Urology
Every diagnosis, condition, procedure, medication, abbreviation, and documentation framework you need to succeed on day one and beyond.
All diagrams on this page are sourced from published educational or institutional materials rather than AI generation. Each figure caption links to the original source, and the full diagram and guideline citations are collected in the references section at the bottom.
01 The Genitourinary System — Anatomy Essentials
Urology covers the entire urinary tract in both sexes and the male reproductive system. That means kidneys, ureters, bladder, urethra, prostate, seminal vesicles, vas deferens, epididymis, testes, penis, and scrotum. Female reproductive organs belong to gynecology, but female urologists (often dual-trained in Female Pelvic Medicine & Reconstructive Surgery, FPMRS, now formally called Urogynecology & Reconstructive Pelvic Surgery) manage pelvic floor disorders, incontinence, and prolapse. The adrenal glands sit on top of the kidneys and historically belonged to urology; in most modern practices they are shared with endocrine surgery.
The Upper Urinary Tract
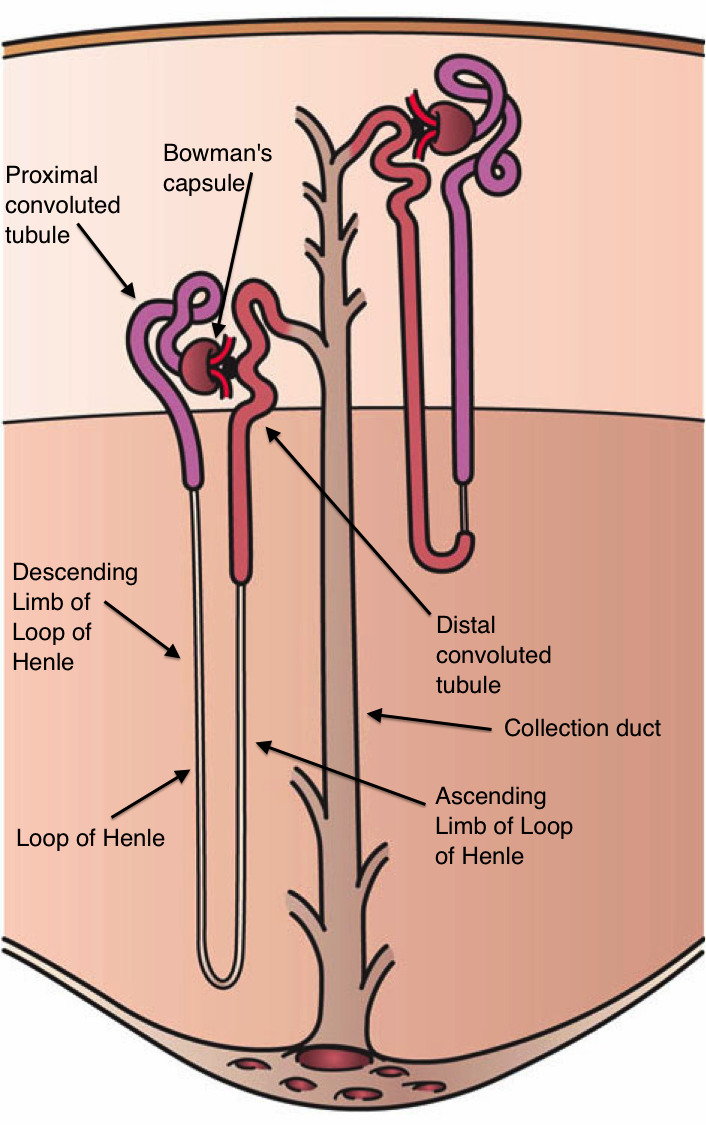
The kidneys are paired retroperitoneal organs located between T12 and L3. The right kidney sits slightly lower than the left because of the liver. Each kidney is surrounded by perirenal fat and Gerota's fascia. The renal parenchyma has two zones — the outer cortex (containing glomeruli) and the inner medulla (containing pyramids and loops of Henle) — draining into minor calyces, then major calyces, then the renal pelvis, and out through the ureter. The ureter is approximately 22–30 cm long and has three anatomic narrowings where stones classically lodge: the ureteropelvic junction (UPJ), the crossing of the iliac vessels, and the ureterovesical junction (UVJ).
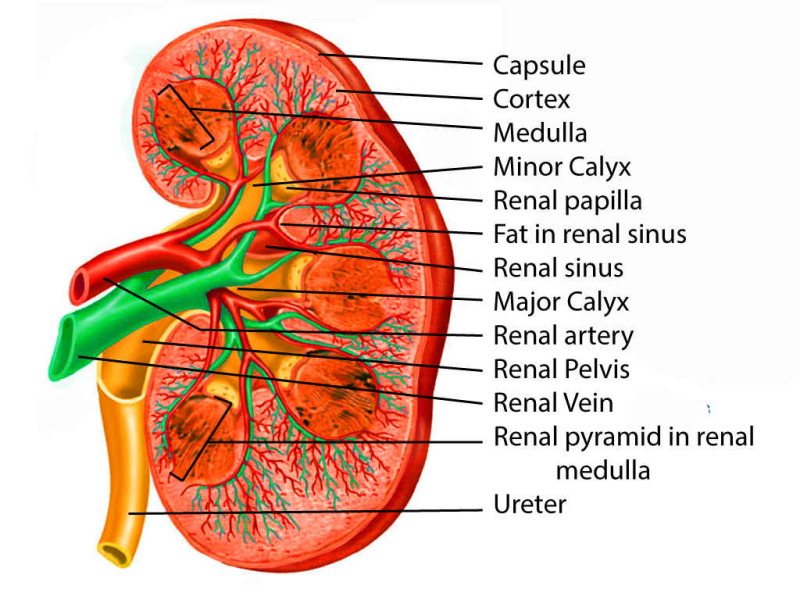
Each kidney is supplied by a single renal artery branching directly off the abdominal aorta, and drained by a renal vein into the IVC. The left renal vein is longer and crosses anterior to the aorta beneath the superior mesenteric artery — this is clinically important for "nutcracker syndrome" and for left-sided donor nephrectomies.
The Lower Urinary Tract
The bladder is a muscular reservoir in the pelvis behind the pubic symphysis. Its wall is composed of the detrusor muscle (smooth muscle under parasympathetic control via S2–S4). The trigone is the triangular area between the two ureteral orifices and the bladder neck. In men the bladder neck sits directly on top of the prostate; in women it sits above the anterior vaginal wall and pelvic floor.
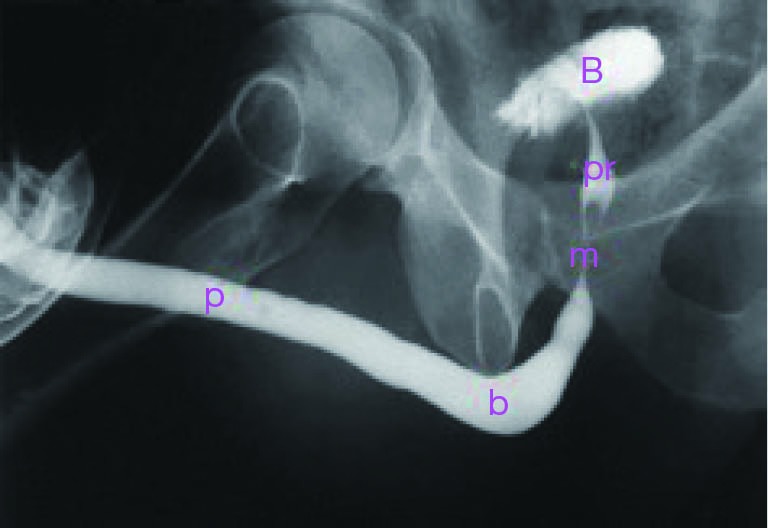
The urethra differs dramatically by sex. The female urethra is 3–4 cm long, mostly straight, and supported by the pelvic floor. The male urethra is approximately 18–22 cm long and divided into four segments: prostatic urethra (through the prostate), membranous urethra (through the urogenital diaphragm — this is where the external sphincter lives, the key structure for continence after prostatectomy), bulbar urethra (within the bulb of the penis, the most common site of traumatic stricture), and pendulous / penile urethra ending at the meatus.
The Prostate
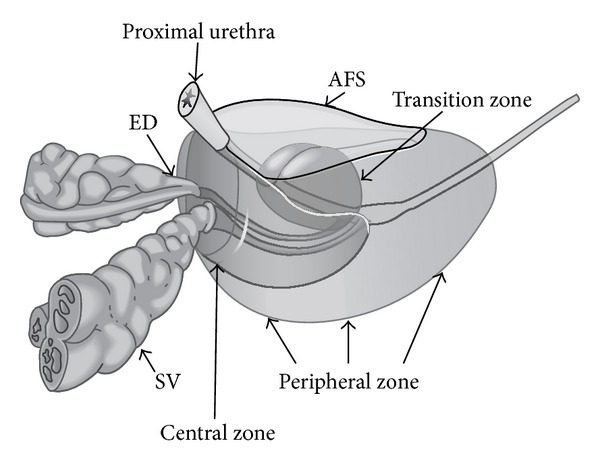
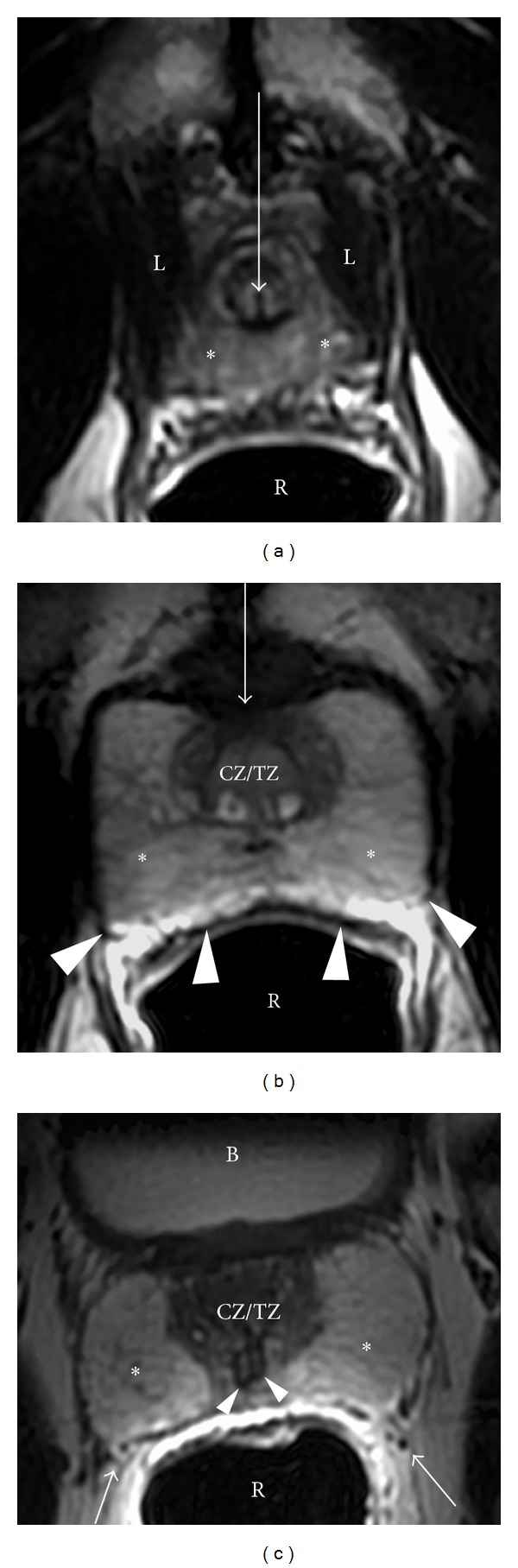
The prostate is a walnut-sized fibromuscular gland surrounding the prostatic urethra at the bladder neck. It has four zones: the peripheral zone (~70% of volume, posterior, site of ~70% of prostate cancers — felt on DRE), the central zone (~25%, surrounding the ejaculatory ducts), the transition zone (~5% in youth but enlarges with BPH — the site of BPH-related obstruction), and the anterior fibromuscular stroma. The prostate secretes prostate-specific antigen (PSA) and components of seminal fluid.
Scrotum & Male Reproductive Tract
Each testis sits within the scrotum, suspended by the spermatic cord which contains the vas deferens, testicular artery, pampiniform venous plexus, lymphatics, and the genital branch of the genitofemoral nerve. Sperm produced in the seminiferous tubules drain into the epididymis (head, body, tail along the posterolateral testis), then into the vas deferens, which ascends through the inguinal canal, crosses the ureter, joins the seminal vesicle duct to form the ejaculatory duct, and empties into the prostatic urethra. Testicular lymphatic drainage is to the retroperitoneum (para-aortic/interaortocaval nodes) — crucial for testicular cancer staging.
Memorize the three ureteral narrowings (UPJ, iliac crossing, UVJ) and the four segments of the male urethra. When the urologist says "stone impacted at the iliac crossing" or "bulbar urethral stricture after prior catheter trauma," you need to know exactly where that is and chart it without asking.
02 Scribe Documentation Framework
The Urology Visit
Urology visits cluster around a handful of chief complaints: LUTS/BPH, hematuria, cancer follow-up, stones, incontinence, ED, scrotal problems, and UTIs. Notes are SOAP-formatted, but the urologic HPI has specific elements that must be captured every time depending on the complaint.
Chief Complaint (CC): "Blood in urine," "cannot empty bladder," "rising PSA," "left flank pain," "leaking with cough," "scrotal swelling."
HPI: Use OLDCARTS plus the urology-specific checklists below. For any LUTS visit you must capture frequency, nocturia count, urgency, hesitancy, weak stream, intermittency, straining, incomplete emptying, and post-void dribbling. For hematuria, capture gross vs microscopic, clots, timing within the stream (initial = urethra, terminal = bladder neck, total = bladder/upper tract), and any associated pain. For stone pain: location of flank pain, radiation to groin/testicle/labia, associated nausea/vomiting, fevers, prior stones. For incontinence: stress (cough/laugh/exercise), urge (with a strong uncontrollable desire), mixed, continuous leakage, pad count per day.
ROS: Focused. Capture constitutional (fevers, weight loss, night sweats — important for cancer), GU (all LUTS elements), GI (constipation affects LUTS and pelvic floor), and MSK (back pain — can mimic flank pain).
PMH/PSH/Meds/SHx/FHx: Always capture prior urologic surgery or instrumentation, prior stones, prior UTIs, catheter history, current anticoagulants (critical before any procedure), smoking (bladder cancer risk), occupational exposures (aromatic amines in dye/rubber industries — bladder cancer), family history of prostate/kidney/bladder cancer, and for males, erectile and ejaculatory function baseline.
Vitals: BP, HR, temperature (key for pyelonephritis, urosepsis, prostatitis, Fournier).
Urologic Exam: Abdominal exam for flank tenderness (CVA tenderness), palpable bladder (distended > 300–400 mL), suprapubic tenderness. Genital exam for males: circumcised vs uncircumcised, meatus position/patency, penile lesions or plaques (Peyronie), testicular size/lie/tenderness, cord/epididymis, cremasteric reflex, hernia evaluation, transillumination for hydrocele. Digital rectal exam (DRE): prostate size (estimated in grams), consistency (smooth, firm, rubbery, nodular, boggy), symmetry, tenderness, and sphincter tone. For females: external genital exam, vaginal exam with speculum and bimanual when indicated, assessment for atrophy, prolapse (POP-Q), and cough stress test.
Data: Urinalysis (UA) and urine culture results, PSA with trajectory, BMP/creatinine, post-void residual (PVR) by bladder scanner, uroflowmetry (Qmax in mL/s and voided volume), imaging findings.
Each problem is listed separately with ICD-10 if available. Plans commonly include medication changes (start tamsulosin, add finasteride, switch to mirabegron), procedures (schedule cystoscopy, TRUS-guided prostate biopsy, URS with stent), imaging (CT urogram, MRI prostate, renal ultrasound), lab follow-up (repeat PSA in 6 weeks, surveillance UA), referrals (radiation oncology for prostate cancer, medical oncology for metastatic disease), and disposition (return to clinic in X weeks/months).
The International Prostate Symptom Score (IPSS) is not optional for BPH/LUTS visits — it is the standard outcome measure. You will enter the 0–35 score in almost every note for an older male with urinary complaints. Learn the seven questions (incomplete emptying, frequency, intermittency, urgency, weak stream, straining, nocturia) and the QoL question separately.
03 Prostate Cancer Oncology
Prostate cancer is the most common non-skin cancer in men and the second leading cause of male cancer death in the US. The vast majority are adenocarcinomas arising in the peripheral zone. Most are indolent; a minority are aggressive and metastasize to regional lymph nodes and bone. The scribe will see prostate cancer across the entire spectrum — from PSA-based screening and active surveillance, through localized treatment (surgery, radiation), to advanced disease (ADT, chemotherapy, androgen-axis inhibitors, radioligand therapy).
Screening & Diagnosis
Screening with PSA is shared decision-making. The USPSTF 2018 prostate cancer screening recommendation endorses individualized shared decision-making about PSA testing in men aged 55–69 (grade C) and recommends against routine screening after age 70 (grade D). The AUA early detection of prostate cancer guideline provides the specific PSA thresholds and retesting intervals. A PSA above age-specific reference (often >4 ng/mL) or an abnormal DRE triggers further workup: repeat PSA, free/total PSA ratio, PSA density, PHI or 4Kscore, and multiparametric MRI of the prostate (reported on PI-RADS 1–5). PI-RADS 3 is equivocal, 4 and 5 trigger targeted biopsy.
Biopsy is typically TRUS-guided (transrectal ultrasound) with 12–14 systematic cores, increasingly combined with MRI fusion targeting of suspicious lesions. Transperineal biopsy is gaining favor for lower infection rates. Pathology is reported with Gleason scoring: two numbers (primary + secondary pattern, each 3–5) summing to the Gleason score (e.g., 3+4=7). The ISUP/Grade Group system translates this into 1–5.
| Grade Group | Gleason Score | Clinical Meaning |
|---|---|---|
| 1 | ≤ 6 (3+3) | Low risk; candidate for active surveillance |
| 2 | 7 (3+4) | Favorable intermediate risk |
| 3 | 7 (4+3) | Unfavorable intermediate risk |
| 4 | 8 (4+4, 3+5, 5+3) | High risk |
| 5 | 9–10 (4+5, 5+4, 5+5) | Very high risk |
AUA Risk Stratification for Localized Disease
| Group | PSA | Grade Group | Stage |
|---|---|---|---|
| Very Low | < 10 | 1 | T1c, < 3 cores, < 50% per core, PSA density < 0.15 |
| Low | < 10 | 1 | T1–T2a |
| Intermediate (favorable) | 10–20 | 2 | T2b–T2c, single intermediate factor, < 50% cores positive |
| Intermediate (unfavorable) | 10–20 | 3 | Multiple intermediate factors or GG3 |
| High | > 20 | 4 | T3a |
| Very High | any | 5 | T3b–T4, primary pattern 5, > 4 cores GG4–5 |
TNM Staging (Simplified)
T1: clinically inapparent (T1c = PSA-detected). T2: palpable, confined to prostate (a = ≤½ of one lobe, b = >½ of one lobe, c = both lobes). T3: extraprostatic extension (a = EPE, b = seminal vesicle invasion). T4: invades adjacent structures (bladder neck, rectum, pelvic wall). N1: regional pelvic lymph nodes. M1a: non-regional nodes. M1b: bone. M1c: other sites.
Management
Active surveillance is the standard for very low and low risk disease: serial PSA, DRE, MRI, and confirmatory biopsy. Localized treatment for intermediate and high risk includes radical prostatectomy (open, laparoscopic, or robotic-assisted — RALP is now dominant in the US) or radiation therapy (external beam, brachytherapy, or SBRT). High-risk patients often get combined therapy (RT + ADT for 18–36 months). Advanced disease is treated with androgen deprivation therapy (ADT) using GnRH agonists (leuprolide, goserelin) or antagonists (degarelix, relugolix), combined early with androgen axis inhibitors (abiraterone, enzalutamide, apalutamide, darolutamide) for metastatic hormone-sensitive disease per landmark trials (LATITUDE, CHAARTED, TITAN, ARCHES). mCRPC (metastatic castration-resistant prostate cancer) is defined by disease progression despite castrate testosterone (< 50 ng/dL). Treatment escalation options include docetaxel, cabazitaxel, radium-223 (bone-only disease), Lu-177 PSMA radioligand therapy, and PARP inhibitors (olaparib, rucaparib) in BRCA/HRR-mutated disease.
When the attending dictates, "PSA 8.4, Grade Group 3, T2c, MRI showed extracapsular extension, intermediate unfavorable risk," you need to chart every one of those phrases. Miss the Grade Group and the oncology referral will bounce back.
04 Benign Prostatic Hyperplasia & LUTS Benign
BPH is the non-cancerous enlargement of the prostatic transition zone. It is nearly universal in aging men — histologic BPH is present in > 80% of men by age 80. BPH causes lower urinary tract symptoms (LUTS) by compressing the prostatic urethra and by altering bladder function over time (detrusor hypertrophy, reduced compliance, overactivity). Not all LUTS are BPH — the differential includes overactive bladder, UTI, bladder stone, bladder cancer, urethral stricture, neurogenic bladder, and medications.
Symptoms & IPSS
LUTS are divided into storage symptoms (frequency, nocturia, urgency, urge incontinence) and voiding symptoms (hesitancy, weak stream, intermittency, straining, incomplete emptying, terminal dribbling). The International Prostate Symptom Score (IPSS) scores seven questions 0–5 for a total of 0–35, plus a separate QoL question 0–6.
| Score | Severity |
|---|---|
| 0–7 | Mild |
| 8–19 | Moderate |
| 20–35 | Severe |
Workup
Workup includes UA to rule out infection/hematuria, PSA to risk-stratify for cancer and estimate prostate volume, creatinine, post-void residual (PVR) by ultrasound (significant if > 100–150 mL), and uroflowmetry (Qmax < 10 mL/s suggests obstruction). Cystoscopy and urodynamics are reserved for complex cases, prior to invasive intervention, or when neurogenic etiology is suspected.
Management
The AUA BPH/LUTS guideline is the authoritative source. Behavioral modifications (fluid timing, avoiding caffeine/alcohol/late fluids, double voiding) are first-line. Medical therapy is the workhorse: alpha blockers (tamsulosin 0.4 mg qHS, alfuzosin 10 mg daily, silodosin 8 mg daily, doxazosin, terazosin) relax prostatic smooth muscle and provide symptomatic relief within days. 5-alpha-reductase inhibitors (finasteride 5 mg daily, dutasteride 0.5 mg daily) shrink the prostate by 20–25% over 6–12 months and are reserved for prostates > 30–40 g; they reduce PSA by ~50% (double the measured value to interpret). Combination therapy (alpha blocker + 5-ARI) outperforms monotherapy in larger prostates per the MTOPS and CombAT trials. Anticholinergics or beta-3 agonists (mirabegron, vibegron) can be added for predominant storage symptoms. PDE5 inhibitors (tadalafil 5 mg daily) treat both LUTS and ED.
Procedural options include TURP (transurethral resection of the prostate — the historical gold standard for prostates 30–80 g), simple prostatectomy (open or robotic, for very large > 80–100 g glands), photoselective vaporization (GreenLight laser), holmium laser enucleation (HoLEP — increasingly preferred for large glands), thulium enucleation, prostatic urethral lift (UroLift), water vapor thermal therapy (Rezūm), Aquablation, and prostate artery embolization.
Acute urinary retention, recurrent UTI, bladder stones, bladder decompensation, hydronephrosis, and obstructive renal failure. AUR triggered by anticholinergic or sympathomimetic medications is extremely common — you will document this history often.
05 Prostatitis & Chronic Pelvic Pain Inflammatory
The NIH classification of prostatitis has four categories: Category I — acute bacterial prostatitis (acute febrile illness with dysuria and perineal pain, boggy tender prostate on DRE — vigorous DRE contraindicated due to bacteremia risk; treat with fluoroquinolone or TMP-SMX for 2–4 weeks); Category II — chronic bacterial prostatitis (recurrent UTIs from a prostatic reservoir, cultures positive; treat with prolonged fluoroquinolone, often 4–6 weeks); Category III — chronic prostatitis / chronic pelvic pain syndrome (CP/CPPS), subdivided into IIIA (inflammatory, WBCs in expressed prostatic secretions) and IIIB (non-inflammatory) — by far the most common; multimodal treatment using alpha blockers, anti-inflammatories, pelvic floor physical therapy, neuromodulators, and antibiotics if any evidence of infection (UPOINT phenotype system); Category IV — asymptomatic inflammatory prostatitis, found incidentally on biopsy or semen analysis.
Failure of acute prostatitis to improve after 48–72 hours of appropriate antibiotics should raise suspicion for prostatic abscess. Diagnosed by transrectal ultrasound or CT. Treated with transurethral or transrectal drainage plus continued antibiotics. Chart fever curves, WBC trajectory, and response to therapy meticulously.
06 Kidney Cancer (RCC & Upper Tract) Oncology
Renal cell carcinoma (RCC) is the most common primary kidney cancer in adults. Clear cell RCC is the most common subtype (~75%), followed by papillary (types 1 and 2) and chromophobe. RCC classically presents incidentally on imaging obtained for another indication — the historical triad of flank pain, hematuria, and palpable mass is now rare. Paraneoplastic syndromes (hypercalcemia, polycythemia, hypertension, Stauffer syndrome of hepatic dysfunction) should be documented when present. Upper tract urothelial carcinoma (UTUC) arising from the renal pelvis or ureter is much less common but behaves like bladder cancer and is managed differently.

Bosniak Renal Cyst Classification
| Class | Description | Malignancy Risk | Management |
|---|---|---|---|
| I | Simple cyst, thin wall, no septations or calcifications | ~0% | No follow-up |
| II | Minimally complex: few thin septa, fine calcifications, hyperdense < 3 cm | < 5% | No follow-up |
| IIF | Minimally complex needing follow-up: multiple thin septa, nodular calcifications | ~5–10% | Imaging surveillance |
| III | Indeterminate: thickened walls, enhancing septa | ~50% | Surgical excision or ablation |
| IV | Clearly malignant features: enhancing solid component | > 90% | Surgical excision |
TNM & Management
T1a ≤ 4 cm, T1b > 4 ≤ 7 cm, T2 > 7 cm, T3a perinephric fat or renal vein, T3b IVC below diaphragm, T3c IVC above diaphragm, T4 beyond Gerota. Partial nephrectomy is preferred for cT1 masses when feasible (open, laparoscopic, or robotic). Radical nephrectomy is reserved for larger or anatomically unfavorable tumors.
UTUC is usually managed with radical nephroureterectomy (including bladder cuff excision). Low-grade, small, papillary lesions may be managed endoscopically (ureteroscopic ablation) and with intracavitary mitomycin reverse thermal gel.
07 Bladder Cancer (NMIBC & MIBC) Oncology
The overwhelming majority of bladder cancers are urothelial (transitional cell) carcinomas. Squamous cell (associated with chronic inflammation, schistosomiasis) and adenocarcinoma (urachal remnant) are uncommon. The dominant risk factor is smoking — document pack-years on every bladder cancer patient. Occupational aromatic amine exposure (rubber, dye, leather, hairdressers) is a classic secondary risk factor. Most patients present with painless gross hematuria.
NMIBC vs MIBC
The critical divide is whether the tumor invades the muscularis propria (detrusor). Non-muscle-invasive bladder cancer (NMIBC) — Tis (carcinoma in situ), Ta (non-invasive papillary), T1 (invades lamina propria but not muscle) — is treated with transurethral resection (TURBT) plus intravesical therapy and surveillance. Muscle-invasive bladder cancer (MIBC) — T2 and above — requires radical cystectomy with urinary diversion (or trimodal therapy: maximal TURBT + chemoradiation).
| Risk | Features | Therapy |
|---|---|---|
| Low | Solitary LG Ta ≤ 3 cm, PUNLMP | TURBT ± single post-op intravesical chemo (mitomycin or gemcitabine) |
| Intermediate | Recurrent LG Ta, solitary LG Ta > 3 cm, multifocal LG Ta, solitary HG Ta ≤ 3 cm | TURBT + induction intravesical BCG or chemo, maintenance considered |
| High | HG T1, any CIS, HG Ta > 3 cm or multifocal, BCG failure | TURBT + re-TURBT + induction/maintenance BCG × 3 years; consider cystectomy |
The AUA/SUO NMIBC guideline and the AUA/ASCO/ASTRO/SUO MIBC guideline cover treatment algorithms. For MIBC, neoadjuvant cisplatin-based chemotherapy (ddMVAC or gemcitabine/cisplatin) before radical cystectomy improves survival. Radical cystectomy in men includes cystoprostatectomy; in women includes anterior pelvic exenteration. Urinary diversion options include ileal conduit (incontinent, most common), continent cutaneous diversion (Indiana pouch), and orthotopic neobladder (continent, requires intact urethra and patient able to self-catheterize).
08 Testicular & Penile Cancer Oncology
Testicular Cancer
Testicular cancer is the most common solid malignancy in men aged 15–35 and one of the most curable. Germ cell tumors account for > 95% and are divided into seminoma and non-seminomatous germ cell tumors (NSGCT — embryonal, yolk sac, choriocarcinoma, teratoma, or mixed). Classic presentation: painless testicular mass noticed incidentally. Risk factors include cryptorchidism, family history, and prior testicular cancer.
Workup: scrotal ultrasound (the single most important test), tumor markers (AFP, beta-hCG, LDH) drawn before orchiectomy, and staging CT chest/abdomen/pelvis after pathology confirms malignancy. AFP is elevated in NSGCT (never pure seminoma); beta-hCG may be elevated in either; LDH reflects tumor burden. Never biopsy the testis transscrotally — the definitive procedure is radical inguinal orchiectomy via an inguinal incision with high ligation of the cord. Stage I disease may be managed with surveillance, adjuvant carboplatin (seminoma) or BEP chemotherapy, or RPLND (NSGCT). Metastatic disease is treated with BEP (bleomycin, etoposide, cisplatin) × 3–4 cycles with retroperitoneal lymph node dissection for residual masses.
Penile Cancer
Rare in developed countries; associated with HPV, phimosis, lack of circumcision, smoking, and poor hygiene. Most are squamous cell carcinomas on the glans or foreskin. Workup includes biopsy and inguinal node exam (with sentinel node biopsy or dynamic lymphoscintigraphy for high-risk lesions). Organ-sparing approaches (topical 5-FU, imiquimod, laser, glansectomy) are preferred for early disease; partial or total penectomy for larger tumors; bilateral inguinal lymphadenectomy for node-positive disease.
09 Nephrolithiasis (Kidney Stones) Stones
Kidney stones are among the most common urologic emergencies and clinic visits. Lifetime prevalence approaches 10%. Recurrence rates are high (50% within 5–10 years), so medical prevention is as important as acute management.
Stone Composition
| Type | % of Stones | Key Features | Prevention |
|---|---|---|---|
| Calcium oxalate | ~70–80% | Radiopaque, envelope or dumbbell crystals; associated with hypercalciuria, hyperoxaluria, hypocitraturia | Fluids, low sodium, normal calcium, thiazide, potassium citrate |
| Calcium phosphate | ~10% | Radiopaque; associated with alkaline urine, RTA, primary hyperparathyroidism | Correct underlying cause, thiazide, citrate |
| Uric acid | ~10% | Radiolucent on plain film (visible on CT); acidic urine pH < 5.5; gout, obesity, diabetes | Alkalinize urine with potassium citrate, allopurinol |
| Struvite (MgNH₄PO₄) | ~5% | "Infection stone" from urease-producing organisms (Proteus, Klebsiella); often staghorn | Complete stone removal (PCNL), culture-directed antibiotics |
| Cystine | < 1% | Autosomal recessive cystinuria; hexagonal crystals; recurrent large stones from childhood | High fluids, alkalinization, tiopronin, captopril |
Presentation & Workup
The classic presentation is sudden-onset severe flank pain (renal colic) radiating to the groin, testicle, or labia majora, often with nausea, vomiting, and microscopic or gross hematuria. The patient is typically writhing and cannot find a comfortable position (distinguishing from peritonitis where patients lie still). Fever + obstruction = infected obstructed kidney = emergency decompression (ureteral stent or percutaneous nephrostomy) plus antibiotics.
Workup includes UA (microhematuria in ~85%), urine culture, BMP, CBC, and non-contrast CT of the abdomen and pelvis ("stone protocol") — the gold standard. Report stone size (mm), location, laterality, density in Hounsfield units (HU > 1000 suggests calcium oxalate monohydrate and poor response to SWL), and presence/degree of hydronephrosis. Ultrasound is an alternative in pregnancy and for reducing radiation.
Management
The AUA surgical management of stones guideline provides size and location thresholds. Stones < 5 mm have a ~70% chance of spontaneous passage; 5–10 mm roughly 50%. Medical expulsive therapy (MET) with tamsulosin 0.4 mg daily is appropriate for distal ureteral stones ≤ 10 mm in hemodynamically stable, afebrile patients. Intervention is required for obstructing infection, intractable pain, AKI, solitary kidney, or failure to pass. Options include ureteroscopy (URS) with laser lithotripsy (preferred for mid/distal stones, stones up to ~2 cm), shock wave lithotripsy (SWL) (non-invasive, for proximal stones < 2 cm, lower density), and percutaneous nephrolithotomy (PCNL) (stones > 2 cm, staghorn, lower pole stones with poor drainage). The AUA medical management of kidney stones guideline covers recurrence prevention including 24-hour urine collection, dietary counseling, and pharmacotherapy.
When the attending says "4 mm distal ureteral stone with mild hydro, afebrile, normal creatinine, good pain control," you chart "trial of passage with tamsulosin, strain urine, return for fever or worsening pain." When they say "8 mm proximal ureteral stone with febrile UTI," you chart "urgent decompression with ureteral stent vs PCN, IV antibiotics, admission."
10 Hematuria Evaluation Symptom
Hematuria is blood in the urine. It is divided into gross hematuria (visible) and microscopic hematuria (≥ 3 RBC/HPF on microscopic UA in the absence of obvious benign cause). Gross hematuria in an adult is bladder cancer until proven otherwise. Microscopic hematuria requires risk-stratified workup.
| Risk | Criteria | Workup |
|---|---|---|
| Low | Women < 50 / men < 40, never smoker, 3–10 RBC/HPF, no risk factors | Shared decision: repeat UA in 6 months OR cystoscopy + renal US |
| Intermediate | Women 50–59 / men 40–59, < 30 pack-years, 11–25 RBC/HPF | Cystoscopy + renal US |
| High | Women ≥ 60 / men ≥ 60, > 30 pack-years, > 25 RBC/HPF, gross hematuria history | Cystoscopy + CT urogram (or MR urogram if contrast contraindicated) |
The AUA microhematuria guideline is the reference. Glomerular causes (IgA nephropathy, thin basement membrane, Alport, post-infectious GN) are suggested by red cell casts, dysmorphic RBCs, and proteinuria — these patients go to nephrology, not cystoscopy.
11 Urinary Tract Infection & Pyelonephritis Infection
Urinary tract infections range from uncomplicated cystitis in healthy women to life-threatening urosepsis. Classification drives management:
Uncomplicated: healthy non-pregnant premenopausal woman, normal GU tract. Complicated: any UTI in a man, pregnant woman, patient with structural/functional GU abnormality, catheter, immunosuppression, or diabetes with complications. Recurrent: ≥ 2 culture-proven UTIs in 6 months or ≥ 3 in 12 months. Pyelonephritis: upper tract infection with fever, flank pain, CVA tenderness, often nausea/vomiting. Urosepsis: sepsis from a urinary source — SIRS/qSOFA criteria, hemodynamic instability, elevated lactate. Perinephric abscess: pyelonephritis that fails to improve after 48–72 hours — image with CT.
The AUA recurrent uncomplicated UTI guideline covers workup and prevention in women. First-line antibiotics for acute uncomplicated cystitis are nitrofurantoin 100 mg BID × 5 days, TMP-SMX DS BID × 3 days (if local resistance < 20%), or fosfomycin 3 g single dose. Pyelonephritis is treated with fluoroquinolones (ciprofloxacin, levofloxacin) or an IV beta-lactam if the patient is ill. Recurrent UTI prevention options include vaginal estrogen in postmenopausal women, cranberry products (limited evidence), methenamine hippurate, and antibiotic prophylaxis (low-dose nightly or postcoital).
12 Scrotal Pain & Testicular Emergencies Emergency
Twisting of the spermatic cord cuts off blood supply to the testis. Peak incidence in adolescents. Presents with sudden severe unilateral scrotal pain, often with nausea/vomiting, high-riding testis with a horizontal lie (bell-clapper deformity), absent cremasteric reflex, and a normal UA. Doppler ultrasound shows absent intratesticular flow. Treat with emergent scrotal exploration and detorsion with bilateral orchiopexy. Testicular salvage is > 90% within 6 hours of pain onset, drops to < 10% after 24 hours. If in doubt, explore.
Epididymitis presents with more gradual onset of scrotal pain, often with dysuria and urethral discharge (in sexually active men < 35, treat for chlamydia and gonorrhea with ceftriaxone + doxycycline; in men > 35, treat for coliforms with fluoroquinolone). Positive Prehn sign (pain relief with scrotal elevation) and preserved cremasteric reflex distinguish from torsion but are unreliable — ultrasound is required.
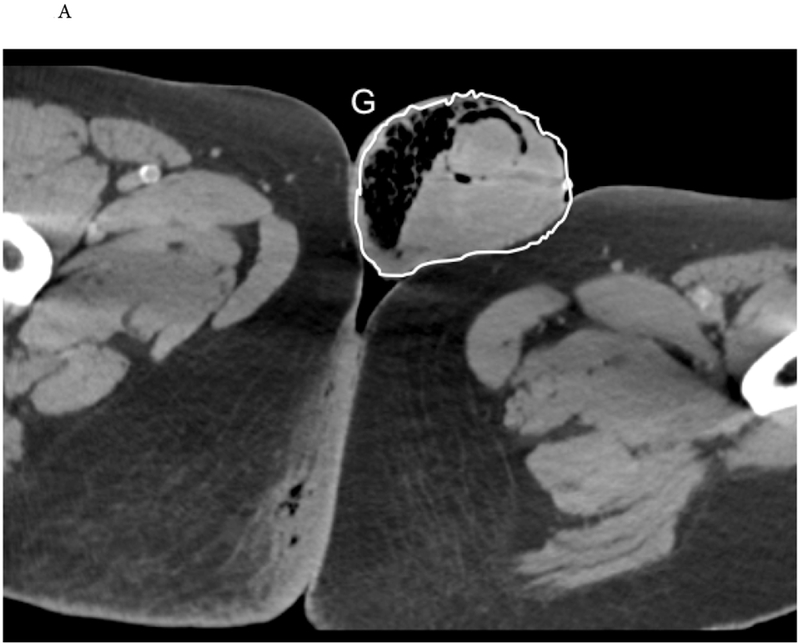
Necrotizing fasciitis of the perineum and genitals. Polymicrobial. Risk factors: diabetes, immunosuppression, obesity, alcoholism. Presents with severe pain out of proportion to findings, systemic toxicity, crepitus, skin necrosis. Surgical emergency — aggressive debridement, broad-spectrum antibiotics, ICU care. Mortality 20–40%.
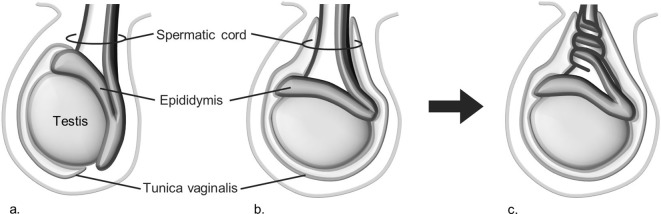
Paraphimosis (retracted foreskin that cannot be reduced, causing glans edema) and priapism (painful erection lasting > 4 hours; ischemic is a compartment syndrome of the corpus cavernosum requiring urgent aspiration, irrigation, phenylephrine injection, and possibly shunt) are additional emergencies. Hydrocele (fluid around the testis, transilluminates), varicocele ("bag of worms," left-sided 90%, worse with Valsalva — new right-sided raises concern for IVC/renal vein compression), and spermatocele (epididymal head cyst) are common non-emergent findings.
13 Male Sexual Health (ED, Peyronie, Hypogonadism, Infertility) Andrology
Erectile dysfunction (ED) is the consistent inability to achieve or maintain an erection adequate for satisfactory sexual activity. Etiology is overwhelmingly vascular (endothelial dysfunction shares risk factors with CAD — ED is often a sentinel for future cardiovascular events). Workup: history, SHIM/IIEF score, morning testosterone, fasting glucose/HbA1c, lipids, TSH, prolactin. First-line therapy: lifestyle, cardiovascular risk factor modification, and PDE5 inhibitors (sildenafil, tadalafil, vardenafil, avanafil). Second-line: intracavernosal or intraurethral alprostadil, vacuum erection devices. Third-line: penile prosthesis (inflatable or malleable). The AUA ED guideline is the reference.
Peyronie disease is a fibrotic plaque of the tunica albuginea causing penile curvature, painful erections, and shortening. Acute (inflammatory, painful) and chronic (stable, painless) phases. Treatment includes intralesional collagenase (Xiaflex), verapamil, mechanical therapy, and surgery (plaque incision/grafting, plication, or prosthesis for severe ED with curvature).
Hypogonadism (low testosterone) is classified as primary (testicular failure — high LH/FSH) or secondary (HPT axis — low/normal LH/FSH). Diagnosis requires two morning total testosterone levels < 300 ng/dL plus symptoms. Per the AUA testosterone deficiency guideline, testosterone replacement (gel, patch, IM injection, pellets, oral, nasal) is indicated for symptomatic hypogonadism after counseling on cardiovascular, fertility, polycythemia, and prostate risks. PSA, hematocrit, and testosterone are monitored on therapy.
Male infertility evaluation includes history, exam, and two semen analyses (volume, concentration, motility, morphology per WHO criteria). Additional workup: hormone panel (testosterone, LH, FSH, prolactin), scrotal ultrasound, karyotype and Y-chromosome microdeletion for severe oligospermia, CFTR gene testing for CBAVD. Causes include varicocele, hypogonadism, obstructive (vasectomy, CBAVD), non-obstructive azoospermia, and idiopathic. Treatment includes varicocelectomy, clomiphene/hCG, surgical sperm retrieval (TESE, microTESE, PESA, MESA) with IVF/ICSI.
Vasectomy is the most common urologic procedure — outpatient, usually under local anesthesia, with no-scalpel technique preferred. Semen analysis at ~12 weeks confirms azoospermia before considering the patient sterile. Vasovasostomy (microsurgical reversal) is an option for patients desiring fertility restoration.
14 Urinary Incontinence & Female Urology Pelvic Floor
Stress (SUI): involuntary leakage with effort, cough, sneeze, or exercise — due to urethral hypermobility or intrinsic sphincter deficiency. Urgency (UUI): involuntary leakage accompanied by a sudden compelling desire to void — a component of overactive bladder (OAB). Mixed: both stress and urgency components. Overflow: leakage from a chronically full bladder (retention). Continuous: ongoing leakage — think fistula (vesicovaginal, ureterovaginal), ectopic ureter.
Stress Incontinence
First-line treatment is behavioral: weight loss, pelvic floor muscle training (Kegels), pessary. No FDA-approved pharmacologic therapy in the US (imipramine and duloxetine are used off-label). Surgical options per the AUA/SUFU stress urinary incontinence guideline include midurethral sling (retropubic or transobturator), autologous fascial pubovaginal sling, Burch colposuspension, and urethral bulking agents. Male stress incontinence (usually post-prostatectomy) is treated with male sling or artificial urinary sphincter (AUS).
Overactive Bladder & Urge Incontinence
Per the AUA/SUFU OAB guideline, first-line is behavioral (bladder training, fluid management, caffeine avoidance, Kegels). Second-line is pharmacotherapy: anticholinergics (oxybutynin, tolterodine, solifenacin, darifenacin, fesoterodine, trospium) — beware anticholinergic burden in elderly; or beta-3 agonists (mirabegron, vibegron) — better tolerated, watch BP. Third-line includes intradetrusor onabotulinumtoxinA (Botox) 100 units (risk of retention — must be willing to self-catheterize), sacral neuromodulation (InterStim), and percutaneous tibial nerve stimulation (PTNS).
Pelvic Organ Prolapse
Anterior wall (cystocele), posterior wall (rectocele), apical (uterine or vault), and enterocele. Staged by POP-Q (Pelvic Organ Prolapse Quantification). Treated with observation, pessary, or surgery (sacrocolpopexy, sacrospinous ligament fixation, uterosacral ligament suspension, colporrhaphy).
Interstitial Cystitis / Bladder Pain Syndrome
Chronic bladder pain with urgency and frequency in the absence of identifiable cause. Diagnosis of exclusion. Management is stepwise: diet modification, stress reduction, pelvic floor PT, amitriptyline, hydroxyzine, pentosan polysulfate (Elmiron — retinal toxicity concern), intravesical DMSO, hydrodistention, and as a last resort cystectomy with diversion.
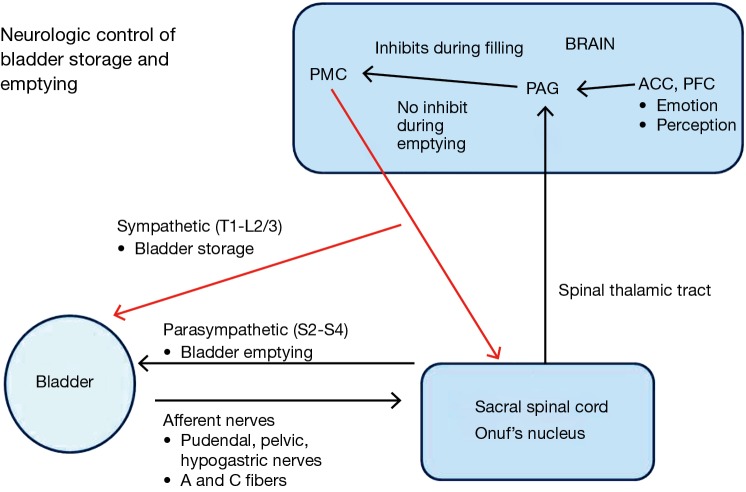
15 Neurogenic Bladder & Urinary Retention Functional
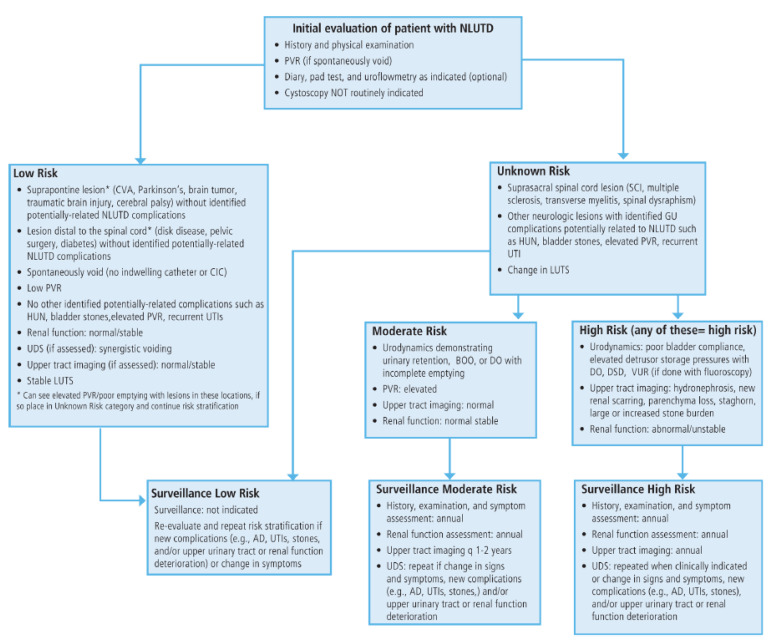
Neurogenic bladder is any bladder dysfunction caused by nervous system injury: spinal cord injury, multiple sclerosis, Parkinson disease, stroke, diabetic neuropathy, spina bifida. Manifestations include detrusor overactivity, detrusor-sphincter dyssynergia (DSD), areflexic bladder, and poor compliance with upper tract deterioration. Urodynamics (filling and voiding cystometry with pressure-flow) is the foundational diagnostic. Management protects the upper tracts: clean intermittent catheterization (CIC), anticholinergics/beta-3 agonists, botox, bladder augmentation, continent catheterizable channels (Mitrofanoff), or diversion.
Acute urinary retention (AUR) presents with the inability to void and a painful distended bladder. Initial management is Foley catheter placement — if difficult (BPH, stricture, false passage), escalate to coudé catheter, flexible cystoscopy with guidewire placement, filiform and followers, or suprapubic cystostomy. Large-volume decompression is generally safe; gross hematuria after decompression may occur but rarely requires intervention. Chronic urinary retention is managed with CIC or indwelling catheter until definitive therapy.
16 Obstructive Uropathy, Strictures & Hydronephrosis Obstruction
Hydronephrosis is dilation of the renal collecting system, usually from obstruction but also from reflux or congenital anomaly. Graded on ultrasound:
| Grade | Findings |
|---|---|
| 0 | No dilation |
| 1 | Mild dilation of renal pelvis only |
| 2 | Moderate pelvis dilation with a few calyces visible |
| 3 | All calyces uniformly dilated; normal parenchyma |
| 4 | Marked caliectasis with parenchymal thinning |
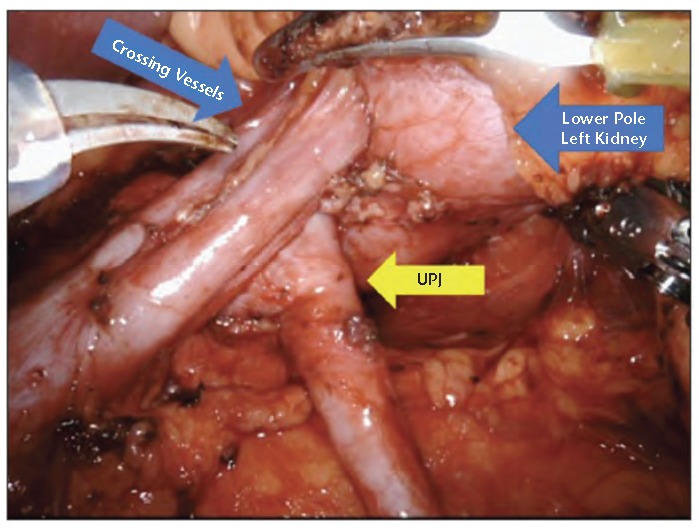
Ureteropelvic junction (UPJ) obstruction is congenital or acquired narrowing at the pelvis-ureter junction causing functional obstruction, often diagnosed antenatally or in young adults with flank pain. Managed with pyeloplasty (open, laparoscopic, robotic — Anderson-Hynes dismembered technique). Ureteral strictures are from prior surgery, stones, radiation, or idiopathic. Management: endoscopic (balloon dilation, endoureterotomy), open reconstruction (ureteroureterostomy, ureteral reimplant, Boari flap, psoas hitch, ileal ureter replacement). Urethral stricture in men is most commonly at the bulbar urethra from trauma, infection, or catheter injury. Management: direct visual internal urethrotomy (DVIU), dilation (temporizing), or definitive urethroplasty (excision with primary anastomosis, buccal mucosa graft urethroplasty).
17 Pediatric Urology Pediatric
Vesicoureteral reflux (VUR) is retrograde flow of urine from bladder to ureter/kidney, predisposing to pyelonephritis and renal scarring. Diagnosed by voiding cystourethrogram (VCUG). Graded I–V:
| Grade | Findings |
|---|---|
| I | Reflux into non-dilated ureter |
| II | Reflux into pelvis and calyces without dilation |
| III | Mild to moderate ureteral and pelvic dilation, minimal blunting of calyces |
| IV | Moderate ureteral tortuosity, blunted calyces |
| V | Gross dilation, tortuous ureter, no papillary impressions |
Low-grade VUR often resolves spontaneously; higher grades may require antibiotic prophylaxis, endoscopic injection (Deflux), or ureteral reimplantation.
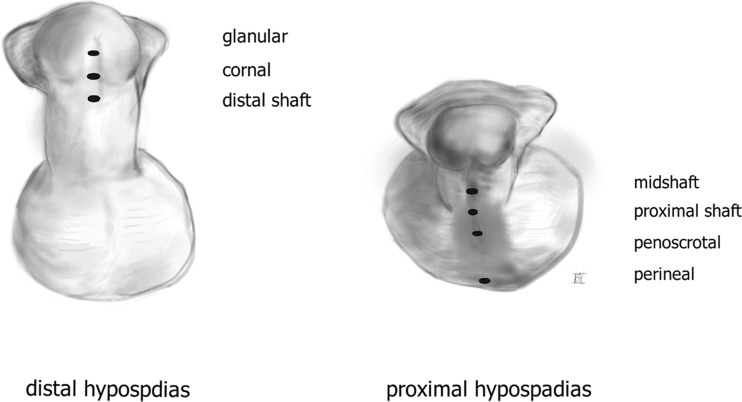
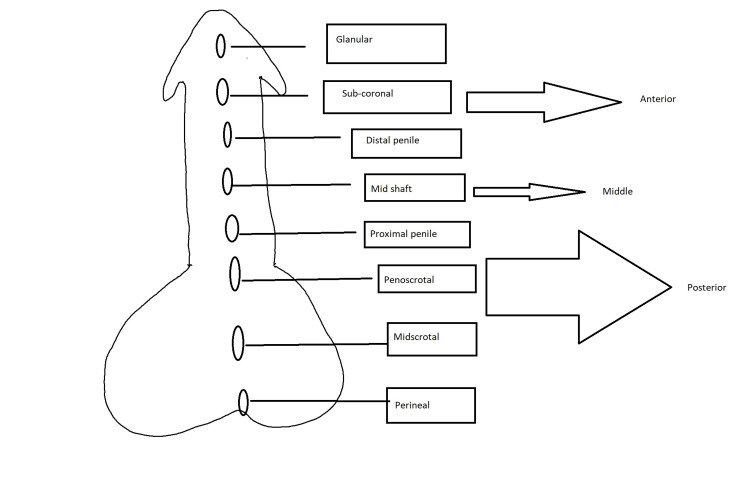
Cryptorchidism (undescended testis) should prompt orchiopexy between 6 and 18 months of age to reduce infertility and (modestly) malignancy risk. Hypospadias is a ventral meatal opening with dorsal hooded foreskin and chordee; repaired at ~6–18 months using tubularized incised plate (TIP/Snodgrass) or other techniques. Posterior urethral valves (PUV) are obstructing mucosal folds in the posterior urethra of newborn males, presenting with prenatal hydronephrosis, oligohydramnios, or postnatal UTI/retention — treated with endoscopic valve ablation. Other pediatric conditions include hydronephrosis from UPJ obstruction, primary megaureter, prune belly syndrome, bladder exstrophy, epispadias, and nocturnal enuresis.
18 Genitourinary Trauma & Urologic Emergencies Trauma
Renal trauma is most commonly blunt (MVC, fall). Graded by the AAST Renal Injury Scale I–V:
| Grade | Description |
|---|---|
| I | Contusion or subcapsular hematoma, no laceration |
| II | Non-expanding perirenal hematoma, cortical laceration < 1 cm, no urinary extravasation |
| III | Cortical laceration > 1 cm, no collecting system involvement |
| IV | Laceration through cortex, medulla, and collecting system with urinary extravasation OR vascular injury with contained hematoma |
| V | Shattered kidney OR renal pedicle avulsion |
Most grades I–IV are managed non-operatively with bed rest, serial H&H, and BP monitoring, with angioembolization for active bleeding. Grade V and hemodynamic instability require surgical exploration. Ureteral injuries are usually iatrogenic (gynecologic, colorectal surgery). Bladder injuries are either extraperitoneal (managed with catheter drainage) or intraperitoneal (requires surgical repair) — diagnosed by CT or retrograde cystography. Pelvic fracture + gross hematuria should prompt a cystogram. Urethral injuries accompany pelvic fractures (posterior urethra) or straddle injuries (bulbar urethra); blood at the meatus, high-riding prostate, and inability to void suggest urethral disruption — retrograde urethrogram before any catheter attempt.
Urologic Emergencies Summary: testicular torsion, Fournier gangrene, priapism, paraphimosis, obstructed infected kidney, urosepsis, renal pedicle avulsion, bladder rupture (intraperitoneal), urethral disruption.
19 Urologic Procedures — A to Z
| Procedure | What It Is | Key Indications |
|---|---|---|
| Flexible cystoscopy | Office-based bladder/urethral inspection with a flexible scope | Hematuria workup, surveillance, LUTS evaluation, catheter placement |
| Rigid cystoscopy | OR-based bladder inspection allowing larger working channel | Stone retrieval, biopsy, stent placement, TURBT setup |
| TURBT | Transurethral resection of bladder tumor with loop electrocautery | Diagnosis and treatment of bladder tumors (Ta, T1, and initial T2) |
| TURP | Transurethral resection of prostate — monopolar or bipolar | BPH with obstruction, 30–80 g gland |
| HoLEP / ThuLEP | Holmium/thulium laser enucleation of prostate | Large (> 80 g) BPH, size-independent outcomes |
| PVP (GreenLight) | Photoselective vaporization of prostate with 532 nm laser | BPH, anticoagulated patients |
| UroLift | Implanted sutures retracting prostate lobes | BPH without median lobe, preserve ejaculation |
| Rezūm | Water vapor thermal ablation of prostate | BPH 30–80 g, office-based |
| Simple prostatectomy | Open or robotic removal of BPH adenoma | BPH > 80–100 g |
| Radical prostatectomy (RALP) | Robotic-assisted laparoscopic prostatectomy with pelvic lymph node dissection | Localized prostate cancer |
| Partial nephrectomy | Nephron-sparing removal of tumor with margin (open, lap, robotic) | cT1 renal masses when feasible |
| Radical nephrectomy | Removal of kidney with Gerota fascia ± adrenal | Large/complex RCC, tumor thrombus |
| Nephroureterectomy | Removal of kidney, ureter, and bladder cuff | Upper tract urothelial carcinoma |
| Radical cystectomy + diversion | Bladder removal with ileal conduit, neobladder, or Indiana pouch | MIBC, BCG-failure high-risk NMIBC |
| URS + laser lithotripsy | Ureteroscopy with holmium laser stone fragmentation and basket extraction | Ureteral and renal stones < 2 cm |
| PCNL | Percutaneous nephrolithotomy through a flank tract | Stones > 2 cm, staghorn, complex lower pole stones |
| SWL (ESWL) | Extracorporeal shock wave lithotripsy | Proximal ureteral/renal stones < 2 cm, non-calcium oxalate monohydrate |
| Ureteral stent | Double-J stent between kidney and bladder | Stone obstruction, post-URS, iatrogenic ureteral injury |
| Percutaneous nephrostomy | Tube from skin to renal pelvis via IR | Obstructed infected kidney, failed retrograde decompression |
| Suprapubic catheter | Catheter through lower abdominal wall into bladder | Difficult urethral access, urethral disruption, long-term drainage |
| DVIU | Direct visual internal urethrotomy | Short urethral strictures |
| Urethroplasty | Open reconstruction — excision/primary anastomosis or buccal mucosa graft | Bulbar or penile urethral strictures |
| Pyeloplasty | Reconstruction of UPJ (Anderson-Hynes dismembered) | UPJ obstruction |
| Varicocelectomy | Ligation of internal spermatic veins (microsurgical, lap, embolization) | Infertility, pain, adolescent testicular atrophy |
| Vasectomy / vasovasostomy | Office vas ligation; microsurgical reversal | Contraception; fertility restoration |
| Hydrocelectomy | Excision/eversion of tunica vaginalis | Symptomatic hydrocele |
| Radical inguinal orchiectomy | Removal of testis with high cord ligation via inguinal incision | Testicular cancer |
| Orchiopexy | Fixation of testis in scrotum | Torsion (bilateral), cryptorchidism |
| Circumcision | Removal of the foreskin | Phimosis, recurrent balanitis, paraphimosis, elective |
| Penile prosthesis | Inflatable or malleable device implanted in corpora cavernosa | Refractory ED |
| Artificial urinary sphincter | Implanted cuff, pump, reservoir | Post-prostatectomy severe stress incontinence |
| Male sling | Transobturator sling compressing bulbar urethra | Mild post-prostatectomy SUI |
| Midurethral sling (MUS) | Synthetic mesh sling (retropubic or transobturator) | Female SUI |
| Sacral neuromodulation (InterStim) | Implanted S3 nerve stimulator | Refractory OAB, urinary retention, fecal incontinence |
| Intradetrusor onabotulinumtoxinA | Cystoscopic injection of 100–200 units of Botox into detrusor | Refractory OAB, neurogenic DO |
| TRUS-guided prostate biopsy | 12–14 core systematic biopsy ± MRI fusion targeting | Suspected prostate cancer |
| Transperineal prostate biopsy | Perineal approach under local or general anesthesia | Reduced infection risk, anterior lesions |
| Retrograde pyelogram | Contrast injection into ureter via cystoscopy | Characterize upper tract filling defect or stricture |
20 Urologic Imaging & Diagnostics
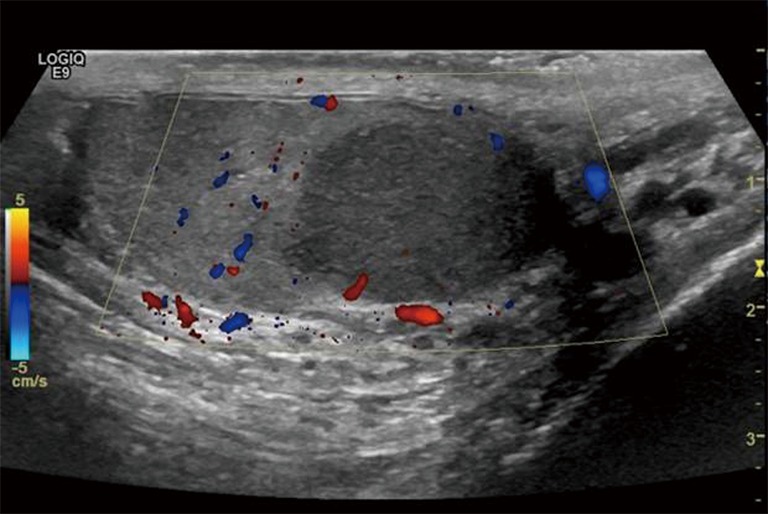
Ultrasound: Renal US shows hydronephrosis, stones, masses, cysts. Scrotal US with Doppler is the go-to for testicular pain, mass, or trauma — reports intratesticular flow. Bladder US measures volume and PVR. Transrectal US (TRUS) evaluates the prostate for biopsy guidance.

CT: Non-contrast CT "stone protocol" (5 mm or thinner cuts) is the gold standard for stone disease. CT urogram has three phases (non-contrast, arterial/nephrographic, and delayed/excretory) and is the recommended imaging for gross hematuria and high-risk microhematuria. CT abdomen/pelvis with contrast characterizes renal masses and stages urologic cancers.
MRI: Multiparametric prostate MRI (mpMRI) with T2, diffusion-weighted, and dynamic contrast-enhanced sequences is reported on the PI-RADS 1–5 scale (5 = highly likely clinically significant cancer). MR urogram is an alternative to CT urogram for patients with contrast contraindications.
Nuclear medicine: MAG3 renal scan assesses differential function and obstruction; DMSA is the gold standard for cortical scarring in pediatric VUR; bone scan stages prostate cancer (> T2 or PSA > 20 or Grade Group ≥ 4). PSMA PET is now standard for staging intermediate/high-risk and biochemical recurrent prostate cancer.
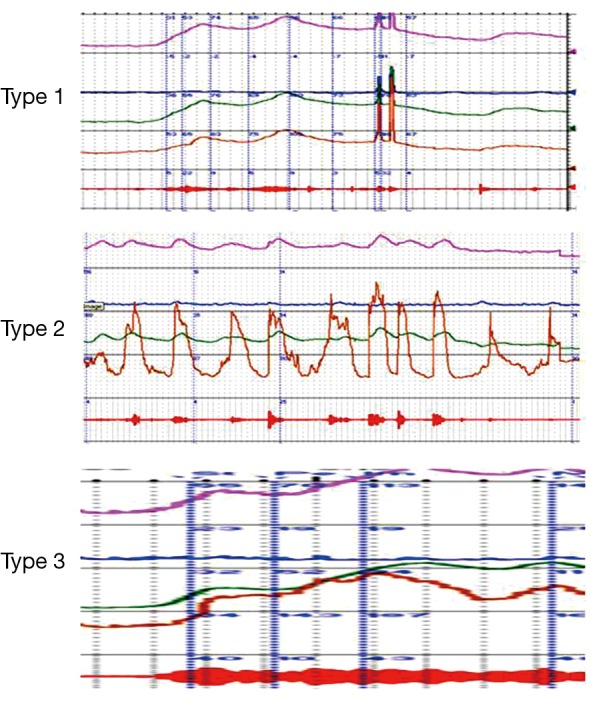
Urodynamics: Filling cystometry (compliance, capacity, detrusor overactivity), pressure-flow study (bladder outlet obstruction index, BOOI), EMG (sphincter activity/DSD), and video urodynamics.
Labs: UA (microscopic sediment, nitrites, leukocyte esterase), urine culture, cytology (low sensitivity but high specificity for high-grade urothelial carcinoma), urine NMP22/BTA/UroVysion FISH, PSA, testosterone, 24-hour urine for stone metabolic workup (volume, Ca, ox, citrate, uric acid, Na, K, Mg, P, pH, supersaturations).
21 Medications You Must Know
Alpha Blockers (BPH, MET)
| Generic | Brand | Dose | Notes |
|---|---|---|---|
| Tamsulosin | Flomax | 0.4 mg qHS | Most common; intraoperative floppy iris syndrome (IFIS) — flag before cataract surgery |
| Alfuzosin | Uroxatral | 10 mg daily | QT prolongation caution |
| Silodosin | Rapaflo | 8 mg daily | Most uroselective; retrograde ejaculation very common |
| Doxazosin | Cardura | 1–8 mg daily | Non-selective; titrate; orthostasis |
| Terazosin | Hytrin | 1–10 mg qHS | Non-selective; older, cheaper |
5-Alpha Reductase Inhibitors
| Generic | Brand | Dose | Notes |
|---|---|---|---|
| Finasteride | Proscar | 5 mg daily | Inhibits type II; ~50% PSA reduction (double the value); sexual side effects |
| Dutasteride | Avodart | 0.5 mg daily | Inhibits type I and II; combined with tamsulosin as Jalyn |
PDE5 Inhibitors
| Generic | Brand | Indication | Notes |
|---|---|---|---|
| Sildenafil | Viagra, Revatio | ED, PAH | On-demand; 4–6 hour duration |
| Tadalafil | Cialis, Adcirca | ED, BPH, PAH | Daily 5 mg or on-demand 10–20 mg; 36-hour duration |
| Vardenafil | Levitra | ED | On-demand; QT caution |
| Avanafil | Stendra | ED | Faster onset |
Concurrent nitrates (any form, any route) are an absolute contraindication due to risk of severe hypotension. Alpha blockers should be initiated carefully with PDE5i use.
OAB Medications
| Generic | Brand | Class | Notes |
|---|---|---|---|
| Oxybutynin | Ditropan, Oxytrol | Anticholinergic | High anticholinergic burden; ER or patch better tolerated |
| Tolterodine | Detrol | Anticholinergic | Standard OAB agent |
| Solifenacin | VESIcare | Anticholinergic | M3-selective |
| Darifenacin | Enablex | Anticholinergic | M3-selective |
| Fesoterodine | Toviaz | Anticholinergic | Prodrug of active tolterodine metabolite |
| Trospium | Sanctura | Anticholinergic | Does not cross BBB — fewer CNS effects in elderly |
| Mirabegron | Myrbetriq | Beta-3 agonist | Monitor BP; alternative to anticholinergics |
| Vibegron | Gemtesa | Beta-3 agonist | No BP signal; once daily |
UTI Antibiotics
| Drug | Dose | Use |
|---|---|---|
| Nitrofurantoin | 100 mg BID × 5 d | Uncomplicated cystitis; avoid if CrCl < 30 |
| TMP-SMX | DS BID × 3 d | Uncomplicated cystitis if resistance < 20% |
| Fosfomycin | 3 g once | Uncomplicated cystitis, single dose |
| Cephalexin | 500 mg QID × 5–7 d | Alternative, safe in pregnancy |
| Ciprofloxacin | 500 mg BID × 7 d | Pyelonephritis, prostatitis, complicated UTI |
| Levofloxacin | 750 mg daily × 5–7 d | Pyelonephritis, prostatitis |
Androgen Deprivation & Advanced Prostate Cancer
| Drug | Brand | Class | Use |
|---|---|---|---|
| Leuprolide | Lupron, Eligard | GnRH agonist | Depot injection; flare phenomenon (cover with antiandrogen) |
| Goserelin | Zoladex | GnRH agonist | Subcutaneous implant |
| Degarelix | Firmagon | GnRH antagonist | Rapid castration, no flare |
| Relugolix | Orgovyx | Oral GnRH antagonist | Daily pill |
| Bicalutamide | Casodex | First-gen antiandrogen | Flare coverage |
| Enzalutamide | Xtandi | 2nd-gen AR blocker | mCRPC, mHSPC, nmCRPC |
| Apalutamide | Erleada | 2nd-gen AR blocker | mHSPC, nmCRPC |
| Darolutamide | Nubeqa | 2nd-gen AR blocker | nmCRPC, mHSPC |
| Abiraterone | Zytiga | CYP17 inhibitor | Combined with prednisone; mCRPC, mHSPC |
Intravesical Therapy
| Drug | Use |
|---|---|
| BCG (Bacillus Calmette-Guérin) | High-risk NMIBC, CIS — induction 6 weekly + maintenance × 3 years |
| Mitomycin C | Single post-TURBT dose for low-risk NMIBC, or induction |
| Gemcitabine | BCG-unresponsive NMIBC (often with docetaxel) |
Other Key Urology Drugs
| Drug | Use |
|---|---|
| Phenazopyridine (Pyridium) | Urinary analgesic; stains urine orange; warn patients |
| Potassium citrate (Urocit-K) | Stone prevention (alkalinize urine) |
| Allopurinol | Uric acid stones, hyperuricosuric calcium oxalate stones |
| Hydrochlorothiazide | Hypercalciuric calcium stones |
| Tiopronin | Cystinuria |
| Desmopressin (DDAVP) | Nocturnal polyuria, pediatric enuresis |
| Imipramine | Off-label SUI, enuresis |
| Testosterone (gel/injection/pellet) | Symptomatic hypogonadism |
22 Classification & Staging Systems
This section collects classifications referenced throughout the guide that are not already fully enumerated in their disease sections. Stone, bladder cancer, VUR, hydronephrosis, renal injury, and Bosniak systems are listed in their respective sections above.
AUA Symptom Score / IPSS (0–35)
Seven questions, each 0–5: (1) incomplete emptying, (2) frequency < 2 hours, (3) intermittency, (4) urgency, (5) weak stream, (6) straining, (7) nocturia (number of times per night). Plus a separate QoL question 0–6 ("How would you feel if you had to live with your urinary condition the way it is now?").
TNM Prostate Cancer (brief)
T1a/b: incidental at TURP. T1c: PSA-detected. T2a/b/c: palpable confined. T3a: EPE. T3b: seminal vesicle. T4: adjacent organs. N1: regional LN. M1a: distant LN. M1b: bone. M1c: other.
TNM RCC (brief)
T1a ≤ 4 cm, T1b 4–7 cm, T2a 7–10 cm, T2b > 10 cm confined, T3a perinephric fat or renal vein, T3b IVC below diaphragm, T3c IVC above diaphragm, T4 beyond Gerota or ipsilateral adrenal.
TNM Bladder (brief)
Ta: noninvasive papillary. Tis: CIS. T1: lamina propria. T2a: inner ½ muscle. T2b: outer ½ muscle. T3a: microscopic perivesical. T3b: gross perivesical. T4a: prostate/uterus/vagina. T4b: pelvic/abdominal wall.
TNM Testis (brief)
Unique in that serum tumor markers (S) are part of stage: S0 normal, S1/S2/S3 by AFP, hCG, LDH levels. Stage I = confined to testis/cord; II = retroperitoneal nodes; III = distant or markedly elevated markers.
Foley Catheter Sizes & Types
| Size (Fr) | Typical Use |
|---|---|
| 8–10 Fr | Pediatric |
| 12–14 Fr | Female adult, clear urine |
| 16–18 Fr | Standard adult male |
| 20–22 Fr | Hematuria, clots, 3-way CBI |
| 24–26 Fr | Heavy clot retention, 3-way CBI |
Types: 2-way (drainage), 3-way (drainage + irrigation for CBI), coudé tip (curved for BPH/false passage), council tip (guidewire compatible), silicone (long-term), latex (short-term).
23 Physical Exam, Abbreviations & Risk Factors
The Urologic Physical Exam
Abd: soft, NT, ND; no CVA tenderness; no palpable bladder
Penis: circumcised, meatus normal, no lesions
Testes: descended bilaterally, normal size, non-tender, no masses
Epididymis/cord: non-tender, no varicocele
Cremasteric reflex: present bilaterally
Inguinal: no hernia or adenopathy
DRE: sphincter tone normal, prostate ~30 g, smooth, non-tender, no nodules
Abd: soft, NT, ND; no CVA tenderness; no palpable bladder
External genitalia: normal, no lesions, no atrophy
Urethra: no hypermobility, no diverticulum
Speculum: normal vaginal mucosa, cervix visualized
POP-Q: Aa 0, Ba 0, C -8, Bp 0, Ap 0 (or stage noted)
Cough stress test: negative/positive at comfortable bladder volume
Bimanual: no pelvic masses or tenderness
Abbreviations Master List
Anatomy & Structures
Diagnoses & Conditions
Procedures
Labs, Imaging & Tools
Risk Factors & Comorbidities
Smoking: Pack-years and quit date. Biggest modifiable risk factor for bladder cancer, RCC, UTUC, and ED.
Diabetes: A1C, complications. Accelerates ED, neurogenic bladder, and infection risk.
Anticoagulation / antiplatelet: Drug, indication, and when last held. Every procedure requires a bleeding risk assessment.
Prior GU surgery / instrumentation: Stricture risk, altered anatomy, prior cancer history.
Prior stones / UTIs: Recurrence risk, metabolic evaluation indications.
Occupational exposures: Aromatic amines (dye, rubber, leather, firefighters, hairdressers) — bladder cancer.
Family history: Prostate cancer (first-degree), BRCA/HOXB13, Lynch syndrome (UTUC), VHL (RCC), polycystic kidney disease.
Medications that affect LUTS: anticholinergics, sympathomimetics, decongestants, opiates, diuretics, alpha agonists.
24 Sample HPI Templates & References
These templates show the rhythm and content expected in a real urology clinic note. Use them as frameworks during your first weeks.
"Mr. [Name] is a 68-year-old male with hypertension and type 2 diabetes who presents for evaluation of progressive LUTS over the past 18 months. He describes weak urinary stream, hesitancy, intermittency, and post-void dribbling, with nocturia 3–4 times per night. He denies gross hematuria, dysuria, fever, or prior urinary retention. IPSS today is 22 (severe) with QoL 5 (mostly dissatisfied). He has not tried any prostate medications. PSA last month was 2.8 ng/mL (prior 2.1 in 2023). PVR in clinic 180 mL. Uroflow Qmax 8 mL/s with voided volume 220 mL. No prior urologic surgery. Current medications include lisinopril 20 mg and metformin 1000 mg BID. He denies taking any decongestants or antihistamines."
"Mr. [Name] is a 62-year-old male with no prior urologic history referred by his PCP for evaluation of a rising PSA. PSA trajectory: 2.1 (2022), 3.4 (2023), 5.2 (2025). Free/total PSA 12% (low). Family history significant for prostate cancer in father diagnosed at age 68. He denies LUTS, hematuria, bone pain, or weight loss. DRE today: prostate ~40 g, symmetric, firm but without discrete nodules. Multiparametric prostate MRI obtained last week demonstrates a PI-RADS 4 lesion in the left peripheral zone mid-gland measuring 12 mm. Plan today is to discuss MRI-fusion TRUS-guided prostate biopsy."
"Mr. [Name] is a 45-year-old male presenting to the ED with acute onset of severe left flank pain that began 6 hours ago and radiates to the left groin and testicle, associated with nausea and one episode of vomiting. Pain is 9/10, colicky, and the patient is unable to find a comfortable position. He denies fever, chills, dysuria, or gross hematuria. History of one prior left renal stone in 2022 that passed spontaneously. Afebrile, HR 98, BP 142/88. UA shows 25–50 RBC/HPF, no nitrites, no leukocyte esterase. Creatinine 1.1. Non-contrast CT demonstrates a 5 mm obstructing calculus at the left UVJ with mild left hydronephrosis. Plan: trial of passage with tamsulosin 0.4 mg daily, ketorolac and oxycodone for pain, strict return precautions for fever or worsening pain."
"Mrs. [Name] is a 65-year-old female with 35-pack-year smoking history (still active) and hypertension referred for asymptomatic microscopic hematuria. UA on routine PCP visit 6 weeks ago showed 20–30 RBC/HPF; repeat UA confirmed 25 RBC/HPF, no infection. She denies gross hematuria, dysuria, flank pain, weight loss, or occupational chemical exposures (homemaker). She is on lisinopril and aspirin 81 mg. Per AUA guidelines this is high-risk microhematuria; plan includes CT urogram and in-office flexible cystoscopy today. Urine cytology obtained."
"Patient is a 16-year-old male presenting to the ED with sudden-onset severe left scrotal pain that began 3 hours ago while playing basketball. Pain is associated with nausea and one episode of vomiting. No dysuria, urethral discharge, trauma, or recent instrumentation. No prior similar episodes. Exam: left testis is high-riding with horizontal lie, diffusely tender, with absent cremasteric reflex. Right testis normal. Scrotal Doppler ultrasound demonstrates absent intratesticular flow on the left, consistent with testicular torsion. Emergent OR for scrotal exploration, detorsion, and bilateral orchiopexy. Consent obtained from patient and parent; discussion of orchiectomy risk if testis non-viable."
"Mrs. [Name] is a 58-year-old postmenopausal female with a history of 5 culture-proven UTIs over the past 12 months (most recent E. coli, pan-sensitive, 3 weeks ago, treated with nitrofurantoin). Symptoms include dysuria, urgency, and suprapubic pressure with each episode. She denies fever, flank pain, hematuria, or incontinence. Sexually active with a single partner; timing of UTIs not clearly post-coital. No history of stones or instrumentation. Prior workup includes normal renal ultrasound and PVR 30 mL. Exam today: vulvovaginal atrophy noted. Plan per AUA recurrent UTI guideline: initiate vaginal estrogen, discuss cranberry and methenamine, consider self-start therapy vs low-dose prophylaxis."
References & Sources
Clinical Practice Guidelines
AUA/SUO Early Detection of Prostate Cancer Guideline (2023).
USPSTF. Screening for Prostate Cancer: Recommendation Statement. JAMA. 2018.
AUA Management of BPH/LUTS Guideline (2023).
AUA/ASTRO/SUO Renal Mass and Localized Renal Cancer Guideline (2021).
AUA/SUO Non-Muscle Invasive Bladder Cancer Guideline (2024).
AUA/ASCO/ASTRO/SUO Muscle-Invasive Bladder Cancer Guideline (2017, amended 2020).
AUA Surgical Management of Stones Guideline (2016).
AUA Medical Management of Kidney Stones Guideline (2014, amended 2019).
AUA/SUFU Microhematuria Guideline (2020).
AUA/CUA/SUFU Recurrent Uncomplicated UTI in Women Guideline (2022 amendment).
AUA/SUFU Overactive Bladder Guideline (2019 amendment).
AUA/SUFU Surgical Treatment of Female Stress Urinary Incontinence Guideline (2017).
Diagram & Figure Sources
Figure 1: The Urinary System. OpenStax College. CC BY 3.0.
Figure 2: Kidney Cross-Section. OpenStax College. CC BY 3.0.
Figure 3: Male Reproductive Anatomy. U.S. National Cancer Institute. Public domain.
Figure 4: Prostate Zonal Anatomy. U.S. National Cancer Institute. Public domain.
Figure 5: Kidney Stone with Hydronephrosis. BruceBlaus. CC BY 3.0.
Urology is a specialty of specifics. Gleason scores, IPSS totals, stone sizes in millimeters, PSA trajectories, PI-RADS scores, AUA risk categories, BCG cycle counts, hydronephrosis grades — every one of these is a number the attending expects to see in the note without having to repeat it. The best urology scribes pre-populate the note from the prior visit, the imaging report, and the lab trends before the patient is seen, so that when the attending walks out of the exam room, 80% of the work is already done.
Learn to distinguish storage from voiding LUTS in your sleep. Know which stone composition is which color on a CT. Understand why a Grade Group 2 is different from a Grade Group 3 and why that changes the plan. Memorize the AUA bladder cancer risk categories and the BCG schedule. Recognize a testicular torsion presentation before the doctor finishes saying it. These are the habits that separate a fast scribe from a great one.
Welcome to urology. The patients are grateful, the procedures are technical and varied, and the specialty covers everything from newborns to nonagenarians. This guide is your foundation — the expertise comes from applying it in clinic every day.