OB/GYN
Every obstetric and gynecologic diagnosis, procedure, medication, classification, and documentation framework you need to succeed on day one and beyond.
All diagrams on this page are sourced from published educational or institutional materials rather than AI generation. Each figure caption links to the original source, and the full diagram and guideline citations are collected in the references section at the bottom.
01 Female Reproductive Anatomy — Essentials
OB/GYN covers both obstetrics (pregnancy, labor, delivery, and the postpartum period) and gynecology (the female reproductive tract across the lifespan). A scribe must understand pelvic anatomy cold because virtually every note, exam, ultrasound, and operative dictation will reference it.
External Genitalia (Vulva)
The vulva includes the mons pubis, labia majora (outer folds), labia minora (inner folds), clitoris, vestibule (the area between the labia minora containing the urethral and vaginal openings), and the Bartholin glands (paired glands at 4 and 8 o'clock of the vaginal introitus that can become obstructed and form a Bartholin cyst or abscess). The Skene glands sit alongside the urethra. The perineum is the tissue between the posterior fourchette and the anus and is the site of obstetric lacerations and episiotomies.
Internal Reproductive Organs
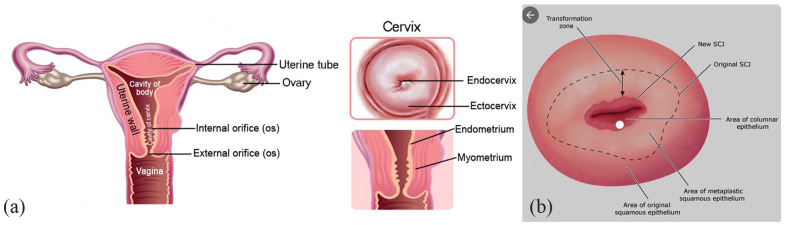
The vagina is a muscular canal approximately 7–10 cm long connecting the introitus to the cervix. The cervix is the lower portion of the uterus, with an external os (facing the vagina) and an internal os (facing the endometrial cavity). The transition between squamous and columnar epithelium is the transformation zone (TZ), where the vast majority of cervical dysplasia and cancers arise — this is why the Pap smear samples this zone.
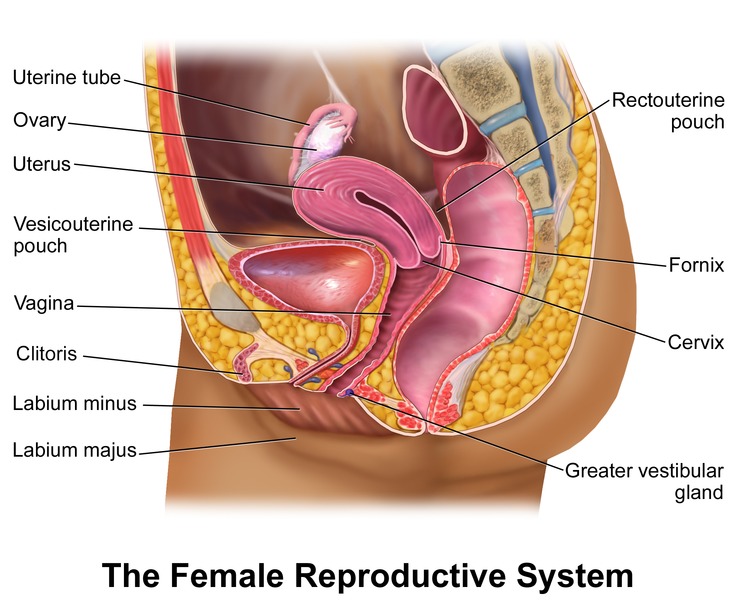
The uterus is a pear-shaped muscular organ with three layers: the inner endometrium (sheds with menses), the middle myometrium (smooth muscle), and the outer perimetrium (serosa). The uterine fundus is the dome, the body is the corpus, and the lower uterine segment transitions into the cervix. Normal position is anteverted and anteflexed; retroverted uteri are a normal variant.
The fallopian tubes extend laterally from the uterine cornua and end in the fimbriae, which sweep ova into the tube. Fertilization typically occurs in the ampulla, the most common site of ectopic implantation. The ovaries sit in the ovarian fossa against the pelvic side wall, suspended by the infundibulopelvic (IP) ligament (carrying the ovarian vessels) and the utero-ovarian ligament.
The Menstrual Cycle
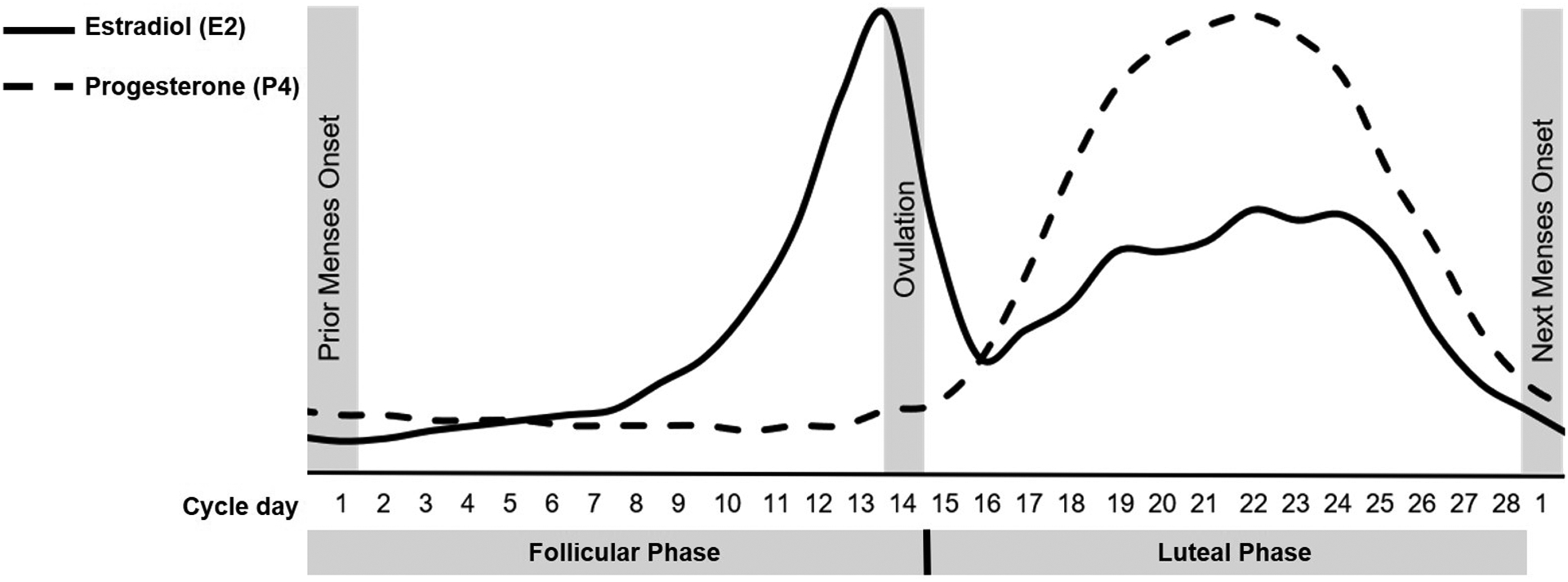
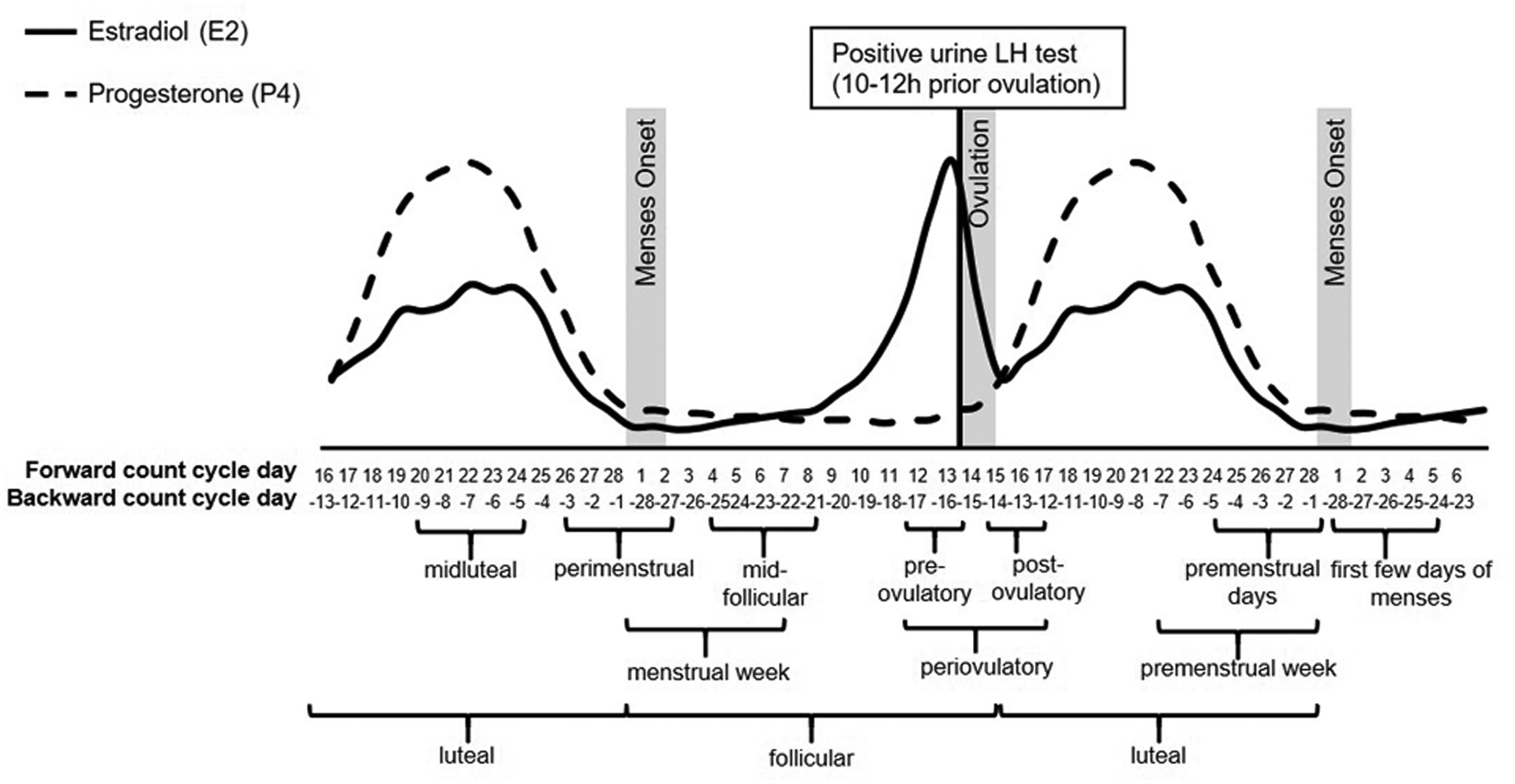
A normal menstrual cycle is 21–35 days with 2–7 days of bleeding. It has two phases driven by the hypothalamic-pituitary-ovarian axis. The follicular phase (day 1 to ovulation) is dominated by FSH, which stimulates follicle growth and rising estradiol. An LH surge triggers ovulation around day 14. The luteal phase follows: the corpus luteum secretes progesterone to prepare the endometrium. Without fertilization, the corpus luteum regresses, progesterone drops, and menstruation begins. Scribes will frequently document "LMP" (last menstrual period) because it anchors pregnancy dating and differential diagnosis of abnormal bleeding.
Know the difference between gestational age (GA) and fetal age. GA is calculated from the first day of the LMP (so at conception the patient is already "2 weeks pregnant"). Fetal age = GA minus 2 weeks. Every OB note uses GA in weeks and days (e.g., "32w4d"). Always write it in that format.
02 Scribe Documentation Framework (OB vs GYN)
OB/GYN notes split into two very different documentation patterns. An OB note centers on the pregnancy — gestational age, fetal status, and any maternal complications. A GYN note behaves more like a general medicine/surgery visit focused on the chief complaint (bleeding, pain, contraception, menopause, cancer screening).
Every obstetric note starts with the same one-line identifier: "G_P_____ at __w__d by __". Example: "32yo G3P1011 at 28w3d by LMP c/w 8w US, presents for routine prenatal visit." The elements: age, gravidity (G = total pregnancies), parity expressed as TPAL (Term, Preterm, Abortions/losses, Living children), current gestational age, and the dating method (LMP, early ultrasound, IVF transfer date).
Always capture: EDD (estimated due date), dating confirmation, prenatal labs status, prior OB history, pertinent complications of this pregnancy, fetal movement, contractions, leaking fluid, vaginal bleeding, and headache/visual changes/epigastric pain (preeclampsia screen).
GYN notes use a standard HPI (OLDCARTS) plus a required GYN history block: LMP, menstrual pattern (cycle length, flow, dysmenorrhea), obstetric history (GTPAL), sexual history (partners, protection, dyspareunia), contraception method, last Pap and result, last mammogram, STI history, and menopausal status. Even a visit for "left breast lump" in a 45-year-old requires this block.
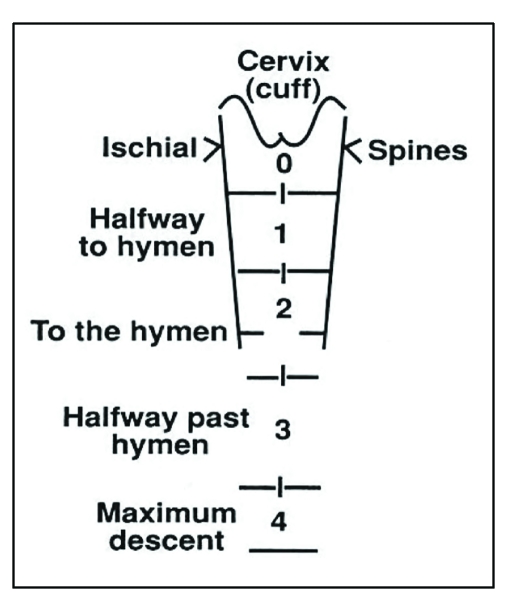
Each prenatal visit captures: BP, weight, urine dip (protein, glucose), fundal height in cm (roughly equal to GA in weeks from 20w onward), fetal heart tones (FHT) in the 110–160 range, fetal movement, and Leopold maneuvers (fetal position) after about 32 weeks. Late pregnancy or symptomatic patients add a cervical exam: dilation (cm), effacement (%), station (-3 to +3), and presenting part.
When the physician says "she is 3/80/-1 vertex," chart it exactly: "Cervix 3 cm dilated, 80% effaced, -1 station, vertex presentation." This shorthand is ubiquitous on labor and delivery and you will hear it dozens of times per shift.
03 Prenatal Care & Routine Obstetric Visits Obstetric
Standard uncomplicated prenatal care consists of a visit schedule from the initial OB intake through delivery. The cadence is approximately every 4 weeks until 28 weeks, every 2 weeks from 28 to 36 weeks, and weekly from 36 weeks to delivery. Each visit has predictable screening and documentation tasks, summarized in ACOG routine prenatal care recommendations.
Gestational Age Dating
Accurate dating is the foundation of every OB decision. The preferred method is LMP confirmed by first-trimester ultrasound. A crown-rump length (CRL) measured before 14 weeks is accurate to within ± 5–7 days. If LMP and ultrasound dating disagree by more than the allowable range, the ultrasound date is used. Dating is "locked" at the initial OB visit and does not change afterward.
First Visit (6–10 Weeks) — OB Intake
The intake visit is the most documentation-heavy encounter of the pregnancy. Labs include CBC, blood type and Rh with antibody screen, rubella and varicella immunity, HIV, RPR/syphilis, hepatitis B surface antigen, hepatitis C, urine culture, gonorrhea/chlamydia, Pap if due, and HbA1C in high-risk patients. Genetic carrier screening (cystic fibrosis, spinal muscular atrophy, hemoglobinopathies, expanded panels) is offered to everyone per ACOG Committee Opinion 690.
Aneuploidy & Anatomy Screening
Prenatal genetic screening options are introduced at the first visit:
- Cell-free DNA (cfDNA, NIPT) — from 10 weeks onward; screens for trisomies 21/18/13 and sex chromosome aneuploidies with the highest sensitivity of any screening test.
- First-trimester combined screen — 11–14 weeks; nuchal translucency (NT) ultrasound + PAPP-A + free β-hCG.
- Quad screen — 15–22 weeks; AFP, hCG, estriol, inhibin A. Elevated AFP flags open neural tube defects.
- Diagnostic testing — CVS (10–13 weeks) or amniocentesis (15+ weeks) provide definitive karyotype.
- Anatomy ultrasound — 18–22 weeks; detailed fetal survey plus placental location.
Second & Third Trimester Screening
At 24–28 weeks, all patients receive a 1-hour 50 g oral glucose challenge test to screen for gestational diabetes. A value ≥ 140 mg/dL triggers the diagnostic 3-hour 100 g GTT. At 28 weeks, Rh-negative patients receive Rho(D) immune globulin (RhoGAM 300 mcg IM), and a repeat antibody screen is drawn. Tdap is given at 27–36 weeks every pregnancy. At 35–37 weeks, a rectovaginal GBS culture is obtained; positive patients receive intrapartum penicillin prophylaxis.
The "prenatal labs status" bar in the EMR is one of the most important documentation elements. Before every visit, skim what labs have resulted since the last visit and what is still pending. The physician will ask about GBS status, 1-hour GTT result, and antibody screen without warning.
04 Hypertensive Disorders of Pregnancy Obstetric
Hypertensive disorders complicate 5–10% of pregnancies and are a leading cause of maternal morbidity. ACOG Practice Bulletin 222 on gestational hypertension and preeclampsia is the governing guideline and defines four overlapping categories.
| Entity | Definition |
|---|---|
| Chronic HTN | BP ≥ 140/90 predating pregnancy or before 20 weeks |
| Gestational HTN | New BP ≥ 140/90 after 20 weeks, no proteinuria, no severe features |
| Preeclampsia | New HTN ≥ 20 weeks + proteinuria (≥ 300 mg/24h or P:Cr ≥ 0.3) or end-organ dysfunction |
| Preeclampsia with severe features | See severe features box below |
| Eclampsia | Preeclampsia + new-onset generalized tonic-clonic seizures |
| HELLP syndrome | Hemolysis, Elevated Liver enzymes, Low Platelets — severe variant |
- BP ≥ 160/110 on two occasions 4 hours apart
- Platelets < 100,000
- AST/ALT > 2× upper limit of normal, severe persistent RUQ/epigastric pain
- Creatinine > 1.1 or doubling of baseline
- Pulmonary edema
- New-onset severe headache unresponsive to medication, visual disturbances (scotomata, blurred vision)
Management
Definitive treatment is delivery. Gestational HTN and preeclampsia without severe features are delivered at 37 weeks; preeclampsia with severe features is delivered at 34 weeks (with betamethasone). Severe-range BP is treated urgently with IV labetalol, IV hydralazine, or oral immediate-release nifedipine. Seizure prophylaxis uses magnesium sulfate (4–6 g IV load, then 1–2 g/hr) continued until 24 hours postpartum; monitor for loss of reflexes and respiratory depression. For chronic HTN, the CHAP trial now supports treating to < 140/90 during pregnancy.
Low-dose aspirin 81 mg daily starting at 12–16 weeks is recommended for preeclampsia prevention in high-risk patients per USPSTF aspirin for preeclampsia prevention.
05 Gestational Diabetes Mellitus (GDM) Obstetric
GDM is glucose intolerance first recognized in pregnancy and affects roughly 6–9% of pregnancies. It increases risk of macrosomia, shoulder dystocia, neonatal hypoglycemia, and future type 2 diabetes per ACOG Practice Bulletin 190.
Screening is universal at 24–28 weeks with the 1-hour 50 g challenge; confirmation uses the 3-hour 100 g GTT. Criteria (Carpenter-Coustan): fasting ≥ 95, 1h ≥ 180, 2h ≥ 155, 3h ≥ 140 — two or more abnormal values confirm GDM. Management begins with medical nutrition therapy and home glucose monitoring (fasting < 95, 1h postprandial < 140, 2h < 120). If targets are not met, insulin is first line; metformin and glyburide are alternatives. Delivery is typically at 39–40 weeks for well-controlled GDM and earlier for poorly controlled or complicated cases. A 6–12 week postpartum 75 g OGTT confirms resolution.
06 Hyperemesis Gravidarum & Intrahepatic Cholestasis Obstetric
Hyperemesis gravidarum is severe nausea and vomiting of pregnancy causing dehydration, electrolyte disturbance, ketonuria, and > 5% weight loss. Stepwise therapy: vitamin B6 (pyridoxine) → add doxylamine → add metoclopramide or promethazine → ondansetron → steroids in refractory cases. IV fluids with thiamine precede dextrose to avoid Wernicke encephalopathy.
Intrahepatic cholestasis of pregnancy (ICP) presents with intense pruritus (often palms/soles) in the third trimester, elevated bile acids, and increased stillbirth risk. Treatment is ursodeoxycholic acid and delivery at 36–37 weeks (earlier for bile acids ≥ 100 µmol/L).
07 Fetal Growth Disorders & Amniotic Fluid Abnormalities Obstetric
Intrauterine growth restriction (IUGR / FGR) is estimated fetal weight < 10th percentile with evidence of pathologic restriction; small for gestational age (SGA) is EFW < 10th percentile (may be constitutional). Large for gestational age (LGA) is EFW > 90th percentile; macrosomia is birth weight > 4000 g (4500 g in diabetics). Surveillance of growth-restricted fetuses uses serial ultrasound plus umbilical artery Doppler and biophysical profile (BPP).
Amniotic fluid is estimated by amniotic fluid index (AFI) or single deepest pocket (SDP). Oligohydramnios (AFI < 5 cm or SDP < 2 cm) is associated with ruptured membranes, placental insufficiency, and renal anomalies. Polyhydramnios (AFI > 24 cm or SDP > 8 cm) is associated with maternal diabetes, fetal anomalies (TE fistula, duodenal atresia), and multiples.
08 Antepartum Bleeding — Previa, Abruption, Vasa Previa Obstetric
- Placenta previa: painless bright red bleeding; placenta covers or is within 2 cm of internal cervical os. NO vaginal exam until previa is excluded by US. Cesarean delivery is mandatory.
- Placental abruption: painful bleeding + uterine tenderness, contractions, "board-like" uterus, non-reassuring FHT. Risk factors: HTN, cocaine, trauma, prior abruption. Bleeding may be concealed.
- Vasa previa: fetal vessels cross the cervical os unprotected by cord or placenta. Rupture of membranes causes fetal (not maternal) exsanguination. Cesarean at 34–36 weeks if diagnosed antenatally.
- Uterine rupture: catastrophic pain, loss of station, fetal distress; most common in TOLAC with prior classical cesarean.
Placenta accreta spectrum (PAS) — accreta, increta, percreta — refers to abnormally adherent/invasive placenta. Risk factors include prior cesarean (especially multiple), placenta previa in a scarred uterus, and prior uterine surgery. Diagnosis is suspected on ultrasound and confirmed on MRI. Planned delivery at a specialized center with cesarean hysterectomy is standard per ACOG Obstetric Care Consensus on placenta accreta spectrum.

09 Early Pregnancy Loss, Ectopic, and Molar Pregnancy Obstetric
Miscarriage Types
| Type | Cervix | Features |
|---|---|---|
| Threatened | Closed | Bleeding, viable IUP on US |
| Inevitable | Open | Bleeding, POC still in uterus |
| Incomplete | Open | Partial passage of POC |
| Complete | Closed | All POC passed, empty uterus on US |
| Missed | Closed | Nonviable pregnancy, no symptoms |
| Septic | Open | Retained POC + infection — emergency |
Management of early pregnancy loss per ACOG Practice Bulletin 200 offers three options: expectant, medical (misoprostol, optionally with mifepristone), or surgical (suction D&C/manual vacuum aspiration). Rh-negative patients receive RhoGAM.
Ectopic Pregnancy
Implantation outside the endometrial cavity; 95% are tubal (most often ampulla). Presents with lower abdominal pain, vaginal bleeding, positive β-hCG with empty uterus (or abnormal hCG rise < 53% in 48 hours). Ruptured ectopic causes hypotension, peritonitis, and hemoperitoneum — a surgical emergency. Stable unruptured ectopics with hCG < 5000, no fetal cardiac activity, and no rupture may be treated with methotrexate; otherwise laparoscopic salpingectomy or salpingostomy.
Gestational Trophoblastic Disease
Complete mole (empty egg + paternal chromosomes, 46XX) and partial mole (triploid) present with markedly elevated hCG, vaginal bleeding, size greater than dates, hyperemesis, and a "snowstorm" on ultrasound. Treatment is suction D&C with serial hCG monitoring to detect persistent trophoblastic disease.
10 Preterm Labor, PROM/PPROM & Chorioamnionitis Obstetric
Preterm labor is regular contractions with cervical change before 37 weeks. PROM is rupture of membranes before labor; PPROM is PROM before 37 weeks. Diagnosis uses pooling of fluid in the posterior fornix, ferning on slide, nitrazine positive (blue), or commercial assays (PAMG-1, IGFBP-1). Avoid digital exam when PPROM is suspected.
Management bundle for preterm labor 24–34 weeks: antenatal corticosteroids (betamethasone 12 mg IM x 2 doses 24 hours apart or dexamethasone), magnesium sulfate for neuroprotection if < 32 weeks, tocolysis (nifedipine or indomethacin < 32 weeks) to allow steroid completion, and GBS prophylaxis. Latency antibiotics (ampicillin + azithromycin, then amoxicillin) are used in PPROM to prolong latency.
Chorioamnionitis (intra-amniotic infection) is diagnosed with maternal fever plus one of: fetal tachycardia, maternal WBC elevation, purulent cervical discharge. Treatment is broad-spectrum IV antibiotics (ampicillin + gentamicin, add clindamycin or metronidazole if cesarean) and delivery.
11 Labor, Delivery & Intrapartum Complications Obstetric
Stages of Labor
- Stage 1 — Latent: onset of regular contractions to 6 cm dilation
- Stage 1 — Active: 6 cm to complete dilation (10 cm)
- Stage 2: complete dilation to delivery of the infant
- Stage 3: delivery of the infant to delivery of the placenta
- Stage 4: first 1–2 hours postpartum (immediate recovery)
Bishop Score — Cervical Favorability for Induction
| Parameter | 0 | 1 | 2 | 3 |
|---|---|---|---|---|
| Dilation (cm) | Closed | 1–2 | 3–4 | ≥ 5 |
| Effacement (%) | 0–30 | 40–50 | 60–70 | ≥ 80 |
| Station | -3 | -2 | -1/0 | +1/+2 |
| Consistency | Firm | Medium | Soft | — |
| Position | Posterior | Mid | Anterior | — |
Bishop score ≥ 8 predicts successful induction; < 6 typically requires cervical ripening (misoprostol, dinoprostone, or Foley balloon).
Leopold Maneuvers & Fetal Position
Four palpations of the gravid uterus to determine fetal lie, presentation, and position: (1) fundal — what is in the fundus; (2) lateral — which side is fetal back; (3) suprapubic (Pawlik) — presenting part; (4) pelvic — engagement and flexion.
Fetal Heart Tracing Categories
Continuous EFM is interpreted by the NICHD three-tier system. Category I (normal) has baseline 110–160, moderate variability, no late/variable decelerations, accelerations present or absent. Category III (abnormal) has absent variability with recurrent late or variable decelerations or bradycardia, or a sinusoidal pattern. Category II is everything in between. Category III requires immediate intrauterine resuscitation and delivery if not resolved.
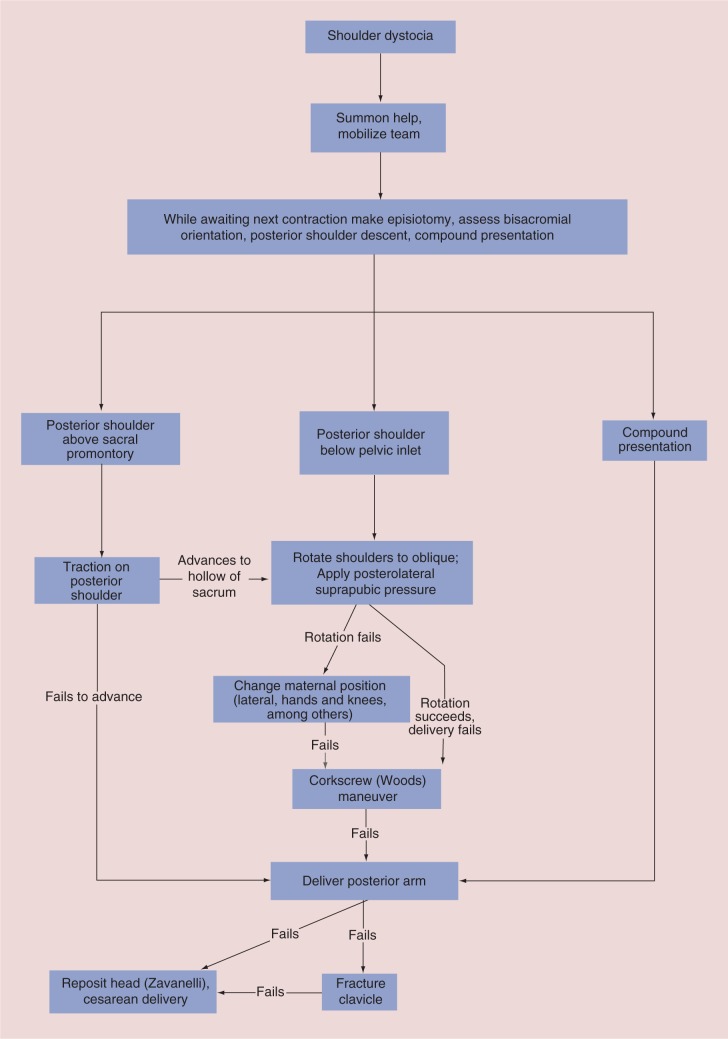
- Shoulder dystocia: head delivers but shoulder impacted behind pubic symphysis. Maneuvers: McRoberts, suprapubic pressure, Rubin, Woods corkscrew, delivery of posterior arm, Gaskin (all-fours), Zavanelli (last resort).
- Cord prolapse: umbilical cord precedes the presenting part through the cervix; obstetric emergency requiring elevation of the presenting part and immediate cesarean.
- Breech presentation: frank, complete, or footling. External cephalic version (ECV) offered at 37 weeks; cesarean is the usual delivery mode in the US.
- Labor dystocia (failure to progress): arrest of dilation (≥ 6 cm with no change for 4 hrs with adequate contractions) or arrest of descent in stage 2.
Apgar Score
| Sign | 0 | 1 | 2 |
|---|---|---|---|
| Appearance (color) | Blue/pale | Acrocyanotic | Fully pink |
| Pulse (HR) | Absent | < 100 | ≥ 100 |
| Grimace (reflex) | None | Grimace | Cry/cough |
| Activity (tone) | Limp | Some flexion | Active motion |
| Respiration | Absent | Weak/irregular | Strong cry |
Assessed at 1 and 5 minutes (and at 10 minutes if the 5-minute score is < 7).
12 Postpartum Care & Complications Obstetric
Postpartum Hemorrhage (PPH)
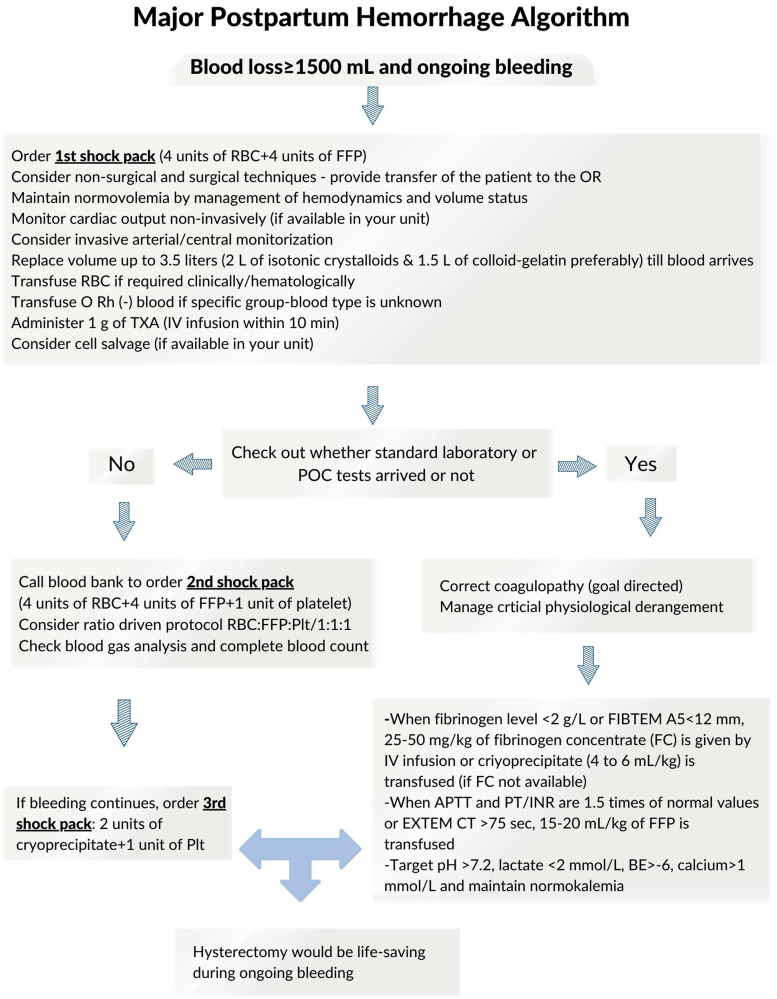
Defined as cumulative blood loss ≥ 1000 mL or blood loss with signs of hypovolemia within 24 hours of birth. Causes follow the Four T's: Tone (uterine atony — 70% of cases), Trauma (lacerations, hematoma), Tissue (retained placenta), Thrombin (coagulopathy). Management per ACOG Practice Bulletin 183 is stepwise: bimanual massage, uterotonics (oxytocin first line, then methylergonovine — avoid in HTN, carboprost/Hemabate — avoid in asthma, misoprostol), tranexamic acid, uterine tamponade (Bakri balloon), B-Lynch suture, uterine artery embolization, and hysterectomy as last resort.
Other Postpartum Conditions
- Endometritis: postpartum fever + uterine tenderness + foul lochia; risk higher after cesarean. Treat with IV clindamycin + gentamicin.
- Mastitis: unilateral breast erythema, tenderness, fever; typically Staph aureus. Treat with dicloxacillin or cephalexin and continued breastfeeding/pumping.
- Postpartum depression: screened with EPDS at postpartum visits. "Baby blues" resolve by 2 weeks; major depression persists and requires treatment (SSRIs, therapy).
- Postpartum preeclampsia: can develop up to 6 weeks postpartum; severe headache/HTN after discharge warrants urgent evaluation.
- Breastfeeding issues: latch difficulty, engorgement, cracked nipples, low supply — lactation referral.
13 Abnormal Uterine Bleeding (PALM-COEIN) Gynecologic
Per FIGO and ACOG PALM-COEIN classification, abnormal uterine bleeding in reproductive-age women is categorized by structural (PALM) and non-structural (COEIN) causes.
| Structural (PALM) | Non-structural (COEIN) |
|---|---|
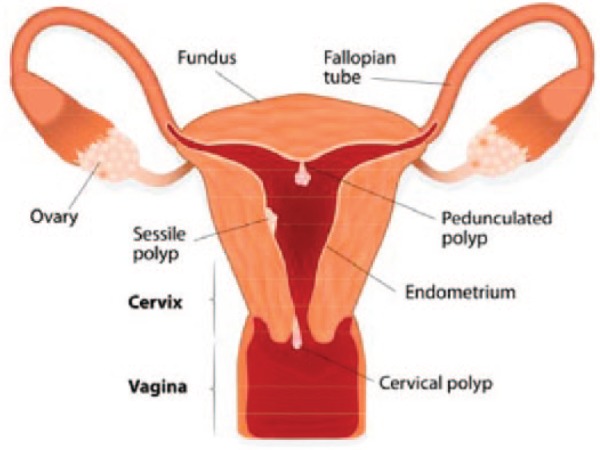
| P — Polyp | C — Coagulopathy |
| A — Adenomyosis | O — Ovulatory dysfunction |
| L — Leiomyoma (fibroid) | E — Endometrial |
| M — Malignancy/hyperplasia | I — Iatrogenic |
| N — Not yet classified |
Workup includes β-hCG (rule out pregnancy), CBC, TSH, prolactin, and pelvic ultrasound. Endometrial biopsy is indicated in women ≥ 45 with AUB, any woman with risk factors for endometrial cancer (obesity, PCOS, tamoxifen, chronic anovulation, Lynch syndrome), or any postmenopausal bleeding. Treatment depends on etiology: combined OCPs, levonorgestrel IUD, tranexamic acid, NSAIDs for dysfunctional/heavy menstrual bleeding; hysteroscopic resection for polyps/submucosal fibroids; myomectomy or hysterectomy for symptomatic fibroids.
14 Contraception — Every Method Gynecologic
Contraception counseling uses the tiered effectiveness framework from the CDC US Medical Eligibility Criteria. LARCs (IUDs, implant) are the most effective reversible methods.
| Method | Type | Duration |
|---|---|---|
| Copper IUD (Paragard) | Non-hormonal LARC | Up to 10–12 years |
| Levonorgestrel IUD (Mirena, Liletta, Kyleena, Skyla) | Progestin LARC | 3–8 years |
| Etonogestrel implant (Nexplanon) | Progestin LARC | 3–5 years |
| DMPA (Depo-Provera) | IM progestin injection | Every 13 weeks |
| Combined OCPs | Estrogen + progestin pill | Daily |
| Progestin-only pill (POP / "mini-pill") | Daily progestin | Daily (strict timing) |
| Transdermal patch (Xulane, Twirla) | Combined hormonal | Weekly |
| Vaginal ring (NuvaRing, Annovera) | Combined hormonal | 3 weeks in / 1 off (or yearly) |
| Condoms, diaphragm, cervical cap | Barrier | Per act |
| BTL / salpingectomy | Permanent | Permanent |
| Vasectomy (partner) | Permanent | Permanent |
| Emergency contraception — Ulipristal (Ella), levonorgestrel (Plan B), copper IUD | Post-coital | Within 72–120 hours |
Combined hormonal methods are contraindicated in women with migraine with aura, uncontrolled hypertension, smokers ≥ 35, history of VTE, breast cancer, or < 3 weeks postpartum. The progestin-only and non-hormonal options are used in these patients.
15 PCOS, Endometriosis, Adenomyosis & Fibroids Gynecologic
Polycystic Ovary Syndrome (PCOS)
A heterogeneous endocrine disorder affecting 6–12% of reproductive-age women. Diagnosis uses the Rotterdam criteria: 2 of 3 of (1) oligo/anovulation, (2) clinical or biochemical hyperandrogenism, (3) polycystic ovaries on ultrasound (≥ 12 follicles or ovarian volume > 10 mL). Associated with insulin resistance, obesity, infertility, and metabolic syndrome. Management includes lifestyle, combined OCPs (menstrual regulation, androgen suppression), metformin, spironolactone for hirsutism, and letrozole for ovulation induction.
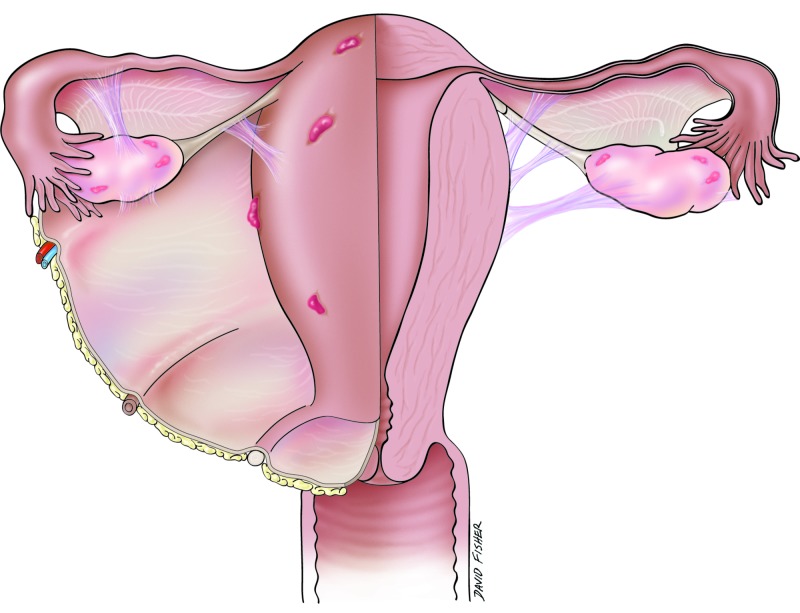
Endometriosis
Ectopic endometrial tissue outside the uterus causing chronic pelvic pain, dysmenorrhea, dyspareunia, and infertility. "Gold standard" diagnosis is laparoscopy with biopsy but empiric treatment is common. Therapies: NSAIDs, combined OCPs (continuous), progestins, GnRH agonists (leuprolide) or antagonists (elagolix), and surgical excision/ablation.
Adenomyosis
Endometrial glands within the myometrium producing a diffusely enlarged "boggy" uterus, heavy bleeding, and dysmenorrhea. MRI shows junctional zone thickening. Definitive treatment is hysterectomy; conservative options include levonorgestrel IUD and GnRH analogs.
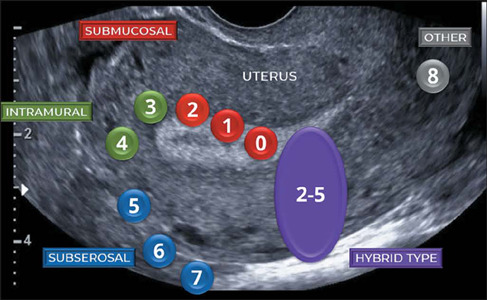
Uterine Fibroids (Leiomyomas)
Benign smooth muscle tumors classified by location: subserosal, intramural, submucosal (FIGO 0–8 system). Symptoms depend on location: submucosal causes heavy bleeding, subserosal causes bulk symptoms. Treatment ranges from expectant management to hormonal suppression, uterine artery embolization, myomectomy, or hysterectomy.
16 Ovarian Cysts, Torsion & PID Gynecologic
Physiologic cysts (follicular, corpus luteum) resolve spontaneously. Hemorrhagic cysts present with acute unilateral pain. Pathologic cysts include endometriomas ("chocolate cysts"), dermoids (mature cystic teratomas), and cystadenomas. Simple cysts < 5 cm in premenopausal women can be observed; complex or persistent cysts warrant further workup with CA-125 and possible surgery.
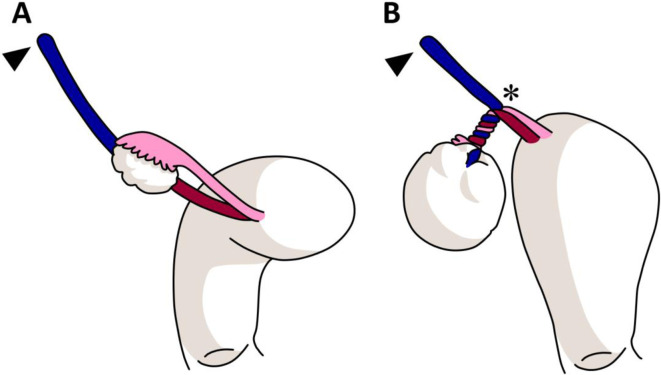
Sudden severe unilateral pelvic pain with nausea/vomiting, often with an adnexal mass. Doppler US may show absent arterial or venous flow (can be preserved in early torsion — clinical suspicion overrides imaging). Treatment is emergent laparoscopic detorsion with ovarian preservation whenever possible.
Pelvic Inflammatory Disease (PID)
Ascending infection of the upper genital tract, typically polymicrobial with gonorrhea and chlamydia as primary organisms. Presents with lower abdominal pain, cervical motion tenderness ("chandelier sign"), adnexal tenderness, fever, and purulent discharge. Tubo-ovarian abscess (TOA) is a severe complication. Outpatient regimen: ceftriaxone 500 mg IM + doxycycline 100 mg BID x 14 days +/- metronidazole. Inpatient: IV cefoxitin + doxycycline. Long-term sequelae include infertility, ectopic, and chronic pelvic pain.
17 Vaginitis, Cervicitis & Vulvar Disorders Gynecologic
| Condition | Discharge | pH | Microscopy | Treatment |
|---|---|---|---|---|
| Bacterial vaginosis (BV) | Thin gray, fishy odor | > 4.5 | Clue cells, positive whiff test | Metronidazole PO/gel or clindamycin |
| Candidiasis | Thick white "cottage cheese" | < 4.5 | Pseudohyphae, budding yeast | Fluconazole 150 mg PO x 1, topical azoles |
| Trichomoniasis | Frothy yellow-green, "strawberry" cervix | > 4.5 | Motile trichomonads | Metronidazole 500 mg BID x 7 days; treat partner |
Cervicitis is commonly gonococcal or chlamydial; test with NAAT and treat empirically (ceftriaxone 500 mg IM + doxycycline). Bartholin abscess is managed with incision and drainage plus Word catheter placement or marsupialization for recurrent cases. Vulvar disorders include lichen sclerosus (classic "figure-of-8" white plaques, treat with high-potency topical steroids), lichen planus, vulvodynia, and VIN (vulvar intraepithelial neoplasia).
18 Cervical, Endometrial & Ovarian Cancer Gynecologic
Cervical Cancer & Screening
Essentially all cervical cancer is caused by persistent high-risk HPV infection (especially 16 and 18). Screening per USPSTF cervical cancer screening and ASCCP 2019 risk-based management guidelines:
- Ages 21–29: cytology every 3 years
- Ages 30–65: cytology every 3 years, hrHPV every 5 years, or co-testing every 5 years
- > 65 or post-hysterectomy (benign): may discontinue with adequate prior screening
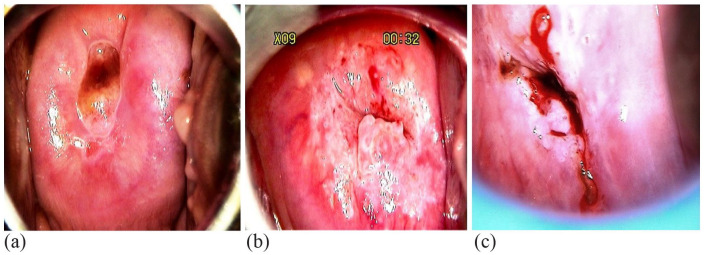
Abnormal Pap results (ASC-US, LSIL, ASC-H, HSIL, AGC) are managed by ASCCP risk estimates, which may lead to colposcopy with biopsy, endocervical curettage, and LEEP/cone biopsy for high-grade lesions.
| Stage | Description |
|---|---|
| I | Confined to cervix |
| II | Beyond cervix but not to pelvic wall or lower third of vagina |
| III | Extends to pelvic wall, lower third of vagina, or causes hydronephrosis; pelvic/para-aortic nodes |
| IV | Invades bladder/rectum (IVA) or distant metastasis (IVB) |
Endometrial Cancer
The most common gynecologic malignancy in the US. Type I (endometrioid, estrogen-driven) is most common and associated with obesity, unopposed estrogen, PCOS, tamoxifen, Lynch syndrome. Classic presentation is postmenopausal bleeding — which always requires endometrial sampling. FIGO stages I–IV parallel cervical staging, with stage I confined to the uterus. Management centers on total hysterectomy with bilateral salpingo-oophorectomy (TH/BSO) and lymph node assessment.
Ovarian Cancer (Overview)
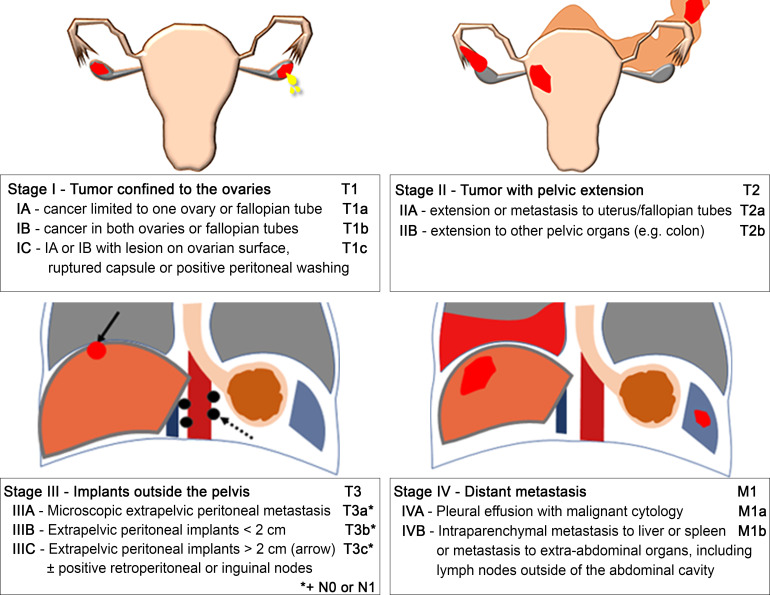
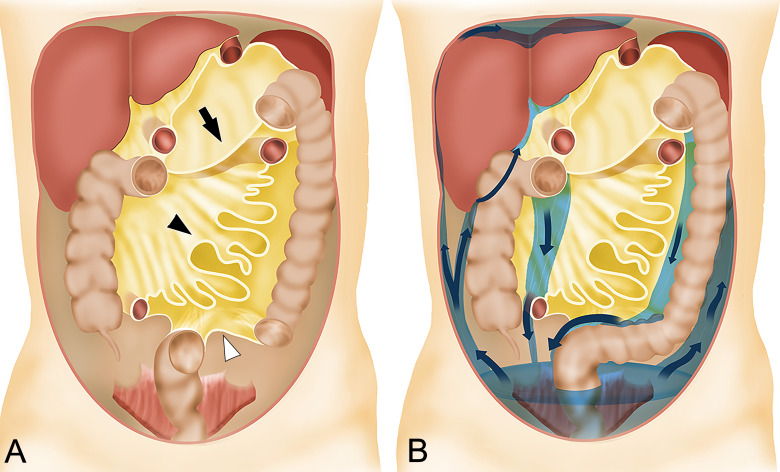
Epithelial ovarian cancer typically presents late with vague abdominal bloating, early satiety, and pelvic mass. CA-125 is used for monitoring, not screening. Risk factors include BRCA1/BRCA2 mutations, Lynch syndrome, nulliparity, and endometriosis. FIGO stage I confined to ovaries, II pelvic extension, III peritoneal/retroperitoneal spread, IV distant metastases. Treatment combines cytoreductive surgery and platinum-based chemotherapy per NCCN Guidelines on Ovarian Cancer.
Breast Cancer Screening
USPSTF 2024 breast cancer screening recommends biennial screening mammography beginning at age 40 through 74. BRCA1/BRCA2 risk assessment and genetic counseling are recommended for women with relevant family history per USPSTF BRCA-related cancer recommendations.
19 Pelvic Organ Prolapse & Urinary Incontinence Gynecologic
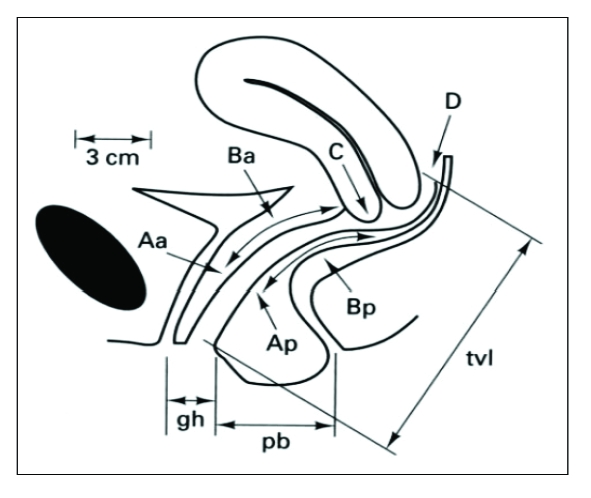
Pelvic organ prolapse (POP) is descent of pelvic organs into the vaginal canal: cystocele (bladder), rectocele (rectum), enterocele (small bowel), uterine prolapse, and vaginal vault prolapse. Quantified by the POP-Q system. Symptoms: vaginal bulge, pressure, splinting to void/defecate, dyspareunia. Treatment ranges from pelvic floor PT and pessary to surgical repair (anterior/posterior colporrhaphy, sacrocolpopexy, uterosacral or sacrospinous ligament suspension).
Urinary Incontinence
- Stress UI: leakage with cough/sneeze/exercise from urethral hypermobility or intrinsic sphincter deficiency. Treatment: Kegels, pessary, urethral bulking, midurethral sling.
- Urge UI (overactive bladder): sudden urge with leakage. Treatment: behavioral therapy, antimuscarinics (oxybutynin, tolterodine), β3-agonists (mirabegron), Botox, sacral neuromodulation.
- Mixed UI: features of both.
- Overflow UI: incomplete emptying with dribbling.
20 Menopause, HRT & Infertility Workup Gynecologic
Menopause is defined as 12 months of amenorrhea, average age 51. Symptoms include vasomotor (hot flashes, night sweats), genitourinary syndrome of menopause (vaginal dryness, dyspareunia, urinary urgency), sleep disturbance, and mood changes. FSH is elevated but is not required for diagnosis in typical cases.
Hormone therapy per The Menopause Society (NAMS) 2022 Position Statement: systemic estrogen (with progestin if uterus present) is the most effective treatment for vasomotor symptoms in women < 60 or within 10 years of menopause without contraindications. Vaginal (low-dose) estrogen treats GSM without systemic risk. Non-hormonal alternatives: SSRIs/SNRIs (paroxetine is FDA-approved), gabapentin, oxybutynin, fezolinetant.
Infertility Workup Overview
Infertility is failure to conceive after 12 months of unprotected intercourse (6 months if ≥ 35). Workup evaluates three domains: ovulatory function (mid-luteal progesterone, menstrual history), tubal/uterine anatomy (hysterosalpingogram, saline infusion sonohysterography), and semen analysis. Advanced therapy includes clomiphene/letrozole ovulation induction, IUI, and IVF. Recurrent pregnancy loss (RPL) is 2 or more clinical losses and triggers a workup for parental karyotypes, uterine anatomy, antiphospholipid syndrome, and thyroid/diabetes control.
21 OB/GYN Procedures — A to Z
| Procedure | Description / Indication |
|---|---|
| Cervical cytology (Pap) | Sampling of ectocervix + endocervical canal for cytology/HPV testing |
| Colposcopy | Magnified cervical exam with acetic acid/Lugol's; directed biopsies of abnormal areas |
| LEEP / cone biopsy | Electrosurgical or cold-knife excision of cervical dysplasia (CIN 2/3, AIS) |
| Endometrial biopsy | Office suction sampling of endometrium with Pipelle for AUB/postmenopausal bleeding |
| IUD insertion / removal | Levonorgestrel or copper; placed through cervix into endometrial cavity |
| Nexplanon insertion/removal | Subdermal etonogestrel rod in upper inner arm |
| Hysteroscopy | Camera through cervix into uterine cavity; diagnostic or operative (polyp/fibroid resection) |
| D&C (dilation and curettage) | Mechanical dilation of cervix + sharp/suction curettage; used for EPL, AUB, retained POC |
| Suction D&C / MVA | Manual or electric vacuum aspiration for early pregnancy loss or molar evacuation |
| Hysterectomy — total/supracervical, vaginal, abdominal, laparoscopic, robotic | Removal of the uterus +/- cervix via various approaches |
| BSO / oophorectomy / salpingectomy | Removal of ovaries, tubes, or both — for cysts, cancer, BRCA risk reduction, ectopic, BTL |
| Myomectomy | Fibroid removal preserving the uterus; hysteroscopic, laparoscopic, or open |
| Anterior / posterior colporrhaphy | Cystocele / rectocele repair |
| Sacrocolpopexy | Mesh suspension of vaginal vault to sacrum for prolapse |
| Midurethral sling | Transvaginal tape/obturator tape for stress incontinence |
| BTL (tubal ligation) / bilateral salpingectomy | Permanent contraception; salpingectomy now preferred for ovarian cancer risk reduction |
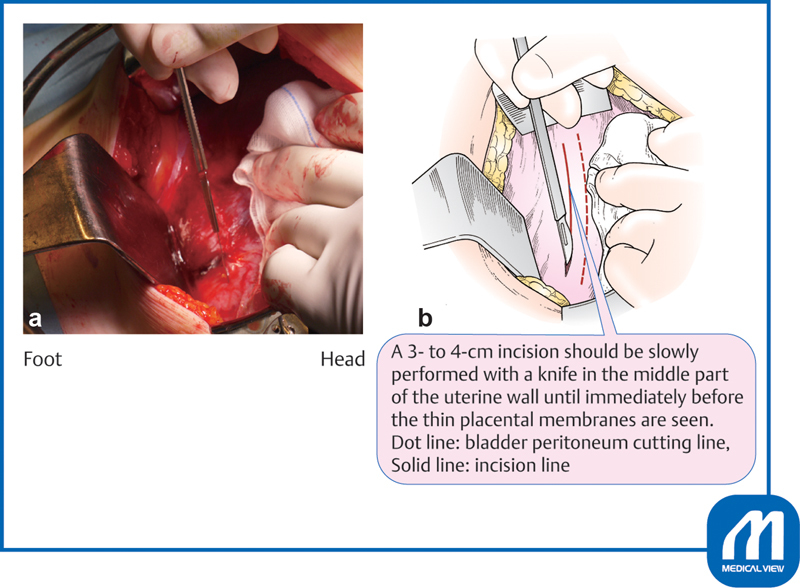
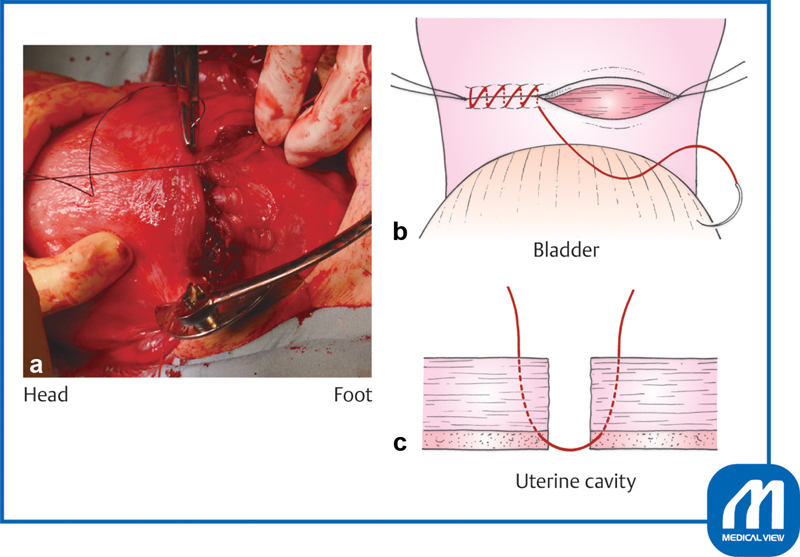
| Cesarean section | Low transverse (most common) or classical uterine incision; indications include arrest, non-reassuring FHT, malpresentation, previa |
| Operative vaginal delivery | Vacuum or forceps assistance when second-stage arrest or fetal distress at low station |
| Episiotomy / perineal repair | Midline or mediolateral; repair graded 1st–4th degree laceration |
| Bartholin I&D / Word catheter / marsupialization | Drainage and prevention of Bartholin abscess recurrence |
| Amniocentesis / CVS | Genetic diagnostic sampling of amniotic fluid (15+ wk) or placental villi (10–13 wk) |
| External cephalic version (ECV) | Manual transabdominal rotation of breech to cephalic at ~37 wks |
| Cerclage | Cervical stitch for cervical insufficiency (McDonald or Shirodkar) |
Perineal laceration grading: 1st = skin/vaginal mucosa only; 2nd = perineal body muscles; 3rd = external anal sphincter involved (3a < 50%, 3b > 50%, 3c includes internal sphincter); 4th = through rectal mucosa.
22 Labs, Imaging & Screening
OB-Specific Labs & Tests
- Quantitative β-hCG: detects pregnancy at ~8–10 days post-conception. In a viable IUP, hCG rises by at least 53% every 48 hours in early pregnancy. Plateau or slow rise raises concern for ectopic or nonviable IUP.
- Discriminatory zone: β-hCG ≥ 3500 with no IUP on transvaginal US is concerning for ectopic.
- Blood type / antibody screen: identifies Rh status and alloimmunization.
- 1h / 3h GTT: GDM screening.
- Maternal serum AFP: elevated in neural tube defects, multiples, abdominal wall defects.
- Cell-free DNA (NIPT): aneuploidy screen from maternal plasma.
- GBS culture: rectovaginal swab at 35–37 weeks.
- Fetal fibronectin (fFN): negative test helps exclude preterm delivery within 7–14 days.
- Biophysical profile (BPP): 5-component test (tone, movement, breathing, fluid, NST); each 0 or 2, max score 10.
- Non-stress test (NST): reactive = ≥ 2 accelerations > 15 bpm for > 15 sec in 20 min.
GYN Imaging
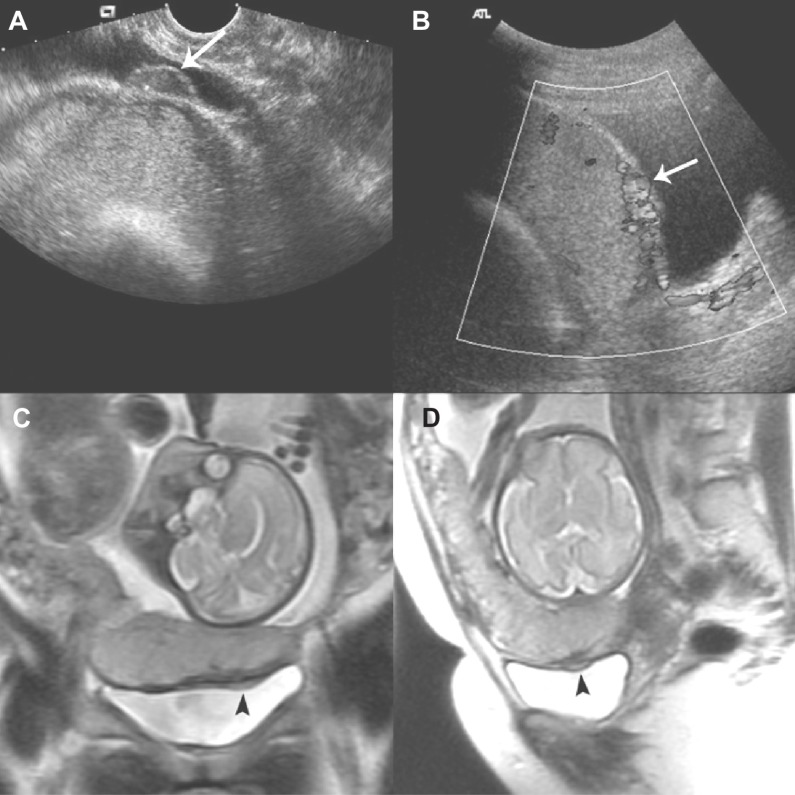
Transvaginal ultrasound (TVUS) is the workhorse of gynecology. Endometrial thickness > 4 mm in a postmenopausal woman with bleeding requires sampling. Saline infusion sonohysterography (SIS) distends the cavity to identify polyps and submucosal fibroids. Hysterosalpingogram (HSG) assesses tubal patency in infertility. Pelvic MRI evaluates complex pelvic masses, adenomyosis, and placenta accreta spectrum.
23 Medications You Must Know
| Class / Indication | Generic (Brand) | Notes |
|---|---|---|
| Prenatal vitamin | PNV with folic acid 400–800 mcg | 4 mg in prior NTD history |
| Iron | Ferrous sulfate, ferrous gluconate, IV iron sucrose | For anemia of pregnancy |
| Antiemetic (N/V of pregnancy) | Vit B6 + doxylamine (Diclegis), ondansetron, promethazine | Step-up therapy |
| BP — pregnancy | Labetalol, nifedipine XL, methyldopa, hydralazine (IV) | Avoid ACE/ARB in pregnancy |
| Preeclampsia seizure ppx | Magnesium sulfate | Monitor DTRs, respiratory rate |
| Tocolytics | Nifedipine, indomethacin (< 32 wk), terbutaline | Magnesium for neuroprotection < 32 wk |
| Antenatal steroids | Betamethasone, dexamethasone | Fetal lung maturation 24–34 wk |
| Induction / augmentation | Oxytocin (Pitocin), misoprostol, dinoprostone, Foley bulb | Misoprostol contraindicated with prior cesarean |
| Uterotonics for PPH | Oxytocin, methylergonovine (avoid HTN), carboprost/Hemabate (avoid asthma), misoprostol, tranexamic acid | Order of use depends on contraindications |
| Rh prophylaxis | Rho(D) immune globulin (RhoGAM) | 28 wks + within 72 hrs of delivery/bleeding |
| GBS prophylaxis | Penicillin G (cefazolin, clindamycin, vancomycin) | Allergy-dependent choice |
| Ectopic pregnancy | Methotrexate | Stable unruptured ectopic, hCG < 5000 |
| Combined OCPs | EE + levonorgestrel/norethindrone/drospirenone | Contraindicated in migraine w/aura, smokers ≥ 35 |
| Progestin-only | Norethindrone (POP), DMPA, LNG-IUD, Nexplanon | Safe in breastfeeding, HTN, migraine with aura |
| Emergency contraception | Ulipristal (Ella), levonorgestrel (Plan B), copper IUD | Copper IUD most effective |
| Menopause HRT | Estradiol +/- progestin, conjugated estrogens, vaginal estrogen | Uterus present → add progestin |
| Endometriosis | OCPs, progestins, GnRH agonists (leuprolide), GnRH antagonists (elagolix) | Add-back therapy to limit bone loss |
| Vaginitis / STI | Metronidazole (BV, trich), fluconazole (yeast), ceftriaxone + doxycycline (GC/CT/PID) | Treat partners when indicated |
24 Classification Systems & Physical Exam
Key Classification Systems (Full Enumeration)
All of the following are fully enumerated in the sections where they first appear: PALM-COEIN (Section 13), Bishop score (Section 11), FIGO cervical/endometrial/ovarian staging (Section 18), Rotterdam criteria for PCOS (Section 15), severe features of preeclampsia (Section 4), Apgar score (Section 11), Leopold maneuvers (Section 11), NICHD fetal heart tracing categories (Section 11), and perineal laceration grades (Section 21).
The OB/GYN Physical Exam
General: well-appearing, NAD. Abdomen: soft, nondistended, nontender, no masses or hepatosplenomegaly. External genitalia: normal BUS (Bartholin/urethra/Skene), no lesions or erythema. Speculum: vagina pink without lesions, cervix parous/nulliparous appearing, no discharge/friability/CMT. Bimanual: cervix firm and mobile, no CMT, uterus anteverted, mobile, normal size, nontender; adnexa without masses or tenderness bilaterally. Rectovaginal (if indicated): no masses, confirms posterior findings.
BP / wt / urine dip. Fundal height: __ cm (= __ wks). FHT: __ bpm by Doppler. Presentation: vertex/breech/transverse by Leopold. Contractions: present/absent, frequency. Vaginal bleeding / leakage of fluid: denied. Fetal movement: +. Cervical exam (if indicated): __ cm / __% / __ station, presenting part __.
25 Abbreviations Master List
Obstetrics
Gynecology
26 Sample HPI Templates
These templates show the kind of documentation expected in OB/GYN clinic and L&D. Use them as frameworks to internalize the rhythm and content of a good OB or GYN HPI.
"Ms. [Name] is a 29-year-old G2P1001 at 9w2d by LMP c/w 8w6d TVUS presenting for initial OB intake. Pregnancy is intended and desired. LMP 8 weeks ago, positive home pregnancy test 4 weeks ago. She reports mild nausea without vomiting, fatigue, and breast tenderness. Denies vaginal bleeding, cramping, dysuria, fever, or chills. Prior OB: NSVD 2022 at 39w2d, uncomplicated, male infant 3400 g. No prior losses. GYN history: regular 28-day cycles, last Pap 2023 NILM with negative hrHPV, LARC removed 3 months ago. PMH unremarkable. Takes prenatal vitamin with folic acid 800 mcg daily. Denies tobacco, alcohol, or illicit drug use. Rh status and initial labs pending today."
"Ms. [Name] is a 42-year-old G3P3003 with a 6-month history of heavy irregular menstrual bleeding. She describes cycles ranging 21–45 days with 8–10 days of heavy flow requiring double protection and passing golf-ball sized clots. She reports dysmenorrhea rated 7/10 relieved partially by ibuprofen. Denies postcoital bleeding, dyspareunia, hot flashes, or weight changes. Pregnancy test negative. Last Pap 2024 normal. No prior fibroid history. PMH: obesity (BMI 34), prediabetes. Meds: metformin 500 mg BID. Family history of endometrial cancer in mother at 68. Referred for evaluation; TVUS today shows 7 cm fundal intramural fibroid and endometrial stripe of 12 mm."
"Ms. [Name] is a 24-year-old G0 presenting for contraception counseling. She has been using condoms inconsistently and desires long-acting reversible contraception. Cycles regular every 30 days with moderate flow and mild dysmenorrhea. LMP 2 weeks ago. No history of STIs; most recent GC/CT NAAT 6 months ago negative. No dyspareunia, abnormal discharge, or postcoital bleeding. PMH: migraine without aura. Non-smoker. She is interested in Nexplanon versus LNG-IUD; counseled on effectiveness, side effects, insertion process, and return-to-fertility for each. Elects to proceed with 52-mg levonorgestrel IUD today."
"Ms. [Name] is a 34-year-old G1P0 at 34w1d by 8w US with history of chronic HTN on labetalol 200 mg BID, presenting to L&D for new-onset severe headache and blurred vision. BP on arrival 172/108 and 168/106 repeated 15 minutes later. Reports progressive bifrontal headache x 12 hours unresponsive to acetaminophen, intermittent scotomata, and RUQ discomfort. Denies contractions, leakage of fluid, or vaginal bleeding. Fetal movement present. Labs notable for platelets 92, AST 140, ALT 128, Cr 1.0 (baseline 0.7), urine P:Cr 0.6. Diagnosis: preeclampsia with severe features. Magnesium sulfate and IV labetalol initiated; betamethasone given; planning delivery."
"Ms. [Name] is a 31-year-old G2P2002 now 6 weeks s/p uncomplicated NSVD at 39w5d with 2nd-degree laceration, presenting for routine postpartum visit. Lochia resolved at week 4. Denies fever, foul discharge, heavy bleeding, dysuria, or calf pain. Breastfeeding exclusively with adequate supply and no mastitis symptoms. EPDS score 4 — no depression symptoms. Resumed intercourse — requests contraception, interested in progestin-only options given lactation. Perineum well healed. No diastasis concerns. Counseled on contraception, return to exercise, and pelvic floor PT if leakage."
"Ms. [Name] is a 53-year-old G2P2002 with 14 months of amenorrhea presenting with bothersome vasomotor symptoms. Reports 8–12 hot flashes daily with drenching night sweats disrupting sleep. Also notes vaginal dryness and dyspareunia. Denies postmenopausal bleeding. Last mammogram 8 months ago — negative. Last Pap with hrHPV 2023 negative. PMH: HLD on rosuvastatin. No personal or family history of breast cancer, VTE, stroke, or CAD. BMI 26. Non-smoker. Counseled on risks/benefits of systemic HT; given timing (< 10 years from menopause, age < 60), she is an appropriate candidate. Starting transdermal estradiol 0.05 mg patch with oral micronized progesterone 100 mg nightly; vaginal estrogen tablets for GSM."
27 References & Sources
Clinical Practice Guidelines
ACOG Practice Bulletin 222. Gestational Hypertension and Preeclampsia. Obstet Gynecol. 2020.
ACOG Practice Bulletin 190. Gestational Diabetes Mellitus. Obstet Gynecol. 2018.
ACOG Practice Bulletin 183. Postpartum Hemorrhage. Obstet Gynecol. 2017.
ACOG Practice Bulletin 200. Early Pregnancy Loss. Obstet Gynecol. 2018.
ACOG/SMFM Obstetric Care Consensus. Placenta Accreta Spectrum. Am J Obstet Gynecol. 2018.
USPSTF. Screening for Cervical Cancer. JAMA. 2018.
USPSTF. Screening for Breast Cancer. JAMA. 2024.
USPSTF. Aspirin for Preeclampsia Prevention. JAMA. 2021.
The Menopause Society (NAMS). 2022 Hormone Therapy Position Statement. Menopause. 2022.
CDC. US Medical Eligibility Criteria for Contraceptive Use. MMWR. 2016.
NCCN Clinical Practice Guidelines in Oncology: Ovarian, Cervical, Endometrial, Breast Cancer.
Landmark Clinical Trials
Diagram & Figure Sources
Figure 1: Female Reproductive System. OpenStax College. CC BY 3.0.
Figure 2: Pregnancy. Wikimedia Commons. Public domain.
Figure 3: Intrauterine Device. Wikimedia Commons. Public domain.
Figure 4: Cervix with Dysplasia. Wikimedia Commons. Public domain.
OB/GYN runs on rhythm and pattern recognition. Every prenatal visit follows the same choreography: BP, weight, urine dip, fundal height, FHT, fetal movement, and the targeted review of preeclampsia and preterm labor symptoms. Every GYN visit starts with LMP, cycles, contraception, last Pap, and last mammogram before the chief complaint is even touched. A great scribe anticipates those blocks and has them populated before the attending walks in the room.
Learn to hear the specific shorthand — "32w4d by 8w US," "3/80/-1 vertex," "Cat II tracing with recurrent lates," "G3P2012" — and chart it the moment it leaves the physician's mouth. Know your preeclampsia severe features, your PALM-COEIN buckets, your contraception contraindications, and your staging systems, because they drive the assessment and plan on half the notes you write.
Welcome to OB/GYN. Few specialties blend continuity, acuity, surgery, and preventive care the way this one does. You will deliver babies and you will diagnose cancers — sometimes in the same day.