Sports Medicine
Every diagnosis, injury, procedure, medication, classification, and documentation framework you need to succeed in a sports medicine clinic from day one.
All diagrams on this page are sourced from published educational or institutional materials rather than AI generation. Each figure caption links to the original source, and the full diagram and guideline citations are collected in the references section at the bottom.
01 Musculoskeletal Anatomy & Exercise Physiology
Sports medicine is the diagnosis, treatment, rehabilitation, and prevention of injuries related to physical activity. The field spans nonoperative orthopedics, primary care sports medicine, athletic training, and return-to-play decision-making. A scribe in a sports medicine clinic will hear joint-by-joint anatomy, tendon and ligament names, and mechanism-of-injury terminology constantly. Mastering the major structures up front is mandatory.
Bones, Joints & The Kinetic Chain
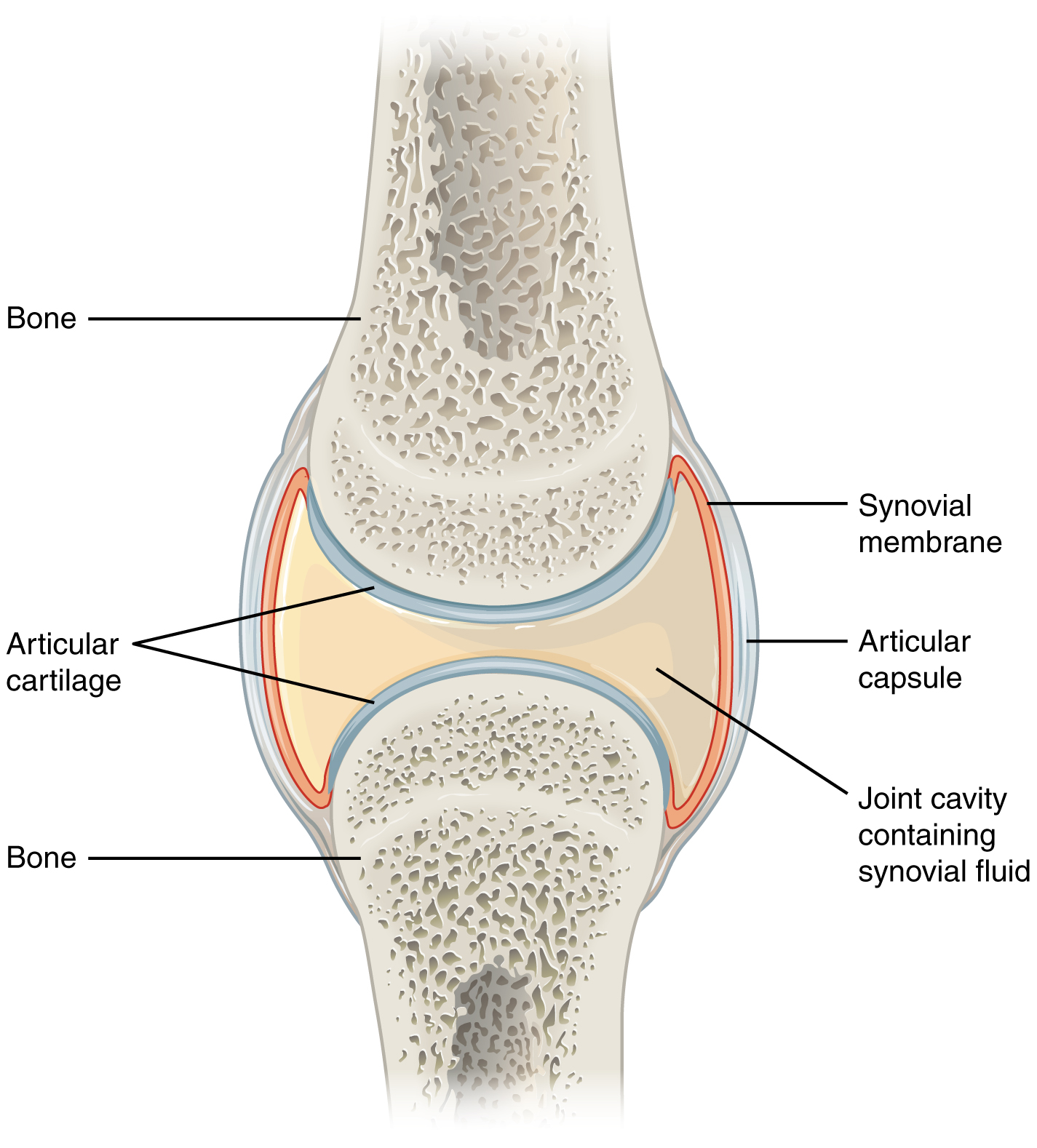
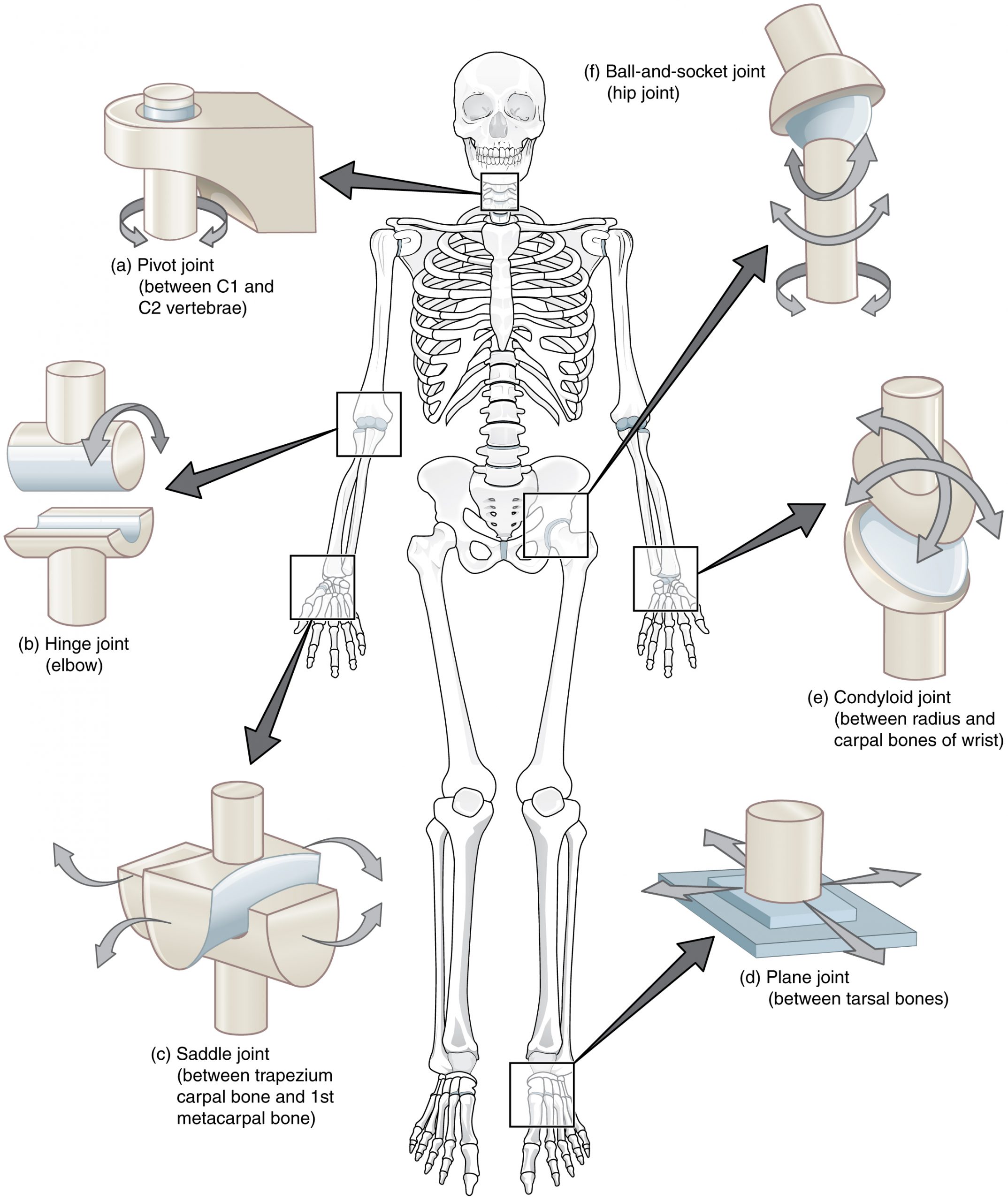
The skeleton has 206 bones organized into axial (skull, spine, thorax) and appendicular (limbs, girdles) components. Joints are classified functionally as synarthroses (immovable, e.g., skull sutures), amphiarthroses (slightly movable, e.g., pubic symphysis), and diarthroses (freely movable synovial joints — the joints sports medicine cares about). Synovial joints contain articular (hyaline) cartilage, synovial fluid, a fibrous capsule, and stabilizing ligaments. The kinetic chain is the concept that force generated in one segment (e.g., the hip) transfers through the trunk to produce motion at a distal segment (e.g., the shoulder in throwing). Breakdown anywhere in the chain — weak hips, poor core, scapular dyskinesis — shifts load and causes injury.
Muscle, Tendon & Ligament
Skeletal muscle is composed of type I (slow-twitch, oxidative, endurance) and type II (fast-twitch, glycolytic, power) fibers. Muscles attach to bone via tendons (dense regular connective tissue, collagen type I) at the myotendinous junction, which is the most common site of muscle strain. Ligaments connect bone to bone and stabilize joints; they are less vascular than tendons and heal slowly. Sprains are ligament injuries; strains are muscle/tendon injuries.
Key Regional Anatomy Cheat Sheet
- Shoulder: glenohumeral (GH) joint, acromioclavicular (AC) joint, sternoclavicular (SC) joint, scapulothoracic articulation. Rotator cuff = SITS (supraspinatus, infraspinatus, teres minor, subscapularis). Long head of biceps tendon runs in the bicipital groove.
- Elbow: humeroulnar, radiocapitellar, and proximal radioulnar joints. UCL (ulnar collateral ligament) resists valgus stress; LCL complex resists varus/posterolateral rotatory instability. Common extensor tendon origin at lateral epicondyle; common flexor/pronator origin at medial epicondyle.
- Wrist/hand: distal radius, distal ulna, 8 carpal bones (mnemonic: Some Lovers Try Positions That They Cannot Handle — scaphoid, lunate, triquetrum, pisiform, trapezium, trapezoid, capitate, hamate). TFCC (triangular fibrocartilage complex) stabilizes the ulnar wrist.
- Spine: 7 cervical, 12 thoracic, 5 lumbar vertebrae plus sacrum/coccyx. Pars interarticularis is the bony bridge whose stress fracture = spondylolysis.
- Hip/pelvis: ball-and-socket femoroacetabular joint with labrum. Hip flexors = iliopsoas; adductors arise from pubis; hamstrings originate at ischial tuberosity.
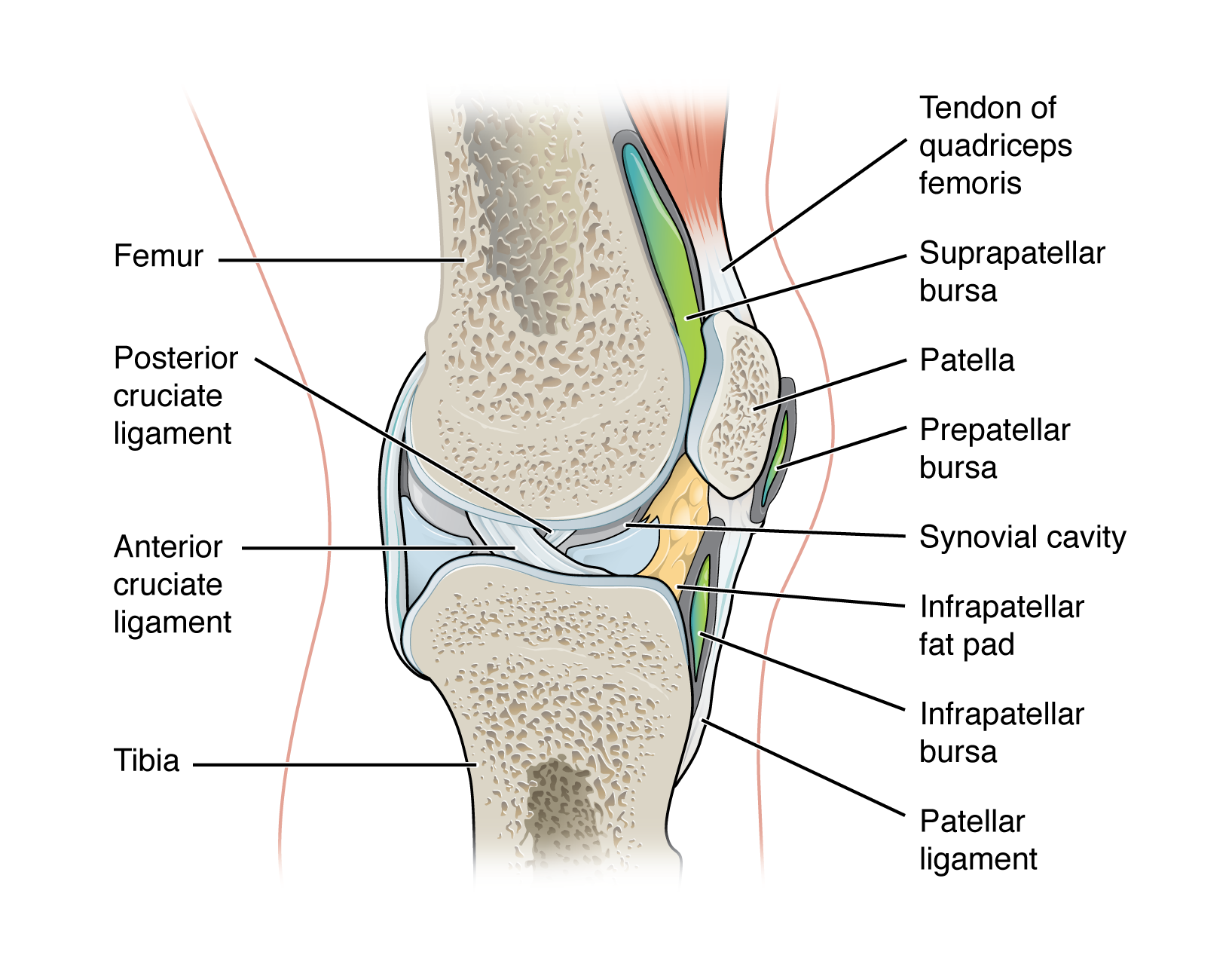
- Knee: tibiofemoral and patellofemoral joints. Four major ligaments: ACL, PCL, MCL, LCL. Two menisci (medial, lateral). Extensor mechanism: quadriceps → patella → patellar tendon → tibial tubercle.
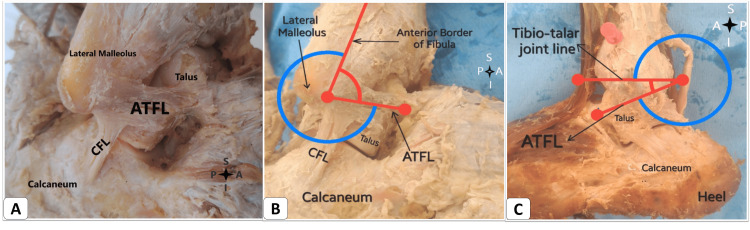
- Ankle/foot: Lateral ligaments = ATFL, CFL, PTFL (anterior talofibular, calcaneofibular, posterior talofibular). Medial deltoid ligament. Syndesmosis (high ankle) = AITFL + interosseous membrane. Plantar fascia spans calcaneus to metatarsal heads.
Exercise Physiology Essentials
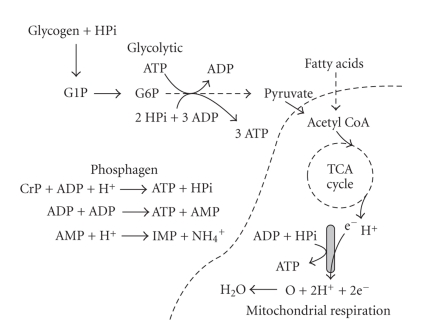
Aerobic energy production uses oxidative phosphorylation to sustain prolonged, low-to-moderate intensity activity; anaerobic glycolysis fuels short bursts via lactate production. VO2max is the peak rate of oxygen consumption and the benchmark of aerobic fitness. Lactate threshold, heart rate reserve, and rating of perceived exertion (RPE) are practical tools for exercise prescription. Strength training produces hypertrophy (fiber size increase) and neural adaptation. Adequate recovery (sleep, nutrition, hydration) is essential; failure of recovery produces overtraining syndrome.
Learn the joint vocabulary cold. When the physician says "positive Neer, positive Hawkins, painful arc 70 to 120 degrees," you must recognize this immediately as subacromial impingement testing. Never wait until the visit ends to look up exam maneuvers.
02 Scribe Documentation Framework
The Sports Medicine SOAP Note
Sports medicine visits are usually structured as SOAP notes with strong emphasis on mechanism of injury, sport/position, training volume, and return-to-play timeline. The HPI is often longer and more mechanism-focused than a typical primary care visit.
Chief Complaint: The body part and the sport context. Examples: "right knee pain after soccer tackle," "left shoulder pain in a pitcher," "concussion evaluation after football helmet-to-helmet contact."
HPI elements specific to sports medicine: Sport and position, level of play (recreational, high school, collegiate, professional), dominant side, mechanism of injury (contact vs noncontact, direction of force, foot-planted-or-not, audible pop), immediate ability to continue play, initial treatment (ice, brace, crutches), prior injury to the same body part, training volume and changes, equipment or footwear change, goals and upcoming events (season opener, playoffs, marathon).
OLDCARTS still applies but layer the above on top. Always document mechanism, swelling timeline (rapid swelling = hemarthrosis / ACL or fracture), and giving way or locking.
Past history: Prior injuries, surgeries, concussion history (number and dates), prior imaging, PT participation, PPE clearance history, family history of sudden cardiac death, and medications including NSAID use and any supplements.
Vitals: Standard. For concussion visits, always capture BP, HR, and orthostatics if indicated.
Physical exam: Inspection (swelling, ecchymosis, deformity, asymmetry, atrophy), palpation (tenderness by landmark), range of motion (active and passive, with degrees), strength (0-5 MRC scale), neurovascular exam distal to the injury, and joint-specific special tests (Lachman, McMurray, Neer, Hawkins, Thompson, etc.).
Imaging/results: Plain radiographs read in clinic, MRI findings, in-office ultrasound. Always document specific findings rather than "abnormal."
Working diagnosis with laterality and ICD-10. Plan typically includes: activity restrictions (no cutting/pivoting, non-weight-bearing, sling immobilization), imaging orders, brace/DME, PT referral with specific protocol, medications, injection plan, and clearly stated return-to-play timeline. Always document the patient's understanding and agreement.
Every sports medicine note should answer three questions explicitly: (1) What is the diagnosis? (2) What can the athlete do and not do today? (3) When and under what conditions can they return to sport? Leaving any of these vague is the most common scribe error.
03 Shoulder Injuries Upper Extremity
The shoulder is the most mobile joint in the body and the most commonly injured upper extremity region in overhead athletes. Injuries fall into overuse tendinopathies, traumatic tears, and instability events.
Rotator Cuff Tendinopathy & Tears
The rotator cuff (SITS muscles) stabilizes the humeral head in the glenoid and powers rotation. Supraspinatus is the most commonly injured — it runs beneath the acromion and is compressed by repetitive overhead motion. Tendinopathy is a degenerative, noninflammatory process characterized by disorganized collagen. Tears are classified as partial-thickness (bursal, articular, or intrasubstance) or full-thickness (small <1 cm, medium 1-3 cm, large 3-5 cm, massive >5 cm or involving ≥ 2 tendons per the Cofield classification).
Patients present with lateral deltoid pain, night pain (classic red flag for cuff pathology), weakness with overhead activity, and inability to sleep on the affected side. Exam shows positive Jobe (empty can), Neer, and Hawkins-Kennedy signs; weakness on external rotation (infraspinatus) or internal rotation lift-off (subscapularis) localizes the torn tendon. Diagnosis is confirmed with MRI or ultrasound. Management for tendinopathy and small partial tears is nonoperative (PT, NSAIDs, subacromial corticosteroid injection). Full-thickness tears in active patients are usually referred for arthroscopic repair, guided in part by AAOS clinical practice guidelines on rotator cuff injury.
Subacromial Impingement
Mechanical compression of the supraspinatus and subacromial bursa between the humeral head and the acromion, classically worsened by repetitive overhead activity. Neer described an impingement continuum from edema (stage I) to fibrosis (stage II) to tear (stage III). Treatment is rehab-focused with scapular stabilization and posterior capsule stretching.
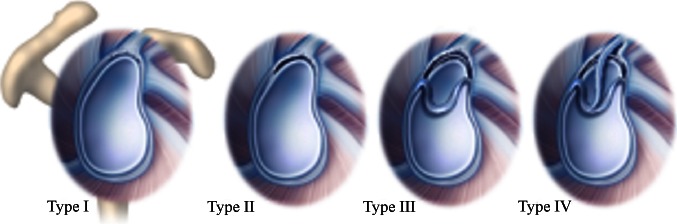
SLAP Lesion
Superior labrum anterior to posterior tear, most common in throwers and patients with a fall on outstretched arm. Causes deep shoulder pain, painful popping/clicking, and decreased throwing velocity. O'Brien active compression test is classic. MRA is the imaging gold standard. Type II (detachment of biceps anchor) is most common.
AC Joint Sprain / Separation
Direct blow to the lateral shoulder (fall, football tackle). Classified Rockwood I-VI (see classification section). Grades I-II managed in a sling with early ROM; grades IV-VI typically surgical.
Biceps Tendinopathy, Long Head Rupture
Anterior shoulder pain at the bicipital groove; Speed and Yergason tests positive. Rupture of the long head of biceps produces the classic "Popeye deformity" and is usually managed nonoperatively in older patients because the short head preserves most function.
Glenohumeral Instability
Anterior dislocations account for 95% (force on abducted, externally rotated arm). A Bankart lesion (anteroinferior labral tear) or Hill-Sachs lesion (posterolateral humeral head impaction) is typical. First-time dislocation in young athletes has a >80% recurrence rate and is often referred for arthroscopic stabilization.
Thrower's Shoulder (Internal Impingement, GIRD)
Pitchers and overhead throwers develop posterior capsule tightness and humeral retroversion, causing glenohumeral internal rotation deficit (GIRD). Leads to posterosuperior labral contact, SLAP lesions, and partial undersurface cuff tears.
Adhesive Capsulitis (Frozen Shoulder)
Progressive stiffening with loss of both active and passive ROM, especially external rotation. Three phases: freezing (painful, 2-9 months), frozen (stiff, 4-12 months), thawing (gradual recovery, 12-24+ months). Associated with diabetes and thyroid disease. Managed with PT, injection, and occasionally capsular release or hydrodilation.
For every shoulder patient, document dominant hand, sport/position, and whether pain is worse at night. Night pain is the classic rotator cuff tell, and clinicians will reliably ask about it.
04 Elbow Injuries Upper Extremity
Lateral Epicondylitis (Tennis Elbow)
Tendinopathy of the common extensor origin (extensor carpi radialis brevis most involved). Pain over the lateral epicondyle reproduced with resisted wrist extension or middle finger extension (Maudsley test) and with a handshake grip. Managed with counterforce brace, eccentric wrist extensor strengthening, NSAIDs, and occasional corticosteroid or PRP injection. Recent evidence supports PRP over corticosteroid for durable relief, reflected in updated AMSSM positioning.
Medial Epicondylitis (Golfer's Elbow)
Common flexor/pronator origin tendinopathy. Pain with resisted wrist flexion and pronation. Frequently coexists with ulnar neuropathy at the cubital tunnel.
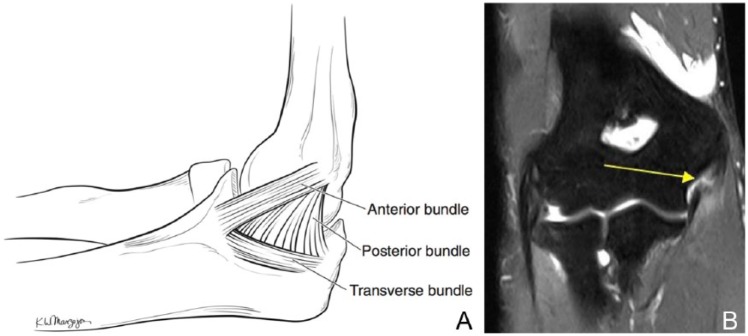
UCL Injury (Tommy John)
Valgus overload in overhead throwers (especially pitchers) causes ulnar collateral ligament injury. Patients describe a pop, sudden loss of velocity, and medial elbow pain. Milking maneuver and moving valgus stress test are classic. MRI or MRA defines the tear. Nonoperative rehab is possible for low-grade injuries; competitive throwers usually undergo UCL reconstruction ("Tommy John surgery") with palmaris longus or gracilis graft.
Olecranon Bursitis
Swelling of the olecranon bursa from direct trauma (wrestler, hockey player) or repetitive friction. Must distinguish septic from aseptic — aspiration with cell count, Gram stain, and culture is indicated if warm, red, or febrile.
Distal Biceps Rupture
Forced eccentric load on the flexed elbow (classically catching a falling object). "Reverse Popeye deformity," positive hook test. Surgical repair within 2-3 weeks recommended in active patients to restore supination strength.
Little League Elbow
Medial epicondyle apophysitis or avulsion in skeletally immature pitchers from repetitive valgus stress. USA Baseball pitch-count guidelines exist to prevent this. Rest and pitch-count education are key.
05 Wrist & Hand Injuries Upper Extremity
TFCC Injury
The triangular fibrocartilage complex stabilizes the distal radioulnar joint and the ulnar carpus. Ulnar-sided wrist pain with gripping and forearm rotation; positive TFCC load and press tests. Palmer classification (I traumatic, II degenerative). MRA is diagnostic.
Scaphoid Fracture
Fall on outstretched hand with anatomic snuffbox tenderness. Initial plain films miss up to 20%. If exam is consistent with scaphoid fracture, thumb spica splint and repeat imaging or MRI in 10-14 days. Proximal pole fractures carry high nonunion/avascular necrosis risk because blood supply is retrograde from the distal pole.
Hook of Hamate Fracture
Classic in baseball, golf, tennis (bat or club strikes hypothenar eminence). Hypothenar pain with gripping. Carpal tunnel view or CT confirms. Often requires excision if symptomatic.
Trigger Finger
Stenosing tenosynovitis at the A1 pulley. Painful catching or locking during finger flexion. Managed with splinting and corticosteroid injection; surgical release for refractory cases.
Mallet, Jersey, and Jammed Finger
Mallet finger = forced flexion of extended DIP avulses the terminal extensor tendon; patient cannot extend DIP. Splint in extension 6-8 weeks continuously. Jersey finger = forced extension of flexed DIP avulses FDP tendon (ring finger most common, "grabbing a jersey"); requires surgical repair within 1-2 weeks for best outcome. Jammed finger is the catch-all for PIP sprains — buddy tape after excluding volar plate injury, fracture, or dislocation.
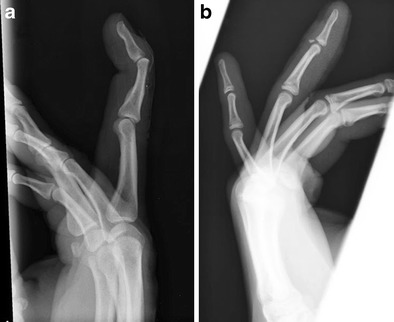
Boxer's Fracture
Fifth metacarpal neck fracture from a closed-fist punch. Acceptable angulation ≤40 degrees in the small finger. Ulnar gutter splint, orthopedic follow-up if rotational deformity or significant angulation.
06 Cervical & Lumbar Spine Injuries Spine
Cervical Strain / Sprain (Whiplash)
Acceleration-deceleration mechanism (football tackle, MVC). Paraspinal pain and limited ROM without neurologic findings. Imaging only if red flags (NEXUS or Canadian C-spine rule positive). Short course of NSAIDs, soft collar <72 hours, early mobilization, PT.
Stinger / Burner
Transient unilateral upper extremity burning, numbness, and weakness following a tackle. Mechanism is brachial plexus traction or nerve root compression (C5-C6). Symptoms typically resolve within minutes to hours. Bilateral or prolonged symptoms require cervical imaging and neurosurgical evaluation — this is never a stinger and raises concern for transient quadriparesis or cord injury.
Transient Quadriparesis / Cervical Cord Neurapraxia
Bilateral burning, numbness, or weakness in all four extremities after axial cervical load. Associated with congenital cervical stenosis (Pavlov ratio <0.8). MRI is mandatory. Return to contact sport is controversial and requires stability of the cervical spine and absence of cord signal change.
Lumbar Strain / Sprain
Most common cause of low back pain in athletes. Paraspinal tenderness without radicular symptoms. Activity modification, NSAIDs, PT with core stabilization.
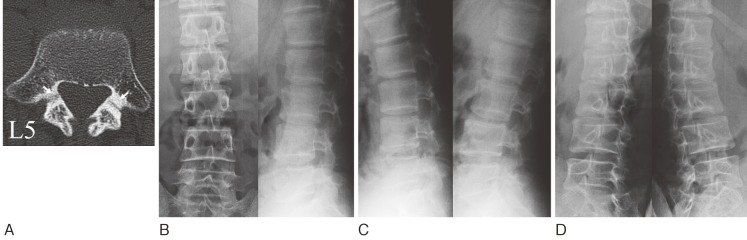
Spondylolysis & Spondylolisthesis
Spondylolysis is a pars interarticularis stress fracture, most common at L5, and the leading cause of low back pain in adolescent athletes (gymnasts, divers, football linemen, cheerleaders). Pain with lumbar extension, positive single-leg hyperextension (stork) test. Plain films may be normal; MRI with STIM or SPECT/CT is sensitive. Spondylolisthesis is forward slippage of one vertebra on another (usually L5 on S1), graded Meyerding I-IV (see classification section). Treatment is activity modification, bracing (controversial), core rehab; surgery for slips progressing beyond grade II or with neurologic deficit.
Lumbar Disc Herniation
Radicular pain following a dermatomal pattern, with positive straight leg raise. MRI confirms. Most (>80%) resolve nonoperatively over 6-12 weeks. Surgery indicated for progressive neurologic deficit, cauda equina syndrome, or refractory pain.
Sacroiliac Dysfunction
Unilateral buttock pain localized to the SI joint. FABER (Patrick), Gaenslen, thigh thrust, compression, and distraction tests. Three positive provocation tests increases likelihood. Managed with PT, NSAIDs, and occasionally fluoroscopy-guided SI joint injection.
07 Hip & Pelvis Injuries Lower Extremity
Hip Flexor & Adductor Strains
Iliopsoas or rectus femoris strains present with anterior hip/groin pain after sprinting or kicking. Adductor strains produce medial groin pain. Graded I-III. Managed with rest, ice, progressive PT; most return to play in 2-6 weeks depending on grade.
Sports Hernia / Athletic Pubalgia
Chronic groin pain from posterior inguinal wall weakness or rectus abdominis/adductor longus aponeurosis disruption. No true hernia is present. Pain with resisted sit-up and adduction. MRI may show pubic bone edema or aponeurotic tear. Initial PT; refractory cases referred for surgical repair.
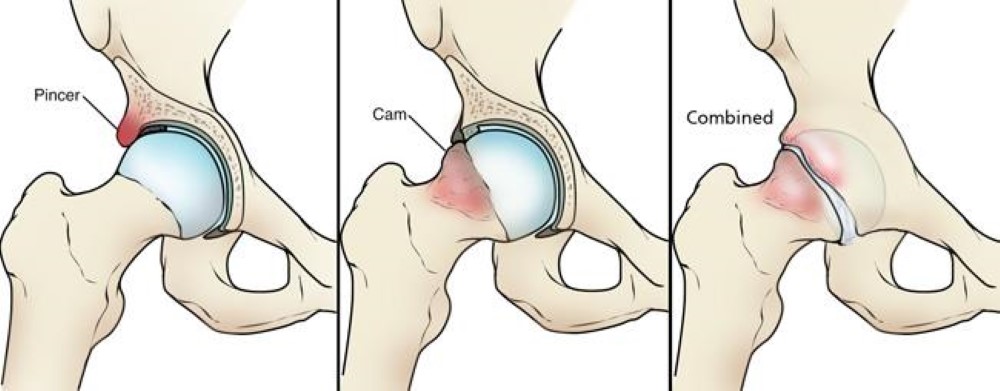
Hip Labral Tear & Femoroacetabular Impingement (FAI)
FAI is abnormal contact between the femoral head-neck and acetabulum, classified as cam (aspherical femoral head), pincer (over-coverage by the acetabulum), or mixed. Chronic impingement tears the labrum. Patients present with anterior groin pain, a positive FADIR (flexion-adduction-internal rotation) test, and a "C sign" when describing pain location. MRA is diagnostic. Management is PT first; arthroscopic labral repair and osteoplasty for refractory symptomatic cases.
Iliopsoas Snapping (Internal Snapping Hip)
Audible, palpable snap of the iliopsoas tendon over the iliopectineal eminence. Usually painless and managed with PT.
Piriformis Syndrome
Deep gluteal pain with sciatic nerve irritation as it passes through/around the piriformis. Pain with prolonged sitting, positive FAIR test. Stretching, PT, occasional injection.
Gluteus Medius Tendinopathy (Greater Trochanteric Pain Syndrome)
Lateral hip pain with side-lying and single-leg stance. Tendinopathy of the gluteus medius/minimus at the greater trochanter. PT focusing on hip abductor strengthening.
Hamstring Strain
Posterior thigh pain with sprinting, typically at the biceps femoris myotendinous junction. Graded I-III. Recurrent hamstring strain is extremely common — inadequate rehab is the main risk. British Athletics classification (BAMIC) categorizes by location and grade.
Avulsion Fractures of the Pelvis
Adolescent athletes avulse apophyses at muscle origins: ASIS (sartorius), AIIS (rectus femoris), ischial tuberosity (hamstrings), lesser trochanter (iliopsoas), pubic symphysis (adductors), iliac crest (abdominal wall). Plain films diagnostic. Most treated nonoperatively.
08 Knee Injuries Lower Extremity
The knee is the highest-volume body part in most sports medicine clinics. Scribes should become fluent in ACL, meniscus, and patellofemoral vocabulary before anything else.
ACL Tear
Noncontact pivot (plant-and-cut), audible pop, immediate hemarthrosis (within 2 hours), and inability to return to play. Lachman test is the most sensitive exam; anterior drawer and pivot shift support the diagnosis. MRI confirms and evaluates associated meniscus and MCL injury (O'Donoghue's unhappy triad: ACL + MCL + medial meniscus). Young, active athletes are typically offered ACL reconstruction with autograft (bone-patellar tendon-bone, hamstring, or quadriceps tendon). Return to sport is typically 9-12 months per AMSSM consensus on ACL return to sport.
MCL, LCL, and PCL Injuries
MCL sprains result from valgus load; LCL from varus. Most isolated MCL injuries heal nonoperatively with hinged knee brace. PCL tears occur with direct anterior blow to the proximal tibia (dashboard injury, falling on flexed knee). Posterior drawer is the key exam. Most isolated PCL injuries are treated nonoperatively.
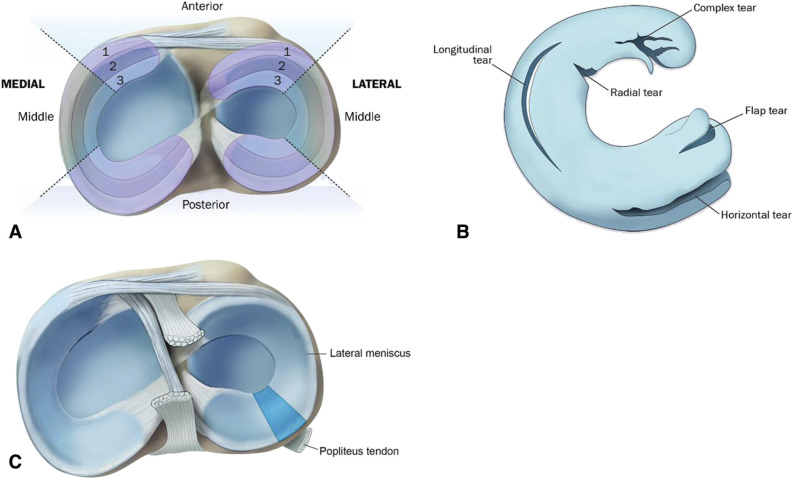
Meniscus Tears
Acute tears (twisting injury) vs degenerative tears (no clear trauma, middle-aged). Joint line tenderness, McMurray and Thessaly tests positive. MRI confirms and characterizes (bucket handle, radial, horizontal, root tear). Root tears and displaced bucket handles warrant early surgical consideration; many degenerative tears are managed nonoperatively per contemporary evidence.
Patellar Tendinopathy (Jumper's Knee)
Infrapatellar pain in jumping athletes. Eccentric decline squats are first-line rehab; PRP or surgery for refractory cases.
Patellofemoral Pain Syndrome (Runner's Knee)
Anterior knee pain worse with stairs, squatting, prolonged sitting ("theater sign"). Often multifactorial: weak hip abductors, quad tightness, overpronation. PT with hip/core strengthening is first-line.
IT Band Syndrome
Lateral knee pain at the lateral femoral epicondyle in runners and cyclists. Ober test tight. Foam rolling, hip strengthening, mileage reduction.
Patellar Dislocation / Subluxation
Usually lateral dislocation in young females with patellar maltracking. Relocates with knee extension. First-time dislocation managed nonoperatively; recurrent instability may warrant MPFL reconstruction.
Osteochondritis Dissecans (OCD)
Subchondral bone lesion (most often medial femoral condyle) in adolescents. May cause locking or effusion. Stable lesions heal with activity restriction; unstable lesions require surgical fixation.
Plica Syndrome
Inflammation of a synovial plica (medial most common). Medial snapping and pain. PT first; arthroscopic resection occasionally.
Osgood-Schlatter & Sinding-Larsen-Johansson
Apophysitis of the tibial tubercle (Osgood-Schlatter) and inferior pole of the patella (Sinding-Larsen-Johansson), both in adolescent athletes. Activity modification, ice, and stretching. Self-limited with skeletal maturity.
09 Lower Leg & Stress Injuries Lower Extremity
Medial Tibial Stress Syndrome (Shin Splints)
Diffuse tenderness along the posteromedial tibia in runners, usually early in training. Rest, ice, gait analysis, gradual return. If focal tenderness and night pain, suspect tibial stress fracture.
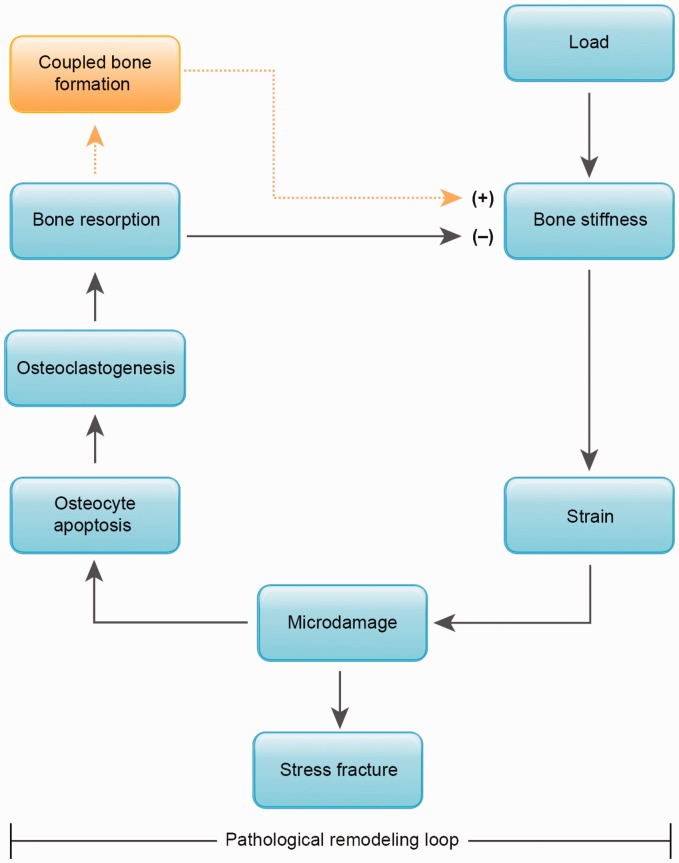
Stress Fractures
Overuse bone injuries from repetitive loading. Low-risk sites (posteromedial tibia, fibula, most metatarsals) heal well with rest. High-risk sites (anterior tibial cortex, femoral neck tension side, navicular, proximal fifth metatarsal (Jones), great toe sesamoids, talus, medial malleolus) can progress to complete fracture, nonunion, or avascular necrosis and often need non-weight-bearing or surgical fixation. MRI is the most sensitive imaging; plain films may show periosteal reaction or the "dreaded black line" on the anterior tibial cortex. Always assess for the female athlete triad in recurrent stress fractures.
Chronic Exertional Compartment Syndrome
Exercise-induced muscle compartment pain that resolves with rest. Compartment pressure testing pre- and post-exercise is diagnostic (post-exercise >30 mmHg at 1 min or >20 mmHg at 5 min). Fasciotomy is the definitive treatment if refractory.
10 Ankle & Foot Injuries Lower Extremity
Lateral Ankle Sprain
Inversion mechanism. ATFL injured most often, then CFL, rarely PTFL. Use the Ottawa ankle rules to decide on radiographs. Grade I-III based on ligament disruption and instability. Functional rehab with bracing, proprioceptive training, and early weight-bearing is superior to prolonged immobilization per NATA position statement on ankle sprain.
Medial (Deltoid) Ankle Sprain
Eversion mechanism, less common than lateral. Always rule out syndesmotic injury and Maisonneuve fracture (proximal fibula + deltoid).
High Ankle / Syndesmotic Sprain
External rotation with a dorsiflexed foot. Pain with the squeeze test, external rotation stress, and proximal to the joint line. Longer recovery than lateral sprain (6-12+ weeks). Unstable injuries require surgical stabilization.
Achilles Tendinopathy & Rupture
Tendinopathy: midportion (2-6 cm above insertion) or insertional. Eccentric loading (Alfredson protocol) is evidence-based first-line therapy. Acute Achilles rupture: sudden "kick to the back of the leg" sensation, positive Thompson test (no plantarflexion with calf squeeze), palpable gap. Operative and functional nonoperative protocols both yield good results in selected patients.
Plantar Fasciitis
Heel pain, worst with first steps in the morning. Tenderness at the medial calcaneal tuberosity. Stretching, night splints, heel cushions, and plantar-specific stretching protocols; injection and extracorporeal shock wave therapy for refractory cases.
Peroneal Tendon Subluxation
Posterolateral ankle pain and popping, usually after forced dorsiflexion/inversion. SPR (superior peroneal retinaculum) injury. Brace trial; surgery for recurrent subluxation.
Sinus Tarsi Syndrome
Lateral foot pain after recurrent ankle sprains. Tenderness at the sinus tarsi. PT, bracing, occasional injection.
Lisfranc Injury
Tarsometatarsal joint complex disruption from axial load on a plantarflexed foot. Plantar ecchymosis is pathognomonic. Weight-bearing radiographs may show widening between the first and second metatarsals. CT or MRI clarifies. Most require surgical fixation — missed Lisfranc injuries produce chronic midfoot arthritis.
Turf Toe
Hyperextension injury to the first MTP capsuloligamentous complex, common on artificial turf. Graded I-III. Grade III requires prolonged immobilization or surgery.
Sesamoiditis & Morton's Neuroma
Sesamoiditis: pain under the first metatarsal head from repetitive loading (runners, dancers). Rest, offloading pad. Morton's neuroma: interdigital nerve (usually 3rd webspace), pain with walking and a "rock in the shoe" sensation, positive Mulder's click. Metatarsal pad, wide toe box, corticosteroid injection, surgical excision for refractory cases.
11 Concussion & Head Injury Neurologic
Concussion is a traumatic brain injury induced by biomechanical forces, producing a functional disturbance without structural abnormality on standard imaging. It is a clinical diagnosis. Sports concussion management is governed by the 2023 Amsterdam CISG Consensus Statement on Concussion in Sport, which updates the Berlin 2016 framework.
Clinical Presentation
Symptoms cluster into four domains: somatic (headache, dizziness, nausea, photophobia, phonophobia), cognitive (fogginess, slowed processing, poor concentration), emotional (irritability, sadness), and sleep (insomnia, hypersomnia). Loss of consciousness occurs in only ~10%. Red flags that demand emergency imaging and neurosurgical evaluation include GCS <15, focal deficit, seizure, repeated vomiting, worsening headache, and signs of cervical spine injury.
SCAT6 / Child SCAT6 Sideline Assessment
The Sport Concussion Assessment Tool (currently version 6, formerly SCAT5) is the sideline standard. Components include:
- Red flag screen and cervical spine assessment
- Immediate observable signs (loss of consciousness, balance problems, blank stare, impact seizure)
- Glasgow Coma Scale
- Maddocks questions (orientation: venue, quarter, last scorer, last game, did we win?)
- Symptom evaluation (22-item checklist, 0-6 severity each)
- Cognitive screening (orientation, immediate memory, concentration, delayed recall)
- Neurologic screen (reading, balance, coordination)
- Balance examination via modified Balance Error Scoring System (mBESS) — double leg, single leg, and tandem stance with errors counted
Historical Concussion Grading
Modern practice has moved away from grading toward symptom-based individualized management, but historical scales still appear in documentation:
| Scale | Grade I | Grade II | Grade III |
|---|---|---|---|
| Cantu (historical) | No LOC, PTA <30 min | LOC <1 min or PTA 30 min-24 h | LOC >1 min or PTA >24 h |
| AAN (historical) | No LOC, symptoms <15 min | No LOC, symptoms >15 min | Any LOC |

Graduated Return-to-Sport Protocol (6 Stages)
- Stage 1 — Symptom-limited activity. Daily activities that do not provoke symptoms (24-48 hours of relative rest).
- Stage 2 — Light aerobic exercise. Walking or stationary cycling at slow-to-medium pace, no resistance.
- Stage 3 — Sport-specific exercise. Running drills, skating drills. No head impact activities.
- Stage 4 — Noncontact training drills. More complex drills, passing, progressive resistance training.
- Stage 5 — Full contact practice. Following medical clearance, normal training activities.
- Stage 6 — Return to sport. Normal game play.
Each stage is at least 24 hours; if symptoms recur, the athlete drops back to the previous asymptomatic stage. Return to learn precedes return to play. The Zackery Lystedt Law in Washington was the first state law mandating concussion education, removal from play, and written clearance — all 50 states now have similar legislation.
Second Impact Syndrome
Catastrophic cerebral edema and loss of autoregulation after a second head impact before a first concussion has fully resolved. Rare but devastating. Rigid enforcement of return-to-play rules is the only prevention.
When documenting a concussion visit, explicitly capture: injury date and mechanism, LOC (yes/no and duration), amnesia (antegrade/retrograde, duration), current symptoms by domain, current stage in the return-to-play progression, and the specific restrictions in place (no contact, light aerobic only, academic accommodations). Vague concussion notes are a liability.
12 Medical Issues in Athletes Medical
Exercise-Induced Bronchoconstriction (EIB)
Transient airway narrowing triggered by exercise. Common in endurance and cold-weather athletes. Symptoms: cough, wheeze, chest tightness 5-15 minutes after exercise onset, resolving with rest. Diagnosis by exercise challenge or eucapnic voluntary hyperventilation (not peak flow alone). Pre-exercise short-acting beta-agonist (albuterol) 15 minutes prior is first-line; daily inhaled corticosteroid if frequent.
Exercise-Induced Anaphylaxis
Urticaria, angioedema, wheezing, hypotension during or after exertion, sometimes with a cofactor (food, NSAID). Epinephrine autoinjector carriage is mandatory.
Anemia in Athletes
Differentiate dilutional "sports anemia" (plasma volume expansion, benign) from true iron-deficiency anemia (low ferritin, microcytic). Common in distance runners and female athletes. Treat iron deficiency; avoid empiric supplementation without labs.
Overtraining Syndrome
Chronic fatigue, performance decline, mood disturbance, sleep disruption after sustained high training load with inadequate recovery. Diagnosis of exclusion. Treatment is extended rest (weeks to months).
Exertional Sickling
Sickle cell trait athletes can develop rhabdomyolysis, collapse, and death during intense conditioning, especially in heat or altitude. NCAA mandates universal sickle cell trait screening. Education and graduated conditioning are key.
Exertional Rhabdomyolysis
Muscle breakdown with CK elevation, myoglobinuria ("tea-colored urine"), and acute kidney injury. Aggressive IV hydration and electrolyte monitoring. Return to activity is cautious and graduated.
13 Cardiovascular Issues & Sudden Cardiac Death Cardiac
Sudden cardiac death (SCD) in athletes is rare (~1 per 50,000-80,000 per year) but catastrophic. The preparticipation physical evaluation (PPE) is the primary screening tool. The AHA/ACC 14-element cardiovascular screening guides history and exam; ECG screening remains controversial in the US and routine in many European and FIFA programs.
Causes of SCD
- Hypertrophic cardiomyopathy (HCM) — most common cause in US athletes. Asymmetric septal hypertrophy, dynamic LVOT obstruction, risk of ventricular arrhythmia.
- Coronary artery anomalies — anomalous origin from the opposite sinus, interarterial course.
- Arrhythmogenic right ventricular cardiomyopathy (ARVC) — fibrofatty RV replacement.
- Long QT, Brugada, CPVT — primary electrical channelopathies.
- Commotio cordis — blunt chest trauma during vulnerable repolarization phase inducing VF. Baseball, lacrosse, hockey.
- Myocarditis — viral or post-viral; exercise restriction 3-6 months. COVID-19 updates have shaped contemporary return-to-play protocols.
Athletic Heart Syndrome
Physiologic cardiac adaptations to sustained endurance training: increased LV wall thickness, chamber enlargement, resting bradycardia. Benign and reversible with detraining. Must distinguish from pathologic hypertrophy — echo, cardiac MRI, detraining response, and genetic testing may be needed.
14 Female Athlete Triad / RED-S & Eating Disorders Medical
The female athlete triad describes the interrelationship among low energy availability (with or without disordered eating), menstrual dysfunction, and low bone mineral density. The broader Relative Energy Deficiency in Sport (RED-S) framework from the IOC acknowledges that both sexes are affected and that the consequences extend to immune, endocrine, cardiovascular, hematologic, and psychological function.
- Low energy availability: Calculated as (energy intake – exercise energy expenditure) / fat-free mass. <30 kcal/kg FFM/day is clinically low; optimal is ≥45.
- Menstrual dysfunction: Ranges from luteal phase deficiency to functional hypothalamic amenorrhea (FHA). Amenorrhea is never to be dismissed as "normal for athletes."
- Low bone mineral density: Z-score ≤-1.0 with risk factors or Z-score ≤-2.0 is concerning. Increased stress fracture risk.
Management is multidisciplinary: sports medicine physician, sports dietitian, mental health, and coach. Increasing energy availability is the foundation. Estrogen-progestin therapy has not been shown to restore bone density in FHA and is not the preferred treatment — correcting energy deficit is. Eating disorders (anorexia nervosa, bulimia, binge-eating, OSFED) are overrepresented in aesthetic and weight-class sports; use validated screening tools.
15 Environmental & Exertional Illness Emergency
Exertional Heat Illness Spectrum
- Heat cramps: Painful muscle cramps, likely sodium depletion. Rest, oral hydration with electrolytes.
- Heat exhaustion: Fatigue, dizziness, nausea, rectal temp typically <40°C (104°F), intact mental status. Move to shade, passive cooling, oral fluids.
- Exertional heat stroke: Rectal temp >40°C PLUS CNS dysfunction (confusion, ataxia, coma, seizure). Medical emergency. Cold water immersion is the gold standard treatment — cool first, transport second. Target core temp <39°C before transport per NATA position statement on exertional heat illness.
Never use oral temperature or axillary temperature to evaluate suspected exertional heat stroke — always rectal. Every venue for football practice in August should have an ice immersion tub ready.
Other Environmental Concerns
Hyponatremia (especially overhydration in marathons), hypothermia and frostbite in winter sports, altitude illness (AMS, HAPE, HACE) in trekking and training at altitude, and lightning safety protocols ("30-30 rule": seek shelter when flash-to-bang ≤30 sec, resume 30 min after last thunder).
16 Procedures & Office-Based Interventions Procedures
Pre-Participation Physical Evaluation (PPE)
The PPE clears athletes for sport and identifies at-risk individuals. Uses the PPE Monograph (AAP/ACSM/AMSSM/AOSSM/AAFP). History is more sensitive than exam; the 14-element AHA cardiovascular screen is embedded. Must document personal and family history of syncope, chest pain, palpitations, SCD <50, known heart disease, and Marfanoid features.
Joint & Soft Tissue Injections
| Injection | Typical Agent | Common Indication |
|---|---|---|
| Corticosteroid (intra-articular) | Triamcinolone 40 mg + lidocaine | Knee OA, subacromial bursa, trigger finger, trochanteric bursa |
| Viscosupplementation | Hyaluronic acid (Supartz, Synvisc, Euflexxa) | Knee osteoarthritis (FDA-approved) |
| Platelet-rich plasma (PRP) | Autologous PRP | Tendinopathy (lateral epicondylitis, patellar, Achilles), early knee OA |
| Prolotherapy | Dextrose 12.5-25% | Chronic tendinopathy, ligament laxity |
| Trigger point | Lidocaine or dry needling | Myofascial pain |
Ultrasound-Guided Injections
Musculoskeletal ultrasound allows real-time, needle-tip visualization for accurate placement in small or deep targets (biceps tendon sheath, piriformis, glenohumeral joint, peroneal tendon sheath, plantar fascia). High-frequency linear probe (10-15 MHz) for superficial structures; curvilinear for hip. Scribes document laterality, target, needle approach (in-plane vs out-of-plane), agent, volume, tolerance, and post-injection sensory/motor status.
Casting, Splinting, Taping, Bracing
Common immobilization: thumb spica (scaphoid), ulnar gutter (boxer's fracture), sugar tong (distal radius), short leg walking boot (metatarsal fractures, mild ankle sprain), stirrup brace (lateral ankle sprain). Kinesiotaping and athletic taping techniques: ankle taping with basketweave, patellar taping (McConnell), shoulder dyskinesis tape. Functional bracing: hinged knee brace (MCL), ACL functional brace, CAM walker.
Cardiac Clearance & Exercise Stress Testing
Bruce protocol is standard for exercise ECG. Indications include chest pain with exertion, syncope, suspected CAD prior to return to competitive sport, and evaluation of athletes with equivocal screening findings. Echocardiogram and cardiac MRI used when structural disease is suspected.
Concussion Baseline & Post-Injury Testing
Computerized neurocognitive tools (ImPACT, CNS Vital Signs, Axon) test memory, attention, processing speed, and reaction time. Baseline values in preseason allow post-injury comparison. SCAT6 is performed acutely; BESS balance testing complements the cognitive assessment. None of these replace clinical judgment.
17 Imaging & Diagnostics Imaging
Plain Radiographs
First-line for fracture, dislocation, arthritis, and bony alignment. Specific views: Ottawa knee/ankle rules (decide if XR is needed), sunrise/Merchant (patellofemoral), stress views (AC joint, syndesmosis), weight-bearing views (Lisfranc, knee OA), scaphoid view (snuffbox tenderness). Key findings the scribe documents: fracture line, displacement, angulation, joint space, effusion (fat pad sign at elbow, suprapatellar at knee), cortical irregularity.
MRI
Gold standard for ligament, tendon, cartilage, and bone marrow pathology. MRA (arthrogram) used for labral tears of shoulder and hip. Key terms scribes document: signal intensity (T2 bright = fluid/edema), bone marrow edema (stress reaction/fracture), complete vs partial tear, retraction, chondral lesion grade, meniscal tear pattern (radial, horizontal, complex, bucket handle, root).
Musculoskeletal Ultrasound
Dynamic assessment of tendons, muscles, bursae, nerves, and effusions. Real-time guidance for injections. Advantages: portable, no radiation, cheaper than MRI, dynamic. Limitations: operator-dependent, limited for deep structures.
CT
Used when fine bone detail is needed: comminuted fractures, occult scaphoid, complex articular fracture patterns, spondylolysis.
DEXA
Bone mineral density screening in female athlete triad/RED-S, recurrent stress fractures, and amenorrhea. Z-score is used in premenopausal athletes (not T-score).
18 Medications You Must Know Medications
| Class | Generic (Brand) | Mechanism | Key Use | Critical Notes |
|---|---|---|---|---|
| Oral NSAIDs | Ibuprofen (Motrin), naproxen (Aleve), celecoxib (Celebrex), meloxicam (Mobic), diclofenac (Voltaren) | COX-1/2 inhibition | Acute sprains, strains, tendinopathy, postop pain | GI, renal, CV risk; avoid with active ulcer or CKD |
| Topical NSAID | Diclofenac gel 1% | Local COX inhibition | Superficial joint/tendon pain | Lower systemic exposure; preferred when oral contraindicated |
| Acetaminophen | Tylenol | Central COX / analgesia | First-line for OA pain, pregnancy | Max 3-4 g/day; hepatotoxic in overdose |
| Muscle relaxants | Cyclobenzaprine (Flexeril), methocarbamol (Robaxin), tizanidine (Zanaflex) | CNS depression | Acute low back spasm, whiplash | Sedating; short-term only |
| Gabapentinoids | Gabapentin (Neurontin), pregabalin (Lyrica) | Alpha-2-delta channel | Neuropathic pain, radiculopathy (limited role) | Sedation, dizziness, misuse potential |
| Topical analgesics | Lidocaine 5% patch, capsaicin | Na channel / TRPV1 | Local musculoskeletal pain | Safer alternative to oral therapy |
| Intra-articular steroid | Triamcinolone, methylprednisolone | Anti-inflammatory | Knee OA flare, shoulder bursitis | Transient hyperglycemia; repeated injections may accelerate cartilage loss |
| Hyaluronic acid | Synvisc, Supartz, Euflexxa, Orthovisc | Viscosupplementation | Knee OA | Series of 1-5 injections; avoid if avian allergy (product-dependent) |
| PRP | Autologous platelet-rich plasma | Growth factor delivery | Tendinopathy, early OA | Limited standardization; cash pay |
| Bone health | Vitamin D, calcium | Mineral metabolism | Stress fracture prevention, RED-S | Target 25-OH vitamin D >40 ng/mL |
| Ergogenic (overview) | Creatine monohydrate, whey protein, BCAA | Energy substrate / protein synthesis | Athletic performance | Creatine and whey well-studied; many supplements contaminated with banned substances |
The World Anti-Doping Agency (WADA) publishes the annual Prohibited List. Categories include anabolic agents, peptide hormones (EPO, hGH), beta-2 agonists (inhaled albuterol has thresholds), diuretics and masking agents, stimulants, narcotics, cannabinoids (in-competition), and glucocorticoids (route-dependent). Therapeutic Use Exemptions (TUE) exist for legitimate medical need. Always check every prescription against the current WADA list before prescribing to a competitive athlete.
19 Classification & Outcome Scales Classification
Muscle & Ligament Injury Grading
| Grade | Muscle Strain | Ligament Sprain |
|---|---|---|
| I (mild) | <5% fiber disruption, mild pain, full strength | Stretching, no instability |
| II (moderate) | Partial tear, weakness, ecchymosis | Partial tear, mild instability |
| III (severe) | Complete rupture, palpable gap, loss of function | Complete tear, gross instability |
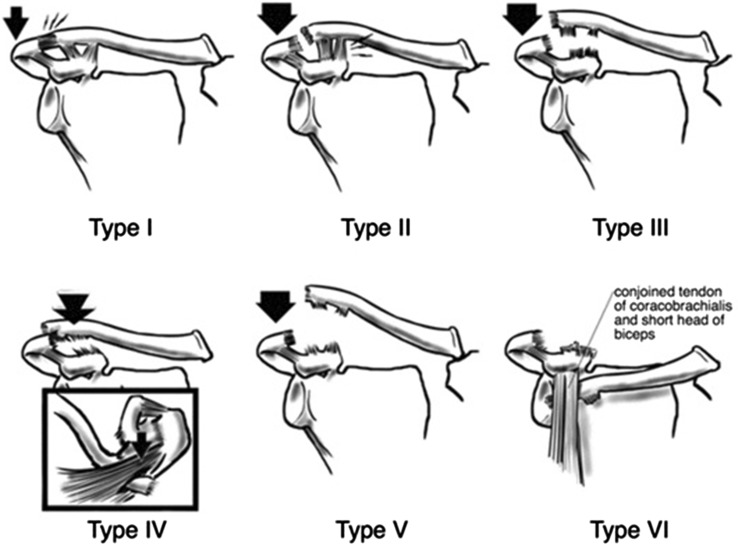
Rockwood AC Joint Separation
| Type | AC Ligament | Coracoclavicular | Displacement |
|---|---|---|---|
| I | Sprain | Intact | None |
| II | Torn | Sprained | <25% superior |
| III | Torn | Torn | 25-100% superior |
| IV | Torn | Torn | Posterior into trapezius |
| V | Torn | Torn | 100-300% superior |
| VI | Torn | Torn | Inferior (subcoracoid) |
Meyerding Spondylolisthesis Grading
| Grade | Slip Percentage | Clinical Note |
|---|---|---|
| I | 0-25% | Usually asymptomatic |
| II | 25-50% | Conservative management typical |
| III | 50-75% | Consider surgical stabilization |
| IV | 75-100% | Surgical candidate |
| V (spondyloptosis) | >100% | Complete slip, surgical |
Glasgow Coma Scale (GCS)
Eye (1-4): 4 spontaneous, 3 to voice, 2 to pain, 1 none. Verbal (1-5): 5 oriented, 4 confused, 3 inappropriate words, 2 incomprehensible sounds, 1 none. Motor (1-6): 6 obeys, 5 localizes, 4 withdraws, 3 flexion (decorticate), 2 extension (decerebrate), 1 none. Total 3-15. TBI severity: severe 3-8, moderate 9-12, mild 13-15.
Outcome & Activity Scales
- Tegner Activity Scale (0-10): 0 = disability, 10 = competitive soccer/rugby/football at national/international level.
- IKDC: International Knee Documentation Committee subjective knee form.
- KOOS: Knee injury and Osteoarthritis Outcome Score (pain, symptoms, ADL, sport, QoL).
- HAGOS: Hip and Groin Outcome Score.
- DASH / QuickDASH: Disabilities of the Arm, Shoulder and Hand.
- Lower Extremity Functional Scale (LEFS).
- Lysholm Knee Score: Historical, still encountered.
Ankle-Brachial Index in Sports
ABI is occasionally used in sports medicine to work up exertional leg pain when vascular etiology (iliac artery endofibrosis in cyclists, popliteal entrapment) is suspected. Normal resting ABI with post-exercise drop is classic for dynamic obstruction.
20 Physical Exam — Special Tests by Joint Exam
| Joint | Test | What It Assesses |
|---|---|---|
| Shoulder | Neer, Hawkins-Kennedy | Subacromial impingement |
| Shoulder | Jobe (empty can), drop arm | Supraspinatus |
| Shoulder | External rotation lag, lift-off, belly press | Infraspinatus, subscapularis |
| Shoulder | Apprehension, relocation | Anterior instability |
| Shoulder | O'Brien active compression | SLAP, AC joint |
| Shoulder | Speed, Yergason | Biceps tendinopathy |
| Elbow | Cozen, Mill | Lateral epicondylitis |
| Elbow | Moving valgus stress, milking | UCL |
| Wrist | Finkelstein | De Quervain tenosynovitis |
| Wrist | TFCC load, ulnar fovea sign | TFCC injury |
| Hip | FADIR | FAI, labral tear |
| Hip | FABER (Patrick) | SI joint, hip joint |
| Hip | Thomas, Ober | Hip flexor / IT band tightness |
| Knee | Lachman, anterior drawer, pivot shift | ACL |
| Knee | Posterior drawer, posterior sag | PCL |
| Knee | Valgus / varus stress | MCL / LCL |
| Knee | McMurray, Thessaly, joint line tenderness | Meniscus |
| Knee | Patellar apprehension, glide | Patellar instability |
| Ankle | Anterior drawer, talar tilt | Lateral ligaments |
| Ankle | Squeeze, external rotation | Syndesmosis |
| Ankle | Thompson | Achilles rupture |
| Foot | Mulder click | Morton neuroma |
| Back | Straight leg raise, slump | Lumbar radiculopathy |
| Back | Single leg hyperextension (stork) | Spondylolysis |
21 Return-to-Play Frameworks RTP
Return-to-play decisions integrate tissue healing, rehab milestones, sport demands, psychological readiness, and legal/medical considerations. A "shared decision-making" model between physician, athlete, family, athletic trainer, and coach is standard.
- Pain-free full ROM
- Strength ≥90% of contralateral side
- Completion of sport-specific functional tests (hop tests for knee, Y-balance, T-test)
- Psychological readiness (ACL-RSI scale for ACL reconstruction)
- Resolution of swelling and effusion
- Satisfactory cardiovascular and concussion clearance when applicable
Specific examples: ACL reconstruction 9-12 months with functional testing; lateral ankle sprain 1-6 weeks by grade; concussion graduated 6-stage protocol; hamstring strain when strength returns to >95% contralateral and sport-specific drills tolerated without guarding; stress fracture when pain-free, tenderness resolved, progressive loading tolerated.
22 Abbreviations Master List Reference
Anatomy
Diagnoses
Procedures / Exam
Medications / Labs
23 Sample HPI Templates Templates
These templates illustrate the rhythm and depth of a sports medicine HPI. Use them as patterns during your first weeks in clinic.
"Ms. [Name] is a 17-year-old right-hand-dominant female varsity soccer forward with no prior knee injury who presents with acute right knee pain and swelling following a noncontact injury during a game yesterday evening. She describes planting her right foot to cut laterally when she felt a pop and immediate give-way. She was unable to continue playing and required assistance off the field. Swelling developed within approximately one hour (consistent with hemarthrosis). She denies locking but reports a sense of instability with any attempt to bear weight. She has been using crutches, ice, and ibuprofen 600 mg q6h with moderate relief. No prior knee surgeries, no family history of connective tissue disease. Menstrual history unremarkable. She is scheduled for a college recruiting showcase in 6 weeks."
"Mr. [Name] is a 22-year-old male recreational basketball player who presents 2 days after an acute right ankle inversion injury sustained when he came down on another player's foot. He felt immediate lateral pain and heard a pop. He was able to hobble off the court and has been weight-bearing with a visible limp. Swelling and ecchymosis developed over the lateral ankle within hours. He denies numbness, tingling, or prior ankle injury. He has been using an elastic wrap, ice, and naproxen 440 mg BID. Ottawa ankle rules reviewed: tenderness over the distal fibula, no tenderness over the navicular or fifth metatarsal base, able to take four steps. Radiographs obtained today are negative for fracture."
"Mr. [Name] is a 16-year-old male high school junior varsity football defensive back presenting for evaluation of a suspected concussion sustained 3 days ago. During a tackling drill, he took a helmet-to-helmet blow. He denies loss of consciousness but reports brief retrograde amnesia for the play. He was removed from play by the athletic trainer, underwent sideline SCAT6 which was positive for headache, dizziness, and fogginess. Symptoms since then: persistent bifrontal headache (6/10), photophobia, difficulty concentrating in class, and irritability. No vomiting, no focal deficit, no worsening. Slept poorly last night. Prior concussion history: 1 prior concussion, sophomore year, resolved in 5 days. He is currently in Stage 1 of graduated return. Academic accommodations requested."
"Mr. [Name] is a 52-year-old right-hand-dominant male recreational tennis player with a history of hypertension who presents with 3 months of progressively worsening right shoulder pain. Pain is localized to the lateral deltoid, worse with overhead activity (serving, reaching into upper cabinets) and is now disrupting sleep — he is unable to lie on the right side. He denies frank trauma. He has tried ibuprofen 400 mg PRN and a month of home stretching with minimal relief. Prior MRI (2 years ago) showed supraspinatus tendinopathy without tear. No prior injections. Goals: return to recreational tennis and sleep comfortably."
"Ms. [Name] is a 28-year-old female marathon runner (training for a half marathon in 10 weeks) presenting with 6 weeks of bilateral anterior knee pain, worse on the right. Pain began after she increased her weekly mileage from 20 to 35 miles in preparation. Pain is peripatellar, aggravated by downhill running, stairs, and prolonged sitting ('theater sign'), and improves with rest. No swelling, no locking, no give-way. She recently transitioned to minimalist shoes. Exam notable for tight ITB, weak hip abductors, and lateral patellar tracking. She denies amenorrhea, stress fractures, or disordered eating."
"Mr. [Name] is an 18-year-old right-hand-dominant male collegiate baseball pitcher, 8 months status post right UCL reconstruction with palmaris longus autograft, presenting for return-to-throwing clearance evaluation. He has completed his PT protocol without setback, is pain-free, and has full ROM. Strength 5/5 throughout the right upper extremity symmetric to left. He has completed a supervised long-toss progression to 180 feet without pain and is ready to advance to mound work. Exam today: well-healed medial incision, no tenderness, negative moving valgus stress test, stable to valgus at 30 degrees. Plan is to advance to the phase 2 mound progression with a pitch count of 25 fastballs at 50% effort over the next 2 weeks."
24 References & Sources
Clinical Practice Guidelines & Position Statements
AAOS Clinical Practice Guideline on the Management of Rotator Cuff Injuries. 2019.
Casa DJ et al. NATA Position Statement: Exertional Heat Illnesses. J Athl Train. 2015.
Herring SA et al. AMSSM Team Physician Consensus Statements (ACL, Return to Sport).
De Souza MJ et al. Female Athlete Triad Coalition Consensus Statement. Br J Sports Med. 2014.
Preparticipation Physical Evaluation (PPE) Monograph. 5th ed. AAP/ACSM/AMSSM/AOSSM/AAFP. 2019.
Zackery Lystedt Law — Washington State Youth Sports Concussion Legislation. 2009.
ACSM Exercise Testing and Prescription Guidelines. 11th ed. 2021.
Diagram & Figure Sources
Figure 1: Major Joints. OpenStax College. CC BY 3.0.
Figure 2: Major Skeletal Muscles. OpenStax College. CC BY 3.0.
Figure 3: Knee Joint. OpenStax College. CC BY 3.0.
Figure 4: Shoulder Joint. OpenStax College. CC BY 3.0.
Figure 5: ACL Injury Illustration. Blausen Medical. CC BY 3.0.
Figure 6: Concussion Mechanics. Patrick J. Lynch & C. Carl Jaffe. CC BY 2.5.
Great sports medicine scribes think in mechanisms. When the physician says "noncontact pivot with immediate effusion," you should already be thinking ACL and drafting the exam template. When they say "helmet-to-helmet with brief fogginess," you should already have the SCAT6 documentation ready and know to ask about prior concussions.
Learn the special tests until you can spell them without thinking. Know the joint vocabulary (Lachman, McMurray, Neer, Thompson, FADIR, Ottawa rules) and the return-to-play stages cold. Understand that every note must answer three things: diagnosis, current restrictions, and RTP timeline. Anticipate the plan — draft PT orders, brace fittings, and follow-up intervals before the physician asks.
Sports medicine is fast-paced, practical, and deeply rewarding. You will watch athletes go from injury to competition over months, and your documentation is part of that journey. Welcome to the clinic.