Urgent Care
Every diagnosis, low-acuity presentation, procedure, medication, and documentation framework a scribe needs to work confidently in an urgent care clinic.
All diagrams on this page are sourced from published educational or institutional materials rather than AI generation. Each figure caption links to the original source, and the full diagram and guideline citations are collected in the references section at the bottom.
01 Urgent Care Scope & Triage Principles
Urgent care sits between the primary care office and the emergency department. Patients walk in (or register online) for problems that need same-day attention but are not immediately life threatening. A scribe in urgent care must learn to recognize the full range of low- and moderate-acuity complaints, understand when a presentation is too sick for the clinic, and document encounters efficiently because volumes are high and visits are short — most clinics aim for door-to-disposition times of under 45 minutes.

The scope of a typical urgent care includes minor illness (URI, flu, COVID, strep, sinusitis, otitis), lower-acuity injuries (sprains, simple fractures, lacerations, minor burns), common infections (UTI, cellulitis, skin abscess), simple women's health (UTI, vaginitis, pregnancy testing, emergency contraception, IUD removal in some clinics), pediatric minor illness, allergic reactions, dehydration requiring IV fluids, occupational medicine (work injuries, drug screens, pre-employment physicals, DOT exams), sports physicals, immunizations, and simple procedures (I&D, suturing, splinting, foreign body removal, cryotherapy).
Many urgent care networks use STARS or a similar rapid-triage mnemonic at the front desk to immediately identify patients who should be redirected to 911/ED rather than waiting in the lobby.
S — Stroke symptoms: facial droop, arm drift, slurred speech, sudden weakness → 911.
T — Trauma, major: high-mechanism falls, head injury with LOC, significant blood loss → ED.
A — Airway / breathing compromise: stridor, retractions, SpO2 < 92%, silent chest → 911.
R — Radiating chest pain / cardiac: pressure, diaphoresis, radiation to arm/jaw, known CAD → 911.
S — Severe bleeding, altered mental status, pregnancy with pain/bleeding, pediatric sepsis signs: → ED.
STEMI, stroke, sepsis with hemodynamic compromise, anaphylaxis after epinephrine (for observation), active major bleeding, open fractures, fractures with neurovascular compromise, ectopic pregnancy, testicular torsion, ocular chemical burns after initial irrigation, suicidal ideation with plan, new focal neurologic deficit, abdominal pain with peritoneal signs, acute abdomen, severe DKA, acute MI equivalent symptoms, high fever with toxic appearance in infants < 90 days.
Urgent care is defined as much by what it does not do as by what it does. If you are charting a patient whose vitals or exam make you uncomfortable, tell the provider immediately. Abnormal vitals (HR > 120, RR > 24, SpO2 < 94%, SBP < 90) should be repeated and flagged. Your early recognition can prevent a bad outcome.
02 Scribe Documentation Framework
Urgent care notes are short, focused, and problem-oriented. The chief complaint drives everything: the HPI, the ROS, the exam, and the plan all orbit a single reason for the visit. Unlike primary care, you are not documenting a comprehensive wellness review — you are creating a defensible same-day problem-focused note that another clinician could read in 30 seconds.
Chief Complaint (CC): One line in the patient's words — "sore throat x3 days," "cut finger slicing onion," "right ankle twisted playing soccer."
HPI — OLDCARTS: Onset, Location, Duration, Character, Aggravating/Alleviating, Radiation, Timing, Severity. Every urgent care HPI should also include pertinent negatives relevant to the red-flag workup (e.g., cough with no chest pain/SOB; ankle injury with no inability to bear weight).
SAMPLE history (especially for injuries and allergic reactions): Signs/symptoms, Allergies, Medications, Past medical/surgical history, Last oral intake, Events leading up to.
ROS: Keep it problem-focused. For a URI, document respiratory, ENT, constitutional. For a laceration, document the extremity and any neurovascular symptoms. Do not pad with unrelated systems.
Vitals: Always chart full vitals on arrival (T, HR, RR, BP, SpO2, pain scale, weight for pediatrics). Recheck abnormals.
General exam: Constitutional (well appearing vs toxic), then the system of concern. For a focused urgent care encounter, a 3–5 system exam is typical and appropriate.
POC results: Document specific numbers and positive/negative results — "Rapid strep positive," "UA: 3+ LE, 2+ nitrite, moderate blood," "SpO2 96% on RA."
Assessment: Each active problem gets an ICD-10-compatible diagnosis and a one-line clinical summary.
Plan: Medication prescribed (name, dose, frequency, duration, route), procedures performed, return precautions, follow-up instructions, work/school notes, and disposition. Always document return precautions verbatim ("return immediately for worsening shortness of breath, inability to tolerate po, fever > 102F not responding to antipyretics...").
Urgent care is a coding-heavy environment. The provider's E/M level depends on medical decision-making complexity and documented data reviewed. Make sure you capture every test ordered, every result reviewed (POC and outside records), and every independent interpretation (EKG read, X-ray wet read) — these contribute to the MDM level that drives billing.
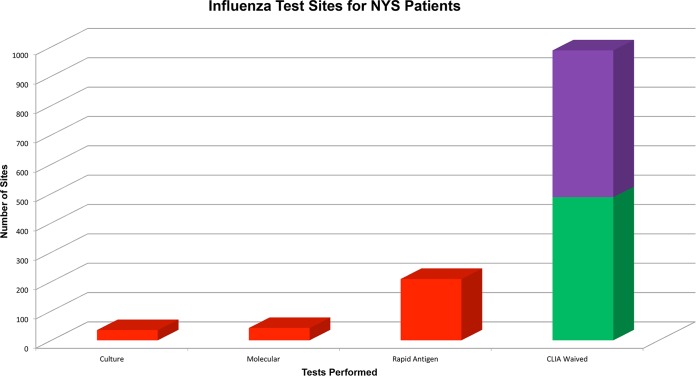
03 Upper Respiratory Infections (URI, Influenza, COVID) Infectious
Viral URI is the single most common presentation in urgent care. Patients arrive with cough, congestion, sore throat, and low-grade fever. The scribe's job is to document a thorough respiratory and ENT exam, capture the correct POC test results, and help the provider make the case for (or against) antibiotics.

Pathophysiology & Presentation
URIs are almost always viral (rhinovirus, coronavirus, adenovirus, RSV, influenza, parainfluenza, SARS-CoV-2). Symptoms evolve: days 1–3 are dominated by rhinorrhea and sore throat, days 3–7 by cough and congestion. Most uncomplicated URIs resolve within 7–10 days. Any worsening after day 7, or new fever after initial improvement, raises suspicion for bacterial superinfection (sinusitis, otitis media, pneumonia).
Influenza: Abrupt onset high fever (102–104F), severe myalgia, headache, dry cough, profound fatigue. Test: rapid flu A/B (nasal swab).
COVID-19: Cough, congestion, sore throat, fatigue, sometimes loss of taste/smell, GI symptoms. Test: rapid antigen or PCR.
Common cold (rhinovirus/coronavirus): Rhinorrhea, congestion, sneezing, mild cough, sore throat. No specific test.
RSV: Cough, wheeze, congestion; important in infants and older adults. Test: RSV antigen swab.
Management
Management is symptomatic: hydration, rest, acetaminophen or ibuprofen for fever, saline nasal spray, honey for cough (> 1 year old), humidified air, OTC decongestants (pseudoephedrine) and antihistamines. Antibiotics are not indicated for uncomplicated viral URI. Influenza within 48 hours of symptom onset can be treated with oseltamivir (Tamiflu) 75 mg BID x 5 days, especially in high-risk patients (age > 65, pregnancy, chronic lung disease, immunocompromised). COVID can be treated with nirmatrelvir-ritonavir (Paxlovid) in high-risk patients within 5 days of onset.
When a patient demands antibiotics for a cold, the provider will spend real time counseling on viral vs bacterial illness. Document this counseling — "extensive discussion regarding viral etiology, antibiotic stewardship, and symptomatic management." This protects the chart and the clinic quality metrics.
04 Streptococcal Pharyngitis & Mononucleosis Infectious
Sore throat is one of the top three urgent care chief complaints. The scribe must help distinguish Group A Streptococcus (treat with antibiotics to prevent rheumatic fever) from viral pharyngitis (no antibiotics), and recognize mononucleosis, which looks similar but is managed very differently.

Centor & McIsaac Criteria
The Centor criteria (modified as the McIsaac score) stratify risk of Group A strep in patients with pharyngitis. Document each element during the exam:
| Criterion | Points |
|---|---|
| Tonsillar exudates | +1 |
| Tender anterior cervical lymphadenopathy | +1 |
| Fever > 38°C (100.4°F) | +1 |
| Absence of cough | +1 |
| Age 3–14 years | +1 |
| Age 15–44 years | 0 |
| Age ≥ 45 years | −1 |
Interpretation: 0–1 = no testing/treatment; 2–3 = rapid antigen test, treat if positive; 4–5 = high likelihood, test or empirically treat. Per IDSA GAS pharyngitis guidelines, confirmed GAS is treated with penicillin V, amoxicillin, or a cephalosporin.
Treatment
First-line: amoxicillin 500 mg BID x 10 days (adults) or 50 mg/kg/day (children). Penicillin-allergic: cephalexin or azithromycin x 5 days. Treatment shortens symptom duration slightly and prevents acute rheumatic fever. Supportive care: ibuprofen or acetaminophen, warm salt-water gargles, throat lozenges.
Mononucleosis
Epstein-Barr virus infection, typically in adolescents and young adults. Presents with sore throat, fever, posterior cervical lymphadenopathy, profound fatigue, and sometimes splenomegaly and hepatomegaly. Exudative tonsillitis can mimic strep. Diagnosis: monospot (heterophile antibody) test. Treatment is supportive. Patients should avoid contact sports for 3–4 weeks because of splenic rupture risk. Never give amoxicillin if mono is suspected — it causes a characteristic morbilliform rash.
05 Sinusitis, Otitis Media & Otitis Externa Infectious
Acute Rhinosinusitis
Inflammation of the paranasal sinuses, usually viral. Symptoms: facial pain/pressure, purulent rhinorrhea, nasal congestion, decreased smell, maxillary tooth pain. The key question: viral or bacterial? Per the IDSA sinusitis guideline, acute bacterial sinusitis is suspected when any of the following are present: symptoms > 10 days without improvement, severe symptoms (fever ≥ 39°C, facial pain) for ≥ 3–4 days, or "double sickening" (initial improvement then worsening).

First-line treatment: amoxicillin-clavulanate (Augmentin) 875 mg BID x 5–7 days. Alternative: doxycycline. Adjuncts: intranasal saline, intranasal steroid (fluticasone), analgesics, decongestants (short course).
Acute Otitis Media (AOM)
Most common in young children. Presents with ear pain, fever, decreased hearing, and sometimes otorrhea (if TM ruptured). Exam: bulging, erythematous, opaque tympanic membrane with loss of landmarks; reduced mobility on pneumatic otoscopy. Per the AAP AOM guideline, treatment decisions depend on age and severity:

| Age | Severity | Approach |
|---|---|---|
| < 6 mo | Any | Antibiotics |
| 6–24 mo | Unilateral mild | Observe 48–72 h or treat |
| 6–24 mo | Bilateral or severe | Antibiotics |
| ≥ 2 yr | Mild unilateral | Observation option |
| ≥ 2 yr | Severe/bilateral | Antibiotics |
First-line: amoxicillin 80–90 mg/kg/day. Recent antibiotic use or treatment failure: amoxicillin-clavulanate.
Otitis Externa (Swimmer's Ear)
Infection of the external auditory canal. Classic presentation: ear pain worse with tragal manipulation or auricle traction, canal edema, debris, sometimes drainage. Usually bacterial (Pseudomonas, Staph aureus). Treatment: ofloxacin otic or ciprofloxacin-dexamethasone (Ciprodex) drops, 4 drops BID x 7 days. Keep ear dry. Ear wick for severe canal swelling.
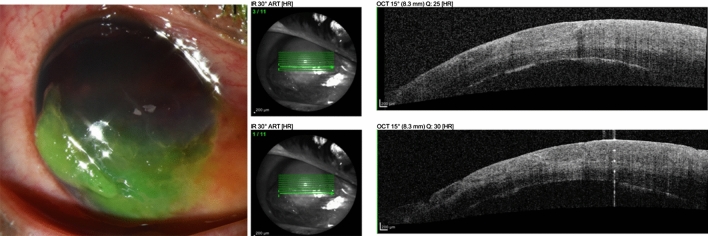
06 Conjunctivitis, Allergic Rhinitis & Eye Complaints Infectious
Conjunctivitis
Viral: Watery discharge, usually starts in one eye and spreads, often with URI symptoms. Highly contagious. Treatment: cool compresses, artificial tears, meticulous hand hygiene.
Bacterial: Thick mucopurulent discharge, eyelids matted shut in the morning. Treatment: erythromycin ointment or polymyxin-trimethoprim drops x 5–7 days.
Allergic: Bilateral, itchy, watery, associated with allergic rhinitis. Treatment: olopatadine drops, oral antihistamines.
Red flags that mean transfer: severe pain, photophobia, vision loss, contact lens wearer with pain (think keratitis), corneal opacity, ciliary flush — these suggest keratitis, iritis, or angle-closure glaucoma and need ophthalmology.
Allergic Rhinitis
Bilateral clear rhinorrhea, sneezing, itchy watery eyes, nasal congestion, often seasonal. Treatment: intranasal corticosteroids (fluticasone, mometasone), second-generation oral antihistamines (loratadine, cetirizine, fexofenadine), nasal antihistamines (azelastine). Avoid sedating antihistamines (diphenhydramine) in most adults.
07 Bronchitis, Pneumonia & Asthma/COPD Exacerbations Pulmonary
Acute Bronchitis
Cough ± sputum production, usually post-URI. Duration can be up to 3 weeks. Almost always viral. Do not prescribe antibiotics. Treatment: symptomatic (dextromethorphan, guaifenesin, honey, bronchodilator if wheezing).
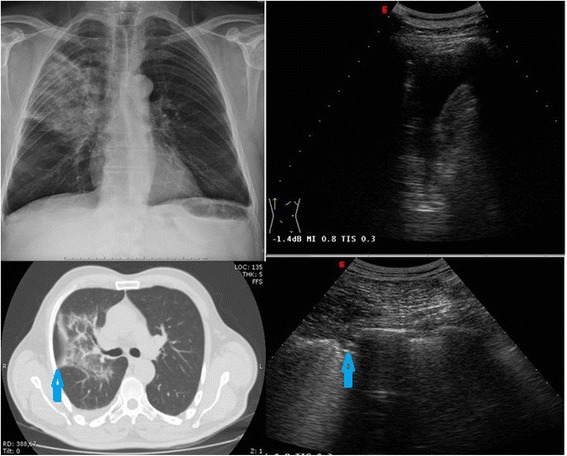
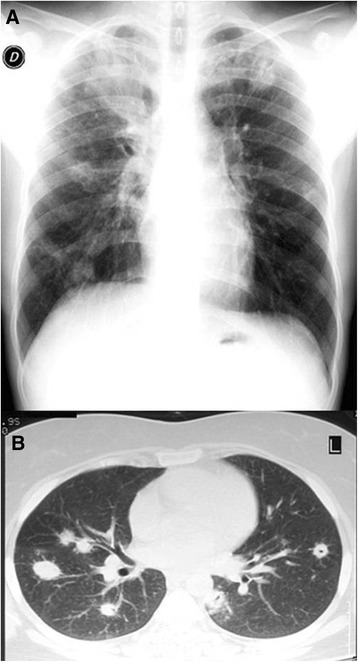
Community-Acquired Pneumonia (Mild, Outpatient)
Cough, fever, dyspnea, pleuritic chest pain, focal crackles on exam. Diagnosis: chest X-ray showing infiltrate. Severity assessment: CURB-65 — Confusion, Urea > 20, Respiratory rate ≥ 30, Blood pressure < 90/60, age ≥ 65. Score 0–1 = outpatient treatment; ≥ 2 = consider ED/admit.
Outpatient treatment (no comorbidities): amoxicillin 1 g TID or doxycycline. With comorbidities (COPD, diabetes, CKD): respiratory fluoroquinolone (levofloxacin) OR beta-lactam + macrolide per IDSA/ATS CAP guidelines.
Asthma Exacerbation (Mild-Moderate)
Wheeze, cough, dyspnea, chest tightness. Assess: SpO2, peak flow if available, work of breathing, speech in full sentences. Treatment: albuterol nebulizer or MDI (4–8 puffs via spacer) q20 min x 3, ipratropium added if moderate, oral prednisone 40–60 mg daily x 5 days. Transfer for persistent SpO2 < 92%, severe work of breathing, silent chest, altered mental status.
COPD Exacerbation (Mild)
Increased dyspnea, cough, sputum change. Treatment: albuterol/ipratropium nebs, prednisone 40 mg x 5 days, and antibiotics (azithromycin or doxycycline) if two of three Anthonisen criteria (increased dyspnea, increased sputum volume, increased sputum purulence).

08 UTI, Vaginitis & STIs Genitourinary
Uncomplicated Cystitis
Dysuria, frequency, urgency, suprapubic pain in an otherwise healthy non-pregnant woman. UA: +LE, +nitrite, +blood. Per IDSA uncomplicated UTI guidelines, first-line therapy is nitrofurantoin 100 mg BID x 5 days, TMP-SMX DS BID x 3 days (if local resistance < 20%), or fosfomycin 3 g single dose. Phenazopyridine (Pyridium) for symptomatic relief x 2 days.
Pyelonephritis
Fever, flank pain, CVA tenderness, ± nausea/vomiting. Outpatient management only if stable and tolerating po: ciprofloxacin 500 mg BID x 7 days or levofloxacin 750 mg daily x 5 days. IM ceftriaxone 1 g as a one-time dose before starting oral therapy is common in urgent care. Transfer if toxic, pregnant, unable to tolerate po, septic.
Vaginitis
Bacterial vaginosis: thin gray discharge, fishy odor, clue cells, pH > 4.5. Rx: metronidazole 500 mg BID x 7 days.
Candida: thick white "cottage cheese" discharge, pruritus. Rx: fluconazole 150 mg single dose.
Trichomonas: frothy yellow-green discharge, strawberry cervix. Rx: metronidazole 2 g single dose (treat partner).
STI Screening & Treatment
Per CDC 2021 STI treatment guidelines:
- Gonorrhea: ceftriaxone 500 mg IM single dose (1 g if ≥ 150 kg).
- Chlamydia: doxycycline 100 mg BID x 7 days (azithromycin 1 g x1 if pregnant or adherence concern).
- Syphilis (primary/secondary): benzathine penicillin G 2.4 million units IM x1.
- Trichomonas: metronidazole 500 mg BID x 7 days (women).
- Herpes (initial): acyclovir 400 mg TID x 7–10 days or valacyclovir 1 g BID x 7–10 days.
09 GI Complaints GI
Acute Gastroenteritis
Nausea, vomiting, diarrhea, ± cramping, usually viral (norovirus, rotavirus). Assess hydration: mucous membranes, skin turgor, capillary refill, orthostatic vitals. Treatment: oral rehydration (Pedialyte, Gatorade), BRAT-like diet as tolerated, ondansetron 4–8 mg ODT for nausea, loperamide for non-bloody diarrhea (avoid if febrile or bloody). IV fluids (1–2 L NS or LR) for moderate dehydration. Transfer if severe dehydration, bloody diarrhea with sepsis, peritoneal signs.
GERD / Dyspepsia
Burning retrosternal pain, regurgitation, worse after meals or lying down. Treatment: PPI (omeprazole 20–40 mg daily), lifestyle modification, H2 blocker as adjunct. Always rule out cardiac etiology first in adults with new epigastric pain.
Constipation
Treatment: increase fiber/fluids, polyethylene glycol (MiraLAX) 17 g daily, docusate, senna, bisacodyl suppository, glycerin suppository, or enema for severe impaction.
Dehydration
Common reason for IV fluids in urgent care. Document orthostatics, vitals, exam findings, and response to therapy. Typical order: NS or LR 1 L IV, reassess vitals, second liter if needed, ondansetron IV 4 mg.
10 Headache, Dizziness, Syncope & Weakness Neurologic
Non-Emergent Headache
Tension-type, migraine, medication overuse. Always ask about red flags: sudden "thunderclap," worst headache of life, focal deficit, fever with neck stiffness, new headache after age 50, headache with trauma, immunocompromised, anticoagulated. Any red flag → ED.
Treatment: hydration, NSAIDs, acetaminophen, triptans for migraine, IV fluids + metoclopramide + ketorolac + diphenhydramine for migraine cocktail if IV access available.
Dizziness
Distinguish vertigo (spinning) from lightheadedness (presyncope) from disequilibrium. Benign paroxysmal positional vertigo (BPPV) — brief episodes with head movement, diagnosed by Dix-Hallpike, treated with Epley maneuver. Vestibular neuritis — constant vertigo lasting days, treated with meclizine and reassurance. Red flags: new hearing loss, neuro deficit, inability to walk → ED for central cause workup.
Syncope (Resolved)
If fully recovered, check EKG, glucose, BP (orthostatic), and pregnancy test if applicable. Vasovagal syncope with clear prodrome is reassuring. Any cardiac history, exertional syncope, family history of sudden death, abnormal EKG → ED.
Generalized Weakness
Vague, often multifactorial. Common urgent care causes: dehydration, viral illness, anemia, medication side effect, UTI in elderly. Screen with vitals, glucose, UA, EKG, and basic labs if available. Focal weakness → ED.
11 Back Pain, Sprains, Strains & Simple Fractures MSK
Acute Low Back Pain
Most commonly mechanical/musculoligamentous. Red flags: saddle anesthesia, bowel/bladder incontinence (cauda equina), IV drug use/fever (epidural abscess), history of cancer, trauma, progressive neuro deficit, severe night pain. Any red flag → imaging and/or ED. Uncomplicated: NSAIDs, acetaminophen, heat, stay active, muscle relaxant (cyclobenzaprine or methocarbamol) short course, no bed rest. Per ACP low back pain guideline, first-line is non-pharmacologic plus NSAIDs.
Sprains & Strains
Grade I = stretch, grade II = partial tear, grade III = complete tear. Treatment: RICE (rest, ice, compression, elevation), NSAIDs, brief immobilization, early mobilization and PT. Use the Ottawa ankle/knee/foot rules to decide on X-ray.
Ankle X-ray indicated if pain in malleolar zone AND any of:
- Bone tenderness along distal 6 cm of posterior tibia / tip of medial malleolus
- Bone tenderness along distal 6 cm of posterior fibula / tip of lateral malleolus
- Inability to bear weight both immediately after injury and in the ED/clinic (4 steps)
Foot X-ray indicated if midfoot pain AND any of:
- Bone tenderness at the base of the 5th metatarsal
- Bone tenderness at the navicular
- Inability to bear weight (4 steps)
Per the Ottawa rules validation, sensitivity approaches 100% for clinically significant fractures.
X-ray indicated if any: age ≥ 55, isolated patellar tenderness, tenderness at head of fibula, inability to flex to 90°, inability to bear weight (4 steps) immediately and now.
Simple Fractures
Common urgent care fractures: distal radius (Colles'), 5th metacarpal (boxer's), toe, finger (tuft/distal phalanx), clavicle, nasal, 5th metatarsal (Jones vs avulsion). Treatment: splint or buddy tape, ice, elevation, analgesia, ortho follow-up within 3–7 days. Open fractures, neurovascular compromise, displacement requiring reduction beyond clinic capability, compartment syndrome → ED.
C-spine imaging is NOT needed if ALL of: (1) no posterior midline cervical tenderness, (2) no focal neurologic deficit, (3) normal level of alertness, (4) no intoxication, (5) no painful distracting injury. If any present, image or transfer.
12 Lacerations, Abscess, Cellulitis & Bites Skin/Wound
Laceration Repair
Document: mechanism, time of injury (ideally closed < 12 h for trunk/extremity, < 24 h for face), contamination, foreign body, neurovascular and tendon exam distal to the wound, tetanus status. Irrigate copiously (100–200 mL per cm of wound) with saline. Close with sutures, staples, skin adhesive, or Steri-Strips depending on location.
| Location | Suture | Remove |
|---|---|---|
| Face | 6-0 nylon/prolene | 5 days |
| Scalp | 4-0 nylon or staples | 7–10 days |
| Trunk | 4-0 nylon | 7–10 days |
| Arm/Leg | 4-0 nylon | 10–14 days |
| Hand/Foot | 4-0 or 5-0 nylon | 10–14 days |
| Over joint | 4-0 nylon | 14 days |
Skin Abscess — Incision & Drainage
Fluctuant, erythematous, tender collection. Treatment: I&D is the cornerstone. After I&D, antibiotics are indicated per IDSA SSTI guidelines if: > 2 cm, multiple sites, systemic illness, immunocompromised, failed initial drainage, indwelling devices, or extremes of age. First-line for MRSA coverage: TMP-SMX DS BID x 5–7 days, doxycycline, or clindamycin.

Cellulitis
Non-purulent: streptococcal, treat with cephalexin 500 mg QID or dicloxacillin x 5–7 days. Purulent: MRSA coverage with TMP-SMX, doxycycline, or clindamycin. Mark borders with pen and instruct patient to return if spreading. Severe cellulitis, systemic symptoms, rapidly spreading erythema, suspected necrotizing fasciitis → ED.
Animal / Human Bites
Cat bites are high-risk for Pasteurella. Human bites (including clenched-fist "fight bites") are high-risk for Eikenella. Treatment: copious irrigation, leave wound open if puncture/cat bite, close face wounds primarily, amoxicillin-clavulanate 875 mg BID x 5–7 days. Tetanus update. Rabies risk assessment for wild animal or unknown-vaccination-status domestic animal bites.
13 Dermatology (Rashes, Shingles, Tinea, Scabies, Warts) Skin/Wound
Contact Dermatitis (Poison Ivy, Nickel, Soaps)
Pruritic, erythematous, vesicular rash in linear streaks (classic for plant contact). Treatment: topical mid-high potency steroid (triamcinolone, clobetasol for limited severe areas), oral antihistamine, calamine, oatmeal baths. Oral prednisone 40–60 mg daily x 5–7 days (or tapered over 10–14 days) for severe cases, especially on face or genitals.
Eczema (Atopic Dermatitis)
Chronic pruritic condition, flexural surfaces in children. Treatment: emollients, low-mid potency topical steroid, antihistamines.
Urticaria (Hives)
Raised, blanching, migratory wheals. Treatment: H1 antihistamine (cetirizine 10 mg or higher), adding H2 blocker (famotidine) and short prednisone course for severe outbreaks. If airway involvement or anaphylaxis → epinephrine + ED.
Drug Rash
Morbilliform, usually 7–14 days after new medication. Stop the drug. Red flags for Stevens-Johnson / TEN: mucosal involvement, skin pain, bullae, systemic symptoms → ED.
Herpes Zoster (Shingles)
Painful vesicular rash in a dermatomal distribution. Treatment within 72 h: valacyclovir 1 g TID x 7 days. Adjunct analgesia. Ophthalmology if V1 involvement (Hutchinson's sign: lesion on tip of nose → risk of herpes zoster ophthalmicus).

Tinea (Corporis, Pedis, Cruris)
Ring-shaped scaling with central clearing. Treatment: topical terbinafine or clotrimazole BID x 2–4 weeks. Tinea capitis and onychomycosis require oral terbinafine.
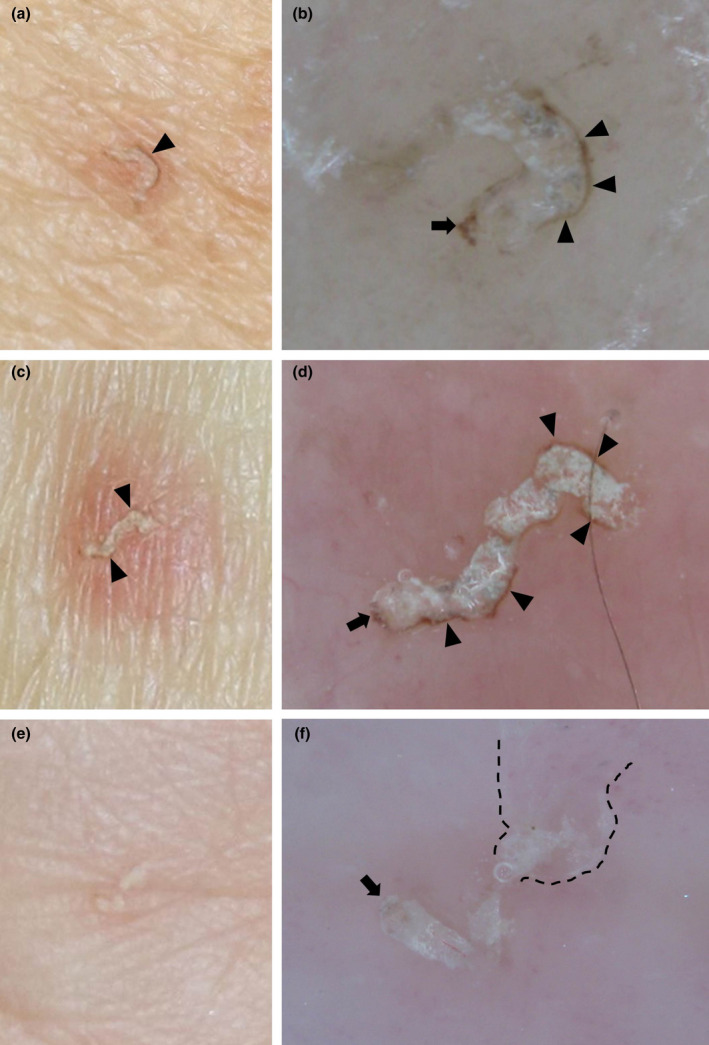
Scabies
Intense pruritus worse at night, interdigital burrows, finger webs, wrists. Treatment: permethrin 5% cream head-to-toe, wash off in 8–14 h, repeat in 1 week. Treat household contacts. Wash linens in hot water.
Warts (Verruca Vulgaris)
HPV-caused. Treatment: cryotherapy with liquid nitrogen (10–20 sec freeze, thaw, refreeze), salicylic acid.
14 Burns, Foreign Bodies, Nail & Eye Injuries Trauma
Minor Burns
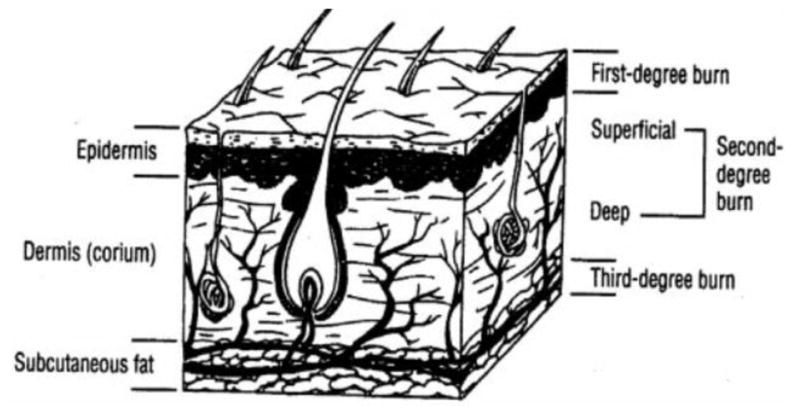
First-degree: erythema only, painful. Superficial partial-thickness (2nd degree): blisters, wet, very painful. Treatment: cool water irrigation, cleanse, debride ruptured blisters, apply bacitracin or silver sulfadiazine (avoid on face), non-adherent dressing. Tetanus. Transfer burns > 10% BSA, circumferential, full-thickness, or involving face/hands/feet/genitals/joints.
Foreign Body Removal
Eye: fluorescein stain, slit lamp or Wood's lamp, topical anesthetic (proparacaine), remove with moistened cotton swab or 25-gauge needle. Rust ring requires ophthalmology if not easily removed. Prescribe erythromycin ointment and follow up.
Ear/Nose: alligator forceps, curette, suction, or irrigation (not for live insects — kill with mineral oil first; not for organic matter like beans that swell).
Skin: splinters, fishhooks, glass. Anesthetize, explore, remove, consider X-ray for radiopaque foreign bodies.
Nail Injuries
Subungual hematoma > 50% of nail bed: trephination with heated paperclip or 18-g needle to relieve pressure. Complex nail bed lacerations: may require nail removal and repair with absorbable suture. Paronychia: warm soaks, drainage if fluctuant.
Corneal Abrasion
Fluorescein uptake, linear defect. Treatment: erythromycin ointment QID, oral analgesia, no patch (increases infection risk), no topical anesthetic prescription, follow up in 24 h. Contact lens wearers need pseudomonal coverage (ciprofloxacin or ofloxacin drops).
15 Chest Pain Workup & Low-Risk Cardiac Presentations Cardiovascular
Chest pain is the highest-liability urgent care presentation. Your job as a scribe is to document thoroughly so the provider's reasoning is clear. The provider will typically risk-stratify using clinical impression plus EKG and, in some clinics, point-of-care troponin. Any concerning presentation → 911/ED.
PE can be excluded clinically in a low-pretest-probability patient if ALL eight are negative:
- Age < 50
- HR < 100
- SpO2 ≥ 95% on room air
- No hemoptysis
- No estrogen use
- No prior DVT/PE
- No unilateral leg swelling
- No surgery/trauma requiring hospitalization in past 4 weeks
Per the PERC derivation study, a negative PERC in a low-risk patient has < 2% PE probability.
Classic red flags suggesting ACS: pressure, exertional, radiation to jaw/left arm, diaphoresis, nausea, known CAD, risk factors (age, HTN, DM, smoking, hyperlipidemia, family history). Atypical presentations in women, diabetics, and elderly. Any red flag → EKG immediately, 911 for transport.
Low-risk presentations that stay in urgent care: reproducible chest wall tenderness (costochondritis), clear musculoskeletal or pleuritic features with no cardiac risk, clearly GI reflux. Treatment: NSAIDs, heat, reassurance, PPI trial if GERD suspected.
16 Allergic Reactions & Anaphylaxis Emergent
Mild allergic reactions (hives, itching, mild facial swelling without airway involvement) are common. Treatment: diphenhydramine 25–50 mg, cetirizine 10 mg, famotidine 20 mg, consider prednisone 40–60 mg x 3–5 days, observe 1–2 hours.
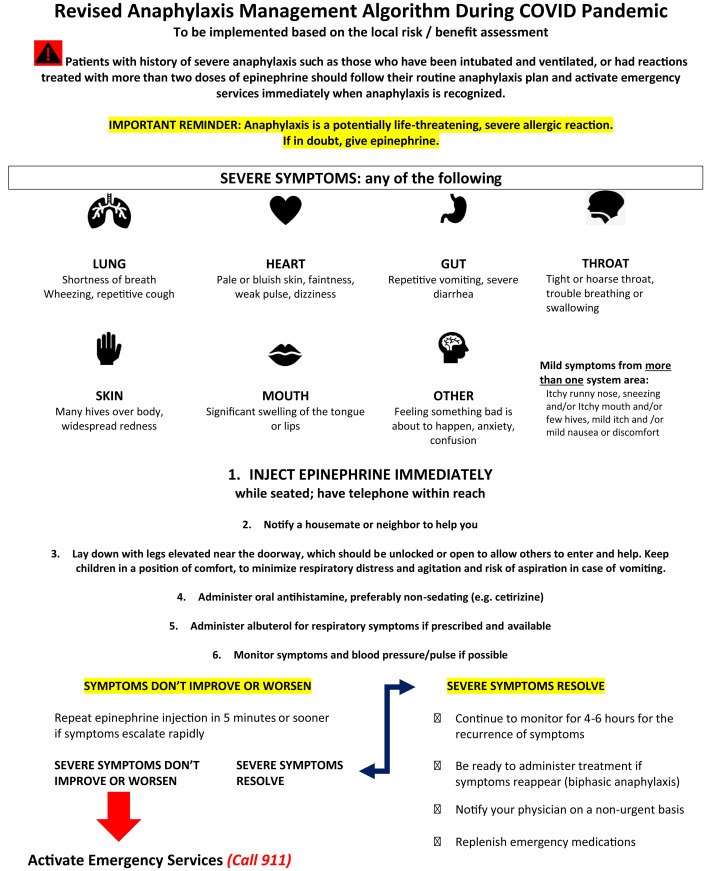
Two or more organ systems involved (skin + respiratory, skin + GI, etc.) OR hypotension after exposure to a likely allergen. Give IM epinephrine 0.3 mg (adult) or 0.15 mg (pediatric) into the lateral thigh immediately. Can repeat every 5–15 min. Support airway, give IV fluids, H1/H2 blockers, nebulized albuterol for wheeze, IV steroids. All anaphylaxis patients go to the ED for observation due to biphasic reaction risk. Prescribe epinephrine auto-injectors (EpiPen) x 2 on discharge and refer to allergy.
17 Occupational Medicine, Physicals & Work Injuries Occupational
Urgent care is the primary site for occupational health services. Scribes should know these documentation patterns cold because they are highly structured and time sensitive.
Work Injuries (Workers' Compensation)
Every work injury requires special documentation: employer name, date/time of injury, mechanism, body part affected, witnesses, first aid rendered, current symptoms, relevant past history, functional status, and work status determination (full duty, modified duty with specific restrictions, or off work with return date). Most clinics have state-specific WC forms to complete.
Pre-Employment / DOT / Sports Physicals
Structured head-to-toe exam with vision screening, hearing, BP, BMI, urine drug screen as applicable. DOT (Department of Transportation) exams have specific federal criteria and require a certified medical examiner. Sports physicals screen for cardiovascular risk (family history of sudden death, syncope, murmur, Marfanoid features).
Drug Screens
Observed or unobserved urine collection, chain of custody, specific panel (5-panel, 10-panel, DOT panel). Document temperature and pH of sample.
Vaccinations
Tetanus (Tdap/Td), influenza, COVID boosters, Hepatitis B for occupational exposure, travel vaccines in some clinics. Always document lot number, site, dose, and VIS date.
18 Urgent Care Procedures A to Z
| Procedure | Indication | Key Documentation Points |
|---|---|---|
| Simple wound repair (sutures) | Lacerations with clean edges | Size (cm), depth, location, irrigation volume, anesthetic, suture type/size, number of sutures, tetanus |
| Skin adhesive (Dermabond) | Short, low-tension wounds | Location, length, approximation |
| Staples | Scalp lacerations | Number of staples, hemostasis |
| Incision & drainage | Skin abscess | Size, location, anesthetic, volume/character of drainage, packing (iodoform) vs no packing, culture |
| Splinting | Sprains, simple fractures | Type (volar, sugar-tong, thumb spica, posterior ankle), materials, neurovascular check pre/post |
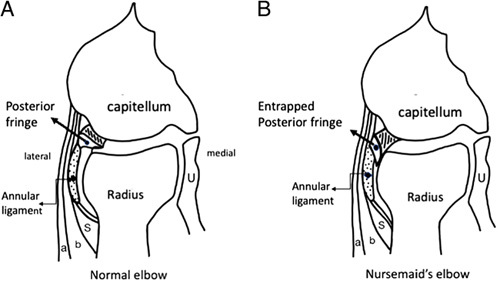
| Joint reduction (simple) | Finger dislocation, nursemaid's elbow | Technique, anesthesia, neurovascular pre/post, post-reduction X-ray |
| Foreign body removal (eye) | Corneal foreign body | Fluorescein exam, anesthetic, method, post-removal erythromycin |
| Foreign body removal (skin) | Splinter, glass, fishhook | Location, size, X-ray if radiopaque, hemostasis, tetanus |
| Ear lavage / curette | Cerumen impaction | Visualization before/after, tolerance |
| Eye irrigation | Chemical exposure, particulate | Morgan lens or saline, duration, pH before/after |
| Nail trephination | Subungual hematoma > 50% | Relief of pressure, amount drained |
| Cryotherapy | Warts, actinic keratoses, skin tags | Freeze time, lesion count, location |
| Skin tag removal | Cosmetic/irritated skin tags | Method (scissor excision, cryo), number, hemostasis |
| IUD removal | Expired IUD, patient request | Speculum exam, strings visible, smooth removal |
| EKG | Chest pain, palpitations, syncope | Rate, rhythm, intervals, axis, ST changes, comparison to prior |
| X-ray (basic interpretation) | Ortho, respiratory | Wet read by provider, radiology overread |
| Spirometry | Asthma/COPD, occupational | FEV1, FVC, FEV1/FVC ratio, pre/post bronchodilator |
| IM injection | Ceftriaxone, Depo-Medrol, toradol, epinephrine | Drug, dose, site, lot # |
| IV access & fluids | Dehydration, abscess, migraine | Site, gauge, fluid type, volume, rate, response |
| Nebulizer treatment | Asthma, COPD, croup | Drug, dose, pre/post vitals and lung exam |
19 Labs, POC Testing & Imaging
Point-of-Care Tests
| Test | Turnaround | Notes |
|---|---|---|
| Rapid strep (GAS) | 5–10 min | Throat swab; negatives in children should reflex to culture |
| Rapid influenza A/B | 10–15 min | Nasal swab; sensitivity ~60–80% |
| COVID-19 antigen | 15 min | Nasal swab; confirm with PCR if high clinical suspicion |
| Monospot | 5 min | Heterophile antibody; may be negative in first week |
| Urinalysis (dipstick) | 2 min | LE, nitrite, blood, protein, glucose, ketones |
| Urine hCG | 3 min | Pregnancy screen; essential before imaging or Rx |
| Fingerstick glucose | < 1 min | Hypoglycemia, hyperglycemia screening |
| RSV antigen | 15 min | Nasal swab; pediatric respiratory illness |
| HIV rapid | 20 min | Blood or oral fluid |
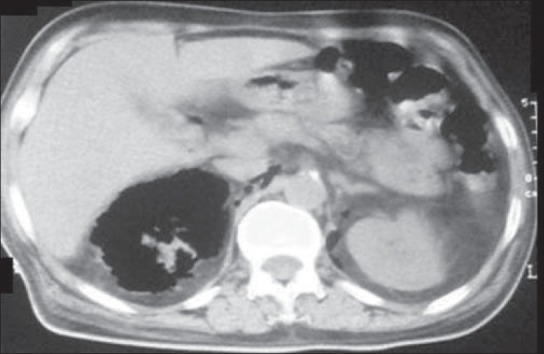
Imaging
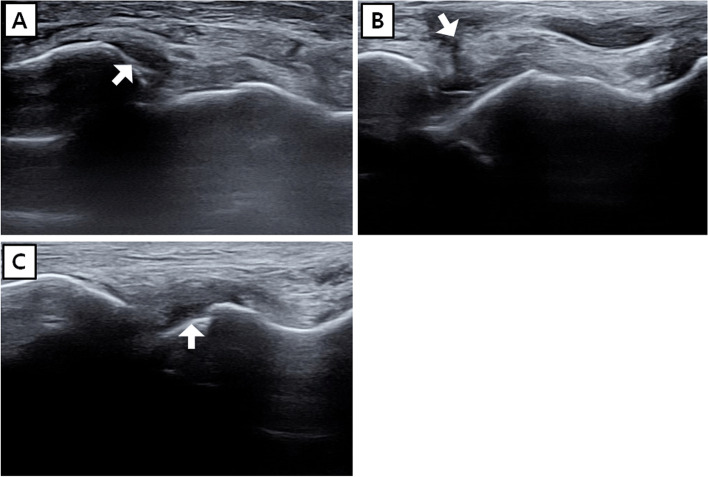
Plain films are the workhorse of urgent care: extremity fractures, chest X-ray for pneumonia workup, abdominal X-ray for foreign bodies and obstruction. Decisions on when to image follow the ACR Appropriateness Criteria. Ultrasound (FAST, bladder scan, abscess vs cellulitis) is available in some urgent care clinics. CT and MRI are not — if needed, transfer to ED or schedule outpatient.
20 Medications You Must Know
| Drug | Class | Common Use |
|---|---|---|
| Amoxicillin | Aminopenicillin | Strep throat, AOM, CAP, sinusitis |
| Amoxicillin-clavulanate (Augmentin) | Beta-lactam + inhibitor | Sinusitis, bite wounds, CAP |
| Cephalexin (Keflex) | 1st-gen cephalosporin | Non-purulent cellulitis, strep |
| Azithromycin (Z-pak) | Macrolide | Atypical pneumonia, chlamydia, pertussis |
| Doxycycline | Tetracycline | CAP, Lyme, chlamydia, MRSA SSTI |
| TMP-SMX (Bactrim DS) | Folate antagonist | UTI, MRSA SSTI |
| Nitrofurantoin (Macrobid) | Nitrofuran | Uncomplicated cystitis |
| Ciprofloxacin | Fluoroquinolone | Pyelonephritis, traveler's diarrhea |
| Levofloxacin | Fluoroquinolone | CAP with comorbidities, pyelonephritis |
| Clindamycin | Lincosamide | MRSA SSTI, dental infection |
| Metronidazole | Nitroimidazole | BV, trichomonas, giardia |
| Fluconazole | Azole | Candida vaginitis |
Oseltamivir (Tamiflu) for influenza. Valacyclovir / acyclovir for HSV, VZV. Nirmatrelvir-ritonavir (Paxlovid) for COVID in high-risk.
Acetaminophen (Tylenol) ≤ 3 g/day. Ibuprofen (Advil, Motrin) 400–600 mg q6h. Naproxen (Aleve) 500 mg BID. Ketorolac (Toradol) IM/IV 15–30 mg. Short-course opioids (hydrocodone-APAP, tramadol) only if necessary. Cyclobenzaprine (Flexeril) 5–10 mg for muscle spasm. Methocarbamol (Robaxin).
Albuterol MDI/neb. Ipratropium (Atrovent). Fluticasone-salmeterol (Advair) and budesonide-formoterol (Symbicort) as maintenance ICS/LABA. Fluticasone nasal spray. Loratadine, cetirizine, fexofenadine, diphenhydramine. Montelukast. Guaifenesin, dextromethorphan, pseudoephedrine.
Ondansetron (Zofran) 4–8 mg. Metoclopramide (Reglan). Promethazine (Phenergan). Omeprazole, pantoprazole, famotidine. Loperamide (Imodium), bismuth subsalicylate (Pepto-Bismol). Polyethylene glycol (MiraLAX), docusate, senna.
Topical steroids: hydrocortisone 1–2.5%, triamcinolone, clobetasol. Topical antifungals: clotrimazole, terbinafine, nystatin. Topical antibiotics: mupirocin, bacitracin. Ophthalmic: erythromycin ointment, polymyxin-trimethoprim, moxifloxacin. Otic: ofloxacin, ciprodex. Injectables: ceftriaxone IM, depo-medrol IM, toradol IM, epinephrine IM, dexamethasone IM.
Prednisone 40–60 mg daily x 5 days for asthma, COPD, poison ivy. Methylprednisolone (Medrol dose pack). IV fluids: normal saline (NS), lactated Ringer's (LR); 500–1000 mL boluses common. IV antibiotics occasionally: ceftriaxone 1 g, vancomycin (rare).
21 Classification & Decision Rules
1 point each: Confusion, Urea (BUN) > 19 mg/dL, Respiratory rate ≥ 30, Blood pressure < 90/60, age ≥ 65.
0–1: outpatient. 2: consider short admission. ≥ 3: inpatient, consider ICU.
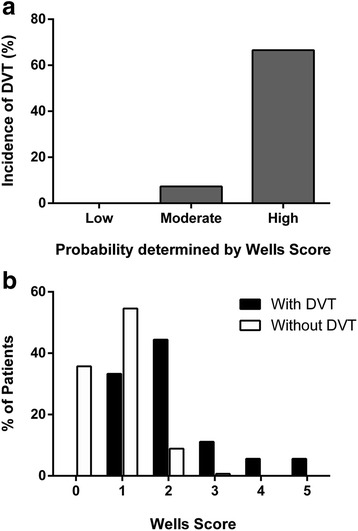
Active cancer, paralysis/immobilization, recent surgery or bedrest, localized tenderness along deep veins, entire leg swollen, calf swelling > 3 cm larger, pitting edema, collateral superficial veins, previous DVT (+1 each); alternative diagnosis more likely (−2).
≥ 2 = DVT likely (imaging); < 2 = unlikely (D-dimer).
(1) Increased dyspnea, (2) increased sputum volume, (3) increased sputum purulence. Two of three = antibiotics indicated.
Eye opening 1–4, verbal response 1–5, motor response 1–6. Range 3–15. ≤ 8 = severe, intubate; 9–12 = moderate; 13–15 = mild.
22 Physical Exam & Abbreviations Master List
Focused Exam by Chief Complaint
In urgent care, a focused problem-oriented exam is standard. For a sore throat: general appearance, vitals, HEENT (tonsils, exudates, cervical nodes, TMs, nares), neck (lymphadenopathy, meningismus), respiratory. For an ankle injury: vitals, inspection (ecchymosis, swelling, deformity), palpation (bony tenderness per Ottawa rules), range of motion, neurovascular (pulses, sensation, capillary refill), ability to bear weight, special tests (anterior drawer, talar tilt).
Gen: well appearing, NAD, AxOx3
HEENT: NCAT, PERRL, EOMI, oropharynx clear, moist mucous membranes
Neck: supple, no lymphadenopathy, no meningismus
CV: RRR, no m/r/g, pulses 2+
Pulm: CTAB, no wheeze/rales/rhonchi, normal WOB
Abd: soft, non-tender, non-distended, +BS
Ext: no edema, no calf tenderness
Skin: warm, dry, intact, no rash
Neuro: CN II-XII intact, 5/5 strength, sensation intact
Abbreviations Master List
23 ED Transfer Criteria & Red Flags
Knowing when to transfer is the single most important safety skill in urgent care. The following list is not exhaustive but covers the most common clean hand-offs.
- Chest pain with red flags (pressure, diaphoresis, radiation, ECG changes)
- Stroke symptoms (facial droop, slurred speech, unilateral weakness)
- Respiratory distress, SpO2 < 92% not rapidly correctable, stridor
- Anaphylaxis after epinephrine (for observation)
- Major trauma, head injury with LOC or anticoagulation
- Active major bleeding, uncontrolled epistaxis
- GI bleeding, hematemesis, melena
- Severe abdominal pain, suspected appendicitis, ectopic, peritonitis
- New altered mental status, seizure, syncope with cardiac features
- DKA, glucose > 500 with symptoms, severe hyperkalemia
- Septic appearance, hemodynamic instability
- Suicidal ideation with plan
- Infants < 90 days with fever ≥ 38°C
- Open fracture, neurovascular compromise, compartment syndrome
- Testicular torsion, priapism
- Ocular trauma with vision loss, chemical burn to eye (after irrigation)
24 Sample HPI Templates & Closing Note
These templates model the rhythm of a real urgent care note — short, focused, and specific. Use them as pattern matching for your first weeks on the job.
"Mr. [Name] is a 34-year-old male with no significant PMH presenting with 4 days of nasal congestion, clear rhinorrhea, mild sore throat, and intermittent dry cough. He reports a low-grade subjective fever (not measured) on day 1 but has been afebrile since. He denies shortness of breath, chest pain, ear pain, facial pressure, rash, or GI symptoms. He has been taking OTC DayQuil with partial relief. No sick contacts identified. He requests evaluation to rule out strep or flu and to obtain a work note. Vitals on arrival unremarkable. No tobacco. No known drug allergies."
"Ms. [Name] is a 28-year-old right-hand dominant female who sustained a laceration to the volar aspect of her left index finger approximately 45 minutes ago while slicing vegetables at home with a chef's knife. She reports immediate bleeding, controlled with direct pressure. She denies numbness, tingling, inability to flex or extend, or retained foreign body. Tetanus last updated 3 years ago per patient report. She takes no medications and has no medical history. The wound appears clean, approximately 1.8 cm, linear, with uniform edges, confined to the dermis. Neurovascular exam distal to the wound is intact: 2-point discrimination < 5 mm, full active ROM, capillary refill < 2 s."
"Mr. [Name] is a 22-year-old male who presents after twisting his right ankle while playing recreational basketball approximately 2 hours ago. He describes an inversion mechanism when landing from a rebound. He felt immediate pain along the lateral aspect of the ankle, heard no pop, and was able to limp off the court. He has since iced and elevated. He reports difficulty bearing weight fully but can take a few steps. Denies numbness, tingling, or injury elsewhere. Ottawa ankle rule: bony tenderness along the distal fibula and inability to take 4 steps immediately after injury — X-ray indicated."
"Ms. [Name] is a 31-year-old otherwise healthy female presenting with 2 days of dysuria, urinary frequency, and mild suprapubic discomfort. She denies fever, chills, flank pain, nausea, vomiting, or vaginal discharge. Last menstrual period 2 weeks ago; sexually active with one male partner, uses condoms. No history of recurrent UTI, nephrolithiasis, or pyelonephritis. No known drug allergies. UA obtained today: 3+ LE, 2+ nitrite, moderate blood, trace protein. Urine hCG negative."
"Mr. [Name] is a 45-year-old male who developed an intensely pruritic, erythematous, vesicular rash on his bilateral forearms and anterior shins approximately 3 days after yard work, during which he cleared underbrush in his backyard without protective clothing. The rash is distributed in linear streaks. He has tried OTC hydrocortisone 1% cream and oral diphenhydramine without significant relief. He denies facial swelling, shortness of breath, fever, or spread to mucous membranes. No new medications, soaps, or detergents. PMH notable for seasonal allergies."
"Mr. [Name] is a 52-year-old male warehouse worker employed by [Company] who presents for evaluation of acute low back pain after lifting a 60-pound box from a low shelf at work this morning at approximately 0830. He reports immediate onset of sharp pain across the lower lumbar region, radiating mildly to the right buttock but not below the knee. He denies numbness, tingling, weakness, bowel or bladder changes, or saddle anesthesia. He has no prior back injury. He reported the injury to his supervisor immediately. He has not taken any medications. He is requesting evaluation and work status determination. WC claim being filed by employer."
Great urgent care scribes are fast, organized, and triage-aware. You will see 25–40 patients per shift across an enormous range of complaints — sore throats, sprains, rashes, UTIs, and the occasional genuine emergency hiding in plain sight. Your superpower is pattern recognition: after a few months you should be able to anticipate the plan for most complaints before the provider says a word, pre-populate the note with relevant ROS and exam templates, and know which POC tests the provider will order.
Be the person who notices the abnormal vital sign the triage tech missed. Be the person who remembers the patient had a penicillin allergy. Be the person who knows the Ottawa rules cold, so when the provider says "Ottawa negative, no X-ray needed," you chart it without asking. Learn each provider's documentation style, favorite templates, and return-precaution phrasing. Read at least one chart from yesterday's shift before today's starts.
Urgent care medicine is the front door of the healthcare system for millions of patients. Your documentation protects patients, providers, and the clinic itself. Welcome.
25 References & Sources
Clinical Practice Guidelines
Workowski KA et al. CDC Sexually Transmitted Infections Treatment Guidelines. MMWR Recomm Rep. 2021.
American College of Radiology Appropriateness Criteria (current edition).
Landmark Studies & Decision Rules
Diagram & Figure Sources
Figure 1: Urgent Care Waiting Room. Wikimedia Commons. Public domain / CC licensed.
Figure 2: Otoscope. Wikimedia Commons. CC licensed.
Figure 3: Splint Application. Wikimedia Commons. Public domain.
Figure 4: Surgeon's Knot. Wikimedia Commons. Public domain.