Otolaryngology (ENT)
Every diagnosis, condition, procedure, medication, abbreviation, and documentation framework you need to succeed on day one and beyond in otolaryngology head & neck surgery.
All diagrams on this page are sourced from published educational or institutional materials rather than AI generation. Each figure caption links to the original source, and the full diagram and guideline citations are collected in the references section at the bottom.
01 Head & Neck Anatomy Essentials
Otolaryngology — head and neck surgery covers the ear, nose, throat, larynx, salivary glands, thyroid/parathyroid, skull base, and all soft-tissue structures of the face and neck above the clavicles (excluding the brain, eyes, and cervical spine). A scribe must understand these regions as interconnected systems because disease in one area (for example, sinus infection) frequently drives symptoms in another (headache, otalgia, pharyngitis).
The Ear — Outer, Middle, and Inner
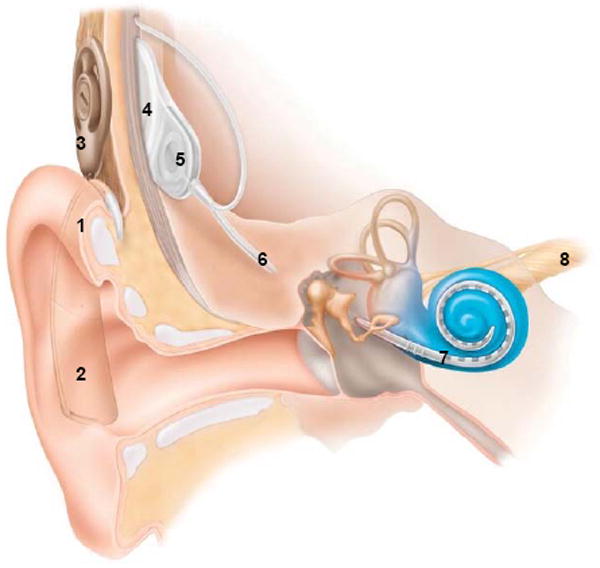
The ear is divided into three compartments. The outer ear comprises the auricle (pinna) and the external auditory canal (EAC), ending at the tympanic membrane (TM). The lateral third of the EAC is cartilaginous and hair-bearing, producing cerumen; the medial two-thirds are bony and very sensitive. The middle ear is an air-filled cavity containing the three ossicles — malleus, incus, and stapes — which transmit vibrations from the TM to the oval window of the cochlea. The middle ear communicates with the nasopharynx via the eustachian tube, which equalizes pressure and drains secretions. The inner ear contains the cochlea (organ of hearing) and the vestibular labyrinth (semicircular canals, utricle, saccule — organs of balance). Cranial nerve VIII (vestibulocochlear) carries signals from the cochlea and vestibular apparatus to the brainstem.
The Nose & Paranasal Sinuses
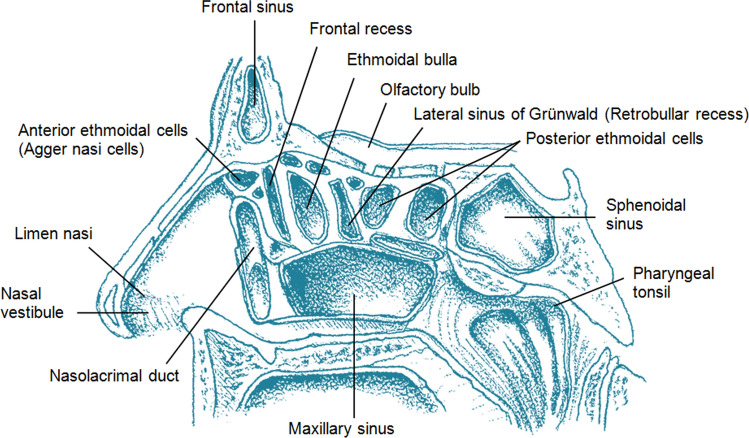
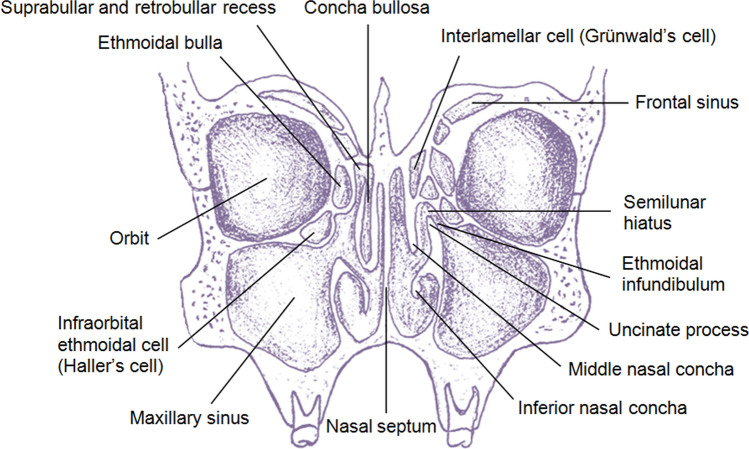
The nasal cavity is divided in the midline by the septum (quadrangular cartilage anteriorly, vomer and perpendicular plate of the ethmoid posteriorly). Each lateral wall carries three turbinates (inferior, middle, superior), with meatuses below each. The ostiomeatal complex (OMC) in the middle meatus is the final common drainage pathway for the frontal, maxillary, and anterior ethmoid sinuses — blockage here underlies most rhinosinusitis. The frontal, maxillary, ethmoid, and sphenoid sinuses are air-filled extensions of the nasal cavity lined by ciliated respiratory epithelium. The cribriform plate of the ethmoid bone separates the nasal roof from the anterior cranial fossa and is a key landmark for CSF leaks and skull-base tumors.
Oral Cavity, Pharynx, and Tonsils
The oral cavity extends from the lips to the junction of the hard and soft palate and circumvallate papillae of the tongue. It contains the anterior two-thirds of the tongue, floor of mouth, buccal mucosa, hard palate, alveolar ridges, and retromolar trigone. The pharynx is divided into three parts: the nasopharynx (behind the nasal cavity, containing the adenoids and eustachian tube orifices), the oropharynx (containing the palatine tonsils, base of tongue/lingual tonsils, soft palate, and posterior pharyngeal wall), and the hypopharynx (containing the pyriform sinuses and postcricoid region). Waldeyer's ring is the ring of lymphoid tissue formed by the adenoids, tubal tonsils, palatine tonsils, and lingual tonsils.
Larynx & Trachea
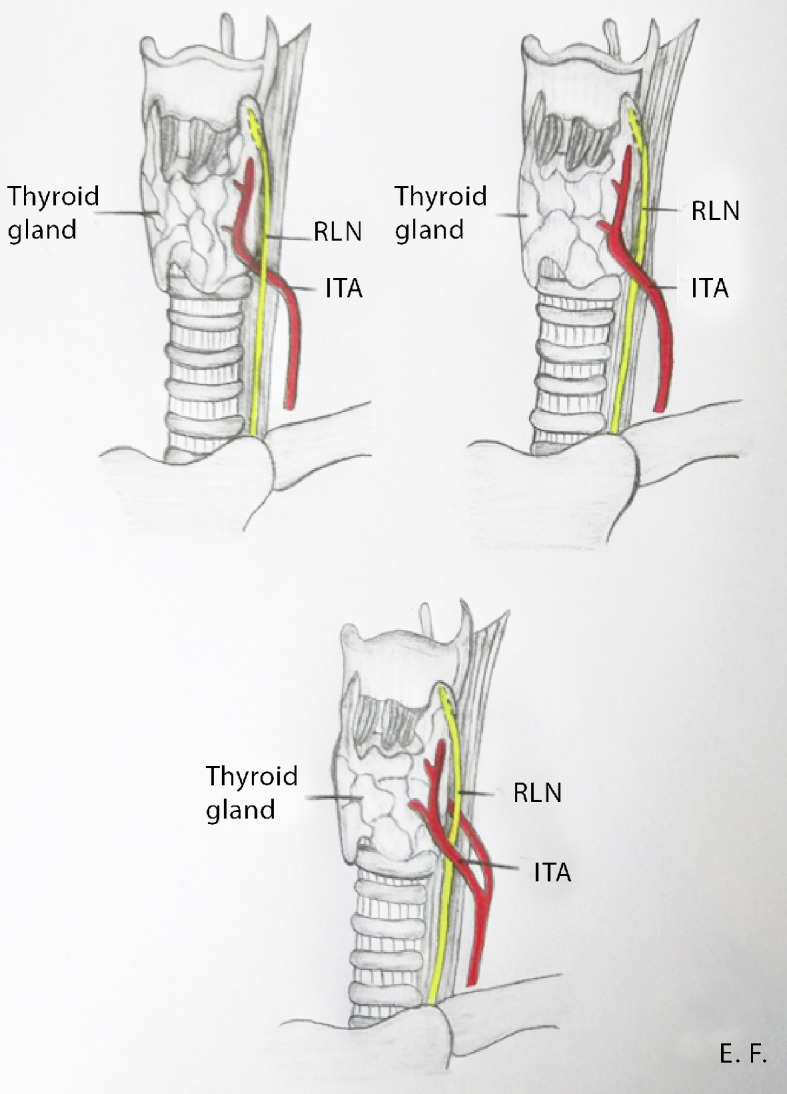
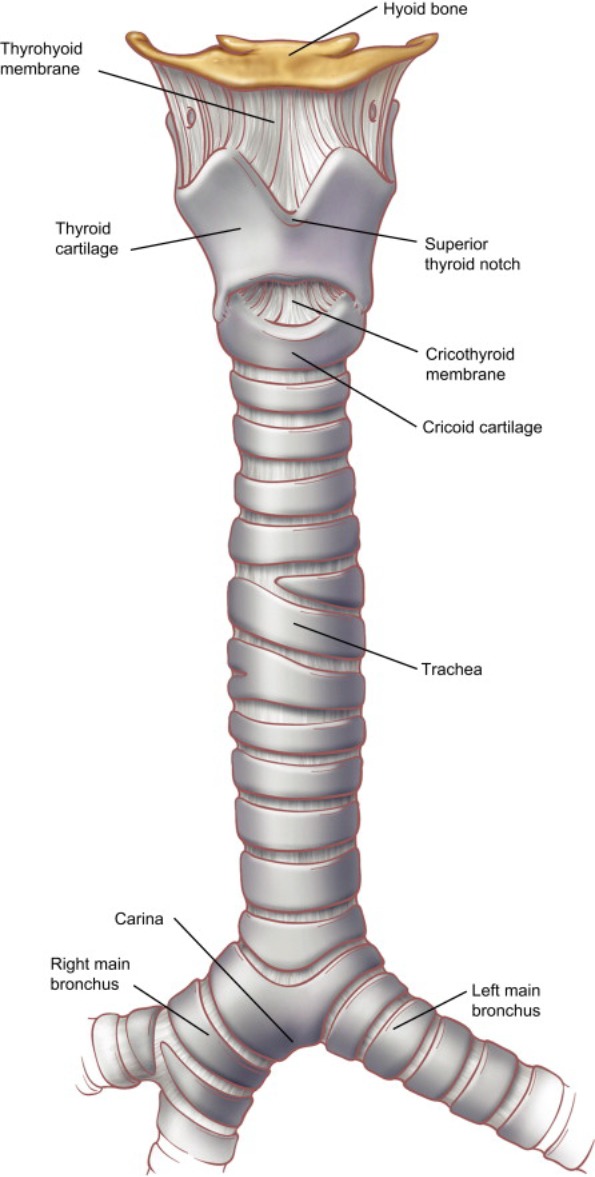
The larynx is composed of cartilages (thyroid, cricoid, arytenoid, corniculate, cuneiform, epiglottis) and the true vocal folds (cords), which vibrate to produce voice. Above the true cords are the false vocal folds and the ventricle between them. The larynx is subdivided into the supraglottis (epiglottis, aryepiglottic folds, false cords, ventricle), glottis (true cords and anterior/posterior commissures), and subglottis (from 1 cm below the true cords to the inferior edge of the cricoid). The recurrent laryngeal nerve (RLN), a branch of the vagus, supplies all intrinsic laryngeal muscles except the cricothyroid; it is the nerve at risk in thyroidectomy and the cause of most vocal fold paralysis.
Neck Levels & Lymphatics
The neck is divided into six lymphatic levels that drive tumor staging and the extent of neck dissection. Level I: submental (IA) and submandibular (IB). Level II: upper jugular (IIA anterior, IIB posterior to spinal accessory nerve). Level III: mid-jugular. Level IV: lower jugular. Level V: posterior triangle (VA above, VB below cricoid). Level VI: central compartment (pretracheal, paratracheal, prelaryngeal — the thyroid drainage basin). Different primary tumor sites drain to predictable levels, which determines which levels are dissected.

Know the neck levels cold. When the surgeon dictates "selective neck dissection of levels II through IV," you need to recognize this as a standard lateral neck dissection for oropharyngeal or laryngeal cancer. Level VI dissection means thyroid cancer. Level V involvement with a primary in the nasopharynx or scalp is a giveaway. Always chart the exact levels dissected in the operative note.
02 Scribe Documentation Framework
ENT encounters move fast. A busy general otolaryngologist may see 30–50 patients per day, each requiring a focused exam of ear, nose, throat, and often flexible laryngoscopy. The scribe's job is to capture a complete, billable note in real time without slowing the clinician down.
Chief Complaint (CC): Examples: "ear pain," "hoarseness for 3 months," "recurrent sinus infections," "hearing loss," "neck mass." Keep it short.
HPI: Use the OLDCARTS framework and always capture laterality (right, left, bilateral), duration, prior treatment (antibiotics, nasal steroids, allergy medications), and response. ENT-specific elements: for otalgia — otorrhea, hearing change, vertigo, tinnitus; for rhinosinusitis — facial pain/pressure, nasal obstruction, purulent discharge, anosmia; for hoarseness — duration (3 weeks is the red-flag threshold), smoking history, GERD/LPR symptoms, voice use (professional voice users); for neck mass — duration, growth rate, pain, B-symptoms, prior skin cancer, HPV risk factors.
ROS: Focused by complaint. Always include HEENT, respiratory, and for cancer patients constitutional symptoms (weight loss, night sweats, fatigue).
PMHx / PSHx / Meds / Allergies / SHx / FHx: Tobacco and alcohol use are critical (document pack-years and drinks/week — these are the two dominant risk factors for head and neck cancer). GERD, allergies, prior tonsillectomy, prior sinus surgery, prior tympanostomy tubes, radiation exposure, noise exposure, ototoxic medications (aminoglycosides, cisplatin, loop diuretics, high-dose aspirin).
Vitals: Standard. BMI matters for OSA evaluation.
ENT Exam: The specialty exam includes otoscopy (EAC, TM, mobility by pneumatic otoscopy or tympanometry), anterior rhinoscopy (septum, turbinates, mucosa, polyps), oral cavity and oropharynx (dentition, tongue, floor of mouth, tonsils graded 0–4+, palate), neck (lymphadenopathy by level, thyroid, salivary glands, trachea midline), cranial nerves, and — for most new patients and cancer follow-ups — flexible fiberoptic laryngoscopy (nasopharynx, base of tongue, vallecula, epiglottis, aryepiglottic folds, pyriform sinuses, vocal fold mobility).
Results: Audiograms (with PTA and SRT numbers), tympanograms (Type A, B, C), CT sinus (Lund-Mackay score), CT neck with contrast, MRI, FNA cytology, pathology reports.
Each diagnosis with ICD-10 plus plan. Common plans include antibiotic courses, nasal steroid initiation or optimization, saline irrigations, allergy testing referral, audiogram orders, CT imaging, in-office procedures (cerumen removal, endoscopy, biopsy, debridement), and surgical scheduling (septoplasty, FESS, tonsillectomy, parotidectomy, etc.).
You will almost always need to document a flexible laryngoscopy for hoarseness, globus, dysphagia, stridor, or cancer surveillance visits. The standard template: "Flexible fiberoptic laryngoscopy performed after topical anesthesia. Nasopharynx clear. Base of tongue and vallecula without lesion. Epiglottis normal. Bilateral true vocal folds with normal mobility and no lesions. Airway patent. No pooling of secretions." Modify as needed. This generates a separate CPT code (31575), so accuracy matters.
03 Otology — Ear Diseases Otology
Otitis Externa (OE)
Infection of the external auditory canal, often called "swimmer's ear." Pseudomonas and Staph aureus are the most common organisms. Patients present with otalgia, otorrhea, and tenderness on manipulation of the tragus or pinna. On otoscopy the canal is edematous, erythematous, and filled with debris. Management is topical: ciprofloxacin-dexamethasone (Ciprodex) or ofloxacin otic drops, aural toilet, and a wick if the canal is too swollen to admit drops. Pain control with NSAIDs or short-course opioids is often needed.

A life-threatening extension of OE into the temporal bone and skull base, occurring almost exclusively in diabetics and immunocompromised patients. Presents with severe, unrelenting otalgia, granulation tissue at the bony-cartilaginous junction of the EAC, and occasionally cranial nerve palsies (classically facial nerve). Workup includes CT temporal bone, gallium or Tc-99m bone scan, and cultures. Management is IV antipseudomonal antibiotics (ciprofloxacin, piperacillin-tazobactam, ceftazidime) for 6–8 weeks. Mortality is significant.
Acute Otitis Media (AOM)
Infection of the middle ear, usually following a viral URI that obstructs the eustachian tube. Most common organisms in children: Streptococcus pneumoniae, nontypeable Haemophilus influenzae, Moraxella catarrhalis. Diagnosis requires: (1) moderate-to-severe bulging of the TM, OR new-onset otorrhea not due to OE, AND (2) acute signs/symptoms including otalgia. The TM appears erythematous, bulging, and opaque with loss of landmarks on otoscopy; pneumatic otoscopy shows decreased mobility. First-line treatment per AAO-HNS/AAP AOM guideline is high-dose amoxicillin (80–90 mg/kg/day). Amoxicillin-clavulanate is used if amoxicillin failed recently, there is concurrent purulent conjunctivitis, or history of recurrent AOM. Observation is an option for non-severe unilateral AOM in children > 2 years.
Chronic Otitis Media (COM) & Cholesteatoma
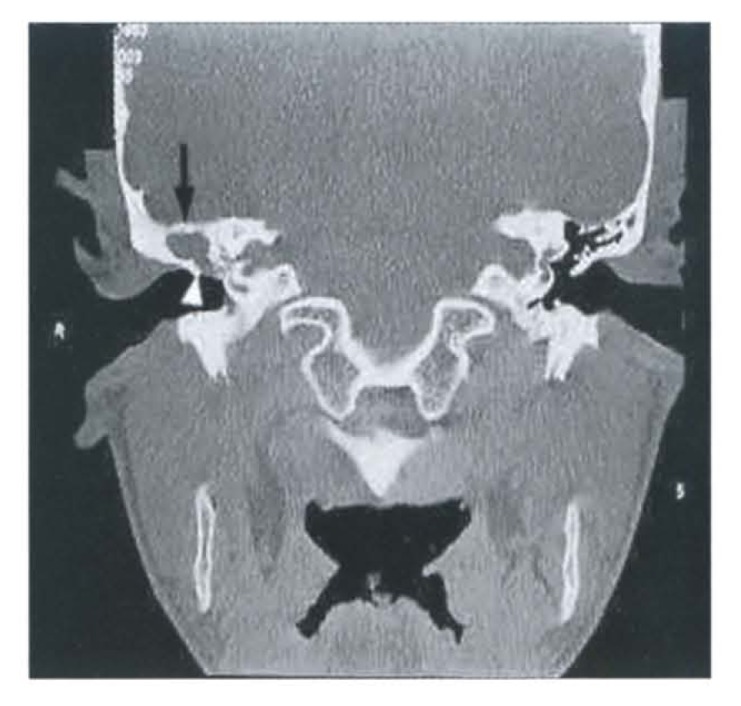
Chronic inflammation of the middle ear with a persistent TM perforation and often intermittent otorrhea. Cholesteatoma is the accumulation of keratinizing squamous epithelium in the middle ear or mastoid, often from a retraction pocket of the pars flaccida. Cholesteatoma is not a true tumor but behaves destructively — it erodes ossicles (causing conductive hearing loss), the scutum, the bony labyrinth (causing SNHL and vertigo), the facial nerve canal, and the tegmen tympani (intracranial extension). On otoscopy, look for a pearly white mass or debris in a retraction pocket. Definitive treatment is surgical: tympanomastoidectomy (canal wall up or canal wall down) with or without ossicular reconstruction.
Eustachian Tube Dysfunction (ETD)
Inability of the eustachian tube to open normally, causing middle ear pressure imbalance, fullness, muffled hearing, and crackling sounds. Often seen with URI, allergic rhinitis, or chronic rhinosinusitis. Management is treating the underlying nasal/sinus disease with topical nasal steroids, decongestants short-term, and autoinflation maneuvers. Refractory cases may undergo balloon eustachian tuboplasty.
Otosclerosis
Abnormal bone remodeling of the otic capsule, classically fixing the stapes footplate and producing progressive conductive hearing loss in young to middle-aged adults (more common in women, often worsens with pregnancy). A characteristic finding is Carhart's notch at 2000 Hz on the bone conduction audiogram. Management is hearing aids or surgical stapedectomy/stapedotomy with prosthesis placement.
Tympanic Membrane Perforation
From infection, trauma (Q-tip, slap to the ear, blast injury), or iatrogenic causes. Small traumatic perforations often heal spontaneously within weeks. Keep the ear dry. If persistent > 3 months, symptomatic, or associated with infection/hearing loss, repair with tympanoplasty (temporalis fascia, tragal cartilage, or fat graft myringoplasty for very small perforations).
Acoustic Neuroma (Vestibular Schwannoma)
Benign schwannoma arising from the vestibular division of CN VIII within the internal auditory canal. Classic presentation is asymmetric sensorineural hearing loss with or without tinnitus, occasional vertigo/imbalance, and in larger tumors trigeminal or facial nerve symptoms. MRI with gadolinium of the internal auditory canals is the test of choice. Management options: observation with serial MRI, stereotactic radiosurgery (Gamma Knife), or microsurgical resection (translabyrinthine, retrosigmoid, or middle fossa approach).
04 Hearing Loss & Audiology Otology
Hearing loss is categorized by type and severity. Conductive hearing loss (CHL) is caused by pathology of the outer or middle ear (cerumen impaction, TM perforation, effusion, ossicular disruption, otosclerosis). Sensorineural hearing loss (SNHL) arises from the cochlea or CN VIII (presbycusis, noise exposure, ototoxicity, Meniere, acoustic neuroma, sudden SNHL). Mixed hearing loss has both components.
A rapid (< 72 hours) SNHL of at least 30 dB across 3 contiguous frequencies. This is an otologic emergency. Evaluation per AAO-HNS SSNHL guideline includes audiogram and MRI (to rule out retrocochlear pathology, particularly vestibular schwannoma). Treatment is high-dose oral prednisone (1 mg/kg/day for 10–14 days with taper) and/or intratympanic dexamethasone injections; recovery is most likely within the first 2–4 weeks.
The Audiogram
Plots hearing threshold in decibels (dB HL) against frequency in Hertz (250 to 8000 Hz). Air conduction is marked O (right) and X (left); bone conduction is marked < (right) and > (left). An air-bone gap indicates CHL; equal loss on both AC and BC indicates SNHL. Pure-tone average (PTA) is the average threshold at 500, 1000, and 2000 Hz. Speech reception threshold (SRT) is the lowest level at which the patient repeats spondaic words correctly 50% of the time. Word recognition score (WRS) is the percentage of phonetically balanced words correctly repeated at a comfortable listening level.
| Severity | PTA (dB HL) | Functional Impact |
|---|---|---|
| Normal | −10 to 25 | No impairment |
| Mild | 26–40 | Difficulty with soft speech |
| Moderate | 41–55 | Difficulty with conversational speech |
| Moderately severe | 56–70 | Loud speech needed |
| Severe | 71–90 | Shouts heard; hearing aids essential |
| Profound | > 90 | Even amplified speech may be inaudible; cochlear implant candidate |
Management depends on type and severity: CHL may be corrected surgically (tympanoplasty, stapedectomy) or with hearing aids, BAHA (bone-anchored hearing aid) if unilateral or if the ear cannot wear a conventional aid. SNHL is managed with amplification; profound bilateral SNHL is the indication for cochlear implant.
05 Vestibular Disorders Otology
Benign Paroxysmal Positional Vertigo (BPPV)
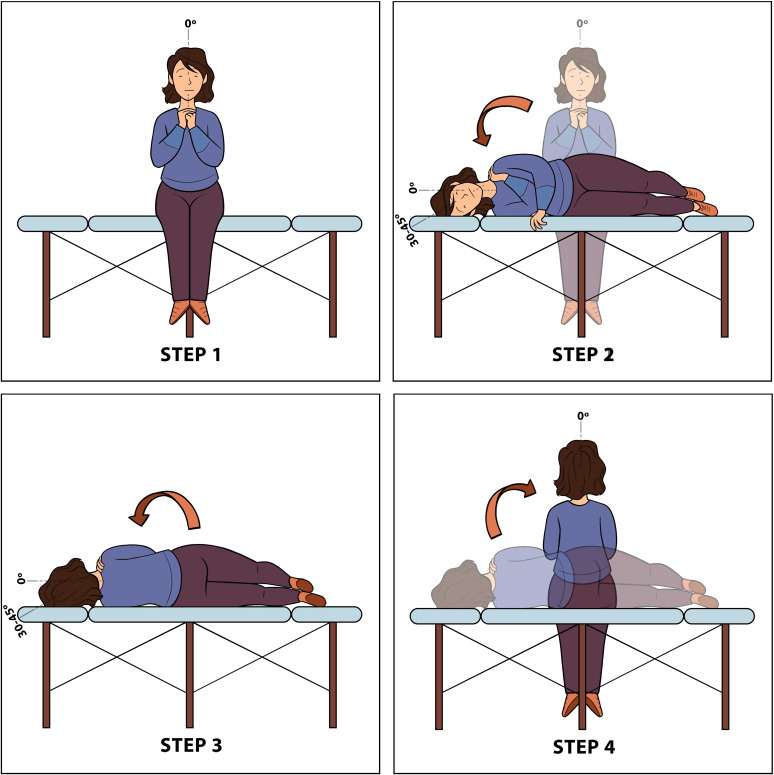
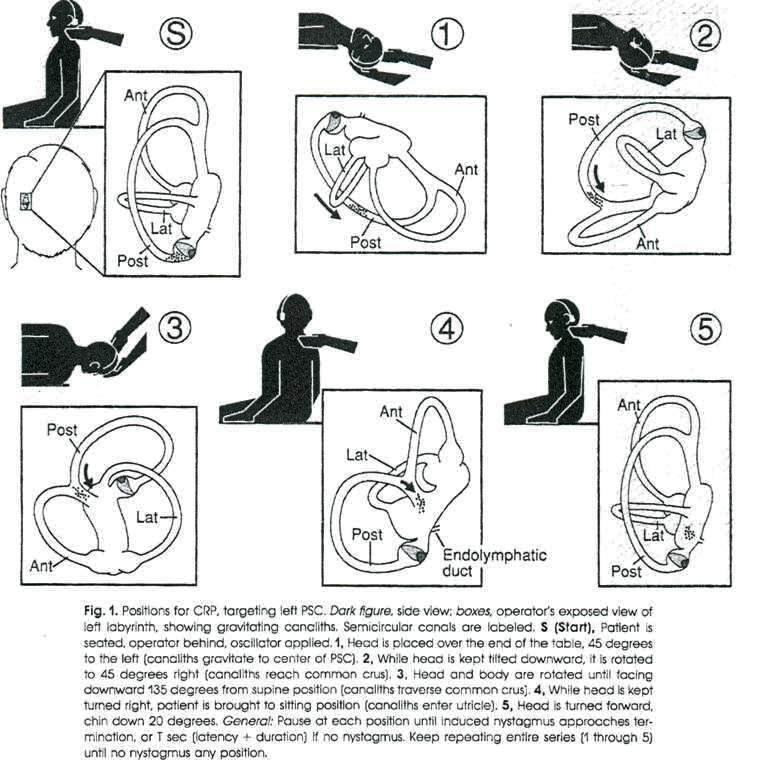
The most common cause of vertigo. Caused by displaced otoconia (calcium carbonate crystals) from the utricle into a semicircular canal, most commonly the posterior canal. Presents with brief (< 1 minute) episodes of spinning triggered by head position change (rolling over in bed, looking up). The AAO-HNS BPPV clinical practice guideline recommends diagnosis by the Dix-Hallpike maneuver for posterior canal BPPV (positive test: transient upbeat-torsional nystagmus with latency of 2–5 seconds, fatigability) and the supine roll test for horizontal canal BPPV. Treatment is canalith repositioning (Epley maneuver) for posterior canal BPPV. Meclizine is not indicated for BPPV and is discouraged by the guideline.
Vestibular Neuritis / Labyrinthitis
Presumed viral inflammation of the vestibular nerve causing acute, sustained vertigo, nausea, vomiting, and gait instability lasting days. If hearing is also affected it is called labyrinthitis. Treatment is supportive: vestibular suppressants (meclizine, diazepam) in the first 24–72 hours only, antiemetics (ondansetron), corticosteroids (methylprednisolone), and early vestibular rehabilitation. Recovery is gradual over weeks.
Meniere Disease
Idiopathic endolymphatic hydrops producing the classic tetrad of: (1) episodic vertigo lasting 20 minutes to 12 hours, (2) fluctuating low-frequency SNHL, (3) tinnitus, and (4) aural fullness. Management begins with sodium restriction (< 2 g/day), thiazide diuretics (HCTZ with triamterene), and avoidance of caffeine and alcohol. Betahistine is used in many countries outside the US. For refractory disease: intratympanic steroid or gentamicin injections, endolymphatic sac decompression, labyrinthectomy, or vestibular nerve section.
Vestibular Migraine
A migraine variant presenting with vertigo lasting minutes to days, often with headache but sometimes isolated. Diagnosis requires current or prior history of migraine. Management overlaps with migraine prophylaxis: avoidance of triggers, magnesium, riboflavin, topiramate, propranolol, venlafaxine. Often a diagnosis of exclusion after ruling out Meniere, BPPV, and central causes.
06 Facial Nerve Disorders Otology
Bell Palsy
Idiopathic (likely HSV-reactivation-related) lower-motor-neuron facial nerve paralysis, presenting with acute unilateral facial weakness including the forehead (distinguishing it from a central lesion, which spares the forehead). Associated symptoms: decreased tearing, hyperacusis, loss of taste on the anterior two-thirds of the tongue. Per the AAO-HNS Bell palsy guideline, treatment is oral corticosteroids (prednisone 60–80 mg/day for 1 week) started within 72 hours of symptom onset, with consideration of adding antivirals (valacyclovir) for severe cases. Eye protection is critical (artificial tears, ointment at night, taping the eye shut) to prevent exposure keratopathy.
Ramsay Hunt Syndrome (Herpes Zoster Oticus)
Varicella zoster reactivation in the geniculate ganglion, producing facial paralysis plus a vesicular rash in the EAC or pinna, often with severe otalgia. SNHL and vertigo may occur. Treatment is oral prednisone plus valacyclovir/famciclovir. Prognosis is worse than Bell palsy.
| Grade | Description | Function |
|---|---|---|
| I | Normal | Normal facial function in all branches |
| II | Mild dysfunction | Slight weakness noticeable on close inspection; normal symmetry at rest; complete eye closure with minimal effort |
| III | Moderate dysfunction | Obvious but not disfiguring asymmetry; complete eye closure with effort; synkinesis may be present |
| IV | Moderately severe dysfunction | Obvious weakness and disfiguring asymmetry; incomplete eye closure; asymmetric mouth movement with max effort |
| V | Severe dysfunction | Only barely perceptible motion; asymmetry at rest; incomplete eye closure |
| VI | Total paralysis | No movement |
07 Rhinology — Nose & Sinus Disease Rhinology
Acute Rhinosinusitis (ARS)
Inflammation of the nasal cavity and paranasal sinuses lasting < 4 weeks. Most cases are viral. Acute bacterial rhinosinusitis (ABRS) is diagnosed per the AAO-HNS adult sinusitis CPG when any one of: (1) symptoms persist > 10 days without improvement, (2) severe symptoms (fever ≥ 39°C with purulent discharge or facial pain) for 3–4 days at onset, or (3) "double worsening" — initial improvement followed by new fever, headache, or increased nasal discharge. First-line antibiotic is amoxicillin-clavulanate. Supportive measures: saline irrigation, intranasal corticosteroids, analgesics.
Chronic Rhinosinusitis (CRS)
Symptoms (at least 2 of: nasal obstruction, facial pain/pressure, anterior/posterior drainage, decreased smell) lasting > 12 weeks with objective evidence of inflammation (mucosal edema, purulence, or polyps on endoscopy, OR mucosal thickening on CT). CRS is phenotypically divided into CRSwNP (with nasal polyps — typically Th2/eosinophilic) and CRSsNP (without polyps). Treatment: daily saline irrigations, intranasal corticosteroids (fluticasone, mometasone, budesonide), oral corticosteroid short courses for flares, treatment of associated allergy, and — for refractory cases — functional endoscopic sinus surgery (FESS). Biologics (dupilumab, omalizumab, mepolizumab) are now approved for severe CRSwNP.

Allergic Rhinitis
IgE-mediated inflammation from aeroallergen exposure. Presents with sneezing, rhinorrhea, nasal congestion, pruritus, and watery eyes. Classify as seasonal (tree, grass, weed pollen) or perennial (dust mite, cockroach, mold, animal dander). Treatment: allergen avoidance, intranasal corticosteroids (first line), oral or intranasal antihistamines (azelastine, olopatadine), leukotriene receptor antagonists, and subcutaneous or sublingual immunotherapy for persistent or refractory disease.
Deviated Septum, Septal Hematoma, Septal Perforation
Septal deviation causing unilateral nasal obstruction is treated surgically with septoplasty. Septal hematoma is a post-traumatic blood collection between the cartilage and mucoperichondrium; it must be drained urgently to prevent cartilage necrosis and saddle nose deformity. Septal perforation causes crusting, epistaxis, and whistling; common causes include prior surgery, cocaine use, intranasal steroids, granulomatous disease (GPA), and nose-picking. Management: nasal hygiene, saline gel, Silastic septal button, or surgical repair.
Anosmia & Nasal Fracture
Anosmia may be conductive (obstruction from polyps, CRS) or sensorineural (post-viral including post-COVID, head trauma, neurodegenerative). Post-viral olfactory training is first line. Nasal fractures present with deformity, epistaxis, and periorbital ecchymosis; reduction (closed reduction) is performed within 7–10 days before the bones set. Rule out septal hematoma and CSF rhinorrhea on exam.
CSF Rhinorrhea
Leakage of cerebrospinal fluid through a skull-base defect, typically the cribriform plate. Causes: trauma, iatrogenic (post-sinus surgery), tumors, or spontaneous (often in obese women with elevated intracranial pressure). Clear unilateral rhinorrhea that increases with bending forward. Diagnosis: beta-2 transferrin of the fluid (gold standard). Treatment: endoscopic endonasal repair.
08 Epistaxis & Nasal Trauma Rhinology
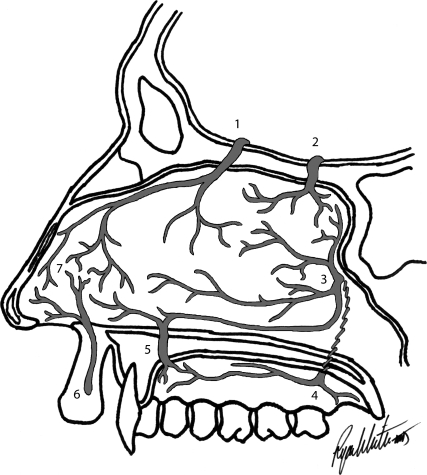
Epistaxis is overwhelmingly anterior (90%), arising from Kiesselbach's plexus at the anterior septum (Little's area), where the anterior ethmoid, superior labial, greater palatine, and sphenopalatine arteries anastomose. Posterior epistaxis originates from the sphenopalatine artery and is more common in older patients, heavier, and harder to control.
(1) Direct pressure on the cartilaginous nose for 15 minutes with the head forward. (2) Topical oxymetazoline or 4% cocaine spray plus pressure. (3) Silver nitrate cautery of a visualized anterior bleed after topical anesthesia. (4) Anterior packing with nasal tampon (Merocel, Rapid Rhino) or gauze with bacitracin. (5) Posterior packing with a Foley balloon or posterior pack (requires admission, monitoring for hypoxia/nasopulmonary reflex). (6) Endoscopic sphenopalatine artery ligation or interventional radiology embolization for refractory bleeding. Always check coagulation status, hold anticoagulants after discussion with prescriber, and humidify.
09 Laryngology — Voice & Airway Laryngology
Persistent hoarseness (dysphonia) lasting > 3 weeks, or any hoarseness in a smoker, requires laryngoscopy per the AAO-HNS dysphonia/hoarseness CPG.
Vocal Fold Lesions
Vocal fold nodules are bilateral, symmetric, callus-like thickenings at the junction of the anterior and middle thirds of the membranous cord, caused by phonotrauma (singers, teachers, cheerleaders, children who yell). Treatment is voice therapy; surgery is rarely needed. Polyps are usually unilateral, often fluid-filled or hemorrhagic, and result from acute phonotrauma; microlaryngoscopy with excision is commonly needed. Cysts (epidermoid, mucus retention) sit within the superficial lamina propria and require surgical excision to restore mucosal wave. Granulomas typically form on the vocal process of the arytenoid from intubation trauma or LPR — treat LPR, voice therapy, and consider injection of botulinum toxin or excision.
Vocal Fold Paralysis
Usually caused by recurrent laryngeal nerve injury — iatrogenic (thyroidectomy, anterior cervical spine surgery, cardiothoracic surgery), tumor along the nerve's path (lung, mediastinal, thyroid, skull base), or idiopathic. Unilateral: breathy voice, aspiration, weak cough. Bilateral: airway compromise often requiring tracheostomy, relatively preserved voice. Workup includes CT from skull base to chest to image the entire vagus/RLN course. Treatment for unilateral: voice therapy, injection medialization (hyaluronic acid, carboxymethylcellulose, calcium hydroxylapatite — temporary; Gore-Tex or silastic medialization thyroplasty with possible arytenoid adduction — permanent).
Laryngitis, LPR, and Paradoxical Vocal Fold Motion
Acute laryngitis is usually viral and self-limited; voice rest and hydration. LPR (laryngopharyngeal reflux) is the retrograde flow of gastric contents to the larynx, causing hoarseness, globus, throat clearing, cough, and posterior laryngeal erythema/edema; treatment is PPI twice daily, dietary and lifestyle changes. Paradoxical vocal fold motion (PVFM) / vocal cord dysfunction is the inappropriate adduction of the true vocal folds on inspiration, mimicking asthma; treated with respiratory retraining therapy by speech pathology.
Laryngomalacia, Subglottic Stenosis, RRP
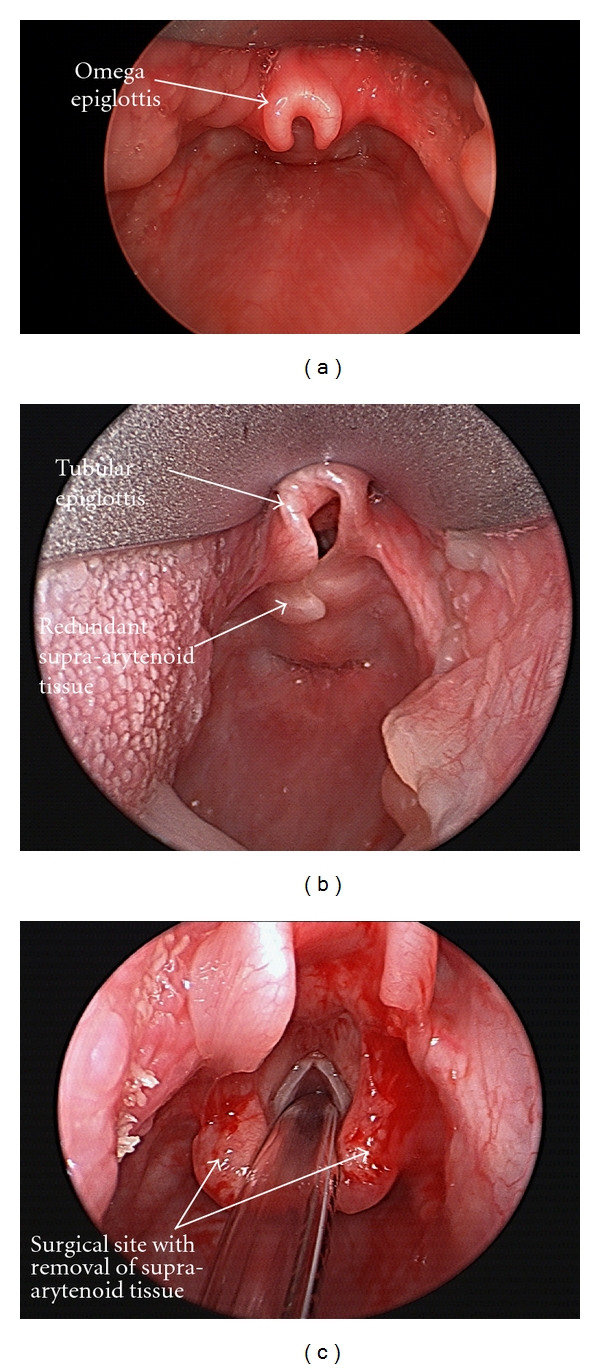
Laryngomalacia is the most common cause of infant stridor — floppy supraglottic tissues collapse inward on inspiration, producing high-pitched stridor that worsens with feeding and supine positioning. Most cases resolve by 18–24 months; severe cases undergo supraglottoplasty. Subglottic stenosis is narrowing at the cricoid level, most commonly iatrogenic (prolonged intubation) or idiopathic (young women). Managed by endoscopic dilation and steroid injection, or open cricotracheal resection. Recurrent respiratory papillomatosis (RRP) is HPV 6/11 induced squamous papillomas of the larynx causing progressive hoarseness and airway obstruction, requiring repeated microlaryngoscopy debulking.
10 Dysphagia Evaluation Laryngology
Dysphagia workup is guided by the AAO-HNS dysphagia evidence statements. Distinguish oropharyngeal dysphagia (transfer failure, coughing with meals, aspiration) from esophageal dysphagia (food sticking after swallowing). Common otolaryngology evaluations:
| Test | What It Shows | Use |
|---|---|---|
| FEES (Fiberoptic Endoscopic Evaluation of Swallowing) | Direct visualization of pharynx during swallowing with dyed food boluses | Bedside/in-office; tracks penetration, aspiration, residue |
| MBSS / VFSS (Modified Barium Swallow) | Fluoroscopic swallow study by SLP with various consistencies | Gold standard for oropharyngeal dysphagia; identifies silent aspiration |
| Video stroboscopy | High-speed imaging of mucosal wave of vocal folds | Evaluates voice, small lesions, scar |
| Esophagram / EGD | Structural esophageal assessment | For esophageal dysphagia; rules out tumor, stricture, ring |
11 Head & Neck Oncology Oncology
Over 90% of head and neck cancers are squamous cell carcinoma (SCC). Risk factors: tobacco, alcohol (synergistic with tobacco), HPV (especially HPV-16 for oropharyngeal SCC), betel nut, radiation, and poor dentition. Staging follows AJCC 8th edition and is managed per NCCN Head and Neck Cancer guidelines.
Oral Cavity SCC
Most common sites: lateral tongue, floor of mouth. Presents with a non-healing ulcer, red/white patch, pain, bleeding, loose tooth, or referred otalgia. Workup: biopsy, CT/MRI of neck, CT chest, dental evaluation pre-radiation. Treatment is primarily surgical (wide local excision ± neck dissection) with adjuvant radiation/chemoradiation for adverse features (positive margin, extranodal extension, multiple nodes, PNI/LVI).
Oropharyngeal SCC (HPV+ vs HPV−)
The oropharynx includes tonsils, base of tongue, soft palate, and posterior pharyngeal wall. HPV+ OPSCC (p16 immunohistochemistry positive) has a dramatically better prognosis and a distinct staging system in AJCC 8th edition. Common presentation: asymptomatic neck mass in a non-smoking middle-aged patient. Treatment: transoral robotic surgery (TORS) ± neck dissection with risk-based adjuvant therapy, or definitive chemoradiation. HPV− OPSCC is smoking/alcohol related with worse outcomes and usually treated with chemoradiation.
| T Stage | Criteria |
|---|---|
| Tis | Carcinoma in situ |
| T1 | Tumor ≤ 2 cm AND depth of invasion ≤ 5 mm |
| T2 | Tumor ≤ 2 cm with DOI > 5 mm, OR 2–4 cm with DOI ≤ 10 mm |
| T3 | Tumor > 4 cm OR DOI > 10 mm |
| T4a | Invades cortical bone, inferior alveolar nerve, maxillary sinus, or facial skin (moderately advanced) |
| T4b | Invades masticator space, pterygoid plates, skull base, or encases ICA (very advanced) |
| N Stage | Criteria |
|---|---|
| N0 | No regional lymph node metastasis |
| N1 | Unilateral nodal mets, all ≤ 6 cm |
| N2 | Contralateral or bilateral nodal mets, all ≤ 6 cm |
| N3 | Any lymph node > 6 cm |
Laryngeal SCC
Subsites: supraglottic, glottic (most common, best prognosis due to early hoarseness and sparse lymphatics), subglottic (rarest, worst prognosis). Early-stage glottic cancer (T1/T2) treated with transoral laser microsurgery (TLM) or radiation. Advanced cancer: chemoradiation (organ preservation) or total laryngectomy with voice rehabilitation (TEP, electrolarynx, esophageal speech).
Hypopharyngeal, Nasopharyngeal & Sinonasal Tumors
Hypopharyngeal SCC presents late with dysphagia, odynophagia, and neck mass; poor prognosis. Nasopharyngeal carcinoma (NPC) is EBV-associated (non-keratinizing types), endemic in Southern Chinese populations; primary treatment is chemoradiation. Sinonasal tumors (SCC, adenocarcinoma, esthesioneuroblastoma, sinonasal undifferentiated carcinoma, inverted papilloma) often present late with unilateral nasal obstruction, epistaxis, or facial numbness; treatment usually combines endoscopic or open resection with radiation.
12 Salivary Gland Disease Oncology
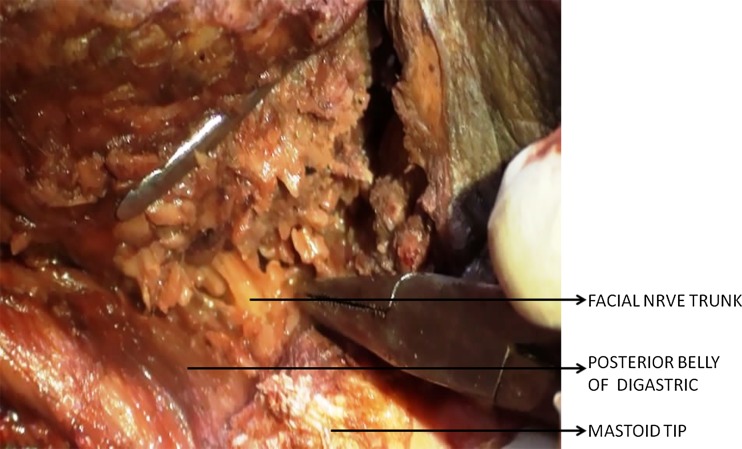
The major salivary glands are the parotid, submandibular, and sublingual. Parotid tumors are most common and the majority (~80%) are benign; the smaller the gland the higher the probability of malignancy (sublingual tumors are ~80% malignant). The facial nerve runs through the parotid, dividing it into superficial and deep lobes; this is the critical structure preserved during parotidectomy.
| Tumor | Behavior | Notes |
|---|---|---|
| Pleomorphic adenoma | Benign, most common salivary tumor | Slow-growing, can recur if incompletely excised; small risk of malignant transformation |
| Warthin tumor | Benign | Often bilateral, strong association with smoking, almost always parotid |
| Mucoepidermoid carcinoma | Malignant, most common salivary malignancy | Low- to high-grade; variable prognosis |
| Adenoid cystic carcinoma | Malignant | Perineural invasion is characteristic; indolent but relentless; late distant recurrence common |
| Acinic cell carcinoma | Malignant (typically low-grade) | Usually parotid |
Sialadenitis & Sialolithiasis
Acute bacterial sialadenitis (classically S. aureus in the parotid of dehydrated elderly patients) presents with painful, swollen gland and purulent drainage from the duct. Treatment: hydration, sialogogues (lemon drops), warm massage, and antibiotics. Sialolithiasis (stones) most commonly affects the submandibular gland (Wharton duct) due to viscous secretions and uphill drainage; presents with postprandial swelling and pain. Small stones may be removed transorally or via sialendoscopy; large obstructing stones or recurrent sialadenitis may require gland excision.
13 Neck Masses & Congenital Lesions Oncology
The age of the patient guides the differential. In children: reactive lymphadenopathy (most common), congenital cysts (thyroglossal duct, branchial cleft), lymphatic malformations, and lymphoma. In young adults: reactive/infectious, lymphoma, thyroid nodules. In adults > 40 with a neck mass persisting > 2 weeks, assume metastatic squamous cell carcinoma until proven otherwise per the AAO-HNS neck mass CPG. Workup: careful H&P including flexible laryngoscopy, CT neck with contrast, and FNA. Do NOT open-biopsy an unknown neck mass — it violates oncologic planes.
Thyroglossal Duct Cyst
Midline neck cyst that moves upward with swallowing or tongue protrusion. Arises from failed obliteration of the thyroglossal duct. Treatment is the Sistrunk procedure (excision of the cyst with central portion of the hyoid bone).
Branchial Cleft Cyst
Lateral neck cyst anterior to the sternocleidomastoid, most commonly second branchial cleft (level II/III). Typically presents in young adults after a URI inflames the cyst. Treatment is surgical excision.
14 Sleep-Disordered Breathing & OSA Sleep
Obstructive sleep apnea (OSA) is recurrent collapse of the upper airway during sleep. ENT is often consulted for surgical management when CPAP fails. Evaluation includes polysomnography (AHI: mild 5–14, moderate 15–29, severe ≥ 30), Mallampati score, tonsil size, BMI, and airway endoscopy (drug-induced sleep endoscopy, DISE). Surgical options include tonsillectomy (highly effective in children), septoplasty/turbinate reduction (nasal adjunct), uvulopalatopharyngoplasty (UPPP), tongue base reduction, maxillomandibular advancement (MMA, the most effective adult skeletal procedure), and hypoglossal nerve stimulation (Inspire) for moderate-to-severe OSA in CPAP-intolerant adults with BMI below a set threshold and favorable DISE anatomy.
15 Pediatric ENT Pediatric
Recurrent AOM & Otitis Media with Effusion (OME)
Recurrent AOM (3 episodes in 6 months or 4 in 12 months with at least one in the past 6 months) and chronic OME with hearing loss are common indications for tympanostomy tube (T-tube) placement. Per the AAO-HNS tympanostomy tubes CPG, tubes are indicated for bilateral OME ≥ 3 months with documented hearing difficulty, and for recurrent AOM with effusion at evaluation. Adenoidectomy is often combined if age > 4 or if there is nasal obstruction.
Tonsillectomy (Recurrent Tonsillitis & OSA)
Per the AAO-HNS tonsillectomy CPG, indications include the Paradise criteria (7 episodes in 1 year, 5/year for 2 years, or 3/year for 3 years with documented fever, exudate, tender cervical nodes, or positive strep) and sleep-disordered breathing. Perioperative dexamethasone is recommended; pain control includes acetaminophen and ibuprofen (NSAIDs no longer contraindicated). Counsel about post-tonsillectomy hemorrhage (primary < 24 hours, secondary 5–10 days postop).
Other Pediatric ENT
Laryngomalacia (most common infant stridor), choanal atresia (bilateral presents with cyclic cyanosis relieved by crying — neonatal airway emergency, part of CHARGE syndrome), subglottic stenosis, tongue tie (ankyloglossia) treated with frenotomy, foreign body airway/esophageal (airway FB: coughing, wheezing, unilateral decreased breath sounds, bronchoscopy; esophageal FB: drooling, dysphagia, esophagoscopy — button batteries and high-powered magnets are emergencies), and vascular rings causing stridor and feeding difficulties.
16 Deep Neck Space Infections Pediatric
Deep neck infections can rapidly compromise the airway, spread to the mediastinum (descending necrotizing mediastinitis), or cause septic thrombophlebitis of the internal jugular vein (Lemierre syndrome). Any patient with trismus, drooling, muffled "hot potato" voice, stridor, or a "tripod" posture needs urgent airway assessment.
Peritonsillar Abscess (Quinsy)
Collection between the tonsil capsule and the superior constrictor muscle. Presents with severe unilateral throat pain, trismus, uvular deviation to the contralateral side, muffled voice, and fever. Treatment is incision and drainage (or needle aspiration) plus antibiotics (ampicillin-sulbactam or clindamycin). Consider immediate tonsillectomy ("quinsy tonsillectomy") in select cases.
Retropharyngeal & Parapharyngeal Abscess
Both are deep neck space infections best imaged by CT neck with contrast. Retropharyngeal abscess classically presents in young children with fever, neck stiffness, and drooling; parapharyngeal with neck swelling and trismus. Treatment is IV antibiotics and surgical drainage when mature or causing airway compromise.
Ludwig Angina
Rapidly progressive cellulitis of the submandibular, sublingual, and submental spaces, usually from a dental infection of a lower molar. Elevated floor of mouth and tongue, drooling, trismus, and impending airway obstruction. Airway management (often awake fiberoptic intubation or tracheostomy) takes precedence; then IV antibiotics and drainage.
17 Facial Plastics & Reconstruction Facial Plastics
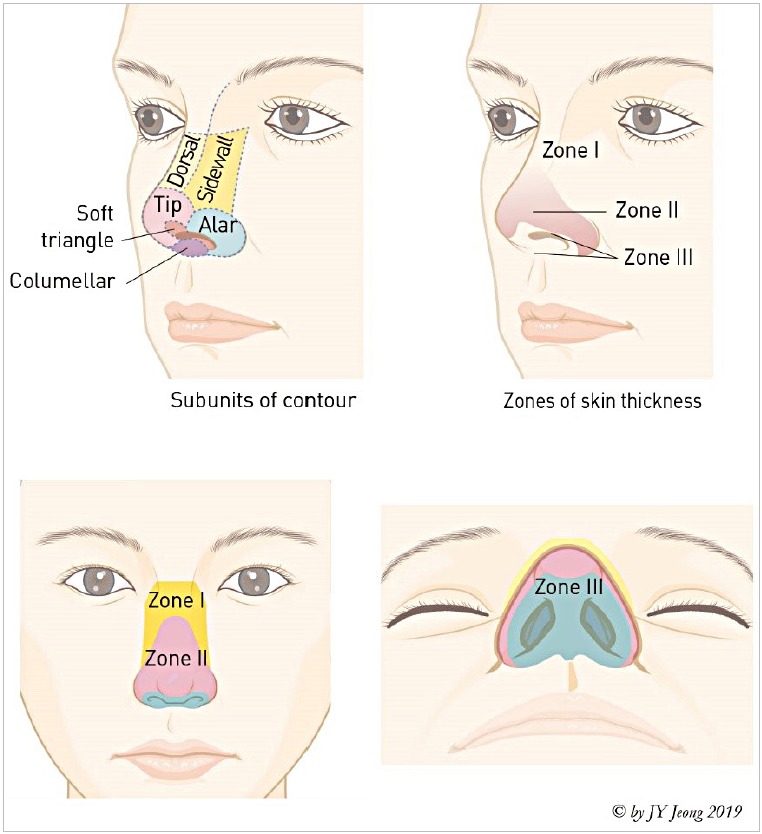
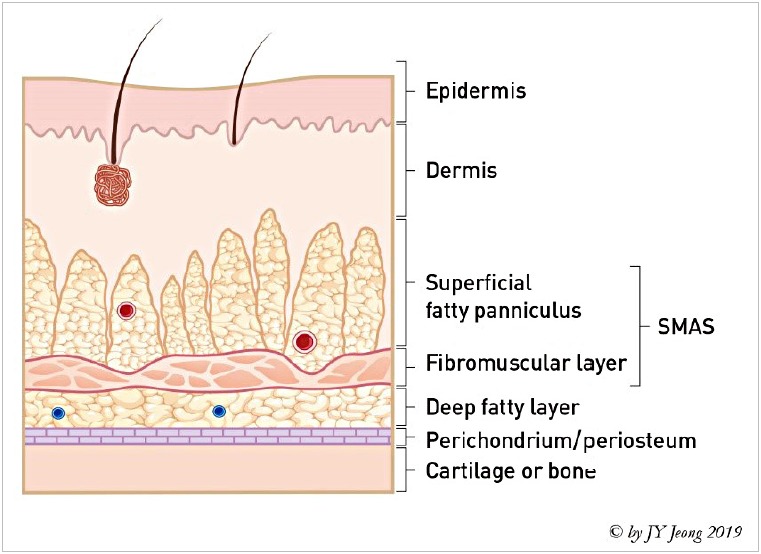
Facial plastic & reconstructive surgery encompasses cosmetic and functional procedures of the face and neck. Common procedures performed or comanaged by ENT: rhinoplasty (cosmetic and functional — often combined with septoplasty as septorhinoplasty), otoplasty (ear pinning for prominent ears), blepharoplasty (upper and lower eyelid), rhytidectomy (facelift), brow lift, neck lift, Mohs reconstruction (for defects after skin cancer resection using local flaps, regional flaps, or full/split-thickness grafts), and scar revision. Microvascular free flap reconstruction for large head and neck cancer defects uses flaps such as radial forearm, anterolateral thigh (ALT), fibula (with bone for mandibular reconstruction), and latissimus dorsi.
18 ENT Procedures — A to Z
| Procedure | Description / Indication |
|---|---|
| Tympanostomy tube placement | Myringotomy + PE tube for OME, rAOM |
| Myringotomy | Incision of TM for drainage |
| Tympanoplasty | Repair of TM perforation with fascia/cartilage graft |
| Stapedectomy / stapedotomy | Prosthetic replacement of stapes for otosclerosis |
| Tympanomastoidectomy (CWU / CWD) | For cholesteatoma and chronic ear disease |
| Cochlear implant | Electrode array in scala tympani for severe/profound SNHL |
| BAHA (bone-anchored hearing aid) | Osseointegrated implant for CHL, mixed HL, SSD |
| Eustachian tube dilation | Balloon catheter dilation for refractory ETD |
| Septoplasty | Correction of deviated nasal septum |
| Turbinate reduction | Submucosal, microdebrider, or radiofrequency |
| FESS | Functional endoscopic sinus surgery for CRS |
| Balloon sinuplasty | Office or OR balloon dilation of sinus ostia |
| Septorhinoplasty | Combined functional + cosmetic nasal surgery |
| Tonsillectomy | Cold steel, coblation, or electrocautery; for recurrent tonsillitis or OSA |
| Adenoidectomy | Curette or microdebrider removal of adenoid pad |
| UPPP | Uvulopalatopharyngoplasty for OSA |
| Hypoglossal nerve stimulator (Inspire) | Implanted neurostimulator for moderate-severe OSA |
| Sialendoscopy | Endoscopic salivary duct exploration and stone retrieval |
| Parotidectomy (superficial / total) | With facial nerve monitoring and preservation |
| Submandibular gland excision | Via transcervical approach; care for marginal mandibular nerve |
| Microlaryngoscopy with lesion excision | For nodules, polyps, cysts, papilloma, early cancer |
| In-office vocal fold injection | Temporary medialization for vocal fold paralysis |
| Medialization thyroplasty (Type 1) | Permanent vocal fold medialization via neck incision |
| Neck dissection (selective / modified radical / radical) | Lymph node removal for head and neck cancer |
| Total laryngectomy | Removal of larynx for advanced laryngeal cancer; creates permanent stoma |
| Glossectomy / mandibulectomy / composite resection | Oral cavity cancer resection |
| Tracheostomy (open / percutaneous) | Surgical airway for prolonged ventilation, obstruction, secretion management |
| Cricothyroidotomy | Emergency airway through cricothyroid membrane |
| Foreign body removal | Ear, nose, throat, esophagus, airway |
| Drainage of peritonsillar / retropharyngeal abscess | I&D or needle aspiration |
19 ENT Imaging & Diagnostics
| Study | Key Uses |
|---|---|
| CT sinus (without contrast) | Chronic rhinosinusitis, preoperative FESS planning; scored by Lund-Mackay |
| CT neck with contrast | Neck mass workup, abscess, head and neck cancer staging |
| CT temporal bone | Cholesteatoma, temporal bone fracture, malignant OE |
| MRI IAC with gadolinium | Vestibular schwannoma, retrocochlear SNHL workup |
| MRI neck with contrast | Tongue, skull base, perineural spread evaluation |
| PET/CT | Initial staging of advanced head and neck cancer; treatment response assessment at 12 weeks post-CRT |
| Ultrasound with FNA | Thyroid nodules, cervical lymph nodes, salivary masses |
| Audiogram / tympanogram | Hearing loss workup, ETD, middle ear effusion |
| Polysomnography | OSA diagnosis and severity |
| FEES / MBSS | Swallowing evaluation |
| Video stroboscopy | Voice disorders, vocal fold mucosal wave assessment |
Tympanometry types: Type A normal middle ear compliance; Type As shallow (stiffness, e.g., otosclerosis); Type Ad deep (ossicular discontinuity); Type B flat (effusion or perforation — correlate with canal volume); Type C negative middle ear pressure (ETD).
20 Medications You Must Know
Antibiotics
| Drug | Typical Use in ENT |
|---|---|
| Amoxicillin (high-dose) | First-line AOM in children |
| Amoxicillin-clavulanate (Augmentin) | ABRS, recurrent AOM, peritonsillar abscess, sialadenitis |
| Cefdinir / cefpodoxime | AOM/ABRS in non-anaphylactic PCN allergy |
| Ceftriaxone IM | AOM failure, severe infections |
| Azithromycin | Alternative for PCN-allergic patients; pharyngitis |
| Levofloxacin | Recurrent sinusitis in PCN-allergic adults; malignant OE |
| Clindamycin | Deep neck infections, tonsillitis, dental source |
| Piperacillin-tazobactam / ceftazidime | Malignant otitis externa (antipseudomonal) |
Otic Drops
| Drug | Use / Notes |
|---|---|
| Ciprofloxacin-dexamethasone (Ciprodex) | AOE, tube otorrhea; safe with perforation |
| Ofloxacin otic | AOE, chronic suppurative OM; safe with perforation |
| Neomycin-polymyxin-hydrocortisone (Cortisporin) | AOE with intact TM only (neomycin ototoxic) |
| Acetic acid 2% | Fungal/bacterial AOE adjunct; acidifies canal |
| Clotrimazole solution | Otomycosis |
Nasal & Allergy Medications
| Drug | Class / Use |
|---|---|
| Fluticasone, mometasone, budesonide | Intranasal corticosteroids; first-line AR and CRS |
| Azelastine, olopatadine | Intranasal antihistamines |
| Loratadine, cetirizine, fexofenadine | Oral second-generation antihistamines |
| Oxymetazoline (Afrin) | Topical decongestant; limit to 3 days (rhinitis medicamentosa) |
| Pseudoephedrine | Oral decongestant; caution with HTN, cardiac disease |
| Montelukast | Leukotriene antagonist; AR, CRSwNP, aspirin-sensitive triad |
| Dupilumab, omalizumab, mepolizumab | Biologics for severe CRSwNP |
| Prednisone taper (Medrol Dosepak) | CRS flare, Bell palsy, SSNHL, severe AR |
Vestibular / Meniere / Other
| Drug | Use |
|---|---|
| Meclizine | Vestibular suppressant (NOT for BPPV); acute vertigo, motion sickness |
| Diazepam, lorazepam | Short-term vestibular suppression |
| Ondansetron, promethazine | Antiemetics for vertigo-associated nausea |
| Scopolamine patch | Motion sickness, refractory vertigo |
| HCTZ + triamterene | Meniere disease diuretic therapy |
| Betahistine | Meniere disease (outside US mainly) |
| PPI (omeprazole, pantoprazole) | LPR, reflux laryngitis |
| Topical epinephrine / TXA | Epistaxis adjunct |
21 Classification Systems
Diagnose ABRS when a patient has signs/symptoms of ARS AND any one of the following:
- Persistent symptoms lasting ≥ 10 days without improvement
- Severe onset — high fever (≥ 39°C) with purulent nasal discharge or facial pain lasting 3–4 consecutive days at the beginning of illness
- Double worsening — a typical viral URI that improves then worsens within 10 days with new fever, headache, or increased nasal discharge
Symptoms of ARS include purulent nasal drainage accompanied by nasal obstruction or facial pain/pressure/fullness.
History of recurrent vertigo triggered by position change PLUS positive Dix-Hallpike maneuver defined as: transient upbeating-torsional (geotropic) nystagmus of the affected ear, latency of 2–5 seconds after positioning, duration < 60 seconds, and fatigability on repeat testing. Horizontal canal BPPV is diagnosed by the supine roll test with horizontal nystagmus.
| Grade | Tonsil Size |
|---|---|
| 0 | Tonsils in fossa, not visible |
| 1+ | Tonsils occupy < 25% of oropharyngeal width |
| 2+ | 25–50% |
| 3+ | 50–75% |
| 4+ | > 75% ("kissing tonsils") |
| Class | Visible Structures (mouth open, tongue out) |
|---|---|
| I | Soft palate, uvula, fauces, tonsillar pillars |
| II | Soft palate, uvula, fauces |
| III | Soft palate, base of uvula |
| IV | Hard palate only |
Combines tonsil size, Friedman tongue position, and BMI to predict UPPP success. Stage I (favorable anatomy) has the best surgical outcomes; Stage IV typically requires multilevel surgery or skeletal advancement.
Scores each of 5 paired sinus regions (maxillary, anterior ethmoid, posterior ethmoid, sphenoid, frontal) 0 (clear) / 1 (partial) / 2 (total opacification), plus 0/2 for the ostiomeatal complex. Max 12 per side, 24 total. Score > 4 supports CRS in the right clinical context.
Skin prick testing graded 0–4+ by wheal size. SAC (Seasonal Allergic Conjunctivitis) and PAC (Perennial Allergic Conjunctivitis) scores and the TNSS (Total Nasal Symptom Score) are used to quantify symptom burden in allergic rhinitis trials and clinic follow-up. The SNAP test and SNAP-25 refer to Sinonasal Assessment Protocol questionnaires for outcome tracking.
22 Physical Exam — The ENT Exam
The ENT exam is fast, focused, and repeats on every patient. A complete exam has ear, nose, oral cavity/oropharynx, neck, and cranial nerve components; most encounters add flexible laryngoscopy.
Ears: Auricles normal. EACs patent without debris or erythema.
TMs intact, translucent, with normal landmarks; mobility normal on pneumatic otoscopy.
Nose: External nose symmetric. Septum midline. Turbinates without edema or polyps.
Mucosa pink and moist. No purulence.
Oral cavity/OP: Lips, tongue, floor of mouth, buccal mucosa without lesion.
Tonsils 1+/1+ without exudate. Palate elevates symmetrically. Dentition in good repair.
Neck: Supple, no cervical, submandibular, or supraclavicular lymphadenopathy.
Thyroid non-tender, no nodules. Trachea midline.
CN II–XII: Grossly intact.
Flex laryngoscopy: Nasopharynx clear. BOT/vallecula normal. Epiglottis normal.
Bilateral TVFs with full mobility and no lesions. Airway patent.
For vestibular complaints you will also document the Dix-Hallpike maneuver (with the result: "positive, with right-beating torsional nystagmus on right-sided positioning"), head impulse test (HIT), head-shake nystagmus, Romberg, and gait. For facial nerve: House-Brackmann grade on every visit. For hearing loss: tuning fork tests (Weber lateralizes to the ear with CHL or the contralateral ear in SNHL; Rinne AC > BC normal or SNHL, BC > AC indicates CHL). Frenzel goggles remove visual fixation and help identify subtle spontaneous or positional nystagmus.
23 Abbreviations Master List
Anatomy
Diagnoses
Procedures
24 Sample HPI Templates
"Mr. [Name] is a 42-year-old male with a longstanding history of right ear drainage and gradually worsening hearing, presenting for otology evaluation. He reports approximately 15 years of intermittent foul-smelling right otorrhea, minimally responsive to multiple courses of topical antibiotics. He endorses progressive right-sided hearing loss, occasional vertiginous episodes, and new right-sided facial twitching over the past month. Denies otalgia, fevers, or headaches. PMHx notable for recurrent AOM as a child. On otoscopy, the right EAC contains keratin debris; after cleaning, there is a large attic retraction pocket with white keratin mass consistent with cholesteatoma. The left ear is normal. Audiogram demonstrates a right mixed hearing loss with PTA 55 dB and ABG of 35 dB. CT temporal bone obtained today shows a soft tissue mass in the epitympanum and antrum with ossicular erosion."
"Ms. [Name] is a 35-year-old female with a 2-year history of nasal obstruction, facial pressure, thick post-nasal drainage, and decreased sense of smell, presenting for evaluation of refractory chronic rhinosinusitis. She has completed 3 courses of amoxicillin-clavulanate and a Medrol Dosepak over the last 6 months with only temporary improvement. She uses fluticasone nasal spray and daily saline sinus rinses. PMHx includes mild persistent asthma and aspirin sensitivity. On anterior rhinoscopy and flexible endoscopy, bilateral grade 2 nasal polyps are visualized in the middle meatus with purulent drainage. CT sinus demonstrates pan-sinus mucosal thickening with a Lund-Mackay score of 18/24. Discussion today focuses on FESS versus initiation of biologic therapy with dupilumab given the aspirin-exacerbated respiratory disease phenotype."
"Ms. [Name] is a 29-year-old elementary school teacher presenting with 4 months of progressive hoarseness, vocal fatigue, and reduced pitch range. She denies hemoptysis, dysphagia, odynophagia, weight loss, or referred otalgia. No tobacco use. She drinks coffee throughout the day and describes frequent throat clearing and globus sensation suggestive of LPR. Voice use is heavy — 6 hours of teaching with minimal amplification. Flexible laryngoscopy today demonstrates bilateral symmetric fusiform lesions at the junction of the anterior and middle thirds of the true vocal folds, consistent with vocal nodules. Posterior laryngeal erythema and interarytenoid edema also noted. Plan includes voice therapy with SLP, omeprazole 20 mg BID for presumed LPR, and reflux precautions with re-evaluation in 8 weeks. Stroboscopy scheduled prior to next visit."
"Mr. [Name] is a 58-year-old male presenting with 6 months of progressive left-sided hearing loss and constant left-sided high-pitched tinnitus. He denies vertigo, facial numbness or weakness, or headaches. No noise exposure or ototoxic medications. Weber lateralizes to the right; Rinne is AC > BC bilaterally. Audiogram demonstrates a left-sided high-frequency SNHL with PTA 40 dB and word recognition score of 68% on the left compared to 100% on the right. Given the asymmetric SNHL and poor word recognition, MRI of the internal auditory canals with gadolinium is ordered to rule out vestibular schwannoma."
"Mr. [Name] is a 62-year-old male with a 30-pack-year smoking history and heavy alcohol use presenting with a right level II neck mass noted 6 weeks ago, gradually enlarging. He endorses referred right otalgia and mild odynophagia but denies hoarseness, hemoptysis, or weight loss. On exam, a firm, non-tender, 3 cm mobile mass is palpated at the angle of the right mandible. Flexible laryngoscopy reveals a right tonsillar lesion with surface irregularity extending to the base of tongue. CT neck with contrast demonstrates a 3.2 cm right tonsillar mass with a 3 cm necrotic level II node. FNA of the node is planned today; biopsy of the tonsillar primary will be obtained under anesthesia along with panendoscopy. Concern is high for HPV-related oropharyngeal SCC pending p16 immunohistochemistry."
"Mrs. [Name] is a 67-year-old female presenting with 5 days of recurrent brief vertigo triggered by rolling over in bed, looking up, and bending forward. Each episode lasts about 20–30 seconds and is associated with nausea but no hearing change, tinnitus, or aural fullness. No headache, facial weakness, diplopia, or focal neurologic symptoms. Right Dix-Hallpike maneuver today is positive with upbeating-torsional nystagmus with 3-second latency, 20-second duration, and fatigability on repeat testing, consistent with right posterior canal BPPV. Left Dix-Hallpike is negative. Epley maneuver performed in clinic with resolution of symptoms on repeat positional testing. Patient counseled on home Brandt-Daroff exercises if symptoms recur."
ENT is a high-volume, high-variety specialty. On a single morning you may see a 3-year-old with recurrent otitis media, an opera singer with a vocal fold cyst, a diabetic with malignant otitis externa, and a retiree with a suspicious neck mass. A great scribe keeps each note's language specific to the subspecialty domain: otology terms for the ear case, voice terms for the singer, oncologic staging for the neck mass. You will hear the clinician move through the otoscopy, nasal endoscopy, and laryngoscopy in rapid succession — learn the clinician's phrasing cadence so you can pre-populate the exam template and only modify what is abnormal.
Know the guidelines cold for the high-volume bread-and-butter conditions: AOM antibiotic choice, adult sinusitis criteria, dysphonia red flags, tonsillectomy (Paradise) criteria, and the BPPV algorithm. Know when the surgeon will order an MRI IAC (asymmetric SNHL) versus a CT sinus (preoperative FESS) versus a CT neck with contrast (neck mass workup). Know your anatomy — especially neck levels, sinus drainage pathways, and facial nerve branches — because it shows up in every op note you will write.
Welcome to otolaryngology. Few specialties are as breadth-demanding, and few are more rewarding to support.
25 References & Sources
Clinical Practice Guidelines
AAO-HNSF Dysphagia Evidence Summary. Otolaryngol Head Neck Surg. 2018.
NCCN Clinical Practice Guidelines in Oncology: Head and Neck Cancers.
Diagram & Figure Sources
Figure 1: Outer Ear Anatomy. OpenStax College. CC BY 3.0.
Figure 2: Middle Ear. OpenStax College. CC BY 3.0.
Figure 3: Cochlea. OpenStax College. CC BY 3.0.
Figure 4: Paranasal Sinuses. Wikimedia Commons. Public domain.
Figure 5: Pharynx Anatomy. NIH/NCI, Wikimedia Commons. Public domain.
Figure 6: External Larynx. Wikimedia Commons. Public domain.
Figure 7: Vocal Folds (endoscopic view). Wikimedia Commons. Public domain.