Plastic & Reconstructive Surgery
Every diagnosis, flap, procedure, medication, classification, and documentation framework you need to succeed on day one and beyond.
All diagrams on this page are sourced from published educational or institutional materials rather than AI generation. Each figure caption links to the original source, and the full diagram and guideline citations are collected in the references section at the bottom.
01 Skin & Soft Tissue — Anatomy Essentials
Plastic and reconstructive surgery is the specialty of form and function of the integument and soft tissues. Plastic surgeons operate everywhere on the body: face, scalp, breast, trunk, perineum, upper extremity, lower extremity, and intraoral/pharyngeal structures. Their expertise is not a specific organ but a technique set — how to move skin, fat, muscle, fascia, bone, and nerve from one place to another and keep the tissue alive. The anatomy you must know, therefore, is the anatomy of the soft tissue envelope, the vascular supply of each region, and the sensory/motor innervation patterns.
Skin Layers
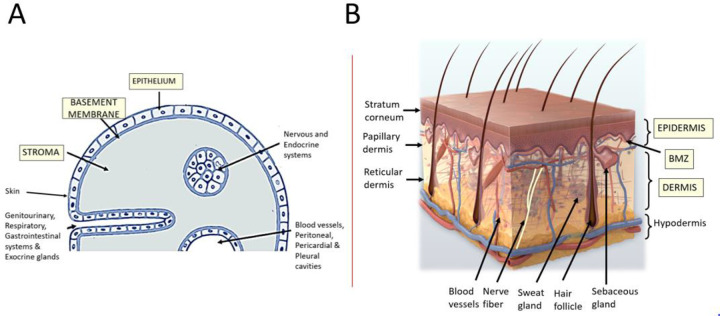
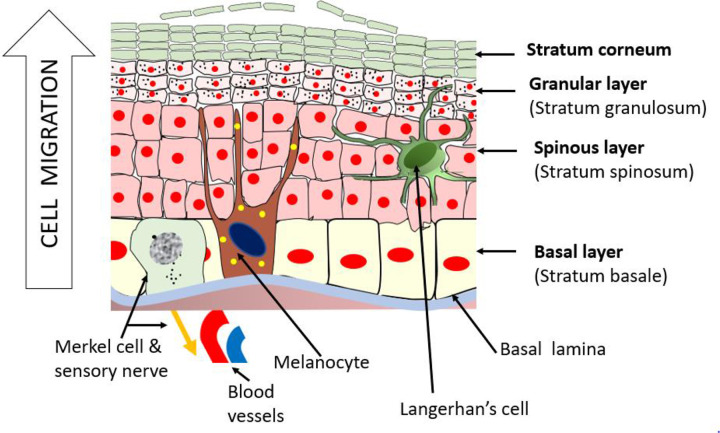
The skin is composed of the epidermis (stratified squamous epithelium), the dermis (papillary and reticular layers containing collagen, elastin, hair follicles, sebaceous and sweat glands, and the deep vascular plexus), and the subcutaneous fat (hypodermis). Beneath the fat lies the superficial fascia, then deep fascia, then muscle and bone. A partial-thickness wound injures epidermis and part of the dermis and heals by re-epithelialization from adnexal structures; a full-thickness wound destroys all dermal appendages and heals by contraction and scarring, or requires grafting/flap coverage.
Facial Anatomy & the SMAS
Facial layers from superficial to deep are: skin, subcutaneous fat, the superficial musculoaponeurotic system (SMAS) (continuous with the platysma in the neck and the temporoparietal fascia in the temple), the parotidomasseteric fascia covering the deep structures, and then the facial nerve branches (temporal, zygomatic, buccal, marginal mandibular, cervical) traveling on the deep surface of the SMAS. Facial arterial supply comes primarily from the facial artery, superficial temporal artery, infraorbital, supraorbital, and supratrochlear branches. The aesthetic subunits of the face (forehead, cheek, nose with its 9 subunits, lip, chin, eyelid) guide local flap design — when possible, reconstruction replaces an entire subunit rather than patching across subunit borders.
Breast Anatomy
The breast sits on the pectoralis major muscle between the 2nd and 6th ribs, anchored by Cooper's ligaments. Blood supply comes from the internal mammary (internal thoracic) artery perforators medially, the lateral thoracic artery laterally, and branches of the thoracoacromial artery superiorly. The nipple-areola complex (NAC) is innervated by the lateral cutaneous branch of the 4th intercostal nerve. Lymphatic drainage is primarily to the axillary nodes (levels I, II, III) with additional drainage to internal mammary nodes — critical for oncologic decision-making.
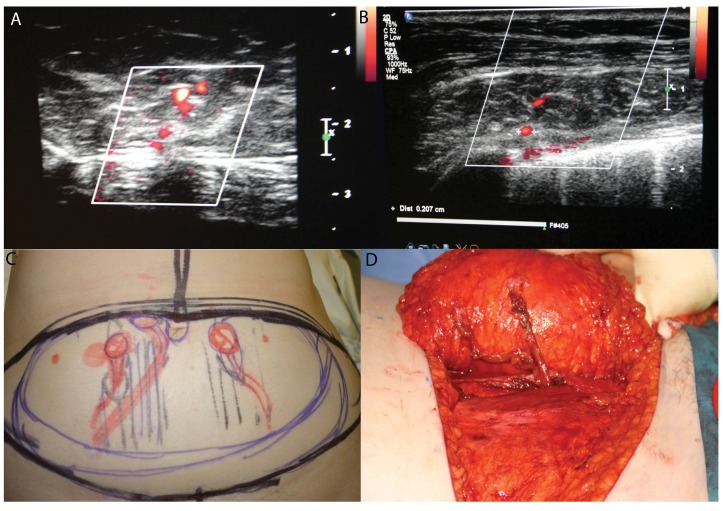
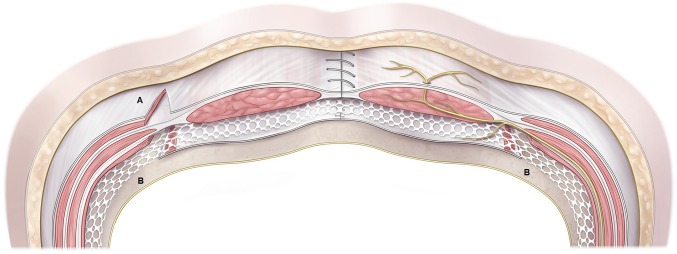
Abdominal Wall & the DIEP Concept
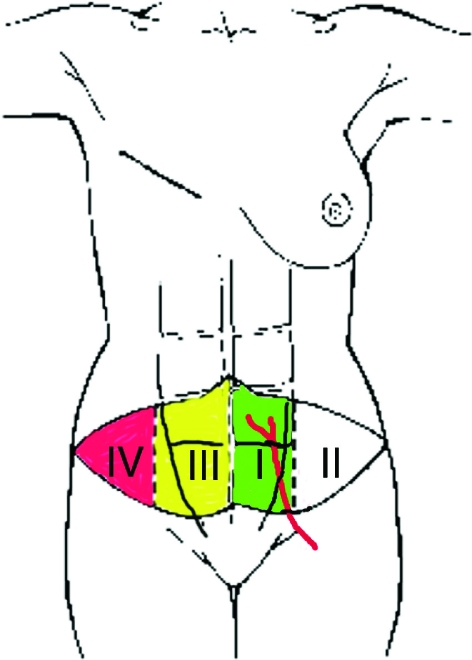
The abdominal wall is supplied by the deep inferior epigastric artery (DIEA), which branches off the external iliac artery and travels deep to the rectus abdominis muscle, sending perforators up through the muscle to supply the overlying skin and fat. These perforators are the basis of the DIEP flap, the workhorse of autologous breast reconstruction. The superficial inferior epigastric artery (SIEA) is a smaller, more variable vessel that can occasionally supply a flap without dissecting through muscle (SIEA flap).
Extremity Angiosomes
The body is divided into angiosomes — three-dimensional territories supplied by a source artery. On the lower leg, the anterior tibial, posterior tibial, and peroneal arteries each supply predictable skin, fascia, and muscle territories, which determines which fasciocutaneous or muscle flap will reliably cover a defect. On the hand, digital arteries course on the volar-lateral aspect of each finger, paired with the digital nerves (Cleland's and Grayson's ligaments anchor the neurovascular bundle).
You will hear "perforator" constantly. A perforator is a small artery/vein that "perforates" through muscle or fascia to supply overlying skin. Perforator flaps (DIEP, ALT, TAP, PAP) preserve the source muscle, reducing donor-site morbidity. Always chart which perforators were used (single, dual, row), their location, and their caliber if mentioned.
02 Scribe Documentation Framework
The Plastic Surgery SOAP Note
Plastic surgery clinics run a wide mix of encounters: post-op flap checks, oncologic reconstruction consults, trauma follow-ups, cosmetic consultations, suture removals, and scar management. Each has a different note rhythm, but all follow a SOAP structure.
Chief Complaint: Examples — "post-op day 3 after left DIEP flap," "non-healing lower leg wound," "consult for breast reconstruction after mastectomy," "facelift consult," "dog bite to face."
HPI: For reconstructive patients, always capture the inciting injury/diagnosis, prior treatments and operations, wound duration, size changes, drainage, pain, functional limitations, and smoking status (critical for flap survival). For aesthetic patients, capture the patient's goals in their own words, prior cosmetic history (injectables, surgeries, implants), and realistic expectations.
PMHx / PSHx: Diabetes, vascular disease, connective tissue disorders, prior radiation, chemotherapy, steroids, anticoagulation, and — for reconstructive oncology — the full oncologic timeline (diagnosis date, staging, neoadjuvant therapy, surgery, adjuvant therapy).
Social: Smoking (nicotine causes flap loss — zero tolerance for microsurgical candidates, typically 4 weeks of cessation required), alcohol, recreational drugs, occupation (affects hand surgery recovery), and psychosocial support for major reconstruction.
Wound / defect description: Location, dimensions (length × width × depth in cm), exposed structures (bone, tendon, hardware, vessel), presence of granulation tissue, slough, eschar, undermining, tunneling, drainage (serous, sanguineous, purulent), and surrounding skin (erythema, induration, maceration).
Flap check: Color (pink, pale, dusky, blue), capillary refill (brisk < 2 sec, sluggish > 3 sec, none), temperature (warm, cool), turgor, Doppler signal (audible, diminished, absent), pinprick bleeding (brisk red, sluggish dark, none).
Donor site: Describe separately — abdomen for DIEP, thigh for ALT, back for LD, etc.
Each diagnosis gets an ICD-10 code (e.g., C50.911 breast cancer, T31.20 burns 20-29% TBSA, S01.91XA open wound scalp). Plans commonly include: wound care regimen, dressing changes, drain management, return to OR for debridement/closure, imaging, physical therapy, scar management, and follow-up interval.
Operative Note Elements Unique to Plastic Surgery
Op notes must capture: (1) the defect — location, size, exposed structures, prior treatment; (2) the reconstructive choice and why (the reconstructive ladder decision); (3) flap design — skin paddle dimensions, pedicle, perforator count; (4) ischemia time for free flaps; (5) microvascular anastomosis details — recipient artery and vein, end-to-end vs end-to-side, coupler size for venous anastomosis, patency confirmation; (6) donor site closure; (7) drains; (8) dressings.
When charting flap operations, memorize the phrase "flap was inset, capillary refill brisk, Doppler signals strong over the skin paddle at [location]". This is the standard close-of-case documentation. If the surgeon says the anastomosis "looks good" you should still ask for the specifics — vessel names, coupler size, and any revision.
03 Skin Cancer Reconstruction Oncologic
Plastic surgeons receive an enormous volume of referrals for reconstruction of skin cancer defects, most commonly from Mohs micrographic surgery dermatologists who have excised the tumor but left a defect that exceeds what can be closed primarily. The three main skin cancers are basal cell carcinoma (BCC), squamous cell carcinoma (SCC), and melanoma.
Basal Cell Carcinoma
BCC is the most common human cancer. It arises from basal keratinocytes, grows slowly, rarely metastasizes, but is locally destructive. Subtypes include nodular (most common, pearly papule with telangiectasias), superficial, morpheaform/infiltrative (aggressive, ill-defined borders — requires Mohs), and pigmented. The face, ears, and scalp are the highest-frequency sites. Management is surgical excision or Mohs, with reconstruction based on defect size, depth, and location.
Squamous Cell Carcinoma
SCC arises from keratinocytes in the spinous layer and has real metastatic potential (2–5% overall, higher for lip, ear, immunosuppressed, perineural invasion, > 2 cm, > 6 mm depth, poorly differentiated). Precursors include actinic keratoses and Bowen's disease (SCC in situ). High-risk SCC may require wider margins, sentinel lymph node biopsy, and post-op radiation. NCCN non-melanoma skin cancer guidelines define high-risk features and management pathways.
Melanoma
Melanoma arises from melanocytes and has the most metastatic potential. The ABCDE rule guides clinical suspicion: Asymmetry, Border irregularity, Color variation, Diameter > 6 mm, Evolution. Breslow depth determines surgical margin and SLN biopsy threshold. NCCN melanoma guidelines recommend margins of 0.5–1 cm for in situ, 1 cm for ≤ 1 mm, 1–2 cm for 1–2 mm, and 2 cm for > 2 mm, with SLN biopsy considered for Breslow > 0.8 mm or with adverse features.
| T Stage | Breslow Depth | Margin | SLN Biopsy |
|---|---|---|---|
| Tis (in situ) | Confined to epidermis | 0.5–1.0 cm | Not indicated |
| T1a | < 0.8 mm, no ulceration | 1.0 cm | Discuss if ≥ 0.8 mm or risk features |
| T1b | < 0.8 mm ulcerated, or 0.8–1.0 mm | 1.0 cm | Recommended |
| T2 | 1.01–2.0 mm | 1–2 cm | Recommended |
| T3 | 2.01–4.0 mm | 2 cm | Recommended |
| T4 | > 4.0 mm | 2 cm | Recommended |
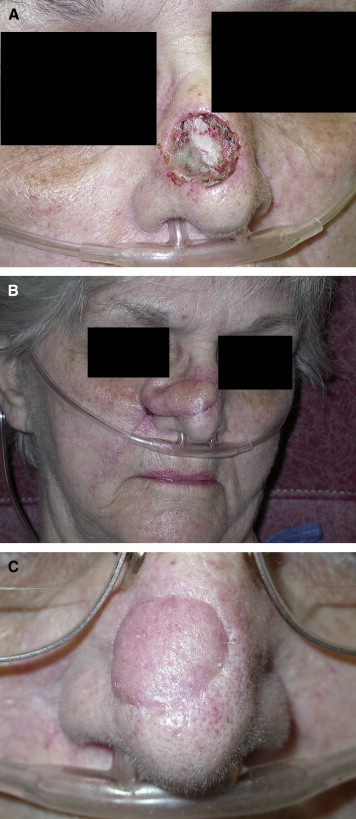
Reconstruction Strategy
Reconstruction of Mohs or wide excision defects follows the reconstructive ladder: secondary intention, primary closure, skin graft, local flap, regional flap, free flap. The face is usually reconstructed with local flaps to match color and texture. Common facial choices include advancement flaps for forehead and cheek, rhomboid (Limberg) flaps for cheek and temple, bilobed flaps and nasolabial flaps for the nose, paramedian forehead flaps for large nasal defects (staged, with pedicle division at 3 weeks), and cervicofacial advancement for large cheek defects.
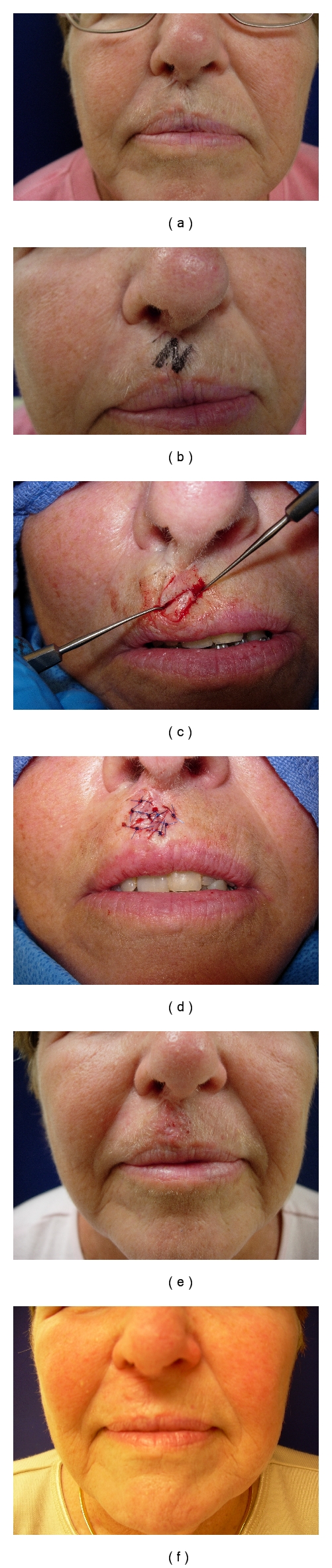
When charting a Mohs reconstruction, always document (1) the pre-op defect size and location (e.g., "2.3 × 1.8 cm full-thickness defect left nasal ala after Mohs for BCC"), (2) exposed structures, (3) the chosen flap with its name, and (4) any cartilage grafts or lining reconstruction needed.
04 Breast Cancer Reconstruction Oncologic
Breast reconstruction restores the shape and appearance of the breast after mastectomy or lumpectomy. It can be immediate (at the time of mastectomy) or delayed (weeks to years later). The two main techniques are implant-based and autologous (flap-based), and the choice depends on body habitus, prior radiation, comorbidities, patient preference, and oncologic timing. ACS NCDB breast reconstruction analysis documents trends and outcomes; NCCN breast cancer guidelines govern the oncologic side.
Implant-Based Reconstruction
Implant reconstruction uses a silicone or saline prosthesis. The modern approaches are:
- Two-stage expander/implant: A tissue expander is placed at mastectomy, gradually inflated with saline over weeks, then exchanged for a permanent implant.
- Direct-to-implant (DTI): A permanent implant is placed at the initial mastectomy, typically when the skin envelope is adequate.
- Prepectoral: Implant placed on top of the pectoralis muscle, usually wrapped in acellular dermal matrix (Alloderm, FlexHD). Less muscle pain, no animation deformity.
- Subpectoral (dual-plane): Implant partially covered by pectoralis major. Older technique; increased animation and pain.
Autologous Reconstruction
Autologous reconstruction uses the patient's own tissue. Options include:
- DIEP flap (deep inferior epigastric perforator) — the workhorse free flap. Takes abdominal skin and fat without sacrificing rectus muscle.
- MS-TRAM (muscle-sparing transverse rectus abdominis myocutaneous) — takes a small cuff of rectus.
- SIEA (superficial inferior epigastric artery) — no muscle dissected but vessel is unreliable in ~30% of patients.
- LD flap (latissimus dorsi) — pedicled or free; often combined with an implant for volume.
- PAP flap (profunda artery perforator) — posterior thigh donor.
- TUG/TMG flap (transverse/vertical upper gracilis) — medial thigh.
- SGAP/IGAP (superior/inferior gluteal artery perforator) — buttock donor.
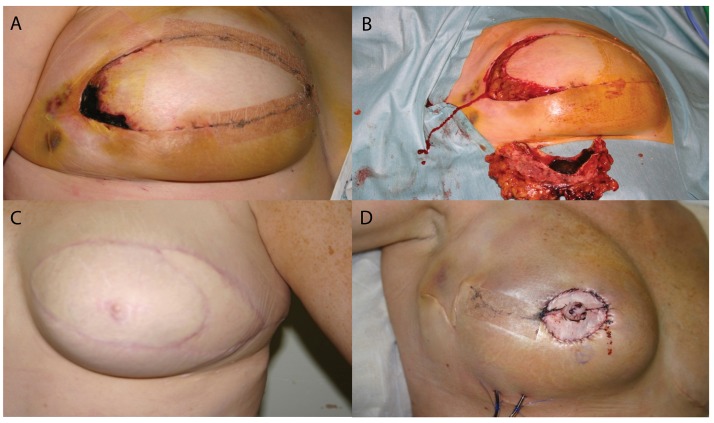
Oncoplastic & Nipple Reconstruction
Oncoplastic breast reconstruction combines lumpectomy with immediate reshaping using breast reduction or mastopexy techniques. It allows wider margins for larger tumors while preserving cosmetic outcome. Nipple reconstruction is performed 3–6 months after flap/implant settle, most commonly using a CV flap (skate flap, star flap), followed months later by 3D tattooing of the areola.
Post-mastectomy radiation (PMRT) damages implant-based reconstruction — causing capsular contracture rates approaching 40–50% — but is much better tolerated by autologous flaps. When PMRT is anticipated, many surgeons prefer delayed autologous reconstruction or a "delayed-immediate" approach with an expander placed at mastectomy and definitive reconstruction after radiation.
05 Head & Neck Reconstruction Oncologic
Head and neck cancer (most commonly oral cavity, oropharynx, larynx, and cutaneous) generates some of the most complex reconstructions in plastic surgery. Defects may involve skin, mucosa, muscle, bone (mandible, maxilla, orbit), and nerves. The plastic surgeon works alongside head and neck oncologic surgeons (ENT/OHNS) who resect the tumor.
Common Defects & Reconstructive Choices
| Defect | Workhorse Flap | Alternative |
|---|---|---|
| Small oral cavity / tongue | Radial forearm free flap (thin, pliable) | Buccal mucosa flap, primary closure |
| Total glossectomy / large tongue | ALT flap (anterolateral thigh) | Rectus abdominis free flap |
| Mandible (segmental) | Fibula free flap (osteocutaneous) | Scapular tip, DCIA, reconstruction plate |
| Maxilla | Fibula, scapular, ALT +/- bone | Obturator prosthesis |
| Pharyngeal / laryngectomy | ALT tubed flap, jejunum free flap | Radial forearm tubed |
| Skull base / scalp | Latissimus dorsi free flap with STSG | ALT free flap |
| Total lower lip | Karapandzic flap, radial forearm with palmaris sling | Abbe-Estlander flap (smaller defect) |
The fibula osteocutaneous free flap is the mandibular workhorse because it provides 20–25 cm of bicortical bone that accepts dental implants, plus a skin paddle for intraoral lining. Before harvest, a CTA of the leg confirms three-vessel runoff so the peroneal can be sacrificed without ischemia. The scapular/parascapular system provides bone and large soft tissue paddles on the circumflex scapular and thoracodorsal vessels.
Head and neck free flap monitoring is more difficult when the skin paddle is buried (intraoral). Many programs use an externalized skin paddle or implantable Doppler for the first 72 hours. Chart Doppler signals every 1–2 hours per the program protocol.
06 Lower Extremity Reconstruction Reconstructive
Lower extremity reconstruction is performed for trauma (Gustilo IIIB/C open fractures), oncologic resection (sarcoma), infection (osteomyelitis), and diabetic/vascular wounds. The principle: cover exposed bone, tendon, or hardware with durable, well-vascularized tissue.
Gustilo Classification of Open Fractures
| Grade | Wound | Soft Tissue | Reconstruction |
|---|---|---|---|
| I | < 1 cm, clean | Minimal injury | Primary closure after irrigation |
| II | 1–10 cm | Moderate, no flap needed | Primary or delayed closure |
| IIIA | > 10 cm | Adequate local coverage | Primary or local closure |
| IIIB | > 10 cm | Exposed bone, periosteal stripping, requires flap | Local or free flap |
| IIIC | Any | Arterial injury requiring repair | Vascular repair + flap |
Coverage by Zone
The classic "thirds" rule of lower leg coverage: upper third — medial gastrocnemius flap (rotation); middle third — soleus flap; lower third / distal tibia / ankle — free flap (ALT, gracilis, latissimus, radial forearm). The foot and heel often require free tissue transfer to provide durable coverage. Fasciocutaneous flaps (reverse sural, propeller flaps based on peroneal or posterior tibial perforators) are alternatives in selected patients.
Diabetic Foot & Chronic Wound Reconstruction
Reconstruction of diabetic foot ulcers requires vascular optimization first (revascularization if ABI < 0.7 or TBI < 0.7), infection control, offloading, and glycemic control. Once the wound bed is ready, options include dermal substitutes (Integra), split-thickness skin grafts, local flaps, or free tissue transfer for limb salvage. IWGDF diabetic foot guidelines provide the evidence base.
07 Upper Extremity & Hand Reconstruction Reconstructive
Hand surgery has a large overlap with plastic surgery — many plastic surgeons complete hand fellowships and run hand call. The specialty covers fingertip injuries, nail bed lacerations, flexor and extensor tendon injuries, digital nerve repair, replantation of amputated digits, Dupuytren contracture, carpal tunnel and cubital tunnel releases, trigger finger, de Quervain tenosynovitis, ganglion cysts, CMC arthroplasty, scaphoid fractures, distal radius fractures, and complex upper extremity trauma.
Key Hand Principles for Scribes
- Zone nomenclature for flexor tendons: Zone I (distal to FDS insertion), Zone II ("no man's land" — A1 pulley to FDS insertion, worst outcomes), Zone III (palm), Zone IV (carpal tunnel), Zone V (proximal to carpal tunnel).
- Fingertip amputations are classified by Allen zones I-IV based on level relative to the nail. Coverage options include healing by secondary intention, V-Y advancement, cross-finger flap, thenar flap, Moberg flap, and homodigital island flaps.
- Replantation indications include thumb amputations, multiple digits, pediatric amputations, and hand/wrist amputations. Ischemia time matters: warm ischemia < 12 h for digits, cold ischemia up to 24 h.
- Nerve repair: Direct primary epineural repair if possible, otherwise nerve autograft (sural, MACN), processed nerve allograft (Avance), or nerve conduit for small gaps.
When charting hand lacerations, always document which structures are intact or injured (skin only vs partial tendon vs full tendon vs neurovascular). Surgeons will use terms like "FDP only," "FDS and FDP," "digital nerve intact by two-point discrimination." Know what FDP (flexor digitorum profundus), FDS (flexor digitorum superficialis), EPL (extensor pollicis longus), EDC (extensor digitorum communis) mean.
08 Burns — Acute Care & Reconstruction Burn
Burn care sits at the intersection of critical care, plastic surgery, and rehabilitation. In the acute phase, burn surgeons (often plastic or general surgery trained) manage fluid resuscitation, airway, debridement, and grafting. In the late phase, reconstruction addresses scars, contractures, and cosmetic sequelae.

Burn Depth
| Depth | Appearance | Sensation | Healing |
|---|---|---|---|
| Superficial (1st deg) | Red, dry, no blisters (sunburn) | Painful | 3–6 days, no scar |
| Superficial partial (2nd) | Red, moist, blistered, blanches | Very painful | 1–3 weeks, minimal scar |
| Deep partial (2nd) | Pale white or mottled, less blanching | Decreased sensation | > 3 weeks, hypertrophic scar; often grafted |
| Full thickness (3rd) | Leathery, white/charred, dry, no blanching | Insensate | Requires excision & grafting |
| Subdermal (4th) | Involves muscle, bone, tendon | Insensate | Requires flap or amputation |
TBSA & Resuscitation
Estimate TBSA using the rule of nines (adults): head 9%, each arm 9%, each leg 18%, anterior trunk 18%, posterior trunk 18%, perineum 1%. For children use the Lund-Browder chart, which adjusts for the proportionally larger head in younger children. Do not count superficial (1st degree) burns in TBSA.
The Parkland formula estimates initial fluid needs: 4 mL × weight (kg) × %TBSA of lactated Ringer's over the first 24 hours, with half in the first 8 hours from the time of burn (not arrival). Titrate to urine output of 0.5 mL/kg/hr adults, 1 mL/kg/hr children. American Burn Association resuscitation guidelines emphasize titration rather than rigid formula adherence to avoid fluid creep.
Escharotomy & Fasciotomy
Circumferential full-thickness burns on extremities can cause compartment syndrome as edema expands beneath inelastic eschar. Escharotomy — longitudinal incision through eschar — releases pressure. Torso escharotomies are performed when chest restriction impairs ventilation.
Burn Surgery
Deep partial and full-thickness burns are excised (tangential or fascial) and covered with split-thickness skin grafts (STSG), often meshed 1:1.5 or 1:3 to cover more area. For massive burns, cultured epidermal autograft (CEA, Epicel) or dermal substitutes (Integra, NovoSorb BTM) are used to buy time. Post-burn reconstruction addresses scar contractures with Z-plasties, skin grafts, tissue expansion, and flaps.

Partial thickness > 10% TBSA; any full thickness; face, hands, feet, genitalia, perineum, major joints; chemical, electrical, or inhalation injury; pediatric or complex comorbidity. Chart these criteria explicitly in transfer notes.
09 Facial Trauma & Fractures Craniofacial
Plastic surgeons cover facial trauma call alongside OMFS and ENT. Fractures are evaluated clinically and with CT maxillofacial (thin-cut, coronal and sagittal reformats).
Major Fracture Patterns
- Mandibular fractures: Most common sites are body, angle, condyle, symphysis, parasymphysis. Patients present with malocclusion, trismus, intraoral laceration, and step-offs. Treatment: maxillomandibular fixation (MMF) alone for favorable fractures, or ORIF with plates/screws (AO mini/micro).
- Maxillary (Le Fort) fractures: Three classic patterns — Le Fort I (transverse, separates maxilla from nasal floor), Le Fort II (pyramidal, through nasal bridge and infraorbital rim), Le Fort III (craniofacial dysjunction, complete separation of face from skull base).
- Zygomaticomaxillary complex (ZMC) "tripod": Fractures at zygomaticofrontal suture, zygomaticomaxillary buttress, zygomatic arch, and infraorbital rim. Treatment: ORIF via upper blepharoplasty, intraoral sulcus, and/or subciliary approaches.
- Orbital floor fracture ("blowout"): Isolated floor fracture from blunt globe trauma. Watch for entrapment (restricted upgaze, diplopia), enophthalmos, infraorbital nerve hypesthesia. Indications for repair: entrapment (urgent), large defect (> 50% floor or > 2 cm2), early enophthalmos.
- Nasoorbitoethmoid (NOE) fractures: Injury to the central midface with telecanthus (widening of medial canthal distance > 35 mm), saddle nose, and CSF rhinorrhea risk. Markowitz classification I-III based on medial canthal tendon status.
- Frontal sinus fractures: Classified by anterior table, posterior table, and nasofrontal outflow tract involvement. Management ranges from observation to obliteration or cranialization.
- Panfacial fractures: Combined upper, middle, and lower face injuries. Reconstruction proceeds by establishing occlusion first, then building outward.
Always document occlusion in facial trauma notes: "patient's occlusion is reproducible and matches reported baseline" or "malocclusion with anterior open bite and right-sided premature contact." Malocclusion = mandibular or Le Fort fracture until proven otherwise.
10 Soft Tissue Facial Wounds & Dog Bites Craniofacial
Lip, cheek, eyelid, ear, and scalp lacerations and dog bites make up the bulk of ED plastic surgery consults. Principles: copious irrigation, conservative debridement (the face has excellent blood supply — preserve tissue), meticulous layered repair, align landmarks (vermillion border, gray line of eyelid, helical rim), tetanus update, and rabies prophylaxis if indicated.
Lip lacerations: The vermillion-cutaneous junction must be aligned with the first suture; a 1 mm misalignment is obvious from across the room. Through-and-through lacerations are repaired in three layers: mucosa, orbicularis oris, skin.
Eyelid lacerations: Evaluate the canalicular system (medial lid lacerations) — canalicular involvement requires repair over a silicone stent. Full-thickness lid lacerations are repaired in layers: tarsus/conjunctiva, orbicularis, skin. Align the gray line.
Ear lacerations: Align the helical rim; cartilage is minimally debrided and covered by skin; avoid through-and-through cartilage sutures. For partial amputations with a pedicle of skin, maintain perfusion; complete amputations may require composite grafting or microvascular replantation (rare).
Dog bites: High risk of infection (Pasteurella, Staphylococcus, Streptococcus, anaerobes). Irrigate copiously, debride devitalized tissue, and typically close primarily on the face (with antibiotic coverage) but leave open on extremities. Amoxicillin-clavulanate (Augmentin) 875/125 BID is standard prophylaxis. Document the dog's vaccination status, the circumstances of the bite, and a rabies risk assessment.
11 Cleft Lip, Cleft Palate & Craniofacial Craniofacial
Craniofacial surgery is a plastic surgery subspecialty addressing congenital and developmental anomalies of the skull and face. Patients are typically managed in multidisciplinary cleft/craniofacial teams (plastic surgery, ENT, orthodontics, speech, audiology, genetics, psychology, pediatric dentistry).
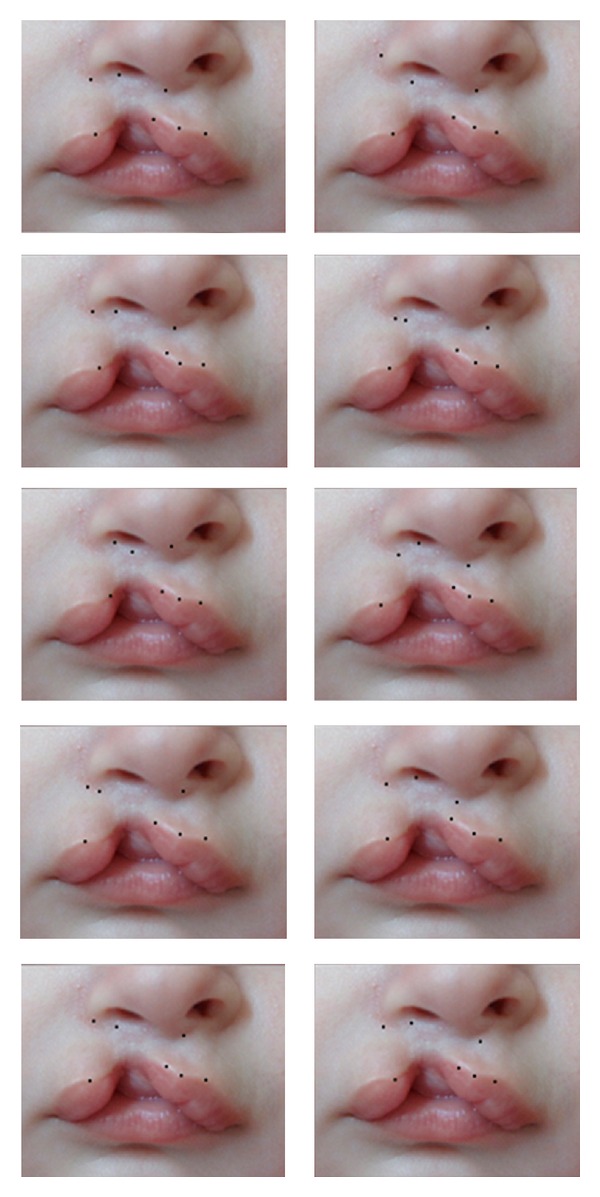
Cleft Lip & Palate
Cleft lip results from failure of fusion of the medial and lateral nasal prominences with the maxillary prominence in weeks 4–7. Cleft palate results from failure of fusion of the palatal shelves in weeks 8–12. Clefts may be unilateral or bilateral, complete or incomplete, and may involve lip, alveolus, primary palate, and/or secondary palate.
Timeline of care (rule of 10s for lip repair): ≥ 10 weeks old, ≥ 10 lbs, ≥ 10 g/dL hemoglobin.
- Nasoalveolar molding (NAM) appliance: 0–3 months
- Cleft lip repair: ~3 months (Millard rotation-advancement, Mohler modification, Fisher anatomic subunit)
- Cleft palate repair: ~10–12 months (Furlow double-opposing Z-plasty, two-flap palatoplasty, von Langenbeck)
- Speech evaluation: 3–5 years, possible pharyngeal flap or sphincter pharyngoplasty for velopharyngeal insufficiency
- Alveolar bone grafting: 7–9 years (iliac crest cancellous bone)
- Orthognathic surgery and rhinoplasty: skeletal maturity (late adolescence)
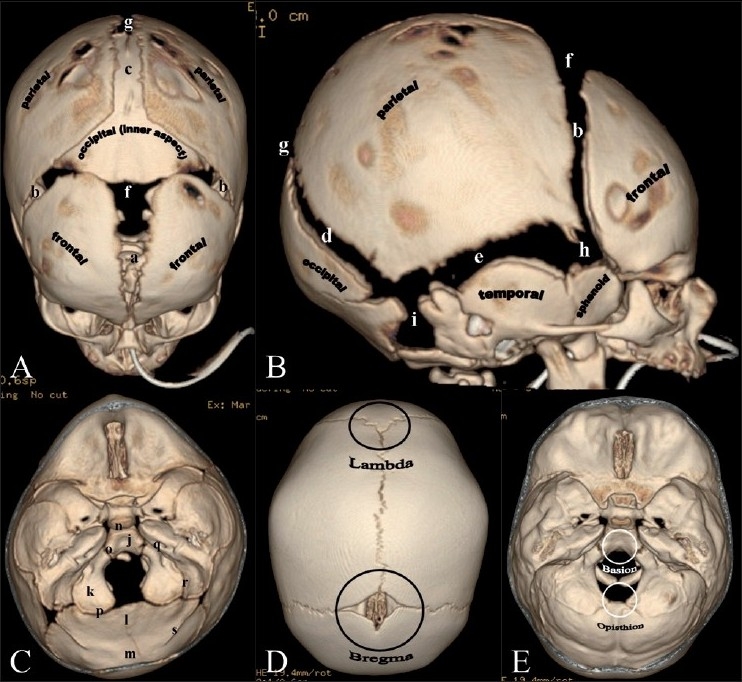
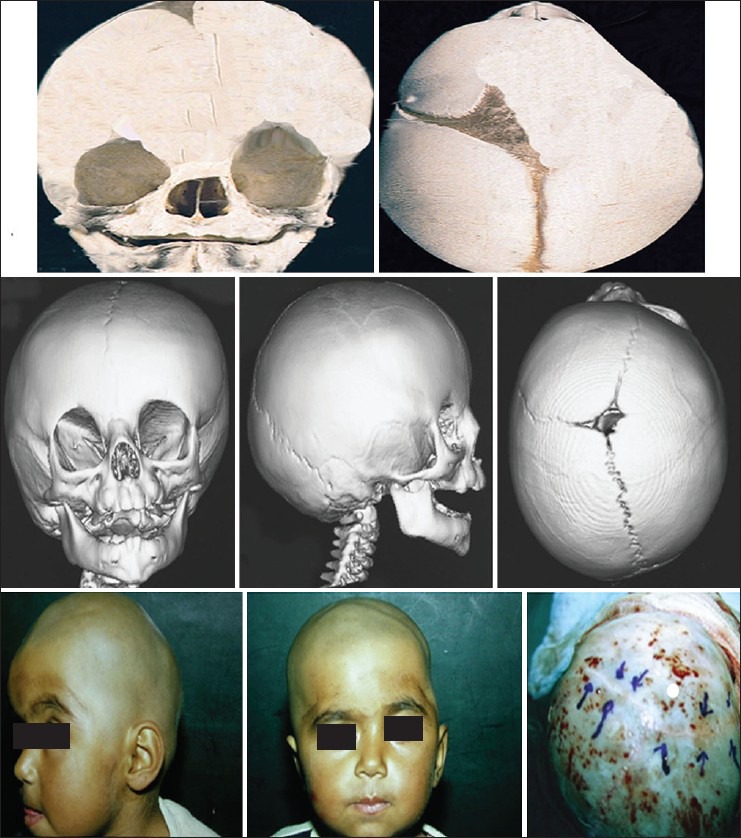
Craniosynostosis
Craniosynostosis is premature fusion of one or more cranial sutures, causing characteristic head shapes: scaphocephaly (sagittal suture, long narrow), trigonocephaly (metopic, triangular forehead), plagiocephaly (unilateral coronal, asymmetric), brachycephaly (bilateral coronal, wide and short), turricephaly (multiple sutures, tower-shaped). Treatment is cranial vault remodeling or endoscopic strip craniectomy with helmet therapy (< 3–4 months).
Craniofacial Syndromes
- Apert syndrome: FGFR2 mutation; bicoronal synostosis, midface hypoplasia, symmetric syndactyly ("mitten hand").
- Crouzon syndrome: FGFR2; multisuture synostosis, exorbitism, midface hypoplasia, normal hands.
- Pfeiffer syndrome: FGFR1/2; synostosis, broad thumbs/great toes, midface hypoplasia.
- Treacher Collins syndrome: TCOF1; mandibular and zygomatic hypoplasia, downslanting palpebral fissures, coloboma, microtia.
- Goldenhar / hemifacial microsomia: Asymmetric mandibular and ear hypoplasia, epibulbar dermoid.
- Pierre Robin sequence: Micrognathia, glossoptosis, airway obstruction +/- cleft palate.
Microtia & Ear Reconstruction
Microtia (small or absent external ear) is reconstructed in stages using autologous costal cartilage carved into a framework (Nagata or Brent technique) or with a porous polyethylene implant (Medpor). Bone-anchored hearing aids (BAHA) may be added for conductive hearing loss.
Tessier Rare Facial Clefts
The Tessier classification numbers rare facial clefts 0 through 14, radiating from the mouth (0–8) and from the orbit (9–14), with pairs summing to 14 lying along a continuous vertical axis. For example, Tessier 0 is a midline cleft of the upper lip; 7 is a transverse facial cleft (macrostomia); 14 is a midline frontal/cranial cleft. The full 15-number system is referenced in craniofacial notes — you don't need to memorize each, but recognize the name and know scribes must document the number assigned by the surgeon.
12 Lymphedema Surgery Reconstructive
Lymphedema is chronic swelling from impaired lymphatic drainage, most commonly after axillary or inguinal lymph node dissection for cancer (secondary) but also congenital (primary). Conservative management includes complete decongestive therapy (manual lymphatic drainage, compression, skin care, exercise). When refractory, surgical options are offered.

- Lymphovenous anastomosis (LVA): Supermicrosurgical anastomosis of subdermal lymphatic channels (0.3–0.8 mm) to nearby venules, shunting lymph into the venous system. Best for early-stage disease.
- Vascularized lymph node transfer (VLNT): Lymph nodes harvested from the groin, supraclavicular fossa, or submental region are transplanted as a free flap with their vascular pedicle to the affected extremity.
- LYMPHA (lymphatic microsurgical preventive healing approach): Performed at the time of axillary dissection; axillary lymphatics are anastomosed to branches of the axillary vein prophylactically.
- Debulking (Charles procedure, suction-assisted lipectomy): Removes fibrofatty tissue in late-stage disease.
Staging uses the ISL (International Society of Lymphology) scale: Stage 0 (subclinical), Stage I (reversible, pitting edema), Stage II (spontaneously irreversible, non-pitting, dermal fibrosis), Stage III (lymphostatic elephantiasis with trophic skin changes).
13 Peripheral Nerve & Brachial Plexus Reconstructive
Plastic surgery peripheral nerve practice includes compression neuropathies (carpal tunnel, cubital tunnel, tarsal tunnel), traumatic nerve lacerations, brachial plexus birth and adult injuries, facial nerve paralysis, and painful neuromas.
Nerve Repair Options
- Primary epineural repair: Best when tension-free coaptation is possible, ideally within 72 hours.
- Autograft: Sural nerve is the workhorse donor (30–40 cm), also medial antebrachial cutaneous.
- Processed allograft (Avance): Decellularized nerve, effective for gaps up to 5 cm.
- Conduit: Bioabsorbable tube (PGA, collagen) for gaps < 3 cm in non-critical sensory nerves.
- Nerve transfer: A healthy, expendable donor nerve is transected and coapted near the target motor endplate. Examples: Oberlin transfer (fascicle of ulnar to musculocutaneous for biceps), double fascicular transfer, SAN to suprascapular, AIN to ulnar motor.
Facial Reanimation
For facial paralysis, timing matters: within 12 months, nerve transfers (masseter to facial, cross-facial nerve grafting) can reinnervate existing muscle. Beyond 18–24 months, the muscle fibrosis, and dynamic reanimation requires free functional gracilis muscle transfer — typically a two-stage approach with a cross-facial sural nerve graft followed by gracilis transfer 9–12 months later, or a single-stage gracilis powered by the masseteric nerve (V3). Static procedures (fascia lata sling, tendon transfers) restore resting symmetry.
Brachial Plexus
Adult brachial plexus injuries (motorcycle accidents) present with flail arm or partial deficits; infant plexus injuries (shoulder dystocia) include Erb's palsy (C5-6, "waiter's tip"), Klumpke's palsy (C8-T1, claw hand), and total plexus injury with Horner syndrome (preganglionic rupture). Early nerve grafting and transfers give the best functional recovery.
14 Pressure Injuries & Chronic Wounds Wounds
Pressure injuries (formerly "pressure ulcers" or "decubiti") occur when prolonged pressure over bony prominences exceeds capillary closing pressure and causes ischemic soft-tissue necrosis. Common locations: sacrum, ischial tuberosity, greater trochanter, heel, occiput.
| Stage | Description |
|---|---|
| Stage 1 | Intact skin with non-blanchable erythema |
| Stage 2 | Partial thickness loss of dermis — shallow open ulcer or blister |
| Stage 3 | Full thickness loss; subcutaneous fat visible; no exposed bone/tendon/muscle |
| Stage 4 | Full thickness with exposed bone, tendon, or muscle |
| Unstageable | Full thickness covered by slough or eschar |
| Deep tissue injury | Intact or non-intact skin with localized area of persistent non-blanchable maroon/purple discoloration |
Reconstruction of stage 3-4 pressure injuries includes aggressive debridement, ostectomy (removal of the prominent bone), and flap coverage. Options include gluteal rotation/advancement flaps, superior/inferior gluteal artery perforator flaps, posterior thigh flap, tensor fascia lata (TFL) flap, and vertical rectus abdominis myocutaneous (VRAM). Offloading, nutrition, and spasm control (for SCI patients) are critical for durable closure.
15 Gender-Affirming Surgery Gender
Gender-affirming surgery (GAS) is a growing subspecialty. Patients are evaluated per WPATH standards of care with mental health and hormone therapy criteria met before surgery.
Top Surgery
- Masculinizing chest (female-to-male): Double incision mastectomy with free nipple graft (larger breasts), periareolar ("keyhole") or circumareolar for smaller breasts. Concealed mastectomy scars follow the inframammary fold.
- Feminizing chest (male-to-female): Breast augmentation with implants (typically subglandular or prepectoral), often after hormone-induced breast development.
Bottom Surgery
- Vaginoplasty (male-to-female): Penile inversion (most common), with or without scrotal skin graft; intestinal (sigmoid) vaginoplasty for re-do or insufficient tissue; peritoneal vaginoplasty.
- Phalloplasty (female-to-male): Radial forearm free flap (sensation, reliable urethra), anterolateral thigh (ALT) pedicled or free, latissimus. Staged: phallus creation, urethral lengthening, glans sculpting, erectile and testicular implants.
- Metoidioplasty: Uses the hormonally hypertrophied clitoris as the neophallus.
Facial Feminization / Masculinization
Facial feminization (FFS) includes frontal bone contouring/reduction, brow lift, rhinoplasty, upper lip lift, genioplasty, mandibular angle reduction, thyroid cartilage ("tracheal shave") reduction, and hairline lowering. Facial masculinization may include chin and jaw augmentation and forehead augmentation.
16 Aesthetic Surgery — Face Aesthetic
Aesthetic (cosmetic) surgery makes up a large portion of many plastic surgery practices. Consultations focus on the patient's goals, realistic expectations, surgical risk, and recovery planning.
Facial Rejuvenation Procedures
- Rhytidectomy (facelift): Various techniques — SMAS plication, SMASectomy, deep plane, extended deep plane, high SMAS. Incisions run in the temporal hair, preauricular/tragal, around the earlobe, and into the occipital scalp.
- Neck lift / platysmaplasty: Addresses platysmal banding and submental fat. Often combined with facelift.
- Blepharoplasty: Upper (skin excision +/- orbicularis and fat), lower (transconjunctival with fat repositioning, or transcutaneous with skin-muscle flap).
- Brow lift: Direct, mid-forehead, pretrichial, coronal, endoscopic, or temporal. AAFPRS publishes aesthetic outcome data.
- Rhinoplasty: Open (transcolumellar incision) or closed (endonasal). Components include dorsal hump reduction, osteotomies, tip refinement (cephalic trim, tip sutures, grafts), and alar base modification. Functional rhinoplasty addresses septal deviation, turbinate hypertrophy, internal valve collapse (spreader grafts), and external valve collapse.
- Otoplasty: For prominent ears — Mustarde sutures create an antihelical fold, Furnas sutures set back the conchal bowl.
- Genioplasty: Sliding osseous or alloplastic implant.
- Fat grafting (lipofilling): Autologous fat harvested by liposuction, centrifuged or decanted, and injected into hollow areas (temples, tear troughs, cheeks, lips, nasolabial folds, jawline).
Non-Surgical Aesthetics
- Neurotoxins: Botulinum toxin A (Botox, Dysport, Xeomin, Jeuveau, Daxxify) for dynamic rhytids — glabella, forehead, crow's feet, masseter hypertrophy, platysmal bands, gummy smile.
- Fillers: Hyaluronic acid (Juvederm, Restylane, Belotero, RHA family), calcium hydroxylapatite (Radiesse), poly-L-lactic acid (Sculptra), PMMA (Bellafill). Hyaluronidase reverses HA fillers in case of vascular occlusion.
- Chemical peels: Glycolic, TCA (10–35%), phenol-croton oil (deep).
- Lasers: Ablative (CO2, erbium:YAG), non-ablative (fractional), vascular (pulsed dye), pigmentary (Q-switched, picosecond).
- Energy-based devices: Radiofrequency microneedling, ultrasound (Ultherapy).
Filler and neurotoxin charting should include: product name/brand, lot number, expiration, total volume/units, specific anatomic sites with amounts, technique (cannula vs needle, plane), and any complications. This is required for both safety and medicolegal documentation.
17 Aesthetic Surgery — Breast & Body Aesthetic
Breast Aesthetic Surgery
- Augmentation mammaplasty: Saline or silicone implants (smooth round, form-stable "gummy bear"), placed subglandular, subfascial, subpectoral (dual plane), or prepectoral. Incisions: inframammary fold (most common), periareolar, transaxillary, transumbilical (saline only).
- Implant exchange / explantation: For capsular contracture (Baker grades), rupture, size change, or BIA-ALCL concern with textured implants. FDA/ASPS BIA-ALCL guidance.
- Mastopexy (breast lift): Crescent, periareolar, vertical (lollipop), inverted-T (Wise pattern, anchor). Chosen by degree of ptosis using the Regnault classification (grades I–III plus pseudoptosis).
- Reduction mammaplasty: Inferior pedicle with Wise pattern, superomedial pedicle with vertical scar, free nipple graft (massive gigantomastia). Documented for pain relief (neck/back/shoulder, grooving from bra straps, intertrigo).
Body Contouring
- Abdominoplasty (tummy tuck): Full, mini, extended, fleur-de-lis. Includes rectus diastasis plication, umbilical transposition, and low transverse scar.
- Liposuction: Suction-assisted (SAL), power-assisted (PAL), ultrasound-assisted (UAL, VASER), laser-assisted (LAL).
- Brazilian butt lift (BBL) / gluteal fat grafting: Subcutaneous-only injection (never intramuscular) to avoid fat embolism, per ASPS/ASAPS safety advisory.
- Body contouring after massive weight loss: Lower body lift (belt lipectomy), upper body lift, brachioplasty (arm lift), medial thigh lift, bra-line back lift.
18 Flaps, Grafts & Reconstructive Ladder Procedural
The reconstructive ladder guides the choice of wound coverage from simplest to most complex:

- Healing by secondary intention
- Primary closure
- Delayed primary closure
- Skin graft (STSG or FTSG)
- Tissue expansion
- Random local flap
- Axial / regional pedicled flap
- Free tissue transfer (microsurgery)
Skin Grafts

- Split-thickness skin graft (STSG): 0.010–0.018 inch, harvested with a dermatome from thigh, buttock, scalp, or back. Meshed (1:1.5, 1:3, 1:6) to increase coverage area and allow drainage. Donor site re-epithelializes from remaining adnexa in 10–14 days.
- Full-thickness skin graft (FTSG): Includes entire dermis. Donor sites include postauricular, supraclavicular, upper eyelid, groin, antecubital. Better color match and less contraction but needs a well-vascularized recipient bed.
- Composite graft: Skin + cartilage (e.g., ear helical rim for nasal ala reconstruction).
- Dermal substitutes: Integra (bilayer collagen-GAG with silicone), Alloderm, NovoSorb BTM. Create a neodermis that accepts a thin STSG at a second stage.
Local Flaps
| Flap | Movement | Typical Use |
|---|---|---|
| Advancement | Linear push into defect | Forehead, cheek |
| Rotation | Arc around a pivot point | Cheek, scalp |
| Transposition (rhomboid/Limberg) | Lifts tissue over intervening skin | Cheek, temple, trunk |
| Bilobed | Double transposition | Nasal tip, dorsum |
| Z-plasty | Lengthens along central limb | Scar release, contracture |
| V-Y advancement | Island advancement | Fingertip, lip, heel |
| Rhomboid (Limberg) | 60/120-degree transposition | Sacral, cheek, temple |
Regional & Free Flaps
Workhorse regional pedicled flaps include paramedian forehead flap (nasal reconstruction, supratrochlear artery), nasolabial flap, pectoralis major myocutaneous flap (head and neck salvage), latissimus dorsi (chest, back, head and neck), medial gastrocnemius and soleus (proximal/middle tibia), and gracilis.
Workhorse free flaps: DIEP (breast), ALT (head and neck, extremities — true workhorse, based on descending branch of lateral circumflex femoral), radial forearm (head and neck, urethral reconstruction), fibula (mandible, tibia), scapular/parascapular, lateral arm, gracilis (functional muscle, facial reanimation), jejunum (pharyngoesophageal).
| Type | Blood Supply | Example |
|---|---|---|
| I | Single vascular pedicle | Gastrocnemius, tensor fascia lata |
| II | Dominant pedicle + minor pedicle(s) | Gracilis, biceps femoris, trapezius (most common type) |
| III | Two dominant pedicles | Rectus abdominis, gluteus maximus, serratus |
| IV | Segmental pedicles | Sartorius, tibialis anterior (poor flap candidates) |
| V | One dominant + segmental | Latissimus dorsi, pectoralis major |
| Type | Vascular Pattern |
|---|---|
| A | Multiple small fasciocutaneous perforators entering at base |
| B | Single large fasciocutaneous perforator, moderate size |
| C | Multiple perforators along a segmental vessel coursing in intermuscular septum |
| D | Type C + bone and/or muscle (osteomyocutaneous septocutaneous) |
Tissue Expansion
A silicone expander is placed beneath skin and gradually inflated with saline over weeks, stretching the overlying skin. The expanded skin is then rotated or advanced to cover an adjacent defect with like tissue. Common for scalp defects, burn reconstruction, and breast reconstruction.

19 Imaging & Diagnostics Imaging
- CTA abdomen/pelvis: Pre-DIEP perforator mapping — shows DIEA/perforator location, size, intramuscular course.
- CTA lower extremity: Pre-fibula harvest — confirms 3-vessel runoff.
- CT maxillofacial: Facial fracture evaluation. Thin cuts with coronal and sagittal reconstructions.
- CT chest/abdomen/pelvis with contrast: Oncologic staging.
- MRI breast: Used for extent of disease in breast cancer; implant integrity (silent rupture).
- MRI brachial plexus: Nerve injury evaluation.
- ICG (indocyanine green) angiography: Intraoperative real-time perfusion assessment of mastectomy skin flaps, perforator flaps, and bowel.
- Duplex ultrasound: Perforator mapping (handheld or imaging duplex), vessel patency assessment.
- Implantable Doppler (Cook-Swartz): Continuous post-op monitoring of microsurgical flaps.
- EMG / nerve conduction studies: Nerve injury workup — timing sensitive (may need 3 weeks for Wallerian degeneration to become visible).
20 Medications You Must Know Medications
Perioperative Antibiotics
- Cefazolin (Ancef) 2 g IV pre-op (3 g if > 120 kg) — standard for clean plastic cases.
- Clindamycin 900 mg IV — penicillin/cephalosporin allergy.
- Ampicillin-sulbactam (Unasyn) 3 g IV — head and neck contaminated cases.
- Amoxicillin-clavulanate (Augmentin) 875/125 mg PO BID — dog and human bite prophylaxis.
- Mupirocin (Bactroban) — topical MRSA decolonization and wound antimicrobial.
- Silver sulfadiazine (Silvadene) — topical burn antimicrobial; avoided on face and near mucosa.
- Bacitracin / petrolatum — standard post-op wound ointment.
Pain Management (Multimodal / Opioid Sparing)
- Acetaminophen IV or PO 1 g q6h scheduled.
- Celecoxib (Celebrex) 200 mg PO (pre-op and post-op) — opioid-sparing.
- Gabapentin / pregabalin — pre-op for neuropathic pain prevention.
- Liposomal bupivacaine (Exparel) — long-acting local anesthetic for surgical sites.
- Ketorolac (Toradol) — avoided in free flap cases by some surgeons (bleeding risk).
- Oxycodone 5 mg PO q4h PRN for breakthrough.
- Scopolamine patch, ondansetron, dexamethasone for PONV.
VTE Prophylaxis
VTE risk is stratified by the Caprini score (see classification section). Low-risk: early ambulation and SCDs. Moderate-to-high risk: enoxaparin 40 mg SC daily (or 30 mg BID) beginning 6–12 hours post-op. Extended prophylaxis may be used after body contouring or oncologic resection. CHEST VTE prophylaxis guidance is the reference.
Microsurgery-Specific Medications
- Aspirin 81 mg PO daily — initiated post-op in many programs for flap patency (controversial but common).
- Heparin — intraoperative irrigation, systemic low-dose, or therapeutic dosing in some protocols.
- Dextran 40 — historically used for flap rheology; largely abandoned due to pulmonary and cardiac complications.
- Heparin flush — irrigation of vessels during anastomosis.
Scar Management
- Silicone sheets / gel — first-line scar therapy 23 hours/day for 3+ months.
- Intralesional triamcinolone (Kenalog) 10–40 mg/mL — keloids and hypertrophic scars.
- 5-Fluorouracil (5-FU) intralesional — adjunct for keloids, often combined with triamcinolone.
- Pressure garments — post-burn scar management.
Other
- Chlorhexidine gluconate (Hibiclens) — surgical skin prep; avoid near eyes and middle ear.
- Povidone-iodine (Betadine) — alternative prep; used for face and mucosa.
- Lanolin / nipple cream — post-mastectomy nipple-sparing reconstruction.
- Botulinum toxin A (Botox, Dysport, Xeomin, Jeuveau, Daxxify) — dosing in units per muscle group.
- Hyaluronidase (Vitrase, Hylenex) — emergency reversal of HA filler vascular occlusion.
21 Classification Systems Reference
Caprini VTE Risk Score (Abbreviated)
| Score | Risk | Recommendation |
|---|---|---|
| 0 | Very low | Early ambulation |
| 1–2 | Low | Mechanical (SCDs) |
| 3–4 | Moderate | Mechanical + chemical (LMWH) |
| 5–8 | High | Mechanical + chemical, consider extended |
| ≥ 9 | Very high (superhigh) | Extended chemoprophylaxis 7–14+ days |
Points come from age, BMI, cancer, prior VTE, central line, OR time, immobility, oral contraceptives/HRT, thrombophilia, etc.
ASA Physical Status
| ASA Class | Description |
|---|---|
| ASA I | Normal healthy patient |
| ASA II | Mild systemic disease (controlled HTN, obesity, smoker) |
| ASA III | Severe systemic disease (poorly controlled DM, COPD) |
| ASA IV | Severe disease that is a constant threat to life |
| ASA V | Moribund, not expected to survive without operation |
| ASA VI | Brain-dead organ donor |
| E suffix | Emergency surgery |
Baker Capsular Contracture
| Grade | Description |
|---|---|
| I | Soft, natural appearance |
| II | Minimal firmness, normal appearance |
| III | Moderate firmness, visible distortion |
| IV | Severe firmness, painful, distorted |
Regnault Ptosis Grade
- Grade I (mild): Nipple at IMF, above lower breast contour
- Grade II (moderate): Nipple below IMF, above most dependent portion of breast
- Grade III (severe): Nipple below IMF and at most dependent portion, pointing downward
- Pseudoptosis: Inferior glandular descent with nipple above IMF
Fitzpatrick Skin Type
| Type | Skin | Sun Response |
|---|---|---|
| I | Very pale | Always burns, never tans |
| II | Pale | Usually burns, tans minimally |
| III | Light brown | Sometimes burns, tans uniformly |
| IV | Moderate brown | Burns minimally, always tans well |
| V | Dark brown | Very rarely burns, tans profusely |
| VI | Deeply pigmented | Never burns, deeply pigmented |
Tessier Rare Facial Clefts
Numbered 0–14, with facial (0–7) and cranial (8–14) clefts. Pairs sum to 14 lying along a continuous axis (e.g., cleft 0 corresponds to cleft 14, cleft 3 to cleft 11). Clinically important examples: 0/14 midline; 3 oral-nasal-ocular; 7 lateral commissural macrostomia (hemifacial microsomia); 30 midline lower lip/mandibular cleft (a non-Tessier entity but referenced in the same conversations).
22 Physical Exam & Flap Monitoring Exam
The Plastic Surgery Exam
The exam varies enormously by encounter but always includes focused inspection and palpation of the affected area. Document dimensions, tissue quality, scar maturity, and functional status.
Flap: pink, warm, soft
Capillary refill: brisk (< 2 sec)
Doppler: audible arterial and venous signals over skin paddle
Pinprick: brisk bright red bleeding
Donor site: clean, dry, intact
Drains: JP x2 — serosanguineous output 30 mL / 25 mL overnight
No hematoma, seroma, dehiscence, or signs of infection
Signs of Flap Compromise
| Finding | Arterial Insufficiency | Venous Congestion |
|---|---|---|
| Color | Pale, white | Dusky, blue, purple |
| Capillary refill | Sluggish or absent | Brisk (< 1 sec, "flash") |
| Temperature | Cool | Normal or warm |
| Turgor | Soft, flat | Tense, swollen |
| Pinprick bleeding | Sluggish dark or absent | Immediate dark blood |
| Doppler | Lost arterial signal | Lost venous signal, arterial may persist |
Flap compromise in the first 24–48 hours is an emergency — the surgeon will return to the OR to explore and revise the anastomosis. Salvage rates drop with time. Document findings every hour in the first 24 hours per program protocol.
Breast Exam
Inspection (symmetry, contour, skin, nipple position), palpation of breast parenchyma, axillary and supraclavicular nodes, implant palpation (capsule, rippling, malposition), and nipple-areola sensation.
Hand Exam
Inspection (swelling, deformity, wounds), range of motion (active and passive at each joint), strength (grip dynamometer, pinch), sensation (two-point discrimination, monofilament), vascular (Allen test, capillary refill, Doppler), and provocative tests (Tinel, Phalen, Finkelstein).
23 Abbreviations Master List Reference
Anatomy
Diagnoses & Conditions
Procedures
Medications & Monitoring
24 Sample HPI Templates Reference
These templates show the rhythm and content of a good plastic surgery clinic note. Use them as frameworks during your first week.
"Ms. [Name] is a 52-year-old premenopausal female with newly diagnosed left breast invasive ductal carcinoma (cT2N0, ER+/PR+/HER2-, grade 2) presenting for delayed breast reconstruction consultation. She completed a left skin-sparing mastectomy with SLNB (0/3 nodes positive) 6 weeks ago by Dr. [Surgeon]. She does not require radiation. She is interested in autologous reconstruction and has reviewed options with her oncologist. BMI 26. She has had two prior C-sections (low transverse). No prior abdominal surgery otherwise. Never-smoker. No diabetes. On exam, the left mastectomy flap is healed, soft, without tenderness. Abdomen has adequate tissue for a DIEP flap with two palpable periumbilical perforators on Doppler. Pannus is mild. We discussed DIEP, PAP, implant-based reconstruction, and the risks/benefits of each. She is interested in proceeding with delayed DIEP reconstruction."
"Mr. [Name] is a 34-year-old male with no significant PMH who presents for reconstruction of a Gustilo IIIB open left tibia fracture sustained in a motorcycle collision 5 days ago. He underwent I&D, external fixation, and VAC placement by orthopedic surgery on day of injury, with repeat I&D on hospital day 2 and 4. The wound is a 12 × 6 cm defect over the middle third of the tibia with exposed periosteum-stripped bone and no viable muscle coverage. Cultures from the last debridement are pending. He is non-smoker, healthy, with no diabetes. CTA runoff demonstrates three-vessel patency. On exam, the wound bed is clean without purulence, pedal pulses 2+ DP/PT, sensation intact. We discussed a free gracilis muscle flap with skin graft vs ALT free flap for soft tissue coverage, and plan to proceed after one more washout tomorrow."
"Ms. [Name] is a 6-year-old female brought to the ED by her mother after being bitten in the face by a family dog (vaccinated, indoor, no prior aggressive behavior) approximately 90 minutes ago. On examination, there is a 3.5 cm stellate laceration of the left upper lip crossing the vermillion border and a 2 cm laceration of the left cheek. No intraoral component. Facial nerve function intact (she can smile and close her eye). No parotid duct involvement by inspection. No bony step-off. Tetanus is up to date. We discussed the risks and benefits of bedside vs operating room repair given her age and cooperation; given the complexity of the lip repair and the need for precise vermillion alignment, we recommend repair under general anesthesia in the OR. Started on amoxicillin-clavulanate."
"Ms. [Name] is a 28-year-old G0 female presenting for breast augmentation consultation. She describes lifelong small breast size (current 34A) and desires a fuller, more proportionate appearance, goal size full B to small C. She denies pregnancy plans within the next 1–2 years and is not currently breastfeeding. No personal or family history of breast cancer. BMI 22. Non-smoker. No prior breast surgery. On exam, symmetric small breasts, nipple position at IMF, minimal ptosis (pseudoptosis), adequate skin envelope, nipple-to-IMF distance 6 cm bilaterally. We reviewed silicone vs saline implants, round vs shaped, subglandular vs dual-plane pocket, inframammary vs periareolar incision, and the BIA-ALCL risk with textured devices. She is interested in smooth round silicone implants in the 300–350 cc range via IMF incision, dual-plane pocket."
"Mr. [Name] is a 42-year-old male status post 35% TBSA flame burn 14 months ago (acute care at regional burn center, multiple excisions and STSG), presenting for reconstruction of post-burn axillary contracture limiting right shoulder abduction to 80 degrees and interfering with activities of daily living. On exam, he has mature hypertrophic scars across the right axilla, anterior chest, and upper arm with a well-defined contracture band. Skin elsewhere is supple. Range of motion limited as above. We discussed scar contracture release with Z-plasty vs full-thickness skin graft vs regional/free flap reconstruction. Plan: OR for release with multiple Z-plasties and possible FTSG from groin, followed by aggressive scar management with silicone, pressure garments, and hand/occupational therapy."
"Mr. [Name] is a 41-year-old right-handed male carpenter presenting with a 2 cm volar laceration at the base of the right ring finger after a table saw injury 3 hours ago. He reports inability to bend the fingertip. On exam, there is a clean transverse laceration in Zone II over the A1 pulley area. He cannot actively flex the DIP joint against resistance (absent FDP function) but can flex the PIP (intact FDS). Digital nerves intact by two-point discrimination < 5 mm, Doppler signals present over both digital arteries. Tetanus up to date. Plan: operative exploration and primary repair of the FDP tendon with 4-strand core suture plus running epitendinous, with early active motion protocol post-op. Cefazolin prophylaxis administered."
25 References & Sources
Clinical Practice Guidelines
NCCN Guidelines: Squamous Cell Skin Cancer & Basal Cell Skin Cancer. JNCCN.
NCCN Guidelines: Cutaneous Melanoma. JNCCN.
NCCN Guidelines: Breast Cancer. JNCCN.
ACS NCDB analysis of breast reconstruction trends and outcomes. Ann Surg Oncol.
American Burn Association (ABA) burn resuscitation guidelines. J Burn Care Res.
IWGDF Guidelines on the prevention and management of diabetic foot disease.
CHEST Antithrombotic Therapy and Prevention of Thrombosis, 9th edition.
AAFPRS membership survey of facial plastic surgery outcomes and trends.
FDA / ASPS guidance on breast implant-associated ALCL (BIA-ALCL).
Landmark Concepts & Classifications
Gustilo RB, Anderson JT. Prevention of infection in the treatment of open fractures. J Bone Joint Surg Am. 1976.
Mathes SJ, Nahai F. Classification of the vascular anatomy of muscles. Plast Reconstr Surg. 1981.
Cormack GC, Lamberty BG. A classification of fascio-cutaneous flaps according to their patterns of vascularisation. Br J Plast Surg. 1984.
Tessier P. Anatomical classification of facial, craniofacial and laterofacial clefts. J Maxillofac Surg. 1976.
Caprini JA. Thrombosis risk assessment as a guide to quality patient care. Dis Mon. 2005.
Holcomb JB et al. Parkland formula and burn resuscitation. J Trauma.
Diagram & Figure Sources
Figure 1: Structure of the skin. OpenStax College. CC BY 3.0.
Figure 2: Skin Anatomy. Blausen Medical. CC BY 3.0.
Figure 3: DIEP flap breast reconstruction diagram. Wikimedia Commons.
Figure 4: Wallace Rule of Nines. Wikimedia Commons. Public domain.
Figure 5: Cleft lip and palate clinical image. Wikimedia Commons. Public domain.
Plastic surgery scribes cover a wider clinical range than almost any other specialty — one morning you are documenting a complex microsurgical breast reconstruction, the afternoon a facelift consult, the next day a pediatric cleft lip repair or a dog bite in the ED. The best scribes master the vocabulary of each subdomain and know the reconstructive ladder cold. When the surgeon says "we'll need an ALT for that middle-third tibial wound," you should immediately understand the anatomy, pedicle, and post-op monitoring expectations.
Learn flap monitoring language early — color, capillary refill, Doppler, pinprick — because you will document it literally every hour on inpatient services. Know the difference between arterial and venous compromise. Pre-populate op notes with the flap name, pedicle, recipient vessels, ischemia time, and coupler size so the surgeon just fills in the specifics. Memorize the standard antibiotic and VTE prophylaxis protocols. Always document smoking status.
Welcome to plastic surgery. Master the technique names and the vocabulary, and you will become indispensable in clinic and the OR.