Podiatry
Every diagnosis, deformity, procedure, medication, classification, and documentation pattern you need to run a podiatry clinic note from day one.
All diagrams on this page are sourced from published educational or institutional materials rather than AI generation. Each figure caption links to the original source, and the full diagram and guideline citations are collected in the references section at the bottom.
01 Foot & Ankle Anatomy and Biomechanics
Podiatry is the medical and surgical specialty of the foot, ankle, and related lower extremity structures. To document intelligently, you must know the bony architecture, the joints that move the foot, the tendons that drive them, the nerve territories that explain pain, and the basic biomechanics of gait.
Bony Architecture
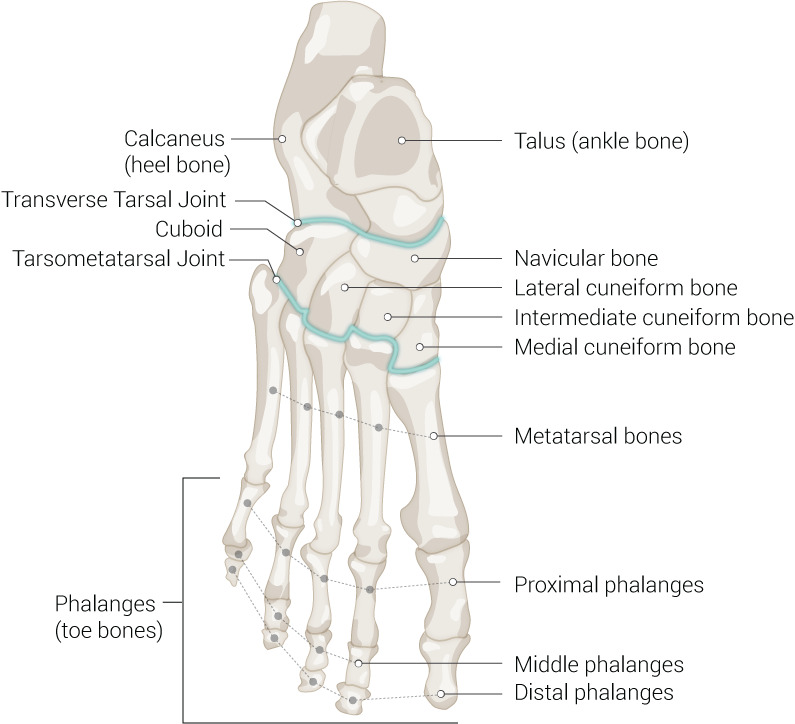
The foot contains 26 bones grouped into three regions. The hindfoot includes the talus (which articulates with the tibia and fibula to form the ankle mortise) and the calcaneus (heel bone). The midfoot consists of the navicular, cuboid, and three cuneiforms (medial, intermediate, lateral). The forefoot consists of five metatarsals and 14 phalanges (two in the great toe, three in each lesser toe). Two small sesamoid bones lie beneath the first metatarsal head within the flexor hallucis brevis tendon.
Joints & Columns
The ankle (tibiotalar) joint is a hinge between the distal tibia/fibula (mortise) and the talar dome, producing dorsiflexion and plantarflexion. The subtalar joint lies between the talus and calcaneus and produces inversion and eversion. The transverse tarsal (Chopart) joint is the combined talonavicular and calcaneocuboid articulation and allows forefoot abduction/adduction and pronation/supination. The tarsometatarsal (Lisfranc) joint separates the midfoot from the forefoot — the second metatarsal base is recessed into the cuneiforms as the "keystone," stabilized by the Lisfranc ligament between the medial cuneiform and second metatarsal base. The first metatarsophalangeal (MTP) joint is the great toe joint where bunions and hallux rigidus develop; the lesser MTP, PIP, and DIP joints are where hammertoes and claw toes form.
Podiatrists also speak in terms of medial, central, and lateral columns of the foot. The medial column (first ray: medial cuneiform, first metatarsal, great toe) is the key weight-bearing column in push-off. The lateral column (cuboid, 4th and 5th metatarsals) provides stability during stance. Understanding columns matters because surgical reconstructions (Lapidus, Evans, Cotton) address specific columns.
Tendons & Muscles
Five extrinsic tendons dominate podiatry charts: the Achilles tendon (gastrocnemius + soleus) inserts onto the calcaneus and is the main plantarflexor. The posterior tibial tendon (PTT) runs behind the medial malleolus, inserts on the navicular tuberosity, and is the primary dynamic stabilizer of the medial longitudinal arch. The peroneus longus and brevis run behind the lateral malleolus and evert the foot; peroneus brevis inserts on the 5th metatarsal base (Jones fracture territory). The tibialis anterior is the main dorsiflexor. The flexor hallucis longus (FHL) passes posterior to the talus and plantarflexes the great toe.
Nerves & Dermatomes
The tibial nerve passes posterior to the medial malleolus under the flexor retinaculum (the tarsal tunnel) and divides into the medial and lateral plantar nerves supplying the sole. The common peroneal nerve divides into the superficial peroneal (dorsum sensation, peroneals motor) and deep peroneal (first web space sensation, tibialis anterior motor) nerves. The sural nerve supplies the lateral foot. The saphenous nerve supplies the medial foot to the first MTP.
Ligaments You Must Know
The lateral ankle ligament complex consists of the anterior talofibular ligament (ATFL), the calcaneofibular ligament (CFL), and the posterior talofibular ligament (PTFL). The ATFL is the weakest and the first injured in an inversion sprain. The deltoid ligament is the medial ankle complex (superficial and deep components) and is rarely injured in isolation. The syndesmosis binds the distal tibia and fibula and includes the AITFL (anterior inferior tibiofibular ligament), PITFL, interosseous ligament, and transverse tibiofibular ligament — injury produces the "high ankle sprain." The spring ligament (plantar calcaneonavicular ligament) supports the talar head and works with the posterior tibial tendon to maintain the medial arch; spring ligament failure is part of PTTD/PCFD. The Lisfranc ligament stabilizes the medial cuneiform to the second metatarsal base and is the key stabilizer of the tarsometatarsal joint.
Biomechanics of Gait

Normal gait has a stance phase (60%) and swing phase (40%). Stance is subdivided into heel strike, foot flat, midstance, heel off, and toe off. At heel strike, the subtalar joint pronates to absorb shock; at midstance, it begins resupinating to create a rigid lever for push-off. The windlass mechanism describes how dorsiflexion of the hallux during toe-off tightens the plantar fascia, elevating the arch and locking the midfoot. Dysfunction of this mechanism drives plantar fasciitis, PTTD, and first MTP pathology.
Podiatry notes frequently reference the "first ray" — this means the medial cuneiform + first metatarsal + hallux as a functional unit. A "hypermobile first ray" is a key concept in bunion pathogenesis and in deciding between an Austin vs. Lapidus procedure. You will hear "first ray insufficiency," "first ray elevation," and "first ray fusion" constantly.
02 Scribe Documentation Framework
A podiatry clinic note is structured as a SOAP but with specialty-specific detail at every level. The HPI always captures laterality (right vs. left foot), location (hindfoot, midfoot, forefoot, specific joint), shoe wear, activity, prior treatments tried (NSAIDs, orthotics, injections, PT), and diabetic/vascular status. The exam always includes vascular, neurologic, dermatologic, and musculoskeletal components.
Chief Complaint: Short, laterality-specific. "Right bunion pain," "left heel pain 3 months," "bilateral diabetic foot exam," "ingrown toenail right hallux."
HPI: OLDCARTS plus podiatry-specific anchors: shoe gear (dress shoes, work boots, athletic), activity level, occupation (prolonged standing?), exacerbating positions (first steps in the morning for plantar fasciitis, downhill walking for Achilles), prior podiatric care, prior injections, prior orthotics, prior imaging.
PMH: Always document diabetes (type, A1C, duration, complications including neuropathy and retinopathy), peripheral arterial disease, venous insufficiency, peripheral neuropathy, gout, rheumatoid arthritis, immunosuppression, chronic kidney disease, smoking, and prior foot surgery.
Meds/Allergies: Insulin and oral diabetic agents, anticoagulants (critical before any procedure), immunosuppressants, gout medications, prior antibiotics for foot infections.
Vascular: Dorsalis pedis (DP) and posterior tibial (PT) pulses bilaterally (0/1+/2+/3+ or "palpable" vs "Dopplerable" vs "absent"), capillary refill (normal < 3 sec), skin temperature, hair distribution, dependent rubor, edema.
Neurologic: Protective sensation tested with a 10-g Semmes-Weinstein monofilament at standard plantar sites (hallux, 1st, 3rd, 5th metatarsal heads, heel). Vibratory sense with 128-Hz tuning fork. Ankle and deep tendon reflexes. Document intact or impaired protective sensation (LOPS = loss of protective sensation).
Dermatologic: Skin integrity, calluses (hyperkeratoses), fissures, ulcerations (size in length x width x depth, location, wound bed appearance, drainage, surrounding erythema/induration), nail appearance (onychomycosis, onychocryptosis, subungual hematoma).
Musculoskeletal: Gait observation, alignment (varus, valgus, cavus, planus), range of motion at ankle, subtalar, midtarsal, and 1st MTP joints, muscle strength (0–5), palpation for point tenderness, specific provocative maneuvers (single-heel-rise, too-many-toes sign, anterior drawer, squeeze test).
Each foot problem documented as its own numbered diagnosis with ICD-10 code, followed by explicit plan items: injection administered (drug, dose, site, technique), orthotic prescribed (custom vs OTC, material), padding/strapping applied, imaging ordered, wound care instructions, offloading device, medication prescribed or refilled, referrals (vascular, endocrine, infectious disease, orthopedics), and return-to-clinic interval. Document patient education and informed consent for any in-office procedure.
Every diabetic foot exam note must explicitly state whether the patient has protective sensation intact or LOPS, and whether DP and PT pulses are palpable. These two sentences determine risk stratification and are required for reimbursement of the comprehensive diabetic foot exam CPT code. Never leave them out.
03 Hallux Valgus (Bunion) & Tailor's Bunion Forefoot
Hallux valgus is a progressive triplanar deformity of the first ray characterized by lateral deviation of the hallux at the first MTP joint, medial prominence of the first metatarsal head (the visible "bunion bump"), and pronation of the great toe. It is the single most common elective podiatric surgery. Tailor's bunion (bunionette) is the analogous deformity of the 5th metatarsal head laterally.

Pathophysiology
Bunions develop from a combination of intrinsic biomechanics (hypermobile first ray, metatarsus primus varus, pes planus, ligamentous laxity) and extrinsic factors (constrictive footwear, high heels, family history). As the first metatarsal drifts medially and the hallux deviates laterally, the windlass mechanism fails, adductor hallucis pulls the hallux further lateral, and the medial capsule stretches while lateral structures contract. The sesamoids "subluxate" laterally relative to the metatarsal head.
Clinical Presentation
Patients report pain over the medial eminence (bunion) aggravated by shoe wear, difficulty fitting shoes, crossover of the hallux under or over the second toe, secondary pain at the second MTP (transfer metatarsalgia from first ray insufficiency), and cosmetic concerns. Numbness over the medial hallux suggests irritation of the dorsomedial cutaneous nerve branch.
Radiographic Measurements
Weight-bearing AP, lateral, and sesamoid axial views are standard. Key angles:
| Measurement | Normal | Mild | Moderate | Severe |
|---|---|---|---|---|
| HVA (Hallux Valgus Angle) | < 15° | 15–20° | 21–39° | ≥ 40° |
| IMA (1-2 Intermetatarsal Angle) | < 9° | 9–11° | 12–15° | > 15° |
| DMAA (Distal Metatarsal Articular Angle) | < 10° | Elevated DMAA = congruent joint, may need biplanar osteotomy | ||
Management
Conservative care is first-line for mild-moderate symptomatic bunions: wide toe-box shoes, bunion splints/spacers, OTC or custom orthotics, NSAIDs, activity modification. ACFAS clinical practice guidance emphasizes matching the procedure to the deformity magnitude and first ray mobility. Surgical options match deformity severity:
- Distal osteotomy (Austin/Chevron): mild-moderate deformity (IMA < 13°). Distal first metatarsal V-cut fixed with a screw.
- Scarf osteotomy: moderate deformity, Z-shaped diaphyseal cut, very stable fixation.
- Proximal osteotomy / Lapidus (first TMT fusion): moderate-severe deformity, hypermobile first ray, revision cases.
- Akin osteotomy: adjunct proximal phalanx wedge for hallux interphalangeus; almost always combined with another procedure, not done alone.
- Keller arthroplasty: salvage in elderly/low-demand patients; resection of proximal phalanx base.
- First MTP fusion: for severe deformity with arthritis or RA.
When the surgeon dictates a bunion op, listen for "IMA of X degrees" and "Lapidus" vs "Austin" — that word choice drives which CPT code and which post-op protocol (Austin is protected weight-bearing in surgical shoe for 4–6 weeks; Lapidus is strict non-weight-bearing for 6 weeks).
04 Hallux Rigidus & First MTP Arthritis Forefoot
Hallux rigidus is osteoarthritis of the first MTP joint producing progressive loss of dorsiflexion, dorsal osteophyte formation, and pain with push-off. It is the second most common condition of the great toe after hallux valgus. Distinguishing hallux rigidus from hallux valgus matters because surgical management differs entirely.
Patients present with pain at the dorsal first MTP worsened by activities requiring toe dorsiflexion (running, squatting, high heels), palpable dorsal bump (dorsal osteophyte, not medial), and reduced hallux dorsiflexion (< 50° is restricted, < 20° is severe). Imaging shows joint space narrowing, subchondral sclerosis, and a dorsal osteophyte. The Coughlin-Shurnas classification grades severity 0–4 based on dorsiflexion range, radiographic findings, and pain:
Grade 0: Stiffness, 40–60° dorsiflexion, normal X-ray, no pain.
Grade 1: Mild pain at extremes, 30–40° dorsiflexion, dorsal osteophyte, minimal joint space changes.
Grade 2: Moderate-to-severe pain, 10–30° dorsiflexion, dorsal/lateral/medial osteophytes, < 50% joint space loss.
Grade 3: Near-constant pain, < 10° dorsiflexion, sesamoid enlargement, > 50% joint space loss.
Grade 4: Grade 3 findings plus pain with passive mid-range motion (mid-range crepitus).
Conservative: rigid-sole shoes or rocker-bottom, carbon-fiber Morton extension orthotic (blocks first MTP motion), NSAIDs, intra-articular corticosteroid injection. Surgical: cheilectomy (dorsal osteophyte excision, grades 1–2), Moberg osteotomy (dorsiflexion wedge from proximal phalanx), first MTP arthrodesis (grades 3–4 — gold standard for severe hallux rigidus), or Cartiva synthetic cartilage implant/hemiarthroplasty in select patients.
05 Lesser Toe Deformities Forefoot
Three related deformities affect the lesser toes and are frequently confused. Know the distinction cold:
Hammertoe: PIP joint flexion, DIP neutral or extended, MTP may be extended. The most common lesser toe deformity.
Claw toe: MTP hyperextension with PIP and DIP flexion. Often bilateral and associated with neuromuscular disease (Charcot-Marie-Tooth, diabetic neuropathy, cavus foot).
Mallet toe: Isolated DIP flexion with normal PIP and MTP. Often affects the second toe (longest ray).
All three begin as flexible (passively correctable) and progress to rigid (fixed). Early they produce dorsal PIP or tip-of-toe calluses from shoe rub; late they cause painful dislocation of the MTP joint. Conservative: toe crests, hammertoe splints, wide toe-box shoes, callus debridement. Surgical: flexor tenotomy (flexible deformity), PIP arthroplasty (resection of distal condyles of proximal phalanx), PIP arthrodesis (fusion with intramedullary implant or K-wire — gold standard for rigid hammertoe), flexor-to-extensor tendon transfer (Girdlestone-Taylor) for flexible deformity with MTP subluxation, and metatarsal shortening osteotomy (Weil) for plantar plate insufficiency and transfer metatarsalgia.
06 Morton Neuroma & Forefoot Pain Forefoot
Morton neuroma is not a true neuroma — it is perineural fibrosis of a common digital nerve, most commonly in the third webspace (between 3rd and 4th metatarsal heads), where the medial and lateral plantar nerves converge and the nerve is tethered by the intermetatarsal ligament. Patients are typically middle-aged women and report burning, electric, "walking on a pebble" pain in the affected webspace that radiates to the adjacent toes, worsened by tight shoes or high heels and relieved by removing the shoe and massaging the foot.
Key exam maneuvers: Mulder click (medial-lateral compression of the forefoot reproduces a palpable clunk and pain), webspace tenderness, and numbness in the adjacent toes. Ultrasound or MRI confirms the diagnosis when clinical picture is unclear. Management progresses through wide shoes, metatarsal pads (placed proximal to the metatarsal heads to spread them), NSAIDs, and ultrasound-guided corticosteroid + local anesthetic injection (up to 3 injections). Refractory cases undergo Morton neurectomy (dorsal or plantar approach) — the scribe documents the webspace involved and whether the procedure is primary or a revision for stump neuroma.
07 Plantar Fasciitis & Heel Pain Syndromes Hindfoot
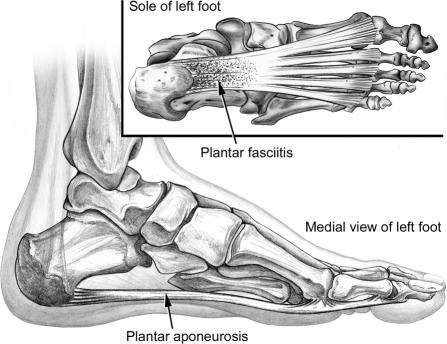
Plantar fasciitis is the most common cause of adult heel pain. It is a degenerative fasciosis (not purely inflammatory) of the plantar aponeurosis at its calcaneal origin. Classic presentation: sharp medial heel pain with the first steps in the morning or after prolonged sitting ("post-static dyskinesia"), improving with walking but worsening at the end of the day. Risk factors include obesity, tight gastrocnemius (equinus), prolonged standing occupations, flat or cavus feet, and sudden increases in activity.
Exam reveals point tenderness at the medial calcaneal tubercle, worsened by passive dorsiflexion of the toes (which tensions the fascia via the windlass mechanism). A heel spur on X-ray is common but not causative — do not attribute pain to the spur itself. Differential diagnosis includes calcaneal stress fracture (positive squeeze test), tarsal tunnel syndrome (neurogenic burning), Baxter nerve entrapment (first branch of lateral plantar nerve), plantar fascia rupture (acute tearing with palpable defect), and S1 radiculopathy.
Treatment is conservative in > 90% of patients: AOFAS clinical consensus statement on plantar heel pain supports a stepwise protocol of stretching (plantar fascia-specific stretching and gastrocnemius stretching), activity modification, NSAIDs, night splints (hold foot in dorsiflexion), prefabricated heel cups or custom orthotics, and corticosteroid injection (used judiciously given small risk of fascia rupture and fat pad atrophy). Refractory cases (> 6 months): extracorporeal shockwave therapy (ESWT), platelet-rich plasma injection, or surgical plantar fasciotomy (open, percutaneous, or endoscopic — release of medial third only to avoid lateral column collapse).
Calcaneal apophysitis (Sever disease) is the pediatric analog — heel pain in active children aged 8–14 at the calcaneal growth plate; managed with activity modification, heel cups, and stretching, and self-limited by skeletal maturity.
08 Achilles Tendinopathy & Rupture Hindfoot
Achilles pathology is split anatomically into insertional (at the calcaneal attachment, within 2 cm of insertion) and midportion/noninsertional (2–6 cm above insertion, the zone of relative hypovascularity). Both represent degenerative tendinosis, not true inflammation.
Insertional Achilles tendinopathy presents with posterior heel pain worse uphill or climbing stairs, associated with Haglund deformity (posterosuperior calcaneal prominence irritating the tendon) and retrocalcaneal bursitis. X-ray shows intratendinous calcification and the Haglund bump. Conservative care emphasizes heel lifts, activity modification, eccentric calf strengthening (though less effective than in midportion), NSAIDs, and shoe modifications. Avoid corticosteroid injection into the Achilles — rupture risk. Surgical options include debridement with Haglund resection and reattachment using suture anchors or FHL tendon transfer for > 50% tendon involvement.
Midportion tendinopathy presents with pain and thickening 2–6 cm above the insertion. Eccentric calf strengthening (Alfredson protocol) is first-line and well-supported. Other options: ESWT, PRP, gastrocnemius recession for refractory cases with equinus contracture.
Achilles tendon rupture is a sudden tear, classically in a "weekend warrior" middle-aged male during push-off or sudden dorsiflexion. Patients describe feeling "shot in the back of the leg" or "kicked," followed by weakness in push-off. Exam: palpable gap 2–6 cm above the insertion, positive Thompson test (squeezing the calf produces no plantarflexion with the patient prone), and weak active plantarflexion (some motion may persist from FHL, peroneals, and posterior tibial). Ultrasound or MRI confirms the diagnosis and measures gap size.
Management is either operative (open end-to-end repair, percutaneous repair with systems like PARS/Achillon, or minimally invasive) or non-operative (functional rehabilitation with early controlled weight-bearing in a boot with heel wedges). Modern AAOS Achilles rupture guidance shows that non-operative functional rehab produces similar re-rupture rates to surgery in many patients, so the choice depends on age, activity, and patient preference.
09 Posterior Tibial Tendon Dysfunction & Adult Flatfoot Hindfoot
Posterior tibial tendon dysfunction (PTTD), now called adult-acquired flatfoot deformity (AAFD) or the newer term progressive collapsing foot deformity (PCFD), is the most common cause of acquired flatfoot in adults. The posterior tibial tendon is the key dynamic stabilizer of the medial longitudinal arch; when it fails, the arch collapses, the heel drifts into valgus, the forefoot abducts, and eventually fixed deformity and arthritis develop.
Classic presentation: middle-aged woman, obese, medial ankle/arch pain (early) progressing to lateral ankle pain (late — from subfibular impingement as the calcaneus drifts into valgus). Exam: unable to perform single-heel-rise (inversion of heel fails when rising on tiptoe), "too-many-toes sign" from behind (more than 2–3 toes visible lateral to the heel due to forefoot abduction), and weakness of inversion against resistance.
The Johnson-Strom classification (with Myerson stage 4) grades severity:
| Stage | Findings | Management |
|---|---|---|
| I | Tendinitis, no deformity, normal heel rise | Immobilization, orthotics, PT |
| II | Flexible flatfoot, abnormal heel rise, tendon elongation | Orthotics, AFO; surgical: FDL transfer, calcaneal osteotomy (medializing MCO), Cotton osteotomy |
| III | Rigid hindfoot deformity, subtalar arthritis | Triple arthrodesis (subtalar + talonavicular + calcaneocuboid) |
| IV | Valgus tilt of talus within ankle mortise | Triple arthrodesis +/- deltoid reconstruction, TAR, or tibiotalocalcaneal fusion |
Surgical reconstruction for stage II is the most common podiatric hindfoot reconstruction. Typical components: FDL tendon transfer to navicular (replaces failed PTT), medializing calcaneal osteotomy (MCO) (corrects heel valgus), lateral column lengthening (Evans osteotomy) (corrects forefoot abduction), and Cotton osteotomy (medial cuneiform opening wedge) to plantarflex the medial column. Consensus statement on the new PCFD classification replaces the older Johnson-Strom system with a class/stage system (flexible vs rigid, plus deformity descriptors).
10 Peroneal Tendon Disorders Lateral
The peroneus longus and brevis tendons share a common sheath behind the lateral malleolus. Disorders include tendinopathy/tenosynovitis, longitudinal tears (most often in peroneus brevis, which becomes "split" as it is compressed between the fibula and peroneus longus), and subluxation/dislocation (retinaculum failure, typically from forced dorsiflexion injury; peroneals snap anterior to the fibula). Patients present with lateral ankle pain, swelling behind the fibula, and a popping or snapping sensation. MRI confirms tears and retinacular injury.
Conservative: immobilization in a CAM boot or brace, NSAIDs, physical therapy focused on eccentric peroneal strengthening, and lateral heel wedge to offload the peroneals. Surgical: tendon debridement and tubularization of split tears, side-to-side repair or tenodesis for severe tears (one tendon sutured to the other when one is irreparable), groove deepening with retinacular repair for recurrent subluxation (the fibular groove is deepened with a burr and the superior peroneal retinaculum is reattached), and fibular osteotomy-based deepening for chronic cases. Always document whether tenosynovitis is isolated or whether there are frank longitudinal split tears of peroneus brevis on MRI.
Peroneal subluxation is often missed. If a patient reports "snapping" or "popping" behind the lateral malleolus after a dorsiflexion-eversion injury, document the dynamic exam: have the patient actively circumduct or evert against resistance and observe whether the tendons visibly jump out of the retrofibular groove.
11 Ankle Sprains & Chronic Instability Lateral
Ankle sprains are extremely common. Understand the three distinct types:
Lateral (inversion) sprain: 85% of all sprains. Injury pattern: ATFL (anterior talofibular ligament, the weakest and first to tear) → CFL (calcaneofibular ligament) → PTFL (posterior talofibular ligament, rarely injured).
Medial (deltoid) sprain: Eversion injury. Less common. Always suspect associated syndesmotic injury or fibular fracture (Maisonneuve at the proximal fibula).
High ankle (syndesmotic) sprain: Injury to the tibiofibular syndesmosis from external rotation and dorsiflexion. Presents with tenderness above the joint line, positive squeeze test (compression of the tibia-fibula at mid-calf produces distal pain) and positive external rotation stress test. Prolonged recovery compared to lateral sprains.
Severity grades: Grade I (ligament stretched, minimal instability), Grade II (partial tear, moderate instability), Grade III (complete tear, gross instability). Apply the Ottawa ankle rules to decide on X-rays: pain in the malleolar zone PLUS either bony tenderness at the posterior edge/tip of either malleolus OR inability to weight-bear four steps immediately and in the ED. Foot films are indicated for midfoot zone pain with bony tenderness at the navicular or base of 5th metatarsal or inability to bear weight.
Management: functional rehabilitation (PRICE → early weight-bearing in brace → peroneal strengthening and proprioception) is the gold standard. Avoid prolonged immobilization. Chronic ankle instability develops in ~20% of ankle sprains and presents with recurrent giving-way episodes. Treatment: PT, lace-up braces, and surgical reconstruction with the Brostrom-Gould procedure (direct repair of ATFL/CFL augmented by the inferior extensor retinaculum) or allograft/tendon augmentation for failed primary repairs.
12 Ankle Arthritis, Impingement & Osteochondral Lesions Ankle
Ankle osteoarthritis is predominantly post-traumatic (in contrast to hip and knee OA, which are primary). Presents with deep anterior ankle pain, morning stiffness, reduced dorsiflexion, and gradual loss of function.
Options: shoe modifications, rocker-bottom soles, ankle-foot orthoses (AFOs), corticosteroid injection, arthroscopic debridement, total ankle arthroplasty (TAR/TAA) in appropriately selected patients (preserves motion), or ankle arthrodesis (gold standard for younger high-demand patients, sacrifices motion for durability).
Anterior ankle impingement ("footballer's ankle") is tibiotalar osteophyte formation producing pain at terminal dorsiflexion. Common in athletes. Treated with arthroscopic debridement of osteophytes. Posterior ankle impingement involves an os trigonum or large posterior talar process getting compressed between tibia and calcaneus in plantarflexion (classic in ballet dancers).
Osteochondral lesion of the talus (OLT/OCD) is a focal injury to the talar dome cartilage and underlying bone, usually from an ankle sprain or trauma. Medial lesions are more common and deeper; lateral lesions are more often traumatic and shallower. MRI is the imaging of choice. Treatment: immobilization for small stable lesions, arthroscopic debridement and microfracture for small unstable lesions, and osteochondral autograft/allograft (OATS, allograft plug) for larger lesions.
13 Foot & Ankle Fractures Trauma
Know these specific fracture patterns cold:

Ankle fractures: Classified by the Weber system (based on fibula fracture level relative to the syndesmosis: A = below, B = at, C = above) and the Lauge-Hansen system (mechanism-based: supination-adduction, supination-external rotation, pronation-abduction, pronation-external rotation). Unstable patterns (bimalleolar, trimalleolar, Weber C) typically require ORIF.
Pilon fracture: High-energy tibial plafond fracture from axial load. Distinct from ankle fractures.
Calcaneal fracture: Usually from fall from height. Sanders classification based on CT coronal plane. Compartment syndrome risk in the foot. Often treated non-op due to soft-tissue concerns; ORIF via extensile lateral or sinus tarsi approach.
Talar neck fracture: Hawkins classification (I–IV) — high risk of avascular necrosis (AVN). Hawkins sign (subchondral lucency at 6–8 weeks on X-ray) predicts intact vascularity.
Lisfranc injury: Tarsometatarsal joint disruption. Mechanism: axial load on plantarflexed foot. Classic sign: plantar ecchymosis, widening between the 1st and 2nd metatarsal bases > 2 mm, "fleck sign" (avulsion fragment). Weight-bearing films mandatory — non-weight-bearing films miss subtle injuries. Treatment: ORIF with screws or plates, or primary arthrodesis for severe ligamentous injuries.
Jones fracture: Fracture at the metadiaphyseal junction of the 5th metatarsal (Zone 2). High non-union rate due to watershed blood supply. Often treated with intramedullary screw fixation in athletes. Distinct from avulsion fractures of the 5th metatarsal base (Zone 1, "dancer's fracture"), which heal reliably with symptomatic treatment.
Metatarsal stress fracture: Classic "march fracture" of the 2nd or 3rd metatarsal neck in runners, soldiers, or dancers. Initially invisible on X-ray; MRI or bone scan confirms. Treated with activity modification and stiff-sole shoe or walking boot.
Imaging workflow: Ottawa ankle/foot rules decide if plain films are needed; for suspected Lisfranc or stress fracture, weight-bearing views and often CT or MRI are required. Document mechanism of injury, ability to weight-bear, neurovascular status, and soft tissue condition (open vs closed, fracture blisters, skin tenting).
14 Turf Toe, Sesamoiditis & First Ray Injuries Forefoot
Turf toe is a sprain of the plantar plate and capsule of the first MTP joint from hyperdorsiflexion of the great toe, classically in football players on artificial turf. Graded I–III. Management: grade I in stiff-sole shoe with taping; grade III with plantar plate repair for severe instability or retraction.
Sesamoiditis is inflammation/stress reaction of the tibial (medial) or fibular (lateral) hallucal sesamoid. Presents with plantar first MTP pain, worse with push-off. Differential includes sesamoid stress fracture, bipartite sesamoid, and AVN. Management: dancer's pad or orthotic with sesamoid cutout, activity modification, walking boot, NSAIDs. Sesamoidectomy for refractory cases — preserve at least one sesamoid to avoid hallux deformity.
15 Nail & Skin Pathology Dermatology
Onychocryptosis (ingrown toenail) is among the most common office procedures in podiatry. The nail border penetrates the soft tissue of the nail fold producing pain, erythema, and often infection with granulation tissue.

Caused by improper nail trimming (rounding the corners), tight shoes, nail pathology, or trauma. Management: warm soaks and proper nail care for mild cases; partial nail avulsion with or without chemical matricectomy using phenol for recurrent or severe cases (matricectomy destroys the germinal matrix to prevent regrowth).
Onychomycosis is fungal infection of the nail, most commonly distal-lateral subungual (Trichophyton rubrum). Thickened, yellow, crumbly, dystrophic nails. Confirm with KOH prep, PAS stain, fungal culture, or PCR before systemic therapy. Topical: efinaconazole, ciclopirox, tavaborole (low efficacy but safe). Oral: terbinafine 250 mg daily for 12 weeks (fingernails 6 weeks) is first-line; check baseline LFTs. Itraconazole pulse therapy is an alternative.
Paronychia is infection of the nail fold (bacterial, usually S. aureus). Treated with warm soaks, topical/oral antibiotics, and I&D if fluctuant.
Plantar warts (verrucae) are HPV infections of the sole. Treat with salicylic acid, cryotherapy, cantharidin, curettage, or laser. Corns and calluses (hyperkeratoses) are protective thickenings over bony prominences; debridement is a routine podiatric procedure ("nails and callus" or "routine foot care"). Blisters and plantar fibroma (Ledderhose disease) (nodular thickening of the plantar fascia, analog of Dupuytren) round out common dermatologic complaints.
16 Diabetic Foot Disease & Charcot Neuroarthropathy Diabetic
Diabetic foot disease is the single highest-stakes domain in podiatry. It is the leading cause of non-traumatic lower extremity amputation worldwide. The pathogenic triad is neuropathy (loss of protective sensation), ischemia (PAD reducing perfusion and healing), and deformity (biomechanical overload creating pressure points and ulcers). Secondary infection and poor glycemic control drive progression to amputation.

Diabetic Foot Ulcer Classification
Two classification systems dominate. Use whichever matches the surgeon's preference.
Grade 0: Intact skin, at-risk foot (deformity, callus)
Grade 1: Superficial ulcer, full skin thickness, no deeper structures
Grade 2: Deep ulcer into tendon, capsule, or bone without osteomyelitis
Grade 3: Deep ulcer with abscess, osteomyelitis, or joint sepsis
Grade 4: Localized gangrene (toe, forefoot, heel)
Grade 5: Gangrene of entire foot
Two-axis system: Grade (depth) × Stage (infection/ischemia).
Grades: 0 = pre/post-ulcer lesion, 1 = superficial, 2 = to tendon or capsule, 3 = to bone or joint.
Stages: A = clean, B = infected, C = ischemic, D = infected & ischemic.
Example: "UT 2B" = ulcer to tendon with infection. UT 3D carries the worst prognosis. The UT system predicts amputation risk better than Wagner.
Diabetic Foot Infection (DFI) Severity
The IDSA/IWGDF DFI guidelines grade infection from uninfected through severe sepsis using PEDIS criteria:
| PEDIS Grade | IDSA Severity | Clinical Features |
|---|---|---|
| 1 | Uninfected | No purulence or inflammation |
| 2 | Mild | Local infection, erythema ≤ 2 cm from ulcer, skin/subcutaneous only |
| 3 | Moderate | Erythema > 2 cm or deeper structures (tendon, bone, joint), no systemic signs |
| 4 | Severe | Systemic inflammatory response (SIRS)/sepsis |
Osteomyelitis in the diabetic foot is evaluated with the probe-to-bone test (probing a sterile metal probe into the wound: positive = high likelihood of osteo), plain radiographs (lag behind disease by 2 weeks), MRI (gold standard), and bone biopsy for definitive diagnosis and culture-directed therapy. Inflammatory markers (ESR > 70 mm/h, CRP) support the diagnosis.
Charcot Neuroarthropathy
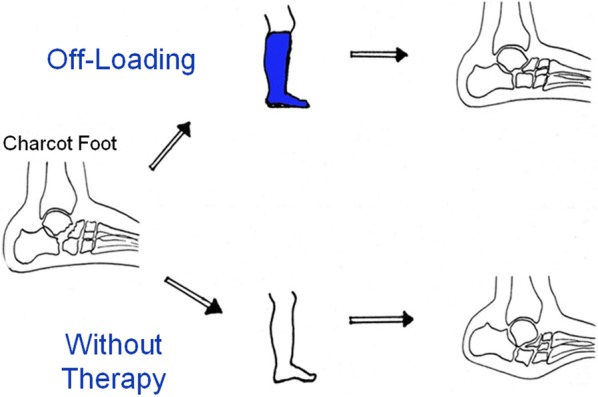
Charcot foot is a destructive neuroarthropathy in the neuropathic patient, classically following a minor unrecognized trauma. The classic presentation is a unilateral, red, hot, swollen foot in a diabetic with neuropathy — often mistaken for cellulitis or DVT. The key differentiator: elevation reduces erythema in Charcot (vascular dependency) but not in cellulitis.
Stage 0 (prodromal): Clinical signs (red, hot, swollen) without radiographic changes. MRI shows marrow edema. This is the ideal window to intervene.
Stage 1 (fragmentation): Joint dislocation, bony fragmentation, debris formation. Foot is unstable.
Stage 2 (coalescence): Decreased warmth/swelling, resorption of debris, early healing.
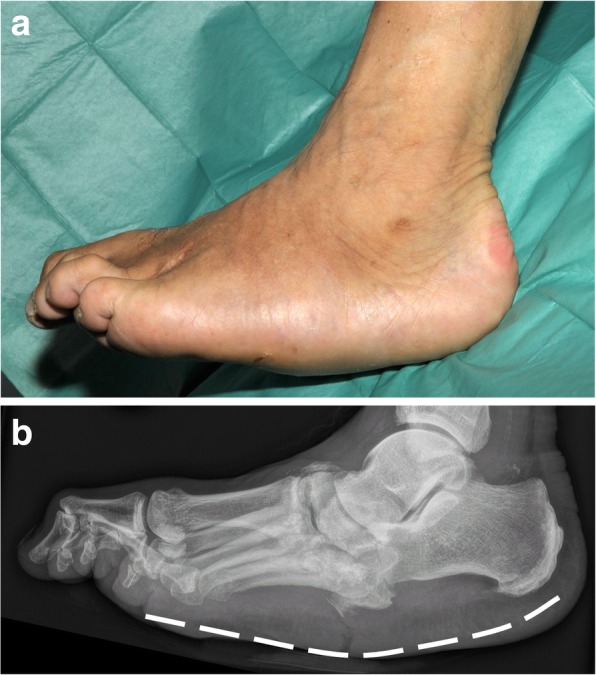
Stage 3 (reconstruction/consolidation): Remodeling complete, stable but deformed foot. Rocker-bottom deformity is the classic end stage.
Management: immediate immobilization and offloading with total contact casting (TCC) is the gold standard for active Charcot (stages 0–1), continued until the foot is "quiet" (less than 2°C warmer than the contralateral foot). Total duration averages 3–6 months. Surgical reconstruction (exostectomy, midfoot or hindfoot fusion with beaming/bolting) is reserved for unstable or ulcerating deformities.
Offloading & Wound Management
Offloading is the single most important treatment for a diabetic foot ulcer — no dressing or antibiotic works if the ulcer keeps getting stepped on. IWGDF offloading guidelines rank options by effectiveness: non-removable knee-high device (TCC or irremovable walker) is first-line; removable cast walker second; therapeutic shoes and felted foam for patients who cannot tolerate a boot. Sharp debridement of callus and non-viable tissue at every visit is standard. Advanced wound therapies: negative pressure wound therapy (wound VAC), bioengineered skin substitutes (Apligraf, Dermagraft), hyperbaric oxygen therapy for selected Wagner 3 ulcers, and skin grafting or flap reconstruction for large defects.
Every diabetic ulcer note should explicitly document: (1) ulcer dimensions in cm (L x W x D), (2) wound bed (granular, fibrous, necrotic, percent each), (3) drainage (none/scant/moderate/copious, serous/sanguineous/purulent), (4) odor, (5) periwound skin (intact, macerated, erythematous, callused), (6) probe-to-bone result, (7) classification (Wagner and/or UT), (8) offloading device in place, and (9) signs of infection. Surgeons and wound care centers require all nine elements.
17 Peripheral Arterial Disease & the Dysvascular Foot Vascular
Podiatry and vascular surgery overlap extensively. A podiatrist cannot heal a wound in an ischemic foot — revascularization comes first. Every new diabetic foot patient, every non-healing wound patient, and every chronic rest pain patient needs a vascular assessment: pulses, ABI (or TBI if ABI is non-compressible), and vascular surgery consultation if perfusion is inadequate.
Key thresholds: ABI < 0.9 confirms PAD; ABI < 0.5 represents critical limb ischemia; toe pressure < 30 mmHg or TcPO2 < 30 mmHg predicts poor wound healing. Diabetics commonly have non-compressible ABIs (> 1.3) from medial calcification, so toe pressures and TBI are more reliable. Referral to vascular surgery is indicated whenever healing is inadequate, baseline perfusion is suspicious, or the wound is failing to progress after 4 weeks of optimal care.
Rest pain (forefoot pain at night relieved by dangling the leg), dry gangrene (black mummified tissue), wet gangrene (infected, foul-smelling, spreading), absent pulses with a new or worsening ulcer, ABI < 0.4 or toe pressure < 30 mmHg, and blue toe syndrome (acute digital ischemia from microemboli). Any of these should trigger same-day vascular surgery contact. Document the time of contact and the recommendation in the note.
The SVS WIfI classification (Wound, Ischemia, foot Infection) is used by vascular surgeons to stratify amputation risk. Podiatry notes on dysvascular wounds should document each of the three domains so the vascular team can apply WIfI directly.
18 Nerve Entrapments & Neuropathic Foot Pain Nerve
Nerve entrapments of the foot and ankle are under-recognized causes of chronic pain and often masquerade as tendinopathy or fasciitis. Always consider a nerve etiology when pain is burning, electric, or associated with numbness.
Tarsal tunnel syndrome is compression of the tibial nerve (or its medial/lateral plantar branches) under the flexor retinaculum behind the medial malleolus. Presents with burning, tingling, and numbness of the plantar foot, often worse at night. Positive Tinel sign at the tarsal tunnel. EMG/NCS can confirm. Management: NSAIDs, orthotics to control pronation, corticosteroid injection, and tarsal tunnel release for refractory cases with a clear compressive etiology.
Baxter nerve entrapment (first branch of lateral plantar nerve) is a mimic of plantar fasciitis with medial heel pain and occasionally motor weakness of the abductor digiti quinti. Sinus tarsi syndrome is persistent lateral hindfoot pain over the sinus tarsi after an ankle sprain, treated with injection and orthotics. Diabetic peripheral neuropathy is managed with glycemic control, gabapentin, pregabalin, duloxetine, or amitriptyline. Topical capsaicin and lidocaine patches are adjuncts.
19 Pediatric & Congenital Foot Conditions Pediatric

Podiatrists see pediatric patients for congenital and developmental deformities. Key entities: pes planus (flatfoot) — flexible (arch returns with heel rise or toe standing — usually physiologic and asymptomatic, no treatment needed) vs. rigid (arch absent in all positions, often from tarsal coalition — requires imaging and surgical evaluation); pes cavus (high arched foot, often neurologic — screen for Charcot-Marie-Tooth); accessory navicular (extra ossicle at the PTT insertion causing medial pain, treated with immobilization then Kidner procedure if refractory); tarsal coalition (congenital fibrous, cartilaginous, or osseous bridge between tarsal bones — calcaneonavicular and talocalcaneal are the most common, present in adolescence with rigid flatfoot and peroneal spasm); clubfoot (talipes equinovarus) (managed with the Ponseti method); and equinus deformity (restricted dorsiflexion from gastrocnemius contracture, addressed with Silfverskiold test to differentiate isolated gastroc tightness from combined gastroc-soleus, and gastrocnemius recession if isolated).
20 Podiatric Procedures — A to Z Procedures
The core podiatric procedural repertoire. Know these by name; the surgeon will dictate them in shorthand.

Office-Based Procedures
| Procedure | Description | Common Indications |
|---|---|---|
| Partial nail avulsion | Removal of ingrown nail border under digital block | Onychocryptosis |
| Matricectomy (phenol) | Chemical ablation of nail matrix after partial avulsion | Recurrent onychocryptosis |
| Nail debridement | Reduction of thickened mycotic nails | Onychomycosis, onychogryphosis |
| Callus/corn debridement | Sharp reduction of hyperkeratotic tissue | Hyperkeratoses, IPKs, heloma |
| I&D | Incision and drainage of abscess or paronychia | Abscess, infected paronychia |
| Wound debridement | Sharp debridement of nonviable tissue | Diabetic ulcer, pressure ulcer |
| Corticosteroid injection | Intra-articular, intralesional, or soft-tissue injection | Plantar fasciitis, neuroma, joint OA, plantar fibroma |
| Digital/ankle block | Local anesthesia with lidocaine or bupivacaine | Prior to any procedure |
| Nail biopsy | Longitudinal biopsy of nail unit | Suspected subungual melanoma, dystrophy |
| Strapping/padding | Low-Dye taping, J-pads, metatarsal pads | Plantar fasciitis, neuroma, metatarsalgia |
Forefoot Surgery
| Procedure | Key Details |
|---|---|
| Austin (Chevron) bunionectomy | Distal first MT V-cut osteotomy + screw fixation; mild-moderate bunion |
| Scarf bunionectomy | Z-shaped diaphyseal osteotomy; moderate deformity |
| Lapidus | Arthrodesis of 1st TMT joint; moderate-severe with hypermobility |
| Akin osteotomy | Medial closing wedge of proximal phalanx; adjunct to correct hallux interphalangeus |
| Keller arthroplasty | Resection of base of proximal phalanx; elderly salvage |
| First MTP arthrodesis | Fusion for hallux rigidus grade 3–4 or severe HV + arthritis |
| Cheilectomy | Dorsal osteophyte excision; hallux rigidus grade 1–2 |
| PIP arthroplasty/arthrodesis | Hammertoe correction |
| Weil osteotomy | Lesser MT head shortening for metatarsalgia or dislocated MTP |
| Morton neurectomy | Excision of common digital nerve (dorsal or plantar approach) |
Hindfoot & Ankle Surgery
| Procedure | Key Details |
|---|---|
| Plantar fasciotomy | Open, percutaneous, or endoscopic release of medial band |
| Gastrocnemius recession (Strayer) | Lengthening of gastroc aponeurosis for isolated equinus |
| Achilles lengthening (TAL) | Percutaneous tripling cuts for gastroc-soleus equinus |
| Achilles repair | Open, percutaneous (PARS), or mini-open for rupture |
| Brostrom-Gould | ATFL/CFL repair + extensor retinaculum augmentation; chronic lateral instability |
| FDL transfer + MCO | Stage II flatfoot reconstruction |
| Evans osteotomy | Lateral column lengthening for flatfoot |
| Cotton osteotomy | Medial cuneiform opening wedge for residual forefoot varus |
| Subtalar arthrodesis | Fusion for hindfoot arthritis, stage III PTTD |
| Triple arthrodesis | Fusion of TN + CC + ST joints for rigid deformity/arthritis |
| Ankle arthroscopy | Debridement of impingement, OLT, loose bodies |
| ORIF ankle fracture | Plate/screw fixation, syndesmotic screws if positive stress test |
| Total ankle arthroplasty (TAR) | Motion-preserving for end-stage ankle OA |
| Ankle arthrodesis | Tibiotalar fusion for end-stage ankle OA |
Diabetic Foot & Amputations
| Procedure | Description / Indication |
|---|---|
| Toe amputation | Digital amputation for gangrene/osteo of a toe |
| Ray amputation | Removal of a toe + metatarsal; common for 1st or 5th ray DFI |
| Transmetatarsal amputation (TMA) | Amputation through the metatarsal shafts; requires TAL to prevent equinovarus |
| Syme amputation | Ankle disarticulation with heel pad preservation |
| Below-knee amputation (BKA) | Referenced to orthopedics/vascular when TMA fails |
| Total contact casting | Non-removable knee-high offloading cast for neuropathic ulcer |
| External fixation / Charcot reconstruction | Beaming, bolting, midfoot/hindfoot fusion for unstable Charcot |
21 Imaging & Diagnostics Imaging
Weight-bearing X-rays are the cornerstone of podiatric imaging. Non-weight-bearing films miss deformity, undersell arch collapse, and hide Lisfranc injuries. Standard views: AP (DP), lateral, and oblique for the foot; AP, mortise, and lateral for the ankle; sesamoid axial for first MTP assessment.
MRI is the modality of choice for soft-tissue pathology: tendon tears (PTT, Achilles, peroneal), plantar plate injury, stress fractures, osteomyelitis, Morton neuroma, OLT, and Charcot marrow edema. Contrast adds value for osteomyelitis and tumor. CT excels for complex fracture characterization (calcaneus, Lisfranc, pilon), tarsal coalition, and preoperative planning. Ultrasound is used for dynamic tendon evaluation, plantar fascia measurement (> 4 mm is abnormal), Morton neuroma, ganglion cysts, and ultrasound-guided injections. Bone scan detects stress fractures, osteomyelitis, and Charcot when MRI is contraindicated. Vascular studies: ABI, TBI, pulse volume recordings, arterial duplex, and CTA when PAD is suspected.
22 Medications You Must Know Meds
| Class | Drugs (Generic / Brand) | Use / Notes |
|---|---|---|
| NSAIDs | Ibuprofen, naproxen, meloxicam, diclofenac (PO/topical Voltaren gel) | First-line analgesia; topical for localized tendinopathy/OA |
| Corticosteroid injections | Triamcinolone (Kenalog) 10–40 mg, methylprednisolone (Depo-Medrol), dexamethasone | Plantar fascia, neuroma, joints, intralesional; avoid Achilles and weight-bearing tendons |
| Local anesthetics | Lidocaine 1–2% (with/without epi), bupivacaine (Marcaine), ropivacaine | Digital and ankle blocks. Never use epinephrine in digital blocks (historical dogma relaxing, but still standard practice). |
| Oral antibiotics (mild-mod DFI) | Cephalexin, amoxicillin-clavulanate, clindamycin, doxycycline, trimethoprim-sulfamethoxazole, ciprofloxacin + metronidazole | Cover strep/MSSA; add MRSA (doxy, TMP-SMX, clindamycin) and gram-neg/anaerobes for moderate infection |
| IV antibiotics (severe DFI) | Vancomycin + piperacillin-tazobactam, ceftriaxone, meropenem, daptomycin, linezolid | Sepsis, limb-threatening infection, prior hospitalization, resistant organisms |
| Topical antifungals | Efinaconazole (Jublia), ciclopirox (Penlac), tavaborole, terbinafine cream | Onychomycosis (limited efficacy), tinea pedis |
| Oral antifungals | Terbinafine 250 mg daily x 12 wk (first-line), itraconazole pulse | Check baseline LFTs. Fluconazole is second-line. |
| Keratolytics | Salicylic acid 17–40% (plasters, pads), urea 20–40% cream | Calluses, warts, xerotic skin, hyperkeratotic nails |
| Neuropathic pain | Gabapentin, pregabalin (Lyrica), duloxetine, amitriptyline | Diabetic peripheral neuropathy, post-op nerve pain |
| Gout therapy | Colchicine, indomethacin, prednisone (acute); allopurinol, febuxostat (chronic urate lowering) | Common podiatry presentation at first MTP |
| Biologics/PRP | Platelet-rich plasma, amniotic tissue products | Chronic tendinopathy, plantar fasciitis, select wounds |
| Tetanus | Tdap booster | Any puncture wound, ulcer, or trauma if > 5 years since last |
| Anticoagulants | Enoxaparin, aspirin, DOACs | VTE prophylaxis after foot/ankle surgery for high-risk patients |
23 Classification Systems Reference
Podiatric practice leans heavily on classification systems. The surgeon will name-drop these and you must chart them correctly.
Weber A: Fibular fracture below the syndesmosis. Syndesmosis intact. Usually stable. Non-operative.
Weber B: Fibular fracture at the syndesmosis. Syndesmosis may be intact or partially disrupted. Stability varies. Often ORIF.
Weber C: Fibular fracture above the syndesmosis (Maisonneuve pattern if proximal fibula). Syndesmosis disrupted. Unstable. ORIF + syndesmotic fixation.
Mechanism-based; names the foot position first and the deforming force second.
SER (supination-external rotation): Most common (40–70%). 4 stages: AITFL tear → spiral fibula fx → PITFL or posterior malleolus → medial malleolus.
SAD (supination-adduction): Transverse fibula fx below plafond + vertical medial malleolus fx.
PER (pronation-external rotation): Medial mal or deltoid first → AITFL → high fibula fx → PITFL. Maisonneuve pattern.
PAB (pronation-abduction): Medial mal or deltoid → AITFL → transverse fibula fx at plafond.
Ankle X-ray required if pain in the malleolar zone AND any of: bony tenderness at posterior edge or tip of lateral or medial malleolus, OR inability to weight-bear four steps both immediately and in the ED.
Foot X-ray required if pain in the midfoot zone AND any of: bony tenderness at the base of the 5th metatarsal or navicular, OR inability to weight-bear four steps.
Grade 0: Normal.
Grade I: Cartilage softening and swelling.
Grade II: Partial-thickness fissures < 1.5 cm diameter.
Grade III: Fissuring to subchondral bone > 1.5 cm diameter.
Grade IV: Exposed subchondral bone.
AOFAS scores: Ankle-Hindfoot, Midfoot, Hallux MTP-IP, Lesser MTP-IP — 100-point clinician-reported outcome scales combining pain, function, and alignment.
Manchester scale for hallux valgus: Photographic comparison (none, mild, moderate, severe) used in screening.
Beighton hypermobility score (0–9): Thumb-to-forearm, 5th finger > 90° hyperextension, elbow hyperextension, knee hyperextension, palms flat on floor with straight knees. ≥ 4 = hypermobile.
Coughlin-Mann hallux valgus grading: Mild (HVA < 20, IMA < 11), moderate (HVA 20–40, IMA 11–16), severe (HVA > 40, IMA > 16).
24 Physical Exam, Abbreviations & Sample HPIs Reference
Physical Exam Template
Vascular: DP 2+/2+, PT 2+/2+, cap refill < 3 sec, no dependent rubor, no edema
Neuro: Protective sensation intact to 10-g monofilament at all 5 plantar sites bilaterally
Vibratory sense intact with 128-Hz tuning fork, Achilles reflex 2+
Derm: Skin intact, no ulcerations, nails clear, mild hyperkeratosis 1st/5th MT heads
MSK: Gait nonantalgic, alignment neutral, full ROM ankle/STJ/1st MTP
Strength 5/5 dorsiflexion, plantarflexion, inversion, eversion
Tenderness: focal medial calcaneal tubercle, negative squeeze test
Special: positive windlass test, negative Mulder click, negative Thompson test
Risk Factors & Comorbidities to Document on Every Patient
Diabetes mellitus: type, A1C, duration, complications (neuropathy, retinopathy, nephropathy, prior ulcers, prior amputations). The strongest predictor of future amputation is a prior amputation.
Peripheral arterial disease: palpable DP/PT, prior ABI/TBI, prior revascularization, claudication distance, rest pain.
Peripheral neuropathy: diabetic, alcoholic, chemotherapy-induced, hereditary (CMT), or idiopathic. Document protective sensation with monofilament testing.
Smoking: pack-years, current vs former. Impairs wound healing, increases surgical complications, and accelerates PAD.
Immunosuppression: chronic steroids, biologics (TNF inhibitors), chemotherapy, HIV, transplant. Masks infection and impairs healing.
Inflammatory arthritis: rheumatoid arthritis, psoriatic arthritis, gout, CPPD. Often cause forefoot deformity, tendon ruptures, and joint destruction.
Prior foot surgery, shoe gear, activity level, and occupation: prolonged standing occupations have a high plantar fasciitis incidence; construction workers need steel-toe boot considerations.
Abbreviations Master List
Sample HPI Templates
"Ms. [Name] is a 54-year-old female presenting with a 5-year history of progressive right great toe deformity and medial forefoot pain. She reports a prominent bunion that has enlarged over the past 2 years, now painful with any closed-toe shoe and preventing her from wearing her usual work shoes. Pain is rated 6/10 at worst, aggravated by prolonged standing and walking, and relieved with rest, ice, and occasional ibuprofen. She has tried wider shoes, OTC bunion splints, and gel spacers without lasting relief. No prior injections or surgery. She denies numbness, neuropathic symptoms, or transfer metatarsalgia. PMH notable for hypothyroidism only; no diabetes or vascular disease. Weight-bearing X-rays today demonstrate right hallux valgus with HVA 32°, IMA 14°, congruent joint, normal sesamoid position."
"Mr. [Name] is a 46-year-old male, BMI 32, who works as a warehouse manager on his feet 10 hours daily, presenting with 4 months of left medial heel pain. Classic post-static dyskinesia with sharp pain with the first steps in the morning and after prolonged sitting, improving after 5–10 minutes of walking, then worsening by end of day. Pain is focal to the medial plantar heel. He has tried OTC heel cups, ibuprofen, and stretching without adequate relief. Denies radiating pain, numbness, or tingling. Denies trauma. No prior injections. PMH: hypertension. On exam: focal tenderness at the medial calcaneal tubercle, positive windlass test, no swelling, neurovascular intact. X-rays show a plantar calcaneal spur without other abnormality. Assessment: chronic plantar fasciitis refractory to conservative care; will proceed with corticosteroid injection and night splint, continue stretching, and consider custom orthotics."
"Ms. [Name] is a 22-year-old collegiate soccer player who sustained a right ankle inversion injury 2 days ago when she landed awkwardly after heading a ball. She felt a pop along the lateral ankle and was unable to continue playing. She has been using ice, compression, and crutches. Pain is 7/10 with weight-bearing, localized to the lateral ankle. No numbness or prior ankle injury. On exam: diffuse swelling and ecchymosis over the lateral ankle, tenderness over the ATFL and CFL, no tenderness at the fibular head (negative Maisonneuve screen), negative squeeze test, positive anterior drawer. Ottawa ankle rules positive for films. Right ankle X-rays negative for fracture. Assessment: Grade II lateral ankle sprain. Plan: functional rehab, CAM boot for comfort 1–2 weeks, early ROM, peroneal strengthening and proprioception, return to sport in 4–6 weeks."
"Mr. [Name] is a 63-year-old male with long-standing type 2 diabetes mellitus (A1C 9.4%, duration 18 years), peripheral neuropathy with LOPS, hypertension, and 30-pack-year smoking history (active), presenting with a 3-week-old ulcer on the plantar aspect of the right first metatarsal head, first noticed when the sock was bloody. He denies constitutional symptoms, fever, or chills. Previously wore regular sneakers. On exam: 1.2 x 0.8 x 0.3 cm full-thickness plantar ulcer at the right 1st MT head, with surrounding hyperkeratotic border, granular base, scant serous drainage, no purulence, probe-to-bone negative, surrounding skin without erythema or fluctuance. DP and PT pulses palpable bilaterally. Monofilament absent at all 5 plantar sites. X-rays without osteomyelitis. Wagner Grade 1, UT 1A. Plan: sharp debridement of callus and non-viable tissue, saline-moistened dressing, CAM walker for offloading, diabetic shoe referral, vascular labs, and close follow-up in 1 week. Reinforce glycemic control and smoking cessation."
"Ms. [Name] is a 19-year-old female with no significant PMH presenting with 2 weeks of worsening right great toe pain along the medial nail border. She recalls trimming her nail tightly into the corner. Now has redness, swelling, mild drainage, and significant pain with shoe wear. Denies fever or systemic symptoms. No diabetes. On exam: medial nail fold erythema and edema with granulation tissue and scant purulent drainage along the medial hallux border, no fluctuance, no streaking. DP and PT pulses intact, no neuropathy. Assessment: right hallux onychocryptosis with paronychia. Plan: partial nail avulsion with phenol matricectomy performed today under digital block with 1% plain lidocaine. Discussed risks, benefits, and alternatives; informed consent obtained. Post-procedure: petrolatum dressing, daily soaks, keep dry 24 hours, return if worsening. No oral antibiotic indicated."
"Mr. [Name] is a 48-year-old recreational basketball player who felt a sudden pop and sharp pain in the back of the right ankle while pushing off during a pickup game 2 hours ago. He describes feeling as though he was 'kicked' from behind. Unable to push off or walk normally. No prior Achilles symptoms or fluoroquinolone exposure. On exam: palpable 3 cm gap approximately 5 cm proximal to the calcaneal insertion, bruising, and swelling in the posterior calf. Positive Thompson test (no plantarflexion with calf squeeze in prone position). Weak active plantarflexion. Neurovascular intact. Assessment: acute right Achilles tendon rupture, midsubstance. Plan: immobilization in a gravity equinus splint, non-weight-bearing with crutches, urgent MRI, and discussion of operative vs. functional rehabilitation tomorrow in clinic."
Podiatry is deceptively deep. The same patient can have a bunion, a neuroma, a diabetic ulcer, neuropathy, and PAD — all in one visit, each needing its own diagnosis, plan, and documentation. A great podiatry scribe thinks in anatomical columns, captures laterality and dimensions precisely, and never forgets the diabetic foot screen elements. Memorize the classifications, learn the surgeon's preferred phrasing, and always document offloading and wound dimensions precisely when ulcers are involved.
When in doubt, document more. The foot is small, but the documentation is not.
25 References & Sources
Clinical Practice Guidelines
AOFAS Clinical Consensus Statement on Plantar Heel Pain. Foot Ankle Int.
ACFAS Clinical Practice Guidelines on Hallux Valgus. J Foot Ankle Surg.
AAOS Clinical Practice Guideline: Management of Acute Achilles Tendon Rupture. 2019.
NICE Guideline NG19: Diabetic Foot Problems — Prevention and Management.
Stiell IG et al. Implementation of the Ottawa Ankle Rules. JAMA. 1994.
Landmark Publications & Classification Sources
Johnson KA, Strom DE. Tibialis Posterior Tendon Dysfunction. Clin Orthop Relat Res. 1989.
Hawkins LG. Fractures of the Neck of the Talus. J Bone Joint Surg. 1970.
Diagram & Figure Sources
Figure 1: Bones of the Foot. OpenStax College. CC BY 3.0.
Figure 2: Dorsal View of the Foot. Gray's Anatomy. Public domain.
Figure 3: Plantar Fascia & Sole. Gray's Anatomy. Public domain.
Figure 4: Hallux Valgus (Bunion). Blausen Medical. CC BY 3.0.
Figure 5: Plantar Fasciitis Diagram. Injurymap. CC BY-SA 4.0.
Figure 6: Diabetic Foot Ulcer. Wikimedia Commons. CC BY-SA 3.0.
Figure 7: Hammertoe Deformity. Wikimedia Commons. Public domain.
Figure 8: Pes Cavus. Wikimedia Commons. Public domain.