Family Medicine
Every diagnosis, condition, procedure, medication, screening guideline, and documentation framework you need to scribe primary care from day one and beyond.
All diagrams on this page are sourced from published educational or institutional materials rather than AI generation. Each figure caption links to the original source, and the full diagram and guideline citations are collected in the references section at the bottom.
01 Primary Care Foundations — The Family Medicine Philosophy
Family medicine is the broadest specialty in American medicine. A family physician cares for patients of every age, every sex, every organ system, and every stage of life — from the newborn nursery visit to end-of-life care. The scribe supporting a family physician must therefore be prepared to document an enormous range of encounters in a single clinic day: a 9-month well-child check, a medication refill for hypertension and type 2 diabetes, an ankle sprain, a contraception consultation, a depression follow-up, a Medicare annual wellness visit, and a pre-op clearance — all before lunch.
Unlike subspecialists, family physicians practice continuity of care: they know the patient, the spouse, and often the children and parents. This changes documentation. You will routinely see references to family context ("patient's husband was just diagnosed with pancreatic cancer, she is overwhelmed"), long-standing habits ("continues to smoke despite multiple cessation attempts over 15 years"), and social determinants ("lost insurance last month, unable to afford metformin").
The Four Principles of Primary Care
Primary care is defined by four principles coined by Barbara Starfield: first contact (patients present here first, with any problem), continuity (an ongoing relationship over years), comprehensiveness (managing all of a patient's health needs rather than a single organ), and coordination (integrating specialty care back into a unified plan). Every note a scribe writes should reinforce these principles — document the patient as a whole person, not as an isolated complaint.
Organ Systems You Will Document Every Day
Family medicine does not belong to a single organ system. Instead, a scribe must hold at least a working map of every major system: cardiovascular (HTN, dyslipidemia, CAD, heart failure), endocrine (diabetes, thyroid, adrenal, obesity), pulmonary (asthma, COPD, URIs, OSA), GI (GERD, IBS, constipation, hepatitis), musculoskeletal (back, knee, shoulder, neck), neurologic (headache, dizziness, neuropathy, dementia), psychiatric (depression, anxiety, ADHD, insomnia), dermatologic (rashes, lesions, acne, eczema), genitourinary (UTI, BPH, erectile dysfunction, STIs), women's health (contraception, menstrual disorders, menopause, prenatal), and pediatric (well-child, fevers, otitis, immunizations).
Family medicine encounters often contain five or six active problems in a single visit. Your job is not to write five separate HPIs — it is to identify the chief reason for today's visit and weave the other problems into the assessment & plan as chronic-problem follow-ups. Always ask the physician, "Is this a follow-up for all of her problems, or just the knee?" before you start typing the HPI.
02 Scribe Documentation Framework
Family medicine notes follow the SOAP format but add a heavy emphasis on problem-based charting — each active chronic or acute issue is addressed individually in the assessment and plan, with its own brief status update and plan. Most EMRs (Epic, Athena, eClinicalWorks) pre-populate problem lists from prior visits; your job is to update each entry with today's data.
Chief Complaint (CC): Short phrase stating the reason for today's visit. Examples: "annual physical," "follow-up HTN and DM," "sore throat x 3 days," "knee pain," "medication refill."
HPI: Use OLDCARTS (Onset, Location, Duration, Character, Aggravating/Alleviating, Radiation, Timing, Severity) for acute complaints. For chronic-disease follow-ups, write an interval history — what has happened since the last visit, symptom control, adherence, side effects, home monitoring data (home BP log, home glucose log, peak flow diary).
ROS: Problem-focused. Most primary care visits document a 2–4 system ROS tied to the chief complaint. Annual physicals require a more complete 10–14 system ROS.
PMHx, PSHx, Meds, Allergies, SHx, FHx: Verified and updated every visit. Social history in family medicine is dense: tobacco (pack-years, quit date, method), alcohol (drinks/week, AUDIT-C if screened), recreational drugs, occupation, housing, exercise, diet, relationships, firearm access when relevant, domestic violence screening, and sexual history (partners, protection, orientation).
Vitals: BP (averaged if elevated), HR, RR, temperature, SpO2, weight, height, BMI, waist circumference when obesity is addressed. Pediatric visits add head circumference (< 24 months) and plot on growth curves (WHO 0–2 years, CDC 2–20 years).
Physical Exam: A focused general exam — General, HEENT, Neck, CV, Lungs, Abdomen, Extremities, Skin, Neuro, Psych. Document only the systems examined. Annual physicals add breast, pelvic, genitourinary, rectal exams as indicated.
Results: Recent labs (A1C, lipid panel, CMP, CBC, TSH), imaging results, POC tests (UA, strep, flu, glucose, INR, urine pregnancy, A1C in-office), and home monitoring data.
Format each active problem separately:
1. Hypertension — controlled, home BPs averaging 128/78. Continue lisinopril 20 mg daily. Recheck BP in 3 months. Labs — BMP for K+/Cr in 6 months.
2. Type 2 diabetes — A1C 7.1% (target <7.0%). Continue metformin 1000 mg BID. Add empagliflozin 10 mg daily given CVD risk. Diabetic eye exam due. Recheck A1C in 3 months.
3. Health maintenance — Due for shingles #2 today, colonoscopy referral placed, influenza vaccine given.
For every chronic disease follow-up, document: (1) current control status (controlled/uncontrolled), (2) latest objective data (home BP, A1C, weight trend), (3) adherence & side effects, and (4) next step (continue, titrate, add, refer). This four-part mini-assessment makes every note auditable and billable.
03 Hypertension (HTN) Cardiovascular
Hypertension is the single most common diagnosis in primary care. Nearly half of all American adults meet the 2017 ACC/AHA criteria, and every family physician manages dozens of hypertensive patients per day. A scribe working in primary care will chart HTN on most of their encounters.
Diagnosis & Staging
The 2017 ACC/AHA Hypertension Guideline reclassified blood pressure categories — you will see these thresholds used in every adult note.
| Category | Systolic | Diastolic |
|---|---|---|
| Normal | < 120 | and < 80 |
| Elevated | 120–129 | and < 80 |
| Stage 1 HTN | 130–139 | or 80–89 |
| Stage 2 HTN | ≥ 140 | or ≥ 90 |
| Hypertensive Urgency | ≥ 180 | and/or ≥ 120 (no end-organ damage) |
| Hypertensive Emergency | ≥ 180 | and/or ≥ 120 WITH end-organ damage |
Workup
Initial workup of newly diagnosed HTN: CMP (creatinine, electrolytes, glucose), lipid panel, TSH, urinalysis with albumin-to-creatinine ratio, EKG, and HbA1c. Home BP monitoring confirms the diagnosis and rules out white coat hypertension.
Management
Lifestyle first: DASH diet, sodium < 1500 mg/day, weight loss (1 mmHg per kg), aerobic exercise, alcohol limits, smoking cessation. First-line drugs per JNC-8 and ACC/AHA: thiazide diuretic (HCTZ, chlorthalidone), ACE-inhibitor (lisinopril), ARB (losartan), or calcium channel blocker (amlodipine). Black patients without CKD start with thiazide or CCB. Patients with CKD or diabetes start with ACE-I or ARB. Target BP < 130/80 for most adults.
BP > 180/120 plus acute target organ damage (chest pain, dyspnea, headache with neuro deficits, vision loss, AKI, papilledema) — send to ED immediately for IV therapy. Urgency without end-organ damage is managed with oral agents and close follow-up.
When the physician calls out a BP number in clinic, note whether it is a single in-office reading, the average of repeat readings, or a home BP log average. Documentation accuracy here determines whether the patient meets diagnostic thresholds.
04 Dyslipidemia & Lipid Management Cardiovascular
Dyslipidemia is managed in primary care based on 10-year atherosclerotic cardiovascular disease (ASCVD) risk. The 2018 AHA/ACC Cholesterol Guideline is the standard of care.
Statin Benefit Groups
| Group | Therapy |
|---|---|
| Clinical ASCVD (MI, stroke, PAD, CAD) | High-intensity statin |
| LDL ≥ 190 mg/dL | High-intensity statin |
| Diabetes, age 40–75, LDL 70–189 | Moderate or high-intensity statin |
| Age 40–75, LDL 70–189, 10-yr ASCVD ≥ 7.5% | Moderate-intensity statin (risk discussion) |
Statin Intensity
High-intensity: atorvastatin 40–80 mg, rosuvastatin 20–40 mg (≥ 50% LDL reduction). Moderate: atorvastatin 10–20, rosuvastatin 5–10, simvastatin 20–40, pravastatin 40–80 (30–49% LDL reduction). Add-ons when LDL target not met: ezetimibe 10 mg, PCSK9 inhibitors (alirocumab, evolocumab), bempedoic acid, icosapent ethyl (for elevated triglycerides with CVD).
Check a baseline lipid panel, LFTs, and CK at initiation. Repeat lipids in 4–12 weeks after starting or titrating, then every 3–12 months. Ask about muscle symptoms at every visit.
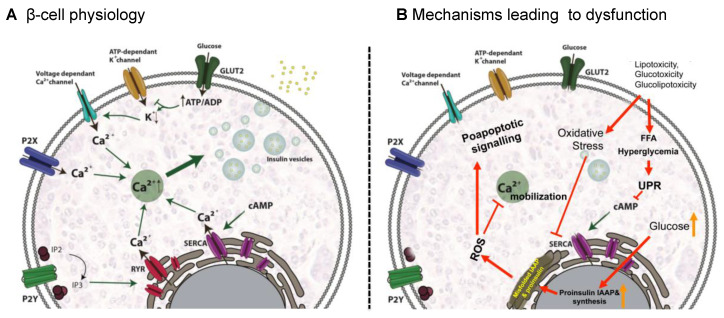
05 Type 2 Diabetes, Prediabetes & Obesity Endocrine
Diabetes management is a dominant share of any primary care panel. The ADA Standards of Care are updated annually and govern diagnostic thresholds, glycemic targets, and medication selection.
Diagnosis
| Category | A1C | FPG | 2-hr OGTT |
|---|---|---|---|
| Normal | < 5.7% | < 100 | < 140 |
| Prediabetes | 5.7–6.4% | 100–125 | 140–199 |
| Diabetes | ≥ 6.5% | ≥ 126 | ≥ 200 |
Glycemic Targets
General adult target A1C < 7.0%. Stricter (< 6.5%) for young, healthy, no hypoglycemia risk. Looser (< 8.0%) for elderly, frail, limited life expectancy, multiple comorbidities, history of severe hypoglycemia. Home fasting glucose 80–130 mg/dL; postprandial < 180 mg/dL.
Medication Cascade
Metformin 500–1000 mg BID remains first-line. Add agents based on comorbidities: GLP-1 receptor agonists (semaglutide, liraglutide, tirzepatide) for ASCVD, obesity, or CKD; SGLT2 inhibitors (empagliflozin, dapagliflozin) for heart failure, CKD, or ASCVD; DPP-4 inhibitors (sitagliptin, linagliptin) when weight-neutral and renal-safe options are needed; sulfonylureas (glipizide, glimepiride) as cheap add-ons; basal insulin (glargine, detemir, degludec) when A1C remains uncontrolled.
Diabetes Visit Checklist
A1C every 3 months (uncontrolled) or 6 months (stable), BP, weight, foot exam with monofilament, home glucose log review, medication adherence, hypoglycemia events, annual diabetic eye exam, annual urine albumin-to-creatinine ratio, annual lipid panel, annual foot exam, vaccination status (flu, pneumococcal, hep B, COVID).
Prediabetes & Obesity
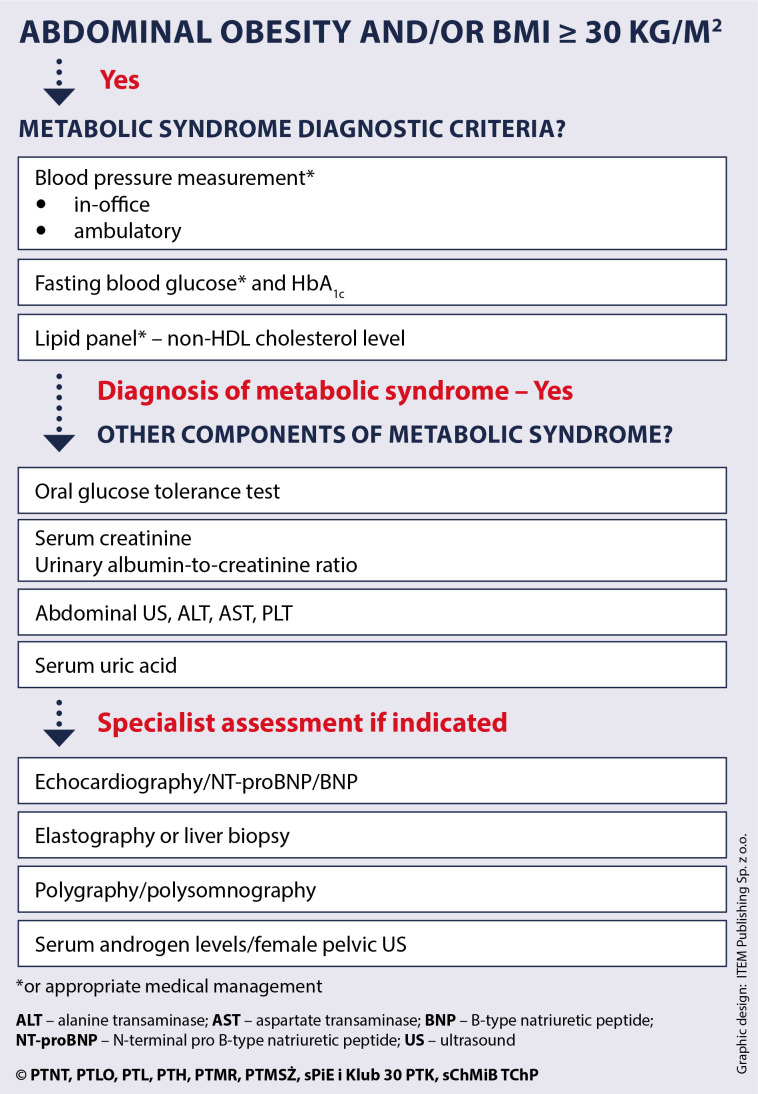
Prediabetes management emphasizes intensive lifestyle intervention (DPP program — 7% weight loss, 150 min/week exercise) with metformin as an option for A1C 6.0–6.4%, BMI > 35, age < 60, or prior gestational DM. Obesity is staged by BMI: overweight 25–29.9, class I 30–34.9, class II 35–39.9, class III ≥ 40. Pharmacotherapy options include semaglutide (Wegovy), tirzepatide (Zepbound), liraglutide (Saxenda), phentermine/topiramate, naltrexone/bupropion, and orlistat. Bariatric surgery is indicated for BMI ≥ 40 or ≥ 35 with comorbidities.
06 Thyroid Disorders Endocrine
Hypothyroidism is common; hyperthyroidism less so but important to recognize. TSH is the screening and monitoring test of choice.
Most often Hashimoto's (autoimmune). Presents with fatigue, weight gain, cold intolerance, constipation, dry skin, bradycardia, depression, menorrhagia. Labs: high TSH, low free T4. Treat with levothyroxine starting 1.6 mcg/kg/day (lower — 25–50 mcg — in elderly or cardiac disease). Recheck TSH in 6–8 weeks. Target TSH 0.5–2.5 in most adults.
Graves' disease, toxic multinodular goiter, toxic adenoma, thyroiditis. Palpitations, heat intolerance, weight loss, tremor, anxiety, diarrhea, exophthalmos (Graves). Labs: low TSH, high free T4/T3. Refer to endocrinology. Temporize with beta-blocker (propranolol, atenolol); definitive treatment is methimazole, radioactive iodine (RAI), or thyroidectomy.
07 URIs, Sinusitis, Pharyngitis, Otitis & Allergic Rhinitis Respiratory
Acute respiratory complaints fill every urgent slot in primary care.
Viral URI (Common Cold)
Rhinorrhea, sore throat, cough, low-grade fever, malaise. Self-limited, 7–10 days. Supportive care: fluids, rest, acetaminophen/ibuprofen, intranasal saline, decongestants (pseudoephedrine), antihistamines. Antibiotics not indicated.
Acute Bacterial Sinusitis
Diagnose when viral URI symptoms persist ≥ 10 days without improvement, worsen after initial improvement (double-sickening), or feature severe symptoms (fever ≥ 39°C, facial pain, purulent nasal discharge) for ≥ 3 days. First-line: amoxicillin-clavulanate 875/125 mg BID x 5–7 days. Doxycycline for penicillin allergy.
Streptococcal Pharyngitis
Use the Centor criteria (fever > 38°C, tonsillar exudate, tender anterior cervical adenopathy, absence of cough). Each criterion = 1 point; add 1 point for age 3–14, subtract 1 for age > 45. Score ≥ 3 warrants rapid strep test; positive test = penicillin V 500 mg BID x 10 days or amoxicillin 500 mg BID x 10 days. Azithromycin or cephalexin if PCN-allergic.
Otitis Media & Externa
Acute otitis media (AOM): bulging erythematous TM, fever, ear pain. Treat with amoxicillin 80–90 mg/kg/day divided BID x 10 days (children < 2), or observation with symptomatic care in older children without severe symptoms. Otitis externa (swimmer's ear): canal erythema, tenderness with tragus manipulation, discharge. Treat with topical ciprofloxacin/dexamethasone drops.
Acute Bronchitis
Cough > 5 days, often with clear or purulent sputum, chest discomfort, wheezing, normal exam or scattered wheezes. Viral in > 90% — antibiotics not indicated. Symptomatic care, albuterol inhaler if wheezing.
Allergic Rhinitis
Chronic rhinorrhea, sneezing, nasal congestion, itchy eyes, throat clearing. Treat with intranasal steroids (fluticasone, mometasone, budesonide) as first-line, oral second-generation antihistamines (loratadine, cetirizine, fexofenadine), intranasal antihistamines (azelastine), leukotriene antagonists (montelukast).
08 Asthma & COPD Respiratory
Asthma
Chronic reversible airway inflammation with bronchospasm. Classic triggers: allergens, viral URIs, exercise, cold air, smoke. Management follows the NAEPP EPR-4 2020 Focused Updates and GINA strategy.
| Step | Controller | Reliever |
|---|---|---|
| Step 1 (intermittent) | As-needed low-dose ICS-formoterol | SABA or ICS-formoterol PRN |
| Step 2 (mild persistent) | Daily low-dose ICS | SABA PRN |
| Step 3 (moderate persistent) | Low-dose ICS-LABA | SABA PRN |
| Step 4 | Medium-dose ICS-LABA | SABA PRN |
| Step 5–6 | High-dose ICS-LABA ± LAMA ± biologic | SABA PRN |
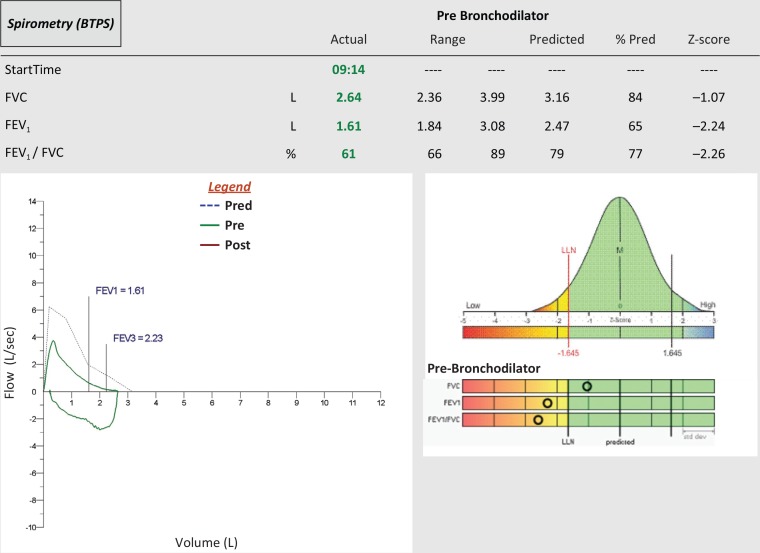
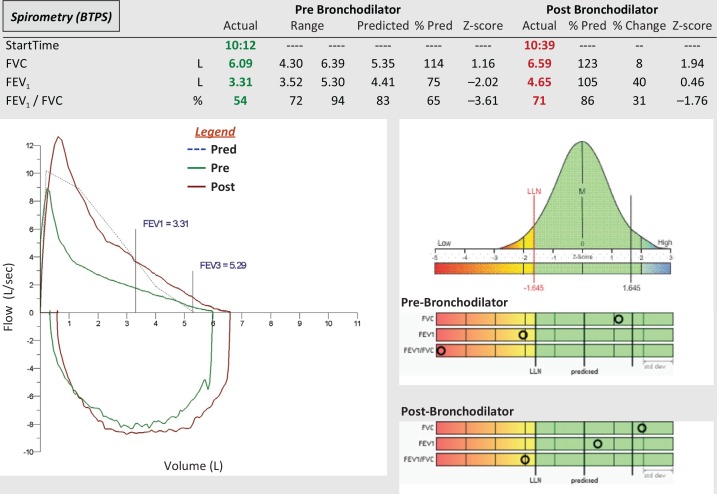
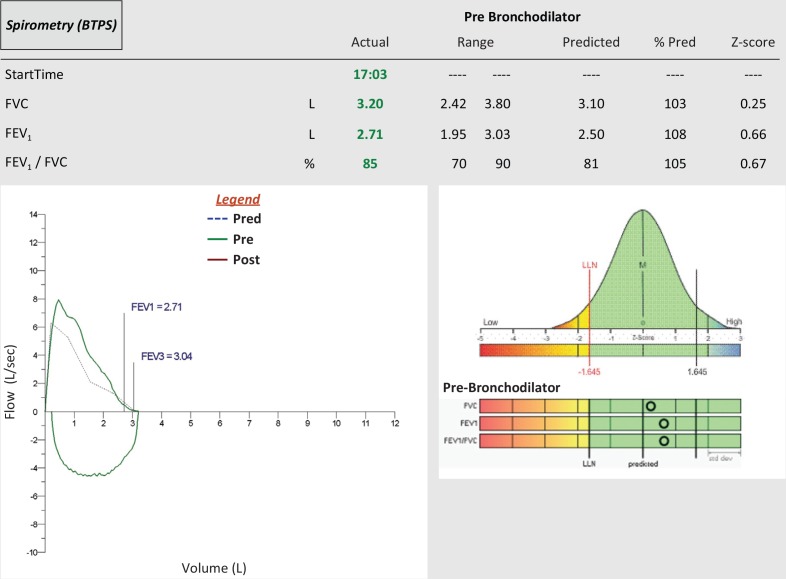
Spirometry with reversibility (≥ 12% and ≥ 200 mL FEV1 improvement post-bronchodilator) confirms asthma. Peak flow diaries for self-management. Every asthma visit documents symptom frequency, nighttime awakenings, rescue inhaler use, and activity limitation (basis for control assessment).
COPD
Chronic airflow limitation, usually from smoking. GOLD 2024 Report defines diagnosis by post-bronchodilator FEV1/FVC < 0.70 with persistent symptoms.
| GOLD Stage | FEV1 (% predicted) | Severity |
|---|---|---|
| GOLD 1 | ≥ 80% | Mild |
| GOLD 2 | 50–79% | Moderate |
| GOLD 3 | 30–49% | Severe |
| GOLD 4 | < 30% | Very severe |
Treatment by GOLD ABE groups: LABA or LAMA (group A), LABA+LAMA (group B), LABA+LAMA (+ICS if eosinophils ≥ 300 or exacerbation phenotype) (group E). Exacerbations are treated with prednisone 40 mg daily x 5 days, azithromycin or doxycycline, and increased bronchodilators. Smoking cessation is the only intervention that alters long-term decline.
09 GERD, IBS & Common GI Complaints Gastrointestinal
GERD
Heartburn, regurgitation, chronic cough, dental erosion. Diagnose clinically; empiric PPI trial (omeprazole 20 mg daily, pantoprazole 40 mg daily, esomeprazole 40 mg) x 8 weeks. Lifestyle: weight loss, head of bed elevation, avoid late meals, avoid triggers (coffee, chocolate, fatty food, alcohol). Alarm features (dysphagia, odynophagia, weight loss, GI bleeding, anemia, age > 60 new-onset) warrant EGD referral.
IBS
Rome IV criteria: recurrent abdominal pain ≥ 1 day/week x 3 months, associated with defecation, change in stool frequency, or change in form. Subtypes: IBS-C (constipation), IBS-D (diarrhea), IBS-M (mixed). Treat symptoms: fiber (psyllium), polyethylene glycol or linaclotide/lubiprostone (IBS-C), loperamide or rifaximin (IBS-D), antispasmodics (dicyclomine, hyoscyamine), low-FODMAP diet, SSRI/TCA for visceral pain.
Constipation, Dyspepsia, H. pylori
First-line constipation: fiber, fluids, PEG 3350 (Miralax). H. pylori testing (stool antigen, urea breath test) for dyspepsia age < 60, treated with triple therapy (PPI + amoxicillin + clarithromycin) or quadruple therapy (PPI + bismuth + metronidazole + tetracycline).
10 MSK — Low Back, Knee, Neck & Headache MSK/Neuro
Low Back Pain
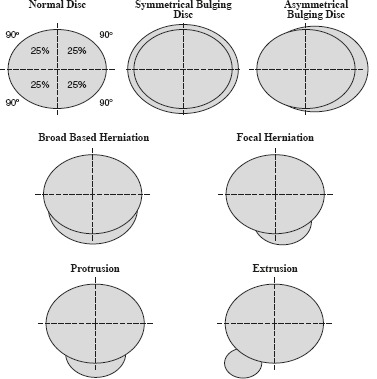
Most acute LBP is mechanical and resolves in 4–6 weeks. Screen for red flags: fever, IV drug use (infection), night pain, weight loss, history of cancer (malignancy), saddle anesthesia, bowel/bladder incontinence (cauda equina), major trauma (fracture), progressive neurologic deficit. Imaging is NOT indicated in the first 6 weeks without red flags. First-line: NSAIDs, acetaminophen, heat, staying active, PT. Second-line: muscle relaxants (cyclobenzaprine, methocarbamol) short-term. Avoid opioids. Refer for persistent radiculopathy or failed conservative care.
Knee Pain
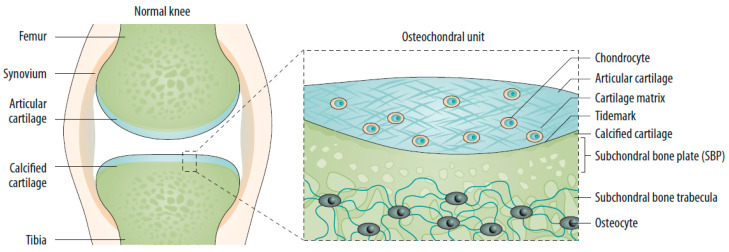
Osteoarthritis (chronic, crepitus, activity-related), meniscal tear (twisting injury, locking, McMurray +), ligament injury (ACL — pop, hemarthrosis, Lachman +; MCL — valgus stress), patellofemoral pain (anterior, worse with stairs). OA treatment: weight loss, quad strengthening, NSAIDs, topical diclofenac, intra-articular corticosteroid injection, hyaluronic acid (limited benefit), referral for TKA when refractory.
Neck Pain & Headache

Mechanical neck pain: conservative care, NSAIDs, PT. Headache types: tension (bilateral, band-like, no nausea), migraine (unilateral, throbbing, photophobia, phonophobia, nausea, aura in 30%), cluster (unilateral periorbital, autonomic features, episodic), medication overuse, secondary (rule out with red flags — thunderclap, focal deficit, fever, worst of life). Migraine acute: triptans, NSAIDs, antiemetics. Prophylaxis: propranolol, topiramate, amitriptyline, CGRP monoclonal antibodies (erenumab, galcanezumab).
11 Depression, Anxiety, Insomnia & ADHD Behavioral
Depression — PHQ-9
The PHQ-9 is administered at essentially every primary care visit where mood is addressed. It scores 9 DSM-5 criteria over the past 2 weeks on a 0–3 scale.
| PHQ-9 Total | Severity | Action |
|---|---|---|
| 0–4 | None/minimal | Monitor |
| 5–9 | Mild | Watchful waiting, repeat in 4 weeks |
| 10–14 | Moderate | Therapy and/or medication |
| 15–19 | Moderately severe | Medication + therapy |
| 20–27 | Severe | Medication + therapy, consider referral |
Always ask about suicidal ideation separately (PHQ-9 question 9 + follow-up assessment — plan, intent, means, prior attempts). First-line: SSRIs (sertraline 25–200, escitalopram 10–20, fluoxetine 20–60), SNRIs (venlafaxine, duloxetine), bupropion (avoid in seizure, eating disorders). Reassess in 4–6 weeks.
Anxiety — GAD-7
The GAD-7 mirrors the PHQ-9 structure for generalized anxiety.
| GAD-7 Total | Severity |
|---|---|
| 0–4 | Minimal |
| 5–9 | Mild |
| 10–14 | Moderate |
| 15–21 | Severe |
First-line: SSRIs, SNRIs, CBT. Buspirone as add-on. Short-term hydroxyzine or propranolol for situational anxiety. Benzodiazepines only short-term or severe cases.
Insomnia
Sleep hygiene first. CBT-I is first-line therapy. Medications: melatonin 0.5–5 mg, trazodone 25–100 mg, doxepin 3–6 mg, ramelteon, zolpidem (short-term), suvorexant/lemborexant. Avoid chronic benzodiazepines.
ADHD
Adult and pediatric diagnoses are common in primary care. Validated rating scales (Vanderbilt for children, ASRS for adults). First-line: stimulants — methylphenidate (Ritalin, Concerta, Daytrana) or amphetamine (Adderall, Vyvanse, Mydayis). Non-stimulant options: atomoxetine, guanfacine ER, clonidine ER, viloxazine. Monitor HR, BP, growth (children), sleep, appetite. Controlled substance agreement required in most practices.
12 Geriatrics — Dementia, Falls, Osteoporosis Geriatric
Cognitive Screening
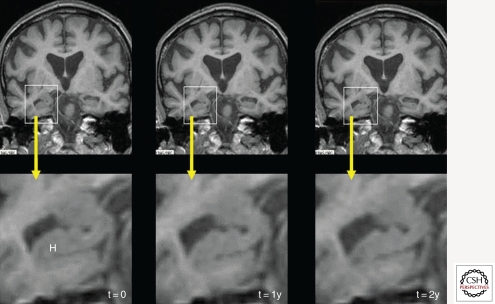
Mini-Cog (3-word recall + clock draw), MoCA (/30, < 26 abnormal), MMSE (/30, < 24 abnormal). Dementia workup: TSH, B12, CMP, CBC, RPR (if risk), MRI brain. Types: Alzheimer's (memory dominant), vascular (stepwise), Lewy body (parkinsonism, visual hallucinations, REM behavior), frontotemporal (behavioral/language). Treatment: cholinesterase inhibitors (donepezil, rivastigmine, galantamine), memantine (moderate-severe), anti-amyloid monoclonals (lecanemab, donanemab) in select patients.
Fall Risk
Annual fall risk screening for age ≥ 65. Ask about falls in past year, gait instability, fear of falling. Perform Timed Up and Go (> 12 sec = risk), orthostatic vitals, medication review (benzos, anticholinergics, antihypertensives, hypoglycemics). Interventions: PT, home safety evaluation, vitamin D, deprescribing.
Osteoporosis
Screen women ≥ 65 with DXA; men ≥ 70 or with risk factors. FRAX score estimates 10-year fracture risk; treat if T-score ≤ -2.5, prior fragility fracture, or FRAX ≥ 20% (major) or ≥ 3% (hip). First-line: oral bisphosphonates (alendronate 70 mg weekly, risedronate). Second-line: zoledronic acid IV, denosumab, teriparatide, romosozumab. Calcium 1200 mg/day + vitamin D 800–1000 IU/day.
13 Women's Health, Contraception & Prenatal Women's Health
Contraception
Use the CDC MEC (Medical Eligibility Criteria) to select safely. Methods in order of effectiveness: implants (Nexplanon — 3 years), IUDs (Mirena/Kyleena/Liletta/Skyla — 3–8 years levonorgestrel; Paragard — 10 years copper), depot medroxyprogesterone (Depo-Provera IM every 12 weeks), combined OCPs, progestin-only pills, contraceptive patch (Xulane), vaginal ring (NuvaRing, Annovera), diaphragm, condoms. Avoid combined estrogen in smokers ≥ 35, migraine with aura, uncontrolled HTN, VTE, active breast cancer.
Well-Woman Exam
Annual visit: BP, breast exam (clinical), pelvic exam as indicated, cervical cancer screening per USPSTF, STI screening, contraception review, domestic violence screening, menopause symptoms, breast cancer screening coordination.
Prenatal Basics
First visit: confirm pregnancy, dating ultrasound, CBC, blood type/Rh, rubella, varicella, HIV, RPR, hep B, hep C, urine culture, pap if due, gonorrhea/chlamydia. Prenatal vitamins with folate 400–800 mcg. Schedule: monthly to 28 weeks, every 2 weeks to 36 weeks, weekly to delivery. Key milestones: NT screen 11–14 wk, anatomy US 18–22 wk, GDM screen 24–28 wk, GBS 35–37 wk, Tdap 27–36 wk.
Menopause
Vasomotor symptoms, GU syndrome, mood, sleep disruption. Treatment: hormone therapy (estrogen + progesterone if intact uterus), vaginal estrogen for GU symptoms, SSRIs/SNRIs (paroxetine, venlafaxine), gabapentin, clonidine, fezolinetant (non-hormonal). Discuss individualized risk/benefit.
14 Pediatrics — Well-Child, Immunizations & Common Infections Pediatric
Well-Child Schedule
AAP Bright Futures: newborn, 3–5 days, 1 month, 2, 4, 6, 9, 12, 15, 18, 24, 30 months, then annually through age 21. Each visit documents growth parameters on CDC/WHO curves, developmental surveillance (Ages & Stages at 9/18/30 mo), autism screening (M-CHAT at 18 and 24 mo), anticipatory guidance, lead screening (12 and 24 mo), hemoglobin (12 mo), vision, hearing, dental, and immunizations.
ACIP Childhood Immunization Highlights
Birth: Hep B #1. 2 mo: DTaP, IPV, Hib, PCV, RV, Hep B #2. 4 mo: DTaP, IPV, Hib, PCV, RV. 6 mo: DTaP, Hib, PCV, RV, Hep B #3, annual flu. 12–15 mo: MMR, Varicella, Hib, PCV, Hep A #1. 18 mo: Hep A #2. 4–6 yr: DTaP, IPV, MMR, Varicella. 11–12 yr: Tdap, HPV (2 doses if started < 15; 3 doses if ≥ 15), Meningococcal ACWY. 16 yr: MenACWY booster, MenB (shared decision). Annual: influenza ≥ 6 mo.
Common Pediatric Infections
Viral URIs dominate. Otitis media (amoxicillin 80–90 mg/kg/d). Bronchiolitis (supportive care, RSV). Croup (dexamethasone ± racemic epi). Hand-foot-mouth (supportive). Fifth disease, roseola, impetigo (topical mupirocin, oral cephalexin), scabies (permethrin 5%), head lice.
Sports Physicals & Well-Child
Pre-participation exam includes focused cardiac history (syncope, family SCD, murmur), MSK history, ROS. Clear for participation unless red flags.
15 Dermatology in Primary Care Dermatologic
Family physicians handle most everyday skin complaints before specialty referral.
Acne
Mild: topical retinoid (tretinoin, adapalene) + benzoyl peroxide. Moderate: add topical or oral antibiotic (clindamycin, doxycycline). Severe: isotretinoin referral (iPLEDGE). Women: combined OCPs or spironolactone 50–100 mg daily.
Eczema (Atopic Dermatitis)
Emollients, topical steroids (hydrocortisone face, triamcinolone body, clobetasol severe), topical calcineurin inhibitors (tacrolimus, pimecrolimus), crisaborole, dupilumab for severe. Trigger avoidance, bleach baths for superinfected.
Common Lesions
Seborrheic keratosis (benign, waxy, "stuck-on"), actinic keratosis (rough, pre-cancerous — cryotherapy or 5-FU/imiquimod), basal cell (pearly, telangiectasia, rolled borders), squamous cell (scaly, indurated), melanoma (ABCDE: Asymmetry, Border irregular, Color varied, Diameter > 6mm, Evolving), nevi, cysts, lipomas, warts, molluscum, tinea, candidiasis, psoriasis, rosacea, contact dermatitis, urticaria, shingles.
16 GU — UTI & Sexual Health Genitourinary
Uncomplicated UTI
Dysuria, frequency, urgency, suprapubic pain. UA with nitrite and leukocyte esterase, culture in complicated cases. First-line: nitrofurantoin 100 mg BID x 5 d, TMP-SMX DS BID x 3 d, fosfomycin 3 g x 1. Avoid fluoroquinolones first-line. Pyelonephritis (fever, flank pain, N/V): ciprofloxacin 7 d, ceftriaxone, TMP-SMX; hospitalize if sepsis.
Sexual Health & STI Screening
USPSTF recommends chlamydia/gonorrhea screening in sexually active women ≤ 24 and older women at risk; HIV screening 15–65; syphilis in at-risk; HCV one-time adult. STI treatment per CDC guidelines: chlamydia (doxycycline 100 mg BID x 7 d), gonorrhea (ceftriaxone 500 mg IM + doxycycline), syphilis (penicillin G benzathine), trichomoniasis (metronidazole), HSV (acyclovir, valacyclovir). PrEP with TDF/FTC (Truvada) or TAF/FTC (Descovy) for HIV prevention.
Men's Health
BPH (tamsulosin, finasteride, combination), erectile dysfunction (PDE5 inhibitors — sildenafil, tadalafil), testosterone deficiency (check 2 morning totals, symptoms; testosterone replacement). Well-man exam covers CV risk, prostate screening discussion (USPSTF shared decision-making age 55–69), colorectal screening, immunizations, mental health, safety.
17 Preventive Care & USPSTF Screening Prevention
Preventive care is central to family medicine billing and quality measures. Memorize the current USPSTF A and B recommendations.
Cancer Screening
| Cancer | Population | Test & Interval |
|---|---|---|
| Colorectal | Age 45–75 | Colonoscopy q 10 yr, FIT annually, Cologuard q 3 yr, flex sig q 5 yr (USPSTF 2021) |
| Breast | Women 40–74 | Mammography every 2 yr (USPSTF 2024) |
| Cervical | Women 21–65 | 21–29: Pap q 3 yr; 30–65: Pap q 3 yr, HPV q 5 yr, or co-test q 5 yr |
| Lung | Age 50–80, ≥ 20 pack-yr, current or quit < 15 yr | Annual low-dose CT |
| Prostate | Men 55–69 | PSA — shared decision-making |
| AAA | Men 65–75 ever-smokers | One-time abdominal ultrasound |
Other Key USPSTF Screenings
HTN (annually adults), lipids (ASCVD risk), diabetes (age 35–70 overweight/obese), obesity (all adults, BMI), depression (all adults), anxiety (adults 19–64), unhealthy alcohol (USAUDIT/AUDIT-C), tobacco, intimate partner violence (women of reproductive age), osteoporosis (women 65+), HIV (15–65), hepatitis B (at risk), hepatitis C (18–79 one-time), latent TB (at risk), statin for CVD prevention.
ACIP Adult Immunizations
Annual influenza. Tdap once then Td/Tdap booster q 10 yr. Zoster (Shingrix) 2 doses age ≥ 50. Pneumococcal (PCV20 or PCV15+PPSV23) age ≥ 65 or high risk. HPV up to 26 (shared 27–45). COVID per ACIP. Hep B all adults 19–59. RSV age ≥ 60 shared; pregnancy 32–36 wks. MMR/varicella if non-immune.
On every annual physical or Medicare AWV, scribes should run the EMR health maintenance tab and list every screening/immunization that is due, overdue, or declined. Document each one with specific plan action — ordered, scheduled, declined, or deferred.
18 Office Procedures Procedures
| Procedure | Indication | Scribe Documentation |
|---|---|---|
| Shave / punch biopsy | Suspicious lesion | Consent, site, size, anesthetic (lido 1% with epi unless digit/ear), technique, hemostasis, specimen to pathology |
| Skin excision | Melanoma suspicious, cyst, lipoma | Elliptical, margins, layered closure, suture material, count |
| Cryotherapy | Actinic keratosis, warts, SK | Liquid nitrogen, freeze-thaw cycles, sites |
| I&D | Abscess | Incision length, pus, packing, culture if MRSA |
| Laceration repair | Traumatic wound | Irrigation, anesthetic, layers, suture type/size, count, tetanus status |
| Nail removal | Ingrown toenail, paronychia | Digital block, partial vs total, phenol ablation |
| Joint injection | OA, bursitis, tendinopathy | Site (knee, shoulder, trochanteric, plantar fascia, trigger finger), lidocaine + triamcinolone/methylprednisolone, volume, approach |
| IUD placement | Contraception | Consent, cervical cleansing, sounding depth, device lot, strings trimmed |
| IUD removal | End of service life, side effects | Strings visualized, traction removal, intact |
| Nexplanon | Contraception | Non-dominant arm, anesthesia, insertion, palpation confirmed, lot number |
| Endometrial biopsy | AUB, post-menopausal bleeding | Consent, Pipelle, depth, sample, cramping |
| Ear lavage | Cerumen impaction | Pre-inspection, warm water, post-inspection TM |
| EKG | CP, palpitations, pre-op | Rate, rhythm, axis, intervals, ST/T wave findings |
| Spirometry | Asthma/COPD dx and monitoring | FEV1, FVC, ratio, pre/post bronchodilator |
| Nebulizer treatment | Acute bronchospasm | Albuterol/ipratropium, pre/post lung exam, SpO2 |
19 Labs, Imaging & Point-of-Care Diagnostics Diagnostics
Common Lab Panels
CBC: WBC, Hgb, Hct, MCV, platelets, differential. BMP/CMP: Na, K, Cl, CO2, BUN, Cr, glucose, Ca (+ LFTs/albumin/total protein for CMP). Lipid panel: total, LDL, HDL, triglycerides, non-HDL. A1C. TSH (± free T4). UA (dip + microscopy). Urine albumin-to-creatinine ratio. Iron studies: ferritin, iron, TIBC, transferrin saturation. Vitamin D 25-OH. B12, folate. PT/INR (warfarin monitoring). Hepatitis panel, HIV, RPR, QuantiFERON.
Imaging Commonly Ordered
CXR (cough, dyspnea, pre-op), plain films (MSK), mammography (screening), bone density DXA, abdominal US (AAA screen, RUQ pain), pelvic US, CT (as indicated), MRI (chronic back/knee after failed conservative), echocardiogram, carotid duplex, lower extremity duplex.
Point-of-Care
Rapid strep, flu, COVID, RSV, UA, pregnancy (urine hCG), glucose (glucometer), A1C (in-office analyzer), INR (Coag-Sense), Hgb (HemoCue), lipid (Cholestech), H. pylori stool antigen, fecal occult blood, urine drug screen.
20 Primary Care Medication Formulary Pharmacology
Antihypertensives
| Class | Examples | Notes |
|---|---|---|
| ACE-I | Lisinopril, enalapril, ramipril, benazepril | Cough, hyperkalemia, avoid pregnancy, angioedema |
| ARB | Losartan, valsartan, olmesartan, telmisartan | Alternative when ACE-I not tolerated |
| Thiazide | HCTZ, chlorthalidone, indapamide | Hyponatremia, hypokalemia, gout |
| CCB (DHP) | Amlodipine, nifedipine | Peripheral edema |
| CCB (non-DHP) | Diltiazem, verapamil | Bradycardia, constipation, AV block |
| Beta-blocker | Metoprolol, carvedilol, atenolol, propranolol, bisoprolol | Post-MI, HFrEF, AFib, migraine |
| Loop diuretic | Furosemide, torsemide, bumetanide | Heart failure, volume overload |
| K-sparing | Spironolactone, eplerenone | HFrEF, resistant HTN, hyperkalemia risk |
| Central alpha-2 | Clonidine | Rebound HTN if stopped abruptly |
Diabetes Agents
| Class | Examples | Notes |
|---|---|---|
| Biguanide | Metformin | First-line; GI side effects; hold for contrast |
| GLP-1 RA | Semaglutide (Ozempic/Wegovy), liraglutide, dulaglutide, tirzepatide (Mounjaro/Zepbound) | Weight loss, ASCVD/CKD benefit, GI, pancreatitis |
| SGLT2 | Empagliflozin, dapagliflozin, canagliflozin | HF/CKD benefit, UTI, DKA, genital mycotic |
| DPP-4 | Sitagliptin, linagliptin, saxagliptin | Weight neutral, mild A1C drop |
| SU | Glipizide, glimepiride | Hypoglycemia, weight gain |
| TZD | Pioglitazone | Weight gain, HF, fracture, bladder ca |
| Basal insulin | Glargine, detemir, degludec | Titrate by fasting glucose |
| Prandial insulin | Lispro, aspart, glulisine | Meal-time coverage |
Lipid
Statins (atorvastatin, rosuvastatin, simvastatin, pravastatin, lovastatin, pitavastatin), ezetimibe, PCSK9 (alirocumab, evolocumab), bempedoic acid, icosapent ethyl, fibrates (fenofibrate, gemfibrozil), niacin, bile acid sequestrants.
Antibiotics (Primary Care)
Amoxicillin, amoxicillin-clavulanate, cephalexin, cefdinir, doxycycline, azithromycin, clindamycin, TMP-SMX, nitrofurantoin, fosfomycin, ciprofloxacin, levofloxacin, metronidazole, fluconazole, nystatin.
Asthma/COPD Inhalers
| Class | Examples |
|---|---|
| SABA | Albuterol (ProAir, Ventolin, Proventil), levalbuterol |
| SAMA | Ipratropium (Atrovent) |
| LABA | Salmeterol, formoterol, vilanterol |
| LAMA | Tiotropium (Spiriva), umeclidinium |
| ICS | Fluticasone, budesonide, beclomethasone, mometasone, ciclesonide |
| ICS-LABA | Advair, Symbicort, Breo, Dulera |
| LAMA-LABA | Anoro, Stiolto, Bevespi |
| Triple | Trelegy, Breztri |
| Leukotriene | Montelukast, zafirlukast |
| Biologics | Omalizumab, mepolizumab, benralizumab, dupilumab, tezepelumab |
Psychiatric & Sleep
SSRI: sertraline, escitalopram, fluoxetine, paroxetine, citalopram. SNRI: venlafaxine, duloxetine, desvenlafaxine. Atypical: bupropion, mirtazapine, trazodone, vilazodone, vortioxetine. Benzodiazepines: lorazepam, alprazolam, clonazepam, diazepam (short-term). Sleep: zolpidem, eszopiclone, ramelteon, suvorexant, doxepin low-dose, melatonin. ADHD: methylphenidate (Ritalin, Concerta, Focalin, Daytrana), amphetamine (Adderall, Vyvanse, Mydayis), atomoxetine, guanfacine ER, clonidine ER, viloxazine.
Contraception, HRT & Women's Health
Combined OCPs (Lo Loestrin, Yaz, Junel), progestin-only ("mini-pill"), Nexplanon, Depo-Provera, Mirena/Kyleena/Liletta/Skyla, Paragard, NuvaRing/Annovera, Xulane patch. HRT: estradiol (oral, patch, gel, vaginal), progesterone (micronized, medroxyprogesterone), combined (Prempro). Vaginal estrogen for GSM. Fezolinetant for vasomotor symptoms.
Topicals
Hydrocortisone 2.5%, triamcinolone 0.1%, clobetasol 0.05%, mupirocin, ketoconazole, terbinafine, nystatin, clindamycin + BPO, tretinoin, adapalene, metronidazole gel, tacrolimus ointment, permethrin, selenium sulfide, lidocaine/prilocaine.
Vaccines
Flu (Fluzone, Fluarix, Flucelvax, Flublok, Fluad, FluMist), Tdap (Adacel, Boostrix), Shingrix, Prevnar 20, Pneumovax 23, MMR, Varivax, HPV (Gardasil-9), Hep B (Engerix, Heplisav-B), Hep A (Havrix, Vaqta), MenACWY (Menveo, Menactra), MenB (Bexsero, Trumenba), RSV (Arexvy, Abrysvo), COVID-19.
21 Classification & Scoring Systems Scoring
PHQ-9 Depression
Nine items scored 0–3: (1) little interest/pleasure, (2) depressed mood, (3) sleep, (4) energy, (5) appetite, (6) self-worth, (7) concentration, (8) psychomotor, (9) suicidal ideation. Totals: 0–4 none, 5–9 mild, 10–14 moderate, 15–19 moderately severe, 20–27 severe.
GAD-7 Anxiety
Seven items 0–3: nervous, cannot stop worrying, worry too much, trouble relaxing, restless, irritable, afraid something awful. Totals: 0–4 minimal, 5–9 mild, 10–14 moderate, 15–21 severe.
AUDIT-C
Three items: frequency of drinking, drinks per day, frequency of ≥ 6 drinks. Positive ≥ 4 (men), ≥ 3 (women).
FRAX
10-year fracture risk estimate using age, sex, BMI, prior fracture, parental hip fracture, current smoking, glucocorticoids, RA, secondary osteoporosis, alcohol, femoral neck T-score. Treat if 10-yr major fx ≥ 20% or hip fx ≥ 3%.
ASCVD Risk Calculator
Pooled Cohort Equations: age, sex, race, TC, HDL, SBP, treatment, diabetes, smoking. 10-year ASCVD risk. Statin consideration at ≥ 7.5%, strong at ≥ 10%.
BMI Classification
| BMI | Classification |
|---|---|
| < 18.5 | Underweight |
| 18.5–24.9 | Normal |
| 25.0–29.9 | Overweight |
| 30.0–34.9 | Class I obesity |
| 35.0–39.9 | Class II obesity |
| ≥ 40.0 | Class III (severe) obesity |
CKD Staging (KDIGO)
| Stage | eGFR | Description |
|---|---|---|
| G1 | ≥ 90 | Normal with markers of kidney damage |
| G2 | 60–89 | Mildly decreased |
| G3a | 45–59 | Mildly-moderately decreased |
| G3b | 30–44 | Moderately-severely decreased |
| G4 | 15–29 | Severely decreased |
| G5 | < 15 | Kidney failure |
NYHA Heart Failure
Class I (no limitation), II (slight with ordinary activity), III (marked with less than ordinary), IV (symptoms at rest).
CHA₂DS₂-VASc
Congestive HF (1), HTN (1), Age ≥ 75 (2), Diabetes (1), Stroke/TIA (2), Vascular disease (1), Age 65–74 (1), Sex female (1). Score ≥ 2 men / ≥ 3 women → anticoagulation.
22 Physical Exam Templates Exam
General: Alert, oriented x 3, no acute distress, well-appearing.
HEENT: NCAT, PERRL, EOMI, sclerae anicteric, conjunctivae pink, oropharynx clear without erythema or exudate, TMs pearly gray bilaterally, moist mucous membranes.
Neck: Supple, no lymphadenopathy, no thyromegaly, no JVD, no carotid bruits.
Cardiovascular: RRR, normal S1/S2, no murmurs, rubs, or gallops. No peripheral edema. 2+ pulses throughout.
Pulmonary: CTA bilaterally, no wheezing, rales, or rhonchi. Good air movement.
Abdomen: Soft, non-tender, non-distended, +BS, no hepatosplenomegaly, no masses, no rebound or guarding.
Extremities: No cyanosis, clubbing, or edema. Full ROM.
Skin: Warm, dry, intact. No rashes or concerning lesions.
Neuro: CN II–XII intact, motor 5/5 throughout, sensation intact, gait steady, DTRs 2+ symmetric.
Psych: Appropriate mood and affect, linear thought process, no SI/HI.
Inspection (skin, nails, interdigital, calluses, ulcers, deformity), pulses (DP/PT), monofilament at 10 sites, vibration (128 Hz tuning fork at hallux), ankle reflexes, temperature.
23 Abbreviations Master List Reference
24 Sample HPI Templates Templates
62-year-old female presents for her annual wellness visit. She reports she has been feeling generally well over the past year. No chest pain, palpitations, or dyspnea. No cough or weight change. Home BPs on lisinopril have averaged 124/76 over the past month. She walks 30 minutes five days per week. Denies mood changes; PHQ-2 negative. She is due for mammography and colonoscopy, last performed in 2020 and 2015 respectively. LMP at age 52; no post-menopausal bleeding. Performs monthly self-breast exam. Current medications reconciled; she takes lisinopril 20 mg, atorvastatin 20 mg, and calcium/vitamin D. No new allergies. Non-smoker, 1 glass of wine 2–3 nights per week. Lives with spouse, feels safe at home.
68-year-old male with HTN, T2DM, HLD, and CKD stage 3a here for 3-month follow-up. Home BPs averaging 138/82 on lisinopril 40 mg and amlodipine 10 mg. Home fasting glucose 140–170s; post-meal 180–220s. Last A1C 8.2% three months ago on metformin 1000 mg BID and glipizide 10 mg. He reports adherence to medications and follows a "low-carb" diet inconsistently. Walks short distances only due to knee OA. No chest pain, dyspnea, orthopnea, PND, or lower extremity edema. No hypoglycemia episodes. No polyuria, polydipsia. No vision changes. Denies foot pain, ulcers, or numbness. Last diabetic eye exam 14 months ago. Smokes half pack per day, willing to discuss cessation.
34-year-old female with no significant PMH presents with 4 days of sore throat, nasal congestion, non-productive cough, and low-grade fever to 100.8°F. Denies ear pain, sinus pressure, shortness of breath, chest pain, or GI symptoms. Has tried acetaminophen and ibuprofen with mild relief. Several coworkers recently had similar symptoms. Up to date on flu and COVID vaccines. No sick contacts with strep confirmed. Denies history of rheumatic fever. No tobacco use. No recent travel.
56-year-old female with obesity (BMI 34) and no prior knee injury presents with 3 months of progressive right medial knee pain. Pain is 5/10 at rest and 8/10 with stairs and prolonged walking. Describes morning stiffness lasting 15 minutes and crepitus with motion. No locking, giving way, or acute trauma. No swelling or erythema. Has been taking OTC ibuprofen 400 mg PRN with partial relief. No fever, rash, or other joint involvement. No history of gout or inflammatory arthritis. Interested in options to avoid surgery.
2-year-old male presents with mother for 24-month well-child check. No acute concerns. Eating a varied diet, drinking whole milk 16–20 oz/day. Sleeps 11 hours nightly plus a 90-minute nap. Speaks 50+ words and combining 2–3 word phrases. Walks, runs, climbs stairs. Potty-training initiated last month. No recent illnesses. Growth parameters tracking along 50th percentile. Up to date on immunizations through 18 months; due today for DTaP, IPV, Hib, PCV, MMR, varicella, Hep A booster per ACIP schedule (verified). M-CHAT completed with no concerns. Parents report safe home, rear-facing car seat, smoke detectors functional, no firearms in home.
29-year-old female returns for 4-week follow-up of newly diagnosed major depressive disorder. At prior visit, PHQ-9 was 17 (moderately severe). Started sertraline 50 mg daily. Today she reports mood "slightly better," sleep improved, appetite returning. PHQ-9 today is 11 (moderate). Denies suicidal ideation, plans, or intent. Tolerating sertraline without nausea, sexual side effects, or insomnia. Engaged with therapist weekly. Adherent to medication. No alcohol or substance use. Safe at home; partner supportive. GAD-7 today 8 (mild).
25 References & Sources
Clinical Practice Guidelines
Grundy SM, et al. 2018 AHA/ACC Guideline on the Management of Blood Cholesterol. Circulation. 2019.
American Diabetes Association. Standards of Care in Diabetes—2024. Diabetes Care. 2024.
GOLD Report 2024. Global Strategy for the Diagnosis, Management and Prevention of COPD.
ACIP Recommended Child and Adolescent Immunization Schedule — United States, 2024. MMWR.
US Preventive Services Task Force. A and B Recommendations.
American Academy of Family Physicians. Clinical Practice Guidelines.
Screening & Scoring Tools
Diagram & Figure Sources
Figure 1: Annual Physical Check-Up. U.S. Air Force. Public domain.
Figure 2: The Endocrine System. OpenStax College. CC BY 3.0.
Figure 3: Components of the Digestive System. OpenStax College. CC BY 3.0.
Figure 4: Major Respiratory Organs. OpenStax College. CC BY 3.0.
Great family medicine scribes are indispensable because they free the physician to look the patient in the eye. You will document more problems, more medications, and more life history per hour than in any other specialty. The best way to get good is to learn the medicine — once you understand why lisinopril is preferred in a diabetic, why a PHQ-9 of 17 warrants medication, and why that 2-year-old needs MMR today, your notes will almost write themselves. Come in curious, ask questions between patients, and remember: every chart you write accurately is a safer patient tomorrow.