Psychiatry
Every diagnosis, condition, procedure, medication, abbreviation, and documentation framework you need to succeed on day one and beyond.
All diagrams on this page are sourced from published educational or institutional materials rather than AI generation. Each figure caption links to the original source, and the full diagram and guideline citations are collected in the references section at the bottom.
01 Neuroanatomy & Neurotransmitter Essentials
Psychiatry is the medicine of thought, mood, perception, cognition, and behavior. Unlike surgical specialties, psychiatry has no radiographic lesion or palpable mass to diagnose. The "anatomy" of psychiatry is the brain's functional circuitry and its chemical messengers, and a scribe who understands both will write sharper notes and anticipate the clinician's reasoning.
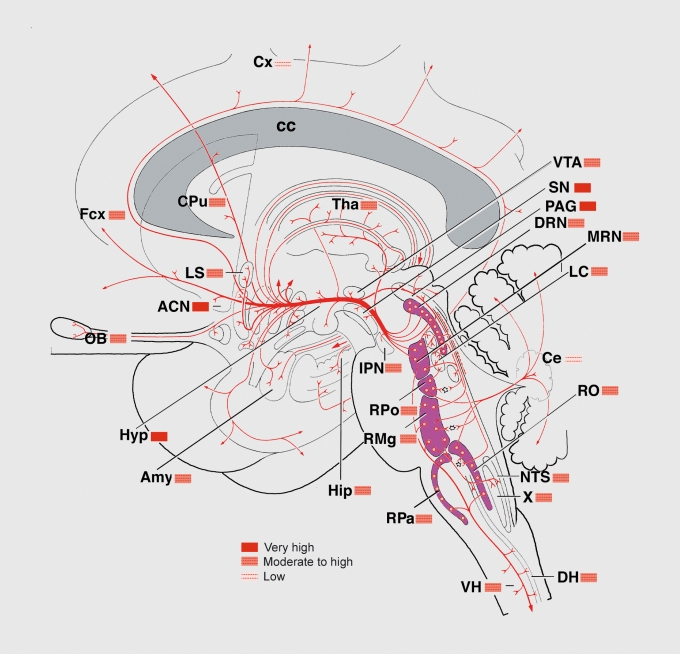
Key Brain Regions
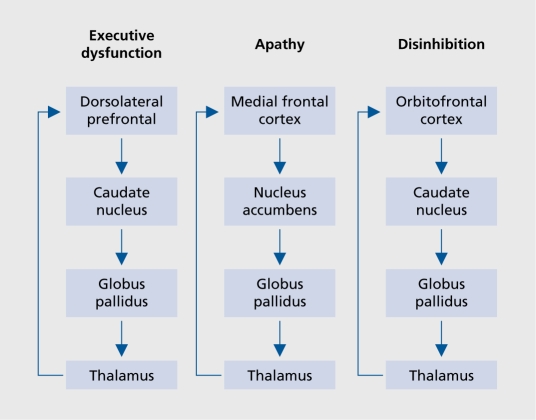
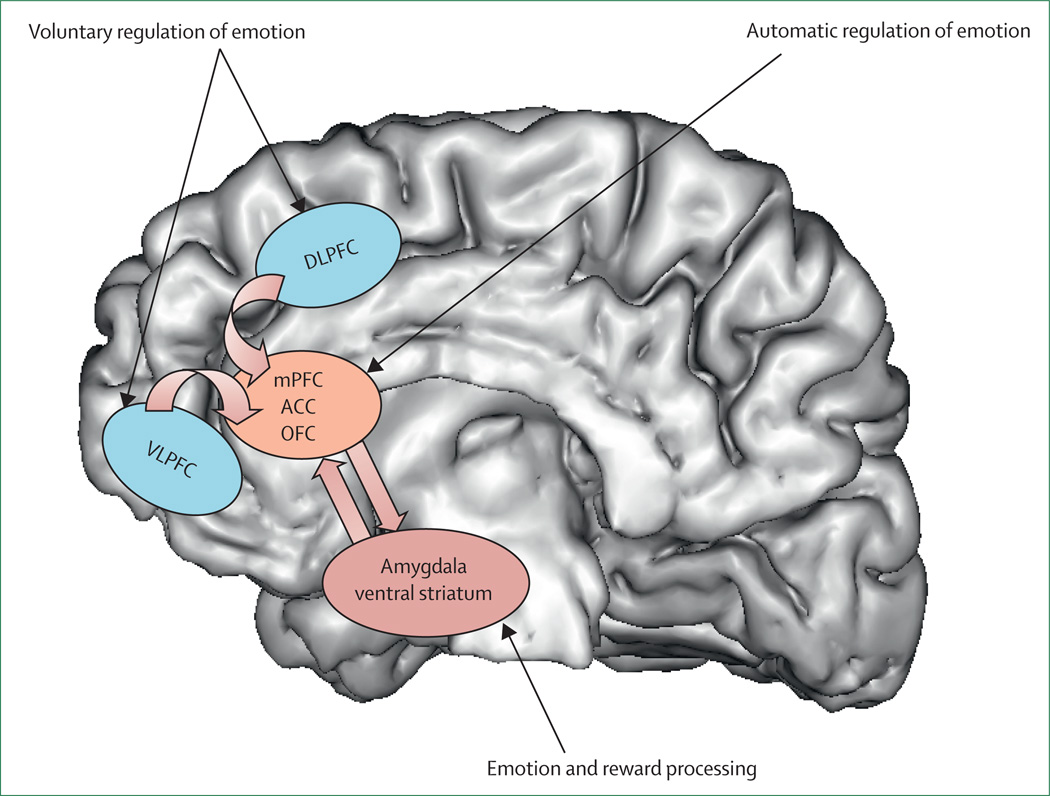
The prefrontal cortex (PFC) governs executive function, impulse control, working memory, and decision-making. Dysfunction here is implicated in ADHD, schizophrenia's negative and cognitive symptoms, depression, and borderline personality disorder. The dorsolateral PFC mediates cognition and planning; the orbitofrontal cortex handles reward valuation and social behavior; the ventromedial PFC regulates emotional responses.
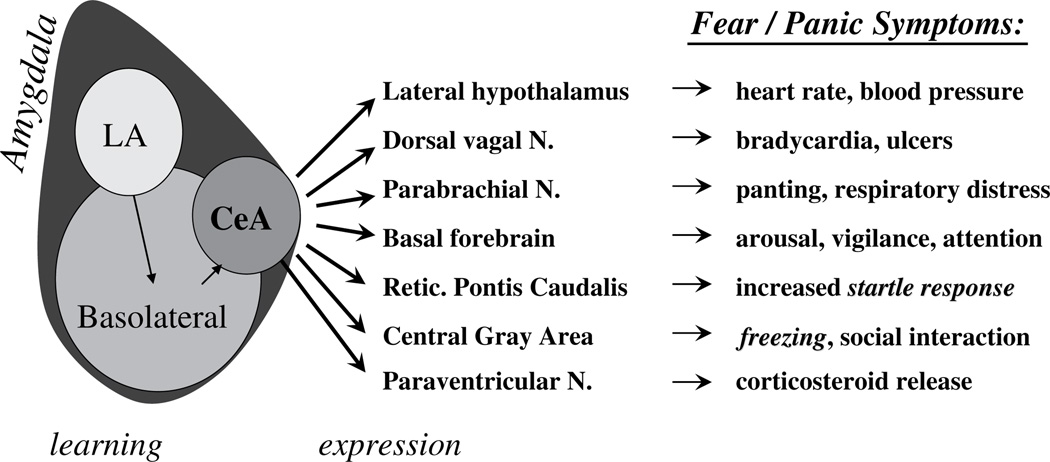
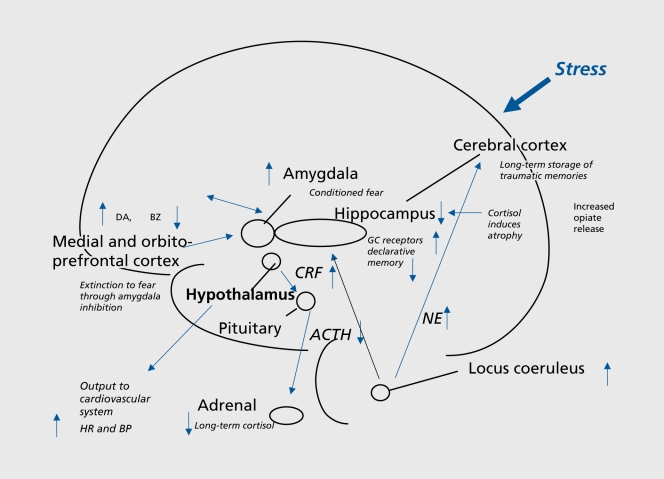
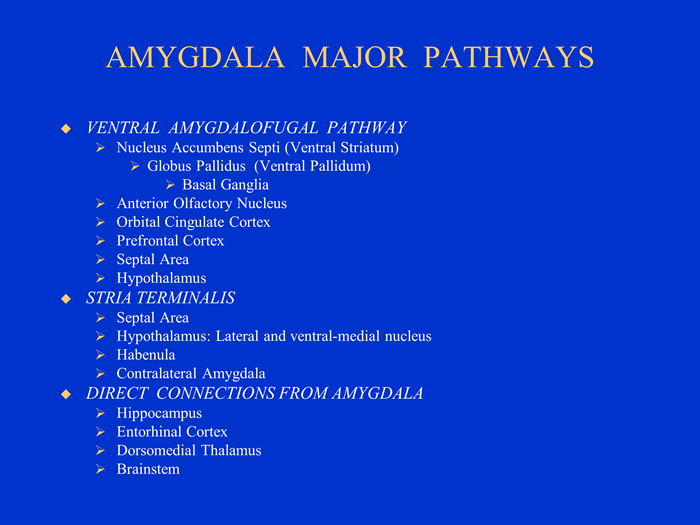
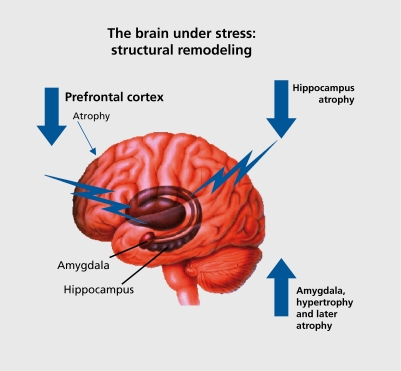
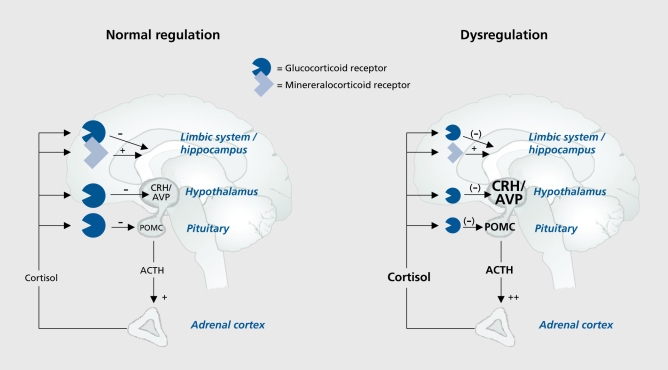
The limbic system is the emotional core of the brain. The amygdala generates fear, threat detection, and emotional memory — it is hyperactive in anxiety disorders and PTSD. The hippocampus encodes declarative memory and is reduced in volume in PTSD, major depression, and Alzheimer disease. The cingulate cortex (anterior and posterior) integrates emotion and cognition; the anterior cingulate is dysregulated in depression and OCD. The hypothalamus drives appetite, sleep, libido, and the hypothalamic-pituitary-adrenal (HPA) stress axis.
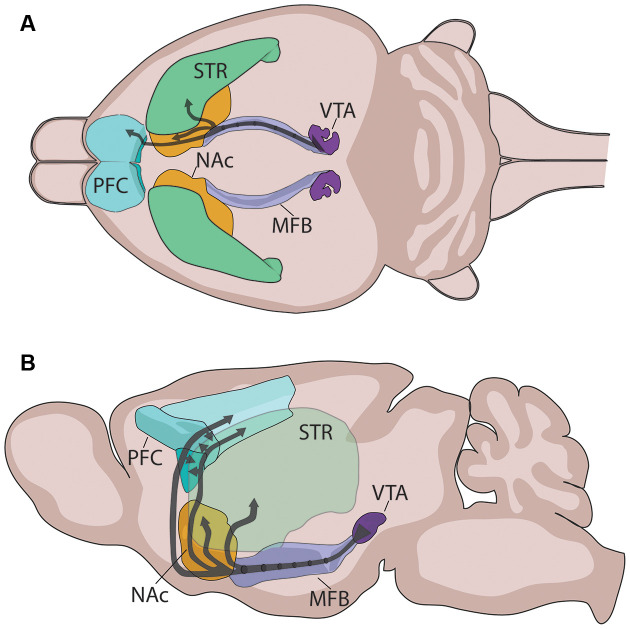
The basal ganglia (caudate, putamen, globus pallidus, substantia nigra, subthalamic nucleus) mediate movement, habit formation, and reward learning. Dopaminergic pathways running through this system are central to schizophrenia, addiction, and movement side effects of antipsychotics. The nucleus accumbens sits at the heart of the reward circuit and is the convergence point for every drug of abuse.
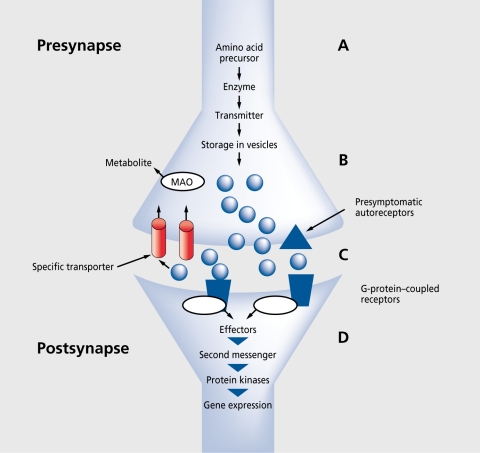
Neurotransmitters — The Chemical Language of Psychiatry
Nearly every psychiatric medication targets one or more neurotransmitter systems. Knowing what each chemical does lets you understand why a drug is chosen and what side effects to expect.
| Neurotransmitter | Primary Functions | Clinical Relevance |
|---|---|---|
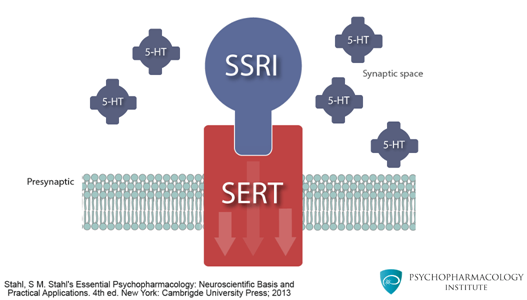
| Serotonin (5-HT) | Mood, anxiety, sleep, appetite, aggression, libido | Target of SSRIs, SNRIs, TCAs, MAOIs, trazodone, vortioxetine |
| Norepinephrine (NE) | Arousal, attention, stress response, vigilance | Target of SNRIs, TCAs, atomoxetine, bupropion (mild), MAOIs |
| Dopamine (DA) | Reward, motivation, motor control, psychosis pathway | Target of all antipsychotics (D2 blockers); stimulants raise DA |
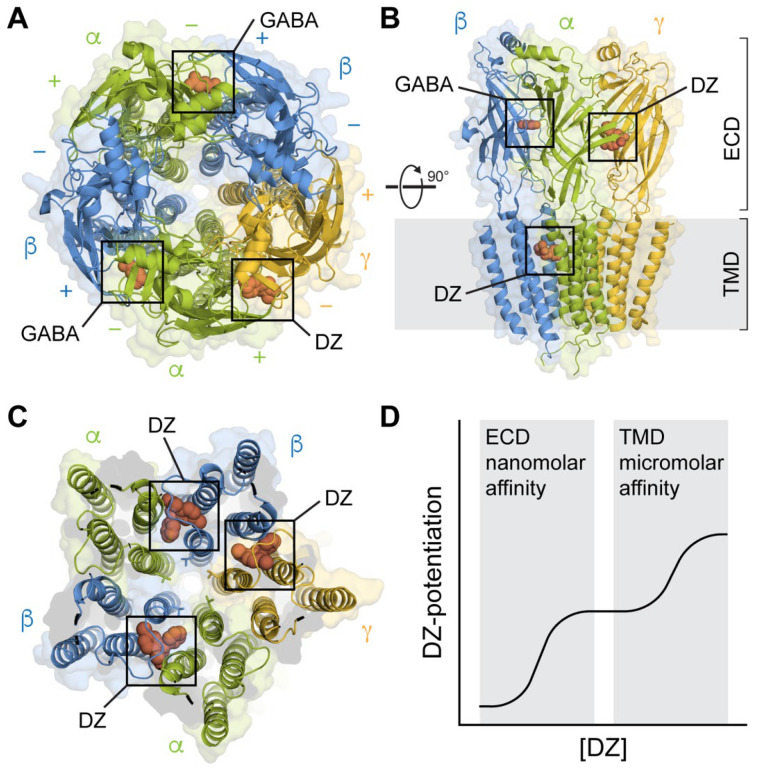
| GABA | Primary inhibitory transmitter, sedation, anxiolysis | Target of benzodiazepines, barbiturates, alcohol, Z-drugs |
| Glutamate | Primary excitatory transmitter, learning, memory | Target of ketamine (NMDA antagonist), memantine, lamotrigine |
| Acetylcholine (ACh) | Cognition, memory, autonomic function | Target of cholinesterase inhibitors; anticholinergic side effects |
| Histamine | Wakefulness, appetite | H1 blockade causes sedation & weight gain (mirtazapine, quetiapine) |
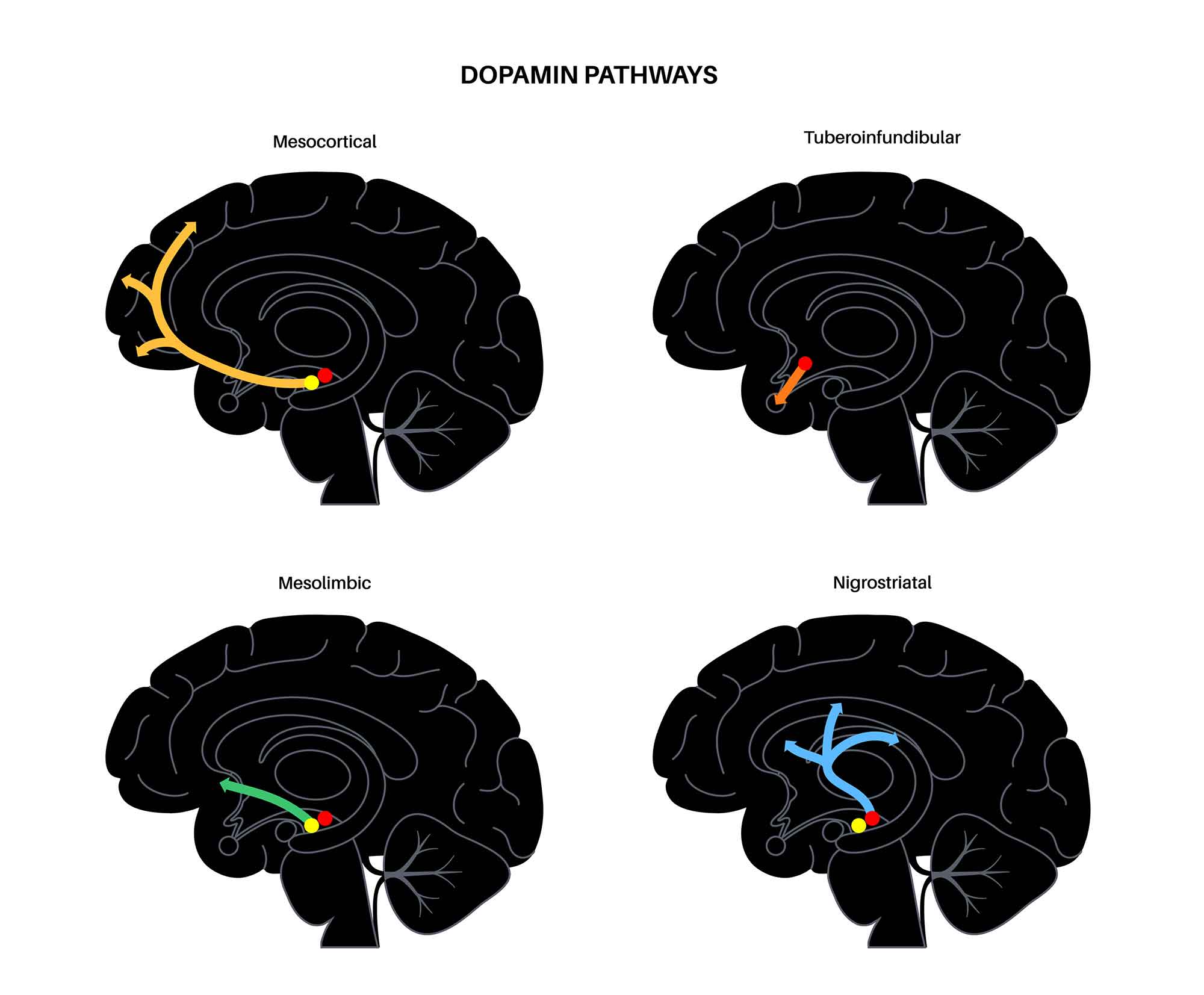
The four dopamine pathways are essential for understanding antipsychotic effects. The mesolimbic pathway (excess DA) produces positive psychotic symptoms; D2 blockade here treats hallucinations and delusions. The mesocortical pathway (reduced DA) is linked to negative and cognitive symptoms. The nigrostriatal pathway controls movement; D2 blockade causes extrapyramidal side effects (EPS). The tuberoinfundibular pathway regulates prolactin; D2 blockade elevates prolactin and causes galactorrhea, amenorrhea, and sexual dysfunction.
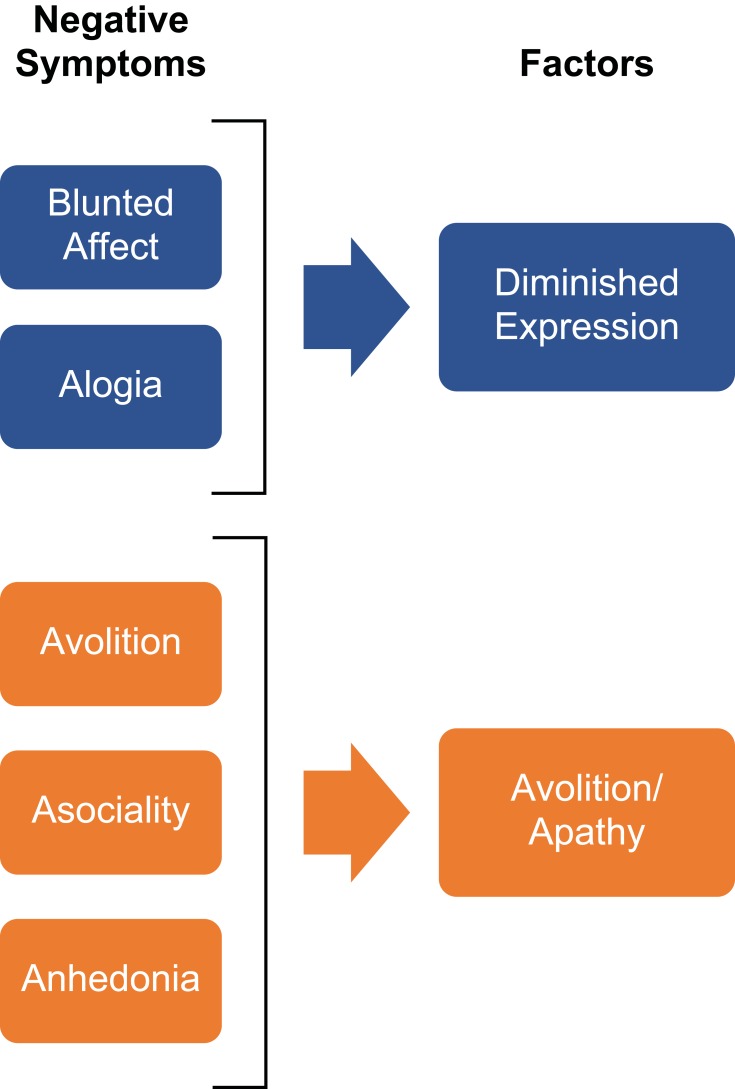
When a psychiatrist says "this patient is having positive symptoms," they mean hallucinations, delusions, or disorganized thinking — things that are added on top of normal experience. "Negative symptoms" are things that are subtracted — flat affect, avolition, alogia, anhedonia, social withdrawal. Chart them as distinct domains, not lumped together.
02 Scribe Documentation Framework & the MSE
The Psychiatric SOAP Note
Psychiatric notes follow SOAP structure but replace the traditional physical exam with a Mental Status Examination (MSE). The assessment often includes a diagnostic formulation and, always, a documented risk assessment.
Chief Complaint (CC): In the patient's own words when possible. "I can't stop crying." "The voices are telling me to hurt myself." "My wife says I've been up for three nights."
HPI: Use OLDCARTS-adapted elements: onset of symptoms, episode duration, associated neurovegetative symptoms (sleep, appetite, energy, concentration, psychomotor changes), psychosocial stressors, precipitating events, prior episodes, response to prior treatment, and functional impact (work, school, relationships, self-care).
Psychiatric ROS: Always screen for depression, mania, anxiety, panic, psychosis, trauma, OCD symptoms, substance use, eating behaviors, and — at every single visit — suicidal and homicidal ideation.
Past Psychiatric Hx, Past Medical Hx, Medications, Allergies, Substance Use Hx, Family Psychiatric Hx, Social Hx (including trauma, abuse, legal, housing, occupation): The social history is far more detailed in psychiatry than in other specialties. Capture childhood history, developmental milestones, education level, relationship status, living situation, supports, and access to firearms.
The MSE is documented in a specific order: Appearance, Behavior, Speech, Mood, Affect, Thought Process, Thought Content, Perception, Cognition, Insight, Judgment. Many clinicians abbreviate this as "ABSMATTPCIJ" or use a standard template.
Vitals & general medical: Weight and BMI (especially on antipsychotics, mood stabilizers, eating disorder patients), vital signs (BP for stimulants and venlafaxine, HR for stimulants), and any relevant physical findings (tardive dyskinesia, tremor, injection site for LAI).
Start with a biopsychosocial formulation naming the primary DSM-5-TR diagnosis with ICD-10 code. Document severity and specifiers (e.g., "Major depressive disorder, recurrent, severe, with anxious distress"). Include an explicit risk assessment: SI, HI, access to means, protective factors, and rationale for disposition. The plan covers medication changes (with rationale), psychotherapy referrals, labs, level of care, safety planning, and follow-up interval.
What Makes a Psychiatric HPI Different
Psychiatric HPIs focus on episodes and timelines. For any mood disorder, you need to document when the current episode started, how long episodes usually last, how many lifetime episodes, and the interval between episodes. For anxiety, document baseline versus flare. For psychosis, anchor to first-break age. Collateral information (family, friends, records) is often critical and should be explicitly attributed (e.g., "per patient's wife").
Every psychiatric note must document suicidal ideation status. Acceptable documentation styles include "Denies SI/HI/AVH" (no ideation, homicidal ideation, or audiovisual hallucinations) or a full C-SSRS entry. Leaving SI/HI blank is never acceptable — it is a liability issue and a quality-of-care issue.
03 Depressive Disorders Mood
Depressive disorders are the highest-frequency diagnosis in outpatient psychiatry. The unifying feature is low mood or anhedonia with functional impairment. Depression is common (lifetime prevalence ~20%), disabling, and treatable — and it is the leading psychiatric risk factor for suicide.
Major Depressive Disorder (MDD)
MDD requires five or more of the DSM-5-TR "SIG E CAPS" symptoms over two weeks, with at least one being depressed mood or anhedonia: Sleep disturbance (insomnia or hypersomnia), Interest loss (anhedonia), Guilt or worthlessness, Energy loss, Concentration impairment, Appetite/weight change, Psychomotor agitation or retardation, and Suicidal ideation. Symptoms must cause functional impairment and not be better explained by substance, medical condition, or bereavement alone.
Specifiers: with anxious distress, with mixed features, with melancholic features, with atypical features, with psychotic features (mood-congruent or incongruent), with catatonia, with peripartum onset, or with seasonal pattern.
The PHQ-9 asks how often, over the past 2 weeks, the patient has experienced each of 9 depressive symptoms (0 = not at all, 1 = several days, 2 = more than half the days, 3 = nearly every day). Total score interpretation:
0–4 none/minimal · 5–9 mild · 10–14 moderate · 15–19 moderately severe · 20–27 severe. Question 9 specifically screens for suicidal ideation and any positive response requires further assessment.
Persistent Depressive Disorder (Dysthymia)
Chronic low-grade depression lasting at least 2 years in adults (1 year in children/adolescents) with at least 2 SIG E CAPS-type symptoms. Patients describe feeling "down" for years. When a major depressive episode is superimposed, this is called "double depression."
Seasonal Affective Disorder (Seasonal Pattern Specifier)
MDD with episodes reliably tied to a season, most commonly fall/winter onset with spring remission. Atypical features (hypersomnia, hyperphagia with carbohydrate craving, weight gain, leaden paralysis) are common. Bright light therapy (10,000 lux, 30 minutes each morning) is first-line, with SSRIs and bupropion XL as adjuncts.
Premenstrual Dysphoric Disorder (PMDD)
Severe affective, behavioral, and somatic symptoms in the luteal phase of most menstrual cycles with resolution within a few days of menses onset. Distinct from PMS by severity and functional impairment. SSRIs are first-line and can be dosed either continuously or only in the luteal phase.
Disruptive Mood Dysregulation Disorder (DMDD)
A pediatric diagnosis (ages 6–18, onset before 10) characterized by severe, recurrent temper outbursts with a persistently irritable/angry mood between outbursts. Created to avoid overdiagnosis of pediatric bipolar disorder.
Management Overview
First-line pharmacotherapy for MDD is an SSRI or SNRI. The APA Practice Guideline for Major Depressive Disorder recommends starting with SSRI/SNRI/bupropion/mirtazapine and combining with evidence-based psychotherapy (CBT, IPT, or behavioral activation). USPSTF 2023 adult depression screening guidance supports universal screening in primary care using the PHQ-9 or similar tool. Treatment-resistant depression (failure of two adequate antidepressant trials) is an indication for augmentation (lithium, T3, atypical antipsychotic), switching classes, ECT, rTMS, or esketamine.
Document all prior antidepressant trials: drug name, dose, duration, response, and reason for discontinuation. This history drives the current treatment decision. A patient who "failed Prozac" after one week at 10 mg has not actually had an adequate trial (6–8 weeks at therapeutic dose).
04 Bipolar & Related Disorders Mood
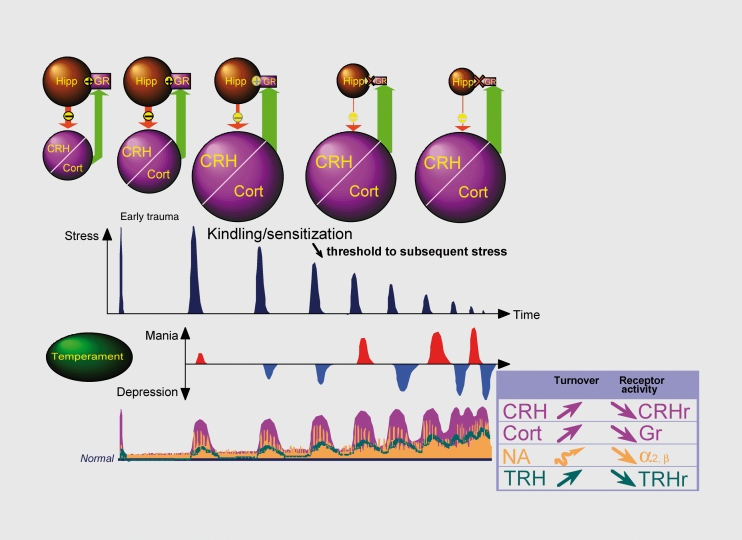
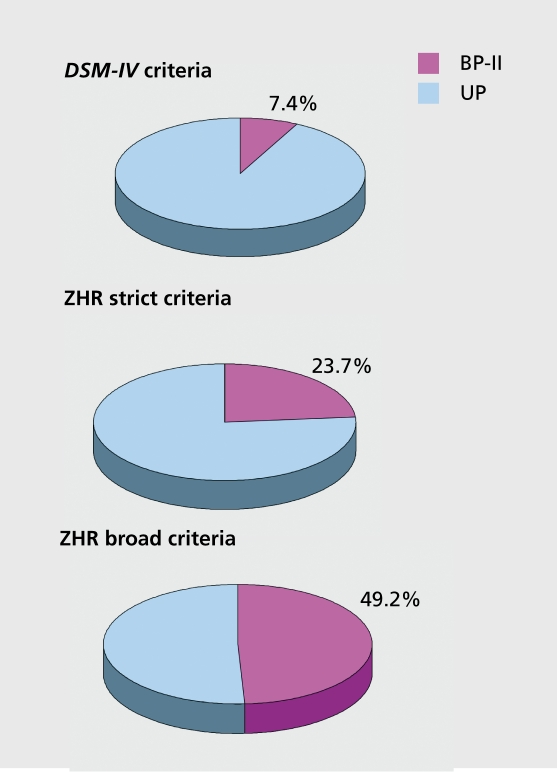
Bipolar disorders are episodic mood disorders defined by the presence of at least one manic (Bipolar I) or hypomanic (Bipolar II) episode, typically interspersed with depressive episodes. Lifetime prevalence is about 1–2%. Bipolar disorder is notoriously underrecognized in primary care because patients usually present during depressive episodes and do not volunteer manic history.
Manic Episode (DIG FAST)
At least 1 week of abnormally elevated, expansive, or irritable mood plus at least 3 (4 if irritable only) of: Distractibility, Insomnia (decreased need for sleep, not insomnia of suffering), Grandiosity, Flight of ideas, Activity increase (goal-directed), Speech (pressured), Thoughtlessness (risky behavior: spending, sex, driving). Must cause marked impairment, hospitalization, or psychotic features. A hypomanic episode is at least 4 days, visible to others, but without marked impairment and no psychosis.
Requires at least one lifetime manic episode. Depressive episodes are common but not required for diagnosis. Psychotic features during mania are common.
At least one hypomanic episode and at least one major depressive episode. Patients usually present during depression. Often misdiagnosed as unipolar MDD until careful history reveals past hypomania.
At least 2 years (1 year in children/adolescents) of numerous periods of hypomanic and depressive symptoms that do not meet full criteria for either episode, with no symptom-free period longer than 2 months.
Management
First-line for acute mania: lithium, valproate, or atypical antipsychotic (olanzapine, risperidone, quetiapine, aripiprazole, asenapine, cariprazine). For bipolar depression, lamotrigine, lurasidone, quetiapine, cariprazine, and lumateperone are evidence-based. Antidepressant monotherapy is contraindicated because of manic switch risk. The CANMAT/ISBD bipolar guidelines and the APA bipolar disorder practice guideline are the major citation sources. Maintenance therapy is lifelong for most Bipolar I patients. Lithium remains the gold standard for preventing suicide in bipolar disorder.
The MDQ (Mood Disorder Questionnaire) is a 13-item yes/no screen. Positive screen: 7+ yes answers AND several occurring at the same time AND moderate/serious problem caused. The YMRS (Young Mania Rating Scale) quantifies manic severity (0–60; >20 indicates significant mania).
05 Anxiety Disorders Anxiety
Anxiety disorders are the most prevalent class of psychiatric conditions (~30% lifetime prevalence). They share a core feature of excessive fear/worry and behavioral avoidance disproportionate to actual threat. DSM-5-TR groups them by the trigger and phenomenology.
Generalized Anxiety Disorder (GAD)
At least 6 months of excessive worry about multiple domains that the patient finds difficult to control, with at least 3 of 6 physical symptoms (restlessness, fatigue, concentration difficulty, irritability, muscle tension, sleep disturbance). The GAD-7 (scores: 0–4 none, 5–9 mild, 10–14 moderate, 15–21 severe) is the standard screening tool.
Panic Disorder
Recurrent unexpected panic attacks (abrupt surge of intense fear peaking within minutes) plus persistent concern about additional attacks or maladaptive behavior change. Panic attacks include palpitations, sweating, trembling, shortness of breath, chest pain, nausea, depersonalization, fear of dying, fear of going crazy. Rule out cardiac, thyroid, and substance causes on first presentation.
Agoraphobia
Fear of situations where escape might be difficult or help unavailable (public transit, open spaces, enclosed spaces, crowds, being alone outside home). Avoidance of at least 2 of these situations for 6+ months.
Specific Phobia
Marked fear about a specific object/situation (animal, natural environment, blood-injection-injury, situational, other). Exposure-based CBT is highly effective.
Social Anxiety Disorder (Social Phobia)
Marked fear of social situations where the person may be scrutinized. SSRIs/SNRIs and CBT are first-line; beta-blockers for performance-only subtype.
Separation Anxiety Disorder
Developmentally inappropriate, excessive fear about separation from attachment figures. Present in children and adults.
Selective Mutism
Consistent failure to speak in specific social situations despite speaking in others, lasting at least 1 month and interfering with function. Usually begins in early childhood.
Management
First-line pharmacotherapy across anxiety disorders is SSRI or SNRI (paroxetine, sertraline, escitalopram, venlafaxine, duloxetine). Buspirone is a non-benzodiazepine option for GAD. Benzodiazepines provide rapid relief but carry dependency and cognitive risks and should be used cautiously and time-limited. CBT with exposure elements is first-line psychotherapy. The APA Practice Guideline for Panic Disorder and USPSTF adult anxiety screening (2023) are the go-to citations.
06 OCD & Related Disorders OC-Spectrum
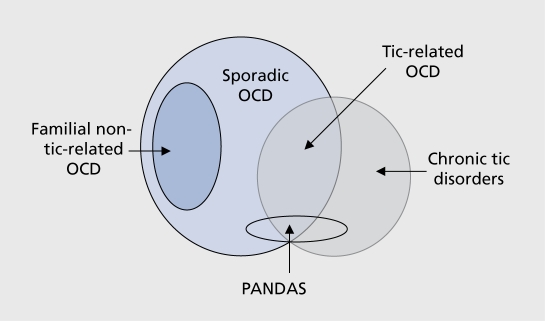
DSM-5-TR separated OCD and related disorders from the anxiety chapter, reflecting distinct neurobiology (cortico-striato-thalamo-cortical circuit dysfunction).
Obsessive-Compulsive Disorder (OCD)
Obsessions are recurrent, unwanted, intrusive thoughts, urges, or images causing distress; the person attempts to suppress or neutralize them. Compulsions are repetitive behaviors or mental acts performed to reduce anxiety or prevent a feared event, and are typically excessive or disconnected from what they are meant to prevent. Symptoms consume >1 hour/day or cause marked distress. Insight specifier: good/fair, poor, or absent/delusional. Y-BOCS (Yale-Brown Obsessive-Compulsive Scale) is the standard severity measure.
Body Dysmorphic Disorder (BDD)
Preoccupation with perceived physical defects not observable or slight to others, with repetitive behaviors (mirror checking, grooming, reassurance seeking). Muscle dysmorphia is a specifier. High suicide risk.
Hoarding Disorder
Persistent difficulty discarding possessions regardless of value, leading to accumulation that compromises living space use. Often ego-syntonic.
Trichotillomania (Hair-Pulling Disorder)
Recurrent pulling out of one's hair resulting in hair loss, with repeated attempts to stop. Can involve scalp, eyebrows, lashes, body hair.
Excoriation (Skin-Picking) Disorder
Recurrent skin picking resulting in lesions, with repeated attempts to stop. Often targets perceived blemishes.
Management
First-line pharmacotherapy for OCD is high-dose SSRI (often above MDD doses: fluoxetine 60–80 mg, sertraline 200 mg, fluvoxamine 300 mg, escitalopram 20–40 mg) or clomipramine. CBT with exposure and response prevention (ERP) is first-line psychotherapy and often more effective than medication. Refractory OCD may warrant augmentation with atypical antipsychotics (aripiprazole, risperidone) or deep brain stimulation (approved for severe refractory OCD). The APA OCD Practice Guideline is the standard reference.
07 Trauma & Stressor-Related Disorders Trauma
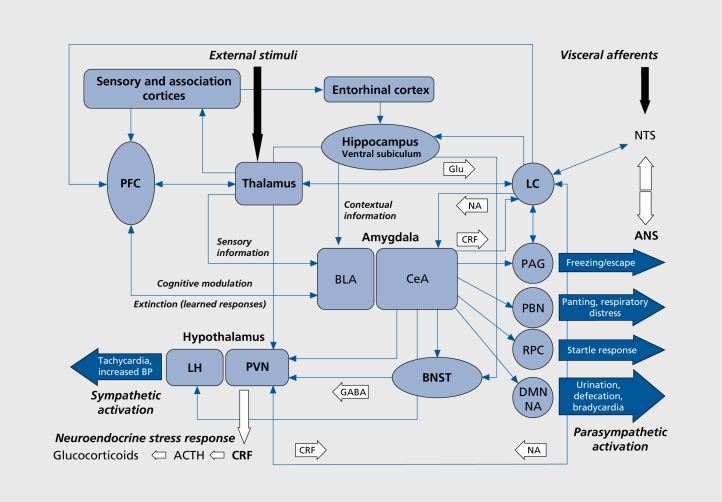
Posttraumatic Stress Disorder (PTSD)
Requires exposure to actual or threatened death, serious injury, or sexual violence (Criterion A), followed by four symptom clusters persisting >1 month: intrusion (flashbacks, nightmares, distressing memories), avoidance (of trauma reminders), negative alterations in cognition/mood (numbing, distorted self-blame, detachment), and alterations in arousal/reactivity (hypervigilance, exaggerated startle, sleep disturbance, irritability). The PCL-5 (PTSD Checklist for DSM-5) is the standard self-report measure.
First-line: trauma-focused CBT, prolonged exposure therapy, or EMDR (eye movement desensitization and reprocessing). Pharmacologic: SSRIs (sertraline and paroxetine are FDA-approved) and SNRIs (venlafaxine). Prazosin is useful for trauma-related nightmares (start 1 mg qHS, titrate). Benzodiazepines are contraindicated. The APA PTSD Clinical Practice Guideline is the key reference.
Acute Stress Disorder
PTSD-like symptoms occurring between 3 days and 1 month after trauma exposure. If symptoms persist beyond 1 month, the diagnosis changes to PTSD.
Adjustment Disorder
Emotional or behavioral symptoms in response to an identifiable stressor occurring within 3 months of onset, resolving within 6 months after the stressor ends. Subtypes: with depressed mood, anxious, mixed, disturbance of conduct, or mixed emotions and conduct.
Reactive Attachment Disorder & Disinhibited Social Engagement Disorder
Childhood disorders following pathogenic care (neglect, institutionalization). RAD presents with inhibited, emotionally withdrawn behavior; DSED presents with disinhibited, overly familiar behavior with strangers.
08 Schizophrenia Spectrum & Other Psychotic Disorders Psychosis
Psychotic disorders share the feature of disturbances in reality testing: hallucinations, delusions, disorganized thought, disorganized or abnormal motor behavior, and negative symptoms. These are among the most disabling conditions in medicine.
Schizophrenia
At least 2 of the following for 1 month (at least 1 from the first 3): delusions, hallucinations, disorganized speech, grossly disorganized/catatonic behavior, negative symptoms. Total duration of disturbance ≥6 months including prodromal and residual phases. Significant functional decline required. Typical onset: late teens to mid-20s (earlier in men).
Hallucinations (most commonly auditory, "voices"), delusions (persecutory, grandiose, referential, somatic, erotomanic, nihilistic, thought broadcasting/insertion/withdrawal), disorganized speech (tangentiality, circumstantiality, loose associations, word salad), bizarre behavior.
Affective flattening, alogia (poverty of speech), avolition (lack of motivation), anhedonia, asociality. These drive most long-term disability and respond poorly to antipsychotics.
Impaired attention, working memory, executive function, and processing speed. These are often the earliest changes and correlate with functional outcome more than positive symptoms do.
Other Psychotic Disorders
- Schizophreniform Disorder — meets schizophrenia criteria but duration is 1–6 months (often becomes schizophrenia if symptoms persist).
- Schizoaffective Disorder — schizophrenia criteria plus a major mood episode (depressive or manic) with at least 2 weeks of psychosis in the absence of mood symptoms.
- Brief Psychotic Disorder — psychotic symptoms lasting >1 day but <1 month with full return to baseline. Often postpartum or following severe stressor.
- Delusional Disorder — ≥1 month of delusions without other psychotic features and without significant functional impairment outside the delusional theme. Subtypes: erotomanic, grandiose, jealous, persecutory, somatic, mixed.
- Substance/Medication-Induced Psychotic Disorder — psychosis directly caused by intoxication, withdrawal, or exposure (stimulants, cannabis, hallucinogens, steroids).
- Psychotic Disorder Due to Another Medical Condition — secondary to medical cause (neurologic, endocrine, autoimmune).
Management
All antipsychotics (first- and second-generation) are equally effective except for clozapine, which is superior for treatment-resistant schizophrenia and the only agent shown to reduce suicidality in schizophrenia. The APA Practice Guideline for Schizophrenia is the definitive treatment reference. Long-acting injectable (LAI) antipsychotics (paliperidone, risperidone, aripiprazole, olanzapine) are preferred for patients with adherence challenges. Psychosocial interventions include assertive community treatment, supported employment, and family psychoeducation.
Clozapine is the most effective antipsychotic for treatment-resistant schizophrenia but requires weekly (then biweekly, then monthly) absolute neutrophil count (ANC) monitoring through the REMS program because of the risk of agranulocytosis. Document the ANC at every clozapine visit.
09 Substance-Related & Addictive Disorders SUD
DSM-5-TR consolidated abuse and dependence into single substance use disorders (SUDs) rated mild (2–3 criteria), moderate (4–5), or severe (6+) of 11 criteria covering impaired control, social impairment, risky use, and pharmacologic features (tolerance, withdrawal). SUDs are chronic, relapsing conditions that deserve longitudinal chronic-disease management.
Alcohol Use Disorder (AUD)
Most prevalent SUD. Withdrawal can be life-threatening: tremor, autonomic hyperactivity, hallucinosis, seizures, delirium tremens. CIWA-Ar (Clinical Institute Withdrawal Assessment for Alcohol, revised; 10 items, max 67) guides symptom-triggered benzodiazepine dosing. AUDIT-C (3-item brief screen; score ≥4 men, ≥3 women is positive) and full AUDIT (10 items) are the validated screens. Pharmacotherapy: naltrexone (PO or IM depot), acamprosate, disulfiram, off-label topiramate and gabapentin.
Opioid Use Disorder (OUD)
Withdrawal scored with COWS (Clinical Opiate Withdrawal Scale; 11 items). Medication-assisted treatment saves lives: methadone (full mu agonist, federally regulated through OTPs), buprenorphine (partial agonist; mono or with naloxone; sublingual, buccal, or LAI Sublocade), naltrexone (antagonist; oral or IM depot Vivitrol). Naloxone (Narcan) for overdose reversal should be prescribed broadly.
Stimulant Use Disorder
Cocaine, methamphetamine, prescription stimulants. No FDA-approved medications; treatment is psychosocial (contingency management, CBT). Acute intoxication mimics mania/psychosis; withdrawal is primarily dysphoric.
Cannabis Use Disorder
Increasingly common with legalization. Withdrawal: irritability, anxiety, sleep disturbance, decreased appetite. Associated with earlier onset of psychosis in predisposed individuals.
Sedative, Hypnotic, or Anxiolytic Use Disorder
Benzodiazepine and z-drug use disorders. Withdrawal can be life-threatening (seizures, delirium). Taper gradually; never abruptly discontinue high-dose chronic benzodiazepines.
Tobacco Use Disorder
First-line: varenicline (Chantix, partial nicotinic agonist), bupropion SR (Zyban), combination nicotine replacement therapy (patch + short-acting). Counseling should accompany every quit attempt.
Gambling Disorder
The only behavioral addiction included in DSM-5-TR substance-related chapter. CBT is first-line; naltrexone is off-label.
The APA Practice Guideline for Substance Use Disorders is the comprehensive reference. USPSTF unhealthy alcohol use screening and USPSTF tobacco cessation interventions support universal screening in primary care.
10 Feeding & Eating Disorders Eating
Anorexia Nervosa
Restriction of energy intake leading to significantly low body weight, intense fear of weight gain, disturbance in body image. Subtypes: restricting or binge-eating/purging. Highest mortality of any psychiatric disorder. Medical complications: bradycardia, hypotension, hypothermia, osteoporosis, amenorrhea, QTc prolongation, refeeding syndrome.
Bulimia Nervosa
Recurrent episodes of binge eating followed by compensatory behaviors (vomiting, laxatives, fasting, exercise) at least once weekly for 3 months. Often normal or overweight. Russell sign (knuckle calluses), parotid enlargement, dental erosions, hypokalemia, metabolic alkalosis. Fluoxetine is the only FDA-approved pharmacotherapy.
Binge Eating Disorder (BED)
Recurrent binges without compensatory behaviors, ≥1/week for 3 months. Most prevalent eating disorder in the US. Lisdexamfetamine (Vyvanse) is FDA-approved for moderate-to-severe BED.
Avoidant/Restrictive Food Intake Disorder (ARFID)
Avoidance or restriction of food based on sensory features, fear of aversive consequences, or lack of interest in eating, leading to nutritional deficiency. No body image disturbance (distinguishing it from anorexia).
Other
Pica (eating non-food items), rumination disorder, night eating syndrome (OSFED).
The APA Practice Guideline for Eating Disorders (2023) is the authoritative reference. EAT-26 is the standard screen.
11 Neurodevelopmental Disorders NDD
Attention-Deficit/Hyperactivity Disorder (ADHD)
Persistent pattern of inattention and/or hyperactivity-impulsivity present before age 12, across multiple settings, for at least 6 months. Requires 6 of 9 symptoms in each domain (5 for adults ≥17). Three presentations: predominantly inattentive, predominantly hyperactive-impulsive, combined. First-line pharmacotherapy: stimulants (methylphenidate or amphetamine-based). Non-stimulants: atomoxetine, guanfacine ER, clonidine ER, viloxazine.
Autism Spectrum Disorder (ASD)
Persistent deficits in social communication and interaction plus restricted, repetitive patterns of behavior/interests/activities, present in early developmental period. Severity graded 1–3 based on support needed. Commonly comorbid with ADHD, anxiety, intellectual disability. Psychiatric scribes will document ASD in context of comorbid psychiatric management; pharmacotherapy targets comorbid symptoms (irritability: risperidone, aripiprazole approved).
Intellectual Disability (ID)
Deficits in intellectual (IQ) and adaptive functioning with onset in developmental period. Severity based on adaptive function: mild, moderate, severe, profound.
Specific Learning Disorder
Persistent difficulty in reading (dyslexia), writing (dysgraphia), or mathematics (dyscalculia) despite intervention.
Tic Disorders
Tourette disorder: both multiple motor and 1+ vocal tics, onset before 18, lasting >1 year. Persistent motor or vocal tic disorder. Provisional tic disorder. Management: habit reversal training (CBIT), alpha-2 agonists, antipsychotics (aripiprazole, haloperidol, pimozide) for severe cases.
Communication Disorders
Language disorder, speech sound disorder, childhood-onset fluency disorder (stuttering), social (pragmatic) communication disorder.
The AAP Clinical Practice Guideline for ADHD (2019) is the key pediatric reference.
12 Disruptive, Impulse-Control, & Conduct Disorders Behavioral
Oppositional Defiant Disorder (ODD)
Pattern of angry/irritable mood, argumentative/defiant behavior, or vindictiveness lasting ≥6 months, with at least 4 symptoms from these domains. Common precursor to conduct disorder.
Conduct Disorder
Repetitive and persistent pattern of violating the basic rights of others or major age-appropriate societal norms (aggression, destruction of property, deceit/theft, serious rule violations). Childhood-onset, adolescent-onset, or unspecified onset. Specifier: with limited prosocial emotions (callous-unemotional traits).
Intermittent Explosive Disorder (IED)
Recurrent behavioral outbursts representing failure to control aggressive impulses grossly out of proportion to provocation.
Pyromania & Kleptomania
Recurrent deliberate fire setting for tension release and fascination; recurrent failure to resist urges to steal items not needed for personal use or monetary value.
Antisocial Personality Disorder
Though listed in personality disorders chapter, it is cross-referenced here because it begins as conduct disorder before age 15.
13 Personality Disorders PD
Personality disorders are enduring, pervasive, inflexible patterns of inner experience and behavior deviating from cultural expectations, stable over time, with onset in adolescence or early adulthood and causing distress/impairment. DSM-5-TR groups the 10 PDs into three clusters.
Paranoid: pervasive distrust, suspiciousness.
Schizoid: detachment from social relationships, restricted emotional expression.
Schizotypal: cognitive/perceptual distortions, eccentric behavior, odd beliefs, few close friends.
Antisocial: disregard for and violation of others' rights (must be ≥18, with conduct disorder before 15).
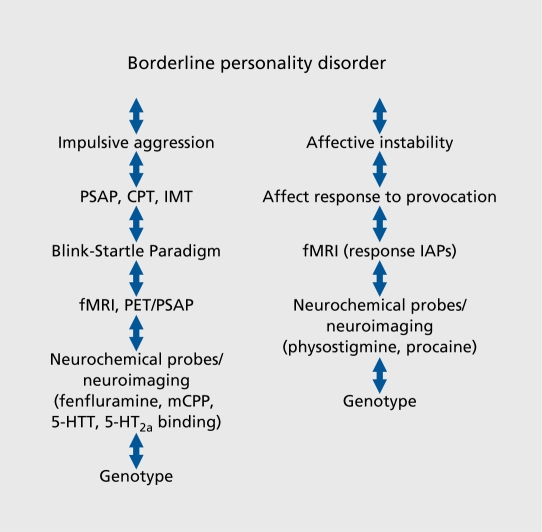
Borderline (BPD): instability of relationships, self-image, affect; impulsivity; fear of abandonment; self-harm and suicidality; transient stress-related paranoia/dissociation. DBT is first-line psychotherapy.
Histrionic: excessive emotionality, attention-seeking.
Narcissistic: grandiosity, need for admiration, lack of empathy.
Avoidant: social inhibition, feelings of inadequacy, hypersensitivity to criticism.
Dependent: excessive need to be cared for, submissive/clinging behavior, fears of separation.
Obsessive-Compulsive Personality Disorder (OCPD): preoccupation with orderliness, perfectionism, control — distinct from OCD.
Management
Psychotherapy is the primary treatment for all PDs. Dialectical Behavior Therapy (DBT), Mentalization-Based Treatment (MBT), Transference-Focused Psychotherapy (TFP), and Schema Therapy have strongest evidence for borderline PD. Medications target comorbid symptoms (mood, anxiety, impulsivity) rather than the PD itself.
14 Somatic, Dissociative, Sexual & Gender-Related Disorders Other
Somatic Symptom & Related Disorders
- Somatic Symptom Disorder — distressing somatic symptoms with excessive thoughts, feelings, or behaviors related to the symptom.
- Illness Anxiety Disorder — preoccupation with having/acquiring a serious illness with minimal somatic symptoms (replaces hypochondriasis).
- Conversion Disorder (Functional Neurological Symptom Disorder) — altered voluntary motor or sensory function incompatible with recognized neurological disease.
- Factitious Disorder — falsification of physical/psychological symptoms in self (imposed on self) or another (imposed on another — formerly Munchausen by proxy).
Dissociative Disorders
- Dissociative Identity Disorder (DID) — two or more distinct personality states with recurrent gaps in memory.
- Dissociative Amnesia — inability to recall important autobiographical information, usually of a traumatic/stressful nature; may include dissociative fugue.
- Depersonalization/Derealization Disorder — persistent or recurrent experiences of feeling detached from self (depersonalization) or from surroundings (derealization) with intact reality testing.
Sexual Dysfunctions
Delayed ejaculation, erectile disorder, female orgasmic disorder, female sexual interest/arousal disorder, genito-pelvic pain/penetration disorder, male hypoactive sexual desire disorder, premature ejaculation, substance/medication-induced sexual dysfunction. SSRIs commonly cause sexual side effects.
Gender Dysphoria
Marked incongruence between one's experienced/expressed gender and assigned gender, with associated distress. Care may include social, hormonal, and surgical transition components. Psychiatrists provide supportive care and manage comorbid conditions.
Paraphilic Disorders
Voyeuristic, exhibitionistic, frotteuristic, sexual masochism, sexual sadism, pedophilic, fetishistic, transvestic disorders. Distinction from paraphilias (non-pathological) requires distress, impairment, or harm to others.
15 Sleep-Wake & Neurocognitive Disorders (Overlap) Cross
Insomnia Disorder
Dissatisfaction with sleep quantity/quality with difficulty initiating, maintaining, or early-morning awakening, ≥3 nights/week for ≥3 months. CBT-I is first-line treatment. Pharmacologic options include zolpidem, eszopiclone, zaleplon, ramelteon, suvorexant, lemborexant, doxepin 3–6 mg, trazodone (off-label), mirtazapine (if comorbid depression).
Narcolepsy
Recurrent irresistible need for sleep, cataplexy, hypocretin deficiency, or REM sleep abnormalities on MSLT. Managed by sleep medicine; psychiatrists co-manage stimulants and wake-promoting agents (modafinil, armodafinil, solriamfetol, pitolisant).
Parasomnias
NREM sleep arousal disorders (sleepwalking, sleep terrors), nightmare disorder (especially in PTSD — prazosin), REM sleep behavior disorder (prodrome to alpha-synucleinopathies — clonazepam, melatonin).
Delirium
Acute disturbance in attention and awareness developing over hours to days, fluctuating, with cognitive change not better explained by prior or evolving dementia. Hyperactive, hypoactive, or mixed. Treat underlying cause; low-dose antipsychotics (haloperidol, quetiapine) for severe agitation. Avoid benzodiazepines except in alcohol/benzo withdrawal delirium.
Major & Mild Neurocognitive Disorders
DSM-5-TR replaced "dementia" with major neurocognitive disorder (significant cognitive decline with loss of independence) and mild neurocognitive disorder (modest decline with preserved independence). Etiological subtypes: Alzheimer disease, vascular, Lewy body, frontotemporal, traumatic brain injury, HIV, substance/medication, Parkinson, Huntington, prion, other. Cognitive screens: MMSE (0–30; <24 suggests impairment), MoCA (0–30; <26 suggests impairment, more sensitive to mild deficits). Pharmacologic: cholinesterase inhibitors (donepezil, rivastigmine, galantamine), NMDA antagonist memantine; newer anti-amyloid antibodies (lecanemab, donanemab) for mild Alzheimer.
16 Psychiatric Emergencies & Safety Assessment Emergency
Every psychiatric encounter includes a risk assessment. Some encounters are the emergency.
Document ideation (passive vs active), intent, plan, means access (especially firearms), prior attempts, current protective factors, chronic vs acute risk factors. The Columbia Suicide Severity Rating Scale (C-SSRS) is the most widely used structured assessment and the one most institutions require. The Beck Scale for Suicidal Ideation (BSS) is also used in research settings.
Disposition levels: outpatient with safety plan, intensive outpatient/PHP, voluntary inpatient, involuntary inpatient (state-specific statutes: "5150" in CA, "201/302" in PA, "Section 12" in MA, etc.). Document the legal basis for any involuntary hold.
Document ideation, intent, plan, identified target, access to means. Most states impose a duty to protect (Tarasoff and successor cases) requiring warning of intended victim, notification of law enforcement, or hospitalization.
Escalating verbal/physical threat requiring de-escalation. Pharmacologic options: IM haloperidol + lorazepam + diphenhydramine ("B-52"), IM olanzapine (not within 1 hour of IM/IV lorazepam because of respiratory depression), IM ziprasidone, IM aripiprazole, po quetiapine, inhaled loxapine.
Marked psychomotor disturbance with features such as stupor, catalepsy, waxy flexibility, mutism, negativism, posturing, mannerisms, stereotypies, agitation, grimacing, echolalia, echopraxia. Can occur with mood, psychotic, and medical conditions. First-line treatment: lorazepam challenge (1–2 mg IM/IV), then ECT if refractory. Avoid antipsychotics in catatonia (can precipitate NMS).
Life-threatening reaction to dopamine blockade: fever, lead-pipe rigidity, autonomic instability, altered mental status, elevated CK (often >1000), leukocytosis. Stop offending agent, supportive ICU care, dantrolene or bromocriptine in severe cases. Onset over days.
Triad of mental status change, autonomic hyperactivity, and neuromuscular abnormalities (clonus — especially lower extremity, hyperreflexia, tremor). Usually from combining serotonergic agents (SSRI + MAOI, tramadol, linezolid, triptans, St. John's wort). Onset within hours. Stop offending agent, supportive care, cyproheptadine in severe cases.
17 Psychiatric Procedures & Neuromodulation Procedure
Electroconvulsive Therapy (ECT)
The most effective treatment for severe depression and catatonia, and an effective treatment for treatment-resistant mania and psychotic depression. Electrical stimulus induces a therapeutic generalized seizure lasting 15–60 seconds under brief general anesthesia (methohexital or propofol) with succinylcholine for paralysis. Typical acute course: 6–12 treatments, 3 times/week. Electrode placement: bilateral (most effective, more cognitive side effects), right unilateral (fewer side effects), bifrontal. Main side effect: transient anterograde/retrograde amnesia. Indications: severe MDD (especially with psychotic features, refusal to eat/drink, suicidality), catatonia, treatment-resistant mania, NMS, pregnancy-associated severe mood episodes.
Repetitive Transcranial Magnetic Stimulation (rTMS)
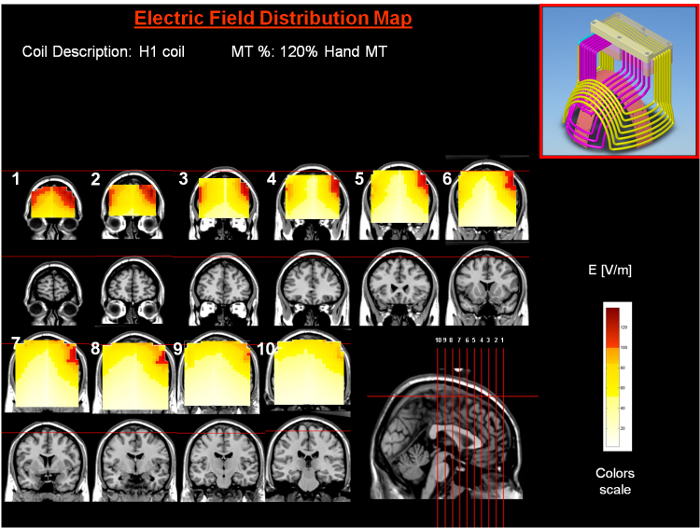
Non-invasive focal magnetic stimulation of the dorsolateral prefrontal cortex. FDA-cleared for MDD, OCD (deep TMS), smoking cessation, and anxious depression. Course: daily sessions (5 days/week) for 4–6 weeks. No anesthesia, no cognitive side effects. Seizure is the main (rare) risk. Deep TMS (dTMS) uses H-coil for deeper penetration.
Ketamine & Esketamine (Spravato)
Racemic IV ketamine (off-label) and intranasal esketamine (Spravato, FDA-approved for treatment-resistant depression and MDD with suicidality) provide rapid-onset (hours to days) antidepressant effects via NMDA antagonism. Esketamine is administered in a REMS-certified clinic with 2-hour monitoring because of dissociation and blood pressure effects. Requires concurrent oral antidepressant.
Light Therapy
10,000 lux broad-spectrum white light, 30 minutes each morning, first-line for seasonal affective disorder and adjunct for non-seasonal depression.
Vagus Nerve Stimulation (VNS)
Implanted device providing intermittent stimulation of the left vagus nerve. FDA-approved for treatment-resistant depression after ≥4 failed trials.
Deep Brain Stimulation (DBS)
Investigational/humanitarian use for severe refractory OCD (FDA HDE approval) and treatment-resistant depression. Stereotactic placement of electrodes typically in anterior limb of internal capsule, ventral capsule/ventral striatum, or subcallosal cingulate.
Psychotherapy Referrals Scribes Document
| Therapy | Primary Indications |
|---|---|
| Cognitive Behavioral Therapy (CBT) | MDD, anxiety, OCD, PTSD, insomnia (CBT-I), eating disorders |
| Dialectical Behavior Therapy (DBT) | Borderline PD, chronic suicidality, emotion dysregulation |
| Interpersonal Therapy (IPT) | MDD, postpartum depression, grief |
| Prolonged Exposure (PE) | PTSD |
| EMDR | PTSD, trauma processing |
| Exposure & Response Prevention (ERP) | OCD, phobias |
| Motivational Interviewing (MI) | Substance use, behavior change |
| Family-Based Treatment (Maudsley) | Adolescent anorexia nervosa |
| Psychodynamic Psychotherapy | Personality disorders, chronic mood/anxiety |
| Supportive Psychotherapy | Severe mental illness, crisis stabilization |
18 Medications You Must Know Pharm
SSRIs (Selective Serotonin Reuptake Inhibitors)
| Generic | Brand | Notes |
|---|---|---|
| Fluoxetine | Prozac | Longest half-life (no taper needed); activating; pediatric MDD approved |
| Sertraline | Zoloft | Broad indications; GI side effects; PTSD/OCD approved |
| Paroxetine | Paxil | Most anticholinergic; short half-life = discontinuation syndrome; pregnancy category D |
| Citalopram | Celexa | Max 40 mg (20 mg if elderly) — QTc prolongation |
| Escitalopram | Lexapro | S-enantiomer of citalopram; fewer interactions |
| Fluvoxamine | Luvox | Primarily OCD; strong CYP inhibitor |
SNRIs (Serotonin-Norepinephrine Reuptake Inhibitors)
| Generic | Brand | Notes |
|---|---|---|
| Venlafaxine | Effexor XR | Dose-dependent NE effect; monitor BP; discontinuation syndrome |
| Desvenlafaxine | Pristiq | Active metabolite of venlafaxine |
| Duloxetine | Cymbalta | Neuropathic pain, fibromyalgia, stress urinary incontinence |
| Levomilnacipran | Fetzima | More NE-selective |
| Milnacipran | Savella | FDA approved for fibromyalgia in US |
Atypical Antidepressants
| Generic | Brand | Notes |
|---|---|---|
| Bupropion | Wellbutrin, Zyban | NDRI; activating; no sexual/weight effects; lowers seizure threshold; contraindicated in eating disorders |
| Mirtazapine | Remeron | Sedation and weight gain (lower doses more sedating); helpful for insomnia and poor appetite |
| Trazodone | Desyrel | Used off-label for insomnia; priapism risk |
| Vilazodone | Viibryd | SSRI + 5-HT1A partial agonist |
| Vortioxetine | Trintellix | Multimodal serotonin; may help cognition |
| Nefazodone | Serzone | Rarely used — hepatotoxicity black box |
TCAs (Tricyclic Antidepressants)
Amitriptyline, nortriptyline, imipramine, clomipramine (OCD), doxepin (insomnia at low dose). Anticholinergic, antihistamine, alpha-blocker, and cardiac conduction effects. Lethal in overdose. Check EKG before starting in older adults.
MAOIs (Monoamine Oxidase Inhibitors)
Phenelzine, tranylcypromine, isocarboxazid, selegiline (transdermal). Require tyramine-free diet (hypertensive crisis risk) and washout from serotonergic agents (serotonin syndrome risk). Reserved for treatment-resistant depression.
Mood Stabilizers
| Drug | Key Points |
|---|---|
| Lithium | Gold standard; narrow therapeutic window (0.6–1.2 mEq/L); monitor levels, TSH, Cr, Ca; toxicity: tremor, ataxia, confusion |
| Valproate (Depakote) | Teratogen (neural tube); monitor LFTs, ammonia, platelets; weight gain, PCOS |
| Carbamazepine (Tegretol) | HLA-B*1502 testing for SJS risk in Asian patients; strong CYP inducer |
| Lamotrigine (Lamictal) | Bipolar depression maintenance; slow titration to avoid SJS/TEN |
| Oxcarbazepine (Trileptal) | Less hepatotoxicity than carbamazepine; hyponatremia |
First-Generation Antipsychotics (Typicals)
Haloperidol (Haldol), chlorpromazine (Thorazine), fluphenazine (Prolixin), perphenazine (Trilafon), thiothixene (Navane), trifluoperazine (Stelazine), loxapine (Loxitane), thioridazine (Mellaril — QTc). High-potency (haldol, fluphenazine): more EPS, less sedation/anticholinergic. Low-potency (chlorpromazine, thioridazine): less EPS, more sedation/anticholinergic/hypotension.
Second-Generation Antipsychotics (Atypicals)
| Generic | Brand | Key Points |
|---|---|---|
| Risperidone | Risperdal | High prolactin; LAI available (Risperdal Consta, Perseris) |
| Paliperidone | Invega, Sustenna, Trinza, Hafyera | Active metabolite of risperidone; monthly, 3-mo, 6-mo LAI |
| Olanzapine | Zyprexa, Relprevv LAI | Significant weight gain, metabolic; LAI requires post-injection monitoring |
| Quetiapine | Seroquel | Highly sedating; used for insomnia off-label; bipolar depression |
| Aripiprazole | Abilify, Maintena, Aristada | Partial D2 agonist; akathisia common; weight-neutral |
| Ziprasidone | Geodon | QTc; must take with food for absorption |
| Lurasidone | Latuda | Weight-neutral; bipolar depression; take with ≥350 kcal food |
| Asenapine | Saphris, Secuado patch | Sublingual; oral hypoesthesia |
| Iloperidone | Fanapt | Orthostasis; slow titration |
| Brexpiprazole | Rexulti | Aripiprazole analog; MDD adjunct; Alzheimer agitation |
| Cariprazine | Vraylar | D3-preferring partial agonist; bipolar, schizophrenia, MDD adjunct |
| Lumateperone | Caplyta | Schizophrenia, bipolar depression; metabolic-neutral |
| Clozapine | Clozaril | Gold standard for treatment-resistant schizophrenia; REMS ANC monitoring; agranulocytosis, myocarditis, seizure, ileus, sialorrhea |
Anxiolytics & Hypnotics
Benzodiazepines: alprazolam, lorazepam, clonazepam, diazepam, oxazepam, temazepam, chlordiazepoxide, midazolam. GABA-A positive allosteric modulators. Dependence, withdrawal seizures, falls in elderly, paradoxical disinhibition. Buspirone: 5-HT1A partial agonist; no dependence; takes weeks. Hydroxyzine: antihistamine anxiolytic. Propranolol: performance anxiety. Z-drugs: zolpidem, eszopiclone, zaleplon. Melatonin receptor agonists: ramelteon. Orexin receptor antagonists: suvorexant, lemborexant, daridorexant.
ADHD Medications
Stimulants: methylphenidate (Ritalin, Concerta, Focalin, Daytrana), amphetamine salts (Adderall, Vyvanse/lisdexamfetamine, Dexedrine, Evekeo, Mydayis). Schedule II; monitor BP, HR, weight, height in children. Non-stimulants: atomoxetine (Strattera), guanfacine ER (Intuniv), clonidine ER (Kapvay), viloxazine (Qelbree).
Substance Use Disorder Medications
AUD: naltrexone PO/Vivitrol IM, acamprosate, disulfiram. OUD: methadone, buprenorphine/naloxone (Suboxone, Zubsolv, Bunavail), buprenorphine LAI (Sublocade, Brixadi), naltrexone IM (Vivitrol). Tobacco: varenicline, bupropion SR, NRT (patch, gum, lozenge, inhaler, nasal). BED: lisdexamfetamine.
Dementia & Other
Donepezil, rivastigmine, galantamine, memantine; lecanemab, donanemab; prazosin for PTSD nightmares; emerging psychedelics (psilocybin, MDMA-assisted therapy) in clinical trials.
19 Rating Scales & Classification Systems Scales
9 items, each 0–3 (past 2 weeks). Total 0–27. 0–4 none, 5–9 mild, 10–14 moderate, 15–19 moderately severe, 20–27 severe. Q9 screens SI.
7 items, 0–3 each. Total 0–21. 0–4 none, 5–9 mild, 10–14 moderate, 15–21 severe.
13 yes/no symptom questions + co-occurrence + functional impact. Positive: 7+ yes AND co-occurrence AND moderate/severe impairment.
11 items, total 0–60. >20 indicates significant mania. Used in clinical trials and inpatient settings.
Clinician-administered. HAM-D (17-item standard): <8 normal, 8–13 mild, 14–18 moderate, 19–22 severe, ≥23 very severe. HAM-A (14-item): <17 mild, 18–24 mild-moderate, 25–30 moderate-severe.
20 items, each 0–4. Total 0–80. Provisional PTSD at ≥31–33.
AUDIT-C: 3 items, 0–12. Positive: ≥4 men, ≥3 women. Full AUDIT: 10 items, 0–40. 8+ indicates hazardous drinking.
10 items, max 67. <10 minimal/no meds, 10–19 moderate (treat), ≥20 severe (high risk seizure/DTs, aggressive treatment).
11 items. 5–12 mild, 13–24 moderate, 25–36 moderately severe, >36 severe. Buprenorphine induction typically begins at COWS ≥8–12.
Both scored 0–30. MMSE <24 impairment. MoCA <26 impairment (add 1 point if ≤12 years education); more sensitive to MCI. Document education level with score.
10 items, 0–40. 0–7 subclinical, 8–15 mild, 16–23 moderate, 24–31 severe, 32–40 extreme.
26 items. Score ≥20 indicates high concern; behavioral items positive also prompt referral regardless of total.
Screens severity (passive wish to die → active ideation with plan and intent) and behavior (preparatory acts, aborted, interrupted, actual attempts). Most widely used structured suicide risk assessment. Any "yes" to plan, intent, or behavior in past month is high concern.
12-item clinician-rated exam for tardive dyskinesia. Items 1–10 scored 0–4, items 11–12 yes/no. Administer at baseline then every 6 months on antipsychotics (every 3 months for first-generation).
20 Medication Monitoring & Lab Work Monitoring
| Medication | Baseline | Ongoing |
|---|---|---|
| Lithium | BMP, TSH, Ca, urine SG, EKG if >40 or cardiac hx, pregnancy test | Level 5 days after dose change then every 3–6 months; TSH, BMP, Ca every 6–12 months |
| Valproate | LFTs, CBC, pregnancy test | Level, LFTs, CBC every 6 months |
| Carbamazepine | CBC, LFTs, Na, HLA-B*1502 in Asian patients | Level, CBC, LFTs, Na every 3–6 months |
| Lamotrigine | None required; rash counseling | Level not routinely needed; watch for rash during titration |
| Atypical antipsychotics | Weight, waist, BP, fasting glucose, lipids, A1C | Metabolic panel at 12 weeks then annually; AIMS every 6 months |
| Clozapine | CBC with ANC, EKG, myocarditis workup | ANC weekly x 6 mo, biweekly x 6 mo, then monthly (REMS) |
| Stimulants | BP, HR, height/weight, cardiac hx | BP, HR, weight every visit; height in children |
| TCAs | EKG (especially >40 or cardiac hx) | Level in select cases (nortriptyline, imipramine) |
| MAOIs | Diet review, medication review | BP; review tyramine avoidance and washout |
| Naltrexone (oral/IM) | LFTs; ensure opioid-free 7–10 days | LFTs periodically |
21 Abbreviations Master List Reference
Diagnoses & Symptoms
Symptoms & Exam
Procedures & Treatments
Medications & Pharm
22 Mental Status Exam & Risk Documentation Exam
Appearance: well-groomed, casually dressed, appears stated age
Behavior/Psychomotor: cooperative, calm, good eye contact, no abnormal movements
Speech: normal rate, rhythm, volume, and prosody
Mood: "depressed" (patient's words)
Affect: constricted, congruent with mood
Thought Process: linear, logical, goal-directed
Thought Content: no SI, HI, delusions; denies obsessions
Perception: no AVH; no illusions
Cognition: A&O x 3, attention and memory grossly intact
Insight: fair
Judgment: fair
Appearance & Behavior
Document grooming, hygiene, clothing appropriateness, posture, eye contact, psychomotor activity (agitation, retardation, catatonia, tics, tremor, tardive dyskinesia), and cooperation with the interview. Note any abnormal involuntary movements — this drives antipsychotic monitoring.
Speech
Rate (pressured, slowed), rhythm (dysprosodic, stuttering), volume (loud, soft), fluency, spontaneity, latency.
Mood vs Affect
Mood is the patient's sustained emotional state, documented in quotes ("sad," "fine," "angry"). Affect is the observed emotional expression: quality (euthymic, dysphoric, euphoric, anxious, irritable), range (full, restricted, constricted, blunted, flat), stability (stable, labile), and congruence with mood and content.
Thought Process
Linear, logical, goal-directed (normal); circumstantial (excessive detail before reaching point); tangential (never returns to point); loose associations (no logical connection); flight of ideas (rapid shifts with connections); word salad (incoherent); thought blocking (abrupt stop); neologisms; clang associations; perseveration.
Thought Content
Suicidal and homicidal ideation (always explicit), delusions (persecutory, grandiose, referential, somatic, etc.), obsessions, compulsions, phobias, preoccupations, paranoia, ideas of reference, thought broadcasting/insertion/withdrawal.
Perception
Hallucinations (auditory, visual, tactile, olfactory, gustatory), illusions, depersonalization, derealization, dissociation.
Cognition
Level of consciousness, orientation x 4 (person, place, time, situation), attention (serial 7s, spell WORLD backward), memory (immediate, recent, remote), language, abstract thinking (proverb interpretation), fund of knowledge.
Insight & Judgment
Insight: awareness of illness and need for treatment (poor, fair, good). Judgment: ability to make sound decisions (poor, fair, good).
Every note must document: (1) current SI/HI with plan and intent, (2) history of attempts, (3) access to lethal means (especially firearms), (4) acute and chronic risk factors, (5) protective factors, and (6) disposition rationale. Template language: "Patient endorses passive suicidal ideation without plan, intent, or preparatory behavior. No access to firearms. Chronic risk factors include prior attempt (2019) and depression; acute risk factors include recent job loss. Protective factors include strong family support and engagement with treatment. Assessed as low acute risk on high chronic baseline. Safety plan reviewed."
23 Sample HPI Templates Templates
These templates show the kind of documentation expected in psychiatric clinic notes. Use them as frameworks to internalize the rhythm and content of a good psychiatric HPI.
"Ms. [Name] is a 34-year-old female with no prior psychiatric history who presents for evaluation of 4 months of progressively worsening low mood. She reports anhedonia, initial insomnia with 2–3 hours of sleep latency, decreased appetite with 10-lb unintentional weight loss, low energy, poor concentration that is interfering with work performance, and feelings of worthlessness. She denies active suicidal ideation but endorses passive thoughts of "not wanting to wake up" several times per week. No history of manic or hypomanic symptoms. No psychosis. She identifies a recent divorce as the precipitating stressor. PHQ-9 today: 18 (moderately severe). GAD-7: 11. Denies substance use beyond occasional wine. Family history notable for MDD in mother (on sertraline)."
"Mr. [Name] is a 28-year-old male with a history of Bipolar I Disorder (dx 2019) brought in by his parents for 10 days of escalating manic symptoms. Per family, he has been sleeping 2–3 hours nightly without fatigue, speaking rapidly, making grandiose plans to start a technology company, spending approximately $8,000 on equipment, and driving recklessly. He reports euphoric mood and "unlimited energy." On exam, speech is pressured with flight of ideas. He denies SI/HI and denies AVH. Recent medication history: self-discontinued lithium 3 weeks ago because he "felt fine." No substance use per patient and family. YMRS: 32. Admission for acute mania being discussed; risks/benefits of voluntary vs involuntary hospitalization reviewed."
"Mr. [Name] is a 52-year-old male with MDD, recurrent, and AUD who presents to the ED by EMS after his wife found a suicide note and loaded firearm on the kitchen table. Patient endorses active suicidal ideation with plan (firearm) and intent. He reports 2 weeks of worsening depression after job termination, increased alcohol use (8–10 drinks daily), and feelings of hopelessness that his family "would be better off without him." Last drink 6 hours ago; CIWA-Ar currently 4. No prior suicide attempts. Firearm has been secured by law enforcement. C-SSRS: positive for active ideation with specific plan and intent in past 24 hours. Patient is agreeable to voluntary inpatient admission for safety, stabilization, and alcohol withdrawal monitoring."
"Mr. [Name] is a 21-year-old male college student with no prior psychiatric history brought in by his roommate for 3 weeks of increasingly bizarre behavior. Roommate reports that patient has been whispering to the walls, accusing classmates of broadcasting his thoughts, refusing to eat food from the dining hall ("they are poisoning it"), and has not attended class in 10 days. Patient reports hearing two male voices commenting on his actions and believes the CIA has implanted a tracking device. He denies SI/HI but acknowledges the voices "sometimes say mean things." Urine drug screen negative. No family history of psychosis but paternal uncle with schizophrenia. This is concerning for a first episode of schizophrenia-spectrum illness; admission for workup (labs, imaging, LP if indicated) and initiation of antipsychotic therapy under discussion."
"Ms. [Name] is a 29-year-old female presenting for follow-up of panic disorder and GAD. She describes 4 panic attacks in the past month, each lasting 10–15 minutes with palpitations, shortness of breath, chest tightness, and fear of dying. Attacks are unpredictable, with one occurring while driving leading to avoidance of highways for the past 2 weeks (developing agoraphobia). She is 3 months into sertraline 100 mg daily with partial benefit. GAD-7 today: 13 (previously 18). She is attending weekly CBT and completing exposure homework. Denies SI/HI, denies substance use. Cardiac workup last month negative (normal EKG, echocardiogram, TSH)."
"Mr. [Name] is a 38-year-old male with severe opioid use disorder presenting for buprenorphine induction. History of 6 years of opioid use that began after a back injury and oxycodone prescription; transitioned to heroin 3 years ago; currently using ~1 gram IV heroin daily. Last use 16 hours ago. He endorses 2 prior overdoses (both reversed with naloxone) and unsuccessful detox attempts x3. He is highly motivated today: recently became a father and his partner has given him an ultimatum. COWS at arrival: 14 (moderate withdrawal). No active SI/HI. Hepatitis C positive (undergoing treatment with gastroenterology). Patient consents to initiation of buprenorphine/naloxone; first dose administered in-office with plan to titrate to effective dose, counseling referral, and naloxone prescription for home."
24 References & Sources Refs
Clinical Practice Guidelines
Screening & Preventive Guidance
USPSTF. Screening for Depression and Suicide Risk in Adults. JAMA. 2023.
USPSTF. Screening for Anxiety Disorders in Adults. JAMA. 2023.
USPSTF. Interventions for Tobacco Smoking Cessation in Adults. JAMA. 2021.
Diagram & Figure Sources
Figure 1: The Human Brain. OpenStax College. CC BY 3.0.
Figure 2: Limbic System. Blausen Medical. CC BY 3.0.
Figure 3: Depression. Wikimedia Commons. Public domain.
Psychiatry is the specialty where the note is the exam. There is no x-ray, no lab, no palpable mass — the chart captures the patient's internal experience, the clinician's observations, and the reasoning behind every decision. A sloppy psychiatric note is indefensible; a great one saves lives. Great psychiatric scribes listen for the things that do not make it into the patient's words: the long pause before answering, the flat tone, the disheveled appearance, the wife who keeps correcting the timeline. They document risk explicitly every time, even when the answer is "denies SI/HI," because the absence of documentation is a legal and clinical failure.
Learn to hear DSM criteria inside a conversation. When a patient describes "not sleeping and having a million ideas," you should already be thinking manic episode and pre-filling the MSE fields. Know your rating scales cold — PHQ-9, GAD-7, C-SSRS, CIWA, COWS — because you will administer and score them every day. Know your medications by class, mechanism, and monitoring requirements. Respect patient dignity in every word you write. This is documentation of the most private parts of a person's life.
Welcome to psychiatry. The work is hard, the stakes are real, and the documentation matters.