Trauma Surgery
Every injury pattern, ATLS principle, procedure, medication, classification, and documentation framework you need to survive the trauma bay and beyond.
All diagrams on this page are sourced from published educational or institutional materials rather than AI generation. Each figure caption links to the original source, and the full diagram and guideline citations are collected in the references section at the bottom.
01 ATLS Principles & Trauma Activation
Trauma surgery is an acuity-driven specialty. Every encounter begins with a structured, time-critical assessment framework derived from Advanced Trauma Life Support (ATLS), the American College of Surgeons Committee on Trauma (ACS COT) curriculum now in its 10th edition. ATLS standardizes the approach to a critically injured patient: identify and treat life-threatening problems in the order in which they will kill the patient. The trauma scribe's first job is to understand ATLS because nearly every word said in the trauma bay maps to an ATLS step.
Trauma Team Activation
Verified trauma centers (Levels I–V) stratify incoming patients by physiologic and mechanistic criteria. A Level 1 (highest tier) activation is reserved for patients with immediate life-threatening injuries; a Level 2 activation captures serious but more stable patients; consultations or "trauma alerts" are lower acuity. Activation criteria follow the CDC Field Triage Criteria and include physiologic (SBP < 90, GCS < 14, RR < 10 or > 29), anatomic (penetrating torso/neck/groin, flail chest, two or more proximal long bone fractures, crush, pelvic fracture, open/depressed skull fracture, paralysis), and mechanistic (ejection, death in same vehicle, fall > 20 ft, auto-pedestrian) criteria.
SBP < 90 mmHg at any time; GCS ≤ 8; respiratory compromise/need for airway; transfer patients receiving blood to maintain vitals; gunshot wound to neck, chest, or abdomen; emergency physician discretion. These patients meet the surgeon at the door.
A typical Level 1 response includes a trauma surgeon (team leader), emergency physician, anesthesia/airway provider, trauma nurses (primary and secondary), respiratory therapist, radiology tech, blood bank runner, chaplain/social work, security, and the scribe/recorder. Your physical position is usually at the foot of the bed with a clear view of the whole team. Write times next to every critical event (intubation, tourniquet, blood transfusion, chest tube, TXA administration).
The two most important things to capture during an activation are times and numbers. Time of arrival, time of intubation, time of each blood product, time to CT, time to OR. Numbers include vitals on arrival, GCS, FAST result, hemoglobin, base deficit, lactate. If you remember nothing else, timestamp everything.
02 Scribe Documentation Framework
Trauma documentation differs fundamentally from clinic documentation. You are not writing a SOAP note in real time; you are writing a trauma flow sheet that captures a resuscitation, then an admission H&P, then operative notes, and finally ICU progress notes. Each format has different rules.
Pre-hospital: Mechanism of injury (MOI), time of injury, vitals en route, interventions performed by EMS (intubation, tourniquet, IV access, blood products, needle decompression), loss of consciousness, and patient-reported history if obtainable.
Arrival vitals & GCS: Temperature, HR, BP, RR, SpO2, GCS (Eye, Verbal, Motor) with individual components.
Primary survey (ABCDE): Airway patency, breath sounds, chest wall, pulses, capillary refill, GCS, pupils, gross neurologic, and full skin exposure.
Interventions & times: Every procedure, medication, blood product, and imaging study with a timestamp.
Secondary survey: Head-to-toe exam documented by region (head, face, neck, chest, abdomen, pelvis, GU, back, extremities, neuro). AMPLE history (Allergies, Medications, PMH/Pregnancy, Last meal, Events).
CC, HPI (narrative of MOI and course), AMPLE history, ROS, exam, imaging/labs with specific numbers, problem list (every injury discretely listed), assessment and plan by problem, code status, and disposition (OR, ICU, step-down, floor, observation).
In trauma, every anatomic injury is its own problem: "Grade III splenic laceration," "Right 5–9 rib fractures with small hemothorax," "Left femur midshaft fracture," "Mild TBI with small right frontal SAH." Each gets its own A/P entry. This format drives billing, follow-up, and hand-off.
Never abbreviate GCS to a single number in the note. Always write it as GCS 13 (E3 V4 M6). The individual components matter clinically and legally. The same rule applies to vitals — always record the full set, not a summary.
03 Primary & Secondary Survey (ABCDE) Core
The primary survey is the first 60 seconds of the resuscitation. Its only purpose is to identify and treat immediately life-threatening problems. It follows the ABCDE mnemonic: Airway with cervical spine protection, Breathing and ventilation, Circulation with hemorrhage control, Disability (neurologic), Exposure and environmental control.
A — Airway with C-Spine Protection
Can the patient speak clearly? A patient phonating normally has a patent airway and adequate cerebral perfusion. Look for stridor, gurgling, pooled blood or secretions, facial burns or soot, expanding neck hematoma, and altered mental status. Patients with GCS ≤ 8 generally require a definitive airway. Always maintain manual in-line stabilization of the cervical spine during airway maneuvers until the C-spine is cleared clinically or radiographically.
B — Breathing and Ventilation
Inspect, palpate, percuss, and auscultate the chest. The six immediately life-threatening thoracic injuries (the "lethal six") identified in the primary survey are: airway obstruction, tension pneumothorax, open pneumothorax, massive hemothorax, flail chest with pulmonary contusion, and cardiac tamponade. Pulse oximetry, capnography, and a STAT portable chest X-ray follow immediately.
C — Circulation with Hemorrhage Control
Assess perfusion by mental status, skin color/temperature, and pulses. External bleeding is controlled with direct pressure, packing, tourniquets (extremity), and junctional devices (groin/axilla/neck). Two large-bore IVs (16G or 14G) go in bilateral antecubitals; if unable, place an IO or central access (IJ/femoral cordis). Draw a trauma panel (type & cross, CBC, CMP, coags, lactate, ABG, ethanol, tox, urine HCG, troponin, fibrinogen, TEG or ROTEM). Initiate balanced resuscitation with blood products if there is any concern for hemorrhagic shock.
D — Disability (Neurologic)
Rapid neurologic assessment: GCS (E/V/M), pupils (size, symmetry, reactivity), gross motor exam of all extremities, and any focal deficit. Check for lateralizing signs (unilateral weakness, fixed/dilated pupil). Document the Glasgow Coma Scale by component.
E — Exposure and Environment
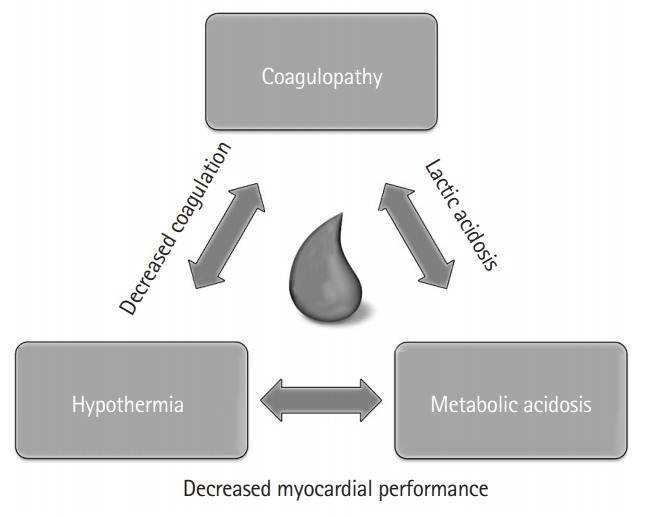
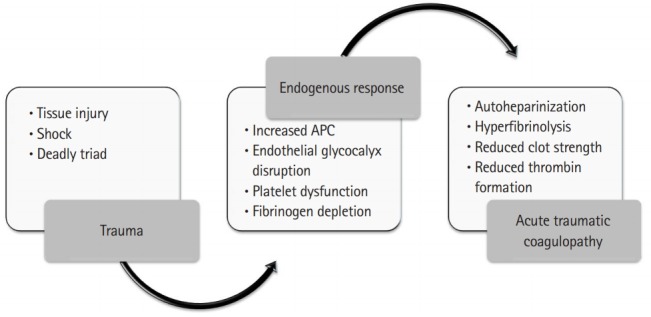
Completely undress the patient, log-roll to inspect the back, and then cover with warm blankets and a Bair Hugger to prevent hypothermia. The lethal triad of trauma — hypothermia, acidosis, and coagulopathy — is worsened by a cold patient. Core temperature should be monitored (rectal or esophageal).
Secondary Survey
After the primary survey and initial resuscitation stabilize the patient, the secondary survey is a head-to-toe exam to catalog every injury. This is where you identify injuries that won't kill the patient in the next 5 minutes but will complicate care if missed (facial fractures, extremity fractures, tendon injuries, small hemothorax, solid organ injuries). The AMPLE history is taken here. A tertiary survey is typically repeated within 24 hours to catch missed injuries, which occur in 2–15% of multi-trauma patients.
If at any point the patient decompensates, you return to the beginning of the primary survey — "A, B, C." Document each re-assessment separately with a new timestamp. The team leader will say out loud, "We are re-assessing the primary survey," and you should chart that verbatim.
04 Airway Management & RSI in Trauma Airway
Airway compromise kills trauma patients faster than anything else. The decision to intubate in trauma is based on inability to protect the airway (GCS ≤ 8, massive facial trauma, expanding neck hematoma, inhalation injury), inability to oxygenate/ventilate, expected clinical course (combative patient requiring imaging, transport to OR), or hemodynamic collapse requiring sedation/paralysis for resuscitation.
Rapid Sequence Intubation (RSI)
RSI is the simultaneous administration of a sedative induction agent and a neuromuscular blocker to achieve optimal intubating conditions with minimal risk of aspiration. Classic sequence: preoxygenation → pretreatment (optional) → paralysis with induction → positioning → placement with proof → post-intubation management.
| Agent | Class | Dose | Notes |
|---|---|---|---|
| Etomidate | Induction | 0.3 mg/kg IV | Hemodynamically neutral; adrenal suppression with repeat dosing |
| Ketamine | Induction | 1–2 mg/kg IV | Preferred in hemorrhagic shock; maintains BP |
| Propofol | Induction | 1.5–2.5 mg/kg IV | Avoid in hypotension; good for head-injured stable patient |
| Succinylcholine | Depolarizing NMB | 1.5 mg/kg IV | Fast on/off; avoid in hyperkalemia, burns > 24h, crush, denervation |
| Rocuronium | Non-depolarizing NMB | 1.2 mg/kg IV | Longer duration; reversible with sugammadex |
Surgical Airway (Cricothyroidotomy)
When intubation fails and bag-mask ventilation is inadequate ("cannot intubate, cannot oxygenate"), an emergent surgical cricothyroidotomy is performed: a vertical skin incision over the cricothyroid membrane, a horizontal stab through the membrane, tracheal hook to elevate, and a 6.0 cuffed tracheostomy or ETT inserted. Needle cricothyroidotomy with jet ventilation is a temporizing measure in children < 12 years, in whom surgical crich is relatively contraindicated.
Expanding neck hematoma, penetrating neck injury with air bubbling, facial burns with singed nasal hairs or soot in oropharynx, hoarseness after blunt neck trauma (tracheobronchial or laryngeal injury), stridor, and subcutaneous emphysema of the neck all demand early definitive airway before the airway distorts beyond recognition.
05 Hemorrhagic Shock & Resuscitation Shock
Hemorrhage is the leading cause of preventable death after trauma. The ATLS classification of hemorrhagic shock is based on estimated blood loss and physiologic parameters.
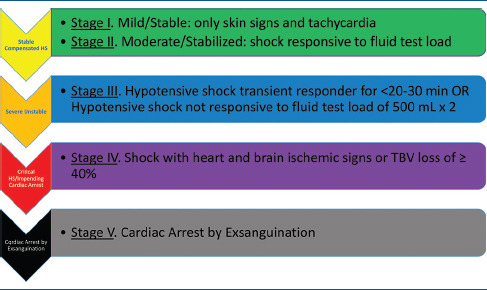
| Class | Blood Loss | HR | BP | RR | Mental Status |
|---|---|---|---|---|---|
| I | < 15% (< 750 mL) | < 100 | Normal | 14–20 | Slightly anxious |
| II | 15–30% (750–1500 mL) | 100–120 | Normal (narrow pulse pressure) | 20–30 | Mildly anxious |
| III | 30–40% (1500–2000 mL) | 120–140 | Decreased | 30–40 | Confused |
| IV | > 40% (> 2000 mL) | > 140 | Markedly decreased | > 35 | Lethargic, obtunded |
Balanced Resuscitation & MTP
Modern trauma resuscitation is hemostatic and blood-product based. Crystalloid is minimized (< 1 L) to avoid dilutional coagulopathy and worsening acidosis. The Massive Transfusion Protocol (MTP) delivers packed red blood cells, fresh frozen plasma, and platelets in a balanced 1:1:1 ratio, supported by the landmark PROPPR trial and observational PROMMTT study. Whole blood, when available, is increasingly preferred.
The ABC score (Assessment of Blood Consumption) predicts massive transfusion: 1 point each for penetrating mechanism, SBP ≤ 90, HR ≥ 120, and positive FAST. A score ≥ 2 is highly predictive. Alternative: shock index (HR/SBP) > 1.0 suggests significant blood loss.
A typical MTP "pack" is 6 units PRBC, 6 units FFP, 1 apheresis platelet, repeated as needed. Cryoprecipitate is added when fibrinogen < 150 mg/dL (or empirically per some protocols).
Permissive Hypotension
In penetrating torso trauma without TBI, targeting an SBP around 80–90 mmHg (MAP ~65) until surgical hemorrhage control reduces rebleeding from clot disruption. This is contraindicated in patients with TBI, where SBP must be kept ≥ 110 to preserve cerebral perfusion pressure.
Tranexamic Acid (TXA)
Per the CRASH-2 trial, TXA (1 g IV over 10 min, then 1 g over 8 h) reduces all-cause mortality when given within 3 hours of injury in bleeding trauma patients. CRASH-3 extended TXA benefit to mild-to-moderate TBI within 3 hours.
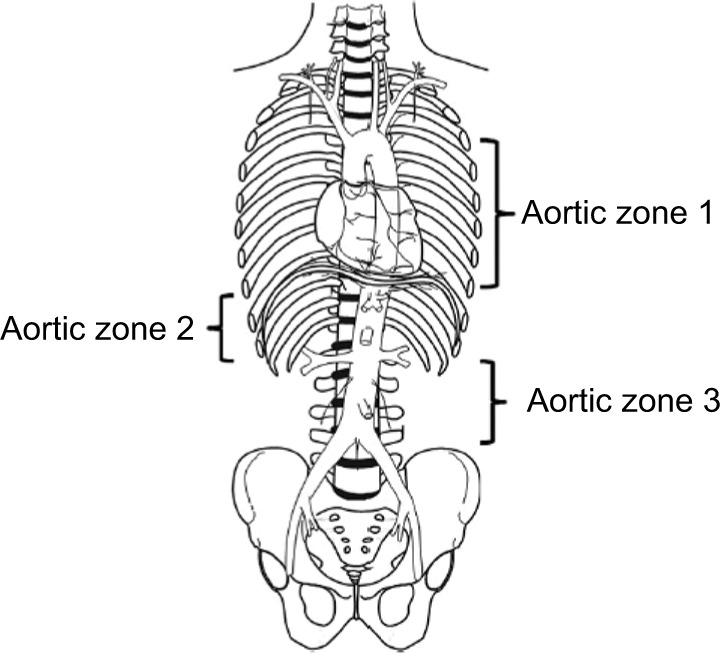
REBOA
Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) is a temporizing measure for non-compressible torso hemorrhage. A balloon catheter is placed via the common femoral artery into either Zone 1 (supraceliac, above T12) for abdominal/pelvic bleeding or Zone 3 (infrarenal, below renals) for pelvic/junctional bleeding. Zone 2 (paravisceral) is generally avoided. REBOA buys time until definitive surgical control.
06 Damage Control Surgery & Resuscitation Core
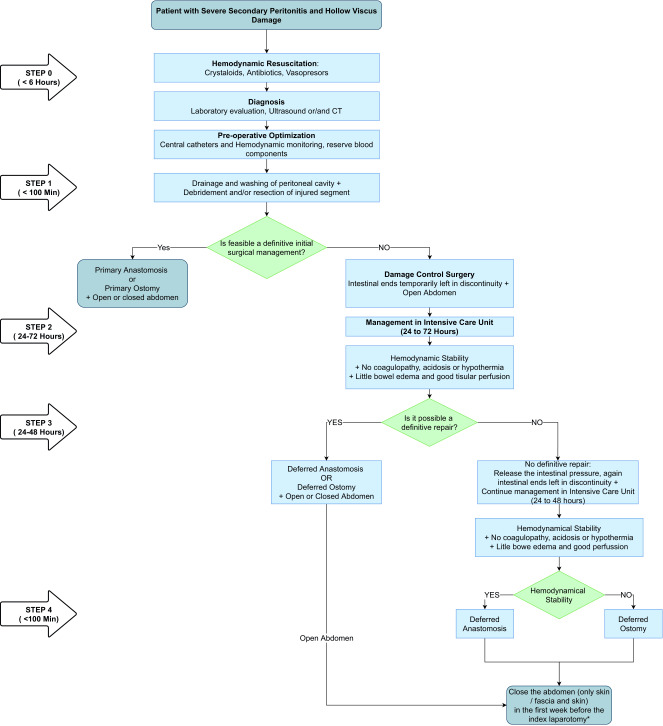
Damage control surgery (DCS) is an abbreviated operative approach for the physiologically compromised trauma patient. Instead of completing a definitive repair, the surgeon controls hemorrhage and contamination, leaves the abdomen open, and returns the patient to the ICU to correct the lethal triad. After 24–48 hours of warming, correction of acidosis, and correction of coagulopathy, the patient returns to the OR for definitive repair.
Stage 1 — Initial operation: Control hemorrhage (packing, clamping, shunting), control contamination (staple off bowel injuries, no anastomosis), temporary abdominal closure (ABTHERA vac or Bogota bag).
Stage 2 — ICU resuscitation: Rewarming, correction of acidosis (base deficit, lactate normalization), correction of coagulopathy (product-driven or goal-directed by TEG/ROTEM).
Stage 3 — Definitive operation: Return to OR at 24–48 h for pack removal, definitive repair, bowel anastomosis or ostomy, and abdominal closure (primary, mesh, or planned ventral hernia).
Damage control resuscitation (DCR) is the parallel ICU/ED strategy: early balanced blood product transfusion, minimal crystalloid, permissive hypotension (where appropriate), TXA, and aggressive warming. DCR and DCS are inseparable concepts in modern trauma.
Persistent hypothermia (< 35°C), acidosis (pH < 7.2 or base deficit > 8), coagulopathy (INR > 1.5, aPTT > 60), ongoing non-surgical bleeding, multiple injuries requiring prolonged operative time, and physiologic exhaustion.
07 Traumatic Brain Injury (TBI) Neuro
TBI is the leading cause of trauma mortality in young adults. Severity is graded by initial GCS: mild TBI (13–15), moderate TBI (9–12), severe TBI (3–8). The Brain Trauma Foundation severe TBI guidelines (4th edition) are the reference standard for ICU management.
Injury Patterns
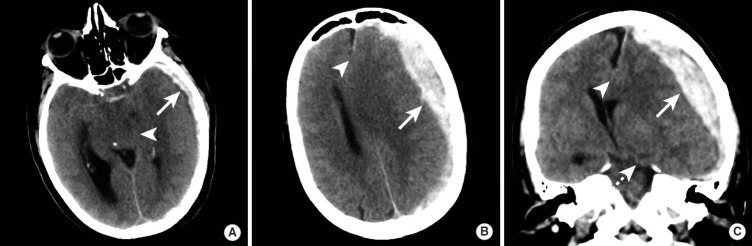
Arterial bleed (classically middle meningeal artery) between skull and dura. Lens-shaped (biconvex) on CT, does not cross suture lines. Classic "lucid interval" then rapid deterioration. Surgical emergency if > 30 cm³ or causing mass effect.
Venous bleed (torn bridging veins) between dura and arachnoid. Crescent-shaped on CT, crosses suture lines but not falx/tentorium. Acute (hyperdense), subacute (isodense), chronic (hypodense). Common in elderly, anticoagulated patients, and alcoholics.
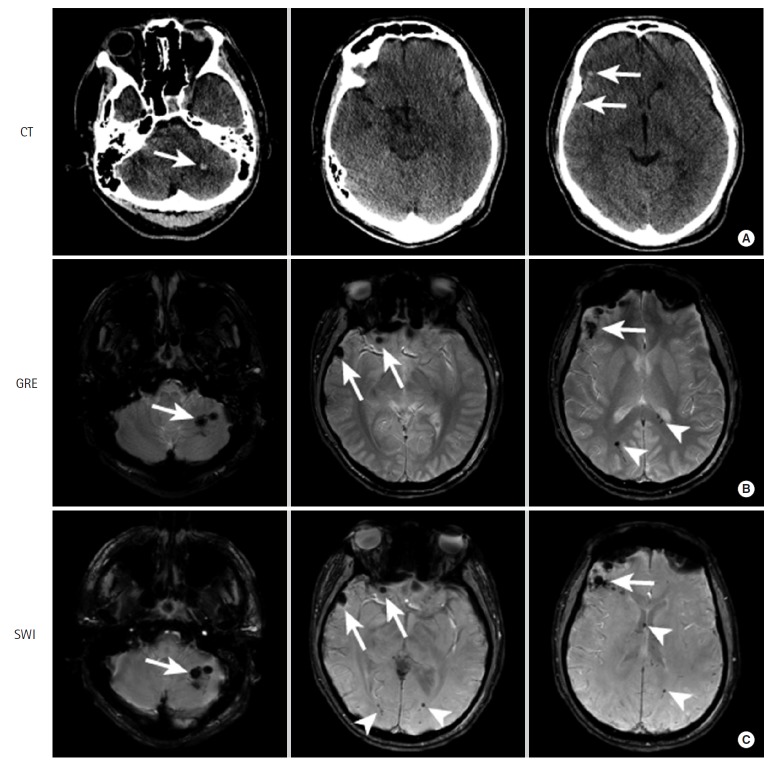
Traumatic SAH is typically found in sulci and adjacent to contusions. IPH represents brain parenchymal bleeding. DAI is shear injury at gray-white junctions from rotational forces, often with minimal CT findings but devastating clinical course (coma out of proportion to imaging).
Basilar skull fracture signs: raccoon eyes (periorbital ecchymosis), Battle sign (retroauricular bruising), hemotympanum, CSF otorrhea/rhinorrhea. Depressed skull fracture: inner table depressed > skull thickness usually requires elevation. Open depressed fractures require washout and antibiotics.
Management of Severe TBI
Goals: cerebral perfusion pressure (CPP = MAP − ICP) 60–70 mmHg, ICP < 22, SBP ≥ 110, SpO2 ≥ 90, normocapnia (PaCO2 35–40), normothermia, euglycemia, Na 140–150. Head of bed 30°, loose C-collar, sedation/analgesia, seizure prophylaxis with levetiracetam for 7 days, and reversal of any anticoagulation. Tiered ICP management: sedation → hypertonic saline or mannitol → CSF drainage via EVD → paralysis → decompressive craniectomy or barbiturate coma.
Imaging severity is often described using the Marshall CT classification (I–VI, based on basal cisterns, midline shift, and lesion type) and the Rotterdam CT score (0–6, incorporating basal cisterns, midline shift, epidural mass, and IVH/SAH).
08 Maxillofacial & Neck Trauma Head/Neck
Le Fort Fractures
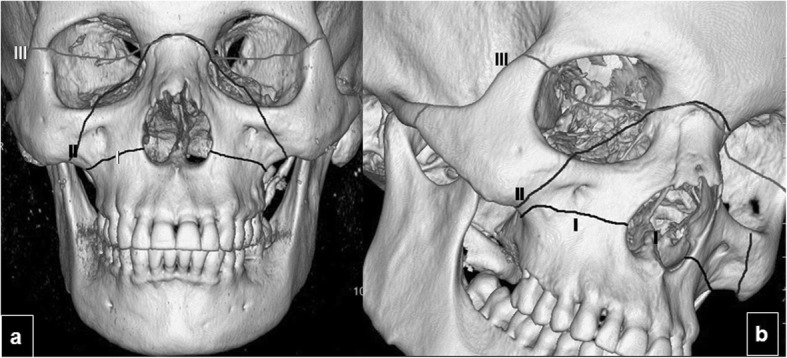
Le Fort I: Transverse fracture of the maxilla above the teeth (palate-separating, "floating palate").
Le Fort II: Pyramidal fracture through nasal bridge, medial orbit, inferior orbital rim, and lateral maxilla ("floating maxilla").
Le Fort III: Craniofacial disjunction; fracture separates the entire midface from the skull base ("floating face"). High association with CSF leak and TBI.
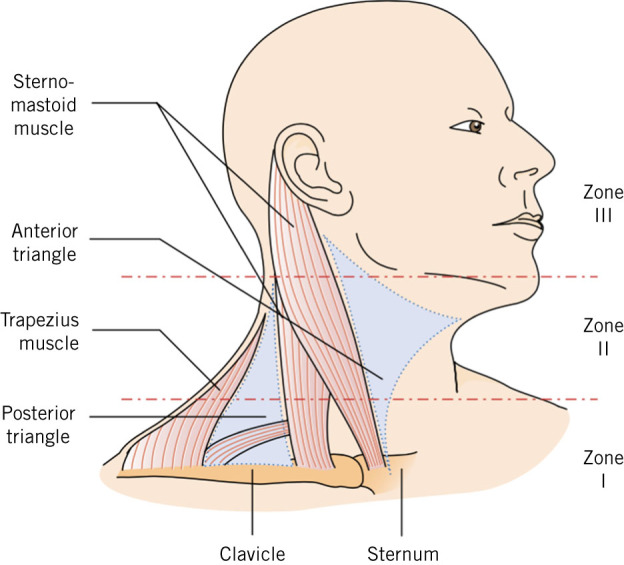
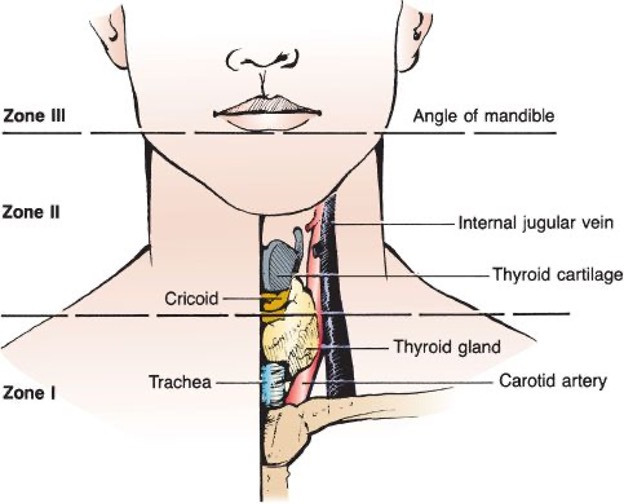
Neck Trauma Zones
Penetrating neck injuries are stratified by anatomic zone for management:
| Zone | Boundaries | Structures at Risk |
|---|---|---|
| Zone 1 | Clavicles to cricoid | Great vessels, trachea, esophagus, lung apex, thoracic duct |
| Zone 2 | Cricoid to angle of mandible | Carotid, IJ, larynx, pharynx, esophagus |
| Zone 3 | Angle of mandible to skull base | Distal carotid/vertebral, parotid, cranial nerves |
Modern management for all stable penetrating neck injuries is no-zone, CTA-first (EAST practice management guidelines): CT angiography of the neck, with selective operative exploration for hard signs (expanding hematoma, air bubbling, massive bleeding, pulse deficit, bruit/thrill). Unstable patients with hard signs go directly to the OR. Blunt cerebrovascular injury (BCVI) is screened with CTA per the Denver or modified Memphis criteria (mechanism + C-spine fracture, basilar skull fracture, Horner syndrome, etc.).
09 Cervical & Spinal Cord Injury Spine
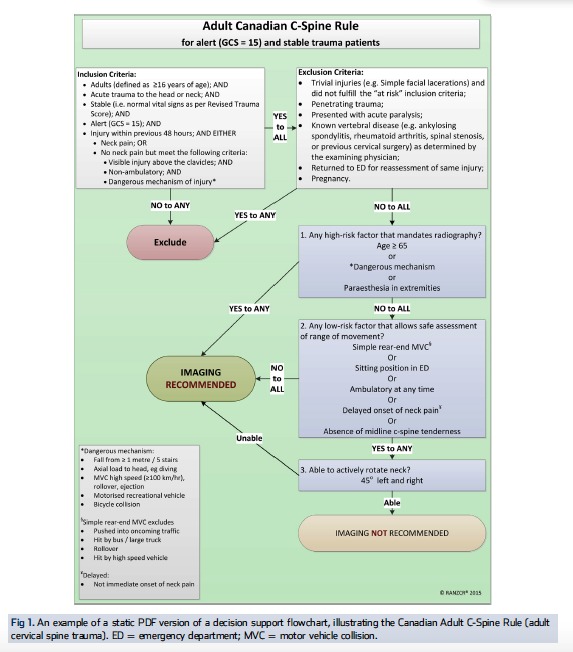
Cervical spine clearance uses validated decision rules. The NEXUS criteria allow clinical clearance if all five are met: no midline tenderness, no focal neurologic deficit, normal alertness, no intoxication, no distracting injury. The Canadian C-spine rule offers similar clearance with additional high-/low-risk factor criteria. When clinical clearance fails, CT C-spine is the first-line imaging.
Spinal Cord Injury Syndromes
Complete cord injury: No sensory or motor function below the level. ASIA A.
Central cord syndrome: Hyperextension in a stenotic canal, upper > lower extremity weakness.
Anterior cord syndrome: Loss of motor, pain, and temperature; preserved proprioception and vibration.
Brown-Séquard syndrome: Hemisection of cord — ipsilateral motor/proprioception loss, contralateral pain/temperature loss.
Cauda equina syndrome: Saddle anesthesia, bowel/bladder dysfunction, lower extremity weakness. Surgical emergency.
Neurogenic shock: Hemodynamic (hypotension with bradycardia and warm skin) from loss of sympathetic tone above T6. Treated with vasopressors (norepinephrine or phenylephrine). Spinal shock: Transient loss of all reflexes and motor function below the level of injury; resolves over days to weeks. Different concept from neurogenic shock.
10 Thoracic Trauma Chest
Chest injuries account for approximately 25% of trauma deaths. Most are managed non-operatively; only ~10–15% require thoracotomy. The EAST rib fracture guidelines are the reference standard for blunt chest trauma.
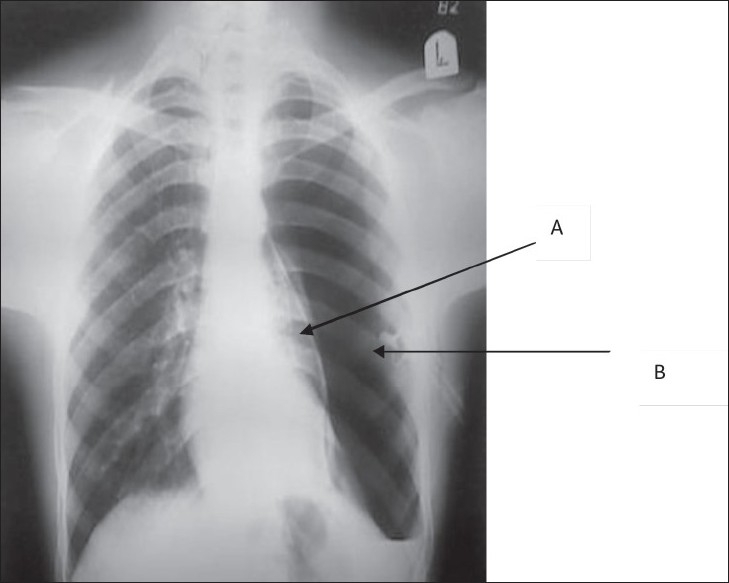
Clinical diagnosis: hypotension, tracheal deviation away, absent breath sounds, hyperresonance, distended neck veins, subcutaneous emphysema. Treatment: immediate needle decompression (large-bore angiocath at 4th–5th ICS anterior axillary line per updated ATLS, or 2nd ICS midclavicular line in older protocols), followed by chest tube (32–36 Fr) at the 5th ICS, anterior to mid-axillary line.
Initial output > 1500 mL, or > 200 mL/hr for 4 hours, or hemodynamic instability = indication for operative thoracotomy (or VATS). Chest tube drains allow monitoring.
Beck's triad (hypotension, distended neck veins, muffled heart sounds) in penetrating chest trauma. Pericardial view on FAST (cardiac FAST) is the diagnostic test of choice. Treatment is pericardial window in the OR; ED pericardiocentesis is temporizing.
Traumatic aortic injury most commonly occurs at the aortic isthmus distal to the left subclavian (ligamentum arteriosum tethering point) after high-energy deceleration. Widened mediastinum on CXR should prompt CTA chest. Treatment is TEVAR in most cases per SVS clinical practice guidelines.

Rib Fractures & Flail Chest
Rib fractures cause pain-mediated hypoventilation, atelectasis, and pneumonia, especially in elderly patients. Flail chest = 3 or more contiguous ribs fractured in 2 or more places, producing a paradoxical segment. The main problem is the underlying pulmonary contusion, not the paradox itself. Management: aggressive analgesia (epidural, PCA, intercostal/paravertebral blocks, serratus anterior plane blocks), pulmonary toilet, early mobilization, and selective surgical stabilization of rib fractures (SSRF) for flail chest or severely displaced fractures.
Pulmonary contusion is bruising of lung parenchyma that produces hypoxemia and ARDS-like physiology over 24–72 hours. Blunt cardiac injury is screened with EKG and troponin; normal EKG and troponin effectively rule out clinically significant BCI per EAST BCI guidelines. Tracheobronchial injury presents with persistent large air leak after chest tube placement and requires bronchoscopy. Esophageal injury is suspected with pneumomediastinum without obvious cause, mediastinitis, or after penetrating transmediastinal injury; diagnosed with CT, esophagram, or endoscopy.
ED Resuscitative Thoracotomy
Per EAST guidelines on ED thoracotomy, the procedure is strongly recommended for pulseless patients with penetrating thoracic injury and signs of life on arrival; conditionally recommended for penetrating extra-thoracic injury with signs of life, and for blunt trauma with signs of life. The goals are: release pericardial tamponade, control pulmonary hemorrhage, cross-clamp the descending thoracic aorta, and perform open cardiac massage.
11 Abdominal Trauma Abdomen
Abdominal trauma is divided into blunt (MVC, fall, assault) and penetrating (GSW, stab). The approach differs radically.
FAST & E-FAST
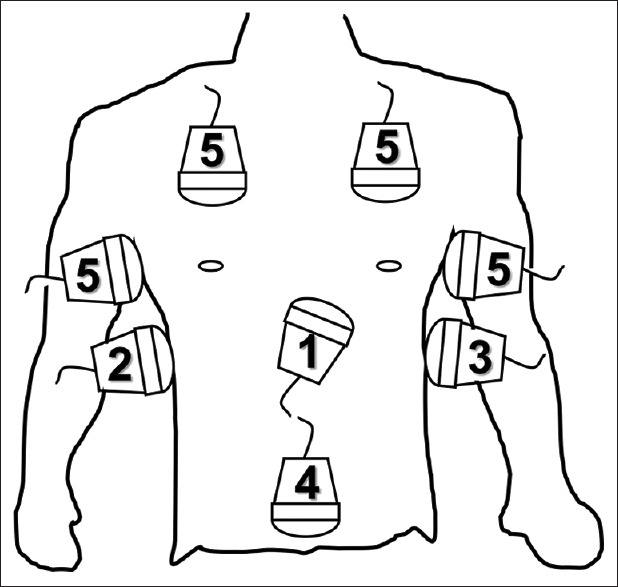
The Focused Assessment with Sonography for Trauma (FAST) examines four views for free intraperitoneal fluid: right upper quadrant (Morison's pouch), left upper quadrant (splenorenal), pelvis (pouch of Douglas), and pericardium (subxiphoid). The Extended FAST (E-FAST) adds bilateral anterior lung views to assess for pneumothorax. FAST is highly specific but not sensitive for small-volume injury. A positive FAST in an unstable blunt trauma patient is an indication for immediate laparotomy.
Blunt Abdominal Trauma Decision Pathway
Unstable + positive FAST: OR for laparotomy.
Unstable + negative FAST: Look elsewhere (chest, pelvis, long bones, external); DPA may be used if diagnosis remains unclear.
Stable: CT with IV contrast is the gold standard.
Solid Organ Injury
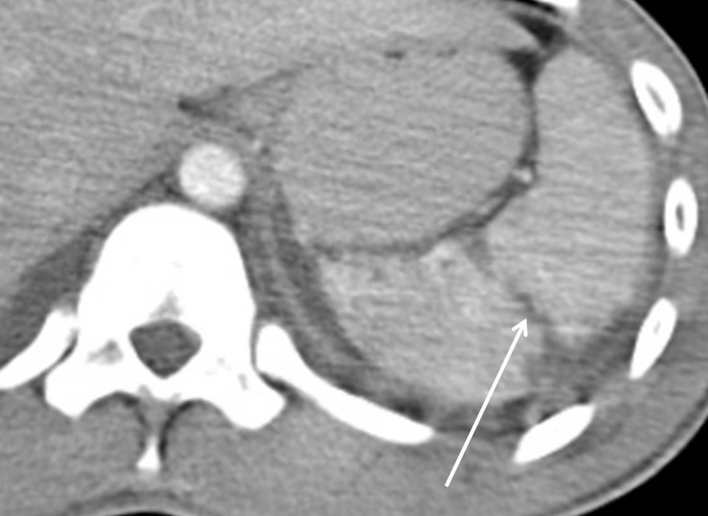
Spleen is the most commonly injured solid organ in blunt trauma. EAST solid organ injury guidelines support non-operative management for hemodynamically stable patients, including higher-grade injuries, with adjunctive splenic artery embolization (SAE) for active extravasation, pseudoaneurysm, or AV fistula.
Liver is the most commonly injured organ in penetrating abdominal trauma and second in blunt. Non-operative management is preferred in stable patients. Operative options include hepatic packing, Pringle maneuver (occlusion of the portal triad with atraumatic clamp to reduce inflow), finger fracture, selective hepatic artery ligation, partial hepatectomy, and atrio-caval shunt for juxta-hepatic IVC injury.
Kidney injuries are graded I–V (AAST); non-operative management is preferred in most cases, even for grade IV with devascularization. Pancreas injuries are rare but morbid; management depends on ductal integrity (main pancreatic duct). Hollow viscus injuries (bowel, mesentery) often present with delayed peritonitis; CT findings include free air, free fluid without solid organ injury, mesenteric stranding, or bowel wall thickening.
Abdominal Compartment Syndrome (ACS)
Sustained intra-abdominal pressure > 20 mmHg with new organ dysfunction. Bladder pressure measurement is the standard. Treatment is decompressive laparotomy with temporary abdominal closure (open abdomen with ABTHERA vac).
12 Pelvic & Genitourinary Trauma Pelvis/GU
Pelvic fractures from high-energy blunt trauma are associated with significant mortality (5–20%), driven largely by retroperitoneal hemorrhage from the posterior venous plexus and small arterial branches. Two classification systems are used:
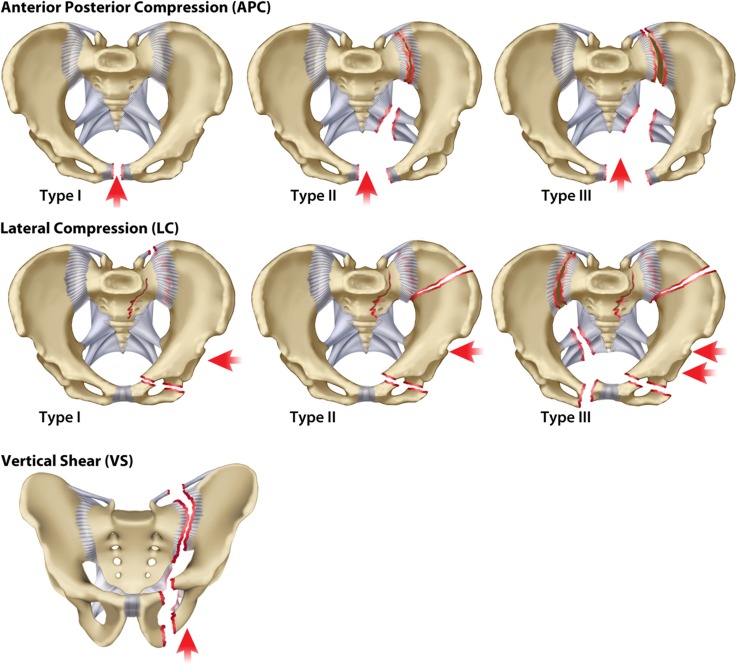
Lateral Compression (LC): I–III by severity; inward rotation of hemipelvis.
Anteroposterior Compression (APC, "open book"): I–III; widening of pubic symphysis, worst with posterior SI joint disruption.
Vertical Shear (VS): Superior displacement of hemipelvis; high-energy fall.
Combined Mechanism (CM): Features of multiple types.
Type A: Stable; posterior arch intact. Type B: Rotationally unstable, vertically stable (open book, LC). Type C: Rotationally and vertically unstable (complete disruption of posterior arch).
Hemorrhage Control
A pelvic binder applied at the level of the greater trochanters is the first step for any unstable pelvic fracture, closing the pelvic volume. Persistent instability requires an escalation pathway: external fixation, preperitoneal pelvic packing, REBOA (Zone 3), and/or angioembolization. Multidisciplinary protocols improve outcomes (WTA pelvic fracture algorithm).
Genitourinary Injuries
Urethral injury is suggested by blood at the meatus, high-riding prostate, or perineal ecchymosis after pelvic fracture — obtain a retrograde urethrogram before Foley placement. Bladder injury is intraperitoneal (requires repair) or extraperitoneal (managed with catheter drainage). Renal injury is graded I–V with non-operative management preferred. Rectal injury in pelvic trauma is evaluated with rigid or flexible proctoscopy; diverting colostomy may be required for destructive or penetrating rectal injuries.
13 Vascular & Extremity Trauma Vascular/MSK
Hard vs. Soft Signs of Vascular Injury
Pulsatile bleeding, expanding hematoma, palpable thrill, audible bruit, signs of distal ischemia (pulseless, pale, paresthetic, paralyzed, poikilothermic, painful — the 6 P's).
History of significant bleeding, non-expanding hematoma, proximity of wound to major vessel, diminished but present pulses, peripheral nerve deficit. Measure injured extremity index (IEI) (analog of ABI) — < 0.9 warrants CTA.
Open Fractures & Compartment Syndrome
Open fractures are graded by the Gustilo-Anderson classification:
| Grade | Wound | Notes |
|---|---|---|
| I | < 1 cm, clean | Low energy, minimal contamination |
| II | 1–10 cm, moderate soft tissue damage | Moderate energy |
| IIIA | > 10 cm, adequate soft tissue coverage | High energy |
| IIIB | > 10 cm, inadequate soft tissue coverage, periosteal stripping | Requires flap coverage |
| IIIC | Any open fracture with arterial injury requiring repair | High amputation risk |
Early IV antibiotics (cefazolin for I–II; add aminoglycoside for III; add penicillin for farm/soil contamination) and tetanus prophylaxis are essential. Formal irrigation and debridement is performed in the OR.
Compartment syndrome presents with pain out of proportion, pain with passive stretch, paresthesia, and — late — pulselessness. Compartment pressures > 30 mmHg or a ΔP (diastolic BP minus compartment pressure) < 30 require emergent 4-compartment fasciotomy.
The Mangled Extremity Severity Score (MESS) incorporates skeletal/soft tissue injury, limb ischemia, shock, and age; a score ≥ 7 historically suggested amputation, though modern decision-making is more individualized.
Vascular trauma is managed with temporary shunts (Javid, Argyle, Pruitt-Inahara) during damage control, followed by definitive reconstruction (primary end-to-end repair, vein interposition graft from contralateral saphenous, or prosthetic graft in clean fields).
14 Burns & Environmental Trauma Burn/Env
TBSA and Depth
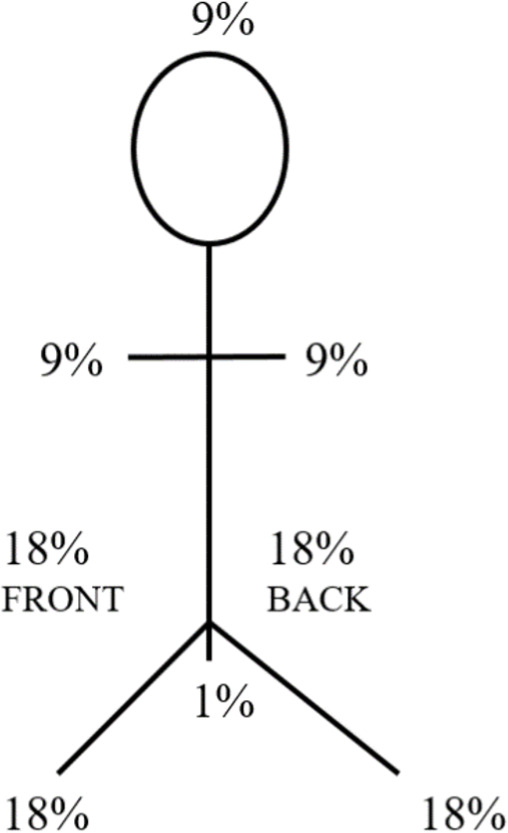
Total body surface area (TBSA) is estimated using the rule of nines (adult) or the more accurate Lund-Browder chart (pediatric). Only partial-thickness (second-degree) and full-thickness (third-degree) burns count toward TBSA.
Superficial (1st degree): Epidermis only; erythema, pain (sunburn). Not counted in TBSA.
Superficial partial thickness (2a): Epidermis and superficial dermis; blisters, moist, painful, blanches.
Deep partial thickness (2b): Epidermis and deep dermis; dry, less sensate, may not blanch.
Full thickness (3rd degree): Entire dermis; leathery, white/charred, painless.
Parkland Formula
Fluid resuscitation for burns ≥ 20% TBSA: 4 mL × weight (kg) × %TBSA of lactated Ringer's over 24 hours, with half given in the first 8 hours from the time of burn. Titrate to urine output 0.5 mL/kg/hr adult, 1 mL/kg/hr child. American Burn Association criteria trigger referral to a burn center for > 10% TBSA partial thickness, any full thickness, burns to face/hands/feet/genitalia/joints, inhalation injury, chemical/electrical burns, and burns with concomitant trauma.
Escharotomy is a full-thickness skin incision through circumferential burn eschar on the extremities (to restore perfusion) or the chest (to restore ventilation). Fasciotomy is required for electrical burns with muscle compartment involvement.
Inhalation Injury & Other Environmental Trauma
Inhalation injury is suspected with closed-space fire, singed nasal hairs, soot in oropharynx, carbonaceous sputum, hoarseness, or elevated carboxyhemoglobin. Early intubation is often mandatory. Cyanide toxicity is treated with hydroxocobalamin.
Electrical injury: risk of cardiac arrhythmia, rhabdomyolysis, compartment syndrome, and deep tissue injury out of proportion to skin findings. Lightning injury: often cardiac arrest (asystole), Lichtenberg figures. Drowning: focus on oxygenation, rewarming, consideration of ECMO. Hypothermia: graded mild (32–35°C), moderate (28–32°C), severe (< 28°C); severe cases may require ECMO rewarming. Blast injury: primary (barotrauma: tympanic membrane, lung, bowel), secondary (fragments), tertiary (displacement), quaternary (burns, crush).
15 Special Populations Special
Pediatric Trauma
Children have unique physiology: larger head relative to body (higher TBI risk), more compliant chest wall (pulmonary contusion without rib fracture), and maintained BP until late (tachycardia is the earliest sign of shock). Use weight-based resuscitation (20 mL/kg crystalloid ×1–2, then 10 mL/kg PRBC). The Broselow tape provides size-based dosing. Non-accidental trauma must be considered in any pediatric injury inconsistent with history.
Geriatric Trauma
Older adults have limited physiologic reserve. "Normal" vitals can mask shock. Age ≥ 65 is an independent predictor of mortality. Liberal CT imaging, early mobility, delirium prevention, and geriatric co-management improve outcomes. The EAST geriatric trauma guidelines recommend triage of elderly patients with ≥ 1 physiologic or anatomic criterion to a trauma center.
Anticoagulation Reversal in Trauma
| Agent | Reversal |
|---|---|
| Warfarin | 4-factor PCC (Kcentra) 25–50 U/kg + IV vitamin K 10 mg |
| Dabigatran | Idarucizumab (Praxbind) 5 g IV |
| Apixaban / Rivaroxaban | Andexanet alfa (Andexxa) or 4-factor PCC 50 U/kg |
| Heparin (UFH) | Protamine sulfate 1 mg per 100 units heparin |
| LMWH | Protamine (partial reversal) |
| Antiplatelets | Platelet transfusion (limited evidence); DDAVP adjunct |
16 Trauma Procedures — A to Z
Procedures that a trauma scribe will see and document. Each procedure note follows a standard template: indication, consent (emergent or obtained), time-out, prep/drape, anesthesia, position, technique, findings, estimated blood loss, complications, disposition.
| Procedure | Indication | Key Points |
|---|---|---|
| Rapid sequence intubation | Airway protection/ventilation | Induction + paralytic + ETT with confirmation |
| Surgical cricothyroidotomy | Failed airway | Vertical skin, horizontal membrane, hook, 6.0 tube |
| Needle decompression | Tension PTX | 14G at 4th–5th ICS AAL (or 2nd ICS MCL) |
| Tube thoracostomy | Pneumothorax, hemothorax | 32–36 Fr, 5th ICS anterior axillary |
| Resuscitative thoracotomy | Penetrating arrest with signs of life | Left anterolateral, pericardiotomy, aortic cross-clamp |
| FAST/E-FAST | Screening for free fluid, pneumothorax | 4 views + bilateral lung sliding |
| Diagnostic peritoneal aspirate/lavage | Unstable blunt with equivocal FAST | Gross blood = positive |
| Exploratory laparotomy | Peritonitis, penetrating, positive FAST + unstable | Midline, 4-quadrant packing, systematic exam |
| Splenectomy / splenorrhaphy | Unstable splenic injury, failed NOM | Vaccines post-op: pneumococcal, meningococcal, Hib |
| Hepatic packing / Pringle maneuver | Liver hemorrhage | Pringle ≤ 60 min; damage control |
| Nephrectomy | Renal pedicle avulsion, destructive | Confirm contralateral kidney function |
| Distal pancreatectomy | Distal pancreatic duct injury | ± splenectomy |
| Bowel resection | Destructive bowel injury | Damage control: staple off, no anastomosis |
| Preperitoneal pelvic packing | Unstable pelvic fracture | With external fixator and/or angioembolization |
| REBOA | Non-compressible torso hemorrhage | CFA access; Zone 1 or Zone 3 |
| 4-compartment fasciotomy | Compartment syndrome lower leg | 2-incision (medial + lateral) technique |
| Escharotomy | Circumferential full-thickness burn | Mid-axial lines to restore perfusion |
| Vascular shunt | Damage control vascular injury | Javid/Argyle/Pruitt-Inahara |
| End-to-end vascular repair / interposition | Definitive vascular repair | Contralateral saphenous preferred |
| External pelvic fixation | Unstable pelvic fracture | Iliac crest or supraacetabular pins |
| ICP monitor / EVD placement | Severe TBI with ICP monitoring indication | Bolt or ventriculostomy |
| Decompressive craniectomy | Refractory intracranial hypertension | Hemicraniectomy; performed by NSGY |
| MTP activation | Ongoing hemorrhage meeting criteria | 1:1:1 product delivery |
| ECMO cannulation | Refractory ARDS, drowning, hypothermia | VV or VA configuration |
17 Trauma Imaging & Diagnostics
Plain radiographs: The "trauma series" traditionally includes chest, pelvis, and lateral C-spine X-rays during the primary survey. In modern Level 1 centers, portable chest and pelvis are obtained while CT is prepared.

CT "pan-scan": CT head without contrast, C-spine without contrast, and CT chest/abdomen/pelvis with IV contrast is the standard imaging work-up for the significantly injured blunt trauma patient. Oral contrast is generally not used. CT angiography is added for suspected vascular injury, BCVI, or TAI.
Ultrasound: FAST/E-FAST is the screening modality at the bedside. Critical care ultrasound is increasingly used for volume status and cardiac function.
Angiography: Therapeutic for splenic artery embolization, pelvic embolization, and extremity/visceral bleeding.
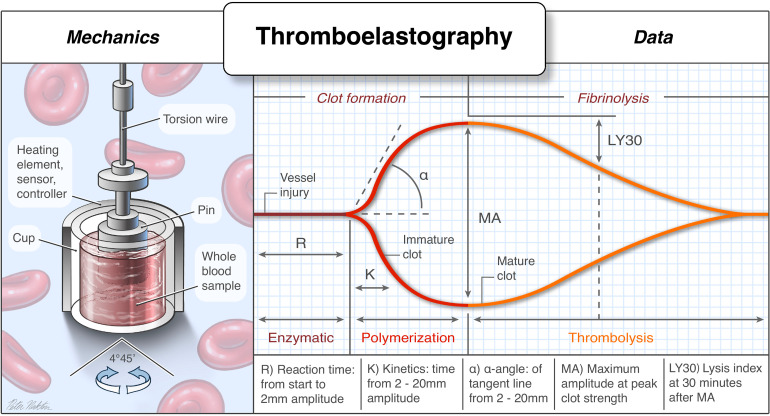
Key lab values to track: hemoglobin/hematocrit trend, lactate (resuscitation marker, goal < 2), base deficit (> 6 abnormal, > 10 severe), INR/aPTT/fibrinogen, TEG/ROTEM (goal-directed coagulation), calcium (ionized, maintain > 1.1 during massive transfusion), potassium (post-transfusion), ABG, troponin (blunt cardiac), CPK (rhabdo), tox screen, EtOH, urine HCG.
18 Medications You Must Know
| Drug | Class | Use | Notes |
|---|---|---|---|
| Tranexamic acid (TXA) | Antifibrinolytic | Bleeding trauma within 3 h | 1 g IV load, 1 g over 8 h (CRASH-2/3) |
| 4-factor PCC (Kcentra) | Coagulation factor concentrate | Warfarin/DOAC reversal | 25–50 U/kg |
| Fresh frozen plasma (FFP) | Plasma product | MTP, coagulopathy | 1:1 with PRBC |
| Cryoprecipitate | Fibrinogen replacement | Fibrinogen < 150 | 10 units per pool |
| Packed red blood cells | Blood product | Hemorrhagic shock | Type O-negative emergency |
| Platelets | Blood product | MTP, < 50 for bleeding | Apheresis unit = ~6 pooled |
| Calcium gluconate / chloride | Electrolyte | Hypocalcemia from citrate | 1 g per 4 units PRBC |
| Norepinephrine | Vasopressor | Neurogenic shock, post-hemorrhage | Only after volume resuscitation |
| Etomidate / Ketamine | Induction | RSI | Ketamine preferred in shock |
| Succinylcholine / Rocuronium | NMB | RSI | Roc reversible with sugammadex |
| Fentanyl / Propofol / Precedex | Sedation/analgesia | Post-intubation ICU | Minimize in unresuscitated shock |
| Cefazolin ± aminoglycoside | Antibiotic | Open fracture prophylaxis | Gustilo-guided |
| Pip-tazo / ertapenem | Antibiotic | Penetrating abdominal/colon | Short-course per EAST |
| Tetanus toxoid / TIG | Immunization | All wounds | Per vaccination history |
| Levetiracetam | Antiepileptic | Severe TBI seizure prophylaxis | 7 days per BTF |
| Hypertonic saline / mannitol | Osmotherapy | Elevated ICP | Hypertonic avoids hypotension |
| Idarucizumab (Praxbind) | Reversal | Dabigatran | 5 g IV |
| Andexanet alfa (Andexxa) | Reversal | Apixaban/rivaroxaban | Cost and availability limit use |
| Vitamin K | Reversal | Warfarin (long-term) | 10 mg IV with PCC |
| Enoxaparin / heparin SC | VTE prophylaxis | Once bleeding controlled | Per EAST VTE guideline |
| Hydroxocobalamin | Antidote | Cyanide (smoke inhalation) | 5 g IV |
19 Classification & Scoring Systems
Glasgow Coma Scale (GCS)
| Component | Response | Score |
|---|---|---|
| Eye (E) | Spontaneous | 4 |
| To voice | 3 | |
| To pain | 2 | |
| None | 1 | |
| Verbal (V) | Oriented | 5 |
| Confused | 4 | |
| Inappropriate words | 3 | |
| Incomprehensible sounds | 2 | |
| None | 1 | |
| Motor (M) | Obeys commands | 6 |
| Localizes pain | 5 | |
| Withdraws from pain | 4 | |
| Abnormal flexion (decorticate) | 3 | |
| Abnormal extension (decerebrate) | 2 | |
| None | 1 |
Total 3–15. Severe TBI 3–8, moderate 9–12, mild 13–15.
Abbreviated Injury Scale (AIS)
Per-injury anatomic severity code used in trauma registries: 1 = minor, 2 = moderate, 3 = serious, 4 = severe, 5 = critical, 6 = unsurvivable. Each injury is assigned an AIS by body region (head/neck, face, chest, abdomen, extremity, external).
Injury Severity Score (ISS)
Sum of squares of the three highest AIS scores from different body regions. Range 1–75. Any AIS of 6 automatically sets ISS to 75. Major trauma conventionally defined as ISS > 15.
Revised Trauma Score (RTS) & TRISS
RTS is a weighted physiologic score combining GCS, SBP, and RR. TRISS combines ISS, RTS, age, and mechanism to estimate probability of survival; it is the standard benchmarking tool for trauma centers via the ACS TQIP program.
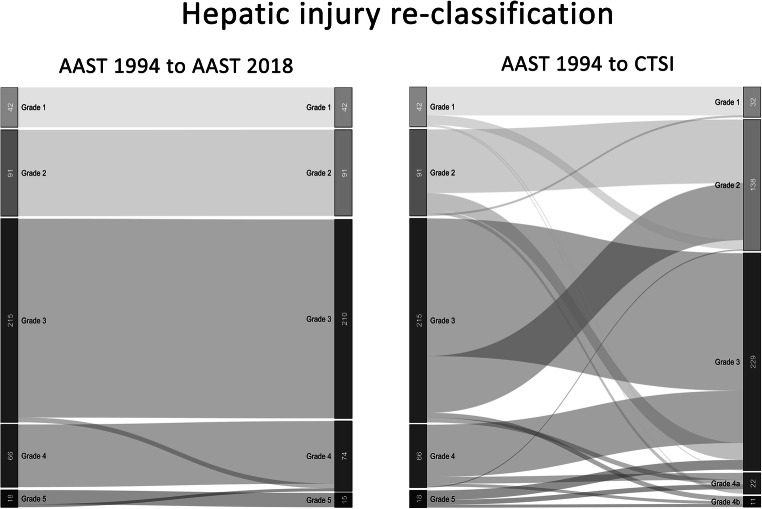
AAST Organ Injury Grading (Highlights)
I: Subcapsular hematoma < 10% SA, laceration < 1 cm.
II: SC hematoma 10–50%, laceration 1–3 cm, no trabecular vessel.
III: SC > 50% or expanding, laceration > 3 cm or trabecular vessel.
IV: Laceration involving segmental/hilar vessels, > 25% devascularization.
V: Shattered spleen or hilar vascular injury devascularizing the spleen.
I: SC < 10%, laceration < 1 cm. II: SC 10–50% or laceration 1–3 cm, < 10 cm length. III: SC > 50% or expanding, laceration > 3 cm depth. IV: Parenchymal disruption 25–75% of a hepatic lobe. V: > 75% lobe, juxtahepatic venous injury. VI: Hepatic avulsion.
I: Contusion, subcapsular hematoma. II: Non-expanding perirenal hematoma, cortical laceration < 1 cm. III: Cortical laceration > 1 cm without urinary extravasation. IV: Laceration through cortex/medulla/collecting system, segmental vascular injury. V: Shattered kidney, main renal pedicle avulsion.
I: Minor contusion/laceration without ductal injury. II: Major contusion/laceration without ductal injury. III: Distal transection with ductal injury. IV: Proximal transection or injury involving ampulla. V: Massive disruption of pancreatic head.
Additional Classifications
Gustilo-Anderson (open fractures): I, II, IIIA, IIIB, IIIC (see Section 13). Tile pelvic stability: A (stable), B (rotationally unstable), C (rotationally + vertically unstable). Young-Burgess pelvic mechanism: LC I–III, APC I–III, VS, CM. MESS: 1–11 total score, historical ≥ 7 cutoff for amputation. Marshall CT (TBI): I (no visible pathology), II (lesions < 25 cm³), III (cisterns compressed, midline shift 0–5), IV (midline shift > 5), V (any evacuated mass), VI (non-evacuated mass > 25 cm³). Rotterdam CT score: 0–6 based on basal cisterns, midline shift, epidural mass, IVH/SAH. Lund-Browder chart for pediatric TBSA.
20 Physical Exam — The Trauma Exam
The trauma exam is a rapid, systematic, head-to-toe assessment, documented region by region. A scribe should memorize the structure so it can be typed while the surgeon dictates.
General: A&Ox_ / sedated / intubated
HEENT: Atraumatic / lacerations / Battle sign / raccoon eyes / hemotympanum / pupils ___ reactive
Neck: C-collar in place / trachea midline / no JVD / no hematoma / no crepitus
Chest: Symmetric rise / CTAB / no crepitus / no tenderness / chest tube output
CV: RRR / no murmur / pulses 2+ throughout
Abdomen: Soft / non-distended / non-tender / no peritonitis / scars
Pelvis: Stable to compression / no perineal hematoma / no blood at meatus
GU/Rectal: Normal tone / no gross blood / prostate in position
Back: No step-off / no midline tenderness (log roll)
Extremities: No deformity / pulses present / cap refill < 2s / compartments soft
Neuro: GCS E_V_M_ / moves all extremities / sensation intact / reflexes
Always document the log roll as its own step. Missed injuries on the back — penetrating wounds, spinous process fractures, sacral injuries — are a classic source of morbidity and medico-legal risk.
21 Abbreviations Master List
Anatomy & Injury Patterns
Assessment & Scores
Procedures & Management
Medications, Labs, Blood Products
22 Sample HPI Templates
These templates show the documentation rhythm expected in a trauma bay and on the trauma admit service. Each template uses realistic mechanism, timing, and injury patterns.
"Patient is a 34-year-old unrestrained male driver involved in a single-vehicle rollover MVC at approximately 70 mph with prolonged extrication (~25 minutes). Per EMS, the patient was found unresponsive, intubated in the field with etomidate and rocuronium, and received 1 g of TXA and 1 unit of prehospital whole blood en route. Arrival vitals: BP 86/52, HR 134, SpO2 94% on vent, GCS 3T (sedated). Primary survey: intubated with breath sounds present bilaterally but diminished on the left; chest with crepitus along left lateral ribs; abdomen firm and distended; pelvis stable; grossly unstable right femur. Pupils 3 mm bilaterally reactive. Bedside FAST positive in the left upper quadrant and pelvis. MTP activated. Patient transferred to OR for exploratory laparotomy; CT head deferred until post-laparotomy resuscitation."
"Patient is a 22-year-old male brought in by police after sustaining a single gunshot wound to the right upper abdomen approximately 20 minutes prior to arrival. Weapon reportedly a handgun at close range. Arrival vitals: BP 92/56, HR 128, GCS 15. Single entry wound in the right mid-clavicular line 3 cm below the costal margin; no clear exit wound identified on the back during log roll. Abdomen with peritonitis on exam. FAST positive in Morison's pouch. Two large-bore IVs placed, uncrossmatched O-negative initiated (2 units), TXA 1 g IV given, tetanus updated, ceftriaxone 2 g administered. Patient taken emergently to OR for exploratory laparotomy."
"Patient is a 45-year-old restrained female driver involved in a moderate-speed (~35 mph) head-on MVC with airbag deployment, presenting with left-sided abdominal and chest pain. She is hemodynamically stable: BP 124/78, HR 92, SpO2 99% RA, GCS 15. Primary survey unremarkable; secondary survey notable for left anterolateral chest wall tenderness and left upper quadrant tenderness without peritonitis. No seatbelt sign. FAST negative. CT chest/abdomen/pelvis with IV contrast demonstrates a Grade III splenic laceration with a small amount of perisplenic hematoma and no active extravasation, left 6th and 7th rib fractures without pneumothorax, and no other injuries. Plan: admit to trauma surgery for non-operative management with serial hemoglobin, bed rest, and continuous telemetry."
"Patient is a 72-year-old male on apixaban for atrial fibrillation, found down at home by family after an unwitnessed fall, estimated down-time 2–4 hours. Arrival GCS 7 (E1 V2 M4), right pupil 5 mm and sluggish, left pupil 3 mm reactive. BP 168/94, HR 72. Intubated with ketamine and rocuronium for airway protection. CT head demonstrates a large right-sided acute subdural hematoma with 9 mm midline shift and effaced basal cisterns. Apixaban reversal initiated with 4-factor PCC 50 U/kg and andexanet per protocol. Neurosurgery consulted for emergent craniectomy. Levetiracetam load given for seizure prophylaxis. Hypertonic saline 3% bolus administered for elevated ICP concern. Transferred to OR."
"Patient is a 28-year-old male pedestrian struck by a vehicle at approximately 40 mph. Arrival vitals: BP 78/42, HR 142, GCS 14. Primary survey notable for unstable pelvis on compression and gross deformity of the right lower extremity. Pelvic binder placed at the greater trochanters. Two units of uncrossmatched PRBC initiated, MTP activated, TXA 1 g IV. FAST negative. Pelvic X-ray demonstrates an APC III open-book pelvic fracture with widened pubic symphysis and bilateral SI joint disruption. Patient taken to hybrid OR for preperitoneal pelvic packing, external fixation, and pelvic angiography with embolization of bilateral internal iliac branches."
"Patient is a 38-year-old male with burns sustained in a residential structure fire approximately 90 minutes prior to arrival. Was in the basement when the fire began; closed-space exposure with brief LOC per fire department. Arrival vitals: BP 118/72, HR 112, SpO2 96% on NRB, GCS 14. Exam reveals circumferential deep partial-thickness burns of bilateral upper extremities, anterior trunk, and face; singed nasal hairs with soot in oropharynx and hoarseness concerning for inhalation injury. Total TBSA estimated 32% by rule of nines. Carboxyhemoglobin 18%. Patient intubated prophylactically for airway protection. Parkland formula resuscitation initiated: 4 × 80 kg × 32 = 10,240 mL LR over 24 h, with half in first 8 hours from time of burn. Transferred to burn unit; burn surgery consulted for escharotomy evaluation of bilateral upper extremities."
Trauma is the most time-compressed documentation environment in medicine. Resuscitations happen fast, voices overlap, and the team leader needs a clean, accurate record at the end. The best trauma scribes anticipate the ATLS rhythm — they know the primary survey comes before the secondary, they know MTP is coming before it's called, they have the GCS template pre-populated before the patient rolls in.
Know your injury patterns, know your scoring systems, and know your procedures. Time-stamp everything. Spell drugs and doses correctly. When the surgeon says "Grade III splenic lac with contrast blush," you already know that means likely angioembolization or splenectomy, and you chart with that framework in mind.
Trauma care is a team sport, and the scribe is the team's memory. Welcome to the trauma bay.
23 References & Sources
Clinical Practice Guidelines
CDC Guidelines for Field Triage of Injured Patients. MMWR. 2011 (updated 2021).
ACS Committee on Trauma. Trauma Quality Improvement Program (TQIP). Best Practice Guidelines.
EAST Practice Management Guidelines: Penetrating Neck Injury. J Trauma. 2008.
EAST Practice Management Guidelines: Rib Fractures in the Elderly. J Trauma. 2012.
EAST Practice Management Guidelines: Geriatric Trauma. J Trauma Acute Care Surg. 2012.
SVS Clinical Practice Guidelines: Management of Traumatic Thoracic Aortic Injury. J Vasc Surg. 2011.
Landmark Clinical Trials
Diagram & Figure Sources
Figure 1: Trauma Room. Wikimedia Commons. Public domain.
Figure 2: ATLS Training. Wikimedia Commons. Public domain.
Figure 3: Tension Pneumothorax Diagram. Wikimedia Commons. Public domain.
Figure 4: FAST Exam. Wikimedia Commons. Public domain.
Figure 5: Burns Rule of Nines. Wikimedia Commons. Public domain.