Hand Surgery
Every diagnosis, condition, procedure, medication, abbreviation, and documentation framework you need to succeed on day one and beyond.
All diagrams on this page are sourced from published educational or institutional materials rather than AI generation. Each figure caption links to the original source, and the full diagram and guideline citations are collected in the references section at the bottom.
01 Hand, Wrist & Forearm Anatomy Essentials
Hand surgery covers the fingertips to the elbow. The hand surgeon operates on bone, tendon, nerve, vessel, skin, and joint in a space the size of a deck of cards — which means anatomic precision is everything. Scribes must master the vocabulary of this anatomy because the surgeon will narrate it continuously during exam and in operative notes.
Osseous Anatomy
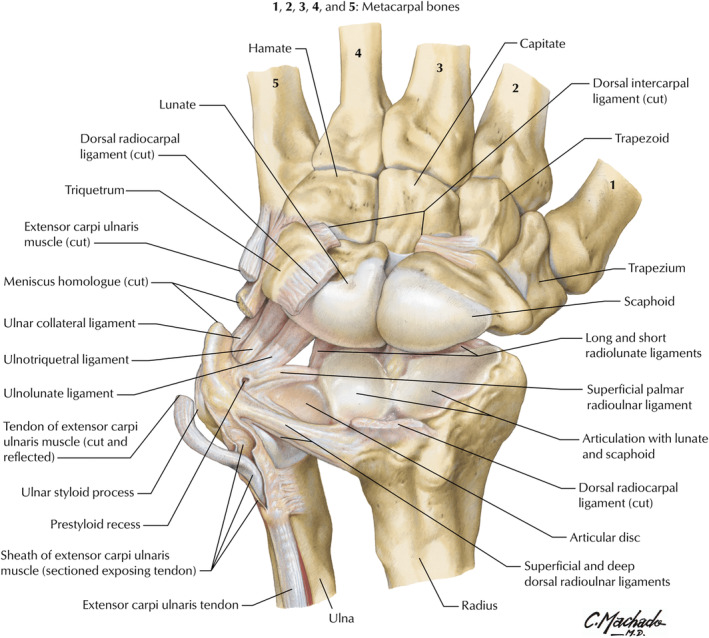
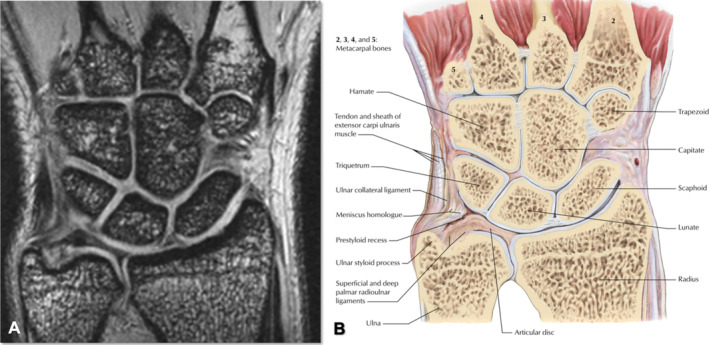
The wrist is built around eight carpal bones arranged in two rows. The proximal row (radial to ulnar) contains the scaphoid, lunate, triquetrum, and pisiform. The distal row contains the trapezium, trapezoid, capitate, and hamate. The mnemonic Some Lovers Try Positions That They Can't Handle captures the order. Distal to the carpus are five metacarpals (MC1 = thumb through MC5 = small finger) and the 14 phalanges: each finger has a proximal (P1), middle (P2), and distal (P3) phalanx, while the thumb has only P1 and P2.
The joints follow the bones: radiocarpal joint (distal radius to scaphoid/lunate), midcarpal joint (between proximal and distal carpal rows), CMC joints (carpometacarpal, especially the saddle-shaped thumb CMC), MCP joints (metacarpophalangeal, the knuckles), PIP joints (proximal interphalangeal), and DIP joints (distal interphalangeal). The thumb has only one IP joint.
Tendons
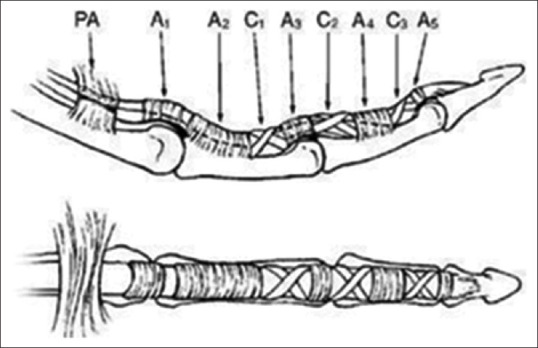
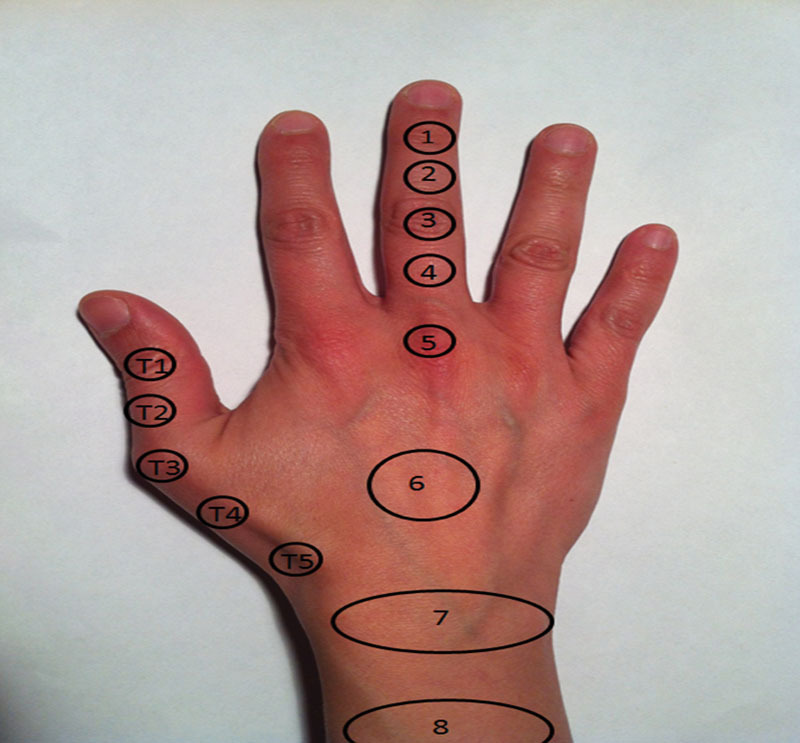
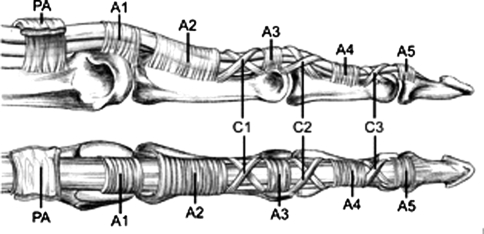
The hand is moved by two sets of tendons. The flexor tendons travel on the palmar side; the superficial flexors include flexor carpi radialis (FCR), palmaris longus (PL, absent in ~15%), and flexor carpi ulnaris (FCU), while the digital flexors are the flexor digitorum superficialis (FDS) inserting on the middle phalanx and flexor digitorum profundus (FDP) inserting on the distal phalanx. The thumb flexor is flexor pollicis longus (FPL). Flexor tendons run through a fibro-osseous sheath with a pulley system — the critical A2 and A4 pulleys must be preserved to prevent bowstringing.
The extensor tendons travel on the dorsum of the wrist in six synovial compartments:
| Compartment | Tendons | Clinical Relevance |
|---|---|---|
| 1 | APL, EPB | de Quervain tenosynovitis |
| 2 | ECRL, ECRB | Intersection syndrome (where EPB crosses) |
| 3 | EPL | Ruptures after distal radius fracture; goes around Lister tubercle |
| 4 | EDC, EIP | Dorsal wrist ganglia; EIP used for tendon transfers |
| 5 | EDM | Vaughan-Jackson lesion in RA |
| 6 | ECU | Ulnar-sided wrist pain; subluxation |
Nerves
Three nerves drive hand function. The median nerve enters the hand through the carpal tunnel, supplies the thenar musculature (abductor pollicis brevis, opponens pollicis, superficial flexor pollicis brevis), the radial two lumbricals, and sensation to the radial 3.5 digits (palmar surface) plus the dorsal tips of index/middle fingers. The ulnar nerve passes through Guyon canal, supplies the hypothenar muscles, interossei, ulnar two lumbricals, adductor pollicis, deep FPB head, and sensation to the ulnar 1.5 digits. The radial nerve divides into the posterior interosseous nerve (PIN) for wrist/finger extension and the superficial radial nerve (SRN) for sensation to the dorsoradial hand.
Intrinsic vs Extrinsic Muscles
The extrinsic muscles originate in the forearm and cross the wrist to act on the hand — these are the powerful flexors and extensors. The intrinsic muscles originate within the hand itself and provide fine motor control: the thenar group (APB, OP, FPB, adductor pollicis), hypothenar group (ADM, FDM, ODM), four lumbricals (arising from FDP tendons), three palmar interossei (adduction, PAD), and four dorsal interossei (abduction, DAB). Intrinsic paralysis (ulnar palsy) produces the classic "claw hand" — MCP hyperextension and IP flexion of the ring and small fingers — because the lumbricals normally balance the long extensors.
Vascular Anatomy
The hand receives dual blood supply from the radial artery (radial side, dorsum, deep palmar arch) and ulnar artery (ulnar side, superficial palmar arch). The two arches anastomose, which is why the Allen test is used to confirm patency of both vessels before radial artery harvest or arterial line placement. The common digital arteries branch from the superficial arch and bifurcate into proper digital arteries that run on the volar/radial and volar/ulnar aspects of each finger.
Know the anatomy cold. The surgeon will rattle off things like "EPL rupture at Lister tubercle after ORIF," "A1 pulley release," or "Zone II flexor tendon laceration" and you are expected to chart the anatomic region immediately. Memorize the flexor tendon zones (I–V) and extensor compartments (1–6) before your first operative day.
02 Scribe Documentation Framework
Hand surgery encounters split into three main flavors: acute trauma (ED consults, fractures, lacerations, infections), chronic elective (carpal tunnel, trigger finger, arthritis, Dupuytren), and post-operative follow-up. Each has a distinct documentation rhythm.
CC: Brief, often anatomic — "right thumb numbness," "fell onto outstretched hand," "mass on dorsal wrist."
HPI: Capture hand dominance, mechanism of injury, time since injury, occupation, hobbies, prior hand procedures, and whether the problem affects activities of daily living (ADLs). For trauma, always document mechanism (fall on outstretched hand/FOOSH, crush, laceration with what object, clean vs contaminated, tetanus status).
ROS: Problem-focused. Include numbness/tingling distribution, weakness, cold intolerance, night symptoms (classic for CTS), triggering/locking, and swelling.
PMHx: Diabetes (major risk factor for CTS, trigger finger, infection), thyroid disease, RA, gout, smoking (relevant for fracture healing and flap survival), anticoagulation (affects OR planning), and prior splints/injections/therapy.
Inspection: Swelling, ecchymosis, deformity, scars, nail changes, muscle atrophy (thenar/hypothenar/first dorsal interosseous). Document using anatomic landmarks, not "on the hand."
Palpation: Point tenderness (snuffbox, scaphoid tubercle, A1 pulley, radial styloid, Lister tubercle, CMC joint).
Range of motion: Active and passive for each joint, often reported as MCP/PIP/DIP = __/__/__ or as composite fingertip-to-distal-palmar-crease (FTP) distance in cm.
Neurovascular: Median/ulnar/radial sensation (2-point discrimination if needed), motor testing (OK sign for AIN, thumb abduction for APB, FDI for ulnar), capillary refill, Allen test.
Provocative tests: Tinel, Phalen, Durkan compression, Finkelstein/Eichhoff, Watson scaphoid shift, grind test (CMC), lunotriquetral ballottement.
Document each diagnosis with laterality and specific anatomic location. Plans commonly involve splinting (thumb spica, volar wrist, ulnar gutter, dorsal blocking), hand therapy (occupational vs certified hand therapist, CHT), injections, medications, imaging, and procedural scheduling. Always capture the surgeon's discussion of risks/benefits, the patient's consent, and the plan for follow-up.
Hand dominance is non-negotiable — it must appear in every single HPI. The difference between a dominant-hand injury and a non-dominant one drives therapy intensity, disability calculations, and occupational implications. If you forget which hand is dominant, ask before the patient leaves the room.
03 Distal Radius Fractures Fracture
The distal radius fracture is the most common fracture of the upper extremity. It occurs across three demographic peaks: pediatric falls, young high-energy trauma (MVCs, sports, falls from height), and low-energy osteoporotic fractures in older adults — particularly postmenopausal women. A scribe will see these in both the ED consult context and the post-reduction follow-up clinic.
Named Patterns
- Colles fracture: Extra-articular distal radius fracture with dorsal angulation ("dinner fork deformity"). The classic FOOSH injury.
- Smith fracture: Reverse Colles — distal radius fracture with volar angulation ("garden spade deformity"). Mechanism is typically a fall on the dorsum of the flexed wrist.
- Barton fracture: Intra-articular fracture-dislocation of the distal radius. Volar (more common) or dorsal rim fragment with carpus displaced along the fragment.
- Chauffeur fracture: Intra-articular radial styloid fracture. Named for hand-crank starters that kicked back; now more often seen with scapholunate ligament injury.
- Die-punch fracture: Depressed lunate facet fragment from axial load.
Evaluation & Parameters
Wrist x-rays (PA, lateral, oblique) are the workhorse. The surgeon will measure and dictate three critical radiographic parameters: radial height (normal ~11 mm), radial inclination (normal ~22°), and volar tilt (normal ~11° volar). Loss of these — especially volar tilt reversing into dorsal angulation — drives the decision to operate. Also document articular step-off, comminution, ulnar styloid involvement, and DRUJ congruence.
Classification
The Frykman classification organizes distal radius fractures by involvement of the radiocarpal joint, DRUJ, and ulnar styloid:
| Type | Radiocarpal | DRUJ | Ulnar styloid |
|---|---|---|---|
| I | Extra-articular | No | No |
| II | Extra-articular | No | Yes |
| III | Intra-articular | No | No |
| IV | Intra-articular | No | Yes |
| V | Extra-articular | Yes | No |
| VI | Extra-articular | Yes | Yes |
| VII | Intra-articular | Yes | No |
| VIII | Intra-articular | Yes | Yes |
Management
Non-displaced or minimally displaced fractures are managed in a sugar-tong or short-arm cast for 4–6 weeks. Displaced fractures are reduced under hematoma block or conscious sedation. Operative indications include intra-articular step-off >2 mm, loss of radial length >5 mm, dorsal angulation >5–10°, and failed closed reduction. The workhorse operation is open reduction internal fixation with a volar locking plate. Alternatives include percutaneous pinning, external fixation, and dorsal bridge plating for severely comminuted fractures. AAOS 2020 clinical practice guideline on distal radius fractures provides current evidence on operative vs nonoperative thresholds, especially in older adults.
Watch for acute carpal tunnel syndrome (progressive median nerve numbness after fracture), compartment syndrome of the forearm (pain out of proportion, tight forearm), and EPL rupture several weeks after injury (inability to retropulse the thumb) — the tendon attritionally ruptures over a dorsal fragment at Lister tubercle.
04 Scaphoid & Carpal Bone Fractures Fracture
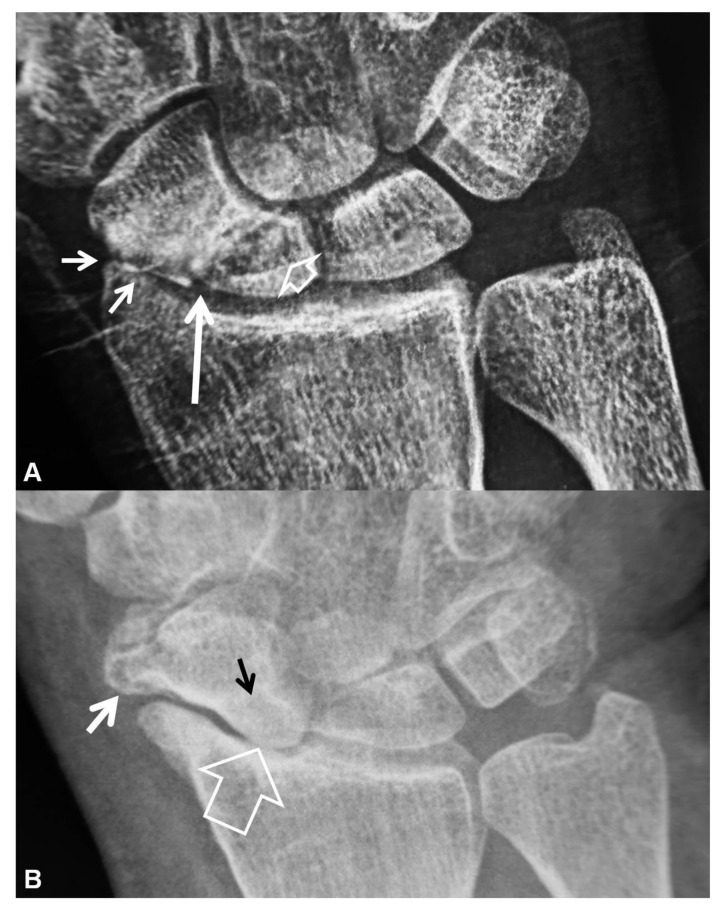
The scaphoid is the most commonly fractured carpal bone (60–70% of carpal fractures). It is notorious for nonunion and avascular necrosis because its blood supply enters through the distal pole — a proximal pole fracture interrupts flow to the proximal fragment. Classic mechanism is FOOSH with the wrist extended.
Presentation & Workup
Anatomic snuffbox tenderness plus scaphoid tubercle tenderness plus pain on axial compression of the thumb is highly suggestive. Initial x-rays (PA, lateral, oblique, scaphoid view with ulnar deviation) miss up to 25% of acute fractures. Patients with a clinical suspicion and negative films are splinted in a thumb spica and brought back at 10–14 days for repeat imaging, or advanced imaging (MRI or CT) is obtained immediately.
Classification & Management
The Mayo classification divides scaphoid fractures by location: distal pole, waist (most common, ~65%), and proximal pole (highest nonunion risk). Non-displaced distal or waist fractures are treated in a thumb spica cast for 8–12 weeks. Displaced fractures (>1 mm), proximal pole fractures, and fractures with humpback deformity are treated with open or percutaneous compression screw fixation (typically a Herbert or Acutrak headless compression screw). Scaphoid nonunion advanced collapse (SNAC wrist) is a late complication requiring salvage procedures such as proximal row carpectomy or four-corner fusion.
Other Carpal Fractures
Hook of hamate fractures (baseball/golf/racquet sports) cause ulnar wrist pain and can irritate the ulnar nerve in Guyon canal. CT of the carpal tunnel is the best imaging study; treatment is hook excision if symptomatic or non-union develops. Triquetral fractures (dorsal avulsion from wrist hyperflexion) are common but usually heal with 4–6 weeks of immobilization in a short-arm cast. Pisiform fractures are treated symptomatically, with pisiformectomy reserved for persistent pain. Capitate, trapezium, and lunate fractures are rare but important — acute lunate fractures can precede Kienböck disease.
When the ED calls with a "negative x-ray wrist sprain" in a patient with snuffbox tenderness after FOOSH, the default response is to splint in a thumb spica and follow up in 10–14 days with repeat films or obtain immediate MRI. Missing a scaphoid fracture is one of the most common and expensive hand surgery malpractice claims.
05 Carpal Instability & Perilunate Injuries Ligament
The carpus is held together by intrinsic (bone-to-bone) and extrinsic (forearm-to-carpus) ligaments. Disruption produces instability patterns.
Scapholunate (SL) Dissociation
The SL ligament links the scaphoid and lunate. Rupture causes the scaphoid to flex and the lunate to extend (DISI — dorsal intercalated segmental instability). On PA x-ray, look for an SL gap >3 mm ("Terry Thomas sign") and a cortical ring sign from the foreshortened, flexed scaphoid. On lateral, the SL angle is >60° (normal 30–60°). Watson scaphoid shift test is provocative. Untreated SL dissociation progresses to scapholunate advanced collapse (SLAC wrist). Treatment ranges from acute ligament repair to reconstruction (Brunelli, SLIC screw) to salvage (PRC, four-corner fusion).
Lunotriquetral (LT) Injury
Less common. Causes ulnar-sided wrist pain. Produces VISI (volar intercalated segmental instability). Diagnosed with lunotriquetral ballottement (Reagan test) and arthrography or MR.
Perilunate Dislocation
A high-energy injury (FOOSH with hyperextension). The carpus dislocates around the lunate in a progressive pattern described by Mayfield stages:
| Stage | Injury |
|---|---|
| I | Scapholunate ligament disruption |
| II | Stage I + capitolunate disruption |
| III | Stage II + lunotriquetral disruption (perilunate dislocation) |
| IV | Lunate dislocation (lunate flipped volarly, "spilled teacup" sign on lateral) |
These are urgent — require emergent reduction, open repair of the ligaments, and pinning. Median nerve compression is common and may require acute carpal tunnel release.
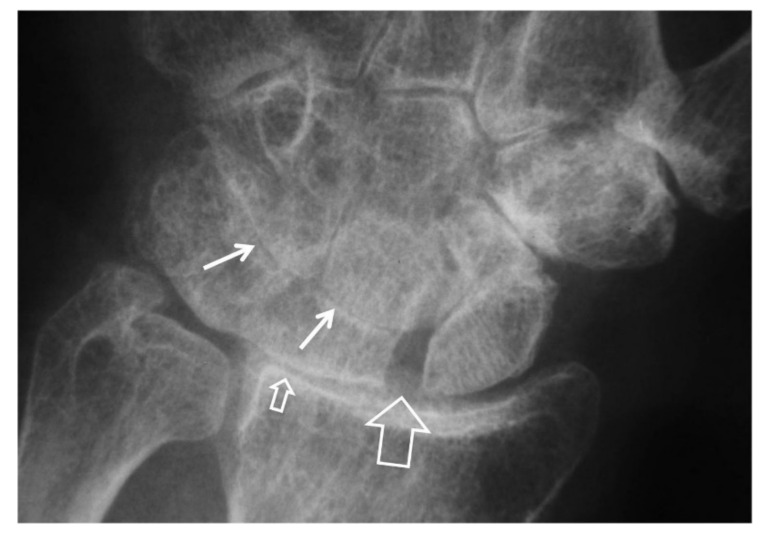
Kienböck Disease
Avascular necrosis of the lunate, often in young manual laborers with negative ulnar variance. Staged using the Lichtman classification:
| Stage | Finding |
|---|---|
| I | Normal x-ray, MRI shows edema |
| II | Sclerosis of lunate without collapse |
| IIIA | Lunate collapse, normal carpal alignment |
| IIIB | Lunate collapse with fixed scaphoid rotation |
| IV | Lunate collapse with radiocarpal and midcarpal arthritis |
Treatment includes immobilization, joint-leveling procedures (radial shortening osteotomy), revascularization, and salvage arthrodesis.
06 TFCC Injury & DRUJ Instability Ligament
The triangular fibrocartilage complex (TFCC) is the meniscus of the wrist — a shock-absorbing and stabilizing structure on the ulnar side. It connects the distal radius to the ulnar styloid and stabilizes the distal radioulnar joint (DRUJ). Injuries cause ulnar-sided wrist pain with clicking, and worsen with forearm rotation and gripping.
The Palmer classification splits TFCC lesions into traumatic (Class 1) and degenerative (Class 2) categories. Class 1A is a central perforation; 1B is an ulnar avulsion (often with DRUJ instability); 1C is a volar distal avulsion; 1D is a radial avulsion. Class 2 lesions represent progressive ulnocarpal impaction, especially in positive ulnar variance wrists.
Evaluation includes ulnar fovea sign, piano key test (for DRUJ instability), and MRI or MR arthrogram. Treatment ranges from splinting and cortisone injection to arthroscopic TFCC debridement or repair, ulnar shortening osteotomy for ulnocarpal impaction, and DRUJ reconstruction (Adams-Berger ligament reconstruction with palmaris longus graft).
DRUJ Instability & Ulnar Variance
The DRUJ allows forearm rotation (pronation/supination). Instability causes painful clunking with rotation and loss of grip strength. Exam: piano key sign (dorsally displaced ulnar head that "springs back"), pain with loaded rotation. Imaging: PA wrist films in neutral rotation to assess ulnar variance (positive, neutral, or negative) — positive variance predisposes to ulnocarpal impaction. Chronic instability after distal radius malunion may require corrective osteotomy of the radius or ulnar shortening.
07 Metacarpal & Phalangeal Fractures Fracture
Metacarpal Fractures
Boxer fracture: fifth metacarpal neck fracture from punching a solid object. Tolerates up to 40° of volar angulation in the small finger before treatment is needed. Always rule out a fight bite — a laceration over the MCP from striking teeth — which is a surgical emergency due to the risk of Eikenella/oral flora septic arthritis.
Bennett fracture: intra-articular fracture-dislocation of the base of the thumb metacarpal. The volar-ulnar fragment remains attached to the anterior oblique ligament while the shaft is pulled proximally and radially by APL. Requires reduction and pinning or ORIF.
Rolando fracture: comminuted (Y- or T-shaped) intra-articular fracture of the thumb metacarpal base. Worse prognosis than Bennett; may require ORIF or external fixation.
Phalangeal Fractures
Proximal, middle, and distal phalanx fractures are managed by location (base, shaft, neck, condyle) and rotation. Malrotation is the critical finding — the fingers should point toward the scaphoid tubercle when flexed. Even 5° of rotation creates significant finger scissoring. Displaced, rotated, or intra-articular fractures are managed with CRPP, ORIF with mini plates and screws, or dynamic traction.
08 Tendon Injuries (Flexor & Extensor) Tendon
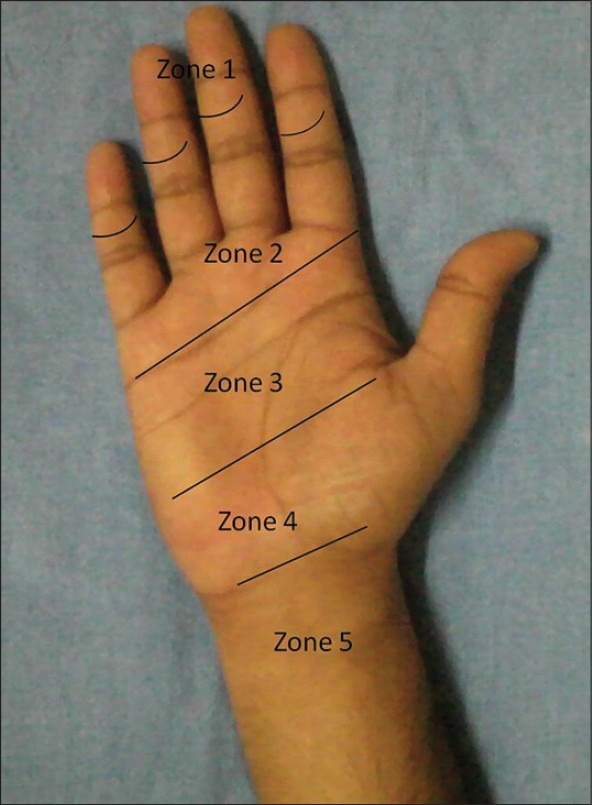
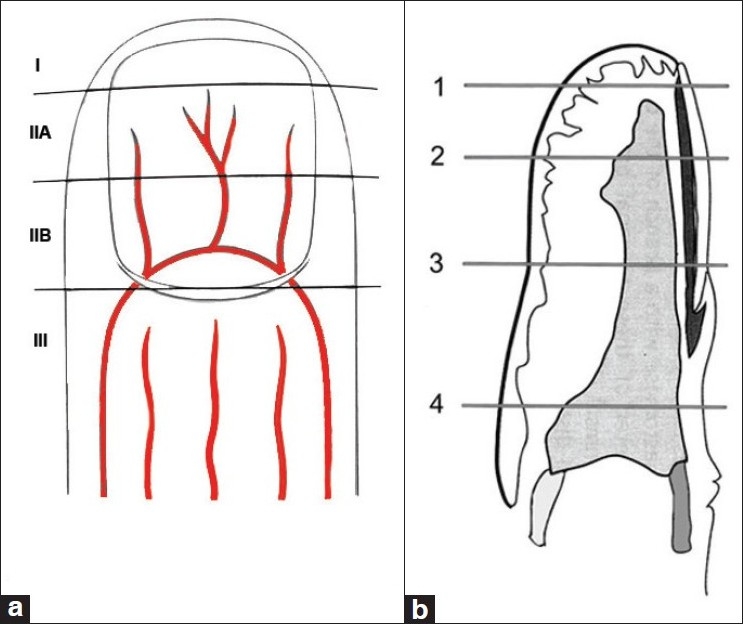
Flexor Tendon Zones (Verdan)
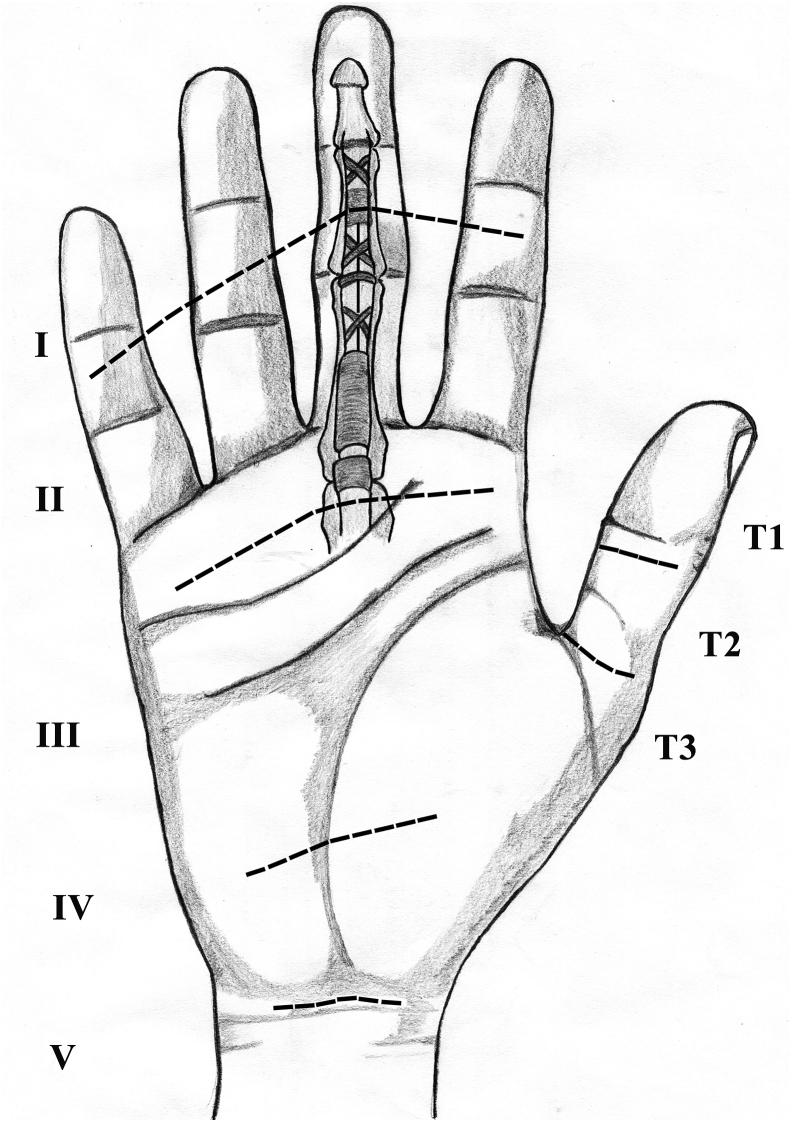
Flexor tendon lacerations are classified by the level at which they occur. The Verdan zones:
| Zone | Location | Clinical note |
|---|---|---|
| I | FDP distal to FDS insertion | Includes jersey finger |
| II | Proximal edge of A1 pulley to FDS insertion | "No man's land" — FDS and FDP run together inside the sheath; technically demanding repair |
| III | Distal edge of carpal tunnel to proximal A1 pulley (palm) | Best prognosis |
| IV | Within the carpal tunnel | Often requires carpal tunnel release at repair |
| V | Proximal to the carpal tunnel (wrist/forearm) | "Spaghetti wrist" if multiple tendons and the median/ulnar nerve |
The thumb uses a separate T1–T3 system.
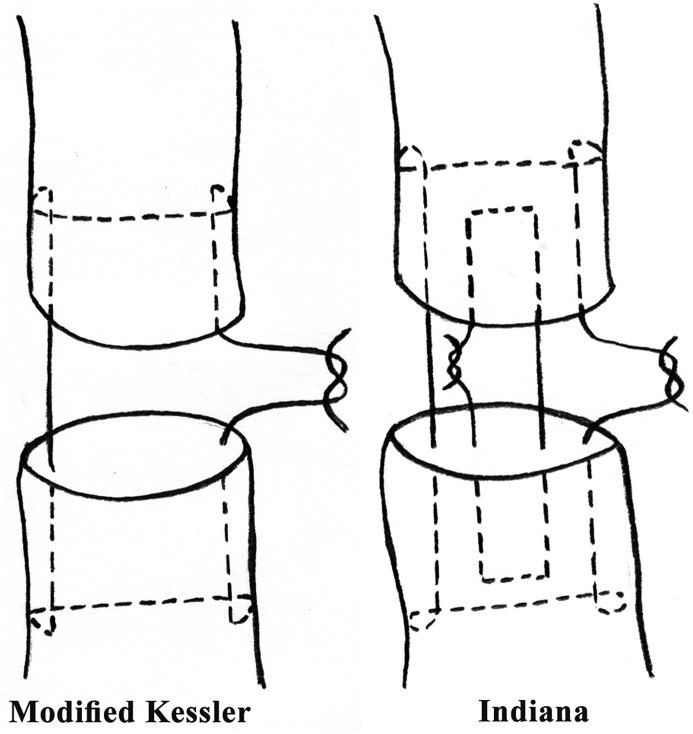
Classic exam: FDS is tested by holding all other digits in extension while the patient flexes the PIP of the tested finger. FDP is tested by isolated DIP flexion. Repair is typically within 7–10 days using a modified Kessler, Tajima, or Massachusetts General Hospital (MGH/Strickland) core suture (often 4- or 6-strand) with a running epitendinous suture. Post-op rehabilitation uses early passive or active motion protocols (Duran, Kleinert, or Indiana). The Strickland formula measures outcome as percentage of normal PIP+DIP motion.
Jersey Finger
Avulsion of the FDP from the distal phalanx, classically when a defender grabs a jersey. Ring finger is most common. Classified by Leddy and Packer (I: retraction into palm, severed vincula — repair within 7–10 days; II: retraction to PIP, vincula intact; III: retraction to A4 with bony fragment).
Extensor Tendon Zones & Injuries
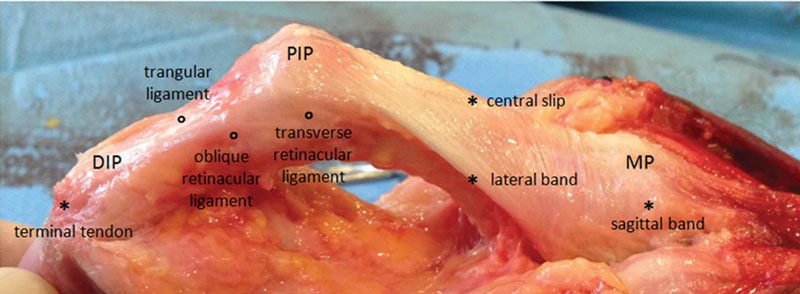
Extensor zones are 1–8 over the fingers/wrist. Mallet finger (Zone 1): terminal extensor tendon avulsion causing DIP droop; treated with 6–8 weeks of continuous DIP extension splinting. Central slip injury / boutonnière deformity (Zone 3): PIP flexion, DIP hyperextension. Swan neck deformity: PIP hyperextension, DIP flexion — often from volar plate laxity or intrinsic tightness. Open extensor lacerations are repaired with a figure-of-eight or mattress suture.
09 Stenosing Tenosynovitis Tendon
Trigger Finger
Thickening of the A1 pulley traps a nodular flexor tendon, causing catching, locking, and pain at the MCP. More common in diabetics and women 40–60. Graded by the Quinnell/Green classification:
| Grade | Finding |
|---|---|
| I | Pain, tenderness at A1 pulley, no triggering |
| II | Active triggering, correctable actively |
| III | Locking requires passive correction |
| IV | Fixed flexion contracture |
Treatment: activity modification and NSAIDs, corticosteroid injection into the flexor sheath (up to 2–3 injections), and A1 pulley release (open or percutaneous) for refractory cases.
de Quervain Tenosynovitis
Stenosing tenosynovitis of the first dorsal extensor compartment (APL and EPB). Presents with radial-sided wrist pain, worse with thumb use (classic in new mothers lifting infants). Provocative tests: Finkelstein (examiner ulnarly deviates the wrist with the thumb in the fist), Eichhoff (patient tucks thumb into fist and ulnar-deviates), WHAT (wrist hyperflexion and abduction of thumb) test. Treatment: thumb spica splint, NSAIDs, corticosteroid injection, and first dorsal compartment release if refractory. Watch for a separate EPB subcompartment during surgery.
Intersection Syndrome
Inflammation where the first dorsal compartment (APL/EPB) crosses over the second (ECRL/ECRB) approximately 4 cm proximal to Lister tubercle. Presents with dorsoradial forearm pain and crepitus. Managed with splinting, NSAIDs, and activity modification.
10 Compressive Neuropathies of the Upper Extremity Nerve
Carpal Tunnel Syndrome (CTS)
The most common compressive neuropathy. Median nerve compression beneath the transverse carpal ligament causes numbness/tingling in the radial 3.5 digits, classically waking patients at night and provoked by activities like driving or holding a phone. Risk factors include female sex, obesity, pregnancy, diabetes, hypothyroidism, and repetitive wrist flexion. Advanced cases produce thenar atrophy and weakness of thumb opposition.
Provocative tests: Phalen (wrist flexion reproduces symptoms in <60 seconds), Tinel sign (tapping over the median nerve at the wrist), and Durkan carpal compression test (direct compression on the median nerve, most sensitive). Electrodiagnostic studies (EMG/NCS) confirm slowed median sensory and motor conduction at the wrist. AAOS clinical practice guideline on carpal tunnel syndrome management endorses nocturnal neutral-wrist splinting, corticosteroid injection, and surgical release — either open carpal tunnel release (OCTR) or endoscopic (ECTR) — for refractory or severe cases.
Cubital Tunnel Syndrome
Ulnar nerve compression at the elbow, the second most common compressive neuropathy. Presents with ring/small finger numbness, weakness of grip and pinch, and positive Froment sign (compensatory thumb IP flexion by FPL when adducting the thumb against a piece of paper) and Wartenberg sign (small finger abducted). Nighttime elbow flexion worsens symptoms. Treatment: avoid prolonged elbow flexion, night extension splint, and surgical decompression — in situ release, subcutaneous transposition, or submuscular transposition, sometimes with medial epicondylectomy.
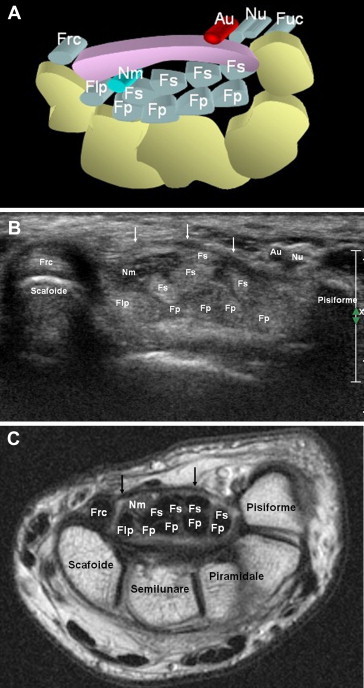
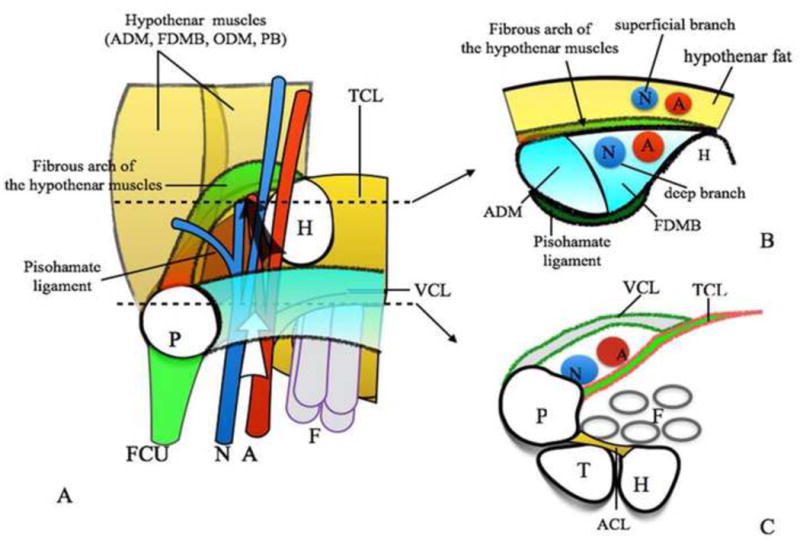
Guyon Canal Syndrome (Ulnar Tunnel)
Ulnar nerve compression at the wrist. Causes include hook of hamate fracture, ganglion cyst, and prolonged handlebar pressure ("cyclist's palsy"). Zone of compression (Shea and McClain) determines whether sensory, motor, or both are affected. Treatment is activity modification, splinting, and surgical release.
Radial Tunnel & PIN Syndrome
Compression of the radial nerve/PIN in the proximal forearm. Radial tunnel syndrome causes lateral elbow pain mimicking lateral epicondylitis but with tenderness ~4 cm distal to the lateral epicondyle. PIN syndrome causes motor weakness (finger drop, radial wrist extension with deviation because ECRL is spared) without sensory loss. Common sites of compression include the arcade of Fröhse (fibrous edge of supinator).
Anterior Interosseous Nerve (AIN) Syndrome / Pronator Syndrome
AIN is a pure motor branch — compression causes weakness of FPL, FDP to index, and pronator quadratus; the patient cannot make the "OK sign" because they can't flex the IP of the thumb and DIP of the index. Pronator syndrome involves median nerve compression at the elbow/proximal forearm (between pronator teres heads or at the lacertus fibrosus) and includes both motor and sensory symptoms — unlike CTS, it affects the palmar cutaneous branch so the thenar palm is also numb.
11 Peripheral Nerve Injuries & Brachial Plexus Nerve
Nerve injuries are graded with the Seddon and Sunderland classifications:
| Seddon | Sunderland | Injury | Recovery |
|---|---|---|---|
| Neurapraxia | I | Myelin injury, axon intact | Days to weeks, complete |
| Axonotmesis | II | Axon disrupted, endoneurium intact | 1 mm/day regeneration |
| III | Endoneurium disrupted | Incomplete, scarring | |
| IV | Perineurium disrupted | Surgery required | |
| Neurotmesis | V | Complete transection | Surgical repair mandatory |
Repair options include direct epineurial repair, nerve grafting (sural, MABC, AIN-to-ulnar transfer), nerve conduits, and motor/sensory nerve transfers. The hand surgeon often works with microsurgery colleagues for brachial plexus reconstruction.
Tendon transfers restore function after high-level nerve palsy: for high radial nerve palsy, a typical set is PT→ECRB, FCR→EDC, PL→EPL. Low median nerve palsy can use an opposition transfer (Camitz/PL, Huber, Bunnell/FDS ring). Low ulnar palsy can use Zancolli lasso, Brand, or FDS ring finger transfers for claw correction.
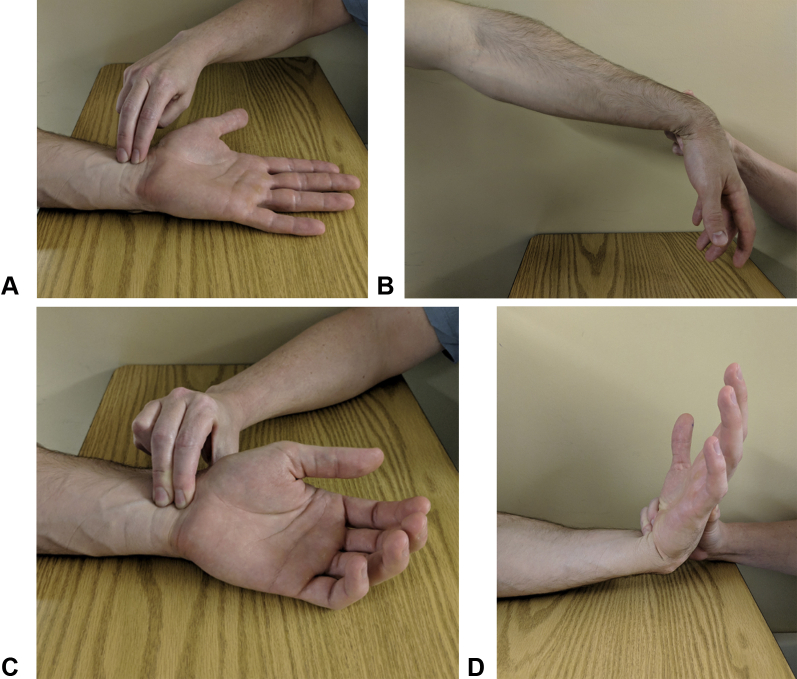
12 Dupuytren Contracture Soft tissue
A progressive fibroproliferative disease of the palmar and digital fascia producing cords and nodules that pull the fingers (especially ring and small) into flexion contracture. Northern European ancestry, diabetes, smoking, alcohol use, and male sex are risk factors (the so-called "Dupuytren diathesis"). The affected structures are pathologic cords derived from the pretendinous band, spiral band, lateral digital sheet, Grayson ligament, and natatory ligament — the Cleland ligament is spared.
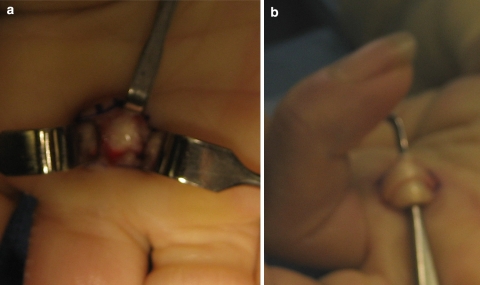
Table-top test: the patient cannot place the palm flat on a table once the MCP contracture exceeds ~30°. Treatment options:
- Observation for mild, non-progressing disease.
- Collagenase clostridium histolyticum injection followed by manipulation (Xiaflex).
- Percutaneous needle aponeurotomy — minimally invasive cord division.
- Open fasciectomy (regional or limited) — the definitive procedure, removing the diseased fascia.
- Dermofasciectomy with skin grafting for recurrent or aggressive disease.
Digital nerves can spiral within the cord and are at risk during surgery. Post-op splinting and hand therapy are standard.
13 Hand & Wrist Masses / Tumors Soft tissue
Ganglion cyst: the most common hand mass (60–70%). Mucinous fluid from a joint or tendon sheath. Dorsal wrist ganglia (70%) arise from the scapholunate ligament; volar wrist ganglia arise from the radiocarpal or STT joint and are adjacent to the radial artery; retinacular cysts come from the flexor tendon sheath. Treatment: observation, aspiration, or excision back to the stalk.
Giant cell tumor of tendon sheath (GCTTS): the second most common hand tumor; firm, slow-growing, often along a flexor tendon sheath. Treatment is marginal excision; recurrence is common.
Mucous cyst: a ganglion arising from the DIP joint in OA, often with nail grooving from pressure on the germinal matrix.
Glomus tumor: rare benign neoplasm of the glomus body, usually subungual. Classic triad: pinpoint tenderness, cold sensitivity, paroxysmal pain. Treatment is excision.
Enchondroma: the most common primary bone tumor of the hand. Usually discovered incidentally or after pathologic fracture. Treated with curettage and bone grafting.
Epidermal inclusion cyst, lipoma, schwannoma, and vascular malformations round out the differential.
14 Hand Infections Infection
The four cardinal signs described by Allen Kanavel: (1) fusiform (sausage-shaped) swelling of the digit; (2) finger held in slight flexion at rest; (3) tenderness along the flexor tendon sheath; (4) severe pain with passive extension of the finger (the most sensitive sign). This is a surgical emergency requiring IV antibiotics and urgent operative irrigation of the sheath.
- Paronychia: infection of the nail fold. Acute — usually Staph aureus; treated with warm soaks, oral antibiotics, and drainage if an abscess is present. Chronic — often Candida, in dishwashers and diabetics.
- Felon: closed-space infection of the pulp of the fingertip. Intensely painful. Drained through a longitudinal or lateral incision, breaking the vertical septa.
- Herpetic whitlow: HSV infection of the finger (clear vesicles, historically in dental/medical workers). Do NOT incise — manage with acyclovir.
- Deep space infections: thenar space, midpalmar space, Parona space. Require operative drainage and IV antibiotics.
- Septic arthritis: often after a fight bite at the MCP joint. Urgent washout, IV antibiotics.
- Animal and human bites: Pasteurella (dog/cat), Eikenella (human). Standard prophylaxis is amoxicillin-clavulanate; consider tetanus and rabies.
- Necrotizing fasciitis: pain out of proportion, crepitus, bullae, rapid progression — emergent debridement and broad-spectrum antibiotics.
IDSA practice guidelines for skin and soft tissue infections inform empiric antibiotic selection and drainage decisions.
Complex Regional Pain Syndrome (CRPS)
CRPS type 1 (reflex sympathetic dystrophy) occurs after trauma without nerve injury; type 2 (causalgia) follows a defined nerve injury. Presentation includes disproportionate burning pain, allodynia, hyperalgesia, edema, temperature asymmetry, trophic skin/nail changes, and motor dysfunction. Diagnosis is clinical via the Budapest criteria. Treatment is multimodal: early hand therapy (desensitization, mirror therapy), neuropathic medications (gabapentin, pregabalin, TCAs), stellate ganglion blocks, and avoidance of unnecessary surgery. Early recognition and aggressive therapy dramatically improve outcomes.
15 Arthritis of the Hand & Wrist Joint
Thumb CMC (Basal Joint) Arthritis
Osteoarthritis of the first carpometacarpal (trapeziometacarpal) joint is extremely common, especially in postmenopausal women. Presents with pain at the base of the thumb, weakness of pinch, and a "shouldered" appearance of the CMC. Grind test (axial compression with rotation) reproduces pain. Staged with the Eaton-Littler classification:
| Stage | Finding |
|---|---|
| I | Normal joint space, possible effusion/laxity |
| II | Joint space narrowing, small (<2 mm) osteophytes/debris |
| III | Joint space narrowing with larger osteophytes (>2 mm) and cystic changes |
| IV | Pantrapezial arthritis (CMC plus scaphotrapezial involvement) |
Treatment: splinting, NSAIDs, injection, and operative options including trapeziectomy with ligament reconstruction and tendon interposition (LRTI), suspensionplasty, CMC arthrodesis, or arthroplasty.
Hand Rheumatoid Arthritis
RA produces symmetric inflammatory arthritis affecting the MCP and PIP joints (DIPs are classically spared). Deformities include ulnar drift at the MCPs, swan neck, boutonnière, and caput ulnae at the wrist. Tendon ruptures at Lister tubercle (EPL) and over the distal ulna (EDC to small/ring — Vaughan-Jackson) are classic. Treatment focuses on DMARDs, biologics, synovectomy, tendon transfers (EIP to EPL, FDS to EDC), and joint arthrodesis or arthroplasty.
16 Fingertip, Nail Bed & Amputation Injuries Trauma
Fingertip injuries are the most common hand injury seen in the ED. Management depends on tissue loss, bone exposure, and the angle/geometry of the defect.
- Subungual hematoma: trephination (nail drill or heated paperclip) if >50% of the nail surface.
- Nail bed laceration: nail removal, nail bed repair with 6-0 or 7-0 absorbable suture, replacement of the nail or a nonadherent splint in the eponychial fold.
- Fingertip amputation with no bone exposed: healing by secondary intention (occlusive dressing).
- Fingertip amputation with bone exposed: local flap (V-Y Atasoy/Kutler advancement, cross-finger flap, thenar flap, Moberg advancement for thumb).
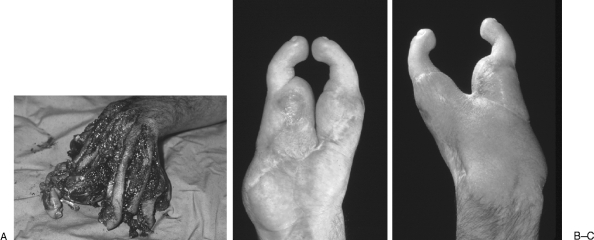
- Digital replantation: considered for thumb amputation (always attempt), multiple digit amputations, sharp amputations distal to FDS insertion, and in children. Generally not indicated for single-digit proximal to FDS insertion in an adult. Performed under operating microscope with bone fixation, extensor repair, flexor repair, arterial anastomosis, nerve repair, vein anastomosis, and skin closure. Leech therapy may be used for venous congestion.
Stener Lesion (Gamekeeper/Skier Thumb)
Rupture of the ulnar collateral ligament of the thumb MCP, often from a ski pole injury. In a true Stener lesion, the ruptured UCL is displaced superficial to the adductor aponeurosis and cannot heal without surgery. Exam reveals thumb MCP laxity >30° with radial stress (or >15° more than the contralateral side). Treatment is operative repair with a suture anchor.
17 Congenital Hand Anomalies Congenital
Congenital hand differences are classified by the Oberg-Manske-Tonkin (OMT) system, which replaced the older Swanson classification. Common entities:
- Syndactyly: webbing of adjacent digits. Simple (skin only) vs complex (bony fusion). Most commonly between the long and ring fingers. Repaired surgically with zigzag incisions and full-thickness skin grafts, typically around 12–18 months of age.
- Polydactyly: extra digit. Preaxial (thumb) is more common in Caucasians; postaxial (small finger) in people of African descent. Treatment depends on Wassel classification for preaxial thumb duplication.
- Trigger thumb in children: FPL nodule causing fixed IP flexion (Notta node). Often resolves spontaneously by age 2; A1 release for persistent cases.
- Radial club hand / radial longitudinal deficiency, cleft hand, camptodactyly, clinodactyly, macrodactyly, and constriction band syndrome are less common but recognized.
18 Hand Surgery Procedures — A to Z
| Procedure | Description / Indication |
|---|---|
| ORIF distal radius (volar locking plate) | Standard operative repair of displaced/unstable distal radius fractures |
| External fixation, distal radius | Severely comminuted or open fractures |
| Dorsal bridge plating | Highly comminuted distal radius fractures spanning the wrist |
| CRPP scaphoid / K-wire fixation | Closed reduction percutaneous pinning |
| Scaphoid compression screw (Herbert, Acutrak) | Headless compression screw for scaphoid fracture/nonunion |
| Wrist arthroscopy | Diagnostic and therapeutic — TFCC, SL ligament, synovectomy |
| TFCC repair / debridement | Arthroscopic for central tears; open for peripheral avulsions |
| Scapholunate ligament reconstruction | Brunelli, modified Brunelli, SLIC screw, capsulodesis |
| Proximal row carpectomy (PRC) | Salvage for SNAC/SLAC wrist, Kienböck III |
| Four-corner fusion | Salvage fusing capitate, lunate, triquetrum, hamate with scaphoid excision |
| Total wrist arthrodesis | End-stage wrist arthritis; definitive pain relief, no motion |
| Metacarpal/phalangeal ORIF | Mini plates, lag screws, K-wires |
| Flexor tendon repair (Kessler/MGH) | Core suture plus epitendinous; Zone II most demanding |
| Extensor tendon repair | Figure-of-eight, mattress, or modified Kessler by zone |
| Trigger finger release | Open A1 pulley release; percutaneous alternative |
| de Quervain release | First dorsal compartment release — beware EPB subcompartment |
| Carpal tunnel release (OCTR / ECTR) | Open or endoscopic release of transverse carpal ligament |
| Cubital tunnel release | In situ, subcutaneous, or submuscular transposition |
| Guyon canal release | Release of Guyon canal for ulnar tunnel syndrome |
| Dupuytren fasciectomy | Open excision of diseased palmar/digital fascia |
| Needle aponeurotomy | Percutaneous needle division of Dupuytren cord |
| Collagenase injection (Xiaflex) | Enzymatic cord lysis with next-day manipulation |
| Ganglion excision | Open or arthroscopic, back to the joint stalk |
| Nail bed repair | With or without nail removal |
| Tendon transfers | For nerve palsy (radial, median, ulnar) |
| Replantation / revascularization | Microsurgical reattachment of amputated digit or hand |
| Free tissue transfer | Free flaps (ALT, radial forearm, groin) for soft tissue coverage |
| Nerve repair / grafting / transfer | Epineurial repair, sural or MABC graft, or motor/sensory transfer |
| LRTI / CMC suspensionplasty | Ligament reconstruction tendon interposition for thumb CMC arthritis |
| Small joint fusion / arthroplasty | MCP, PIP, DIP arthrodesis or silicone/pyrocarbon arthroplasty |
| Fasciotomy (forearm/hand) | Volar forearm and carpal tunnel release for compartment syndrome |
| Escharotomy | Longitudinal release of circumferential burn eschar |
| Amputation (digital, ray, transmetacarpal) | For non-reconstructable trauma, infection, tumor |
Many hand procedures are now performed under WALANT (wide-awake local anesthesia no tourniquet) — typically 1% lidocaine with 1:100,000 epinephrine, injected in advance of the case. The patient is fully awake and can actively demonstrate tendon function intraoperatively. Carpal tunnel release, trigger finger release, and tendon transfers are commonly WALANT cases.
19 Imaging & Diagnostics
- Plain radiographs: PA, lateral, oblique; dedicated scaphoid view; stress views; clenched fist view for SL gap.
- CT: fracture characterization, occult scaphoid fractures, intra-articular step-off, malunion/nonunion evaluation.
- MRI: TFCC tears, ligament injuries, occult fractures, AVN, tumors, tendon ruptures.
- MR arthrogram: gold standard for TFCC and intrinsic carpal ligament tears.
- Ultrasound: dynamic assessment of trigger fingers, ganglia, foreign bodies, tendon ruptures.
- EMG/NCS: confirm compressive neuropathy diagnosis and severity; typical CTS findings include prolonged distal motor and sensory latencies.
- Fluoroscopy (mini C-arm): intraoperative and in-clinic for reduction confirmation and K-wire placement.
- Bone scan: occult scaphoid fracture when MRI unavailable; complex regional pain syndrome (three-phase bone scan shows periarticular uptake).
Reading a Hand X-Ray
The hand surgeon will dictate in a predictable pattern: bone (cortices, alignment, articular surfaces), joint (congruence, space, subchondral change), soft tissue (swelling, foreign body, gas). Document specific measurements verbatim: "volar tilt -15°, radial inclination 18°, radial height 8 mm, 2 mm articular step-off, comminution of the dorsal rim." Never paraphrase numeric findings. When the surgeon says "positive ulnar variance of 3 mm" or "SL gap of 5 mm on clenched fist view," write the number exactly.
Learn to recognize the difference between PA, lateral, and oblique views of the wrist at a glance — the surgeon will often say "look at the lateral" and expect you to know which image they mean without interrupting the exam.
20 Medications You Must Know
| Class / Name | Brand | Use | Notes |
|---|---|---|---|
| Cephalexin | Keflex | Cellulitis, paronychia | 500 mg PO QID x 7 d |
| Dicloxacillin | — | Staph skin infection | Alternative to cephalexin |
| Amoxicillin-clavulanate | Augmentin | Bite wounds (human/animal) | Covers Pasteurella, Eikenella, oral anaerobes |
| TMP-SMX | Bactrim | MRSA coverage | Combine with cephalexin for strep |
| Doxycycline | Vibramycin | MRSA, Pasteurella alternative | Avoid in children <8 |
| Clindamycin | Cleocin | Penicillin-allergic, MRSA | C. difficile risk |
| Vancomycin IV | — | MRSA, deep infection | Trough monitoring |
| Piperacillin-tazobactam | Zosyn | Deep space, polymicrobial | Broad-spectrum IV |
| Acyclovir | Zovirax | Herpetic whitlow | Do NOT incise |
| Ibuprofen / naproxen | Motrin / Naprosyn | Pain, tenosynovitis, arthritis | First-line for most overuse |
| Acetaminophen | Tylenol | Multimodal pain | Max 3–4 g/day |
| Tramadol | Ultram | Moderate pain | Weak opioid; lower risk |
| Oxycodone / hydrocodone | Percocet / Norco | Post-op pain | Short course, typically 3–5 days |
| Gabapentin / pregabalin | Neurontin / Lyrica | Neuropathic pain, CRPS | Titrate; sedation |
| Triamcinolone / methylprednisolone | Kenalog / Depo-Medrol | Trigger finger, de Quervain, CTS injections | Max 2–3 injections per site |
| Lidocaine 1% +/- epi | Xylocaine | Local anesthetic, WALANT | Epi safe in digits (modern evidence) |
| Bupivacaine 0.25–0.5% | Marcaine | Long-acting local/regional | Cardiotoxic if intravascular |
| Collagenase | Xiaflex | Dupuytren cord | Injected, manipulated next day |
| Tetanus toxoid (Tdap/Td) | — | Contaminated wounds | Booster if >5 years |
21 Classification Systems
All major classifications used in hand surgery are enumerated within their respective condition sections above. Key references include:
- Frykman — distal radius fractures (Section 03)
- Mayo — scaphoid fractures (Section 04)
- Mayfield — perilunate injury progression (Section 05)
- Lichtman — Kienböck disease (Section 05)
- Palmer — TFCC lesions (Section 06)
- Bennett / Rolando — thumb metacarpal base fractures (Section 07)
- Verdan — flexor tendon zones I–V (Section 08)
- Leddy and Packer — jersey finger (Section 08)
- Strickland / Boyes — flexor tendon outcome (Section 08)
- Quinnell / Green — trigger finger (Section 09)
- Seddon / Sunderland — nerve injury (Section 11)
- Eaton-Littler — thumb CMC arthritis (Section 15)
- Wassel — thumb polydactyly (Section 17)
- Oberg-Manske-Tonkin (OMT) — congenital hand differences (Section 17)
22 Physical Exam — The Hand Exam
Inspection: Resting posture, cascade, swelling, ecchymosis, deformity, scars, nail changes, thenar/hypothenar bulk.
Palpation: Snuffbox, scaphoid tubercle, Lister tubercle, radial/ulnar styloid, DRUJ, CMC, MCP, PIP, DIP joints, A1 pulley, first dorsal compartment.
ROM: Wrist flexion/extension, radial/ulnar deviation, pronation/supination; digital MCP/PIP/DIP; composite fingertip-to-distal palmar crease.
Strength: Grip (dynamometer, Jamar), pinch (key, tip, tripod), intrinsic strength (FDI, abductor digiti minimi), thumb opposition (APB).
Sensation: Light touch and two-point discrimination (<6 mm normal) in median, ulnar, and radial distributions.
Vascular: Capillary refill, Allen test, radial and ulnar artery palpation.
Provocative tests: Tinel, Phalen, Durkan, Finkelstein/Eichhoff, Watson scaphoid shift, grind, LT ballottement, piano key, Froment, Wartenberg, elbow flexion test, scratch collapse.
23 Abbreviations Master List
24 Sample HPI Templates
68-year-old right-hand-dominant retired teacher with history of osteoporosis, hypertension, and hypothyroidism who presents as a transfer from outside ED for evaluation of a left distal radius fracture. She was walking her dog yesterday when she tripped on a curb and fell onto her outstretched left hand. She reports immediate pain, swelling, and deformity of the left wrist. She denies numbness, tingling, or weakness in the fingers. She was splinted in a sugar-tong at the outside facility. X-rays today demonstrate a comminuted, dorsally angulated intra-articular distal radius fracture with 20° of dorsal tilt, 6 mm of radial shortening, and a 3 mm articular step-off. Neurovascularly intact. Patient is here to discuss operative fixation.
54-year-old right-hand-dominant accountant with history of type 2 diabetes and obesity presents with a 9-month history of bilateral hand numbness, right worse than left. She describes burning and tingling in the thumb, index, and long fingers that wake her at night several times per week, and worsen with driving and typing. She has to "shake out" her hands to get relief. She reports dropping small objects and describes thenar weakness. She has tried OTC night splints and ibuprofen without benefit. EMG/NCS performed last month demonstrates moderate to severe right median mononeuropathy at the wrist with prolonged distal motor and sensory latencies and mild-to-moderate left CTS. She presents today to discuss surgical carpal tunnel release.
61-year-old right-hand-dominant diabetic woman presents with a 4-month history of right long finger catching and locking. Symptoms began insidiously and have progressed to the point where the finger locks in flexion each morning and she must passively extend it with her other hand. She reports pain at the base of the finger on the palmar side. She has not had prior injection or therapy. On exam, there is a palpable nodule at the A1 pulley of the right long finger with active triggering (Quinnell grade II). She is interested in a corticosteroid injection today.
28-year-old right-hand-dominant male line cook presents as an ED consult for evaluation of a right ring finger laceration. He cut his finger with a kitchen knife approximately 3 hours ago while prepping food. On exam, there is a clean 2 cm transverse laceration over the volar proximal phalanx in Zone II. He is unable to flex the DIP or PIP of the right ring finger. Sensation is intact in both radial and ulnar digital nerve distributions and capillary refill is brisk. X-rays show no bony injury. Assessment: right ring finger Zone II FDS and FDP laceration. Tetanus up to date. Plan for operative repair within 48 hours.
42-year-old left-hand-dominant male dishwasher with history of poorly controlled diabetes presents with 3 days of right thumb swelling, redness, and pain beginning at the nail fold after "picking at a hangnail." He reports throbbing pain that is worse overnight, subjective fevers, and pus draining from the eponychial fold this morning. On exam, there is a fluctuant acute paronychia of the right thumb with extension of erythema to the mid-proximal phalanx. No streaking. He is afebrile, VSS. Flexor tendon sheath is nontender with no Kanavel signs. Plan: bedside I&D, cephalexin, warm soaks, and 48-hour recheck.
66-year-old right-hand-dominant male of Northern European descent with history of hyperlipidemia and remote alcohol use presents with progressive inability to fully extend the right ring finger over the past 2 years. He describes a thickening band in the palm that has pulled the finger into flexion. He cannot put his hand flat in his pocket or shake hands normally. Family history positive for his father having similar hand problems. On exam, there is a palpable pretendinous cord extending from the distal palmar crease to the proximal phalanx of the right ring finger with an MCP contracture of 45° and a PIP contracture of 20°. Positive tabletop test. Sensation is intact in both digital nerves. He is interested in treatment options including collagenase injection versus open fasciectomy.
A great hand surgery scribe captures three things in every HPI: hand dominance, mechanism/time course, and the functional impact on work and ADLs. If any of those are missing, the note is incomplete regardless of how detailed the rest is.
25 References & Sources
Clinical Practice Guidelines
Landmark Publications
Lalonde D. Wide-awake hand surgery and therapy: WALANT. Journal of Hand Surgery. 2013.
Hurst LC et al. CORD I Trial — Collagenase for Dupuytren Contracture. NEJM. 2009.
Strickland JW. Flexor tendon repair: results and techniques. Hand Clinics. 1994.
Palmer AK. Triangular fibrocartilage complex lesions: a classification. J Hand Surg Am. 1989.
Diagram & Figure Sources
Figure 1: Skeletal Anatomy of the Hand. OpenStax College. CC BY 3.0.
Figure 2: Carpal Bones. Wikimedia Commons. Public domain.
Figure 3: Carpal Tunnel Anatomy. NIH/NIAMS. Public domain.
Figure 4: Median and Ulnar Nerve Distribution. After Gray's Anatomy. Public domain.
Figure 5: Colles-Type Distal Radius Fracture. Wikimedia Commons. CC BY-SA.
Figure 6: Trigger Finger. Wikimedia Commons. CC BY-SA.
Hand surgery is a specialty of millimeters and minutes. A great hand scribe learns the anatomy, masters the zones and compartments, and writes notes that capture exactly what the surgeon sees. Document hand dominance, mechanism, neurovascular exam, and functional status on every patient. Learn the names of the provocative tests and what they are testing. When you can hear "Zone II flexor tendon injury with intact digital nerves, planning for modified Kessler repair under WALANT" and chart it verbatim without flinching, you have arrived.