Hospitalist Medicine
Every admission diagnosis, inpatient workflow, procedure, medication, classification, and documentation framework a hospital medicine scribe needs to succeed on day one and beyond.
All diagrams on this page are sourced from published educational or institutional materials rather than AI generation. Each figure caption links to the original source, and the full diagram and guideline citations are collected in the references section at the bottom.
01 Hospital Medicine — The Systems You Must Know
Hospital medicine (hospitalist medicine) is the specialty of inpatient adult general medicine. Hospitalists admit, manage, and discharge patients on the medical wards, run rapid responses and code blues, co-manage surgical patients, coordinate transitions of care, and handle everything from community-acquired pneumonia to decompensated cirrhosis. A hospitalist's workday is a churn of new admissions, teaching-round progress notes, family meetings, consult placement, and discharge coordination — and a scribe is expected to keep pace across every one of these documentation streams.
Because hospitalists see virtually every organ system, your anatomy foundation has to be broad rather than deep. You do not need the granular detail a surgical scribe needs, but you must recognize the physiology the hospitalist is treating minute by minute.
Cardiopulmonary Essentials
The heart is a four-chamber pump. Deoxygenated blood from the systemic veins enters the right atrium, passes through the tricuspid valve to the right ventricle, is ejected through the pulmonic valve into the pulmonary artery for oxygenation in the lungs, returns via the pulmonary veins to the left atrium, passes the mitral valve to the left ventricle, and is ejected through the aortic valve into the aorta. Preload (venous return to the right heart), afterload (systemic vascular resistance), and contractility are the three levers hospitalists pull in heart failure. The cardiac conduction system drives rhythm: SA node → AV node → His bundle → right and left bundle branches → Purkinje fibers.
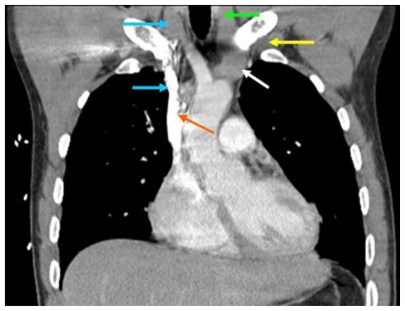
The lungs are divided into right (three lobes — upper, middle, lower) and left (two lobes plus lingula) hemithoraces. Air enters through the trachea, which bifurcates at the carina into the right and left mainstem bronchi. The right mainstem is more vertical, which is why aspiration and misplaced endotracheal tubes preferentially lodge on the right. Alveoli are the gas-exchange units. The pleural space sits between the visceral and parietal pleurae — a potential space where effusions, blood (hemothorax), or air (pneumothorax) collect.
Renal, Hepatic & GI Essentials
The kidneys filter blood through the glomeruli, regulate volume through the tubules, and produce urine that drains via the ureters into the bladder. Creatinine and BUN are the crude bedside markers of renal function; eGFR is calculated from creatinine. The liver clears bilirubin, synthesizes albumin and clotting factors, and metabolizes most drugs. The portal venous system drains the gut into the liver before systemic return; portal hypertension produces varices, ascites, and encephalopathy. The gut runs from the esophagus through the stomach, small bowel (duodenum, jejunum, ileum), and colon (cecum, ascending, transverse, descending, sigmoid, rectum).
Neurological Essentials
Altered mental status is a hospitalist's daily companion. You should know the basics of the Glasgow Coma Scale (eye, verbal, motor components; range 3–15), the difference between delirium (acute, fluctuating, reversible), dementia (chronic, progressive), and encephalopathy (global brain dysfunction from a metabolic cause), and the major stroke syndromes (MCA, ACA, PCA, brainstem, cerebellar).
On the wards you will hear the hospitalist say things like “he’s in Afib with RVR, rate 140s, SBP 90s” or “new O2 requirement, 4L NC, bibasilar crackles, BNP 2800” and be expected to chart it in real time. Learn the rhythm of a hand-off: diagnosis → vitals → exam finding → plan. That is the unit of thought in hospital medicine.
The Hospitalist Workday
A typical hospitalist workday begins with sign-out from the night team at 6–7 AM, followed by pre-rounds on the existing list, chart review, morning rounds with the team (nursing, pharmacy, case management, social work), new admissions from the ED throughout the day, rapid responses or code calls as they arise, afternoon family meetings, and finally discharge coordination and sign-out to the night team. Every hand-off point is a documentation opportunity. The hospitalist carries 12–18 patients on a typical day service — meaning scribe efficiency directly determines whether the team finishes on time.
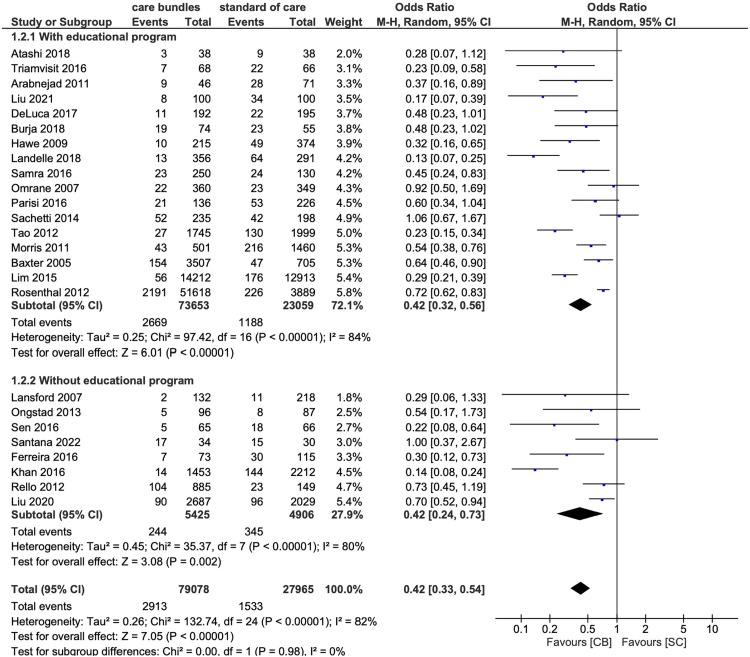
Understand the difference between admission orders (the initial order set: diet, activity, IV fluids, DVT prophylaxis, home meds, code status, monitor, labs, imaging, consults) and daily orders (tweaks to the running plan). Know where your hospital’s order sets live — CAP, HF, DKA, sepsis, and alcohol withdrawal all have pre-built bundles you will see referenced constantly.
02 Scribe Documentation Framework (H&P, Progress, Discharge)
Hospital medicine generates three core note types every single day: the admission history and physical (H&P), the daily progress note (SOAP), and the discharge summary. Consultation notes, procedure notes, and event notes (rapid response, code, family meeting) appear as needed. Your job is to know what belongs in each.
CC: one line, patient’s stated reason or referring physician’s reason for admission.
HPI: a narrative story of the presenting illness. Always capture onset, character, severity, associated symptoms, prior episodes, outpatient workup, and ER course (triage vitals, labs drawn, imaging obtained, treatments given, response).
ROS: a 10–14 system review. Hospitalists routinely document a complete ROS on admission.
PMH / PSH / FH / SH: capture every chronic condition, surgical history, family cardiac/cancer history, tobacco (pack-years, quit date), alcohol (standard drinks per week, AUDIT-C if relevant), illicit drugs, living situation, functional baseline, advance directives, code status.
Medications & Allergies: reconcile home meds with what was given in the ED. List allergies with reaction type.
Vitals & Physical Exam: head-to-toe exam. Document abnormals specifically and pertinent negatives.
Data: labs (with trends when available), imaging, EKG, cultures.
Assessment & Plan: problem-based. Each problem gets a short reasoning paragraph and a bulleted plan.
Subjective: overnight events, patient’s current symptoms, appetite, pain, bowel/bladder, sleep, ambulation.
Objective: Tmax/Tcurrent, vital range (24h), I/O, weight, telemetry summary, pertinent exam, new labs/imaging.
Assessment: one-line summary (“68M admitted for CAP on HD3, clinically improving”).
Plan by problem: each active problem with current status and next steps. Always include DVT prophylaxis, GI prophylaxis (when appropriate), code status, disposition.
Admission date, discharge date, admitting and discharge diagnoses, brief HPI, hospital course by problem, procedures performed, consultations, pertinent labs/imaging, discharge medications (with changes highlighted), discharge condition, discharge disposition, follow-up appointments, pending results, code status, and patient/family education. Medication reconciliation is mandatory.
Hospitalists bill on medical decision making and time under current inpatient E/M rules. The A&P is where the billing lives — be meticulous about capturing the number of problems addressed, data reviewed (labs, imaging, old records), and risk (decisions around admission, meds, procedures). A sloppy A&P is a sloppy bill.
03 Community-Acquired & Hospital-Acquired Pneumonia Infectious
Pneumonia is infection of the lung parenchyma. It is one of the top three reasons for medical admission. Classification is by where it was acquired: CAP (community-acquired), HAP (hospital-acquired, ≥48 hours after admission), VAP (ventilator-associated), and aspiration pneumonia.
Pathophysiology & Microbiology
Organisms colonize the oropharynx and are microaspirated into the lower airways, overwhelming mucociliary clearance and alveolar macrophages. Streptococcus pneumoniae remains the most common CAP pathogen. Other CAP organisms include Haemophilus influenzae, Moraxella catarrhalis, atypicals (Mycoplasma, Chlamydia pneumoniae, Legionella), and respiratory viruses (influenza, RSV, SARS-CoV-2). HAP and VAP shift the spectrum to Pseudomonas aeruginosa, MRSA, and Gram-negative rods. Aspiration pneumonia in frail elderly adds anaerobes and oral flora.
Clinical Presentation
Fever, productive cough, dyspnea, pleuritic chest pain, and focal crackles or bronchial breath sounds. Elderly or immunocompromised patients may present only with altered mental status, falls, or tachypnea without classic symptoms. Always document RR and SpO2 on room air at presentation — both matter for severity scoring.
Workup
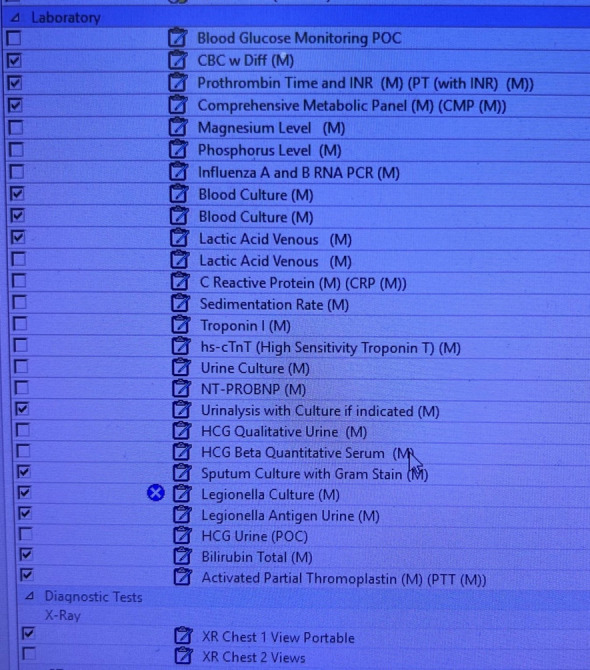
CBC, BMP, lactate, procalcitonin (if used locally), blood cultures × 2 before antibiotics in severe CAP/HAP, sputum Gram stain and culture, respiratory viral panel, urinary Legionella and Pneumococcal antigens in severe disease, MRSA nasal PCR, and chest X-ray (two-view if possible). CT chest if X-ray is ambiguous or complications are suspected (empyema, abscess).
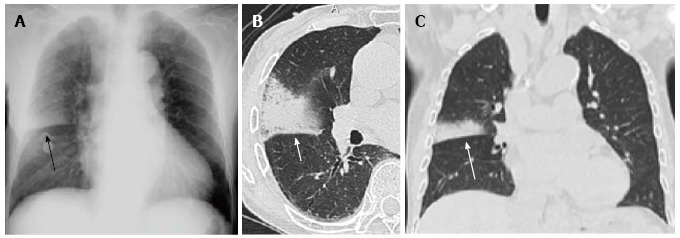
On X-ray, you will hear the hospitalist describe “lobar consolidation,” “patchy bilateral infiltrates,” “interstitial pattern,” “cavitary lesion,” or “parapneumonic effusion.” Chart the reader’s description in the radiology section verbatim when possible — ambiguous findings often drive CT and repeat imaging decisions.
Each criterion scores 1 point: Confusion (new), Urea (BUN > 19 mg/dL), Respiratory rate ≥ 30, Blood pressure (SBP < 90 or DBP ≤ 60), age ≥ 65.
0–1: outpatient. 2: short admission or observation. 3–5: inpatient, consider ICU (especially 4–5). Severe CAP is also defined by ATS/IDSA minor criteria (e.g., RR ≥ 30, PaO2/FiO2 ≤ 250, multilobar infiltrates, confusion, uremia, leukopenia, thrombocytopenia, hypothermia, hypotension requiring fluids) or major criteria (mechanical ventilation, septic shock requiring pressors).
Management
Non-severe inpatient CAP: a beta-lactam (ceftriaxone 1–2 g IV daily) plus a macrolide (azithromycin 500 mg IV/PO daily), or respiratory fluoroquinolone monotherapy (levofloxacin 750 mg IV/PO daily). Severe CAP: same plus MRSA and Pseudomonas coverage if risk factors present (vancomycin or linezolid, and piperacillin-tazobactam or cefepime). HAP/VAP: empirically cover MRSA and Pseudomonas, de-escalate on cultures. The 2019 ATS/IDSA CAP guideline is the standard citation, and the 2016 IDSA/ATS HAP/VAP guideline covers hospital-acquired disease.
Always document the first antibiotic dose and time — door-to-antibiotic time is a quality metric. Document the O2 requirement at every visit: room air, NC liters, Venturi mask FiO2, NRB, HFNC flow/FiO2, BiPAP settings. These drive severity scoring and daily clinical decisions.
04 COPD Exacerbation Pulmonary
COPD exacerbation (AECOPD) is an acute worsening of baseline dyspnea, cough, or sputum production beyond normal day-to-day variation. It is triggered most commonly by viral or bacterial lower respiratory infections (H. influenzae, M. catarrhalis, S. pneumoniae, Pseudomonas in advanced disease) and environmental exposures.
Pathophysiology
Chronic bronchitis and emphysema produce fixed airflow obstruction from airway inflammation, mucus hypersecretion, and destruction of alveolar walls. Acute triggers increase airway resistance, worsen air trapping, and produce hypercapnic respiratory failure in severe cases. The classic ABG shows a mixed respiratory acidosis with compensated chronic CO2 retention acutely worsening.
Workup
Chest X-ray (rule out pneumonia, pneumothorax, pulmonary edema), ABG or VBG for pH and pCO2, BNP to differentiate from heart failure, viral panel, sputum culture if purulent, and EKG if any cardiac concern. Document smoking pack-years, home O2, home BiPAP, baseline ambulatory saturation, and GOLD stage if known.
| Group | Symptoms (mMRC/CAT) | Exacerbation History | Initial Therapy |
|---|---|---|---|
| A | Low (mMRC 0–1, CAT < 10) | 0–1 moderate, no hospitalization | Bronchodilator |
| B | High (mMRC ≥ 2 or CAT ≥ 10) | 0–1 moderate, no hospitalization | LABA + LAMA |
| E | Any | ≥ 2 moderate or ≥ 1 hospitalization | LABA + LAMA (± ICS if eos ≥ 300) |
Management
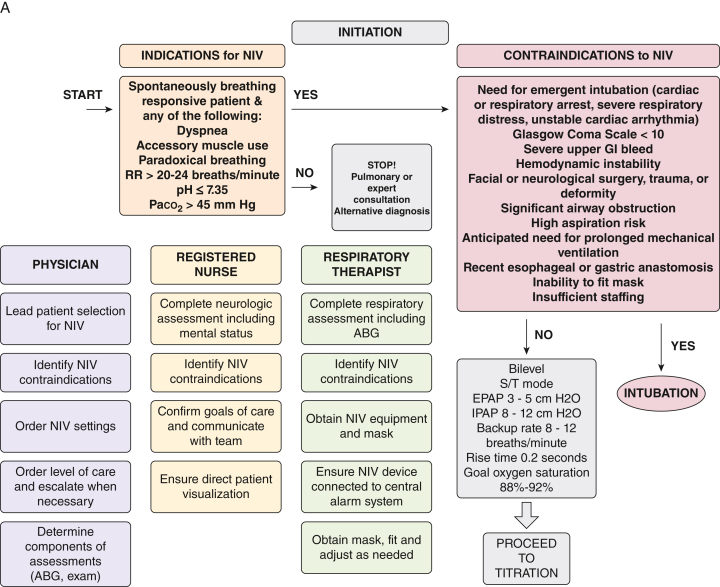
The inpatient bundle is bronchodilators + corticosteroids + antibiotics + oxygen. Albuterol 2.5 mg and ipratropium 0.5 mg nebulized q4–6h (or MDI equivalents), prednisone 40 mg PO daily × 5 days (or methylprednisolone 40–60 mg IV q12h if NPO), and azithromycin or doxycycline or amoxicillin-clavulanate for 5–7 days if increased sputum purulence. Target SpO2 88–92% to avoid CO2 retention. BiPAP (start 10/5, titrate) is first-line for hypercapnic respiratory failure; intubate for failure of NIV, altered mental status, or hemodynamic instability. Guideline reference: GOLD 2024 Strategy.
05 Acute Heart Failure (ADHF) Cardiac
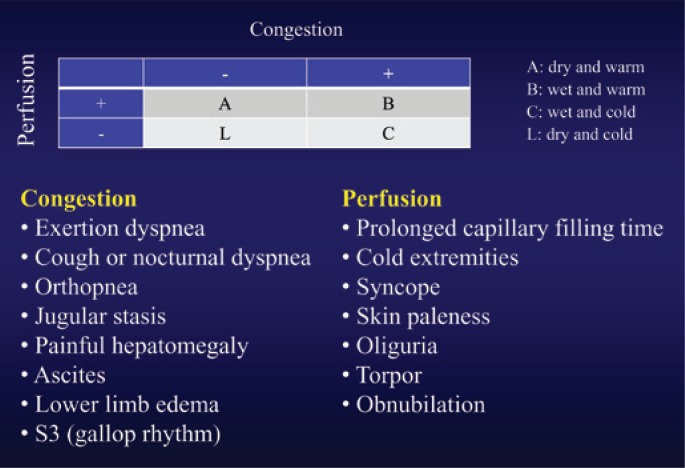
Acute decompensated heart failure is a clinical syndrome of congestion and/or hypoperfusion in a patient with underlying structural or functional cardiac disease. It is subclassified by ejection fraction into HFrEF (EF ≤ 40%), HFmrEF (41–49%), and HFpEF (≥ 50%).
Pathophysiology
Decompensation arises from volume overload (dietary sodium, medication non-adherence, IV fluids), pressure overload (uncontrolled hypertension), arrhythmia (new AF), ischemia, or high-output states (anemia, thyrotoxicosis). The result is elevated left-sided filling pressures, pulmonary edema, and in severe cases low cardiac output.
Clinical Presentation & Workup
Dyspnea, orthopnea, PND, leg edema, weight gain, and fatigue. Exam shows JVD, bibasilar crackles or rales, S3 gallop, hepatomegaly, peripheral edema. BNP or NT-proBNP (> 400 supports HF, with caveats in obesity and AKI), chest X-ray (cephalization, Kerley B lines, interstitial edema, effusions), EKG, troponin (rule out ischemia), and echocardiogram to assess EF and structure.
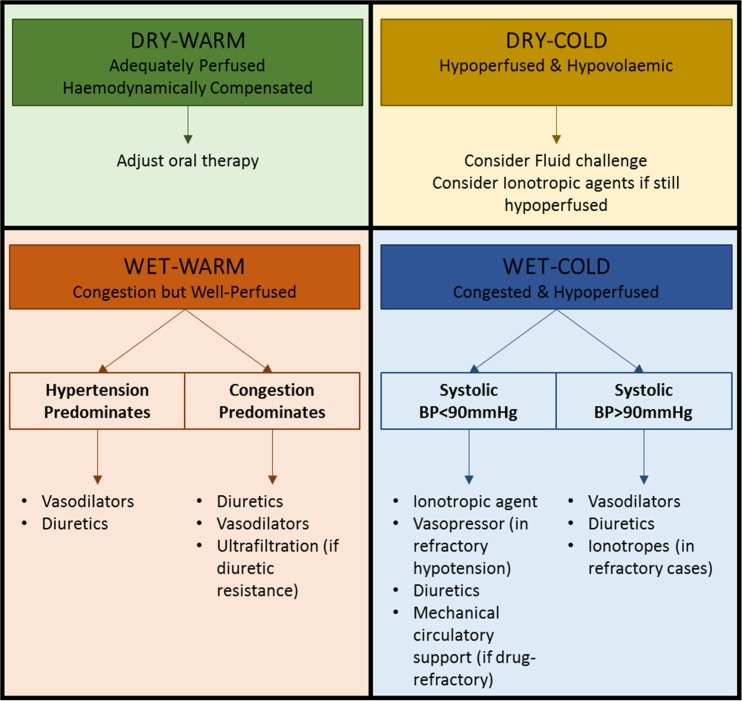
Warm & dry (well-compensated). Warm & wet (congested but perfused — most ADHF admissions; give diuretics). Cold & wet (congested and hypoperfused; diuretics + inotropes ± pressors). Cold & dry (hypoperfused without congestion; cautious fluids, evaluate for alternative diagnosis). This mental model drives management.
Management
IV loop diuretic is first-line for wet profiles. Furosemide 40–80 mg IV (or 2.5× the home oral dose) with goal net negative 1–2 L/day. Strict I/O and daily weights are mandatory. Add a thiazide (metolazone 5 mg, chlorothiazide 500 mg IV) for diuretic resistance. Continue guideline-directed medical therapy (GDMT) for HFrEF: the four pillars are ARNI/ACEi/ARB, evidence-based beta-blocker (carvedilol, metoprolol succinate, bisoprolol), MRA (spironolactone, eplerenone), and SGLT2 inhibitor (dapagliflozin, empagliflozin). Reference: 2022 AHA/ACC/HFSA Heart Failure Guideline.
06 Sepsis & Septic Shock Infectious
Sepsis is life-threatening organ dysfunction caused by a dysregulated host response to infection (Sepsis-3 definition). Septic shock is sepsis with circulatory and cellular/metabolic dysfunction requiring vasopressors to maintain MAP ≥ 65 mmHg AND lactate > 2 mmol/L despite adequate fluid resuscitation.
Pathophysiology
An infectious insult triggers widespread cytokine release, endothelial dysfunction, capillary leak, microvascular thrombosis, and distributive shock. End-organ hypoperfusion produces AKI, hepatic dysfunction, encephalopathy, coagulopathy (DIC), and respiratory failure (ARDS).
qSOFA (bedside screen, ≥ 2 = higher risk): altered mental status (GCS < 15), SBP ≤ 100 mmHg, RR ≥ 22.
SOFA (full organ failure score; ≥ 2 point rise from baseline defines organ dysfunction): respiration (PaO2/FiO2), coagulation (platelets), liver (bilirubin), cardiovascular (MAP/pressors), CNS (GCS), renal (creatinine/UOP).
Management — Hour-1 Bundle
The Surviving Sepsis Campaign 2021 bundle: (1) measure lactate, remeasure if initial > 2; (2) blood cultures before antibiotics; (3) broad-spectrum antibiotics within one hour; (4) 30 mL/kg crystalloid for hypotension or lactate ≥ 4; (5) vasopressors (norepinephrine first-line) for MAP < 65 despite fluids. Source control is critical — drain abscesses, remove infected lines, debride necrotic tissue.
Document the exact time of first lactate, first blood culture, first antibiotic dose, and fluid start/complete times. CMS SEP-1 and most institutional quality programs live or die on these timestamps. If the hospitalist mentions “source,” chart it: “Suspected source: urinary (pyuria, flank pain).”
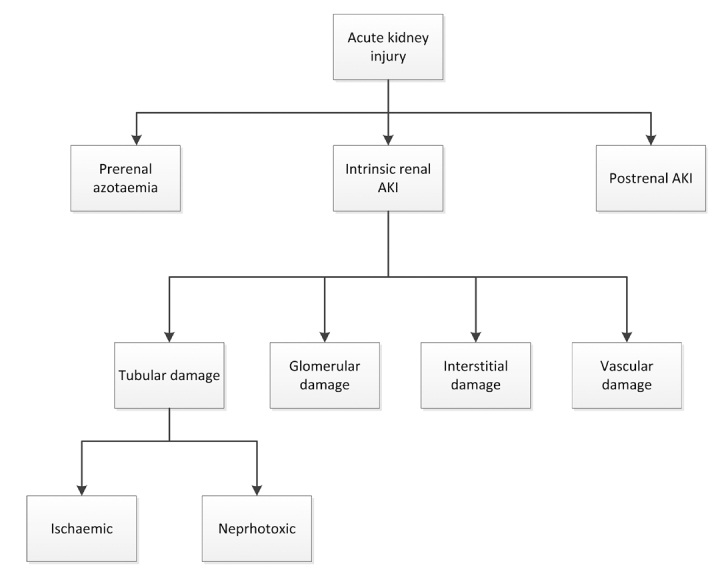
07 Acute Kidney Injury (AKI) Renal
AKI is an abrupt decline in kidney function. Causes are classified as prerenal (hypoperfusion — volume depletion, hypotension, HF, cirrhosis, NSAIDs, ACEi/ARB), intrinsic (ATN from ischemia or nephrotoxins, AIN, glomerulonephritis, rhabdomyolysis), and postrenal (obstruction).
| Stage | Creatinine Criteria | Urine Output Criteria |
|---|---|---|
| 1 | 1.5–1.9× baseline OR ≥ 0.3 mg/dL increase | < 0.5 mL/kg/h for 6–12 h |
| 2 | 2.0–2.9× baseline | < 0.5 mL/kg/h for ≥ 12 h |
| 3 | ≥ 3.0× baseline OR Cr ≥ 4.0 OR initiation of RRT | < 0.3 mL/kg/h for ≥ 24 h OR anuria ≥ 12 h |
Workup
BMP (and trend), urinalysis with microscopy, urine sodium, urine creatinine, FeNa or FeUrea, renal ultrasound to exclude obstruction, review meds for nephrotoxins, review I/O and weight trends. Muddy brown casts suggest ATN, RBC casts glomerulonephritis, WBC casts AIN or pyelonephritis.
Management
Treat the cause. Prerenal: fluids if volume-depleted, vasopressors if hypoperfused. Intrinsic: stop offending drugs, supportive care. Postrenal: Foley catheter, urology consult for upper-tract obstruction. Indications for urgent dialysis (mnemonic AEIOU): Acidosis refractory, Electrolytes (hyperkalemia refractory), Ingestions (toxic alcohols, salicylates, lithium), Overload refractory, Uremia (pericarditis, encephalopathy, bleeding).
08 Hyperglycemic Crises (DKA / HHS) & Inpatient Glucose Endocrine
Diabetic ketoacidosis (DKA): insulin deficiency produces hyperglycemia, ketogenesis, and an anion-gap metabolic acidosis. Classic triad: glucose > 250, pH < 7.30 or bicarb < 18, positive serum or urine ketones. Hyperosmolar hyperglycemic state (HHS): profound hyperglycemia (often > 600), osmolality > 320, minimal ketosis, severe volume depletion, and altered mental status.
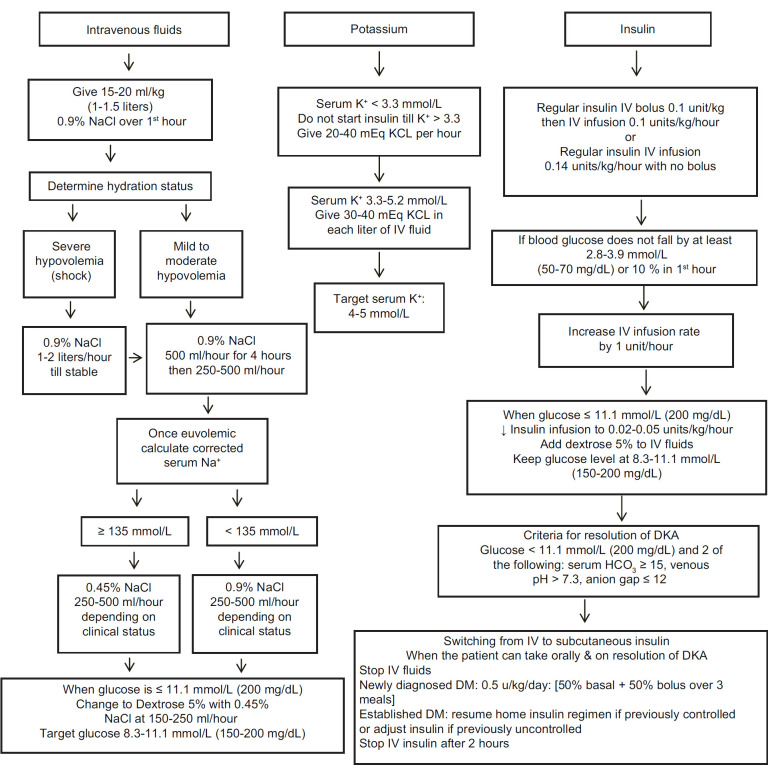
Management
The DKA/HHS bundle: fluids, insulin, potassium, identify trigger. 0.9% NS at 15–20 mL/kg/h for the first 1–2 hours, then transition to 0.45% NS. Regular insulin IV drip at 0.1 units/kg/h after potassium is confirmed > 3.3. Add dextrose to the fluids once glucose < 200–250 to continue insulin until the anion gap closes. Replace potassium aggressively — total body K is depleted even if the serum level looks normal. Trigger workup: infection, missed insulin, MI, pancreatitis, medications (steroids, SGLT2i — think euglycemic DKA).
Inpatient Glucose
Target glucose 140–180 mg/dL for most inpatients per the ADA Standards of Care (Inpatient Hyperglycemia). Use basal-bolus insulin regimens, not sliding scale alone, for persistent hyperglycemia. Hold oral agents on admission for most patients. Document A1C on admission for every diabetic or hyperglycemic patient.
Every DKA note must have the three lab trends: glucose, anion gap, and bicarbonate. The insulin drip keeps running until the anion gap closes, not when the glucose normalizes. If you only chart the glucose you will miss the whole story.
09 Gastrointestinal Bleeding (Upper & Lower) GI
Upper GIB (proximal to the ligament of Treitz): peptic ulcer disease, gastritis, esophagitis, variceal hemorrhage, Mallory-Weiss tear, Dieulafoy lesion, malignancy. Lower GIB: diverticulosis, angiodysplasia, colitis (ischemic, infectious, IBD), hemorrhoids, malignancy, post-polypectomy.
Presentation & Resuscitation
Hematemesis, coffee-ground emesis, melena, and hematochezia. Rapid hematochezia can be from a brisk upper source. Establish two large-bore IVs, type and cross, transfuse to a hemoglobin goal of 7 (9 in ACS), correct coagulopathy, reverse anticoagulants if needed, hold antihypertensives and diuretics, and consult GI.
Used to stratify upper GIB risk and identify patients safe for outpatient management (score 0). Incorporates BUN, hemoglobin (separate thresholds for men/women), SBP, pulse ≥ 100, melena, syncope, hepatic disease, and cardiac failure. A GBS of 0 has near-zero risk of intervention. Higher scores indicate need for inpatient care and earlier endoscopy. Reference: Blatchford et al., Lancet 2000.
Management — GI Bleed Bundle
Pantoprazole 80 mg IV bolus then 8 mg/h infusion (or 40 mg IV BID) for upper GIB. For suspected variceal bleed: octreotide 50 mcg IV bolus then 50 mcg/h infusion, ceftriaxone 1 g IV daily prophylaxis, urgent EGD. Reverse anticoagulation: vitamin K + 4-factor PCC for warfarin, andexanet or PCC for DOACs, idarucizumab for dabigatran. Reference: ACG 2021 upper GIB guideline.
10 Atrial Fibrillation with RVR & Inpatient Arrhythmias Cardiac
Atrial fibrillation is an irregularly irregular supraventricular arrhythmia without discrete P waves. “RVR” means rapid ventricular response (HR typically > 110). Triggers in the hospital include sepsis, hypovolemia, anemia, pain, withdrawal, hypoxia, PE, thyrotoxicosis, electrolyte derangement, and post-op stress.
Management
First decide stable vs unstable. Unstable (hypotension, chest pain, pulmonary edema, altered mental status) → synchronized cardioversion. Stable → rate control: metoprolol 5 mg IV q5 min × 3, then PO; or diltiazem 0.25 mg/kg IV bolus (avoid in HFrEF), then drip 5–15 mg/h. Amiodarone for rate control in critically ill patients or those who cannot tolerate beta-blockers. Address triggers.
Anticoagulation
Stroke risk estimation uses CHA2DS2-VASc: CHF (1), HTN (1), Age ≥ 75 (2), Diabetes (1), Stroke/TIA/TE (2), Vascular disease (1), Age 65–74 (1), Sex category female (1). Anticoagulate for score ≥ 2 in men, ≥ 3 in women. DOACs (apixaban, rivaroxaban, dabigatran, edoxaban) are first-line except in moderate-to-severe mitral stenosis or mechanical valves, where warfarin is required. Reference: 2023 ACC/AHA AF Guideline.
11 Syncope & Inpatient Falls Neuro/Geri
Syncope is transient loss of consciousness from global cerebral hypoperfusion. Categories: reflex (vasovagal, situational, carotid sinus), orthostatic (volume depletion, meds, autonomic), and cardiac (arrhythmia, structural, outflow obstruction, PE). Cardiac syncope carries the worst prognosis and must be ruled out.
Workup
Orthostatic vitals, EKG, telemetry, CBC/BMP/troponin, BNP, pregnancy test in women of childbearing age, echo when structural disease is suspected, and carotid ultrasound/CT head only when focal neuro findings or trauma are present. Syncope is rarely stroke.
Inpatient Falls
Document fall circumstances: witnessed vs unwitnessed, mechanism, pre-fall symptoms (dizzy, chest pain, palpitations, LOC), injuries sustained, any change in exam, post-fall vitals, anticoagulant status, head CT if on anticoagulants or altered. File an institutional event report.
Two validated tools used in the ED to risk-stratify syncope. The SFSR mnemonic is CHESS: CHF history, Hematocrit < 30, EKG abnormal, Shortness of breath, SBP < 90 at triage — any positive suggests higher risk of serious outcome at 30 days. The Canadian Syncope Risk Score adds finer gradations and is increasingly used to decide who can go home from the ED versus who needs admission and telemetry.
12 Cellulitis, SSTI & Bone/Joint Infection Infectious
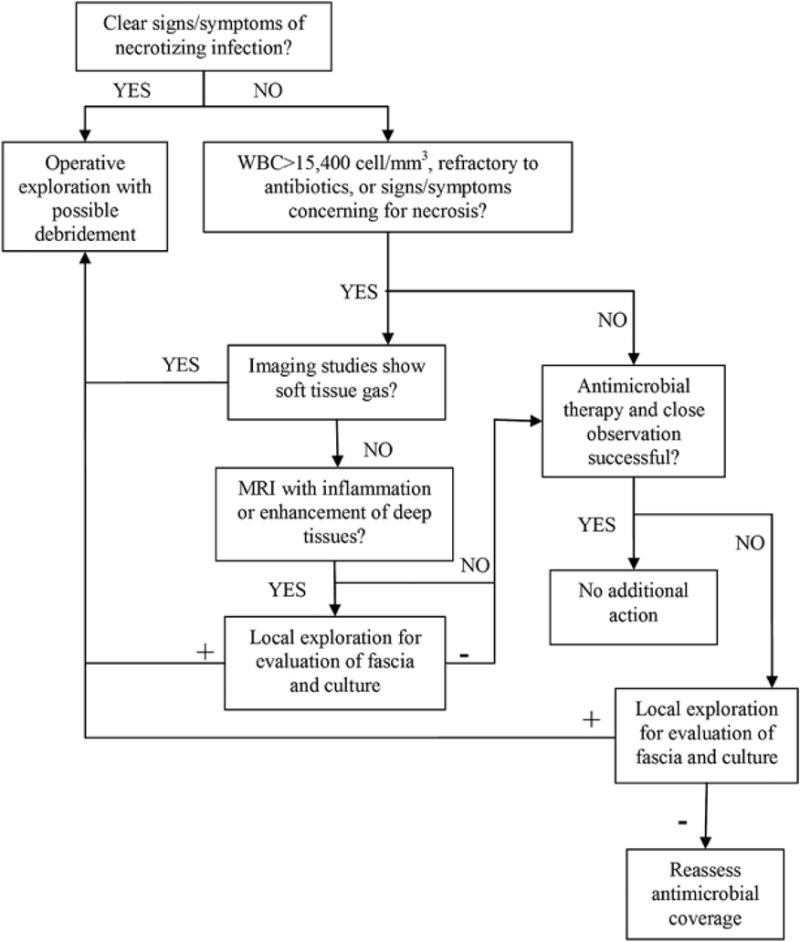
Cellulitis is a non-purulent skin and soft tissue infection usually caused by beta-hemolytic streptococci. Purulent SSTI (abscess, furuncle, carbuncle) is most often Staphylococcus aureus, including MRSA. Always consider necrotizing fasciitis as a red-flag diagnosis — pain out of proportion, crepitus, rapid progression, systemic toxicity → emergent surgical consult.
Management
Non-purulent cellulitis: cefazolin 1–2 g IV q8h or ceftriaxone 1 g IV daily; step down to cephalexin 500 mg PO QID. Purulent: I&D + MRSA coverage (vancomycin IV, or doxycycline/TMP-SMX/linezolid PO). Elevate the limb, mark the erythema border, reassess daily. Diabetic foot infection and osteomyelitis require longer courses, MRI for bone involvement, and ID/podiatry consults. Guideline: IDSA SSTI guideline 2014.
The LRINEC score (Laboratory Risk Indicator for Necrotizing Fasciitis) uses CRP, WBC, Hgb, Na, Cr, and glucose — a score ≥ 6 warrants strong suspicion and ≥ 8 is highly predictive. Clinically, pain out of proportion to exam, rapidly spreading erythema, crepitus, bullae, skin necrosis, or hemodynamic instability require emergent surgical consult. Do not wait for labs or imaging when the exam is alarming — delay is the primary predictor of mortality.
13 UTI & Pyelonephritis Infectious
Cystitis: dysuria, frequency, urgency, suprapubic pain. Pyelonephritis: adds flank pain, fever, rigors, nausea, vomiting. Most common pathogens: E. coli, Klebsiella, Proteus, Enterococcus. Catheter-associated UTI (CAUTI) is a hospital-acquired condition and is reported to CMS.
Management
Urinalysis + urine culture before antibiotics. Pyelonephritis: ceftriaxone 1 g IV daily, or cefepime/piperacillin-tazobactam if recent healthcare exposure. De-escalate on cultures. Duration 7 days for uncomplicated pyelonephritis with rapid response; 10–14 days for complicated. Remove unnecessary Foleys early — document indication daily.
Asymptomatic bacteriuria should not be treated in most patients (exceptions: pregnancy, pre-urologic procedures). Document the clinical reasoning when the team defers treatment — this is a Choosing Wisely quality metric.
14 Electrolyte Abnormalities Endocrine/Metabolic
The hospitalist manages electrolyte derangements all day. Know the thresholds and the replacement protocols.
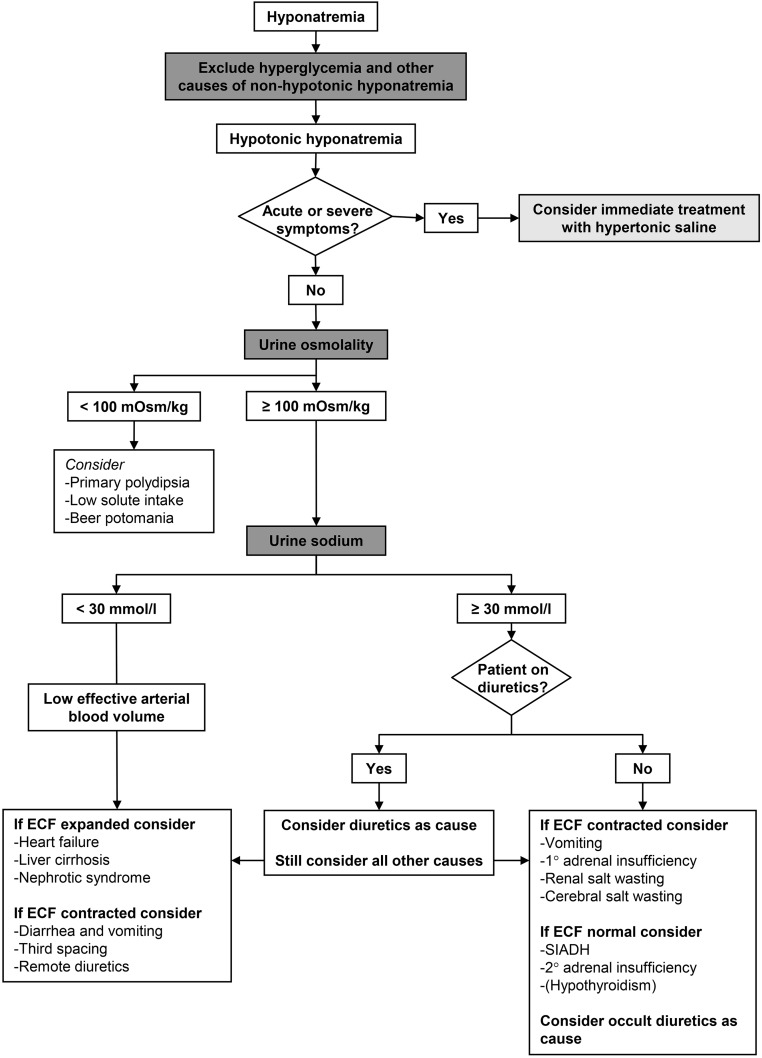
Hyponatremia: mild 130–135, moderate 125–129, severe < 125. Classify by volume status (hypo-, eu-, hypervolemic). Correct < 8–10 mEq/L/24h to avoid osmotic demyelination. Severe symptomatic: 3% saline 100 mL bolus × up to 3.
Hypernatremia: free water deficit, often elderly with poor access. Replace with D5W or PO water. Correct < 10–12 mEq/L/24h.
Hypokalemia: KCl 10 mEq PO raises K ~0.1. IV limits: 10 mEq/h peripheral, 20 mEq/h central. Always replete Mg first — hypomagnesemia causes refractory hypokalemia.
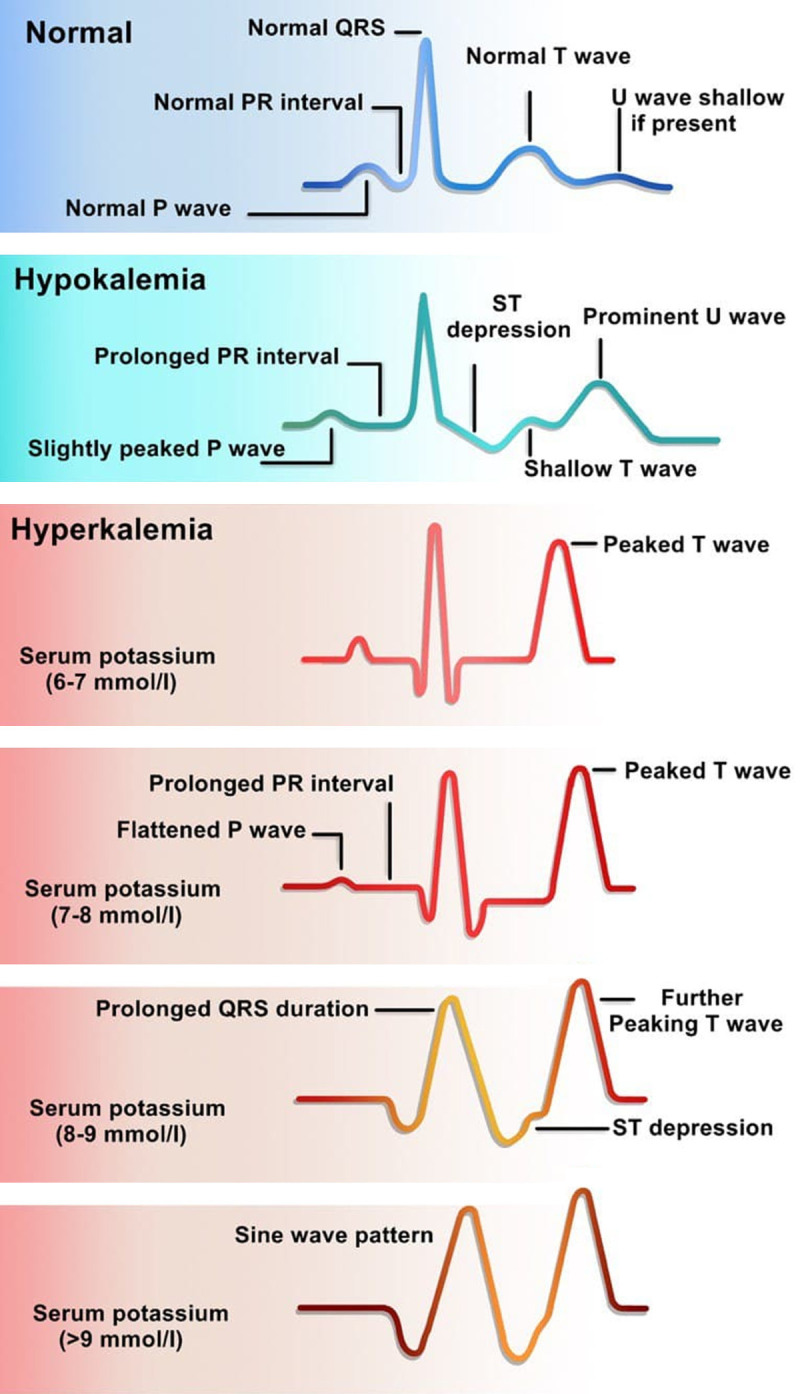
Hyperkalemia: EKG changes (peaked T, wide QRS, sine wave), stabilize myocardium (calcium gluconate), shift (insulin 10 units + D50, albuterol, bicarb if acidotic), remove (loop diuretic, kayexalate/patiromer/lokelma, dialysis).
Hypocalcemia: correct for albumin or use ionized Ca. Symptomatic: calcium gluconate 1–2 g IV.
Hypomagnesemia: 2–4 g MgSO4 IV. Hypophosphatemia: K- or Na-phos IV or PO, monitor calcium.
15 Encephalopathy & Altered Mental Status Neuro
Altered mental status is a symptom, not a diagnosis. The differential is vast: metabolic (hypoglycemia, hyponatremia, uremia, hepatic encephalopathy, hypercapnia), infectious (sepsis, meningitis, encephalitis, UTI in elderly), toxic (alcohol, drugs, meds, anticholinergics), neurologic (stroke, seizure, post-ictal state, ICH), hypoxic, and psychiatric.
Workup
Finger-stick glucose first. Then CBC, BMP, LFTs, ammonia (if cirrhotic), TSH, B12, UA, blood cultures if febrile, ABG for CO2, troponin/EKG, CT head non-contrast, and LP if meningitis is suspected. Medication review for anticholinergics, benzodiazepines, opioids. Screen for delirium with the CAM (Confusion Assessment Method).
Hepatic Encephalopathy
West Haven grades I (mild) to IV (coma). Treat with lactulose titrated to 2–3 soft bowel movements daily, add rifaximin 550 mg BID for recurrent cases, identify precipitants (GI bleed, infection, constipation, electrolyte derangement, meds).
16 Alcohol & Opioid Withdrawal Addiction
Alcohol withdrawal: autonomic hyperactivity, tremor, anxiety, nausea, insomnia, agitation, seizures (6–48h), hallucinosis (12–48h), delirium tremens (48–96h, mortality up to 5% untreated). Screen every admission with AUDIT-C.
Ten-item scale (0–67): nausea/vomiting, tremor, paroxysmal sweats, anxiety, agitation, tactile disturbances, auditory disturbances, visual disturbances, headache, orientation. Thresholds: < 10 mild, 10–18 moderate, ≥ 19 severe. Used to drive symptom-triggered benzodiazepine dosing (lorazepam, diazepam, chlordiazepoxide). Document CIWA scores in the note. Add thiamine 100 mg IV/IM/PO daily, folate, multivitamin, and magnesium.
Eleven-item scale (0–48): resting pulse, sweating, restlessness, pupil size, bone/joint aches, runny nose/tearing, GI upset, tremor, yawning, anxiety/irritability, gooseflesh skin. 5–12 mild, 13–24 moderate, 25–36 moderately severe, > 36 severe. Used to time buprenorphine induction (typically start at COWS ≥ 8–12 to avoid precipitated withdrawal).
Treat alcohol withdrawal with symptom-triggered benzodiazepines and supportive care; phenobarbital protocols exist at some centers for severe cases. Treat opioid withdrawal with buprenorphine/naloxone induction (preferred inpatient standard of care), or methadone (requires federal OTP for outpatient), with supportive care (clonidine, ondansetron, loperamide, NSAIDs).
Always document the last drink time and the peak daily drinks for alcohol use, and the last use time and typical dose for opioid use. These anchor the CIWA/COWS timeline and determine when dangerous withdrawal is likely to peak. Document that thiamine was given before any glucose-containing fluids to prevent Wernicke’s encephalopathy.
17 VTE — DVT and Pulmonary Embolism Vascular
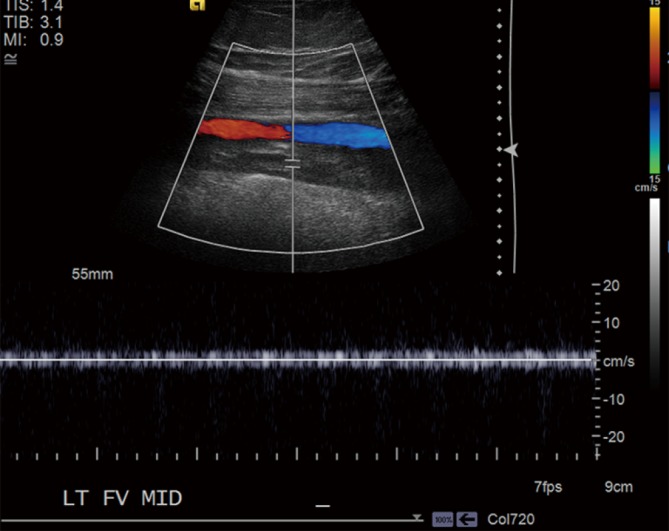
DVT is deep venous thrombosis, most commonly in the lower extremity (proximal: iliac, femoral, popliteal; distal: calf veins). PE is pulmonary embolism — thrombus in the pulmonary arterial tree, usually embolized from a lower-extremity DVT.
Clinical signs of DVT (3), PE most likely diagnosis (3), HR > 100 (1.5), immobilization/surgery in past 4 weeks (1.5), prior DVT/PE (1.5), hemoptysis (1), malignancy (1). ≤ 4 = PE unlikely (consider D-dimer); > 4 = PE likely (CT angiography). Age-adjusted D-dimer (age × 10 for age > 50) improves specificity.
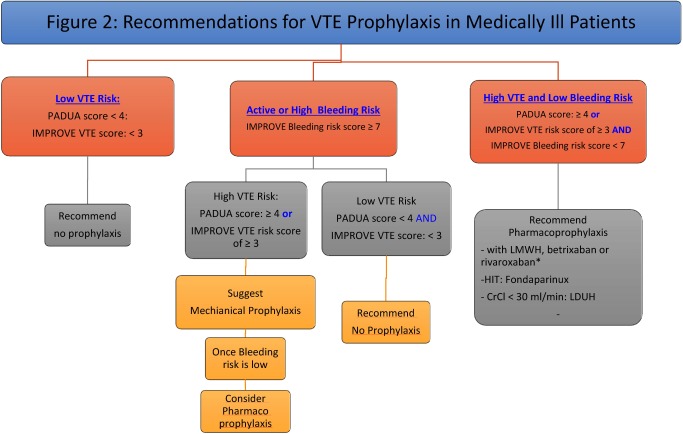
VTE Prophylaxis
Every admitted medical patient needs VTE risk assessment. The Padua Prediction Score (medical patients) and the Caprini Score (surgical patients) are the standard tools. Prophylactic options: enoxaparin 40 mg SC daily (30 mg BID in obesity or high-risk surgery), heparin 5000 units SC q8–12h (preferred in severe renal failure), mechanical prophylaxis (SCDs) when anticoagulation is contraindicated. The CHEST ACCP VTE prophylaxis guidelines are the standard citation.
VTE Treatment
Therapeutic anticoagulation: apixaban (10 mg BID × 7 days, then 5 mg BID) or rivaroxaban (15 mg BID × 21 days, then 20 mg daily) are preferred for most patients. LMWH bridge to warfarin remains the standard for pregnancy, active cancer (though DOACs are now acceptable in most cancers), severe renal failure, and mechanical valves. Massive PE (hemodynamic instability) warrants systemic thrombolytics or catheter-directed therapy; submassive PE is individualized. Reference: CHEST 2016 Antithrombotic Therapy for VTE.
18 Chest Pain Rule-Out & ACS on the Floor Cardiac
Chest pain on a hospitalist service is usually a rule-out. Know the can’t-miss differential: ACS, PE, aortic dissection, tension pneumothorax, esophageal rupture, pericardial tamponade.
Workup
EKG within 10 minutes, high-sensitivity troponin at presentation and 1–3 hours, chest X-ray, telemetry. The HEART score stratifies ED chest pain (History, EKG, Age, Risk factors, Troponin; 0–3 low, 4–6 intermediate, 7–10 high). For inpatient chest pain, troponin trending with serial EKGs and a cardiology phone call if there is any meaningful concern.
Management of NSTEMI / Unstable Angina
ASA 325 mg chewed, P2Y12 inhibitor (ticagrelor or clopidogrel) per cardiology, anticoagulation (heparin drip or enoxaparin), high-intensity statin, nitrates for pain, beta-blocker when hemodynamically appropriate, and cardiology consult for risk stratification (early invasive vs ischemia-guided). Reference: 2023 AHA/ACC Chronic Coronary Disease Guideline and 2014 AHA/ACC NSTE-ACS Guideline.
19 Rapid Response, Code Blue & Post-Op Complications Emergency
A rapid response is activated when a patient deteriorates acutely — meeting institutional triggers such as HR > 130, SBP < 90, RR > 28, SpO2 < 90, new altered mental status, or nursing concern. A code blue is activated for cardiopulmonary arrest.
Time of arrest recognition, witnessed/unwitnessed, initial rhythm, time CPR started, time of each epinephrine dose, defibrillation attempts and energies, airway management (bag-mask, LMA, ETT), medications given with doses and times, ROSC time or time of death, code leader, family notification. This becomes a defended legal document — precision matters.
NEWS2 (National Early Warning Score 2)
An aggregate early-warning score used on medical wards to flag deteriorating patients: respiratory rate, SpO2, supplemental O2, systolic BP, pulse, level of consciousness, and temperature. Score ≥ 5 typically triggers urgent clinical review, ≥ 7 a full rapid response. Reference: RCP NEWS2.
Post-Op Complications on the Medicine Service
Hospitalists routinely co-manage post-op patients. Watch for fever workup (atelectasis, pneumonia, UTI, SSI, DVT/PE, drug, C. difficile), post-op AKI, ileus, delirium, MI (type 2 from demand ischemia), and bleeding. Document POD number (post-op day), procedure, and surgeon of record on every note.
Wind (atelectasis/pneumonia, POD 1–2), Water (UTI, often from Foley, POD 3–5), Walking (DVT/PE, POD 4–6), Wound (SSI, POD 5–7), Wonder drugs (drug fever, C. difficile, transfusion reaction, any POD). Use this to organize the differential when charting a post-op fever assessment.
20 Perioperative Medicine & Palliative Care Consults Periop/Pall
Cardiac Risk Assessment
The Revised Cardiac Risk Index (RCRI) and newer NSQIP MICA or Gupta calculators estimate perioperative cardiac risk. RCRI components: high-risk surgery, ischemic heart disease, CHF, cerebrovascular disease, insulin-dependent diabetes, creatinine > 2.0. Reference: 2024 ACC/AHA Perioperative Cardiovascular Management Guideline.
Antithrombotic Management
For warfarin, INR goal < 1.5 before most surgery; bridge with LMWH only in high-thrombotic-risk patients (mechanical mitral valve, recent VTE, high-risk AF). DOACs: hold 2–3 days before low-bleed-risk and 3–5 days before high-bleed-risk procedures, adjusted for renal function. Aspirin: continue for most cardiac patients; hold for high-bleeding-risk surgery. Reference: ACC Periop Antithrombotic Expert Consensus.
Palliative Care & Goals of Care
Hospitalists run family meetings. Document attendees, substitute decision-maker, clinical update given, prognosis discussed, patient/family values, and the goals-of-care decision (full code, DNR/DNI, comfort measures only, hospice referral). Know the Medicare hospice eligibility criteria (prognosis ≤ 6 months if the disease follows its expected course). Symptom management at end of life: morphine for dyspnea/pain, haloperidol for agitation/delirium, glycopyrrolate for secretions, lorazepam for anxiety.

21 Bedside Procedures on the Floor Procedures
| Procedure | Indication | Key Documentation |
|---|---|---|
| Lumbar puncture | Meningitis workup, idiopathic intracranial hypertension, CSF analysis | Consent, landmarks (L3/4 or L4/5), opening pressure, fluid appearance, tube collection, complications (post-LP headache) |
| Paracentesis | New ascites workup, tense ascites, SBP rule-out | LUQ or RLQ site, ultrasound guidance, volume removed, albumin (25% 6–8 g/L removed > 5 L), cell count/SAAG/culture results |
| Thoracentesis | Symptomatic pleural effusion, diagnostic workup | Side, ultrasound, volume removed (< 1.5 L to avoid re-expansion edema), Light’s criteria (LDH, protein), post-procedure CXR |
| Central line (IJ, SC, femoral) | Vasopressors, poor peripheral access, hemodialysis (temporary) | Site, ultrasound guidance, wire technique, number of attempts, line tip confirmation on CXR (IJ/SC), sterile barrier/CHG |
| Arterial line | Continuous BP monitoring, frequent ABGs | Site (radial, femoral), Allen test if radial, sterile technique, waveform quality |
| Intubation (usually by anesthesia/ICU) | Respiratory failure, airway protection, hemodynamic collapse | Indication, RSI meds (etomidate/ketamine + rocuronium/succinylcholine), Mallampati/Cormack-Lehane, ETT size, depth, CO2 confirmation, post-intubation CXR |
| NG tube | Bowel obstruction decompression, enteral access | Indication, size, depth, placement confirmation (CXR or pH), output volume/character |
| Advance care planning | Goals-of-care clarification, code status documentation | Attendees, decision-maker, discussion content, resulting code status, time spent (billable as ACP) |
22 Labs, Imaging & Telemetry on the Wards Diagnostics
Labs — Daily Bread
CBC: WBC (differential matters — bandemia suggests acute infection), hemoglobin/hematocrit, platelets. BMP: Na, K, Cl, CO2, BUN, Cr, glucose. Calculate anion gap (Na − Cl − HCO3; normal 8–12). CMP adds LFTs and albumin. Coags: PT/INR, PTT, fibrinogen. Cardiac: troponin, BNP/NT-proBNP. Inflammatory: CRP, ESR, procalcitonin, lactate. Infection: blood cultures, urine culture, sputum culture, C. difficile PCR, respiratory viral panel, MRSA nasal PCR.
Imaging
Chest X-ray: pneumonia, pulmonary edema, pneumothorax, line/tube placement. CT chest: PE (with contrast), pneumonia complications, masses. CT abdomen/pelvis: obstruction, abscess, ischemia, bleeding. CT head: stroke, bleed, trauma. US abdomen: gallbladder, kidneys, ascites. MRI: osteomyelitis, epidural abscess, cord compression, stroke.
Telemetry & EKG
Document rhythm daily: normal sinus, sinus tach, sinus brady, AF, Aflutter, SVT, PVCs, frequency of ectopy, any pauses, any events. Learn the classic EKG patterns: STEMI (ST elevation in contiguous leads), NSTEMI (ST depression, T-wave inversion), pericarditis (diffuse ST elevation with PR depression), hyperkalemia (peaked T), LVH, bundle branch blocks.
Know the numbers that trigger a phone call from the lab: Na < 120 or > 160, K < 2.8 or > 6.0, glucose < 50 or > 500, Ca < 6.5 or > 13, Mg < 1.0, Hgb < 7, platelets < 50, INR > 5, troponin positive, lactate > 4, positive blood culture, critical imaging findings. When the team is called with a critical value, chart the time, the value, the acknowledging provider, and the response.
23 Inpatient Medications You Must Know Medications
| Drug | Typical Dose | Use Case |
|---|---|---|
| Ceftriaxone | 1–2 g IV q24h | CAP, UTI/pyelo, meningitis (2 g q12h), SBP |
| Cefepime | 1–2 g IV q8–12h | Pseudomonal coverage, HAP, febrile neutropenia |
| Piperacillin-tazobactam (Zosyn) | 3.375–4.5 g IV q6–8h | Broad-spectrum with anaerobes |
| Meropenem | 1 g IV q8h | ESBL, severe HAP, complicated intra-abdominal |
| Vancomycin | 15–20 mg/kg IV q8–12h, trough/AUC-guided | MRSA, empiric gram-positive coverage |
| Linezolid | 600 mg IV/PO q12h | MRSA (bacteremia limitation), VRE |
| Daptomycin | 6–10 mg/kg IV q24h | MRSA bacteremia (not pneumonia) |
| Metronidazole | 500 mg IV/PO q8h | Anaerobes, C. difficile (oral vanco preferred now) |
| Azithromycin | 500 mg IV/PO q24h | Atypical coverage in CAP |
| Levofloxacin | 750 mg IV/PO q24h | Respiratory FQ for CAP, complicated UTI |
| Ampicillin-sulbactam | 3 g IV q6h | Aspiration pneumonia, SSTI, bite wounds |
| Oral vancomycin | 125 mg PO QID | C. difficile |
| Fidaxomicin | 200 mg PO BID | C. difficile, lower recurrence |
Unfractionated heparin: weight-based nomogram, goal PTT or anti-Xa. Reversible with protamine. First-line for renal failure, suspected HIT workup pending.
Enoxaparin (LMWH): 1 mg/kg SC BID (treatment) or 40 mg SC daily (prophylaxis). Renal dose-adjust below CrCl 30.
Apixaban: 10 mg BID × 7 d then 5 mg BID (VTE); 5 mg BID (AF, dose-adjust to 2.5 mg BID for 2 of 3: age ≥ 80, weight ≤ 60 kg, Cr ≥ 1.5).
Rivaroxaban: 15 mg BID × 21 d then 20 mg daily (VTE); 20 mg daily with food (AF).
Dabigatran: 150 mg BID (reversal with idarucizumab).
Warfarin: goal INR 2–3 (most indications), 2.5–3.5 for mechanical mitral valves. Bridge with LMWH during initiation or perioperative in high-risk patients.
Reversal: vitamin K + 4F-PCC (warfarin); andexanet alfa or 4F-PCC (apixaban/rivaroxaban); idarucizumab (dabigatran); protamine (heparin/LMWH partial).
Basal: glargine (Lantus, Basaglar, Toujeo), detemir (Levemir), degludec (Tresiba), NPH.
Prandial / bolus: aspart (Novolog), lispro (Humalog), glulisine (Apidra), regular insulin.
IV drip: regular insulin, typically 0.1 units/kg/h for DKA/HHS; ICU hyperglycemia protocols.
Inpatient rules: hold oral agents (metformin, SGLT2i, sulfonylureas) on admission for most patients, target 140–180 mg/dL, transition to home regimen 24–48 hours before discharge when stable.
Norepinephrine: first-line vasopressor for septic and most undifferentiated shock.
Vasopressin: 0.03–0.04 units/min, adjunct in septic shock.
Epinephrine: second-line in septic shock, first-line in anaphylaxis and cardiac arrest.
Phenylephrine: pure alpha, bolus or drip, useful when tachycardia is a problem.
Dopamine: rarely used now given arrhythmia risk.
Dobutamine / Milrinone: inotropes for cardiogenic shock and bridge decompensated HF.
Antiarrhythmics: amiodarone (150 mg IV load then 1 mg/min × 6h then 0.5 mg/min), diltiazem drip, metoprolol IV.
GI prophylaxis: pantoprazole 40 mg IV/PO daily, famotidine 20 mg BID.
Steroids: hydrocortisone 50–100 mg IV q6–8h (stress dose, shock), methylprednisolone 40–125 mg IV (asthma/COPD), dexamethasone 4–10 mg IV (antiemetic, neuro).
Diuretics: furosemide (Lasix), bumetanide (Bumex), torsemide (Demadex), metolazone, chlorothiazide.
Electrolyte replacement: KCl 10–40 mEq PO/IV, MgSO4 2–4 g IV, K-phos/Na-phos IV, calcium gluconate 1–2 g IV.
Analgesics: acetaminophen 650–1000 mg q6h (max 3–4 g/day), ketorolac 15–30 mg IV (caution in AKI/elderly), morphine 2–4 mg IV q4h, hydromorphone 0.2–0.5 mg IV q4h, oxycodone 5–10 mg PO q4h.
24 Classification & Risk Scores Reference
Hospitalists live inside risk scores. Every one listed below should be familiar enough that you can capture the components when the clinician references them.
20 variables across demographics, comorbidities, exam, and labs. Classes I (lowest risk, outpatient) through V (highest risk, ICU). More granular than CURB-65 and often used to justify discharge disposition.
Active cancer (3), prior VTE (3), reduced mobility (3), thrombophilia (3), trauma/surgery < 1 mo (2), age ≥ 70 (1), HF or resp failure (1), MI/stroke (1), acute infection/rheum (1), obesity BMI ≥ 30 (1), hormone therapy (1). ≥ 4 = high risk → pharmacologic prophylaxis.
Multi-factor surgical risk tool. 0 very low, 1–2 low, 3–4 moderate, ≥ 5 high. Drives choice and duration of perioperative prophylaxis.
Weighted index of 17 comorbidities predicting 10-year mortality. Used for risk adjustment and research — not a bedside clinical tool, but you will see it in discharge summaries and registries.
Three questions (frequency, typical drinks, heavy-drinking episodes). Score range 0–12. Positive: ≥ 4 men, ≥ 3 women → further assessment for alcohol use disorder.
Additional scores referenced throughout the guide: CURB-65 (CAP severity, Section 3), qSOFA/SOFA (sepsis, Section 6), KDIGO (AKI, Section 7), Glasgow-Blatchford (GIB, Section 9), CHA2DS2-VASc (AF stroke, Section 10), Wells (PE, Section 17), HEART (chest pain, Section 18), RCRI (perioperative cardiac, Section 20), NEWS2 (deterioration, Section 19), CIWA-Ar (alcohol withdrawal, Section 16), COWS (opioid withdrawal, Section 16).
25 Physical Exam & Abbreviations Reference
The Hospitalist Exam — Head to Toe
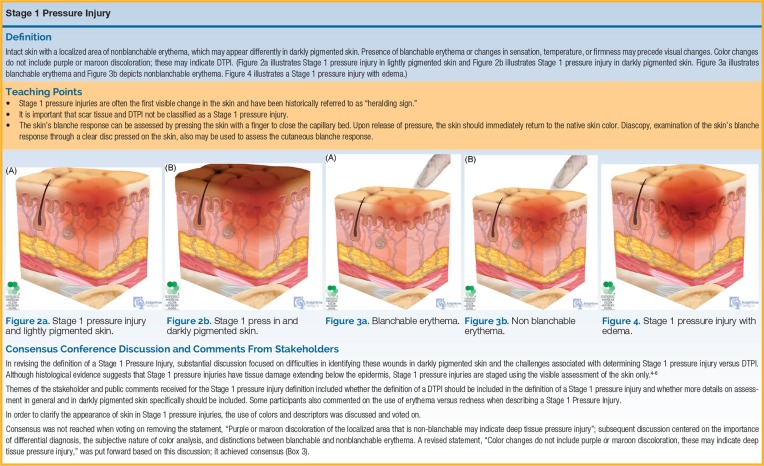
General: alert, oriented, NAD vs ill-appearing, body habitus. HEENT: PERRL, EOMI, conjunctivae, oropharynx (moist, erythema, thrush), JVP (measured in cm above sternal angle). Neck: supple, lymphadenopathy, thyromegaly, bruits. Cardiac: rate, rhythm, S1/S2, murmurs (grade, location, radiation), rubs, gallops (S3/S4). Pulmonary: respiratory effort, auscultation by lobe (clear, crackles, wheezes, rhonchi, decreased breath sounds), dullness to percussion, egophony. Abdomen: bowel sounds, soft/distended, tenderness, guarding, rebound, organomegaly, ascites, bruits. Extremities: pulses (radial, DP, PT), edema (1–4+), calf tenderness, capillary refill, temperature. Skin: color, turgor, rashes, wounds, pressure injuries. Neurologic: alert/oriented, cranial nerves II–XII, motor (strength 0–5), sensation, reflexes (0–4+), gait, coordination, NIH stroke scale if applicable. Psychiatric: mood, affect, thought process, suicidal/homicidal ideation.
Abbreviations Master List
ADL — activities of daily living
ADHF — acute decompensated heart failure
AECOPD — acute exacerbation of COPD
AKI — acute kidney injury
AMS — altered mental status
A&O x 3/4 — alert and oriented
BMP / CMP — basic / comprehensive metabolic panel
BNP — B-type natriuretic peptide
C. diff — Clostridioides difficile
CAP / HAP / VAP — community / hospital / ventilator-associated pneumonia
CBC — complete blood count
CHF — congestive heart failure
CIWA — Clinical Institute Withdrawal Assessment
COWS — Clinical Opiate Withdrawal Scale
COPD — chronic obstructive pulmonary disease
Cr / eGFR — creatinine / estimated glomerular filtration rate
CTA — CT angiography
DKA / HHS — diabetic ketoacidosis / hyperosmolar hyperglycemic state
DNR / DNI — do not resuscitate / do not intubate
DVT / PE — deep vein thrombosis / pulmonary embolism
EF — ejection fraction
EGD — esophagogastroduodenoscopy
ETT — endotracheal tube
FEN — fluids, electrolytes, nutrition
GCS — Glasgow Coma Scale
GIB — gastrointestinal bleed
H&P — history & physical
HFrEF / HFpEF — heart failure with reduced / preserved EF
HFNC — high-flow nasal cannula
I/O — intake/output
ICU — intensive care unit
JVD — jugular venous distension
LOS — length of stay
LP — lumbar puncture
MAP — mean arterial pressure
MDI — metered-dose inhaler
MRSA / MSSA — methicillin-resistant/sensitive S. aureus
NC — nasal cannula
NG / OG — nasogastric / orogastric
NIV / BiPAP / CPAP — non-invasive ventilation
NPO — nothing by mouth
NSTEMI / STEMI — non-ST-elevation / ST-elevation MI
POD — post-operative day
PRBC / FFP — packed red blood cells / fresh frozen plasma
RRT — renal replacement therapy or rapid response team
ROSC — return of spontaneous circulation
SBP — systolic blood pressure or spontaneous bacterial peritonitis
SCD — sequential compression device
SIRS — systemic inflammatory response syndrome
SNF — skilled nursing facility
SSI — surgical site infection
TTE / TEE — transthoracic / transesophageal echo
UA / UCx — urinalysis / urine culture
VTE — venous thromboembolism
WBC — white blood cell count
26 Sample HPIs & Hospital Course Templates Templates
These templates show the rhythm of real hospitalist documentation. Use them as frameworks when you are building a note in real time.
“Mrs. [Name] is a 78-year-old female with a history of hypertension, type 2 diabetes (A1C 8.1), stage 3 CKD (baseline Cr 1.5), and recurrent UTIs presenting from her assisted living facility with 2 days of progressive confusion, dysuria, and low back pain. Per family, she was at baseline 48 hours ago. This morning she was found diaphoretic and minimally responsive. EMS vitals: T 39.1, HR 118, BP 88/50, RR 24, SpO2 94% RA. In the ED she received 2 L LR, ceftriaxone 1 g IV, and blood/urine cultures. UA showed large leukocyte esterase, positive nitrites, > 100 WBC/hpf. Lactate 3.4 (down to 2.1 after fluids). Creatinine 2.3 (up from 1.5). She is being admitted for sepsis, suspected urinary source, with AKI and delirium.”
“Mr. [Name] is a 66-year-old male with severe COPD (GOLD group E, FEV1 38% predicted, on 2 L home O2), HFpEF, and 60-pack-year smoking history (active) presenting with 4 days of progressive dyspnea, increased sputum production (yellow), and wheezing following a household cold. He has required 4 L NC to maintain saturations in the high 80s at home. Denies chest pain, fever, hemoptysis, or leg swelling. In the ED he received continuous albuterol/ipratropium nebulizers, methylprednisolone 125 mg IV, azithromycin 500 mg IV, and was placed on BiPAP 10/5 for hypercapnia (pH 7.30, pCO2 62). Chest X-ray without focal consolidation. He is being admitted for acute COPD exacerbation.”
“Mr. [Name] is a 72-year-old male with stage 3b CKD (baseline Cr 1.9), HTN, HFrEF (EF 35%), and type 2 diabetes presenting with 3 days of decreased urine output, fatigue, and lower extremity swelling. He was recently started on lisinopril 20 mg daily and had his furosemide increased from 40 mg to 80 mg BID by his PCP. He has had poor PO intake. ED vitals stable. Labs: Cr 3.8 (from 1.9), K 5.9, BUN 72, HCO3 19. UA bland. Renal US pending. He is being admitted for AKI on CKD, likely multifactorial (ACEi, diuretic over-diuresis, poor PO intake); lisinopril held, furosemide held pending volume assessment, kayexalate given for hyperkalemia.”
“Mr. [Name] is a 58-year-old male with alcohol use disorder (active, ~1 pint vodka/day), cirrhosis (Child-Pugh B), known esophageal varices on prior EGD, and NSAID use presenting with hematemesis × 3 episodes and melena beginning this morning. In the ED: HR 112, BP 96/58, Hgb 6.8 (baseline 11), platelets 78, INR 1.9. He has received 2 units PRBCs, 2 units FFP, pantoprazole 80 mg IV bolus and 8 mg/h drip, octreotide 50 mcg IV bolus and drip, ceftriaxone 1 g IV, and IV PPIs. GI consulted for urgent EGD. He is being admitted to the ICU for upper GIB with hemodynamic instability, likely variceal source.”
“Ms. [Name] is an 81-year-old female with AF on apixaban, HTN, and aortic stenosis (moderate on last echo) presenting after a witnessed syncopal episode at home. She was walking from the kitchen when she abruptly lost consciousness, fell, and struck her head. Family reports no seizure activity; she was out < 30 seconds and woke spontaneously. No prodrome, no chest pain, no palpitations beforehand. In the ED: HR 62, BP 108/62, orthostatic with a 22-point drop; EKG NSR no acute changes; troponin negative × 1; CT head without acute findings; telemetry in place. She is being admitted for syncope workup, telemetry monitoring, and fall evaluation.”
“76-year-old male admitted for community-acquired pneumonia (CURB-65 of 3) on HD1, started on ceftriaxone/azithromycin. Blood cultures no growth. Legionella and pneumococcal urinary antigens negative. Influenza and COVID PCR negative. Oxygen requirement weaned from 4 L NC on admission to room air by HD3. Complicated by new-onset AF with RVR on HD2, rate controlled with IV metoprolol transitioned to PO; CHA2DS2-VASc of 4 — started on apixaban 5 mg BID after discussion with cardiology. Discharged on HD5 with a prescription for cefpodoxime to complete a 7-day total antibiotic course, apixaban for new AF, and outpatient follow-up with PCP in 1 week and cardiology in 2 weeks.”
The best hospital medicine scribes think in problems. When the hospitalist says “this is CAP with CURB-65 of 3 and new AF,” a great scribe has already started two A&P problems, anticipated the CHA2DS2-VASc calculation, and staged the pneumonia workup in their head. When the patient goes into rapid response, a great scribe captures every vital, every medication, and every time-stamped decision so the event note is legally sound.
Be an active listener. Learn your hospitalist’s rhythm for rounding and problem lists. Read the overnight notes, new labs, and imaging before rounds so you can pre-populate the progress notes. Know the medications by generic and brand. Anticipate the plan based on the diagnosis. Keep a running list of pending results. Never let discharge medication reconciliation slip.
Welcome to hospital medicine. The breadth is enormous, the pace is real, and the satisfaction of safely moving a patient from ED to discharge is what the job is all about.
27 References & Sources
Clinical Practice Guidelines
GOLD 2024 Global Strategy for the Diagnosis, Management, and Prevention of COPD.
Kahn SR et al. Prevention of VTE in Nonsurgical Patients: CHEST Antithrombotic Therapy. Chest. 2012.
Kearon C et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline. Chest. 2016.
Society of Hospital Medicine — Clinical Guidelines & Position Statements.
Risk Scores & Tools
Royal College of Physicians. National Early Warning Score (NEWS) 2. 2017.
Barbar S et al. Padua Prediction Score for Hospitalized Medical Patients. J Thromb Haemost. 2010.
Diagram & Figure Sources
Figure 1: Cardiac Conduction System. OpenStax College via Wikimedia Commons. CC BY 3.0.
Figure 2: Major Respiratory Organs. OpenStax College via Wikimedia Commons. CC BY 3.0.