Orthopedic Surgery
Every musculoskeletal diagnosis, fracture, procedure, medication, classification system, and documentation framework you need to survive day one in ortho clinic, the OR, and the ED.
All diagrams on this page are sourced from published educational or institutional materials rather than AI generation. Each figure caption links to the original source, and the full diagram and guideline citations are collected in the references section at the bottom.
01 Musculoskeletal Anatomy Essentials
Orthopedic surgery is the care of the musculoskeletal (MSK) system — bones, joints, ligaments, tendons, muscles, cartilage, menisci, peripheral nerves, and the spinal column. A scribe in ortho must be able to picture every major joint in three dimensions and know the structures the surgeon is about to name before they say them. Unlike most specialties, ortho documentation is relentlessly anatomic: "grade III MCL sprain," "full-thickness supraspinatus tear with 2 cm retraction," "Garden III left femoral neck fracture." If you do not know what the surgeon is describing, you cannot chart it.
Bones, Joints, and Joint Types
The skeleton is divided into the axial skeleton (skull, vertebral column, rib cage) and the appendicular skeleton (upper and lower extremities, pelvic and shoulder girdles). Long bones have a diaphysis (shaft), metaphysis (flare between shaft and end), epiphysis (articular end), and in skeletally immature patients a physis (growth plate). Fractures are described by which region they involve, because this changes fixation strategy.
Joints are classified as synovial (ball-and-socket hip/shoulder, hinge elbow/knee, saddle thumb CMC, plane facet joints, pivot radioulnar, condyloid wrist), cartilaginous (intervertebral discs, pubic symphysis), or fibrous (skull sutures, tibiofibular syndesmosis). Synovial joints have hyaline articular cartilage, a synovial membrane producing synovial fluid, a fibrous capsule, and supporting ligaments.
The Shoulder
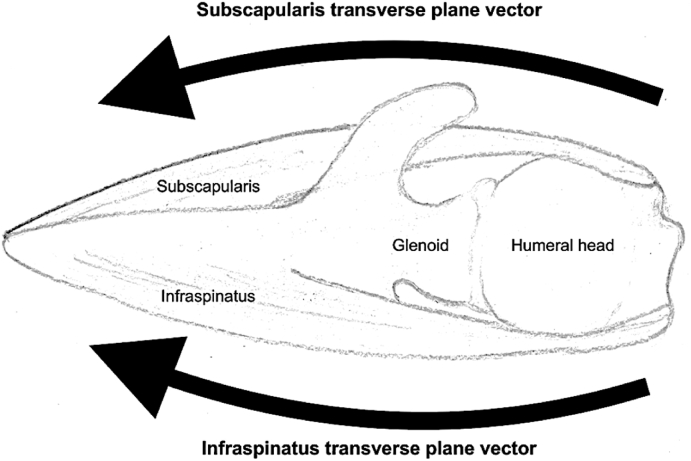
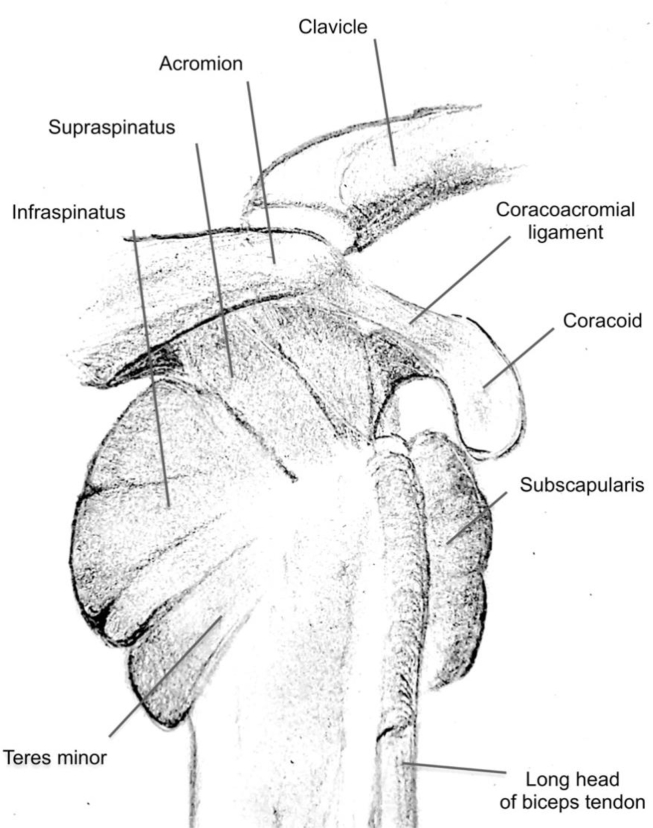
The shoulder is really three joints: the glenohumeral (GH) joint (humeral head on glenoid), the acromioclavicular (AC) joint, and the sternoclavicular (SC) joint, with a functional fourth — the scapulothoracic articulation. The rotator cuff is a group of four muscles: supraspinatus (abduction, the most commonly torn), infraspinatus and teres minor (external rotation), and subscapularis (internal rotation). The long head of the biceps tendon runs through the bicipital groove and inserts on the superior labrum. The glenoid labrum is a fibrocartilaginous ring that deepens the glenoid.
The Elbow, Wrist, and Hand
The elbow is a hinge (humeroulnar) combined with a pivot (radiocapitellar and proximal radioulnar). Key ligaments: ulnar collateral ligament (UCL) resists valgus (the "Tommy John" ligament), lateral ulnar collateral ligament (LUCL) resists posterolateral rotatory instability. The wrist has a proximal carpal row (scaphoid, lunate, triquetrum, pisiform) and distal row (trapezium, trapezoid, capitate, hamate). The scaphoid is clinically critical because of its tenuous retrograde blood supply from the radial artery, making fractures prone to nonunion and avascular necrosis. The hand has metacarpals and phalanges; the flexor tendons run in fibro-osseous sheaths (zones I–V), and the extensor mechanism has a complex hood apparatus over each digit.
The Spine
7 cervical, 12 thoracic, 5 lumbar vertebrae, plus sacrum and coccyx. Each motion segment has an intervertebral disc (nucleus pulposus surrounded by annulus fibrosus), paired facet (zygapophyseal) joints, ligamentum flavum, and anterior and posterior longitudinal ligaments. Nerve roots exit below their numbered pedicle in the cervical spine except C8 (there is no C8 vertebra) and above in the lumbar spine. Know the dermatomes and myotomes: C5 deltoid/biceps, C6 wrist extensors/brachioradialis, C7 triceps/wrist flexors, C8 finger flexors, T1 hand intrinsics, L2–L4 quadriceps/hip flexors, L5 EHL/tibialis anterior, S1 gastrocnemius/peroneals.
The Hip and Pelvis
Ball-and-socket joint: femoral head in the acetabulum, surrounded by the acetabular labrum. Blood supply to the femoral head comes mostly from the medial femoral circumflex artery via the deep branch; this is why displaced femoral neck fractures cause avascular necrosis. Landmarks you will hear: greater trochanter, lesser trochanter, intertrochanteric line, subtrochanteric region, femoral neck, and the iliopsoas inserting on the lesser trochanter.
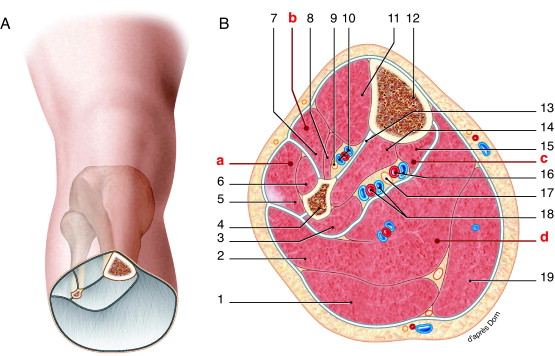
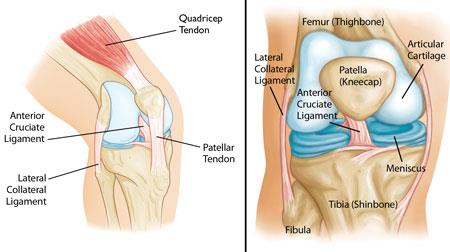
The Knee
A hinge joint with complex ligamentous and meniscal support. Four main ligaments: ACL (resists anterior tibial translation), PCL (posterior), MCL (valgus), LCL (varus). Two menisci (medial C-shaped, lateral more circular) distribute load and stabilize. The extensor mechanism is quadriceps tendon → patella → patellar tendon → tibial tubercle. The medial patellofemoral ligament (MPFL) is the primary restraint to lateral patellar dislocation.
The Ankle and Foot
The ankle mortise is formed by the distal tibia (plafond and medial malleolus), distal fibula (lateral malleolus), and talus. Lateral ligaments (ATFL, CFL, PTFL) are sprained most commonly. The syndesmosis (AITFL, PITFL, interosseous ligament) holds the distal tib-fib together and is disrupted in "high ankle sprains." The foot has hindfoot (talus, calcaneus), midfoot (navicular, cuboid, cuneiforms), and forefoot (metatarsals, phalanges). The Lisfranc ligament links the medial cuneiform to the 2nd metatarsal base and is critical to midfoot stability.
Ortho surgeons speak a hyper-specific anatomic language. When the attending says "full-thickness tear of the supraspinatus with retraction to the glenoid, Goutallier 3 fatty infiltration," you need to picture exactly what that means. Before each clinic, spend five minutes reviewing the joint anatomy of whatever sub-specialty you are in that day.
02 Scribe Documentation Framework
Ortho-Specific HPI Elements
An orthopedic HPI is anatomy-first and mechanism-driven. For every musculoskeletal complaint capture: laterality (right vs left vs bilateral, and hand dominance), mechanism of injury (MVC with restraint? fall from standing? twisting non-contact? overuse? insidious?), onset and duration, precise location (point tenderness vs diffuse), quality (mechanical, aching, burning, radiating), severity (VAS 0–10), aggravating/alleviating factors (activity, rest, NSAIDs, ice, bracing), prior treatments tried (PT, injections, bracing, activity modification, meds), prior injuries or surgeries to the same joint, imaging already performed, functional impact (work, ADLs, sleep disturbance), and neurovascular symptoms (numbness, tingling, weakness, color/temperature change).
CC: "Right knee pain," "s/p R THA POD 14," "left distal radius fracture s/p fall."
HPI must include: laterality, dominance, mechanism, date of injury, prior imaging (with findings), prior treatments, functional impact (job, sport, ADLs), prior ortho history at the involved joint, and neurovascular status.
ROS: Always a focused MSK ROS plus constitutional (fever/chills for infection), neuro (numbness, weakness), and for spine patients: bowel/bladder, saddle anesthesia (cauda equina screen).
PMHx: diabetes, smoking (affects fusion/healing), osteoporosis (DEXA T-score), inflammatory arthritis, gout, anticoagulation, prior DVT/PE, allergies (especially IV contrast, latex, cement).
Inspection: swelling, ecchymosis, deformity, erythema, surgical scars, gait (antalgic, Trendelenburg, foot drop).
Palpation: point tenderness at specific landmarks (the surgeon's finger location is the diagnosis half the time — document it).
Range of motion: active and passive, in degrees. "R shoulder: forward flexion 140, abduction 130, ER 40, IR to L3."
Strength: graded 0–5 by muscle group or specific manual test (empty can, lift-off, belly press, resisted knee extension).
Special tests: Lachman, anterior drawer, McMurray, Hawkins, Neer, Jobe, O'Brien, apprehension, Spurling, straight leg raise, FABER, FADIR — these are condition-specific and must be charted verbatim.
Neurovascular: pulses (DP, PT, radial), capillary refill, sensation to light touch in dermatomes, motor strength in myotomes. Always charted after injury/cast/post-op.
Numbered problem list with ICD-10 when available, followed by the specific plan: imaging ordered, PT referral, injection with drug/dose/site, medications, bracing, weight-bearing status (NWB, TTWB, PWB, WBAT, FWB), activity restrictions, work status/disability paperwork, follow-up interval, and surgical scheduling if applicable. For post-op visits, document POD number, wound status, suture/staple removal, and progression of WB and ROM.
Weight-bearing status is non-negotiable documentation. NWB (non-weight-bearing), TTWB (toe-touch), PWB (partial, usually 50%), WBAT (weight-bearing as tolerated), FWB (full). Every post-op and every fracture visit must have a WB status charted. Getting this wrong has medicolegal consequences.
03 Osteoarthritis — Hip, Knee, Shoulder, Hand, Ankle Degenerative
Osteoarthritis (OA) is the most common diagnosis in any general orthopedic clinic. It is a degenerative, wear-and-tear arthropathy characterized by progressive loss of articular hyaline cartilage, subchondral sclerosis, osteophyte formation, and subchondral cyst development. Unlike rheumatoid arthritis, it is non-inflammatory and non-systemic, although low-grade synovitis is common.
Pathophysiology & Presentation
Mechanical stress and biochemical changes lead to chondrocyte dysfunction, cartilage thinning and fibrillation, and eventual bone-on-bone contact. Patients describe activity-related joint pain, morning stiffness lasting less than 30 minutes (contrast to RA >1 hour), crepitus, reduced ROM, and functional decline. Hip OA classically presents as groin pain with weight-bearing, often with limp (Trendelenburg gait). Knee OA causes medial joint line pain, varus deformity ("bowlegged"), and difficulty with stairs. Shoulder OA presents with loss of external rotation, night pain, and crepitus. Hand OA targets the DIP (Heberden nodes), PIP (Bouchard nodes), and first CMC (thumb base). Ankle OA is most often post-traumatic (unlike the others).
Diagnostic Workup
OA is a clinical diagnosis supported by plain radiographs: weight-bearing AP and lateral of the knee/hip, bilateral standing for comparison. Findings follow the LOSS mnemonic: Loss of joint space, Osteophytes, Subchondral sclerosis, Subchondral cysts. MRI is not routinely needed for diagnosis but is ordered if there is concern for internal derangement (labral tear, meniscal tear, osteonecrosis). Labs are obtained only to rule out inflammatory, infectious, or crystal arthropathy.
Classification
| Grade | Findings |
|---|---|
| 0 | No radiographic features of OA |
| 1 | Doubtful joint-space narrowing, possible osteophytic lipping |
| 2 | Definite osteophytes, possible narrowing |
| 3 | Moderate multiple osteophytes, definite narrowing, some sclerosis, possible deformity |
| 4 | Large osteophytes, marked narrowing, severe sclerosis, definite deformity (bone-on-bone) |
| Grade | Findings |
|---|---|
| 0 | No signs of OA |
| 1 | Increased sclerosis, slight joint-space narrowing, no/slight loss of head sphericity |
| 2 | Small cysts, moderate joint-space narrowing, moderate loss of sphericity |
| 3 | Large cysts, severe narrowing/obliteration, severe deformity, avascular necrosis |
| Grade | Description |
|---|---|
| 0 | Normal cartilage |
| I | Softening and swelling |
| II | Partial-thickness defect with fissures < 1.5 cm, not reaching subchondral bone |
| III | Fissuring to subchondral bone, diameter > 1.5 cm |
| IV | Exposed subchondral bone |
Management
AAOS Management of Osteoarthritis of the Knee (3rd Edition) Clinical Practice Guideline and ACR/AF OA guidelines outline a stepwise approach. First-line: weight loss, activity modification, low-impact aerobic exercise, quadriceps strengthening, and patient education. Pharmacologic: topical NSAIDs (preferred for hand/knee), oral NSAIDs, acetaminophen (weak evidence but low risk), duloxetine for chronic pain. Intra-articular corticosteroid injections provide short-term relief (weeks to months). Hyaluronic acid injections (viscosupplementation) have weak evidence and are not recommended by AAOS. PRP remains investigational. Opioids are discouraged.
When non-operative therapy fails and the patient has end-stage radiographic OA plus functional impairment, the definitive treatment is arthroplasty — total hip, total knee, total shoulder, or reverse shoulder replacement. Indications and technique are covered in Section 16.
The surgeon will usually document "failed conservative management" as a prerequisite for insurance approval of arthroplasty. Chart this explicitly: list which PT sessions, which medications, which injections, and over what duration. Insurance denials frequently turn on this sentence.
04 Shoulder — Rotator Cuff, Impingement, AC Joint, Biceps Upper Extremity
Rotator Cuff Tears
Rotator cuff tears are among the most common shoulder diagnoses. They are categorized as partial-thickness (articular-sided, bursal-sided, or intrasubstance) or full-thickness (complete communication through the tendon). Full-thickness tears are further described by tear size: small (<1 cm), medium (1–3 cm), large (3–5 cm), or massive (>5 cm or involving ≥2 tendons). The supraspinatus is most commonly involved.
Tears may be acute traumatic (fall on outstretched hand, sudden traction) or chronic degenerative (attritional from impingement, vascular compromise at the critical zone). Patients present with lateral deltoid pain, night pain (classically "can't sleep on the affected side"), weakness in abduction and external rotation, and difficulty with overhead activities. Physical exam: positive Jobe's empty can test (supraspinatus), lift-off and belly press (subscapularis), external rotation lag and hornblower's (infraspinatus/teres minor). Drop arm suggests full-thickness tear.
Workup: radiographs (proximal humeral migration suggests chronic massive tear), MRI (gold standard). The AAOS CPG on Rotator Cuff Injuries guides management: non-operative first (PT, NSAIDs, subacromial steroid injection) for most degenerative tears; surgical repair for young active patients with acute traumatic tears, or those who fail conservative therapy. Arthroscopic rotator cuff repair (single-row, double-row, transosseous-equivalent) is standard. Massive irreparable tears in older patients are treated with reverse total shoulder arthroplasty.
| Stage | Muscle Appearance |
|---|---|
| 0 | Normal muscle, no fat |
| 1 | Some fatty streaks |
| 2 | Fat < muscle |
| 3 | Fat = muscle |
| 4 | Fat > muscle (irreparable territory) |
Subacromial Impingement
Impingement refers to painful compression of the rotator cuff (usually supraspinatus) and subacromial bursa between the humeral head and coracoacromial arch. Patients report anterolateral shoulder pain with overhead activity and a painful arc between 60°–120° of abduction. Positive Neer and Hawkins-Kennedy tests. Often associated with type II or III (hooked) acromion. Managed with PT, NSAIDs, subacromial injections; rarely, arthroscopic subacromial decompression.
AC Joint Pathology
AC osteoarthritis presents with focal pain at the AC joint, positive cross-body adduction, and relief with diagnostic injection. Traumatic AC separations are graded by the Rockwood classification (I–VI), based on coracoclavicular ligament disruption and direction of clavicle displacement. Grades I–II are managed non-operatively with sling; grade III is controversial; grades IV, V, VI are surgical.
Biceps Tendinopathy & Rupture
The long head of the biceps (LHB) commonly becomes inflamed, unstable in the bicipital groove, or frankly ruptures. LHB tendinitis presents with anterior shoulder pain and positive Speed's and Yergason's tests. LHB rupture produces the classic "Popeye" deformity (retracted muscle belly) with surprisingly minimal functional loss — often managed conservatively. Tenodesis (securing the tendon to the humerus) or tenotomy is indicated for symptomatic patients or as a concomitant procedure during rotator cuff or SLAP surgery.
05 Shoulder Instability, Labral Tears & Frozen Shoulder Upper Extremity
Glenohumeral Dislocation & Instability
The glenohumeral joint is the most commonly dislocated joint in the body. Over 95% of dislocations are anterior, caused by an abducted and externally rotated arm receiving a force. Posterior dislocations are classically associated with seizures and electrocution. Reduction is performed in the ED (Stimson, traction-countertraction, scapular manipulation), followed by post-reduction films and neurovascular check (axillary nerve sensation over the lateral deltoid).
A first-time anterior dislocation frequently causes a Bankart lesion (anteroinferior labral tear, with or without bony fragment) and a Hill-Sachs lesion (posterosuperior humeral head impaction fracture). Recurrence risk is high in young athletes (>50% in patients <25). Chronic instability is treated with arthroscopic Bankart repair; in patients with significant glenoid bone loss (>20–25%), the Latarjet procedure (transfer of coracoid with conjoined tendon to the anterior glenoid) is preferred.
SLAP Tears
Superior Labrum Anterior to Posterior (SLAP) tears involve the superior labrum at the biceps anchor. Classified by Snyder I–IV: I = fraying, II = detachment of biceps anchor, III = bucket handle, IV = bucket handle extending into biceps tendon. Presents with deep shoulder pain, painful clicking, and positive O'Brien active compression test. Managed with PT first, then arthroscopic SLAP repair or biceps tenodesis depending on age and demand.
Adhesive Capsulitis (Frozen Shoulder)
Idiopathic progressive stiffness with loss of both active and passive ROM, classically affecting external rotation first. Three phases: freezing (painful, 2–9 months), frozen (stiff, less painful, 4–12 months), thawing (gradual recovery, 5–26 months). Strongly associated with diabetes, thyroid disease, and post-immobilization states. Treatment: aggressive PT, intra-articular corticosteroid injection, occasionally manipulation under anesthesia (MUA) or arthroscopic capsular release for refractory cases.
06 Shoulder & Humerus Fractures Fracture
Proximal Humerus Fractures
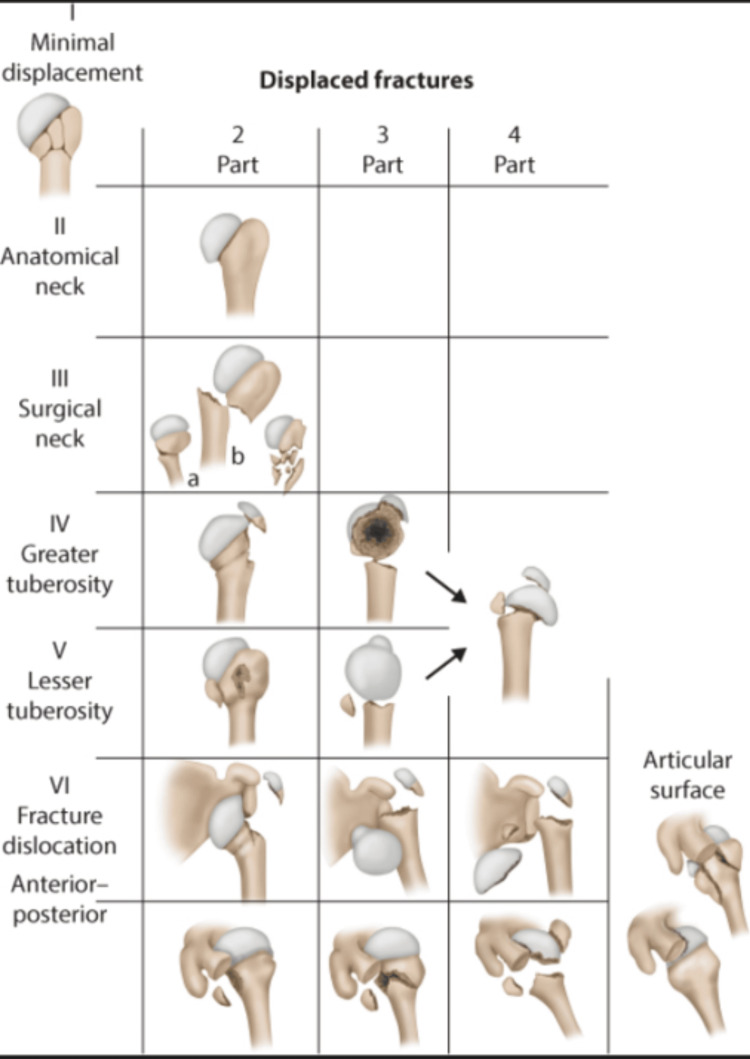
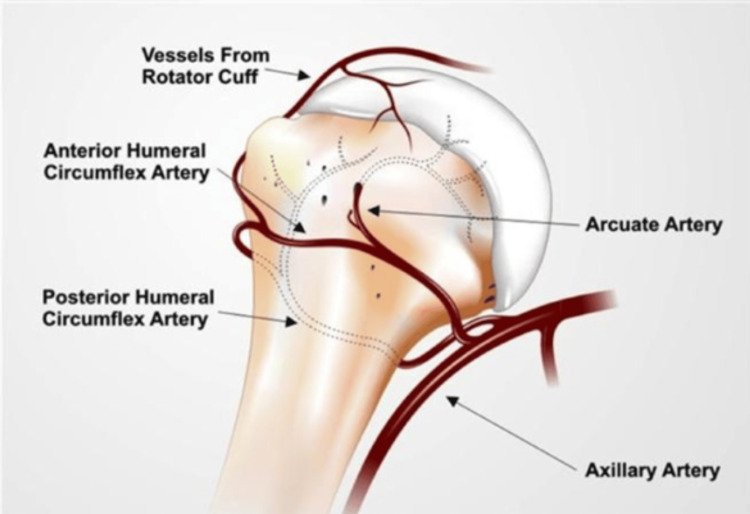
Common in elderly osteoporotic patients after low-energy falls. Classified by the Neer classification based on displacement (>1 cm or >45° angulation) of four segments: humeral head, greater tuberosity, lesser tuberosity, shaft. One-part (minimally displaced) fractures — 85% — are managed non-operatively with sling and early ROM. Two-, three-, and four-part fractures are displaced; management is individualized (ORIF with locking plate, intramedullary nail, hemiarthroplasty, or reverse total shoulder arthroplasty in elderly patients with poor bone quality). Key complication: avascular necrosis of the humeral head, especially in four-part fractures.

Humeral Shaft Fractures
Often from a direct blow or twisting injury. The radial nerve runs in the spiral groove and is at risk (up to 18% present with radial nerve palsy — "wrist drop"). Most are managed non-operatively in a Sarmiento functional brace, tolerating up to 30° varus, 20° anterior angulation, 3 cm shortening. ORIF is indicated for open fractures, vascular injury, polytrauma, segmental fractures, "floating elbow," and failed closed treatment.
07 Elbow — Epicondylitis, Tendon Ruptures, UCL, Fractures Upper Extremity
Lateral Epicondylitis ("Tennis Elbow")
Tendinosis of the extensor carpi radialis brevis origin at the lateral epicondyle. Overuse (not just tennis) in 35–55 year olds. Pain and tenderness at the lateral epicondyle, worse with resisted wrist extension and gripping. Treatment: activity modification, counterforce brace, eccentric strengthening, NSAIDs, corticosteroid injection (short-term benefit only), PRP (mixed evidence). Surgical debridement for refractory cases >6–12 months.
Medial Epicondylitis ("Golfer's Elbow")
Tendinosis of the flexor-pronator origin at the medial epicondyle. Less common than lateral. Beware the nearby ulnar nerve during injection or surgery.
Distal Biceps Tendon Rupture
Middle-aged men lifting heavy load with a flexed elbow. Sudden pop, ecchymosis, "reverse Popeye" (biceps retracts proximally), positive hook test (examiner cannot hook a finger under the tendon). Surgical repair within 3–4 weeks (single-incision or two-incision) is standard to preserve supination strength.
Triceps Tendon Rupture
Rare. Forced eccentric contraction against resistance. Inability to extend against gravity. Usually surgical repair.
UCL Injury
Overhead throwing athletes (baseball pitchers). Valgus stress during late cocking/early acceleration. Medial elbow pain, loss of velocity. MRI arthrogram is gold standard. Treatment: rest, PT, platelet-rich plasma, or UCL reconstruction (the "Tommy John" procedure) using palmaris longus or gracilis autograft.
Elbow Fractures
Distal humerus fractures (supracondylar in children, intra-articular in adults) often require ORIF with dual plating; watch for ulnar nerve and brachial artery injury. Olecranon fractures are treated with tension-band wiring (simple transverse fractures) or plate fixation (comminuted/oblique). Radial head fractures are classified by Mason: I = nondisplaced, II = displaced > 2 mm, III = comminuted, IV = with dislocation. Type I: sling and early motion. Type II: ORIF if mechanical block. Type III/IV: radial head arthroplasty or excision.
08 Forearm, Wrist & Hand Fractures Fracture
Forearm Shaft Fractures
"Both-bone forearm" fractures in adults require anatomic ORIF with compression plating because any malunion disrupts forearm rotation. Special named patterns: Monteggia (proximal ulnar shaft fracture with radial head dislocation), Galeazzi (distal radial shaft fracture with DRUJ disruption), Essex-Lopresti (radial head fracture with interosseous membrane disruption and DRUJ injury).
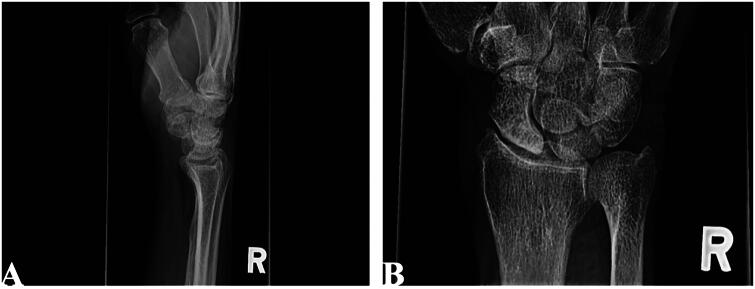
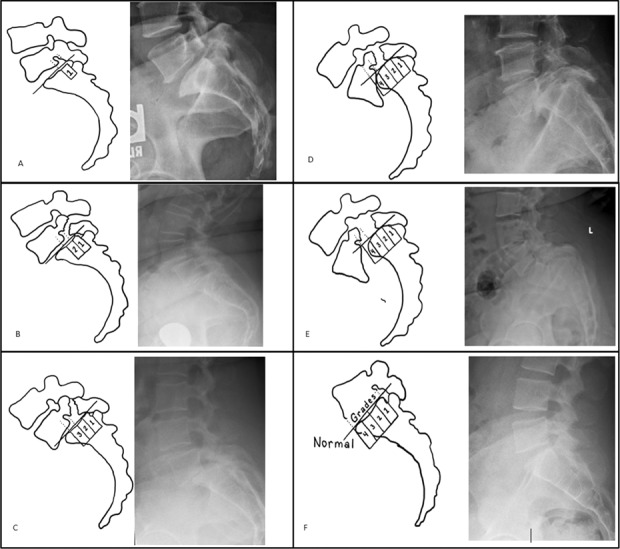
Distal Radius Fractures
The most common fracture in adults. Mechanism: FOOSH (fall on outstretched hand). Classic named patterns: Colles (dorsally angulated extra-articular, "dinner fork" deformity), Smith (volarly angulated, "garden spade"), Barton (intra-articular fracture-dislocation), chauffeur's (radial styloid).

| Type | Description |
|---|---|
| I | Extra-articular, no ulnar styloid fracture |
| II | Extra-articular, with ulnar styloid fracture |
| III | Intra-articular radiocarpal, no ulnar styloid |
| IV | Intra-articular radiocarpal, with ulnar styloid |
| V | Intra-articular radioulnar, no ulnar styloid |
| VI | Intra-articular radioulnar, with ulnar styloid |
| VII | Intra-articular radiocarpal + radioulnar, no ulnar styloid |
| VIII | Intra-articular radiocarpal + radioulnar, with ulnar styloid |
Management follows the AAOS Distal Radius Fracture CPG. Acceptable alignment: <5° dorsal tilt (from 11° volar tilt normal), <5 mm radial shortening, <2 mm articular step-off. Treatment: closed reduction with sugar-tong splint if acceptable; ORIF with volar locking plate for unstable or intra-articular patterns; external fixation or K-wires for severely comminuted fractures.
Scaphoid Fracture
Mechanism: FOOSH in young adult. Pain in the anatomic snuffbox. High index of suspicion because radiographs are often initially negative; MRI or repeat films at 2 weeks if clinical suspicion is high. Blood supply is retrograde from the radial artery through the distal pole — proximal pole fractures are at high risk for nonunion and AVN. Non-displaced fractures: long-arm thumb spica cast for 6–12 weeks. Displaced, proximal pole, or nonunion: percutaneous or open screw fixation (Herbert screw).
Hand Fractures
Metacarpal fractures: The "boxer's fracture" is a 5th metacarpal neck fracture from a closed-fist punch — up to 40° of angulation is tolerated at the 5th. Phalanx fractures: most managed with buddy taping or splinting; ORIF for rotational deformity (check with fingernail alignment on flexion) or intra-articular displacement. Bennett/Rolando fractures of the thumb base CMC are intra-articular and usually need fixation.
09 Hand & Wrist Soft-Tissue Conditions Upper Extremity
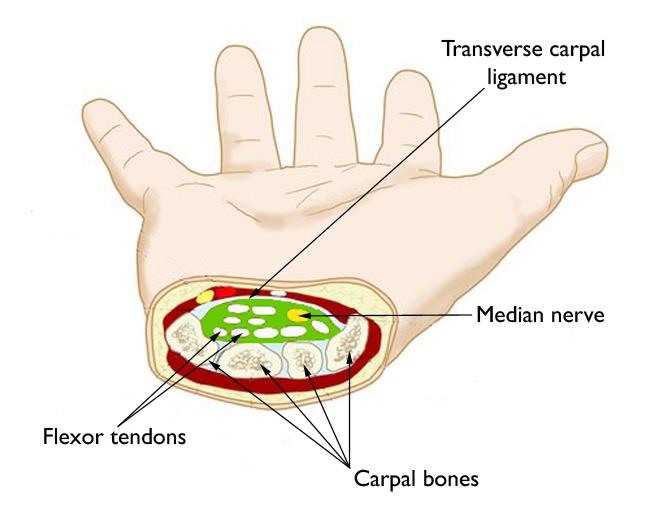
Carpal Tunnel Syndrome
Median nerve compression at the wrist under the transverse carpal ligament. Numbness and paresthesia in the thumb, index, middle, and radial half of the ring finger; worse at night; relieved by shaking the hand ("flick sign"). Thenar atrophy in advanced disease. Exam: positive Tinel, Phalen, carpal compression test. EMG/NCS confirms. Treatment: night splinting, NSAIDs, corticosteroid injection, and carpal tunnel release (open or endoscopic) for refractory cases.
Cubital Tunnel Syndrome
Ulnar nerve compression at the elbow. Numbness in the small finger and ulnar half of the ring finger, weak grip (first dorsal interosseous weakness), positive Tinel at the medial elbow, Froment sign, Wartenberg sign. Treatment: elbow extension splinting at night, activity modification, and ulnar nerve decompression with or without transposition.
Trigger Finger (Stenosing Tenosynovitis)
Thickening/inflammation of the A1 pulley causing catching or locking of the flexor tendon. Palmar nodule at the MCP level. Treated with corticosteroid injection (successful in 60–80%) or A1 pulley release.
de Quervain Tenosynovitis
Stenosing tenosynovitis of the first dorsal compartment (APL and EPB). Pain over the radial styloid, positive Finkelstein test. Treatment: thumb spica splint, NSAIDs, corticosteroid injection, surgical release.
Dupuytren Contracture
Progressive fibroproliferative disorder of the palmar fascia causing nodules, cords, and flexion contractures (usually ring and small fingers). Northern European descent, males, diabetics. Treatment: observation for non-disabling disease; collagenase (Xiaflex) injection, needle aponeurotomy, or fasciectomy for MCP contracture >30° or any PIP contracture.
Finger Tendon Injuries
Mallet finger: avulsion of the terminal extensor tendon from the distal phalanx ("baseball finger"); DIP stuck in flexion. Treated with full-time DIP extension splinting for 6–8 weeks. Boutonnière deformity: central slip disruption causing PIP flexion and DIP hyperextension. Swan-neck deformity: PIP hyperextension and DIP flexion from volar plate insufficiency or mallet finger sequelae.
Ganglion Cyst
Most common wrist mass; fluid-filled from joint or tendon sheath. Dorsal (over scapholunate ligament) or volar (over radial artery — beware). Observation, aspiration, or excision.
10 Spine — Disc Herniation, Stenosis, Cervical Disease Spine
Lumbar Disc Herniation
Nucleus pulposus herniates through a defect in the annulus fibrosus, compressing a nerve root. Most common at L4–L5 and L5–S1. Patients report acute low back pain radiating down the leg (sciatica) in a dermatomal distribution, worse with flexion, sitting, coughing, Valsalva. Exam: positive straight leg raise, sensory loss, weakness, and reflex loss in the affected dermatome/myotome. Most resolve with conservative care (NSAIDs, PT, epidural injection) over 6–12 weeks. Microdiscectomy for refractory radiculopathy, progressive weakness, or cauda equina.
Saddle anesthesia, bowel/bladder dysfunction (urinary retention is the classic finding), bilateral lower extremity weakness. Requires emergent MRI and urgent surgical decompression within 24–48 hours to avoid permanent deficit. Always screen for this in any back pain patient.
Lumbar Spinal Stenosis
Age-related narrowing of the central canal, lateral recess, or foramen from hypertrophy of ligamentum flavum, facet arthropathy, and disc bulging. Classic presentation: neurogenic claudication — bilateral lower extremity heaviness, burning, or cramping with walking or standing, relieved by sitting or leaning forward (the "shopping cart sign"). Distinguish from vascular claudication (relieved by simply stopping). Treatment: PT, epidural injections; decompressive laminectomy ± fusion for refractory cases.
Cervical Disc Herniation & Myelopathy
Cervical radiculopathy presents with neck pain radiating to the arm in a dermatomal pattern, positive Spurling test. Cervical myelopathy is cord compression with upper motor neuron signs: hand clumsiness, gait imbalance, hyperreflexia, positive Hoffmann, clonus, Babinski. Treatment: ACDF (anterior cervical discectomy and fusion), cervical disc arthroplasty, or posterior laminectomy/laminoplasty for multi-level disease.
11 Hip & Femur Fractures Fracture
Hip Fractures Overview
Hip fractures in the elderly are a major source of morbidity and mortality — 1-year mortality approaches 20–30%. Divided anatomically into: femoral neck (intracapsular), intertrochanteric (extracapsular), and subtrochanteric.
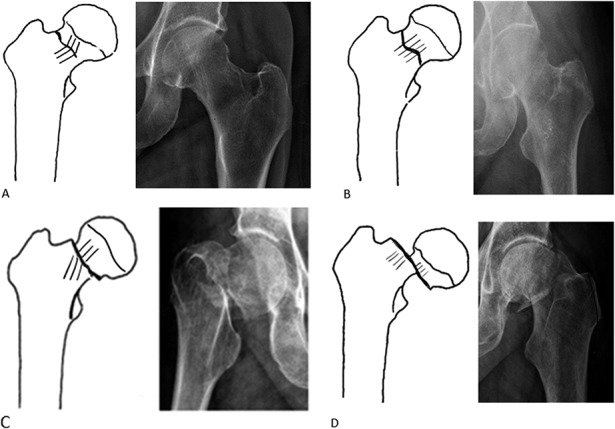
Femoral Neck Fractures
| Type | Description |
|---|---|
| I | Incomplete, valgus impacted |
| II | Complete, nondisplaced |
| III | Complete, partially displaced |
| IV | Complete, fully displaced |
Garden I–II: percutaneous cannulated screws or sliding hip screw. Garden III–IV in the elderly: hemiarthroplasty or total hip arthroplasty (THA is preferred for active, cognitively intact patients per AAOS Management of Hip Fractures in Older Adults CPG). In young patients, urgent ORIF within 12–24 hours is preferred to preserve the femoral head. Pauwels classification (I < 30°, II 30–50°, III > 50° from horizontal) predicts shear forces and nonunion risk.
Intertrochanteric Fractures
Extracapsular, between the greater and lesser trochanters. Good blood supply, heal well. Fixed with sliding hip screw (DHS) for stable patterns or cephalomedullary nail (CMN) for unstable patterns.
Subtrochanteric Fractures
Within 5 cm distal to the lesser trochanter. High mechanical stress region. Almost always treated with long cephalomedullary nail. Watch for atypical femur fractures in patients on long-term bisphosphonates.
Femoral Shaft Fractures
High-energy injury in young patients (MVCs, falls from height). Usually treated with reamed, locked, antegrade intramedullary nail. Assess for ipsilateral femoral neck fracture (10%) and ligamentous knee injury.
Distal Femur Fractures
Bimodal distribution: young high-energy or elderly osteoporotic. Intra-articular involvement common. Treated with lateral locked plating or retrograde intramedullary nail.
12 Knee — Ligament & Meniscus Injuries, Patellar Disorders Lower Extremity
ACL Tear
Non-contact pivoting injury in an athlete. Audible "pop," immediate swelling (hemarthrosis), giving way. Exam: positive Lachman (most sensitive), anterior drawer, pivot shift. MRI confirms. Treatment: PT with bracing for low-demand patients; ACL reconstruction (autograft: bone-patellar tendon-bone, hamstring, quadriceps tendon; or allograft) for young, active, or multi-ligament injured patients.
PCL Tear
Dashboard injury (posteriorly directed force on flexed knee) or hyperflexion. Positive posterior drawer and posterior sag. Isolated grade I–II tears are managed non-operatively. Grade III, multi-ligament, or avulsion injuries are surgical.
MCL and LCL Injuries
MCL: valgus blow to lateral knee. Most heal with bracing alone. LCL: varus blow (rare, usually part of posterolateral corner injury). PLC injuries often need surgical reconstruction.
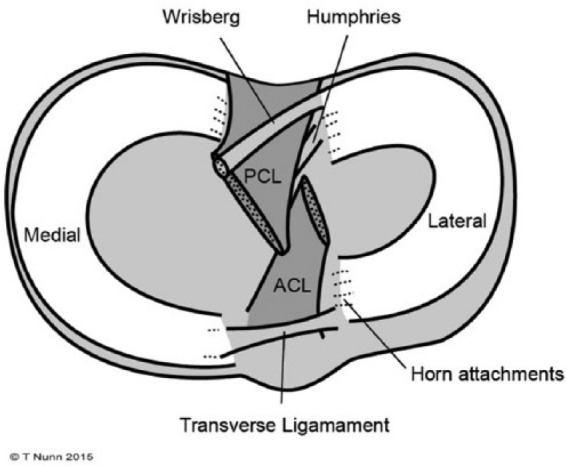
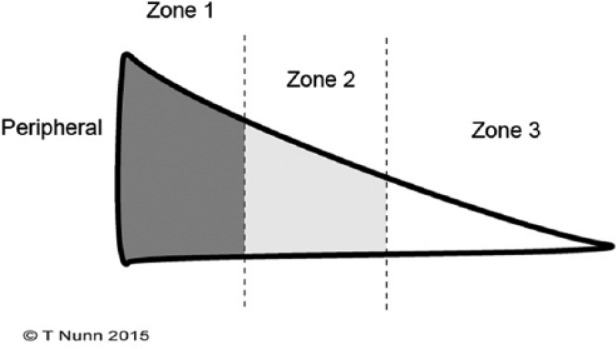
Meniscus Tears
Twisting on a planted foot. Joint line tenderness, effusion, positive McMurray, Thessaly, catching/locking. MRI confirms. Degenerative tears in older patients: conservative care (PT, NSAIDs, injection). Acute traumatic tears in young patients: arthroscopic meniscal repair (if in vascular "red zone") or partial meniscectomy. Evidence supports PT before arthroscopy for degenerative tears.
Patellar Dislocation & Patellofemoral Pain
Patellar dislocation is usually lateral, with MPFL rupture. First-time dislocations are typically reduced and braced; recurrent instability is treated with MPFL reconstruction. Patellofemoral pain syndrome ("runner's knee") presents with anterior knee pain worse with stairs and prolonged sitting ("theater sign"); treated with PT emphasizing VMO and hip abductor strengthening.
IT Band Syndrome
Lateral knee pain in runners at the lateral femoral epicondyle; positive Ober test. PT, activity modification, foam rolling.
13 Tibia, Ankle & Foot Fractures Fracture
Patellar Fracture
Direct blow or forceful eccentric quadriceps contraction. Inability to perform straight leg raise indicates extensor mechanism disruption. Nondisplaced: cylinder cast 4–6 weeks. Displaced or extensor lag: ORIF with tension-band wiring.
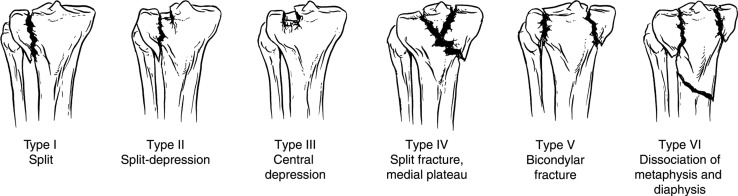
Tibial Plateau Fracture
Axial load with varus/valgus force. The Schatzker classification guides management.
| Type | Description |
|---|---|
| I | Lateral plateau split (no depression) |
| II | Lateral plateau split with depression |
| III | Lateral plateau pure depression |
| IV | Medial plateau fracture |
| V | Bicondylar (both plateaus) |
| VI | Plateau fracture with metaphyseal/diaphyseal dissociation |
Tibial Shaft Fractures
Most common long-bone fracture. High rate of open injury because of thin anterior soft-tissue envelope. Reamed intramedullary nailing is standard for diaphyseal fractures; external fixation for contaminated open fractures initially. Always assess for compartment syndrome.
Ankle Fractures
Classified by Weber (level of fibular fracture) and Lauge-Hansen (mechanism).

| Type | Description | Syndesmosis |
|---|---|---|
| A | Fibula fracture below syndesmosis | Intact |
| B | Fibula fracture at level of syndesmosis | Partial/variable injury |
| C | Fibula fracture above syndesmosis | Disrupted, requires fixation |
Lauge-Hansen divides fractures by foot position + deforming force: supination-adduction, supination-external rotation (most common), pronation-abduction, pronation-external rotation. Trimalleolar fracture involves medial, lateral, and posterior malleoli — almost always surgical. Management: stable isolated lateral malleolus fractures may be treated in a walking boot; unstable patterns and any talar shift require ORIF.
Pilon Fractures
High-energy axial load driving the talus into the tibial plafond. Massive soft-tissue injury. Staged protocol: external fixation first, ORIF when soft tissues permit (often 10–21 days).
Lisfranc Injury
Tarsometatarsal joint disruption from axial load on a plantarflexed foot. Subtle — watch for midfoot ecchymosis, tenderness at the base of the 2nd metatarsal, and widening between the 1st and 2nd metatarsals on weight-bearing films. Missed injuries cause permanent disability. Treatment: ORIF or primary arthrodesis.

Calcaneal Fracture
Fall from height. Assess for associated lumbar burst fracture. Intra-articular fractures (Sanders classification) may need ORIF via extensile lateral or sinus tarsi approach; high wound complication rate. Non-operative treatment remains common because of complications.
14 Foot & Ankle Soft-Tissue Conditions Lower Extremity
Achilles Tendon Rupture
Middle-aged "weekend warrior" with sudden calf pain and "pop" during push-off. Positive Thompson test (squeezing the calf does not plantarflex the foot). Palpable gap. Treatment: functional bracing with progressive weight-bearing protocol OR surgical repair — both acceptable with similar re-rupture rates if early functional rehab is used.

Plantar Fasciitis
Heel pain worst with the first steps in the morning. Tenderness at the medial calcaneal tubercle. Treatment: stretching (plantar fascia and gastrocnemius), night splinting, orthotics, NSAIDs, corticosteroid injection (risk of fat-pad atrophy and rupture), ESWT, endoscopic release in refractory cases.
Morton Neuroma
Perineural fibrosis of the interdigital nerve, typically in the 3rd webspace. Burning forefoot pain radiating to toes, positive Mulder click. Treated with metatarsal pads, wide-toe-box shoes, injection, or surgical excision.
Hallux Valgus (Bunion)
Lateral deviation of the great toe with medial prominence of the 1st metatarsal head. Treated conservatively with wide-toe shoes, spacers, orthotics. Surgical bunionectomy (chevron, scarf, Lapidus, Akin osteotomy) for refractory pain.
Hammer Toe
Flexion deformity of the PIP joint. Managed with padding and shoe modification; surgical correction with PIP arthrodesis or flexor tenotomy/transfer for refractory cases.
15 Infection, Tumor, Pediatric & Compartment Syndrome Miscellaneous
Septic Arthritis
Acute joint pain, warmth, effusion, refusal to move, fever. Most common in knee and hip; Staph aureus is the #1 pathogen. Urgent arthrocentesis: synovial WBC typically >50,000 with >75% PMN. Treatment is emergent surgical washout (arthroscopic or open) plus IV antibiotics. Kocher criteria (pediatric hip): fever >38.5, ESR >40, WBC >12,000, NWB on affected side.
Osteomyelitis
Bone infection. Acute hematogenous (children, metaphysis) or contiguous/post-traumatic (adults). Labs: elevated ESR/CRP. MRI is the imaging of choice. Treatment: 4–6 weeks IV antibiotics, surgical debridement for sequestrum or hardware involvement.
Compartment Syndrome
The 6 Ps: Pain out of proportion, Pain with passive stretch, Pressure (tense compartment), Paresthesia, Pallor, Pulselessness (late). Most often after tibial shaft fractures, supracondylar humerus fractures in kids, and crush injuries. Compartment pressures >30 mmHg or ΔP (DBP − compartment pressure) <30 mmHg confirms. Treatment: emergent fasciotomy of all compartments. Delay causes Volkmann ischemic contracture.
Bone Tumors (Overview)
Benign: osteochondroma (most common benign bone tumor), giant cell tumor (GCT, "soap bubble" around the knee in young adults), non-ossifying fibroma, enchondroma. Malignant primary: osteosarcoma (teens, around the knee, Codman triangle, sunburst periosteal reaction), Ewing sarcoma (teens, diaphysis, onion-skinning, translocation t(11;22)), chondrosarcoma (adults). Metastatic: far more common than primary — breast, prostate, lung, renal, thyroid (BLT with a Kosher Pickle). Pathologic fractures and impending fractures (Mirels score ≥9) are treated with prophylactic IM nailing or plating plus postop radiation.
Pediatric Orthopedics
DDH (developmental dysplasia of the hip): Ortolani and Barlow maneuvers in newborns; treated with Pavlik harness (<6 months), closed/open reduction and spica (older). SCFE (slipped capital femoral epiphysis): overweight adolescent with hip or knee pain and out-toeing; urgent in situ screw fixation. Legg-Calvé-Perthes: idiopathic AVN of the femoral head in 4–8 year olds; treated based on age and extent of head involvement. Clubfoot (talipes equinovarus): Ponseti casting followed by Achilles tenotomy. Scoliosis: observation, bracing (Cobb angle 25–45° in growing child), posterior spinal fusion (>45–50°).
| Type | Description |
|---|---|
| I | Straight through physis (Slip) |
| II | Through physis and up through metaphysis (Above) — most common |
| III | Through physis and down through epiphysis (Lower) |
| IV | Through metaphysis, physis, and epiphysis (Through) |
| V | Crush injury of physis (cRushed) — worst prognosis |
Open Fractures
| Type | Description |
|---|---|
| I | Wound < 1 cm, clean, minimal soft-tissue damage |
| II | Wound 1–10 cm, moderate soft-tissue damage |
| IIIA | Wound > 10 cm, adequate soft-tissue coverage |
| IIIB | Extensive soft-tissue loss, periosteal stripping, requires flap |
| IIIC | Any open fracture with arterial injury requiring repair |
All open fractures require tetanus prophylaxis, IV antibiotics within 1 hour (cefazolin ± gentamicin for IIIA+; add penicillin for farm/contaminated wounds), and urgent debridement within 24 hours per OTA open fracture guidelines.
Fracture Nonunion & Malunion
Nonunion = failure to heal within 6–9 months; classified as atrophic (poor biology/vascularity) or hypertrophic (inadequate stability). Treated with revision ORIF, bone grafting, BMP, or bone stimulator. Malunion = healed in unacceptable alignment; may need corrective osteotomy.

16 Orthopedic Procedures A–Z
Arthroplasty (Joint Replacement)
- Total Hip Arthroplasty (THA): Replacement of femoral head with metal/ceramic ball on a stem, and acetabulum with a polyethylene-lined metal cup. Approaches: direct anterior (Hueter interval, muscle-sparing, lower dislocation rate), posterior (Kocher-Langenbeck, most common, higher posterior dislocation rate), lateral (Hardinge). Cemented vs. cementless fixation.
- Hip Resurfacing: Alternative that preserves the femoral head and neck; metal-on-metal; used in younger active males.
- Hemiarthroplasty: Replacement of the femoral head only (acetabulum native); used for displaced femoral neck fractures in low-demand elderly.
- Total Knee Arthroplasty (TKA): Resurfacing of distal femur, proximal tibia, and often patella with metal and polyethylene components. Cruciate-retaining vs. posterior-stabilized designs.
- Total Shoulder Arthroplasty (TSA): For primary glenohumeral OA with intact rotator cuff; anatomic humeral head and glenoid component.
- Reverse Total Shoulder Arthroplasty (rTSA): Ball on glenoid, socket on humerus — used for rotator cuff arthropathy, massive irreparable cuff tears, failed TSA, and complex proximal humerus fractures. Relies on deltoid rather than rotator cuff.
Arthroscopy
- Knee arthroscopy: partial meniscectomy, meniscal repair, ACL reconstruction (with BTB, hamstring, quad, or allograft), MPFL reconstruction, loose body removal, chondroplasty.
- Shoulder arthroscopy: rotator cuff repair (single-row, double-row, transosseous-equivalent), subacromial decompression, Bankart repair, SLAP repair, biceps tenodesis, AC joint resection (Mumford), capsular release.
- Hip arthroscopy: labral repair, femoroacetabular impingement (cam/pincer) decompression.
- Elbow arthroscopy: loose body removal, OCD debridement, capsular release.
- Wrist arthroscopy: TFCC repair, ganglion excision.
- Ankle arthroscopy: anterior impingement, OCD lesions.
Fracture Fixation
- ORIF (open reduction and internal fixation): plates and screws (compression, locking, bridge); used everywhere.
- CRPP (closed reduction and percutaneous pinning): K-wires placed percutaneously; common in pediatric supracondylar humerus and distal radius fractures.
- Intramedullary (IM) nailing: reamed/unreamed nails in femur (antegrade or retrograde), tibia, humerus. Cephalomedullary nails for intertrochanteric/subtrochanteric hip fractures.
- External fixation: pin-based frame outside the skin; used as temporizing ("damage control") or definitive for open/contaminated fractures.
- Hemiarthroplasty / arthroplasty: for displaced femoral neck fractures, comminuted proximal humerus.
Other Major Procedures
- Arthrodesis (fusion): surgical fusion of a joint — wrist, ankle, subtalar, 1st MTP, cervical/lumbar spine — to eliminate painful motion.
- Osteotomy: cutting and realigning bone to offload an arthritic compartment (high tibial osteotomy for medial compartment knee OA).
- Amputation: BKA (below-knee), AKA (above-knee), transmetatarsal, ray, toe, finger.
- Soft-tissue: carpal tunnel release, cubital tunnel release/transposition, trigger finger release, de Quervain release, tendon repair, tenodesis, bunionectomy, hammer toe correction (PIP fusion, flexor transfer).
17 Post-Op Care & Complications
Standard Post-Op Course
For every post-op visit you must document: POD number, wound status (incision clean/dry/intact, erythema, drainage, dehiscence), surgical site pain, sensation and motor function distal to surgery, pulses/perfusion, ROM achieved, WB status progression, PT/OT engagement, DVT prophylaxis compliance, and pain medication use.
POD 0–1: out of bed, PT initiated, WBAT with walker. POD 1–2: home or SNF discharge for most. Week 2: suture/staple removal, incision check. Week 6: off walker to cane. Week 12: most ADLs resumed. Full recovery 6–12 months.
Common Complications
- VTE (DVT/PE): Highest risk after TKA/THA and hip fracture. Prophylaxis with aspirin, LMWH (enoxaparin), DOACs (rivaroxaban, apixaban), or warfarin per AAOS VTE prophylaxis CPG and CHEST guidelines.
- Periprosthetic joint infection (PJI): Early (<3 months), delayed, or late. Fever, drainage, pain, elevated ESR/CRP. Aspirate: synovial WBC >3,000 and PMN >80% suggest PJI. Treatment: debridement and implant retention (DAIR), 1- or 2-stage revision with antibiotic spacer.
- Dislocation (post THA): Posterior approach > anterior. Precautions: avoid flexion > 90°, internal rotation, adduction past midline.
- Aseptic loosening: Most common cause of revision arthroplasty in the long term.
- Neurovascular injury: Peroneal nerve (TKA), sciatic nerve (THA posterior approach), axillary nerve (shoulder).
- Fat embolism: Long-bone or pelvic fractures, typically 24–72 hours after injury. Triad: hypoxemia, neurologic changes, petechial rash.
- CRPS (complex regional pain syndrome): Disproportionate burning pain, allodynia, trophic changes, edema. Early recognition and PT.
- Nonunion, malunion, hardware failure (covered in Section 15).
18 Imaging & Diagnostics
Plain Radiographs
The workhorse of orthopedics. Always order at least two orthogonal views (AP and lateral) — "one view is no view." For joints, add obliques; for hips, add pelvis AP and frog-leg lateral; for knees, add weight-bearing PA flexion (Rosenberg) view and sunrise/merchant; for feet/ankles, always weight-bearing. Describe fractures by: bone, location (proximal/middle/distal third or specific region), pattern (transverse, oblique, spiral, comminuted, segmental), displacement (percent and direction), angulation (degrees and apex), shortening, rotation, articular involvement, and open vs. closed.
CT
For complex fractures (tibial plateau, pilon, calcaneus, acetabulum, spine), pre-op planning (arthroplasty templating), occult scaphoid or hip fractures (after negative XR), and tumor workup. CT angiography for suspected arterial injury with fracture/dislocation.
MRI
Soft-tissue and occult bone pathology: rotator cuff tears, labral tears, meniscal/ligamentous knee injuries, disc herniation, stress fractures, osteomyelitis, AVN, bone/soft-tissue tumors. MR arthrogram improves sensitivity for labral tears (hip, shoulder).
Ultrasound
Dynamic evaluation of tendons (rotator cuff, Achilles, biceps), guidance for injections and aspirations.
DEXA
Bone mineral density. T-score > −1 normal, −1 to −2.5 osteopenia, < −2.5 osteoporosis. Screening recommended in women ≥65 and men ≥70 per USPSTF.
Labs
CBC, CMP, ESR, CRP for infection workup; coagulation and type/screen pre-op; uric acid and synovial fluid crystals for gout; RF, anti-CCP, ANA for inflammatory arthritis workup.
19 Medications You Must Know
| Drug | Brand | Class / Mechanism | Use | Notes |
|---|---|---|---|---|
| Acetaminophen | Tylenol | Analgesic | First-line OA pain | Max 3 g/day; caution in liver disease |
| Ibuprofen | Motrin, Advil | NSAID (COX-1/2) | OA, tendonitis, post-op | GI, renal, CV risk |
| Naproxen | Aleve | NSAID | OA, musculoskeletal pain | Lowest CV risk of NSAIDs |
| Meloxicam | Mobic | Preferential COX-2 | OA, RA | Once daily dosing |
| Celecoxib | Celebrex | Selective COX-2 | OA, RA | Sulfa allergy caution |
| Diclofenac gel | Voltaren | Topical NSAID | Hand/knee OA | First-line in elderly |
| Tramadol | Ultram | Weak opioid / SNRI | Moderate pain | Seizure risk, serotonin syndrome |
| Oxycodone | OxyContin, Roxicodone | Opioid | Short-term post-op pain | Controlled; limit to 3–7 days |
| Hydrocodone/APAP | Norco, Vicodin | Opioid combo | Post-op | Watch APAP ceiling |
| Cyclobenzaprine | Flexeril | Muscle relaxant | Acute muscle spasm | Sedating; short-term |
| Methocarbamol | Robaxin | Muscle relaxant | Low back pain | Less sedating |
| Gabapentin | Neurontin | Gabapentinoid | Neuropathic pain, sciatica | Renal dose adjust |
| Pregabalin | Lyrica | Gabapentinoid | Neuropathic pain | Controlled substance |
| Duloxetine | Cymbalta | SNRI | Chronic OA/back pain | FDA-approved for chronic MSK pain |
| Methylprednisolone | Depo-Medrol | IA corticosteroid | IA injection (knee, shoulder, hip) | Limit to 3–4/year/joint |
| Triamcinolone | Kenalog | IA corticosteroid | IA injection | Watch subcutaneous atrophy |
| Hyaluronic acid | Synvisc, Euflexxa | Viscosupplement | Knee OA | Weak evidence, not AAOS-recommended |
| Enoxaparin | Lovenox | LMWH | VTE prophylaxis post-op | Renal dose adjust |
| Rivaroxaban | Xarelto | DOAC (Xa inhibitor) | VTE prophylaxis post TKA/THA | 10 mg daily |
| Apixaban | Eliquis | DOAC | VTE prophylaxis post TKA/THA | 2.5 mg BID |
| Aspirin | ASA | Antiplatelet | VTE prophylaxis post-TJA | Acceptable for low-risk patients |
| Cefazolin | Ancef | Cephalosporin | Perioperative prophylaxis | Within 60 min of incision |
| Vancomycin | Vancocin | Glycopeptide | MRSA coverage, PJI | Trough monitoring |
| Alendronate | Fosamax | Bisphosphonate | Osteoporosis | Atypical femur fracture, ONJ risk |
| Zoledronic acid | Reclast | IV bisphosphonate | Osteoporosis | Annual infusion |
| Denosumab | Prolia | RANKL inhibitor | Osteoporosis | Rebound vertebral fractures if stopped |
| Teriparatide | Forteo | PTH analog (anabolic) | Severe osteoporosis | Daily SQ injection, 2-year max |
| Vitamin D3 | — | Supplement | Bone health | Target 25-OH > 30 ng/mL |
| Calcium carbonate/citrate | — | Supplement | Bone health | 1,000–1,200 mg/day |
The surgeon will often say "start the patient on their VTE prophylaxis protocol." Know which drug the practice uses by default, the dose, and the duration (usually 10–14 days after TKA, up to 35 days after THA). Chart it verbatim in the plan.
20 Classification Systems
Orthopedics is obsessed with classification systems because they dictate treatment. Memorize these — they will appear in nearly every surgeon's dictation. The most important systems are enumerated within their respective condition sections above; this section is a consolidated quick-reference.
- Garden (femoral neck I–IV): see Section 11.
- Pauwels (femoral neck shear angle): I <30°, II 30–50°, III >50°.
- Salter-Harris (physeal I–V): see Section 15.
- Gustilo-Anderson (open I, II, IIIA/B/C): see Section 15.
- Mason (radial head I–IV): see Section 7.
- Weber (ankle A/B/C): see Section 13.
- Lauge-Hansen (ankle): SA, SER, PA, PER.
- Schatzker (tibial plateau I–VI): see Section 13.
- Frykman (distal radius I–VIII): see Section 8.
- Neer (proximal humerus): 1-, 2-, 3-, 4-part based on displaced segments.
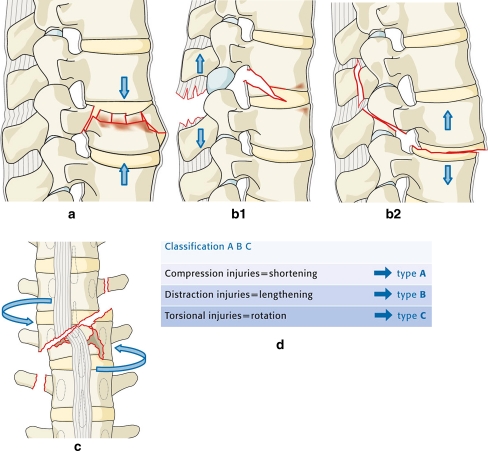
- Tile (pelvic ring): A (stable), B (rotationally unstable), C (rotationally + vertically unstable).
- Young-Burgess (pelvic ring by mechanism): APC I–III, LC I–III, VS, CMI.
- Sanders (calcaneus intra-articular): I–IV by coronal CT fragments.
- OTA/AO: alphanumeric universal fracture coding (bone-segment-type).
- Kellgren-Lawrence (knee OA 0–4): see Section 3.
- Tonnis (hip OA 0–3): see Section 3.
- Outerbridge (cartilage 0–IV): see Section 3.
- Goutallier (cuff fatty infiltration 0–4): see Section 4.
- Snyder (SLAP tears I–IV): see Section 5.
- Rockwood (AC separation I–VI): see Section 4.
21 Physical Exam — The Ortho Exam
The orthopedic exam is joint-specific. You will memorize the sequence for each joint and chart it almost verbatim. Below are the must-know special tests by joint.
Shoulder: Neer, Hawkins-Kennedy (impingement); Jobe/empty can (supraspinatus); lift-off, belly press, bear hug (subscapularis); external rotation lag, hornblower (infraspinatus/teres minor); O'Brien (SLAP/AC); Speed, Yergason (biceps); apprehension, relocation (anterior instability); sulcus sign (inferior laxity); cross-body adduction (AC).
Elbow: Mill's, Cozen's (lateral epicondylitis); hook test (distal biceps); moving valgus stress, milking (UCL); Tinel at cubital tunnel (ulnar nerve).
Wrist/Hand: Tinel, Phalen, carpal compression (median nerve); Finkelstein (de Quervain); scaphoid shift (Watson); TFCC load; Froment (ulnar nerve); Allen test (vascular).
Hip: FABER (SI joint/hip), FADIR (impingement), Thomas (flexion contracture), Trendelenburg (abductor weakness), log roll (intra-articular pathology), Stinchfield (resisted SLR), Ober (IT band).
Knee: Lachman, anterior drawer, pivot shift (ACL); posterior drawer, posterior sag (PCL); valgus stress (MCL); varus stress (LCL); McMurray, Thessaly, joint line tenderness (meniscus); patellar apprehension, grind, glide (patellofemoral).
Ankle/Foot: anterior drawer, talar tilt (ATFL/CFL); squeeze test, external rotation stress (syndesmosis); Thompson (Achilles); Mulder click (Morton neuroma); Silfverskiöld (gastroc vs. soleus contracture).
Spine: straight leg raise, crossed SLR, slump (lumbar radiculopathy); Spurling, Lhermitte (cervical); Hoffmann, clonus, Babinski (myelopathy); saddle sensation, rectal tone (cauda equina).
Right knee: no effusion, well-healed arthroscopy portals.
ROM: 0–130° active, symmetric.
TTP medial joint line, no lateral.
Lachman 1A, neg pivot shift, neg ant/post drawer.
Stable to varus/valgus at 0 and 30°.
McMurray positive medially. Neg Thessaly.
5/5 quad/HS. Pulses 2+ DP/PT. Sensation intact.
22 Abbreviations Master List
Anatomy & Joints
Diagnoses & Findings
Procedures
Workflow & Weight-Bearing
23 Sample HPI Templates
These templates show the rhythm and content of a real orthopedic HPI. Pattern-match off them during your first week.
"Mr. [Name] is a 67-year-old right-hand-dominant male with BMI 31, HTN, and type 2 DM (A1C 6.9) presenting for evaluation of chronic right knee pain. Symptoms have progressed insidiously over 5 years, now rated 8/10 at worst, medial-sided, worse with stairs and prolonged walking, with morning stiffness lasting 15 minutes. He has failed 6 months of formal PT, scheduled NSAIDs (meloxicam 15 mg daily), three intra-articular corticosteroid injections (last 4 months ago with 3 weeks relief), and activity modification. He cannot walk more than 2 blocks without stopping, cannot golf, and has disturbed sleep from night pain. He denies instability, locking, or constitutional symptoms. Weight-bearing radiographs from 2 weeks ago demonstrate Kellgren-Lawrence grade 4 tricompartmental OA with bone-on-bone medial joint space loss, subchondral sclerosis, osteophytes, and varus alignment. He understands the risks and benefits and wishes to proceed with right TKA."
"Ms. [Name] is a 72-year-old right-hand-dominant female with osteoporosis (on alendronate) who presents after a mechanical fall from standing onto an outstretched left hand earlier today. She landed on the kitchen floor and immediately noted wrist deformity and pain. She denies LOC, head strike, chest pain, hip/knee pain, or other injury. She is neurovascularly intact with 2+ radial pulse, normal median/ulnar/radial nerve sensation and motor, and normal capillary refill. Radiographs demonstrate a dorsally angulated, extra-articular, comminuted distal radius fracture with 25° dorsal tilt, 4 mm radial shortening, and associated ulnar styloid fracture — consistent with Frykman II. Closed reduction was performed under hematoma block with improvement in alignment, and she was placed in a well-padded sugar-tong splint. She will return in 7 days for repeat imaging and consideration of ORIF with volar locking plate given her activity level."
"Mr. [Name] is a 24-year-old right-hand-dominant male, recreational soccer player, who sustained a non-contact twisting injury to his right knee 10 days ago. He was planting and cutting when he felt an audible pop, immediate pain, and was unable to continue playing. The knee swelled within 2 hours. He reports instability and giving way with lateral movement. Denies mechanical locking. Initial ED evaluation showed hemarthrosis; radiographs negative for fracture. MRI obtained 3 days ago demonstrates a complete ACL mid-substance tear, grade I MCL sprain, and a small medial meniscus posterior horn tear in the red-red zone. On exam today: moderate effusion, ROM 5–115°, Lachman 2B with soft endpoint, positive pivot shift, 1+ laxity to valgus stress at 30°, joint line tenderness medially. He wishes to proceed with ACL reconstruction with BTB autograft and medial meniscus repair once the swelling subsides and ROM is restored."
"Mrs. [Name] is an 84-year-old female with a history of osteoporosis (T-score −3.2), HTN, and A-fib on apixaban, brought to the ED after a ground-level fall in her living room approximately 6 hours ago. She reports severe left groin pain and is unable to bear weight. The left lower extremity is shortened and externally rotated. Neurovascular exam intact with palpable DP and PT pulses and normal sensation. AP pelvis and cross-table lateral demonstrate a displaced left femoral neck fracture, Garden IV. Labs: Hgb 11.2, platelets normal, INR 1.1, Cr 1.0. Cardiology has been consulted for perioperative risk; geriatrics co-management initiated. Plan is for left hip hemiarthroplasty (given age, cognitive status, and pre-fracture household ambulator status) within 24 hours of admission per AAOS hip fracture CPG. Apixaban held, VTE prophylaxis plan per standard protocol, DEXA to follow outpatient."
"Mr. [Name] is a 58-year-old right-hand-dominant male electrician presenting with 4 months of progressive right shoulder pain and weakness. He denies a specific inciting injury but notes worsening after a day of overhead wiring. Pain is lateral deltoid, 6/10, worse at night (cannot sleep on the right side), worse with overhead activity. He has failed 8 weeks of PT and one subacromial corticosteroid injection (2 weeks of partial relief). On exam: intact deltoid; forward flexion 140° active / 160° passive, abduction 130° / 150°, ER 40°, IR to L3. 4/5 supraspinatus strength with positive Jobe, positive drop arm, negative lift-off and belly press, positive Hawkins and Neer. MRI demonstrates a full-thickness tear of the supraspinatus measuring 2.5 cm in the AP dimension with 1 cm of medial retraction, Goutallier grade 1 fatty infiltration, and minor infraspinatus articular-sided fraying. He wishes to proceed with arthroscopic rotator cuff repair."
"Mr. [Name] is a 22-year-old right-hand-dominant male college rugby player who presents to the ED with right shoulder pain and deformity after a tackle approximately 1 hour ago. His arm was forced into abduction and external rotation. He reports immediate pain and inability to move the arm. On arrival: arm held in slight abduction and external rotation, prominent acromion with anterior fullness, squared-off appearance, intact axillary nerve sensation over the lateral deltoid, intact distal pulses and motor. Pre-reduction radiographs confirm anterior glenohumeral dislocation without fracture. Closed reduction performed under conscious sedation with scapular manipulation technique; immediate relief. Post-reduction neurovascular exam intact. Post-reduction films show concentric reduction with a small Hill-Sachs lesion. He will be placed in a sling for 2 weeks, followed by PT and outpatient MR arthrogram to evaluate for Bankart lesion given his age and activity level; he may require arthroscopic Bankart repair given the high recurrence risk in young athletes."
24 References & Sources
Clinical Practice Guidelines
AAOS. Management of Rotator Cuff Injuries Clinical Practice Guideline. J Am Acad Orthop Surg. 2020.
OTA. Open Fracture Management Clinical Guidelines. J Orthop Trauma. 2022.
USPSTF. Screening for Osteoporosis to Prevent Fractures: Recommendation Statement. JAMA. 2018.
NICE Osteoarthritis in Over 16s: Diagnosis and Management (NG226). 2022.
Diagram & Figure Sources
Figure 1: Major Joints of the Body. OpenStax College. CC BY 3.0.
Figure 2: Types of Synovial Joints. OpenStax College. CC BY 3.0.
Figure 3: Major Skeletal Muscles. OpenStax College. CC BY 3.0.
Figure 4: Rotator Cuff Muscles. Blausen Medical 2014. CC BY 3.0.
Figure 5: Knee Joint Anatomy. OpenStax College. CC BY 3.0.
Figure 6: Distal Radius Fracture Radiograph. Wikimedia Commons. Public domain.
Figure 7: Total Hip Replacement. National Cancer Institute. Public domain.
The best ortho scribes speak the surgeon's anatomic language. When the attending dictates "Garden IV femoral neck fracture, displaced, Pauwels III, will proceed with hemiarthroplasty via posterior approach," a great scribe immediately understands: this is an intracapsular hip fracture with a steep shear angle, high AVN risk, and the surgeon is choosing a ball-on-stem replacement through the most common but higher-dislocation-risk approach. The plan writes itself.
Be anatomic. Be precise. Always chart laterality, weight-bearing status, and neurovascular exam. Pre-read the imaging before the patient is roomed. Learn your attending's preferred classification system and treatment algorithms. Know the difference between Kellgren-Lawrence and Tonnis, between Weber and Lauge-Hansen, between Garden and Pauwels. When in doubt, ask — but the best scribes ask fewer questions over time because this guide becomes second nature.
Welcome to orthopedics. It is the most mechanically satisfying specialty in medicine — broken things, fixed.