Internal Medicine
Every diagnosis, workup, procedure, medication, score, and documentation framework you need to survive inpatient and outpatient adult medicine from day one.
All diagrams on this page are sourced from published educational or institutional materials rather than AI generation. Each figure caption links to its original source, and the full diagram and guideline citations are collected in the references section at the bottom.
01 Organ Systems — Physiology Essentials
Internal medicine is the specialty of adult general medicine. Internists diagnose and manage every non-surgical adult condition, from an outpatient with newly discovered hypertension to a critically ill septic patient in the ICU. As a scribe, you will rotate across outpatient primary care, inpatient hospital medicine (sometimes called hospitalist service), and occasionally the MICU or subspecialty clinics. To document intelligently, you need working knowledge of the major organ systems the internist touches every day.
The Cardiovascular System
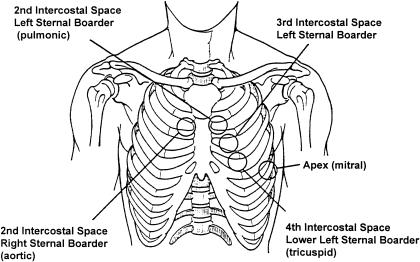
The heart has four chambers — two atria and two ventricles — and four valves: tricuspid, pulmonic, mitral, and aortic. Deoxygenated blood returns through the vena cavae to the right atrium, crosses the tricuspid valve to the right ventricle, and is pumped through the pulmonic valve to the pulmonary arteries. Oxygenated blood returns via the pulmonary veins to the left atrium, crosses the mitral valve to the left ventricle, and is ejected through the aortic valve to the systemic circulation. The coronary arteries (LAD, LCx, RCA) perfuse the myocardium during diastole. The conduction system runs from the SA node in the right atrium through the AV node, bundle of His, and left/right bundle branches to the Purkinje fibers.
The Respiratory System
Air enters through the upper airway (nose, pharynx, larynx), descends through the trachea, bifurcates at the carina into mainstem bronchi, and travels through progressively smaller bronchioles to the alveoli where gas exchange occurs. The A–a gradient (alveolar-arterial oxygen difference) helps distinguish hypoxemia due to V/Q mismatch or shunt (elevated gradient) from hypoventilation (normal gradient). Know that oxygen delivery depends on hemoglobin, oxygen saturation, and cardiac output — not just PaO2.
The Gastrointestinal & Hepatobiliary System
The GI tract runs continuously from esophagus to rectum. The liver is the metabolic factory — it synthesizes albumin and clotting factors, conjugates bilirubin, metabolizes drugs, and processes nutrients via the portal vein. The gallbladder stores bile; the pancreas produces digestive enzymes (exocrine) and insulin/glucagon (endocrine). Portal hypertension from cirrhosis drives varices, ascites, and hepatic encephalopathy.
The Renal System
Each kidney contains roughly one million nephrons. Filtration begins at the glomerulus; the tubules then reabsorb sodium, water, potassium, bicarbonate, and glucose, and secrete hydrogen ions and drugs. The kidney regulates volume, electrolytes, acid-base status, blood pressure (renin-angiotensin-aldosterone axis), and erythropoiesis (erythropoietin). eGFR — estimated glomerular filtration rate — is the key functional number.
The Nervous System
The brain has cortical lobes (frontal, parietal, temporal, occipital), the cerebellum, brainstem (midbrain, pons, medulla), and deep structures (basal ganglia, thalamus, hippocampus). The internist sees neurologic problems constantly: stroke, delirium, seizures, neuropathy, dementia. Scribes should recognize common territories — MCA (contralateral face/arm weakness, aphasia if dominant), ACA (contralateral leg weakness), PCA (visual field cuts), and posterior circulation (vertigo, ataxia, cranial nerve deficits).
Internal medicine is the most documentation-heavy adult specialty. On a busy hospitalist service you may chart 15–20 patients in a single shift, each with a problem list of 5–15 active issues. Build templated mental frameworks early: every admission needs a one-liner, active problem list, pertinent PMH, home meds reconciliation, and a problem-based assessment and plan.
02 Scribe Documentation Framework
The Problem-Based Note
Unlike surgical SOAP notes organized around a single diagnosis, internal medicine notes are problem-oriented. The assessment and plan is written as a numbered list of active problems, each with a brief assessment sentence and a bulleted plan. A typical hospitalist progress note has an Interval History, Vitals, I/Os, PE, Labs, Imaging/Studies, and an A/P organized by problem.
Chief Complaint: Single phrase ("chest pain," "shortness of breath," "altered mental status").
HPI: Full narrative OLDCARTS story, pertinent positives and negatives, prior workup, what brought them in today. In IM you almost always include prior cardiac/pulmonary/renal history relevant to the complaint.
ROS: At least 10 systems for a comprehensive admission; focused ROS for follow-up visits.
PMH/PSH/FH/SH: Full problem list, surgeries, family history of early CAD/cancer, tobacco/alcohol/drug use, living situation, code status.
Medications & Allergies: Full home med reconciliation with doses and frequencies.
Exam & Data: Vitals, full PE, labs, imaging, EKG.
Assessment & Plan: One-liner summary, then problem-based plan.
Every IM note starts with a one-sentence summary: "Mr. Smith is a 68-year-old male with a PMH of HFrEF (EF 30%), type 2 DM, CKD stage 3, and HTN who presents with 3 days of progressive dyspnea and lower extremity edema." This is the single most read sentence in any IM note — the attending, consultants, and overnight team all start here.
S: Patient's subjective update overnight — symptom changes, sleep, pain, appetite.
O: Vitals (ranges and most recent), I/Os, weight, focused exam, new labs, new studies.
A/P: Problem list updated from yesterday. Each problem gets a brief interval assessment and updated plan: what improved, what is pending, what changed. Problems are typically ordered by acuity and relevance.
Standard closing items: DVT prophylaxis, GI prophylaxis (if indicated), diet, code status, disposition, dispo barriers.
Outpatient IM Notes
Clinic notes are shorter and more focused. A follow-up for diabetes might include a brief interval history, home glucose log review, current medications, A1C and metabolic panel, a focused exam (feet, cardiovascular), and an updated plan for each chronic problem. The 2021 E/M coding changes eliminated the old element-counting system for office visits — levels are now determined by medical decision-making complexity or total time spent on the encounter day.
In IM, the problem list is sacred. Every active issue must appear in the A/P every single day — chronic stable problems still get a one-line "continue home regimen." Never silently drop a problem; if it resolves, say "resolved" explicitly. Billing, handoffs, and quality metrics all depend on a complete problem list.
03 Chest Pain Workup Cardiovascular
Chest pain is the single most common presenting complaint that triggers an IM admission or ED evaluation. The job of the internist is to risk-stratify the patient along two questions: is this acute coronary syndrome (ACS), and if not, what else life-threatening could this be (PE, aortic dissection, tension pneumothorax, esophageal rupture, pericardial tamponade)?
History & Risk Stratification
Classic anginal pain is substernal, pressure-like, radiates to the jaw or left arm, occurs with exertion, and is relieved by rest or nitroglycerin. Atypical features include sharp, positional, or reproducible-with-palpation pain — but diabetics, women, and the elderly frequently have atypical presentations. Document onset, duration, character, radiation, associated symptoms (diaphoresis, nausea, dyspnea), risk factors (HTN, DM, HLD, smoking, family history of premature CAD, prior MI/PCI/CABG), and any recent cocaine or stimulant use.
Initial Workup
EKG within 10 minutes of arrival (STEMI rule-out), serial high-sensitivity troponins (0 and 1–3 hours), CBC, BMP, Mg, coagulation panel, chest X-ray, lipid panel, and a risk score (HEART, TIMI, or GRACE). If PE is considered, add a d-dimer and Wells score. If dissection is possible, CTA chest.
History (0–2), EKG (0–2), Age (0–2), Risk factors (0–2), initial Troponin (0–2). Total 0–10. Score 0–3 = low risk (discharge with follow-up), 4–6 = moderate (observation, serial troponins, stress test), 7–10 = high (admit, cardiology).
STEMI vs NSTEMI vs Unstable Angina
STEMI is an ST-elevation MI on EKG — this is a transmural infarct from complete occlusion. Treatment is immediate reperfusion (PCI within 90 minutes door-to-balloon, or thrombolytics if PCI unavailable). NSTEMI shows elevated troponin without ST elevation; treated with antiplatelet therapy (aspirin + P2Y12 inhibitor), anticoagulation (heparin or enoxaparin), statin, and cardiac catheterization, typically within 24–72 hours depending on GRACE risk score. Unstable angina is ischemic chest pain without troponin elevation — managed similarly to NSTEMI. Guidelines: 2023 ACC/AHA Chest Pain Guideline and AHA/ACC chest pain evaluation.
You will hear "trop bump" a lot. Document the exact troponin value and the delta (change from prior). A rising troponin in a clinically consistent presentation = MI. A flat troponin elevation can represent chronic injury (CKD, HF). Always chart the specific numbers.
04 Dyspnea & Respiratory Failure Pulmonary
Dyspnea is another huge IM complaint. The differential is broad: cardiac (HF, ACS, pericardial effusion, arrhythmia), pulmonary (COPD/asthma exacerbation, pneumonia, PE, pneumothorax, effusion), hematologic (anemia), metabolic (acidosis), neuromuscular, and anxiety.
Initial Workup
Every dyspneic patient gets vitals including SpO2 on room air, a focused cardiac/pulmonary exam, chest X-ray, EKG, CBC, BMP, BNP (or NT-proBNP), troponin, lactate, and often a d-dimer. Arterial blood gas (ABG) if respiratory failure is suspected. Bedside ultrasound (POCUS) is increasingly used for B-lines (pulmonary edema), pleural effusion, pneumothorax, and IVC assessment.
| Type | Definition | Examples |
|---|---|---|
| Type I (Hypoxemic) | PaO2 < 60 mmHg with normal/low PaCO2 | Pneumonia, PE, ARDS, pulmonary edema |
| Type II (Hypercapnic) | PaCO2 > 50 mmHg with acidosis | COPD exacerbation, neuromuscular weakness, opioid overdose |
| Type III (Perioperative) | Atelectasis-related | Post-op, obesity |
| Type IV (Shock) | Hypoperfusion of respiratory muscles | Cardiogenic or septic shock |
Oxygen Delivery Devices
| Device | Flow | FiO2 Range |
|---|---|---|
| Nasal cannula | 1–6 L/min | 24–44% |
| Simple face mask | 6–10 L/min | 35–55% |
| Non-rebreather | 10–15 L/min | 60–90% |
| High-flow nasal cannula (HFNC) | up to 60 L/min | 21–100% |
| BiPAP | Variable | Positive pressure, hypercapnia |
| CPAP | Variable | Positive pressure, hypoxemia/OSA |
| Mechanical ventilation | Variable | Full support |
Document SpO2 with the oxygen requirement every single time — "94% on 4 L NC" is useful; "94%" is not. An 88% sat on 6 L NC is very different from 88% on room air.
05 Heart Failure (Acute & Chronic) Cardiovascular
Heart failure (HF) is one of the top causes of hospital admission in adults over 65. It is classified by ejection fraction: HFrEF (reduced EF, ≤40%), HFmrEF (mildly reduced, 41–49%), and HFpEF (preserved, ≥50%).
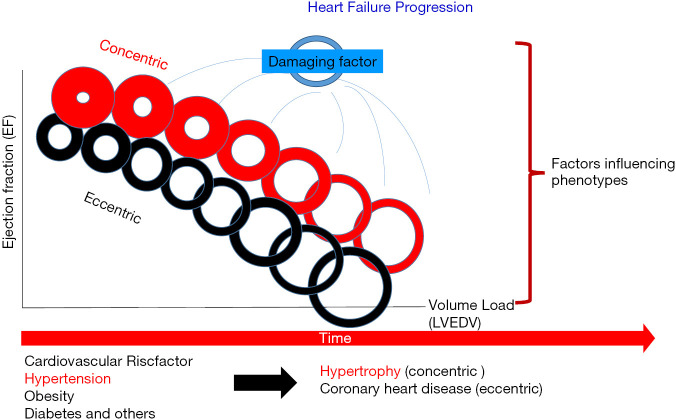
Pathophysiology
HFrEF reflects systolic dysfunction — the ventricle cannot contract effectively, often from prior MI, long-standing HTN, valve disease, or cardiomyopathy. HFpEF reflects diastolic dysfunction — the stiff ventricle cannot fill normally, typically in elderly patients with HTN, DM, and obesity. Both produce the same downstream physiology: elevated left-sided filling pressures, pulmonary congestion, and decreased cardiac output.
Acute Decompensated HF
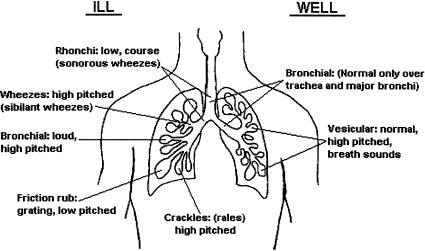
Patients present with dyspnea (especially exertional and orthopnea), lower extremity edema, weight gain, PND (paroxysmal nocturnal dyspnea), and fatigue. Exam shows elevated JVP, S3 gallop, bibasilar crackles, hepatomegaly, and pitting edema. BNP or NT-proBNP is elevated (BNP > 400 is typical of acute HF; 100–400 is a gray zone; < 100 essentially rules out HF). Chest X-ray shows cardiomegaly, cephalization, Kerley B lines, and interstitial edema.
Lasix (furosemide IV, typically 40–80 mg or double the home oral dose), Morphine (controversial, limited use), Nitrates, Oxygen, Position (upright). Monitor I/Os strictly and daily weights. Address precipitants: ischemia, arrhythmia (AFib RVR), dietary indiscretion, medication nonadherence, infection, PE, thyroid disease, uncontrolled HTN.
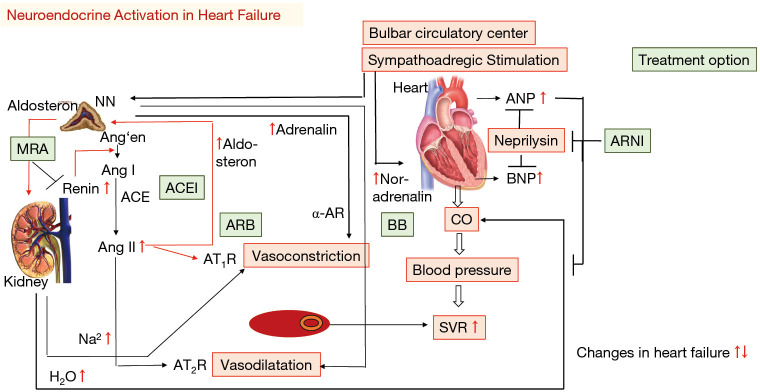
Chronic HFrEF — Guideline-Directed Medical Therapy
Modern GDMT has four pillars, guided by the 2022 AHA/ACC/HFSA Heart Failure Guideline:
- ARNI (sacubitril/valsartan) preferred, or ACEi/ARB
- Beta-blocker (carvedilol, metoprolol succinate, or bisoprolol)
- MRA (spironolactone or eplerenone)
- SGLT2 inhibitor (dapagliflozin or empagliflozin)
Loop diuretics are added for volume control but are not disease-modifying. Device therapy (ICD, CRT) is considered for EF ≤ 35% on optimal GDMT with QRS ≥ 150 ms.
Document dry weight on every HF patient — it is the target weight at euvolemia. Daily weights and I/Os drive diuresis. "Net negative 1.2 L" or "weight down 2.3 kg from admission" are the phrases attendings use to track progress.
06 Atrial Fibrillation & Arrhythmias Cardiovascular
Atrial fibrillation (AFib) is the most common sustained arrhythmia in adults. The two management questions are always: rate vs rhythm control, and stroke prevention.
Classification
| Type | Definition |
|---|---|
| Paroxysmal | Self-terminates within 7 days |
| Persistent | Lasts > 7 days, requires cardioversion |
| Long-standing persistent | > 12 months continuous |
| Permanent | Accepted, no rhythm control attempted |
| Valvular | Associated with moderate-to-severe mitral stenosis or mechanical valve |
CHA2DS2-VASc Score (Stroke Risk)
CHF (1), HTN (1), Age ≥ 75 (2), DM (1), Stroke/TIA/thromboembolism (2), Vascular disease (1), Age 65–74 (1), Sex category female (1). Max 9 points.
Anticoagulation recommended for score ≥ 2 in men or ≥ 3 in women. Preferred agents are DOACs (apixaban, rivaroxaban, dabigatran, edoxaban) unless valvular AFib (use warfarin). See the 2023 ACC/AHA/HRS AFib Guideline.
HAS-BLED Score (Bleeding Risk)
HTN uncontrolled (1), Abnormal renal/liver function (1 each), Stroke history (1), Bleeding history (1), Labile INR (1), Elderly > 65 (1), Drugs/alcohol (1 each). Score ≥ 3 = high bleeding risk — does NOT automatically exclude anticoagulation but prompts closer follow-up.
Rate vs Rhythm Control
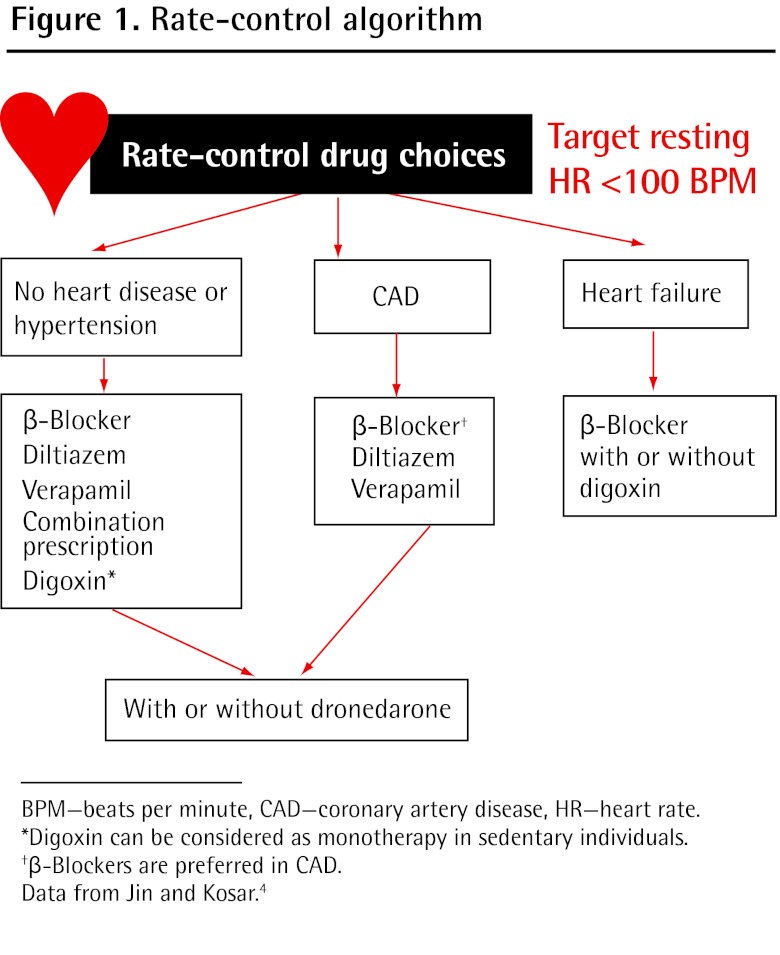
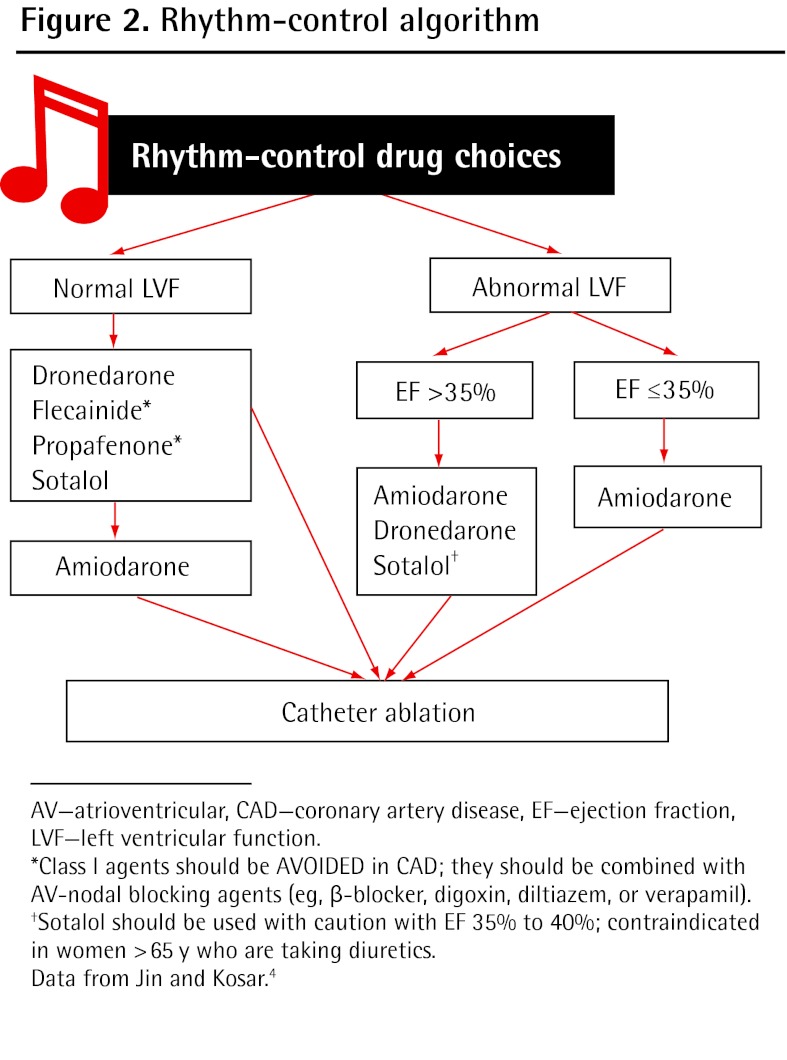
Rate control: Beta-blockers (metoprolol), non-dihydropyridine CCBs (diltiazem, verapamil), digoxin. Target resting HR < 110 in asymptomatic patients (lenient) or < 80 if symptomatic (strict). Rhythm control: Antiarrhythmics (amiodarone, flecainide, dofetilide, sotalol), direct current cardioversion, or catheter ablation. Modern trials (EAST-AFNET 4) favor early rhythm control in recently-diagnosed AFib.
07 Hypertension — Chronic, Urgency, Emergency Cardiovascular
HTN affects nearly half of US adults and is a major driver of stroke, MI, HF, CKD, and dementia. The 2017 ACC/AHA HTN Guideline defines stages.
| Category | SBP (mmHg) | DBP (mmHg) |
|---|---|---|
| Normal | < 120 | < 80 |
| Elevated | 120–129 | < 80 |
| Stage 1 HTN | 130–139 | 80–89 |
| Stage 2 HTN | ≥ 140 | ≥ 90 |
| Hypertensive crisis | > 180 | > 120 |
Chronic HTN Management
First-line agents: thiazide diuretics (chlorthalidone, HCTZ), ACEi/ARB, or calcium channel blockers. Beta-blockers are not first-line for uncomplicated HTN but are preferred for HF, post-MI, and AFib with RVR. Target BP < 130/80 for most adults; < 140/90 is acceptable in frail elderly per some guidelines.
Urgency: SBP > 180 or DBP > 120 without end-organ damage. Managed with oral agents, gradual BP reduction over 24–48 hours. No IV therapy needed.
Emergency: Severe HTN with acute end-organ damage — encephalopathy, stroke, MI, aortic dissection, pulmonary edema, acute kidney injury, eclampsia, retinal hemorrhage. Requires IV therapy (nicardipine, labetalol, nitroprusside, esmolol) in an ICU with arterial line. Lower MAP by no more than 25% in the first hour (except aortic dissection, where SBP should be rapidly lowered to < 120).
08 COPD & Asthma Pulmonary
COPD
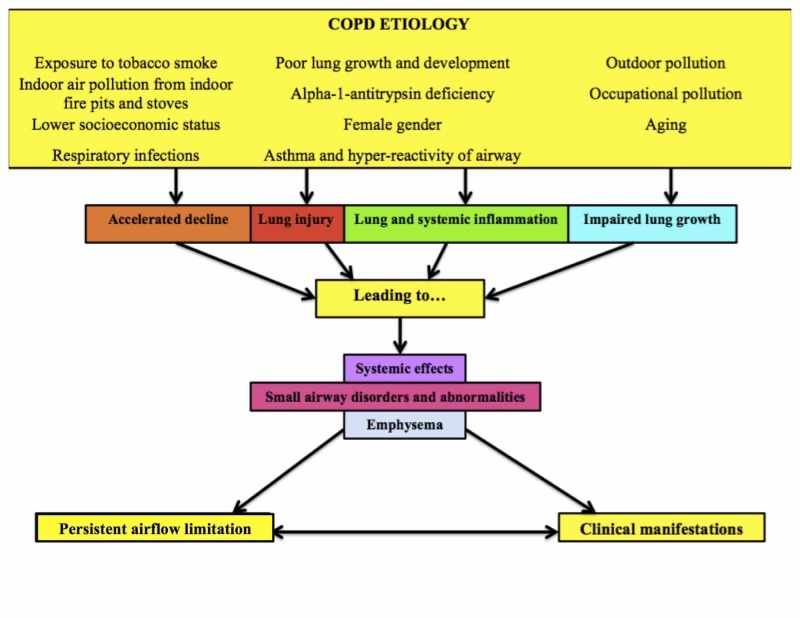
COPD is progressive airflow limitation from chronic bronchitis and/or emphysema, overwhelmingly caused by smoking (also alpha-1 antitrypsin deficiency, occupational exposures). Diagnosis requires spirometry with post-bronchodilator FEV1/FVC < 0.70. Severity by GOLD 2024 is based on FEV1 % predicted:
| GOLD Stage | FEV1 (% predicted) | Severity |
|---|---|---|
| GOLD 1 | ≥ 80% | Mild |
| GOLD 2 | 50–79% | Moderate |
| GOLD 3 | 30–49% | Severe |
| GOLD 4 | < 30% | Very severe |
GOLD also classifies patients by symptom burden (mMRC, CAT) and exacerbation history into groups A, B, and E, which guides inhaler selection.
COPD Exacerbation (AECOPD)
Short-acting bronchodilators (albuterol + ipratropium neb), systemic steroids (prednisone 40 mg PO × 5 days or methylprednisolone IV), antibiotics if increased sputum purulence/volume or need for ventilation (azithromycin, doxycycline, or amoxicillin-clavulanate), controlled oxygen (target SpO2 88–92% to avoid CO2 retention), and NIV (BiPAP) for hypercapnic respiratory failure.
Asthma
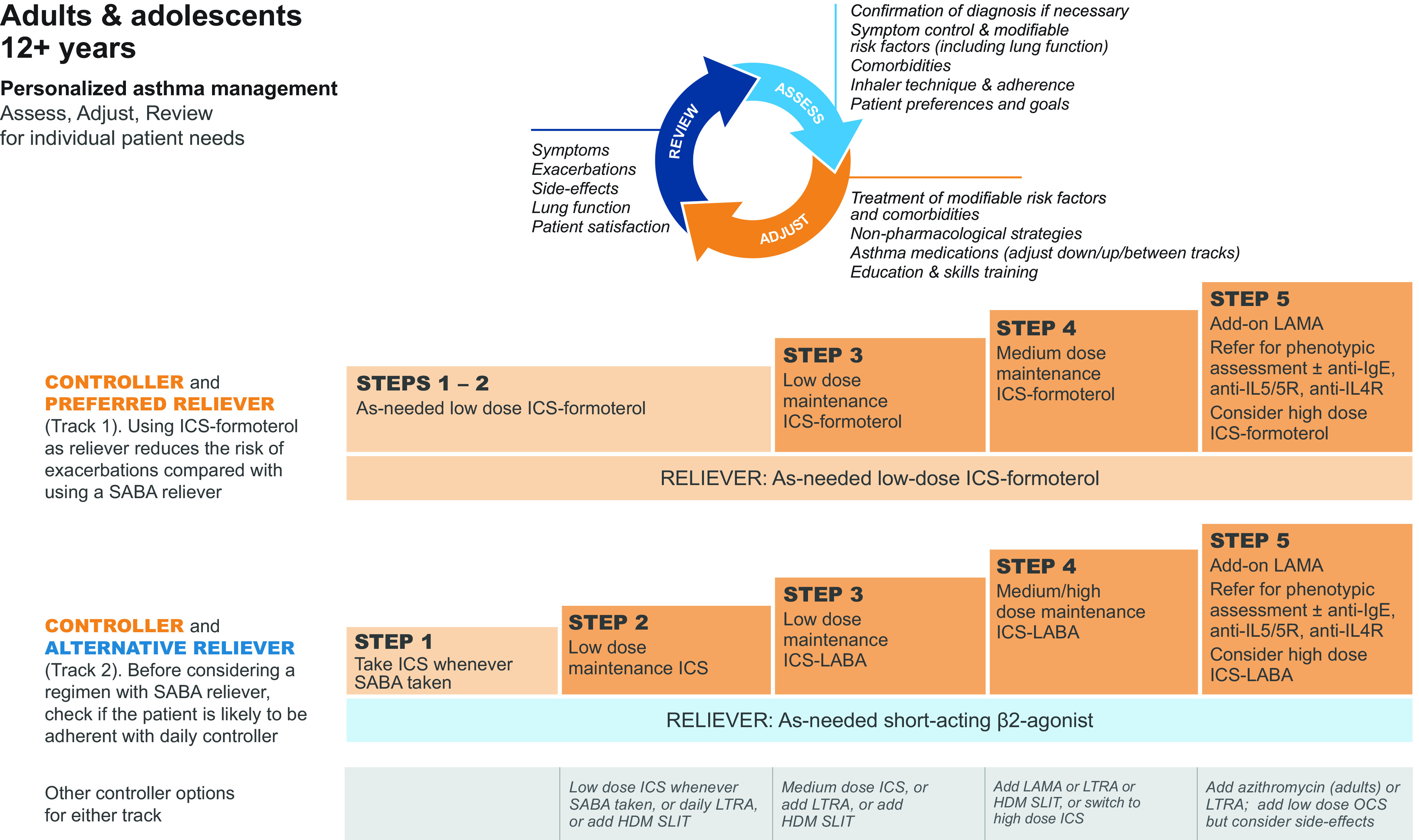
Asthma is reversible airflow obstruction from airway hyperresponsiveness and inflammation. Classified by severity and control. Stepwise therapy per GINA progresses from low-dose ICS-formoterol PRN (step 1–2), to low-dose ICS-LABA maintenance (step 3), to medium-dose (step 4), to high-dose plus biologics (step 5). Severe exacerbations require albuterol, ipratropium, systemic steroids, IV magnesium, and escalation to NIV or intubation if severe.
09 Community-Acquired Pneumonia Infectious
CAP is a leading infectious cause of hospital admission. Typical organisms: Streptococcus pneumoniae (#1), H. influenzae, Moraxella. Atypicals: Mycoplasma, Chlamydia pneumoniae, Legionella. Viral: influenza, RSV, SARS-CoV-2.
Diagnosis
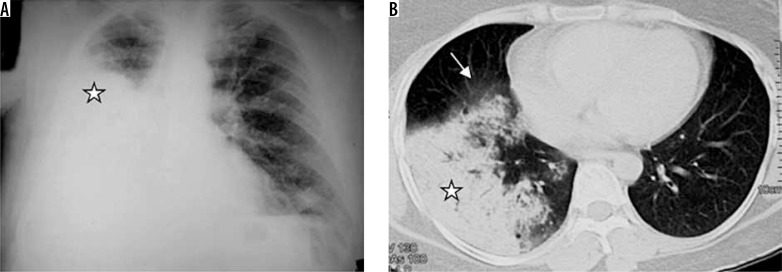
Clinical + imaging: fever, cough, dyspnea, pleuritic chest pain, leukocytosis, and a new infiltrate on chest X-ray or CT. Obtain sputum Gram stain/culture, blood cultures (if severe), urinary antigens for Legionella and pneumococcus, and a respiratory viral panel. Procalcitonin may help distinguish bacterial from viral.
Severity Scoring — CURB-65
Confusion, Urea > 19 mg/dL (BUN), Respiratory rate ≥ 30, BP (SBP < 90 or DBP ≤ 60), age ≥ 65. Each 1 point.
0–1 = outpatient; 2 = short inpatient or observation; 3–5 = inpatient, consider ICU. PSI (Pneumonia Severity Index) is a more complex alternative stratifying to risk classes I–V.
Treatment (IDSA/ATS 2019)
Per the 2019 IDSA/ATS CAP Guideline:
- Outpatient, healthy: amoxicillin, doxycycline, or a macrolide (if local pneumococcal resistance < 25%)
- Outpatient, comorbidities: amoxicillin-clavulanate or cefuroxime PLUS macrolide/doxycycline, OR respiratory fluoroquinolone (levofloxacin, moxifloxacin) alone
- Inpatient, non-severe: ceftriaxone + azithromycin, OR respiratory fluoroquinolone alone
- ICU: ceftriaxone + azithromycin (or fluoroquinolone); add vancomycin/linezolid if MRSA risk factors, add antipseudomonal coverage (pip-tazo, cefepime) if Pseudomonas risk
Duration: minimum 5 days, clinically stable for 48–72 hours before stopping.
10 Venous Thromboembolism (DVT/PE) Hematologic
DVT and PE together constitute venous thromboembolism (VTE). PE is the third most common cardiovascular cause of death after MI and stroke. Risk factors include immobility, surgery, malignancy, pregnancy/postpartum, estrogen therapy, obesity, prior VTE, and inherited thrombophilias (Factor V Leiden, prothrombin gene mutation).
Wells Scores
Active cancer (+1), paralysis/recent immobilization (+1), recently bedridden > 3 days or major surgery within 12 wk (+1), localized tenderness along deep veins (+1), entire leg swollen (+1), calf swelling > 3 cm compared to contralateral (+1), pitting edema (+1), collateral superficial veins (+1), prior DVT (+1), alternative diagnosis as likely (−2). ≥ 2 = likely, < 2 = unlikely.
Clinical signs of DVT (3), PE most likely diagnosis (3), HR > 100 (1.5), immobilization/surgery < 4 wk (1.5), prior DVT/PE (1.5), hemoptysis (1), malignancy (1). > 6 = high, 2–6 = moderate, < 2 = low. Combined with d-dimer, PERC, and CTA for diagnosis.
Treatment
Per CHEST 2021 VTE guidance, DOACs (apixaban, rivaroxaban) are first-line for most patients. For cancer-associated thrombosis, apixaban, rivaroxaban, or edoxaban (without luminal GI cancers) is preferred. LMWH (enoxaparin) remains a strong alternative in pregnancy and advanced cancer. Duration is 3 months minimum; indefinite for unprovoked recurrent or persistent risk factor VTE.
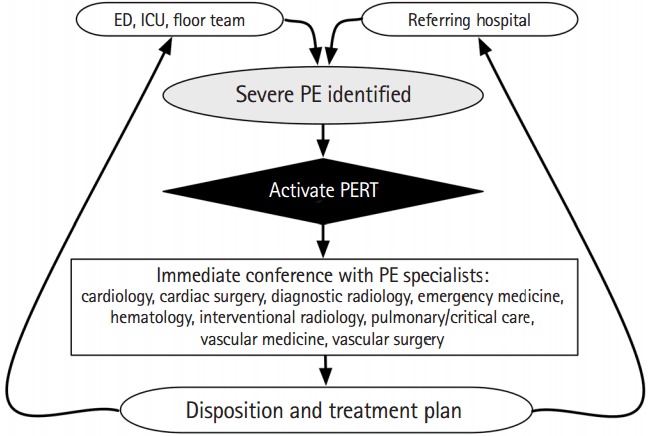
Massive PE = hypotension (SBP < 90) — consider systemic thrombolytics (alteplase 100 mg over 2 hours), catheter-directed thrombolysis, or surgical embolectomy. Submassive PE = RV dysfunction on echo/CT with elevated troponin/BNP but normotensive — judicious use of catheter-directed thrombolysis, otherwise anticoagulation alone.
11 Sepsis & Septic Shock Infectious
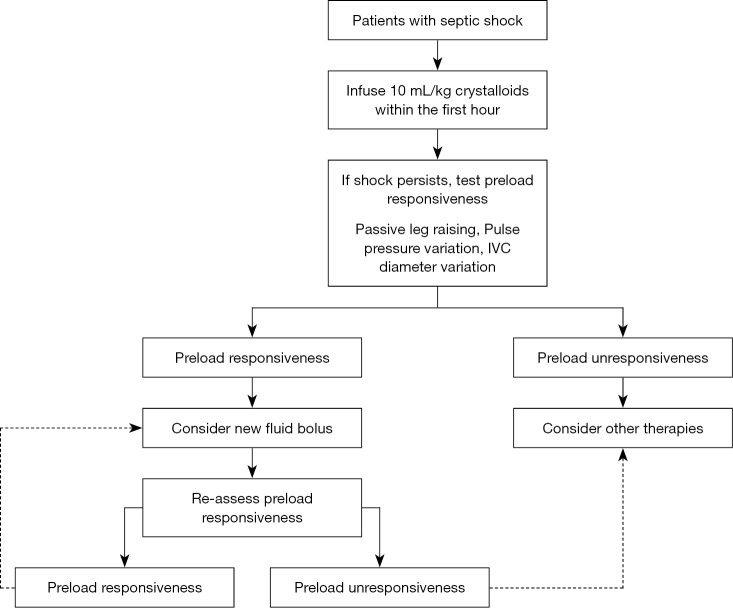
Sepsis is life-threatening organ dysfunction caused by a dysregulated host response to infection. Septic shock is sepsis with circulatory failure requiring vasopressors to maintain MAP ≥ 65 and lactate > 2 despite adequate fluid resuscitation.
Screening & Severity Scores
Respiratory rate ≥ 22 (1), altered mentation GCS < 15 (1), SBP ≤ 100 (1). ≥ 2 = high risk of poor outcome.
Six organ systems scored 0–4: respiratory (PaO2/FiO2), coagulation (platelets), liver (bilirubin), cardiovascular (MAP, vasopressors), CNS (GCS), and renal (creatinine, urine output). An increase of ≥ 2 over baseline defines sepsis.
Ward-based deterioration score using RR, SpO2, O2 supplementation, temp, SBP, HR, and level of consciousness. Total ≥ 5 triggers escalation; ≥ 7 suggests critical illness.
Surviving Sepsis Bundle
The Surviving Sepsis Campaign 2021 one-hour bundle: measure lactate, obtain blood cultures before antibiotics, administer broad-spectrum antibiotics, begin 30 mL/kg crystalloid for hypotension or lactate ≥ 4, start vasopressors (norepinephrine first-line) if hypotensive during or after fluids to maintain MAP ≥ 65.
Document the sepsis time zero — the clock starts when sepsis is recognized. Hospitals are audited on whether lactate, cultures, antibiotics, and fluids all happen within 1–3 hours. Always chart the source of infection (urinary, pulmonary, skin, intraabdominal, CLABSI).
12 Acute Kidney Injury & CKD Renal
AKI Definition (KDIGO)
Per KDIGO 2012: AKI is defined as any of: (1) increase in serum creatinine by ≥ 0.3 mg/dL within 48 hours, (2) increase to ≥ 1.5× baseline within 7 days, or (3) urine output < 0.5 mL/kg/hr for 6 hours.
| Stage | Creatinine | Urine Output |
|---|---|---|
| 1 | 1.5–1.9× baseline OR ≥ 0.3 mg/dL rise | < 0.5 mL/kg/hr × 6–12 h |
| 2 | 2.0–2.9× baseline | < 0.5 mL/kg/hr × ≥ 12 h |
| 3 | ≥ 3.0× baseline OR cr ≥ 4.0 OR RRT initiation | < 0.3 mL/kg/hr × 24 h or anuria 12 h |
Pre-renal / Intrinsic / Post-renal
Pre-renal (hypoperfusion): volume depletion, hypotension, HF, hepatorenal. FeNa < 1%, BUN:Cr > 20. Intrinsic: ATN (ischemia, contrast, nephrotoxic drugs), AIN (medications, especially PPIs, NSAIDs, antibiotics), glomerulonephritis, vasculitis. FeNa > 2% in ATN. Post-renal: obstruction — BPH, stones, tumors, neurogenic bladder. Diagnose with bladder scan and renal ultrasound (hydronephrosis).
CKD Staging
| Stage | eGFR (mL/min/1.73m²) | Description |
|---|---|---|
| G1 | ≥ 90 | Normal with markers of damage (albuminuria) |
| G2 | 60–89 | Mildly decreased |
| G3a | 45–59 | Mild-moderate |
| G3b | 30–44 | Moderate-severe |
| G4 | 15–29 | Severe — pre-dialysis |
| G5 | < 15 | Kidney failure — dialysis or transplant |
Indications for Urgent Dialysis (AEIOU)
Acidosis (refractory), Electrolytes (hyperkalemia refractory), Ingestions (methanol, ethylene glycol, ASA, lithium, metformin), Overload (refractory pulmonary edema), Uremia (pericarditis, encephalopathy, bleeding).
13 Electrolyte & Acid-Base Derangements Renal
Hyperkalemia
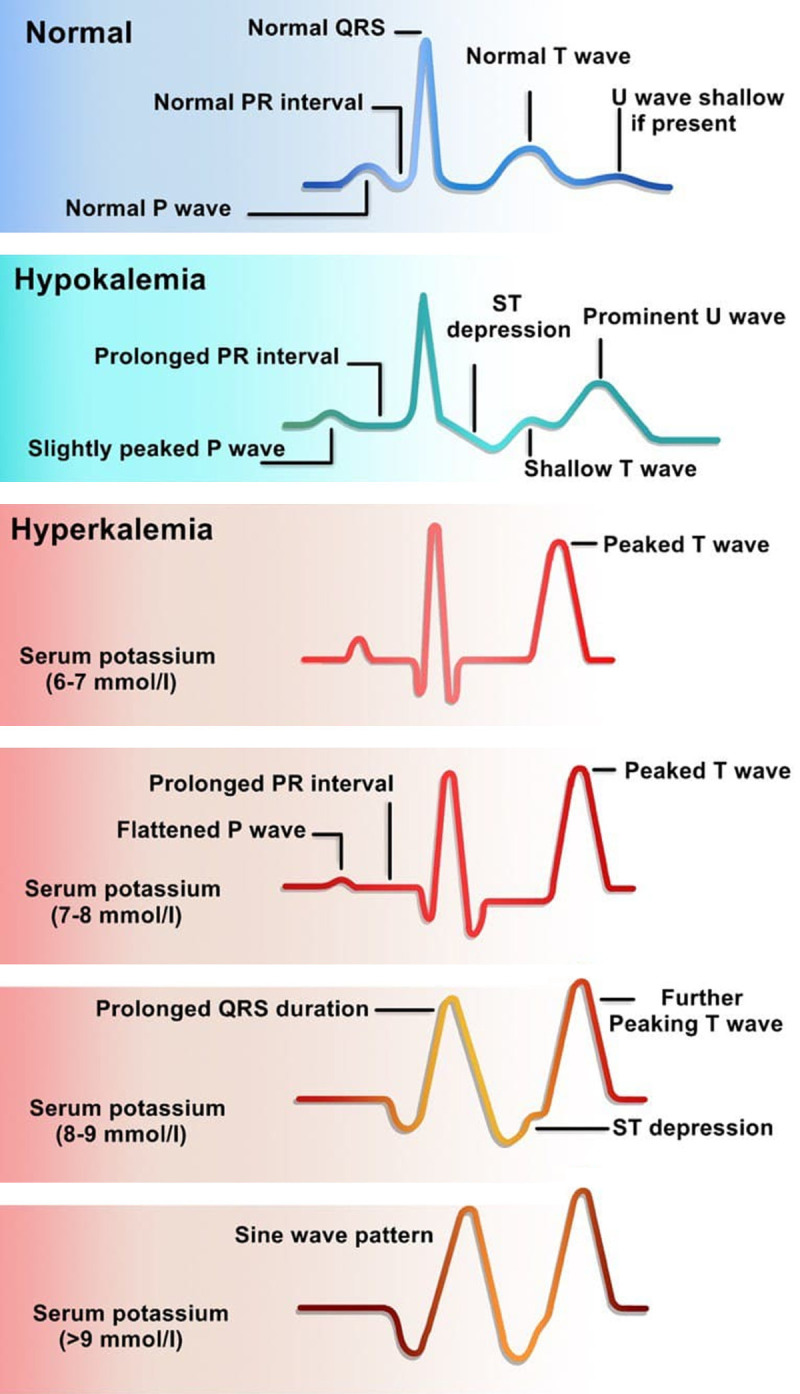
Causes: renal failure, ACEi/ARB, spironolactone, rhabdomyolysis, tumor lysis, adrenal insufficiency, hemolyzed sample. EKG changes: peaked T waves, PR prolongation, QRS widening, sine wave, VFib/asystole. Treatment: calcium gluconate (membrane stabilization), insulin + D50, albuterol neb, sodium bicarbonate (if acidotic), loop diuretics, potassium binders (patiromer, SZC, SPS), and dialysis for refractory cases.
Hyponatremia
Classify by volume status: hypovolemic (GI losses, diuretics, adrenal insufficiency), euvolemic (SIADH, hypothyroidism, psychogenic polydipsia), hypervolemic (HF, cirrhosis, nephrotic, CKD). Acute symptomatic severe hyponatremia: 3% saline cautiously. Correct no faster than 8 mEq/L per 24 hours to avoid osmotic demyelination.
Hypernatremia
Almost always water deficit — dehydration, diabetes insipidus, inability to access water. Treat with free water (oral or D5W), correct at ≤ 10–12 mEq/L/day.
Other Key Derangements
| Problem | Common Causes | Core Treatment |
|---|---|---|
| Hypokalemia | Diuretics, GI losses, hypomagnesemia | Oral/IV KCl, replace Mg |
| Hypomagnesemia | Diuretics, alcoholism, PPIs | IV/PO magnesium |
| Hypocalcemia | Hypoparathyroidism, vit D deficiency, CKD, pancreatitis | Calcium gluconate / carbonate |
| Hypercalcemia | Malignancy, hyperparathyroidism | IV fluids, calcitonin, bisphosphonates |
| Hypophosphatemia | Refeeding syndrome, alcoholism, DKA | PO/IV phosphate |
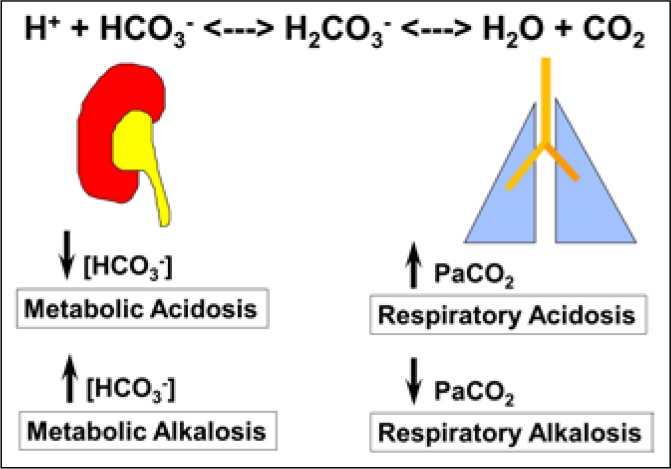
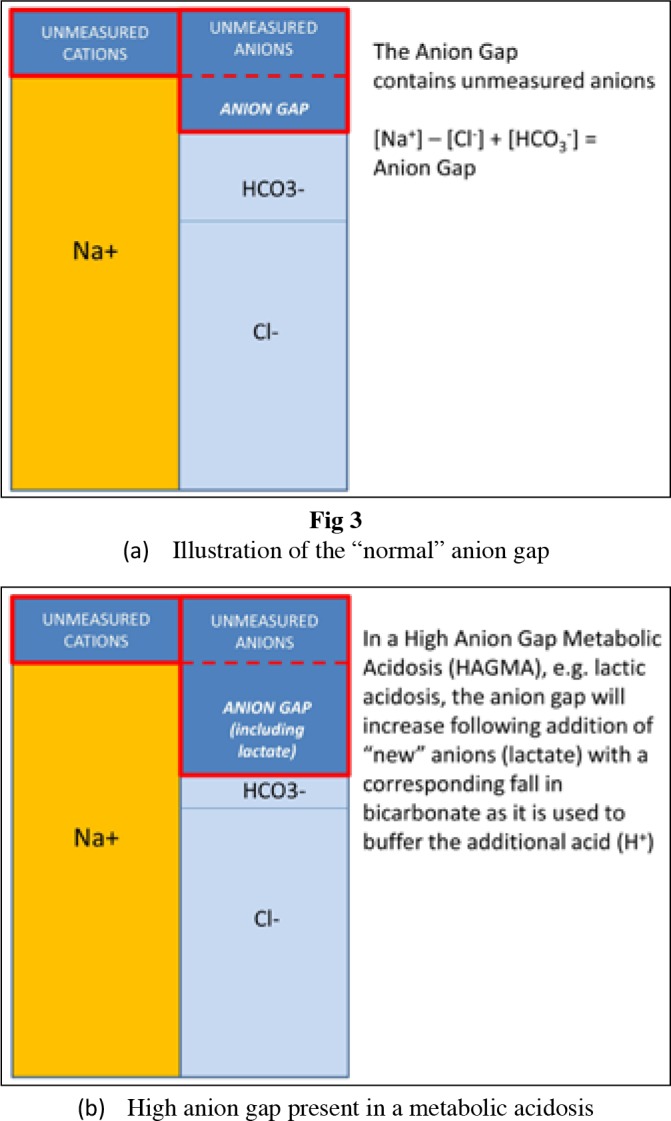
Acid-Base Analysis
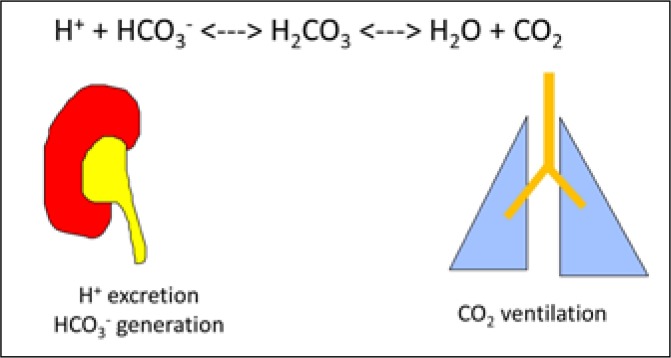
Step 1: pH (acidemia or alkalemia?). Step 2: is it metabolic (HCO3) or respiratory (PaCO2)? Step 3: for metabolic acidosis, calculate anion gap (Na − Cl − HCO3, normal 8–12). AG acidosis causes: MUDPILES (Methanol, Uremia, DKA, Propylene glycol, Iron/INH, Lactic acidosis, Ethylene glycol, Salicylates). Non-gap: diarrhea, RTA, TPN. Step 4: check appropriate compensation (Winters formula: expected PaCO2 = 1.5×HCO3 + 8 ± 2).
14 Diabetes, DKA & HHS Endocrine
Type 2 DM Management
Per the ADA Standards of Care 2024, first-line therapy is metformin plus lifestyle modification. For patients with established ASCVD, HF, or CKD, add an SGLT2 inhibitor or GLP-1 receptor agonist with proven cardiovascular benefit regardless of A1C. Targets: A1C < 7% for most; < 6.5% if achievable without hypoglycemia; < 8% in frail elderly. Annual screening for retinopathy, nephropathy (urine albumin/creatinine), and neuropathy (monofilament foot exam).
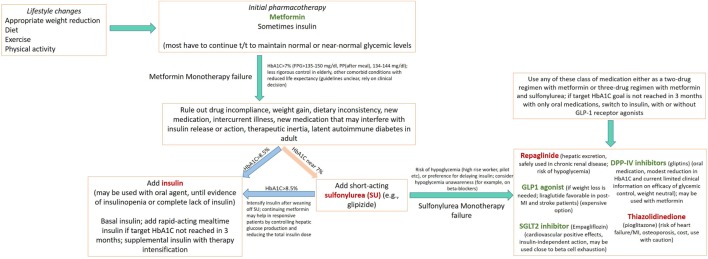
Drug Classes
| Class | Examples | Key Points |
|---|---|---|
| Biguanide | Metformin | First line; avoid eGFR < 30; risk of lactic acidosis |
| SGLT2 inhibitor | Empagliflozin, dapagliflozin, canagliflozin | HF/CKD benefit; risk of DKA, UTI, volume loss |
| GLP-1 RA | Semaglutide, liraglutide, dulaglutide, tirzepatide (GIP/GLP-1) | Weight loss, CV benefit; GI side effects, pancreatitis risk |
| DPP-4 inhibitor | Sitagliptin, linagliptin | Weight neutral, mild A1C effect |
| Sulfonylurea | Glipizide, glimepiride | Cheap but causes hypoglycemia and weight gain |
| Thiazolidinedione | Pioglitazone | Avoid in HF, fracture risk |
| Insulin | Glargine, detemir, degludec (basal); lispro, aspart, glulisine (bolus) | Most potent; risk of hypoglycemia |
DKA vs HHS
| Feature | DKA | HHS |
|---|---|---|
| Typical population | Type 1 DM, younger | Type 2 DM, elderly |
| Glucose | > 250 mg/dL (often 300–600) | > 600 mg/dL (often > 1000) |
| pH | < 7.3 | > 7.3 |
| Bicarbonate | < 18 | > 18 |
| Ketones | Positive (anion gap acidosis) | Negative/minimal |
| Osmolality | Variable | > 320 mOsm/kg |
| Mental status | Usually alert | Often altered/comatose |
Management: Aggressive IV fluids (NS then 1/2 NS), insulin drip (0.1 U/kg/hr after ensuring K > 3.3), potassium replacement (always, even if initial K is normal), dextrose added when glucose < 250. Treat the precipitant: infection, MI, medication nonadherence, new-onset DM. Close the anion gap before stopping the insulin drip in DKA.
15 GI Bleeding & Hepatology GI/Hepatic
Upper vs Lower GI Bleeding
Upper GI bleed (UGIB): Proximal to the ligament of Treitz. Presents with hematemesis, coffee-ground emesis, or melena. Causes: peptic ulcer disease (#1), variceal bleeding, Mallory-Weiss tear, gastritis, malignancy, angiodysplasia. BUN is disproportionately elevated. Initial: IV fluids, transfuse to Hgb > 7 (> 8 if CAD), pantoprazole drip, NPO, octreotide if variceal, emergent EGD within 24 hours. Glasgow-Blatchford score > 0 = admit. Lower GI bleed: Distal to Treitz. Causes: diverticulosis, angiodysplasia, ischemic colitis, hemorrhoids, IBD, malignancy. Colonoscopy is diagnostic and therapeutic.
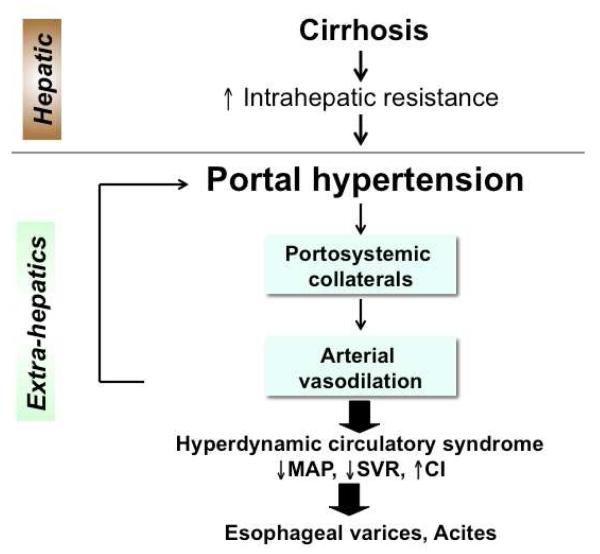
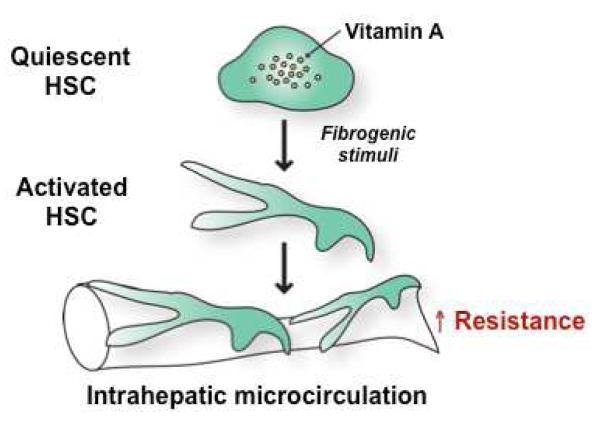
Cirrhosis & Its Complications
Cirrhosis staging uses the Child-Pugh score (bilirubin, albumin, INR, ascites, encephalopathy — A/B/C) and MELD-Na (bilirubin, INR, creatinine, sodium — used for transplant listing). Complications: ascites, spontaneous bacterial peritonitis (SBP), variceal bleeding, hepatic encephalopathy, hepatorenal syndrome, hepatocellular carcinoma. AASLD cirrhosis guidance is the standard citation.
Ascites: Sodium restriction, spironolactone + furosemide (100:40 ratio), large-volume paracentesis with albumin replacement.
SBP diagnosis: Ascitic PMN count ≥ 250 cells/mm³. Treat with ceftriaxone; add albumin to prevent hepatorenal syndrome.
Variceal bleeding: Octreotide, IV PPI, ceftriaxone prophylaxis, emergent EGD with band ligation.
Hepatic encephalopathy: Lactulose (titrate to 3 bowel movements/day), rifaximin. Identify and treat precipitants (infection, GI bleed, constipation, dehydration).
Common Outpatient GI (AGA)
Per AGA guidance, GERD is managed with PPIs; IBS with dietary modification and symptom-based pharmacotherapy; IBD (Crohn and UC) with mesalamine, steroids, immunomodulators, and biologics (anti-TNF, anti-integrin, anti-IL-23).
16 UTI, Pyelonephritis & Cellulitis Infectious
UTI
Uncomplicated cystitis in non-pregnant women: nitrofurantoin 100 mg BID × 5 days, TMP-SMX DS BID × 3 days (if local E. coli resistance < 20%), or fosfomycin 3 g × 1. Complicated UTI (males, catheterized, pregnant, immunocompromised, urologic abnormality): longer course with a fluoroquinolone, beta-lactam, or culture-directed therapy.
Pyelonephritis
Fever, flank pain, CVA tenderness, dysuria, nausea/vomiting. Outpatient mild cases: oral fluoroquinolone 7 days. Hospitalized: IV ceftriaxone, piperacillin-tazobactam, or fluoroquinolone; blood and urine cultures; imaging (CT) if not improving or if complicated.
Cellulitis & Skin Infections
Non-purulent cellulitis: streptococcal predominance — cephalexin or cefazolin. Purulent (abscess): I&D first, MRSA coverage with TMP-SMX, doxycycline, or clindamycin. Severe/systemic: IV vancomycin. Necrotizing fasciitis is a surgical emergency — pain out of proportion, crepitus, bullae, rapid progression — call surgery immediately, broad-spectrum antibiotics with clindamycin (toxin suppression).
17 Anemia & Hematology Hematologic
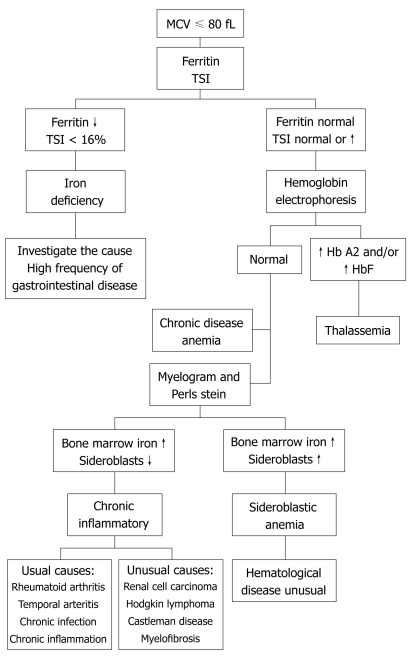
Anemia Workup by MCV
Microcytic (MCV < 80): Iron deficiency (low ferritin, high TIBC), thalassemia (normal-high ferritin, target cells), anemia of chronic disease (can be normocytic or microcytic), lead poisoning, sideroblastic.
Normocytic (MCV 80–100): Anemia of chronic disease, early iron deficiency, CKD (low erythropoietin), acute blood loss, hemolysis, aplastic anemia, bone marrow infiltration.
Macrocytic (MCV > 100): B12 deficiency, folate deficiency, alcoholism, liver disease, hypothyroidism, medication-induced (methotrexate, hydroxyurea), MDS.
Key Tests
Initial: CBC with retic count, peripheral smear, iron studies (Fe, TIBC, ferritin, transferrin sat), B12, folate, reticulocyte count, LDH, haptoglobin, total and direct bilirubin (if hemolysis suspected), Coombs test. Iron deficiency in a post-menopausal woman or any adult male requires GI evaluation with EGD/colonoscopy.
Other Hematologic Issues
Thrombocytopenia: ITP, TTP (MAHA + thrombocytopenia + fever + renal + neuro — emergency, plasma exchange), DIC, HIT (platelet drop with heparin exposure), liver disease, medications. Hypercoagulable states: Factor V Leiden, prothrombin gene mutation, protein C/S deficiency, antithrombin deficiency, antiphospholipid syndrome. Transfusion thresholds: Hgb < 7 in most stable patients; < 8 in active ACS or cardiac surgery. Platelets < 10 prophylactic; < 20 with fever; < 50 for procedures.
18 Altered Mental Status, Syncope & Falls Neurologic
AMS Workup
AMS is a final common pathway with an enormous differential — use the AEIOU TIPS mnemonic: Alcohol/Acidosis, Epilepsy/Electrolytes/Encephalopathy, Insulin (hypo/hyperglycemia), Oxygen/Opioids, Uremia, Trauma/Temperature, Infection, Psychiatric/Poisoning, Stroke/Shock. Initial workup: glucose, electrolytes, CBC, LFTs, ammonia (if cirrhosis), UA, blood cultures, CT head, EKG, ABG, tox screen, TSH, B12. In delirium, identify and treat precipitants — medications (especially anticholinergics, benzodiazepines, opioids), infection, metabolic derangements, pain, constipation, urinary retention, sleep disruption. Non-pharmacologic measures first.
Syncope
Transient loss of consciousness from global cerebral hypoperfusion. Categories: reflex/vasovagal (most common, benign), orthostatic (volume loss, medications, autonomic dysfunction), cardiac (arrhythmia, structural heart disease — aortic stenosis, HCM, PE, MI; most dangerous). Workup: orthostatic vitals, EKG on everyone, echo if cardiac suspected, Holter or event monitor for recurrent episodes. San Francisco Syncope Rule and Canadian Syncope Risk Score help risk-stratify for admission.
Falls in the Elderly
Leading cause of injury and hospitalization in patients > 65. Multifactorial: polypharmacy (especially benzodiazepines, opioids, antihypertensives), visual impairment, orthostasis, neuropathy, muscle weakness, cognitive impairment, environmental hazards. Always perform a Timed Up-and-Go, review medications, check orthostatic vitals, screen for osteoporosis and vitamin D, consider PT/OT referral and home safety evaluation.
19 Thyroid, Adrenal & Endocrine Essentials Endocrine
Hypothyroidism
Elevated TSH with low free T4. Most common cause: Hashimoto thyroiditis. Symptoms: fatigue, cold intolerance, weight gain, constipation, dry skin, bradycardia, depression. Treatment: levothyroxine starting 1.6 mcg/kg/day (lower in elderly and CAD), recheck TSH in 6 weeks and titrate. Target TSH 0.5–4.5 mIU/L in most adults.
Hyperthyroidism
Suppressed TSH with elevated T4/T3. Causes: Graves disease (TSH receptor antibodies, ophthalmopathy), toxic multinodular goiter, toxic adenoma, thyroiditis. Treatment: methimazole (first-line), radioactive iodine, or thyroidectomy. Beta-blockers (propranolol, atenolol) for symptom control. Thyroid storm is a medical emergency (hyperthermia, tachyarrhythmia, AMS) — PTU, beta-blocker, steroids, cooling, ICU care.
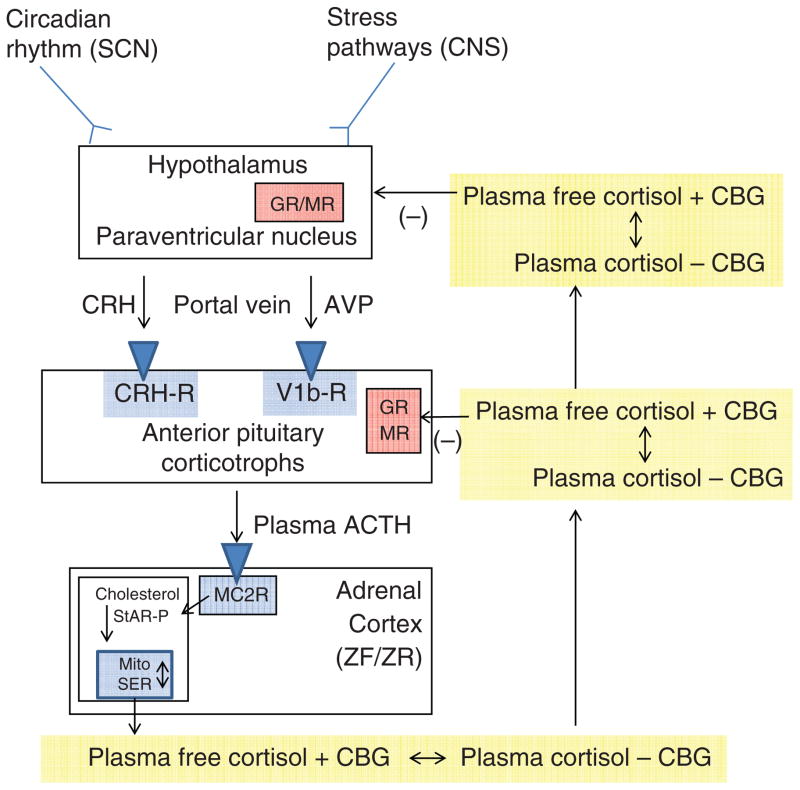
Adrenal
Adrenal insufficiency: Primary (Addison, autoimmune most common) or secondary (pituitary or chronic steroid use with abrupt discontinuation). Symptoms: fatigue, weight loss, hypotension, hyperpigmentation (primary only), hyponatremia, hyperkalemia. Diagnosed with morning cortisol and cosyntropin stimulation test. Treatment: hydrocortisone and fludrocortisone. Adrenal crisis = stress-dose IV hydrocortisone 100 mg, fluids, glucose.
20 Preventive Medicine & Cancer Screening Preventive
Preventive care is a core outpatient IM function. The USPSTF is the authoritative source for screening recommendations.
| Cancer | Population | Test & Interval |
|---|---|---|
| Breast | Women 40–74 | Biennial mammography |
| Cervical | Women 21–65 | Pap q3y (21–29); Pap + HPV q5y or Pap q3y (30–65) |
| Colorectal | Adults 45–75 | Colonoscopy q10y, FIT annually, or Cologuard q3y |
| Lung | 50–80, ≥ 20 pack-years, current or quit < 15 y | Annual low-dose CT |
| Prostate | Men 55–69 (individualized) | Shared decision-making for PSA |
| AAA | Men 65–75 who ever smoked | One-time abdominal ultrasound |
Vaccinations
Annual influenza. Tdap once then Td every 10 years (Tdap each pregnancy). COVID-19 per current CDC recommendations. Pneumococcal (PCV20 or PCV15+PPSV23) for adults ≥ 65 or high-risk. Zoster (recombinant Shingrix) ≥ 50. HPV through age 26 (shared decision through 45). Hepatitis B for all adults 19–59. RSV for adults ≥ 75 (and 60–74 high-risk).
Chronic Disease Management Snapshot
Dyslipidemia: Per 2018 ACC/AHA Cholesterol Guideline, statins for secondary prevention, LDL ≥ 190, diabetics 40–75, or primary prevention in 40–75 with 10-year ASCVD risk ≥ 7.5%. High-intensity: atorvastatin 40–80, rosuvastatin 20–40. Add ezetimibe or PCSK9 inhibitor if LDL target not reached.
21 Perioperative Medicine & Transitions of Care Preventive
Preoperative Evaluation
The IM consultant (or hospitalist) is asked to "medically optimize" and "risk stratify" surgical candidates. The framework comes from the ACC/AHA Perioperative Guideline: (1) urgency of surgery, (2) active cardiac conditions (unstable angina, decompensated HF, significant arrhythmia, severe valve disease), (3) functional capacity (METs), (4) surgery-specific risk, (5) stepwise testing if unclear.
RCRI (Revised Cardiac Risk Index): 1 point each for high-risk surgery, ischemic heart disease, HF, CVA, insulin-requiring DM, creatinine > 2. ≥ 2 points = elevated cardiac risk. Consider stress testing only if it would change management.
VTE Prophylaxis
Padua Prediction Score (medical inpatients): active cancer (3), prior VTE (3), reduced mobility (3), thrombophilia (3), recent trauma/surgery (2), age ≥ 70 (1), heart/respiratory failure (1), acute MI/stroke (1), infection/rheum (1), BMI ≥ 30 (1), hormonal therapy (1). ≥ 4 = high risk — start pharmacologic prophylaxis.
Caprini Score (surgical patients): comprehensive checklist including age, BMI, cancer, surgery type, central line, and thrombophilia. Higher scores mandate mechanical plus pharmacologic prophylaxis.
Standard pharmacologic prophylaxis: enoxaparin 40 mg SC daily (30 mg BID if high risk, 30 mg daily if CrCl < 30), heparin 5000 U SC BID/TID, or DOAC in select populations. Mechanical: sequential compression devices (SCDs).
Transitions of Care & Discharge
Every hospital discharge should include: medication reconciliation (what's new, what's stopped, what's changed), follow-up appointments (within 7–14 days for high-risk patients), red-flag teaching, functional and cognitive assessment, dispo (home, SNF, rehab, LTAC), and a concise discharge summary sent to the PCP. The Charlson Comorbidity Index (weighted burden of 19 conditions) is used for risk adjustment and mortality prediction.
22 Procedures in Internal Medicine Procedural
Inpatient internists perform a defined set of bedside procedures. As a scribe, you are often responsible for the procedure note including indication, consent, time-out, technique, operator, complications, estimated blood loss, and post-procedure plan.
Core Procedures
| Procedure | Purpose | Key Documentation |
|---|---|---|
| Lumbar puncture (LP) | Meningitis, SAH, MS, idiopathic intracranial HTN | Opening pressure, CSF appearance, tubes 1–4 (cell count, protein, glucose, culture, cytology) |
| Paracentesis | New ascites, SBP rule-out, symptomatic relief | Volume removed, albumin given (8 g per L if > 5 L), cell count, SAAG |
| Thoracentesis | Diagnostic (new effusion) or therapeutic (dyspneic effusion) | Volume, appearance, Light's criteria (protein ratio, LDH ratio, LDH) |
| Central line (CVC) | Vasopressors, poor peripheral access, TPN, dialysis | Site (IJ, subclavian, femoral), ultrasound guidance, number of attempts, post-procedure CXR |
| Arterial line | Continuous BP monitoring, frequent ABGs | Site (radial most common), Allen test, waveform |
| NG tube | Decompression (ileus, SBO), gastric lavage, feeding | Size (French), position confirmation by X-ray or aspirate |
| Foley catheter | Retention, strict I/O in critical illness, immobility | Size, sterile insertion, residual volume |
| Arthrocentesis | Evaluate joint effusion, septic joint, crystal disease | Volume, appearance, cell count, crystals, Gram stain |
Lumbar Puncture Detail
Patient in lateral decubitus (gold standard for opening pressure) or sitting flexed forward. Mark L4 at the iliac crest, insert at L3/L4 or L4/L5 interspace, advance through skin, supraspinous ligament, interspinous ligament, ligamentum flavum, dura, and into the subarachnoid space. Collect 4 tubes: (1) cell count/diff, (2) glucose/protein, (3) Gram stain/culture, (4) additional (cytology, viral PCR, oligoclonal bands). Note opening pressure if in lateral decubitus.
Paracentesis Detail
Left lower quadrant (two finger breadths medial and cephalad to the anterior superior iliac spine) is the standard site. Ultrasound guidance should be used whenever possible to identify a large pocket and avoid bowel. Send fluid for cell count with differential (PMN ≥ 250 = SBP), total protein, albumin (calculate SAAG: serum albumin − ascites albumin; ≥ 1.1 = portal HTN), culture (bedside inoculation of blood culture bottles), and cytology if malignancy suspected. Replace albumin 6–8 g per liter removed if > 5 L.
Thoracentesis Detail
Patient sitting upright leaning forward. Posterior approach 1 interspace below the top of the effusion (usually 7th–9th intercostal space in the posterior axillary line), over the top of the rib to avoid the neurovascular bundle. Send fluid for Light's criteria to distinguish transudate from exudate: fluid is exudative if any of protein ratio > 0.5, LDH ratio > 0.6, or fluid LDH > 2/3 the upper limit of normal serum LDH. Also send cell count, pH, glucose, Gram stain/culture, cytology. Post-procedure CXR to rule out pneumothorax.
Always document ultrasound guidance, time-out, informed consent, sterile prep, operator, attending supervision, complications, and EBL for every bedside procedure. Missing any of these elements can cause billing rejection or compliance problems.
23 Medications You Must Know
Internal medicine touches almost every non-controlled-substance drug class. Learn the generic-brand mappings and the indication in a sentence.
Cardiovascular
| Class | Examples (generic / brand) | Use |
|---|---|---|
| ACEi | lisinopril (Zestril), enalapril, ramipril | HTN, HFrEF, post-MI, DM nephropathy |
| ARB | losartan (Cozaar), valsartan, irbesartan | Same as ACEi; used when ACEi causes cough |
| ARNI | sacubitril/valsartan (Entresto) | HFrEF — first-line per current guidelines |
| Beta-blocker | metoprolol succ (Toprol XL), carvedilol (Coreg), bisoprolol, atenolol | HTN, HFrEF, CAD, AFib rate control |
| CCB (DHP) | amlodipine (Norvasc), nifedipine | HTN, angina |
| CCB (non-DHP) | diltiazem (Cardizem), verapamil | Rate control in AFib |
| Thiazide | HCTZ, chlorthalidone | HTN first-line |
| Loop diuretic | furosemide (Lasix), torsemide, bumetanide | HF volume overload, edema |
| MRA | spironolactone (Aldactone), eplerenone | HFrEF, resistant HTN, ascites |
| Nitrate | isosorbide mononitrate, SL nitroglycerin | Angina, preload reduction in acute HF |
| Statin | atorvastatin (Lipitor), rosuvastatin (Crestor), pravastatin | Dyslipidemia, secondary prevention |
| Antiplatelet | aspirin, clopidogrel (Plavix), ticagrelor (Brilinta), prasugrel | CAD, post-stent, CVA |
| Anticoagulant | warfarin (Coumadin), apixaban (Eliquis), rivaroxaban (Xarelto), dabigatran (Pradaxa), edoxaban | AFib, VTE, mechanical valves (warfarin) |
Pulmonary
| Class | Examples | Use |
|---|---|---|
| SABA | albuterol (ProAir, Ventolin) | Rescue inhaler, asthma/COPD |
| SAMA | ipratropium (Atrovent) | COPD exacerbation combined with albuterol |
| LABA | salmeterol, formoterol | Maintenance (always with ICS in asthma) |
| LAMA | tiotropium (Spiriva), umeclidinium | COPD maintenance |
| ICS | fluticasone, budesonide, mometasone | Asthma maintenance, COPD with ACO |
| ICS-LABA | fluticasone/salmeterol (Advair), budesonide/formoterol (Symbicort) | Asthma/COPD maintenance |
| Triple therapy | fluticasone/umeclidinium/vilanterol (Trelegy) | Severe COPD |
| Leukotriene modifier | montelukast (Singulair) | Asthma, allergic rhinitis |
| Biologic | omalizumab, mepolizumab, dupilumab | Severe refractory asthma |
GI / Hepatic
| Class | Examples | Use |
|---|---|---|
| PPI | omeprazole, pantoprazole, esomeprazole | GERD, PUD, UGIB, stress ulcer prophylaxis |
| H2 blocker | famotidine (Pepcid) | Dyspepsia, GERD |
| Antiemetic | ondansetron (Zofran), metoclopramide, prochlorperazine | Nausea, gastroparesis |
| Laxative | polyethylene glycol (Miralax), senna, lactulose, bisacodyl, docusate | Constipation, hepatic encephalopathy |
| Antidiarrheal | loperamide | Non-infectious diarrhea |
| Rifaximin | Xifaxan | Hepatic encephalopathy, IBS-D |
Endocrine
| Class | Examples | Use |
|---|---|---|
| Biguanide | metformin (Glucophage) | Type 2 DM first-line |
| SGLT2i | empagliflozin (Jardiance), dapagliflozin (Farxiga) | DM, HF, CKD |
| GLP-1 RA | semaglutide (Ozempic/Wegovy), liraglutide (Victoza), dulaglutide (Trulicity), tirzepatide (Mounjaro/Zepbound) | DM, obesity |
| Basal insulin | glargine (Lantus/Basaglar), detemir (Levemir), degludec (Tresiba) | DM basal coverage |
| Bolus insulin | lispro (Humalog), aspart (Novolog), glulisine (Apidra) | Mealtime/correction dosing |
| Thyroid | levothyroxine (Synthroid) | Hypothyroidism |
| Antithyroid | methimazole, PTU | Hyperthyroidism |
| Steroid | prednisone, methylprednisolone, hydrocortisone, dexamethasone | Inflammatory, adrenal insufficiency, asthma/COPD exacerbation |
Infectious / Other
| Class | Examples | Typical Use |
|---|---|---|
| Penicillin | amoxicillin, amoxicillin-clavulanate (Augmentin), pip-tazo (Zosyn) | CAP, strep, broad spectrum |
| Cephalosporin | cephalexin, cefazolin, ceftriaxone (Rocephin), cefepime | SSTI, CAP, complicated infections |
| Fluoroquinolone | levofloxacin, moxifloxacin, ciprofloxacin | CAP, UTI, intra-abdominal |
| Macrolide | azithromycin, clarithromycin | CAP, atypicals |
| Glycopeptide | vancomycin | MRSA coverage |
| Carbapenem | meropenem, ertapenem | MDR gram-negatives, ESBL |
| TMP-SMX | Bactrim | UTI, MRSA SSTI, PJP |
| Nitrofurantoin | Macrobid | Uncomplicated cystitis |
| Metronidazole | Flagyl | C. diff, anaerobes, BV |
24 Classification & Risk Scores
Internists live inside risk scores and clinical decision rules. Every one of these will come up on rounds. Full enumerations below.
| Letter | Criterion | Points |
|---|---|---|
| C | CHF / LV dysfunction | 1 |
| H | Hypertension | 1 |
| A2 | Age ≥ 75 | 2 |
| D | Diabetes | 1 |
| S2 | Stroke/TIA/thromboembolism | 2 |
| V | Vascular disease (MI, PAD, aortic plaque) | 1 |
| A | Age 65–74 | 1 |
| Sc | Sex category (female) | 1 |
H = Hypertension uncontrolled (1), A = Abnormal renal/liver function (1 each), S = Stroke history (1), B = Bleeding predisposition/history (1), L = Labile INR (1), E = Elderly > 65 (1), D = Drugs/alcohol (1 each). Max 9. Score ≥ 3 = high bleeding risk.
qSOFA: RR ≥ 22, altered mentation, SBP ≤ 100. ≥ 2 = high mortality risk.
SOFA: 6 organ systems scored 0–4: respiration (PaO2/FiO2), coagulation (platelets), liver (bilirubin), CV (MAP/vasopressor), CNS (GCS), renal (Cr/UOP). Increase ≥ 2 from baseline = sepsis.
| Parameter | Range (0 points) |
|---|---|
| RR | 12–20 |
| SpO2 | ≥ 96% |
| O2 supplement | Room air |
| Temp | 36.1–38.0 |
| SBP | 111–219 |
| HR | 51–90 |
| Consciousness | Alert |
Total score triggers escalation: 0–4 (low), 5–6 (medium — urgent team review), ≥ 7 (high — emergency assessment, consider ICU).
CURB-65: Confusion, Urea > 19 mg/dL, RR ≥ 30, BP (SBP < 90 or DBP ≤ 60), age ≥ 65. Each 1 point. 0–1 outpatient, 2 short admission, 3–5 ICU consideration.
PSI / PORT Score: 20 variables (demographics, comorbidities, exam, labs, imaging) produce risk classes I–V; classes IV and V are admitted, class V to ICU.
Wells DVT: Active cancer (+1), paralysis/immobilization (+1), recently bedridden/surgery (+1), localized tenderness (+1), entire leg swollen (+1), calf swelling > 3 cm (+1), pitting edema (+1), collateral superficial veins (+1), prior DVT (+1), alternative dx as likely (−2). ≥ 2 = DVT likely.
Wells PE: Clinical signs of DVT (3), PE most likely dx (3), HR > 100 (1.5), immobilization/surgery < 4 wk (1.5), prior DVT/PE (1.5), hemoptysis (1), malignancy (1). > 6 high, 2–6 moderate, < 2 low.
| Factor | Points |
|---|---|
| Active cancer | 3 |
| Previous VTE | 3 |
| Reduced mobility | 3 |
| Known thrombophilia | 3 |
| Recent trauma/surgery (≤ 1 mo) | 2 |
| Age ≥ 70 | 1 |
| Heart or respiratory failure | 1 |
| Acute MI or stroke | 1 |
| Acute infection or rheumatologic disease | 1 |
| BMI ≥ 30 | 1 |
| Hormonal therapy | 1 |
≥ 4 = high risk, start pharmacologic prophylaxis.
Comprehensive VTE risk assessment for surgical patients. Points awarded for age (0–3), surgery type (1–5), BMI, history of VTE, cancer, central line, immobilization, inherited thrombophilia, pregnancy, hormone therapy, and inflammatory conditions. Score ≥ 5 = high risk; mechanical + pharmacologic prophylaxis. Score 3–4 moderate; 1–2 low; 0 very low.
Weighted score across 19 conditions used to predict 10-year mortality:
| Weight | Conditions |
|---|---|
| 1 | MI, CHF, PVD, CVA, dementia, COPD, connective tissue disease, PUD, mild liver disease, DM |
| 2 | Hemiplegia, moderate-severe CKD, DM with end-organ damage, any tumor, leukemia, lymphoma |
| 3 | Moderate-severe liver disease |
| 6 | Metastatic solid tumor, AIDS |
Plus age adjustment: +1 for every decade over 40 (e.g., 50s +1, 60s +2, 70s +3).
25 Abbreviations Master List
Diagnoses
Labs & Studies
Medications & Orders
26 Sample HPI Templates
These templates show the rhythm and content of real IM notes covering the most common encounter types on both inpatient and outpatient services.
"Mr. [Name] is a 62-year-old male with a PMH of HTN, HLD, type 2 DM (A1C 7.4), 30-pack-year smoking history, and family history of early MI (father, age 58) who presents with 2 hours of substernal chest pressure. The pain began at rest while watching television, is described as 7/10 pressure with radiation to the left jaw and arm, and is associated with diaphoresis and mild dyspnea. He denies syncope, palpitations, or prior similar episodes. He took one of his wife's nitroglycerin tablets without relief. Home medications include lisinopril 20 mg, atorvastatin 40 mg, metformin 1000 mg BID, and aspirin 81 mg. On arrival: BP 162/94, HR 98, RR 18, SpO2 96% on room air. EKG demonstrates 1–2 mm ST depression in V4–V6. Initial high-sensitivity troponin 45 ng/L (ULN 14). HEART score 7. Admitted to telemetry for NSTEMI; cardiology consulted for cath within 24 hours."
"Mrs. [Name] is an 81-year-old female with PMH of dementia, CKD stage 3 (baseline Cr 1.6), DM type 2, and recurrent UTIs who presents from her skilled nursing facility with 1 day of fever, confusion, and decreased oral intake. She is accompanied by her daughter who reports that she has been more lethargic than baseline since yesterday evening. Vitals: T 38.7, HR 112, RR 24, BP 92/54, SpO2 94% room air. Exam shows dry mucous membranes, mild CVA tenderness on the right, and no focal neurologic deficit. qSOFA 2 (RR ≥ 22, altered mentation). Labs: WBC 18.2 with 12% bands, lactate 3.2, Cr 2.4 (up from 1.6), urinalysis with > 100 WBC and positive leukocyte esterase and nitrites. Blood and urine cultures drawn. IV ceftriaxone 1 g started within 45 minutes of presentation. Received 30 mL/kg lactated Ringer's. Admitted for sepsis secondary to complicated UTI/pyelonephritis with AKI on CKD."
"Mr. [Name] is a 74-year-old male with HFrEF (last EF 28%), ischemic cardiomyopathy s/p CABG 2018, HTN, type 2 DM, and CKD stage 3 who presents with 5 days of progressive dyspnea on exertion, 3-pillow orthopnea, PND, and 4 kg weight gain. Denies chest pain, fever, or cough. Reports running out of his furosemide 1 week ago and eating several meals of takeout food over the weekend. Home medications: sacubitril/valsartan 49/51 mg BID, carvedilol 25 mg BID, spironolactone 25 mg daily, dapagliflozin 10 mg, furosemide 40 mg daily, atorvastatin 40 mg, aspirin 81 mg. Exam: BP 148/88, HR 96, RR 22, SpO2 91% room air. JVP elevated at 12 cm, bibasilar crackles to mid-lung fields, S3 gallop, 2+ pitting edema to the knees. BNP 2400 (baseline 800). CXR with pulmonary vascular congestion and bilateral effusions. Troponin negative. Admitted for acute decompensated HFrEF; started on IV furosemide, home GDMT continued, precipitant identified as dietary indiscretion and medication interruption."
"Ms. [Name] is a 68-year-old female returning to primary care 7 days after a 3-day hospitalization for community-acquired pneumonia. She was treated with ceftriaxone and azithromycin and discharged on cefpodoxime to complete a 5-day course. Today she reports significant improvement in cough and dyspnea; occasional productive cough but no fever or pleuritic pain. She is completing the oral antibiotic course without side effects. She is using her albuterol inhaler less often than during the hospital stay. Medication reconciliation performed — patient's home lisinopril and metformin were continued throughout admission. She has no red flags. Lung exam is clear bilaterally. Plan: complete antibiotic course, recheck CXR in 6 weeks given age, ensure pneumococcal and influenza vaccination up to date, and return to usual outpatient follow-up in 3 months."
"Mr. [Name] is a 67-year-old male referred for medical optimization prior to elective total hip arthroplasty scheduled in 3 weeks. PMH is notable for HTN (well-controlled on amlodipine 10 mg), type 2 DM (A1C 6.9 on metformin 1000 mg BID), HLD (on atorvastatin 40 mg), and 30-pack-year smoking history (quit 2015). No prior cardiac history; last stress test 2 years ago was negative. Functional capacity is estimated at > 4 METs (walks 1 mile on flat ground without stopping). RCRI score 1 (insulin-requiring DM × 0, but elevated creatinine × 0, ischemic heart disease × 0, HF × 0, CVA × 0, high-risk surgery × 1 for major orthopedic). No indication for further cardiac testing. Anticoagulation: none. Assessment: low perioperative cardiac risk; continue beta-blocker (none currently), continue statin, hold metformin morning of surgery, resume post-op when eating. VTE prophylaxis per ortho protocol (typically enoxaparin or DOAC). Recommended cleared for surgery."
"Mrs. [Name] is a 72-year-old female returning for routine follow-up of her multiple chronic conditions: HTN, type 2 DM, HFpEF, CKD stage 3a, HLD, and hypothyroidism. Since last visit 3 months ago she reports stable dyspnea on exertion (1 flight of stairs), no orthopedic chest pain, no edema, and good medication adherence. Home glucose log reviewed — fasting 110–140, post-prandial 150–190. Home BP log 128–142/76–84. No symptoms of thyroid derangement. Current medications: losartan 100 mg, amlodipine 5 mg, metoprolol succinate 25 mg, metformin 1000 mg BID, empagliflozin 10 mg, atorvastatin 40 mg, levothyroxine 75 mcg, aspirin 81 mg. Labs today: A1C 7.2 (last 7.5), Cr 1.3 (eGFR 44), K 4.4, LDL 78, TSH 2.8. Exam unremarkable, BP 134/82. Plan: continue current regimen, increase empagliflozin to 25 mg for both glycemic and cardiorenal benefit, reinforce low-sodium and DASH-style diet, ensure age-appropriate cancer screening (due for colonoscopy), update pneumococcal and shingles vaccines, follow up in 3 months with repeat BMP and A1C."
The best IM scribes are pattern recognizers. When the hospitalist says "72 year old with HFrEF, CKD, and DM admitted with SOB, BNP 2800, weight up 5 kg, lasix 40 IV given," you should already know this is an acute HF exacerbation, the A/P will have problems for HF exacerbation (with GDMT and diuresis), CKD (monitor creatinine through diuresis), and DM (hold or continue metformin based on renal function). You should anticipate the attending will ask about precipitants (diet, meds, arrhythmia, infection) and discharge planning.
Know the drug classes cold. When the attending says "bump her metop to 50 BID and add spironolactone 25," you should already know both are GDMT pillars, spironolactone requires K and Cr monitoring, and the discharge summary will need updated reconciliation. Pre-chart the vitals ranges, I/Os, relevant labs, and imaging before rounds so the attending can move through the list efficiently.
Welcome to internal medicine. It is the broadest, most cognitively demanding specialty in adult care — and the scribe sitting next to an excellent internist gets a running master class in clinical reasoning every single day.
27 References & Sources
Clinical Practice Guidelines
Writing Committee. 2023 ACC/AHA/ACCP/ASPC Chest Pain Guideline. Circulation. 2023.
Joglar JA et al. 2023 ACC/AHA/ACCP/HRS Guideline for Atrial Fibrillation. Circulation. 2024.
Whelton PK et al. 2017 ACC/AHA High Blood Pressure Guideline. Hypertension. 2018.
Grundy SM et al. 2018 AHA/ACC Multisociety Guideline on Cholesterol. Circulation. 2019.
GOLD 2024: Global Strategy for Prevention, Diagnosis and Management of COPD.
GINA Global Strategy for Asthma Management and Prevention.
Metlay JP et al. 2019 IDSA/ATS CAP Guideline. Am J Respir Crit Care Med. 2019.
Evans L et al. Surviving Sepsis Campaign: International Guidelines 2021. Crit Care Med. 2021.
KDIGO Clinical Practice Guideline for AKI. Kidney Int Suppl. 2012.
American Diabetes Association. Standards of Care in Diabetes — 2024. Diabetes Care.
Stevens SM et al. CHEST Guideline: Antithrombotic Therapy for VTE. Chest. 2021.
Diagram & Figure Sources
Figure 1: Conduction System of the Heart. OpenStax College. CC BY 3.0.
Figure 2: Major Respiratory Organs. OpenStax College. CC BY 3.0.
Figure 3: Components of the Digestive System. OpenStax College. CC BY 3.0.
Figure 4: The Kidney. OpenStax College. CC BY 3.0.
Figure 5: The Brain. OpenStax College. CC BY 3.0.