Hand Surgery
Every diagnosis, fracture pattern, tendon injury, nerve compression, reconstruction, classification, complication, medication, and management algorithm across the full scope of hand and upper extremity surgery in one place.
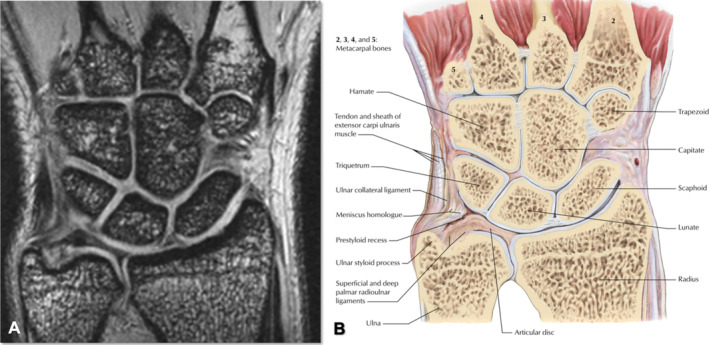
01 Hand & Wrist Skeletal Anatomy
Bony Architecture
The hand and wrist skeleton comprises 27 bones: 8 carpal bones, 5 metacarpals, and 14 phalanges (2 in the thumb, 3 in each finger). The carpal bones are arranged in two rows. The classic mnemonic for the proximal-to-distal, radial-to-ulnar arrangement is "Some Lovers Try Positions That They Can't Handle":
| Row | Bone | Mnemonic Word | Key Feature |
|---|---|---|---|
| Proximal | Scaphoid | Some | Most commonly fractured carpal; retrograde blood supply |
| Proximal | Lunate | Lovers | Most commonly dislocated carpal; Kienböck disease (AVN) |
| Proximal | Triquetrum | Try | Second most commonly fractured carpal (dorsal chip) |
| Proximal | Pisiform | Positions | Sesamoid bone within FCU tendon; protects Guyon's canal |
| Distal | Trapezium | That | Articulates with 1st MC; CMC arthritis site |
| Distal | Trapezoid | They | Least commonly fractured carpal; keystone of distal row |
| Distal | Capitate | Can't | Largest carpal; articulates with 3rd MC |
| Distal | Hamate | Handle | Hook prone to fracture; ulnar nerve/artery lie adjacent |
Joints of the Hand
The carpometacarpal (CMC) joints connect the distal carpal row to the metacarpal bases. The 1st CMC (thumb basal joint) is a biconcave saddle joint allowing flexion-extension, abduction-adduction, and opposition — it is the most commonly affected by osteoarthritis (Eaton-Littler staging). The 2nd and 3rd CMC joints are nearly rigid, providing a stable central pillar, while the 4th and 5th CMC joints allow 15–30° of flexion for cupping the hand.
The metacarpophalangeal (MCP) joints are condyloid joints permitting flexion-extension, abduction-adduction, and circumduction. The collateral ligaments are tight in flexion and lax in extension — therefore, MCP joints must be splinted in flexion (70–90°) to prevent collateral ligament contracture ("safe position" or intrinsic-plus position).
The proximal interphalangeal (PIP) joints are hinge joints and the most commonly injured joints in the hand. The volar plate is a critical stabilizer preventing hyperextension. The distal interphalangeal (DIP) joints are similarly hinge joints; the terminal extensor tendon inserts on the distal phalanx dorsum.
Key Ligaments
The scapholunate (SL) ligament is the most important intrinsic carpal ligament. It has dorsal, proximal (membranous), and volar components; the dorsal portion is the strongest and most important for stability. Disruption leads to scapholunate dissociation (widened SL interval >3 mm = "Terry Thomas sign") and the DISI (dorsal intercalated segment instability) pattern.
The lunotriquetral (LT) ligament connects the lunate to the triquetrum; disruption leads to VISI (volar intercalated segment instability) pattern. The triangular fibrocartilage complex (TFCC) is the primary stabilizer of the DRUJ and the ulnocarpal joint — it bears ~20% of axial load across the wrist (increasing to ~40% with positive ulnar variance).
The ulnar collateral ligament (UCL) of the thumb MCP joint is the structure injured in "gamekeeper's thumb" or "skier's thumb." The Stener lesion occurs when the torn UCL displaces superficial to the adductor aponeurosis, preventing healing — this requires surgical repair.
Kienböck Disease (Lunate AVN)
Kienböck disease is avascular necrosis of the lunate, most common in males aged 20–40. Associated with negative ulnar variance (short ulna increases load on the lunate). The Lichtman classification guides treatment:
| Stage | Radiographic Finding | Treatment |
|---|---|---|
| I | Normal X-ray; MRI shows decreased signal | Immobilization; consider core decompression |
| II | Lunate sclerosis on X-ray; no collapse | Unloading procedures: radial shortening osteotomy (if ulnar negative), capitate shortening, or vascularized bone graft |
| IIIA | Lunate collapse; no scaphoid rotation | Radial shortening osteotomy or vascularized bone graft (4+5 ECA pedicled graft) |
| IIIB | Lunate collapse + scaphoid flexion (fixed rotation) | Scaphocapitate fusion, PRC, or STT fusion |
| IV | Generalized degenerative changes | PRC (if capitate head intact), total wrist fusion, or total wrist arthroplasty |
02 Tendon Anatomy & Zones of Injury
Extensor Compartments of the Wrist
There are six dorsal compartments at the wrist, each containing specific extensor tendons beneath the extensor retinaculum:
| Compartment | Contents | Clinical Relevance |
|---|---|---|
| 1st | APL, EPB | De Quervain tenosynovitis; subsheath variants in up to 40% |
| 2nd | ECRL, ECRB | Intersection syndrome (crossing of 1st and 2nd compartments) |
| 3rd | EPL | Lister's tubercle acts as a pulley; EPL rupture after distal radius fracture |
| 4th | EDC, EIP | Largest compartment; EIP available as tendon transfer donor |
| 5th | EDM | EDM commonly has two slips |
| 6th | ECU | ECU subsheath separate from retinaculum; ECU tendinitis/subluxation |
Flexor Tendons & Pulley System
The flexor digitorum profundus (FDP) inserts on the base of the distal phalanx and flexes the DIP joint. The flexor digitorum superficialis (FDS) splits (forming Camper's chiasm) and inserts on the middle phalanx, flexing the PIP joint. The flexor pollicis longus (FPL) is the only extrinsic flexor of the thumb IP joint.
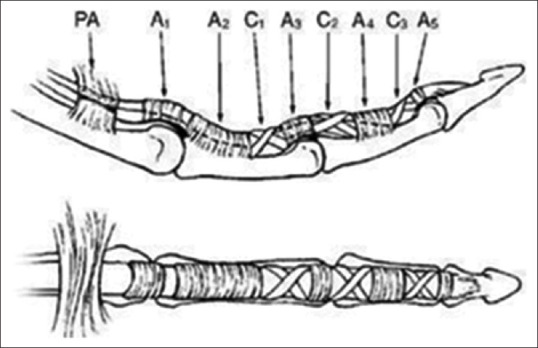
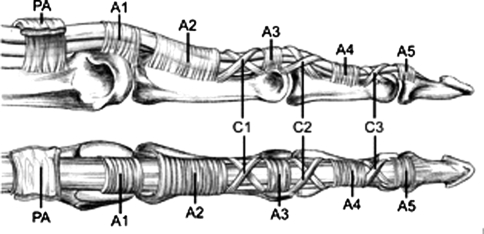
The digital pulley system maintains tendon-bone proximity for efficient flexion:
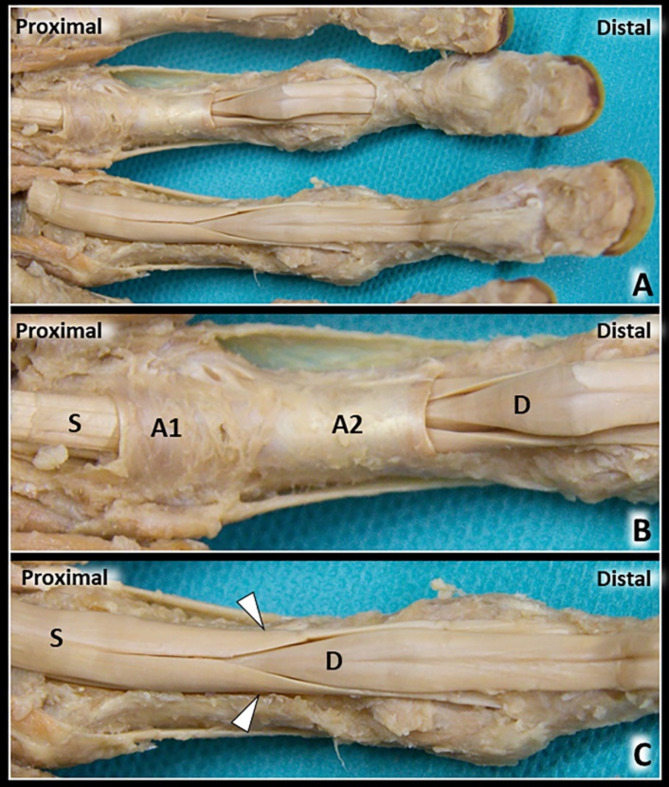
| Pulley | Location | Importance |
|---|---|---|
| A1 | MCP joint volar plate | Involved in trigger finger; release is therapeutic |
| A2 | Proximal phalanx (proximal half) | Critical — must preserve to prevent bowstringing |
| A3 | PIP joint volar plate | May be sacrificed if needed |
| A4 | Middle phalanx (middle third) | Critical — must preserve to prevent bowstringing |
| A5 | DIP joint volar plate | May be sacrificed if needed |
| C1–C3 | Between annular pulleys | Cruciate pulleys; allow tendon gliding during flexion |
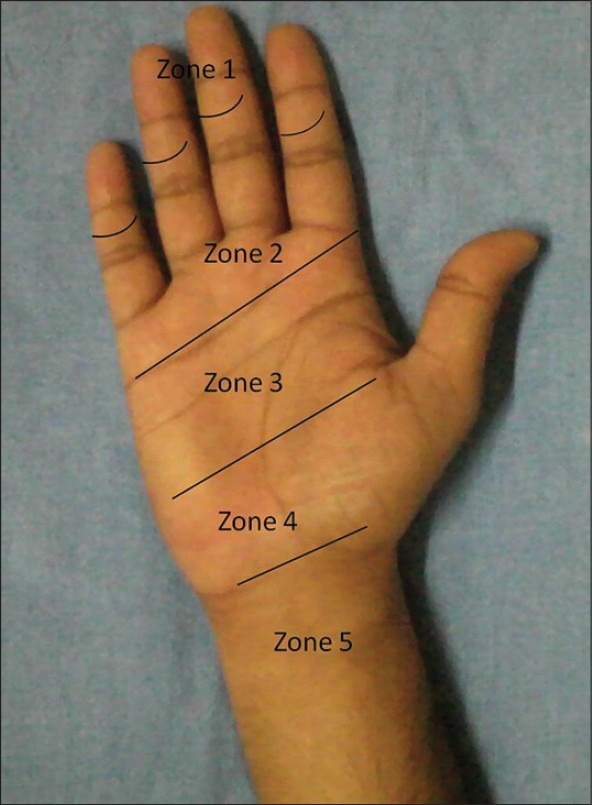
Flexor Tendon Zones
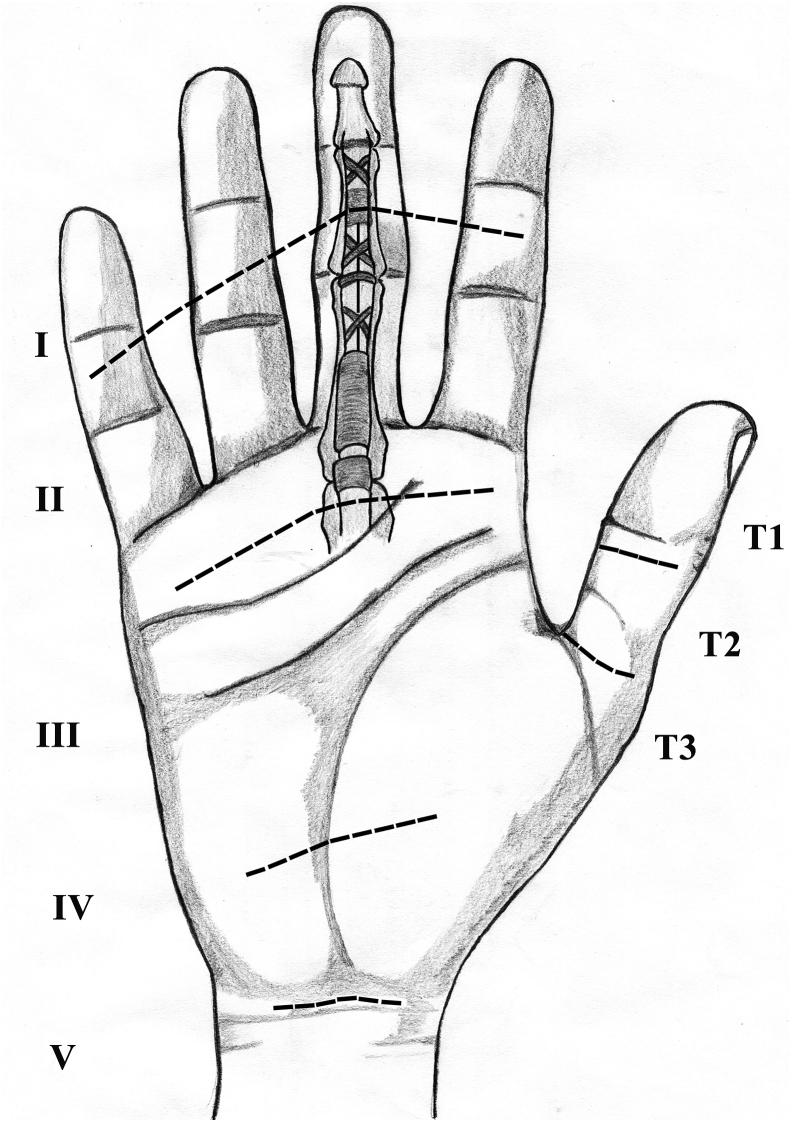
| Zone | Boundaries | Key Feature |
|---|---|---|
| Zone I | FDS insertion to FDP insertion | FDP only; "jersey finger" |
| Zone II | A1 pulley to FDS insertion | "No man's land" — both FDP and FDS within fibro-osseous sheath; most challenging repairs |
| Zone III | Distal carpal tunnel to A1 pulley | Lumbrical origin; better prognosis than Zone II |
| Zone IV | Within carpal tunnel | Nine tendons + median nerve in confined space |
| Zone V | Proximal to carpal tunnel | Musculotendinous junction; associated with nerve/vessel injury |
Extensor Tendon Zones
| Zone | Location | Injury Pattern |
|---|---|---|
| I | DIP joint | Mallet finger (terminal tendon disruption) |
| II | Middle phalanx | Rare isolated injuries |
| III | PIP joint | Boutonnière deformity (central slip disruption) |
| IV | Proximal phalanx | Often partial lacerations |
| V | MCP joint | Sagittal band rupture; "fight bite" |
| VI | Metacarpal dorsum | Good prognosis; direct repair |
| VII | Wrist (under retinaculum) | Adhesion risk; retinaculum partially preserved |
| VIII | Distal forearm | Musculotendinous junction injuries |
| IX | Proximal forearm | Muscle belly injuries; may not hold suture well |
Intrinsic Muscles of the Hand
The intrinsic muscles are essential for fine motor function. The thenar muscles (opponens pollicis, abductor pollicis brevis, flexor pollicis brevis superficial head — all median nerve) provide opposition. The hypothenar muscles (abductor digiti minimi, flexor digiti minimi brevis, opponens digiti minimi — all ulnar nerve) control the small finger. The interossei (4 dorsal = abduction, "DAB"; 4 palmar = adduction, "PAD" — all ulnar nerve) and lumbricals (1–2 = median nerve; 3–4 = ulnar nerve) flex the MCP joints while extending the IP joints through their insertion into the lateral bands. This dual action is the basis for intrinsic-minus (claw) and intrinsic-plus hand deformities.
03 Neurovascular Anatomy
Median Nerve
The median nerve (C5–T1) enters the hand through the carpal tunnel deep to the transverse carpal ligament (flexor retinaculum). The carpal tunnel contains: the median nerve, 4 FDP tendons, 4 FDS tendons, and the FPL tendon (9 tendons + 1 nerve). The recurrent motor branch (thenar branch) arises from the radial side of the median nerve at or just distal to the transverse carpal ligament and innervates the opponens pollicis, abductor pollicis brevis, and superficial head of the flexor pollicis brevis (the "LOAF" muscles: Lumbricals 1–2, Opponens pollicis, Abductor pollicis brevis, Flexor pollicis brevis superficial head).
Variations in the recurrent motor branch course are critical: extraligamentous (46–90%), subligamentous (31%), and transligamentous (23%). The transligamentous variant is at greatest risk during carpal tunnel release. The palmar cutaneous branch arises ~5 cm proximal to the wrist crease, courses superficial to the transverse carpal ligament (not within the tunnel), and supplies sensation to the thenar eminence — injury causes "pillar pain" after CTR.
The anterior interosseous nerve (AIN) is a pure motor branch of the median nerve arising in the proximal forearm. It innervates FPL, FDP to the index and long fingers, and pronator quadratus. AIN syndrome presents with inability to make an "OK" sign (loss of thumb IP and index DIP flexion).
Ulnar Nerve
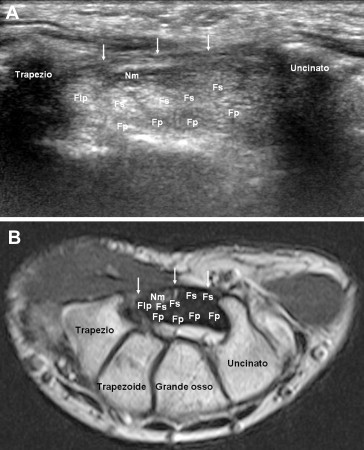
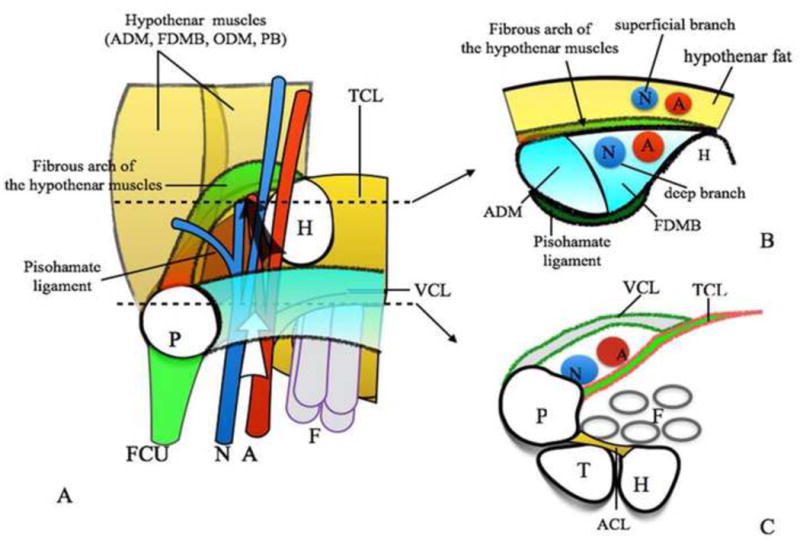
The ulnar nerve (C8–T1) enters the hand through Guyon's canal (bounded by the pisiform ulnarly, the hook of hamate radially, the volar carpal ligament as the roof, and the transverse carpal ligament as the floor). Within Guyon's canal, the nerve divides into a superficial sensory branch (ring and small finger ulnar sensation) and a deep motor branch (all interossei, hypothenar muscles, adductor pollicis, deep head of FPB, lumbricals 3–4).
Guyon's canal has three zones: Zone 1 (proximal, before bifurcation — mixed motor and sensory deficit), Zone 2 (deep branch — pure motor deficit), and Zone 3 (superficial branch — pure sensory deficit). Hook of hamate fractures classically cause Zone 2 compression.
The dorsal sensory branch of the ulnar nerve arises ~5–8 cm proximal to the wrist and courses dorsally to supply sensation to the dorsum of the small finger and ulnar half of the ring finger. It is at risk during ulnar-sided wrist approaches and ECU tendon surgery.
Radial Nerve
The posterior interosseous nerve (PIN) is the deep motor branch of the radial nerve. It enters the supinator muscle through the arcade of Frohse (the fibrous proximal edge of the superficial head of the supinator). The PIN innervates all wrist and finger extensors except the ECRL (which is innervated by the radial nerve proper before the bifurcation). PIN palsy causes finger drop and wrist radial deviation with extension (ECRL intact) but no sensory loss.
The superficial branch of the radial nerve (SBRN) is purely sensory, supplying the dorsal first web space, dorsum of the thumb, and dorsum of the index/long fingers proximal to the DIP. It runs beneath the brachioradialis and becomes subcutaneous ~8 cm proximal to the radial styloid. Injury (during surgery or venipuncture) causes numbness and painful neuroma (Wartenberg syndrome).
Arterial Anatomy & Allen Test
The radial artery enters the anatomic snuffbox, passes deep to the EPL and through the first dorsal interosseous muscle to form the deep palmar arch (with the deep branch of the ulnar artery). The ulnar artery enters the hand through Guyon's canal, radial to the ulnar nerve, and forms the superficial palmar arch (with the superficial palmar branch of the radial artery). The superficial arch lies at the level of the distal palmar crease and gives off common digital arteries that bifurcate into proper digital arteries.
The Allen test assesses collateral flow: compress both radial and ulnar arteries at the wrist, have the patient squeeze the fist then open it (blanched palm), then release one artery at a time. Normal reperfusion occurs within 5–7 seconds. A positive Allen test (delayed refill >10 seconds) indicates incomplete arch and is a contraindication to radial artery harvest for CABG conduit.
04 Hand Examination & Provocative Tests
Motor Testing
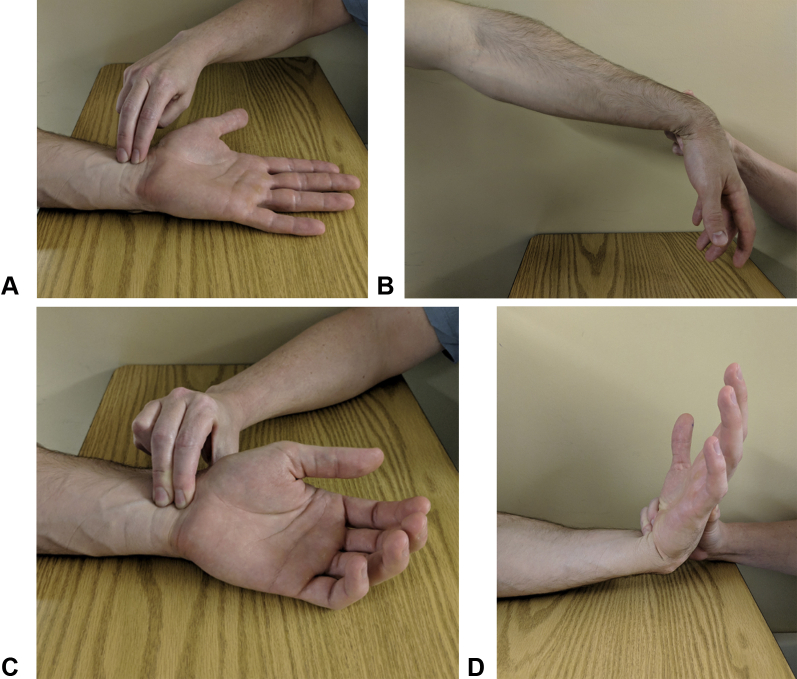
Intrinsic muscle testing: Interossei (finger abduction — dorsal interossei, finger adduction — palmar interossei; both ulnar nerve). Test adductor pollicis with Froment's sign: ask patient to pinch paper between thumb and index finger; compensation with FPL (thumb IP flexion) indicates ulnar nerve palsy. Wartenberg's sign: persistent small finger abduction at rest due to unopposed EDM (loss of 3rd palmar interosseous).
Extrinsic muscle testing: Test FDP by isolating DIP flexion while holding PIP in extension. Test FDS by holding all other fingers in full extension (eliminates quadriga effect of FDP) and asking patient to flex PIP. Test EPL by thumb retropulsion (lift thumb off table with palm flat). Test APL/EPB by thumb radial abduction against resistance.
Sensory Testing
Two-point discrimination (2PD) is the gold standard for sensory assessment in the hand. Normal static 2PD: <6 mm in fingertips. Results: <6 mm = normal; 6–10 mm = fair; 11–15 mm = poor; >15 mm or only one point perceived = protective sensation only. Moving 2PD is more sensitive and recovers earlier; normal moving 2PD is 2–3 mm.
Semmes-Weinstein monofilament testing evaluates threshold of pressure perception using calibrated nylon filaments. Results: 2.83 (green) = normal light touch; 3.61 (blue) = diminished light touch; 4.31 (purple) = diminished protective sensation; 4.56 (red) = loss of protective sensation; 6.65 (red-lined) = deep pressure only; no response = anesthetic.
Provocative Tests
| Test | Technique | Positive Finding | Condition |
|---|---|---|---|
| Phalen's test | Maximal wrist flexion for 60 seconds | Paresthesias in median nerve distribution | Carpal tunnel syndrome (sensitivity 68%, specificity 73%) |
| Tinel's sign | Percussion over nerve at site of compression | Electric/tingling sensation distally | Nerve compression or regeneration (sensitivity 50%, specificity 77%) |
| Durkan's test | Direct pressure over carpal tunnel for 30 seconds | Paresthesias in median distribution | Carpal tunnel syndrome (sensitivity 87%, specificity 90%) |
| Finkelstein's test | Fist over tucked thumb, ulnar deviate wrist | Pain over 1st dorsal compartment | De Quervain tenosynovitis |
| Watson's scaphoid shift | Pressure on scaphoid tubercle; radial-to-ulnar deviation | Painful clunk or apprehension | Scapholunate instability (sensitivity 69%, specificity 66%) |
| TFCC grind (press) test | Axial load + ulnar deviation | Ulnar-sided wrist pain | TFCC tear |
| Froment's sign | Pinch paper between thumb and index | Thumb IP flexion (FPL compensation) | Ulnar nerve palsy (adductor pollicis weakness) |
| Elson test | Flex PIP over table edge at 90°; resist middle phalanx extension | DIP becomes rigid in extension (or hyperextends) | Central slip disruption (boutonnière) |

05 Distal Radius Fractures
Fracture Patterns
Distal radius fractures are the most common fractures of the upper extremity, with a bimodal distribution (young males — high energy; postmenopausal women — low energy/osteoporotic). Key patterns:
| Fracture | Mechanism | Deformity | Key Feature |
|---|---|---|---|
| Colles fracture | Fall on outstretched hand (FOOSH), wrist extension | Dorsal angulation, dorsal displacement ("dinner fork") | Most common pattern; extra-articular |
| Smith fracture | Fall on flexed wrist or direct dorsal blow | Volar angulation, volar displacement ("garden spade") | "Reverse Colles"; typically requires ORIF |
| Barton fracture | High energy; axial load + shear | Volar or dorsal rim fracture-subluxation | Intra-articular; volar Barton more common; ORIF indicated |
| Chauffeur fracture | Radial styloid fracture from direct blow or compression | Radial styloid fragment | Intra-articular; assess for scapholunate injury |
| Die-punch fracture | Axial load through lunate fossa | Depressed lunate fossa fragment | Intra-articular; often missed; requires CT |
Classification
The Frykman classification (I–VIII) is based on involvement of the radiocarpal joint, DRUJ, and both. Odd numbers = without ulnar styloid fracture; even numbers = with ulnar styloid fracture. Types I–II are extra-articular; III–IV involve the radiocarpal joint; V–VI involve the DRUJ; VII–VIII involve both joints.
The AO/OTA classification is the most comprehensive: Type A = extra-articular; Type B = partial articular; Type C = complete articular. Each is subdivided (A1–A3, B1–B3, C1–C3) based on complexity and comminution.
Acceptable Reduction Parameters
| Parameter | Acceptable | Normal |
|---|---|---|
| Radial inclination | >15° | 22–23° |
| Radial height | >7 mm | 11–12 mm |
| Volar tilt | Neutral to 20° volar | 11–12° volar |
| Articular step-off | <2 mm | 0 mm |
| Ulnar variance | <2 mm positive | 0 mm (neutral) |
Treatment
Non-operative: Closed reduction and casting (sugar-tong splint → short arm cast) is appropriate for stable, extra-articular fractures meeting acceptable parameters in low-demand patients. Reduction technique: finger traps with 10–15 lbs traction, recreate the deformity, then reduce. Immobilize 4–6 weeks. Follow-up radiographs at 1, 2, and 6 weeks — displacement commonly recurs in the first 2 weeks.
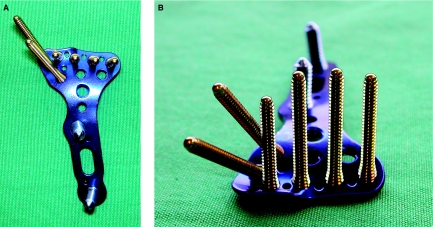
Operative (ORIF): Volar locking plate fixation is the current standard for unstable fractures. Indications: intra-articular displacement >2 mm, dorsal tilt >10°, radial shortening >3 mm, fractures that cannot be maintained in a cast, associated carpal injuries. The volar (Henry) approach between FCR and radial artery provides access to the volar surface. The watershed line on the volar distal radius is the most distal extent of the volar cortex — plates placed distal to this line risk FPL rupture from tendon irritation. PMID: 16264065
Complications of Distal Radius Fractures
| Complication | Incidence | Management |
|---|---|---|
| Malunion | 5–15% (higher with casting alone) | Corrective osteotomy if symptomatic; volar opening wedge + structural bone graft + volar plate |
| EPL rupture | 1–5% (2–3 months after injury) | Attritional rupture over Lister's tubercle; EIP to EPL tendon transfer (repair not possible) |
| Median neuropathy (acute CTS) | 0.5–8% | Urgent carpal tunnel release |
| CRPS | 7–37% | Early hand therapy; vitamin C prophylaxis (500 mg/day); stellate ganglion block if refractory |
| Tendon irritation/rupture (FPL) | 2–12% (volar plate) | Plate placed distal to watershed line; hardware removal + tendon reconstruction |
| DRUJ instability | 10–15% | Fix radius first; reassess DRUJ; TFCC repair if unstable |
06 Scaphoid Fractures
Blood Supply & AVN Risk
The scaphoid has a retrograde blood supply from the dorsal branch of the radial artery, which enters the dorsal ridge and supplies 70–80% of the bone in a distal-to-proximal direction. This makes proximal pole fractures highly susceptible to avascular necrosis (AVN) — AVN rate: proximal pole 30–40%, waist 10–20%, distal pole <5%. The volar scaphoid branch supplies only the distal 20–30%.
Classification
The Herbert classification divides scaphoid fractures into:
| Type | Description | Treatment |
|---|---|---|
| A1 | Tubercle fracture | Short arm thumb spica cast 4–6 weeks |
| A2 | Incomplete waist fracture | Thumb spica cast 8–12 weeks |
| B1 | Distal oblique fracture | Cast or percutaneous screw |
| B2 | Complete waist fracture | Percutaneous or open screw fixation |
| B3 | Proximal pole fracture | Open reduction + headless compression screw |
| B4 | Trans-scaphoid perilunate fracture-dislocation | Emergency ORIF + ligament repair |
| C | Delayed union | Screw fixation ± bone graft |
| D1 | Fibrous nonunion | ORIF + bone graft |
| D2 | Sclerotic nonunion (pseudarthrosis) | Vascularized bone graft (1,2 ICSRA) |
Occult Fracture Management
Clinical suspicion (anatomic snuffbox tenderness, scaphoid tubercle tenderness, pain with axial loading of thumb) with negative initial radiographs requires: thumb spica immobilization and repeat radiographs in 10–14 days, or advanced imaging. MRI is the gold standard for early detection (sensitivity 100%, specificity 99% after 24 hours). CT provides excellent fracture detail but may miss non-displaced fractures early. Bone scan is sensitive but non-specific.
Surgical Fixation
Percutaneous screw fixation (headless compression screw — Herbert, Acutrak, or similar) is indicated for displaced waist fractures (>1 mm displacement), proximal pole fractures, and in athletes/laborers desiring faster return to activity. The screw is placed along the central axis of the scaphoid for maximum purchase. Open reduction is required for displaced fractures, comminution, or associated ligament injuries.
Nonunion & Bone Grafting
Scaphoid nonunion occurs in 5–10% of treated waist fractures and up to 30–40% of untreated fractures. Progressive nonunion leads to SNAC (scaphoid nonunion advanced collapse) wrist. Grafting options: Matti-Russe technique (corticocancellous iliac crest graft), 1,2 intercompartmental supraretinacular artery (1,2 ICSRA) vascularized bone graft for proximal pole AVN — brings vascularized bone from the distal radius with a pedicle from the 1,2 ICSRA branch of the radial artery. PMID: 10073964
07 Metacarpal Fractures
Boxer's Fracture (5th Metacarpal Neck)
The most common metacarpal fracture, typically from a closed-fist punch. Presents with loss of the 5th knuckle prominence and pain with grip. Acceptable angulation varies by digit:
| Metacarpal | Acceptable Neck Angulation | Rationale |
|---|---|---|
| 2nd (index) | 10–15° | Minimal CMC motion; poor compensation |
| 3rd (long) | 10–15° | Minimal CMC motion; poor compensation |
| 4th (ring) | 20–30° | Moderate CMC motion |
| 5th (small) | 40–50° (up to 70° in some literature) | 30° CMC flexion-extension compensates |
Treatment of isolated boxer's fracture meeting acceptable angulation: ulnar gutter splint with MCP at 70–90° (intrinsic-plus position) for 3–4 weeks. Buddy taping and early motion at 3 weeks. Surgical indications: angulation exceeding acceptable limits, rotational malalignment (any degree), open fracture, or multiple metacarpal fractures.
Bennett Fracture (1st MC Base)
An intra-articular fracture-dislocation of the base of the first metacarpal. The volar-ulnar fragment remains attached to the trapezium by the anterior oblique (beak) ligament while the metacarpal shaft is pulled proximally and radially by the APL. Always requires operative fixation (closed reduction and percutaneous K-wire fixation or ORIF with screws) because the joint is incongruent. Articular step-off >1 mm is associated with post-traumatic arthritis.
Rolando Fracture
A comminuted intra-articular fracture of the first metacarpal base (three-part Y or T pattern, or more). Worse prognosis than Bennett fracture. Treatment: ORIF if fragments are large enough to fix; external fixation with ligamentotaxis for highly comminuted fractures.
Metacarpal Shaft Fractures
Acceptable angulation for shaft fractures is approximately 10° less than for neck fractures. No rotational malalignment is acceptable — assess by evaluating the finger cascade and nail plate alignment. Fixation options: K-wires, lag screws, plate and screws (dorsal plating), or intramedullary fixation. Dorsal plating provides the most rigid fixation but may cause extensor tendon adhesions.
08 Phalangeal Fractures & Dislocations
PIP Joint Dislocations
Dorsal dislocation (most common — ~80%): The middle phalanx displaces dorsally. Mechanism: hyperextension. The volar plate ruptures distally from the middle phalanx. Treatment: closed reduction (traction + flexion), buddy taping, early motion. Assess for fracture-dislocation (if >30–40% of articular surface, the joint is unstable in extension). Stable if concentric reduction maintained in <30° flexion.
Volar dislocation (uncommon, serious): Middle phalanx displaces volarly. Implies central slip rupture — Emergency risk of boutonnière deformity. Treatment: reduce, splint PIP in full extension for 6 weeks with DIP free (to allow lateral band gliding).
Lateral dislocation: Implies collateral ligament disruption. If stable after reduction: buddy taping. If grossly unstable: may need operative repair or pinning.
Mallet Finger
Disruption of the terminal extensor tendon at the DIP joint. Presents with DIP flexion lag (inability to actively extend DIP). Two types: tendinous mallet (tendon rupture only) and bony mallet (avulsion fracture of the dorsal base of the distal phalanx).
The Doyle classification: Type I = closed, with or without small avulsion; Type II = open (laceration); Type III = open (deep abrasion with skin and tendon loss); Type IV = subdivided into IVa (epiphyseal fracture in children), IVb (hyperflexion with >20–50% articular surface), IVc (hyperextension with >20–50% articular surface + volar subluxation of distal phalanx).
Treatment: Tendinous mallet — continuous DIP extension splinting for 6–8 weeks (Stack splint or aluminum foam), followed by 4–6 weeks of night splinting. Bony mallet with <30% articular involvement and no subluxation — extension splinting. Bony mallet with >30% articular surface or volar subluxation of the distal phalanx — operative fixation (extension block pinning per Ishiguro technique or ORIF).
Gamekeeper's / Skier's Thumb (UCL Injury)
Injury to the ulnar collateral ligament of the thumb MCP joint. Gamekeeper's thumb = chronic (repetitive stress); skier's thumb = acute (forced radial deviation). Clinical test: stress the UCL at 0° and 30° MCP flexion. Laxity >30° absolute or >15° compared to contralateral side indicates complete tear.
The Stener lesion occurs when the torn UCL displaces superficial to the adductor aponeurosis (present in ~80% of complete tears). The interposed aponeurosis prevents healing — surgical repair or reconstruction is mandatory. Partial tears (grade I–II): thumb spica cast for 4–6 weeks. Complete tears without Stener: cast or surgery depending on patient factors. Complete tears with Stener: surgery always required.
Pilon Fractures of the PIP Joint
High-energy axial load injuries causing comminuted depression of the base of the middle phalanx. Treatment depends on fragment size: if reconstructable, ORIF with mini-screws; if highly comminuted, dynamic external fixation (Suzuki frame or compass hinge) with ligamentotaxis to maintain length and alignment while allowing early motion.
09 Carpal Instability & Perilunate Injuries
Scapholunate Dissociation
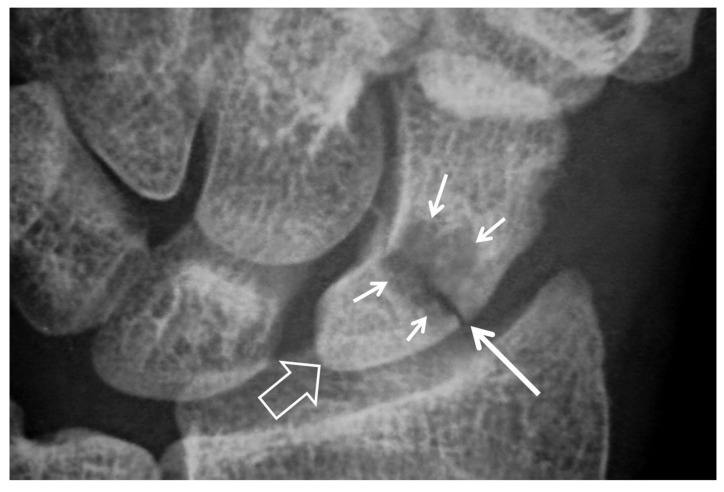
The most common carpal instability pattern. Disruption of the scapholunate ligament allows the scaphoid to flex and the lunate to extend, producing a DISI (dorsal intercalated segment instability) pattern (SL angle >70° on lateral radiograph; normal = 45–60°). Radiographic findings on PA view: Terry Thomas sign (SL gap >3 mm), scaphoid ring sign (cortical ring appearance from flexed scaphoid on PA), and scaphoid cortical ring distance <7 mm.
Treatment by stage: Acute complete tear — open repair with dorsal capsulodesis and K-wire fixation. Chronic without arthritis — ligament reconstruction (e.g., modified Brunelli tenodesis, SLAM procedure, or scapholunate axis method). Chronic with arthritis — proceeds to SLAC wrist treatment algorithm (see Section 10).
VISI Pattern
Results from lunotriquetral ligament disruption. The lunate flexes volarly (capitolunate angle >15°, SL angle <30°). Less common and generally less disabling than DISI. Often responds to immobilization; if persistent, LT ligament repair or LT arthrodesis may be indicated.
Perilunate Dislocations & Fracture-Dislocations
A Emergency spectrum of high-energy carpal injuries described by the Mayfield classification:
| Stage | Pathology | Key Finding |
|---|---|---|
| I | Scapholunate dissociation | SL ligament rupture; scaphoid flexion |
| II | Perilunate dislocation (capitolunate disruption) | Capitate dislocates dorsally from lunate |
| III | Lunotriquetral disruption added | LT ligament torn; progressive midcarpal disruption |
| IV | Lunate dislocation | Lunate rotates/displaces volarly into carpal tunnel; "spilled teacup" on lateral |
Key radiographic finding on lateral: in perilunate dislocation, the lunate stays aligned with the radius but the capitate dislocates dorsally. In lunate dislocation, the capitate is aligned with the radius but the lunate displaces volarly. Both are commonly missed on initial presentation (up to 25% diagnostic delay).
Treatment: emergent closed reduction (traction + wrist extension then flexion) to decompress the carpal tunnel, followed by definitive open surgical treatment — combined dorsal and volar approach for ligament repair + K-wire fixation. Persistent lunate dislocation causes acute carpal tunnel syndrome.
10 Wrist Arthritis — SNAC & SLAC
SLAC Wrist (Scapholunate Advanced Collapse)
The most common pattern of wrist arthritis, resulting from chronic scapholunate ligament incompetence. Predictable progression:
| Stage | Arthritic Location | Treatment Options |
|---|---|---|
| I | Radial styloid — scaphoid | Radial styloidectomy + SL pinning or capsulodesis |
| II | Entire radioscaphoid joint | Scaphoid excision + 4-corner fusion (4CF) or proximal row carpectomy (PRC) |
| III | Radioscaphoid + capitolunate | Scaphoid excision + 4CF (PRC contraindicated due to capitate head arthritis) |
| IV | Pancarpal arthritis | Total wrist arthrodesis or total wrist arthroplasty |
SNAC Wrist (Scaphoid Nonunion Advanced Collapse)
Same arthritic progression as SLAC but caused by scaphoid nonunion rather than SL ligament disruption. The nonunion site (usually the waist) acts as the pathologic hinge. Treatment follows the same stage-based algorithm as SLAC. The key difference: in Stage I SNAC, addressing the scaphoid nonunion (ORIF + bone graft) may halt progression if articular cartilage is preserved.
Proximal Row Carpectomy vs Four-Corner Fusion
PRC: Excision of scaphoid, lunate, and triquetrum. The capitate articulates directly with the lunate fossa of the radius. Advantages: single procedure, preserves some wrist motion (~50% of normal), no risk of nonunion. Contraindication: capitate head articular cartilage loss (Stage III). Requires intact capitate articular cartilage (inspect intraoperatively).
Four-corner fusion (4CF): Scaphoid excision + fusion of capitate, lunate, triquetrum, and hamate (with circular plate or K-wires + bone graft). Preserves ~50% of wrist motion through the radiocarpal joint. Can be used in Stage III. Nonunion rate 3–10%. PMID: 15888095
Thumb CMC Arthritis (Basal Joint Arthritis)
The most common site of hand arthritis in women over age 50. The Eaton-Littler classification stages the disease:
| Stage | Radiographic Finding | Treatment |
|---|---|---|
| I | Normal joint; may have widening from effusion | Splinting, NSAIDs, corticosteroid injection (1 mL triamcinolone 40 mg) |
| II | Slight joint space narrowing; osteophytes <2 mm; subluxation <1/3 | Above + volar ligament reconstruction, metacarpal extension osteotomy |
| III | Joint space loss; osteophytes >2 mm; subluxation >1/3; sclerosis/cysts | Trapeziectomy + LRTI (ligament reconstruction tendon interposition using FCR), or suture-button suspensionplasty |
| IV | Stage III + STT (scaphotrapeziotrapezoid) arthritis | Complete trapeziectomy + LRTI; or CMC arthrodesis (young laborer) |
Trapeziectomy + LRTI: The most commonly performed procedure. The entire trapezium is excised, and the FCR tendon (half or full) is used to reconstruct the volar beak ligament and fill the dead space ("anchovy" interposition). Postoperative: thumb spica cast 4–6 weeks, then progressive ROM and strengthening. Expected outcomes: pain relief in 90–95%; 10–20% loss of pinch strength compared to normal; proximal metacarpal migration is common but rarely symptomatic. PMID: 15136539
Alternative procedures: suture-button suspensionplasty (TightRope — creates a suspensory sling between the 1st and 2nd metacarpal bases after trapeziectomy; avoids sacrificing the FCR tendon; early results comparable to LRTI), CMC arthrodesis (fusion of the trapeziometacarpal joint at ~35° abduction, 15° extension, 10° pronation; best for young, high-demand patients; sacrifice of motion traded for stability and strength; nonunion rate 8–15%), and CMC arthroplasty (pyrocarbon interposition or total joint replacement; reserved for low-demand elderly patients).
11 DRUJ Injuries & TFCC Tears
TFCC Anatomy & Palmer Classification
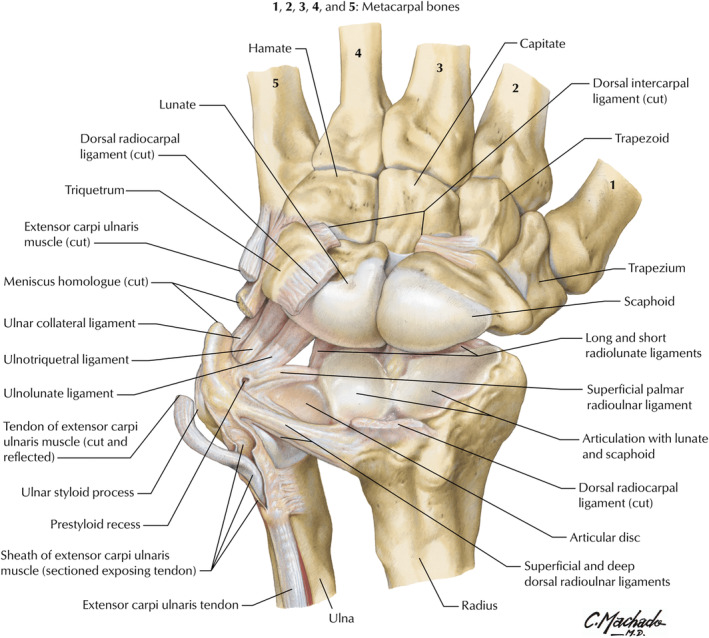
The triangular fibrocartilage complex consists of the articular disc (TFC proper), dorsal and volar radioulnar ligaments, meniscus homologue, ulnocarpal ligaments (ulnolunate, ulnotriquetral), and ECU subsheath. It is the primary stabilizer of the DRUJ and bears 20% of axial load (increasing with positive ulnar variance).
| Palmer Classification of TFCC Tears | |
|---|---|
| Class | Description |
| Class 1 — Traumatic | |
| 1A | Central perforation (avascular zone) — arthroscopic debridement |
| 1B | Ulnar avulsion ± ulnar styloid fracture — peripheral repair (best healing potential due to vascularity) |
| 1C | Distal avulsion (ulnocarpal ligaments) — repair |
| 1D | Radial avulsion ± sigmoid notch fracture — reattachment to radius |
| Class 2 — Degenerative (Ulnar Impaction Syndrome) | |
| 2A | TFCC wear |
| 2B | TFCC wear + lunate chondromalacia |
| 2C | TFCC perforation + lunate chondromalacia |
| 2D | TFCC perforation + lunate chondromalacia + LT ligament perforation |
| 2E | TFCC perforation + lunate chondromalacia + LT perforation + ulnocarpal arthritis |
DRUJ Instability
Assessment: compare translation of the distal ulna relative to the radius with the forearm in neutral, pronation, and supination (compare to contralateral side). The "piano key" test assesses dorsal DRUJ instability. CT scan in pronation and supination (bilateral comparison) is the most reliable imaging for DRUJ instability.
Treatment: acute DRUJ instability with distal radius fracture — fix the radius first, then reassess DRUJ stability. If still unstable: immobilize in supination (if dorsal instability) for 4–6 weeks with sugar-tong splint or repair TFCC. Chronic DRUJ instability: TFCC repair or reconstruction (Adams-Berger procedure using palmaris longus graft).
Essex-Lopresti Injury
A Emergency triad of: radial head fracture + interosseous membrane disruption + DRUJ instability. The radial head must NOT be excised without replacement (metallic radial head arthroplasty is mandatory) to prevent proximal migration of the radius. Missed diagnosis leads to chronic wrist pain and progressive DRUJ arthritis.
Ulnar Impaction Syndrome
Chronic loading of the ulnar carpus due to positive ulnar variance (long ulna relative to radius). Causes TFCC degeneration (Palmer Class 2 tears), chondromalacia of the lunate and/or triquetrum, and LT ligament attenuation. Presents with ulnar-sided wrist pain exacerbated by grip and ulnar deviation. Diagnosis: PA radiograph (ulnar variance ≥2 mm positive), MRI (TFCC tear + lunate edema/chondromalacia). Treatment: ulnar shortening osteotomy (2–4 mm shortening of the ulnar shaft with plate fixation) is the workhorse procedure. Arthroscopic TFCC debridement alone is insufficient if ulnar variance is positive — must address the underlying cause. Alternative: wafer procedure (arthroscopic distal ulna resection of 2–4 mm).
Salvage Procedures
Darrach procedure: Distal ulna resection. Best for low-demand elderly patients. Complication: painful radioulnar convergence with grip ("Darrach stump impingement"). Sauvé-Kapandji procedure: DRUJ fusion + proximal ulna pseudarthrosis (creates a "proximal DRUJ"). Maintains ulnar head as a buttress. Better for young/active patients. Ulnar head replacement: Prosthetic replacement preserving forearm stability.
12 Flexor Tendon Injuries
Zone II — "No Man's Land"
Zone II (from A1 pulley to FDS insertion) is the most challenging zone for flexor tendon repair because both FDP and FDS travel within the tight fibro-osseous sheath. Historically, primary repair in Zone II had poor results (hence the name "no man's land" coined by Bunnell), but modern repair techniques and rehabilitation protocols have dramatically improved outcomes.
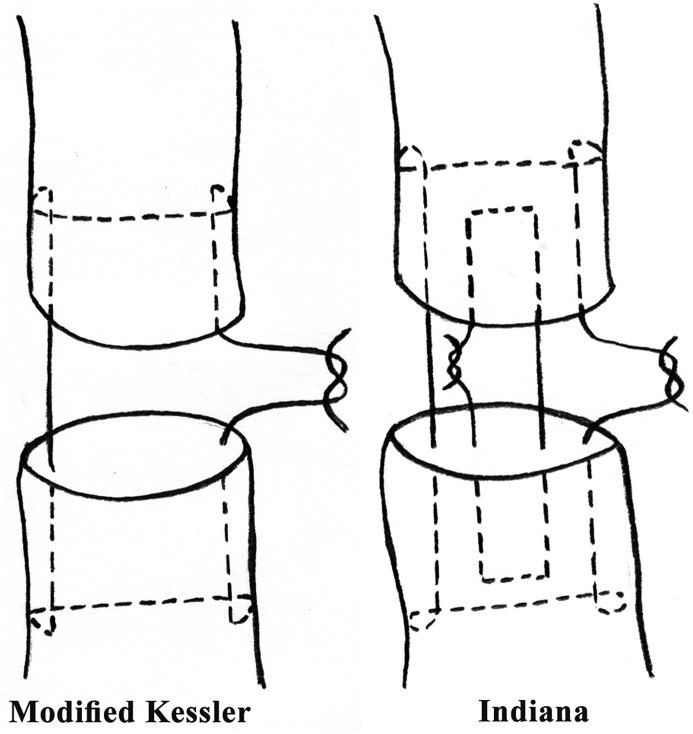
Repair Techniques
Current standard of care demands a strong core suture (minimum 4-strand, ideally 6-strand) combined with a running epitendinous (peripheral) suture. Repair strength is directly proportional to the number of core strands crossing the repair site:
| Repair | Strands | Gap Resistance (N) | Clinical Use |
|---|---|---|---|
| Modified Kessler | 2 | ~20–25 N | Historical standard; rarely used alone now |
| Cruciate | 4 | ~40–50 N | Good strength; commonly used |
| Adelaide (cross-stitch) | 4 | ~45–55 N | Excellent gap resistance |
| Savage | 6 | ~60–70 N | Strongest single-technique repair |
| 4-strand + epitendinous | 4 + running | ~55–65 N | Epitendinous adds 10–50% to strength |
Key principles: (1) core suture purchases should be ≥7–10 mm from the cut end; (2) locking loops are stronger than grasping loops; (3) 3-0 or 4-0 braided polyester (Ethibond) or polypropylene for core suture; (4) 5-0 or 6-0 running epitendinous suture; (5) repair both FDP and FDS if possible, though one slip of FDS may be excised to reduce bulk in Zone II. PMID: 15888090
Jersey Finger (Zone I FDP Avulsion)
FDP avulsion from the distal phalanx, typically the ring finger (75% of cases). Mechanism: forced extension of the DIP while actively flexing (grabbing a jersey). Leddy and Packer classification:
| Type | Retraction Level | Vinculum Status | Treatment Timeline |
|---|---|---|---|
| I | Palm | Both vincula ruptured | Repair within 7–10 days (tendon loses blood supply) |
| II | PIP joint (most common) | Long vinculum intact | Repair within weeks (tendon has blood supply) |
| III | DIP joint (bony avulsion fragment caught at A4/A5) | Both vincula intact | Repair within weeks; ORIF of fragment |
Rehabilitation Protocols
Duran passive motion protocol: Passive flexion and extension exercises within a dorsal blocking splint (wrist 30° flexion, MCP 50–70° flexion) starting 3–5 days post-repair. Minimizes adhesion formation while protecting the repair. Kleinert rubber band traction: Dynamic rubber band from fingertip to volar forearm provides passive flexion; patient actively extends against the band. Early active motion (EAM): Place and hold exercises within protective splint starting at 3–5 days. Requires a strong repair (≥4-strand core). Lowest adhesion rate but highest re-rupture risk (4–6% vs 1–2% with passive protocols). EAM is the current preferred protocol when repair strength is adequate.
13 Extensor Tendon Injuries
Mallet Finger (Zone I)
Terminal extensor tendon disruption at the DIP joint. Tendinous mallet: continuous DIP extension splinting (Stack splint) for 6–8 weeks; full-time followed by 4–6 weeks night splinting. Success rate 80–90% with compliant splinting. If the DIP is allowed to flex even once during the treatment period, the 6–8 week clock resets. Chronic mallet (>12 weeks) may still respond to splinting. Swan-neck deformity (PIP hyperextension + DIP flexion) can develop as a late complication from volar plate laxity at the PIP.
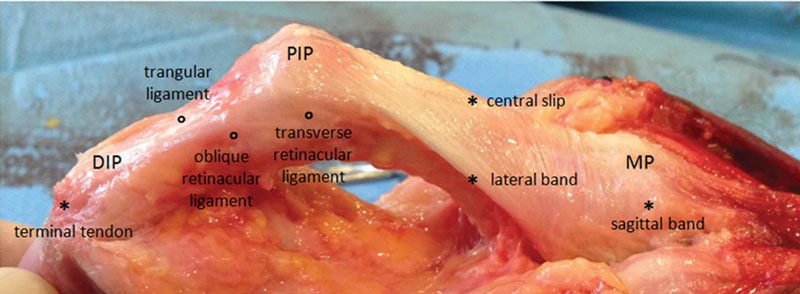
Boutonnière Deformity (Zone III)
Central slip disruption at the PIP joint allows the lateral bands to migrate volarly, becoming PIP flexors instead of extensors. Classic deformity: PIP flexion + DIP hyperextension. The Elson test (described in Section 4) detects acute central slip injury before the deformity develops.
Acute treatment: splint PIP in full extension for 6 weeks with the DIP free for active flexion exercises (to keep lateral bands gliding dorsally). Surgical indications: displaced bony avulsion of the central slip, irreducible PIP dislocation, failed conservative treatment. Chronic boutonnière with supple PIP: terminal tendon tenotomy (Fowler procedure) or central slip reconstruction. Fixed PIP contracture: requires serial casting/splinting or surgical release before tendon reconstruction.
Sagittal Band Rupture (Zone V)
The sagittal bands center the extensor tendon over the MCP joint. Rupture (usually radial side of the long finger) allows the extensor to subluxate ulnarly, causing inability to initiate MCP extension from the flexed position (but can maintain extension once passively started). Acute: extension splinting of MCP for 4–6 weeks. Chronic: surgical repair or reconstruction using juncturae tendinae or extensor retinaculum graft.
Fight Bite (Zone V Open Injury)
A Emergency human tooth puncture wound over the MCP joint (from a closed-fist punch to the mouth). The wound penetrates the extensor tendon and may violate the MCP joint capsule. Must be treated as a contaminated joint injury: irrigation and debridement in the OR, IV antibiotics (ampicillin-sulbactam or piperacillin-tazobactam to cover Eikenella corrodens, streptococci, staphylococci, and oral anaerobes). Never close primarily. Delayed tendon repair after infection is controlled.
14 Tendon Transfers
Principles
Essential requirements for a successful tendon transfer: (1) expendable donor — loss of the donor tendon should not cause unacceptable functional deficit; (2) adequate strength — a transferred muscle loses approximately one grade of strength (thus donor must be ≥M4); (3) synergistic motion — muscles that normally fire simultaneously with the desired action are easier to re-train (e.g., wrist extensors synergistic with finger flexors); (4) straight line of pull — the transfer should cross the fewest joints and run the most direct course; (5) one tendon = one function; (6) adequate excursion (wrist motors ~33 mm, finger extensors ~50 mm, finger flexors ~70 mm); (7) supple joints with full passive ROM (no contractures); (8) stable soft tissue bed.
Transfers for Radial Nerve Palsy (High)
Loss: wrist extension, finger MCP extension, thumb extension/abduction. Standard transfers:
| Lost Function | Transfer | Alternative |
|---|---|---|
| Wrist extension | PT → ECRB | FCU → ECRB (less preferred, loses dart-throwing motion) |
| Finger extension | FCR → EDC | FDS (ring, long) → EDC |
| Thumb extension | PL → rerouted EPL | FDS (ring) → EPL |
Transfers for Ulnar Nerve Palsy (Low)
Loss: interossei, hypothenar muscles, adductor pollicis, lumbricals 3–4. Problems: clawing (ring/small > index/long because intact lumbricals 1–2 prevent index/long clawing), weak pinch (Froment's sign), loss of power grip. Transfers:
| Problem | Transfer |
|---|---|
| Claw correction | FDS (ring) → lateral bands of ring and small (Stiles-Bunnell; Brand modification: through lumbrical canal, insert into lateral bands of all 4 fingers) |
| Thumb adduction (Froment's) | ECRB + tendon graft → adductor pollicis insertion; or FDS (ring) → adductor insertion; or brachioradialis → adductor |
| First dorsal interosseous | EIP → 1st dorsal interosseous insertion (for index abduction) |
Opponensplasty (Median Nerve Palsy)
Loss of thumb opposition (abductor pollicis brevis, opponens pollicis). Common donor options: FDS ring finger (Royle-Thompson transfer — passed through a pulley at the FCU insertion or pisiform), EIP (Burkhalter transfer), ADM (Huber transfer — particularly useful in children and congenital thumb hypoplasia because it adds bulk to the thenar eminence). The transfer must be routed around the ulnar border of the hand to achieve the correct vector for opposition (pronation + abduction + flexion).
15 Trigger Finger & De Quervain Tenosynovitis
Trigger Finger (Stenosing Tenosynovitis)
A1 pulley stenosis causes mechanical catching/locking of the finger during flexion-extension. Most common in the ring finger and thumb. Associated with diabetes (up to 10% prevalence), rheumatoid arthritis, repetitive gripping. The Green classification: Grade I = pain/tenderness at A1 pulley without catching; Grade II = catching, passively correctable; Grade III = locking, requiring active force or passive manipulation to unlock; Grade IIIA (can actively extend), IIIB (passively extended); Grade IV = fixed flexion contracture.
Injection technique: 1 mL of corticosteroid (betamethasone 6 mg/mL or triamcinolone 40 mg/mL) mixed with 0.5–1 mL of 1% lidocaine injected into the tendon sheath at the A1 pulley. Success rate: 57–93% after single injection; up to 3 injections over 6 months before considering surgery. Diabetic patients have lower response rates (~50%). Surgical release: longitudinal incision over A1 pulley, identify and protect the digital nerves (especially the radial digital nerve of the thumb, which crosses over the A1 pulley), release A1 pulley completely.
Trigger Thumb in Children
Presents as a flexed IP joint (Notta's node — thickening of FPL at A1 pulley). Not congenital — it is an acquired condition that may present in infancy. 30% resolve spontaneously by age 1 year; observation until age 3–4 years is reasonable. If persistent, surgical A1 pulley release (oblique incision at the thumb MCP crease). Protect the digital nerves, which are more superficial and radially displaced in children.
De Quervain Tenosynovitis
Stenosing tenosynovitis of the first dorsal compartment (APL and EPB). More common in women, new mothers (repetitive lifting), and patients with inflammatory arthritis. Diagnosis: positive Finkelstein test (pain with ulnar deviation of the wrist while the thumb is grasped in the fist).
Subsheath variants: In up to 40% of individuals, the first dorsal compartment contains a septum (subcompartment) separating the EPB from the APL. During surgical release, both subcompartments must be released — failure to identify and release the EPB subcompartment is the most common cause of surgical failure.
Treatment: thumb spica splint, NSAIDs, corticosteroid injection (up to 80% response). Surgical release if conservative measures fail: longitudinal incision over the first dorsal compartment, identify and protect the superficial branch of the radial nerve (multiple branches cross the surgical field), release the retinaculum, inspect for and release any subsheath.
16 Tendon Reconstruction & Tenolysis
Staged Flexor Tendon Reconstruction
Indicated when primary repair has failed or is not possible (delayed presentation, scarred tendon bed, absent pulley system). The Hunter rod technique (two-stage reconstruction):
Stage 1: Insert a silicone (Hunter) rod through the tendon sheath to form a pseudosheath. Reconstruct deficient pulleys (A2 and A4 at minimum) using extensor retinaculum, tendon graft, or volar plate remnants. Allow 3–6 months for the pseudosheath to mature around the rod.
Stage 2: Remove the rod and pass a tendon graft (palmaris longus, plantaris, or toe extensor) through the new sheath. Distal attachment by weave or bone anchor into the distal phalanx. Proximal juncture outside the sheath in the forearm. Begin controlled motion protocol.
Pulley Reconstruction
If A2 or A4 pulleys are absent, reconstruction is required before or simultaneously with tendon grafting. Techniques: extensor retinaculum graft wrapped around the phalanx (Weilby technique), a rim of the volar plate, or a loop of tendon graft (e.g., palmaris longus). The reconstructed pulley should be at least 1 cm wide.
Tenolysis
Indicated when a repaired or grafted tendon has adequate continuity and strength but poor gliding due to adhesions. Timing: typically ≥3–6 months after repair, once soft tissues are supple and joints have full passive ROM. Performed under local anesthesia (wide-awake surgery — WALANT technique) so the patient can actively demonstrate tendon glide intraoperatively. If the tendon does not glide after adhesion release, the repair may be deficient, and staged reconstruction may be needed.
17 Carpal Tunnel Syndrome
Clinical Presentation & Diagnosis
The most common peripheral nerve compression. Median nerve entrapment beneath the transverse carpal ligament. Classic presentation: nocturnal paresthesias in the thumb, index, long, and radial half of ring finger; thenar atrophy (late); decreased grip/pinch strength. Provocative tests: Phalen's (68% sensitivity), Tinel's (50%), Durkan's (87%). The "flick sign" (shaking the hand to relieve symptoms) is 93% sensitive.
Electrodiagnostic Criteria
| Parameter | Normal | CTS Threshold | Notes |
|---|---|---|---|
| Median motor distal latency (DML) | <4.2 ms | >4.2 ms | Recording from APB |
| Median sensory NCV (wrist to digit) | >50 m/s | <50 m/s | Most sensitive single test |
| Median SNAP amplitude | >20 µV | Reduced or absent | Indicates axonal loss |
| Median-ulnar sensory latency difference | <0.4 ms | >0.5 ms | Most sensitive comparison study |
| EMG (thenar muscles) | No denervation | Fibrillations, positive sharp waves | Indicates axonal damage; worse prognosis |
Treatment
Non-operative: Neutral wrist splinting (especially nocturnal), activity modification, corticosteroid injection (80 mg methylprednisolone or 40 mg triamcinolone). Injection provides short-term relief in 70–90% but only 30–40% maintain benefit at 1 year. Best for mild-to-moderate CTS without thenar atrophy or denervation.
Carpal tunnel release (CTR): Definitive treatment. Indications: failed conservative therapy, thenar atrophy, denervation on EMG, severe symptoms. Open CTR: 2–3 cm incision ulnar to thenar crease (in line with radial border of ring finger), divide transverse carpal ligament under direct vision. Success rate 85–95%. Endoscopic CTR: Single or dual portal technique (Agee single-portal or Chow dual-portal). Advantages: less pillar pain, faster return to work (by ~1 week). Disadvantages: higher risk of nerve injury and incomplete release. Both techniques have equivalent long-term outcomes. PMID: 12045855
Recurrent CTS
Occurs in 3–12% of cases. Most common cause: incomplete release of the transverse carpal ligament (especially the distal edge). Evaluation: repeat EMG/NCS, MRI or ultrasound to assess for incomplete release, perineural fibrosis, or space-occupying lesion. Revision surgery: open approach with internal neurolysis, hypothenar fat flap (provides vascularized coverage over the nerve to prevent re-scarring), or synovial flap.
18 Cubital Tunnel Syndrome
Anatomy & Sites of Compression
The second most common upper extremity compression neuropathy. The ulnar nerve passes posterior to the medial epicondyle in the cubital tunnel, whose roof is formed by Osborne's ligament (arcuate ligament of the cubital tunnel — the fascial band between the two heads of the FCU). Other sites of compression: medial intermuscular septum (arcade of Struthers), anconeus epitrochlearis (accessory muscle present in ~11% — a congenital anomaly replacing Osborne's ligament), and the FCU aponeurosis.
Clinical presentation: paresthesias in the small finger and ulnar half of the ring finger, hand clumsiness, weak grip, intrinsic wasting (first dorsal interosseous hollow), Wartenberg's sign, Froment's sign. The elbow flexion test (maximal elbow flexion for 60 seconds reproduces symptoms) is the most sensitive provocative test (sensitivity 75%).
McGowan Grading (Modified by Goldberg)
| Grade | Description |
|---|---|
| I (Mild) | Intermittent paresthesias; no weakness or wasting; normal 2PD |
| IIA (Moderate) | Intermittent paresthesias + weak interossei; no wasting |
| IIB (Moderate) | Intermittent paresthesias + weak interossei + abnormal 2PD (>6 mm) |
| III (Severe) | Persistent paresthesias + muscle wasting + abnormal 2PD + weakness |
Surgical Options
In situ decompression: Release Osborne's ligament and the FCU aponeurosis without moving the nerve. Simplest procedure; lowest complication rate. Best for patients without subluxation of the nerve. Medial epicondylectomy: Remove the medial epicondyle to eliminate the compressive groove. Risk: MCL instability if excessive bone removed. Anterior transposition: Move the nerve anterior to the medial epicondyle. Three variants: subcutaneous (nerve under skin flap), intramuscular (within flexor-pronator mass), and submuscular (deep to the flexor-pronator origin — most reliable decompression but most extensive dissection). PMID: 17079403
19 Radial Tunnel & PIN Syndrome
Radial Tunnel Syndrome
Pain syndrome (without motor deficit) caused by compression of the posterior interosseous nerve within the radial tunnel. The radial tunnel extends from the radial head to the distal edge of the supinator. Five sites of compression: (1) fibrous bands anterior to the radial head, (2) radial recurrent vessels (leash of Henry), (3) tendinous margin of ECRB, (4) arcade of Frohse (most common site — fibrous proximal edge of the superficial head of the supinator), (5) distal edge of the supinator.
Differentiation from lateral epicondylitis: both cause lateral elbow/forearm pain, but radial tunnel syndrome produces maximal tenderness 3–4 cm distal to the lateral epicondyle (over the radial tunnel) rather than at the epicondyle itself. The "middle finger extension test" (pain reproduced by resisted middle finger extension with elbow extended) is suggestive of radial tunnel syndrome because the ECRB tendon compresses the PIN during this maneuver. Note: EMG/NCS are typically normal in radial tunnel syndrome (it is a pain syndrome, not a motor deficit).
Posterior Interosseous Nerve (PIN) Syndrome
A pure motor syndrome caused by compression of the PIN, usually at the arcade of Frohse. Presents with finger drop (inability to extend fingers at MCP joints) and wrist radial deviation with extension (ECRL intact; ECRB variably affected). No sensory loss (the PIN is a pure motor nerve at the level of compression). Distinguish from extensor tendon rupture by demonstrating intact tenodesis effect (passive wrist flexion causes finger extension).
Treatment: observation for 3 months if spontaneous recovery expected (e.g., after lipoma removal, compression neuropathy). Surgical decompression if no recovery: explore the radial tunnel, release the arcade of Frohse, decompress through the supinator. EMG showing denervation in the finger extensors confirms the diagnosis. If no recovery after 6–9 months of decompression, tendon transfers as for radial nerve palsy.
Wartenberg Syndrome
Compression or neuritis of the superficial branch of the radial nerve (SBRN) as it exits between the brachioradialis and ECRL tendons ~8 cm proximal to the radial styloid. Causes dysesthesias and pain over the dorsal first web space and radial wrist. Often iatrogenic (after wrist surgery, De Quervain release, radial artery cannulation) or from tight wristbands/watches. The Tinel sign is typically positive over the nerve course. Differentiate from De Quervain: Wartenberg causes sensory symptoms; De Quervain causes pain with thumb motion. Treatment: wrist splint, activity modification, remove offending compressive source. Surgical decompression of the nerve through the fascial tunnel if conservative measures fail (4–6 months).
Pronator Syndrome
Compression of the median nerve in the proximal forearm at one of four sites: (1) ligament of Struthers (supracondylar process to medial epicondyle), (2) lacertus fibrosus (bicipital aponeurosis), (3) between the two heads of pronator teres (most common), (4) proximal arch of FDS. Presents with forearm aching and median nerve paresthesias. Unlike CTS, pronator syndrome causes numbness in the palmar cutaneous branch territory (thenar eminence — not affected in CTS because the palmar cutaneous branch is superficial to the carpal tunnel). EMG/NCS may be normal or show slowing across the forearm segment. Treatment: rest, splinting, surgical decompression at all four sites if conservative treatment fails.
20 Peripheral Nerve Injury & Repair
Seddon Classification
| Type | Pathology | Recovery |
|---|---|---|
| Neurapraxia | Focal demyelination; axon intact; no Wallerian degeneration | Complete recovery in days to 12 weeks |
| Axonotmesis | Axon disrupted; endoneurium intact; Wallerian degeneration occurs | Spontaneous recovery at ~1 mm/day (1 inch/month); guided by intact endoneurial tubes |
| Neurotmesis | Complete nerve transection; all layers disrupted | No spontaneous recovery; surgical repair required |
Sunderland Classification
| Grade | Structure Damaged | Equivalent | Recovery |
|---|---|---|---|
| I | Myelin only | Neurapraxia | Complete; weeks |
| II | Axon + myelin (endoneurium intact) | Axonotmesis | Complete; months (1 mm/day) |
| III | Axon + endoneurium (perineurium intact) | — | Variable; intrafascicular scarring may impede recovery |
| IV | Entire fascicle (epineurium intact) | — | Neuroma-in-continuity; surgical repair needed |
| V | Entire nerve | Neurotmesis | None; requires surgical repair |
| VI (Mackinnon) | Mixed pattern (combination of I–V in different fascicles) | — | Variable; may need partial repair |
Nerve Repair Principles
Key principles: (1) tension-free repair is paramount — excessive tension is the #1 cause of poor outcomes; (2) fascicular alignment — match motor to motor and sensory to sensory fascicles using intraoperative nerve stimulation and fascicular topography; (3) timing — primary repair (within 72 hours) is ideal; delayed primary repair (up to 7 days) is acceptable; secondary repair after 3–6 months has inferior results; (4) suture technique — epineurial repair (most common; 8-0 or 9-0 nylon) or grouped fascicular repair for larger nerves; (5) if a gap exists and tension-free repair is not possible, use a nerve graft (sural nerve, medial antebrachial cutaneous nerve) or nerve conduit.
Nerve conduits are synthetic or biologic tubes used to bridge nerve gaps. Effective for gaps <3 cm in sensory nerves. Materials: collagen (NeuraGen), polyglycolic acid (Neurotube), processed nerve allograft (Avance — decellularized human cadaveric nerve). Autograft remains the gold standard for gaps >3 cm and motor nerve repairs. Common donor nerves: sural nerve (most common — provides 30–40 cm of graft from the posterolateral calf; causes numbness over the lateral foot), medial antebrachial cutaneous nerve (MABC — provides 8–20 cm; donor site numbness over the medial forearm), and lateral antebrachial cutaneous nerve (LABC — terminal sensory branch of the musculocutaneous nerve). PMID: 24003181
Nerve Regeneration & Recovery
After axonotmesis or neurotmesis with repair, axonal regeneration proceeds at approximately 1 mm/day (1 inch/month). Recovery time is calculated by measuring the distance from the repair site to the target muscle or sensory end-organ. A Tinel sign advancing at the expected rate indicates active regeneration. Failure of Tinel advancement by 3–4 months post-repair suggests poor regeneration and may warrant revision. Motor end plates degenerate after 12–18 months of denervation — this is the "window" for reinnervation. Sensory end-organs survive longer (up to 3–5 years), allowing later sensory recovery even with delayed repair.
Nerve Transfers
Transfer of a functioning but expendable donor nerve (or fascicle) to a denervated recipient nerve. Advantages over grafting: places the nerve coaptation site closer to the target muscle (shorter reinnervation distance), avoids donor site morbidity of a long graft, and allows reinnervation even when the proximal nerve is unavailable (e.g., root avulsion). Key examples in upper extremity: Oberlin transfer (see Section 21), AIN to PIN transfer (for radial nerve palsy), median to musculocutaneous nerve transfer (for biceps reinnervation).
21 Brachial Plexus Injuries
Anatomy
The brachial plexus is formed from the ventral rami of C5–T1, organized as: Roots → Trunks → Divisions → Cords → Branches (mnemonic: "Robert Taylor Drinks Cold Beer"). Three trunks: upper (C5–C6), middle (C7), lower (C8–T1). Each trunk divides into anterior and posterior divisions. Three cords named by relationship to the axillary artery: lateral (anterior divisions of upper and middle trunks), posterior (all posterior divisions), medial (anterior division of lower trunk).
Injury Patterns
| Pattern | Roots | Deficit | Eponym |
|---|---|---|---|
| Upper plexus | C5–C6 | Shoulder abduction/ER, elbow flexion, forearm supination; "waiter's tip" | Erb-Duchenne palsy |
| Extended upper | C5–C7 | Above + wrist/finger extension | — |
| Lower plexus | C8–T1 | Hand intrinsics, finger/wrist flexion; claw hand | Klumpke palsy |
| Total plexus | C5–T1 | Flail arm | — |
Preganglionic vs Postganglionic
Preganglionic (root avulsion): injury at or proximal to the dorsal root ganglion. Signs: Horner syndrome (T1 avulsion), winged scapula (long thoracic nerve — C5,6,7), paralyzed hemidiaphragm (phrenic nerve — C3,4,5), pseudomeningoceles on MRI, preserved SNAP despite clinical sensory loss (the dorsal root ganglion is intact, so the sensory axon does not undergo Wallerian degeneration). Root avulsion cannot be repaired directly — requires nerve transfers.
Postganglionic: injury distal to the DRG. SNAP is absent (Wallerian degeneration occurs). Can be treated with nerve repair, grafting, or transfers.
Timing & Surgical Strategy
Closed injuries: observe for 3–6 months for spontaneous recovery (Tinel's sign advancement). If no recovery by 3–6 months: surgical exploration. Open/sharp injuries: early exploration and repair (within 72 hours if clean laceration). Priorities for reconstruction: (1) elbow flexion, (2) shoulder stability/abduction, (3) hand function.
Oberlin Transfer
The Oberlin transfer (nerve transfer for elbow flexion): transfer a redundant fascicle from the ulnar nerve (specifically, the FCU fascicle) directly to the biceps motor branch of the musculocutaneous nerve. This is a short-distance transfer performed at the mid-arm level, allowing rapid reinnervation of the biceps (mean recovery time 5–7 months). Results: M4 or greater biceps strength in 80–90% of patients. The double Oberlin (Mackinnon modification) adds a median nerve fascicle (FCR fascicle) to the brachialis branch for stronger elbow flexion. PMID: 8120971
22 Digital Nerve Injuries
Repair Technique
Digital nerves are mixed nerves (predominantly sensory in the digits) with a diameter of ~1.5–2 mm. Repair is indicated for all clean lacerations. Technique: identify the nerve ends under loupe magnification (3.5× or 4.5×), trim the ends back to healthy fascicular pattern, and perform epineurial repair with 2–3 interrupted sutures of 9-0 or 10-0 nylon under no tension. If a gap exists, options include: nerve conduit for gaps <3 cm (collagen, PGA, or processed nerve allograft), or autograft (posterior interosseous nerve, medial antebrachial cutaneous nerve) for gaps >3 cm.
Outcomes
Results of digital nerve repair: static 2PD <10 mm in 50–70% of adults, with better outcomes in younger patients. Factors affecting recovery: age (children <10 have the best outcomes), mechanism (clean laceration > crush > avulsion), level of injury (more distal = better), timing (primary repair > delayed). Sensory re-education protocols improve functional outcomes after nerve repair.
Digital Nerve Block Techniques
Traditional digital block: Inject 1–2 mL of 1% or 2% lidocaine (with or without epinephrine) on each side of the finger base at the level of the web space, targeting the proper digital nerves. Use a 25- or 27-gauge needle. Block both radial and ulnar digital nerves. Onset: 3–5 minutes. Duration: 1–2 hours (without epinephrine), 2–4 hours (with epinephrine).
Transthecal (flexor sheath) block: Single volar injection into the flexor tendon sheath at the level of the palmar digital crease. The anesthetic diffuses through the sheath to both digital nerves. Advantages: single injection, faster, less painful. Inject 2–3 mL of 1% lidocaine with resistance (into the sheath, not the tendon).
Metacarpal block: Injection at the level of the metacarpal head dorsum. Useful when the finger base is injured or infected. Inject 3–5 mL between the metacarpal heads on each side of the target digit.
23 Dupuytren Disease
Pathology & Epidemiology
Dupuytren disease is a fibroproliferative disorder of the palmar fascia leading to progressive flexion contracture of the fingers. It arises from myofibroblast proliferation within the palmar and digital fascia. Most commonly affects the ring and small fingers. Prevalence: highest in Northern European descent (Viking disease); male-to-female ratio 7:1; associated with diabetes, epilepsy (phenytoin), alcoholism, and HIV. Dupuytren diathesis (aggressive disease) is characterized by: early onset (<50 years), bilateral disease, ectopic disease (Garrod's pads — knuckle pads, Ledderhose disease — plantar fibromatosis, Peyronie disease — penile fibromatosis), positive family history, and male sex.
Anatomy of Disease
Key pathological structures: pretendinous cord (from palmar aponeurosis), central cord (causes MCP contracture), spiral cord (most dangerous — displaces the neurovascular bundle centrally, superficially, and proximally, placing it at risk during surgery), natatory cord (in web space, causes abduction contracture), lateral cord and retrovascular cord (cause PIP contracture).
Tubiana Staging
| Stage | Total Flexion Contracture (MCP + PIP + DIP) |
|---|---|
| 0 | No disease |
| N | Palmar nodule, no contracture |
| I | 0–45° |
| II | 45–90° |
| III | 90–135° |
| IV | >135° |
Treatment
Indications for intervention: MCP contracture ≥30° (positive "table-top test" — cannot place palm flat on table) or any PIP contracture. Treatment options:
Needle aponeurotomy (percutaneous fasciotomy): Office-based procedure using a needle to perforate and weaken the cord, then manipulate the finger to rupture it. Best for isolated MCP contracture with palpable cord. Recurrence rate: 50–65% at 3–5 years. Lowest complication rate of all options.
Collagenase injection (Xiaflex — collagenase clostridium histolyticum): 0.58 mg injected directly into the cord. Finger manipulation 24–72 hours later to rupture the enzymatically weakened cord. Efficacy: 64–92% achieve <5° residual contracture for MCP joints (less effective for PIP: 28–50%). Recurrence: 35–50% at 5 years. Complications: skin tear (10–15%), swelling, ecchymosis, rare tendon rupture (0.3%). PMID: 19726763
Limited (selective) fasciectomy: Surgical excision of diseased fascia. Most common surgical treatment. Recurrence rate: 20–40% at 5 years. Can address both MCP and PIP contractures. Complication rate: 17–19% (digital nerve injury, skin necrosis, hematoma, infection, CRPS).
Dermofasciectomy: Excision of diseased fascia and overlying skin with full-thickness skin graft (usually from medial arm or groin). Lowest recurrence rate (~8–12% at 5 years). Reserved for recurrent disease or Dupuytren diathesis patients.
24 Hand Infections
Felon
Closed-space infection of the fingertip pulp. The septae of the pulp create a confined compartment — infection causes intense pressure and pain, risking osteomyelitis of the distal phalanx. Treatment: incision and drainage (unilateral longitudinal approach or "fish-mouth" incision — avoid the midline volar pad to prevent a painful scar). Antibiotics covering staphylococci (cephalexin or dicloxacillin).
Paronychia
Infection of the lateral nail fold (acute = bacterial; chronic = Candida). Acute treatment: if no abscess, warm soaks + oral antibiotics. If abscess present: elevate the eponychial fold with a #11 blade or #15 blade (no hemostat — avoid damage to the nail matrix). If subungual component: partial nail removal. Chronic paronychia: topical antifungals, marsupialization of the eponychial fold.
Flexor Tenosynovitis
A Emergency surgical emergency. Infection within the flexor tendon sheath. Diagnosed by Kanavel's signs (all four should be present, though sensitivity is 91.4% with at least one sign):
- Fusiform (sausage-shaped) swelling of the entire finger
- Flexed posture of the involved digit
- Tenderness along the entire flexor sheath
- Pain with passive extension of the finger (most sensitive and specific sign)
Treatment: IV antibiotics (ampicillin-sulbactam or cefazolin + metronidazole) and urgent surgical irrigation. Closed catheter irrigation: make incisions at the A1 pulley and distal to the A5 pulley, place a 5-Fr pediatric feeding tube antegrade, irrigate with saline until clear. If fulminant or late presentation: open drainage (midaxial or Bruner zigzag approach) with debridement. Untreated, infection destroys the tendon and may spread to deep spaces.
The radial and ulnar bursae are continuous with the flexor sheaths of the thumb and small finger, respectively. "Horseshoe abscess" = infection spreading from the thumb (radial bursa) across the Parona space (potential space anterior to pronator quadratus in the distal forearm between the flexor tendons and pronator quadratus) to the small finger (ulnar bursa), or vice versa.
Deep Space Infections
Thenar space: Between the adductor pollicis and first palmar interosseous. Infected thumb or index finger web space. Treatment: I&D through dorsal first web space approach. Midpalmar space: Deep to the flexor tendons, superficial to the metacarpals (3rd, 4th, 5th). Infected long, ring, or small finger. Treatment: I&D through palmar incision between thenar and hypothenar creases. Parona space: Distal forearm, between FDP and pronator quadratus. Involved in horseshoe abscess.
Bite Wounds
| Bite Type | Key Organism | Antibiotic | Notes |
|---|---|---|---|
| Human (fight bite) | Eikenella corrodens | Ampicillin-sulbactam or amoxicillin-clavulanate | Eikenella is resistant to 1st-gen cephalosporins and clindamycin |
| Cat | Pasteurella multocida | Amoxicillin-clavulanate | Deep puncture wounds; high infection rate (~80%); Pasteurella resistant to dicloxacillin |
| Dog | Pasteurella, Capnocytophaga | Amoxicillin-clavulanate | Lower infection rate than cat bites; Capnocytophaga can cause fulminant sepsis in asplenic patients |
Herpetic Whitlow
HSV-1 or HSV-2 infection of the finger. Presents with vesicles containing clear fluid, burning pain. Do NOT incise — surgical drainage worsens infection and risks bacterial superinfection and systemic dissemination. Treatment: self-limited (2–3 weeks); acyclovir or valacyclovir may shorten the course if started early. Recurrence in 20–50%. Differentiate from felon (which has purulent drainage and tense pulp).
25 Replantation & Ring Avulsion
Indications for Replantation
General indications (absolute): thumb (most important digit for hand function), multiple digits, pediatric patients (excellent regenerative capacity), sharp amputation (clean injury, best success), wrist/forearm level. Relative indications: single digit distal to FDS insertion, ring finger avulsion (assess individually).
Contraindications: severe crush or avulsion mechanism, multilevel injury, prolonged warm ischemia (>12 hours for digits, >6 hours for proximal amputations with muscle), significant comorbidities (uncontrolled diabetes, heavy smoking), single finger proximal to the FDS insertion in an adult (causes PIP stiffness and impairs overall hand function), mangled/severely contaminated parts.
Ischemia times: digits (no muscle) — up to 12 hours warm, 24 hours cold; proximal amputations (containing muscle) — up to 6 hours warm, 12 hours cold. Cooling prolongs viability dramatically. Transport the amputated part wrapped in saline-moistened gauze inside a sealed bag, placed on ice (NOT in direct contact with ice).
Structure of Repair
Sequence of replantation (mnemonic: "BEFANV" or bone-extensor-flexor-artery-nerve-vein):
- Bone — shorten to allow tension-free repair; K-wire or plate fixation
- Extensor tendon — repair (may be done before bone)
- Flexor tendon — repair
- Arteries — repair at least one (two preferred in thumb); vein graft if needed
- Nerves — repair both digital nerves
- Veins — repair at least two veins per artery (2:1 vein-to-artery ratio) to prevent venous congestion
Ring Avulsion Injuries (Urbaniak Classification)
| Class | Description | Treatment |
|---|---|---|
| I | Circulation adequate; standard soft tissue injury | Standard wound care; treat skeletal and tendon injuries |
| II | Circulation inadequate; vessel repair required | Revascularization with vein grafts (attempt to preserve finger) |
| III | Complete degloving or amputation | Replantation (if appropriate candidate) or revision amputation; consider ray resection for optimal hand function |
Postoperative Monitoring & Management
Monitor replanted digits hourly for 72 hours: color, turgor, capillary refill, temperature (should be >30°C; <2°C difference from adjacent digits). Pulse oximetry on replanted digit (waveform more important than number). Arterial insufficiency: pale, cool, absent cap refill — return to OR for exploration. Venous congestion: blue/purple, turgid, brisk cap refill <1 second, dark blood on pin-prick — treatment: release sutures, leech therapy (medicinal leeches — Hirudo medicinalis; requires prophylactic ciprofloxacin to prevent Aeromonas hydrophila infection), pin-prick bleeding, or return to OR for vein repair.
Replantation Success Rates & Outcomes
Overall survival rates for replanted digits range from 80–90% for sharp amputations to 50–70% for crush/avulsion injuries. Thumb replantation survival exceeds 90% in experienced centers. Functional outcomes are measured by TAM (total active motion), grip/pinch strength, and sensory recovery (2PD). Most patients achieve S3+ sensory recovery (2PD 7–15 mm) and good functional use. Cold intolerance affects 60–80% of patients and is the most common long-term complaint. Return to work: 70–80% of patients return to their previous occupation.
Key prognostic factors: mechanism (sharp > crush > avulsion), ischemia time, patient age (children do best), smoking status (smoking doubles the failure rate), level of injury (more distal injuries have better outcomes), and surgeon experience (high-volume centers have significantly better outcomes). PMID: 11050200
26 Vascular Conditions of the Hand
Hypothenar Hammer Syndrome
Thrombosis or aneurysm of the ulnar artery at the hook of hamate due to repetitive blunt trauma to the hypothenar eminence (mechanics, carpenters, cyclists). The ulnar artery is vulnerable as it crosses superficial to the hook of hamate. Presentation: digital ischemia (ring and small fingers), cold intolerance, Raynaud-like color changes, Allen test positive for ulnar artery occlusion. Diagnosis: CT angiography or conventional angiography. Treatment: smoking cessation, calcium channel blockers (nifedipine 30–60 mg/day), antiplatelet therapy. Surgical: resection of thrombosed/aneurysmal segment with vein graft interposition, or arterial ligation if Allen test confirms adequate radial dominance.
Digital Ischemia
Differential diagnosis: thromboembolism (cardiac source, aneurysm), vasospasm (Raynaud), vasculitis (scleroderma, SLE, Buerger disease), trauma. Workup: Allen test, Doppler, CT angiography, hypercoagulability panel, ANA/ESR. Treatment depends on etiology: anticoagulation for thromboembolic, vasodilators (CCB, nitroglycerin paste) for vasospasm, immunosuppression for vasculitis.
Raynaud Phenomenon in the Hand
Episodic vasospasm of digital arteries producing white (vasoconstriction) → blue (cyanosis) → red (reperfusion) color changes. Primary Raynaud: young women, bilateral, symmetric, no tissue loss. Secondary Raynaud: associated with connective tissue disease (scleroderma most common), may cause digital ulceration and gangrene. Treatment: avoidance of cold, smoking cessation, calcium channel blockers (nifedipine), topical nitroglycerin, phosphodiesterase inhibitors (sildenafil). Severe refractory cases: botulinum toxin injection around digital arteries, digital sympathectomy (periarterial stripping).
Complex Regional Pain Syndrome (CRPS)
CRPS Type I (reflex sympathetic dystrophy) occurs without identifiable nerve injury. CRPS Type II (causalgia) occurs with identifiable nerve injury. Diagnosis requires the Budapest criteria: (1) continuing pain disproportionate to inciting event; (2) at least one sign in ≥2 of 4 categories; (3) at least one symptom in ≥3 of 4 categories (sensory, vasomotor, sudomotor/edema, motor/trophic); (4) no alternative diagnosis. Common after distal radius fracture (7–37% incidence), Colles fracture, and carpal tunnel surgery.
Treatment: aggressive hand therapy (the cornerstone of treatment), mirror therapy, stress loading (scrubbing and carrying), desensitization. Pharmacologic: gabapentin/pregabalin, corticosteroids (early, short course: prednisone 30 mg/day tapering over 2–3 weeks), vitamin C 500 mg/day for prevention (reduces CRPS incidence after distal radius fracture by 50%). Interventional: stellate ganglion block, IV regional anesthesia (Bier block with lidocaine ± bretylium). PMID: 17995489
27 Hand Tumors
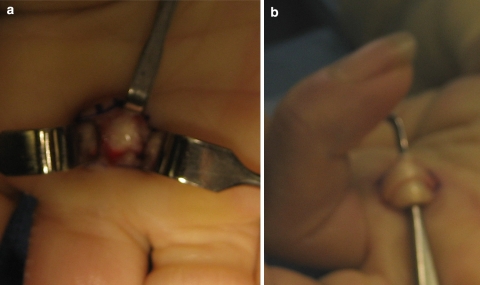
Ganglion Cyst
The most common mass in the hand (60–70% of all hand tumors). Mucin-filled cyst arising from a joint capsule or tendon sheath. Most common location: dorsal wrist (60–70%, arising from the scapholunate ligament). Second most common: volar wrist (18–20%, arising from the radiocarpal or scaphotrapezial joint, near the radial artery). Treatment: observation (up to 50% resolve spontaneously), aspiration (50–70% recurrence), surgical excision (5–10% recurrence; must excise the stalk and cuff of capsule). Mucous cyst: ganglion cyst of the DIP joint; often associated with osteophyte and Heberden's node; may cause nail ridging; excise with osteophyte to reduce recurrence.
Giant Cell Tumor of Tendon Sheath (GCTTS)
The most common solid tumor of the hand (second most common hand tumor overall). Also called pigmented villonodular synovitis (PVNS) of the tendon sheath. Presents as a firm, painless, slow-growing nodule on the volar surface of the finger. Yellow-brown color on gross examination (hemosiderin deposition). Recurrence rate after marginal excision: 9–44% (related to completeness of excision and satellite nodules). Treatment: marginal excision. MRI is useful for surgical planning.
Enchondroma
The most common primary bone tumor of the hand. Benign cartilaginous tumor, most commonly in the proximal phalanges. Often discovered incidentally on radiograph (well-defined lytic lesion with stippled calcifications, endosteal scalloping) or after pathologic fracture. Treatment: observation if asymptomatic; if pathologic fracture, allow fracture to heal (6–8 weeks), then curettage and bone grafting. Malignant transformation is exceedingly rare in the hand (<1%). Ollier disease: multiple enchondromas (non-hereditary); Maffucci syndrome: multiple enchondromas + soft tissue hemangiomas (higher malignant transformation risk — up to 25%).
Glomus Tumor
Benign vascular tumor arising from the glomus body (temperature-regulating arteriovenous shunt). Classic triad: (1) severe paroxysmal pain (out of proportion to size), (2) point tenderness (Love's test — apply pin pressure to fingertip), (3) cold intolerance (Hildreth's test — pain relief with tourniquet inflation). Most common location: subungual (75%). MRI shows a 3–7 mm enhancing lesion in the nail bed. Transillumination may reveal a reddish-blue spot. Treatment: surgical excision (subungual approach with nail removal and direct visualization). Recurrence after complete excision is uncommon (<5%).
Epidermal Inclusion Cyst
Second most common soft tissue mass in the hand. Arises from traumatic implantation of epidermis into subcutaneous tissue (history of puncture wound or laceration in ~50%). Typically on the volar surface of the fingers. Firm, non-tender, non-transilluminant (distinguishes from ganglion). Contains cheesy keratin material. Treatment: marginal excision including the cyst wall. Recurrence is common if the wall is not completely excised.
Soft Tissue Sarcoma of the Hand
Rare (<5% of hand tumors). Epithelioid sarcoma is the most common primary soft tissue sarcoma of the hand and wrist in young adults. Presents as a painless, firm nodule on the volar hand or wrist, often misdiagnosed as a ganglion cyst or Dupuytren nodule. Key: any solid, firm mass in the hand that is not a classic ganglion or GCTTS should be imaged (MRI with gadolinium) and biopsied before excision. Treatment: wide excision with tumor-free margins; sentinel lymph node biopsy (epithelioid sarcoma has higher lymph node metastasis rate than other sarcomas — 16–48%). PMID: 16294088
28 Congenital Hand Differences
Swanson Classification (Modified IFSSH)
| Category | Examples |
|---|---|
| I. Failure of formation | Radial longitudinal deficiency (radial club hand), transverse deficiency (congenital amputation), phocomelia |
| II. Failure of differentiation | Syndactyly, symphalangism, radioulnar synostosis, camptodactyly, clinodactyly, trigger thumb |
| III. Duplication | Polydactyly (preaxial = thumb, postaxial = small finger) |
| IV. Overgrowth | Macrodactyly |
| V. Undergrowth | Thumb hypoplasia (Blauth classification), brachydactyly |
| VI. Constriction band syndrome | Amniotic band syndrome |
| VII. Generalized skeletal abnormalities | Apert syndrome, Marfan syndrome, achondroplasia |
Syndactyly
Failure of separation of the digits. Most common congenital hand anomaly. Types: simple (skin/soft tissue only) vs complex (bony connection); complete (extends to fingertip) vs incomplete (does not reach fingertip). Most commonly involves the long-ring web space. Treatment: surgical separation typically at 12–18 months. If border digits are involved (thumb-index or ring-small with size discrepancy), operate earlier (6 months) to prevent growth tethering. Technique: interdigitating flaps with full-thickness skin grafting of deficient areas. Never release both sides of a digit simultaneously (risk of vascular compromise).
Polydactyly
Preaxial (radial/thumb) polydactyly: Wassel classification (types I–VII based on level of duplication). Type IV (duplicated proximal phalanx) is most common. Treatment: reconstruct one functional thumb from the duplicated components (not simply amputating the smaller thumb). Usually performed at 1–2 years. Postaxial (ulnar) polydactyly: More common in African American children. Type A (well-formed digit) = surgical excision. Type B (pedunculated nubbin) = suture ligation in the nursery or surgical excision.
Thumb Hypoplasia (Blauth Classification)
| Type | Description | Treatment |
|---|---|---|
| I | Minor hypoplasia (small but functional thumb) | Observation; may need augmentation |
| II | Adducted 1st web space, UCL insufficiency, thenar hypoplasia | 1st web deepening, UCL reconstruction, opponensplasty (Huber) |
| IIIA | Above + stable CMC joint, extrinsic tendon abnormalities | Reconstruction (as type II + tendon transfers) |
| IIIB | Above + unstable or deficient CMC joint | Pollicization (index finger transfer to thumb position) |
| IV | "Pouce flottant" (floating thumb) — attached by skin bridge only | Pollicization |
| V | Aplasia (absent thumb) | Pollicization |
Pollicization: Transfer of the index finger to the thumb position with neurovascular pedicle intact. The index metacarpal is shortened and repositioned in opposition; the interossei are rebalanced to act as thenar muscles. Best performed at 6–12 months of age for types IIIB–V. Excellent functional outcomes with grip and pinch adapted from childhood.
Radial Longitudinal Deficiency (Radial Club Hand)
Spectrum of hypoplasia/aplasia of structures on the radial side of the forearm and hand (radius, scaphoid, trapezium, thumb). Associated with systemic conditions: VACTERL, Holt-Oram syndrome (cardiac + radial deficiency), Fanconi anemia (must obtain CBC and chromosomal breakage study before any surgery), TAR syndrome (thrombocytopenia-absent radius). Treatment: serial stretching and splinting in infancy, centralization/radialization of the carpus on the ulna at 6–12 months, pollicization if thumb absent/deficient.
29 Classification Systems
Fracture & Injury Classifications
| Classification | Condition | Key Feature |
|---|---|---|
| Frykman (I–VIII) | Distal radius fractures | Joint involvement (radiocarpal, DRUJ) ± ulnar styloid fracture |
| AO/OTA (A, B, C) | Distal radius fractures | A = extra-articular, B = partial articular, C = complete articular |
| Herbert (A–D) | Scaphoid fractures | A = stable, B = unstable, C = delayed union, D = nonunion |
| Mayfield (I–IV) | Perilunate injuries | Progressive perilunar instability from SL to lunate dislocation |
| Eaton-Littler (I–IV) | Thumb CMC arthritis | Progressive joint space narrowing and subluxation |
| Leddy-Packer (I–III) | Jersey finger | Level of FDP retraction and vinculum status |
| Doyle (I–IV) | Mallet finger | Closed vs open; with or without bony avulsion/subluxation |
| Gustilo-Anderson (I–IIIC) | Open fractures | I = <1 cm; II = 1–10 cm; IIIA = adequate soft tissue; IIIB = requires flap; IIIC = vascular injury |
| Urbaniak (I–III) | Ring avulsion injuries | I = adequate circulation; II = inadequate circulation; III = complete degloving/amputation |
Nerve & Soft Tissue Classifications
| Classification | Condition | Key Feature |
|---|---|---|
| Seddon (3 types) | Nerve injury | Neurapraxia, axonotmesis, neurotmesis |
| Sunderland (I–V) | Nerve injury | Graded by structural layer involved (myelin → entire nerve) |
| Mackinnon (VI) | Nerve injury (addition to Sunderland) | Mixed injury pattern within same nerve |
| McGowan (I–III) | Cubital tunnel syndrome | Mild → severe based on sensory/motor deficit and wasting |
| Palmer (1A–1D, 2A–2E) | TFCC tears | Class 1 = traumatic, Class 2 = degenerative |
| Tubiana (N, I–IV) | Dupuytren disease | Total flexion contracture in degrees |
| Green (I–IV) | Trigger finger | Pain → catching → locking → fixed contracture |
| Blauth (I–V) | Thumb hypoplasia | Minor hypoplasia → aplasia; determines reconstruction vs pollicization |
| Wassel (I–VII) | Thumb polydactyly | Level of duplication (distal phalanx to metacarpal) |
30 Medications Master Table
Antibiotics for Hand Infections
| Indication | First-Line | Alternative | Notes |
|---|---|---|---|
| Simple skin infection (felon, paronychia) | Cephalexin 500 mg PO QID | Dicloxacillin 500 mg PO QID | Cover staphylococci; add TMP-SMX for MRSA risk |
| Flexor tenosynovitis | Ampicillin-sulbactam 3 g IV q6h | Cefazolin 2 g IV q8h + metronidazole 500 mg IV q8h | Broad coverage; surgical I&D is definitive |
| Human bite (fight bite) | Amoxicillin-clavulanate 875/125 mg PO BID | Ampicillin-sulbactam 3 g IV q6h | Must cover Eikenella (resistant to 1st-gen ceph, clindamycin) |
| Cat/dog bite | Amoxicillin-clavulanate 875/125 mg PO BID | Doxycycline 100 mg PO BID (PCN allergy) | Pasteurella resistant to dicloxacillin and 1st-gen ceph |
| Leech therapy (Aeromonas prophylaxis) | Ciprofloxacin 500 mg PO BID | TMP-SMX DS PO BID | Continue for duration of leech therapy |
| Osteomyelitis | Nafcillin 2 g IV q4h (MSSA) or vancomycin 15–20 mg/kg IV q12h (MRSA) | Ceftriaxone 2 g IV q24h (if gram-negative suspected) | 6 weeks IV; culture-guided therapy |
Local Anesthetics for Digital Block
| Agent | Concentration | Onset | Duration | Max Dose |
|---|---|---|---|---|
| Lidocaine (without epi) | 1–2% | 2–5 min | 1–2 hours | 4.5 mg/kg |
| Lidocaine (with epi) | 1–2% | 2–5 min | 2–4 hours | 7 mg/kg (epi is safe in digits) |
| Bupivacaine (without epi) | 0.25–0.5% | 5–10 min | 4–8 hours | 2.5 mg/kg |
| Ropivacaine | 0.5–0.75% | 5–15 min | 4–8 hours | 3 mg/kg |
Other Key Medications
| Drug | Dose | Indication in Hand Surgery |
|---|---|---|
| Collagenase clostridium histolyticum (Xiaflex) | 0.58 mg intralesional | Dupuytren contracture (inject into cord) |
| Triamcinolone acetonide | 10–40 mg/mL (0.5–1 mL) | Trigger finger injection, De Quervain injection, CTS injection |
| Methylprednisolone acetate | 40–80 mg | Carpal tunnel injection |
| Nifedipine | 30–60 mg PO daily (extended-release) | Raynaud phenomenon, digital vasospasm |
| Aspirin | 81–325 mg PO daily | Post-replantation/revascularization antiplatelet therapy |
| Heparin (unfractionated) | Protocol-dependent (drip or subcutaneous) | Post-replantation/revascularization anticoagulation |
| Dexamethasone | 4–10 mg IV/PO | Perioperative anti-inflammatory; nerve decompression adjunct |
| Gabapentin | 300–1200 mg PO TID | Neuropathic pain; CRPS adjunct |
| Acyclovir | 400 mg PO TID × 7–10 days | Herpetic whitlow |
31 Imaging & Diagnostics
Radiographic Views
| View | Technique | Best For |
|---|---|---|
| PA (posteroanterior) | Standard; shoulder abducted 90°, elbow flexed 90° | SL interval, Gilula's arcs, carpal alignment, ulnar variance |
| Lateral | True lateral with ulna and radius superimposed | Volar/dorsal tilt (distal radius), SL angle, carpal alignment (DISI/VISI), perilunate injuries |
| Oblique | 45° pronated | Metacarpal fractures, CMC joints, pisiform/triquetral fractures |
| Scaphoid view | PA with ulnar deviation + fist clenching | Scaphoid fractures (elongates the scaphoid), SL widening |
| Carpal tunnel view | Wrist hyperextended, beam tangential | Hook of hamate fracture, carpal tunnel bony anatomy |
| Roberts view | Thumb CMC: pronated AP with beam perpendicular to thumbnail | 1st CMC arthritis, Bennett/Rolando fractures |
| Brewerton view | MCP flexed 65°, beam 15° ulnar-to-radial | MCP joint erosions (RA), metacarpal head pathology |
Advanced Imaging
MRI: Gold standard for occult scaphoid fractures (sensitivity 100% after 24h), TFCC tears, scapholunate ligament assessment, Kienböck disease staging, soft tissue tumors, and carpal tunnel syndrome (increased signal in median nerve, bowing of flexor retinaculum). 1.5T or 3T with dedicated wrist coil. Gadolinium enhancement useful for tumors and AVN assessment.
CT scan: Best for fracture characterization (comminution, articular step-off, displacement), scaphoid nonunion assessment, distal radius fracture surgical planning, hook of hamate fracture. CT arthrography: useful for TFCC and intercarpal ligament tears.
Ultrasound: Dynamic assessment of tendon pathology (trigger finger, De Quervain), ganglion cysts, guided injections. Advantages: no radiation, real-time, low cost. Operator-dependent. Increasingly used for CTS diagnosis (cross-sectional area of median nerve at the carpal tunnel inlet >10–12 mm² is suggestive).
Electrodiagnostic Studies (EMG/NCS)
Nerve conduction studies (NCS): Measure conduction velocity and amplitude of motor and sensory nerves. Key for CTS (see Section 17), cubital tunnel syndrome (ulnar motor NCV across the elbow <50 m/s, or >10 m/s drop across the elbow), and differentiating radiculopathy from peripheral neuropathy. Electromyography (EMG): Needle examination of muscles for denervation (fibrillations, positive sharp waves) and reinnervation (polyphasic potentials). Timing: denervation potentials take 3–4 weeks to develop after nerve injury; EMG performed too early may be falsely normal.
32 Abbreviations Master List
| Abbreviation | Full Term |
|---|---|
| ADM | Abductor digiti minimi |
| AIN | Anterior interosseous nerve |
| APB | Abductor pollicis brevis |
| APL | Abductor pollicis longus |
| AVN | Avascular necrosis |
| CMC | Carpometacarpal |
| CRPS | Complex regional pain syndrome |
| CTR | Carpal tunnel release |
| CTS | Carpal tunnel syndrome |
| DIP | Distal interphalangeal |
| DISI | Dorsal intercalated segment instability |
| DML | Distal motor latency |
| DRUJ | Distal radioulnar joint |
| ECRB | Extensor carpi radialis brevis |
| ECRL | Extensor carpi radialis longus |
| ECU | Extensor carpi ulnaris |
| EDC | Extensor digitorum communis |
| EDM | Extensor digiti minimi |
| EIP | Extensor indicis proprius |
| EMG | Electromyography |
| EPB | Extensor pollicis brevis |
| EPL | Extensor pollicis longus |
| FCR | Flexor carpi radialis |
| FCU | Flexor carpi ulnaris |
| FDP | Flexor digitorum profundus |
| FDS | Flexor digitorum superficialis |
| FPB | Flexor pollicis brevis |
| FPL | Flexor pollicis longus |
| ICSRA | Intercompartmental supraretinacular artery |
| MC | Metacarpal |
| MCP | Metacarpophalangeal |
| NCS | Nerve conduction studies |
| NCV | Nerve conduction velocity |
| ORIF | Open reduction internal fixation |
| PIN | Posterior interosseous nerve |
| PIP | Proximal interphalangeal |
| PL | Palmaris longus |
| PRC | Proximal row carpectomy |
| PT | Pronator teres |
| SBRN | Superficial branch of radial nerve |
| SL | Scapholunate |
| SLAC | Scapholunate advanced collapse |
| SNAP | Sensory nerve action potential |
| SNAC | Scaphoid nonunion advanced collapse |
| TFCC | Triangular fibrocartilage complex |
| UCL | Ulnar collateral ligament |
| VISI | Volar intercalated segment instability |
| WALANT | Wide awake local anesthesia no tourniquet |
| 2PD | Two-point discrimination |
| 4CF | Four-corner fusion |
33 Key Rehabilitation Protocols
Flexor Tendon Repair (Zone II) Rehabilitation
| Phase | Timeline | Protocol | Key Points |
|---|---|---|---|
| Protective | 0–4 weeks | Dorsal blocking splint (wrist 20–30° flexion, MCP 50–70°, IP joints extended). Early active motion: place-and-hold exercises within splint, tendon gliding exercises | No active flexion against resistance; no passive extension beyond splint limits |
| Early active | 4–6 weeks | Wean from dorsal block splint. Begin gentle active ROM. Composite fist exercises. Differential tendon gliding (hook fist, straight fist, full fist) | Still no resistance; protect from forceful extension |
| Strengthening | 8–12 weeks | Progressive resistive exercises. Putty exercises, grip strengthening. Return to light activities | Full active ROM expected by 8 weeks |
| Return to full activity | 12–16 weeks | Unrestricted activity. Heavy labor and sports | Maximum strength recovery at 6 months |
Distal Radius Fracture (ORIF) Rehabilitation
| Phase | Timeline | Protocol |
|---|---|---|
| Immobilization | 0–2 weeks | Volar splint. Finger ROM (full fist), shoulder/elbow ROM. Edema control (elevation, compressive wrap) |
| Early motion | 2–6 weeks | Remove splint for gentle wrist ROM exercises (flexion, extension, radial/ulnar deviation, pronation/supination). Grip strengthening with putty |
| Progressive strengthening | 6–12 weeks | Progressive resistive exercises. Weight-bearing as tolerated. Dart-throwing motion exercises. Return to light duties |
| Full activity | 12+ weeks | Unrestricted activity based on radiographic healing and clinical exam. Contact sports at 3–4 months |
Carpal Tunnel Release Rehabilitation
| Timeline | Protocol |
|---|---|
| Day 1 | Remove bulky dressing; apply light compressive wrap. Begin finger, thumb, and wrist ROM immediately. Scar management: gentle scar massage starting at 2 weeks |
| 2 weeks | Suture removal. Full wrist ROM. Light grip activities. Scar desensitization. Nerve gliding exercises |
| 4–6 weeks | Progressive strengthening. Return to full duties (light work by 2–3 weeks, heavy labor by 4–6 weeks for open CTR; ~1 week earlier for endoscopic) |
| 3–6 months | Pillar pain gradually resolves. Grip strength returns to baseline by 3 months. Sensory recovery continues for up to 12 months |
Mallet Finger Splinting Protocol
| Phase | Duration | Protocol |
|---|---|---|
| Full-time splinting | 0–6 weeks (tendinous) or 0–8 weeks (bony) | Continuous DIP extension splint (Stack splint or custom thermoplastic). Do NOT allow any DIP flexion — if splint removed for skin care, support the DIP in extension. PIP and MCP must remain free for full ROM |
| Weaning | 6–10 weeks | Night splinting only. Gentle active DIP flexion during the day. If extensor lag develops or recurs, return to full-time splinting for 6 more weeks |
| Discontinue splint | 10–12 weeks | Discontinue splint when no extensor lag with active extension. Expect slight residual lag (5–10°) in many patients — this is acceptable |
Dupuytren Fasciectomy / Collagenase Rehabilitation
| Timeline | Protocol |
|---|---|
| 0–2 weeks | Light dressing, hand elevation. Begin active finger ROM immediately. Extension splint at night |
| 2–6 weeks | Scar management (silicone, massage). Progressive grip strengthening. Night extension splinting continues |
| 6 weeks – 6 months | Continue night splinting (reduces recurrence). Full activities. Monitor for recurrence at follow-up visits |
Scaphoid Fracture (Cast) Rehabilitation
| Phase | Duration | Protocol |
|---|---|---|
| Immobilization | 0–8 weeks (waist) or 0–12 weeks (proximal pole) | Thumb spica cast. Maintain shoulder, elbow, and uninvolved finger ROM. Edema control |
| Early mobilization | Cast removal to 12 weeks | Gentle active wrist and thumb ROM. Scar management. Grip strengthening with putty (begin at 8 weeks post-cast removal) |
| Progressive strengthening | 12–16 weeks | Progressive resistance. Dart-throwing motion exercises. Sport-specific training |
| Return to full activity | 16–20 weeks (cast); 8–12 weeks (screw fixation) | Unrestricted activity when radiographic union confirmed and painless grip |
Cubital Tunnel Surgery Rehabilitation
| Timeline | Protocol |
|---|---|
| 0–2 weeks | Posterior splint at 45° elbow flexion (in situ) or 90° (transposition). Gentle finger ROM to prevent stiffness |
| 2–4 weeks | Begin active elbow ROM (avoid full extension for transposition patients until 4 weeks). Nerve gliding exercises: ulnar nerve glide (elbow extension + wrist extension + finger extension) |
| 4–8 weeks | Full ROM. Begin grip strengthening. Intrinsic muscle strengthening exercises (finger abduction/adduction against rubber bands) |
| 8–12 weeks | Progressive return to activities. Full recovery expected by 3–6 months for motor function; sensory recovery may continue for 12–18 months |
Tendon Transfer Rehabilitation
| Phase | Duration | Protocol |
|---|---|---|
| Immobilization | 0–4 weeks | Protective splint positioning the transferred tendon in slack (relaxed position). No active use of the transfer |
| Active motion | 4–6 weeks | Begin active use of the transfer within a protective splint. Re-education exercises: initially activate the donor muscle function (synergistic motion), then transition to the new function |
| Strengthening | 6–8 weeks | Progressive resistance. Remove protective splint. Biofeedback and EMG-guided re-training if needed |
| Integration | 8–12 weeks | Functional tasks. Independent use of transfer without conscious activation (automaticity). Full activities by 3–4 months |