Occupational & Environmental Medicine
Every workplace exposure, regulatory framework, evaluation, diagnosis, procedure, medication, and documentation template you need to succeed in an occupational and environmental medicine clinic.
All diagrams on this page are sourced from published educational or institutional materials rather than AI generation. Each figure caption links to the original source, and the full diagram and guideline citations are collected in the references section at the bottom.
01 Occupational Medicine — Principles & Regulatory Framework
Occupational and environmental medicine (OEM) is the medical specialty devoted to the prevention, diagnosis, and treatment of work-related illness and injury, and the promotion of fitness-for-work and return-to-work. Unlike most clinical specialties, OEM exists at the intersection of clinical medicine, public health, epidemiology, toxicology, ergonomics, and a dense web of federal and state regulation. A single clinic day may include a sprained-ankle work injury, a DOT commercial driver physical, a post-needlestick bloodborne pathogen exposure, a respiratory surveillance exam for an asbestos abatement worker, and an independent medical evaluation (IME) for a workers' compensation claim.
The Hierarchy of Hazard Control
The foundational concept in occupational medicine is the hierarchy of controls, a ranked framework for eliminating or reducing workplace hazards. From most to least effective: Elimination (physically remove the hazard), Substitution (replace with something safer — e.g., water-based solvents instead of benzene), Engineering controls (isolate people from the hazard with ventilation, enclosure, or guarding), Administrative controls (change the way people work — rotation, training, job task limits), and Personal protective equipment (PPE) as the last line of defense (respirators, gloves, hearing protection, fall harnesses). PPE is listed last because it relies on the worker using it correctly every time; engineering controls protect everyone regardless of behavior.
Key Regulatory Bodies
The alphabet soup of OEM regulation is dense and you will hear these agencies referenced constantly:
OSHA (Occupational Safety and Health Administration): Part of the U.S. Department of Labor. Sets and enforces legally binding workplace safety standards, including permissible exposure limits (PELs), respiratory protection (29 CFR 1910.134), bloodborne pathogens (29 CFR 1910.1030), and hearing conservation (29 CFR 1910.95).
NIOSH (National Institute for Occupational Safety and Health): Part of the CDC. The research arm of occupational health; publishes recommended exposure limits (RELs), the NIOSH Pocket Guide to Chemical Hazards, and the NIOSH Lifting Equation.
ACGIH (American Conference of Governmental Industrial Hygienists): A professional society that publishes the annually updated Threshold Limit Values (TLVs) and Biological Exposure Indices (BEIs). TLVs are not legally binding but are widely considered the gold standard scientific benchmark.
DOT / FMCSA: Department of Transportation / Federal Motor Carrier Safety Administration. Regulates the medical certification of commercial drivers (CDL holders) under 49 CFR 391.
FAA: Federal Aviation Administration. Regulates medical certification of pilots (Class 1, 2, 3).
EPA: Environmental Protection Agency. Regulates environmental (vs. occupational) exposures, pesticide worker protection, and toxic substances under TSCA.
IARC (International Agency for Research on Cancer): WHO body that classifies chemical and physical agents by carcinogenicity (Group 1 = carcinogenic to humans; Group 2A = probably; Group 2B = possibly; Group 3 = not classifiable).
ACOEM (American College of Occupational and Environmental Medicine): The primary professional society; publishes clinical practice guidelines and the widely used ACOEM Practice Guidelines (formerly Occupational Medicine Practice Guidelines) that define return-to-work expectations for hundreds of conditions.
Workers' Compensation — The Parallel System
Most occupational injury care is paid for through the state workers' compensation system, not private health insurance. Workers' comp is a no-fault system: the worker receives medical care and partial wage replacement for a work-related injury, and in exchange gives up the right to sue the employer. The key documentation concept is causation — you must establish that the injury "arose out of and in the course of employment." You will routinely document mechanism of injury in forensic detail, including date, time, location, specific task, and witnesses.
Every occupational visit has a "dual client" problem: the patient is seated in front of you, but the note may also be read by the employer, workers' comp insurer, attorneys, OSHA, and IME reviewers. Keep your documentation factual, dated, time-stamped, and free of editorializing. Write "patient reports he lifted a 60-lb box" — not "patient claims" or "alleges."
02 Scribe Documentation Framework (DOT, FCE, IME, RTW)
Occupational medicine notes differ from general practice notes because the documentation often serves a legal or regulatory function. You will write several distinct note types, each with its own required elements.
The Work Injury Note
Mechanism: Exactly what the worker was doing when the injury occurred — task, posture, weight lifted, tool used, surface, footwear. Use the worker's own language when possible.
Date, time, and location: Specific date (not "last week") and time of day. Location down to the area of the facility.
Witnesses and reporting: Was the injury witnessed? Was it reported to a supervisor? When?
Body parts involved: Be specific — "right lateral ankle" not "ankle." Document all body parts even if the chief complaint is one.
Prior injury or condition: Any preexisting problem to the same body part is critical for apportionment. Ask directly.
First aid and treatment since injury: Ice, NSAIDs, ED visit, urgent care.
Current symptoms and functional impact: What can and cannot the worker do now? This drives the work status.
Work Status & Return-to-Work
Every occupational injury note ends with a work status determination, typically one of: Regular Duty (no restrictions), Modified/Light Duty (specific restrictions — no lifting > 10 lb, no overhead reaching, sit-down work only, no driving), or Off Work (totally temporarily disabled). Restrictions must be specific, time-limited, and tied to the injury. Vague restrictions ("take it easy") are unusable by employers.
DOT Commercial Driver Medical Examination
DOT physicals are performed under the FMCSA Medical Examiner Handbook by a provider listed on the National Registry of Certified Medical Examiners. The physical follows a standardized form (MCSA-5875) and certification (MCSA-5876). Certification periods can be 24 months (standard), 12 months, 6 months, or 3 months, depending on findings. Disqualifying conditions include uncontrolled diabetes on insulin without exemption, uncontrolled hypertension (≥ 180/110 disqualifies until controlled), seizure disorder, current methadone use, and certain cardiovascular conditions.
Independent Medical Examination (IME) & Impairment Rating
An IME is a one-time evaluation performed by a physician who is not the treating physician, usually at the request of an insurer or attorney, to answer specific medicolegal questions: Is this injury work-related? Has the patient reached maximum medical improvement (MMI)? What is the impairment rating? What are permanent work restrictions? Impairment ratings are expressed as a percentage of whole person impairment (WPI) using the AMA Guides to the Evaluation of Permanent Impairment, 6th Edition.
An FCE is a multi-hour standardized assessment of a worker's physical capacity to perform work tasks: lifting, carrying, pushing, pulling, reaching, squatting, sitting, standing, walking. Results are reported in Dictionary of Occupational Titles (DOT) physical demand categories: Sedentary (≤ 10 lb), Light (≤ 20 lb), Medium (≤ 50 lb), Heavy (≤ 100 lb), Very Heavy (> 100 lb).
On a DOT physical, the driver's blood pressure, vision (20/40 each eye with/without correction, 70° horizontal field), hearing (must perceive forced whisper at 5 ft), and urine dipstick (protein, blood, sugar) are the four measurements you must never leave blank. The BP reading drives the certification length — memorize the thresholds.
03 Occupational Lung Disease & Pneumoconioses Respiratory
Inhaled occupational dusts, fibers, fumes, and gases cause a spectrum of lung disease that includes pneumoconioses (fibrotic lung diseases from mineral dusts), hypersensitivity pneumonitis, occupational asthma, and occupational lung cancers. These diseases have long latency periods — often 10 to 40 years between first exposure and clinical presentation — which makes a careful occupational history the cornerstone of diagnosis.
Asbestosis
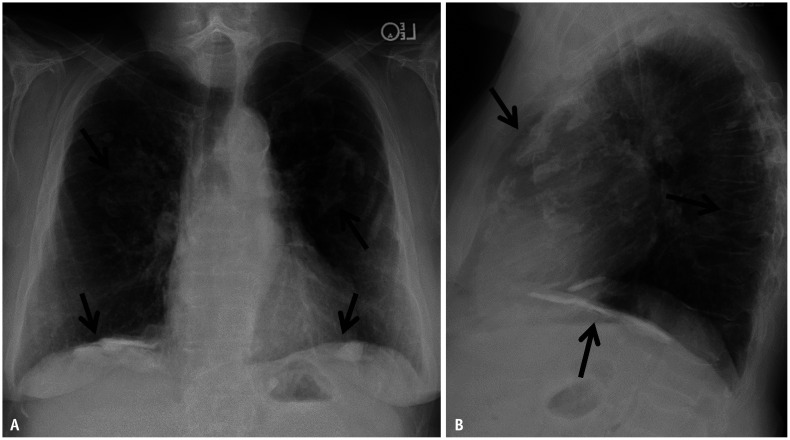
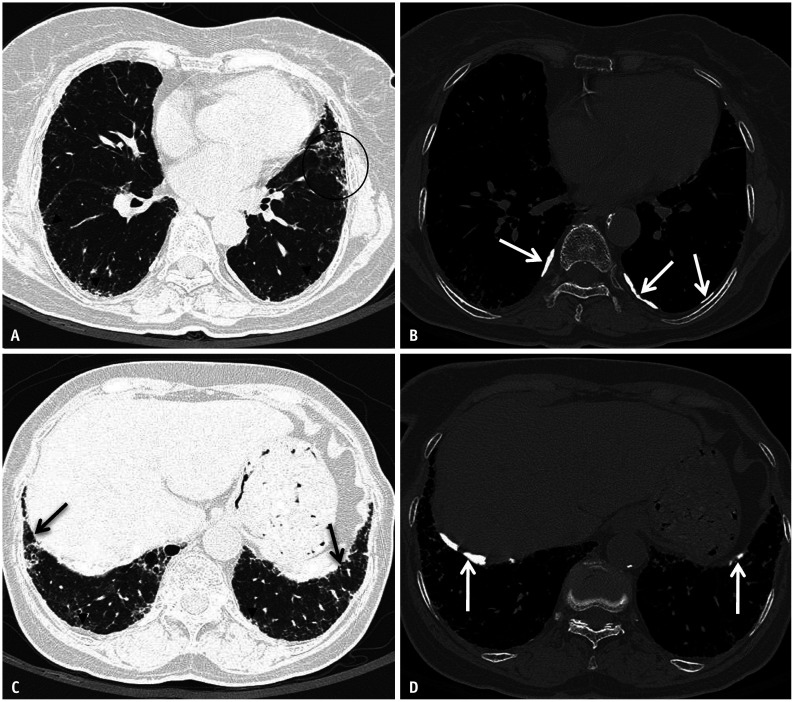
Asbestosis is diffuse interstitial pulmonary fibrosis caused by the inhalation of asbestos fibers. Historical exposures include shipbuilding, insulation work, brake manufacturing, pipefitting, boiler work, and building demolition. Latency is typically 20 to 40 years. Patients present with progressive exertional dyspnea, nonproductive cough, and bibasilar dry (Velcro) crackles on auscultation. Chest imaging shows bilateral lower-zone reticular opacities and pleural plaques (the radiographic marker of asbestos exposure, not asbestosis per se). Diagnosis rests on exposure history, consistent imaging, and exclusion of alternative causes. Spirometry shows a restrictive pattern with reduced DLCO. There is no specific treatment; management is supportive with smoking cessation (smoking multiplies lung cancer risk), pneumococcal and influenza vaccination, and oxygen when indicated. Asbestos is IARC Group 1 and exposure causes asbestosis, lung cancer, mesothelioma, and laryngeal and ovarian cancers.

Silicosis
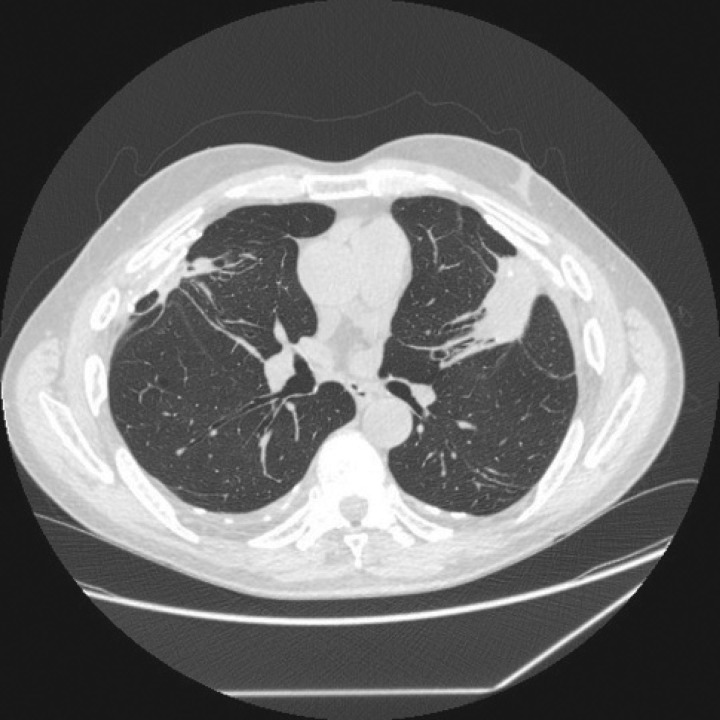
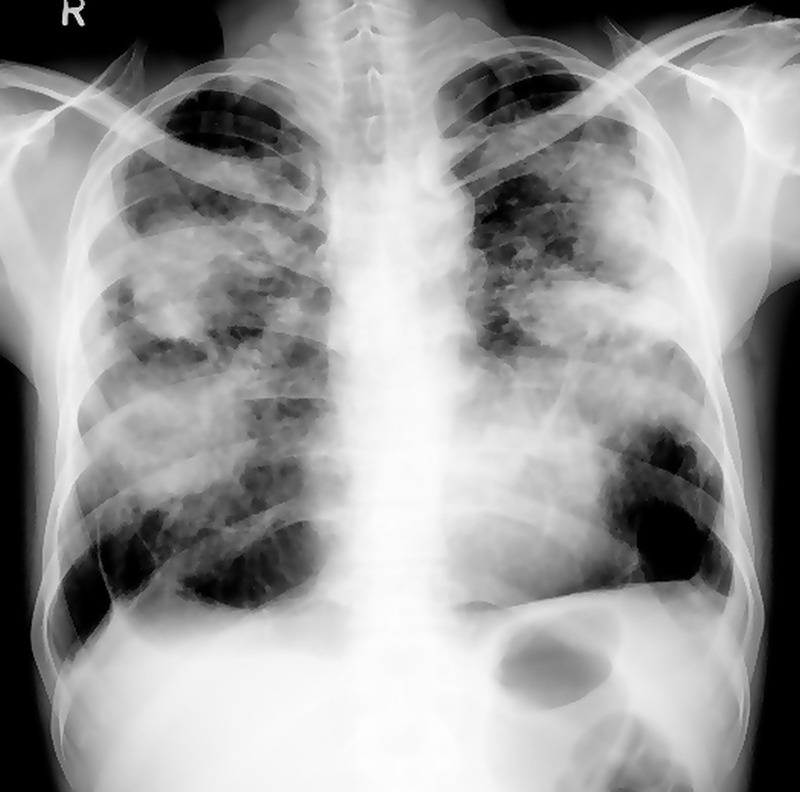
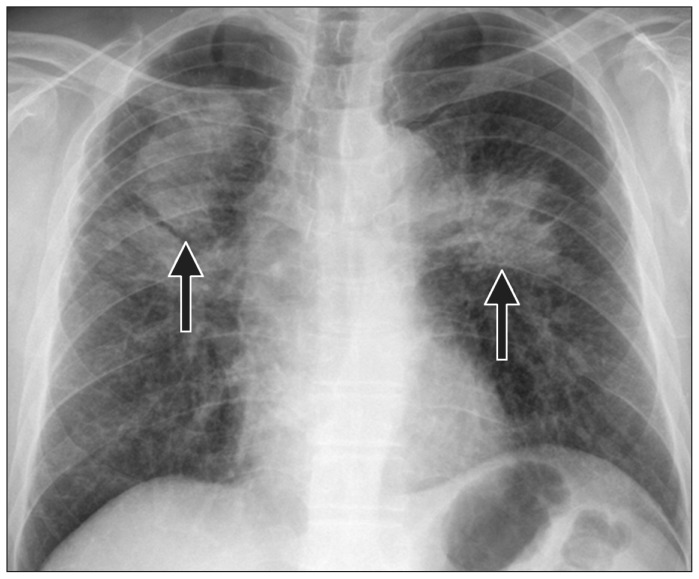
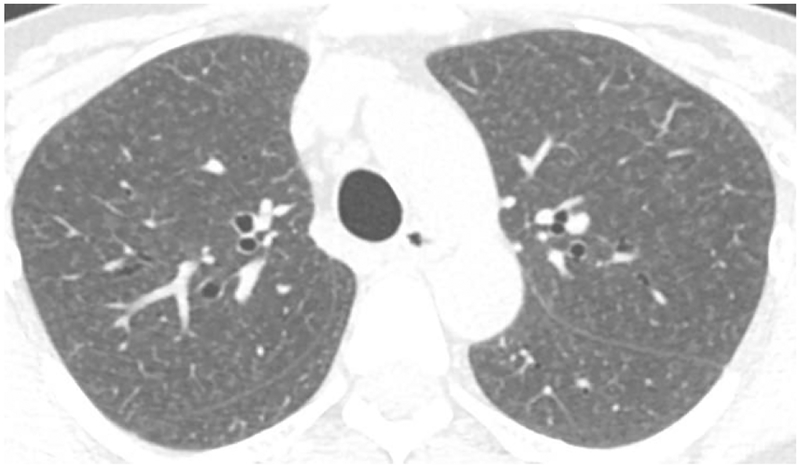
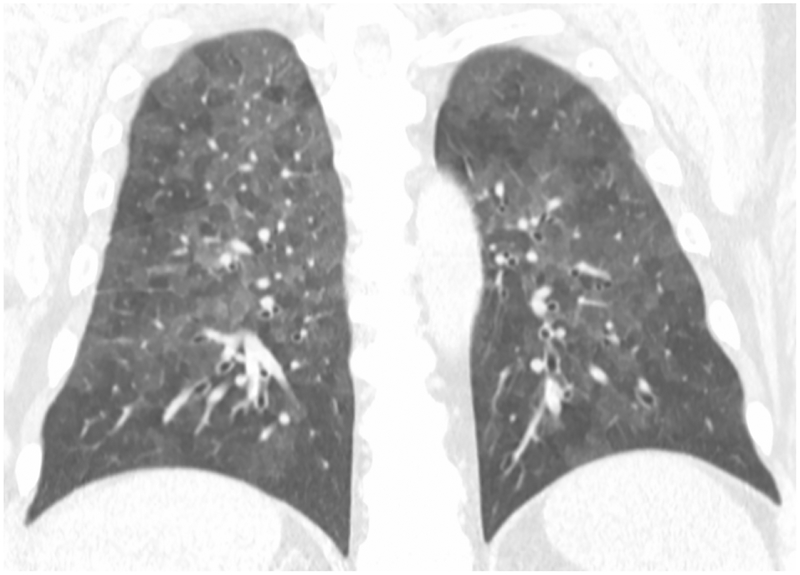
Silicosis is caused by inhalation of crystalline silica dust from sandblasting, mining, quarrying, stone countertop fabrication (engineered stone silicosis is a rising epidemic), tunneling, and foundry work. Three clinical forms: chronic simple silicosis (10+ years of exposure, small upper-lobe nodules, often asymptomatic early), accelerated silicosis (5 to 10 years, more rapid progression), and acute silicoproteinosis (massive exposure over months, alveolar filling, often fatal). Progressive massive fibrosis (PMF) develops when nodules coalesce into large conglomerate masses > 1 cm. Silica exposure triples the risk of tuberculosis — TB screening is mandatory in silica-exposed workers. Silica is IARC Group 1.
Coal Workers' Pneumoconiosis (CWP)
CWP (also called black lung) is caused by inhalation of coal mine dust. Simple CWP presents with small rounded upper-lobe opacities; complicated CWP (PMF) develops with larger conglomerate lesions. Caplan syndrome is the association of CWP (or other pneumoconiosis) with rheumatoid arthritis, producing multiple pulmonary nodules. The Federal Black Lung Benefits Program provides compensation for disabled coal miners and their survivors.
Hypersensitivity Pneumonitis
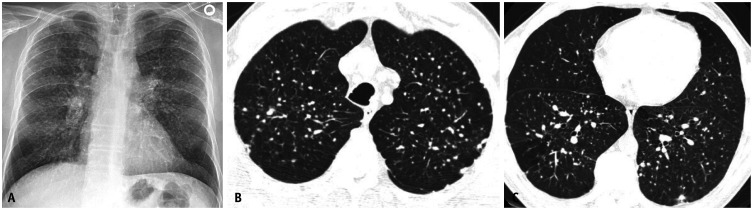
Hypersensitivity pneumonitis (HP) is an immune-mediated interstitial lung disease caused by inhalation of organic antigens. Classic named forms include farmer's lung (thermophilic actinomycetes in moldy hay), bird fancier's lung (avian proteins from pigeons, parakeets), humidifier lung, hot tub lung (nontuberculous mycobacteria), and maple bark stripper's lung. Acute HP presents 4 to 8 hours after exposure with fever, chills, cough, dyspnea, and myalgia — often misdiagnosed as pneumonia. Chronic HP causes progressive fibrosis. Treatment is antigen avoidance and corticosteroids.
Berylliosis
Chronic beryllium disease (CBD) is a granulomatous lung disease caused by beryllium exposure in aerospace, nuclear, electronics, and dental alloy industries. It is clinically and histologically indistinguishable from sarcoidosis without a specific test. The beryllium lymphocyte proliferation test (BeLPT) confirms sensitization. CBD is Group 1 carcinogenic per IARC.

Byssinosis
Byssinosis (brown lung) is caused by cotton, flax, and hemp dust exposure in textile workers. The classic feature is "Monday morning chest tightness" — symptoms returning on the first workday after a weekend away and progressively reducing through the week. Chronic byssinosis can evolve into fixed airflow obstruction.
The International Labour Organization (ILO) Classification is the standardized system for coding chest radiograph findings in pneumoconiosis surveillance. Key elements:
Small opacities: Profusion categories 0/0 through 3/3 (12 gradations), shape (rounded p/q/r or irregular s/t/u), and zone (upper, mid, lower; right, left).
Large opacities: Category A (one opacity < 50 mm or several < 50 mm with combined < 50 mm), B (one or more between 50 mm and one-third of right lung), C (combined > one-third of right lung).
Pleural abnormalities: Pleural plaques (localized thickening), diffuse pleural thickening, costophrenic angle obliteration, and calcification. Readings are performed by certified NIOSH B Readers.
04 Occupational Asthma & Airway Disorders Respiratory
Occupational asthma (OA) is asthma caused or triggered by workplace exposures, and is the most common occupational lung disease in developed economies. There are two major categories: sensitizer-induced OA (after a latency period of weeks to years, an IgE- or non-IgE-mediated sensitization develops) and irritant-induced OA, including Reactive Airways Dysfunction Syndrome (RADS), which follows a single high-intensity exposure to an irritant with asthma symptoms persisting beyond 3 months.
Classic high-molecular-weight sensitizers include flour (baker's asthma), animal dander (laboratory animal workers), latex (healthcare workers), and enzymes (detergent manufacturing). Low-molecular-weight sensitizers include isocyanates (spray painters, polyurethane manufacturing — the most common cause worldwide), western red cedar dust (plicatic acid), acid anhydrides, and metals (nickel, chromium, platinum).
Diagnosis requires objective documentation of variable airflow obstruction and a temporal relationship to work. Key tools include serial peak expiratory flow (PEF) monitoring every 2 hours for 4 weeks (2 work weeks plus 2 off weeks), methacholine challenge, and specific inhalation challenge in specialized centers. Management begins with exposure elimination — sensitizer-induced OA rarely resolves with continued exposure, even with aggressive pharmacotherapy.
05 Occupational Cancers Oncology
Occupational exposures account for an estimated 4% to 10% of all cancers. The IARC Monographs are the authoritative reference for carcinogen classification and you will see them cited on every workers' comp cancer claim.
| Cancer | Classic Occupational Exposure | Industries |
|---|---|---|
| Mesothelioma | Asbestos | Shipbuilding, insulation, brake repair, demolition |
| Lung cancer | Asbestos, silica, radon, diesel exhaust, arsenic, chromium VI, nickel, beryllium, BCME | Mining, construction, welding, chemical |
| Bladder cancer | Aromatic amines (benzidine, beta-naphthylamine) | Dye, rubber, leather workers; hairdressers |
| Acute myeloid leukemia | Benzene, ionizing radiation, ethylene oxide, formaldehyde | Petrochemical, rubber, refinery, radiology |
| Angiosarcoma of the liver | Vinyl chloride monomer | PVC polymerization |
| Nasal/sinus adenocarcinoma | Hardwood dust, nickel refining, formaldehyde | Furniture, cabinetry, nickel |
| Skin cancer (SCC) | UV radiation, arsenic, coal tar, mineral oil | Outdoor workers, roofers, metalworkers |
| Scrotal cancer | Coal tar, soot (historical — Percivall Pott) | Chimney sweeps |
Mesothelioma
Malignant pleural mesothelioma is a signature tumor of asbestos exposure with latency typically 30 to 50 years. Even brief, distant, or secondhand (take-home) asbestos exposure can cause mesothelioma. Patients present with dyspnea and unilateral pleural effusion. Imaging shows pleural thickening and nodularity; diagnosis is confirmed by thoracoscopic pleural biopsy. Prognosis remains poor despite multimodal therapy.
Benzene-Induced Hematologic Malignancy
Benzene is a leukemogen causing AML, myelodysplastic syndrome, and aplastic anemia. Historical exposures include rubber manufacturing, petrochemical refining, and gasoline distribution. Benzene is IARC Group 1. Biological monitoring uses urinary S-phenylmercapturic acid (S-PMA) or trans,trans-muconic acid.
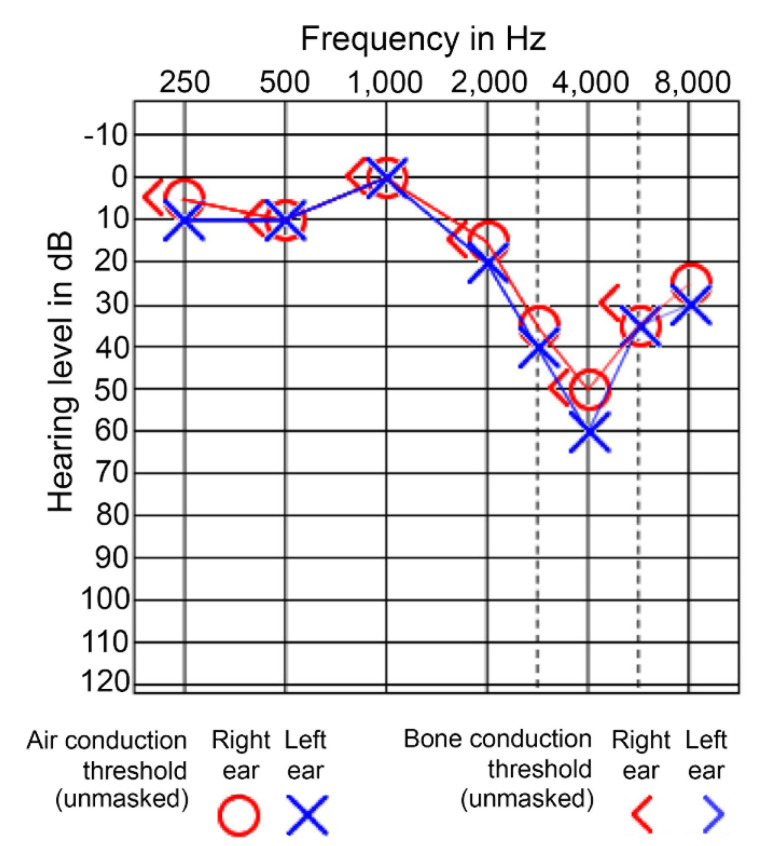
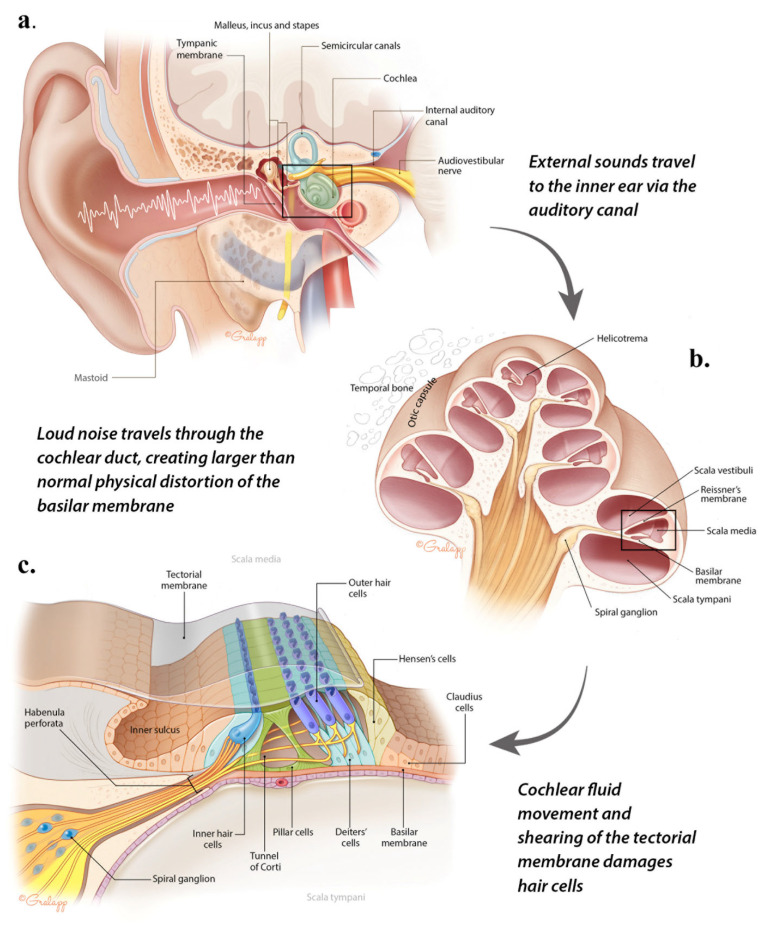
06 Noise-Induced Hearing Loss & Audiometry Sensory
Noise-induced hearing loss (NIHL) is the most common preventable occupational illness. Chronic exposure to noise > 85 dBA causes a characteristic bilateral, symmetric, sensorineural hearing loss with a notch at 4000 Hz on audiometry. With continued exposure, the notch deepens and widens to involve 3000 and 6000 Hz, and eventually 2000 Hz, which is where speech-frequency impairment begins.
OSHA's Hearing Conservation Standard (29 CFR 1910.95) requires a hearing conservation program whenever the 8-hour time-weighted average (TWA) exposure reaches 85 dBA (the action level), including annual audiometric testing, noise monitoring, and hearing protection. The permissible exposure limit (PEL) is 90 dBA over 8 hours, with a 5 dBA exchange rate (every 5 dBA increase halves the allowable exposure time). NIOSH recommends a stricter 85 dBA REL with a 3 dBA exchange rate.
Standard Threshold Shift (STS)
OSHA defines a Standard Threshold Shift as a change in hearing threshold of 10 dB or more at 2000, 3000, and 4000 Hz averaged in either ear compared to baseline. An STS triggers required follow-up including retesting, counseling, and either mandatory use or refit of hearing protection. An STS with an overall level ≥ 25 dB is OSHA recordable.
| Average Threshold (500–4000 Hz) | Classification |
|---|---|
| ≤ 25 dB HL | Normal hearing |
| 26–40 dB HL | Mild hearing loss |
| 41–55 dB HL | Moderate |
| 56–70 dB HL | Moderately severe |
| 71–90 dB HL | Severe |
| > 90 dB HL | Profound |
07 Occupational Dermatoses Skin
Skin disease is the second-most-reported category of occupational illness after MSK injuries. The major entities you will document are irritant contact dermatitis, allergic contact dermatitis, contact urticaria, occupational acne (including chloracne), latex allergy, and occupational skin cancers (covered separately).
Contact Dermatitis
Irritant contact dermatitis (ICD) accounts for 80% of occupational dermatitis. It is a non-immune, dose-dependent direct injury from detergents, solvents, acids, alkalis, metalworking fluids, and wet work (prolonged glove occlusion). Typical locations are the hands and forearms. Allergic contact dermatitis (ACD) is a type IV delayed hypersensitivity reaction to a sensitizer such as nickel, chromate (cement dermatitis), rubber accelerators (thiurams, carbamates), epoxies, and acrylates. Patch testing is the diagnostic gold standard.

Chloracne
Chloracne is a pathognomonic dermatologic marker of dioxin, polychlorinated biphenyl (PCB), and chlorinated naphthalene exposure — seen historically in Agent Orange exposure and the Seveso disaster. Presents with open comedones, straw-colored cysts, and pustules in the malar region, postauricular area, and axillae.
Latex Allergy
Natural rubber latex allergy in healthcare workers can be type IV (ACD to rubber chemicals) or type I (true IgE-mediated, with contact urticaria, rhinoconjunctivitis, asthma, or anaphylaxis). Latex-fruit cross-reactivity (banana, kiwi, avocado, chestnut) is common. Switching to nitrile gloves and latex-free environments is mandatory.
08 Work-Related Musculoskeletal Disorders (WMSDs) Musculoskeletal
Work-related musculoskeletal disorders are the largest single category of occupational illness and workers' compensation claims in the United States. They include acute traumatic injuries (lumbar strains from lifting, fractures from falls) and chronic cumulative trauma disorders (CTDs) arising from repetition, force, awkward posture, and vibration.
Low Back Pain & Lumbar Strain
Work-related low back pain is usually a soft-tissue lumbar sprain/strain associated with a lifting, twisting, or sudden-loading event. Red flags (saddle anesthesia, bowel/bladder dysfunction, progressive weakness, fever, history of cancer) require urgent imaging. Otherwise, imaging is not indicated in the first 6 weeks of nonspecific back pain per ACP low back pain guidelines. Management is activity modification (not bed rest), NSAIDs, heat, and early return to modified duty. The NIOSH Lifting Equation calculates a Recommended Weight Limit (RWL) and a Lifting Index (LI) for a given lifting task.
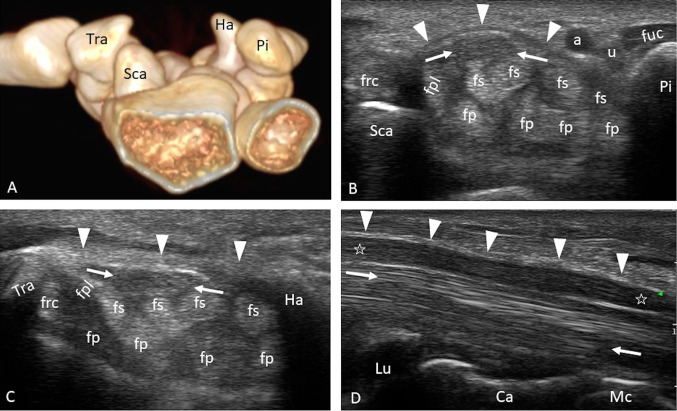
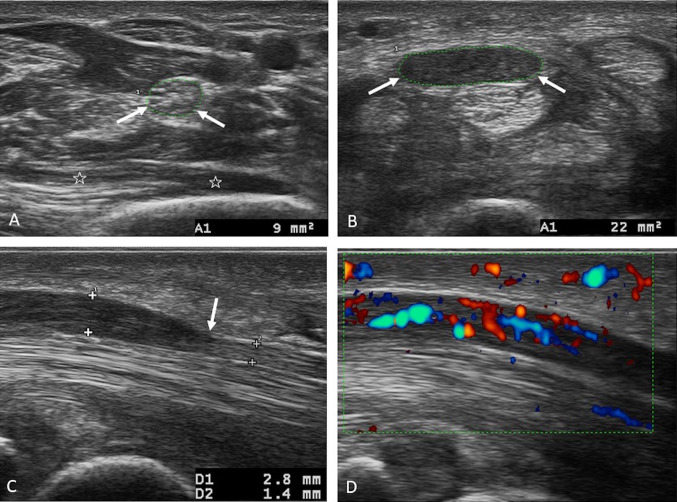
Carpal Tunnel Syndrome (CTS)
CTS is compressive neuropathy of the median nerve at the wrist. Workplace risk factors include high force, high repetition, vibrating tools, and extreme wrist postures. Patients report nocturnal paresthesia of the thumb, index, middle, and radial half of the ring finger, shaking the hand for relief ("flick sign"), and thenar weakness in advanced cases. Phalen and Tinel signs may be present. Diagnosis is confirmed by nerve conduction studies. Management is night splinting, activity modification, corticosteroid injection, and carpal tunnel release surgery.
Lateral Epicondylitis (Tennis Elbow)
Tendinopathy of the common extensor origin at the lateral epicondyle, caused by repetitive gripping and wrist extension (carpentry, electricians, assembly). Pain with resisted wrist extension; treatment is activity modification, counterforce bracing, eccentric exercise, and NSAIDs.
Rotator Cuff Tendinopathy & Impingement
Repetitive overhead work (painters, electricians, warehouse, construction) produces subacromial impingement and rotator cuff tendinopathy. Positive Neer, Hawkins, and empty-can tests. MRI characterizes full- vs partial-thickness tears. Full-thickness tears in manual workers often require surgical repair with prolonged restricted duty.
NIOSH Lifting Equation: Calculates the Recommended Weight Limit from load constant 51 lb multiplied by six task-specific factors (horizontal, vertical, distance, asymmetry, frequency, coupling). LI = actual weight / RWL; LI > 1.0 is above recommendation; LI > 3.0 is high risk.
REBA (Rapid Entire Body Assessment): Scores neck, trunk, legs, and upper limbs for whole-body ergonomic risk.
RULA (Rapid Upper Limb Assessment): Focused upper-extremity ergonomic assessment.
Heinrich's Pyramid (safety triangle): For every major injury there are approximately 29 minor injuries and 300 near misses — reported injuries are the tip of a much larger iceberg.
09 Heat Illness & Cold Injury Environmental
Heat-Related Illness
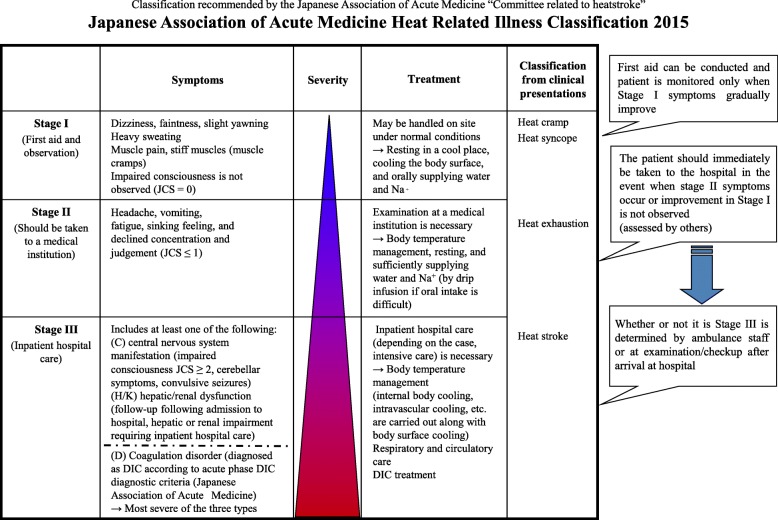
Heat illness forms a spectrum: heat rash (miliaria), heat cramps, heat syncope, heat exhaustion, and heat stroke. Heat exhaustion presents with core temperature 37–40°C (100–104°F), profuse sweating, tachycardia, headache, nausea, and preserved mentation. Heat stroke is defined by core temperature > 40°C (> 104°F) with central nervous system dysfunction (confusion, seizure, coma) — this distinction from heat exhaustion is critical. Exertional heat stroke is a medical emergency; first-line treatment is cold-water immersion, the intervention with the best outcomes. OSHA has no specific heat standard federally but enforces the General Duty Clause.
Cold Injury
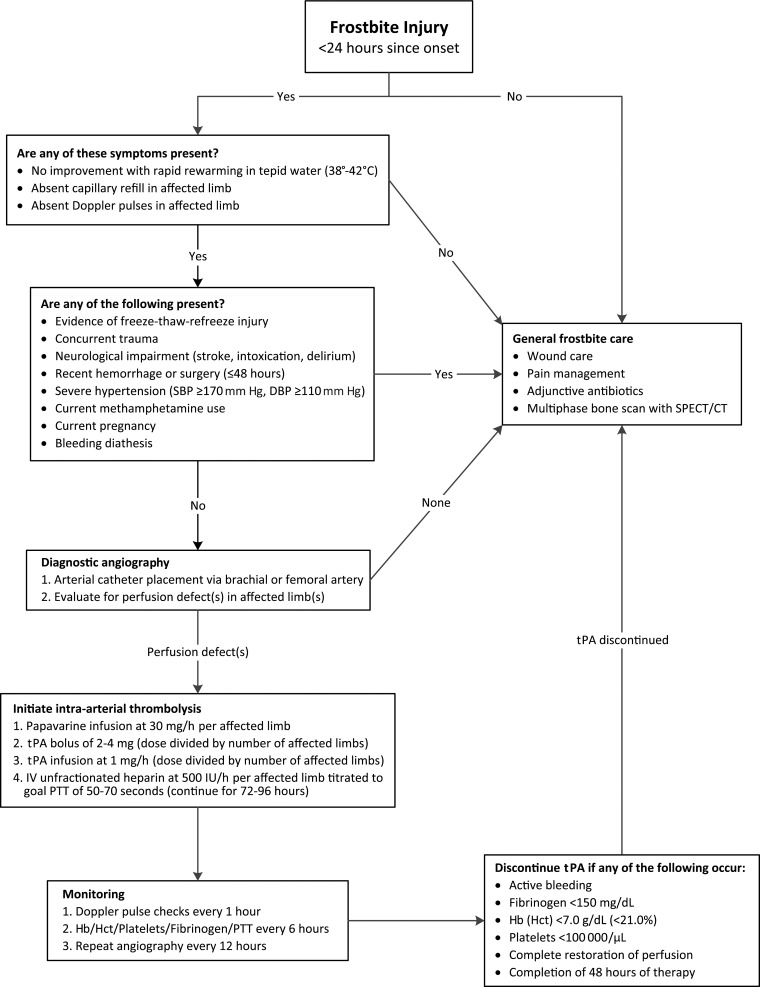
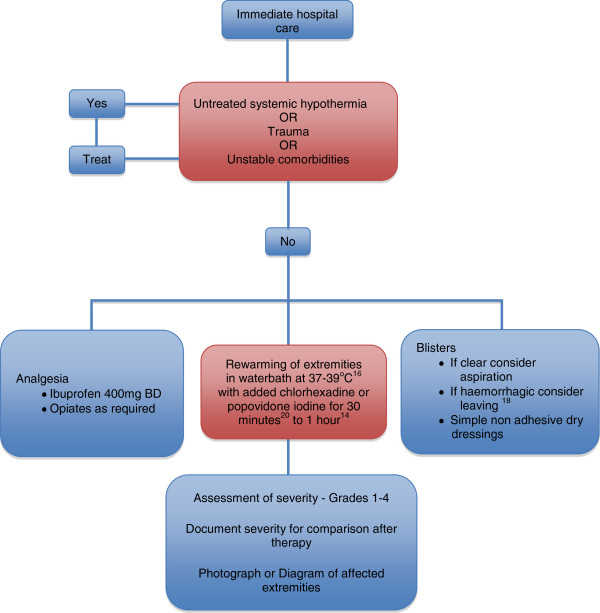
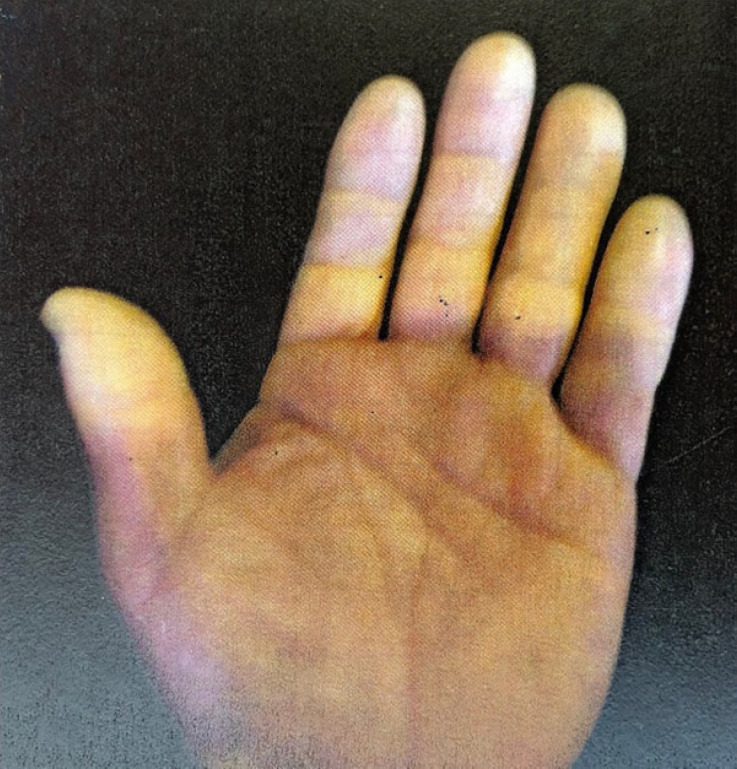
Frostbite is tissue freezing classified by depth: first-degree (erythema, no blistering), second-degree (clear blisters), third-degree (hemorrhagic blisters), fourth-degree (full-thickness, muscle/bone involvement). Treat with rapid rewarming in 37–39°C water. Hypothermia is core temperature < 35°C (95°F) and is staged: mild (32–35°C), moderate (28–32°C), severe (< 28°C).
10 High-Altitude Illness & Decompression Sickness Environmental
High-altitude illness includes Acute Mountain Sickness (AMS), High-Altitude Pulmonary Edema (HAPE), and High-Altitude Cerebral Edema (HACE). AMS presents > 2500 m with headache plus nausea, fatigue, dizziness, or sleep disturbance; treat with descent, rest, acetazolamide, and ibuprofen. HAPE presents with dyspnea at rest, cough, crackles, and pink frothy sputum; treat with descent, oxygen, and nifedipine. HACE is AMS plus ataxia or altered mental status; treat with immediate descent, oxygen, and dexamethasone.
Decompression sickness (DCS) or "the bends" occurs in divers, caisson workers, and aviators after rapid pressure reduction causes dissolved nitrogen to form bubbles in tissues and blood. Type I is musculoskeletal and cutaneous; Type II involves neurologic, cardiopulmonary, or inner ear symptoms. Treatment is 100% oxygen and recompression in a hyperbaric chamber.
11 Vibration Injury & Ergonomic Hazards Physical Agents
Hand-Arm Vibration Syndrome (HAVS), previously called vibration white finger, results from prolonged use of vibrating hand tools (chainsaws, jackhammers, grinders, chipping hammers). The syndrome has three components: vascular (episodic blanching of fingers on cold exposure, mimicking Raynaud), sensorineural (numbness, tingling, reduced dexterity), and musculoskeletal. The Stockholm Workshop Scale grades severity. Whole-body vibration (WBV) from heavy equipment operation (truck drivers, forklift operators) is associated with low back pain and degenerative disc disease.

12 Radiation Exposure (Acute & Chronic) Physical Agents
Radiation exposures in the workplace include ionizing radiation (X-ray, gamma, alpha, beta, neutron) in nuclear, medical, dental, industrial radiography, and research settings, and non-ionizing radiation (UV, microwave, RF, laser). OSHA and NRC set dose limits: the annual whole-body occupational dose limit is 5 rem (50 mSv).
Acute Radiation Syndrome (ARS)
ARS follows high-dose whole-body exposure and has four phases: prodrome, latent, manifest illness, and recovery/death. Three classic subsyndromes by dose: hematopoietic (> 1 Gy, bone marrow suppression), gastrointestinal (> 6 Gy, mucositis, diarrhea, sepsis), and cerebrovascular/cardiovascular (> 20 Gy, rapidly fatal). Early lymphocyte count depression is the most useful biologic dosimeter.
Chronic Radiation Effects
Stochastic effects (cancer, heritable effects) have no threshold and are probabilistic. Deterministic effects (cataracts, skin erythema, fibrosis, sterility) have thresholds. Radiation workers wear dosimeters (film badge, TLD, OSL) and undergo medical surveillance.
13 Heavy Metal & Chemical Toxicology Toxicology
Lead
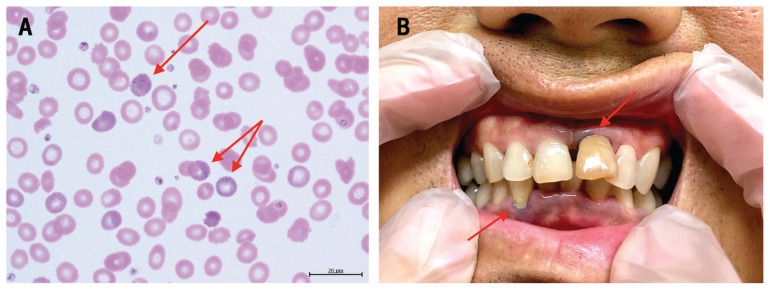
Lead exposure occurs in battery manufacturing, lead smelting, radiator repair, construction (lead paint abatement, bridge painting, demolition), and firing ranges. Inorganic lead causes abdominal colic, constipation, anemia (basophilic stippling, microcytic), peripheral motor neuropathy (wrist drop), nephropathy, hypertension, and encephalopathy at high levels. Organic (tetraethyl) lead causes predominantly neuropsychiatric effects. OSHA's lead standard (29 CFR 1910.1025) requires blood lead level (BLL) monitoring; medical removal is triggered at BLL ≥ 60 µg/dL (construction) or ≥ 50 µg/dL (general industry), with return permitted when BLL < 40 µg/dL. Public health action levels are now much lower (5–10 µg/dL). Chelation uses succimer (DMSA) orally, EDTA (CaNa2-EDTA) parenterally, and BAL (dimercaprol) for encephalopathy.
Mercury
Elemental (metallic) mercury vaporizes and is inhaled — thermometer manufacturing, dental amalgam, gold mining, chloralkali plants. Chronic exposure produces the classic triad of tremor (intention), erethism (shyness, emotional lability, memory loss — "mad hatter"), and gingivostomatitis. Organic (methylmercury) exposure is primarily dietary. Chelation: DMSA, DMPS, or BAL (avoid BAL in organic mercury).
Arsenic
Arsenic exposure occurs in smelting, wood preservatives, pesticide manufacture, and microelectronics. Acute inorganic arsenic poisoning causes gastroenteritis, hypotension, QT prolongation. Chronic exposure produces hyperkeratoses (palms, soles), Mees lines on nails, peripheral neuropathy, and elevated risk of skin, lung, bladder, kidney, and liver cancer. Treat with BAL or DMSA.
Cadmium
Cadmium exposure occurs in battery (NiCd), pigment, plating, and alloy work. Acute inhalation of cadmium fumes causes chemical pneumonitis and ARDS (welding galvanized steel is a classic cause). Chronic exposure causes renal tubular damage (low-molecular-weight proteinuria — beta-2-microglobulin elevation), osteomalacia, and lung cancer. There is no effective chelator.
Manganese
Manganese exposure in mining, welding, and ferroalloy work causes manganism, a parkinsonian syndrome with extrapyramidal features distinct from idiopathic Parkinson disease (less tremor, more dystonia and "cock walk" gait).
Organophosphate & Carbamate Pesticides
Organophosphates irreversibly inhibit acetylcholinesterase, producing the cholinergic toxidrome: SLUDGE (Salivation, Lacrimation, Urination, Defecation, GI distress, Emesis) plus DUMBELS or the "killer Bs" (bradycardia, bronchorrhea, bronchospasm). Treatment: atropine (titrated to dry bronchial secretions) and pralidoxime (2-PAM). Carbamates produce similar but reversible inhibition.
Organic Solvents
Solvent exposure (toluene, xylene, methylene chloride, trichloroethylene, n-hexane, carbon disulfide) produces acute CNS depression (narcosis), chronic encephalopathy (painters' syndrome), peripheral neuropathy (n-hexane, carbon disulfide), hepatotoxicity, and reproductive effects. Methylene chloride is metabolized to carbon monoxide.
14 Asphyxiants, CO & H2S Exposures Toxicology
Simple asphyxiants (nitrogen, methane, CO2, propane, argon) displace oxygen in enclosed spaces. Confined space deaths follow a classic pattern: the first worker collapses, and rescuers without SCBA enter and also die. Chemical asphyxiants interfere with oxygen transport or cellular respiration.
Carbon Monoxide
CO binds hemoglobin with 240x the affinity of oxygen, forming carboxyhemoglobin (COHb) and shifting the oxyhemoglobin dissociation curve leftward. Sources: fires, faulty furnaces, indoor gas heaters, unvented generators, methylene chloride metabolism, vehicle exhaust. Symptoms correlate loosely with COHb: headache and nausea (10–20%), confusion (20–40%), syncope and seizure (40–60%), coma and death (> 60%). Pulse oximetry is falsely normal — must measure COHb by co-oximetry. Treatment: 100% non-rebreather oxygen; hyperbaric oxygen (HBO) for COHb > 25%, loss of consciousness, neurologic deficit, cardiac ischemia, or pregnancy.
Hydrogen Sulfide
H2S (sewer gas, manure pits, oil and gas operations, paper mills) smells like rotten eggs at low concentration but causes olfactory fatigue at higher concentrations — the worker can no longer smell it. H2S inhibits cytochrome oxidase like cyanide and is rapidly fatal. Treatment: removal, 100% oxygen, and consideration of nitrites or hydroxocobalamin.
Cyanide
Cyanide exposure occurs in electroplating, fumigation, and fires (polyurethane and wool combustion). Inhibits cytochrome oxidase. Classic findings: severe lactic acidosis with a narrowed venous-arterial O2 difference. Antidotes: hydroxocobalamin (first line), or the cyanide antidote kit (amyl nitrite, sodium nitrite, sodium thiosulfate).
Methemoglobinemia
Oxidizing exposures (aniline dyes, nitrites, nitrates, dapsone, benzocaine) convert hemoglobin iron from ferrous to ferric, producing methemoglobin which cannot carry oxygen. Chocolate-brown blood, cyanosis unresponsive to oxygen, and a "saturation gap" between SpO2 and PaO2. Treatment: methylene blue.
15 Occupational Infectious Disease & Bloodborne Pathogens Infectious
Healthcare workers, laboratory workers, first responders, and agricultural workers face occupational infectious exposures. The OSHA Bloodborne Pathogens Standard (29 CFR 1910.1030) governs HCW protection including hepatitis B vaccination, PPE, sharps handling, and post-exposure management.
Sharps/Needlestick Exposures
Immediate: Wash site with soap and water (do not bleach or use caustic agents); flush mucous membranes with saline.
Source patient: Test for HBsAg, anti-HCV and HCV RNA, HIV Ag/Ab.
HBV: If exposed worker is vaccinated and anti-HBs ≥ 10 mIU/mL, no action. If unvaccinated or non-responder, give HBIG within 24 hours and initiate vaccine series.
HCV: No post-exposure prophylaxis available. Baseline and 3- and 6-month follow-up testing; treat if seroconversion occurs (direct-acting antivirals have made HCV curable).
HIV: Initiate PEP within 2 hours if source is HIV-positive or high-risk unknown — standard regimen is tenofovir/emtricitabine + raltegravir or dolutegravir for 28 days per USPHS PEP guidelines. Follow-up HIV testing at baseline, 6 weeks, 12 weeks, and 6 months (4 months with 4th-generation assay).
Tuberculosis
Healthcare workers undergo annual TB screening per CDC guidelines using tuberculin skin test (TST/PPD) or interferon-gamma release assay (IGRA — QuantiFERON, T-SPOT). New conversions require chest X-ray and LTBI treatment with isoniazid or rifampin-based regimens.
COVID-19 & Respiratory Pathogens
Healthcare workers must be fit-tested annually for N95 respirators per OSHA 29 CFR 1910.134. Qualitative (saccharin, Bitrex) or quantitative (PortaCount) testing confirms an adequate seal with a specific make, model, and size.
Zoonoses & Agricultural Infections
Brucellosis (livestock, unpasteurized dairy), leptospirosis (water contaminated by animal urine), Q fever (sheep, goats, cattle), anthrax (wool sorters), rabies (animal control, veterinarians), hantavirus (rodent droppings), and histoplasmosis (bat and bird guano).
16 Traumatic, Agricultural & Eye Injuries Trauma
Agricultural work is one of the most dangerous occupations in the United States. Hazards include tractor rollovers (ROPS reduce mortality), grain engulfment, power take-off entanglement, pesticide exposure, livestock injury, and zoonotic disease. Fatality rates in agriculture, construction, fishing, logging, and mining far exceed other sectors.
Occupational Eye Injuries
Eye injuries include corneal foreign body and abrasion (grinding, machining), welder's flash (photokeratitis from UV exposure without proper shielding), chemical burns (alkali > acid in severity — immediate copious irrigation for 30+ minutes with Morgan lens, pH testing), and open globe from projectile injuries. ANSI-rated safety eyewear with side shields is the core PPE; full face shields add protection during grinding and chemical work.
17 Mental Health, Stress, Shift Work & Reproductive Hazards Behavioral
Workplace Stress & Burnout
Occupational burnout is recognized by the WHO as an occupational phenomenon (ICD-11) with three dimensions: exhaustion, cynicism/depersonalization, and reduced professional efficacy. PTSD in first responders, veterans, and healthcare workers is a major occupational mental health concern. Workplace violence prevention programs are mandated in high-risk settings (healthcare, corrections, retail).
Shift Work Disorder
Shift work disorder (SWD) is circadian misalignment presenting with insomnia during intended sleep and excessive sleepiness during intended wake. Night-shift and rotating-shift workers are at increased risk for cardiovascular disease, metabolic syndrome, and (per IARC Group 2A) breast cancer. Countermeasures include strategic lighting, scheduled naps, and modafinil/armodafinil for symptomatic sleepiness.
Reproductive Hazards
Reproductive hazards include ionizing radiation (fetal dose < 0.5 rem/month for declared pregnant workers), ethylene oxide, glycol ethers, lead, mercury, antineoplastic drugs (pharmacy, oncology nursing), organic solvents, and anesthetic gases. Counseling pregnant workers requires careful balance of protection and non-discrimination under the Pregnancy Discrimination Act and Pregnant Workers Fairness Act.
Workplace Substance Use & Drug Testing
DOT drug testing panel tests five classes: marijuana (THC metabolite), cocaine, amphetamines/methamphetamines, opiates/opioids, and PCP. Specimen validity (creatinine, pH, specific gravity, adulterants) is checked. Non-negative results go to a Medical Review Officer (MRO) who contacts the donor to evaluate legitimate medical explanations before reporting a verified positive.
18 Evaluations & Procedures (Physicals, FCE, IME, Surveillance) Procedures
Occupational medicine is evaluation-heavy. Most "procedures" are structured assessments that produce documented determinations rather than interventional acts.
| Evaluation | Purpose / Key Elements |
|---|---|
| Pre-placement physical | Performed after conditional offer of employment (post-offer, pre-employment) to determine fitness for essential job functions. ADA requires job-related and consistent with business necessity. |
| Periodic medical surveillance | OSHA-required for workers exposed to regulated substances (lead, asbestos, benzene, cadmium, silica, noise). Frequency and content dictated by the specific standard. |
| DOT/FMCSA physical | Commercial driver medical certification per 49 CFR 391.41. BP, vision 20/40 each eye, hearing, urine dipstick, mandatory form. Certificate up to 24 months. |
| FAA medical exam | Class 1 (ATP), Class 2 (commercial), Class 3 (private). Performed by Aviation Medical Examiners per the FAA Aviation Medical Examiners Guide. |
| Fit-testing (respirator) | Qualitative (saccharin, Bitrex, irritant smoke, isoamyl acetate) or quantitative (PortaCount). Required annually for every N95/half/full-face respirator per 29 CFR 1910.134. |
| Audiometry | Pure-tone air-conduction testing at 500, 1k, 2k, 3k, 4k, 6k Hz in each ear. Baseline and annual for noise-exposed workers. |
| Spirometry | FEV1, FVC, FEV1/FVC. Standardized per ATS/ERS; NIOSH-approved course required for OSHA surveillance spirometry. |
| Vision screening | Snellen distance, near, depth, color, phoria, horizontal field. |
| Drug & alcohol testing | DOT 5-panel or non-DOT panels; urine, hair, oral fluid, breath alcohol. MRO review of non-negatives. |
| Fitness-for-duty exam | Performed when an employer questions whether an employee can safely perform essential job functions after illness, injury, or behavioral concern. |
| Independent Medical Exam (IME) | One-time evaluation, not for treatment, answering specific causation, MMI, and impairment questions. |
| Functional Capacity Evaluation (FCE) | Multi-hour physical demand test; reports per DOT physical demand levels. |
| Impairment rating | Whole-person impairment via AMA Guides 6th Edition. |
| Return-to-Work (RTW) evaluation | Determines readiness to resume work, modified or full duty. |
| Ergonomic evaluation | Job-site or workstation analysis using NIOSH Lifting Equation, REBA, RULA. |
| Blood lead monitoring | BLL and ZPP per OSHA lead standard; frequency by exposure level. |
| Biological monitoring | Urine, blood, exhaled breath for specific exposures (e.g., urinary mercury, blood cadmium, urinary trichloroacetic acid for TCE). |
On every surveillance exam, confirm three things before the provider walks in: (1) the specific OSHA standard or regulation driving the exam (lead, asbestos, silica, noise, respiratory, etc.), (2) the worker's job title and specific exposures, and (3) any previous surveillance results available to trend. The note structure follows directly from the regulation.
19 Laboratory, Imaging & Biological Monitoring Diagnostics
Biological Exposure Indices (BEIs)
ACGIH publishes Biological Exposure Indices (BEIs) alongside TLVs — reference values for the concentration of a chemical or metabolite in blood, urine, or exhaled air that corresponds to air exposure at the TLV.
| Exposure | Biomarker | Matrix |
|---|---|---|
| Lead | Blood lead, ZPP | Blood |
| Cadmium | Cadmium, β-2-microglobulin | Blood, urine |
| Mercury (inorganic) | Mercury | Urine (24 hr) |
| Arsenic (inorganic) | Inorganic As + metabolites | Urine |
| Benzene | S-phenylmercapturic acid, trans,trans-muconic acid | Urine (end-shift) |
| Toluene | o-Cresol, hippuric acid | Urine |
| Trichloroethylene | Trichloroacetic acid | Urine |
| Carbon monoxide | Carboxyhemoglobin | Blood |
| Organophosphates | RBC / plasma cholinesterase | Blood |
| PAHs | 1-hydroxypyrene | Urine |
Imaging
Chest radiography remains the workhorse for pneumoconiosis surveillance; B-reader interpretation using the ILO classification is the standard. High-resolution CT is more sensitive but not used for routine surveillance. MRI is routine for MSK injuries; EMG/NCS confirms neuropathy and CTS.
Spirometry Interpretation
Occupational spirometry surveillance uses ATS/ERS 2019 technical standards. Key measurements are FEV1 (forced expiratory volume in 1 second), FVC (forced vital capacity), and the FEV1/FVC ratio. An FEV1/FVC below the lower limit of normal (LLN) or < 0.70 indicates obstruction; a reduced FVC with preserved ratio suggests restriction. Longitudinal monitoring uses a > 15% decline from baseline (or > 10% year over year, per NIOSH) as a trigger for further evaluation. Surveillance spirometry must be performed by a NIOSH-approved spirometry technician.
Risk Factors & Comorbidities to Document on Every Occupational Patient
Occupational history: Current job title, specific tasks, hours, shift pattern, duration in role. Prior jobs in reverse chronological order — the latency of many occupational diseases makes a 30-year-old exposure clinically relevant today.
Specific exposures: Chemicals, dusts, fumes, noise, vibration, radiation, ergonomic stressors, infectious hazards. Ask about known high-hazard tasks: welding, sandblasting, spray painting, pesticide application, solvent use, confined space entry.
PPE use: Type, consistency, fit-test history. "Wears an N95 when he remembers" is very different from "fit-tested to an N95 annually and uses one for all exposures."
Smoking: Pack-years and quit date. Many occupational exposures (asbestos, silica, radon, arsenic) interact multiplicatively with tobacco.
Alcohol and substances: Relevant for hepatotoxic co-exposures and DOT/safety-sensitive roles.
Hobbies: Home welding, woodworking, gun cleaning (lead), stained-glass soldering, auto body work can produce exposures as significant as occupational ones.
Residential environment: Home age (lead paint), well water (arsenic, nitrates), mold, radon, secondhand smoke.
Military history: Agent Orange, burn pits, Gulf War exposures, ionizing radiation, hearing hazards.
Comorbidities affecting fitness for duty: Cardiovascular disease, diabetes (especially insulin-treated), seizure disorder, OSA, substance use disorder, psychiatric conditions — all affect DOT/FAA/safety-sensitive certification.
20 Medications & Antidotes Pharmacology
| Medication | Use in OEM | Key Notes |
|---|---|---|
| Ibuprofen, naproxen (NSAIDs) | MSK injury, lateral epicondylitis, low back strain | Caution in CKD, ulcer disease |
| Acetaminophen | Analgesia when NSAIDs contraindicated | ≤ 3 g/day in liver disease |
| Cyclobenzaprine, methocarbamol | Acute muscle spasm | Sedating; flag for DOT drivers |
| Gabapentin, pregabalin | Neuropathic pain after CTS, peripheral neuropathy | Sedation, dizziness |
| Topical corticosteroids | Contact dermatitis | Mid/high potency for hand dermatitis |
| Antihistamines (cetirizine, loratadine) | Occupational urticaria, rhinitis | Non-sedating preferred for DOT |
| Inhaled corticosteroids, SABA, LABA | Occupational asthma | Exposure removal essential |
| Atropine + pralidoxime | Organophosphate toxicity | Atropine titrated to dry secretions; 2-PAM within hours |
| 100% O2, hyperbaric O2 | CO poisoning | HBO for severe / pregnancy |
| Hydroxocobalamin | Cyanide poisoning | Turns urine red; first-line |
| Sodium thiosulfate, sodium nitrite | Cyanide poisoning | Classic cyanide kit |
| Methylene blue | Methemoglobinemia | Avoid in G6PD deficiency |
| Succimer (DMSA) | Lead, arsenic, mercury chelation | Oral, outpatient |
| CaNa2-EDTA | Lead chelation (severe) | Parenteral, inpatient |
| BAL (dimercaprol) | Lead encephalopathy, arsenic, inorganic mercury | IM only; peanut oil vehicle |
| Deferoxamine | Iron overload / acute iron poisoning | Parenteral |
| Penicillamine | Copper chelation (Wilson, occupational) | Numerous adverse effects |
| Tetanus (Td, Tdap) | Wound prophylaxis ≥ every 10 y (5 y for dirty wounds) | Document last dose on every injury |
| HIV PEP (TDF/FTC + DTG or RAL) | Occupational HIV exposure | Start within 2 h; 28-day course |
| HBIG + HBV vaccine | Post-exposure in unvaccinated/non-responder | Within 24 h |
| Rabies PEP (HRIG + vaccine) | Animal bite in veterinarians, animal control | Day 0, 3, 7, 14 vaccine |
| Hepatitis B vaccine | Mandatory offer to HCWs per OSHA BBP standard | 3-dose series; check anti-HBs |
21 Classification Systems (AMA Guides, ILO, DOT, FAA, TLVs) Reference
ACGIH TLV Categories
TLV-TWA (Time-Weighted Average): Average airborne concentration for a conventional 8-hour workday, 40-hour workweek, to which nearly all workers may be repeatedly exposed without adverse effect.
TLV-STEL (Short-Term Exposure Limit): 15-minute TWA exposure that should not be exceeded at any time during a workday.
TLV-C (Ceiling): Concentration that should not be exceeded at any time.
Skin notation: Cutaneous absorption is a significant contribution to total body burden.
OSHA PEL Framework
OSHA Permissible Exposure Limits are legally enforceable (vs. advisory TLVs): PEL-TWA (8-hour average), PEL-STEL (15-min, where applicable), PEL-C (ceiling, never to be exceeded), and Action Level (typically half the PEL; triggers surveillance and training).
AMA Guides to the Evaluation of Permanent Impairment (6th Ed.) — Impairment Class Structure
| Class | Impairment Level | Typical WPI Range |
|---|---|---|
| Class 0 | No objective impairment | 0% |
| Class 1 | Mild | 1–13% |
| Class 2 | Moderate | 14–25% |
| Class 3 | Severe | 26–49% |
| Class 4 | Very Severe / Catastrophic | 50–100% |
Class placement is determined by diagnosis; grade within class is adjusted by functional history, physical exam, and clinical studies modifiers.
DOT/FMCSA Medical Certification (49 CFR 391.41)
Vision: 20/40 each eye (with or without correction), 70° horizontal field, distinguish red/amber/green.
Hearing: Perceive forced whisper at 5 ft or ≤ 40 dB average loss at 500/1000/2000 Hz.
Blood pressure: < 140/90 = 2-year certification; 140–159/90–99 = 1-year; 160–179/100–109 = 3-month one-time then 1-year; ≥ 180/110 = disqualified until controlled.
Diabetes: Insulin-treated diabetics require ITDM assessment form MCSA-5870.
Seizure disorder: Generally disqualifying; FMCSA exemptions available after long seizure-free intervals.
FAA Medical Certification Classes
| Class | For | Validity (under 40 / 40+) |
|---|---|---|
| Class 1 | Airline transport pilot (ATP) | 12 mo / 6 mo |
| Class 2 | Commercial pilot | 12 mo / 12 mo |
| Class 3 | Private / recreational | 60 mo / 24 mo |
NIOSH Lifting Equation — Recommended Weight Limit (RWL)
RWL = LC × HM × VM × DM × AM × FM × CM, where LC = 51 lb load constant, HM = horizontal multiplier, VM = vertical, DM = distance, AM = asymmetry, FM = frequency, CM = coupling. Lifting Index = actual weight / RWL; LI > 1 = above recommended limit; LI > 3 = high risk.
Heinrich's Safety Triangle
For every 1 major/disabling injury, there are approximately 29 minor injuries and 300 near-miss events with no injury. Used in safety culture to emphasize reporting of near-misses before they become major events.
22 Physical Exam — The Occupational Exam Exam
The occupational exam varies enormously by visit type, but these components appear across most encounters:
General: Vital signs including BP in the correct cuff size (large adult cuff if upper-arm circumference > 32 cm) seated after 5 minutes rest; BMI; grip strength bilaterally for MSK/hand evaluations.
HEENT: Uncorrected and corrected visual acuity each eye, visual fields, color vision (Ishihara), tympanic membranes, oral mucosa (for gingival lead line, mercury stomatitis).
Respiratory: Inspection, symmetric expansion, percussion, auscultation for crackles (Velcro in asbestosis), wheeze (OA, RADS), prolonged expiration.
Cardiovascular: Rate, rhythm, murmurs, peripheral pulses, edema.
Musculoskeletal/Neuro (focused by injury): Inspection, palpation for tenderness and swelling, active and passive range of motion (document in degrees), strength (0–5/5 MRC scale), provocative tests (Phalen, Tinel, Spurling, straight-leg raise, Neer, Hawkins, empty-can, Finkelstein), reflexes (0–4+), sensory exam (light touch, pinprick, monofilament for diabetic foot or neuropathy).
Skin: Document contact dermatitis distribution, callosities, Mees lines, hyperkeratosis, chloracne.
DOT-specific: Include hernia exam (male drivers), urine dipstick (protein, blood, sugar), and document all medications on the MER form.
23 Abbreviations Master List Reference
Regulatory & Agencies
Exposure Limits & Monitoring
Evaluations & Documentation
Clinical & Diagnostic
24 Sample HPI Templates Templates
These templates show the documentation rhythm expected in a busy occupational medicine clinic. Each one combines mechanism-specific detail with the regulatory/administrative elements that distinguish OEM notes from general practice.
"Mr. [Name] is a 42-year-old male warehouse order-picker referred by his employer for evaluation of low back pain sustained at work. Date of injury: [date] at approximately 10:30 AM. While lifting a 55-lb box from a lower shelf to a pallet at waist height, he felt a sudden sharp pain in the right lumbar paraspinal region. He reported the injury to his shift supervisor immediately and completed a written incident report. He denies prior history of back injury or chronic back pain. No radiation below the knee, no numbness, no weakness, no bowel or bladder dysfunction. Pain is rated 6/10 at rest, 8/10 with movement, worse with bending and twisting, better with rest and ice. He has taken over-the-counter ibuprofen with partial relief. He is right-hand dominant. No ED visit. Job duties include lifting 10–60-lb boxes approximately 200 times per shift. Work status since injury: off work since the injury for 1 day."
"Ms. [Name] is a 34-year-old female hair stylist presenting with a 3-month history of bilateral hand dermatitis. She describes dry, cracked, erythematous skin on the dorsal hands and web spaces that worsens during the workweek and partially improves on weekends. She uses permanent hair dye containing paraphenylenediamine, bleach, and shampoos without gloves for approximately 30% of her day. She has tried over-the-counter moisturizers and 1% hydrocortisone without significant improvement. Denies respiratory symptoms, facial involvement, or systemic features. No prior atopic dermatitis history. No nickel allergy. Currently performing regular duty with significant discomfort. Patch testing not previously performed."
"Mr. [Name] is a 56-year-old male Class A CDL holder presenting for DOT recertification. He drives long-haul refrigerated freight, approximately 2500 miles per week. Medical history is notable for hypertension on lisinopril 20 mg daily (self-reported home BP averaging 128/78), type 2 diabetes managed with metformin 1000 mg BID (last A1C 6.9% per PCP records), and obstructive sleep apnea on CPAP with documented ≥ 4 hours nightly use per compliance download. He denies seizures, cardiac events, syncope, vision changes, or new medications. He reports no symptomatic hypoglycemia in the past 12 months. Last DOT certification was 12 months ago (1-year card due to OSA). He brings current CPAP compliance report, PCP BP log, and most recent A1C."
"Ms. [Name] is a 28-year-old female registered nurse presenting for evaluation 90 minutes after a hollow-bore needlestick injury to the left index finger that occurred while recapping a 22-gauge needle after an IV start on the medical-surgical floor. The source patient is a 62-year-old male with known hepatitis C (last viral load undetectable on direct-acting antivirals) and HIV-negative status documented within the past month. Hepatitis B status of the source is pending. The exposed worker completed her full hepatitis B vaccine series in nursing school with documented anti-HBs > 10 mIU/mL. She immediately washed the site with soap and water and notified her charge nurse. She denies prior bloodborne pathogen exposures. She is not pregnant and is not breastfeeding. No current medications. Baseline labs drawn today; HIV PEP has been deferred pending further source testing and this evaluation."
"Mr. [Name] is a 51-year-old male drywall installer referred for Independent Medical Examination regarding a right shoulder injury sustained on [date of injury] while lifting a 12-ft sheet of drywall overhead. He initially presented to urgent care, was diagnosed with rotator cuff strain, and underwent 12 weeks of physical therapy followed by MRI demonstrating a full-thickness supraspinatus tear. Arthroscopic rotator cuff repair was performed on [date] by orthopedics; post-operative course included 6 weeks of sling immobilization and 16 weeks of physical therapy. He reports ongoing pain (4/10) with overhead activity and difficulty lifting more than 20 lb above shoulder level. This IME is requested to address: (1) causation, (2) whether he has reached maximum medical improvement, (3) permanent impairment rating, and (4) permanent work restrictions. Records reviewed include initial urgent care note, MRI report, operative report, and 34 physical therapy notes."
"Mr. [Name] is a 47-year-old male forklift operator returning for a return-to-work evaluation after a left ankle fracture sustained at work 10 weeks ago. He underwent open reduction and internal fixation with orthopedic follow-up confirming radiographic union and clearance for full weight-bearing. He has completed 6 weeks of physical therapy; he reports 80% recovery with mild residual stiffness and occasional aching at the end of a long day. He denies pain with walking on level surfaces, climbing in and out of the forklift cab, or operating foot pedals. His essential job functions include operating a sit-down forklift, occasional lifting up to 50 lb, and climbing 3 cab steps repeatedly. Employer has offered full-duty reinstatement pending medical clearance. Functional testing today demonstrated intact single-leg stance bilaterally, pain-free repetitive squatting, and full ankle range of motion within 10° of the unaffected side."
Occupational medicine notes serve more masters than any other specialty's documentation. The same chart is read by the patient, the employer, the workers' compensation insurer, the case manager, the claimant's attorney, the defense attorney, and occasionally OSHA investigators or IME reviewers. A great scribe in OEM understands this from day one and writes with precision, dates, specific mechanisms, and clean causation language.
Learn the regulatory vocabulary. When the physician says "this is a 1-year DOT card for BP in Stage 1 range," you should already be selecting the correct MCSA-5876 checkbox. When the physician says "work status: modified duty, no lifting over 15 lb, no overhead reaching, no ladder climbing for 2 weeks," you should write it exactly that way, with specific numbers and a specific review date. When a worker has a needlestick, you should already know what source testing to order and which PEP decision tree the physician will follow.
Occupational medicine is where clinical care, regulation, and workplace reality meet. The best scribes in this specialty bring a sharp eye for detail, a steady factual voice, and a deep respect for the worker on the other side of the desk. Welcome to the field.
25 References & Sources
Clinical Practice Guidelines
Regulatory Standards & Handbooks
OSHA. Occupational Noise Exposure. 29 CFR 1910.95.
OSHA. Respiratory Protection. 29 CFR 1910.134.
OSHA. Bloodborne Pathogens. 29 CFR 1910.1030.
OSHA. Lead (General Industry). 29 CFR 1910.1025.
OSHA. Asbestos. 29 CFR 1910.1001.
OSHA. Respirable Crystalline Silica. 29 CFR 1910.1053.
FMCSA. Medical Examiner Handbook and 49 CFR 391.41.
FAA. Guide for Aviation Medical Examiners.
NIOSH. Applications Manual for the Revised NIOSH Lifting Equation. DHHS Publication No. 94-110.
ACGIH. TLVs and BEIs (annual).
IARC Monographs on the Identification of Carcinogenic Hazards to Humans.
AMA Guides to the Evaluation of Permanent Impairment, 6th Edition.
Diagram & Figure Sources
Figure 1: Construction worker in safety equipment. Wikimedia Commons. Public domain.
Figure 2: Major Respiratory Organs. OpenStax College. CC BY 3.0.
Figure 3: Audiogram grid. Wikimedia Commons. Public domain.
Figure 4: Anatomy of the Human Ear. Chittka L, Brockmann A. CC BY 2.5.