observed; larger or symptomatic ones are managed with needle aspiration, pigtail catheter, or chest tube.
05 Abdominal Pain & GI Emergencies GI/GU
Abdominal pain is the single highest-volume complaint in most EDs. The scribe must recognize the geography of the complaint and the "can't miss" diagnoses lurking behind it: appendicitis, cholecystitis, pancreatitis, small bowel obstruction (SBO), AAA rupture, mesenteric ischemia, perforated viscus, ectopic pregnancy, and ovarian/testicular torsion.
Appendicitis
Classic presentation is periumbilical pain migrating to the right lower quadrant, anorexia, nausea, low-grade fever, and focal RLQ tenderness at McBurney's point. Rovsing, psoas, and obturator signs may be present. WBC is usually elevated. Diagnosis is confirmed by CT abdomen/pelvis with IV contrast (adults) or ultrasound (children, pregnancy). Treatment is surgical (laparoscopic appendectomy); uncomplicated cases may be managed with antibiotics alone in selected patients.
Cholecystitis & Biliary Disease
Biliary colic presents with post-prandial RUQ pain lasting 2–6 hours. Acute cholecystitis adds fever, leukocytosis, Murphy's sign, and sonographic findings of gallbladder wall thickening, pericholecystic fluid, and a sonographic Murphy's sign. Choledocholithiasis (stone in the CBD) elevates bilirubin, alk phos, and transaminases; ERCP is required. Ascending cholangitis is defined by Charcot's triad (RUQ pain, fever, jaundice) or Reynolds' pentad (adds hypotension and altered mental status) and requires emergent biliary decompression and broad-spectrum antibiotics.
Pancreatitis
Diagnosis requires 2 of 3: characteristic epigastric pain radiating to the back, lipase > 3× upper limit of normal, or imaging findings. The most common causes are gallstones and alcohol (remember "I GET SMASHED"). Severity is assessed with BISAP or Ranson criteria. Treatment is aggressive IV fluids (Lactated Ringer's), pain control, and treatment of the underlying cause. CT is reserved for severe cases or when the diagnosis is uncertain.
Small Bowel Obstruction (SBO)
Presents with crampy abdominal pain, bilious vomiting, distension, and obstipation. The most common cause is adhesions from prior abdominal surgery. CT shows dilated loops of bowel proximal to a transition point with decompressed bowel distally. Management is NPO, NG tube decompression, IV fluids, and surgical consult. Signs of strangulation (fever, peritonitis, lactic acidosis, leukocytosis) mandate emergent laparotomy.
AAA Rupture
Classic triad is hypotension, back or flank pain, and a pulsatile abdominal mass. Most patients do not have the full triad. Any older patient (especially male smoker) with syncope, back pain, and hypotension should get bedside ultrasound of the aorta immediately. Rupture is a surgical emergency with mortality > 50%.
Mesenteric Ischemia
Classic teaching is "pain out of proportion to exam" in an older patient with atrial fibrillation or atherosclerosis. Lactic acidosis is a late finding. CTA is the test of choice. Management is emergent vascular surgery or endovascular intervention; bowel resection is often required.
Perforation & Peritonitis
Viscus perforation (peptic ulcer, diverticulitis, appendicitis, cancer) presents with sudden, severe abdominal pain, rigidity, rebound tenderness, and free air on upright CXR or CT. Management is IV fluids, broad-spectrum antibiotics, and emergent surgery.
Ectopic Pregnancy & Ovarian Torsion
Any female of reproductive age with abdominal pain gets a urine pregnancy test. A positive HCG with no intrauterine pregnancy on ultrasound raises concern for ectopic, particularly if HCG is above the discriminatory zone (~1500–2000 mIU/mL). Ruptured ectopic presents with hypotension, shoulder pain (referred from hemoperitoneum), and positive FAST. Ovarian torsion presents with sudden, severe unilateral pelvic pain, nausea/vomiting, and adnexal tenderness; Doppler ultrasound shows reduced or absent ovarian flow.
Every female of reproductive age with abdominal pain needs a pregnancy test documented before imaging or analgesia, and every older patient with abdominal pain deserves an EKG (inferior MI frequently presents as epigastric pain). Document both explicitly.
06 Headache & Neurologic Emergencies Neuro
Subarachnoid Hemorrhage (SAH)
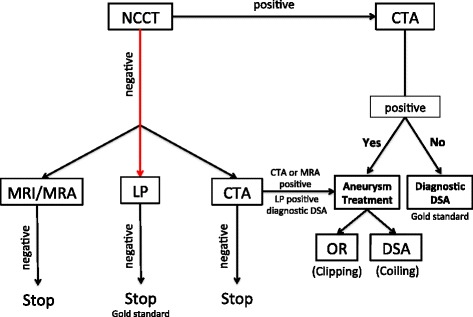
Classic presentation is a sudden, "thunderclap" headache, described as the "worst headache of my life," maximal at onset. Often associated with nausea, vomiting, neck stiffness, photophobia, and transient or persistent focal neurologic deficits. Non-contrast CT within 6 hours of symptom onset is > 98% sensitive; beyond 6 hours, LP is required to look for xanthochromia and RBCs that do not clear between tubes 1 and 4. CTA identifies the culprit aneurysm. Management includes BP control (target SBP < 140), reversal of anticoagulation if applicable, nimodipine for vasospasm prophylaxis, and emergent neurosurgical consult.
Meningitis
Classic triad is fever, nuchal rigidity, and altered mental status, though only a minority of patients have all three. Kernig and Brudzinski signs may be present. LP is required for diagnosis: bacterial shows high WBC (neutrophil predominant), high protein, low glucose; viral shows moderate WBC (lymphocyte predominant), normal glucose. Empiric antibiotics (ceftriaxone + vancomycin, adding ampicillin for Listeria coverage in neonates, elderly, or immunocompromised) and dexamethasone should be given before LP if LP is delayed for imaging (IDSA Bacterial Meningitis Guidelines).
Giant Cell Arteritis (GCA)
Older patient (> 50) with new unilateral temporal headache, jaw claudication, visual changes, and markedly elevated ESR/CRP. Untreated GCA can cause permanent blindness. Treatment is high-dose prednisone (60 mg PO) started immediately, before temporal artery biopsy confirms the diagnosis.
Migraine & Benign Headache
After ruling out dangerous causes, primary headaches are managed with IV fluids, antiemetics (metoclopramide, prochlorperazine), ketorolac, and sometimes dexamethasone to prevent recurrence. Triptans may be used in appropriate patients.
Cerebral Venous Sinus Thrombosis & Posterior Reversible Encephalopathy (PRES)
CVST presents with gradually worsening headache, papilledema, focal deficits, or seizures in patients with hypercoagulable states (pregnancy, OCPs, thrombophilia). Diagnosis is by MR venography or CT venography. Treatment is anticoagulation even in the presence of hemorrhagic transformation. PRES presents with headache, vision changes, and seizures in the setting of severe hypertension or immunosuppressive drugs; MRI shows posterior white matter vasogenic edema. Treatment is BP control and removal of offending agent.
Idiopathic Intracranial Hypertension (IIH)
Young, obese female with headache, transient visual obscurations, and papilledema. LP demonstrates elevated opening pressure with normal composition. Treatment is weight loss, acetazolamide, and, in severe cases, CSF diversion or optic nerve sheath fenestration.
07 Stroke, Weakness & Altered Mental Status Neuro
Acute Ischemic Stroke
Time is brain. Any patient with new focal neurologic deficit is a "stroke alert." The ED workflow is last known well (LKW) time, NIHSS, immediate non-contrast CT head (to exclude hemorrhage), point-of-care glucose (hypoglycemia mimics stroke), and consideration of IV thrombolytics (alteplase or tenecteplase within 4.5 hours of LKW) and mechanical thrombectomy for large vessel occlusion (within 24 hours for selected patients). BP is permissive up to 185/110 for tPA candidates (2019 AHA/ASA Acute Ischemic Stroke Guidelines).
A 15-item scale scored 0–42. Higher scores indicate more severe stroke. Items: 1a consciousness, 1b LOC questions, 1c LOC commands, 2 best gaze, 3 visual fields, 4 facial palsy, 5a/5b motor arm (L/R), 6a/6b motor leg (L/R), 7 limb ataxia, 8 sensory, 9 best language, 10 dysarthria, 11 extinction/neglect. Score 0 = normal; 1–4 = minor; 5–15 = moderate; 16–20 = moderate-severe; 21–42 = severe.
Intracerebral Hemorrhage (ICH)
Presents similarly to ischemic stroke but often with headache, vomiting, and rapid decline. CT shows hyperdense blood. Management includes aggressive BP control (target SBP < 140), reversal of any anticoagulant (vitamin K + 4F-PCC for warfarin, andexanet or PCC for DOACs, idarucizumab for dabigatran, protamine for heparin), and neurosurgical consult.
Altered Mental Status (AMS)
The AEIOU-TIPS mnemonic organizes the differential: Alcohol, Endocrine/Electrolytes/Encephalopathy, Insulin (hypo/hyperglycemia), Opiates/Overdose, Uremia, Trauma/Temperature, Infection, Psychiatric/Poisoning, Stroke/Seizure/Shock. Initial workup: glucose, vitals, exam, ABCs, labs (CBC, BMP, LFTs, ammonia, TSH, troponin), UA, tox screen, EKG, and CT head.
08 Syncope & Seizure Neuro
Syncope
Syncope is defined as transient loss of consciousness with spontaneous recovery. Causes are vasovagal (most common), orthostatic, cardiac (arrhythmia, structural), and neurologic (rare). ED workup includes EKG, orthostatics, glucose, and targeted workup based on history. The San Francisco Syncope Rule identifies high-risk patients (CHESS: CHF history, Hematocrit < 30, EKG abnormal, Shortness of breath, Systolic BP < 90 at triage); any positive criterion warrants admission. Cardiac syncope (especially exertional, without prodrome, or with family history of sudden death) requires cardiac telemetry admission.
Seizure & Status Epilepticus
First-time seizures need neuroimaging (CT or MRI), labs (glucose, electrolytes, calcium, magnesium, tox, pregnancy, anticonvulsant levels if applicable), and often EEG. Status epilepticus is a seizure lasting > 5 minutes or recurrent seizures without return to baseline. Management is a stepwise escalation: benzodiazepine (lorazepam 4 mg IV or midazolam 10 mg IM) → second-line antiepileptic (levetiracetam 60 mg/kg, fosphenytoin 20 mg/kg PE, or valproate 40 mg/kg) → intubation and continuous infusion (midazolam, propofol, or ketamine).
09 Sepsis, Fever & Infectious Emergencies Infectious
Sepsis & Septic Shock
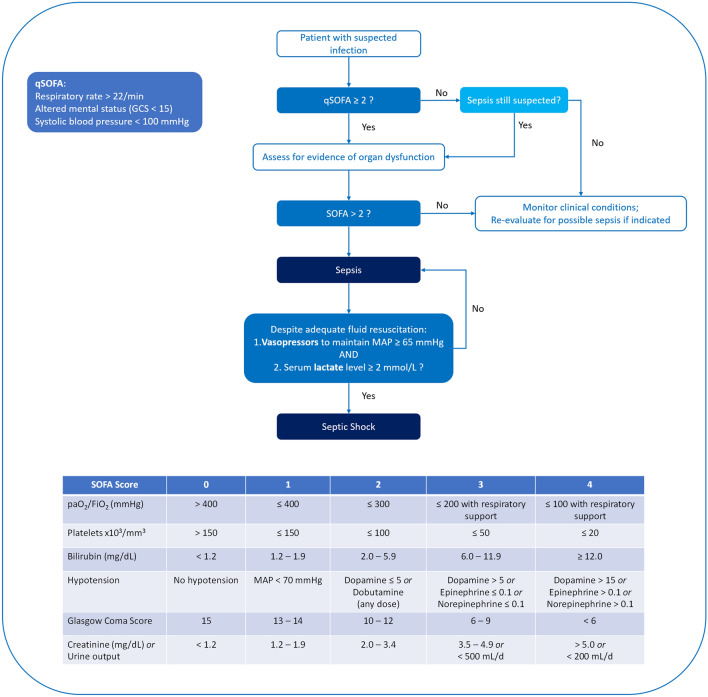
Sepsis is life-threatening organ dysfunction caused by a dysregulated host response to infection (Sepsis-3 definition). Septic shock is sepsis with persistent hypotension requiring vasopressors to maintain MAP ≥ 65 and a lactate > 2 mmol/L despite adequate fluid resuscitation. The qSOFA screening tool (RR ≥ 22, altered mentation, SBP ≤ 100) flags patients likely to have poor outcomes; ≥ 2 criteria prompts full sepsis workup. The Surviving Sepsis Campaign's 1-hour bundle includes measuring lactate, obtaining blood cultures before antibiotics, broad-spectrum antibiotics, 30 mL/kg crystalloid for hypotension or lactate ≥ 4, and vasopressors for persistent hypotension (Surviving Sepsis Campaign 2021 Guidelines).
Lactate measurement, blood cultures, broad-spectrum antibiotics, 30 mL/kg IV crystalloid, and vasopressors (norepinephrine first-line) — all within 1 hour of sepsis recognition. Scribes must document the exact time of each intervention for quality-metric tracking.
Urinary Tract Infection & Pyelonephritis
Uncomplicated cystitis presents with dysuria, frequency, and suprapubic pain in an otherwise healthy female. Treatment is nitrofurantoin, TMP-SMX, or fosfomycin. Pyelonephritis adds flank pain, fever, and systemic symptoms; treatment is ceftriaxone or fluoroquinolone, with admission for toxic appearance, pregnancy, or inability to tolerate PO.

Cellulitis & Necrotizing Fasciitis
Cellulitis is a superficial soft tissue infection with erythema, warmth, tenderness, and often fever. Treatment is cephalexin or clindamycin for outpatient, IV cefazolin or vancomycin for admission. Necrotizing fasciitis is a life-threatening deep infection with rapid progression, severe pain out of proportion to exam, crepitus, and systemic toxicity. LRINEC score helps risk-stratify. Treatment is emergent surgical debridement plus broad-spectrum antibiotics (piperacillin-tazobactam + vancomycin + clindamycin).
10 GI Bleeding & OB/GYN Emergencies GI/GU
Upper GI Bleed
Presents with hematemesis, coffee-ground emesis, or melena. Common causes: peptic ulcer disease, esophageal varices, Mallory-Weiss tear, gastritis, malignancy. Initial management: 2 large-bore IVs, type and crossmatch, fluid resuscitation, transfusion (target Hb 7 in stable patients, higher in cardiac disease), IV PPI (pantoprazole), IV octreotide and ceftriaxone if varices suspected, and urgent GI consult for endoscopy. The Glasgow-Blatchford score risk-stratifies for outpatient management.
Lower GI Bleed
Hematochezia in an older patient most often represents diverticular bleeding, angiodysplasia, ischemic colitis, hemorrhoids, or malignancy. In younger patients, consider IBD. Workup includes CBC, coags, type and screen, and colonoscopy or CT angiography for brisk bleeding.
Vaginal Bleeding in Pregnancy
First-trimester bleeding raises concern for threatened, inevitable, incomplete, or missed abortion, as well as ectopic. Workup: quantitative HCG, Rh type (RhoGAM if Rh-negative), pelvic ultrasound. Third-trimester bleeding raises concern for placental abruption and placenta previa — no vaginal exam until ultrasound rules out previa. OB consult is mandatory.
Postpartum Hemorrhage
Defined as blood loss > 500 mL after vaginal delivery or > 1000 mL after C-section. Causes are the "4 Ts": Tone (atony), Trauma (laceration), Tissue (retained products), Thrombin (coagulopathy). Management includes uterine massage, oxytocin, methylergonovine, carboprost, misoprostol, tranexamic acid, and emergent OB intervention.
11 Trauma — Head to Toe Trauma
Trauma documentation follows the ATLS framework: primary survey (ABCDE) with immediate life-saving interventions, secondary survey (head-to-toe exam with AMPLE history: Allergies, Medications, PMH, Last meal, Events), and tertiary survey (detailed re-examination once the patient is stable) (ATLS 10th Edition).
Head Trauma
TBI severity is graded by GCS: mild 13–15, moderate 9–12, severe ≤ 8 (intubate). CT head indications in adults use Canadian CT Head Rules or New Orleans Criteria; in children, PECARN. Epidural hematoma classically shows a lucid interval and a biconvex (lens-shaped) hyperdensity on CT. Subdural hematoma is crescent-shaped and may be acute (hyperdense) or chronic (hypodense). Elevated ICP is managed with head-of-bed elevation, hyperventilation (short-term), hypertonic saline or mannitol, and neurosurgical intervention.
| Eye (1–4) | Verbal (1–5) | Motor (1–6) |
|---|---|---|
| 4 Spontaneous 3 To voice 2 To pain 1 None | 5 Oriented 4 Confused 3 Inappropriate 2 Incomprehensible 1 None | 6 Obeys 5 Localizes 4 Withdraws 3 Flexion 2 Extension 1 None |
Total 3–15. GCS ≤ 8 = intubate.
Chest Trauma
Life-threatening injuries on primary survey ("deadly dozen"): airway obstruction, tension pneumothorax, open pneumothorax, massive hemothorax, flail chest, cardiac tamponade, traumatic aortic injury, tracheobronchial injury, myocardial contusion, esophageal injury, diaphragmatic rupture, pulmonary contusion. Initial evaluation includes CXR, eFAST, and CT chest for stable patients.
Abdominal & Pelvic Trauma
Blunt abdominal trauma is evaluated with FAST exam (free fluid), CT abdomen/pelvis with contrast if stable, or emergent laparotomy if unstable with positive FAST. Penetrating trauma (especially gunshot wounds) to the abdomen typically requires exploratory laparotomy. Pelvic fractures can cause massive retroperitoneal bleeding; pelvic binder and angioembolization may be life-saving.
Extremity & Spine Trauma
Document neurovascular status distal to any extremity injury (pulses, capillary refill, motor, sensation). Open fractures need immediate IV antibiotics, tetanus, and orthopedic consult. Compartment syndrome presents with the "5 P's" (pain out of proportion, paresthesia, pallor, pulselessness, paralysis) and is diagnosed by measuring compartment pressures; fasciotomy is definitive. Spinal immobilization decisions use NEXUS or Canadian C-spine Rule.
Imaging required if any high-risk factor (age ≥ 65, dangerous mechanism, paresthesia in extremities); if none, patient can attempt 45° rotation if any low-risk factor present (simple rear-end MVC, sitting in ED, ambulatory, delayed onset, no midline tenderness). Inability to rotate → image.
12 Burns, Environmental & Envenomation Environmental
Burns
Burns are classified by depth (superficial, partial-thickness, full-thickness) and by body surface area (BSA) using the Rule of Nines. Fluid resuscitation uses the Parkland formula: 4 mL × weight (kg) × %TBSA, with half given in the first 8 hours. Transfer to a burn center is indicated for > 10% TBSA partial-thickness, any full-thickness, burns to face/hands/feet/genitalia/major joints, electrical, chemical, inhalational, or circumferential burns.
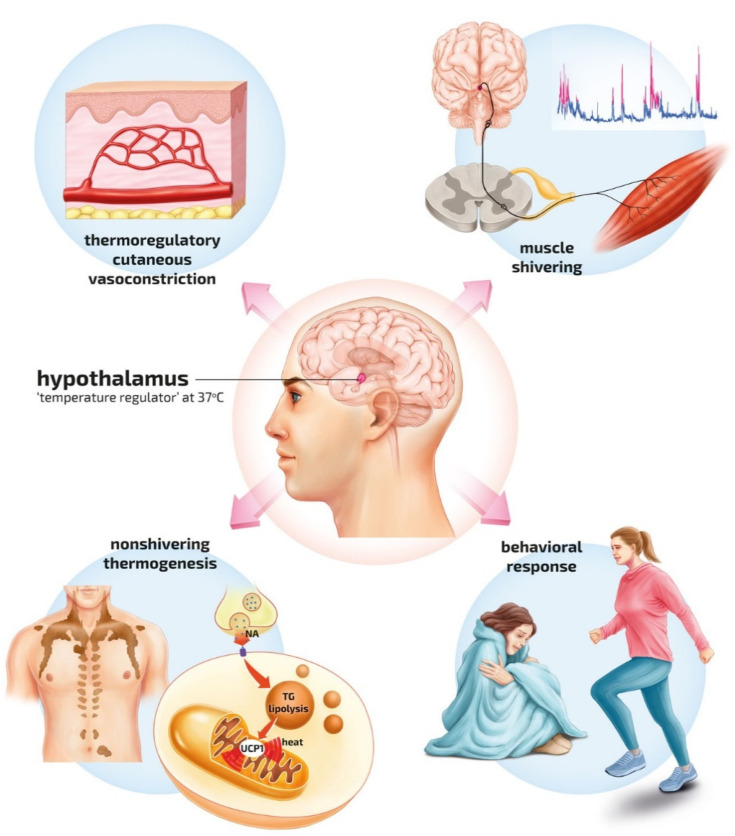
Hypothermia & Hyperthermia
Hypothermia is graded: mild 32–35°C, moderate 28–32°C, severe < 28°C. Rewarming is passive external, active external, or active internal (warm IV fluids, warm gastric/bladder lavage, ECMO for severe). Hyperthermia includes heat exhaustion and heat stroke (core temp > 40°C with CNS dysfunction); treatment is rapid cooling with evaporative or immersion techniques and supportive care.
Drowning
Initial management focuses on airway, ventilation, oxygenation, and warming. Any symptomatic patient is observed for delayed ARDS. Asymptomatic patients with normal vitals and exam after 4–6 hours of observation can be discharged.
Envenomation
North American pit viper bites (rattlesnake, copperhead, cottonmouth) cause local swelling, ecchymosis, coagulopathy, and thrombocytopenia. Treatment is CroFab antivenom for progressive envenomation. Black widow bites cause painful muscle cramping; treatment is analgesia, benzodiazepines, and occasionally antivenom. Brown recluse bites cause local necrosis; treatment is supportive.
13 Toxicology & Overdose Toxicology
The toxicology differential is organized by toxidrome: a recognizable clinical syndrome from a drug class.
| Toxidrome | Findings | Examples | Antidote/Treatment |
|---|---|---|---|
| Anticholinergic | Hot, dry, red, blind, mad ("mad as a hatter") | Diphenhydramine, TCAs, atropine | Physostigmine (select cases) |
| Cholinergic | SLUDGE/DUMBELS (salivation, lacrimation, urination, defecation, bradycardia) | Organophosphates, carbamates, nerve agents | Atropine + pralidoxime (2-PAM) |
| Sympathomimetic | Tachycardia, HTN, hyperthermia, mydriasis, diaphoresis, agitation | Cocaine, amphetamines, meth, bath salts | Benzodiazepines, cooling |
| Opioid | Respiratory depression, miosis, AMS | Heroin, fentanyl, oxycodone | Naloxone |
| Sedative-hypnotic | CNS depression, normal pupils, normal vitals | Benzodiazepines, alcohol, barbiturates | Supportive; flumazenil rarely |
| Serotonin syndrome | AMS, clonus (lower extremities), hyperreflexia, hyperthermia | SSRIs, MAOIs, tramadol, linezolid | Benzos, cyproheptadine, cooling |
Specific Overdoses
Acetaminophen: Rumack-Matthew nomogram at 4+ hours post-ingestion; N-acetylcysteine (NAC) is the antidote. Salicylate: tinnitus, mixed respiratory alkalosis + anion-gap metabolic acidosis; treatment is aggressive urinary alkalinization with bicarbonate and hemodialysis for severe toxicity. TCA overdose: wide QRS, hypotension, seizures; sodium bicarbonate is the antidote. Beta-blocker/CCB overdose: bradycardia and hypotension; treatment is glucagon, calcium, high-dose insulin euglycemia, lipid emulsion. Toxic alcohols (methanol, ethylene glycol): high osmolar gap, anion-gap metabolic acidosis; treatment is fomepizole and dialysis. Carbon monoxide: headache, confusion, cherry-red skin (rare); hyperbaric oxygen for severe cases. Cyanide: smoke inhalation with lactic acidosis; treatment is hydroxocobalamin.
Alcohol Withdrawal & Opioid Overdose
Alcohol withdrawal is scored with CIWA-Ar; treatment is symptom-triggered benzodiazepines (lorazepam, diazepam) and thiamine. Severe withdrawal can progress to delirium tremens and seizures. Opioid overdose is treated with naloxone (0.04–0.4 mg IV or 2–4 mg intranasal), titrated to respiratory rate, not level of consciousness.
14 Endocrine, Electrolyte & Metabolic Emergencies Metabolic
Diabetic Ketoacidosis (DKA)
Diagnostic triad: hyperglycemia (> 250), anion-gap metabolic acidosis (pH < 7.3, bicarbonate < 18), and ketonemia/ketonuria. Treatment is aggressive IV fluids (normal saline, then half-normal), insulin infusion (0.1 units/kg/hr after initial bolus), and potassium replacement (hold insulin if K < 3.3). Transition to subcutaneous insulin when the anion gap closes. Identify and treat the precipitant (infection, non-adherence, MI).
Hyperosmolar Hyperglycemic State (HHS)
Older Type 2 diabetics with glucose > 600, serum osmolality > 320, minimal ketosis, and profound dehydration and altered mental status. Treatment is similar to DKA but emphasizes fluid resuscitation over insulin.
Hyperkalemia
K > 5.5 with EKG changes (peaked T waves → PR prolongation → wide QRS → sine wave → VF) requires emergent treatment: calcium gluconate (membrane stabilization), insulin + D50 (shift K intracellularly), albuterol, bicarbonate if acidotic, and definitive removal with loop diuretics, potassium-binding resins (patiromer, SZC), or dialysis.
Diabetic Foot Infection & Euglycemic DKA
Diabetic foot infections range from superficial cellulitis to deep abscess and osteomyelitis. Imaging (plain films, MRI) and probe-to-bone testing guide the extent. Broad-spectrum antibiotics, surgical consult, and glycemic control. Euglycemic DKA (glucose < 250 with anion gap acidosis and ketosis) is increasingly seen with SGLT2 inhibitors and requires the same treatment as classic DKA.
Hypoglycemia
Glucose < 70 mg/dL in a symptomatic patient. Symptoms progress from adrenergic (tremor, diaphoresis, tachycardia) to neuroglycopenic (confusion, seizure, coma). Treatment: IV D50 (1 amp = 25 g) if IV access, glucagon 1 mg IM if no access, oral glucose if alert. Identify precipitants (insulin overdose, sulfonylureas, sepsis, adrenal insufficiency, alcohol). Sulfonylurea overdose requires prolonged observation and octreotide.
Other Key Electrolyte Emergencies
Hyponatremia: severe (Na < 120) with seizures or coma gets 3% saline bolus; correct no faster than 8–10 mEq/L per 24 hours to avoid osmotic demyelination. Hypocalcemia: Chvostek/Trousseau signs; IV calcium. Thyroid storm: fever, tachycardia, AMS, CHF in a hyperthyroid patient; treatment is beta-blocker, PTU/methimazole, iodine (1 hour after thionamide), hydrocortisone. Adrenal crisis: hypotension refractory to fluids; IV hydrocortisone 100 mg.
15 Anaphylaxis, Eye, ENT & Skin Emergencies Allergy/HEENT
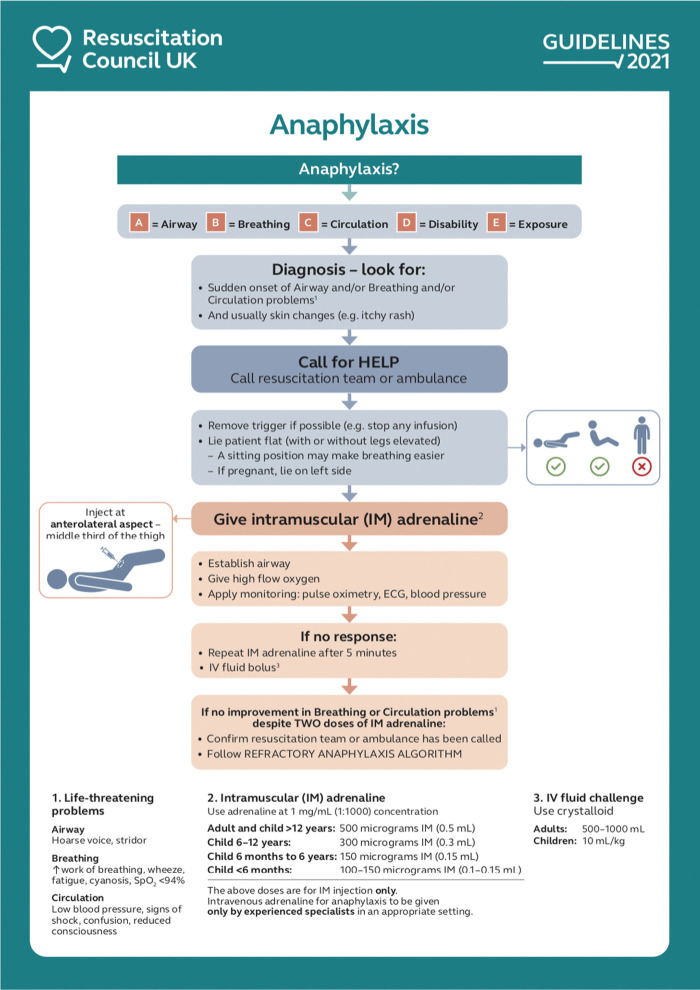
Anaphylaxis
Diagnostic criteria: (1) acute onset with skin/mucosal involvement AND respiratory or cardiovascular compromise, OR (2) two or more organ systems involved after likely allergen exposure, OR (3) hypotension after known allergen exposure. Treatment is IM epinephrine 0.3–0.5 mg (0.01 mg/kg) in the anterolateral thigh, repeated every 5–15 minutes as needed. Adjuncts include IV fluids, H1 and H2 antihistamines, steroids, albuterol, and airway management. Observation for biphasic reaction is 4–6 hours minimum.
Acute Angle-Closure Glaucoma
Severe eye pain, headache, nausea/vomiting, halos around lights, fixed mid-dilated pupil, rock-hard eye. Measure IOP (> 30 mmHg). Treatment: topical timolol, brimonidine, pilocarpine, oral acetazolamide, IV mannitol; ophthalmology for definitive iridotomy.
Epistaxis & ENT Bleeding
Anterior bleeds (Kiesselbach's plexus) are managed with direct pressure, topical oxymetazoline, silver nitrate cautery, or anterior nasal packing. Posterior bleeds (sphenopalatine artery) require posterior packing or balloon catheter and admission for airway monitoring.
Dental, Peritonsillar Abscess, Ludwig's Angina
Peritonsillar abscess presents with severe sore throat, trismus, uvular deviation, and "hot potato" voice; treatment is needle aspiration or I&D plus antibiotics. Ludwig's angina is a bilateral submandibular cellulitis that can cause airway compromise — early airway control is paramount.
16 Orthopedic Emergencies & Lacerations Ortho
Fractures & Dislocations
Document mechanism, neurovascular status, open vs closed, and deformity. Common reductions performed in the ED: shoulder (anterior dislocation most common), elbow, finger, hip (prosthetic), patella, and ankle. All reductions require pre- and post-reduction neurovascular exams and post-reduction imaging. Splinting protects the injury until definitive orthopedic management. Specific high-yield injuries: hip fracture (common in elderly falls, requires ortho admission), scaphoid fracture (snuff box tenderness, splint even if X-ray negative), Colles fracture (dorsally angulated distal radius), Boxer's fracture (5th metacarpal neck), Lisfranc injury (midfoot), and Achilles rupture (positive Thompson test).

Ottawa Ankle Rule: X-ray if pain in the malleolar zone AND any of: bone tenderness at posterior edge/tip of lateral malleolus, bone tenderness at posterior edge/tip of medial malleolus, or inability to bear weight both immediately and in the ED (4 steps).
Ottawa Foot Rule: X-ray if pain in midfoot zone AND any of: tenderness at base of 5th metatarsal, tenderness at navicular, or inability to bear weight.
Ottawa Knee Rule: X-ray if age ≥ 55, isolated patellar tenderness, tenderness at fibular head, inability to flex to 90°, or inability to bear weight (4 steps) both immediately and in ED.
Lacerations & Wound Care
Document location, size, depth, wound edges, contamination, tendon/nerve/vascular involvement, tetanus status, and foreign body evaluation. Irrigate with normal saline (100 mL per cm of laceration), explore, and close with appropriate materials (5-0 or 6-0 nylon for face, 4-0 or 5-0 for extremities, absorbable for mucosa and pediatric scalp). Tetanus prophylaxis per CDC schedule. Bite wounds usually get prophylactic antibiotics (amoxicillin-clavulanate); high-risk bites (cat, hand, deep) may be left open. Abscesses require I&D; antibiotics are added for surrounding cellulitis, immunocompromise, or systemic signs.
17 Psychiatric Emergencies Psych
Psychiatric presentations in the ED include suicidal ideation, homicidal ideation, psychosis, mania, severe anxiety/panic, substance-induced states, and acute agitation. Every psychiatric patient first gets medical clearance: vitals, glucose, and a targeted exam to exclude reversible medical causes (hypoglycemia, hypoxia, intoxication, delirium, infection, CNS pathology). The Columbia Protocol (C-SSRS) is used to assess suicidality.
Acute Agitation
Verbal de-escalation first. If medications are needed, options include oral or IM benzodiazepines (lorazepam 2 mg), antipsychotics (haloperidol 5 mg, olanzapine 10 mg, droperidol 5 mg), or combinations (e.g., "B-52" — Benadryl 50 mg + Haldol 5 mg + Ativan 2 mg, though individual drug selection is preferred). Ketamine (4–5 mg/kg IM) is used for excited delirium. Document behavioral indications, medications given, response, and need for restraints.
Suicidality & Involuntary Holds
Patients with active suicidal ideation, a plan, intent, or recent attempt require a safety evaluation and often psychiatric hospitalization (voluntary or on an involuntary hold under state-specific statutes, commonly called "5150" in California or "Section 12" in Massachusetts). Remove belongings and clothing, place in a safe room, and assign a sitter.
Substance Use Disorders in the ED
The ED is an entry point for substance-use treatment. Opioid use disorder patients can be started on buprenorphine directly from the ED once they demonstrate objective withdrawal (COWS ≥ 8), with a "warm handoff" to an outpatient clinic for continuation. Alcohol use disorder patients benefit from naltrexone or acamprosate prescribing, thiamine/folate/multivitamin supplementation, and social work consultation. Documenting harm-reduction counseling (naloxone distribution, safe injection practices, referral to treatment) is an increasingly expected part of ED care.
Excited Delirium & Restraints
Excited delirium is a clinical syndrome of severe agitation, hyperthermia, tachycardia, and superhuman strength, often in the setting of stimulant intoxication. Management requires rapid chemical sedation (ketamine 4–5 mg/kg IM is effective), aggressive cooling, large-volume IV fluids, and monitoring for rhabdomyolysis, hyperkalemia, and sudden cardiac arrest. Physical restraints must be documented with indication, type, duration, and frequent re-assessment per hospital policy.
18 ED Procedures — A to Z
| Procedure | Indication | Key Documentation |
|---|---|---|
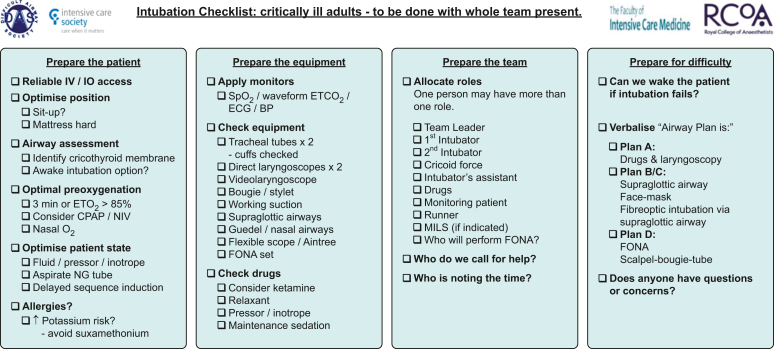
| Rapid sequence intubation (RSI) | Airway failure, hypoxemia, hypercapnia, protection against aspiration, anticipated clinical course | Pre-oxygenation, induction agent (etomidate, ketamine, propofol), paralytic (rocuronium, succinylcholine), blade and tube size, number of attempts, cord view (Cormack-Lehane), confirmation (ETCO2), post-tube vitals |
| Cricothyroidotomy | Can't intubate, can't oxygenate | Indication, technique (Seldinger vs open), tube size, confirmation, complications |
| Central venous catheter | Vasopressors, poor peripheral access, large-volume resuscitation | Site (IJ, subclavian, femoral), ultrasound guidance, number of attempts, complications, CXR for confirmation (non-femoral) |
| Intraosseous (IO) access | Emergency access when IV unavailable | Site (proximal tibia, humeral head), confirmation by aspirate or fluid flow |
| Chest tube (tube thoracostomy) | Pneumothorax, hemothorax, empyema | Side, size, location (4th/5th ICS mid-axillary), technique, output, suction vs water seal, post-procedure CXR |
| Needle thoracostomy | Tension pneumothorax | Side, location (2nd ICS MCL or 4th/5th ICS AAL) |
| Pericardiocentesis | Cardiac tamponade | Approach (subxiphoid US-guided), volume removed, hemodynamic response |
| ED thoracotomy | Penetrating chest trauma with signs of life lost within 15 minutes | Technique (left anterolateral), findings, interventions |
| Paracentesis | New ascites, suspected SBP, therapeutic drainage | Approach (LLQ US-guided), volume, fluid characteristics, albumin replacement if > 5 L |
| Lumbar puncture | Meningitis, SAH (CT-negative), elevated ICP evaluation | Position, level (L3-L4 or L4-L5), opening pressure, fluid characteristics, tubes sent |
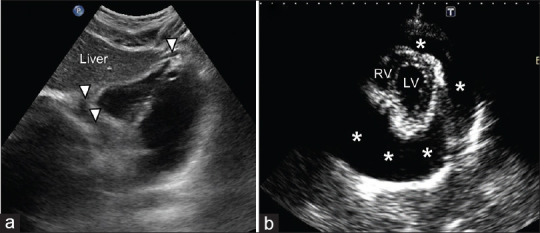
| FAST / eFAST | Blunt trauma, shock evaluation | Views (pericardial, RUQ/Morrison's, LUQ, pelvis, plus bilateral lung and cardiac for eFAST), findings |
| POCUS | Cardiac, lung, abdominal, DVT, ocular, procedural guidance | Indication, findings, clinical correlation |
| Splinting | Fracture immobilization | Type (sugar tong, volar, posterior slab, etc.), position, neurovascular check |
| Joint reduction | Dislocation | Joint, direction, technique, sedation, pre/post neurovascular exam, post-reduction imaging |
| Laceration repair | Open wound requiring closure | Anesthesia, irrigation, exploration, closure (suture material, number, technique) |
| Incision & drainage | Abscess | Site, size, anesthesia, technique, culture sent, packing |
| Foreign body removal | Retained FB (eye, ear, nose, skin) | Technique, imaging if needed, complications |
| Cardioversion | Unstable tachyarrhythmia or elective for afib | Sedation, synchronized shock, energy, response |
| Defibrillation | VF/pulseless VT | Energy, number of shocks, rhythm post-shock |
| Transcutaneous pacing | Unstable bradycardia | Rate, mA for capture, sedation, transition to transvenous |
| NG tube | SBO, gastric decompression, gastric lavage | Size, confirmation, output |
| Foley catheter | Urinary retention, strict I/O monitoring | Size, technique, residual volume |
| Procedural sedation | Painful procedures | Agent (ketamine, propofol, etomidate, fentanyl, midazolam), dose, monitoring, recovery |
Procedure notes must include time, indication, consent (verbal or implied emergency), technique, findings, complications, and post-procedure assessment. For sedation, always document ASA class, NPO status (if time permits), and recovery to baseline.
19 Labs, Imaging & POCUS
Core ED Labs
CBC: WBC (infection, stress), Hb/Hct (bleeding, anemia), platelets. BMP/CMP: electrolytes, renal function, glucose, liver function. Coags (PT/INR, PTT): bleeding, anticoagulation status. Troponin: myocardial injury; high-sensitivity assays allow 0/1 or 0/2 hour rule-out protocols. Lactate: tissue hypoperfusion, sepsis, mesenteric ischemia. BNP/NT-proBNP: heart failure. D-dimer: PE/DVT rule-out in low pre-test probability. VBG/ABG: acid-base status, oxygenation. Lipase: pancreatitis. LFTs: hepatic/biliary disease. UA: UTI, hematuria, ketones. HCG: pregnancy. Tox screen: overdose evaluation. Lactate, procalcitonin: infection severity. Type and screen/cross: transfusion preparation.
Imaging
Plain radiographs: chest, abdomen (obstruction series), extremities, spine. Ultrasound/POCUS: FAST, cardiac, lung, biliary, renal, aorta, DVT, pelvis, ocular, procedural guidance. CT: head (non-contrast for acute stroke/hemorrhage), chest (PE protocol with contrast, or without for pneumothorax/infiltrate), abdomen/pelvis (with IV contrast for most indications), CTA for vascular emergencies. MRI: cord compression, posterior circulation stroke, osteomyelitis, certain soft tissue pathology. V/Q scan: PE evaluation when CT contraindicated.
EKG Interpretation Basics
Every ED scribe should recognize a handful of EKG patterns that drive immediate action. STEMI shows ST elevation in a vascular territory (anterior V1-V4 LAD, lateral I/aVL/V5-V6 LCx, inferior II/III/aVF RCA) with reciprocal ST depression. NSTEMI/ischemia shows ST depression or T-wave inversion. Wellens syndrome shows biphasic or deeply inverted T waves in V2-V3 and signals proximal LAD occlusion. Hyperkalemia progresses from peaked T waves → PR prolongation → QRS widening → sine wave. PE classically shows sinus tach, S1Q3T3, or RBBB. Pericarditis shows diffuse concave ST elevation with PR depression. Brugada, prolonged QT, WPW, and heart block are additional patterns the scribe will encounter. Document rate, rhythm, axis, intervals (PR, QRS, QTc), and any abnormalities.
POCUS in the ED
Point-of-care ultrasound is routine in modern ED practice. Core applications include FAST for trauma, cardiac (pericardial effusion, LV function, RV strain), lung (pneumothorax, B-lines, pleural effusion), aorta (AAA), biliary, renal (hydronephrosis), DVT compression study, pelvic (intrauterine pregnancy), ocular (retinal detachment, elevated ICP via optic nerve sheath diameter), and procedural guidance for central lines, paracentesis, thoracentesis, and nerve blocks.
20 ED Medications & Antidotes
| Class | Generic (Brand) | Use | Key Notes |
|---|---|---|---|
| Analgesic | Morphine, hydromorphone (Dilaudid), fentanyl | Moderate-severe pain | Monitor respiratory rate; naloxone available |
| Analgesic | Ketorolac (Toradol) | Renal colic, MSK pain | Avoid in CKD, GI bleed, elderly |
| Analgesic | Acetaminophen, ibuprofen | Mild-moderate pain, fever | Avoid acetaminophen in hepatic failure |
| Procedural sedation | Ketamine | Dissociative sedation, analgesia, RSI induction | Laryngospasm rare; emergence reactions |
| Procedural sedation | Propofol, etomidate, midazolam | Induction, sedation | Etomidate causes adrenal suppression |
| RSI paralytic | Rocuronium, succinylcholine | Neuromuscular blockade for intubation | Succinylcholine contraindicated in hyperkalemia, burns > 24h |
| Antiemetic | Ondansetron (Zofran), metoclopramide (Reglan), prochlorperazine (Compazine), promethazine (Phenergan) | Nausea/vomiting | Ondansetron QTc prolongation |
| Anticoagulant | Heparin, enoxaparin (Lovenox), rivaroxaban (Xarelto), apixaban (Eliquis) | ACS, PE/DVT, stroke prevention | Weight-based dosing; renal adjustment |
| Reversal | Vitamin K, 4F-PCC (Kcentra), andexanet (Andexxa), idarucizumab (Praxbind), protamine | Anticoagulant reversal | Specific to drug; expensive |
| Antiplatelet | Aspirin, clopidogrel (Plavix), ticagrelor (Brilinta) | ACS, stroke | Load dose in ACS |
| Thrombolytic | Alteplase (tPA), tenecteplase (TNKase) | Stroke, massive PE, STEMI (rarely) | Strict inclusion/exclusion criteria |
| Antiarrhythmic | Adenosine, amiodarone, diltiazem, metoprolol, procainamide, magnesium | SVT, VT, afib rate/rhythm control | Adenosine for SVT; amiodarone for stable VT |
| Vasopressor | Norepinephrine (Levophed), epinephrine, phenylephrine, vasopressin, dopamine | Shock | Norepinephrine first-line for septic shock |
| Antibiotic | Ceftriaxone, vancomycin, piperacillin-tazobactam, cefepime, meropenem, metronidazole, azithromycin | Empiric sepsis/infection coverage | Broaden per source; de-escalate |
| Antidote | Naloxone (Narcan) | Opioid overdose | Titrate to respiratory rate |
| Antidote | Flumazenil | Benzodiazepine overdose | Rarely used; seizure risk in chronic users |
| Antidote | N-acetylcysteine (NAC) | Acetaminophen overdose | Rumack-Matthew nomogram guides |
| Antidote | Fomepizole | Toxic alcohols (methanol, ethylene glycol) | Plus dialysis in severe |
| Antidote | Atropine + pralidoxime | Organophosphate/nerve agent | Atropine titrated to drying of secretions |
| Antidote | Hydroxocobalamin | Cyanide (smoke inhalation) | Turns urine red |
| Antidote | Calcium, glucagon, high-dose insulin, lipid emulsion | Beta-blocker/CCB overdose | HDI protocol: 1 unit/kg bolus + infusion |
| Antidote | Sodium bicarbonate | TCA overdose, salicylate, wide QRS | Target urine pH > 7.5 |
| Antidote | Physostigmine | Anticholinergic toxicity (select) | Avoid in TCA overdose |
| Steroid | Methylprednisolone (Solu-Medrol), dexamethasone | Asthma, COPD, croup, anaphylaxis, meningitis | Early in asthma/anaphylaxis |
| Bronchodilator | Albuterol, ipratropium (DuoNeb) | Asthma, COPD | Continuous nebs in severe |
| Antihypertensive | Labetalol, esmolol, nicardipine, hydralazine, clevidipine | Hypertensive emergency, dissection | IV titratable |
21 Classification Systems & Clinical Scores
History: 0 slightly suspicious, 1 moderately, 2 highly. EKG: 0 normal, 1 non-specific repolarization, 2 significant ST deviation. Age: 0 <45, 1 45–64, 2 ≥65. Risk factors: 0 none, 1 one or two, 2 three or more / known atherosclerosis. Troponin: 0 normal, 1 1–3× normal, 2 >3× normal. Total 0–3: low risk (~1.7% MACE); 4–6: moderate (~17%); 7–10: high (~50%).
Clinical signs of DVT (3), PE most likely diagnosis (3), HR > 100 (1.5), immobilization/surgery (1.5), previous DVT/PE (1.5), hemoptysis (1), malignancy (1). > 4 likely; ≤ 4 unlikely.
All eight must be absent to rule out PE without D-dimer in low pre-test probability: age ≥ 50, HR ≥ 100, SaO2 < 95%, unilateral leg swelling, hemoptysis, recent trauma/surgery, prior DVT/PE, hormone use.
Active cancer (1), paralysis/immobilization (1), recently bedridden > 3d or surgery < 12 weeks (1), local tenderness along deep veins (1), entire leg swollen (1), calf swelling > 3 cm (1), pitting edema (1), collateral superficial veins (1), previous DVT (1), alternative diagnosis as likely (−2). ≥ 2 likely; < 2 unlikely.
CHF history, Hematocrit < 30, abnormal EKG, Shortness of breath, Systolic BP < 90. Any positive → high risk for serious outcome at 7 days.
No imaging needed if ALL: no midline posterior cervical tenderness, no focal neurologic deficit, normal alertness, no intoxication, no distracting injury.
1 point each: tonsillar exudates, tender anterior cervical adenopathy, fever > 38°C, absence of cough. Modified adds age < 15 (+1), > 44 (−1). 0–1 no testing; 2–3 rapid strep; 4–5 treat empirically.
RR ≥ 22, altered mental status, SBP ≤ 100. ≥ 2 → sepsis screening positive.
The American Association for the Surgery of Trauma grades solid organ injuries on a 1–5 (or 6 for destroyed) scale. Liver/spleen grades: I = subcapsular hematoma < 10% or laceration < 1 cm; II = hematoma 10–50% or laceration 1–3 cm; III = hematoma > 50% or laceration > 3 cm; IV = parenchymal disruption 25–75% of a lobe; V = parenchymal disruption > 75% or major vascular; VI = hepatic avulsion/destroyed spleen.
22 Physical Exam & Abbreviations
The Focused ED Exam
General: Well/ill/toxic appearing, alert, in no acute distress. HEENT: PERRL, EOMI, conjunctivae, oropharynx, tympanic membranes. Neck: supple, no meningismus, no JVD, no bruits, no LAD. Cardiovascular: rate, rhythm, murmurs, rubs, gallops, peripheral pulses, capillary refill, edema. Pulmonary: respiratory effort, breath sounds, symmetric chest rise, accessory muscle use. Abdomen: soft, distension, bowel sounds, tenderness with specific quadrant, guarding, rebound, organomegaly, CVA tenderness, rectal exam if indicated. Extremities: range of motion, deformity, swelling, pulses, neurovascular distally. Skin: rashes, petechiae, ecchymosis, wounds. Neuro: mental status, cranial nerves, motor, sensory, reflexes, gait, coordination, NIHSS if stroke.
Abbreviations Master List
23 Disposition & Documentation
Disposition is the final ED decision and must be clearly documented with supporting reasoning. Options include discharge home, admit (to observation, medicine, ICU, or specialty service), transfer to another facility, AMA (against medical advice), elopement, or death in the ED. Every disposition needs: final diagnosis, condition at disposition, vital signs at disposition, medications given, follow-up instructions, return precautions, and any patient counseling. Discharge instructions must be written at an appropriate literacy level and include specific symptoms that warrant return.
Diagnosis, vital signs (last set), medications given in ED, new prescriptions, work/school notes, follow-up provider and timeframe, return precautions ("return for worsening pain, fever, vomiting, shortness of breath, chest pain, weakness, or any concerning new symptom"), patient understands and agrees with plan.
For admissions, the ED note handoff to the admitting team includes current status, pending studies, medications started, response to treatment, and outstanding tasks. The CMS 2-midnight rule guides the observation vs inpatient decision for admitted patients. EMTALA obligates every ED to provide a medical screening exam and stabilizing treatment to every patient regardless of ability to pay, and to arrange appropriate transfer when the ED cannot provide definitive care.
24 Sample HPI Templates & References
These templates show the rhythm and content of an ED note for common presentations. Use them as frameworks during your first shifts.
"Mr. [Name] is a 62-year-old male with hypertension, hyperlipidemia, type 2 diabetes, and a 30-pack-year smoking history who presents with 2 hours of substernal chest pressure that began while mowing the lawn. He describes the pain as 7/10, squeezing, non-radiating, associated with diaphoresis and mild dyspnea. Pain was partially improved with rest but did not fully resolve. He denies syncope, palpitations, leg swelling, recent travel or immobilization, calf pain, hemoptysis, tearing back pain, fevers, or prior similar episodes. He takes aspirin 81 mg, atorvastatin, lisinopril, and metformin. No allergies. Initial EKG shows 1 mm ST depression in V4-V6; initial troponin pending. HEART score 6 (history 2, EKG 1, age 1, risk factors 2, troponin pending)."
"Ms. [Name] is a 78-year-old female from an assisted living facility with a history of type 2 diabetes, CKD stage 3, and a chronic indwelling Foley catheter who presents with 1 day of fever, altered mental status, and decreased PO intake. Staff report she was confused and lethargic this morning. Vitals on arrival: T 39.2, HR 118, BP 84/52, RR 24, SpO2 93% on room air. She is arousable but disoriented. Exam notable for dry mucous membranes, tachycardia, clear lungs, soft abdomen, cloudy urine in the Foley bag, no focal neurologic deficits. Lactate 4.1, WBC 18.2 with 22% bands, creatinine 2.4 (baseline 1.6), UA with > 100 WBC and positive nitrites. qSOFA 3. Meets criteria for septic shock; urosepsis most likely source. Blood cultures drawn, broad-spectrum antibiotics (ceftriaxone + vancomycin) initiated, 30 mL/kg LR bolus started, norepinephrine standing by."
"Mr. [Name] is a 55-year-old male with hypertension and hyperlipidemia who presents after a witnessed syncopal episode at work. He reports he was standing at his desk when he felt lightheaded, diaphoretic, and nauseated for approximately 30 seconds before losing consciousness. A coworker caught him as he fell; he was unresponsive for approximately 20 seconds, did not have tonic-clonic activity, tongue biting, or incontinence, and returned to baseline immediately with no post-event confusion. He denies chest pain, palpitations, dyspnea, headache, focal neurologic deficits, or prior similar episodes. No family history of sudden cardiac death. Medications: lisinopril, atorvastatin. Initial EKG shows normal sinus rhythm without ischemic changes or prolonged QT. Orthostatics positive. Glucose 98. San Francisco Syncope Rule negative."
"Ms. [Name] is a 24-year-old female G0P0, LMP 4 weeks ago, who presents with 6 hours of progressive right lower quadrant abdominal pain. Pain started periumbilically, migrated to the RLQ, is 8/10, sharp, worse with movement. She reports anorexia, one episode of non-bloody non-bilious emesis, and a low-grade subjective fever. Denies diarrhea, dysuria, vaginal bleeding or discharge, and has no history of similar pain. Sexually active, no known STIs, no contraception. Vitals: T 38.1, HR 104, BP 118/72, RR 16. Exam notable for focal tenderness at McBurney's point with voluntary guarding, positive Rovsing sign, no rebound. Urine HCG negative. WBC 14.8 with left shift. CT abdomen/pelvis ordered."
"Mr. [Name] is a 28-year-old male unrestrained driver in a high-speed single-vehicle MVC, GCS 13 at the scene per EMS. On arrival, GCS 14 (E3 V5 M6), BP 92/54, HR 128, RR 24, SpO2 94% on NRB. Primary survey: airway patent, breath sounds decreased on the right with subcutaneous emphysema, strong radial pulses, abdomen soft but tender diffusely, no external hemorrhage, GCS 14, no obvious deformities. Two 18g IVs placed, 1 L LR bolus, TXA administered, type and cross for 4 units. eFAST positive for free fluid in the RUQ and a right pneumothorax. CT torso pending after right chest tube placement. Trauma surgery at the bedside; OR activated."
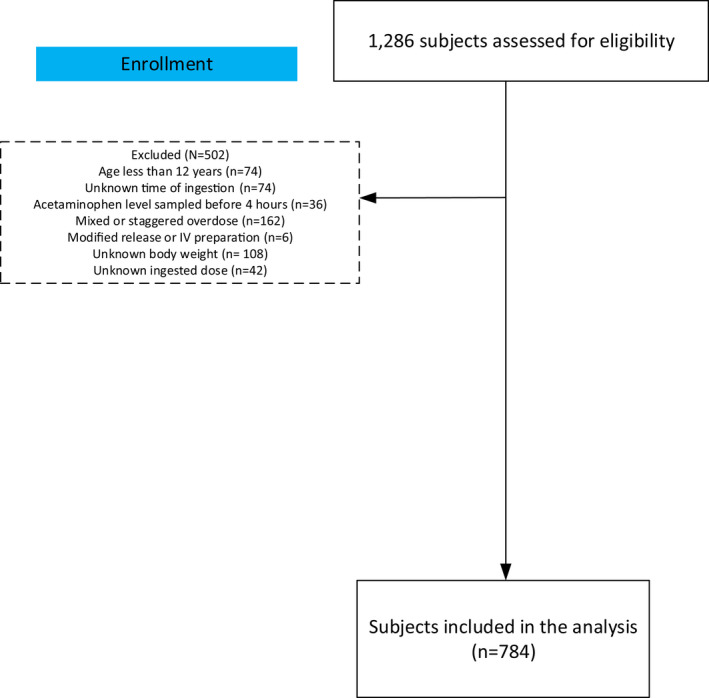
"Ms. [Name] is a 32-year-old female with a history of depression and prior suicide attempts brought in by EMS after being found unresponsive at home with empty bottles of acetaminophen (extra strength) and ibuprofen. Unclear time of ingestion, reportedly within the past 4–6 hours per family. On arrival: GCS 10 (E2 V3 M5), HR 112, BP 108/66, RR 14, SpO2 98% on room air, glucose 102. Pupils 3 mm reactive. No focal deficits. Initial labs: acetaminophen level pending, salicylate pending, ethanol pending, comprehensive metabolic panel, LFTs, INR, ABG, UA tox. N-acetylcysteine loading dose (150 mg/kg) initiated empirically pending 4-hour level plotted on the Rumack-Matthew nomogram. Psychiatry consulted for post-medical-clearance evaluation and involuntary hold."
References & Sources
American College of Emergency Physicians (ACEP) Clinical Policies Library.
Figure 1: Emergency Room. Wikimedia Commons. Public domain.
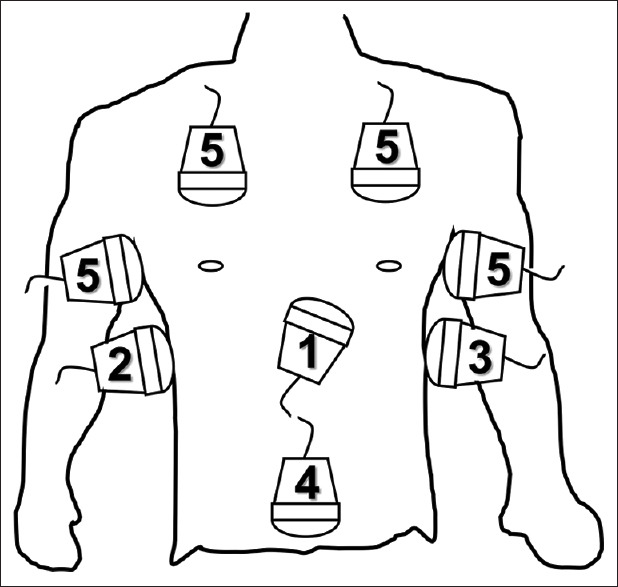
Figure 2: Triage Tag. Wikimedia Commons. Public domain.
Figure 3: Conduction System of the Heart. OpenStax College. CC BY 3.0.
Figure 4: Major Respiratory Organs. OpenStax College. CC BY 3.0.
Figure 5: Rule of Nines for Burns. Wikimedia Commons. Public domain.
The best ED scribes understand the rhythm of the department. They anticipate the next order before the physician speaks it. When a stroke alert rolls in, they already have the NIHSS template open and know the last-known-well question is coming. When a "chest pain" is triaged, they know a HEART score is forming in the attending's head and they have the EKG time-stamped. They document vital sign trends, the exact time of key interventions, and the rationale behind every disposition.
Learn the medications by generic and brand name. Learn the common orders. Learn the classic presentations of every "can't miss" diagnosis so you can recognize them as they unfold. Read imaging reports before the attending opens them. Ask questions during downtime — never during a resuscitation. And remember that the patients in front of you are having one of the worst days of their lives; treat every note as if it will be read in court, because it might be.
Welcome to emergency medicine. The pace is relentless, but the work matters more than you know.