PM&R
Every diagnosis, procedure, medication, classification, abbreviation, and documentation framework you need to succeed as a physiatry scribe on day one and beyond.
All diagrams on this page are sourced from published educational or institutional materials rather than AI generation. Each figure caption links to the original source, and the full diagram and guideline citations are collected in the references section at the bottom.
01 Rehabilitation Medicine — Scope & Anatomy Essentials
Physical Medicine & Rehabilitation (PM&R), also called physiatry, is the medical specialty focused on restoring function after illness or injury. While most specialties ask "what is the disease?", physiatrists ask "what can this patient do, and how do we get them doing more?" The unit of analysis is not the organ but the activity — walking, dressing, transferring, swallowing, communicating, returning to work. A scribe in a PM&R clinic or inpatient rehabilitation unit must learn to chart function alongside pathology.
Physiatrists work across a spectrum of settings: acute inpatient rehabilitation facilities (IRFs), long-term acute care (LTACH), skilled nursing facilities (SNF), outpatient rehabilitation clinics, electrodiagnostic labs, interventional spine clinics, and sports medicine practices. Subspecialties include spinal cord injury medicine, brain injury medicine, pediatric rehab, sports medicine, pain medicine, neuromuscular medicine, and cancer rehabilitation.
Neuroanatomy Essentials
Every physiatrist uses neuroanatomy daily. You need a working knowledge of the motor cortex (precentral gyrus — the homunculus), the corticospinal tract (descending motor pathway that decussates at the medullary pyramids), the dorsal column-medial lemniscus pathway (vibration, proprioception, fine touch), the spinothalamic tract (pain and temperature, crosses within 1–2 levels of entry), the cerebellum (coordination, balance), the basal ganglia (movement initiation, tone), and the brainstem (cranial nerves, consciousness, cardiorespiratory control).
The spinal cord extends from the foramen magnum to approximately L1–L2, where it ends at the conus medullaris. Below the conus, the lumbosacral nerve roots form the cauda equina. Each spinal segment has a corresponding dermatome (sensory) and myotome (motor). Landmarks scribes must memorize: C4 — shoulder top; C6 — thumb; C7 — middle finger; C8 — small finger; T4 — nipple line; T10 — umbilicus; L1 — inguinal crease; L4 — medial malleolus/knee extension; L5 — dorsum of foot/great toe extension; S1 — lateral foot/plantarflexion; S4–S5 — perianal sensation.
Musculoskeletal Essentials
MSK rehab requires fluency in joint structure and the muscles driving each joint. The shoulder is a ball-and-socket joint stabilized by the rotator cuff (supraspinatus, infraspinatus, teres minor, subscapularis — "SITS"). The hip is a deep ball-and-socket joint with powerful flexors (iliopsoas), extensors (gluteus maximus, hamstrings), abductors (gluteus medius), and adductors. The knee is a hinge joint stabilized by four ligaments (ACL, PCL, MCL, LCL) and two menisci. The spine is composed of 33 vertebrae (7 cervical, 12 thoracic, 5 lumbar, 5 fused sacral, 4 fused coccygeal) with intervertebral discs consisting of an outer annulus fibrosus and inner nucleus pulposus.
PM&R notes constantly mix anatomy with function. When the physiatrist says "C6 motor-incomplete tetraplegia, AIS C, with preserved wrist extension," you must chart both the anatomic level (C6) and the functional impairment (motor-incomplete, partial preservation). Never write "paralysis" without specifying level, completeness, and what the patient can still do.
02 Scribe Documentation Framework (Function-Focused)
PM&R notes look similar to other specialty notes on the surface but have a distinctive functional layer baked into every section. Whereas a hospitalist might write "weakness, ambulating with assistance," a physiatrist will document exactly which muscles are weak (MRC grade), the assistive device used, the level of assist required, and the distance walked in feet. Quantification is everything.
Chief Complaint: A functional goal as often as a symptom — "difficulty transferring," "worsening gait," "low back pain limiting work," "evaluation for acute rehab."
HPI: Use OLDCARTS for pain complaints, but always add a functional history: What could the patient do before the injury or illness? What can they do now? Specifically, document prior and current levels of independence in mobility (bed mobility, transfers, ambulation, wheelchair propulsion, stairs) and activities of daily living (ADLs: bathing, dressing, grooming, toileting, feeding). Document living situation (stairs at home? caregiver support? single level?). Document prior therapies attended, home exercise program compliance, and any assistive devices currently used.
ROS: Focused on neuro, MSK, and rehab complications — bowel/bladder function (continence, retention, constipation), sleep, fatigue, mood, cognition, dysphagia, falls.
PMHx/PSHx/Meds/Allergies/Social/Family: Document the baseline functional status prior to the index event, prior rehab admissions, equipment at home, driving status, and work/school status.
Vitals: Include orthostatic BP (critical in SCI and deconditioning), resting HR, oxygen saturation on activity.
Exam: Mental status, cranial nerves, motor (MRC 0–5), sensory (light touch, pinprick, proprioception by dermatome), tone (Modified Ashworth), deep tendon reflexes, coordination, gait description with assistive device and level of assist, and functional testing (sit-to-stand, Timed Up and Go, Berg Balance if performed).
Results: EMG/NCS findings, imaging, labs, therapy progress notes (PT, OT, SLP notes are part of the chart and should be synthesized).
A PM&R plan is organized around problems (diagnoses + impairments) linked to goals. Each problem lists therapy frequency ("PT 5x/week, OT 5x/week, SLP 3x/week"), equipment ordered, medication changes, pending consults, and discharge planning status (anticipated disposition, durable medical equipment, home modifications needed).
Always capture level-of-assist language precisely: Independent, Modified Independent (uses a device but no help), Supervision, Contact Guard Assist (CGA), Minimum Assist (<25% help), Moderate Assist (25–50%), Maximum Assist (50–75%), Total/Dependent. These terms drive FIM scoring and IRF admission decisions.
03 Stroke Rehabilitation Neuro Rehab
Stroke is the most common diagnosis on an acute inpatient rehab unit. Rehabilitation begins within 24–48 hours of medical stability. The physiatrist inherits a patient from neurology or neurosurgery and must now translate the acute infarct or hemorrhage into a functional recovery plan.
Pathophysiology & Presentation
Ischemic strokes (87%) result from thromboembolic occlusion; hemorrhagic strokes (13%) from intraparenchymal bleeding. Clinical syndromes depend on vascular territory: MCA — contralateral face/arm weakness > leg, aphasia (dominant) or neglect (non-dominant); ACA — contralateral leg > arm weakness, abulia; PCA — contralateral homonymous hemianopia, memory loss; lacunar — pure motor, pure sensory, ataxic hemiparesis, or dysarthria-clumsy hand; brainstem — crossed deficits, cranial nerve palsies, vertigo, dysphagia.
Rehabilitation Approach
Recovery follows Brunnstrom stages of motor recovery (see Classifications section). Management emphasizes early mobilization, task-specific training, constraint-induced movement therapy (CIMT) for eligible upper-limb patients, mirror therapy, functional electrical stimulation (FES), gait training with body-weight support treadmill or robotic assistance, and intensive speech therapy for aphasia and dysarthria. Secondary prevention is critical: antiplatelet or anticoagulation (based on etiology), statin, BP control, diabetes control, and lifestyle modification. The AHA/ASA Guidelines for Adult Stroke Rehabilitation and Recovery recommend comprehensive, interdisciplinary rehabilitation in a stroke-specialized setting whenever feasible.
New or worsening focal deficit (recurrent stroke, hemorrhagic conversion), sudden headache, seizure, new-onset atrial fibrillation, DVT, aspiration pneumonia, urinary retention, and post-stroke depression. Document any change and notify the team immediately.
Common Impairments Documented
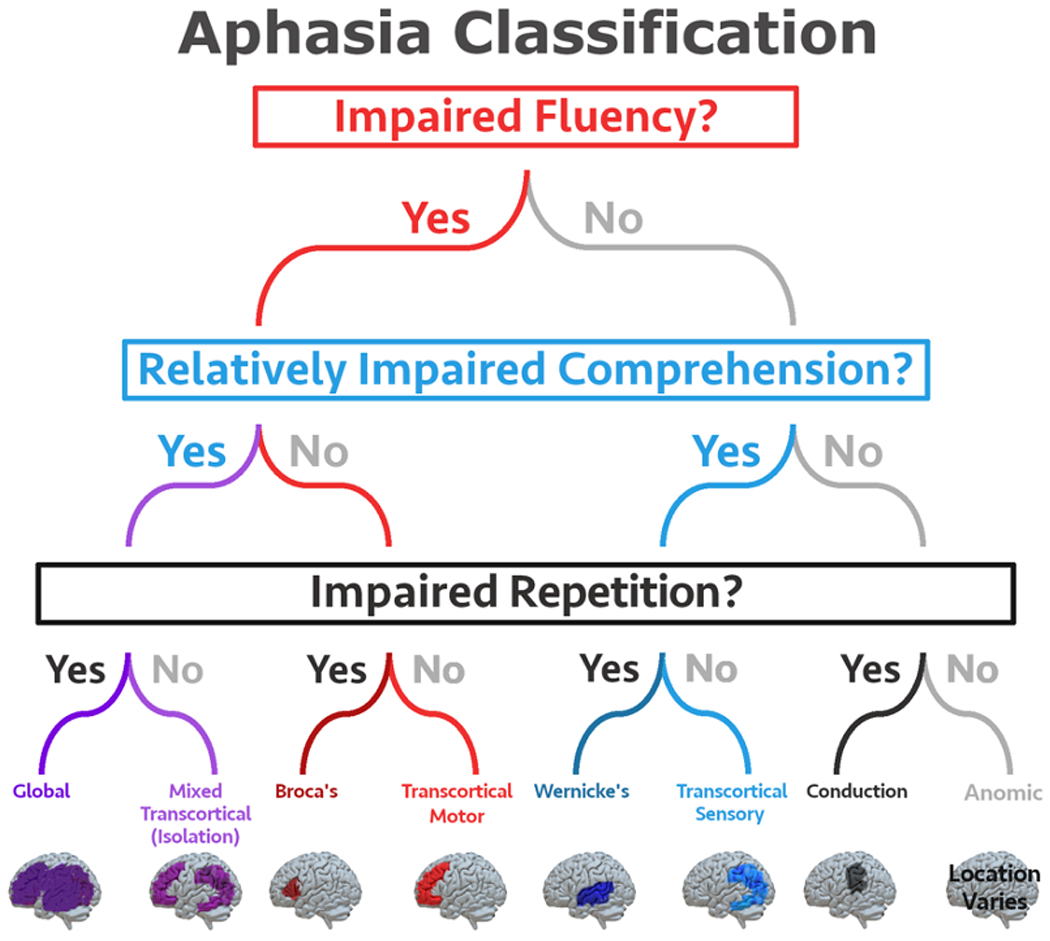
Hemiparesis/hemiplegia, spasticity (especially UE flexor, LE extensor pattern), aphasia (Broca expressive, Wernicke receptive, global, conduction), dysarthria, apraxia, dysphagia, hemineglect, hemianopia, shoulder subluxation, central post-stroke pain, pseudobulbar affect, cognitive impairment, urinary incontinence, and depression. Each is an individual problem with its own interdisciplinary plan.
04 Spinal Cord Injury (SCI) Rehabilitation Neuro Rehab
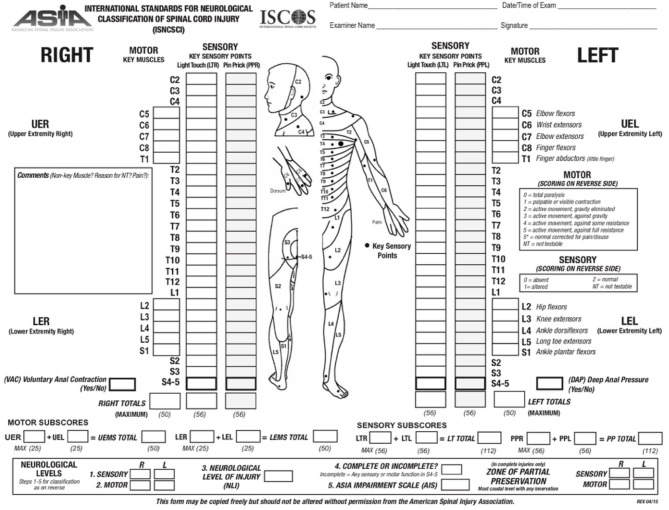
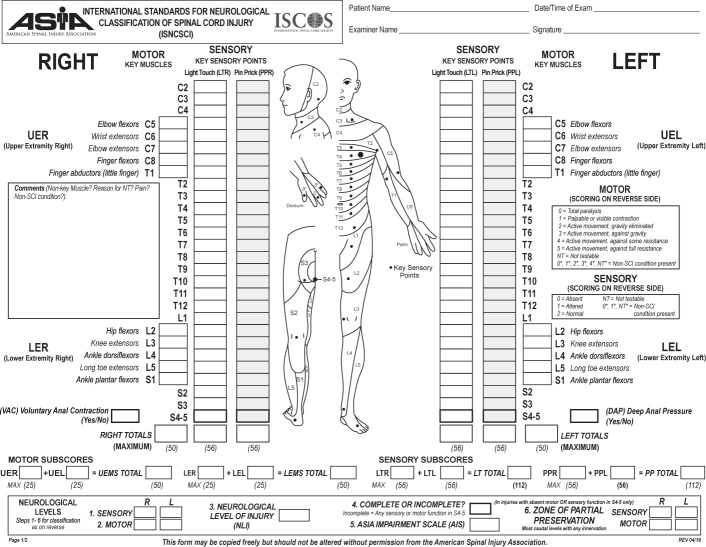
SCI is classified by level (the most caudal segment with normal motor and sensory function bilaterally) and by completeness, using the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) maintained by ASIA/ISCoS. Tetraplegia (formerly quadriplegia) refers to injury at C1–T1 affecting all four limbs. Paraplegia refers to injury at T2 and below affecting lower limbs and potentially trunk.
| Grade | Definition |
|---|---|
| A — Complete | No motor or sensory function preserved in S4–S5 sacral segments. |
| B — Sensory Incomplete | Sensory but no motor function preserved below neurologic level, including sacral S4–S5; no motor more than 3 levels below motor level. |
| C — Motor Incomplete | Motor preserved below level, more than half of key muscles below level have MRC < 3. |
| D — Motor Incomplete | Motor preserved below level, at least half of key muscles below level have MRC ≥ 3. |
| E — Normal | Sensation and motor function normal in all segments, patient had prior deficits. |
Incomplete Cord Syndromes
Central Cord Syndrome: The most common incomplete SCI, typically from cervical hyperextension in an elderly patient with preexisting spondylosis. Upper extremity weakness > lower extremity weakness, variable sensory loss, bladder dysfunction.
Anterior Cord Syndrome: Infarction of anterior spinal artery. Loss of motor, pain, and temperature below level; preserved dorsal column (vibration, proprioception). Poor prognosis for recovery.
Brown-Séquard Syndrome: Cord hemisection (usually from penetrating trauma). Ipsilateral motor and dorsal column loss, contralateral pain/temperature loss beginning 1–2 levels below the injury. Best prognosis of the incomplete syndromes.
Posterior Cord Syndrome: Rare. Loss of vibration and proprioception with preserved motor, pain, and temperature.
Conus Medullaris Syndrome: Injury at the conus (~L1–L2). Areflexic bladder/bowel, saddle anesthesia, variable lower extremity weakness; often mixed upper and lower motor neuron findings.
Cauda Equina Syndrome: Injury to lumbosacral nerve roots below the conus. Pure lower motor neuron pattern: flaccid weakness, areflexia, saddle anesthesia, bladder/bowel dysfunction. Surgical emergency.

Functional Outcomes by Level
| Level | Expected Functional Outcome (Complete Injury) |
|---|---|
| C1–C4 | Ventilator dependent (C1–C3) or phrenic preserved; power wheelchair with sip-and-puff or head control; total care for ADLs. |
| C5 | Deltoids, biceps intact. Can feed self with adaptive equipment; power wheelchair; total assist for transfers. |
| C6 | Wrist extension preserved — tenodesis grasp. Independent feeding, grooming, upper body dressing; manual wheelchair possible; assists with transfers. |
| C7–C8 | Triceps (C7) and finger flexors (C8). Independent transfers, dressing, manual wheelchair, driving with adaptive controls. |
| T1–T9 | Full upper extremity function. Independent manual wheelchair, transfers. Standing frame for therapy; ambulation not typically functional. |
| T10–L1 | Trunk control. Ambulation with KAFOs and assistive device for therapy; manual wheelchair for community. |
| L2–S1 | Community ambulation with AFOs and possibly canes. |
SCI Complications to Document
Neurogenic bladder (reflexic vs areflexic), neurogenic bowel, autonomic dysreflexia (T6 or above), orthostatic hypotension, pressure injuries, spasticity, heterotopic ossification, DVT, respiratory compromise, syringomyelia, osteoporosis, and chronic pain. Management per the Consortium for Spinal Cord Medicine Clinical Practice Guidelines.
05 Traumatic Brain Injury (TBI) & Post-Concussion Neuro Rehab
TBI severity is classified by initial Glasgow Coma Scale (GCS), duration of loss of consciousness (LOC), and duration of post-traumatic amnesia (PTA).
| Severity | GCS | LOC | PTA |
|---|---|---|---|
| Mild (concussion) | 13–15 | 0–30 min | < 24 hr |
| Moderate | 9–12 | 30 min – 24 hr | 1–7 days |
| Severe | 3–8 | > 24 hr | > 7 days |
Mechanisms include focal contusion, diffuse axonal injury (DAI — shearing of white matter tracts from rotational forces, often normal CT but visible on MRI), epidural and subdural hematomas, and subarachnoid hemorrhage. Polytrauma patients (often military) have combined TBI, blast injury, orthopedic injuries, and PTSD.
Post-Concussion Syndrome
Persistent headache, dizziness, fatigue, irritability, insomnia, memory and concentration problems after mild TBI. Vestibular therapy, graded return-to-activity, and sleep hygiene are first-line. The Brain Injury Association of America (BIAA) guidelines and Concussion in Sport Group consensus statements guide return-to-play and return-to-learn protocols.
Rancho Los Amigos Scale (Cognitive Recovery)
| Level | Description |
|---|---|
| I | No response; total assistance. |
| II | Generalized response; total assistance. |
| III | Localized response; total assistance. |
| IV | Confused, agitated; maximal assistance. |
| V | Confused, inappropriate, non-agitated; maximal assistance. |
| VI | Confused, appropriate; moderate assistance. |
| VII | Automatic, appropriate; minimal assistance for daily living. |
| VIII | Purposeful, appropriate; stand-by assistance. |
| IX | Purposeful, appropriate; stand-by assist on request. |
| X | Purposeful, appropriate; modified independent. |
Common post-TBI impairments scribed daily include agitation, confusion, memory impairment, executive dysfunction, anosmia, diplopia, spasticity, heterotopic ossification, post-traumatic hydrocephalus, post-traumatic epilepsy, and endocrinopathy (post-traumatic hypopituitarism).
06 Amputee Rehabilitation & Prosthetics MSK Rehab
Amputation is most commonly performed for complications of diabetes and peripheral arterial disease, followed by trauma and malignancy. The physiatrist coordinates pre-prosthetic training, residual limb shaping, prosthetic prescription, and gait training.

Levels & Prosthetic Options
| Level | Name | Prosthetic Features |
|---|---|---|
| Partial foot | Toe, ray, transmetatarsal (TMA), Lisfranc, Chopart | Toe filler, rigid shank, custom shoe insert |
| Ankle | Syme | End-bearing socket, low-profile foot |
| Below knee | Transtibial (BKA) | Patellar-tendon-bearing or total-surface-bearing socket, SACH or energy-storing foot |
| Knee disarticulation | Knee disart | End-bearing, outside hinge knee |
| Above knee | Transfemoral (AKA) | Ischial containment or quadrilateral socket, mechanical or microprocessor knee (C-Leg, Genium) |
| Hip disarticulation / hemipelvectomy | — | Canadian-style socket, endoskeletal components |
| Upper limb | Partial hand, transradial, transhumeral, shoulder disart, forequarter | Body-powered (cable, hook) or myoelectric prosthesis |
Phases of Amputee Rehab
Pre-operative counseling → acute post-op (wound healing, edema control with shrinker or rigid dressing, pain management, phantom limb education) → pre-prosthetic (ROM, strengthening, desensitization, transfer training) → prosthetic training (donning/doffing, weight shifting, gait training) → community reintegration. Phantom limb pain and residual limb pain are managed with desensitization, mirror therapy, gabapentin/pregabalin, TCAs, and sometimes targeted muscle reinnervation (TMR).


07 Neurodegenerative & Neuromuscular Rehab Neuro Rehab
Demyelinating autoimmune disease of CNS. Rehab targets fatigue (amantadine, modafinil), spasticity, gait, bladder dysfunction, and cognitive symptoms. Exercise is safe and beneficial. Disease-modifying therapies managed by neurology (interferons, glatiramer, natalizumab, ocrelizumab, fingolimod, dimethyl fumarate).
Progressive upper and lower motor neuron disease. Rehab focuses on preserving function and quality of life: AFOs for foot drop, AAC devices for speech loss, power wheelchair with tilt/recline, swallowing evaluation and eventual PEG tube, BiPAP for respiratory support. Multidisciplinary clinic is standard of care. Riluzole and edaravone are disease-modifying.
Bradykinesia, resting tremor, rigidity, postural instability. Rehab uses LSVT BIG (amplitude-based PT) and LSVT LOUD (voice therapy), cueing strategies (visual lines on floor, metronome), balance training, and fall prevention. Medications include carbidopa/levodopa, dopamine agonists (pramipexole, ropinirole), MAO-B inhibitors (selegiline, rasagiline), amantadine, and COMT inhibitors (entacapone).
Acute ascending flaccid paralysis, often post-infectious. After IVIG or plasmapheresis, rehab emphasizes gentle ROM, gradual strengthening (avoiding overuse), respiratory therapy, and AFOs for residual foot drop. Recovery can take months to years.
Late-onset weakness, fatigue, and pain 15–40 years after acute polio. Management is energy conservation, pacing, lightweight orthoses, and avoiding overexertion (which can worsen weakness).
Duchenne (most common childhood form, dystrophin mutation), Becker (milder dystrophin variant), myotonic, limb-girdle, FSHD. Rehab includes gentle stretching, avoidance of eccentric overload, orthoses, power mobility, respiratory support, and cardiac monitoring. Corticosteroids (deflazacort, prednisone) slow progression in DMD.

Peripheral neuropathies (diabetic, chemotherapy-induced, idiopathic) are common outpatient referrals; management is symptomatic (gabapentin, pregabalin, duloxetine, TCAs), AFOs for foot drop, and fall prevention.
08 Pediatric Rehabilitation Pediatric Rehab
Pediatric physiatry manages congenital and acquired disability in children. The core diagnoses:
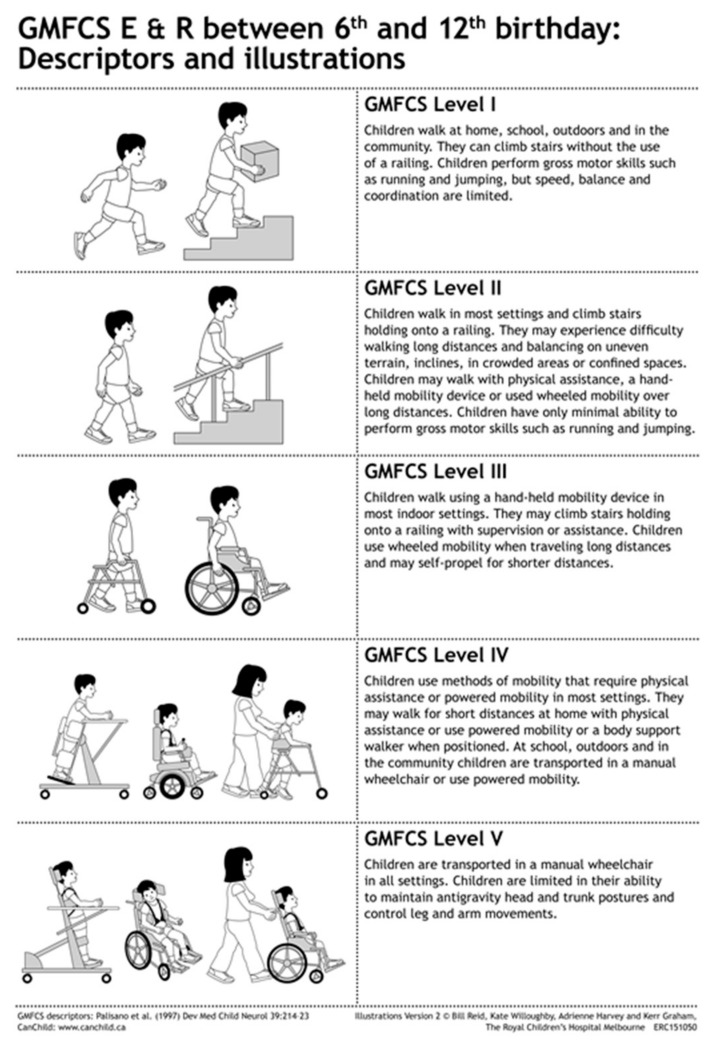
Non-progressive disorder of movement and posture from early brain injury. Subtypes: spastic (diplegic, hemiplegic, quadriplegic), dyskinetic, ataxic, mixed. Gross Motor Function Classification System (GMFCS) levels I–V describe functional mobility. Management: PT, OT, SLP, orthotics (AFOs, KAFOs), oral spasticity meds, botulinum toxin injections, selective dorsal rhizotomy, intrathecal baclofen, and orthopedic interventions (single-event multilevel surgery).
Neural tube defect with exposed spinal cord; functional level determines mobility (thoracic — wheelchair; lumbar — KAFO/HKAFO ambulation; sacral — community ambulation with AFOs). Chronic issues include neurogenic bladder (clean intermittent catheterization), neurogenic bowel, hydrocephalus (VP shunt), tethered cord, Chiari II, latex allergy (high risk), scoliosis, and pressure injury prevention.
Also seen: pediatric TBI, pediatric SCI (often SCIWORA — SCI without radiographic abnormality), brachial plexus birth palsy (Erb-Duchenne C5–C6, Klumpke C8–T1), developmental coordination disorder, and global developmental delay. Early intervention services (0–3 years) and school-based therapy (IEPs/504 plans) are core parts of the plan.
09 Spasticity, Dystonia & Contracture Management Management
Spasticity is velocity-dependent increased muscle tone from upper motor neuron injury (stroke, SCI, TBI, MS, CP). Untreated, it causes pain, contractures, impaired hygiene, and functional loss. Dystonia is involuntary sustained muscle contraction producing abnormal postures. Contracture is fixed shortening of soft tissues across a joint.
| Grade | Description |
|---|---|
| 0 | No increase in tone. |
| 1 | Slight increase; catch and release or minimal resistance at end of ROM. |
| 1+ | Slight increase; catch followed by minimal resistance through less than half of ROM. |
| 2 | Marked increase through most of ROM; affected part easily moved. |
| 3 | Considerable increase; passive movement difficult. |
| 4 | Affected part rigid in flexion or extension. |
The Tardieu Scale complements Ashworth by measuring the angle of catch at different velocities (V1 slow, V2 gravity, V3 fast) and better differentiates spasticity from contracture.
Management Ladder
Stretching, positioning, orthoses, and serial casting are first-line. Oral medications include baclofen, tizanidine, dantrolene, diazepam, and gabapentin. Focal spasticity is treated with botulinum toxin injections (onabotulinumtoxinA/Botox, abobotulinumtoxinA/Dysport, incobotulinumtoxinA/Xeomin, rimabotulinumtoxinB/Myobloc) guided by EMG or ultrasound. Generalized severe spasticity may require intrathecal baclofen (ITB) pump implantation, with scheduled refills every 3–6 months. Phenol and alcohol neurolysis are alternatives. Surgical options include tendon lengthening, selective dorsal rhizotomy, and orthopedic correction of fixed contractures.
10 Musculoskeletal & Spine Disorders MSK Rehab
Low Back Pain
The most common outpatient physiatry complaint. Categories: mechanical/axial (strain, facet arthropathy, discogenic, sacroiliac joint dysfunction), radicular (disc herniation compressing a nerve root — L5 or S1 most common), and specific causes (fracture, infection, malignancy, cauda equina). Red flags: age > 50 or < 20, fever, weight loss, history of cancer, IV drug use, saddle anesthesia, bowel/bladder dysfunction, progressive neurologic deficit. Management follows the ACP guidelines on low back pain — start with non-pharmacologic care (exercise, physical therapy, manipulation, acupuncture, mindfulness), then NSAIDs, then consider muscle relaxants, injections, or referral for surgery.

Cervical Pain
Mechanical neck pain, cervical radiculopathy, cervical myelopathy (UMN signs, gait disturbance, hand clumsiness). Whiplash-associated disorder after MVC. Management: PT, cervical traction, NSAIDs, epidural injections for radiculopathy refractory to conservative care.
Sacroiliac Joint Dysfunction
Pain over the SI joint reproduced by provocative maneuvers (FABER, Gaenslen, thigh thrust, compression, distraction). Treated with PT, SI belt, intra-articular SIJ injection under fluoroscopy.
Shoulder, Hip, and Knee
Shoulder: rotator cuff tendinopathy/tear, subacromial impingement, adhesive capsulitis (frozen shoulder), glenohumeral OA, biceps tendinitis. Hip: OA, greater trochanteric pain syndrome, labral tear, femoroacetabular impingement. Knee: OA, patellofemoral pain, meniscal tear, ACL/PCL/MCL injury, pes anserine bursitis, IT band syndrome. Post-joint replacement rehab (THA, TKA) is a major inpatient and outpatient rehab indication — document precautions (posterior THA: no flexion > 90, no adduction past midline, no internal rotation).
Gait Abnormalities
Antalgic (shortened stance phase on painful side), Trendelenburg (gluteus medius weakness, hip drop), steppage (foot drop — L5 or peroneal), scissoring (bilateral spastic adduction), ataxic (wide-based, unsteady), parkinsonian (shuffling, festination), hemiplegic (circumduction).
11 Chronic Pain, Fibromyalgia, CRPS Pain
Chronic pain is defined as pain lasting > 3 months. PM&R manages it biopsychosocially: exercise, cognitive behavioral therapy, graded activity, pacing, sleep hygiene, mood management, and judicious use of medication and interventional procedures.
Widespread chronic pain with fatigue, non-restorative sleep, cognitive dysfunction ("fibro fog"), and mood symptoms. Diagnosed by the 2016 ACR criteria (Widespread Pain Index + Symptom Severity Scale). Management: aerobic exercise (strongest evidence), CBT, sleep optimization, duloxetine, milnacipran, pregabalin, low-dose amitriptyline. Opioids should be avoided.
Regional pain out of proportion to inciting event, often after distal extremity trauma. Type I (no nerve injury) and Type II (with identifiable nerve injury). Budapest criteria require signs or symptoms in sensory, vasomotor, sudomotor/edema, and motor/trophic categories. Early mobilization, desensitization, mirror therapy, sympathetic blocks (stellate ganglion, lumbar sympathetic), gabapentinoids, bisphosphonates, and spinal cord stimulation in refractory cases.
12 Rehab Complications Complications
A life-threatening reflex in patients with SCI at T6 or above. Noxious stimulus below the injury (most commonly bladder distention or fecal impaction) triggers sympathetic surge causing severe HTN, pounding headache, flushing and sweating above the level, and bradycardia. Management: sit upright, loosen constrictive clothing, identify and remove the trigger (catheterize the bladder first, then check for impaction), and if BP remains > 150 mmHg systolic, administer nitroglycerin paste or nifedipine.
DVT/PE: Immobilized rehab patients are high-risk. Prophylaxis with enoxaparin or UFH during acute rehab phase. Screen clinically, image with duplex for suspicion.
Heterotopic Ossification (HO): Abnormal bone formation in soft tissues, most commonly around hips (SCI) or elbows (TBI). Presents with loss of ROM, warmth, swelling. Diagnosed by alkaline phosphatase elevation and triple-phase bone scan (most sensitive early). Treatment: NSAIDs, etidronate, radiation, surgical excision when mature.
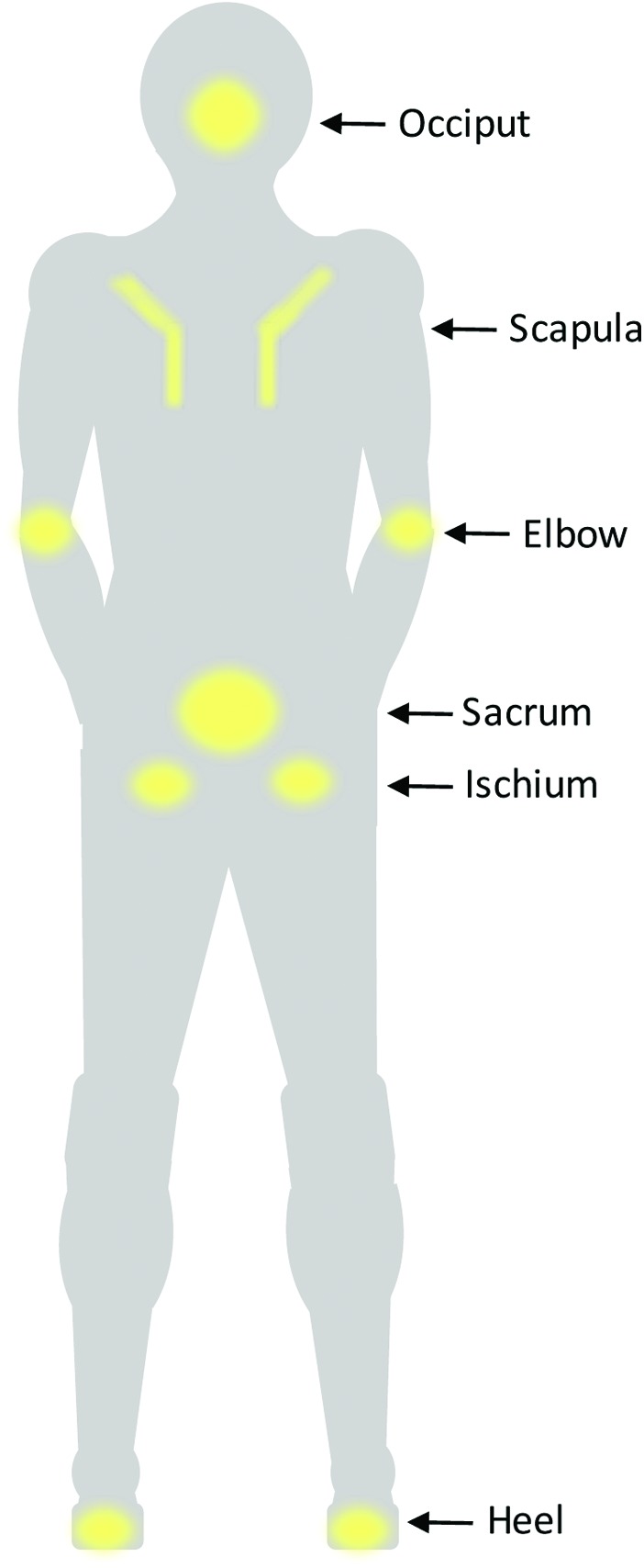
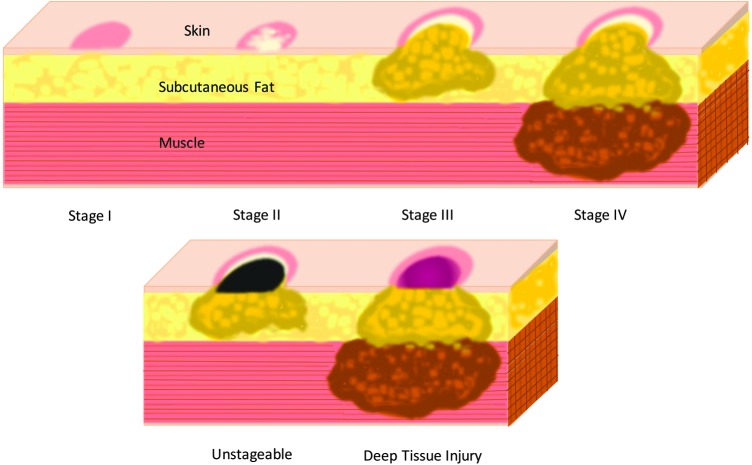
Pressure Injuries (NPIAP Staging I–IV, Unstageable, Deep Tissue Injury): Prevention by frequent turning (every 2 hours), pressure-redistribution surfaces, skin inspection, moisture management, and nutrition optimization. Document stage, location, dimensions, drainage, and treatment.
Neurogenic Bladder: Reflexic (UMN, above sacral micturition center) vs areflexic (LMN, at or below sacral cord). Managed with timed voiding, clean intermittent catheterization (CIC), indwelling catheter, anticholinergics (oxybutynin, tolterodine), beta-3 agonists (mirabegron), alpha blockers, and sometimes intravesical botulinum toxin.
Neurogenic Bowel: Bowel program including scheduled evacuation, digital stimulation, suppositories (bisacodyl, glycerin), stool softeners, and fiber.
Dysphagia: Evaluated by SLP clinical swallow, Modified Barium Swallow Study (MBSS/VFSS), or Fiberoptic Endoscopic Evaluation of Swallowing (FEES). Diet modifications per IDDSI levels. Aspiration precautions.
13 Cognitive, Speech & Swallowing Disorders Neuro Rehab
Aphasia: Broca (non-fluent, expressive, comprehension intact), Wernicke (fluent but nonsensical, comprehension impaired), global (both), conduction (impaired repetition), anomic (word-finding). Treated by SLP with constraint-induced language therapy, melodic intonation therapy, and AAC devices.
Dysarthria: Motor speech disorder — slurred, imprecise speech. Subtypes: flaccid, spastic, ataxic, hypokinetic (PD), hyperkinetic, mixed.
Apraxia of Speech: Impaired motor planning for speech despite intact strength and comprehension.
Cognitive Impairment: Screened with MMSE or MoCA. PM&R cognitive rehab addresses attention, memory, executive function, and visuospatial deficits through compensatory strategies and structured tasks.
14 Cancer, Cardiac, Pulmonary & Post-COVID Rehab Rehab
Cancer Rehabilitation: Addresses deconditioning, chemotherapy-induced peripheral neuropathy, radiation fibrosis, cognitive impairment ("chemo brain"), lymphedema, and post-surgical functional loss. Prehabilitation before cancer surgery improves outcomes.
Lymphedema: Swelling from lymphatic dysfunction, most common after axillary or inguinal lymph node dissection. Staged 0 (latent) through III (elephantiasis). Complete Decongestive Therapy (CDT): manual lymphatic drainage, multilayer compression bandaging, exercise, skin care, followed by maintenance compression garments.
Cardiac Rehabilitation: Phase I (inpatient post-MI or post-CABG), Phase II (supervised outpatient, 12 weeks of monitored exercise and risk factor modification), Phase III (community maintenance). PM&R oversight in some programs.
Pulmonary Rehabilitation: Structured exercise, breathing techniques (pursed-lip, diaphragmatic), energy conservation, and disease education for COPD, ILD, and post-transplant patients.
Post-COVID (Long COVID) Rehabilitation: Multisystem syndrome with fatigue, dyspnea, cognitive dysfunction, dysautonomia, and PEM (post-exertional malaise). Careful pacing to avoid PEM, autonomic rehab, cognitive strategies.
15 Geriatric Rehab, Deconditioning, Falls & Sarcopenia Rehab
Geriatric rehab addresses post-hospitalization deconditioning, post-fracture rehabilitation (especially hip fracture), fall prevention, and sarcopenia. Sarcopenia is age-related loss of muscle mass and strength, diagnosed by low grip strength, low muscle mass, and slow gait speed (< 0.8 m/s). Management: resistance training, adequate protein intake (1.0–1.2 g/kg/day), vitamin D optimization.
Falls assessment: Timed Up and Go (> 12 seconds suggests fall risk), Berg Balance Scale (< 45/56 suggests fall risk), Tinetti Performance-Oriented Mobility Assessment (POMA), Mini-BESTest, 30-second sit-to-stand. Multifactorial interventions (medication review, home safety, vision correction, strength and balance training, vitamin D) reduce fall rates.
Vertigo & Vestibular Disorders: BPPV (treated with Epley or Semont maneuver), vestibular neuritis, Meniere disease, bilateral vestibular hypofunction. Vestibular rehabilitation therapy uses gaze stabilization, habituation, and substitution exercises.
16 Electrodiagnostics & Injection Procedures Procedures
Electrodiagnostics (EMG/NCS)
The nerve conduction study (NCS) records the electrical response of a nerve to supramaximal stimulation. Measured parameters include amplitude (axonal integrity), latency and conduction velocity (myelination), and presence of conduction block or temporal dispersion. Needle electromyography (EMG) records electrical activity from muscle fibers at rest and during voluntary activation, assessing for spontaneous activity (fibrillations, positive sharp waves, fasciculations — signs of denervation), motor unit morphology, and recruitment patterns. Single-fiber EMG is used for neuromuscular junction disorders (myasthenia gravis).
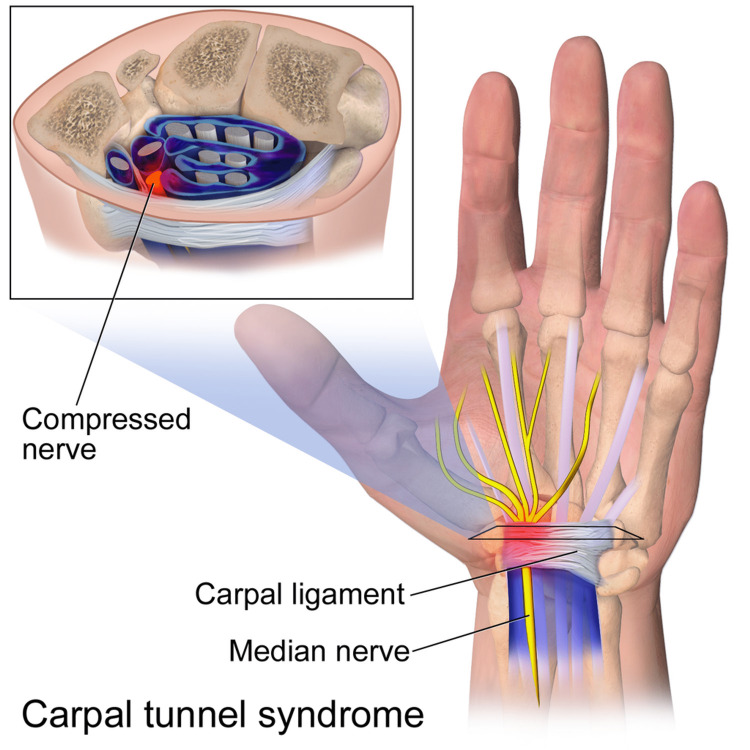
Common indications: carpal tunnel syndrome, ulnar neuropathy at the elbow/wrist, peroneal neuropathy, radiculopathy, polyneuropathy, motor neuron disease (ALS), brachial plexopathy, and myopathy. Studies are performed per AANEM practice guidelines.
Injection Procedures
| Procedure | Use |
|---|---|
| Intra-articular corticosteroid (shoulder, knee, hip, SI) | OA, bursitis, adhesive capsulitis |
| Hyaluronic acid injection (knee) | Knee OA viscosupplementation |
| PRP injection | Tendinopathy, early OA (off-label) |
| Trigger point injection | Myofascial pain |
| Epidural steroid injection (interlaminar, transforaminal, caudal) | Radiculopathy |
| Medial branch block / radiofrequency ablation | Facet-mediated pain |
| Botulinum toxin | Focal spasticity, cervical dystonia, blepharospasm, hemifacial spasm, chronic migraine (PREEMPT protocol) |
| Intrathecal baclofen pump refill | Severe generalized spasticity |
| Spinal cord stimulator trial / implant | Failed back surgery syndrome, CRPS, refractory neuropathic pain |
| Dorsal root ganglion stimulation | Focal neuropathic pain (foot, groin) |
| Peripheral nerve block (diagnostic/therapeutic) | Targeted pain sources, pre-procedural assessment |
Functional procedures: gait and motion analysis, urodynamics, video swallow studies (MBSS/FEES), wheelchair seating and positioning evaluation, prosthetic fitting, and orthotic prescription.
17 Orthotics, Prosthetics & Adaptive Equipment Equipment
| Device | Description & Use |
|---|---|
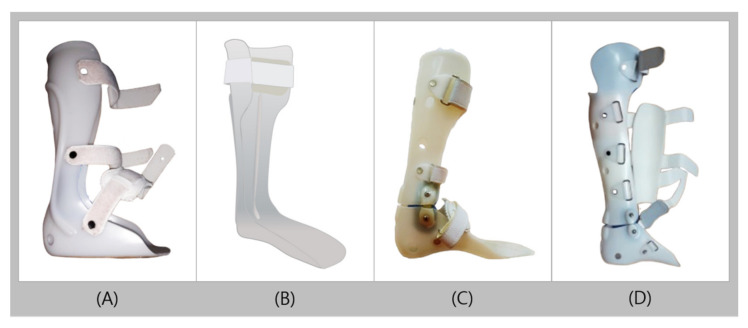
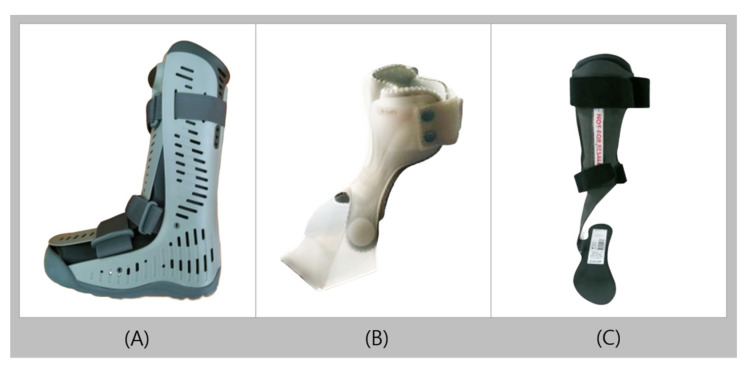
| AFO (Ankle-Foot Orthosis) | Plastic or carbon-fiber brace crossing the ankle; foot drop, stroke, CMT, post-polio. |
| KAFO (Knee-Ankle-Foot Orthosis) | Extends to the thigh with a knee joint; quadriceps weakness, SCI ambulation. |
| HKAFO (Hip-KAFO) | Adds hip joint; higher-level SCI therapy ambulation. |
| Lumbosacral Orthosis (LSO) | Back brace for compression fractures, post-op fusion. |
| TLSO | Thoracolumbosacral orthosis for scoliosis, thoracic fractures. |
| Cervical collar (soft, rigid, Miami J, Philadelphia) | Cervical spine stabilization. |
| Resting hand splint, cock-up wrist splint | Spasticity positioning, carpal tunnel. |
| Manual wheelchair | Standard, ultralight, tilt-in-space options. |
| Power wheelchair | Joystick, head array, sip-and-puff controls. |
| Walker, cane, crutches | Ambulation aids graded by stability needs. |
18 Inpatient Rehab Levels of Care & Team Model Systems
| Setting | Intensity | Typical Stay | Who Qualifies |
|---|---|---|---|
| Acute Inpatient Rehab Facility (IRF) | 3 hours of therapy/day, 5 days/week; daily MD visits | 10–20 days | Stroke, SCI, TBI, amputation, hip fracture; must tolerate 3 hrs/day and need ≥ 2 therapy disciplines |
| Long-Term Acute Care Hospital (LTACH) | Medical complexity with rehab as they tolerate | 25+ days | Vent weaning, complex wounds, multi-organ issues |
| Skilled Nursing Facility (SNF) | 1–2 hours therapy/day | Days to weeks | Can't tolerate IRF intensity; post-op, lower acuity |
| Home Health | Few visits per week | Variable | Homebound patients |
| Outpatient Rehab | 1–3 visits per week | Weeks to months | Community-dwelling |
| Day Rehab | Several hours/day without overnight stay | Weeks | TBI, stroke bridging home and outpatient |
The interdisciplinary team includes: physiatrist (team leader), rehab nurse, PT, OT, SLP, neuropsychologist, rehabilitation psychologist, social worker/case manager, dietitian, recreational therapist, vocational counselor, prosthetist/orthotist, and chaplain. Weekly team conferences review goals, progress, barriers, and discharge planning.
19 Imaging & Diagnostics in PM&R Diagnostics
| Modality | Use in PM&R |
|---|---|
| X-ray | Fractures, joint alignment, hardware assessment, scoliosis, HO. |
| MRI brain | Stroke, TBI (DAI on SWI/GRE), MS plaques, tumor. |
| MRI spine | Disc herniation, stenosis, cord compression, syrinx, SCI level, cauda equina. |
| MSK MRI | Rotator cuff, meniscus, ligament, labral tear, tendinopathy. |
| CT head | Acute bleed, skull fracture, shunt check. |
| CT myelogram | When MRI contraindicated. |
| Bone scan (triple phase) | HO (early detection), CRPS, occult fracture, osteomyelitis. |
| DEXA | Osteoporosis screening, especially SCI, post-menopausal, chronic steroid users. |
| EMG/NCS | Peripheral nerve, radiculopathy, motor neuron, NMJ, myopathy. |
| Urodynamics | Neurogenic bladder characterization. |
| MBSS / FEES | Dysphagia evaluation. |
| Gait analysis | Quantitative kinematic/kinetic assessment (CP, prosthetics). |
20 Medications You Must Know Meds
Spasticity
| Drug | Brand | Mechanism | Notes |
|---|---|---|---|
| Baclofen | Lioresal | GABA-B agonist | Oral or intrathecal (ITB pump); sedation, withdrawal risk if abruptly stopped |
| Tizanidine | Zanaflex | Central alpha-2 agonist | Sedation, hypotension, hepatotoxicity |
| Dantrolene | Dantrium | Direct muscle action (ryanodine receptor) | Hepatotoxicity; less sedating |
| Diazepam | Valium | GABA-A positive modulator | Sedation, tolerance, dependence |
| Gabapentin | Neurontin | Alpha-2-delta calcium channel | Also for neuropathic pain, spasticity adjunct |
| Botulinum toxin A/B | Botox, Dysport, Xeomin, Myobloc | Presynaptic ACh release blockade | Focal injection q 3 months |
Neuropathic Pain
| Drug | Brand | Class | Notes |
|---|---|---|---|
| Gabapentin | Neurontin | Gabapentinoid | Renal dosing; sedation, edema |
| Pregabalin | Lyrica | Gabapentinoid | Faster titration, similar profile |
| Duloxetine | Cymbalta | SNRI | DPN, fibromyalgia, chronic LBP |
| Amitriptyline, Nortriptyline | Elavil, Pamelor | TCA | Anticholinergic caution in elderly |
| Lidocaine 5% patch | Lidoderm | Sodium channel blocker | PHN, focal neuropathic pain |
| Capsaicin | Qutenza | TRPV1 agonist | PHN, DPN |
Bladder & Bowel
| Drug | Brand | Use |
|---|---|---|
| Oxybutynin | Ditropan | Overactive/neurogenic bladder (anticholinergic) |
| Tolterodine | Detrol | Overactive bladder |
| Mirabegron | Myrbetriq | Beta-3 agonist; fewer anticholinergic effects |
| Tamsulosin | Flomax | Alpha-blocker for bladder outlet / DSD |
| Bisacodyl, Senna, Docusate, PEG | — | Neurogenic bowel program |
Other
| Drug | Use |
|---|---|
| Amantadine | TBI arousal, MS fatigue, PD |
| Modafinil (Provigil) | Fatigue, narcolepsy, post-stroke cognition |
| Methylphenidate | Post-TBI attention, arousal |
| Carbidopa/levodopa (Sinemet) | Parkinson disease |
| SSRIs/SNRIs | Post-stroke depression, pseudobulbar affect (also dextromethorphan/quinidine) |
| Nifedipine, nitroglycerin paste | Autonomic dysreflexia |
| Enoxaparin, UFH | DVT prophylaxis in rehab |
| Vitamin D, calcium, bisphosphonates | Bone health (SCI, immobility) |
| Riluzole, edaravone | ALS disease-modifying |
21 Classification & Outcome Measures Scales
| Grade | Finding |
|---|---|
| 0 | No contraction |
| 1 | Flicker of contraction, no movement |
| 2 | Active movement with gravity eliminated |
| 3 | Active movement against gravity |
| 4 | Active movement against gravity and some resistance (4−, 4, 4+) |
| 5 | Normal strength |
| Stage | Description |
|---|---|
| 1 | Flaccidity; no voluntary movement. |
| 2 | Spasticity begins; minimal voluntary movement; synergies emerging. |
| 3 | Spasticity increases; voluntary movement only in synergy patterns. |
| 4 | Spasticity decreases; movement combinations out of synergy begin. |
| 5 | More complex movements possible; synergy dominance fades. |
| 6 | Spasticity nearly absent; coordinated movements near normal. |
| 7 | Normal motor function. |
| Score | Definition |
|---|---|
| 0 | No symptoms. |
| 1 | No significant disability; able to carry out all usual activities. |
| 2 | Slight disability; unable to carry out all previous activities but independent in ADLs. |
| 3 | Moderate disability; requires some help but walks unassisted. |
| 4 | Moderately severe; unable to walk without assistance, unable to attend to bodily needs. |
| 5 | Severe disability; bedridden, incontinent, requires constant care. |
| 6 | Death. |
Additional scales scribes will chart: FIM (Functional Independence Measure) — 18 items scored 1 (total assist) to 7 (complete independence); Barthel Index — 10 ADL items, 0–100; Berg Balance Scale — 14 items, 0–56; Tinetti POMA — 28 points (gait + balance); Timed Up and Go (TUG) — > 12 seconds suggests fall risk; Mini-BESTest — balance evaluation; Glasgow Outcome Scale (Extended) — TBI outcomes; SCIM (Spinal Cord Independence Measure); MMSE / MoCA — cognitive screening; House-Brackmann — facial nerve I–VI; GMFCS I–V for cerebral palsy; NPIAP Stage I–IV for pressure injuries.
22 Physical Exam — Functional, MSK & Neurologic Exam
General: Alert, oriented x3 (or note deficits), cooperative, in no acute distress.
Mental status: MMSE/MoCA if performed; attention, memory, executive function descriptors.
Cranial nerves: II–XII grossly intact or list deficits (visual fields, EOMs, facial symmetry, palate, tongue).
Motor: MRC grading by muscle group and side, tone (normal, spastic with Modified Ashworth grade, rigid, flaccid), bulk.
Sensory: Light touch, pinprick, vibration, proprioception by dermatome.
Reflexes: Biceps, triceps, brachioradialis, patellar, Achilles (0–4+), Babinski, clonus, Hoffmann.
Coordination: Finger-nose-finger, heel-shin, rapid alternating movements.
Musculoskeletal: Joint ROM (active and passive), tenderness, stability, special tests (Neer, Hawkins, Empty Can, McMurray, Lachman, SLR, FABER, etc.).
Functional: Bed mobility, transfers (sit-to-stand, bed-to-chair), gait description with device and assist level, distance, and stairs.
Skin: Integrity, pressure areas, surgical incisions.
23 Abbreviations Master List
Diagnoses & Conditions
Assessments & Scales
Procedures & Equipment
Team, Setting & Workflow
24 Sample HPI Templates & References
"Mr. [Name] is a 68-year-old right-handed male with PMH of HTN, HLD, T2DM (A1C 8.1), and atrial fibrillation on apixaban admitted to acute inpatient rehab following a left MCA ischemic stroke on [date]. He underwent mechanical thrombectomy with successful TICI 2b recanalization. He is transferred to IRF with right hemiparesis (UE 2/5, LE 3/5 MRC), expressive (Broca) aphasia, right facial droop, and mild dysphagia on modified diet (IDDSI 5 minced moist, thin liquids). Baseline: independent community ambulator, drove, worked part-time. Currently requires min assist for bed mobility, mod assist for sit-to-stand transfers, and CGA for ambulation 15 feet with quad cane. Goals: return to home with wife, independent transfers and household ambulation, communication improvement. Plan: PT/OT/SLP 3 hours daily x 5 days/week, continue apixaban for secondary prevention, atorvastatin 80 mg, BP and glycemic control, DVT prophylaxis with enoxaparin, post-stroke depression screening, aspiration precautions."
"Mr. [Name] is a 27-year-old previously healthy male who sustained a C5 burst fracture after a diving accident 2 weeks ago, status post C4–C6 anterior cervical corpectomy and fusion. Initial ASIA exam today demonstrates motor level C6 bilaterally, sensory level C6, AIS B (sensory incomplete — preserved sacral sensation, no motor below level). Zone of partial preservation: motor C7 on the right. Currently total assist for bed mobility, transfers, and ADLs; requires manual cough assist. Bladder managed with indwelling Foley (plan to transition to q6h CIC), bowel program initiated. On enoxaparin 40 mg SC daily for DVT prophylaxis, pantoprazole, oxycodone PRN, baclofen 10 mg TID for emerging spasticity. Goals of acute rehab: tenodesis grasp training, power wheelchair evaluation, bowel/bladder program, family training for discharge to home with 24-hour caregiver support."
"Ms. [Name] is a 32-year-old female pedestrian struck by motor vehicle 3 weeks ago with initial GCS 6, CT showing bifrontal contusions and traumatic SAH, MRI showing diffuse axonal injury. S/p craniectomy, tracheostomy now decannulated, PEG in place. Currently Rancho Los Amigos Level V (confused, inappropriate, non-agitated). Follows simple 1-step commands intermittently, disoriented, post-traumatic amnesia ongoing. Motor exam grossly intact but poor safety awareness and impulsive. Requires max assist for all mobility. Plan: transfer to acute brain injury rehab program, continue methylphenidate for arousal, amantadine 100 mg BID, behavioral management strategies, SLP for cognitive-linguistic therapy, family education."
"Mr. [Name] is a 62-year-old male with T2DM, PAD, and CKD stage 3 who underwent right BKA 10 days ago for non-healing diabetic foot ulcer with osteomyelitis. Residual limb with clean, dry incision, no drainage, mildly edematous, currently in shrinker sock. Phantom limb pain 6/10 at rest, described as burning and cramping, partially relieved by gabapentin 300 mg TID. Left lower extremity with intact sensation and 2+ DP/PT pulses, no wounds. Prior ambulation: community distances with cane. Current: max assist sit-to-stand, uses wheelchair. Admitted for pre-prosthetic rehabilitation: ROM, strengthening, desensitization, transfer training, and left LE protection. Pending prosthetic fitting in 4–6 weeks pending residual limb maturation."
"Ms. [Name] is a 45-year-old female nurse presenting for evaluation of 4 months of low back pain radiating into the right posterior thigh and lateral calf, worse with prolonged sitting and bending, partially relieved by walking and ibuprofen. Pain 6/10 average, 9/10 at worst. No bowel/bladder dysfunction, no saddle anesthesia, no fevers, no weight loss. Failed 6 weeks of physical therapy with modest improvement. MRI lumbar spine shows L5–S1 right paracentral disc extrusion with compression of traversing right S1 nerve root. Exam: positive right straight leg raise at 45 degrees, decreased right Achilles reflex, S1 sensory dermatome hypesthesia, right gastrocnemius 4/5. Plan: right L5–S1 transforaminal epidural steroid injection under fluoroscopic guidance, continue PT with McKenzie-based extension program, gabapentin 300 mg TID, reassess in 4 weeks; refer to spine surgery if no improvement or progressive deficit."
"Mrs. [Name] is a 74-year-old female s/p elective right total hip arthroplasty (posterior approach) POD#2 for severe OA, transferred to IRF. Posterior hip precautions in place (no flexion > 90, no adduction past midline, no internal rotation). Currently min assist for bed mobility, min-mod assist for transfers, ambulating 20 feet with front-wheeled walker and CGA. Pain well controlled on acetaminophen and oxycodone PRN. DVT prophylaxis with apixaban x 35 days. Lives alone in single-story home with grab bars in bathroom. Goals: independent transfers, ambulation 150 feet with walker, stair negotiation with railing, independent ADLs with adaptive equipment (reacher, sock aid, long-handled sponge) prior to discharge home."
References & Sources
Winstein CJ et al. Guidelines for Adult Stroke Rehabilitation and Recovery. AHA/ASA. Stroke. 2016.
Consortium for Spinal Cord Medicine Clinical Practice Guidelines.
AANEM Practice Guidelines for Electrodiagnostic Medicine.
AAPM&R Evidence-Based Practice Guidelines for Rehabilitation Care.
NICE NG211: Stroke Rehabilitation in Adults. 2023.
Brain Injury Association of America (BIAA) Clinical Resources.
Figure 1: Brain and Spinal Cord. OpenStax College. CC BY 3.0.
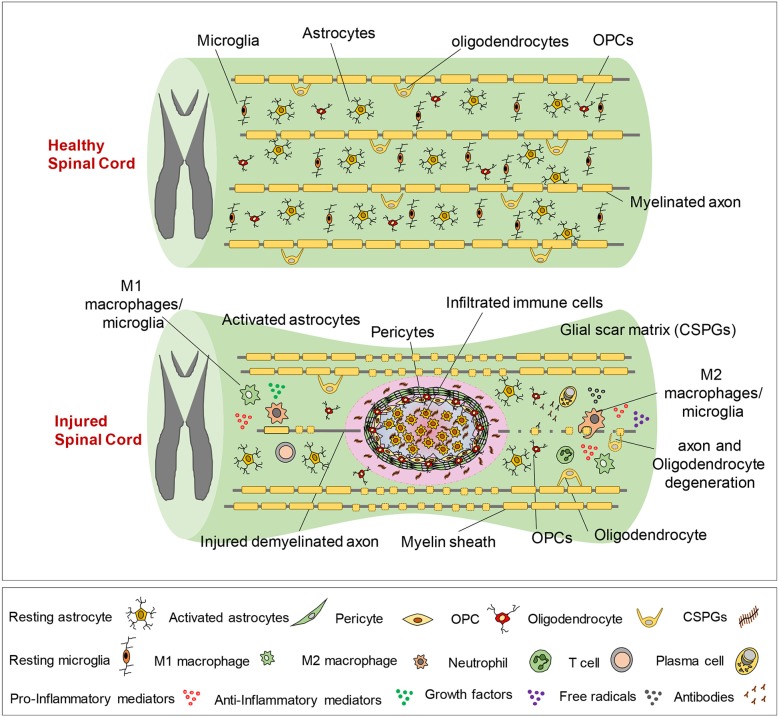
Figure 2: Spinal Cord Tracts. Polarlys, Wikimedia Commons. CC BY-SA 3.0.
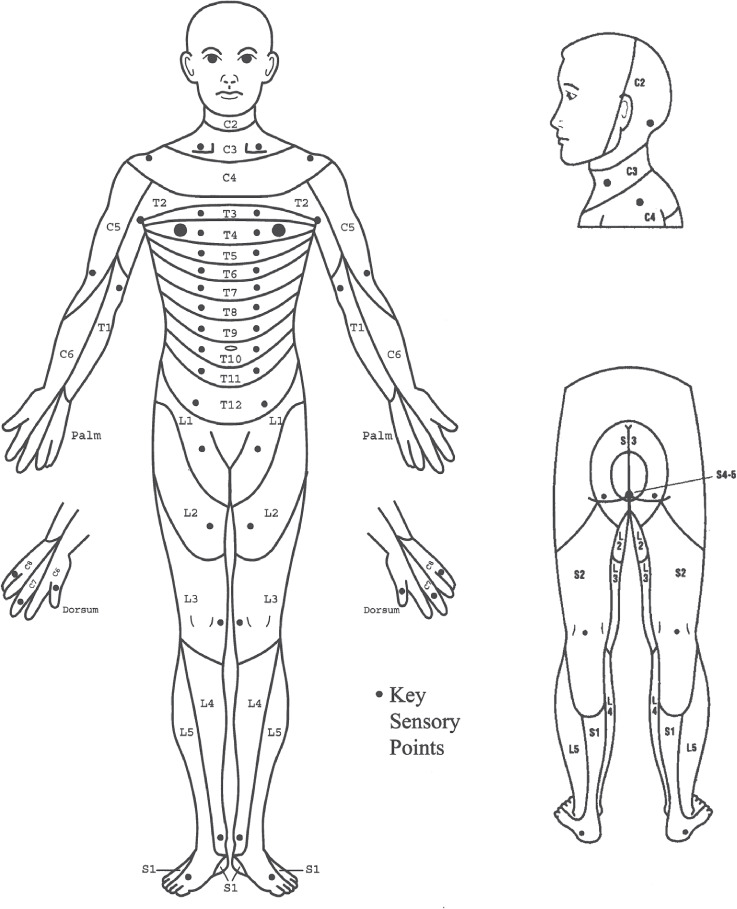
Figure 3: Dermatome Map (anterior). Ralf Stephan, Wikimedia Commons. Public domain.
Figure 4: MCA Territory Infarct. Wikimedia Commons. Public domain.
Figure 5: Prosthetic Leg. Wikimedia Commons. Public domain.
Figure 6: Manual Wheelchair. Wikimedia Commons. Public domain.
The best PM&R scribes listen for function as carefully as they listen for diagnoses. When the physiatrist says "the patient is AIS C, C6 tetraplegia with tenodesis grasp and min-assist transfers," a great scribe already understands the anatomic level, the completeness grade, the functional capability this implies, and the likely equipment plan. When the attending says "MAS 3 in the gastrocs with dynamic equinus limiting gait," the scribe hears the spasticity grade, the muscle, and the functional consequence, and knows botulinum toxin and AFO are on the table.
Be obsessive about quantification. "Ambulates" is worthless; "ambulates 50 feet with front-wheeled walker and CGA on level surfaces" tells the whole story. Pre-read the PT, OT, and SLP notes before rounds so you can pre-populate the functional summary. Learn the equipment catalog — AFO, KAFO, HKAFO, LSO, walker, quad cane, manual and power chairs — because orders often fly by in seconds. Always capture the disposition plan: PM&R is a specialty where the discharge is the outcome.
Welcome to physiatry. In this specialty, you will watch patients who could not move a finger walk out of the unit. The documentation you write is part of how that happens.