Pediatrics
Every diagnosis, condition, procedure, medication, abbreviation, and documentation framework you need to succeed on day one in a pediatric clinic, urgent care, or inpatient service.
All diagrams on this page are sourced from published educational or institutional materials rather than AI generation. Each figure caption links to the original source, and the full diagram and guideline citations are collected in the references section at the bottom.
01 Pediatric Principles — Age Groups, Growth & Development
Pediatrics is the care of humans from birth through age 18 (and in many practices, into the early 20s). The foundational principle that separates pediatrics from adult medicine is that children are not small adults. Normal vital signs, drug dosing, disease presentations, differential diagnoses, and even the goals of the visit change dramatically depending on the child's age. A scribe in pediatrics must mentally classify every patient into an age group before interpreting any complaint, because the differential for fever in a 3-week-old is entirely different from fever in a 3-year-old.
Age Group Classification
| Term | Age Range | Key Clinical Points |
|---|---|---|
| Neonate | 0 – 28 days | Fever is a medical emergency; immature immune system; bilirubin, feeding, weight gain dominant concerns |
| Young infant | 29 – 90 days | Still high risk for occult serious bacterial infection (SBI); limited physical exam clues |
| Infant | 3 – 12 months | Rapid developmental changes; bronchiolitis peak; solid food introduction |
| Toddler | 1 – 3 years | Otitis media peak; URIs constant; accidental ingestions; autonomy struggles |
| Preschooler | 3 – 5 years | Language explosion; readiness screening; frequent viral illness |
| School-age | 6 – 11 years | Sports injuries; strep pharyngitis; ADHD recognition; asthma management |
| Adolescent | 12 – 18 years | Puberty; confidentiality; mental health; HEEADSSS; risk behaviors |
Growth — The Pediatric Obsession
Every pediatric visit revolves around growth. Weight, length (< 2 years, measured lying down) or height (≥ 2 years, standing), head circumference (until age 2–3), and body mass index (BMI, from age 2) are plotted on standardized growth charts. The WHO growth standards are used 0–2 years and CDC growth charts from age 2 through 20. Normal tracking stays within two major percentile lines; crossing percentiles downward triggers a workup for failure to thrive (FTT). Key rules of thumb: birth weight doubles by 4–6 months, triples by 12 months, and quadruples by 24 months. Average infants gain roughly 20–30 g/day in the first 3 months. Head circumference grows about 2 cm/month for the first 3 months, then slows.
Development — Milestones by Domain
Development is tracked in four domains: gross motor, fine motor, language, and social/cognitive. The scribe is expected to know the landmark milestones for each well-child visit because the clinician will verbally confirm them during the encounter ("rolls over? sits? pulls to stand? walks? runs? first words?") and expects them captured in the note.
| Age | Gross Motor | Fine Motor | Language | Social |
|---|---|---|---|---|
| 2 mo | Lifts head prone | Opens hands | Coos | Social smile |
| 4 mo | Rolls front to back | Grasps rattle | Laughs | Recognizes parents |
| 6 mo | Sits with support | Transfers objects | Babbles | Stranger anxiety begins |
| 9 mo | Pulls to stand, crawls | Pincer grasp emerging | "Mama/dada" nonspecific | Waves bye-bye |
| 12 mo | First steps | Mature pincer grasp | 1–3 words | Follows 1-step command w/ gesture |
| 15 mo | Walks well | Scribbles | 3–5 words | Points to wants |
| 18 mo | Runs, walks up steps | Tower of 2–4 cubes | 10–25 words | Imitates parent |
| 2 yr | Kicks ball, jumps | Tower of 6 cubes | 2-word phrases, 50+ words, 50% intelligible | Parallel play |
| 3 yr | Tricycle, up stairs alternating | Copies circle | 3-word sentences, 75% intelligible | Knows name/age |
| 4 yr | Hops, balances | Copies cross, draws person | Tells stories, 100% intelligible | Cooperative play |
| 5 yr | Skips | Copies square/triangle | Full sentences, counts to 10 | Has friends, follows rules |
You will hear the clinician say "meeting milestones" or "global delay" — both trigger specific documentation. If the clinician confirms milestones verbally, always chart the specific skills demonstrated (e.g., "walks independently, 5–10 words, points to request"), not just "meets milestones." When they use the ASQ or M-CHAT, record the exact score.
02 Scribe Documentation Framework — Well vs Sick Visits
Pediatric notes split cleanly into two templates: the well-child check (WCC) and the sick visit. Every pediatric scribe must learn both rhythms because they are structured entirely differently. WCCs are scheduled, preventive, and heavily templated around Bright Futures/AAP recommendations. Sick visits are problem-focused SOAP notes driven by the chief complaint.
Interval history: What has happened since the last visit — illnesses, ER visits, new medications, behavioral changes.
Nutrition: Breastfed vs formula fed (brand, ounces, frequency); solid food introduction; picky eating; juice/milk intake; appetite.
Elimination: Stool frequency/consistency; voiding; toilet training progress.
Sleep: Total hours, naps, sleep location (crib, own bed), night wakings, safe sleep practices for infants (back-to-sleep, no bumpers, no co-sleeping).
Development: Domain-specific milestones achieved; ASQ-3 or M-CHAT-R/F results if performed.
Safety: Car seat, home safety, firearm storage, sunscreen, helmet, water safety, screen time.
Social: Family structure, daycare/school, stressors.
Exam, growth parameters, immunizations given, anticipatory guidance, and plan complete the note.
CC: Usually in parent's words: "fever," "cough," "pulling at ear," "vomiting," "rash."
HPI (OLDCARTS adapted): Onset, duration, quality, associated symptoms (fever max temp, cough quality, appetite, oral intake, urine output, stool pattern, sleep, behavior change), sick contacts, daycare exposures, recent travel, immunization status, prior similar episodes.
ROS: Focused. Always ask about fever, feeding/PO intake, urine output, activity level, breathing difficulty, rash, vomiting/diarrhea.
PMHx, birth history (gestational age, mode of delivery, NICU stay, complications), meds, allergies, FHx, immunizations up to date: These carry more weight than in adult medicine, especially for children under 2.
The three questions that drive nearly every pediatric sick-visit decision: Is the child well-hydrated? Is the child working to breathe? Is the child toxic-appearing? Document each one explicitly. "Well-appearing, well-hydrated, no respiratory distress" is the most important line in many pediatric notes.
03 Well-Child Care & Anticipatory Guidance Preventive
The AAP Bright Futures guidelines define the recommended schedule of well-child visits: at 3–5 days, 1, 2, 4, 6, 9, 12, 15, 18, 24, and 30 months, then annually through age 21. Each visit has age-specific anticipatory guidance, screening, immunizations, and developmental surveillance.
Screening Schedule Highlights
| Screen | Ages | Tool |
|---|---|---|
| Newborn hearing | Birth | OAE / ABR |
| Newborn metabolic (NBS) | 24–48 h | Heel-stick panel (PKU, CH, CAH, SCD, CF, etc.) |
| Critical congenital heart disease | 24 h | Pre/post-ductal pulse oximetry |
| Developmental surveillance | Every WCC | Milestone review |
| Formal developmental screen | 9, 18, 30 mo | ASQ-3 or PEDS |
| Autism screen | 18 and 24 mo | M-CHAT-R/F |
| Anemia / lead | 12 and 24 mo | Hgb, capillary lead (risk-based) |
| Lipid screen | 9–11 yr, 17–21 yr | Non-fasting lipid panel |
| Depression & suicide risk | ≥ 12 yr annually | PHQ-9 modified for teens, ASQ |
| Vision / hearing | 3, 4, 5, 6, 8, 10, 12, 15, 18 yr | Snellen / audiometry |
| STI screening | Sexually active teens | GC/CT NAAT, HIV, syphilis |
USPSTF pediatric preventive recommendations overlap with but are sometimes narrower than Bright Futures — the AAP schedule is the default for outpatient pediatrics.
Newborn/2 mo: Back to sleep, rear-facing car seat, breastfeeding support, vitamin D 400 IU, fever action plan, shaken baby prevention.
6–9 mo: Childproofing, introduction of solids and allergens (peanut per LEAP), choking hazards, no honey < 12 mo, fluoride varnish.
12–18 mo: Whole milk transition, tantrum management, language stimulation, no screen time < 18 mo, pool/water safety.
2–5 yr: Toilet training, preschool readiness, limiting screen time to 1 hr/day, healthy eating, dental home.
School age: Helmet, seat belts, sports safety, bullying, stranger awareness, sleep hygiene.
Adolescent: HEEADSSS interview (see §15), driving safety, contraception, substance use, mental health, confidentiality.
04 Neonatal Problems — Jaundice, GERD, Colic, FTT Neonatal
Neonatal Jaundice
Jaundice — yellow discoloration of skin and sclerae from elevated unconjugated bilirubin — is extraordinarily common: up to 60% of term and 80% of preterm newborns. Most is physiologic, from the combination of high bilirubin load (RBC turnover), immature hepatic conjugation, and enterohepatic recirculation. Pathologic jaundice — appearing in the first 24 hours, rising more than 5 mg/dL per day, or involving conjugated hyperbilirubinemia — demands a workup (hemolysis, sepsis, biliary atresia). Management is guided by the 2022 AAP hyperbilirubinemia guideline, which plots total serum bilirubin against age in hours on nomograms to decide on phototherapy vs exchange transfusion. Kernicterus — bilirubin deposition in the basal ganglia — is the feared, preventable complication.
Infantile GERD vs GER
Gastroesophageal reflux (GER) is normal "spitting up" in happy infants who gain weight — the "happy spitter." Gastroesophageal reflux disease (GERD) involves poor weight gain, feeding refusal, back arching (Sandifer), recurrent pneumonia, or apnea. First-line management is reassurance, upright positioning after feeds, smaller more frequent feeds, and — if formula fed — a trial of extensively hydrolyzed formula for 2 weeks. Acid suppression (H2 blockers, PPIs) is reserved for true GERD and used sparingly due to risks of gastroenteritis, pneumonia, and fracture.
Colic
Defined by the Wessel "rule of 3s": crying > 3 hours/day, > 3 days/week, for > 3 weeks in an otherwise healthy infant. Peaks at 6 weeks, resolves by 3–4 months. Workup is to exclude serious causes (hair tourniquet, corneal abrasion, UTI, incarcerated hernia, intussusception, NAT). Management is parental support and reassurance; no medication is definitively helpful.
Failure to Thrive (FTT)
Weight < 2nd percentile for age, weight-for-length < 2nd percentile, or crossing two major percentile lines downward. The vast majority of cases are non-organic (inadequate caloric intake). Workup combines a detailed 24-hour diet recall, feeding observation, CBC, CMP, UA, TSH, and celiac screen if on gluten. Referral to a nutritionist and close weight checks are the first step; admission is needed if dehydration or a failure of outpatient management.
05 Fever in the Neonate & Infant Emergency
Fever is defined as rectal temperature ≥ 38.0°C (100.4°F). In a neonate (≤ 28 days), fever is a medical emergency. The 2021 AAP Clinical Practice Guideline on evaluating the well-appearing febrile infant 8–60 days old is the single most important guideline in general pediatrics.
Full sepsis workup, always: CBC with differential, blood culture, urinalysis + urine culture (catheterized), lumbar puncture (CSF cell count, protein, glucose, culture, HSV PCR if indicated), often chest X-ray, procalcitonin, CRP. Empiric antibiotics (ampicillin + gentamicin or cefotaxime) and admission. Add acyclovir if HSV features.
Low-risk criteria (all must be met): well-appearing, no focal infection, procalcitonin < 0.5 ng/mL, ANC < 4,000–5,200, CRP < 20 mg/L, normal urinalysis. If inflammatory markers are unavailable, risk stratification falls back to the Rochester / Philadelphia / Boston criteria. Management ranges from observation with follow-up (low risk, good access) to full workup + empiric ceftriaxone.
Fever > 3 Months (Older Child)
The workup shifts from "rule out bacteremia" to "identify the source." Focused history (URI symptoms, cough, ear pain, diarrhea, rash, dysuria, limp) and exam usually localize the infection. Common sources: viral URI, otitis media, pharyngitis, pneumonia, UTI, viral gastroenteritis. Unexplained fever > 39°C in an unimmunized child, or prolonged fever > 5 days, triggers broader workup. Always consider Kawasaki disease in a child with fever ≥ 5 days.
Fever of Unknown Origin & Red Flags
Red flags: toxic appearance, petechiae/purpura (meningococcemia), nuchal rigidity, altered mental status, prolonged capillary refill, cool extremities, persistent tachycardia after fever reduction, respiratory distress, focal neurological findings.
06 Upper Respiratory Infections (URI, OM, Strep, Croup) Infectious
Viral URI ("Common Cold")
Rhinovirus, coronavirus, RSV, adenovirus, parainfluenza. Children average 6–8 URIs per year (more in daycare). Symptoms: rhinorrhea, nasal congestion, cough, low-grade fever, sore throat — resolving in 7–10 days. Management is supportive (saline drops, bulb suction, hydration, acetaminophen/ibuprofen). Antibiotics are not indicated. OTC cough/cold medicines are contraindicated under 4 years and discouraged under 6.
Acute Otitis Media (AOM)
The single most common bacterial infection in children. Pathogens: Streptococcus pneumoniae, non-typeable Haemophilus influenzae, Moraxella catarrhalis. The AAP 2013 AOM guideline requires three features for diagnosis: moderate-to-severe bulging of the tympanic membrane, new onset otorrhea not from otitis externa, or mild bulging with ear pain or intense erythema.
Under 6 months: Always treat with antibiotics.
6–24 months: Treat unilateral/bilateral AOM with antibiotics; or observation if unilateral non-severe with reliable follow-up.
≥ 2 years: Observation is reasonable for non-severe unilateral AOM with close follow-up.
First-line: Amoxicillin 80–90 mg/kg/day divided BID × 10 days (< 2 yr) or 5–7 days (older). Second-line / prior beta-lactamase exposure: Amoxicillin-clavulanate. Penicillin allergy: Cefdinir, cefuroxime, or azithromycin.
Streptococcal Pharyngitis ("Strep Throat")
Group A Streptococcus (GAS). Peak age 5–15. Classic: fever, sore throat, tonsillar exudate, tender anterior cervical adenopathy, absence of cough/rhinorrhea. Scarlet fever — GAS pharyngitis plus a sandpapery rash, strawberry tongue, and Pastia's lines — is from erythrogenic toxin. Diagnosis: rapid antigen detection test (RADT); if negative in a child, confirm with throat culture. Centor/McIsaac criteria guide testing. Treatment: amoxicillin or penicillin VK × 10 days to prevent rheumatic fever. Do not treat without a positive test (except clinical scarlet fever).
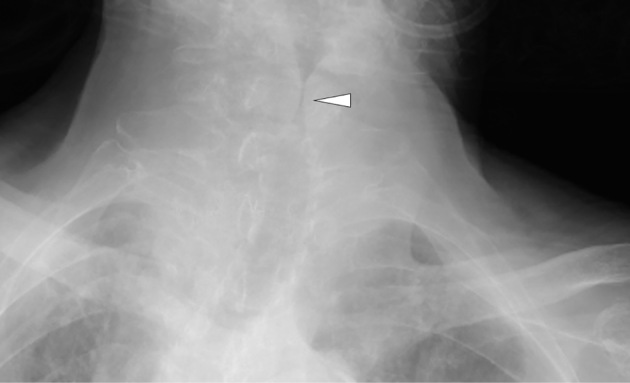
Croup (Laryngotracheobronchitis)
Parainfluenza virus (usually type 1 or 3); age 6 months to 3 years. Classic triad: barky "seal-like" cough, inspiratory stridor, hoarseness, often with a 1–2 day URI prodrome. Worse at night. Steeple sign on AP neck X-ray (rarely needed). Management graded by the Westley croup score (see §21). Mild: dexamethasone 0.6 mg/kg PO single dose. Moderate/severe: dex + nebulized racemic epinephrine and observe 3–4 hours for rebound.
07 Lower Respiratory Disease (Bronchiolitis, Pneumonia, Asthma) Respiratory
Bronchiolitis
Viral (RSV most common; also rhino, metapneumo, parainfluenza, COVID) infection of the small airways in children < 2 years, peaking at 2–6 months. Presents with URI prodrome followed by cough, tachypnea, wheeze, and retractions. The AAP bronchiolitis guideline is decidedly minimalist: diagnosis is clinical; routine CXR, RSV testing, bronchodilators, steroids, and antibiotics are not recommended. Management is supportive: nasal suctioning, hydration, supplemental O2 for SpO2 < 90%, and high-flow nasal cannula / CPAP for severe cases. Nirsevimab (long-acting RSV monoclonal) is now recommended for all infants < 8 months entering their first RSV season.
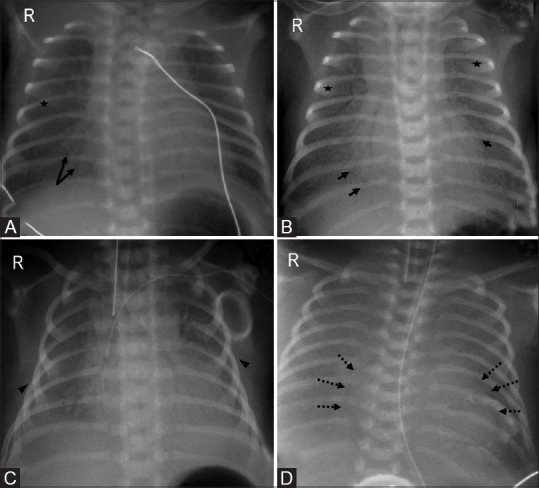
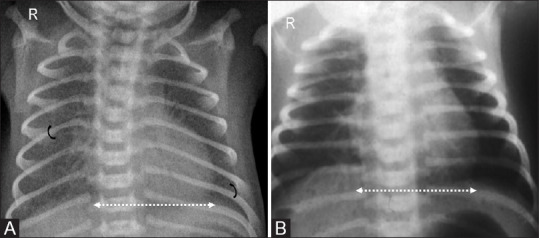
Pneumonia
Etiology shifts by age: neonates (GBS, E. coli), 1–3 months (C. trachomatis, viral), 4 months–4 years (viral dominant, then pneumococcus), school age (Mycoplasma, pneumococcus). Presentation: fever, cough, tachypnea, focal crackles, hypoxia. Tachypnea is the most sensitive sign (> 60 < 2 mo, > 50 2–12 mo, > 40 1–5 yr, > 20 > 5 yr). CXR is not routine for outpatient uncomplicated CAP. First-line outpatient: high-dose amoxicillin (90 mg/kg/day). Atypical coverage (azithromycin) for school age and adolescents. Admission for hypoxia, dehydration, respiratory distress, or infants.
Asthma
Chronic airway inflammation with bronchial hyperreactivity. Diagnosed clinically in children too young for spirometry; classic triad is episodic cough, wheeze, and dyspnea triggered by viral URIs, exercise, allergens, cold air, or smoke. The 2020 NAEPP Focused Updates are the standard. Severity is classified as intermittent, mild persistent, moderate persistent, or severe persistent based on symptom frequency, nighttime awakenings, SABA use, activity limitation, and lung function.
| Step | Preferred |
|---|---|
| 1 (intermittent) | PRN SABA (albuterol) |
| 2 (mild persistent) | Low-dose ICS daily, or ICS+SABA PRN (SMART) |
| 3 (moderate persistent) | Low-dose ICS + LABA, or medium-dose ICS |
| 4 | Medium-dose ICS + LABA |
| 5 | High-dose ICS + LABA ± biologic |
| 6 | High-dose ICS + LABA + oral steroid |
Acute exacerbation management uses the PRAM score (see §21) to grade severity. Treat with albuterol (0.15 mg/kg nebulized or MDI with spacer 4–8 puffs) every 20 minutes × 3, ipratropium for moderate/severe, systemic steroids (dexamethasone 0.6 mg/kg PO × 1–2 doses or prednisolone 1–2 mg/kg/day × 5), oxygen for SpO2 < 92%, magnesium sulfate IV for severe refractory cases, and admission for persistent hypoxia or inability to space albuterol.
08 GI Disorders (Gastroenteritis, Constipation, Dehydration) GI
Acute Gastroenteritis (AGE)
Usually viral (norovirus, rotavirus — now rare post-vaccine, enteric adenovirus, astrovirus). Bacterial causes include Salmonella, Shigella, Campylobacter, E. coli (including Shiga-toxin producing — avoid antibiotics due to HUS risk), C. difficile. Presentation: vomiting, diarrhea, fever, abdominal pain. The scribe's job is to document the hydration status with precision because it drives management.
| Finding | Mild (3–5%) | Moderate (6–9%) | Severe (≥ 10%) |
|---|---|---|---|
| Mental status | Alert | Irritable | Lethargic |
| Capillary refill | < 2 s | 2–3 s | > 3 s |
| Mucous membranes | Slightly dry | Dry | Parched |
| Tears | Present | Decreased | Absent |
| Fontanelle | Normal | Slightly sunken | Sunken |
| Skin turgor | Normal | Slow recoil | Tenting |
| Heart rate | Normal | Mild tachy | Tachy, weak pulses |
| Urine output | Decreased | Markedly dec. | Anuric |
Oral rehydration solution (ORS, e.g., Pedialyte) is first-line for mild-to-moderate dehydration: 50–100 mL/kg over 2–4 hours, given in small frequent sips (5 mL every 1–2 minutes). A single dose of ondansetron (0.15 mg/kg, max 8 mg, ODT) dramatically improves success of oral rehydration in vomiting children. IV fluids (20 mL/kg NS bolus, repeat as needed) are reserved for severe dehydration, failed ORS, or altered mental status.
Functional Constipation
Rome IV criteria: ≤ 2 defecations/week, ≥ 1 episode of incontinence/week, history of stool retention, painful/hard stools, large fecal mass in rectum, or large-diameter stools. Extraordinarily common — often triggered by toilet training, dietary change, or school transitions. First step: disimpaction (PEG 3350 1–1.5 g/kg/day × 3 days). Maintenance: PEG 3350 0.4–0.8 g/kg/day titrated to 1–2 soft stools/day for months, plus behavioral measures (scheduled toilet sits after meals, fiber, fluids).
Other GI Entities
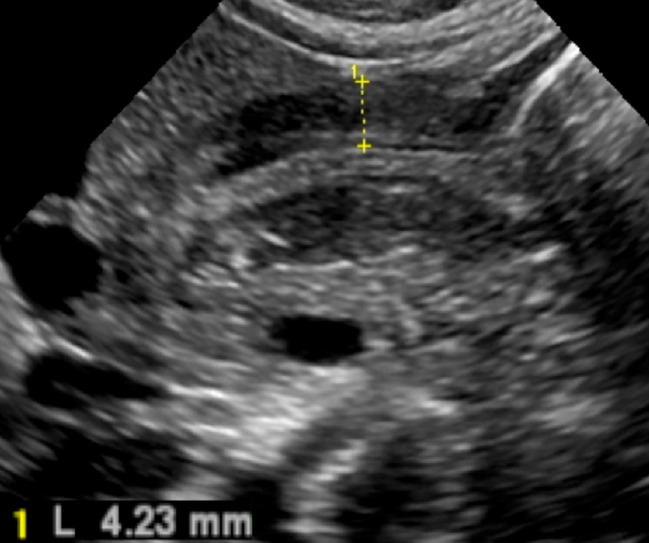
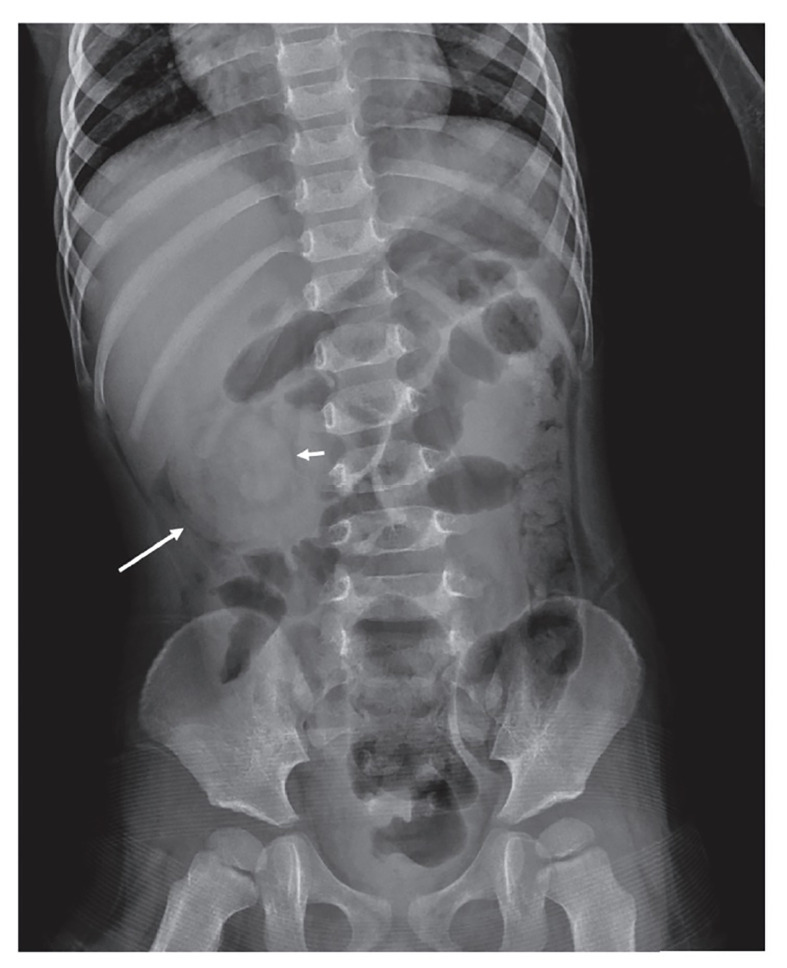
Pyloric stenosis — first-born males, 3–6 weeks, projectile non-bilious vomiting, "olive" on exam, hypochloremic hypokalemic metabolic alkalosis, "target sign" on ultrasound, pyloromyotomy. Intussusception — 3 mo to 3 yr, colicky pain, currant-jelly stool, sausage-shaped mass, "target sign" on ultrasound, air or contrast enema reduction. Appendicitis — atypical in young children, high perforation rate; Alvarado or PAS score guides workup. Encopresis — fecal soiling after age 4, usually from chronic constipation with overflow.
09 Urinary Tract Infection & Renal Issues GU
UTI is a frequent occult source of fever in young children. Under 2 years, symptoms are nonspecific (fever, fussiness, poor feeding). School-age children present with classic dysuria, frequency, urgency, and suprapubic pain. E. coli accounts for 80–90% of cases.
The AAP UTI guideline (2011, reaffirmed) governs the workup of the febrile infant 2–24 months. Diagnosis requires both a positive UA (pyuria and/or bacteriuria) and a urine culture with ≥ 50,000 CFU/mL from a catheterized specimen. Bag specimens can rule out UTI but cannot rule one in. First-line treatment: cephalexin, cefdinir, or TMP-SMX for 7–14 days. Renal/bladder ultrasound is indicated after first febrile UTI in infants. VCUG is obtained if US is abnormal or after a second febrile UTI to evaluate for vesicoureteral reflux (VUR).
Other Common Renal/GU Issues
Enuresis (bedwetting) — primary nocturnal enuresis is common through age 6; reassurance, scheduled voids, limit evening fluids, bedwetting alarm, desmopressin for short-term use. Vulvovaginitis — prepubertal girls, non-specific irritation, hygiene advice. Balanitis, phimosis vs paraphimosis. Cryptorchidism — refer by 6 months if not descended. Testicular torsion — surgical emergency, sudden severe pain, high-riding testis, absent cremasteric reflex.
10 Classic Pediatric Exanthems & Viral Illnesses Infectious
The "childhood exanthems" are a core recognition task. Many are now rare because of immunization (measles, rubella, varicella), but scribes must recognize them all.


| Name (Number) | Agent | Clinical |
|---|---|---|
| Measles (1st) | Measles virus | Fever, cough, coryza, conjunctivitis, Koplik spots; cephalocaudal maculopapular rash |
| Scarlet fever (2nd) | GAS toxin | Sandpaper rash, strawberry tongue, Pastia lines, pharyngitis |
| Rubella (3rd) | Rubella virus | Mild fever, posterior auricular LAD, pink macules face → body |
| Dukes disease (4th) | Uncertain | Historical, not distinct today |
| Erythema infectiosum (5th) | Parvovirus B19 | Slapped cheek rash, reticular rash trunk/limbs, arthralgia in adults; aplastic crisis in SCD |
| Roseola (6th) | HHV-6/HHV-7 | 3–5 days high fever, then rash appears as fever breaks; infants 6 mo–2 yr |
| Varicella | VZV | Pruritic vesicles in crops, "dewdrop on rose petal," different stages simultaneously |
| Hand-foot-mouth | Coxsackie A16/EV71 | Oral ulcers + vesicles on palms/soles/buttocks |
| Kawasaki disease | Unknown (vasculitis) | See below — not infectious |
Kawasaki Disease
A medium-vessel vasculitis of unknown etiology, and the most common cause of acquired heart disease (coronary artery aneurysms) in children in developed countries. Think Kawasaki in any child with fever ≥ 5 days. Classic diagnosis: fever ≥ 5 days plus 4 of 5: Conjunctivitis (bilateral, non-exudative, limbal sparing), Rash (polymorphous), Extremity changes (edema, erythema, later desquamation), Adenopathy (cervical, > 1.5 cm, often unilateral), Mucous membrane changes (strawberry tongue, cracked red lips) — mnemonic CREAM. Treatment: IVIG 2 g/kg + high-dose aspirin; echo at diagnosis, 2 weeks, and 6–8 weeks.
11 Dermatologic Conditions (Atopic Dermatitis, Impetigo, Lice) Dermatologic
Atopic Dermatitis (Eczema)
Chronic relapsing itchy dermatitis; part of the atopic triad (eczema, allergic rhinitis, asthma). Infants: face and extensor surfaces. Children/adolescents: flexural surfaces (antecubital, popliteal fossae, neck). Management: liberal emollients (thick creams/ointments, multiple times daily), low-potency topical steroids (hydrocortisone 1–2.5%) for face, mid-potency (triamcinolone 0.1%) for body, bleach baths for recurrent infections, topical calcineurin inhibitors (tacrolimus, pimecrolimus) for steroid-sparing, antihistamines for itch. Dupilumab for severe disease.
Diaper Dermatitis
Irritant contact dermatitis from urine/stool (spares creases) vs Candida (beefy red, satellite lesions, involves creases). Treat irritant with zinc oxide barrier and frequent changes; Candida with topical nystatin or clotrimazole.
Impetigo
Superficial bacterial skin infection by GAS or Staph aureus. Non-bullous: honey-crusted lesions on face/extremities. Bullous: flaccid bullae from staph exotoxin. Treatment: topical mupirocin for limited disease; oral cephalexin or clindamycin for extensive or bullous.
Head Lice & Scabies
Pediculosis capitis — itching, nits on hair shafts; permethrin 1% or ivermectin; wet combing. Not a hygiene problem; no school exclusion per AAP. Scabies — intense pruritus worse at night, interdigital burrows, infants with diffuse rash involving palms/soles. Permethrin 5% cream applied neck-down (head-to-toe in infants), repeat in 1 week; treat all household contacts and wash linens.
12 Pediatric Neurology (Febrile Seizure, Headache, Concussion) Neurologic
Febrile Seizure
Seizure associated with fever in a child 6 months–5 years without CNS infection, metabolic disturbance, or prior afebrile seizures. Simple: generalized, < 15 minutes, no recurrence within 24 hours. Complex: focal, > 15 minutes, or recurrent within 24 hours. Simple febrile seizures carry a small increased risk of future febrile seizures but only marginally increased risk of epilepsy. No EEG, imaging, or LP is routinely needed for simple febrile seizure in a well-appearing immunized child > 12 months. Parent reassurance is central.
Headache
Primary: migraine (with or without aura), tension-type. Secondary red flags: thunderclap onset, early morning vomiting, positional worsening, focal neuro findings, new onset, < 3 years old — all warrant neuroimaging. Migraine management: triggers identification, hydration, sleep, acetaminophen/ibuprofen for acute; topiramate, propranolol, amitriptyline for prevention.
Concussion / Sports-Related mTBI
Clinical diagnosis after head impact with altered mental status (does not require LOC). Symptoms: headache, dizziness, nausea, photo/phonophobia, cognitive slowing, emotional lability, sleep disturbance. Management: relative rest for 24–48 hours, then gradual return to learn (RTL) before return to play (RTP). Full symptom resolution and completion of a graduated 6-step RTP protocol required. Second-impact syndrome is the rationale for conservative return.
Seizure Disorders
Generalized (absence, tonic-clonic, myoclonic) vs focal. Absence epilepsy (4–10 yr, staring spells, 3 Hz spike-wave on EEG, treated with ethosuximide). Benign rolandic epilepsy. Infantile spasms (hypsarrhythmia on EEG; ACTH/vigabatrin). First afebrile seizure workup: EEG, MRI brain, electrolytes, glucose.
13 Chronic Disease & Genetic Conditions Chronic
Asthma, Allergies, Anaphylaxis
Already covered in §7. Food allergies — the "Big 9" (milk, egg, peanut, tree nut, wheat, soy, fish, shellfish, sesame). Early peanut introduction (LEAP) is now recommended to reduce peanut allergy. Anaphylaxis — IM epinephrine (0.01 mg/kg, max 0.3 mg, auto-injector 0.15 mg < 25 kg, 0.3 mg ≥ 25 kg), position supine, oxygen, IV fluids, observation 4–6 hours, Epi-Pen prescription, allergy referral.
Type 1 Diabetes
Polyuria, polydipsia, weight loss, fatigue. Can present as DKA (fruity breath, Kussmaul breathing, altered mental status). Management: basal-bolus insulin, carb counting, CGM, A1C < 7.0–7.5% per ADA pediatric target.
Sickle Cell Disease
Autosomal recessive hemoglobinopathy, detected on NBS. Vaso-occlusive crises, acute chest syndrome, splenic sequestration, stroke. Penicillin prophylaxis through age 5, hydroxyurea, transfusion for severe complications, transcranial Doppler screening 2–16 years for stroke risk.
Iron Deficiency Anemia
The most common pediatric anemia. Risk: prolonged exclusive breastfeeding without iron supplementation > 6 months, excessive cow's milk > 24 oz/day in toddlers. Screen at 12 months. Hgb < 11, low MCV, low ferritin, high RDW. Treat with ferrous sulfate 3–6 mg/kg elemental iron daily; recheck in 4 weeks.
Congenital Heart Disease Overview
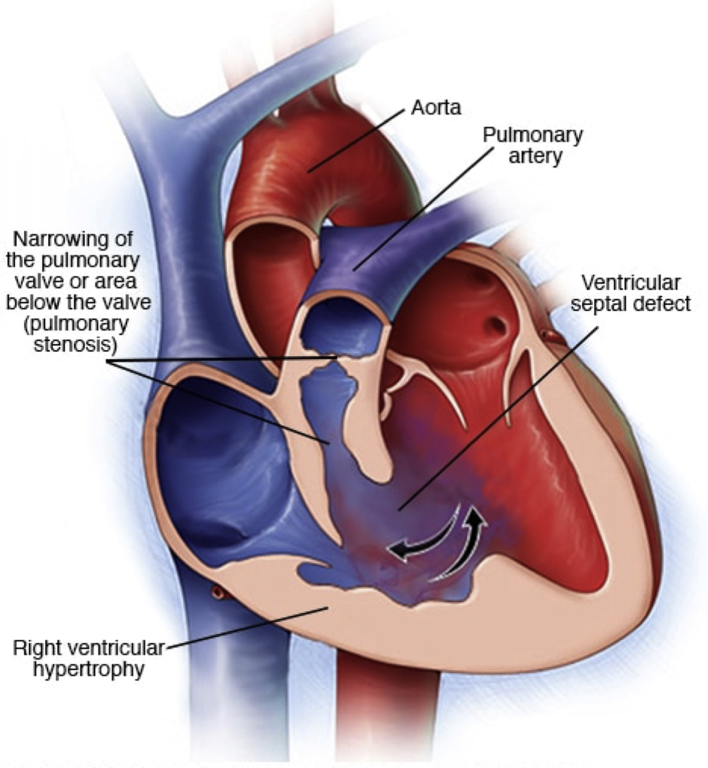
Acyanotic (L→R shunts): VSD, ASD, PDA, coarctation, AS. Cyanotic (R→L or mixing): tetralogy of Fallot, transposition of great arteries, truncus arteriosus, TAPVR, tricuspid atresia, hypoplastic left heart. Innocent murmurs (Still's, venous hum) are common and benign: soft, grade 1–2, musical, position/phase variable. Pathologic murmurs: grade ≥ 3, harsh, diastolic, pansystolic, with clicks or abnormal S2 — warrant echo.
Cystic Fibrosis
Autosomal recessive CFTR mutation. Detected on NBS (IRT). Presentation: recurrent pulmonary infections (Pseudomonas), steatorrhea, failure to thrive, meconium ileus in neonates. Multidisciplinary CF center management, pancreatic enzyme replacement, CFTR modulators (ivacaftor, elexacaftor/tezacaftor/ivacaftor).
Congenital Hypothyroidism
Detected on NBS. Untreated causes cretinism. Treat with levothyroxine within 2 weeks of life to preserve IQ.
14 Behavioral, Developmental & Mental Health Behavioral
ADHD
AAP ADHD guideline: DSM-5 criteria require 6+ inattentive and/or hyperactive-impulsive symptoms for ≥ 6 months, present before age 12, in ≥ 2 settings, causing impairment. Use Vanderbilt or Conners rating scales from parents and teachers. Preschool (4–5 yr): behavior therapy first. School age: behavior therapy plus stimulant (methylphenidate or amphetamine) first-line. Second-line: atomoxetine, guanfacine ER, clonidine ER.
Autism Spectrum Disorder
Persistent deficits in social communication and interaction plus restricted/repetitive behaviors. Screen with M-CHAT-R/F at 18 and 24 months. Early red flags: no eye contact, no social smile by 6 months, no babbling by 12 months, no single words by 16 months, no 2-word phrases by 24 months, regression at any age. Refer to developmental pediatrics and Early Intervention; ABA therapy is mainstay intervention.
Anxiety, Depression, Eating Disorders
Screen for depression annually from age 12 (AAP & USPSTF). PHQ-9 modified for adolescents. SSRIs (fluoxetine, escitalopram) are first-line; monitor black box warning for suicidality in first 4 weeks. Eating disorders: anorexia nervosa (restriction, weight < expected, fear of gain), bulimia nervosa, avoidant/restrictive food intake disorder (ARFID). SCOFF screening. Medical admission criteria include bradycardia, hypotension, electrolyte disturbance, or weight < 75% expected.
Learning Disabilities, Enuresis, Encopresis, Oppositional Behavior
Document school performance and IEP/504 status. Refer for neuropsych testing when academic failure diverges from cognitive ability. Behavioral approaches with positive reinforcement remain first line for oppositional behavior and enuresis.
15 Adolescent Medicine & HEEADSSS Adolescent
Adolescent care requires a major shift in interview style. The parent is asked to step out and the teen is interviewed alone (at minimum for part of the visit), with a clear explanation of confidentiality and its limits (harm to self, harm to others, abuse). The HEEADSSS psychosocial interview is the backbone of the adolescent HPI.
Home — who lives with you, relationships, safety, recent changes.
Education/Employment — grades, attendance, bullying, goals, job.
Eating — meals, body image, exercise, dieting behaviors.
Activities — friends, hobbies, social media, screen time.
Drugs — tobacco/vaping, alcohol, marijuana, other substances, CRAFFT screening.
Sexuality — orientation, activity, partners, protection, STI testing, pregnancy, abuse.
Suicide/Mood — depression, anxiety, self-harm, prior attempts, ASQ/PHQ-9.
Safety — violence, firearms at home, seat belts/helmets, driving/texting.
Tanner (Sexual Maturity Rating) Stages
| Stage | Female Breast | Male Genitalia | Pubic Hair (both) |
|---|---|---|---|
| I | Prepubertal, no glandular tissue | Prepubertal testes < 4 mL | None (vellus) |
| II | Breast bud, areolar enlargement | Testes 4–6 mL, scrotum thins | Sparse, long, slightly pigmented at base of penis/labia |
| III | Breast/areola enlarge together | Penis lengthens, testes 6–12 mL | Darker, coarser, curlier; spreads over pubis |
| IV | Areola/papilla form secondary mound | Penis thickens, testes 12–15 mL, scrotum darkens | Adult type but not to thighs |
| V | Mature adult breast, areola recesses | Adult genitalia, testes > 15 mL | Adult distribution, extending to medial thighs |
16 Child Abuse, Neglect & Safety Safety
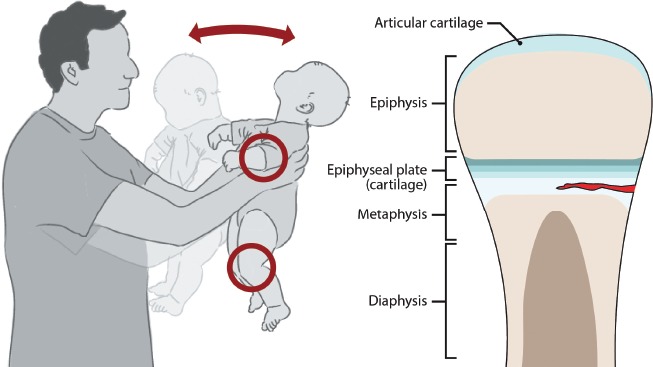
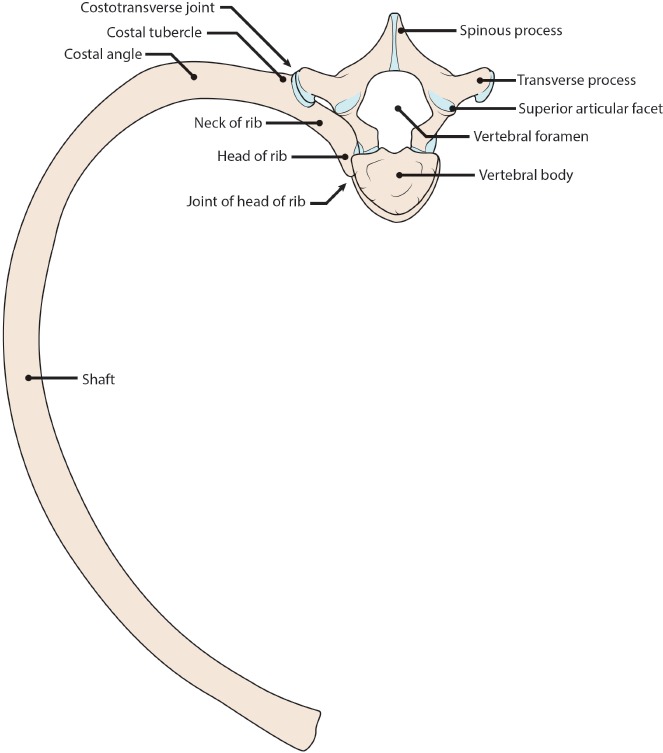
All pediatric clinicians and scribes are mandated reporters. The scribe does not make reports but may hear the clinician say "I'm concerned for non-accidental trauma (NAT)" — and will document the concern, the findings, and the disposition precisely. Red flags for NAT: history inconsistent with injury or changing story, delay in seeking care, injury incompatible with developmental stage (e.g., fracture in a non-ambulatory infant), TEN-4-FACESp bruising (torso, ear, neck in < 4 yr; any bruising < 4 mo old), posterior rib fractures, metaphyseal corner fractures, retinal hemorrhages, burns with stocking/glove pattern. Workup: skeletal survey (< 2 yr), head CT/MRI, ophthalmology, full labs including CK, coagulation. Involve social work and CPS. Sexual abuse follows separate protocols.
Lead Toxicity
Screening recommended at 12 and 24 months in high-risk areas (older housing, Medicaid, immigrant populations). CDC reference value now 3.5 mcg/dL (lowered 2021). Levels ≥ 45 mcg/dL require chelation (succimer). Most commonly asymptomatic; neurodevelopmental harm is the concern.
17 Pediatric Procedures & Screening Tests Procedures
Outpatient pediatric procedures are low-complexity but high-volume. Inpatient and ED pediatrics adds several invasive procedures the scribe must document with precision.
| Procedure | Indication / Description |
|---|---|
| Vaccinations | IM (anterolateral thigh < 2 yr, deltoid ≥ 2 yr), SC, oral (rotavirus), intranasal (LAIV). Document site, route, lot, VIS date. |
| Urethral catheterization | Sterile urine for infants with fever; 5–8 Fr feeding tube or Coude catheter. |
| Suprapubic aspiration (SPA) | Bladder tap with 22 ga needle, ultrasound-guided, infants when cath fails. |
| Lumbar puncture (infant) | L4–L5 interspace, lateral or sitting position; send CSF for cell count, protein, glucose, culture, HSV PCR, enterovirus PCR, meningitis panel. |
| IV/IO access | Standard peripheral; intraosseous (proximal tibia) for emergency. |
| Growth measurements | Length on length-board < 2 yr, stadiometer ≥ 2 yr, weight on infant/child scale, head circumference with paper tape over occiput. |
| Vision screening | Red reflex (newborn), cover/uncover, photoscreener, HOTV or Lea symbols ≥ 3 yr, Snellen ≥ 5–6 yr. |
| Hearing screening | OAE/ABR newborn; pure-tone audiometry school age. |
| Developmental screening | ASQ-3 (parent, 9/18/30 mo), PEDS, M-CHAT-R/F (autism 18/24 mo), SWYC. |
| Point-of-care tests | Rapid strep, rapid flu, rapid RSV/COVID, urine dip, capillary glucose, bedside hemoglobin. |
| Tympanogram | Middle ear effusion detection. |
| Nebulizer / MDI-spacer | Asthma, bronchiolitis. |
| Simple laceration repair | Dermabond, Steri-Strips, or sutures depending on location/depth. |
| Fracture splinting | Sugar tong, volar, posterior slab, thumb spica. |
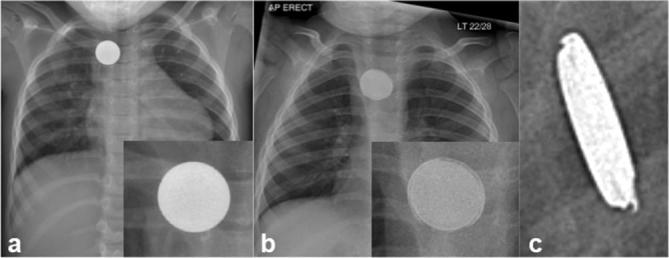
| Foreign body removal | Nose, ear, skin. |
18 Immunizations & the ACIP Schedule Preventive
The ACIP childhood & adolescent immunization schedule is the authoritative reference — updated annually. Scribes must know which vaccines are given at each visit to document accurately.
| Age | Vaccines |
|---|---|
| Birth | HepB #1 |
| 1–2 mo | HepB #2 |
| 2 mo | DTaP, Hib, IPV, PCV, Rotavirus |
| 4 mo | DTaP, Hib, IPV, PCV, Rotavirus |
| 6 mo | DTaP, Hib (varies), IPV, PCV, Rotavirus (RV5 only), HepB #3, annual influenza from 6 mo |
| 12–15 mo | MMR, Varicella, HepA #1, Hib booster, PCV booster |
| 15–18 mo | DTaP #4 |
| 18–24 mo | HepA #2 |
| 4–6 yr | DTaP, IPV, MMR, Varicella |
| 11–12 yr | Tdap, HPV (2-dose series, 3 doses if starting ≥ 15 yr), MenACWY |
| 16 yr | MenACWY booster, MenB (shared decision) |
| 6 mo and up | Influenza annually; COVID per current ACIP |
| RSV | Nirsevimab < 8 mo entering first RSV season, or maternal RSVpreF 32–36 wk |
Catch-up schedules follow a separate ACIP table. True contraindications are few (anaphylaxis to prior dose or vaccine component; encephalopathy within 7 days of pertussis for DTaP). Fever, mild illness, breastfeeding, prematurity, and family history of vaccine reaction are not contraindications.
19 Labs, Imaging & Diagnostic Interpretation Diagnostics
Common Labs
Pediatric reference ranges shift dramatically by age. Newborn Hgb is 14–22, drops to a physiologic nadir of 9–11 at 2–3 months, then rises. WBC trends from neutrophil-predominant (newborn) to lymphocyte-predominant (toddler) and back to neutrophil-predominant after age 5. Always document age-appropriate reference.
Inflammatory markers (CRP, procalcitonin, ESR) are central in the febrile infant workup. Urinalysis uses leukocyte esterase and nitrites for screening; culture confirms. Rapid strep and rapid influenza/RSV/COVID are routine POCT.
Common Imaging
CXR (pneumonia, foreign body, CHF), AP/lateral neck X-ray (steeple sign in croup, thumbprint in epiglottitis, retropharyngeal abscess), abdominal X-ray (obstruction, constipation, FB), abdominal ultrasound (pyloric stenosis, intussusception, appendicitis, renal/bladder), head US through anterior fontanelle (< 1 yr), echocardiogram (murmur, Kawasaki follow-up). Radiation stewardship is a constant theme — ALARA principle; ultrasound first whenever possible.
20 Medications & Weight-Based Dosing Pharmacology
Pediatric dosing is weight-based in mg/kg with a ceiling at adult dose. Always document the child's weight (today's weight, in kg) before prescribing. Common pitfalls: concentration confusion for liquid medications (e.g., amoxicillin 250/5 vs 400/5), teaspoons vs milliliters (use mL only), and forgetting to convert pounds to kilograms.
Acetaminophen (Tylenol): 10–15 mg/kg PO/PR q4–6h; max 75 mg/kg/day or 4,000 mg/day. Safe from birth.
Ibuprofen (Motrin/Advil): 5–10 mg/kg PO q6–8h; max 40 mg/kg/day. Not under 6 months. Avoid in dehydration and suspected hemorrhagic dengue.
| Drug | Dose | Use |
|---|---|---|
| Amoxicillin | 45–90 mg/kg/day div BID/TID | AOM, CAP, strep, sinusitis |
| Amox-clav | 45–90 mg/kg/day (amox) | Recurrent OM, bite wounds |
| Cephalexin | 25–50 mg/kg/day div QID | SSTI, UTI |
| Cefdinir | 14 mg/kg/day div BID | OM, CAP alt. |
| Azithromycin | 10 mg/kg day 1, 5 mg/kg day 2–5 | Atypical CAP, pertussis |
| Clindamycin | 20–40 mg/kg/day div TID/QID | MRSA SSTI, PCN allergy |
| TMP-SMX | 8–10 mg/kg/day (TMP) div BID | UTI, MRSA SSTI |
| Ceftriaxone | 50–75 mg/kg/day (100 for meningitis) | Serious infections, UTI IM |
Albuterol: Nebulized 0.15 mg/kg (min 2.5 mg, max 5 mg); MDI 4–8 puffs with spacer.
Dexamethasone: 0.6 mg/kg PO/IM/IV (max 16 mg) × 1–2 doses for asthma or croup.
Prednisolone: 1–2 mg/kg/day × 5 days for asthma exacerbation.
Ondansetron: 0.15 mg/kg (max 4–8 mg) PO ODT for vomiting.
Epinephrine (anaphylaxis): 0.01 mg/kg IM (1 mg/mL, max 0.3 mg); auto-injector 0.15 or 0.3 mg.
Diphenhydramine: 1 mg/kg PO/IV q6h; avoid in < 2 yr.
PEG 3350: 0.4–0.8 g/kg/day for constipation; 1–1.5 g/kg/day × 3 d for disimpaction.
ORS: 50–100 mL/kg over 2–4 hours plus replacement for ongoing losses.
21 Classification Systems & Scoring Tools Reference
| Parameter | 0 | 1 | 2 |
|---|---|---|---|
| Appearance (color) | Blue/pale | Body pink, extremities blue | All pink |
| Pulse | Absent | < 100 | ≥ 100 |
| Grimace (reflex irritability) | None | Grimace | Cry, cough, sneeze |
| Activity (tone) | Flaccid | Some flexion | Active motion |
| Respiration | Absent | Slow/irregular | Strong cry |
| Sign | 0 | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|---|
| Stridor | None | With agitation | At rest | |||
| Retractions | None | Mild | Moderate | Severe | ||
| Air entry | Normal | Decreased | Markedly decreased | |||
| Cyanosis | None | With agitation | At rest | |||
| LOC | Normal | Altered |
Mild ≤ 2, Moderate 3–5, Severe 6–11, Impending respiratory failure ≥ 12.
Scored from 0–12 using suprasternal retractions, scalene contractions, air entry, wheezing, and SpO2. Mild 0–3, moderate 4–7, severe 8–12.
New Ballard Score combines 6 neuromuscular criteria (posture, square window, arm recoil, popliteal angle, scarf sign, heel-to-ear) with 6 physical criteria (skin, lanugo, plantar surface, breast, eye/ear, genitalia). Sum gives gestational age 20–44 weeks.
Additional scales commonly referenced: Rochester / Philadelphia / Boston criteria (febrile infant risk), Centor/McIsaac (strep pharyngitis), Alvarado & PAS (pediatric appendicitis score), Yale Observation Scale (ill-appearing child), modified Kawasaki criteria (CREAM), NAEPP asthma severity/control, Rome IV (functional GI), DSM-5 (ADHD, autism, depression).
22 Physical Exam by Age Exam
The pediatric exam is performed in an order that respects the child's cooperation — from least to most distressing. Crying children are examined while held by the parent. Heart/lung auscultation is done early while the child is calm. Ear and throat exams are saved for last.
General: Well-appearing, active, playful, non-toxic / ill-appearing, lethargic, irritable. Describe level of consolability.
Vitals: HR, RR, SpO2, temp (site), BP if indicated. Weight, length/height, HC, BMI, percentiles.
HEENT: Fontanelles (anterior open/flat until ~18 mo), red reflex, PERRL, EOMI, TMs (color, position, landmarks, mobility), nares, oropharynx, dentition, neck suppleness.
Lungs: Work of breathing (retractions, grunting, nasal flaring, head bobbing), air entry, adventitious sounds, symmetry.
Cardiac: RRR, S1/S2, murmurs (grade, location, quality, radiation), femoral pulses (coarctation), perfusion/cap refill.
Abdomen: Soft, NT/ND, no HSM, no masses, BS normoactive, umbilicus.
GU: Tanner stage, external genitalia, testes descended, circumcision status.
MSK: Hip (Barlow/Ortolani < 3 mo, Galeazzi thereafter), spine, gait, ROM.
Skin: Rash, birthmarks, bruising (document pattern), turgor.
Neuro: Tone, primitive reflexes (Moro, suck, root, grasp, tonic neck, stepping) < 6 mo, gross/fine motor, cranial nerves, DTRs, gait.
Development: Age-appropriate milestones demonstrated or reported.
Always document general appearance first and last. Pediatricians make decisions largely on how the child looks — "well-appearing and non-toxic" is shorthand for "does not need an aggressive workup," and "toxic-appearing" is an alarm bell that must be charted verbatim when the clinician says it.
23 Abbreviations Master List Reference
Visits & Documentation
Diagnoses
Procedures & Scores
Medications & Labs
24 Sample HPI Templates & References Templates
These templates show the rhythm of a typical pediatric note. Use them as scaffolding during your first weeks of scribing.
"[Name] is a 12-month-old previously healthy, full-term female presenting with mother for routine 12-month well-child check. Interval history unremarkable — one mild URI 6 weeks ago managed supportively. Nutrition: transitioning from formula to whole milk, eating 3 meals/day of table foods, no food allergies. Sleep: 10–11 hours overnight plus one 2-hour nap, in own crib, back to sleep. Elimination: 1–2 formed stools/day, 6–8 wet diapers. Development: walks with one hand held, pulls to stand, says 'mama' and 'dada' specifically plus 'ba' for bottle, waves bye-bye, mature pincer grasp, follows simple gesture commands — all consistent with 12-month milestones. Safety: rear-facing car seat, home childproofed, no firearms, smoke detectors in place. Immunizations up to date. Mother has no concerns today."
"[Name] is a 22-day-old full-term (39+2 wks) male born via uncomplicated SVD to a GBS-negative mother with an unremarkable prenatal and nursery course, presenting with fever. Parents report a rectal temperature of 38.4°C at home 2 hours prior to arrival. Baby has been feeding slightly less (2 oz of formula every 3 hours instead of usual 3 oz), with 4 wet diapers today and one yellow seedy stool. No vomiting, diarrhea, cough, congestion, rash, or respiratory distress noted. No sick contacts; no recent travel. Delivery unremarkable, discharged at 48 hours, no NICU stay. On arrival, rectal temperature 38.2°C, HR 168, RR 48, SpO2 99% room air. Well-appearing but parents report decreased activity compared to baseline. Plan per AAP febrile infant guideline: full sepsis workup with CBC, blood culture, catheterized UA/culture, LP, procalcitonin, CRP, CXR and empiric ampicillin + gentamicin with admission to pediatrics."
"[Name] is a 7-year-old male with a history of moderate persistent asthma (on fluticasone 88 mcg 2 puffs BID and albuterol PRN) presenting with 2 days of worsening cough and wheezing triggered by a URI. Mother reports he has required albuterol MDI every 3–4 hours today with partial relief. Last oral steroid course was 3 months ago. No fever, no chest pain. Prior ED visits for asthma: 2 in the past 12 months, no prior intubations. On arrival, RR 36, SpO2 91% room air, HR 128, with suprasternal and subcostal retractions and diffuse end-expiratory wheezing. PRAM score 7 (moderate). Initial management: albuterol 5 mg + ipratropium neb, dexamethasone 0.6 mg/kg PO (max 16 mg), supplemental O2 via NC to maintain SpO2 ≥ 92%. Will reassess in 20 minutes."
"[Name] is a 2-year-old previously healthy female presenting with 2 days of non-bloody, non-bilious vomiting (6–8 episodes/day) and watery, non-bloody diarrhea (5–6 episodes/day). Onset after attending daycare where multiple children had similar symptoms. Mother reports decreased oral intake, 2 wet diapers in the past 12 hours (normally 6–8), no tears with crying, fussy but consolable. Low-grade fever (max 38.1°C) yesterday, no fever today. No abdominal distension, no blood in stools, no bilious emesis, no recent antibiotic use. On exam, mucous membranes dry, capillary refill 2–3 seconds, mildly sunken eyes, abdomen soft and non-tender — estimated 6–8% dehydration. Plan: ondansetron 2 mg ODT, begin ORS 5 mL every 1–2 minutes, reassess hydration in 1 hour; IV fluids if failed trial."
"[Name] is a 15-month-old male with no significant PMH presenting with 2 days of fussiness, tugging at the right ear, and fever to 39.0°C. URI prodrome of 4 days with rhinorrhea and cough. Tylenol has been helpful intermittently. PO intake mildly decreased but adequate urine output. Immunizations UTD including PCV. No daycare attendance. No prior episodes of otitis media. On exam, well-appearing, mildly fussy but consolable. Right TM bulging and erythematous with loss of landmarks; left TM normal. No mastoid tenderness. Diagnosis: unilateral AOM. Plan: amoxicillin 90 mg/kg/day divided BID × 10 days, acetaminophen/ibuprofen for pain, return precautions reviewed."
"[Name] is a 15-year-old female presenting with her mother for evaluation of declining school performance and low mood over the past 3 months. Mother stepped out for confidential interview. Patient reports persistent sadness, difficulty sleeping, loss of interest in band and softball, decreased appetite with 5 lb weight loss, and feelings of worthlessness. PHQ-A score 14 (moderate depression). Denies active suicidal ideation, plan, intent, or prior self-harm. HEEADSSS: lives with both parents, no recent stressors at home; grades declining from B's to D's; eating 1–2 meals/day; limited activities; denies substance use; not sexually active; no access to firearms in the home; seat belt always. Prior medical/psych history unremarkable. No family psychiatric history. Plan: counseling referral, consider SSRI trial, safety plan reviewed with patient and mother at end of visit, close follow-up in 2 weeks."
References & Sources
AAP Bright Futures. Guidelines for Health Supervision of Infants, Children, and Adolescents.
Lieberthal AS et al. The Diagnosis and Management of Acute Otitis Media. AAP. Pediatrics. 2013.
NHLBI/NAEPP 2020 Focused Updates to the Asthma Management Guidelines.
ACIP Childhood & Adolescent Immunization Schedule. CDC.
US Preventive Services Task Force pediatric recommendations.
CDC Growth Charts (2–20 yr) & WHO Growth Standards (0–2 yr).
Figure 1: CDC Growth Chart. Centers for Disease Control and Prevention. Public domain.
Figure 2: Otitis Media Otoscopic Findings. B. Welleschik, Wikimedia Commons. CC BY-SA 3.0.
Figure 3: Hand, Foot and Mouth Disease. KlatschmohnAcker, Wikimedia Commons. CC BY-SA 3.0.
Figure 4: Tanner Stages. M.Komorniczak, Wikimedia Commons. CC BY-SA 3.0.
Pediatrics is the specialty where tiny details change everything: a rectal temperature 0.4°C higher, a weight dropping one percentile line, a missed milestone, a parent's offhand comment about a bruise. Great pediatric scribes listen for all of it and chart it without being asked. They know the AAP guidelines well enough to anticipate the workup the attending will order. They pre-populate growth curves and immunization records. They notice that a 3-week-old with fever means a full sepsis workup and they start building the note accordingly.
Above all, great pediatric scribes understand that the medical record is often a child's only ongoing narrative — the place where growth, development, milestones, and family context accumulate across years. Your notes today become the baseline the next clinician compares against. Write them with that in mind.
Welcome to pediatrics.